A ccepting failure is tricky, and more so when it’s not due to your own failings but a result of circumstances beyond your control—or, indeed, a pandemic. We will, in time, move beyond continually reporting on covid-19 cases and deaths, to a future where we start talking about vaccines, recovering services, and trying to regain a degree of normality. And healthcare staff will need to appreciate that, in some areas, we may indeed have “failed” as a result of factors outside our control. The world was caught on the back foot by this pandemic, despite the warnings that one was due. It’s been a once in a lifetime event with global ramifications, the likes of which we’ve never seen and hopefully won’t again. Healthcare systems have been flummoxed by the challenges of prioritisation—and the sinking realisation of the scale of wider harm when care has had to be stopped or scaled down. The problem for those of us who work in the NHS, of course, is that we have to accept that the service is capable of failing. My own view is that it does fail at times, as any system does, and when someone points this out it doesn’t necessarily constitute a personal slight or an attack on the NHS’s founding principles. The NHS is amazing, but it can’t be everything for everyone all of the time. Part of acknowledging and accepting failure is to appreciate that we did the best we could. Great care has been provided to covid patients and others during this pandemic, but NHS care, with finite resources and staff, has almost certainly suffered in other areas. That harm isn’t anyone’s fault, but we do need to accept that it may have occurred. The next step is to start looking at data to understand the impact of any harm caused. Using the example of diabetes, we need to ask what impact the change in services has had in the short and long term. The chronic nature of the pathology of diabetes means that some of the impact will take time to emerge, while some should already be identifiable. Have amputation rates changed? Have more eye problems emerged? Are admissions up? Has lockdown made things look different? Different specialties will need to examine different issues around the impact on their patients, but all areas will need to look at questions like those. The answers we get back may be interesting, even unpalatable, but we mustn’t shy away from asking. As we start to look ahead to a world recovering from covid, the time is ripe to begin examining datasets and asking those questions. Clinicians will be the ones who have to pick up the pieces, as well as working out how to focus our efforts accordingly. Owning the problem is key, as is having data to highlight the problems and make the case for focus on relevant areas. The question is whether we, as clinicians, can start by accepting the failures—after which will come the gargantuan task of leading on interventions to tackle them. Partha Kar, consultant in diabetes and endocrinology , Portsmouth Hospitals NHS Trust [email protected] Twitter @parthaskar Cite this as: BMJ 2020;371:m4304 comment comment the bmj | 14 November 2020 275 The harm isn’t anyone’s fault, but we do need to accept that it may have occurred THE BOTTOM LINE Partha Kar Learning to live with failure ”The hospital transmission study shows we all have to be more vigilant” DAVID OLIVER “It’s hard not to be angry—but that isn’t good for our mental health either” HELEN SALISBURY PLUS Benefits of pooled testing; second wave pinch points for the NHS

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Accepting failure is tricky, and more so when it’s not due to your own failings but a result of circumstances beyond your control—or, indeed, a pandemic.
We will, in time, move beyond continually reporting on covid-19 cases and deaths, to a future where we start talking about vaccines, recovering services, and trying to regain a degree of normality. And healthcare staff will need to appreciate that, in some areas, we may indeed have “failed” as a result of factors outside our control.
The world was caught on the back foot by this pandemic, despite the warnings that one was due. It’s been a once in a lifetime event with global ramifi cations, the likes of which we’ve never seen and hopefully won’t again. Healthcare systems have been fl ummoxed by the challenges of prioritisation—and the sinking realisation of the scale of wider harm when care has had to be stopped or scaled down.
The problem for those of us who work in the NHS, of course, is that we have to accept that the service is capable of failing. My own view is that it does fail at times, as any system does, and when someone points this out it doesn’t necessarily constitute a personal slight or an attack on the NHS’s founding principles.
The NHS is amazing, but it can’t be everything for everyone all of the time. Part of acknowledging and accepting failure is to appreciate that we did the best we could. Great care has been provided to covid patients and others during this pandemic, but NHS care, with fi nite resources and staff , has almost certainly suff ered in other areas. That harm isn’t anyone’s fault, but we do need to accept that it may have occurred.
The next step is to start looking at data to understand the impact of any harm caused. Using the example of diabetes, we need to ask what impact the change in services has had in the short and long term. The chronic nature of the pathology of diabetes means that some of the impact will take time to emerge, while some should already be identifi able. Have amputation rates changed? Have more
eye problems emerged? Are admissions up? Has lockdown made things look diff erent?
Diff erent specialties will need to examine diff erent issues around the impact on their patients, but all areas will need to look at questions like those. The answers we get back may be interesting, even unpalatable, but we mustn’t shy away from asking.
As we start to look ahead to a world recovering from covid, the time is ripe to begin examining datasets and asking those questions. Clinicians will be the ones who have to pick up the pieces, as well as working out how to focus our eff orts accordingly. Owning the problem is key, as is having data to highlight the problems and make the case for focus on relevant areas. The question is whether we, as clinicians, can start by accepting the failures—after which will come the gargantuan task of leading on interventions to tackle them. Partha Kar, consultant in diabetes and
endocrinology , Portsmouth Hospitals
NHS Trust [email protected] @parthaskar
Cite this as: BMJ 2020;371:m4304
commentcomment
the bmj | 14 November 2020 275
The harm isn’t anyone’s fault, but we do need to accept that it may have occurred
THE BOTTOM LINE Partha Kar
Learning to live with failure
”The hospital transmission study shows we all have to be more vigilant” DAVID OLIVER “It’s hard not to be angry—but that isn’t good for our mental health either” HELEN SALISBURYPLUS Benefits of pooled testing; second wave pinch points for the NHS

276 14 November 2020 | the bmj
Mass diagnostic testing for infectious disease—whether for surveillance or for targeted screening—is logistically and fi nancially
challenging. This is particularly true when disease prevalence is relatively low and when other unrelated infections present with very similar symptoms. In this kind of scenario, as we have seen for community SARS-CoV-2 testing, the low rate of positivity means a signifi cant outlay of resources, time, and eff ort to identify relatively low numbers of cases.
But this challenge isn’t new, nor is the potential solution. Testing pooled samples, rather than each individual one, was used in the 1990s to identify virus specifi c antibodies in both human and veterinary settings. When used in HIV antibody surveillance studies in a low prevalence setting, testing many pools, each containing fi ve samples, reduced costs by 80%, even with a subsequent confi rmatory test to identify seropositive people.
It was realised that mass testing could also be applied to virus detection. For example, screening of blood donations for common bloodborne viruses could be performed by pooling serum samples, then testing them
directly with polymerase chain reaction tests, albeit with an intermediate concentration step to improve overall sensitivity.
Sample pooling continued to be used widely in veterinary diagnostics for both antibody and direct virus detection, but its use in human medicine declined. So, what parameters need to be considered to ensure reliable diagnostic outputs? And how is pooling achieved?
Pooling size A key consideration in determining optimum pooling size is how much sensitivity decreases as the pool size increases, and this will be determined by the viral load in a positive sample and its prevalence in a background of negative samples. One recent study suggested that pooling up to 30 samples had minimal impact on overall detection rates of SARS-CoV-2, although others have raised concerns that when using large pool sizes it can be diffi cult to to identify individual positives. It might also hide technical defi ciencies, such as insuffi cient sampling, and miss low viral loads. One way to tackle the challenges of identifying individual positives is to perform matrix pool testing—a two way matrix being the most simple option.
