Acta Neurochir (2003) 145: 273–282 DOI 10.1007/s00701-003-0003-8 Acta Neurochirurgica Printed in Austria Clinical Article Large sphenocavernous meningiomas: Is there still a role for the intradural approach via the pterional-transsylvian route?* F. Tomasello, O. de Divitiis, F. F. Angileri, F. M. Salpietro, and D. d’Avella Neurosurgical Clinic, Department of Neurosciences, Psychiatric and Anesthesiological Sciences University of Messina, Messina, Italy Published online April 28, 2003 6 Springer-Verlag 2003 Summary Background. Large-sized sphenocavernous meningiomas repre- sent a surgical challenge. Although the role of skull base techniques with combined extra- and intradural steps has been recently empha- sized, pure intradural resection tactics via the pterional route consti- tute the traditional microsurgical approach for resection of such tumours. Method. We report the application of the pterional-transsylvian approach in 13 patients with sphenocavernous meningiomas. This series is unique because it includes only patients with tumours ex- ceeding 5 cm in their greatest dimension. Findings. A gross total resection was accomplished in 10 patients (77%). Eight patients had a good outcome, one had a persistent mild hemiparesis, and one died. No recurrences occurred in this group. Three patients (23%) had subtotal resections owing to invasion of the cavernous sinus in one instance and encasement of the middle cere- bral artery in the others. Two had a good outcome and one died. In these patients minimal asymptomatic tumour progression was seen 3 and 6 years after surgery. The overall surgical outcome was good in 10 patients (77%), fair in one, and death in two. Interpretation. In our experience, large sphenocavernous menin- giomas may be operated on adopting pure intradural resection tactics via the pterional-transsylvian route with rates of gross total removal and surgical complications related to brain retraction or vascular manipulation comparable to those of extensive skull base approaches. The traditional intradural pterional trans- sylvian approach continues to have a place in the treatment of these lesions. Keywords: Surgical approach; meningioma; skull base surgery; cavernous sinus. Introduction Sphenocavernous meningiomas, arising from the dura covering the medial portion of the sphenoid bone, occupy the region of the anterior clinoid and adjacent medial sphenoid wing and involve the pericavernous or cavernous sinus structures [16, 24]. These tumours are di¤erentiated from clinoidal meningiomas on the basis of their dural attachment, growth pattern, neu- rovascular relationships and clinical presentation. Tu- mours with an ‘‘en masse’’ [3, 4] growth pattern may attain surprisingly large size with relatively minimal symptoms. Such huge ( b 5 cm in diameter) meningi- omas still represent a surgical challenge. Recent reports have emphasized the role of con- temporary skull base surgical techniques with com- bined extra- and intradural steps for resection of large sphenocavernous meningiomas [2, 9]. Nevertheless, the ‘‘pure’’ intradural resection tactics via the pterional route, that are the traditional microsurgical approach to these lesions, can result in excellent outcomes after operation [3, 4, 5, 10, 16, 24]. Very large tumours, however, were not specifically considered in these publications. This paper describes the application of the pterional transsylvian approach in 13 patients who had a sphenocavernous meningioma, larger than 5 cm in the greatest dimension. The aims of this article are: 1) to consider specifically the issue of suitability of the intradural pterional-transsylvian route for large-sized sphenocavernous meningiomas; and 2) to investigate if this approach contributes to minimizing morbidity after operation. * This paper was supported in part by Grant ‘‘Piano B008 – P.R. 2’’ from M.U.R.S.T. and European Community.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Acta Neurochir (2003) 145: 273–282
DOI 10.1007/s00701-003-0003-8 Acta NeurochirurgicaPrinted in Austria
Clinical ArticleLarge sphenocavernous meningiomas: Is there still a role for the intraduralapproach via the pterional-transsylvian route?*
F. Tomasello, O. de Divitiis, F. F. Angileri, F. M. Salpietro, and D. d’Avella
Neurosurgical Clinic, Department of Neurosciences, Psychiatric and Anesthesiological Sciences University of Messina, Messina, Italy
Published online April 28, 20036 Springer-Verlag 2003
Summary
Background. Large-sized sphenocavernous meningiomas repre-
sent a surgical challenge. Although the role of skull base techniques
with combined extra- and intradural steps has been recently empha-
sized, pure intradural resection tactics via the pterional route consti-
tute the traditional microsurgical approach for resection of such
tumours.
Method. We report the application of the pterional-transsylvian
approach in 13 patients with sphenocavernous meningiomas. This
series is unique because it includes only patients with tumours ex-
ceeding 5 cm in their greatest dimension.
Findings. A gross total resection was accomplished in 10 patients
(77%). Eight patients had a good outcome, one had a persistent mild
hemiparesis, and one died. No recurrences occurred in this group.
Three patients (23%) had subtotal resections owing to invasion of the
cavernous sinus in one instance and encasement of the middle cere-
bral artery in the others. Two had a good outcome and one died. In
these patients minimal asymptomatic tumour progression was seen 3
and 6 years after surgery. The overall surgical outcome was good in
10 patients (77%), fair in one, and death in two.
Interpretation. In our experience, large sphenocavernous menin-
giomas may be operated on adopting pure intradural resection
tactics via the pterional-transsylvian route with rates of gross total
removal and surgical complications related to brain retraction
or vascular manipulation comparable to those of extensive skull
base approaches. The traditional intradural pterional trans-
sylvian approach continues to have a place in the treatment of these
lesions.
Keywords: Surgical approach; meningioma; skull base surgery;
cavernous sinus.
Introduction
Sphenocavernous meningiomas, arising from the
dura covering the medial portion of the sphenoid bone,
occupy the region of the anterior clinoid and adjacent
medial sphenoid wing and involve the pericavernous
or cavernous sinus structures [16, 24]. These tumours
are di¤erentiated from clinoidal meningiomas on the
basis of their dural attachment, growth pattern, neu-
rovascular relationships and clinical presentation. Tu-
mours with an ‘‘en masse’’ [3, 4] growth pattern may
attain surprisingly large size with relatively minimal
symptoms. Such huge (b5 cm in diameter) meningi-
omas still represent a surgical challenge.
