Education Laparoscopic Training on Bench Models: Better and More Cost Effective than Operating Room Experience? Daniel J Scott, MD, Patricia C Bergen, MD, FACS, Robert V Rege, MD, FACS, Royce Laycock, MD, FACS, Seifu T Tesfay, RN, R James Valentine, MD, FACS, David M Euhus, MD, FACS, D Rohan Jeyarajah, MD, William M Thompson, MD, FACS, Daniel B Jones, MD, FACS Background: Developing technical skill is essential to surgical training, but using the operating room for basic skill acquisition may be inefficient and expensive, especially for laparoscopic operations. This study de- termines if laparoscopic skills training using simulated tasks on a video-trainer improves the operative perfor- mance of surgery residents. Study Design: Second- and third-year residents (n 5 27) were prospectively randomized to receive formal laparoscopic skills training or to a control group. At baseline, residents had a validated global assessment of their ability to perform a laparoscopic cholecystectomy based on direct observation by three evaluators who were blinded to the residents’ randomization status. Residents were also tested on five standardized video- trainer tasks. The training group practiced the video- trainer tasks as a group for 30 minutes daily for 10 days. The control group received no formal training. All residents repeated the video-trainer test and under- went a second global assessment by the same three blinded evaluators at the end of the 1-month rotation. Within-person improvement was determined; im- provement was adjusted for differences in baseline performance. Results: Five residents were unable to participate be- cause of scheduling problems; 9 residents in the train- ing group and 13 residents in the control group com- pleted the study. Baseline laparoscopic experience, video-trainer scores, and global assessments were not significantly different between the two groups. The training group on average practiced the video-trainer tasks 138 times (range 94 to 171 times); the control group did not practice any task. The trained group achieved significantly greater adjusted improvement in video-trainer scores (five of five tasks) and global as- sessments (four of eight criteria) over the course of the four-week curriculum, compared with controls. Conclusions: Intense training improves video-eye- hand skills and translates into improved operative per- formance for junior surgery residents. Surgical curric- ula should contain laparoscopic skills training. (J Am Coll Surg 2000;191:272–283. © 2000 by the Amer- ican College of Surgeons) Developing technical skills is essential to surgical resident training. William Halsted 1,2 introduced the surgical residency system in the United States al- most a century ago, whereby residents learn in the operating room through graded responsibility un- der direct supervision. Teaching residents in the op- erating room is effective but may be inefficient, costly, and may increase patient morbidity. 3,4 Man- aged care has placed increasing financial constraints on hospital and physician reimbursements. With more pressure on physicians to maximize efficiency, faculty may have less time available for teaching. No competing interests declared. Funding was provided by the Southwestern Center for Minimally In- vasive Surgery as supported in part by an educational grant from United States Surgical—A Division of Tyco Healthcare Group. The video- trainer was provided by Karl Storz Endoscopy. Presented, in part, at the American College of Surgeons 85th Annual Clinical Congress, Surgical Forum, San Francisco, CA, October 13, 1999. Received September 14, 1999; Revised January 12, 2000; Accepted April 3, 2000. From the Department of Surgery, University of Texas Southwestern Medical Center, Dallas, TX. Correspondence address: Daniel B Jones, MD, Department of Surgery, Uni- versity of Texas Southwestern Medical Center, 5323 Harry Hines Blvd, Dal- las, TX 75235-9092. 272 © 2000 by the American College of Surgeons ISSN 1072-7515/00/$21.00 Published by Elsevier Science Inc. PII S1072-7515(00)00339-2

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Education
Laparoscopic Training on Bench Models: Better and MoreCost Effective than Operating Room Experience?
Daniel J Scott, MD, Patricia C Bergen, MD, FACS, Robert V Rege, MD, FACS, Royce Laycock, MD, FACS,Seifu T Tesfay, RN, R James Valentine, MD, FACS, David M Euhus, MD, FACS, D Rohan Jeyarajah, MD,William M Thompson, MD, FACS, Daniel B Jones, MD, FACS
Background: Developing technical skill is essential tosurgical training, but using the operating room forbasic skill acquisition may be inefficient and expensive,especially for laparoscopic operations. This study de-termines if laparoscopic skills training using simulatedtasks on a video-trainer improves the operative perfor-mance of surgery residents.
Study Design: Second- and third-year residents (n527) were prospectively randomized to receive formallaparoscopic skills training or to a control group. Atbaseline, residents had a validated global assessment oftheir ability to perform a laparoscopic cholecystectomybased on direct observation by three evaluators whowere blinded to the residents’ randomization status.Residents were also tested on five standardized video-trainer tasks. The training group practiced the video-trainer tasks as a group for 30 minutes daily for 10days. The control group received no formal training.All residents repeated the video-trainer test and under-went a second global assessment by the same threeblinded evaluators at the end of the 1-month rotation.Within-person improvement was determined; im-
provement was adjusted for differences in baselineperformance.
Results: Five residents were unable to participate be-cause of scheduling problems; 9 residents in the train-ing group and 13 residents in the control group com-pleted the study. Baseline laparoscopic experience,video-trainer scores, and global assessments were notsignificantly different between the two groups. Thetraining group on average practiced the video-trainertasks 138 times (range 94 to 171 times); the controlgroup did not practice any task. The trained groupachieved significantly greater adjusted improvement invideo-trainer scores (five of five tasks) and global as-sessments (four of eight criteria) over the course of thefour-week curriculum, compared with controls.
Conclusions: Intense training improves video-eye-hand skills and translates into improved operative per-formance for junior surgery residents. Surgical curric-ula should contain laparoscopic skills training. (J AmColl Surg 2000;191:272–283. © 2000 by the Amer-ican College of Surgeons)
Developing technical skills is essential to surgicalresident training. William Halsted1,2 introduced thesurgical residency system in the United States al-most a century ago, whereby residents learn in theoperating room through graded responsibility un-der direct supervision. Teaching residents in the op-erating room is effective but may be inefficient,costly, and may increase patient morbidity.3,4 Man-aged care has placed increasing financial constraintson hospital and physician reimbursements. Withmore pressure on physicians to maximize efficiency,faculty may have less time available for teaching.
No competing interests declared.
Funding was provided by the Southwestern Center for Minimally In-vasive Surgery as supported in part by an educational grant from UnitedStates Surgical—A Division of Tyco Healthcare Group. The video-trainer was provided by Karl Storz Endoscopy.
Presented, in part, at the American College of Surgeons 85th AnnualClinical Congress, Surgical Forum, San Francisco, CA, October 13,1999.
Received September 14, 1999; Revised January 12, 2000; Accepted April 3,2000.From the Department of Surgery, University of Texas Southwestern MedicalCenter, Dallas, TX.Correspondence address: Daniel B Jones, MD, Department of Surgery, Uni-versity of Texas Southwestern Medical Center, 5323 Harry Hines Blvd, Dal-las, TX 75235-9092.
