UPDATES IN RELAPSED/REFRACTORY B-CELL ACUTE LYMPHOBLASTIC LEUKEMIA (ALL) Larry W. Buie, Pharm.D., BCOP, FASHP Manager, Adult Clinical Pharmacy Services PGY2 Adult Oncology Residency Program Director Memorial Sloan Kettering Cancer Center 5 August 2017

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

UPDATES IN RELAPSED/REFRACTORY B-CELL ACUTE LYMPHOBLASTIC LEUKEMIA (ALL)
Larry W. Buie, Pharm.D., BCOP, FASHP Manager, Adult Clinical Pharmacy Services PGY2 Adult Oncology Residency Program Director Memorial Sloan Kettering Cancer Center 5 August 2017

Faculty Disclosures • Advisory board member for Pfizer regarding
inotuzumab
• Advisory board member for Amgen regarding blinatumomab
– Other Advisory Board Participation
• Taiho Oncology, Inc
• Onconova Therapeutics, Inc
• ProStrakan, Inc
• Teva Pharmaceuticals, Inc
• Off-label and investigational use of medications will be discussed

Objectives
• Discuss the role of conventional chemotherapy and hematopoietic stem cell transplantation in the management of relapsed or refractory (r/r) B-cell ALL
• Review appropriate strategies and monitoring plans with tyrosine kinase inhibitors (TKIs) in r/r Philadelphia-Chromosome positive (Ph+) ALL
• Describe the role of immunotherapy in patients with r/r B-cell ALL, with emphasis on monoclonal antibodies, BiTE® therapy with blinatumomab and cellular therapy with CAR T- cells

ALL Overview
• Proliferation of immature lymphoid cells in bone marrow, peripheral blood or other organs
• 6590 new cases and 1430 deaths estimated in US in 2017
– 80% less than 20 years of age
– 20% adult leukemias
• Risk factors
– >70 years of age
– Exposure to chemotherapy or radiation
– Genetic disorders
• 5 year survival decreases substantially with age
NCCN. Acute Lymphoblastic Leukemia.Version 1. 2017. Available at http://www.nccn.org/professionals/physician_gls/pdf/all.pdf. Accessed 7/1/2017.
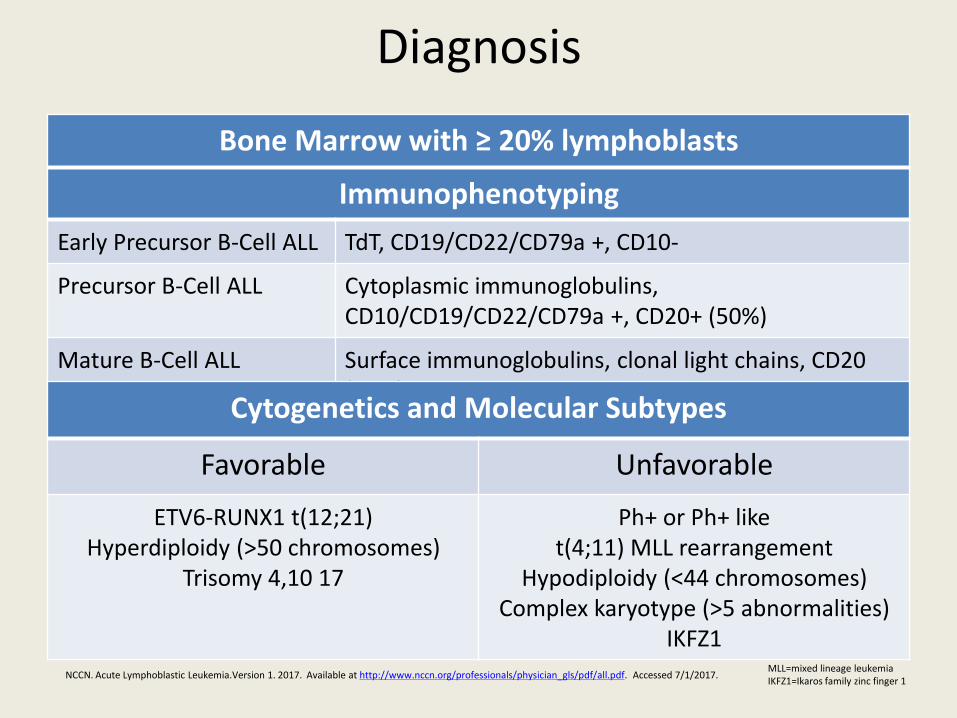
Diagnosis
Immunophenotyping
Early Precursor B-Cell ALL TdT, CD19/CD22/CD79a +, CD10-
Precursor B-Cell ALL Cytoplasmic immunoglobulins, CD10/CD19/CD22/CD79a +, CD20+ (50%)
Mature B-Cell ALL Surface immunoglobulins, clonal light chains, CD20 (80%), TdT -
Cytogenetics and Molecular Subtypes
Favorable Unfavorable
ETV6-RUNX1 t(12;21) Hyperdiploidy (>50 chromosomes)
Trisomy 4,10 17
Ph+ or Ph+ like t(4;11) MLL rearrangement
Hypodiploidy (<44 chromosomes) Complex karyotype (>5 abnormalities)
IKFZ1
Bone Marrow with ≥ 20% lymphoblasts
MLL=mixed lineage leukemia IKFZ1=Ikaros family zinc finger 1
NCCN. Acute Lymphoblastic Leukemia.Version 1. 2017. Available at http://www.nccn.org/professionals/physician_gls/pdf/all.pdf. Accessed 7/1/2017.

