This article was downloaded by: [UVA Universiteitsbibliotheek SZ] On: 23 March 2015, At: 06:17 Publisher: Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Journal of Clinical Child & Adolescent Psychology Publication details, including instructions for authors and subscription information: http://www.tandfonline.com/loi/hcap20 Late-Onset PTSD in Unaccompanied Refugee Minors: Exploring the Predictive Utility of Depression and Anxiety Symptoms Geert E. Smid a , Gerty J. L. M. Lensvelt-Mulders b , Jeroen W. Knipscheer c a , Berthold P. R. Gersons d a & Rolf J. Kleber c a a Foundation Centrum ′45 b Department of Theory of Sciences and Methodology , University for Humanistics c Department of Clinical and Health Psychology , Utrecht University d Academic Medical Centre , Amsterdam Published online: 14 Sep 2011. To cite this article: Geert E. Smid , Gerty J. L. M. Lensvelt-Mulders , Jeroen W. Knipscheer , Berthold P. R. Gersons & Rolf J. Kleber (2011) Late-Onset PTSD in Unaccompanied Refugee Minors: Exploring the Predictive Utility of Depression and Anxiety Symptoms, Journal of Clinical Child & Adolescent Psychology, 40:5, 742-755, DOI: 10.1080/15374416.2011.597083 To link to this article: http://dx.doi.org/10.1080/15374416.2011.597083 PLEASE SCROLL DOWN FOR ARTICLE Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) contained in the publications on our platform. However, Taylor & Francis, our agents, and our licensors make no representations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of the Content. Any opinions and views expressed in this publication are the opinions and views of the authors, and are not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be relied upon and should be independently verified with primary sources of information. Taylor and Francis shall not be liable for any losses, actions, claims, proceedings, demands, costs, expenses, damages, and other liabilities whatsoever or howsoever caused arising directly or indirectly in connection with, in relation to or arising out of the use of the Content. This article may be used for research, teaching, and private study purposes. Any substantial or systematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in any form to anyone is expressly forbidden. Terms & Conditions of access and use can be found at http:// www.tandfonline.com/page/terms-and-conditions

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
This article was downloaded by: [UVA Universiteitsbibliotheek SZ]On: 23 March 2015, At: 06:17Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House,37-41 Mortimer Street, London W1T 3JH, UK
Journal of Clinical Child & Adolescent PsychologyPublication details, including instructions for authors and subscription information:http://www.tandfonline.com/loi/hcap20
Late-Onset PTSD in Unaccompanied Refugee Minors:Exploring the Predictive Utility of Depression andAnxiety SymptomsGeert E. Smid a , Gerty J. L. M. Lensvelt-Mulders b , Jeroen W. Knipscheer c a , Berthold P. R.Gersons d a & Rolf J. Kleber c aa Foundation Centrum ′45b Department of Theory of Sciences and Methodology , University for Humanisticsc Department of Clinical and Health Psychology , Utrecht Universityd Academic Medical Centre , AmsterdamPublished online: 14 Sep 2011.
To cite this article: Geert E. Smid , Gerty J. L. M. Lensvelt-Mulders , Jeroen W. Knipscheer , Berthold P. R. Gersons & Rolf J.Kleber (2011) Late-Onset PTSD in Unaccompanied Refugee Minors: Exploring the Predictive Utility of Depression and AnxietySymptoms, Journal of Clinical Child & Adolescent Psychology, 40:5, 742-755, DOI: 10.1080/15374416.2011.597083
To link to this article: http://dx.doi.org/10.1080/15374416.2011.597083
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) containedin the publications on our platform. However, Taylor & Francis, our agents, and our licensors make norepresentations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of theContent. Any opinions and views expressed in this publication are the opinions and views of the authors, andare not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be relied upon andshould be independently verified with primary sources of information. Taylor and Francis shall not be liable forany losses, actions, claims, proceedings, demands, costs, expenses, damages, and other liabilities whatsoeveror howsoever caused arising directly or indirectly in connection with, in relation to or arising out of the use ofthe Content.
This article may be used for research, teaching, and private study purposes. Any substantial or systematicreproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in anyform to anyone is expressly forbidden. Terms & Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions
Late-Onset PTSD in Unaccompanied RefugeeMinors: Exploring the Predictive Utility of
Depression and Anxiety Symptoms
Geert E. Smid
Foundation Centrum 045
Gerty J. L. M. Lensvelt-Mulders
Department of Theory of Sciences and Methodology, University for Humanistics
Jeroen W. Knipscheer
Department of Clinical and Health Psychology, Utrecht University andFoundation Centrum 045
Berthold P. R. Gersons
Academic Medical Centre, Amsterdam and Foundation Centrum 045
Rolf J. Kleber
Department of Clinical and Health Psychology, Utrecht University andFoundation Centrum 045
Following resettlement in Western countries, unaccompanied refugee minors (URM)are at risk of developing posttraumatic stress disorder (PTSD). It is unclear to whatextent PTSD in this group may become manifest at later stages following resettlementand which factors are associated with late onset. We examined data from URM col-lected 1 (T1) and 2 years (T2) following resettlement for differences between groups withno PTSD, PTSD at T1, and late-onset PTSD (at T2 only) using multinomial regressionand path analysis. Of the children and adolescents (ages 12–18) completing both assess-ments (N¼ 554), 223 (40%) met criteria for PTSD at T1, and 88 (16%) endorsedlate-onset PTSD. Late-onset PTSD was associated with traumatic event exposure, olderage, and low education. In the late-onset PTSD group, the predictive effects oftraumatic event exposure on symptom severity at T2 were fully mediated by depressionand anxiety symptoms at T1. These results suggest that late-onset PTSD is a clinicallyrelevant problem among URM that may be heralded by early depression and anxietysymptoms.
According to the Convention on the Rights of the Child(United Nations, 1989), states carry the responsibility topromote the psychological recovery of child victims ofarmed conflicts, torture, or abuse. Unaccompanied refu-gee minors (URM; hereafter also referred to as refugeeminors or simply minors) have been separated fromboth parents and other relatives and are at the time of
The studies were supported by Foundation Achmea Victim and
Society and the Netherlands Organization for Health Research and
Development (ZonMw).Correspondence should be addressed to Geert E. Smid, Foun-
dation Centrum ’45, Nienoord 5, 1112 XE Diemen, The Netherlands.
E-mail: [email protected]
Journal of Clinical Child & Adolescent Psychology, 40(5), 742–755, 2011
Copyright # Taylor & Francis Group, LLC
ISSN: 1537-4416 print=1537-4424 online
DOI: 10.1080/15374416.2011.597083
Dow
nloa
ded
by [
UV
A U
nive
rsite
itsbi
blio
thee
k SZ
] at
06:
17 2
3 M
arch
201
5
their asylum application not being cared for by an adultwho, by law or custom, is responsible for doing so(UNHCR, 2004). In 21 European countries, 63,500unaccompanied minors applied for asylum during 2000–2003, most of them originating from war-torn countries.The Netherlands received the largest number of unac-companied minors seeking asylum in Europe, followedby the United Kingdom and Austria (UNHCR, 2004).
Refugee minors have often repeatedly been exposedto potentially traumatic experiences and have sufferedpersonal losses, including loss of home, belongings,friends, and family (Derluyn & Broekaert, 2007; Lustiget al., 2004). They need to adapt to a new culture, theyhave limited access to resources, and their future issurrounded by great uncertainty (Guarnaccia & Lopez,1998). Furthermore, accomplishment of developmentaltasks (e.g., identity formation) may be impeded by theeffects of traumatic experiences as well as lack ofsupport and guidance (Ajdukovic & Ajdukovic, 1998).Refugee minors are therefore at increased risk of suffer-ing severe distress (Bean, Eurelings-Bontekoe, &Spinhoven, 2007). Knowledge regarding onset andcauses of psychological distress is essential for providingcare to this vulnerable group in order to enable earlydetection, secondary prevention, and treatment.
In refugees following resettlement in Western coun-tries, posttraumatic stress disorder (PTSD) is probablythe most prevalent serious mental disorder in adults aswell as children and adolescents (Fazel, Wheeler, &Danesh, 2005). In a landmark study of Cambodian ado-lescents who survived the Pol Pot concentration camps,late-onset PTSD was found as late as 14 years followingresettlement (Sack, Him, & Dickason, 1999). Accordingto the Diagnostic and Statistical Manual of Mental Disor-ders (4th ed., text rev. [DSM–IV–TR]), if the ‘‘onset ofsymptoms is at least six months after the stressor’’ in anindividual endorsing PTSD, a diagnosis of PTSD ‘‘withdelayed onset’’ must be given (American PsychiatricAssociation, 2000, p. 468). This diagnostic category high-lights the capacity of traumatic events to be associatedwith psychological complaints that may not manifestthemselves in the immediate aftermath of an event. Inrefugee minors, the timing of traumatic event exposureand the symptom course immediately following thisexposure may be impossible to establish, given the com-plex migration circumstances. Therefore, late-onset PTSDin refugee minorsmay be defined, consistent with previousliterature (Andrews, Brewin, Philpott, & Stewart, 2007;Sack et al., 1999; Smid, Mooren, Van der Mast, Gersons,& Kleber, 2009), as a progression of PTSD symptomsfollowing resettlement in the host country. In the currentstudy, we chose the term ‘‘late-onset’’ instead of ‘‘delayed’’to emphasize our long-term perspective.
