Late cardiac outcomes after pregnancy in women with congenital aortic stenosis Nikolaos Tzemos, MD, a Candice K. Silversides, MD, SM, a Jack M. Colman, MD, a Judith Therrien, MD, b Gary D. Webb, MD, c Jennifer Mason, RN, a Evelyn Cocoara, a Mathew Sermer, MD, a and Samuel C. Siu, MD, SM a,d Toronto and London, Ontario, and Montreal, Quebec, Canada; and Philadelphia, PA Background Late cardiac outcomes in women with aortic stenosis (AS) who have undergone pregnancy have not been well defined. Methods We examined 51 consecutive women with congenital AS who underwent 70 pregnancies. Late cardiac events (pulmonary edema, cardiac arrhythmia, cardiac death, cardiac interventions N1 year since baseline evaluation) were the outcome of interest. The frequency of late cardiac events in the postpregnant group were compared to age- and lesion-matched women with congenital AS who have never been pregnant. Results During the follow-up period (6 + 4 years), 43% of women underwent cardiac interventions which comprised all late cardiac events. Independent baseline predictors of late cardiac events were (1) moderate or severe AS (hazard ratio = 4.5, P = .045) and (2) New York Functional Class II (hazard ratio = 4.6, P = .014). When outcomes in 26 women from the postpregnant group were compared to 26 age- and lesion-matched women who have never been pregnant, the postpregnant group had a higher late cardiac event rate than the never-pregnant group (31% vs 0%, P = .021). Conclusion Women with moderate or severe AS and symptomatic during pregnancy are at high likelihood of requiring cardiac interventions late after pregnancy. Women with congenital AS who have undergone pregnancy have a higher frequency of late cardiac events compared to those who have never been pregnant. Late cardiac outcomes after pregnancy should be considered in the counseling of women with AS who are contemplating pregnancy. (Am Heart J 2009;157:474-80.) Left ventricular outflow tract obstruction in women with congenital aortic stenosis (AS) can result in maternal and fetal deterioration during pregnancy. Prior studies of pregnancy outcomes in women with AS have focused on ante- and peripartum outcomes. 1-6 Whether the pro- longed hemodynamic changes of pregnancy affect clinical compensation or valve function over the long term is unknown. Understanding the natural history of AS after pregnancy would enable women with AS to make an informed choice with regard to the timing of pregnancy and/or interventions. We performed a cohort study examining late outcomes after pregnancy in women with congenital AS. Their late outcomes were also compared to a group of age- and lesion matched women with AS who have never been pregnant. Methods The study (postpregnant) group consisted of 51 consecutive pregnant women with congenital AS (identified from the University of Toronto Pregnancy and Heart Disease Research Program's database) referred for consultation or care to Toronto General or Mount Sinai Hospitals between 1986 and 2004. 5,7 Aortic stenosis was defined as stenosis at the valvular, subvalvular, or supravalvular levels with peak transaortic velocity N2 m/s. We excluded women (n = 5) in whom their only pregnancy was terminated or complicated by miscarriage (fetal demise b20 weeks gestation) as well as women with hyper- trophic cardiomyopathy (n = 11) or prosthetic aortic valves (n = 24). Thirty women in the study group were included in an earlier case series examining shorter term outcomes. 4 The study was approved by the research ethics boards of Toronto General and Mount Sinai Hospitals. In the study group, clinical data were systematically recorded during the ante-, peri-, and postpartum (first 6 months after delivery) periods, as previously described. 5,7 Baseline clinical and echocardiographic assessments were performed at the From the a University of Toronto Pregnancy and Heart Disease Research Program and Toronto Congenital Cardiac Centre for Adults, Toronto General and Mount Sinai Hospitals, Toronto, Ontario, Canada, b Division of Cardiology, Sir M B Davis Jewish General Hospital, McGill University, Montreal, Quebec, Canada, c Philadelphia Adult Congenital Heart Centre, Children's Hospital of Philadelphia, University of Pennsylvania, Philadelphia, PA, and d Division of Cardiology (SCS), University of Western Ontario, London, Ontario, Canada. Submitted August 15, 2008; accepted October 26, 2008. Reprint requests: Samuel Siu, MD, C6-005, University Hospital, 339 Windermere Road, London, Ontario, Canada N6A 5A5. E-mail: [email protected] 0002-8703/$ - see front matter © 2009, Mosby, Inc. All rights reserved. doi:10.1016/j.ahj.2008.10.020

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Late cardiac outcomes after pregnancy in women withcongenital aortic stenosisNikolaos Tzemos, MD,a Candice K. Silversides, MD, SM,a Jack M. Colman, MD,a Judith Therrien, MD,b
Gary D. Webb, MD,c Jennifer Mason, RN,a Evelyn Cocoara,a Mathew Sermer, MD,a and Samuel C. Siu, MD, SMa,d
Toronto and London, Ontario, and Montreal, Quebec, Canada; and Philadelphia, PA
Background Late cardiac outcomes in women with aortic stenosis (AS) who have undergone pregnancy have notbeen well defined.
Methods We examined 51 consecutive women with congenital AS who underwent 70 pregnancies. Late cardiacevents (pulmonary edema, cardiac arrhythmia, cardiac death, cardiac interventions N1 year since baseline evaluation)were the outcome of interest. The frequency of late cardiac events in the postpregnant group were compared to age- andlesion-matched women with congenital AS who have never been pregnant.
Results During the follow-up period (6 + 4 years), 43% of women underwent cardiac interventions which comprisedall late cardiac events. Independent baseline predictors of late cardiac events were (1) moderate or severe AS (hazardratio = 4.5, P = .045) and (2) New York Functional Class II (hazard ratio = 4.6, P = .014). When outcomes in 26 womenfrom the postpregnant group were compared to 26 age- and lesion-matched women who have never been pregnant,the postpregnant group had a higher late cardiac event rate than the never-pregnant group (31% vs 0%, P = .021).