Poor Prognostic Factors in Adult ALL
Prognostic Variable Negative Prognostic Association
Age >35 years
Initial WBC >30 X 109 cells/L
Cytogenetics Philadelphia chromosome + t(4;11) MLL rearrangement t(8;14) MYC Complex karyotype (>5 abnormalities) Hypodiploidy (30-39 chromosomes)
Risk stratification Standard High-Risk
Fielding AK et al. Blood 2007; 109:944-950
NCCN. Acute Lymphoblastic Leukemia.Version 1. 2017. Available at http://www.nccn.org/professionals/physician_gls/pdf/all.pdf. Accessed 7/1/2017.

Management of Adult ALL Induction Goal: Reduce tumor burden
•Backbone: vincristine, anthracycline, steroids ± asparaginase •Linker, Hyper-CVAD, AYA protocols •±CD 20 targeted therapy •TKI if Ph+
CNS Prophylaxis Goal: Prevent CNS disease •Radiation •IT chemotherapy •High dose systemic therapy
Consolidation/ Intensification
Goal: Eliminate residual leukemia •High dose chemotherapy •6-MP/thioguanine •Asparaginase •TKI if Ph+ •HSCT if high risk
Maintenance Goal: Prevent disease relapse •POMP •TKI if Ph+ •Radiation to scrotal sac if testicular involvement
AYA=adolescent and young adult
6-MP=6-mercaptopurine
POMP=6-MP, vincristine, methotrexate and prednisone
NCCN. Acute Lymphoblastic Leukemia.Version 1. 2017. Available at http://www.nccn.org/professionals/physician_gls/pdf/all.pdf Accessed 7/1/2017.

Meet Patient KS
40 yo male with Ph- B-cell ALL diagnosed in 12/2012
• Pediatric inspired protocolCR1; relapse 5/2014
– BM Bx
• 40% blasts
• Abnormal B-cell population detected – CD10(bright), CD19 (bright),CD20 (subset, <20%),CD22+,
CD38/CD45 (dim), CD34 (absent)
• Plan is for a clofarabine containing regimen
• His brother is determined to be a donor option

Predictors for Outcomes in R/R ALL
• Duration of first remission
• Response to salvage
• Age
• Ability to undergo HSCT
• Molecular response
Gokbuget N, et al. Blood 2012;120:2032-2041 Frey NV, et al. Blood 2015;126:589-596

Minimal Residual Disease (MRD)
• MRD is the presence of leukemic cells below the threshold of detection by conventional morphologic methods
• May have a CR with MRD positivity • Flow cytometry
– Detects abnormal phenotypes
• PCR – Fusion genes – Clonal rearrangements in immunoglobulin heavy chain genes – T-cell receptor gene rearrangements
• MRD increases risk of relapse • MRD may emerge due to immune escape mechanisms • MRD persistence may be useful in predicting future course of treatment
PCR=polymerase chain reaction NCCN. Acute Lymphoblastic Leukemia.Version 1. 2017. Available at http://www.nccn.org/professionals/physician_gls/pdf/all.pdf. Accessed 7/1/2017.

Myth: The Second Remission
Trial
First CR Rate
Relapse Rate
Time to Relapse
Median Survival
1-year OS
5 year OS
ECOG 2993 (N=1508)
91% 44% 11 months 6 months 22% 7%
PETHEMA (N=589)
89% 50% 11 months 4.5 months
24% 10%
Oriol A et al. Haematologica 2010;95;589-596 Fielding AK et al. Blood 2007; 109:944-950
Bottom line: Survival is poor for patients with r/r B-Cell ALL without consolidative transplant

Role of HSCT in ALL
• Benefit of HSCT in CR1 has been seen in multiple clinical trials and meta-analyses for high risk patients
• No consensus for transplantation with standard risk ALL in CR1 • Ph+ patients have best results from allogeneic stem cell
transplantation in first CR with molecular remission • Minimal residual disease presence after CR has been shown to
predict relapse-free survival • Allogeneic HSCT is the best curative option for patients achieving
CR2 • Allogeneic HSCT is preferred over autologous HSCT
NCCN. Acute Lymphoblastic Leukemia.Version 1. 2017. Available at http://www.nccn.org/professionals/physician_gls/pdf/all.pdf Accessed 7/1/2017.