The development of PTSD in children and adoles-cents can be explained using a longitudinal framework
comprising factors that operate on different times withregard to the traumatic event exposure. Thus, factorscan be divided into preexisting (e.g., demographic),trauma-related, and posttraumatic (postmigration) vari-ables. In addition, variables may be further dividedaccording to the level of evidence. Variables found tobe associated statistically with psychopathology maybe termed risk markers. In contrast, associated variablesfrom rigorously designed studies that explicitly studycausal relations and embed the variables under studyin a causal theory may be termed causal risk factors(Layne et al., 2010; Layne, Warren, Watson, & Shalev,2007). These variables may either have etiological sig-nificance or act as maintenance factors that cause per-sistence or exacerbation of psychopathology. Riskmarkers are useful for risk identification and can serveas candidates for rigorously designed studies that ident-ify causal risk factors. Established causal risk factorsprovide a solid basis for theory building, intervention,and social policy (Layne et al., 2007). In the presentstudy, variables found to be associated with late-onsetPTSD that have previously been shown to be causal riskfactors for PTSD in general across different populationswere considered candidate causal risk factors forlate-onset PTSD.
Previous analyses of a comprehensive sample ofURM showed that 44% of the variance in PTSD symp-toms in URM 2 years following resettlement could beexplained by older age; reported number of traumaticevents; and baseline symptoms of PTSD, depression,and anxiety (Bean, Eurelings-Bontekoe, et al., 2007).The association of older age with PTSD symptoms inURM has also been demonstrated in another study(Hodes, Jagdev, Chandra, & Cunniff, 2008). Advancingage may increase feelings of uncertainty about thefuture, as the legal status of URM will be reviewed atage 18 (Hodes et al., 2008). In addition, this last studyreported an association of female gender and PTSD inrefugee minors (Hodes et al., 2008). Girls generallyshowed increased vulnerability for PTSD followingexposure to potentially traumatic events (Tolin & Foa,2006), thus moderating risk for PTSD. Likewise, lowereducation has been shown to be a risk factor for PTSDacross a large number of studies (Brewin, Andrews, &Valentine, 2000). The association of cumulative traumawith symptoms of PTSD, often referred to as dose-response relationship, has been established in severalstudies of adolescent refugees (Derluyn & Broekaert,2007; Ellis, MacDonald, Lincoln, & Cabral, 2008;Hodes et al., 2008; Thabet, Abed, & Vostanis, 2004) aswell as other populations (Brewin et al., 2000; Ozer,Best, Lipsey, & Weiss, 2003).
A posttraumatic factor specific to refugee minors isthe amount and intensity of supervision and supportthat is determined by the residential setting in the new
LATE-ONSET PTSD IN REFUGEE MINORS 743
Dow
nloa
ded
by [
UV
A U
nive
rsite
itsbi
blio
thee
k SZ
] at
06:
17 2
3 M
arch
201
5

country. In a study among unaccompanied asylum-seeking minors, posttraumatic stress and depressivesymptoms were significantly higher among those inlow-support living arrangements (Hodes et al., 2008).
Depression and anxiety symptoms have been shownto be closely related to PTSD in adolescent refugees(Stein, Comer, Gardner, & Kelleher, 1999; Thabetet al., 2004). Specifically, in studies of adolescent refu-gees, traumatic event exposure was found to be moststrongly related to PTSD, whereas postmigration factorswere most strongly related to depression symptoms(Ellis et al., 2008; Heptinstall, Sethna, & Taylor, 2004).Therefore, an important question concerns the role ofdepression and anxiety symptoms in late-onset PTSD.The relationship of PTSD and depression symptomsover time has been examined in a sample of Gulf Warveterans using a prospective cross-lagged panel design(Erickson, Wolfe, King, King, & Sharkansky, 2001).In this study, a reciprocal relation between PTSD anddepression was found. Specifically, both early PTSDand early depression predicted PTSD and depression18 months later, and early symptoms mediated thepredictive effects of traumatic event exposure on latersymptoms (Erickson et al., 2001). Therefore, inlate-onset PTSD, as it is defined by low early PTSDsymptoms, it may be hypothesized that early symptomsof depression and anxiety may have incremental utilityin predicting later PTSD severity. These symptomscould serve as risk markers that can assist in identifyingand intervening early with at-risk youth.
The aim of the present study was (a) to call attentionto the high risk for trauma-related mental distress,including symptoms of PTSD, depression, and anxietyin refugee minors throughout the resettlement process;(b) to highlight the capacity of PTSD symptoms to pro-gress over time, as some youth who meet full diagnosticcriteria of PTSD at a later point in time do not meetthose criteria initially, placing them at risk for notreceiving supportive services that may reduce their (riskof) distress; (c) to identify markers of risk for late-onsetPTSD, thereby facilitating efforts at early risk detectionand triage to preventive mental health services; and last,(d) to build theory and inform social policy by identify-ing candidate causal risk factors that, given sufficientempirical evidence, may serve as targets for intervention.
We hypothesized that late-onset PTSD would beassociated with traumatic event exposure and withfactors, including older age and low education, thatmay convey an increased susceptibility to postmigrationstresses. In addition, we hypothesized that in late-onsetPTSD, early symptoms of depression and anxiety wouldbe predictive of PTSD severity 2 years following resettle-ment, such that predictive effects of traumatic exposureon PTSD severity would be mediated by early symptomsof depression and anxiety.
METHODS
Participants
From the total population of 12,000 URM younger thanage 17.5 years in the Netherlands, approximately 4,000children and adolescents, whose ages ranged from 11to 17.5 years and who had resided for at least 4 and atmost 24 months in the Netherlands, were randomlyselected from the national register of the child protectionagency ‘‘Nidos’’ in 2002. Information about the studyand permission waivers (available in translated versions)was sent to the guardians to discuss with the minors.Both the minor and his or her guardian needed to givewritten permission to participate. Roughly 2,300 formswere returned; 1,300 (57%) minors wished to participate.Of those who consented in participation, 280 did notparticipate for a wide range of practical reasons, suchas not having received the invitation, being ill, loosingthe way, or the interpreter being unavailable. An addi-tional 100 had been transferred and therefore did notparticipate. The final sample completing the first assess-ment (n¼ 920) was representative for the main charac-teristics of the total refugee minors population 12 to18 years old in 2002 in the Netherlands. Study parti-cipants were mainly boys (75%) and came from 46 coun-tries, most often Angola (43%), Sierra Leone (9%),China (9%), Guinea (7%), and Afghanistan (4%). Threefourths of study participants had no family in theNetherlands. Potentially traumatic events reported byat least two thirds of participants were loss of a lovedone (86%), other (not specified) stressful life events(75%), witnessing mistreatment (71%), forced separationfrom family (68%), experiencing war or armed conflict(68%), and physical mistreatment (67%).
Procedures
Three research assistants administered the question-naires to groups of 10 to 15 minors during 1 hr at schoolor at their residential setting. Assistants provided expla-nation and obtained additional demographic informa-tion from the participants. After 12 months, contactwas again sought with the same 920 minors who hadparticipated in the first assessment period. Of these,152 (16%) refused to participate again, 90 (10%) couldnot be contacted, and 85 (9%) had left to an unknowndestination; 582 (63%) adolescents completed the secondassessment. Refreshments (T1, or 1 year followingresettlement) and a gift certificate for the cinema (T2,or 2 years following resettlement), worth about $10,were given to the participants as a token of appreciationfor their participation. Ethical approval to conduct thestudy was given by the Medical Ethics Committee ofLeiden University Medical Center. Additional details
744 SMID ET AL.
Dow
nloa
ded
by [
UV
A U
nive
rsite
itsbi
blio
thee
k SZ
] at
06:
17 2
3 M
arch
201
5

about the sample have been published elsewhere (Bean,Eurelings-Bontekoe, Mooijaart, & Spinhoven, 2006;Bean, Eurelings-Bontekoe, et al., 2007).
Measures
It was necessary tomakemodifications to existing standar-dized instruments to make them both adolescent friendlyand more cross-culturally valid. Instead of using onlywords for the rating scale (see next), colored circles thatincreased in size were presented as well. The items werecomposed using a vocabulary list for 12- to 15-year-oldsto make the questionnaires suitable for the reading levelof this population. Data supporting the validity of thesemodified instruments have been published elsewhere(Bean, Derluyn, Eurelings-Bontekoe, Broekaert, &Spinhoven, 2007b; Bean, Derluyn, Eurelings-Bontekoe,Broekaert, & Spinhoven, 2006). The questionnaires wereavailable in 19 different languages: Dutch, Albanian,Amharic, Arabic, Badini, Chinese (Mandarin), Dari,English, Farsi, French, German, Mongolian, Portuguese,Russian, Servo-Croatian, Somali, Sorani, Spanish, andTurkish. All language versions were bilingual: The foreignlanguage was featured in the first column, and Dutch wasused in the second column.
Demographic variables. Demographic variables,including gender, age, residential setting, and date ofarrival in the Netherlands, were recorded, and infor-mation concerning the number of education years wasobtained at T1. For the present study, we made a dis-tinction between minors reporting 3 years or less ofeducation (23% of the sample) and those reporting 4or more education years. In addition, an interview aboutreceiving mental health care was conducted. For thepresent analysis, we included only T2 responses to thequestion: Have you been to a ‘‘(mental) health pro-fessional’’ (for your emotional problems)? Data onobtaining temporary residence permits at T2 werecollected from the legal guardians of the URM andwere missing for 217 cases at T2 notwithstanding threereminders on three separate occasions to the guardianto send this information via their supervisor.
