Laying the Groundwork in Laying the Groundwork in Policy and Practice: The Policy and Practice: The Massachusetts Early Childhood Massachusetts Early Childhood Linkage Initiative Linkage Initiative Children and Family Futures Children and Family Futures February 1, 2007 February 1, 2007 Institute for Health and Institute for Health and Recovery Recovery The Heller School, Brandeis The Heller School, Brandeis University University

Laying the Groundwork in Policy and Practice: The Massachusetts Early Childhood Linkage Initiative Laying the Groundwork in Policy and Practice: The Massachusetts.
Dec 25, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Laying the Groundwork in Laying the Groundwork in Policy and Practice: The Policy and Practice: The
Massachusetts Early Childhood Massachusetts Early Childhood Linkage InitiativeLinkage Initiative
Children and Family FuturesChildren and Family FuturesFebruary 1, 2007February 1, 2007
Institute for Health and Institute for Health and RecoveryRecovery
The Heller School, Brandeis The Heller School, Brandeis UniversityUniversity

Laying the Groundwork in Laying the Groundwork in Policy and PracticePolicy and Practice
• Science-based policy for young children• Effective implementation• Collaboration• Evidence-based practice• Appropriate resources: funding,
expertise

Who We AreWho We Are
• Katharine Thomas, Assistant Director, Institute for Health and Recovery (IHR), since 2006…2001-2006, Policy Director, Part C Early Intervention, MA DPH…1991-2001, Systems Developer at IHR
• John Lippitt, Ph.D, Project Director, Identification and Treatment of Infants and Families (MA DPH), since 2006…2003-2006 , Senior Research Associate, Heller School for Social Policy and Management, Brandeis University, Waltham, MA

Institute for Institute for Health and RecoveryHealth and Recovery
• State resource for development of family focused substance abuse services
• History of systems work with providers, communities, state agencies
• Outside agency: ability to transcend perceived “turf” issues
• Inside agency: partner with state agencies as “arm” for specialized services
Institute for Health and Institute for Health and Recovery: Core PrinciplesRecovery: Core Principles
• Establish collaborative models of service delivery
• Integrate gender-specific, trauma-informed, and relational/cultural models
• Foster family-centered, strengths-based approaches: support resiliency
• Advance multicultural competency within service delivery
Institute for Institute for Health and RecoveryHealth and Recovery
• 1989: Federal grant: integrate parenting support and skill-building into women’s residential substance abuse treatment
• 1990: Contract: state Bureau of Substance Abuse Services to build capacity in women’s SA treatment system
• 1994: Manage central access to Family Residential Programs

Institute for Institute for Health and RecoveryHealth and Recovery
•Tobacco addiction education/policy
•WELL Project: Integrate substance abuse, mental health, and trauma services for women and their children
•WELL Child: Curriculum developed to build resilience in children of substance abusers

Massachusetts Massachusetts Department of Public HealthDepartment of Public Health
•….“To promote healthy people, healthy families, healthy communities and healthy environments through compassionate care, education and prevention”….
•Lead Agency in MA for Part C Early Intervention Services
Early Intervention (EI) in Early Intervention (EI) in MassachusettsMassachusetts
•MA Department of Public Health (MDPH)
•Bureau of Family and Community Health
•Division for Perinatal, Early Childhood and Special Health Needs (DPECSHN)

EI Program History in MAEI Program History in MA
•Early 70’s: EI system in clinical settings, DMH/DMR
•1983: MGL 111G •1985: EI Medicaid reimbursement
begins•1986: Individuals with Disabilities
Education Act, reauthorized in 1997 •1990: Legislation mandating private
insurance coverage of EI
EI Program History in MAEI Program History in MA(continued)(continued)
•2001: Insurance legislation revised to include reimbursement for developmental specialists (aka early childhood educators)
•2004: Annual insurance cap increased from $3200-$5200
•2004: IDEA re-authorized, adds language regarding specific populations
MA General Law (MGL) MA General Law (MGL) Chapter 111G, 1983Chapter 111G, 1983
• Named DPH as Lead Agency
• Ensured universal access to EI
• Specified inclusion of staff of different disciplines
• Provided EI option to children with established, environmental, and biological risk

EI In Massachusetts: EI In Massachusetts: 3 Broad Categories3 Broad Categories
• Established Condition / Diagnosis• Developmental Delay (25% in one
domain)• At Risk (optional category for
states): 4 of 20 risk factors, including CW case, SA, DV, homeless, lacking social supports
• MA serves highest percentage of birth to three-year-olds nationally

Child Well-Being and Child Well-Being and DevelopmentDevelopment
“From Neurons to
Neighborhoo
ds”Published in 2000
National Research Council /
Institute of Medicine
Jack Shonkoff Deborah Phillips

Child Well-Being and Child Well-Being and DevelopmentDevelopment
TOXIC STRESS in early childhood•Strong, frequent or prolonged activation
of body’s stress management system•Impacts brain architecture particularly in
the absence of nurturing parent or caregiver
Distinguished from:•Positive stress: moderate, short-lived;
normal part of life; essential to healthy development
•Tolerable stress: significant but infrequent; nurturing parent or caregiver helps child feel safe; calms stress response

Child Well-Being and Child Well-Being and DevelopmentDevelopment
Neurons to Neighborhoods Recommendation:
“…require that all children who are referred to a protective services agency for evaluation of suspected abuse or neglect be automatically referred for a developmental-behavioral screening under Part C of the Individuals with Disabilities Education Act.”