Conclusion Women with moderate or severe AS and symptomatic during pregnancy are at high likelihood ofrequiring cardiac interventions late after pregnancy. Women with congenital AS who have undergone pregnancy have ahigher frequency of late cardiac events compared to those who have never been pregnant. Late cardiac outcomes afterpregnancy should be considered in the counseling of women with AS who are contemplating pregnancy. (Am Heart J2009;157:474-80.)
Left ventricular outflow tract obstruction in womenwith congenital aortic stenosis (AS) can result in maternaland fetal deterioration during pregnancy. Prior studies ofpregnancy outcomes in women with AS have focused onante- and peripartum outcomes.1-6 Whether the pro-longed hemodynamic changes of pregnancy affectclinical compensation or valve function over the longterm is unknown. Understanding the natural history of ASafter pregnancy would enable womenwith AS to make aninformed choice with regard to the timing of pregnancyand/or interventions. We performed a cohort study
From the aUniversity of Toronto Pregnancy and Heart Disease Research Program andToronto Congenital Cardiac Centre for Adults, Toronto General andMount Sinai HospitalsToronto, Ontario, Canada, bDivision of Cardiology, Sir M B Davis Jewish GeneraHospital, McGill University, Montreal, Quebec, Canada, cPhiladelphia Adult CongenitaHeart Centre, Children's Hospital of Philadelphia, University of Pennsylvania, PhiladelphiaPA, and dDivision of Cardiology (SCS), University of Western Ontario, LondonOntario, Canada.Submitted August 15, 2008; accepted October 26, 2008.Reprint requests: Samuel Siu, MD, C6-005, University Hospital, 339 Windermere RoadLondon, Ontario, Canada N6A 5A5.E-mail: [email protected]/$ - see front matter© 2009, Mosby, Inc. All rights reserved.doi:10.1016/j.ahj.2008.10.020
,ll,,
,
examining late outcomes after pregnancy in women withcongenital AS. Their late outcomes were also comparedto a group of age- and lesion matched women with ASwho have never been pregnant.
MethodsThe study (postpregnant) group consisted of 51 consecutive
pregnant women with congenital AS (identified from theUniversity of Toronto Pregnancy and Heart Disease ResearchProgram's database) referred for consultation or care to TorontoGeneral or Mount Sinai Hospitals between 1986 and 2004.5,7
Aortic stenosis was defined as stenosis at the valvular,subvalvular, or supravalvular levels with peak transaorticvelocity N2 m/s. We excluded women (n = 5) in whom their onlypregnancy was terminated or complicated by miscarriage (fetaldemise b20 weeks gestation) as well as women with hyper-trophic cardiomyopathy (n = 11) or prosthetic aortic valves(n = 24). Thirty women in the study group were included in anearlier case series examining shorter term outcomes.4 The studywas approved by the research ethics boards of Toronto Generaland Mount Sinai Hospitals.In the study group, clinical data were systematically recorded
during the ante-, peri-, and postpartum (first 6 months afterdelivery) periods, as previously described.5,7 Baseline clinicaland echocardiographic assessments were performed at the

Tzemos et al 475American Heart JournalVolume 157, Number 3
woman's first antepartum visit at our centre. Follow-up data upto September 2007 were prospectively updated by review ofhealth records, clinic visit, or telephone calls with patient withscripted interviews. Follow-up data included New York HeartAssociation (NYHA) functional class, cardiac symptoms (chestpain, syncope, dyspnea), and occurrence of cardiac events(pulmonary edema, sustained cardiac arrhythmia requiringtreatment, stroke, cardiac death, or cardiac interventions).Cardiac events were verified by review of clinic letter, operativereport, or hospital discharge summary.A group of 30 consecutive women of childbearing age
(16-50 years) with congenital AS who had never been pregnantand with N1 year of follow-up was identified from the TorontoCongenital Cardiac Centre for Adults database. Each woman inthe study group was individually matched with another womanfrom the comparison group, initially by AS severity and then byage. If several women in the comparison group had the sameseverity of AS as the study patient of interest, the woman whoseage corresponded closest with that of the study patient wasselected. Of these 30 women, 26 could be matched to an equalnumber of women in the study group by severity of AS and agerange (16-45 years) and comprised the never-pregnant group.The absence of prior pregnancies was documented by review ofclinic records and confirmed with each woman at the time offollow-up. Baseline clinical data were obtained from thestandardized record of their first ambulatory visit at TorontoCongenital Cardiac Centre for Adults. Follow-up was obtained inthe same manner as in the postpregnant group.Transthoracic echocardiography was performed either at the
first antenatal visit (postpregnant group) or first ambulatory visit(never-pregnant group). Aortic stenosis and aortic regurgitationwere classified using current guidelines.8,9 Aortic stenosis severitywas classified as mild (valve area N1.5 cm2, peak velocity b3m/s),moderate (valve area 1.0-1.5 cm2, peak velocity 3-4m/s), or severe(valve area b1.0 cm2, peak velocity N4 m/s).9 For women to beclassified as having moderate or severe valvular AS, the peakvelocity and valve area criteria had to be present. Critical AS wasdefined as valve area b0.75 cm2 or peak velocity N4.5 m/s.10,11
Left ventricular (LV) dimension, left atrial dimension, aorticroot dimension (at sinus of Valsalva level), and proximalascending aortic dimensions were determined using currentguidelines.8,12 Left ventricular mass was indexed to height;LV hypertrophy was defined as LV mass index N44 g/m2.7.12 Leftventricular ejection fraction was quantitated; visual estimationof ejection fraction was used if images were suboptimal forquantitation.13,14 Dilated aortic root and ascending aorta weredefined as N35 and N34 mm, respectively.15 Left atrial dilatationwas defined by an end systolic anterior-posterior dimensionN38 mm.15 The follow-up echocardiogram was defined as eitherthe most recent echocardiogram or the last echocardiogrambefore the occurrence of the first late cardiac complication. Inthe postpregnant group, follow-up echocardiographic data wereobtained no earlier than the sixth postpartum month.Late maternal cardiac events were the primary outcome of
interest and were defined as: pulmonary edema, sustained cardiacarrhythmia requiring treatment, stroke, cardiac death, cardiacsurgery or percutaneous aortic valvuloplasty occurringN12monthsafter the baseline visit. The period of 12 months was chosen toexclude events that occurred either during pregnancy or sympto-matic deterioration during the first year of follow-up. At our center,invasive intervention for AS was primarily based on symptoms.