272© 2000 by the American College of Surgeons ISSN 1072-7515/00/$21.00Published by Elsevier Science Inc. PII S1072-7515(00)00339-2

Financial constraints may further compromise theavailability of operating room time for teachingpurposes. The cost of using operating room time fortraining surgical residents in the United States is anestimated $53 million per year.3
Laparoscopy has emerged as a very useful surgi-cal modality but complicates the problems of teach-ing residents in the operating room.5,6 Laparoscopyposes a new obstacle to skill acquisition becausesignificant experience is required before compe-tency is achieved.7-10 Depth perception is altered bya two-dimensional video imaging system and newcues must be learned before spatial relationships canbe reliably established. Long instruments diminishtactile feedback and can be awkward to use. Rangeof motion is limited by trocars, and video-eye-handcoordination must be developed to correctly posi-tion instruments in the operative field. Teachingjunior residents basic laparoscopic skills in the op-erating room can be frustrating for both the attend-ing and resident surgeons, as well as time consum-ing and inefficient.11
Several options exist for teaching surgical skilloutside the operating room. Cadavers offer a highdegree of fidelity to the living patient and a non-pressured learning atmosphere. But cadavers arecostly, of limited availability, and have noncompli-ant tissue that may be difficult to use for opera-tions.11 Live animal models may also be useful.6 Butanimals differ in anatomy from humans, can becostly, require appropriate facilities and personnel,and raise ethical concerns.12 Inanimate models haverecently become popular, especially for laparoscopictraining in residency programs.4,7,9,13-18 They aresafe, reproducible, readily available, offer unlimitedpractice, and require no supervision. Comparedwith cadavers and animals, they are more cost effec-tive.4,9,11 But bench models may not realisticallymimic human anatomy and living tissue. Even so,bench models may be the best option for trainingresidents outside of the operating room. Althoughtraining programs using inanimate models have be-come increasingly widespread, to date there is noevidence that such programs provide residents withskills that are transferable to the operating room.11,19
The purpose of this study was to develop amodel to provide intense laparoscopic skills train-ing to residents on surgical rotations and to deter-mine if improvement of skill level on a video-trainer
translates into an improvement in operativeperformance.
METHODS
A total of 27 second- and third-year surgery resi-dents rotating for one-month periods on the gen-eral surgery services at Parkland Memorial Hospitalwere available to participate in the study from Au-gust 1998 through January 1999. A nonparametricpower analysis20 was performed to ascertain if ameaningful training effect could be detected with ahigh probability using a sample of this size. It wasdetermined that this sample would provide a powerof at least 0.8 with a type I error of 0.05 if theequivalent effect size21 equalled or exceeded unity.
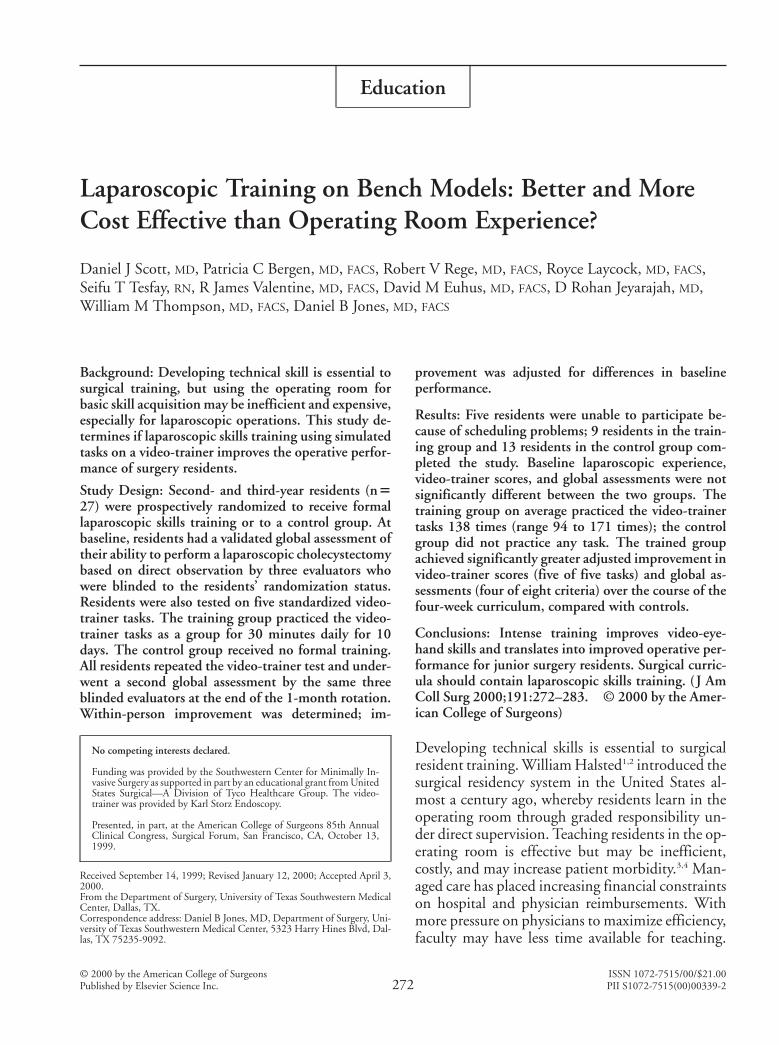
Residents gave informed consent under a pro-tocol approved by the University of Texas South-western Medical Center Institutional ReviewBoard. All patients gave consent for photographs tobe taken (operations were videotaped for investiga-tions outside the scope of this study). Residentswere randomized (Fig. 1) at the beginning of thestudy to either a training or a control group using arandom digits table. The original randomizationscheme included 13 residents assigned to the train-ing group and 14 residents assigned to the controlgroup.
During the first week of their rotation, all resi-dents were asked to complete a baseline question-naire regarding earlier laparoscopic experience andcompetency in laparoscopic skills. Global assess-ments (Table 1) were used to measure baseline op-erative performance as each resident performed alaparoscopic cholecystectomy in the operatingroom. Patients with the diagnosis of symptomaticcholelithiasis for whom an elective cholecystectomywas indicated were scheduled for the observed cases.All operations were supervised by one of three des-ignated faculty surgeons who were blinded to thetraining status of the residents. The designated fac-ulty member served as first assistant during the en-tire operation. Residents performed the laparo-scopic cholecystectomy in a one-handed or two-handed fashion, according to the faculty surgeon’spreference. The assistants were instructed to allowthe resident to perform the operation with as muchindependence as possible, while assuring patientsafety. The resident was to make key decisions re-
273Vol. 191, No. 3, September 2000 Scott et al Laparoscopic Training on Bench Models
garding the sequence of dissection and was told todirect the assistant to provide adequate retraction.The assistants were instructed to quiz the residenton the locations of key anatomic landmarks, such as
the cystic-common bile duct junction, the bordersof the triangle of Calot, and the cystic artery. Theassistants were also instructed to quiz the residenton key points of the procedure and to ask “what step
Figure 1. Algorithm for testing and randomization. Second- and third-year surgery residents were randomized to atraining or a control group and underwent testing at the beginning and end of the rotation.
274 Scott et al Laparoscopic Training on Bench Models J Am Coll Surg

is next,” so that residents would vocalize their oper-ative plan. In this way, the information the evalua-tors could use for global assessments wasmaximized.