Anxiety and depression. The 25-items version ofthe Hopkins Symptoms Checklist is a widely usedscreening instrument consisting of 10 items for anxietysymptoms and 15 items for depression symptoms. Thescale for each question includes four categories ofresponse, ranging 1 (never), 2 (sometimes), 3 (often),and 4 (always). Because its first translation (Mollica,Wyshak, de Marneffe, Khuon, & Lavelle, 1987), theHopkins Symptoms Checklist–25 has been used innumerous studies of refugees, including adolescent
populations (e.g., Mghir, Freed, Raskin, & Katon,1995). Cronbach’s alpha for the Hopkins SymptomsChecklist–25 in our sample was 0.92. The scale hasbeen adapted for refugee adolescents and demon-strated good validity as well as invariance of factorstructure despite sample heterogeneity (Bean, Derluyn,et al., 2007b).
Stressful life events. The Stressful Life Events(SLE) checklist (Bean, Derluyn, et al., 2006; Spinhoven,Bean, & Eurelings-Bontekoe, 2006) consists of 12dichotomous (yes=no) questions and an open questionon the occurrence of stressful life events of relevancefor refugee minors (e.g., ‘‘Have you ever experienced awar or an armed military conflict going on around youin your country of birth?’’ or ‘‘Has someone ever hit,kicked, shot at or some other way tried to physicallyhurt you?’’). Having experienced a traumatic event isthe first diagnostic criterion for PTSD according to theDSM–IV–TR (APA, 2000). We assessed traumatic eventexposure by summing affirmative responses to SLEitems at the first assessment to yield the number of typesof traumatic events endorsed. We evaluated eventendorsement consistency by examining whether eachendorsed event was endorsed consistently across bothassessments. Items endorsed at T2 only were termedcommissions (Spinhoven et al., 2006). Given the vulner-ability of the minors, we strove to reduce the emotionalimpact of research participation. The brevity of the SLEtakes into account the importance of not overburdeningapprehensive adolescents.
PTSD. The Reactions of Adolescents to TraumaticStress (RATS; Bean, Derluyn, et al., 2006) is a self-report questionnaire developed to assess posttraumaticstress reactions with culturally diverse adolescents. TheRATS consists of 22 items that correspond directly tothe intrusion, numbing=avoidance, and hyperarousalcriteria of the DSM–IV–TR for PTSD (APA, 2000).The items are scored on a 4-point Likert scale, ranging1 (not), 2 (a little), 3 (much), and 4 (very much). Parti-cipants are instructed to report if they have beenbothered by symptoms during the past 4 weeks. Parti-cipants are explained that questions involve problemsyoung people may have after stressful life events. Ques-tionnaire items refer to ‘‘the events.’’ Six items (1–6)correspond to the intrusion symptom cluster, nine items(7–15) correspond to the avoidance=numbing symptomcluster, and seven items (16–22) correspond to thehyperarousal symptom cluster. The psychometricproperties of the RATS demonstrate invariance offactor structure in a heterogeneous sample, strongreliability, and good validity, which are remarkable con-sidering the diversity of the populations (Bean, Derluyn,et al., 2006). Cronbach’s alpha of the RATS was 0.91.
LATE-ONSET PTSD IN REFUGEE MINORS 745
Dow
nloa
ded
by [
UV
A U
nive
rsite
itsbi
blio
thee
k SZ
] at
06:
17 2
3 M
arch
201
5

In the present study, administration of the RATSimmediately followed administration of the SLE check-list. Posttraumatic stress symptom (PTSS) severity wascalculated by summing responses to all RATS items.For the present analysis, a probable diagnosis of PTSDaccording to DSM criteria was given if participants (a)endorsed at least one stressful life event on the SLEand (b) on the RATS scored 3 (much) or 4 (very much)on at least one item of the intrusion cluster, on at leastthree items in the avoidance and numbing cluster, andon at least two items in the hyperarousal cluster. Thisscoring method is known as symptom cluster methodof scoring (Brewin, 2005). In a recent study (Elhaiet al., 2009), measurement invariance testing revealedthat no substantial differences in PTSD factor structureexist if PTSD is assessed in trauma-exposed participantswith versus without reference to a single, worst trau-matic event.
Data Analyses
Descriptive analyses. Preceding the final analyses,we compared study participants who completed bothassessments with those who dropped out from the studyfollowing the T1 assessment using chi-square testsfor categorical variables and independent t tests forcontinuous variables. We divided the sample into threeoutcome groups: participants never meeting probablePTSD criteria (no PTSD group), those meeting probablePTSD criteria at T1 (PTSD-T1 group), and those meet-ing those criteria only at T2 (late-onset PTSD group).The PTSD-T1 group included cases who also met prob-able PTSD criteria at T2 as well as cases who no longermet those criteria at T2. We listwise deleted data ofstudy completers whose PTSD status at either T1 orT2 could not be established due to missing data. Specifi-cally, we deleted incomplete cases whose responses weremissing to all RATS items at T1 (n¼ 25) or T2 (n¼ 1) orwho endorsed sufficient items in one or two PTSDsymptom clusters to meet probable PTSD criteria butwhose responses to all items in the remaining PTSDsymptom clusters were missing at T1 (n¼ 1) or T2(n¼ 1). Thus, of 582 study participants completing bothassessments, 554 provided sufficient data to establishprobable PTSD status at both times.
To ascertain the validity of the late-onset PTSD diag-nosis in our sample, we examined late-onset PTSD casesendorsing one or more stressful life events at T2 only(commissions) for the presence at T1 of subthresholdPTSD, defined as meeting one or two PTSD criteria.As late-onset PTSD is most likely to occur in individualsalready endorsing prodromal subthreshold PTSD symp-toms (Andrews et al., 2007; Smid et al., 2009), thesesymptoms indicate a likely relationship between eventsreported at T1 and symptoms of PTSD at T2. We
compared the three outcome groups using chi-squaretests for categorical variables and analysis of variancefor continuous variables.
Multinomial regression analysis. To identify mar-kers of risk of late-onset PTSD, we applied multinomialregression analyses with the three outcome groups asdependent variable. The no-PTSD and PTSD-T1 groupsacted as reference groups for comparison with thelate-onset PTSD group. These analyses produced oddsratios and 95% confidence intervals for the associationsof each variable adjusted for the influence of all theother variables. Cases with missing values in any multi-nomial regression model variable (N¼ 18 of 554) werenot included in the analysis. We evaluated model fitusing the model chi-square and pseudo-R2 (Nagelkerke).We screened the data for absence of multicollinearity bycalculating tolerance values. In our final multinomialregression model, no indication of multicollinearitywas found (tolerance �0.6). Because of the small samplesize of the late-onset PTSD group, we limited thenumber of independent variable categories by dichoto-mizing the variables education into 3 years or less and4 years or more (see Measures section) and age at themedian value (16 years). The overall effect of each inde-pendent variable on outcome group membership wasassessed using likelihood ratio tests.
Path analysis. We used path analysis to confirm inour sample the relations over time between traumaticevent exposure, symptoms of depression=anxiety, andPTSS severity as previously found in a different popu-lation (Erickson et al., 2001). We included covariatesin the model that in previous analyses (Bean, Eurelings-Bontekoe, et al., 2007) accounted for a high percentageof the variance in PTSS severity, specifically, age, and avariable related to the type of residential setting. Theminors were housed in five types of residential settingdiffering in both the available amount and the intensityof supervision, listed hereafter in increasing order: inde-pendent (with no routine supervision), large-scale recep-tion centre, living units (4-hr daily supervision), livinggroups (24-hr daily supervision), and nonkinship or kin-ship foster care. Because both the amount and the inten-sity of supervision increased across these different typesof housing, we treated the ordered categorical variableas a scale variable termed ‘‘supervision’’ with levels ran-ging from 1 to 5. We specified a model according to thefollowing theoretical assumptions:
1. The number of reported traumatic events at T1(exposure) predicts PTSS severity and depression=anxiety at T1.
746 SMID ET AL.
Dow
nloa
ded
by [
UV
A U
nive
rsite
itsbi
blio
thee
k SZ
] at
06:
17 2
3 M
arch
201
5

3. Age covaries with exposure and predicts intensityof supervision (with advancing age, less super-vision will be offered).
4. Age influences PTSS severity and depression=anxiety at T2 (Bean, Eurelings-Bontekoe, et al.,2007; Hodes et al., 2008).
5. Supervision level (assessed at T1) predicts PTSSseverity and depression=anxiety at T1.
6. PTSS severity and depression=anxiety havecross-lagged relations over time, with correlatedresiduals (Erickson et al., 2001).
We screened our data for the presence of multivariatenonnormality by calculating multivariate kurtosis(Mardia, 1970) across five completed data sets obtainedby stochastic regression imputation. Multivariate kurtosisranged from 4.1 to 5.1, indicating moderate multivariatenonnormality. To test robustness of the maximum likeli-hood (ML) estimation method against normality viola-tions in our data, we applied bootstrapping (250iterations). We calculated differences between ML andbootstrap estimates and standard errors and found theseto be negligible. We used Bollen-Stine bootstrap (2,000iterations) to examine how nonnormality affected theML chi-square statistic and found that Bollen-Stine pvalues and asymptotic p values were very close (Bollen& Stine, 1992). We concluded that the ML estimationmethod was robust against normality violations in ourdata. We therefore chose to handle missing data usingthe full information maximum likelihood procedure(Enders & Bandalos, 2001) and to present ML estimatesusing the full sample (Nmax¼ 920). We evaluated modelfit using the discrepancy chi-square, root mean squareerror of approximation, comparative fit index, non-normed fit index, and Akaike information criterion.