Recent reports have emphasized the role of con-
temporary skull base surgical techniques with com-
bined extra- and intradural steps for resection of large
sphenocavernous meningiomas [2, 9]. Nevertheless,
the ‘‘pure’’ intradural resection tactics via the pterional
route, that are the traditional microsurgical approach
to these lesions, can result in excellent outcomes after
operation [3, 4, 5, 10, 16, 24]. Very large tumours,
however, were not specifically considered in these
publications. This paper describes the application of
the pterional transsylvian approach in 13 patients who
had a sphenocavernous meningioma, larger than 5 cm
in the greatest dimension. The aims of this article are:
1) to consider specifically the issue of suitability of the
intradural pterional-transsylvian route for large-sized
sphenocavernous meningiomas; and 2) to investigate
if this approach contributes to minimizing morbidity
after operation.* This paper was supported in part by Grant ‘‘Piano B008 – P.R.
2’’ from M.U.R.S.T. and European Community.
Patients and methods
Clinical presentation
Thirteen patients harbouring a large-sized sphenocavernous men-
ingioma were operated on by the senior author (F.T.) between June
1988 and June 2000 at the Neurosurgical Clinic of the University of
Messina School of Medicine in Messina, Italy. They were 11 women
and 2 men with a mean age of 57.6 years (range 43 to 71 years). The
clinical records, neuroradiological examinations, and operative
notes and videotape recordings of the procedures of these patients
were examined retrospectively. Signs on presentation consisted of
chronic headache present in eight of thirteen patients (61.5%), sei-
zures in eight (61.5%), visual acuity or visual field impairment in
three (23%), and altered mental status and personality changes in
four (30.7%) (Table 1). The beginning of symptoms preceded diag-
nosis by 3 to 36 months (average 14.6 months). No patient was
admitted in comatose condition requiring emergency craniotomy.
Fourteen operations were performed in thirteen patients. Karnofsky
performance status was taken as a gross measure of neurological
functional impairment [13]. When graded preoperatively, Karnofsky
index averaged 70% (range 60 to 90%). Post-operative clinical and
neuroradiological follow-up periods ranged from 12 to 156 months
(average 48.3 months).
Preoperative neuroradiological findings
All but one patient (in whom a contrast-enhanced CT scan was
obtained) underwent sequential contrast-enhanced magnetic reso-
nance imaging (including T1 weighted, T2 weighted, spin-echo and
gradient echo multiplanar images), preoperatively, in the early post-
operative period, and at subsequent follow-up examinations (6–12
months postoperatively and when this series was reviewed for publi-
cation purposes). Preoperative MR images were evaluated for tu-
mour size, direction of growth in anterior and middle cranial fossa,
cavernous sinus involvement, involvement of the carotid, anterior
and middle cerebral arteries as well as the optic apparatus, and de-
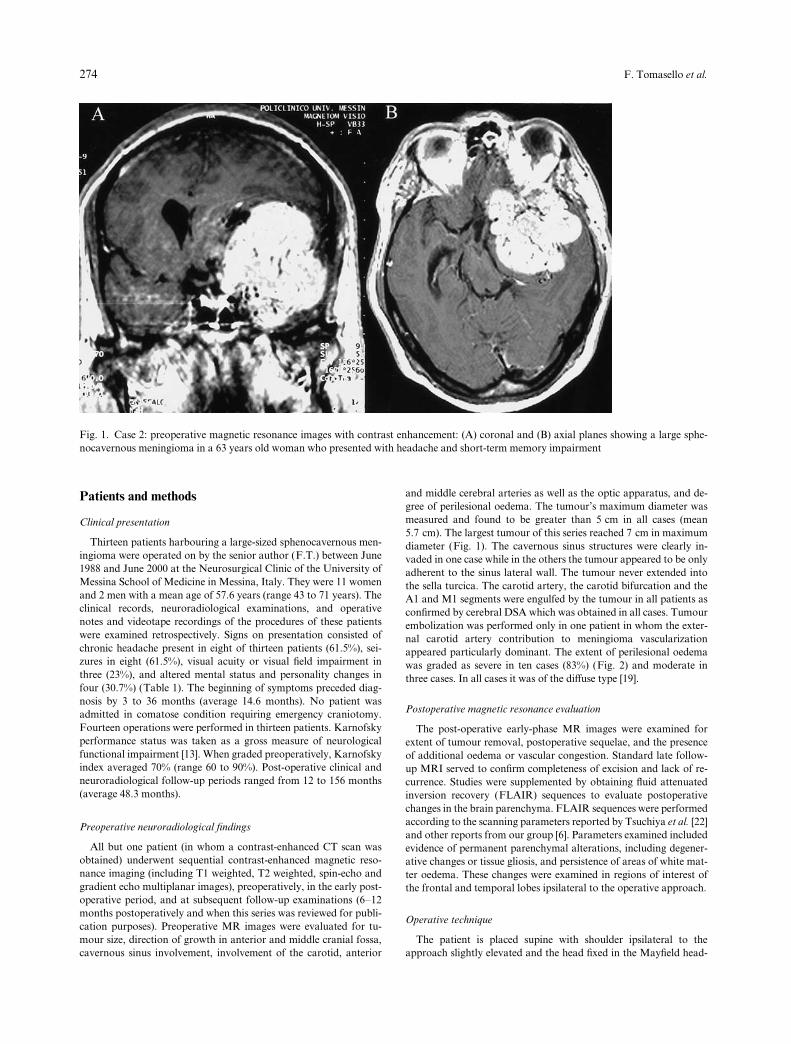
gree of perilesional oedema. The tumour’s maximum diameter was
measured and found to be greater than 5 cm in all cases (mean
5.7 cm). The largest tumour of this series reached 7 cm in maximum
diameter (Fig. 1). The cavernous sinus structures were clearly in-
vaded in one case while in the others the tumour appeared to be only
adherent to the sinus lateral wall. The tumour never extended into
the sella turcica. The carotid artery, the carotid bifurcation and the
A1 and M1 segments were engulfed by the tumour in all patients as
confirmed by cerebral DSA which was obtained in all cases. Tumour
embolization was performed only in one patient in whom the exter-
nal carotid artery contribution to meningioma vascularization
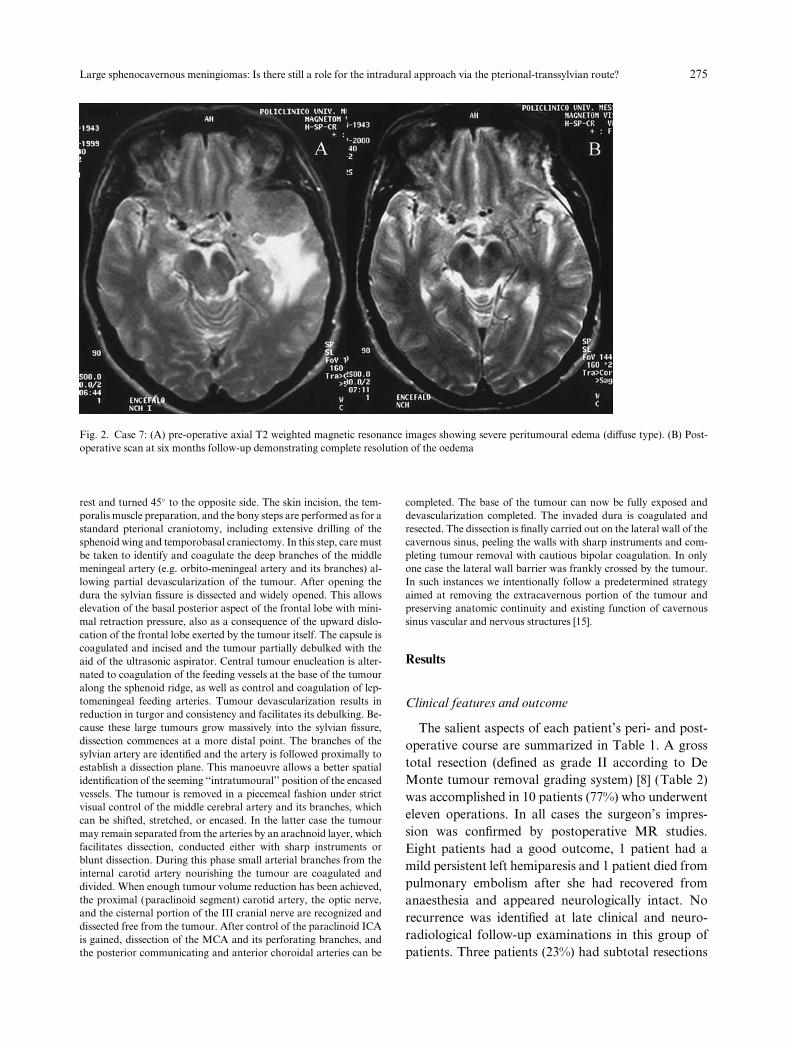
appeared particularly dominant. The extent of perilesional oedema
was graded as severe in ten cases (83%) (Fig. 2) and moderate in
three cases. In all cases it was of the di¤use type [19].
Postoperative magnetic resonance evaluation
The post-operative early-phase MR images were examined for
extent of tumour removal, postoperative sequelae, and the presence
of additional oedema or vascular congestion. Standard late follow-
up MRI served to confirm completeness of excision and lack of re-
currence. Studies were supplemented by obtaining fluid attenuated