Residents were briefed on the nature of the ex-periment but were not knowledgeable regarding thespecific content of the global assessment. Confiden-tiality of the results was guaranteed. Global assess-ments were performed by three additional facultysurgeons who were independent observers and didnot participate in the operation. The evaluatorswere also blinded to the training status of the resi-dent. The evaluators were present in the operatingroom during the key parts of the case and rated theresident according to eight criteria, each relating tosome aspect of operative performance. The eightperformance criteria included “respect for tissue,”“time and motion,” “instrument handling,”“knowledge of instruments,” “flow of operation,”“use of assistants,” “knowledge of specific proce-dure,” and “overall performance.” Each area of per-formance was rated on a scale of 1 (worst) to 5
(best), with the middle and extreme endpoints ofthe scale anchored by explicit descriptors, as de-scribed by Reznick and colleagues.11,22,23
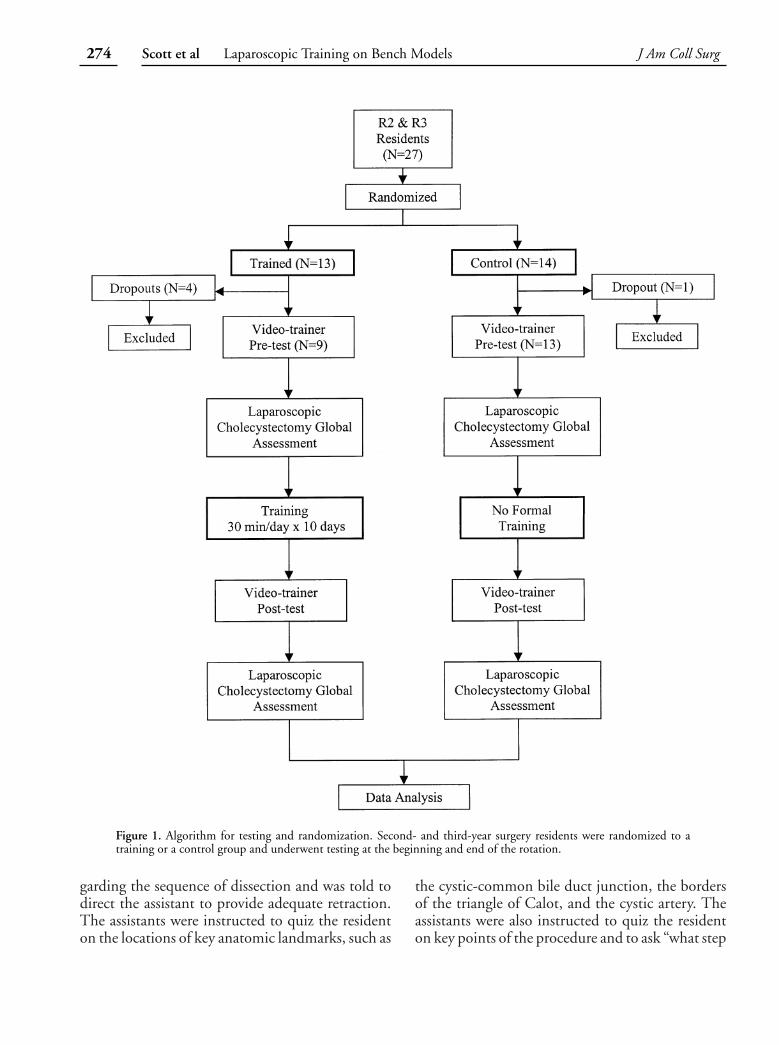
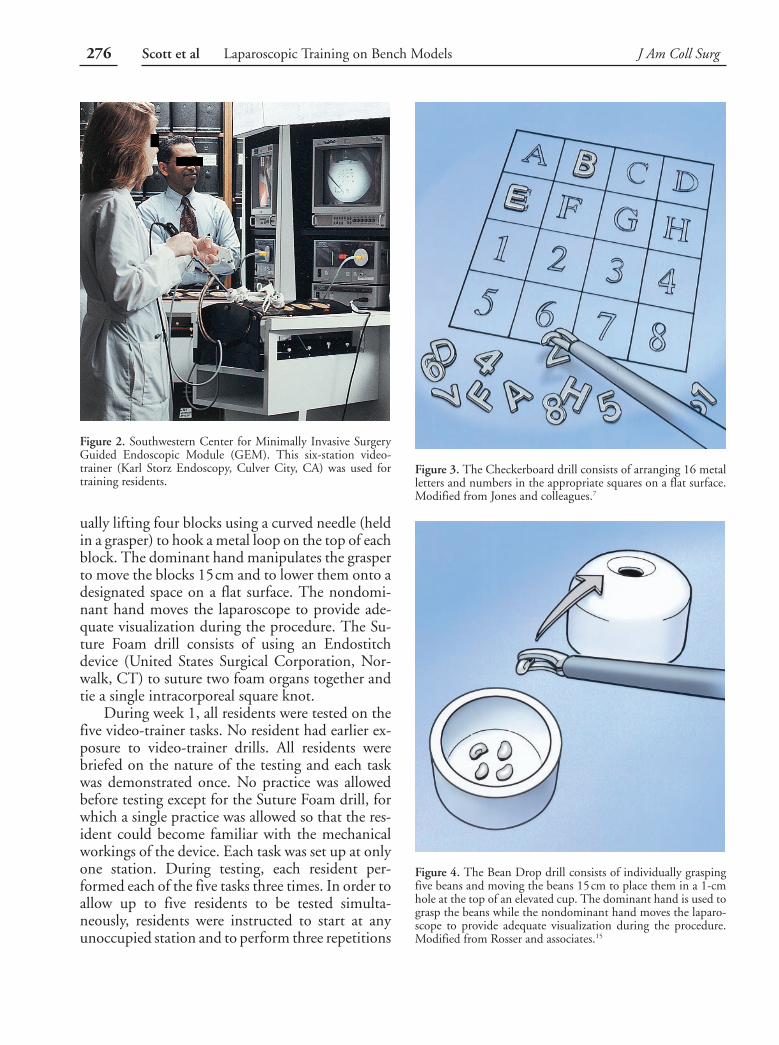
We based our curriculum on five establishedlaparoscopic drills suitable for novice surgeons thatcould be performed on a video-trainer (Fig.2).7,13,15,24 The five tasks included Checkerboard(Fig. 3), Bean Drop (Fig. 4), Running String (Fig.5), Block Move (Fig. 6), and Suture Foam (Fig. 7).The Checkerboard drill involves arranging 16 metalletters and numbers in the appropriate squares on aflat surface. The Bean Drop drill consists of indi-vidually grasping five beans and moving the beans15cm to place them in a 1-cm hole at the top of anelevated cup. The dominant hand is used to graspthe beans while the nondominant hand moves thelaparoscope to provide adequate visualization dur-ing the procedure. The Running String drill mimicsrunning bowel; two graspers are used to run a140-cm string from one end to the other, graspingthe string only at colored sections marked at 12-cmintervals. The Block Move drill consists of individ-
Table 1. Global Rating Scale of Operative Performance*
PerformanceCharacteristic
Scale
1 2 3 4 5
Respect for tissue Frequently used unnecessaryforce on tissue or causeddamage by inappropriateuse of instruments
Careful handling of tissue butoccasionally causedinadvertent damage
Consistently handled tissuesappropriately with minimaldamage
Time and motion Many unnecessary moves Efficient time/motion butsome unnecessary moves
Clear economy of movement andmaximum efficiency
Instrumenthandling
Repeatedly makes tentativeawkward or inappropriatemoves with instruments
Competent use ofinstruments butoccasionally stiff orawkward
Fluid moves with instruments andno awkwardness
Knowledge ofinstruments
Frequently asked for wronginstrument or usedinappropriate instrument
Knew names of mostinstruments and usedappropriate tool for task
Obviously familiar with theinstruments and their names
Flow of operation Frequently stoppedoperating and seemedunsure of next move
Demonstrated some forwardplanning with reasonableprogression of procedure
Planned course of operationeffortless from one move to thenext
Use of assistants Failed to use assistants Appropriate use of assistantsmost of the time
Strategically used assistants to thebest advantage at all times
Knowledge ofspecificprocedure
Required specific instructionat most steps
Knew all important steps ofthe operation
Familiar with all aspects of theoperation
Overallperformance
Unable to perform operationindependently
Competent, could performoperation with minimalteaching assistance
Clearly superior, able to performoperation independently withconfidence
*Modified from Reznick and colleagues.22 15worst possible score, 55best possible score.