Data analyses were performed using the SPSS for Windows(Version 15.0, Chicago, IL). Continuous data were presentedas mean ± 1 SD. Variables were compared using Wilcoxon, χ2
or Fisher exact tests, wherever appropriate. P values were setat .05 (2-sided) unless otherwise indicated. Event-free survivalwas displayed using the Kaplan-Meier method. In womenwho had undergone N1 pregnancies, follow-up was measuredfrom the first antepartum visit of the index pregnancy (thefirst pregnancy in which the diagnosis of AS was established)until either the time of late cardiac event or the most recentfollow-up visit. As the primary end point was events N1 yearof follow-up, women who underwent cardiac interventionsb1 year of their baseline visit were censored at the time oftheir intervention.Univariate analysis of possible predictors (baseline clinical,
echocardiographic variables and maternal pregnancy complica-tions) of late cardiac events in the postpregnant group wasperformed using Cox regression analyses. Univariate predictorswith P b .10 were evaluated by a multivariate Cox regression;highly correlated variables (r N 0.70) were combined. Late event-free survival of the postpregnant group was compared to that ofthe never-pregnant group using log-rank test.In women who underwent both their baseline and follow-up
echocardiograms at Toronto General or Mount Sinai hospitals,the rate of change in aortic gradients, area, and LV mass index(difference between follow-up and baseline measurementsdivided by follow-up time) was determined. In women whoexperienced a late cardiac event, follow-up echocardiographicdata were obtained from the latest study performed prior to theoccurrence of the late event.
Support by Fellowship Award from the University of Toronto(NT) (Toronto, Ontario, Canada), Ramsay GuntonProfessorship in Cardiology from the Schulich School ofMedicine and Dentistry (SCS) (London, Ontario, Canada),Operating Grants from Canadian Institutes of Health Research(53130), and Heart and Stroke Foundation of Canada (NA5662) (Ottawa, Ontario, Canada).
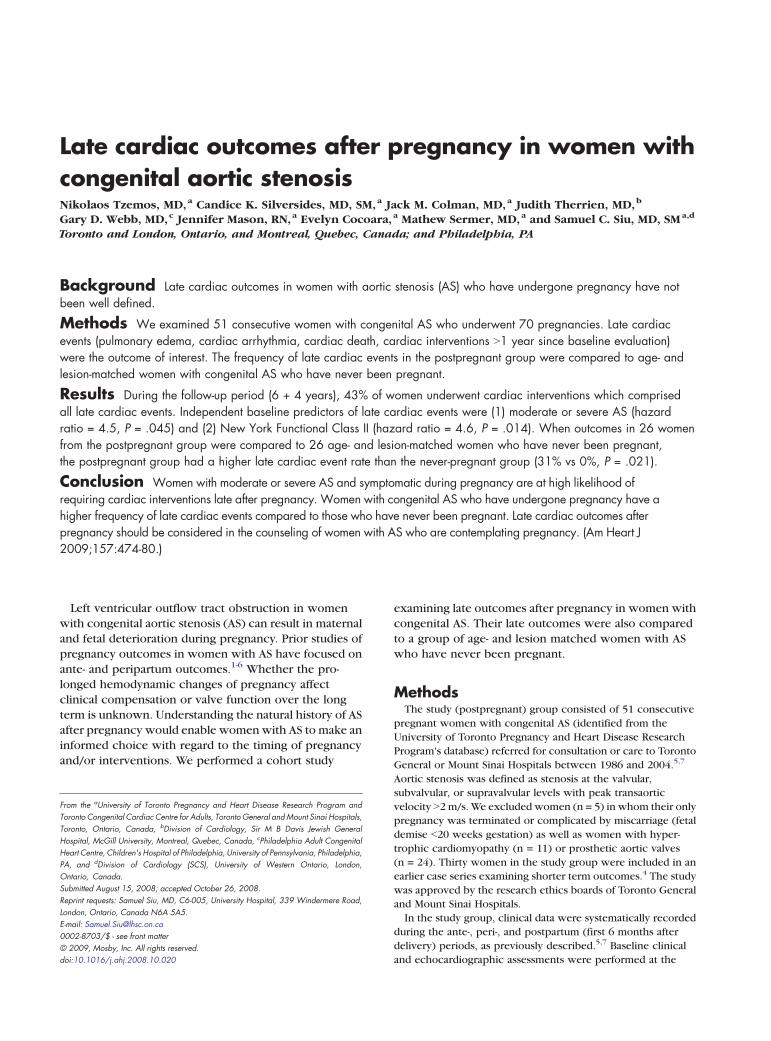
ResultsBaseline characteristicsBaseline characteristics of the study group are
displayed in Tables I and II. Most women (n = 46 [90%])were asymptomatic at their baseline antenatal visit; theother 5 women were experiencing exertional dyspnea.Baseline maternal age was 28 ± 6 years, and all patientswere ambulatory. In those women who had undergoneprior procedures for aortic coarctation, there was nosignificant residual coarctation. Most women hadvalvular AS from bicuspid aortic valve (BAV) (90%); nowomen had supravalvular AS. No woman was receivingcardiac medications. Seventy-one percent of women hadmoderate or severe AS (echocardiography performed at19 ± 8 weeks of gestation). The LV ejection fraction inall women was N50%. Forty percent of women had LVhypertrophy. Fourteen percent had baseline dilatation ofeither the aortic root or proximal ascending aorta, butthese parameters were not obtained in all women.