inversion recovery (FLAIR) sequences to evaluate postoperative
changes in the brain parenchyma. FLAIR sequences were performed
according to the scanning parameters reported by Tsuchiya et al. [22]
and other reports from our group [6]. Parameters examined included
evidence of permanent parenchymal alterations, including degener-
ative changes or tissue gliosis, and persistence of areas of white mat-
ter oedema. These changes were examined in regions of interest of
the frontal and temporal lobes ipsilateral to the operative approach.
Operative technique
The patient is placed supine with shoulder ipsilateral to the
approach slightly elevated and the head fixed in the Mayfield head-
Fig. 1. Case 2: preoperative magnetic resonance images with contrast enhancement: (A) coronal and (B) axial planes showing a large sphe-
nocavernous meningioma in a 63 years old woman who presented with headache and short-term memory impairment
274 F. Tomasello et al.
rest and turned 45� to the opposite side. The skin incision, the tem-
poralis muscle preparation, and the bony steps are performed as for a
standard pterional craniotomy, including extensive drilling of the
sphenoid wing and temporobasal craniectomy. In this step, care must
be taken to identify and coagulate the deep branches of the middle
meningeal artery (e.g. orbito-meningeal artery and its branches) al-
lowing partial devascularization of the tumour. After opening the
dura the sylvian fissure is dissected and widely opened. This allows
elevation of the basal posterior aspect of the frontal lobe with mini-
mal retraction pressure, also as a consequence of the upward dislo-
cation of the frontal lobe exerted by the tumour itself. The capsule is
coagulated and incised and the tumour partially debulked with the
aid of the ultrasonic aspirator. Central tumour enucleation is alter-
nated to coagulation of the feeding vessels at the base of the tumour
along the sphenoid ridge, as well as control and coagulation of lep-
tomeningeal feeding arteries. Tumour devascularization results in
reduction in turgor and consistency and facilitates its debulking. Be-
cause these large tumours grow massively into the sylvian fissure,
dissection commences at a more distal point. The branches of the
sylvian artery are identified and the artery is followed proximally to
establish a dissection plane. This manoeuvre allows a better spatial
identification of the seeming ‘‘intratumoural’’ position of the encased
vessels. The tumour is removed in a piecemeal fashion under strict
visual control of the middle cerebral artery and its branches, which
can be shifted, stretched, or encased. In the latter case the tumour
may remain separated from the arteries by an arachnoid layer, which
facilitates dissection, conducted either with sharp instruments or
blunt dissection. During this phase small arterial branches from the
internal carotid artery nourishing the tumour are coagulated and
divided. When enough tumour volume reduction has been achieved,
the proximal (paraclinoid segment) carotid artery, the optic nerve,
and the cisternal portion of the III cranial nerve are recognized and
dissected free from the tumour. After control of the paraclinoid ICA
is gained, dissection of the MCA and its perforating branches, and
the posterior communicating and anterior choroidal arteries can be
completed. The base of the tumour can now be fully exposed and
devascularization completed. The invaded dura is coagulated and
resected. The dissection is finally carried out on the lateral wall of the
cavernous sinus, peeling the walls with sharp instruments and com-
pleting tumour removal with cautious bipolar coagulation. In only
one case the lateral wall barrier was frankly crossed by the tumour.
In such instances we intentionally follow a predetermined strategy
aimed at removing the extracavernous portion of the tumour and
preserving anatomic continuity and existing function of cavernous
sinus vascular and nervous structures [15].
Results
Clinical features and outcome
The salient aspects of each patient’s peri- and post-
operative course are summarized in Table 1. A gross
total resection (defined as grade II according to De
Monte tumour removal grading system) [8] (Table 2)
was accomplished in 10 patients (77%) who underwent
eleven operations. In all cases the surgeon’s impres-
sion was confirmed by postoperative MR studies.
