Large Intestine Physiology Harvey Davies & Sean Botham Peer Support

Large Intestine Physiology Harvey Davies & Sean Botham Peer Support.
Dec 16, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Large Intestine PhysiologyHarvey Davies & Sean Botham
Peer Support

What is the large intestine composed of? [4]
A combination of the: o Cecumo Colono Rectumo Anal canal

What are the functions of the large intestine? [3]
3 main functionso Extract sodium and
water from the luminal contents
o Make and store faeces
o Move faeces towards the rectum

Why is water absorption in the large intestine so important? [3]
1500ml of water per day enters the large intestine
100ml is lost in faeces
An imbalance can lead to constipation or diarrhoea

How is water absorbed in the large intestine? [4] Na+/H+ exchanger on
luminal surface Electrogenic Na+
transporter also moves sodium in
Water follows transcellularly
Na+ released via Na+/K+-ATPase on the basolateral membrane

What structures allow the large intestine to move it’s contents? [3]
Taeniae coli – three bands of smooth muscle
Circular smooth muscle
Haustra – bulges caused by the taeniae coli
The ileocaecal valve prevents backflow
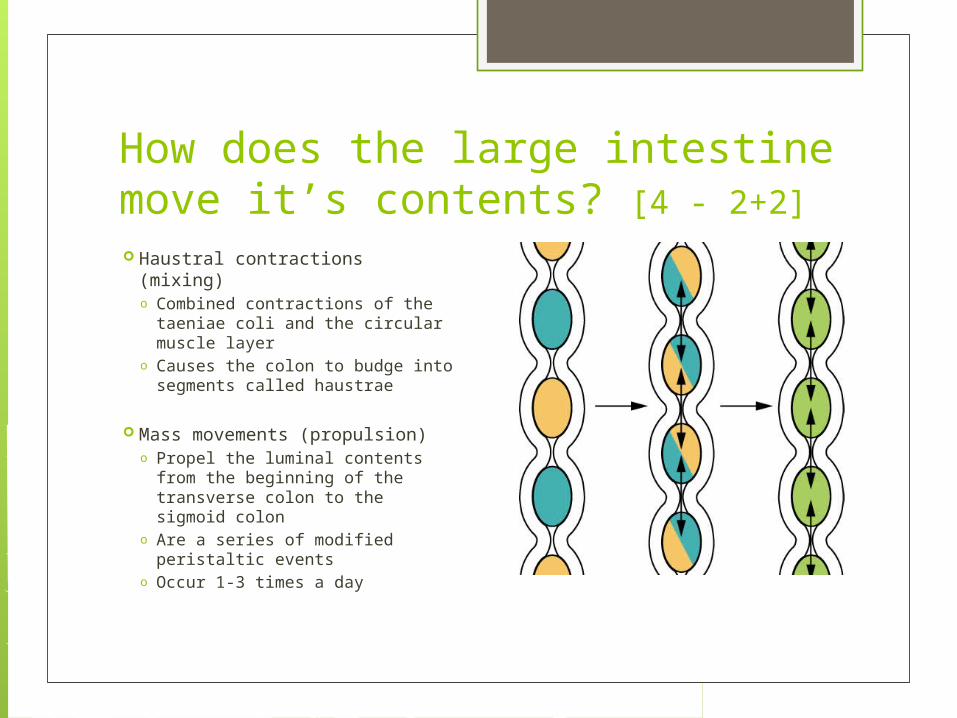
How does the large intestine move it’s contents? [4 - 2+2] Haustral contractions (mixing)
o Combined contractions of the taeniae coli and the circular muscle layer
o Causes the colon to budge into segments called haustrae
Mass movements (propulsion) o Propel the luminal contents
from the beginning of the transverse colon to the sigmoid colon
o Are a series of modified peristaltic events
o Occur 1-3 times a day

What is the defecation reflex? [3] Rectum normally empty
of faeces The defecation reflex is
a response to distension of the rectal wall
Mediated by mechanoreceptors
Can be self-induced via the Valsalva Manoeuvre
Rectoanal inhibitory reflex