Multiple group analysis. Using multiple groupanalysis, we explored whether late-onset PTSD groupmembership moderates the relations over time betweendepression=anxiety and PTSD symptoms. Specifically,we sought to answer the question of whether earlysymptoms of depression and anxiety are predictive oflater PTSD severity in late-onset PTSD. In multiplegroup analysis, a model is estimated simultaneouslyacross groups. Through the specification of cross-groupequality constraints, group differences on any individualparameter or set of parameters can be tested (Joreskog,1971; Kaplan, 2008; Kline, 2004). The fit of the modelwith parameters constrained to be equal across thegroups is compared with that of the unrestricted modelwith the chi-square difference (Dv2) statistic. If thechi-square difference is statistically significant, and ifgroup differences in values of the unstandardized pathcoefficients are meaningful, then the hypothesis of equaldirect effects may be rejected (Kline, 2004). Joreskog
(1971) suggested a strategy for assessing the comparabil-ity of factor structures between groups based on a seriesof tests of increasingly restricted hypotheses. This mod-eling strategy can be extended to the general structuralequation model (Kaplan, 2008). Thus, we examineddifferences in direct effects between the PTSD-T1 andlate-onset PTSD groups by applying the path analysismodel to these two groups simultaneously and subse-quently testing models corresponding to increasinglyrestricted hypotheses. Initially, all paths were freely esti-mated within groups. We added cross-group equalityconstraints stepwise according to specified hypotheses:(a) exposure, age, and supervision effects are equalacross PTSD-T1 and late-onset PTSD groups; (b) effectsof depression=anxiety T1 are equal across groups; (c)effects of PTSS severity T1 are equal across groups;and (d associations between residuals are equal acrossgroups. Nonsignificant paths in one group were deletedfrom the final multiple group model to increase modelparsimony. All analyses were carried out using softwareprovided by SPSS and Amos, versions 15.0 and 17.0.
RESULTS
Attrition and Prevalence of Late-Onset PTSD
The attrition group was older than the retained sample(16.1 vs. 15.5 years, 95% confidence intervals of differ-ence, .40–.80, p< .001). Older minors were more difficultto find for the T2 assessment because many were nolonger registered. Participants in a residential settingcharacterized by less residential supervision (living inde-pendent or in a large-scale reception centre) were alsomore likely to drop out than those receiving more super-vision, v2(1)¼ 16.4, p< .001. The mean ages for the dif-ferent types of residential settings of the attrition groupand the T2 sample were significantly different from eachother. This could explain, in part, why significant differ-ences were found between the lost and retained samplesfor residential setting.
Of the final sample completing both assessments(N¼ 554), 223 (40%) minors met criteria for probablePTSD at the first assessment. Of these, 82 met criteriathe first assessment only, and the remaining 141 metcriteria at both assessments. Eighty-eight (16%) metcriteria for probable PTSD only at the second assess-ment and were thus considered to endorse late-onsetPTSD. Thus, the prevalence rate of probable PTSDequaled 41% at the second assessment, and so this ratedid not decrease over time. Of all minors meeting cri-teria for probable PTSD at either one or both assess-ments, 28% endorsed late-onset PTSD. Of minorsendorsing late-onset PTSD, 25 (28%) met one and52 (59%) met two symptom criteria for PTSD at T1indicating subthreshold PTSD.
LATE-ONSET PTSD IN REFUGEE MINORS 747
Dow
nloa
ded
by [
UV
A U
nive
rsite
itsbi
blio
thee
k SZ
] at
06:
17 2
3 M
arch
201
5

Validity of Late-Onset PTSD
Given our study aim to build theory related to late-onsetPTSD, we needed to ascertain the validity of ourresearch diagnosis of late-onset PTSD. Central to adiagnosis of late-onset PTSD is the presumed relationbetween PTSD symptoms and a remote traumatic event(for a diagnosis of delayed onset, the DSM requires atleast 6 months to have passed between the event andthe onset of the disorder). If stressful events interveneduring the interval between the traumatic event andthe onset of the disorder, this relation must still beapparent. Consequently, the relation between earlierevents and late-onset PTSD should pertain to all indi-vidual cases in our study, and increases in PTSD symp-toms should not solely be accounted for by possiblyintervening traumatic events. We therefore examinedwhether late-onset PTSD could be related to possiblyintervening events endorsed at T2 only. In our sample,27 of 88 (31%) late-onset PTSD cases at T2 exclusivelyendorsed events that they had already endorsed at T1.In 52 (59%) other late-onset PTSD cases in which theindividual did endorse one or several events only at T2(commissions), the presence at T1 of subthresholdPTSD (i.e., meeting one or two PTSD symptom criteria)indicated a likely relationship between events reportedat T1 and symptoms of PTSD at T2.
Nine remaining minors in the late-onset PTSD groupendorsed at least one event at T2 only without endorsingsubthreshold PTSD at T1. In three of these ninecases, the number of consistently reported events out-weighed the number of events only reported at T2,and therefore these consistently reported events werelikely to be related to the PTSD symptoms reported atT2. In three other cases, the newly reported events atT2 included experiencing war, indicating inconsistentreporting instead of intervening events. In the remainingthree cases, the large number of missing responses on theSLE and=or RATS questionnaire prevented anyconclusion from being drawn regarding the possibilitythat they might endorse PTSD primarily related to inter-vening events. An example is a 14-year-old girl who atT1 did not endorse a single event but at T2 endorsedthe death of a loved one and a life-threatening medicalproblem. At T1, this girl on the RATS very muchendorsed one avoidance=numbing symptom (‘‘I try notto think or to talk about the event(s)’’) and muchendorsed one hyperarousal symptom (‘‘I have angryoutbursts (so angry that I throw things, hit, kick, orscream)’’). Given the clear endorsement of avoidanceof thoughts, the girl appeared to have underreportedstressful life events at T1, possibly motivated by a wishto avoid confrontation with distressing memories.
In sum, the diagnostic validity of late-onset PTSDappeared to be well supported in the large majority of
cases, in which individuals did not report any new eventat T2 and=or met one or two symptom criteria for PTSDat T1. A detailed examination of nine less certainlate-onset PTSD cases did not provide indications thatthe individuals endorsed PTSD primarily related topostmigration events.
Factors Associated with Late-Onset PTSD
Characteristics of the three outcome groups are shownin Table 1. Of particular interest is the associationbetween late-onset PTSD and having received help atT2. Compared with the no PTSD group, the late-onsetPTSD group was more likely to report having receivedhelp at T2, v2(1)¼ 11.8, p< .001. In addition, theabsence of an association between late-onset PTSDand (not) having a residence permit is of note. Finally,the number of stressful life events reported at T2 only(commissions) was not associated with late-onset PTSD.
Table 2 shows specific associations between preexis-tent, trauma-related, and posttraumatic variables, onone hand, and late-onset PTSD, on the other hand,corrected for the effects of all other included variablesin the multivariate multinomial regression model. Ofthe demographic variables, age and education level wereassociated with late-onset PTSD. Specifically, minorsage 16 years or older were more likely to endorselate-onset PTSD than no PTSD, and minors reporting3 or fewer years of education were more likely to belongto the late-onset PTSD group than to the PTSD-T1group. A trend existed for girls to be more likely tobelong to the late-onset group than to the no PTSDgroup. Exposure to traumatic events was reported moreoften in the late-onset PTSD group than in the no PTSDgroup. However, the late-onset PTSD group reportedfewer traumatic events than the PTSD-T1 group.
Path Analysis of Depression=Anxiety inLate-Onset PTSD
Figure 1 illustrates the results of the path analysis, withstandardized coefficients given for each model para-meter. Proportions of explained variance are given foreach endogenous (i.e., dependent) variable. The modelis a cross-lagged panel model (Erickson et al., 2001),comprising two symptom outcomes (PTSS severity anddepression=anxiety) at two times, and three influencingvariables (exposure, age, and supervision). All fit indicesshowed good model fit. The results indicated three directpaths to PTSS severity at T2 from age, PTSS severity atT1, and depression=anxiety at T1. They also showedseveral indirect paths to PTSS severity at T2 fromexposure and supervision. More specifically, PTSSseverity at T1 and depression=anxiety at T1 served as
