This article was downloaded by: [Norrlands Universitetssjukehus] On: 13 October 2014, At: 23:18 Publisher: Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Neurocase: The Neural Basis of Cognition Publication details, including instructions for authors and subscription information: http://www.tandfonline.com/loi/nncs20 Laterality and deep brain stimulation of the subthalamic nucleus: applying a dichotic listening task to patients treated for Parkinson’s disease Rickard L. Sjöberg a , Björn Häggström a , Johanna Philipsson a , Jan Linder a , Marwan Hariz ab & Patric Blomstedt a a Department of Pharmacology and Clinical Neuroscience, Umeå University, Umeå, Sweden b Institute of Neurology, University College London, London, UK Published online: 25 Sep 2014. To cite this article: Rickard L. Sjöberg, Björn Häggström, Johanna Philipsson, Jan Linder, Marwan Hariz & Patric Blomstedt (2014): Laterality and deep brain stimulation of the subthalamic nucleus: applying a dichotic listening task to patients treated for Parkinson’s disease, Neurocase: The Neural Basis of Cognition, DOI: 10.1080/13554794.2014.960427 To link to this article: http://dx.doi.org/10.1080/13554794.2014.960427 PLEASE SCROLL DOWN FOR ARTICLE Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) contained in the publications on our platform. However, Taylor & Francis, our agents, and our licensors make no representations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of the Content. Any opinions and views expressed in this publication are the opinions and views of the authors, and are not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be relied upon and should be independently verified with primary sources of information. Taylor and Francis shall not be liable for any losses, actions, claims, proceedings, demands, costs, expenses, damages, and other liabilities whatsoever or howsoever caused arising directly or indirectly in connection with, in relation to or arising out of the use of the Content. This article may be used for research, teaching, and private study purposes. Any substantial or systematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in any form to anyone is expressly forbidden. Terms & Conditions of access and use can be found at http:// www.tandfonline.com/page/terms-and-conditions

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

This article was downloaded by: [Norrlands Universitetssjukehus]On: 13 October 2014, At: 23:18Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House,37-41 Mortimer Street, London W1T 3JH, UK
Neurocase: The Neural Basis of CognitionPublication details, including instructions for authors and subscription information:http://www.tandfonline.com/loi/nncs20
Laterality and deep brain stimulation of thesubthalamic nucleus: applying a dichotic listening taskto patients treated for Parkinson’s diseaseRickard L. Sjöberga, Björn Häggströma, Johanna Philipssona, Jan Lindera, Marwan Harizab &Patric Blomstedta
a Department of Pharmacology and Clinical Neuroscience, Umeå University, Umeå, Swedenb Institute of Neurology, University College London, London, UKPublished online: 25 Sep 2014.
To cite this article: Rickard L. Sjöberg, Björn Häggström, Johanna Philipsson, Jan Linder, Marwan Hariz & Patric Blomstedt(2014): Laterality and deep brain stimulation of the subthalamic nucleus: applying a dichotic listening task to patientstreated for Parkinson’s disease, Neurocase: The Neural Basis of Cognition, DOI: 10.1080/13554794.2014.960427
To link to this article: http://dx.doi.org/10.1080/13554794.2014.960427
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) containedin the publications on our platform. However, Taylor & Francis, our agents, and our licensors make norepresentations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of theContent. Any opinions and views expressed in this publication are the opinions and views of the authors, andare not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be relied upon andshould be independently verified with primary sources of information. Taylor and Francis shall not be liable forany losses, actions, claims, proceedings, demands, costs, expenses, damages, and other liabilities whatsoeveror howsoever caused arising directly or indirectly in connection with, in relation to or arising out of the use ofthe Content.
This article may be used for research, teaching, and private study purposes. Any substantial or systematicreproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in anyform to anyone is expressly forbidden. Terms & Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions

Laterality and deep brain stimulation of the subthalamic nucleus: applying a dichotic listeningtask to patients treated for Parkinson’s disease
Rickard L. Sjöberga*, Björn Häggströma, Johanna Philipssona, Jan Lindera, Marwan Hariza,b and Patric Blomstedta
aDepartment of Pharmacology and Clinical Neuroscience, Umeå University, Umeå, Sweden; bInstitute of Neurology, University CollegeLondon, London, UK
(Received 12 July 2013; accepted 26 August 2014)
Ear advantage during a dichotic listening task tends to mirror speech lateralization. Previous studies in stroke patients haveshown that lesions in the dominant hemisphere often seem to produce changes in ear advantage. In this study sixParkinson’s disease (PD) patients treated for motor symptoms with deep brain stimulation (DBS) of the left subthalamicnucleus (STN) were tested preoperatively and at approximately 6 and 18 months postoperatively with a dichotic listeningtask. Results show a significant decline of the right ear advantage over time. In three of the patients a right ear advantagepreoperativley changed to a left ear advantage 18 months postoperatively. This suggests the possibility that additionallongitudinal studies of this phenomenon could serve as a model for understanding changes in indirect measures of speechlateralization in stroke patients.