Eight patients had a good outcome, 1 patient had a
mild persistent left hemiparesis and 1 patient died from
pulmonary embolism after she had recovered from
anaesthesia and appeared neurologically intact. No
recurrence was identified at late clinical and neuro-
radiological follow-up examinations in this group of
patients. Three patients (23%) had subtotal resections
Fig. 2. Case 7: (A) pre-operative axial T2 weighted magnetic resonance images showing severe peritumoural edema (di¤use type). (B) Post-
operative scan at six months follow-up demonstrating complete resolution of the oedema
Large sphenocavernous meningiomas: Is there still a role for the intradural approach via the pterional-transsylvian route? 275

(defined as grade IVa in De Monte grading system)
owing to invasion of the cavernous sinus in one in-
stance and encasement with frank tumoural infiltra-
tion of the MCA trunk in the others. Of these patients,
one died from a surgical complication and 2 had a
good outcome. In these patients, minimal asympto-
matic tumour progression was seen 3 and 6 years after
surgery, respectively (Figs. 3, 4). No patient received
post-operative radiotherapy. Karnofsky performance
status graded 6 months postoperatively averaged 90%
(range 70 to 100%). The overall surgical outcome was
good in 10 patients (77%) who had resumed indepen-
dent activity by 3 months after surgery, fair in one
patient, and death in two. Seven patients (53.8%)
required blood replacement in the perioperative time.
The mean amount of blood replaced was 208 cc. There
were no permanent cranial nerve deficits; however,
three patients experienced a transient III nerve palsy
that had recovered completely three months after
surgery.
Magnetic resonance imaging investigations
In the total removal group, early post-operative
studies revealed no evidence of a surgical complication
and confirmed completeness of excision (Figs. 5, 6).
Lack of recurrence was documented by late follow-up
contrast-enhanced MR scans, also demonstrating no
evidence of any significant structural change and the
resolution of the intense perilesional oedema demon-
strated in preoperative studies. Late post-operative
changes in the frontal and temporal lobes ipsilateral to
the approach were specifically examined on FLAIR
MR sequences (Fig. 7). These lobes consistently ex-
hibited a repetitive pattern of post-operative alter-
ations, which were thought to represent permanent
parenchymal gliosis. It should be noted, however, that
the extent of such structural alterations was limited
and that they did not result in specific functional mor-
bidity in the present series.
Table 1. Summary of thirteen patients with sphenocavernous meningiomas
Case n�, age,
sex
Symptoms on admission Max
dimension
(cm)
Surgical
approach
Extent of
resection (De
Monte Grade)
Outcome Follow-up
(months)
Case 1 58/F headache, visual deficit, seizures 5.3 left pterional IVa, II1 Good 156 (*)
Case 2 63/F headache, short term memory impairment 7 left pterional II Died2 N/A
Case 3 62/M headache, seizures 5.4 right pterional II Good 96
Case 4 45/F intracranial hypertension 5 right pterional IVa Fair 88
Case 5 66/M headache, frontal syndrome, seizures 6 left pterional IVa Good 53
Case 6 69/F headache, visual deficit 6 left pterional II Good 39
Case 7 46/F frontal syndrome 5 left pterional II Good 21
Case 8 43/F headache, seizure 5.2 right pterional II Good 21
Case 9 52/F seizure 6.6 left pterional IVa Died3 N/A
Case 10 67/F seizure 5 left pterional II Good 18
Case 11 71/F headache, visual deficit 6 left pterional II Good 15
Case 12 54/F seizure, frontal syndrome 6 left pterional II Good 12
Case 13 58/F headache, seizure 6.5 left pterional II Good 12
1 Recurrence 3 years later, 2nd operation, total resection with a good outcome. 2 Pulmonary embolism 2 days after surgery. 3 Surgical com-
plication (*) Time length from the second operation in 1991.
Good: return to previous occupation; Fair: no major neurological deficit, but not able to return to previous occupation.
Table 2. De Monte tumour removal grading system [8]
Grade Definition
I complete microscopic removal of tumour and dural
attachment with any abnormal bone
II complete microscopic removal of tumour with diathermy
coagulation of its dural attachment
IIIa complete microscopic removal of intra- and extradural
tumour without resection or coagulation of its dural
attachment
IIIb complete microscopic removal of intradural tumour
without resection or coagulation of its dural attachment
or of any extradural extension
IVa intentional subtotal removal to preserve cranial nerves or
blood vessels with complete microscopic removal of
attachment
IVb partial removal leaving tumour < 10% in volume
V partial removal leaving tumour > 10% in volume, or
decompression with or without biopsy
276 F. Tomasello et al.
Discussion
In this era of microneurosurgical technique refine-
ments, excellent surgical results can be achieved in ex-
cising skull base meningiomas. However, meningi-
omas arising from the medial sphenoid ridge with
involvement of the lateral wall of the cavernous sinus
or invasion of the sinus itself, and achieving very large
size, still represent a surgical challenge.