Criteria for Complete Response
• No circulating blasts or extramedullary disease
• Trilineage hematopoiesis with <5% blasts
• ANC >1000/microL
• Platelets >100,000/microL
• No recurrence at 4 weeks
• May have a CR with incomplete count recovery
NCCN. Acute Lymphoblastic Leukemia.Version 2. 2015. Available at http://www.nccn.org/professionals/physician_gls/pdf/all.pdf. Accessed 10/21/2015

Historical Salvage Experience • MD Anderson
– 288 patients treated between 1980 and 2007
– 53% had a CR after salvage chemotherapy
– Median duration of remission was 7 months
Response Rates by Therapy Received
Therapy Number of Patients Number of CRs (%)
VAD/Hyper-CVAD 61 17 (28)
Cytarabine Combinations 54 17 (32)
Allogeneic HSCT 22 9 (41)
Methotrexate/Asparaginase 52 3 (6)
Other combinations 29 4(14)
Single Agent 70 3 (4)
O’Brien S et al. Cancer 2008;113:3186-3191

Cytarabine Containing Regimens
N=88 Previously treated ALL Relapsed or refractory
disease after induction
chemotherapy
Hyper-CVAD X 8 alternating
courses Vincristine 2 mg IV d1,8,15
Dexamethasone 80 mg IV or PO d1-4,15-18
Weekly Asparaginase or monthly pegasparaginase with each cycle
IT prophylaxis
Maintenance X 12 months
Faderl S et al. Clinical Lymphoma, Myeloma & Leukemia 2011;11:54-59
Primary Endpoints: CR and induction mortality rates

Cytarabine Containing Regimens Results from Augmented Hyper-CVAD
CR CRp (incomplete PLT recovery) ORR
47% 13% 64%
Median remission duration 5 months
Median OS for CR 10.2 months
HSCT 32%
Safety Induction mortality Asparaginase Associated Anaphylactic reactions Coagulopathy
9% 4% 2%
Faderl S et al. Clinical Lymphoma, Myeloma & Leukemia 2011;11:54-59

Clofarabine Containing Regimens
N=55 Previously treated ALL Relapsed or refractory
disease after induction
chemotherapy
VANDEVOL N=37 Dexamethasone 10 mg/m2/q12h
d1-5 Mitoxantrone 8 mg/m2/d d3-4 Etoposide 150 mg/m2/d d3-5
Peg-asparaginase 2500 UI/m2 d7 Clofarabine 30 mg/m2/d d1-5
ENDEVOL N=18 Cyclophosphamide 300
mg/m2/d d1-3 Clofarabine 30 mg/m2/d d1-5
Primary Endpoints: CR rate
OR
Pigneux A, et al. Blood 2011;118:Abstract 2586 d=day

Clofarabine Containing Regimens
Results from Clofarabine Containing Regimens
VANDEVOL ENDEVOL
CR 41% 50%
Early death 14% 6%
HSCT rate 29% in both groups
Safety Grade 3-4 infection Neurological GI Liver Abnormality
59% 14% 14% 30%
56% None None 11%
Pigneux A, et al. Blood 2011;118:Abstract 2586

Vincristine Sulfate Liposome Injection (VSLI)
N=65 Ph- ALL
Second or greater relapse (chemo or HSCT)
At least one CR with 90 day leukemia free interval
Weekly VSLI 2.25 mg/m2 without dose capping on
D 1,8,15,22 of a 28 day cycle
Response Progression
Toxicity HSCT
O’Brien S, et al. J Clin Oncol 2013;31:676-683
Primary Endpoint: CR and CRi rates Secondary Endpoints: CR/CRi duration, OS, HSCT, ORR
CRi=complete remission with incomplete count recovery

Vincristine Sulfate Liposome Injection Results for Vincristine Sulfate Liposome Injection (VSLI)
CR CRi ORR
11% 9% 35%
Time to CR (median) 54 days
CR and CRi duration 23 weeks
OS OS rates
4.6 months 35% at 6 months, 8% at 12-18 months, 4% at 2 years
HSCT OS
19% 9.3 months
MRD negativity among responders 67%
Adverse Events Neuropathy grade 3 Constipation grade 3 30 day mortality
23% 3% 12%
O’Brien S, et al. J Clin Oncol 2013;31:676-683
Back to KS, ARS #1
• KS received the clofarabine containing regimen with no response. He went on to complete 2 cycles of VSLI. His repeat bone marrow shows CR2 with MRD negativity. What should be the next step?
1. Continue VSLI until disease progression
2. Offer HSCT
3. Place on maintenance therapy with POMP
4. Hold additional treatment until MRD positive