Keywords: dichotic listening; aphasia; hemispheric dominance; deep brain stimulation; subthalamic nucleus
When verbal material is simultaneously presented to boththe ears, healthy subjects typically perceive and/or remem-ber stimuli presented in the right ear better than stimulipresented in the left ear. This advantage is shown providedthat their language functions reside in the left hemisphere,which is almost always the case for right-handed indivi-duals (Hiscock & Kinsbourne, 2011; Hugdahl et al., 2009;Kimura, 1961). However, in patients with stroke-inducedaphasia this tendency is often absent or even reversed. Aconsistent finding in studies of patients with stroke-induced aphasia, published primarily during the 1980s,was that they, unlike in healthy controls, often showed aleft ear advantage (LEA) during dichotic listening tasks(Crosson & Warren, 1981; Moore & Papanicolaou, 1988;Niccum & Speaks, 1991; Papanicolaou, Moore, Deutsch,Levin, & Eisenberg, 1988).
Even though longitudinal studies of ear advantage(EA) – as measured both before and after these kinds oflesions – are lacking, it has been assumed that this findingrepresents a change in EA produced by the stroke. Onepossible explanation for this change is that it mirrors ahemispheric shift with regard to certain language func-tions. According to this hypothesis, a compensatory reor-ganization of language functions takes place after a strokein the dominant hemisphere so that lost functions willgradually be compensated for by homologous areas inthe contralateral hemisphere (i.e., Crosson et al., 2007;Crosson & Warren, 1981; Moore & Papanicolaou, 1988).
However, based on longitudinal data collected duringthe first 6 months after a series of aphasia-induced strokes,
Niccum, Selnes, Speaks, Risse, and Rubens (1986) arguedagainst this interpretation. These authors concluded thattheir “data did not support the hypothesis that languagerecovery is mediated by a progressive shift in languagedominance from the left to the right hemisphere during thefirst 6 months post onset.” Instead, Niccum et al. (1986)suggested that the effect might be caused by lesions of theprimary auditory system rather than compensatorymechanisms. However, because recovery of languagefunction is a process that often continues over the firstyear after a lesion, it may be argued that short-term obser-vations do not settle the issue. It has consequently beenargued that an ideal study should follow patients long-itudinally for a longer period of time (Moore &Papanicolaou, 1992).
During the late 1990s, the subthalamic nucleus (STN)emerged as an increasingly popular target for treatmentwith deep brain stimulation (DBS) of advanced motorsymptoms of Parkinson’s disease (PD) (Deuschl et al.,2006; Weaver et al., 2009; Williams et al., 2010).Neuropsychological studies of the effects of STN DBS inPD patients have relatively consistently demonstratednegative effects on verbal fluency (Heo et al., 2008;Parsons, Rogers, Braaten, Woods, & Tröster, 2006;Weaver et al., 2009; York et al., 2008). The neurophysio-logical nature of the changes induced by DBS is not fullyunderstood but is most often believed to mimic the effectsof a lesion. Recent data indicate that unilateral STN DBSof the speech-dominant hemisphere is associated with sig-nificantly lower declines in measures of verbal fluency as
*Corresponding author. Email: [email protected]
Neurocase, 2014http://dx.doi.org/10.1080/13554794.2014.960427
© 2014 Taylor & Francis
Dow
nloa
ded
by [
Nor
rlan
ds U
nive
rsite
tssj
ukeh
us]
at 2
3:18
13
Oct
ober
201
4

compared to bilateral stimulation (Sjöberg et al., 2012).One possible explanation for these findings is that unilat-eral STN DBS allows for similar compensatory mechan-isms in the contralateral hemisphere as has been discussedas an explanation for shifts of ear preference in stroke-induced aphasia.
The purpose of the present study was to examine howunilateral DBS of the STN affects EA as measured pre-operatively and approximately 6 and 18 months postopera-tively. More specifically, we explored whether there wouldbe a tendency toward a shift in EA similar to that observedin stroke patients discussed earlier. A second aim was toinvestigate whether such an effect is immediate, which hasbeen described as consistent with a lesional hypothesis, ordevelops over time, as would be expected if the explana-tion is a reorganization of cortical networks.