In one way pool testing, if a pooled sample tests negative, then all samples within that pool are deemed negative. If a pool tests positive, then its individual samples are repeat tested—either in sequentially reducing pool sizes or as individual samples—to identify which were positive. That's why it is more challenging to identify individual samples. In two way pooling, however, a grid or matrix of samples is formed, and column and row pools are generated and tested. For example, a 10 x 10 matrix of 100 samples could produce 20 pools for testing. Only the samples that lie at the intersections of positive columns and rows then need to be tested to identify the positive ones. An additional advantage of pool testing is the increased positive predictive value resulting from confi rmatory testing.
The challenges faced by pillar 2 swab testing for the wider population show that a new way of thinking is required in our testing strategy to get ahead of virus transmission. Much of our testing capacity is taken up by what is essentially asymptomatic screening,
As England embarks on a second national lockdown, we need to reflect on how our hospitals are “feeling” and what we can hope for over the coming weeks and months.
First, we must recognise that, in acute secondary care, we are in a different place to March and April. Then there was a decrease, often quite dramatic, in the number of people presenting for acute care in the secondary sector. That is not the case now.
As we enter the winter period areas of hospital care are already struggling. In terms of staffing we are in a poor place. The impact of the first wave of the pandemic is still being felt and staff numbers are increasingly being strained by high levels of absence, fed by illness and self-isolation. Most feel that these shortages are incompatible with the usual safe care of elective and emergency patients.
On top of this is the pressure on trusts to meet elective care targets that are frankly impossible to achieve with a worn out workforce and limited beds and diagnostics. As I write, targets with accompanying financial penalties are still in place. Trying to achieve these puts emergency care at risk.
Many wonder whether lockdown 2.0 will help. Admission rates will fall only seven to 10 days after infection rates decline, and referrals to intensive care will change a few days after that. Mortality probably would not change with the time of the lockdown. The other vital question is how the NHS will cope with demand. The most obvious thing would be to relax elective targets. However painful
Pooled sampling would allow rolling surveillance programmes in schools, care homes, universities, and colleges
Relax elective targets: we need to work without unnecessary diversionsWill lockdown 2.0
relieve the immense strain on the NHS?
PERSONAL VIEW Jonathan Ball , Alan McNally
Pooled testing could be the answer to failing strategyThe challenges being faced by the UK's pandemic response show that a new way of thinking is required
BMJ OPINION Nick Scriven

the bmj | 14 November 2020 277
whether it is testing of hospital inpatients and staff , testing in care homes, or lack of triage for members of the public arriving at test centres. At the same time there is no surveillance supporting schools, universities, and businesses.
Pooled sampling of what is essentially asymptomatic swabs would allow rolling surveillance programmes in schools, care homes, universities, and colleges, and high risk factory settings without having a major impact on the daily test capacity. Pooled samples could be tested in dedicated labs, so other labs need not change their protocols. This would allow the UK to improve monitoring of high risk populations, while still having the testing capacity to deal with true symptomatic people. It would also allow testing to be used to follow tracing of cases, something which does not currently drive the test and trace strategy but is essential to destroy transmission chains of SARS-CoV-2. Jonathan Ball , professor of molecular virology ,
University of Nottingham
[email protected] Alan McNally , professor in microbial genomics ,
University of Birmingham
Cite this as: BMJ 2020;371:m4312
this is in the long run, we need all our staff working without unnecessary diversions.
Likewise, we need recognition that junior doctors and others will again have to work beyond their immediate job descriptions, without detriment to their training. In terms of beds, the pinch points will be critical care and advanced respiratory support. I am not certain how reopening Nightingale units will help, as all staff with critical care skills will be needed “at base,” and taking them elsewhere will be a step too far in terms of staffing.
Nosocomial infection is also a major risk. Most years we hear stories of crowding and “corridor care”; this year we have to consider not only the usual risks to safety and dignity but also the risk of covid cross infection.Nick Scriven, immediate past president of the Society
of Acute Medicine
Investigators highlighted staff use of shared computers, desks, and sinks
The Healthcare Safety Investigation Branch recently published its report of a four month study of covid-19 transmission in hospitals.
The fi ndings are complex and nuanced, and its recommendations are many. It has signifi cant implications for staff and patients. Hospital acquired covid infection can’t easily be separated from transmission to, and infection of, patients and colleagues or our ability to access testing or PPE.
In July the Academy of Medical Sciences reported that “at least 10% of all covid-19 infections in England between 26 April and 7 June were among patient facing healthcare workers and resident facing social care workers.” It didn’t give defi nitive data on the percentage of cases transmitted in hospital, noting only limited data sources on infections acquired in hospitals. However, these infections were of particular concern since patients often had comorbid conditions, while staff illness leads to workforce gaps and many staff are at risk of poor covid outcomes.
Last month a major Scottish cohort study in The BMJ showed that patient facing health workers and their immediate families were three times as likely as the general population to be admitted to hospital with covid. Meanwhile, since June in England, the government has published data on covid cases that are “probably acquired in hospital,” with the percentage around 10%.
In this context, the HSIB reviewed the literature on hospital covid transmission and carried out detailed fi eldwork in six acute NHS hospital trusts. Readers won’t
be surprised to learn that the availability of safe, appropriate, fi t tested PPE was a major issue. Another concern was the lack of rapid, regular covid testing for staff .
The HSIB noted the diffi culty in trying to practise optimal infection control by separating streams and ward bases into covid and non-covid areas, as the UK has a low number of beds per 1000 people.
Beyond those perhaps more familiar fi ndings, investigators also identifi ed signifi cant issues with hospital design—not least a lack of ventilation and air circulation and the lack of isolation rooms in many wards. They highlighted the use of shared computer consoles, desks, and sinks. Similar risks were identifi ed from shared patient equipment and the poor uptake of remote patient assessment and review.
Perhaps more concerning is that the investigators, and the families they spoke to, noted many instances of patient facing staff congregating in off -ward areas, such as coff ee rooms, and perhaps being too casual in areas away from the bedside and wearing PPE in more public areas.
So, what do we do about the fi ndings? Hospital design and capacity, the purchase of equipment, and testing and staffi ng levels are not in the gift of shop fl oor clinical staff to solve. However, they do highlight the need for us all to be more vigilant about group meetings, infection control, PPE use, sterilising surfaces,
and avoiding unnecessary patient contact by many professionals .
David Oliver, consultant in geriatrics and
acute general medicine , Berkshire
[email protected] @mancunianmedic
Cite this as: BMJ 2020;371:m4306
ACUTE PERSPECTIVE David Oliver
Heed HSIB on hospital transmission
SOPA
IMAG
ES /G
ETTY
IMAG
ES

278 14 November 2020 | the bmj
England is now in a second lockdown, this time for four weeks. Some patients with the virus in our local hospital require ventilation,
but at much lower numbers than reported in the north of England. At our surgery we’re bracing for the new wave of coronavirus patients, but it hasn’t yet arrived—perhaps because most of the recent cases are in young people, many of them students who have limited interactions with vulnerable adults.