MONOCLONAL ANTIBODIES

Rituximab for CD20+ Disease: Phase III
N=209 Ph- B-lineage ALL NEWLY diagnosed
>20% CD20 expression on leukemic cells
N=105 Chemotherapy Plus Rituximab 375 mg/m2:
Induction D1, 7 Salvage (if needed) D1, 7
Consolidation Blocks 1,3 4,6 Late intensification D1,7 Maintenance 6 infusions
Total 16-18 doses of rituximab
Maury S, Chevret S, Thomas X, et al. N Engl J Med 2016;375:1044-53.
Primary Endpoint: EFS
Secondary Endpoints: hematologic remission, relapse during first remission, death during first remission, OS, safety
CD20 present on majority of B cells Present on 30-50% of B-cell precursor ALL Blasts
GRAALL-2005/R
N-104 Chemotherapy Alone

GRAALL-2005/R Results Variable Rituximab Group
(N=105) Control Group (N=104)
P-Value, HR
EFS, 2 years 65% 52% 0.04, 0.66
Relapse, 2 years 18% 32% 0.02, 0.52
Death during first remission
12% 12% 0.96, 0.98
OS, 2 years 71% 61% 0.10
CR, Induction 92% 90%
MRD-, induction 65% 61%
MRD-, consolidation 91% 82%
Transplant first CR 34% 20%
Older age, CNS involvement, High WBC associated with poorer EFS Fewer asparaginase allergic reactions in rituximab group, P=0.002
Rituximab should be considered during r/r ALL disease if CD20 expression>20%
Maury S, Chevret S, Thomas X, et al. N Engl J Med 2016;375:1044-53.

Inotuzumab Ozogamicin
• Humanized monoclonal antibody targeting CD22
• Antibody-drug (calicheamicin) conjugate
• Low levels of CD22 expression results in high intracellular calicheamicin levels
• Results in G2/M cell cycle arrest
Ohanian M, et al. Expert Opinion on Biological Therapy 2015;15 (4):601-611

Phase III INO-VATE: Inotuzumab versus Chemotherapy
N=218 B-lineage ALL :
-relapsed or refractory CD22-positive
Ph+ or Ph- -first or second salvage
N=109
Inotuzumab Ozogamicin 0.8 mg/m2 d1
0.5 mg/m2 d8, 15 Cycle 1=21 days
≥ Cycle2=28 days
Kantarjian HM, et al. Inotuzumab ozogamicin versus standard therapy for acute lymphoblastic leukemia. N Engl J Med 2016;375:740-53.
Primary Endpoint: CR, OS Secondary Endpoints: Duration of remission, progression-free survival, rate of stem
cell tranplantation, MRD response, safety
Prospective, randomized, phase III trial
N=109
Chemotherapy: FLAG
Cytarabine + mitoxantrone High dose Cytarabine

Inotuzumab Ozogamicin End Point Inotuzumab Standard
Therapy Between Group
Difference P-value
No/total % No/total % %
Complete remission or complete remission with Incomplete hematologic recovery
Total BM blasts below MRD
88/109 69/88
80.7 78.4
32/109 9/32
29.4 28.1
51.4 50.3
<0.001 <0.001
Complete Remission
Total BM blasts below MRD
39/109 35/39
35.8 89.7
19/109 6/19
17.4 31.6
18.3 58.2
0.002 <0.001
Complete remission with Incomplete hematologic recovery
Total BM blasts below MRD
49/109 34/49
45.0 69.4
13/109 3/13
11.9 23.1
33.0 46.3
<0.001 0.004
Kantarjian HM, et al. Inotuzumab ozogamicin versus standard therapy for acute lymphoblastic leukemia. N Engl J Med 2016;375:740-53.

Inotuzumab Ozogamicin: Secondary Endpoints
Inotuzumab Ozogamicin
Standard-Therapy Group HR (P=)
Duration of Remission
4.6 Months 3.1 Months 0.55 (P=0.003)
PFS 5.0 Months 1.8 Months 0.45 (P<0.001)
OS 7.7 Months 6.7 Months 0.77 (P=0.04)
Kantarjian HM, et al. Inotuzumab ozogamicin versus standard therapy for acute lymphoblastic leukemia. N Engl J Med 2016;375:740-53.

Inotuzumab Ozogamicin: Safety
Serious Adverse Event
Inotuzumab Ozogamicin (N=139)
Standard-Therapy Group (N=120)
Any Grade Grade ≥3 Any Grade Grade ≥3
Any Event 67 (48) 64 (46) 55 (46) 52 (43)
Febrile Neutropenia
16 (12) 15 (11) 22 (18) 21 (18)
VOD 15 (11) 13 (9) 1 (1) 1 (1)
Sepsis 3 (2) 3 (2) 6 (5) 6 (5)
Pyrexia 4 (3) 2 (1) 3 (2) 1 (1)
Kantarjian HM, et al. Inotuzumab ozogamicin versus standard therapy for acute lymphoblastic leukemia. N Engl J Med 2016;375:740-53.