748 SMID ET AL.
Dow
nloa
ded
by [
UV
A U
nive
rsite
itsbi
blio
thee
k SZ
] at
06:
17 2
3 M
arch
201
5
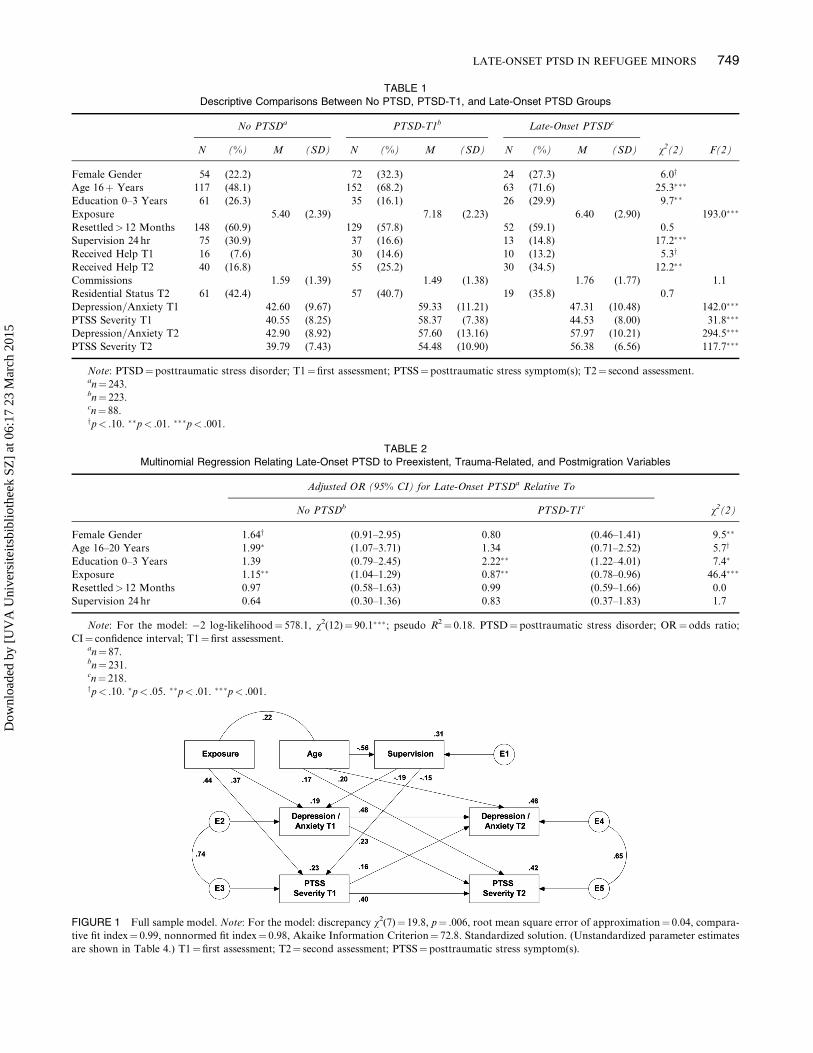
TABLE 1
Descriptive Comparisons Between No PTSD, PTSD-T1, and Late-Onset PTSD Groups
No PTSDa PTSD-T1b Late-Onset PTSDc
N (%) M (SD) N (%) M (SD) N (%) M (SD) v2(2) F(2)
Female Gender 54 (22.2) 72 (32.3) 24 (27.3) 6.0y
Age 16þ Years 117 (48.1) 152 (68.2) 63 (71.6) 25.3���
Education 0–3 Years 61 (26.3) 35 (16.1) 26 (29.9) 9.7��
Exposure 5.40 (2.39) 7.18 (2.23) 6.40 (2.90) 193.0���
Resettled> 12 Months 148 (60.9) 129 (57.8) 52 (59.1) 0.5
Supervision 24 hr 75 (30.9) 37 (16.6) 13 (14.8) 17.2���
Received Help T1 16 (7.6) 30 (14.6) 10 (13.2) 5.3y
Received Help T2 40 (16.8) 55 (25.2) 30 (34.5) 12.2��
Commissions 1.59 (1.39) 1.49 (1.38) 1.76 (1.77) 1.1
Residential Status T2 61 (42.4) 57 (40.7) 19 (35.8) 0.7
Depression=Anxiety T1 42.60 (9.67) 59.33 (11.21) 47.31 (10.48) 142.0���
PTSS Severity T1 40.55 (8.25) 58.37 (7.38) 44.53 (8.00) 31.8���
Depression=Anxiety T2 42.90 (8.92) 57.60 (13.16) 57.97 (10.21) 294.5���
PTSS Severity T2 39.79 (7.43) 54.48 (10.90) 56.38 (6.56) 117.7���
Note: PTSD¼ posttraumatic stress disorder; T1¼first assessment; PTSS¼posttraumatic stress symptom(s); T2¼ second assessment.an¼ 243.bn¼ 223.cn¼ 88.yp< .10. ��p< .01. ���p< .001.
TABLE 2
Multinomial Regression Relating Late-Onset PTSD to Preexistent, Trauma-Related, and Postmigration Variables
Adjusted OR (95% CI) for Late-Onset PTSDa Relative To
No PTSDb PTSD-T1c v2(2)
Female Gender 1.64y (0.91–2.95) 0.80 (0.46–1.41) 9.5��
Age 16–20 Years 1.99� (1.07–3.71) 1.34 (0.71–2.52) 5.7y
Education 0–3 Years 1.39 (0.79–2.45) 2.22�� (1.22–4.01) 7.4�
Exposure 1.15�� (1.04–1.29) 0.87�� (0.78–0.96) 46.4���
Resettled> 12 Months 0.97 (0.58–1.63) 0.99 (0.59–1.66) 0.0
Supervision 24 hr 0.64 (0.30–1.36) 0.83 (0.37–1.83) 1.7
Note: For the model: �2 log-likelihood¼ 578.1, v2(12)¼ 90.1���; pseudo R2¼ 0.18. PTSD¼ posttraumatic stress disorder; OR¼odds ratio;
CI¼ confidence interval; T1¼first assessment.an¼ 87.bn¼ 231.cn¼ 218.yp< .10. �p< .05. ��p< .01. ���p< .001.
FIGURE 1 Full sample model. Note: For the model: discrepancy v2(7)¼ 19.8, p¼ .006, root mean square error of approximation¼ 0.04, compara-
tive fit index¼ 0.99, nonnormed fit index¼ 0.98, Akaike Information Criterion¼ 72.8. Standardized solution. (Unstandardized parameter estimates
are shown in Table 4.) T1¼first assessment; T2¼ second assessment; PTSS¼posttraumatic stress symptom(s).
LATE-ONSET PTSD IN REFUGEE MINORS 749
Dow
nloa
ded
by [
UV
A U
nive
rsite
itsbi
blio
thee
k SZ
] at
06:
17 2
3 M
arch
201
5
mediators between exposure and PTSS severity at T2.In addition, supervision served as a mediator betweenage and PTSS severity at T1 as well as depression=anxiety at T1, and the effects of supervision on PTSSseverity at T2 were fully mediated by depression=anxietyat T1 and PTSS severity at T1, respectively. Depression=anxiety at T1 served as a partial mediator of supervisioneffects on PTSS severity at T2.
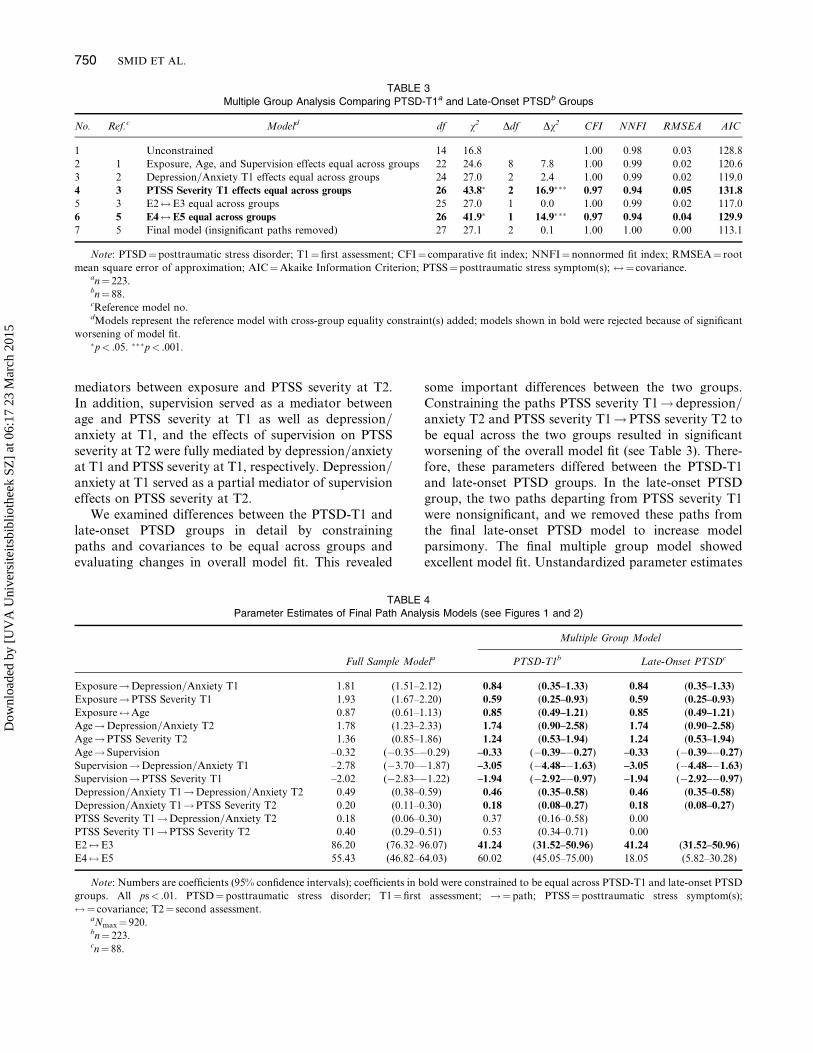
We examined differences between the PTSD-T1 andlate-onset PTSD groups in detail by constrainingpaths and covariances to be equal across groups andevaluating changes in overall model fit. This revealed
some important differences between the two groups.Constraining the paths PTSS severity T1! depression=anxiety T2 and PTSS severity T1!PTSS severity T2 tobe equal across the two groups resulted in significantworsening of the overall model fit (see Table 3). There-fore, these parameters differed between the PTSD-T1and late-onset PTSD groups. In the late-onset PTSDgroup, the two paths departing from PTSS severity T1were nonsignificant, and we removed these paths fromthe final late-onset PTSD model to increase modelparsimony. The final multiple group model showedexcellent model fit. Unstandardized parameter estimates
TABLE 3
Multiple Group Analysis Comparing PTSD-T1a and Late-Onset PTSDb Groups
No. Ref.c Modeld df v2 Ddf Dv2 CFI NNFI RMSEA AIC
1 Unconstrained 14 16.8 1.00 0.98 0.03 128.8
2 1 Exposure, Age, and Supervision effects equal across groups 22 24.6 8 7.8 1.00 0.99 0.02 120.6
3 2 Depression=Anxiety T1 effects equal across groups 24 27.0 2 2.4 1.00 0.99 0.02 119.0
4 3 PTSS Severity T1 effects equal across groups 26 43.8� 2 16.9��� 0.97 0.94 0.05 131.8
5 3 E2$E3 equal across groups 25 27.0 1 0.0 1.00 0.99 0.02 117.0
6 5 E4$E5 equal across groups 26 41.9� 1 14.9��� 0.97 0.94 0.04 129.9
7 5 Final model (insignificant paths removed) 27 27.1 2 0.1 1.00 1.00 0.00 113.1
Note: PTSD¼ posttraumatic stress disorder; T1¼ first assessment; CFI¼ comparative fit index; NNFI¼ nonnormed fit index; RMSEA¼ root
mean square error of approximation; AIC¼Akaike Information Criterion; PTSS¼posttraumatic stress symptom(s); $¼ covariance.an¼ 223.bn¼ 88.cReference model no.dModels represent the reference model with cross-group equality constraint(s) added; models shown in bold were rejected because of significant
worsening of model fit.�p< .05. ���p< .001.