275Vol. 191, No. 3, September 2000 Scott et al Laparoscopic Training on Bench Models
ually lifting four blocks using a curved needle (heldin a grasper) to hook a metal loop on the top of eachblock. The dominant hand manipulates the grasperto move the blocks 15cm and to lower them onto adesignated space on a flat surface. The nondomi-nant hand moves the laparoscope to provide ade-quate visualization during the procedure. The Su-ture Foam drill consists of using an Endostitchdevice (United States Surgical Corporation, Nor-walk, CT) to suture two foam organs together andtie a single intracorporeal square knot.
During week 1, all residents were tested on thefive video-trainer tasks. No resident had earlier ex-posure to video-trainer drills. All residents werebriefed on the nature of the testing and each taskwas demonstrated once. No practice was allowedbefore testing except for the Suture Foam drill, forwhich a single practice was allowed so that the res-ident could become familiar with the mechanicalworkings of the device. Each task was set up at onlyone station. During testing, each resident per-formed each of the five tasks three times. In order toallow up to five residents to be tested simulta-neously, residents were instructed to start at anyunoccupied station and to perform three repetitions
Figure 3. The Checkerboard drill consists of arranging 16 metalletters and numbers in the appropriate squares on a flat surface.Modified from Jones and colleagues.7
Figure 4. The Bean Drop drill consists of individually graspingfive beans and moving the beans 15cm to place them in a 1-cmhole at the top of an elevated cup. The dominant hand is used tograsp the beans while the nondominant hand moves the laparo-scope to provide adequate visualization during the procedure.Modified from Rosser and associates.15
Figure 2. Southwestern Center for Minimally Invasive SurgeryGuided Endoscopic Module (GEM). This six-station video-trainer (Karl Storz Endoscopy, Culver City, CA) was used fortraining residents.
276 Scott et al Laparoscopic Training on Bench Models J Am Coll Surg
of the task set up at that station. When finished,residents were instructed to rotate to another unoc-cupied station. If more than one station was unoc-cupied, the resident could choose which station togo to next. Scores were recorded as the average timenecessary for task completion. After baseline testingwas completed, the residents were told to whichgroup they had been randomized.
In the second and third weeks of their rotation,
residents randomized to training met as a group forat least 30 minutes daily for 10 days. All residentswere excused from clinical duties to attend trainingsessions, which were held at 7:00 AM, Mondaythrough Friday, for 2 weeks. During this structuredtraining time, residents practiced the video-trainertasks; the choice of which tasks to practice was leftup to the resident, but residents were encouraged topractice all five tasks during each session. Addi-
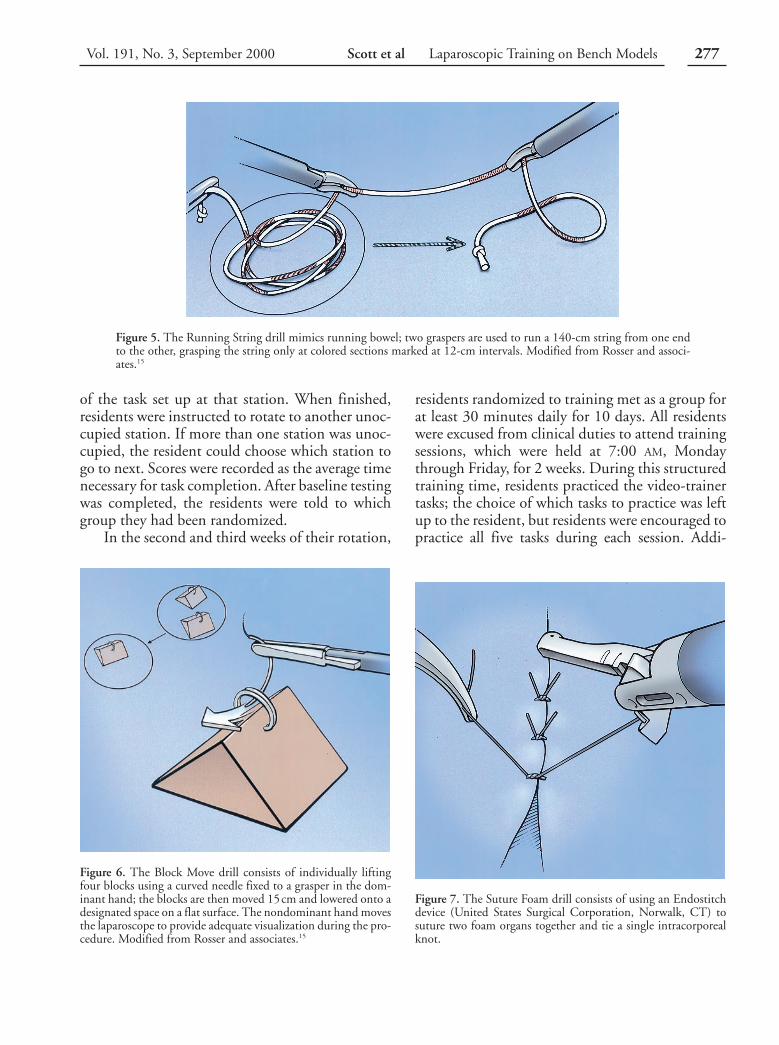
Figure 5. The Running String drill mimics running bowel; two graspers are used to run a 140-cm string from one endto the other, grasping the string only at colored sections marked at 12-cm intervals. Modified from Rosser and associ-ates.15
Figure 6. The Block Move drill consists of individually liftingfour blocks using a curved needle fixed to a grasper in the dom-inant hand; the blocks are then moved 15cm and lowered onto adesignated space on a flat surface. The nondominant hand movesthe laparoscope to provide adequate visualization during the pro-cedure. Modified from Rosser and associates.15
Figure 7. The Suture Foam drill consists of using an Endostitchdevice (United States Surgical Corporation, Norwalk, CT) tosuture two foam organs together and tie a single intracorporealknot.
277Vol. 191, No. 3, September 2000 Scott et al Laparoscopic Training on Bench Models
tional demonstration of tasks was rarely given andonly on specific request by the resident. Residentsrandomized to the control group received no struc-tured skills training outside of the operating roomand were not allowed access to the video-trainerduring the study. Didactic lectures on how to per-form a laparoscopic cholecystectomy were not givento either group during the study interval.