Child Well-Being and Child Well-Being and DevelopmentDevelopment
• Child safety, health, and all the developmental domains are inextricably intertwined
• Nurturing relationship with parents or other key caregivers is essential to safety and development
• Child maltreatment and parental SA put both safety and development at high risk

Young Children at RiskYoung Children at RiskLack of resources, substance abuse, mental
health, family violence, and increased family stress impact child development:
• Physical (motor challenges, unsafe spaces)• Social-emotional ( insecure attachment,
behavior, low self-esteem)• Cognitive (lack of appropriate stimulation,
fears/worries may affect ability to focus)• Communication (limited or inappropriate
language stimulation/interaction)• Adaptive (inability to develop needed
independence and skills for self-care)
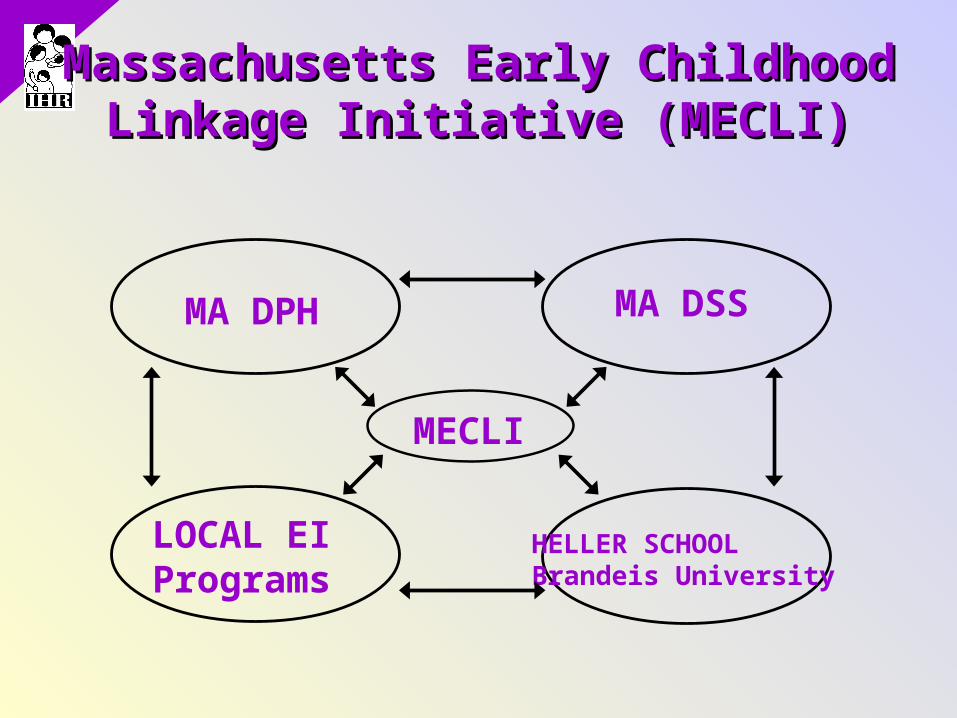
Massachusetts Early Childhood Massachusetts Early Childhood Linkage Initiative (MECLI)Linkage Initiative (MECLI)
MECLI
MA DSS MA DPH
LOCAL EI Programs
HELLER SCHOOLBrandeis University
MECLI OverviewMECLI Overview
•Goal: Refer all young children under three years of age involved with a newly substantiated case of child abuse or neglect to EI
• 3 Pilot sites in MA, Nov. 2002 – Dec. 2004
• Both CW and EI were supportive• Robust EI system able to handle
referrals
The MECLI project was funded by the U.S. Department of Health and Human Services, Administration for Children and Families, Children's Bureau; The A.L. Mailman Family Foundation; The Annie E. Casey Foundation; and The Frank and Theresa Caplan Endowment for Early Childhood and Parenting Education at The Heller School for Social Policy and Management, Brandeis University. We thank these organizations for their support but acknowledge that the findings and conclusions presented in this report are those of the author(s) alone and do not necessarily reflect the opinions of these organizations.