Methods
Participants
The participants consisted of one woman and five men withPD who received unilateral electrode implantation on theleft STN. The mean age at the time of surgery was59.5 years (SD = 11.2). Mean time since PD diagnosiswas 5.2 years (SD = 2.8). (Data on age and time since PDdiagnosis were estimated by subtracting year of birth fromyear of PD diagnosis and year of surgery, respectively.)Further details on these patients have been presented bySjöberg et al. (2012). The preoperative mean score on themotor part of the Unified Parkinson’s Disease Rating Scale(UPDRS III) was 16.2 (SD = 7.2) with 29.8 (SD = 5.8)without medication. With medication and stimulation on,the UPDRS III score was 10 (SD = 5.5) at the 6-monthfollow-up and 13.2 (SD = 5.3) at the 18-month follow up.All patients were treated with Levodopa; five withPramipexole; four with Benserazide; three with Carbidopa,and one patient with Selegeline and Entacapone. Eachpatient was treated with virtually the same medicationsboth pre- and postoperatively. The indication for unilateralleft-sided DBS was in all patients right-sided hemi-parkin-sonistic symptoms and insufficient relief with pharmacolo-gical treatment. The patients were selected for unilateralprocedure on clinical grounds. They were considered bythe responsible surgeon as having dominating right-sidedmotor symptoms, which led to the decision of unilateralleft-sided STN DBS. The data included in this manu-script were obtained in compliance with the regulationsof our institution and the guidelines of the HelsinkiDeclaration.
Surgical procedure
Targets, coordinates, and trajectories for the stereotacticprocedures were derived from T2-weighted MR images
using the Frame Link planning station (Medtronic,Minneapolis, MN, USA). The target was chosen about1.5 mm lateral of the STN’s medial border, at the levelof the maximum diameter of the red nucleus and at a linejoining the anterior borders of these nuclei. The procedurewas performed with local anesthesia. Microelectroderecording was not used, but the effect of stimulationfrom the DBS electrode (model 3389, Medtronic,Minneapolis, MN, USA) was evaluated clinically duringthe procedure. A stereotactic CT was performed duringsurgery, and the images were fused with the preoperativeMRI for verification of electrode positions.
Dichotic listening test
Patients were, as part of a comprehensive neuropsycholo-gical evaluation that has previously been described else-where (Sjöberg et al., 2012), subjected to a dichoticlistening task preoperatively and at approximately 6 and18 months postoperatively. The Bergen Dichotic ListeningTask (Hugdahl & Asbjørnsen, 1994) consists of dichoticstimuli in the form of six different consonant-vowel sylla-bles (CV-syllables). Each CV-syllable is constructed fromthe vowel “a” in combination with the six stop-consonants“b,” “d,” “g,” “p,” “t,” and “k,” thus forming the followingsix basic CV-syllables: “ba,” “da,” “ga,” “pa,” “ta,” and“ka.” In making the dichotic pairs of stimuli, each syllableis combined with each of the other syllables including withitself, thus making a total of 6 × 6 = 36 dichotic pairs ofsyllables including six pairs with the same stimulus to boththe ears (homonyms) and 30 pairs with different syllablesto each ear, which are the “real” dichotic stimuli. Thehomonyms are used to get a check that the subject isable to correctly perceive each syllable when it is pre-sented in isolation, which is a prerequisite for adequateinterpretation of the dichotic results. The syllables are readby a synthetic, male, Swedish-sounding voice with intona-tion and intensity held constant. Each syllable has a dura-tion of approximately 350 ms, and there is a short intervalof approximately 4 s between each pair of syllables. Thisdichotic material is recorded three times with a pause ofapproximately 45 s between recordings. The pause allowsthe implementation of three different listening conditions –in this case a non-forced attention condition and twoforced attention conditions. The order of the dichoticpairs is randomized during each of the three recordings.In this study a compact disc (CD) produced by theSwedish Psykologiförlaget (2000) was used to presentthe material to the subjects with stereophonic earphones.
The test begins with the non-forced listening conditionin which the subject listens with “free floating” attentionand is simply instructed to report the syllable that isperceived most clearly after each pair. The accuracy ofthe reporting of the stimuli from each ear is calculated as a“percentage correct” score of the 30 dichotic stimuli to
2 R.L. Sjöberg et al.
Dow
nloa
ded
by [
Nor
rlan
ds U
nive
rsite
tssj
ukeh
us]
at 2
3:18
13
Oct
ober
201
4

each ear. The total from the non-forced condition is thepercentage correct score of the total number of dichoticitems presented to the right and left ear; that is,30 + 30 = 60 items. After the completion of the non-forcedcondition, it is possible to compute an “EA,” which isdefined as the difference of the percent correct score ofthe two ears. As previously mentioned, a right-handedindividual is expected to have a “right ear advantage”(REA) due to language dominance of the left hemisphere(Kimura, 1961). People with right-hemisphere dominancefor speech (e.g., left handers) are expected to show a LEA.In order to avoid false positives we followed recommen-dations by Professor Hugdahl (personal communication,14 February 2014), who developed the Bergen DichoticListening Task, by requiring at least a 10% differencebetween the two ears to establish a REA or LEA asindicative of language dominance for the contralateralhemisphere instead of relying on a smaller difference.