In the fourth week, all residents were againtested on the five video-trainer tasks. Each task wasperformed three times and the average time forcompletion of each task was recorded. All residentsperformed a second laparoscopic cholecystectomyin the operating room with the same first assistantsurgeon, who was blinded to the resident’s trainingstatus. The same three independent faculty evalua-tors performed global assessments based on directobservation; the evaluators were also blinded to theresident’s training status. At the completion of therotation, all residents were asked to complete ques-tionnaires regarding their laparoscopic experience;those who underwent training were asked if they per-ceived improvement in their laparoscopic abilities.
After their rotation, residents randomized tothe control group were offered, for their own edu-cational benefit, the same training that the traininggroup received; data from repeat trainees were notincluded as part of this study.
Questionnaire data regarding comfort withlaparoscopic surgery were analyzed using Fisher’sexact test. Baseline performance was analyzed bycomparing video-trainer and global assessmentscores for the control and trained groups. To test thehypothesis that there was no difference between thecontrol and trained groups at baseline testing, atwo-tailed Wilcoxon rank-sum test was used.
To determine if training was beneficial, within-person changes in performance were compared forthe control and trained groups. Improvement was
defined as the difference in performance at the pre-and posttesting intervals. Improvement was deter-mined for both video-trainer and global assessmentscores. Because the amount of improvement variedwith baseline performance, a linear covariance ad-justment was used to compensate for differences inbaseline scores. The covariance-adjusted improve-ments for residents in the control and trainedgroups were compared using a Wilcoxon rank-sumtest. To test the hypothesis that the trained groupachieved greater adjusted improvement than thecontrol group, a one-tailed test was used. Tests wereconsidered significant at p#0.05.
RESULTS
Over the 6-month course of the study, one residentin the control group and four residents in thetrained group were unable to participate because ofscheduling problems, caused by vacations andchanges in rotation schedules. So, 22 residents com-pleted the study, with 13 in the control group and 9in the trained group. There was no crossover be-tween groups, except for 6 of 13 control group res-idents who subsequently underwent training fortheir own benefit. Data from repeat trainees werenot included in this study.
Faculty assistant surgeons and evaluators wereinterviewed to verify blinding. All of the assistantsurgeons and evaluators reported being blinded tothe randomization status of the residents 100% ofthe time during the study.
On the baseline questionnaire, both groups re-ported comparable laparoscopic experience; themean number of cases per resident as surgeon orfirst assistant was 18 for control versus 15 fortrained (p50.501).
Baseline scores for the video-trainer test andglobal assessment during laparoscopic cholecystec-
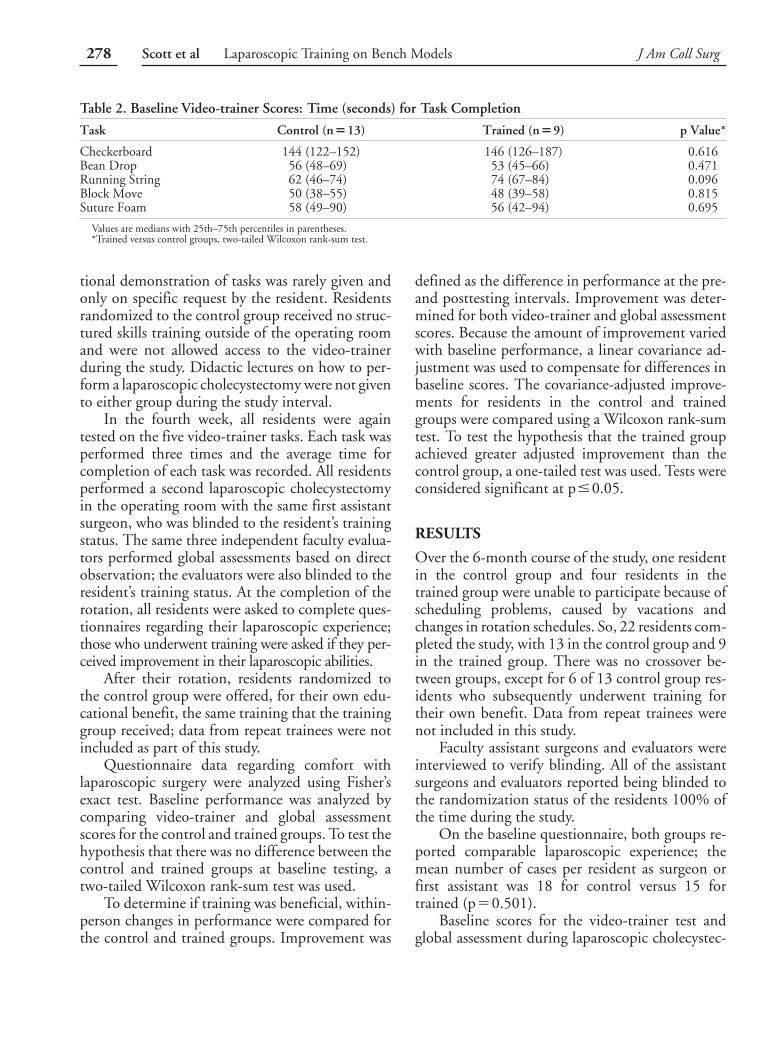
Table 2. Baseline Video-trainer Scores: Time (seconds) for Task Completion
Task Control (n513) Trained (n59) p Value*
Checkerboard 144 (122–152) 146 (126–187) 0.616Bean Drop 56 (48–69) 53 (45–66) 0.471Running String 62 (46–74) 74 (67–84) 0.096Block Move 50 (38–55) 48 (39–58) 0.815Suture Foam 58 (49–90) 56 (42–94) 0.695
Values are medians with 25th–75th percentiles in parentheses.*Trained versus control groups, two-tailed Wilcoxon rank-sum test.
278 Scott et al Laparoscopic Training on Bench Models J Am Coll Surg
tomy are listed in Tables 2 and 3. There were nosignificant differences between the trained and con-trol groups.
All nine residents in the training group com-pleted 10 practice sessions lasting 30 minutes. Onaverage, trained residents practiced 138 video-trainer tasks (range 94 to 171 tasks). Each of the fivetasks was practiced 28 times (range 19 to 34 times).Residents randomized to the control group did notpractice any video-trainer task.