MECLI GoalsMECLI Goals
• Support referrals through local collaborations (EI Programs and DSS Area Offices)
• Anticipate CAPTA/IDEA requirements to refer children from CW to EI services
• Collect data on offering of referral at CW and engagement in EI
MECLI Goals (continued)MECLI Goals (continued)
• Collect data on EI eligibility and services
• Enhance understanding of impact of bio-psycho-social factors on young children’s development
• Identify strategies to engage and serve children/families
MECLI ResultsMECLI Results
• 540 children offered referral to EI
• 18% of parents refused the referral (99)
• 19% of families referred did not engage
with EI (103)
• 40% of children were assessed (218)
MECLI Results (continued)MECLI Results (continued)
• 74% of children assessed were eligible (161/218) under MA broad eligibility criteria
• 49% had an eligible delay (107/218)• 17% eligible due to 4 of 20 risk
factors (37/218)• 1% eligible by established condition
or clinical judgment• 6% eligibility criterion unknown

CAPTA, June 2003 CAPTA, June 2003 New Language HighlightsNew Language Highlights
The Keeping Children and Families Safe Act reauthorizes CAPTA, requires states to establish:
“provisions and procedures for referral of a child under the age of 3 who is involved in a substantiated case of child abuse or neglect to early intervention services funded under Part C of the Individuals with Disabilities Education Act”
AND
CAPTA, June 2003 CAPTA, June 2003 New Language HighlightsNew Language Highlights
• “policies and procedures … to address the needs of infants born and identified as being affected by illegal substance abuse or withdrawal symptoms resulting from prenatal drug exposure, including a requirement that health care providers involved in the delivery or care of such infants notify the child protective services system … [and] the development of a plan of safe care for the infant”
IDEA, December 2004 IDEA, December 2004 New Language HighlightsNew Language Highlights
• “a description of the State policies and procedures that require the referral for early intervention under this part of a child under the age of 3 who
“(A) is involved in a substantiated case of abuse or neglect; or
“(B) is identified as affected by illegal substance abuse, or withdrawal symptoms resulting from prenatal drug exposure;”
• “…..premature infants, or infants with other physical risk factors associated with learning or developmental complications….”
• “…underserved groups, including minority, low-income, homeless, and rural families and children with disabilities who are wards of the State…”

ACF-Funded Projects 2005ACF-Funded Projects 2005
Model Development or Replication to Implement the CAPTA Requirement to Identify and Serve Substance Exposed Newborns (CFDA # 93.551)
• Denver Department of Human Services, Denver, CO
• University of Oregon, Office of Research Services and Administration, Eugene, OR
• Saint Vincent Mercy Medical Center, Toledo, OH
• Department of Public Health, Boston, MA

Substance Exposed NewbornsSubstance Exposed Newborns
• A combination of bio-medical and environmental conditions
• Demonstration project builds on MECLI
• Uses 2 of 3 pilot sites• Builds on inter-agency relationships• Adds SA and other services to
MECLI collaboration

Substance Exposed Newborns Substance Exposed Newborns (continued)(continued)
• Identification and Treatment for substance exposed Infants and their Families (ITIF)
• A Helping Hand: Mother to Mother• The Family Support Specialist: a peer
mentor, support, & advocate• Enhanced care coordination at CW• Use one-time grant funding to do pilot
to work toward full implementation

Systems ChangeSystems Change
Begin by Identifying:•Barriers/Gaps•Common values•Common goals based on values
•Key resources system wide•Stakeholders•Key resources
ConclusionsConclusions
• CW and SA treatment need to build linkages with developmental services
• Family-centered and strengths-based to engage and motivate parents AND keep families together
• Build collaborations for comprehensive, coordinated services

Conclusions (continued)Conclusions (continued)
• Part C Early Intervention for children from birth to 3rd birthday
• Part C EI needs resources: funding and enhanced expertise
• Part C systems’ roles and eligibility criteria vary by state
• Part C eligibility should address key environmental conditions

Conclusions (continued)Conclusions (continued)
Some environmental conditions present similar likelihood of developmental problems as bio-medical conditions:
• Child abuse or neglect• Parental substance abuse• Parental mental health problems,
especially maternal depression• Intimate partner violence

Conclusions (continued)Conclusions (continued)
WE MUST ADDRESS:• Turf issues• Differing systems characteristics,
including eligibility and policies• ResourcesTogether we CAN do a better job of
supporting child well-being including safety and healthy development, which are key to good family outcomes

Institute for Institute for Health and Recovery (IHR)Health and Recovery (IHR)
Katharine ThomasKatharine Thomas349 Broadway349 Broadway
Cambridge, MA 02139Cambridge, MA 02139Ph 617.661.3991 Fax Ph 617.661.3991 Fax
617.661.7277617.661.7277Email: Email:
[email protected]@healthrecovery.orgorg
www.healthrecovery.orgwww.healthrecovery.org

Massachusetts Department Massachusetts Department of Public Healthof Public Health
John LippittJohn Lippitt250 Washington Street, 5250 Washington Street, 5thth
FloorFloorBoston, MA 02108Boston, MA 02108
Ph 617.624.6017 Fax Ph 617.624.6017 Fax 617.624.5990617.624.5990
Email: Email: [email protected]/dph/fchwww.mass.gov/dph/fch
Related Documents