The non-forced condition is followed by a forced rightcondition in which the subject is instructed to pay attentiononly to the stimuli perceived in the right ear and onlyreport these stimuli. The last phase is the forced left con-dition in which the subject is instructed to pay attention toand report only the stimuli from the left ear. Hugdahl et al.(2009) argue that by varying instructions about attentionfocus, a cognitive conflict situation is set up that demandsa higher degree of cognitive control. The forced attentioncondition is thereby thought to involve a top-down mod-ulation of a bottom-up lateralized REA effect. The forced-left condition thus involves inhibitory control to a greaterextent than the forced-right condition and requires execu-tive attention in individuals showing a REA. The oppositeeffect should be expected in individuals with a LEA. Thethree conditions measure three different kinds of cognitiveprocesses: a lateralized perceptual process (nonforced con-dition), an attention process (forced-right), and an execu-tive cognitive control process (forced-left condition). Thenon-forced condition is the condition normally used todetermine speech lateralization. The results from theforced attention conditions are calculated as a percentcorrect score of the 30 dichotic stimuli presented to theright and left ear respectively.
Data analysis
An initial analysis by means of a 2 (right or left ear) × 3(testing preoperatively, and at 6 and 18 months postopera-tively) repeated measures ANOVAwas performed for boththe forced and the non-forced conditions, respectively. Ifeffects were found, these were further explored usingqualitative measures (mainly for non-forced EA) andpaired Student’s t-test for related samples. Our data onEA were of course parametric. However, because of thesmall number of observations, we also validated all ourreported t-tests with a non-parametric test (Wilcoxonsigned-rank test). The results were similar to thosereported in the manuscript. That is, all t-tests that werereported as significant were also significant with the non-parametric test, all t-tests that were non-significant werealso non-significant using the non-parametric test, and alltests that were reported as “not quite significant” (i.e.,p > .05 but p < .1) were at the same level of significanceusing the non-parametric test.
Results
Ear advantage in non-forced attention
An initial 2 × 3 ANOVA revealed a main effect of ear(F(5) = 68.957, p < 0.0001) and a significant interactionbetween ear and time of testing (F(4) = 17.968, p = 0.010).As seen in Table 1, the right ear performance tended todecrease over time, and by 18 months postoperativelythere had been a 29% change in REA (decrease of 14percentage points) from the preoperative test. However, atthis time there had also been a compensatory increase inthe left ear performance of 38% (9.4 percentage points)and as a consequence the REA shown at the group levelhad been reduced to only 1.1%.
When these trends were investigated with Student’st-test, the difference between the right and left ear condi-tions was significant preoperatively (t(5) = 3.194,p = 0.024) and at the 6-month follow-up (t(5) = 4.326,p = 0.008), whereas the 1.1% difference seen at the18-month follow-up was not significant.
Table 1. Means and standard deviations for right and left ear performances in forced and non-forced conditions during a dichoticlistening tasks for six Parkinson’s disease patients receiving deep brain stimulation of the left subthalamic nucleus.
Non-forced Forced
Mean (%) SD (%) Mean (%) SD (%)
Preoperatively Right ear 49.4 8.8 59.4 15.3Left ear 24.5 11.3 34.4 15.3
6 months postoperatively Right ear 46.1 12.4 53.3 19.3Left ear 23.3 4.2 37.7 17.4
18 months postoperatively Right ear 35.0 9.6 46.1 18.5Left ear 33.9 9.0 38.3 20.1
Note: Testing made preoperatively, and at 6 and 18 months postoperatively.
Neurocase 3
Dow
nloa
ded
by [
Nor
rlan
ds U
nive
rsite
tssj
ukeh
us]
at 2
3:18
13
Oct
ober
201
4
Regarding right ear performance deterioration over time,the difference between right ear performance preoperativelyand at the 6-month follow-up was not significant, whereasthe difference between the 6- and 18-month follow-ups wassignificant (t(5) = 3.627, p = 0.015). The difference betweenthe preoperative testing and the 18-month follow-up did notquite reach significance (t(5) = 2.025, p = 0.099).With regardto the increase in left ear performance, there was actually aslight, but non-significant deterioration between the preo-perative testing and the 6-month follow-up. However therewas a clear increase between the 6-month and 18-monthfollow-up that was significant (t(5) = –3.629, p = 0.015).The difference between the preoperative testing and the 18-month follow-up was close to significant (t(5) = –2.025,p = 0.099).