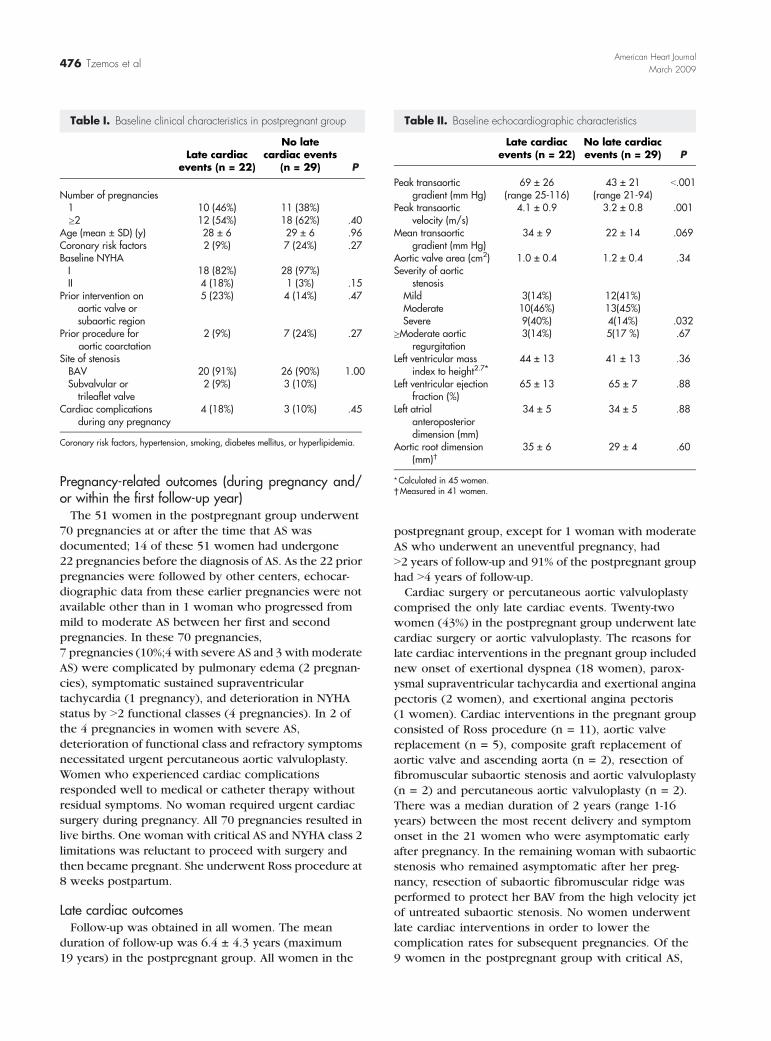
Table I. Baseline clinical characteristics in postpregnant group
Late cardiacevents (n = 22)
No latecardiac events
(n = 29) P
Number of pregnancies1 10 (46%) 11 (38%)≥2 12 (54%) 18 (62%) .40
Age (mean ± SD) (y) 28 ± 6 29 ± 6 .96Coronary risk factors 2 (9%) 7 (24%) .27Baseline NYHAI 18 (82%) 28 (97%)II 4 (18%) 1 (3%) .15
Prior intervention onaortic valve orsubaortic region
5 (23%) 4 (14%) .47
Prior procedure foraortic coarctation
2 (9%) 7 (24%) .27
Site of stenosisBAV 20 (91%) 26 (90%) 1.00Subvalvular ortrileaflet valve
2 (9%) 3 (10%)
Cardiac complicationsduring any pregnancy
4 (18%) 3 (10%) .45
Coronary risk factors, hypertension, smoking, diabetes mellitus, or hyperlipidemia.
Table II. Baseline echocardiographic characteristics
Late cardiacevents (n = 22)
No late cardiacevents (n = 29) P
Peak transaorticgradient (mm Hg)
69 ± 26(range 25-116)
43 ± 21(range 21-94)
b.001
Peak transaorticvelocity (m/s)
4.1 ± 0.9 3.2 ± 0.8 .001
Mean transaorticgradient (mm Hg)
34 ± 9 22 ± 14 .069
Aortic valve area (cm2) 1.0 ± 0.4 1.2 ± 0.4 .34Severity of aortic
stenosisMild 3(14%) 12(41%)Moderate 10(46%) 13(45%)Severe 9(40%) 4(14%) .032
≥Moderate aorticregurgitation
3(14%) 5(17 %) .67
Left ventricular massindex to height2.7⁎
44 ± 13 41 ± 13 .36
Left ventricular ejectionfraction (%)
65 ± 13 65 ± 7 .88
Left atrialanteroposteriordimension (mm)
34 ± 5 34 ± 5 .88
Aortic root dimension(mm)†
35 ± 6 29 ± 4 .60
⁎Calculated in 45 women.†Measured in 41 women.