I have no illusions that this will be anything other than a brief reprieve. Meanwhile, our mental health workload is growing. Patients are increasingly anxious—about their own health, or that of their relatives—and their fears are mostly well founded.
Many people are struggling to fi nd work and are worried about rent and food bills; others are fi nding working from home particularly stressful. Apart from fulfi lling the obvious need for an income, work provides conversation with colleagues and a change of scene. If all of your social interactions are done by computer and your commute is from the bedroom to the kitchen table, many of the pleasures of working life have gone.
Patients tell me about the impossibility of switching off , having lost the spatial separation of work and home. They also report huge anxiety about job security, being afraid to take any breaks in case
the boss should ring and fi nd that they are not at their desk.
Some of their stress and anxiety rubs off on me: partly, this is worry about the developing pandemic and the discomfort of maintaining the brace position for weeks at a time. More immediately, however, it’s the sinking feeling in response to “mental health crisis” as the reason for a call when I’m the duty doctor. If I’m to do this well it will take time, while more calls of variable urgency stack up (baby won’t feed, chest pain, swollen knee). It’s also because I question how much I can help. Pills are unlikely to be the answer, and although I can direct patients to the self-referral site for psychological therapy, they won’t receive immediate support. What I can off er is listening, reassurance, and sometimes certifi ed time away from work if patients aren’t well enough to continue.
Adding to our stress is the knowledge that we’re in our dire position not because of the unavoidable nature of this virus but because of poor leadership and worse decision making. Looking to the East, to countries that have handled this pandemic better, with so much less loss of life and livelihood, it’s hard not to be angry—but that isn’t good for our mental health either. So, I try to smile behind my mask and to
spread good cheer where I can . Helen Salisbury , GP, Oxford
[email protected] Twitter @HelenRSalisbury
Cite this as: BMJ 2020;371:m4276
Listen and subscribe to The BMJ podcast on Apple Podcasts, Spotify, and other major podcast apps
Edited by Kelly Brendel, deputy digital content editor, The BMJ
We’re in our dire position because of poor leadership and worse decision making
Making the lockdown work The BMJ’s editor in chief, Fiona Godlee, takes stock of the latest lockdown in England with clinicians from primary care, secondary care, and public health. Here Matt Morgan, a columnist for The BMJ and intensive care doctor, talks about the difficulty of communicating with the public about the risks of covid-19:
“It’s unfortunate that this virus’s metrics are almost tuned to be dangerous enough to be a disaster, but not quite dangerous enough to be like the bubonic plague or polio, where everybody knew someone who was ill. And so that kind of fosters this questioning of things. It’s also a bit like speeding or texting while driving—we know it’s an awful idea, we know it kills people, but linking that action to the outcome is really hard. So when people think, ‘Oh, I’ve broken the rules, it doesn’t really matter,’ A doesn’t lead to B in their mind, although epidemiologically it clearly does.”
A lump in the throatA lump in the throat is a classic GP presentation.In the latest episode of Deep Breath In, Nick Hamilton, a clinical lecturer in otorhinolaryngology, discusses how to diagnose people with this symptom and the key differentiating features you should look for when taking history:
“Most commonly, when patients present to our clinic with a lump in the throat, it tends to be because of laryngopharyngeal reflux, but obviously, the main thing to exclude is that it doesn’t represent throat cancer. One of the key questions that you can ask is whether they notice the sensation of the lump when they swallow food, fluids, or just their saliva. That last one, where it’s only noticed on swallowing saliva, is typical of laryngopharyngeal reflux. A lump that is noticed when you swallow food or fluid is more in keeping or more concerning for a malignant cause.”
EDUCATION, p 285
PRIMARY COLOUR Helen Salisbury
Coping with pandemic stressLATEST PODCAST S

the bmj | 14 November 2020 279
Since the start of the novel coronavirus outbreak, a record number of studies have been launched to test potential treatments for covid-19. 1 An analysis by the
news organisation STAT identifi ed more than 1000 trials registered on ClinicalTrials.gov between January and June 2020. 2
However, the large volume of studies may paradoxically limit the generation of robust evidence and complicate the formulation of trustworthy guidance and decisions related to drug use if the current research is duplicative and redundant or produces confl icting data. 3- 5
Users of evidence across the healthcare system (patients, clinicians, assessment bodies, guideline developers, payers) need timely data on how treatments compare with each other in terms of their benefi ts and harms—their comparative eff ectiveness. Producing comparative evidence and ensuring its rapid translation into trustworthy guidance requires extensive coordination and collaboration between the researchers conducting clinical trials, those conducting comparative eff ectiveness assessments, and those producing guidance. 8 9 The experience of covid-19 highlights the diffi culties in making comparative assessments and suggests areas for improvement.
Limitations of covid-19 research Three main limitations have characterised the system for evaluating repurposed or investigational therapeutics for covid-19. First, global clinical research activity is fragmented. The drug trials rarely have similar design features. For example, study endpoints have been shown to be highly heterogeneous 10 and few of the late stage randomised trials measure all cause mortality. 11 Even when randomised trials evaluate seemingly similar endpoints such as recovery, outcome defi nitions and follow-up time durations vary.
Second, the research agenda seems to be partly driven by hype and anecdote rather than informativeness and social value, 12 skewing the amount of available data. For example, a disproportionately large number
of studies were launched to evaluate the antimalarial drugs hydroxychloroquine and chloroquine phosphate after the publication of a controversial uncontrolled study that received substantial attention. 13
Third, studies have not routinely adopted robust designs. We estimate that fewer than one third of studies evaluating covid-19 therapeutics on ClinicalTrials.gov are randomised controlled trials, the gold standard for evaluating treatments. 14 Many studies test investigational agents without a control group, 15 which can be misleading as they provide no data on what would have happened in the absence of the treatment.
The combination of these factors has fuelled confusion and sensationalism. Psychological distress and anxiety have increased in the general population. 16 Findings of individual studies are watched closely and with suspense. Doing “science by press release”—publicising study fi ndings before they are shared as preprints or published in peer reviewed journals—has become common. Healthcare professionals have not been immune to hype. During the early days of the pandemic, shortages of hydroxychloroquine were reported, driven by clinicians’ prescriptions after it was hailed as a potential breakthrough.