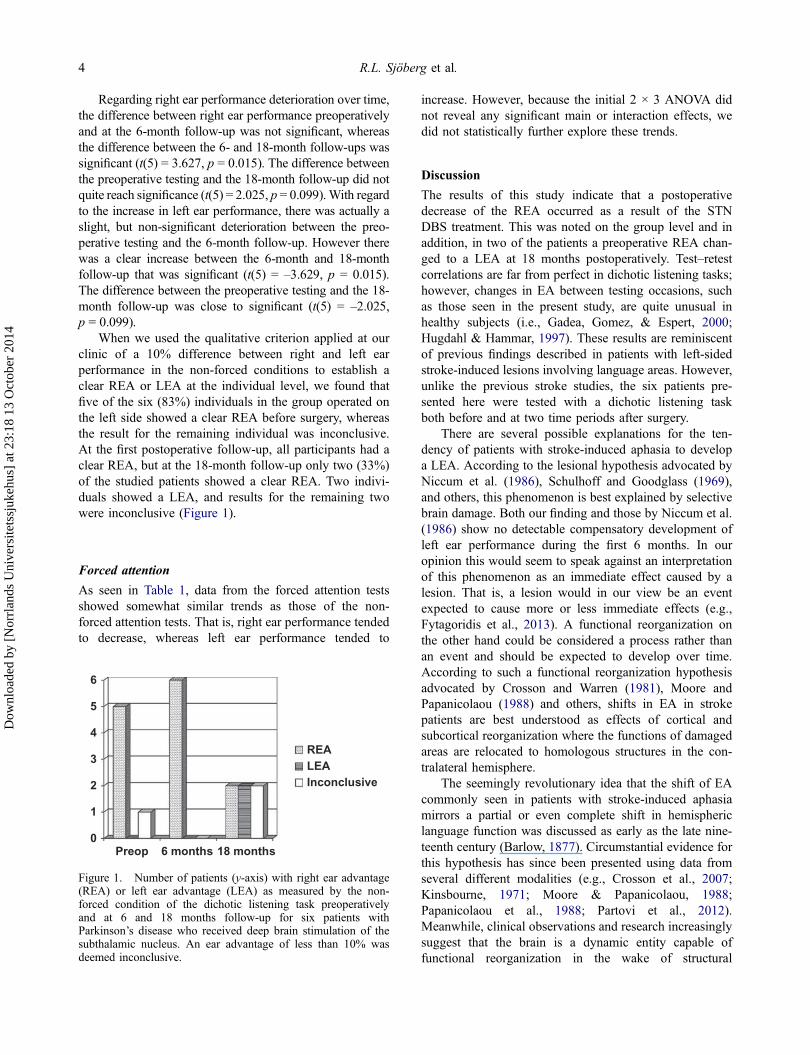
When we used the qualitative criterion applied at ourclinic of a 10% difference between right and left earperformance in the non-forced conditions to establish aclear REA or LEA at the individual level, we found thatfive of the six (83%) individuals in the group operated onthe left side showed a clear REA before surgery, whereasthe result for the remaining individual was inconclusive.At the first postoperative follow-up, all participants had aclear REA, but at the 18-month follow-up only two (33%)of the studied patients showed a clear REA. Two indivi-duals showed a LEA, and results for the remaining twowere inconclusive (Figure 1).
Forced attention
As seen in Table 1, data from the forced attention testsshowed somewhat similar trends as those of the non-forced attention tests. That is, right ear performance tendedto decrease, whereas left ear performance tended to
increase. However, because the initial 2 × 3 ANOVA didnot reveal any significant main or interaction effects, wedid not statistically further explore these trends.
Discussion
The results of this study indicate that a postoperativedecrease of the REA occurred as a result of the STNDBS treatment. This was noted on the group level and inaddition, in two of the patients a preoperative REA chan-ged to a LEA at 18 months postoperatively. Test–retestcorrelations are far from perfect in dichotic listening tasks;however, changes in EA between testing occasions, suchas those seen in the present study, are quite unusual inhealthy subjects (i.e., Gadea, Gomez, & Espert, 2000;Hugdahl & Hammar, 1997). These results are reminiscentof previous findings described in patients with left-sidedstroke-induced lesions involving language areas. However,unlike the previous stroke studies, the six patients pre-sented here were tested with a dichotic listening taskboth before and at two time periods after surgery.
There are several possible explanations for the ten-dency of patients with stroke-induced aphasia to developa LEA. According to the lesional hypothesis advocated byNiccum et al. (1986), Schulhoff and Goodglass (1969),and others, this phenomenon is best explained by selectivebrain damage. Both our finding and those by Niccum et al.(1986) show no detectable compensatory development ofleft ear performance during the first 6 months. In ouropinion this would seem to speak against an interpretationof this phenomenon as an immediate effect caused by alesion. That is, a lesion would in our view be an eventexpected to cause more or less immediate effects (e.g.,Fytagoridis et al., 2013). A functional reorganization onthe other hand could be considered a process rather thanan event and should be expected to develop over time.According to such a functional reorganization hypothesisadvocated by Crosson and Warren (1981), Moore andPapanicolaou (1988) and others, shifts in EA in strokepatients are best understood as effects of cortical andsubcortical reorganization where the functions of damagedareas are relocated to homologous structures in the con-tralateral hemisphere.