476 Tzemos et alAmerican Heart Journal
March 2009
Pregnancy-related outcomes (during pregnancy and/or within the first follow-up year)The 51 women in the postpregnant group underwent
70 pregnancies at or after the time that AS wasdocumented; 14 of these 51 women had undergone22 pregnancies before the diagnosis of AS. As the 22 priorpregnancies were followed by other centers, echocar-diographic data from these earlier pregnancies were notavailable other than in 1 woman who progressed frommild to moderate AS between her first and secondpregnancies. In these 70 pregnancies,7 pregnancies (10%;4 with severe AS and 3 with moderateAS) were complicated by pulmonary edema (2 pregnan-cies), symptomatic sustained supraventriculartachycardia (1 pregnancy), and deterioration in NYHAstatus by N2 functional classes (4 pregnancies). In 2 ofthe 4 pregnancies in women with severe AS,deterioration of functional class and refractory symptomsnecessitated urgent percutaneous aortic valvuloplasty.Women who experienced cardiac complicationsresponded well to medical or catheter therapy withoutresidual symptoms. No woman required urgent cardiacsurgery during pregnancy. All 70 pregnancies resulted inlive births. One woman with critical AS and NYHA class 2limitations was reluctant to proceed with surgery andthen became pregnant. She underwent Ross procedure at8 weeks postpartum.
Late cardiac outcomesFollow-up was obtained in all women. The mean
duration of follow-up was 6.4 ± 4.3 years (maximum19 years) in the postpregnant group. All women in the
postpregnant group, except for 1 woman with moderateAS who underwent an uneventful pregnancy, hadN2 years of follow-up and 91% of the postpregnant grouphad N4 years of follow-up.Cardiac surgery or percutaneous aortic valvuloplasty
comprised the only late cardiac events. Twenty-twowomen (43%) in the postpregnant group underwent latecardiac surgery or aortic valvuloplasty. The reasons forlate cardiac interventions in the pregnant group includednew onset of exertional dyspnea (18 women), parox-ysmal supraventricular tachycardia and exertional anginapectoris (2 women), and exertional angina pectoris(1 women). Cardiac interventions in the pregnant groupconsisted of Ross procedure (n = 11), aortic valvereplacement (n = 5), composite graft replacement ofaortic valve and ascending aorta (n = 2), resection offibromuscular subaortic stenosis and aortic valvuloplasty(n = 2) and percutaneous aortic valvuloplasty (n = 2).There was a median duration of 2 years (range 1-16years) between the most recent delivery and symptomonset in the 21 women who were asymptomatic earlyafter pregnancy. In the remaining woman with subaorticstenosis who remained asymptomatic after her preg-nancy, resection of subaortic fibromuscular ridge wasperformed to protect her BAV from the high velocity jetof untreated subaortic stenosis. No women underwentlate cardiac interventions in order to lower thecomplication rates for subsequent pregnancies. Of the9 women in the postpregnant group with critical AS,

Figure 1
Late cardiac outcomes in postpregnant group.
Table III. Baseline characteristics of comparison groups
Postpregnant(n = 26)
Never-pregnant(n = 26) P
Baseline age (y) 24 ± 5 23 ± 8 0.021Coronary risk factor 6 (23%) 7 (27%) 0.75NYHA class II 1 (4%) 1 (4%) 1.00Prior intervention for valvular or
subvalvular aortic stenosis4 (15%) 6 (23%) 0.48
Prior procedure for aorticcoarctation
8 (31%) 7 (27%) 0.76
Site of stenosisBicuspid aortic valve 24 (92%) 25 (96%) 0.55Subvalvular or Trileaflet valve 2 (8%) 1 (4%)Peak transaortic gradient(mm Hg)
38 ± 20 41 ± 21 0.46
Peak transaortic velocity (m/s) 3.0 ± 0.7 3.2 ± 0.7 0.36Aortic valve area (cm2) 1.1 ± 0.4 1.1 ± 0.3 0.95
Severity of aortic stenosisMild 15 (58%) 15 (58%)Moderate 9 (34%) 9 (34%)Severe 2 (8%) 2 (8%) 1.00
Left ventricular mass index⁎ 42 ± 13 40 ± 14 0.37Left ventricular ejection
fraction (%)67 ± 8 68 ± 8 0.72
⁎Calculated in 48 women; coronary risk factors, hypertension, smoking, diabetemellitus, or hyperlipidemia.
Figure 2
Tzemos et al 477American Heart JournalVolume 157, Number 3
s
Late cardiac outcomes in matched women from postpregnant andnever-pregnant groups.