According to Yasargil [24] sphenocavernous men-
ingiomas are a distinct subgroup of medial sphenoid
meningiomas. Day [9] defined sphenocavernous men-
ingiomas as those arising from the dura covering the
sphenoid ridge, with or without invasion of the peri
cavernous and cavernous sinus structures. This classi-
fication is important from the nosographic point of
view, and has clinical implications. Sphenocavernous
meningiomas are distinguished from medial sphenoi-
dal meningiomas originating from the superior and/or
lateral aspect of the anterior clinoid process [2]. Due to
their growth pattern, clinoidal meningiomas are char-
acterized by an earlier involvement of the optic nerve
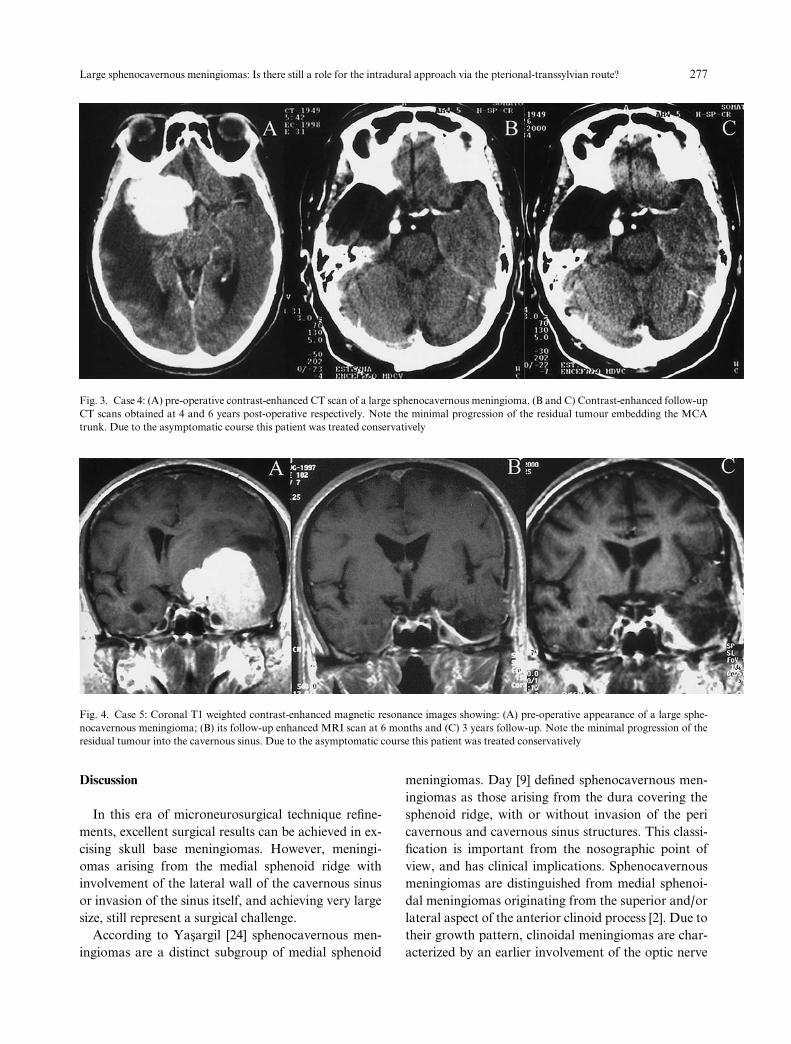
Fig. 3. Case 4: (A) pre-operative contrast-enhanced CT scan of a large sphenocavernous meningioma. (B and C) Contrast-enhanced follow-up
CT scans obtained at 4 and 6 years post-operative respectively. Note the minimal progression of the residual tumour embedding the MCA
trunk. Due to the asymptomatic course this patient was treated conservatively
Fig. 4. Case 5: Coronal T1 weighted contrast-enhanced magnetic resonance images showing: (A) pre-operative appearance of a large sphe-
nocavernous meningioma; (B) its follow-up enhanced MRI scan at 6 months and (C) 3 years follow-up. Note the minimal progression of the
residual tumour into the cavernous sinus. Due to the asymptomatic course this patient was treated conservatively
Large sphenocavernous meningiomas: Is there still a role for the intradural approach via the pterional-transsylvian route? 277
and proximal carotid artery. In contrast sphenoca-
vernous meningiomas tend to spread lateral-inferiorly
into the middle cranial fossa so that ICA and optic and
oculomotor nerves are generally involved later. This
di¤erence may explain the huge dimensions they may
attain before becoming symptomatic. For example,
while visual disturbances were present in 84% of cases
of clinoidal meningiomas reported by A1-Mefty [2],
only 3 of our 13 patients (23%) had visual impairment.
The foregoing anatomical, radiological and clinical
considerations, lead us to suggest the use of the term
sphenocavernous meningiomas should be reserved for
this particular subgroup of lesions.
Literature review
The pterional approach followed by intradural de-
bulking and microsurgical resection of the tumour is
the most widely used surgical route for large-sized
meningiomas of the middle cranial base. The standard
pterional intradural approach for the removal of such
tumours has been comprehensively described by Do-
lenc [10], Bonnal [3], Ojemann [16], and systematically
adopted by Yasargil [24]. The advantages and dis-
advantages of this surgical strategy have been recently
discussed and compared with those o¤ered by con-
temporary cranial base surgical techniques in a paper
reporting six patients with large sphenocavernous
meningiomas [9]. The present report presents our ex-
perience using the pterional-transsylvian route fol-
lowed by intradural microsurgical tumour resection in
a selected series of thirteen patients with a large sphe-
nocavernous meningioma. To our knowledge, this
series is the largest in the literature that specifically in-
cludes only patients with a sphenocavernous meningi-
oma larger than 5 cm diameter. A gross total removal
was achieved in 77% of patients and 77% resumed an
independent life, with marked improvement in their
neurological symptoms.
It is well known that the likelihood of unsatisfactory
surgical results and of failure to achieve complete
removal increases when a tumour is larger than 3 cm
[1, 21]. When compared to the results in published
series of Sphenocavernous meningiomas, the results
from the present series support the suitability of the
intradural approach, via the pterional-transsylvian
route, for resection of such large-sized meningiomas
(Table 3). In 1979 Dolenc reported on 10 patients who
had been operated upon via a bifrontal approach (in 2
cases) or a pterional approach (8 cases). Two deaths
occurred, 2 patients developed a transient IIIrd nerve
paresis, and four patients experienced a transient
hemiparesis. Nevertheless, the final outcomes were
good for these 8 patients [10]. In 1991 Bonnal pre-
sented 15 patients with an en masse sphenocavernous
meningioma; eight of these patients had slight or
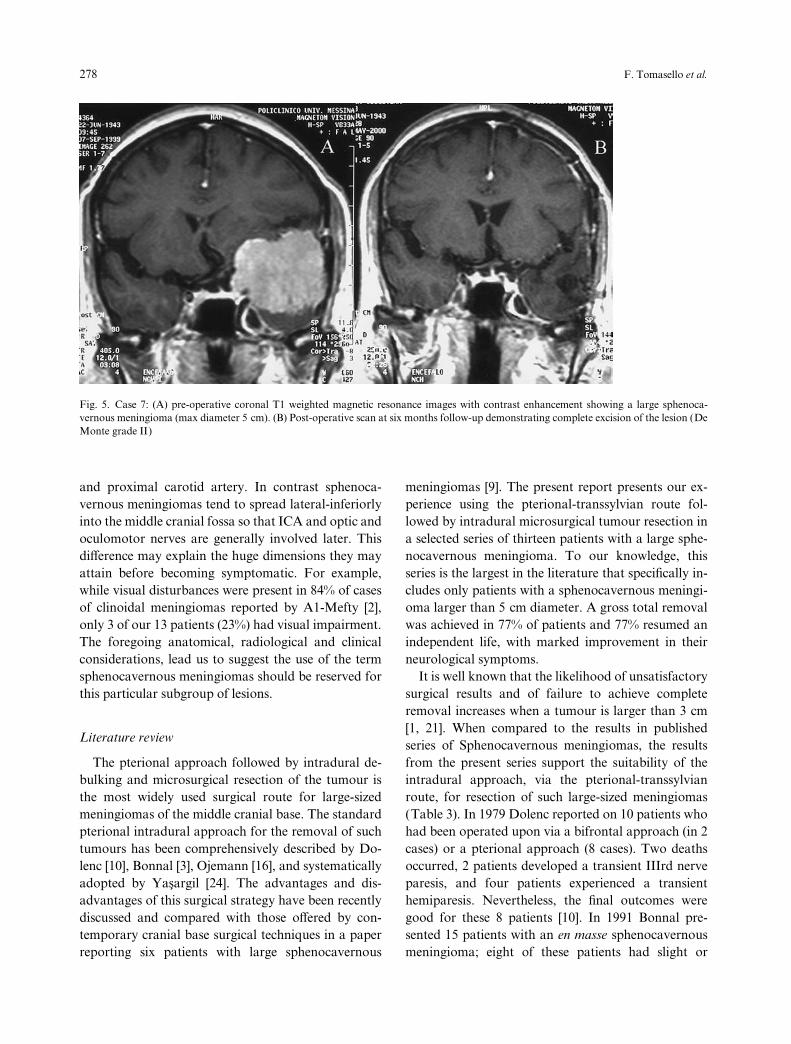
Fig. 5. Case 7: (A) pre-operative coronal T1 weighted magnetic resonance images with contrast enhancement showing a large sphenoca-
vernous meningioma (max diameter 5 cm). (B) Post-operative scan at six months follow-up demonstrating complete excision of the lesion (De
Monte grade II)