TABLE 4
Parameter Estimates of Final Path Analysis Models (see Figures 1 and 2)
Multiple Group Model
Full Sample Modela PTSD-T1b Late-Onset PTSDc
Exposure!Depression=Anxiety T1 1.81 (1.51–2.12) 0.84 (0.35–1.33) 0.84 (0.35–1.33)
Exposure!PTSS Severity T1 1.93 (1.67–2.20) 0.59 (0.25–0.93) 0.59 (0.25–0.93)
Exposure$Age 0.87 (0.61–1.13) 0.85 (0.49–1.21) 0.85 (0.49–1.21)
Age!Depression=Anxiety T2 1.78 (1.23–2.33) 1.74 (0.90–2.58) 1.74 (0.90–2.58)
Age!PTSS Severity T2 1.36 (0.85–1.86) 1.24 (0.53–1.94) 1.24 (0.53–1.94)
Age! Supervision –0.32 (�0.35–�0.29) –0.33 (�0.39–�0.27) –0.33 (�0.39–�0.27)
Supervision!Depression=Anxiety T1 –2.78 (�3.70–�1.87) –3.05 (�4.48–�1.63) –3.05 (�4.48–�1.63)
Supervision!PTSS Severity T1 –2.02 (�2.83–�1.22) –1.94 (�2.92–�0.97) –1.94 (�2.92–�0.97)
Depression=Anxiety T1!Depression=Anxiety T2 0.49 (0.38–0.59) 0.46 (0.35–0.58) 0.46 (0.35–0.58)
Depression=Anxiety T1!PTSS Severity T2 0.20 (0.11–0.30) 0.18 (0.08–0.27) 0.18 (0.08–0.27)
PTSS Severity T1!Depression=Anxiety T2 0.18 (0.06–0.30) 0.37 (0.16–0.58) 0.00
PTSS Severity T1!PTSS Severity T2 0.40 (0.29–0.51) 0.53 (0.34–0.71) 0.00
E2$E3 86.20 (76.32–96.07) 41.24 (31.52–50.96) 41.24 (31.52–50.96)
E4$E5 55.43 (46.82–64.03) 60.02 (45.05–75.00) 18.05 (5.82–30.28)
Note: Numbers are coefficients (95% confidence intervals); coefficients in bold were constrained to be equal across PTSD-T1 and late-onset PTSD
groups. All ps< .01. PTSD¼ posttraumatic stress disorder; T1¼ first assessment; !¼path; PTSS¼posttraumatic stress symptom(s);
$¼ covariance; T2¼ second assessment.aNmax¼ 920.bn¼ 223.cn¼ 88.
750 SMID ET AL.
Dow
nloa
ded
by [
UV
A U
nive
rsite
itsbi
blio
thee
k SZ
] at
06:
17 2
3 M
arch
201
5
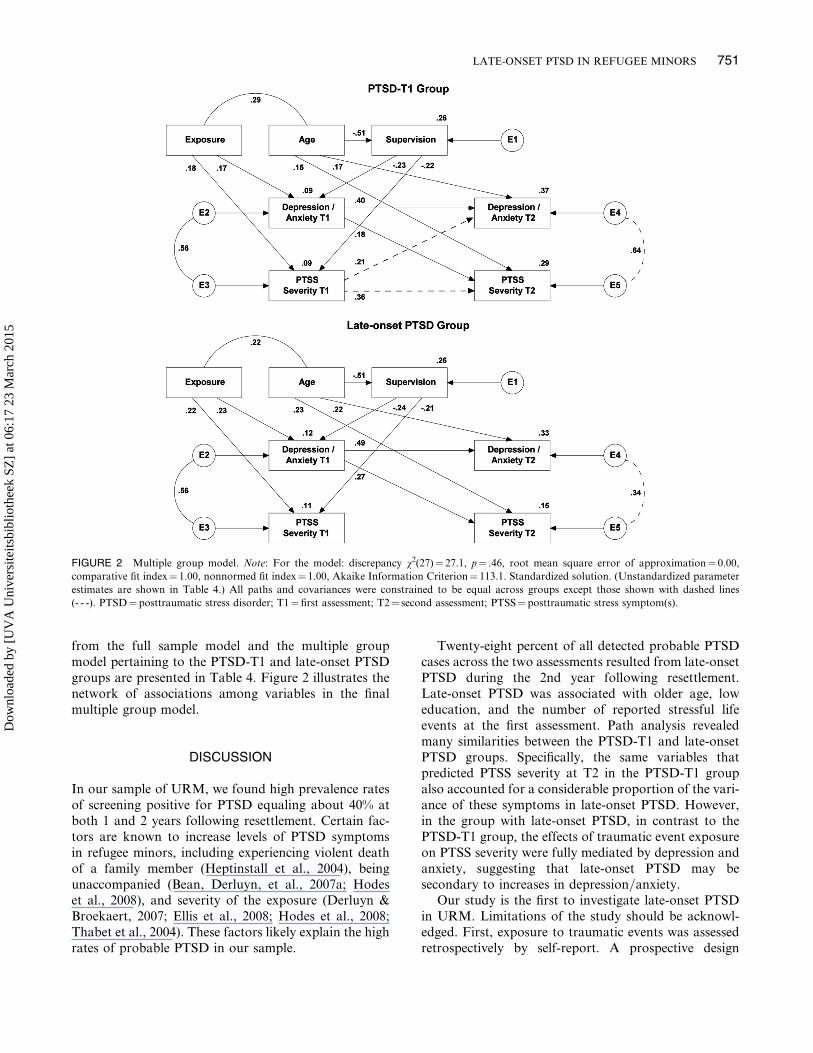
from the full sample model and the multiple groupmodel pertaining to the PTSD-T1 and late-onset PTSDgroups are presented in Table 4. Figure 2 illustrates thenetwork of associations among variables in the finalmultiple group model.
DISCUSSION
In our sample of URM, we found high prevalence ratesof screening positive for PTSD equaling about 40% atboth 1 and 2 years following resettlement. Certain fac-tors are known to increase levels of PTSD symptomsin refugee minors, including experiencing violent deathof a family member (Heptinstall et al., 2004), beingunaccompanied (Bean, Derluyn, et al., 2007a; Hodeset al., 2008), and severity of the exposure (Derluyn &Broekaert, 2007; Ellis et al., 2008; Hodes et al., 2008;Thabet et al., 2004). These factors likely explain the highrates of probable PTSD in our sample.
Twenty-eight percent of all detected probable PTSDcases across the two assessments resulted from late-onsetPTSD during the 2nd year following resettlement.Late-onset PTSD was associated with older age, loweducation, and the number of reported stressful lifeevents at the first assessment. Path analysis revealedmany similarities between the PTSD-T1 and late-onsetPTSD groups. Specifically, the same variables thatpredicted PTSS severity at T2 in the PTSD-T1 groupalso accounted for a considerable proportion of the vari-ance of these symptoms in late-onset PTSD. However,in the group with late-onset PTSD, in contrast to thePTSD-T1 group, the effects of traumatic event exposureon PTSS severity were fully mediated by depression andanxiety, suggesting that late-onset PTSD may besecondary to increases in depression=anxiety.
Our study is the first to investigate late-onset PTSDin URM. Limitations of the study should be acknowl-edged. First, exposure to traumatic events was assessedretrospectively by self-report. A prospective design
FIGURE 2 Multiple group model. Note: For the model: discrepancy v2(27)¼ 27.1, p¼ .46, root mean square error of approximation¼ 0.00,
comparative fit index¼ 1.00, nonnormed fit index¼ 1.00, Akaike Information Criterion¼ 113.1. Standardized solution. (Unstandardized parameter
estimates are shown in Table 4.) All paths and covariances were constrained to be equal across groups except those shown with dashed lines
(- - -). PTSD¼ posttraumatic stress disorder; T1¼ first assessment; T2¼ second assessment; PTSS¼ posttraumatic stress symptom(s).
LATE-ONSET PTSD IN REFUGEE MINORS 751
Dow
nloa
ded
by [
UV
A U
nive
rsite
itsbi
blio
thee
k SZ
] at
06:
17 2
3 M
arch
201
5

would have allowed for more firm conclusions.However, given the nature of the population studied,this design was not feasible. Use of interview assessmentof stressor exposure has been considered most valid(Monroe, 2008). However, given the large size of ourmultilingual sample, questionnaire assessments weremore feasible than interviews.