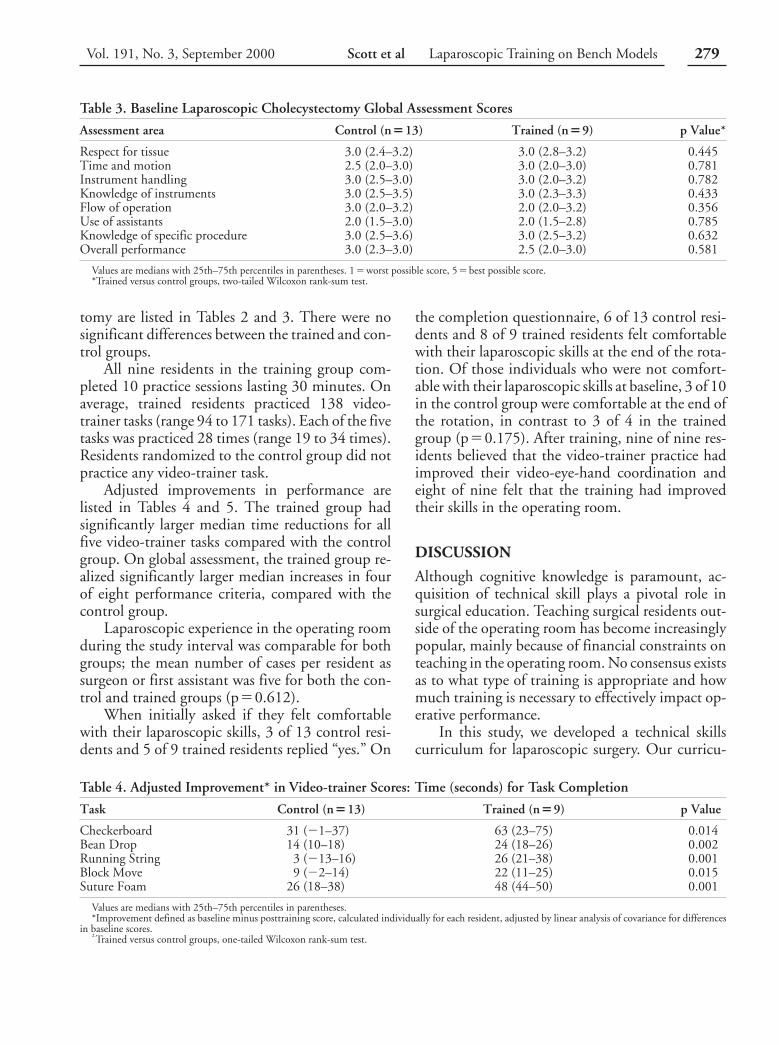
Adjusted improvements in performance arelisted in Tables 4 and 5. The trained group hadsignificantly larger median time reductions for allfive video-trainer tasks compared with the controlgroup. On global assessment, the trained group re-alized significantly larger median increases in fourof eight performance criteria, compared with thecontrol group.
Laparoscopic experience in the operating roomduring the study interval was comparable for bothgroups; the mean number of cases per resident assurgeon or first assistant was five for both the con-trol and trained groups (p50.612).
When initially asked if they felt comfortablewith their laparoscopic skills, 3 of 13 control resi-dents and 5 of 9 trained residents replied “yes.” On
the completion questionnaire, 6 of 13 control resi-dents and 8 of 9 trained residents felt comfortablewith their laparoscopic skills at the end of the rota-tion. Of those individuals who were not comfort-able with their laparoscopic skills at baseline, 3 of 10in the control group were comfortable at the end ofthe rotation, in contrast to 3 of 4 in the trainedgroup (p50.175). After training, nine of nine res-idents believed that the video-trainer practice hadimproved their video-eye-hand coordination andeight of nine felt that the training had improvedtheir skills in the operating room.
DISCUSSION
Although cognitive knowledge is paramount, ac-quisition of technical skill plays a pivotal role insurgical education. Teaching surgical residents out-side of the operating room has become increasinglypopular, mainly because of financial constraints onteaching in the operating room. No consensus existsas to what type of training is appropriate and howmuch training is necessary to effectively impact op-erative performance.
In this study, we developed a technical skillscurriculum for laparoscopic surgery. Our curricu-
Table 3. Baseline Laparoscopic Cholecystectomy Global Assessment Scores
Assessment area Control (n513) Trained (n59) p Value*
Respect for tissue 3.0 (2.4–3.2) 3.0 (2.8–3.2) 0.445Time and motion 2.5 (2.0–3.0) 3.0 (2.0–3.0) 0.781Instrument handling 3.0 (2.5–3.0) 3.0 (2.0–3.2) 0.782Knowledge of instruments 3.0 (2.5–3.5) 3.0 (2.3–3.3) 0.433Flow of operation 3.0 (2.0–3.2) 2.0 (2.0–3.2) 0.356Use of assistants 2.0 (1.5–3.0) 2.0 (1.5–2.8) 0.785Knowledge of specific procedure 3.0 (2.5–3.6) 3.0 (2.5–3.2) 0.632Overall performance 3.0 (2.3–3.0) 2.5 (2.0–3.0) 0.581
Values are medians with 25th–75th percentiles in parentheses. 15worst possible score, 55best possible score.*Trained versus control groups, two-tailed Wilcoxon rank-sum test.
Table 4. Adjusted Improvement* in Video-trainer Scores: Time (seconds) for Task Completion
Task Control (n513) Trained (n59) p Value†
Checkerboard 31 (21–37) 63 (23–75) 0.014Bean Drop 14 (10–18) 24 (18–26) 0.002Running String 3 (213–16) 26 (21–38) 0.001Block Move 9 (22–14) 22 (11–25) 0.015Suture Foam 26 (18–38) 48 (44–50) 0.001
Values are medians with 25th–75th percentiles in parentheses.*Improvement defined as baseline minus posttraining score, calculated individually for each resident, adjusted by linear analysis of covariance for differences
in baseline scores.†Trained versus control groups, one-tailed Wilcoxon rank-sum test.
279Vol. 191, No. 3, September 2000 Scott et al Laparoscopic Training on Bench Models

lum was aimed at teaching basic skills to juniorsurgery residents when they were beginning to per-form laparoscopic operations. We chose a curricu-lum based on five established laparoscopic drillsthat foster the development of video-eye-hand co-ordination.7,13,15,24 The Checkerboard drill is de-signed to develop spatial relationships on a planarsurface and to facilitate accurate motor skills. TheBean Drop and Block Move drills both require us-ing the nondominant hand to move the laparoscopeto provide adequate visualization during the proce-dure; so, two-handed video-eye-hand coordinationis developed. The Bean Drop drill requires fine mo-tor skill to accurately grasp the beans. The BlockMove drill requires supination and pronation tohook the metal ring with the curved needle duringblock lifting and releasing; depth perception andwrist articulation skills are developed. The RunningString drill requires two-handed coordination anddevelops spatial relationships along a linear struc-ture. The Suture Foam drill requires manual dexter-ity to manipulate the Endostitch device and devel-ops two-handed coordination during suturing ofthe foam organs. Depth perception is also critical tosuccessful knot tying. Compared with conventionalintracorporeal suturing, using the Endostitch de-vice is faster and preferred by surgery residents.24
Whereas conventional laparoscopic suturing is anadvanced skill suitable for senior residents, the En-dostitch device may be more suitable for novicesurgeons.
Each of the video-trainer drills could be com-pleted quickly (in less than 3 minutes) and multiplerepetitions of each task were possible during the30-minute training sessions. Although each drill re-
quired a specific subset of technical abilities, all ofthe drills focused on the development of video-eye-hand coordination. A multitask curriculum withmultiple repetitions was chosen to facilitate skillacquisition. We hypothesized that if residents mas-tered basic laparoscopic skills, they would be betterprepared to perform actual operations.