Even regulators have been under pressure to act without suffi cient evidence. 17 18 In the US, the Food and Drug Administration granted emergency use authorisation for hydroxychloroquine without any solid data suggesting that it was eff ective in covid-19. The FDA later revoked this authorisation when randomised trials found no benefi ts. The European Medicines Agency granted a conditional marketing authorisation for remdesivir on the basis of “non-comprehensive” data and without access to clinical study reports. 19
Progress on research coordination and collaboration
Mechanisms already exist for global research coordination during public health emergencies. Initiatives such as the Global Research Collaboration for Infectious Disease
Preparedness (GloPID-R), 20 established in 2013 after agreement by the heads of international (biomedical) research funding organisations, and the World Health Organization’s research and development blueprint, 21 which was developed after the Ebola outbreak in 2014-16, are platforms for collaboration. New models are also emerging. The G20 countries and WHO have established the Access to Covid-19 Tools (ACT) Accelerator, a global collaboration to accelerate the development, production, and equitable access to new diagnostics, therapeutics, and vaccines. 22
These eff orts have already paid off . Several large randomised trials have been launched in record speed. Many of these compare multiple treatments simultaneously. Three of the largest “mega” trials—the Solidarity trial led by WHO, Discovery initiated by Inserm in France, and Recovery trial in the UK—have comparable protocols and collect data on similar endpoints (including death and need for ventilation). The Recovery trial has recruited over 13 500 patients, accounting for 15% of those admitted to hospital with covid-19 across the UK. 23 Some of the most important insights about candidate therapeutics have emerged from Recovery, including the meaningful survival benefi t associated with using dexamethasone in severely ill patients. 24 The Solidarity trial, of which Discovery is an add-on, has included more than 7000 patients across more than 20 countries and can now follow the pandemic where it is globally most active.
KEY MESSAGES
• The record number of studies evaluating drugs for covid-19 has exposed important shortcomings in the evidence ecosystem
• Despite several large multi-arm trials, evidence on the comparative eff ectiveness of potential therapeutic alternatives has been delayed
• Heterogeneity of trial design and outcomes makes comparison diffi cult
• Producing comparative evidence and ensuring its rapid translation into trustworthy guidance will require greater coordination among trialists, meta-analysts, and others
ANALYSIS
L essons from covid-19 on producing and using timely comparative evidence on drugs Huseyin Naci and colleagues call for greater collaboration among trialists, meta-analysts, and guidance developers to improve the evidence base for new treatments
280 14 November 2020 | the bmj
However, eff orts to date have not managed to avoid research waste and ensure that all relevant studies contribute to the formulation of guidance and decisions in practice and policy. 25 Most studies on covid-19 treatments have methodological limitations (eg, small samples and diverse designs and outcomes). 26
Areas for improvement Determining the comparative eff ectiveness of drugs requires streamlining the design, analysis, reporting, and data sharing practices of clinical studies. These objectives are not new but progress towards achieving them has been slow. 25 27 28 Despite several large multi-arm trials, most research on covid-19 therapeutics is not fi t for generating comparative evidence. We outline fi ve priorities for greater collaboration and coordination among trialists, meta-analysts, guideline developers, and other stakeholders to facilitate producing and using trustworthy comparative evidence and guidance (table 1, see bmj.com). These are also relevant to studies evaluating other types of interventions, including supportive care and non-drug interventions.
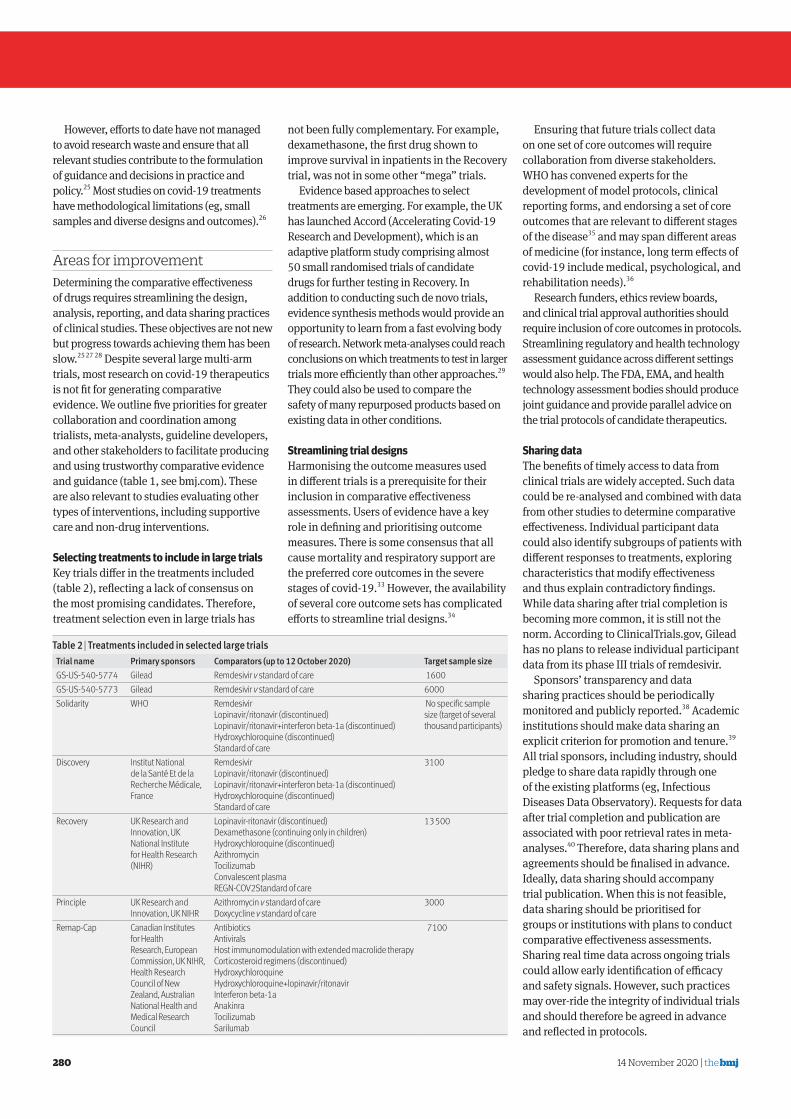
Selecting treatments to include in large trials Key trials diff er in the treatments included (table 2), refl ecting a lack of consensus on the most promising candidates. Therefore, treatment selection even in large trials has
not been fully complementary. For example, dexamethasone, the fi rst drug shown to improve survival in inpatients in the Recovery trial, was not in some other “mega” trials.
Evidence based approaches to select treatments are emerging. For example, the UK has launched Accord (Accelerating Covid-19 Research and Development), which is an adaptive platform study comprising almost 50 small randomised trials of candidate drugs for further testing in Recovery. In addition to conducting such de novo trials, evidence synthesis methods would provide an opportunity to learn from a fast evolving body of research. Network meta-analyses could reach conclusions on which treatments to test in larger trials more effi ciently than other approaches. 29 They could also be used to compare the safety of many repurposed products based on existing data in other conditions.
Streamlining trial designs Harmonising the outcome measures used in diff erent trials is a prerequisite for their inclusion in comparative eff ectiveness assessments. Users of evidence have a key role in defi ning and prioritising outcome measures. There is some consensus that all cause mortality and respiratory support are the preferred core outcomes in the severe stages of covid-19. 33 However, the availability of several core outcome sets has complicated eff orts to streamline trial designs. 34
Ensuring that future trials collect data on one set of core outcomes will require collaboration from diverse stakeholders. WHO has convened experts for the development of model protocols, clinical reporting forms, and endorsing a set of core outcomes that are relevant to diff erent stages of the disease 35 and may span diff erent areas of medicine (for instance, long term eff ects of covid-19 include medical, psychological, and rehabilitation needs). 36
Research funders, ethics review boards, and clinical trial approval authorities should require inclusion of core outcomes in protocols. Streamlining regulatory and health technology assessment guidance across diff erent settings would also help. The FDA, EMA, and health technology assessment bodies should produce joint guidance and provide parallel advice on the trial protocols of candidate therapeutics.