5 required intervention (1 early, 4 later interventions). Inaddition to the aforementioned woman with critical ASwho underwent postpartum valve replacement, 5 of theother 6 women who experienced pregnancy-relatedcardiac events subsequently underwent cardiac surgeryin the late follow-up period despite being asymptomaticin the postpartum period, including both women whorequired percutaneous valvuloplasty during pregnancy.The late event rate was 40% in the 44 women who wereevents-free at 1 year. The only mortality was frompostoperative hemorrhage in a woman who underwent
redo valve surgery for symptomatic prosthetic aorticvalve regurgitation.On multivariate analysis, the following baseline vari-
ables were predictive of the need for late cardiacinterventions: moderate or severe AS (HR 4.5, 95% CI1.1-19.4, P = .045), and NYHA functional class II (HR 4.6,95% CI 1.4-15.4, P = .014). Due to small patient numbers,the categories of moderate and severe AS were combinedfor the purpose of multivariate analysis. In women withmild, moderate, and severe AS at the time of their baselineantenatal visit, 5-year event-free survival was 92%, 67%,and 14% respectively (Figure 1); freedom from latecardiac events was 50% in the moderate or severe ASgroup. Women with valvular AS (n = 47) have 5 yearevent-free survival of 92%, 65%, and 16% in those withmild, moderate, or severe AS, respectively. There was nosignificant difference in the late event rate between thosewomen who presented to our centre during their firstpregnancy (15 [41%] of 37 women) compared to thosewho were followed at other centers during their priorpregnancies(7 [50%] of 14 women, P = .54). Onunivariate Cox regression, multiple pregnancies with ASwas not predictive of late cardiac events (P = .95).The baseline characteristics of the 26 women from the
postpregnant group and the corresponding 26 age range-and lesion-matched women from the never-pregnantgroup are displayed in Table III. There were no significantdifferences between the 2 groups other than a 1-yeardifference in mean maternal age. Follow-up duration wassimilar in the 2 groups (8 ± 4 vs 6 ± 4 years, postpregnantvs never-pregnant groups, P = .11). Eight women in thepostpregnant group (31%) underwent late cardiac inter-ventions compared to none in the never-pregnant group
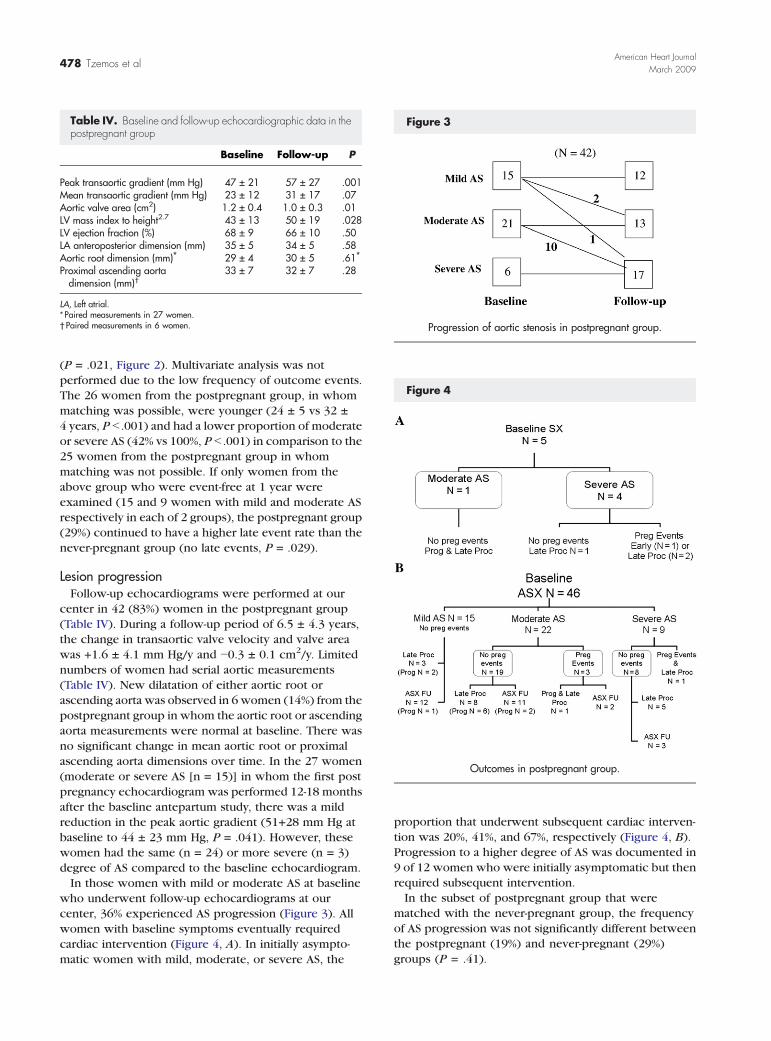
Table IV. Baseline and follow-up echocardiographic data in thepostpregnant group
Baseline Follow-up P
Peak transaortic gradient (mm Hg) 47 ± 21 57 ± 27 .001Mean transaortic gradient (mm Hg) 23 ± 12 31 ± 17 .07Aortic valve area (cm2) 1.2 ± 0.4 1.0 ± 0.3 .01LV mass index to height2.7 43 ± 13 50 ± 19 .028LV ejection fraction (%) 68 ± 9 66 ± 10 .50LA anteroposterior dimension (mm) 35 ± 5 34 ± 5 .58Aortic root dimension (mm)⁎ 29 ± 4 30 ± 5 .61⁎Proximal ascending aortadimension (mm)†
33 ± 7 32 ± 7 .28
LA, Left atrial.⁎ Paired measurements in 27 women.† Paired measurements in 6 women.
Figure 3
Progression of aortic stenosis in postpregnant group.
478 Tzemos et alAmerican Heart Journal
March 2009
Figure 4
Outcomes in postpregnant group.
(P = .021, Figure 2). Multivariate analysis was notperformed due to the low frequency of outcome events.The 26 women from the postpregnant group, in whommatching was possible, were younger (24 ± 5 vs 32 ±4 years, P b .001) and had a lower proportion of moderateor severe AS (42% vs 100%, P b .001) in comparison to the25 women from the postpregnant group in whommatching was not possible. If only women from theabove group who were event-free at 1 year wereexamined (15 and 9 women with mild and moderate ASrespectively in each of 2 groups), the postpregnant group(29%) continued to have a higher late event rate than thenever-pregnant group (no late events, P = .029).