NOVEL IMMUNOTHERAPY: BITE ANTIBODIES AND CAR T-CELLS

Tumor Immune Escape
• Metabolically hostile microenvironment • Thymic selection • T-cell anergy • Impaired tumor MHC antigen presentation • Increased expression of negative co-stimulatory ligands • Expansion of Tregs • Increased production of inhibitory enzymes and cytokines • Downregulation of NK cells
Dunn GP, et al. Annu Rev Immunol 2004;22:329-360
Tregs=regulatory T-cells
NK=natural killer

Harnessing the Immune System
• Stem cell transplant
• Vaccination
• Cytokine therapy
• Immune checkpoint inhibitors
• Adoptive transfer of tumor infiltrating cells
• Bi-specific T-cell engaging antibody (BiTE®) therapy
• Chimeric antigen receptor (CAR) T-cells
Dunn GP, Old JL et al. The three Es of Cancer Immunoediting. Annu Rev Immunol 2004;22:329-60

BiTE® Antibodies: Blinatumomab
• Produced by Chinese hamster ovary cells
– 2 single chain antibodies • Heavy and light chains of larger antibodies
• Joined by a linker
• Force the formation of an immunologic synapse between T-cells and tumor cells – Occurs by simultaneous binding of BiTE antibodies to CD3ε on T-cells
and a surface target antigen on cancer cells
– Independent of MHC presentation and T cell receptor specificity
Frankel SR, et al. Current Opinion in Chemical Biology 2013;17:385-392 .Permission granted. MHC=major histocompatibility complex
Blinatumomab Mechanism of Action
• Binds CD19 on target B-Cell and CD3 on T-Cell – Induces a cytolytic synapse – Granules containing granzymes and perforin fuse with T-
cell membrane and release – Granzymes penetrate target cells perforated by perforin – Apoptosis of target CD19 cell is activated by granzyme B – Activation markers on T-cell (CD69 and CD25) remain
expressed and T-cells are capable of serial lysis and expansion
Nagorsen D, et al. Experimental Cell Research 2011;317:1255-1260

Blinatumomab Pharmacokinetics
Pharmacokinetics Linear over dose range of 5 to 90 mcg/m2/day
Distribution Vd 4.52 L with continuous infusion
Metabolism Degraded to small peptides and amino acids via catabolic pathways
Elimination Half-life was 2.11 hr; negligible amounts excreted in the urine
Special populations Age, gender, body weight and body surface area do not influence PK of blinatumomab
Renal impairment No information for dialysis or severe renal impairment; mild to moderate impairment similar to normal renal function
Buie LW et al. Ann Pharmacother 2015;49:1057-1067

Blinatumomab Pharmacodynamics
Peripheral T-cell redistribution
Occurred after initiation of infusion or dose escalation; T-cell counts declined within 1-2 days and returned to baseline with 7 to 14 days
Peripheral B-cell Counts Decreased to less than 10 cells/microliter during the initial treatment; no recovery of peripheral B-cell counts during the treatment free period
Cytokines IL-6, IL-10 and IFN-γ were increased within the first 2 days and returned to normal within 48 hours; subsequent cycles resulted in lower cytokine elevations
Topp MS, et al. J Clin Oncol 2011;29:2493-2498

Activity/Safety Expanded in R/R B-ALL
N=189 Ph- B-lineage ALL refractory after
induction Relapsed within 12
months of first remission or HSCT
≥10% blasts ECOG ≤2
Life expectancy ≥12 weeks
>50% blasts or WBC ≥15000 cells/μL
Elevated LDH
Prephase dexamethasone
10-24 mg/m2/d for up to 5 days
Blinatumomab CI 9 mcg/day for 1 week
28 mcg/day for 3 weeks
Dexamethasone 20 mg premedication
Two weeks treatment free between cycles
Topp MS, Gokbuget N et al. Lancet Oncol 2015;16:57-66
Primary Endpoint: CR or CRh at 2 cycles
Secondary Endpoints: RFS, OS, HSCT, 100 day HSCT mortality, adverse events Exploratory Endpoint: MRD Response
CRh=complete remission with partial hematologic recovery

Activity/Safety Expanded in R/R B-ALL
Response Rates
Category Patient Numbers %
Overall Response (CR/CRh)
81/189 43
Best Response CR CRh No response Not Evaluable
63/189 18/189 90/189 18/189
33 10 48 10
HSCT after CR or CRh Allo after CR Allo after CRh 100 day mortality
32/81 28/63 4/18
40 44 22 11
MRD Response 60/73 82
OS 6.1 months Topp MS, et al. Lancet Oncol 2015;16:57-66