Sharing data The benefi ts of timely access to data from clinical trials are widely accepted. Such data could be re-analysed and combined with data from other studies to determine comparative eff ectiveness. Individual participant data could also identify subgroups of patients with diff erent responses to treatments, exploring characteristics that modify eff ectiveness and thus explain contradictory fi ndings. While data sharing after trial completion is becoming more common, it is still not the norm. According to ClinicalTrials.gov, Gilead has no plans to release individual participant data from its phase III trials of remdesivir.
Sponsors’ transparency and data sharing practices should be periodically monitored and publicly reported. 38 Academic institutions should make data sharing an explicit criterion for promotion and tenure. 39 All trial sponsors, including industry, should pledge to share data rapidly through one of the existing platforms (eg, Infectious Diseases Data Observatory). Requests for data after trial completion and publication are associated with poor retrieval rates in meta-analyses. 40 Therefore, data sharing plans and agreements should be fi nalised in advance. Ideally, data sharing should accompany trial publication. When this is not feasible, data sharing should be prioritised for groups or institutions with plans to conduct comparative eff ectiveness assessments. Sharing real time data across ongoing trials could allow early identifi cation of effi cacy and safety signals. However, such practices may over-ride the integrity of individual trials and should therefore be agreed in advance and refl ected in protocols.
Table 2 | Treatments included in selected large trials
Trial name Primary sponsors Comparators (up to 12 October 2020) Target sample size
GS-US-540-5774 Gilead Remdesivir v standard of care 1600
GS-US-540-5773 Gilead Remdesivir v standard of care 6000
Solidarity WHO Remdesivir
Lopinavir/ritonavir (discontinued)
Lopinavir/ritonavir+interferon beta-1a (discontinued)
Hydroxychloroquine (discontinued)
Standard of care
No specific sample
size (target of several
thousand participants)
Discovery Institut National
de la Santé Et de la
Recherche Médicale,
France
Remdesivir
Lopinavir/ritonavir (discontinued)
Lopinavir/ritonavir+interferon beta-1a (discontinued)
Hydroxychloroquine (discontinued)
Standard of care
3100
Recovery UK Research and
Innovation, UK
National Institute
for Health Research
(NIHR)
Lopinavir-ritonavir (discontinued)
Dexamethasone (continuing only in children)
Hydroxychloroquine (discontinued)
Azithromycin
Tocilizumab
Convalescent plasma
REGN-COV2 Standard of care
13 500
Principle UK Research and
Innovation, UK NIHR
Azithromycin v standard of care
Doxycycline v standard of care
3000
Remap-Cap Canadian Institutes
for Health
Research, European
Commission, UK NIHR,
Health Research
Council of New
Zealand, Australian
National Health and
Medical Research
Council
Antibiotics
Antivirals
Host immunomodulation with extended macrolide therapy
Corticosteroid regimens (discontinued)
Hydroxychloroquine
Hydroxychloroquine+lopinavir/ritonavir
Interferon beta-1a
Anakinra
Tocilizumab
Sarilumab
7100

the bmj | 14 November 2020 281
Assessing comparative effectiveness No single trial can compare the effi cacy of all potential treatments for covid-19. Several groups are working in parallel to identify trials and pool results in network meta-analyses as they emerge. 41 42 Such “living” syntheses could provide useful evidence, but even small diff erences in study eligibility criteria and analytical strategies may yield confl icting results, 43 which may delay the development of trustworthy guidance. It is therefore essential to coordinate ongoing activities, pool resources across groups, and minimise duplication.
A consortium should coordinate the design, implementation, and replication of comparative eff ectiveness assessments, ideally using individual participant data network meta-analyses. A network of leading independent research organisations, 44 regulatory agencies, health technology assessment bodies, and payers could lead this eff ort in collaboration with WHO. A recent health technology assessment of biological agents for rheumatoid arthritis in Germany has shown the feasibility of this approach. The Institute for Quality and Effi ciency in Health Care (IQWiG) requested re-analysis of individual participant data from several industry sponsored randomised trials to harmonise patient populations and primary endpoints before fi ndings could be combined in network meta-analyses. 45
Prompt access to comparative data is critical. Comparative assessments should ideally accompany the publication of individual trial results. This would allow study results to be interpreted within their broader context and
greatly increase speed in updating guidance. Prospectively designing comparative
eff ectiveness assessments would balance speed with rigour. At a minimum, data from trials with the most robust designs should be shared with third party researchers to conduct prospectively designed network meta-analyses. Such close collaboration would ensure data completeness, standardisation, and quality issues are resolved promptly, and the results can be re-analysed and combined shortly after the database is locked.
Translating data into guidance Covid-19 has created an unprecedented need for living and trustworthy guidance based on comparative evidence. 47 Recent experience with Australia’s National Covid-19 Clinical Evidence Taskforce shows how a comprehensive set of recommendations can be dynamically updated based on new evidence, facilitated by innovative processes and digitally structured data in interoperable platforms (eg, MAGICapp). 48 Such platforms allow for immediate global dissemination of recommendations, interactive evidence summaries, and decision aids that can be reused, adapted, or implemented. WHO and prominent guideline development organisations are now moving towards producing such living guidance for covid-19.
The BMJ ’s Rapid Recommendations entry on remdesivir shows how such global collaboration and iterative guidance development can work, informed by living network meta-analysis. 42 49 WHO
living guidance on drugs for covid-19 is developed in a similar way, fi rst published for corticosteroids. 50 The guideline panel convened and created recommendations for corticosteroids two days after unpublished data from Recovery was made available through a prospective meta-analysis. This shows the value of close collaboration between trialists, meta-analysts, and guideline developers. Global dissemination of WHO guidance was delayed for six weeks, however, as it had to wait for publication of Recovery results in a scientifi c journal, underscoring remaining challenges.
Progress in producing timely evidence on comparative eff ectiveness to date has been too slow. However, covid-19 highlights the pressing need and the opportunity to harness new collaborations among relevant stakeholders. Huseyin Naci, associate professor of health policy,
London School of Economics and Political Science
Aaron S Kesselheim, professor of medicine, Brigham and
Women’s Hospital and Harvard Medical School, Boston
John-Arne Røttingen, chief executive, Research Council of
Norway, Oslo, Norway
Georgia Salanti, associate professor of biostatistics and
epidemiology, University of Bern, Switzerland
Per O Vandvik, professor of medicine, University of Oslo,
Norway
Andrea Cipriani, professor of psychiatry, University of
Oxford
Cite this as: BMJ 2020;371:m3869
Prospectively designing comparative effectiveness assessments would balance speed with rigour
MAL
COLM
WIL
LETT

282 14 November 2020 | the bmj
LETTERS Selected from rapid responses on bmj.com
LETTER OF THE WEEK
Committing to a carbon neutral NHS NHS England’s report on achieving “net zero” (Editorial, 17 October) leaves out three important considerations. It states that food and catering account for 6% of total emissions but makes no reference to the vastly greater emissions generated by meat and dairy products compared with plant based diets. Adopting plant based catering for the whole of the NHS would be straightforward to implement and would have knock-on effects, in terms of changing attitudes to diet beyond the NHS.