Lesion progressionFollow-up echocardiograms were performed at our
center in 42 (83%) women in the postpregnant group(Table IV). During a follow-up period of 6.5 ± 4.3 years,the change in transaortic valve velocity and valve areawas +1.6 ± 4.1 mm Hg/y and −0.3 ± 0.1 cm2/y. Limitednumbers of women had serial aortic measurements(Table IV). New dilatation of either aortic root orascending aorta was observed in 6 women (14%) from thepostpregnant group in whom the aortic root or ascendingaorta measurements were normal at baseline. There wasno significant change in mean aortic root or proximalascending aorta dimensions over time. In the 27 women(moderate or severe AS [n = 15)] in whom the first postpregnancy echocardiogram was performed 12-18 monthsafter the baseline antepartum study, there was a mildreduction in the peak aortic gradient (51+28 mm Hg atbaseline to 44 ± 23 mm Hg, P = .041). However, thesewomen had the same (n = 24) or more severe (n = 3)degree of AS compared to the baseline echocardiogram.In those women with mild or moderate AS at baseline
who underwent follow-up echocardiograms at ourcenter, 36% experienced AS progression (Figure 3). Allwomen with baseline symptoms eventually requiredcardiac intervention (Figure 4, A). In initially asympto-matic women with mild, moderate, or severe AS, the
proportion that underwent subsequent cardiac interven-tion was 20%, 41%, and 67%, respectively (Figure 4, B).Progression to a higher degree of AS was documented in9 of 12 women who were initially asymptomatic but thenrequired subsequent intervention.In the subset of postpregnant group that were
matched with the never-pregnant group, the frequencyof AS progression was not significantly different betweenthe postpregnant (19%) and never-pregnant (29%)groups (P = .41).

Tzemos et al 479American Heart JournalVolume 157, Number 3
DiscussionPrior studies on pregnancy outcome in women with
AS have focused on ante- and peripartum complica-tions.1-3,5,6,16 The frequency of pregnancy-relatedmaternal cardiac complications in the present study,with the largest number of patients to date, is one ofthe lowest reported. In contrast, long-term cardiacoutcomes in women with congenital AS undergoingpregnancy have not been systematically examined. Ina prior report examining 30 women with AS whounderwent pregnancy, 30% required surgical interven-tion at follow-up.4 The present study provided incre-mental information by the incorporation of acomparison group and by extending the mean follow-up to N5 years, allowing comparison with otheroutcome studies.11
Freedom from late cardiac events in our post pregnancygroup was better than that previously reported in patientswith valvular AS.11,17,18 Women with moderate andsevere valvular AS in our study have a 2 year event-freesurvival of 92% and 90% respectively, compared to 66%and 21% to 67% in prior studies examining nonpregnantpopulations with moderate and severe AS, respec-tively.11,17,18 The lower frequency of cardiac eventsobserved in the present study is likely a result of youngerage, ambulatory status, and the low frequency ofcomorbidities.11,17,18 The degree of valvular degenerationmay have been less advanced in our study groups, as4 women had valve morphology suitable for percuta-neous valvuloplasty.Similar to prior studies examining nonpregnant patients
with AS, cardiac intervention was the primary cardiacevent in our study.11,17,18 It was reassuring to note thatcardiac death was not the initial cardiac event in ourstudy. Our finding that baseline severity of AS predictedlate cardiac events extended the results of prior studiesexamining nonpregnant patients.11,17 The significant rateof late cardiac interventions in women with moderate ASwho underwent pregnancy is important for risk stratifi-cation, as current guidelines have focused on pregnantwomen with severe AS.9,19,20 In addition, the presence ofmild antepartum symptoms, likely a sign of inadequatecardiac reserve, predicted late cardiac outcomes even ifthe pregnancy was uneventful.Our study is the first to report that prior pregnancy is
associated with an increase in the frequency of latecardiac interventions in women with AS. While oneshould be cautious in applying the findings from a nonrandomized study, the 2 groups were well matchedwith respect to baseline characteristics. We were notable to identify a difference in AS progression betweenthe study and comparison groups, possibly due to smallsample size. It is possible that pregnancy may adverselyaffect LV mechanics and peripheral adaptation to AS,resulting in symptomatic deterioration without detect-
able changes in aortic valve area or LV ejectionfraction.21,22 Unfortunately, LV mechanics could not beanalyzed as most baseline echocardiograms were not indigital format. Stress echocardiography, with reportedclinical use in identifying a higher-risk subgroup ofasymptomatic patients with severe AS,10 was not astandard practice at our center nor mandated by currentguidelines.9
The rate of progressive narrowing of the aortic valvewas lower than reported in prior studies examiningnonpregnant older patients despite a follow-up durationthat exceeded that of previous studies.11,17,18 Thereduced lesion progression of congenital AS in youngerwomen may be related to the paucity of risk factorsimplicated in disease progression.23,24
LimitationsOur difficulty in achieving a match for the entire
postpregnant group was most likely a result of lowfrequency of AS in young women with BAV and themale predominance of BAV.25 To use men as controlsmay introduce confounding influence of sex, making itdifficult to interpret the results of between groupcomparisons. It is not possible to objectively documentthe absence of any pregnancy in the comparisongroup since this data was based on self-report. Wecannot fully evaluate the temporal trends in ASprogression, as subjects were retrospectively identifiedand follow-up evaluations during intermediate timepoints were not always performed at our center. Serialdata regarding aorta dimension need to be interpretedcautiously, as ascending aorta dimension was routinelymeasured only in recent years with the increasingrecognition of the association of aortopathy withBAV.26 Small sample size may have limited the abilityto determine whether the number of pregnanciesaffected late outcomes.Our study, the first to systematically examine late
cardiac outcomes in women with congenital AS under-going pregnancy, has important clinical implications.Firstly, the high rate of late cardiac interventions shouldbe incorporated into prepregnancy counseling. Thelong-term prognosis of women with AS who wish toundergo pregnancy should incorporate the severity ofAS and the presence/absence of even mild symptomaticlimitations. The novel observation that pregnancy wasassociated with a higher frequency of late cardiacinterventions in women with AS will require furtherevaluation. Our study data provide additional justifica-tion for current recommendations that women withsevere AS should be considered for interventions priorto pregnancy.9 However, for those who decline inter-vention or are already pregnant, our findings alsohighlight the importance of close follow-up of womenwith AS both during and after pregnancy.