Activity/Safety Expanded in R/R B-ALL
Adverse Events
Event Number (%) Grade 3 to 4 (%)
Any Event 188 (99) 68
Febrile neutropenia 53 (28) 25
Neutropenia 33 (17) 16
Anemia 38 (20) 14
Pneumonia 18 (10) 9 ( 2 grade 5)
Thrombocytopenia 21 (11) 8
Hyperglycemia 24 (13) 8
Leucopenia 19 (10) 8
Transaminitis 24 (13) 7
Hypokalemia 45 (24) 7
Pyrexia 113 (60) 7
Sepsis 13 (7) 4 (4 grade 5)
Hypophosphatemia 13 (7) 5
Topp MS, et al. Lancet Oncol 2015;16:57-66

Activity/Safety Expanded in R/R B-ALL
Neurologic Adverse Events
Event Number (%) Grade 3 to 4
Any Event 98 (52) 13
Tremor 33 (17) 1
Dizziness 26(14) 1
Confusion 14 (7) 2
Encephalopathy 10 (5) 4
Ataxia 9 (5) 2
Somnolence 9 (5) 1
Mental status change 7 (4) 1
Convulsion 4 (2) 1
Syncope 1 (<1) <1
Neurological toxicities, which may be severe, life-threatening, or fatal, occurred in patients receiving blinatumomab. Interrupt or
discontinue blinatumomab as recommended.
Topp MS, et al.. Lancet Oncol 2015;16:57-66

Cytokine Release Syndrome
• Cytokine release syndrome
– Increased IL-6, IL-10 and INF-γ
– Fever, headache, chills, flu-like symptoms, nausea
– Elevated LFTs
– Hypotension
– Severe Cases: capillary leak syndrome, DIC, HLH/MAS
– May be indistinguishable from infusion reactions
Cytokine Release Syndrome (CRS), which may be life-threatening or fatal, occurred in patients receiving blinatumomab. Interrupt or
discontinue blinatumomab as recommended.
Teachey DT, et al. Blood 2013;121:5154-57
HLH=hemophagocytic lymphohistiocytosis
MAS=macrophage-activation syndrome

Phase III Tower: Blinatumomab verus Chemotherapy
N=405 Ph- B-lineage ALL :
-Refractory to primary induction or salvage with
intensive chemo -Relapsed within 12 months
of first remission -Second or greater relapse
-Relapse after HSCT > 5% blasts ECOG ≤ 2
N=271
Blinatumomab: 6-week cycle 9 mcg/day ->
28 mcg/day x 4 weeks 2 weeks off
Stratification:
Age Salvage
Prior HSCT
Kantarjian H, Stein A, Gokbuget N, et al. Blinatumomab verus chemotherapy for advanced acute lymphoblastic leukemia. N Engl J Med 2017;376:836-47.
Primary Endpoint: OS Secondary Endpoints:CR rates, duration of repsonse, MRD response, EFS, rate of
AlloSCT, adverse events
Prospective, randomized, phase III trial
N=134
Chemotherapy: FLAG ± Anthracycline High-dose AraC based High dose MTX based
Clofarabine based

Tower Results: Overall Survival
Kantarjian H, Stein A, Gokbuget N, et al. Blinatumomab verus chemotherapy for advanced acute lymphoblastic leukemia. N Engl J Med 2017;376:836-47.

Tower Results: Remission Rates
MRD response: 76% blinatumomab 48% chemotherapy
Allogeneic Stem Cell Transplantation:
24% in each group
Kantarjian H, Stein A, Gokbuget N, et al. Blinatumomab verus chemotherapy for advanced acute lymphoblastic leukemia. N Engl J Med 2017;376:836-47.

Tower: Adverse Events Adverse Events, N (%)
Event Blinatumomab (N=267) Chemotherapy (N=109)
Any adverse event 263 (98.5) 108 (99.1)
Event leading to premature discontinuation
33 (12.4) 9 (8.3)
Serious adverse event 165 (61.8) 49 (45.0)
Fatal serious adverse event
51 (19.1) 19 (17.4)
≥ grade 3 event Neutropenia Infection Elevated liver enzymes Neurologic events CRS Infusion reaction Lymphopenia
231 (86.5) 101 (37.8) 91 (34.1) 34 (12.7) 25 (9.4) 13 (4.9) 9 (3.4) 4 (1.5)
100 (91.7) 63 (57.8) 57 (52.3) 16 (14.7)
9 (8.3) 0
1 (0.9) 4 (3.7)
Kantarjian H, Stein A, Gokbuget N, et al. Blinatumomab verus chemotherapy for advanced acute lymphoblastic leukemia. N Engl J Med 2017;376:836-47.