Secondly, although the report rightly mentions the need to measure and report on the embedded carbon in the supply chain of medicines and other equipment, it overlooks the need to systematically calculate the carbon footprint of all NHS procedures. This is of course partly made up of the embedded carbon in consumables but will also include emissions associated with hospital visits and stays, and so on. Only when we know the carbon footprint of an intervention can we seek ways to reduce it. Then trusts could be allocated a “carbon budget,” which could be reduced progressively over time. This might lead to consideration of whether the health benefit of the intervention justifies the emissions released.
Finally, although incorporating net zero ambitions into the NHS’s constitution would be welcome, as would the requirement that every organisation has a board level lead, the report does not specify the “national and local levers” that will be used to support the delivery of the commitments. These must have real power to make change so that environmental sustainability becomes one of the central considerations of trust boards. The Care Quality Commission should add it as a domain in their assessment of trust performance, so that “Is this service environmentally sustainable” is asked of every service it inspects. That way, boards will sit up and take notice. Jeremy Wight, retired director of public health , Hope
Cite this as: BMJ 2020;371:m4274
Healthcare should not cost us the Earth The pandemic has given us opportunities to reduce our carbon footprint (Editor’s Choice, 17 October), but it has also placed hidden environmental challenges on the NHS.
Vast quantities of personal protective equipment (PPE) are now required. WHO estimated that some 89 million medical masks, 76 million examination gloves, and 1.6 million pairs of goggles would be required worldwide in each month of the pandemic. These figures are a stark reminder of our plastic waste. Most of our PPE is imported from China rather than locally sourced, unnecessarily increasing the carbon footprint.
To add insult to injury, recycling systems in place before covid-19 are now largely obsolete owing to potential contamination. We urgently need an NHS-wide recycling policy to identify areas in which we can reduce waste to landfill or incineration.
At a time of pressure and austerity in the NHS, we must not take financial shortcuts for less environmentally sustainable options.
Ruth Bennett, specialty trainee year 3 in plastic
surgery ; Jane Maraka, specialty trainee year 6 in
plastic surgery , Durham
Cite this as: BMJ 2020;371:m4289
The many benefits of video consulting In response to covid-19, the Welsh government offered all primary, secondary, and community care NHS services unlimited use of a new video consulting service, which was implemented and robustly evaluated by Technology Enabled Care Cymru.
The National Video Consulting Service has delivered 55 000 video consultations across more than 100 specialties. Over 20 000 research participants have reported huge benefits to patients, professionals, and the environment—for example, 5539 hours of patient and clinician travel has been saved, along with 55 tonnes of CO 2 . Other benefits included saved clinical and patient time, space, and preparation, less paper waste, less need for room bookings and costs, savings on childcare, and less time off work or school.
The Welsh health minister has now issued a statement saying that “digital is here to stay,” supporting the use of technology to deliver healthcare as the way forward to improve patient care, the NHS, and the environment. Gemma Johns, research and evaluation lead; Sara
Khalil , programme lead; Mike Ogonovsky, senior
responsible offi cer ; Alka Ahuja, clinical lead ,
Technology Enabled Care Cymru
Cite this as: BMJ 2020;371:m4300
COVID-19 AND NET ZERO FOR HEALTH
Hayek and colleagues found that cardiac arrest is common and associated with poor survival in patients critically ill with covid-19 (Research, 3 October).
The sharp decline in admissions for coronary syndromes during the covid-19 pandemic is complex. We are seeing a lower rate of presentations and a higher rate of delayed presentations. Patients might be underestimating their symptoms and seeking medical attention later than usual, but also many cardiac and emergency units were
restructured and became less functional.
The excess death rate from untreated coronary syndromes is likely to be substantial. A drop in admissions for coronary syndromes is a risk factor for increased in-hospital cardiac arrest as well as out-of-hospital mortality and morbidity, leading to a predictably higher rate of heart failure in a “third
wave” of this pandemic. Primary care can play a critical role by encouraging all patients with symptoms compatible with coronary syndromes to seek treatment. José Ramón Seco Vasco,
emergency doctor, cardiologist,
and researcher ; Raul Curado
Castano, emergency doctor and
researcher ; Ana Maria Mateos
Gomez, emergency doctor and
researcher , Sevilla
Cite this as: BMJ 2020;371:m4250
CARDIAC ARREST IN COVID-19
Untreated coronary syndromes

the bmj | 14 November 2020 283
POLL ON BMA OPPOSITION TO ASSISTED DYING
Survey results misrepresented The headline “BMA should drop its opposition to assisting dying, say members in landmark poll” (This Week, 17 October) misrepresents the results of the BMA survey, which show a clear difference between support for physician assisted suicide and for voluntary euthanasia. Excluding those who were neutral or undecided, more respondents said that the BMA should be in favour of supporting attempts to change the law around physician assisted suicide (40% versus 33%); the percentages were reversed for voluntary euthanasia (30% versus 40%).
Interestingly, more respondents were against prescribing drugs for physician assisted suicide and performing voluntary euthanasia, showing an interesting divergence between respondents’ views of what might be legally permitted and what they personally felt was right. Only 6% of respondents in palliative medicine would be happy to administer drugs for voluntary euthanasia. Thus the suggestion by some respondents that palliative medicine could accept responsibility for implementation is disturbing. Robert Twycross, emeritus clinical reader in palliative medicine , Oxford
Cite this as: BMJ 2020;371:m4305
Doctors’ views don’t matter We’ve had a Royal College of Physicians poll, a Royal College of General Practitioners poll, and now the BMA poll on assisted dying.
But the response rates were too low to make any conclusions about the questions asked.
These polls should be ignored, and it is hard to understand how a scientifically sophisticated group of professionals can argue otherwise. Perhaps an explanation lies in the BMA’s justification that it was “higher than other surveys we have carried out of our full membership and higher than or in line with the typical market research response rate for this type of survey.”
We still don’t have a good measure of doctors’ views. But that doesn’t matter so much as the opinions of the patients. If assisted dying is the wish of some people, then the inevitable practical and theoretical associates, including our three poor polls, should not stand in its way. Sam Shuster, emeritus professor of dermatology , Woodbridge
Cite this as: BMJ 2020;371:m4310
“NORMAL” RISK AND DANGERS OF COVID-19
Awareness of normal risk is not normal Epidemiological rates and disease risks often do not resonate with the public (Analysis, 3 October). Human beings are generally more attuned to anecdotes than hard data. The “Jade Goody effect” on cervical cancer screening amply demonstrates the power of anecdotes. So “excess normal risk information” is unlikely to have a substantial effect on public awareness.
People are more likely to seek health information about personal vulnerability, not population level risks. Clinicians on the front line would prefer an easy-to-use risk stratification score that can inform clinical judgment. So “normal risk” terminology is neither useful nor relevant for individuals or clinicians.
Finally, awareness of normal risk is not normal. The public do not go about their daily life thinking of their mortality risk. Even patients with incurable cancer use hope and optimism as coping mechanisms. Educating the public about extra mortality risk over and above “normal risk” would be a tall order. Santhanam Sundar , consultant oncologist , Nottingham
Cite this as: BMJ 2020;371:m4121
VALUE OF OLDER LIVES
Older lives are valuable but not equal Salisbury wants her older patients to leave with the feelgood factor (Helen Salisbury, 17 October).