278 F. Tomasello et al.
severe post-operative morbidity. The other seven
patients had good outcomes [3]. In 1992 Ojemann
reported 17 patients, some of whom had a clinoidal
meningioma, operated upon via a fronto-temporal
craniotomy. A subtotal removal was achieved in 14
patients and a radical subtotal removal in the remain-
ing three. The outcome was good in 16 patients. One
patient had a permanent dysphasia and hemiparesis
[16]. In his monograph (1996) Yasargil described 9
patients with ‘‘medial sphenoid’’ meningiomas oper-
ated upon via a pterional approach. Seven patients
experienced a good outcome and the other two had a
‘‘fair’’ outcome [24]. Contemporary cranial base sur-
gical techniques do have a major role in the treatment
of such tumours, particularly when a large spheno-
cavernous meningioma has extensively crossed the wall
of the cavernous sinus [11, 14, 18]. Very recently, Day
[9] reported six patients in whom an aggressive skull
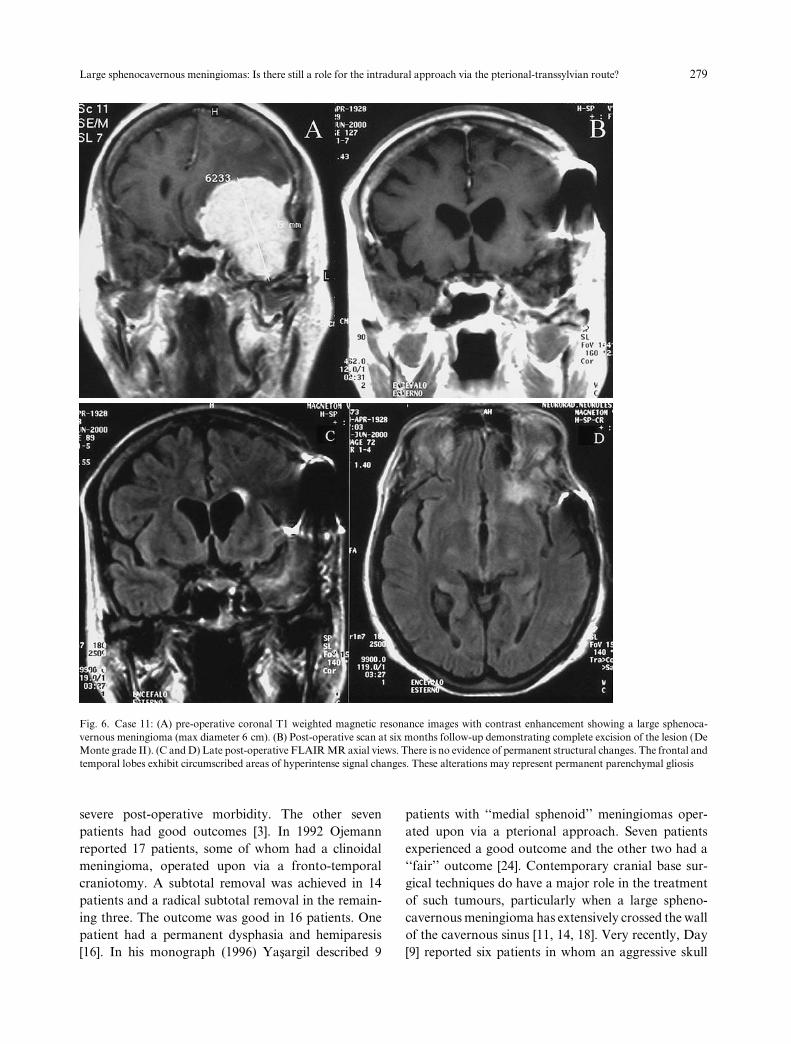
Fig. 6. Case 11: (A) pre-operative coronal T1 weighted magnetic resonance images with contrast enhancement showing a large sphenoca-
vernous meningioma (max diameter 6 cm). (B) Post-operative scan at six months follow-up demonstrating complete excision of the lesion (De
Monte grade II). (C and D) Late post-operative FLAIR MR axial views. There is no evidence of permanent structural changes. The frontal and
temporal lobes exhibit circumscribed areas of hyperintense signal changes. These alterations may represent permanent parenchymal gliosis
Large sphenocavernous meningiomas: Is there still a role for the intradural approach via the pterional-transsylvian route? 279

base surgical strategy was adopted to resect a large
sphenocavernous meningioma. Extensive bone work
at the cranial base was performed in each patient. Un-
roofing of the foramina rotundum, ovale, and spino-
sum of the superior orbital fissure, and of the optic
canal, removal of the anterior clinoid process, and
elevation of the undersurface of the temporal lobe, were
performed before opening the dura. Following this
strategy, four patients had a gross total resection, and
two had only a subtotal resection as result of invasion
of the cavernous sinus or the middle cerebral artery.