Treatment of CRS/Neurotoxicity
• Dexamethasone
– 24 mg IV or PO/day
– Tapered to off over a 4 day period
• Tocilizumab
– 8 mg/kg over 60 minutes
– Rarely necessary
MSK IRB 12-069. Accessed online 10/21/2015. Website Not Publically Available

Additional Blinatumomab Information Dose modification If an interruption is >7 days, begin new cycle
Grade 4 CRS or neurotoxicity Discontinue permanently
Grade 3 CRS Hold until resolved, restart at 9 mcg/day
Grade 3 Neurotoxicity Discontinue permanently if >1 seizure occurs Withhold until toxicity is not greater than grade 1 and at least 3 days, restart at 9 mcg/day Greater than 7 days to resolve, discontinue permanently
Hepatotoxicity Interrupt if transaminases >5X ULN or bilirubin >3X ULN
Drug Interactions No formal drug interaction studies Cytokines may suppress CYP metabolic enzymes Monitor patients receiving CYP substrates that have a narrow therapeutic index Highest risk is at drug initiation and when the dose is increased
Admixture and Administration
Must add IV solution stabilizer to the bag prior to blinatumomab Infusions must be calculated to run for 24 hours to 7 days as per the package insert May use CADD® pumps for outpatient or inpatient administration Efforts to minimize drug waste should be utilized Patients should never run out of drug waiting for a bag to be changed
Buie LW et al. Ann Pharmacother 2015;49:1057-1067 CADD=computerized ambulatory delivery device

Chimeric Antigen Receptor T-Cells (CAR-T)
• Autologous Transfer
– Apheresis
– Gene transfer • CAR design
– CD3ζ signaling element
– Costimulatory receptor
– Anti-CD19 single chain variable fragment
• Armored CAR T-cells – Multiple costimulatory receptors
• Suicide genes may be incorporated
– Expansion
– Reinfusion
Davila ML and Brentjens R. Hematol Oncol Clin N Am 2013;27:341-353 . Permission granted.

Dose, Tumor Burden, and Conditioning
• No significant correlation between T-cell expansion and clinical outcome
• Results are best in patients that have the lowest tumor burden
– T-cells may become exhausted in patients with excessive tumor bulk or antigen specific burden
• Conditioning with chemotherapy or radiation improves efficacy
– Optimal conditioning regimen remains unknown • Should include a tumor-responsive conditioning regimen
– Reduction in tumor bulk – Enhances antigen presentation for endogenous immune
response – Enhances persistence and function of CAR-Ts
Davila ML and Brentjens R. Hematol Oncol Clin N Am 2013;27:341-353

CAR-Ts in B-Cell ALL: Eliana
N=88 Pediatric and adults
CD19+ R/R B-cell ALL
≥5% lymphoblasts 59% prior alloSCT
Leukapheresis
Conditioning
T-Cell Infusion (N=68)
Primary Outcome:
Overall Remission Rates
(CR+Cri) Within 3 months
Buechner J, Grupp SA, Maude SL, et al. European Hematology Association 2017; Abstract S476.
Single-arm, open-label, multicenter, phase II study
Secondary Endpoints: Duration of Remission, OS, safety, cellular kinetics

CAR-Ts in B-Cell ALL: Eliana
• 83% achieved CR/CRi within 3 months
• All had MRD negative bone marrow – 13% proceeded to alloSCT within 6 months
• Relapse free survival 75% at 6 months
• Median duration of response not reached
• 6 month overall survival 89%, 75% at 12 months
• CRS 78% and no deaths – 38% received tocilizumab
• Other non-hematologic toxicities: hypotension, hypoxia, LFT abnormalities
Buechner J, Grupp SA, Maude SL, et al. European Hematology Association 2017; Abstract S476.
ODAC greenlights tisagenlecleucel (Novartis CTL019) for FDA approval later this year based on Eliana results

Safety of CAR-Ts in ALL
• Cytokine-release syndrome (CRS)
– Associated with peak cytokine elevations consistent with T-cell expansion and proliferation
– Can be mild to moderate or severe and life-threatening
– Systemic markers of inflammation were elevated in all patients
• C-reactive protein
• Ferritin
– Disease burden was associated with CRS • Treat with tocilizumab 8 mg/kg X 1 if necessary—AVOID STEROIDS!
• Encephalopathy with aphasia, confusion, delirium and hallucinations
• B-cell aplasia
Maude SL, Frey N, Shaw PA et al. N Engl J Med 2014;371:1507-17

Grading of CRS CRS revised grading system
Grade Toxicity
1 Symptoms are not life threatening and require symptomatic treatment only
2 Symptoms require and respond to moderate intervention Oxygen requirement < 40% or Hypotension responsive to fluids or low dose of one vasopressor or Grade 2 organ toxicity
3 Symptoms require and respond to aggressive intervention Oxygen requirement ≥ 40% or Hypotension requiring high-dose or multiple vasopressors or Grade 3 organ toxicity
4 Life-threatening symptoms Requirement for ventilator support or Grade 4 organ toxicity (excluding transaminitis)
5 Death
Lee DW, Gardner R, Porter DL, et al. Blood 2014;124:188-195.