Older people are unlikely to have paid for their care in full if we allow for increases in treatment costs and longer survival with lower spending on the NHS in the past. They have had a lifetime of support from the NHS, and younger people should be entitled to this too.
Covid priorities for high risk older people might mean more time on waiting lists for younger people. My health priorities are now geared to maximising quality in what remains rather than to the current obsession with mere length. I suspect that many older people feel likewise.
Any decision favouring a younger patient, taking account of likely length of life, burden of treatment, and likelihood of co-existing morbidity, is open to accusations of ageism. Not all of us older people see ourselves as a burden. Simon Kenwright , retired physician , Stowting
Cite this as: BMJ 2020;371:m4311
HONESTY ABOUT NHS LIMITS
Unacknowledged rationing Kar says that patients deserve honesty about the limits of the NHS (Partha Kar, 17 October). To quote Enoch Powell: “The worst kind of rationing is that which is unacknowledged; for it is the essence of a good rationing system to be intelligible and consciously accepted.”
If we continue with the collusion of denial between politicians and media, and assuming that technology advances faster than (any) government can keep up with, we are heading for a two tier system once again, as before 1948. Roger W Burns, retired GP , Haverfordwest
Cite this as: BMJ 2020;371:m4315

the bmj | 14 November 2020 293
OBITUARIES
Longer versions are on bmj.com. Submit obituaries with a contact telephone number to [email protected]
Kamalini Narayan General practitioner
Birmingham (b 1929;
q Lucknow, India, 1952;
DObst RCOG, DCH), died
from ischaemic heart
disease on 29 January 2020
Kamalini Narayan was a thoughtful doctor, loving mother, and devoted wife. She was a gold medallist at King George’s Medical College, Lucknow, where she met her future husband, Prakash. After moving to the UK in 1953, Kamalini pursued paediatrics at the Great Ormond Street Hospital for Sick Children network, and was paediatric registrar at West Hertfordshire Hospitals in 1961. She and Prakash moved to Birmingham as partners in general practice in 1966. They retired in 1997. Kamalini was a maternal figure to numerous nieces, nephews, and friends, whom she inspired with her warmth, immense practicality, and creativity. She was a de facto expert on botany and co-founded the Shree Gita Bhawan Hindu temple in Birmingham. She leaves three children and five grandchildren in the UK and California. Sanjiv M Narayan
Cite this as: BMJ 2020;370:m3539
Prakash Narayan General practitioner
Birmingham (b 1928;
q Lucknow 1951; DTM&H),
died from complications of
prostatic carcinoma on
21 May 2020
Prakash Narayan was gregarious, a quintessential general practitioner, and a loving and inspiring husband and father . He met his future wife, Kamalini, at King George’s Medical College, Lucknow. On coming to the UK in 1953, Prakash initially pursued surgery before changing to general practice. He and Kamalini became GP principals in Birmingham in 1966. He relished long surgery hours, performed extensive home visits, and loved the NHS. They both retired in 1997. Prakash engaged friends, patients, and relatives with his affability, humour, and encyclopaedic knowledge of geography, world affairs, and Hollywood trivia. He co-founded the Shree Gita Bhawan Hindu temple in Birmingham in the 1960s. He travelled widely with Kamalini well into their 80s and encircled the globe multiple times. He leaves three children and five grandchildren in the UK and California. Sanjiv M Narayan
Cite this as: BMJ 2020;370:m3542
Deryk Anthony Lawrence General practitioner
(b 1926; q St Thomas’
Hospital Medical
School; FRCGP), died
from heart failure,
complicated by
pneumonia, on
12 January 2020
Deryk Anthony Lawrence did his house jobs at Epsom Hospital and at the General Lying-In Hospital in Waterloo. At Epsom he met Myra Coyne, and in 1952 the nurse married the doctor. Deryk did national service as a surgeon lieutenant in the Royal Navy from 1952 to 1954. He subsequently decided on a career in general practice and joined a two doctor practice in Dartford, Kent, in 1955. He was a representative on the Kent local medical committee in the 1970s and was a police surgeon for 30 years. He went part time in 1995 and continued in practice until retiring fully at the age of 86. Predeceased by Myra in 2001, he leaves two children and three grandchildren. David Lawrence
Cite this as: BMJ 2020;370:m3527
Bob Leeming
Consultant ear, nose, and
throat surgeon Wrexham
Maelor Hospital (b 1931;
q Dublin 1957; DLO Eng,
FRCS Ed), died from heart
failure on 30 July 2020
Bob Leeming was born to an Anglo-Indian family in what was then Calcutta, India. A few years after Indian independence in 1947, his family moved to Europe. Bob trained in medicine in Dublin. He worked as a junior doctor in Newport before joining the Royal Air Force. He specialised in ear, nose, and throat medicine and served in Aden, Yemen, during the early 1960s. There he met his future wife, Esther, a teacher for the RAF. Bob held posts in the UK and Cyprus. After leaving the RAF in 1976, he became ENT consultant at Wrexham Maelor Hospital in north Wales—a post he held until his retirement in 1997. He leaves his wife, five children, eight grandchildren, and one great grandchild. Ciara Leeming
Cite this as: BMJ 2020;370:m3538
Maurice McConnell Burrows
Consultant anaesthetist Wirral Hospital
(b 1926; q Queen’s University Belfast 1949;
FFARCS), died from old age on 28 July 2020
Maurice McConnell Burrows trained as an anaesthetist in Liverpool and was appointed consultant anaesthetist in 1958. He soon showed his managerial aptitude, which would be employed locally, regionally, and nationally, while he maintained his heavy clinical workload. As chair of the Consultants Committee for Hospital Medical Services, and later as chair of the Wirral hospitals, he dealt with trenchantly held and often incompatible views. He negotiated the middle way by his careful preparatory homework, his networking, and understanding his adversaries. His velvet glove covered a resolute hand. Maurice was a gentleman, modest, unpretentious, approachable, and interesting. His jokes were memorable. His family and his strong Christian faith were bedrocks of his moral compass. He leaves his wife of 64 years, a son, and a brother. A daughter predeceased him. John Sprigge