The seemingly revolutionary idea that the shift of EAcommonly seen in patients with stroke-induced aphasiamirrors a partial or even complete shift in hemisphericlanguage function was discussed as early as the late nine-teenth century (Barlow, 1877). Circumstantial evidence forthis hypothesis has since been presented using data fromseveral different modalities (e.g., Crosson et al., 2007;Kinsbourne, 1971; Moore & Papanicolaou, 1988;Papanicolaou et al., 1988; Partovi et al., 2012).Meanwhile, clinical observations and research increasinglysuggest that the brain is a dynamic entity capable offunctional reorganization in the wake of structural
0
1
2
3
4
5
6
Preop 6 months 18 months
REALEAInconclusive
Figure 1. Number of patients (y-axis) with right ear advantage(REA) or left ear advantage (LEA) as measured by the non-forced condition of the dichotic listening task preoperativelyand at 6 and 18 months follow-up for six patients withParkinson’s disease who received deep brain stimulation of thesubthalamic nucleus. An ear advantage of less than 10% wasdeemed inconclusive.
4 R.L. Sjöberg et al.
Dow
nloa
ded
by [
Nor
rlan
ds U
nive
rsite
tssj
ukeh
us]
at 2
3:18
13
Oct
ober
201
4

challenges and injuries (e.g., Benzagmout, Gatignol, &Duffau, 2007; Duffau, 2012; Hamilton, Chrysikou, &Coslett, 2011; Musso et al., 1999).
Even though our findings may be interpreted as con-sistent with a reorganizational hypothesis, it is of coursenot possible to pinpoint exactly if and, in such case, towhat extent such reorganization involves hemispherictransfer of specific language functions. Thus, perhaps themost important conclusion that can be drawn from ourresults is that additional longitudinal studies of patientswho have been subject to unilateral STN DBS procedures,for instance with functional MRI techniques, can provideuseful clues in understanding this issue. Another possibi-lity would be to do a similar study in on/off conditions todetermine the impact of DBS stimulation. However, ourresults indicate that there is considerable need of time forshift of EA to take place and short-term effects areunlikely.
Some limitations of our findings are that the main resultsrely on a few statistical analyses and, from a statistical pointof view, a limited number of patients. The small sample sizemay of course make the results sensitive to outliers but mayalso lead to false-negative findings because of a lack ofstatistical power to detect differences. It should also benoted that even though previous literature demonstrates thatchanges in ear performance on the individual level are unu-sual, we did not apply the dichotic testing procedures pre-sented in this study to non-operated PD controls. The lack ofa control group means that there is a theoretical possibilitythat the tendency of the right EA to disappear over time mayhave other causes than the surgery. One such possible causewould be aging.
Age effects in the dichotic listening task have previouslybeen reported. The results are to our knowledge inconclu-sive. This might be due to differences in study design anddifferent versions of the dichotic listening task have also beenused. Hugdahl et al. (2009) suggested that elderly individuals(aged 60 and above) show impaired performance in theforced-left condition, due to cognitive decline with regardto cognitive control and executive functioning. In the othertwo conditions (forced-right and non-forced) the elderlygroup showed no significant differences. A similar conclu-sion was drawn in a study by Gootjes, Van Strien, andBouma (2004), where an increased asymmetry was foundin the focused attention task in an elderly population. Thiswas however not seen in the non-forced attention condition,suggesting declined frontal activity in the elderly. Since wedetermined EA using the non-forced attention task, thesefindings are not directly relevant to our results. However, itshould be noted that Passow et al. (2012) found weaker orabsent REA in their study of attentional control of auditoryperception and suggested that this might be due to bilater-alized functional language networks and more perceptionallydriven behavior and less efficient attentional control in olderadults.
All patients received traditional medication for theirParkinson, both prior to surgery and after. This may ofcourse have an effect on neuropsychological tests of atten-tion. However, earlier studies on the same group ofpatients (Sjöberg et al., 2012) revealed no significantchanges on neuropsychological tests pre- or postopera-tively. As stated earlier, the dichotic listening task mea-sures three different kinds of cognitive processes: alateralized perceptual process, an attention process, andan executive cognitive control process. We only seechanges in the first lateralized perceptual condition. Thisis the condition during which EA as an indication ofspeech lateralization is commonly tested.
In sum, the result of the present study, which to ourknowledge is the first to longitudinally apply a dichoticlistening task to PD patients operated with left-sided STNDBS, demonstrated significant effects of the treatment on EAas measured with the dichotic listening task under the non-forced condition. This suggests the possibility that additionallongitudinal studies of this phenomenon could serve as amodel for understanding changes in indirect measures ofspeech lateralization in, for example, stroke patients.