We tailored the course schedule to train resi-dents while they were on a four-week surgical rota-tion. Training was conducted in group sessions on afree-standing six-station video-trainer developed bythe Southwestern Center for Minimally InvasiveSurgery at the University of Texas SouthwesternMedical Center (Fig. 2). Multistation video-trainers have never previously been available. Theadvantages of group-session training may be en-hanced esprit de corps, as evidence by all nine resi-dents in the trained group completing all 10 train-ing sessions. A healthy sense of competition maydevelop when residents train side by side, enhanc-ing motivation to improve their skills.
Our data indicate that the trained and controlgroups were not significantly different at baselineaccording to self-reported laparoscopic experience,video-trainer scores, and global assessments. Addi-tionally, there was no difference in laparoscopic op-erative experience during the study interval be-tween the two groups. So, the measured differencein the final skill level between the two groups can beattributed to the training received in the skillslaboratory.
The difference between individual baseline andposttest scores was used to assess the effect of train-ing. An individual who performed poorly on thebaseline test had a greater opportunity to improve
Table 5. Adjusted Improvement* in Laparoscopic Cholecystectomy Global Assessment Scores
Assessment area Control (n513) Trained (n59) p Value†
Respect for tissue 0.1 (20.6–0.5) 0.3 (0.3–0.5) 0.035Time and motion 20.3 (20.5–0.6) 0.3 (0.1–0.8) 0.075Instrument handling 0.3 (20.4–0.3) 0.6 (0.4–0.8) 0.005Knowledge of instruments 0.4 (0.0–1.0) 0.6 (0.5–1.5) 0.058Flow of operation 0.4 (20.5–1.2) 1.0 (0.6–1.2) 0.090Use of assistants 0.7 (20.4–1.0) 1.0 (0.8–1.6) 0.035Knowledge of specific procedure 0.4 (0.0–1.1) 1.0 (0.4–1.3) 0.100Overall performance 0.2 (20.5–0.6) 0.7 (0.6–1.0) 0.007
Values are medians with 25th–75th percentiles in parentheses.*Improvement defined as posttraining minus baseline score, calculated individually for each resident, adjusted by linear analysis of covariance for differences
in baseline scores.†Trained versus control groups, one-tailed Wilcoxon rank-sum test.
280 Scott et al Laparoscopic Training on Bench Models J Am Coll Surg

than did a person who did well on the initial assess-ment. The statistical technique of covariance anal-ysis25 provided a means of compensating for indi-vidual differences in baseline test scores. The neteffect of this analysis was to adjust each individual’simprovement score to an equivalent score, as if eachbaseline test score had been equal to the overallbaseline test average.
Using the covariance adjustment, we detectedimprovement in video-trainer skills for both groupsover the course of the 4-week study period (Table4). Improvement in the control group was expectedbecause these residents were exposed to each taskthree times during the initial testing session andbecause they were undergoing “on-the-job” trainingwhile performing operative cases on their surgicalrotation. The trained group, however, achieved sig-nificantly larger median time reductions for all fivevideo-trainer tasks. Similarly, improvement wasnoted on global assessments for both groups. Buttrained residents achieved greater median improve-ment in the operating room compared with controlresidents (Table 5). The differences in global assess-ment improvement for the control versus trainedresidents had observed significances that did notexceed 0.1 for all eight criteria, and were less than0.05 for four of eight criteria. The difference in“overall performance” improvement for trained andcontrol residents was significant at p50.007. Ourconclusion from this data is that training worked.Not only did training improve performance on thevideo-trainer, but more importantly training im-proved performance in the operating room.
The questionnaire data indicate that juniorlevel residents believe they need additional laparo-scopic training. Only 36% of the residents reportedfeeling comfortable with their skill level at the be-ginning of the rotation. Of those individuals whowere not comfortable with their laparoscopic skillsat baseline, 3 out of 4 in the trained group werecomfortable at the end of the rotation, in contrast to3 out of 10 in the control group. Despite the largerproportion of trained residents feeling comfortablewith their laparoscopic skills compared with con-trols, the observed significance was 0.175. The ma-jority of trained residents felt that training had im-proved their skill level in the training center (100%)and in the operating room (89%), further support-
ing the video-trainer and global assessment datathat showed the same effects.
Several authors have reported training pro-grams based on inanimate models for both conven-tional open surgery and for laparoscopicsurgery.4,7,9,11,13-16,22,23 Rosser and associates15 showedthat laparoscopic skills may be taught outside of theoperating room using simulators. Similarly severalstudies have shown that laparoscopic skills can bemeasured on a video-trainer and that proficiencyimproves with task repetition.7,18 The limitation ofthese studies is that the outcomes (improved skills)are measured on the same simulator on which train-ing took place and not in the operating room. Sev-eral investigators have asked whether improved pro-ficiency in the laboratory setting correlates withexcellent surgical performance in clinical prac-tice.11,19 Martin and colleagues23 showed that foropen operations, testing skill level on a benchmodel is equally effective as testing on live animalmodels. Anastakis and coworkers11 showed thattraining for open operations on bench modelsyields an equivalent skill level as training on cadavermodels, suggesting that skills acquired in the drylaboratory may be transferable to human opera-tions. No such data exist for laparoscopic proce-dures. Until now, no data existed for open or lapa-roscopic procedures, which definitively correlatesimprovement in skill level on inanimate modelswith improved skill level in live human opera-tions.11,19 Our study shows that skills acquired on alaparoscopic simulator are transferable to the oper-ating room.
Several obstacles made reaching this conclusiondifficult. In addition to the difficulties associatedwith developing a training model and a schedulecapable of accommodating residents while on sur-gical rotations, the ability to measure skill level inthe operating room was a major undertaking. Sev-eral authors have reported using a procedure-specific checklist for open11,22,23,26,27 and laparo-scopic28 procedures, in an effort to evaluateoperative performance. Global assessments of oper-ative performance based on direct observation havesuperior validity and reliability to checklist evalua-tions and may be used for different operations with-out modification.11,22,23,29 Global assessments maycurrently be the best tools available for evaluatingskill level in the operating room.
281Vol. 191, No. 3, September 2000 Scott et al Laparoscopic Training on Bench Models

Although standardizing the operating room ex-perience proved difficult, we controlled for poten-tial problems related to differing operative condi-tions by using three designated staff membersblinded to the resident’s randomization status asfirst assistants for all cases. All staff assistants weregiven standardized instructions regarding their role.Residents were instructed to use either a one-handed or a two-handed technique at the attendingphysician’s discretion. Some faculty members werenot comfortable allowing junior residents to use atwo-handed technique. The choice of which tech-nique to use was left up to the faculty surgeons,because they were ultimately responsible for patientsafety. The use of either a one-handed or a two-handed technique may have created a bias in ourmethodology; fortunately, evaluators were able toperform global assessments regardless of technique.
A prospective randomized design was chosen toovercome variability between groups. Evaluatorswere blinded to the resident’s randomization statusand were independent observers who did not par-ticipate in the operations. Despite our efforts toinclude only elective cholecystectomies in the study,the severity of underlying disease varied. Outcomessuch as operative time, length of stay, and compli-cations were not prospectively measured. Despitethe variability present in the operating room, globalassessments were able to reliably measure differ-ences in operative performance.