Second, a diagnosis of probable PTSD was based onquestionnaire assessments in our study. PTSD pre-valence rates should be interpreted with caution, asscreening diagnoses may over or underestimate trueprevalence. Again, given the large sample size, question-naire assessments were more feasible than interviews.Also, in a meta-analysis (Smid et al., 2009), prevalenceof late-onset PTSD did not differ between prospectivestudies using interview as compared to questionnairediagnoses of PTSD. The RATS used in the present studydoes not assess DSM–IV–TR criterion A2 of the PTSDdiagnosis concerning the subjective response to thetraumatic event involving intense fear, helplessness, orhorror (APA, 2000). In several studies, this criterionhardly affected the estimated PTSD prevalence (e.g.,Creamer, McFarlane, & Burgess, 2005). In addition,the RATS does not contain information on the dis-ability criterion of DSM–IV–TR. However, the clinicalrelevance of late-onset PTSD in this group is under-scored by our finding that minors in the late-onsetPTSD group were likely to report having received help.
Third, attrition in our sample appeared to be associa-ted with age and residential setting. It is important tonote that symptoms of PTSD, depression, and anxietyat the initial assessments did not predict attrition.Rather, attrition may be partly attributable to regis-tration failures associated with residential settings char-acterized by less supervision and advancing age of theminors. Therefore, we believe that attrition is unlikelyto have significantly biased our results.
Explaining Late-Onset PTSD in UnaccompaniedRefugee Minors
Increasing age emerged as a risk marker for late-onsetPTSD. This finding highlights the importance of thetransitions for URM at the age of 18 years (Hodeset al., 2008). They will be moved to more independentliving arrangements, if they had previously lived in livingarrangements with more supervision. Furthermore, theirlegal status will be reviewed and they will be aware ofuncertainty regarding their future right to remain inthe Netherlands.
The finding that low education differentiated minorswith late-onset PTSD from those with PTSD at T1 hasnot been reported previously. Lower education appearsto be a maintenance factor for PTSD in general (Brewinet al., 2000). Lower education may lead to feelings of
inadequacy and helplessness in refugee minors whenconfronted with the demands of a Western society,which in turn may lead to PTSD symptom increase.
Consistent with expectations, the number of reportedstressful life events at the first assessment was higher inthe late-onset PTSD group than in the no-PTSD group.This result is consistent with findings in different popu-lations (Smid et al., 2009) that traumatic event exposureis a causal risk factor for late-onset PTSD. Participantsendorsing late-onset PTSD reported fewer traumaticevents at T1 compared to those endorsing PTSD atT1. This could explain why participants with late-onsetPTSD initially endorsed fewer symptoms of PTSD.However, because traumatic exposure was assessedretrospectively, no definitive conclusions can be drawnfrom our study regarding the relation between exposureand time of PTSD onset.
The validity of late-onset PTSD has been questionedbecause increased symptom reporting over time may bemotivated by secondary gains (Sparr & Pankratz, 1983).Thus, asylum seekers presenting apparently trauma-related complaints at later stages following theirresettlement may be suspected of exaggerating theircomplaints, because they may consider the possibilitythat being in need of medical care might increasechances of obtaining a residence permit. In our sample,there were no significant differences in percentages ofrefugees without a residential status across outcomegroups. Therefore, secondary gains do not appear tobe an important explanation for late-onset PTSD inour study.
Role of Depression=Anxiety in Late-Onset PTSD
In refugee minors with late-onset PTSD, predictiveeffects of traumatic exposure reported 1 year followingresettlement on number of PTSD symptoms 2 yearsfollowing resettlement appeared to be mediated bysymptoms of depression and anxiety. PTSD symptomsin late-onset PTSD were thus secondary to symptomsof depression and anxiety. This clinically important find-ing has not been reported previously. Previous researchhas emphasized the elevated risk of individuals endors-ing PTSD to develop depressive symptoms (Breslau,Davis, Peterson, & Schultz, 2000). The possibility thatPTSD may be secondary to depressive symptoms hasbeen suggested by some studies in adults (Carlier, Voer-man, & Gersons, 2000; Erickson et al., 2001; King,King, McArdle, Shalev, & Doron-LaMarca, 2009). Ina recent study of late-onset PTSD in military veterans(Andrews, Brewin, Stewart, Philpott, & Hejdenberg,2009), participants with late-onset PTSD were likely toreport major depressive disorder prior to PTSD onset.
Our results are consistent with cognitive models ofPTSD and depression. According to the cognitive model
752 SMID ET AL.
Dow
nloa
ded
by [
UV
A U
nive
rsite
itsbi
blio
thee
k SZ
] at
06:
17 2
3 M
arch
201
5

of depression (Beck, 2008), depressive symptoms arerelated to cognitive biases, including (a) a deficientreappraisal of negative cognitions and (b) an exagger-ation of stressful events. Negative cognitions mayinclude negative interpretations of intrusive symptoms,which according to the cognitive model of PTSD (Ehlers& Clark, 2000) contribute to the development or persist-ence of PTSD. Exaggeration of stressful events mayexacerbate posttraumatic distress when minors areconfronted with intercurrent stressors.
The risk of exposure to intercurrent stressors inrefugee minors may be increased as a direct consequenceof earlier traumatic events, or because depressive symp-toms may increase the likelihood of exposure to inter-personal stress. Secondary stressors are generallydefined as stressors that are the direct consequence ofprior traumatic events or losses. Indeed, resettlement-specific secondary adversities and ongoing exposuresto trauma reminders have been found to explain a sig-nificant proportion of posttraumatic distress in youthsexposed to war (Layne et al., 2010). According to thetheory of stress generation in depression (Hammen,2006), individuals endorsing depressive symptoms areat increased risk of generating stressful interpersonalevents, including conflicts. Several studies in adolescents(Harkness & Stewart, 2009; Kercher & Rapee, 2009)have provided evidence of stress generation.
In sum, cognitive biases associated with depressionsymptoms may be implicated in progression of post-traumatic distress in refugee minors. In addition, bothdepressive symptoms and prior traumatic eventexposure may increase the risk of intercurrent stressorsthat in turn may contribute to posttraumatic distress.Future studies seeking to establish causal maintenancefactors in late-onset PTSD should therefore integrateaffective symptoms and their associated cognitive biasesas well as intercurrent stressors.
Implications for Research, Policy, and Practice
Research focusing on URM is still scarce despite theobvious vulnerability of this group (Huemer et al.,2009). Comprehensive long-term follow-up studies,ideally comprising several repeated interview assess-ments, are needed to extend our findings and to enablecausal inferences that may guide both mental health careprovision and responsible immigration policies regard-ing URM. Such studies should employ a rigorouslyarticulated conceptual framework and include a rangeof variables that may causally influence long-termadjustment, including cognitive and coping aspects,intercurrent stressors, resources, and protective factors,such as supervision and social support. These studiesmay also shed further light on the close relationshipbetween PTSD and affective symptoms.
Late-onset PTSD in refugee minors was not unusualand may therefore be an important focus for secondaryand tertiary prevention. Screening for trauma-relatedmorbidity in this population is warranted and shouldtake place on multiple occasions. Mental health profes-sionals should undertake efforts to increase stakeholders’awareness of the frequent psychological symptoms of theminors. Early detection by health practitioners, immi-gration officers, child protection services, and legal guar-dians dealing with refugee minors can thus be stimulated.Mental health professionals should structurally beinvolved early in the asylum procedure of URM, forinstance, by providing education to the minors abouthow to cope with their situation and the complicatingsymptoms. Education to the minors should include infor-mation about the psychological risks associated withtraumatic experiences and available evidence-basedtreatments. Treatment aimed at relieving symptoms ofdepression and anxiety in refugee minors endorsing sub-threshold PTSD may be useful, as this may contribute tothe prevention of late-onset PTSD.
REFERENCES
Ajdukovic, M., & Ajdukovic, D. (1998). Impact of displacement on the
psychological well-being of refugee children. International Review of
Psychiatry, 10, 186–195.
American Psychiatric Association. (2000). Diagnostic and statistical
manual of mental disorders (4th ed., text rev.). Washington, DC:
Author.
Andrews, B., Brewin, C. R., Philpott, R., & Stewart, L. (2007). Delayed-
onset posttraumatic stress disorder: A systematic review of the
evidence. American Journal of Psychiatry, 164, 1319–1326.
Andrews, B., Brewin, C. R., Stewart, L., Philpott, R., & Hejdenberg, J.
(2009). Comparison of immediate-onset and delayed-onset post-
traumatic stress disorder in military veterans. Journal of Abnormal
Psychology, 118, 767–777.
Bean, T., Derluyn, I., Eurelings-Bontekoe, E. H. M., Broekaert, E., &
Spinhoven, P. (2006). Validation of the multiple language versions
of the Reactions of Adolescents to Traumatic Stress questionnaire.
Journal of Traumatic Stress, 19, 241–255.
Bean, T., Derluyn, I., Eurelings-Bontekoe, E. H. M., Broekaert, E. &
Spinhoven, P. (2007a). Comparing psychological distress, traumatic
stress reactions, and experiences of unaccompanied refugee minors
with experiences of adolescents accompanied by parents. Journal
of Nervous and Mental Disease, 195, 288–297.
Bean, T., Derluyn, I., Eurelings-Bontekoe, E. H. M., Broekaert, E. &
Spinhoven, P. (2007b). Validation of the multiple language versions
of the Hopkins Symptom Checklist–37 for refugee adolescents.
Adolescence, 42, 51–71.
Bean, T., Eurelings-Bontekoe, E. H. M., Mooijaart, A., & Spinhoven,
P. (2006). Factors associated with mental health service need and
utilization among unaccompanied refugee adolescents. Administra-
tion and Policy in Mental Health and Mental Health Services
Research, 33, 342–355.
Bean, T., Eurelings-Bontekoe, E. H. M., & Spinhoven, P. (2007).
Course and predictors of mental health of unaccompanied refugee
minors in the Netherlands: One-year follow-up. Social Science &
Medicine, 64, 1204–1215.