Two patients experienced a transient III nerve paresis,
and two developed transient postoperative cerebral
oedema that required intensive treatment. All six pa-
tients, however, had a good outcome. The use of this
technique resulted in low blood loss during the opera-
tion and obviated the need for preoperative emboliza-
tion [9].
Technical considerations
The principal advantages claimed for aggressive
skull base approaches to these lesions include: 1) better
control of arterial blood supply to the tumour 2) wider
exposure and minimization of brain retraction 3) con-
trol of neurovascular structures at the cranial base 4)
more possibility of complete excision and hence long
term, recurrence-free tumour control. These issues de-
serve detailed discussion.
1) Interruption of its blood supply before a debulk-
ing tumour is undoubtedly a great advantage. In our
experience, however, pure intradural resection tactics
did not result in significant intraoperative blood losses
as judged from blood replacement needs. In this con-
text we emphasize that a component of the vasculari-
zation of these meningiomas is from the ICA dural and
leptomeningeal branches [23], which can be dissected
and controlled during the intradural phase of the op-
eration.
2) According to Yasargil [24], the pterional-
transsylvian approach takes advantage of those planes
and spaces naturally provided to expose the base of the
brain without significant brain retraction. Moreover,
large tumours produce large ‘‘birth’’ canals through
which atraumatic brain tissue decompression can be
performed. The most striking complication, which oc-
curred in one third of patients reported by Day, was
post-operative oedema of the temporal lobe requiring
ICU management. We agree with Dolenc [12] that
venous drainage problems, related to extradural tem-
poral lobe manipulation were probably the cause of
the brain swelling. Retraction of oedematous paren-
chyma, chronically compressed by an underlying mass
may precipitate postoperative oedema, infarction, and
intracerebral haemorrhage. This holds particularly
true with a huge meningioma. Indeed, in a previous
paper by our group we showed a positive correlation
between tumour size and extent of perifocal edemata.
A positive correlation was also found between grade
of oedema and cortical penetration [19]. Minimal re-
traction and preservation of the venous drainage are
therefore crucially important. The extradural strategy
described by Day [9] involves extensive temporal lobe
manipulation, in which the undersurface of the tem-
poral lobe is separated from the cavernous sinus wall.
In our experience, the choice of the pterional trans-
sylvian intradural approach resulted in venous drain-
age preservation and avoided frontal and temporal
lobes damage from retraction. A satisfactory preser-
vation of brain structural integrity was demonstrated
by late follow-up FLAIR MR studies. We choose this
particular sequence for its capability to show brain
tissue oedema or degenerative and gliotic components
more clearly than conventional T2-weighted and pro-
Table 3. Summary of selected published series of sphenocavernous meningiomas
Author, year N� of
patients
Approach Excision Follow-up Outcome
Cook, 1968 (5) 11 pterional, intradural 2 D, 4 SD
Dolenc, 1979 (10) 10 bifrontal, pterional 2 D
Bonnal, 1980 (3) 7 pterional intra-extradural 7 subtotal 1–13 years 3 D, 1 SD, 3 GO
Ojemann, 1992 (16) 17 pterional intradural 3 RST, 14 ST 5 (1–11) years 1 SD, 16 GO
Yasargil, 1996 (24) 9 pterional intradural 2 MD, 7 GO
Day, 2000 (9) 6 extensive extradural 2 ST, 4 T 24 months (max) 6 GO
Present series, 2001 13 pterional intradural 3 ST, 10 T 48.3 (12–156) months 10 GO, 1 MD, 2 D
RST Radical subtotal resection; ST subtotal resection; T total resection; D Death; SD severe disability; MD Moderate disability; GO good
outcome.
280 F. Tomasello et al.

ton density-weighted images [22]. Its clinical usefulness
in neuroimaging has been described in regard to sev-
eral conditions [7, 22]. The frontal and temporal lobes
ipsilateral to the approach consistently showed post-
operative alterations consistent with permanent pa-
renchymal gliosis. These changes, however, were of
limited extent, were not associated with any specific
neurological morbidity, and correlated well with the
neurobehavioral outcome in this series.
3) A sphenocavernous meningioma usually spares
the paraclinoid segment of the ICA and proximal
control of this vessel can be safely achieved through a
pure intradural strategy. In our experience the optic
apparatus was frequently shifted and compressed, but
never embedded in the tumour and it was always pos-
sible to dissect it free. Although the cisternal portion of
the III nerve could be displaced, stretched, and rarely,
half surrounded by the tumour it was always possible
to dissect it free. A transient III nerve palsy was ob-
served in three patients. One patient’s investigations
showed an intracavernous component of the tumour
which was not removed. We believe with others [15,
16, 20] that, in a giant tumour in which the main part
responsible for the clinical features is extracavernous,
operation should be directed at the extracavernous
portion of the tumour.
4) None of our patients had a recurrence after
undergoing a grade II resection. One patient, who had
a subtotal resection (grade IVa), showed symptomatic
tumour progression and required reoperation. These
low rates of recurrence are based on an observation
period averaging 42.3 months.
Conclusions
Large meningiomas arising from the dura cover-
ing the medial portion of the sphenoid bone, with
or without invasion of the pericavernous and cavern-
ous sinus structures, may be operated on adopting
pure intradural resection tactics via the traditional
pterional-transsylvian route. The major indications for
this pure intradural approach are lateral growth of the
tumour into the middle cranial fossa that limits the
possibility of temporal lobe retraction, and a lack of
frank cavernous sinus invasion. In our experience, the
rates of gross total removal and surgical complications
related to brain retraction or vascular manipulation
are acceptable and not worse those reported for com-
plex extra-intradural skull base approaches. These, on
the other hand, still need validation based on long-
term follow-up evaluations for this group of meningi-
omas. We believe that the major hazards of perioper-
ative morbidity in these patients are related to the
intradural vascular and neural dissection phase, and
these steps therefore represent the most important
focus in defining the strategy for approaching these
meningiomas.
We conclude that, although contemporary skull
base approaches, with intra and extradural strategies,
represent the gold standard to approach cranial base
meningiomas, the traditional intradural pterional
transsylvian approach continues to have a role in the
treatment of selected subgroups of cranial base tu-
mours such as giant sphenocavernous meningiomas.
References
1. Alaywan M, Sindou M (1993) Facteurs pronostiques dans la
chirurgie des meningiomas intracraniens. Role de la taille de la
tumeur et de sa vascularisation arterielle d’origine piemerienne.