Proving that skills acquired on a video-trainerare transferable to the operating room has signifi-cant ramifications. If residents first master basiclaparoscopic skills in the laboratory setting, theymay be better prepared to enter the operating roomto perform laparoscopic procedures. The resident’sfirst few laparoscopic cases will no longer be nerve-racking experiences in which a staff surgeon pain-fully tries to teach the resident basic video-eye-handcoordination, resulting in frustration for all thoseinvolved. Once the learning curve of using longlaparoscopic instruments in a disorienting two-dimensional environment is overcome, residents nolonger will use up vast amounts of expensive oper-ating room time learning basic skills. Instead, resi-dents will be able to concentrate on learning ana-tomic details, nuances of surgical technique, anddiscussing patient management. So, the educa-
tional experience in the operating room is enhancedby laboratory skills training. For hospitals, im-proved operator skill may decrease operative timesand lower hospital costs. Better-trained residentsmay mean improved patient care. Training resi-dents before they actually enter the operating roomseems credible.
How long the benefit of training will last is notyet known. How long it would take for the controlresidents to “catch up” with their trained peers isalso not known. A followup study on the residentswho underwent our curriculum would be interest-ing. Because a number of control residents subse-quently underwent training for their own educa-tional benefit, such a study may not be feasible. It isintuitive that providing residents with basic video-eye-hand coordination boosts their skills to a levelthat is necessary to adequately perform laparoscopiccases and should be longlasting. Once basic skillsare learned, it is unlikely that they will be forgotten.
A final note concerning costs. The list price ofthe Guided Endoscopic Module (GEM, Karl StorzEndoscopy, Culver City, CA) ranges from$215,000 to $285,000, depending on the quality ofvideo-imaging equipment installed. At the Univer-sity of Texas Southwestern Medical Center, 186 res-idents train in general surgery, urology, and gyne-cology. The cost of training residents using thevideo-trainer is $270 per graduating resident. Incomparison, Bridges and Diamond,3 at the Univer-sity of Tennessee Medical Center—Knoxville, esti-mate that using operating room time to train resi-dents costs about $48,000 per graduating resident.Training outside of the operating room, using avideo-trainer such as the GEM, seems cost effective.
Acknowledgment: The authors gratefully ac-knowledge funding and research design assistancefrom the Association for Surgical Education. Fund-ing was provided by the Southwestern Center forMinimally Invasive Surgery as supported in part by aneducational grant from United States Surgical—A Di-vision of Tyco Healthcare Group. The video-trainerwas provided by Karl Storz Endoscopy. Statistical anal-ysis was performed by William H Frawley, PhD, at theDepartment of Academic Computing, University ofTexas Southwestern Medical Center.
282 Scott et al Laparoscopic Training on Bench Models J Am Coll Surg

References1. Halsted WS. The training of the surgeon. Bull Johns Hopkins
Hosp 1904;15:267.2. Barnes RW, Lang NP, Whitesede MF. Halstedian technique re-
visited: innovations in teaching surgical skills. Ann Surg 1989;210:118–121.
3. Bridges M, Diamond DL. The financial impact of teachingsurgical residents in the operating room. Am J Surg 1999;177:28–32.
4. Hawasli A, Featherstone R, Lloyd L, Vorhees M. Laparoscopictraining in residency program. J Laparoendosc Surg 1996;6:171–174.
5. Scott-Conner CEH, Hall TJ, Anglin BL, et al. The integrationof laparoscopy into a surgical residency and implications for thetraining environment. Surg Endosc 1994;8:1054–1057.
6. Hunter JG, Sackier JM, Berci G. Training in laparoscopic cho-lecystectomy: quantifying the learning curve. Surg Endosc 1994;8:28–31.
7. Jones DB, Brewer JD, Soper NJ. The influence of three-dimensional video systems on laparoscopic task performance.Surg Laparosc Endosc 1996;6:191–197.
8. Wolfe BM, Szabo Z, Moran ME, et al. Training for minimallyinvasive surgery: need for surgical skills. Surg Endosc 1993;7:93–95.
9. Melvin WS, Johnson JA, Ellison EC. Laparoscopic skills en-hancement. Am J Surg 1996;172:377–379.
10. Dent TL. Training, credentialing, and evaluation in laparo-scopic surgery. Surg Clin North Am 1992;72:1003–1010.
11. Anastakis DJ, Regehr G, Reznick RK, et al. Assessment of tech-nical skills transfer from the bench training model to the humanmodel. Am J Surg 1999;177:167–170.
12. Rowan AN. Is justification of animal research necessary? JAMA1993;269:1114.
13. Rosser JC, Rosser LE, Savalgi RS. Skill acquisition and assess-ment for laparoscopic surgery. Arch Surg 1997;132:200–204.
14. Shapiro SJ, Paz-Partlow M, Daykhovsky L, et al. The use of amodular skills center for the maintenance of laparoscopic skills.Surg Endosc 1996;10:816–819.
15. Rosser JC, Rosser LE, Savalgi RS. Objective evaluation of alaparoscopic surgical skill program for residents and senior sur-geons. Arch Surg 1998;1333:657–661.
16. Derossis AM, Fried GM, Abrahamowicz M, et al. Developmentof a model for training and evaluation of laparoscopic skills.Am J Surg 1998;175:482–487.
17. Macmillan AIM, Cuschieri A. Assessment of innate ability andskills for endoscopic manipulations by the advanced Dundeeendoscopic psychomotor tester: predictive and concurrent valid-ity. Am J Surg 1999;177:274–277.
18. Derossis AM, Bothwell J, Sigman HH, Fried GM. The effect ofpractice on performance in a laparoscopic simulator. Surg En-dosc 1998;12:1117–1120.
19. Gagner M. Objective evaluation of a laparoscopic surgical skillprogram [letter]. Arch Surg 1998;133:911–912.
20. Hollander M, Wolfe DA. Nonparametric statistical methods.New York: Wiley; 1999:119–120.
21. Kirk RE. Statistics, an introduction. Fort Worth: Holt, Rinehart& Winston; 1990:334.
22. Reznick R, Regehr G, MacRae H, et al. Testing technical skill viaan innovative “bench station” examination. Am J Surg 1996;173:226–230.
23. Martin JA, Regehr G, Reznick R, et al. Objective structuredassessment of technical skills (OSATS) for surgical residents. Br JSurg 1997;84:273–278.
24. Nguyen NT, Ho HS, Mayer KL, et al. Laparoscopic knot tyingtechniques: a comparison of performance and preference amongsurgery residents. J Surg Res 1999;86:291.
25. Fleiss JL. Design and analysis of clinical experiments. New York:Wiley; 1986.
26. Kopta JA. An approach to the evaluation of operative skill. Surg1971;70:297–303.
27. Lossing A, Gretsch G. A prospective controlled trial of teachingbasic surgical skills with 4th year medical students. Med Teacher1992;14:49–52.
28. Eubanks TR, Clements R, Pohl D, et al. A valid and reliablescoring system for assessing technical skills during laparoscopiccholecystectomy. Surg Endosc 1999;13[suppl]:S32.
29. Winckel CP, Reznick RK, Cohen R, Taylor B. Reliability andconstruct validity of a structured technical skills assessmentform. Am J Surg 1994;167:423–427.
283Vol. 191, No. 3, September 2000 Scott et al Laparoscopic Training on Bench Models
Related Documents