LATE-ONSET PTSD IN REFUGEE MINORS 753
Dow
nloa
ded
by [
UV
A U
nive
rsite
itsbi
blio
thee
k SZ
] at
06:
17 2
3 M
arch
201
5

Beck, A. T. (2008). The evolution of the cognitive model of depression
and its neurobiological correlates. American Journal of Psychiatry,
165, 969–977.
Bollen, K. A., & Stine, R. A. (1992). Bootstrapping goodness-of-fit
measures in structural equation models. Sociological Methods &
Research, 21, 205–229.
Breslau, N., Davis, G. C., Peterson, E. L., & Schultz, L. R. (2000). A
second look at comorbidity in victims of trauma: The posttraumatic
stress disorder-major depression connection. Biological Psychiatry,
48, 902–909.
Brewin, C. R. (2005). Systematic review of screening instruments
for adults at risk for PTSD. Journal of Traumatic Stress, 18,
53–62.
Brewin, C. R., Andrews, B., & Valentine, J. D. (2000). Meta-analysis
of risk factors for posttraumatic stress disorder in trauma-
exposed adults. Journal of Consulting and Clinical Psychology, 68,
748–766.
Carlier, I. V. E., Voerman, B. E., & Gersons, B. P. R. (2000). Intrusive
traumatic recollections and comorbid posttraumatic stress disorder
in depressed patients. Psychosomatic Medicine, 62, 26–32.
Creamer, M., McFarlane, A. C., & Burgess, P. (2005). Psychopath-
ology following trauma: The role of subjective experience. Journal
of Affective Disorders, 86, 175–182.
Derluyn, I., & Broekaert, E. (2007). Different perspectives on emo-
tional and behavioural problems in unaccompanied refugee children
and adolescents. Ethnicity and Health, 12, 141–162.
Ehlers, A., & Clark, D. M. (2000). A cognitive model of posttraumatic
stress disorder. Behaviour Research and Therapy, 38, 319–345.
Elhai, J. D., Engdahl, R. M., Palmieri, P. A., Naifeh, J. A., Schweinle,
A., & Jacobs, G. A. (2009). Assessing posttraumatic stress disorder
with or without reference to a single, worst traumatic event: Exam-
ining differences in factor structure. Psychological Assessment, 21,
629–634.
Ellis, B. H., MacDonald, H. Z., Lincoln, A. K., & Cabral, H. J. (2008).
Mental health of Somali adolescent refugees: The role of trauma,
stress, and perceived discrimination. Journal of Consulting and
Clinical Psychology, 76, 184–193.
Enders, C. K., & Bandalos, D. L. (2001). The relative performance of
Full Information Maximum Likelihood estimation for missing data
in structural equation models. Structural Equation Modeling, 8,
430–457.
Erickson, D. J., Wolfe, J., King, D. W., King, L. A., & Sharkansky, E.
J. (2001). Posttraumatic stress disorder and depression symptoma-
tology in a sample of Gulf War veterans: A prospective analysis.
Journal of Consulting and Clinical Psychology, 69, 41–49.
Fazel, M., Wheeler, J., & Danesh, J. (2005). Prevalence of serious
mental disorder in 7000 refugees resettled in western countries: A
systematic review. The Lancet, 365, 1309–1314.
Guarnaccia, P. J., & Lopez, S. (1998). The mental health and
adjustment of immigrant and refugee children. Child and Adolescent
Psychiatric Clinics of North America, 7, 537–553.
Hammen, C. (2006). Stress generation in depression: Reflections on
origins, research, and future directions. Journal of Clinical
Psychology, 62, 1065–1082.
Harkness, K. L., & Stewart, J. G. (2009). Symptom specificity and the
prospective generation of life events in adolescence. Journal of
Abnormal Psychology, 118, 278–287.
Heptinstall, E., Sethna, V., & Taylor, E. (2004). PTSD and depression
in refugee children: Associations with pre-migration trauma and
post-migration stress. European Child and Adolescent Psychiatry,
13, 373–380.
Hodes, M., Jagdev, D., Chandra, N., & Cunniff, A. (2008). Risk and
resilience for psychological distress amongst unaccompanied asylum
seeking adolescents. Journal of Child Psychology and Psychiatry, 49,
723–732.
Huemer, J., Karnik, N., Voelkl-Kernstock, S., Granditsch, E., Dervic,
K., Friedrich, M., et al. (2009). Mental health issues in unaccompan-
ied refugee minors. Child and Adolescent Psychiatry and Mental
Health, 3, 13.
Joreskog, K. (1971). Simultaneous factor analysis in several popula-
tions. Psychometrika, 36, 409–426.
Kaplan, D. W. (2008). Structural equation modeling: Foundations and
extensions (2nd ed.). Thousand Oaks, CA: Sage.
Kercher, A., & Rapee, R. (2009). A test of a cognitive diathesis–stress
generation pathway in early adolescent depression. Journal of
Abnormal Child Psychology, 37, 845–855.
King, D. W., King, L. A., McArdle, J. J., Shalev, A. Y., &
Doron-LaMarca, S. (2009). Sequential temporal dependencies in
associations between symptoms of depression and posttraumatic
stress disorder: An application of bivariate latent difference score
structural equation modeling. Multivariate Behavioral Research,
44, 437–464.
Kline, R. B. (2004). Principles and practice of structural equation
modeling (2nd ed.). New York: Guilford.
Layne, C. M., Olsen, J. A., Baker, A., Legerski, J. P., Isakson, B.,
Pasalic, A., et al. (2010). Unpacking trauma exposure risk factors
and differential pathways of influence: Predicting postwar
mental distress in Bosnian adolescents. Child Development, 81,
1053–1076.
Layne, C. M., Warren, J. S., Watson, P. J., & Shalev, A. Y. (2007).
Risk, vulnerability, resistance, and resilience: Toward an integrative
conceptualization of posttraumatic adaptation. In M. J. Friedman,
T. M. Keane & P. A. Resnick (Eds.), Handbook of PTSD: Science
and practice (pp. 497–520). New York: Guilford.
Lustig, S. L., Kia-Keating, M., Knight, W. G., Geltman, P., Ellis, H.,
Kinzie, J. D., et al. (2004). Review of child and adolescent refugee
mental health. Journal of the American Academy of Child &
Adolescent Psychiatry, 43, 24–36.
Mardia, K. V. (1970). Measures of multivariate skewness and kurtosis
with applications. Biometrika, 57, 519–530.
Mghir, R., Freed, W., Raskin, A., & Katon, W. (1995). Depression
and posttraumatic stress disorder among a community sample of
adolescent and young adult Afghan refugees. Journal of Nervous
and Mental Disease, 183, 24–30.
Mollica, R. F., Wyshak, G., de Marneffe, D., Khuon, F., & Lavelle, J.
(1987). Indochinese versions of the Hopkins Symptom Checklist–25:
A screening instrument for the psychiatric care of refugees.
American Journal of Psychiatry, 144, 497–500.
Monroe, S. M. (2008). Modern approaches to conceptualizing and
measuring human life stress. Annual Review of Clinical Psychology,
4, 33–52.
Ozer, E. J., Best, S. R., Lipsey, T. L., & Weiss, D. S. (2003). Predictors
of posttraumatic stress disorder and symptoms in adults: A
meta-analysis. Psychological Bulletin, 129, 52–73.
Sack, W. H., Him, C., & Dickason, D. (1999). Twelve-year follow-up
study of Khmer youths who suffered massive war trauma as
children. Journal of the American Academy of Child & Adolescent
Psychiatry, 38, 1173–1179.
Smid, G. E., Mooren, T. T. M., Van der Mast, R. C., Gersons, B. P.
R., & Kleber, R. J. (2009). Delayed posttraumatic stress disorder:
Systematic review, meta-analysis, and metaregression analysis of
prospective studies. Journal of Clinical Psychiatry, 70, 1572–1582.
Sparr, L., & Pankratz, L. D. (1983). Factitious posttraumatic stress
disorder. American Journal of Psychiatry, 140, 1016–1019.
Spinhoven, P., Bean, T., & Eurelings-Bontekoe, L. (2006). Inconsisten-
cies in the self-report of traumatic experiences by unaccompanied
refugee minors. Journal of Traumatic Stress, 19, 663–673.
Stein, B., Comer, D., Gardner, W., & Kelleher, K. (1999). Prospective
study of displaced children’s symptoms in wartime Bosnia. Social
Psychiatry and Psychiatric Epidemiology, 34, 464–469.
754 SMID ET AL.
Dow
nloa
ded
by [
UV
A U
nive
rsite
itsbi
blio
thee
k SZ
] at
06:
17 2
3 M
arch
201
5

Thabet, A. A. M., Abed, Y., & Vostanis, P. (2004). Comorbidity of
PTSD and depression among refugee children during war conflict.
Journal of Child Psychology and Psychiatry and Allied Disciplines,
45, 533–542.
Tolin, D. F., & Foa, E. B. (2006). Sex differences in trauma and post-
traumatic stress disorder: A quantitative review of 25 years of
research. Psychological Bulletin, 132, 959–992.
UNHCR. (2004). Trends in unaccompanied and separated children
seeking asylum in industrialized countries, 2001–2003. Retrieved
from the United Nations High Commissioner for Refugees website:
http://www.unhcr.org/40f646444.pdf
United Nations (1989). Convention on the Rights of the Child. Retrieved
from the Office of the United Nations High Commissioner for Human
Rights website: http://www2.ohchr.org/english/law/pdf/crc.pdf
LATE-ONSET PTSD IN REFUGEE MINORS 755
Dow
nloa
ded
by [
UV
A U
nive
rsite
itsbi
blio
thee
k SZ
] at
06:
17 2
3 M
arch
201
5
Related Documents