What are the steps involved in the defecation reflex? [6] Contraction of the rectum Relaxation of the internal
anal sphincter An initial contraction of
the external anal sphincter Increased peristaltic
activity in the sigmoid colon
Relaxation of the external anal sphincter
Expulsion of faeces

ConstipationWhat is it?
• < 3 bowel movements/week.
• Straining >25% of bowel movements/sensation of hard stool.
• Tenesmus (sensation of incomplete bowel evacuation).
Signs/Symptoms?
• Painful defaecation.
• Hemorrhoids/anal fissures.
• Distended & diffusely tender abdomen with enhanced bowel sounds.

Purgatives – speed things up!Bulk laxatives: increase the volume of non-absorbable residue.
• Example = Methylcellulose.
Osmotic laxatives: increase stool H2O content.
• Example = Milk of Magnesia.
Faecal softeners: alter faecal consistency.
• Example = Ex-Lax.
Stimulant purgatives: increase GI motility.
• Example = Bisacodyl or Senna.

Bulk Laxatives• Example – Methylcellulose.
• MOA – Polysaccharide polymers that are not broken down by normal digestive process (1). Retain water in GI lumen (2), softening and increasing faecal bulk (3) and promoting increasing motility (4).
• Acts for 1-3 days.
• (Contra) Indications – good first choice in constipation & IBS.
• S/E = may decrease absorbance. Stomach cramps.

Osmotic Laxatives• Example – Milk of Magnesia (Magnesium Sulphate + Magnesium Hydroxide).
• MOA – By osmosis, maintain an increased volume of fluid in GI tract (1). This accelerates small intestine transit (2) and an abnormally large volume of fluid entering the colon (3). Distension (4) leads to purgation (5).
• Potent, rapid action for a watery evacuation (1-2 hours).
• (Contra) Indications – bowel prep for surgery. Avoid in small children & poor renal function.
• S/E – dehydration, electrolyte depletion.

Faecal Softeners• Example – Ex-Lax.
• MOA – Surface-eating compounds that act similar to detergents and produce softer faesces.
• Slow acting, 3-5 days.
• (Contra) Indications – fissures, piles (soft faesces = less likely to rupture).
• S/E – few. Some stomach/intestinal cramps.

Stimulant Purgatives• Example – Senna.
• MOA – passes unchanged into colon where colonic bacterial action releases free anthracene derivatives (1). These are absorbed and have a direct effect on the myenteric plexus (2), decreasing tone and haustrations leading to less mixing and water absorption (3) and an overall purgative effect (4).
• (Contra) Indications = very common use. Avoid in breast-feeding mothers.
• S/E – N+V, diarrhoea, cathartic colon, can appear in breast milk.
Cathartic Colon• What is it?
• Anatomical & Physiological changes in colon with chronic use of stimulant laxative (>3 times/week for 1 year).
• What happens?
• Laxative dependency to defecate.• Tachyphylaxis (need higher doses to achieve therapeutic effect).
• How does it present?
• Incomplete faecal evacuation.• Steatorrhoea.• Fluid and electrolyte imbalance.

Diarrhoea – 4 TypesSecretory diarrhoea
Osmotic diarrhoea
Motility-related diarrhoea
Inflammatory diarrhoea

Treatment of Diarrhoea1. Oral Rehydration Therapy
• Treats dehydration. Isotonic solution of glucose & NaCl (glucose enhances Na+ absorption and so H2O.
2. Anti-infective agents (if required).
3. Anti-motility agents – Loperamide.
• Act on µ-opioid receptors in the myenteric plexus.• Increases tone & rhythmic haustral contractions of colon, but diminishes
propulsive activity.• Pyloric, ileocaecal & anal sphincters are contracted.• Increased tone of haustral contractions increased mixing & opportunity
to reabsorb Na+ & H2O production of harder stool.
Related Documents