Disclosure statementM.H. has received occasional travel expenses and honoraria fromMedtronic and St Jude for speaking at meetings. J.L. served onthe scientific advisory board for Glaxo Smith Kline, H Lundbeck,and Boehringer Ingelheim and received lecture honoraria fromMedtronic Inc., Solvay, Orion Pharma, UCB Pharma, and NordicInfu Care.
FundingThis work was supported by grants from Olle EngkvistByggmästare, the University of Umeå and the Foundation forClinical Neuroscience at the University Hospital of Umeå. M.H. issupported by the Edmond J. Safra Philanthropic Foundation, theMonument Trust and the Parkinsons Appeal, UK.
ReferencesBarlow, T. (1877). On a case of double hemiplegia, with cerebral
symmetrical lesions. The British Medical Journal, 2,103–104. doi:10.1136/bmj.2.865.103
Benzagmout, M., Gatignol, P., & Duffau, H. (2007). Resection ofWorld Health Organization Grade II gliomas involvingBroca’s area. Neurosurgery, 61, 741–753. doi:10.1227/01.NEU.0000298902.69473.77
Crosson, B., McGregor, K., Gopinath, K. S., Conway, T. W.,Benjamin, M., Chang, Y.-L., … White, K. D. (2007).Functional MRI of language in aphasia: A review of the litera-ture and the methodological challenges. NeuropsychologyReview, 17, 157–177. doi:10.1007/s11065-007-9024-z
Crosson, B., & Warren, R. L. (1981). Dichotic ear preference forC-V-C words in Wernicke’s and Broca’s aphasias. Cortex,17, 249–258. doi:10.1016/S0010-9452(81)80045-7
Deuschl, G., Schade-Brittinger, C., Krack, P., Volkmann, J.,Schäfer, H., Bötzel, K., … Voges, J. German ParkinsonStudy Group, Neurostimulation Section. (2006). A
Neurocase 5
Dow
nloa
ded
by [
Nor
rlan
ds U
nive
rsite
tssj
ukeh
us]
at 2
3:18
13
Oct
ober
201
4

randomized trial of deep-brain stimulation for Parkinson’sdisease. New England Journal of Medicine, 355, 896–908.doi:10.1056/NEJMoa060281
Duffau, H. (2012). The challenge to remove diffuse low-gradegliomas while preserving brain functions. ActaNeurochirurgica (Wien), 154, 569–574. doi:10.1007/s00701-012-1275-7
Fytagoridis, A., Sjöberg, R. L., Åström, M., Fredricks, A.,Nyberg, L., & Blomstedt, P. (2013). Effects of deep brainstimulation in the caudal zona incerta on verbal fluency.Stereotactic and Functional Neurosurgery, 91, 24–29.doi:10.1159/000342497
Gadea, M., Gomez, C., & Espert, R. (2000). Test-retest perfor-mance for the consonant-vowel dichotic listening test withand without attentional manipulations. Journal of Clinicaland Experimental Neuropsychology, 22, 793–803.doi:10.1076/jcen.22.6.793.959
Gootjes, L., Van Strien, J. W., & Bouma, A. (2004). Age effects inidentifying and localising dichotic stimuli: A corpus callosumdeficit? Journal of Clinical and Experimental Neuropsychology,26, 826–837. doi:10.1080/13803390490509448
Hamilton, R. H., Chrysikou, E. G., & Coslett, B. (2011).Mechanisms of aphasia recovery after stroke and the roleof noninvasive brain stimulation. Brain and Language, 118,40–50. doi:10.1016/j.bandl.2011.02.005
Heo, J.-H., Lee, K.-M., Paek, S. H., Kim, M.-J., Lee, J.-Y., Kim,J.-Y., … Jeon, B. S. (2008). The effects of bilateral subtha-lamic nucleus deep brain stimulation (STN DBS) on cogni-tion in Parkinson disease. Journal of the NeurologicalSciences, 273, 19–24. doi:10.1016/j.jns.2008.06.010
Hiscock, M., & Kinsbourne, M. (2011). Attention and the right-ear advantage: What is the connection? Brain & Cognition,76, 263–275. doi:10.1016/j.bandc.2011.03.016
Hugdahl, K., & Asbjørnsen, A. (1994). Dikotisk lyssning medCV-stavelser: Manual. Stockholm: Psykologiförlaget.