Etude sur 150 cas. Neurochirurgie 39: 337–347
2. Al-Mefty O (1990) Clinoidal meningiomas. J Neurosurg 73:
840–849
3. Bonnal J, Thibaut A, Brotchi J, Born J (1980) Invading menin-
giomas of the sphenoid ridge. J Neurosurg 53: 587–599
4. Brotchi J, Bonnal JP (1991) Lateral and middle sphenoid wing
meningiomas. In: Al Mefty O (ed) Meningiomas. Raven Press,
New York, pp 413–425
5. Cook A (1971) Total removal of large global miningiomas at the
medial aspect of the sphenoid ridge: technical note. J Neurosurg
34: 107–113
6. d’Avella D, Salpietro FM, Alafaci C, Tomasello F (1999) Giant
olfactory meningiomas: The pterional approach and its rele-
vance for minimizing surgical morbidity. Skull Base Surgery 9:
23–31
7. De Coene B, Hajnal JV, Gatehouse P, Longmore DB, White SJ,
Oatridge A, Pennock JM, Young IR, Bydder JM (1992) MR of
the brain using fluid-attenuated inversion recovery (FLAIR)
pulse sequence. AJNR 13: 1555–1564
8. De Monte F, Smith H, Al-Mefty O (1994) Outcome of aggres-
sive removal of cavernous sinus meningiomas. J Neurosurg 81:
245–251
9. Diaz Day J (2000) Cranial base surgical techniques for large
sphenocavernous meningiomas: technical note. Neurosurgery
46: 754–760
10. Dolenc V (1979) Microsurgical removal of large sphenoidal
bone meningiomas. Acta Neurochir (Wien) [Suppl] 28: 391–396
11. Dolenc V, Kregar T, Ferluga M, Fettich M, Morina A (1987)
Treatment of tumours invading the cavernous sinus. In Dolenc
V (ed) The cavernous sinus: a multidisciplinary approach to tu-
mours and vascular lesions. Springer, Berlin Heidelberg New
York Tokyo, pp 377–391
12. Dolenc V (2000) Cranial base surgical techniques for large
sphenocavernous meningiomas: technical note. Neurosurgery
46: 760 (comment)
13. Karnofsky DA, Burchenal HH, Armistead GC (1951) Tri-
ethylene melamine in the treatment of neoplastic disease: a
compund with nitrogen-mustrad-like activity suitable for oral or
intravenous use. AMA Arch Int Med 87: 477–516
14. Kawase T, Toya S, Shiobara R, Kimura C, Nagajima H (1986)
Large sphenocavernous meningiomas: Is there still a role for the intradural approach via the pterional-transsylvian route? 281

Skull base approaches for meningiomas invading the cavernous
sinus, in Proceedings International Symposium on cavernous
sinus. Llubbjana, pp 380–389
15. O’Sullivan MG, van Loveren HR, Tew MJ Jr (1997) The surgi-
cal respectability of meningiomas of the cavernous sinus. Neu-
rosurgery 40: 238–247
16. Ojemann R (1992) Medial sphenoid wing (clinoidal) meningi-
omas. Clin Neurosurg 40: 321–383
17. Ojeman R (1997) The surgical respectability of meningiomas of
the cavernous sinus. Neurosurgery 40: 9–247 (comment)
18. Pompili A, Derome PJ, Visot A, Guiot G (1982) Hyperostosing
meningiomas of the sphenoid ridge: clinical features, surgical
therapy, and long term observations – teview of 49 cases. Surg
Neurol 17: 411–416
19. Salpietro FM, Alafaci C, Lucerna S, Iacopino DG, Todaro C,
Tomasello F (1994) Peritumoural edema in meningiomas: mi-
crosurgical observations of di¤erent brain tumour interfaces
related to computed tomography. Neurosurgery 35: 638–642
20. Samii M (1997) The surgical respectability of meningiomas of
the cavernous sinus. Neurosurgery 40: 9–247 (comment)
21. Symon L, Rosenstein J (1984) Surgical management of supra-
sellar meningiomas. Part I: the influence of tumour size, dura-
tion of symptoms, and microsurgery on surgical outcome in 101
consecutive cases. J Neurosurg 61: 633–641
22. Tsuchiya K, Mizutani Y, Hachiya J (1996) Preliminary evalua-
tion of fluid-attenuated inversion-recovery MR in the diagnosis
of intracranial tumours. AJNR 17: 1081–1086
23. Yamaki T, Tanabe S, Sohma T, Uede T, Shinya T, Hashi K
(1988) Feeding arteries of parasellar meningiomas: angiographic
study of medial sphenoid ridge and tuberculum sellae meningi-
omas. Neurol Med Chir (Tokyo) 28: 553–558
24. Yasargil MG (1996) Microneurosurgery: microneurosurgery
of CNS tumours. Georg Thieme Verlag, New York, vol. IVB,
p 136
Comment
This is a very well written paper on the surgical treatment of large
spheno-cavemous meningiomas. The tenor of the article appeals be-
cause the authors go back to basics and prove in a convincing way
that a well executed, straightforward pterional approach is very ef-
fective in treating these tumours. In the light of all the skull-base
surgery violence it is a relief to find an article that points out the
merits of such a time-honoured approach.
The results presented are as least as good as the results in those
studies where extensive portions of the skull-base were removed to
get better access to the tumor, enabling the surgeon to carry out a
more complete resection. In this respect the message of the paper is a
very timely one since there seems to be a tendency among skull-base
surgeons to perform much more limited resections than some years
ago, because of the often very slow growth-rate of these meningi-
ornas and because of the possibility to treat the remnant or the re-
currence by way of stereotactic irradiation.
The advice of the authors to expose the distal middle cerebral ar-
tery and its branches first before starting the removal of the tumor is
well taken. However, in my opinion it might be advisable to delay
the tumor-resection and to look for the intracranial portion of the
Internal Carotid Artery and from there to follow the Middle Cere-
bral Artery in a distal direction. The extra time spent in performing
these manoeuvres is well invested since when the operation has a
poor outcome it is in the majority of cases caused by a lesion of the
ICA or the MCA, or one of its branches.
K. Tulleken
Correspondence: Domenico d’Avella, M.D., Neurosurgical
Clinic, Department of Neuroscience, Psychiatric and Anesthesiol-
gical Sciences, Policlinico Universitario, via Consolare Valeria 1,
98122 Messina, Italy.
282 F. Tomasello et al.: Large sphenocavernous meningiomas
Related Documents