Cite this as: BMJ 2020;370:m3522
Anthony Lyn Power
Consultant radiologist
Swansea (b 1946; q Cardiff
1969; FRCR), died from
gastric cancer on
20 August 2020
Anthony Lyn Power (“Tony”) became a consultant radiologist in his home city of Swansea in 1978. He pioneered the introduction and setting up of an early pregnancy ultrasound service running seven days a week from the outset. With his diplomatic demeanour he was a natural to be departmental clinical director, gaining the unit staffing expansion and equipment including computed tomography and magnetic resonance scanners to meet the increasing demands on his expanding specialty. His management skills were recognised by all in his hospital. Tony was also a skilled negotiator and a key member of the team who negotiated the consultants’ contract for Wales in 2003, for which he was awarded a fellowship of the BMA. He retired in 2008. He leaves his wife, Jennifer; two children; and two granddaughters. Ian Millington, Martin White
Cite this as: BMJ 2020;370:m3521
294 14 November 2020 | the bmj
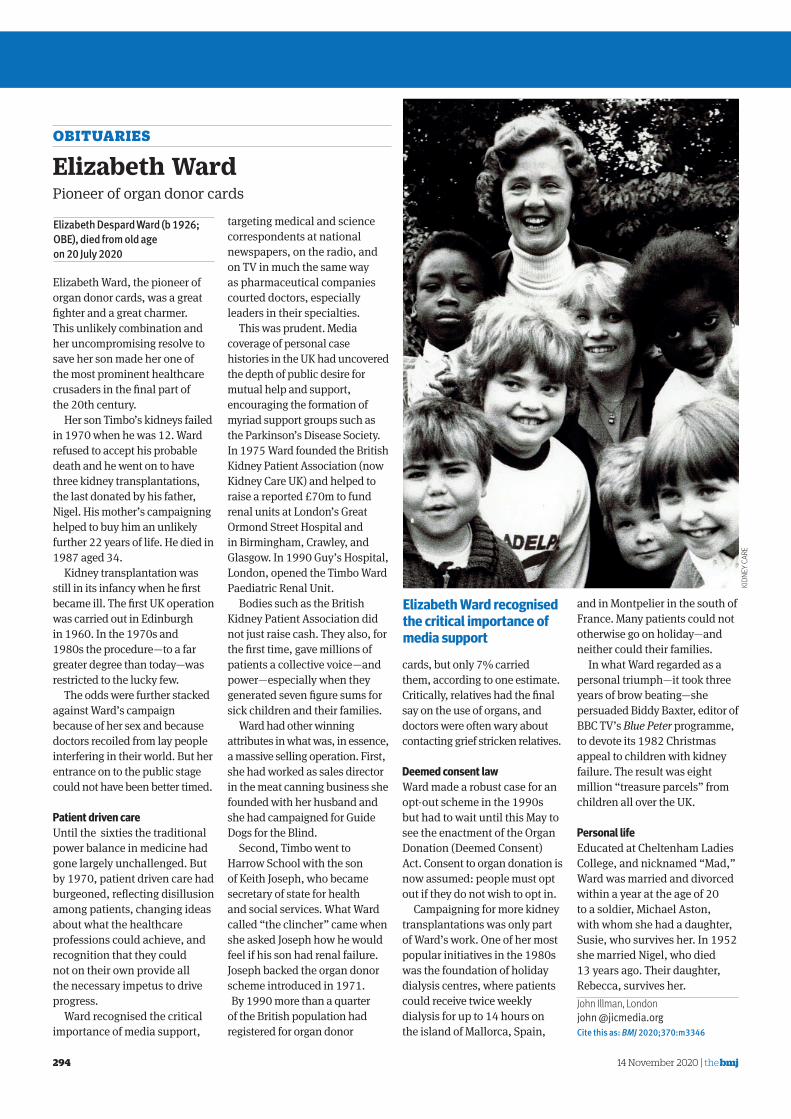
Elizabeth Ward, the pioneer of organ donor cards, was a great fi ghter and a great charmer. This unlikely combination and her uncompromising resolve to save her son made her one of the most prominent healthcare crusaders in the fi nal part of the 20th century.
Her son Timbo’s kidneys failed in 1970 when he was 12. Ward refused to accept his probable death and he went on to have three kidney transplantations, the last donated by his father, Nigel. His mother’s campaigning helped to buy him an unlikely further 22 years of life. He died in 1987 aged 34.
Kidney transplantation was still in its infancy when he fi rst became ill. The fi rst UK operation was carried out in Edinburgh in 1960. In the 1970s and 1980s the procedure—to a far greater degree than today—was restricted to the lucky few.
The odds were further stacked against Ward’s campaign because of her sex and because doctors recoiled from lay people interfering in their world. But her entrance on to the public stage could not have been better timed.
Patient driven care Until the sixties the traditional power balance in medicine had gone largely unchallenged. But by 1970, patient driven care had burgeoned, refl ecting disillusion among patients, changing ideas about what the healthcare professions could achieve, and recognition that they could not on their own provide all the necessary impetus to drive progress.
Ward recognised the critical importance of media support,
targeting medical and science correspondents at national newspapers, on the radio, and on TV in much the same way as pharmaceutical companies courted doctors, especially leaders in their specialties.
This was prudent. Media coverage of personal case histories in the UK had uncovered the depth of public desire for mutual help and support, encouraging the formation of myriad support groups such as the Parkinson’s Disease Society. In 1975 Ward founded the British Kidney Patient Association (now Kidney Care UK) and helped to raise a reported £70m to fund renal units at London’s Great Ormond Street Hospital and in Birmingham, Crawley, and Glasgow. In 1990 Guy’s Hospital, London, opened the Timbo Ward Paediatric Renal Unit.
Bodies such as the British Kidney Patient Association did not just raise cash. They also, for the fi rst time, gave millions of patients a collective voice—and power—especially when they generated seven fi gure sums for sick children and their families.
Ward had other winning attributes in what was, in essence, a massive selling operation. First, she had worked as sales director in the meat canning business she founded with her husband and she had campaigned for Guide Dogs for the Blind.
Second, Timbo went to Harrow School with the son of Keith Joseph, who became secretary of state for health and social services. What Ward called “the clincher” came when she asked Joseph how he would feel if his son had renal failure. Joseph backed the organ donor scheme introduced in 1971. By 1990 more than a quarter
of the British population had registered for organ donor
cards, but only 7% carried them, according to one estimate. Critically, relatives had the fi nal say on the use of organs, and doctors were often wary about contacting grief stricken relatives.
Deemed consent law Ward made a robust case for an opt-out scheme in the 1990s but had to wait until this May to see the enactment of the Organ Donation (Deemed Consent) Act. Consent to organ donation is now assumed: people must opt out if they do not wish to opt in.
Campaigning for more kidney transplantations was only part of Ward’s work. One of her most popular initiatives in the 1980s was the foundation of holiday dialysis centres, where patients could receive twice weekly dialysis for up to 14 hours on the island of Mallorca, Spain,
and in Montpelier in the south of France. Many patients could not otherwise go on holiday—and neither could their families .
In what Ward regarded as a personal triumph—it took three years of brow beating—she persuaded Biddy Baxter, editor of BBC TV’s Blue Peter programme, to devote its 1982 Christmas appeal to children with kidney failure. The result was eight million “treasure parcels” from children all over the UK.
Personal life Educated at Cheltenham Ladies College, and nicknamed “Mad,” Ward was married and divorced within a year at the age of 20 to a soldier, Michael Aston, with whom she had a daughter, Susie, who survives her. In 1952 she married Nigel, who died 13 years ago. Their daughter, Rebecca, survives her. John Illman , Londonjohn @jicmedia.org Cite this as: BMJ 2020;370:m3346
OBITUARIES
Elizabeth Despard Ward (b 1926;
OBE), died from old age
on 20 July 2020
KIDN
EY C
ARE
Elizabeth Ward Pioneer of organ donor cards
Elizabeth Ward recognised the critical importance of media support
Related Documents