480 Tzemos et alAmerican Heart Journal
March 2009
DisclosuresThis study was supported in part by a generous
donation from Mrs Josephine Rogers.
References1. Arias F, Pineda J. Aortic stenosis and pregnancy. J Reprod Med
1978;20:229-32.2. Hameed A, Karaalp IS, Tummala PP, et al. The effect of valvular heart
disease on maternal and fetal outcome of pregnancy. J Am CollCardiol 2001;37:893-9.
3. Lao TT, Sermer M, Magee L, et al. Congenital aortic stenosis andpregnancy—a reappraisal. Am J Obstet Gynecol 1993;169:540-5.
4. Silversides CK, Colman JM, Sermer M, et al. Early and intermediate-term outcomes of pregnancy with congenital aortic stenosis. Am JCardiol 2003;91:1386-9.
5. Siu SC, Sermer M, Colman JM, et al. Prospective multicenter study ofpregnancy outcomes in women with heart disease. Circulation 2001;104:515-21.
6. Yap SC, Drenthen W, Pieper PG, et al. Risk of complications duringpregnancy in women with congenital aortic stenosis. Int J Cardiol2008;126:240-6.
7. Siu SC, Sermer M, Harrison DA, et al. Risk and predictors forpregnancy-related complications in women with heart disease.Circulation 1997;96:2789-94.
8. Zoghbi WA, Enriquez-Sarano M, Foster E, et al. Recommendationsfor evaluation of the severity of native valvular regurgitation with two-dimensional and Doppler echocardiography. J Am Soc Echocardiogr2003;16:777-802.
9. Bonow RO, Carabello BA, Chatterjee K, et al. ACC/AHA 2006guidelines for the management of patients with valvular heart disease:a report of the American College of Cardiology/American HeartAssociation Task Force on Practice Guidelines (writing Committee toRevise the 1998 guidelines for the management of patients withvalvular heart disease) developed in collaboration with the Society ofCardiovascular Anesthesiologists endorsed by the Society forCardiovascular Angiography and Interventions and the Society ofThoracic Surgeons. J Am Coll Cardiol 2006;48:e1-e148.
10. Lancellotti P, Lebois F, Simon M, et al. Prognostic importance ofquantitative exercise Doppler echocardiography in asymptomaticvalvular aortic stenosis. Circulation 2005;112(9 Suppl):I377-82.
11. Pellikka PA, Sarano ME, Nishimura RA, et al. Outcome of622 adults with asymptomatic, hemodynamically significant aorticstenosis during prolonged follow-up. Circulation 2005;111:3290-5.
12. Lang RM, Bierig M, Devereux RB, et al. Recommendations forchamber quantification: a report from the American Society ofEchocardiography's Guidelines and Standards Committee and theChamber Quantification Writing Group, developed in conjunctionwith the European Association of Echocardiography, a branch of theEuropean Society of Cardiology. J Am Soc Echocardiogr 2005;18:1440-63.
13. Quinones MA, Waggoner AD, Reduto LA, et al. A new, simplifiedand accurate method for determining ejection fraction withtwo-dimensional echocardiography. Circulation 1981;64:744-53.
14. Stamm RB, Carabello BA, Mayers DL, et al. Two-dimensionalechocardiographic measurement of left ventricular ejection fraction:prospective analysis of what constitutes an adequate determination.Am Heart J 1982;104:136-44.
15. Weyman A. Normal cross-sectional echocardiographic measure-ments. In: Weyman A, editor. Principles and practice of echocar-diography. 2nd ed. Malvern: Lea and Febiger; 1994. p. 1289-98.
16. Lesniak-Sobelga A, Tracz W, KostKiewicz M, et al. Clinical andechocardiographic assessment of pregnant women with valvularheart diseases—maternal and fetal outcome. Int J Cardiol 2004;94:15-23.
17. Otto CM, Burwash IG, Legget ME, et al. Prospective study ofasymptomatic valvular aortic stenosis. Clinical, echocardiographic,and exercise predictors of outcome. Circulation 1997;95:2262-70.
18. Rosenhek R, Binder T, Porenta G, et al. Predictors of outcome insevere, asymptomatic aortic stenosis. N Engl J Med 2000;343:611-7.
19. Expert consensus document on management of cardiovasculardiseases during pregnancy. Eur Heart J 2003;24:761-81.
20. Elkayam U, Bitar F. Valvular heart disease and pregnancy part I:native valves. J Am Coll Cardiol 2005;46:223-30.
21. Schaefer BM, Lewin MB, Stout KK, et al. Usefulness of bicuspid aorticvalve phenotype to predict elastic properties of the ascending aorta.Am J Cardiol 2007;99:686-90.
22. Tzemos N, Silversides CK, Carasso S, et al. Effect of pregnancy on leftventricular motion (twist) in women with aortic stenosis. Am J Cardiol2008;101:870-3.
23. Yap SC, Kouwenhoven GC, Takkenberg JJ, et al. Congenital aorticstenosis in adults: Rate of progression and predictors of clinicaloutcome. Int J Cardiol 2007;122:224-31.
24. Palta S, Pai AM, Gill KS, et al. New insights into the progression ofaortic stenosis: implications for secondary prevention. Circulation2000;101:2497-502.
25. Lewin MB, Otto CM. The bicuspid aortic valve: adverse outcomes frominfancy to old age. Circulation 2005;111:832-4.
26. Keane MG, Wiegers SE, Plappert T, et al. Bicuspid aortic valves areassociated with aortic dilatation out of proportion to coexistentvalvular lesions. Circulation 2000;102(19 Suppl 3):III35-9.
Related Documents