Hugdahl, K., & Hammar, Å. (1997). Test-retest reliability for theconsonant-vowel syllables dichotic listening paradigm.Journal of Clinical and Experimental Neuropsychology, 19,667–675. doi:10.1080/01688639708403752
Hugdahl, K., Westerhausen, R., Alho, K., Medvedev, S., Laine,M., & Hämäläinen, H. (2009). Attention and cognitive con-trol: Unfolding the dichotic listening story. ScandinavianJournal of Psychology, 50, 11–22. doi:10.1111/j.1467-9450.2008.00676.x
Kimura, D. (1961). Cerebral dominance and the perception ofverbal stimuli. Canadian Journal of Psychology, 15,166–171. doi:10.1037/h0083219
Kinsbourne, M. (1971). The minor cerebral hemisphere. Archivesof Neurology, 25, 302–306. doi:10.1001/archneur.1971.00490040028003
Moore, B. D., & Papanicolaou, A. C. (1988). Dichotic-listeningevidence of right-hemisphere involvement in recovery fromaphasia following stroke. Journal of Clinical andExperimental Neuropsychology, 10, 380–386. doi:10.1080/01688638808408246
Moore, B. D., & Papanicolaou, A. C. (1992). Dichotic listening inaphasics: Response to Niccum and Speaks. Journal of Clinicaland Experimental Neuropsychology, 14, 641–645. doi:10.1080/01688639208402851
Musso, M., Weiller, C., Kiebel, S., Müller, S. P., Bülau, P., &Rijntjes, M. (1999). Training-induced brain plasticity inaphasia. Brain, 122, 1781–1790. doi:10.1093/brain/122.9.1781
Niccum, N., Selnes, O. A., Speaks, C., Risse, G. L., & Rubens,A. B. (1986). Longitudinal dichotic listening patterns foraphasic patients III: Relationship to language and memoryvariables. Brain and Language, 28, 303–317. doi:10.1016/0093-934X(86)90107-0
Niccum, N., & Speaks, C. (1991). Interpretation of outcome ondichotic listening tests following stroke. Journal of Clinicaland Experimental Neuropsychology, 13, 614–628.doi:10.1080/01688639108401076
Papanicolaou, A. C., Moore, B. D., Deutsch, G., Levin, H. S., &Eisenberg, H. M. (1988). Evidence for right-hemisphereinvolvement in recovery from aphasia. Archives ofNeurology, 45, 1025–1029. doi:10.1001/archneur.1988.00520330117020
Parsons, T. D., Rogers, S. A., Braaten, A. J., Woods, S. P., &Tröster, A. (2006). Cognitive sequelae of subthalamicnucleus deep brain stimulation in Parkinson’s disease: Ameta analysis. The Lancet Neurology, 5, 578–588.doi:10.1016/S1474-4422(06)70475-6
Partovi, S., Jacobi, B., Rapps, N., Zipp, L., Karimi, S., Rengier,F., … Stippich, C. (2012). Clinical standardized fMRIreveals altered language lateralization in patients with braintumor. American Journal of Neuroradiology, 33, 2151–2157.doi:10.3174/ajnr.A3137
Passow, S., Westerhausen, R., Wartenburger, I., Hugdahl, K.,Heekeren, H. R., Lindenberger, U., & Li, S.-C. (2012).Human aging compromises attentional control of auditoryperception. Psychology and Aging, 27, 99–105.doi:10.1037/a0025667
Schulhoff, C., & Goodglass, H. (1969). Dichotic listening, sideof brain injury and cerebral dominance. Neuropsychologia,7, 149–160. doi:10.1016/0028-3932(69)90012-8
Sjöberg, R. L., Lidman, E., Häggström, B., Hariz, M. I., Linder,J., Fredricks, A., & Blomstedt, P. (2012). Verbal fluency inpatients receiving bilateral versus left-sided deep brain sti-mulation of the subthalamic nucleus for Parkinson’s disease.Journal of the International Neuropsychological Society, 18,606–611. doi:10.1017/S1355617711001925
Weaver, F. M., Follet, K., Stern, M., Hur, K., Harris, C., MarksJr., W. J., … Huang, G. D. (2009). Bilateral deep brainstimulation vs best medical therapy for patients withadvanced Parkinson disease: A randomized controlled trial.JAMA, 301, 63–73. doi:10.1001/jama.2008.929
Williams, A., Gill, S., Varma, T., Jenkinson, C., Quinn, N.,Mitchell, R., … Wheatley, K. (2010). Deep brain stimula-tion plus best medical therapy versus best medical therapyalone for advanced Parkinson’s disease (PD SURG trial):A randomised, open-label trial. The Lancet Neurology, 9,581–591. doi:10.1016/S1474-4422(10)70093-4
York, M. K., Dulay, M., Macias, A., Levin, H. S., Grossman,R., Simpson, R., & Jankovic, J. (2008). Cognitive declinesfollowing bilateral subthalamic nucleus deep brain stimu-lation for the treatment of Parkinson’s disease. Journal ofNeurology, Neurosurgery and Psychiatry, 79, 789–795.doi:10.1136/jnnp.2007.118786
6 R.L. Sjöberg et al.
Dow
nloa
ded
by [
Nor
rlan
ds U
nive
rsite
tssj
ukeh
us]
at 2
3:18
13
Oct
ober
201
4
Related Documents