Back to KS, ARS #2
• KS eventually received CAR-T cells. He experienced altered mental status, fevers, hypotension and tachycardia. He was transferred to the ICU. Should there be an intervention?
1. Yes, dexamethasone 24 mg per day for 3 days, followed by a 4 day taper
2. Yes, he should be offered pressor support until the episode resolves
3. Yes, he should be given a one time dose of tocilizumab
4. Yes, he should receive IV fluids until the episode resolves

Follow-Up on KS, ARS Question #3
• KS has a transplant following a third CR from CAR-T cells. However, he relapses again with 60% blasts. His flow reveals an abnormal B-cell population that is now CD19 negative and CD22 positive. KS strongly desires additional treatment. What is a reasonable option?
1. Blinatumomab
2. Second HSCT
3. Supportive Care
4. Inotuzumab

Philadelphia Chromosome Positive ALL
• Suppose KS was philadelphia chromosome positive (Ph+)…
– Induction received with an AYA protocol plus dasatinib
– What should the approach be at relapse?

R/R Philadelphia Chromosome + B-Cell ALL • Mutation testing for ABL gene
• Use a TKI not used during initial induction
• Clinical Trial or HSCT if donor available
Mutations TKI Choice
Y253H E255K/V F359V/C/I
Dasatinib
V299L T315A F317L/V/I/C
Nilotinib
E255K/V F317L/V/I/C F359V/C/I T315A Y253H
Bosutinib
T315I Ponatinib NCCN. Acute Lymphoblastic Leukemia.Version 2. 2015. Available at http://www.nccn.org/professionals/physician_gls/pdf/all.pdf. Accessed 10/21/2015 Soverini S , et al. Blood 2011;118:1208-1215

TKI + Intensive Chemotherapy Hyper-CVAD +
Imatinib, N=54
Dasatinib, N=72
Ponatinib, N=37
CR 93% 96% 100%
Cytogenetic CR
95% 83% 100%
CMR or MMR 83% 93% 100%
MRD negativity
88% 94% 97%
Median OS 31 months 47 months Not Reached
HSCT 30% 17% 24%
Daver N, et al. Haematologica 2015;100:653-661 Ravandi F, et al. Cancer 2015;000:000-000 Jabbour E, et al. Lancet 2015;000:000-000
MMR=major molecular response

N=45 R/R Ph+ ALL
Progressed on 2nd or later generation TKI
Intolerant to 2nd generation or later TKI
with documented intolerance/progressi
on on imatinib >5% BM blasts
Blinatumomab: 6-week cycle 9 mcg/day ->
28 mcg/day x 4 weeks 2 weeks off
Up to 5 cycles
CR/CRh after 2 cycles 36%
Martinelli G, Dombret H, Chevallier P, et al. ASH 2015. Abstract 679.
Secondary Endpoints: MRD, RFS, OS, AlloSCT rate
Prospective, Phase II
Blinatumomab in Ph+ ALL: ALCANTARA

ARS Question #4 • JV is a 50 yo Ph+ B-cell ALL patient who received initial
treatment with Hyper-CVAD + Dasatinib and achieved a MMR. Six months later he is noted to have a rising PCR for BCR-ABL transcripts while on maintenance dasatinib. What should happen next?
1. Perform ABL gene mutation testing
2. Change dasatinib to ponatinib given MMR rates with ponatinib
3. Discontinue TKI therapy and offer more traditional chemotherapy
4. Offer autologous stem cell transplantation

The Future… • Ongoing clinical trials
– Ph+
– Initial treatment in B-ALL
– Investigational agents
• Best sequence of agents to be determined
• The best bridge to transplant unknown

In Summary • Clinical trials should be offered for induction and relpase or
refractory disease
• HSCT should be offered in CR1 for high risk disease
• MRD status predicts disease response
• Conventional chemotherapies may give second CR rates as high as 50%, but not all patients will be candidates
• Monoclonal antibodies should be considered in patients with targetable antigens present on leukemic blasts
• Novel immune therapies may help patient overcome immune escape mechanisms
• The best sequence for therapy in r/r ALL is unknown

UPDATES IN RELAPSED/REFRACTORY B-CELL ACUTE LYMPHOBLASTIC LEUKEMIA (ALL)
Larry W. Buie, Pharm.D., BCOP, FASHP Manager, Adult Clinical Pharmacy Services PGY2 Adult Oncology Residency Program Director Memorial Sloan Kettering Cancer Center 5 August 2017
Related Documents











