CLINICAL GUIDELINE, PART 2 Laboratory Evaluation in the Diagnosis of Lyme Disease Peter Tugwell, MD; David T. Dennis, MD; Arthur Weinstein, MD; George Wells, PhD; Beverley Shea, BScN; Graham Nichol, MD; Robert Hayward, MD; Robert Lightfoot, MD; Philip Baker, BSc; and Allen C. Steere, MD Purpose: To provide a quantitative and qualitative eval- uation of the predictive value of the laboratory diagnosis of Lyme disease and to use the resultant data to formulate guidelines for clinical diagnosis. Data Sources: A MEDLINE search of English-language articles or articles with English-language abstracts pub- lished from 1982 to 1996. Data Extraction: Sensitivity, specificity, and likelihood ratios were calculated, and a random-effects model was used to combine the proportions from the eligible studies. Prespecified criteria were used to determine which studies were eligible for analysis. Data Synthesis: Laboratory testing in general is not clin- ically useful if the pretest probability of Lyme disease is less than 0.20 or greater than 0.80. When the pretest probabil- ity is 0.20 to 0.80, sequential testing with enzyme-linked immunosorbent assay and Western blot is the most accu- rate method for ruling in or ruling out the possibility of Lyme disease. Conclusions: Laboratory testing is recommended only in patients whose pretest probability of Lyme disease is 0.20 to 0.80. If the pretest probability is less than 0.20, testing will result in more false-positive results than true-positive results; a negative test result in this situation effectively rules out the disease. This paper is also available at http://www.acponline.org. Ann Intern Med. 1997;127:1109-1123. From the University of Ottawa, Ottawa, Ontario, Canada; Cen- ters for Disease Control and Prevention, Fort Collins, Colorado; New York Medical College, Valhalla, New York; New England Medical Center, Boston, Massachusetts; and McMaster Univer- sity Medical Centre, Hamilton, Ontario, Canada. For current author addresses, see end of text. 1. Introduction 1.1 Lyme disease is the most common tick-borne disease in North America. From 1982 through 1994, more than 70 000 cases were reported in North America; most of these cases were in the United States (1). It is important that clinicians diagnose Lyme disease correctly because efficacious therapy is available and delayed or inadequate treatment can lead to many morbid sequelae. Lyme disease is a complex multisystem disease caused by the spiro- chete Borrelia burgdorferi (2). It affects persons of all ages and both sexes. Since the disease was recog- nized in Connecticut in 1975 (3), endemic areas have been identified in several regions in North America. In more restricted areas in some north- eastern and upper midwestern U.S. states, the dis- ease has assumed the characteristics of an emerging epidemic (4-9). The true incidence is almost cer- tainly underestimated because of under-reporting (10, 11). 1.2 Most patients develop a distinctive rash, ery- thema migrans, that is accompanied by such flu-like symptoms as fatigue, headache, mild stiff neck, joint and muscle aches, and fever (12). Some weeks or months after the initial exposure, symptoms and signs of disseminated disease (particularly neuro- logic, cardiac, or articular disease) may develop in untreated patients (13, 14). 1.3 Case definitions of Lyme disease have been developed in the United States for national disease surveillance purposes. A positive serologic test re- sult was initially required for patients who had er- ythema migrans alone and had not been exposed to Lyme disease in endemic areas (15), but the 1990 criteria established in the Centers for Disease Con- trol and Prevention's (CDC's) U.S. Lyme disease national surveillance definition reduced this require- ment to a recommendation (Table 1) (16). These criteria were developed for an epidemiologic case definition intended for surveillance purposes only. However, previous national disease surveillance cri- teria have been used in clinical studies (17, 18), and such definitions do provide standardization. Stan- dardization allows comparisons of clinical studies and permits the performance of meta-analysis to facilitate development of clinically useful guidelines. 1.4 Requests for laboratory testing for Lyme dis- ease have increased rapidly. In Wisconsin, for ex- ample, it was reported that more than 60 000 tests were being done annually (19); in New Jersey, 5000 tests were done in 1 week in 1989 (20). According to market projections for the United States, 2.79 million rapid tests were to have been done for Lyme disease in 1995 (21). Testing is often done in per- sons who have only nonspecific signs and symptoms of illness, such as headache, fatigue, myalgia, or arthralgia. Even in highly endemic areas, the pretest probability of Lyme disease in such patients is less © 1997 American College of Physicians 1109

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

CLINICAL GUIDELINE, PART 2
Laboratory Evaluation in the Diagnosis of Lyme Disease Peter Tugwell, MD; David T. Dennis, MD; Arthur Weinstein, MD; George Wells, PhD; Beverley Shea, BScN; Graham Nichol, MD; Robert Hayward, MD; Robert Lightfoot, MD; Philip Baker, BSc; and Allen C. Steere, MD
Purpose: To provide a quantitative and qualitative evaluation of the predictive value of the laboratory diagnosis of Lyme disease and to use the resultant data to formulate guidelines for clinical diagnosis.
Data Sources: A MEDLINE search of English-language articles or articles with English-language abstracts published from 1982 to 1996.
Data Extraction: Sensitivity, specificity, and likelihood ratios were calculated, and a random-effects model was used to combine the proportions from the eligible studies. Prespecified criteria were used to determine which studies were eligible for analysis.
Data Synthesis: Laboratory testing in general is not clinically useful if the pretest probability of Lyme disease is less than 0.20 or greater than 0.80. When the pretest probability is 0.20 to 0.80, sequential testing with enzyme-linked immunosorbent assay and Western blot is the most accurate method for ruling in or ruling out the possibility of Lyme disease.
Conclusions: Laboratory testing is recommended only in patients whose pretest probability of Lyme disease is 0.20 to 0.80. If the pretest probability is less than 0.20, testing will result in more false-positive results than true-positive results; a negative test result in this situation effectively rules out the disease.
This paper is also available at http://www.acponline.org.
Ann Intern Med. 1997;127:1109-1123.
From the University of Ottawa, Ottawa, Ontario, Canada; Centers for Disease Control and Prevention, Fort Collins, Colorado; New York Medical College, Valhalla, New York; New England Medical Center, Boston, Massachusetts; and McMaster University Medical Centre, Hamilton, Ontario, Canada. For current author addresses, see end of text.
1. Introduction
1.1 Lyme disease is the most common tick-borne disease in North America. From 1982 through 1994, more than 70 000 cases were reported in North America; most of these cases were in the United States (1). It is important that clinicians diagnose Lyme disease correctly because efficacious therapy is available and delayed or inadequate treatment can lead to many morbid sequelae. Lyme disease is a complex multisystem disease caused by the spirochete Borrelia burgdorferi (2). It affects persons of all
ages and both sexes. Since the disease was recognized in Connecticut in 1975 (3), endemic areas have been identified in several regions in North America. In more restricted areas in some northeastern and upper midwestern U.S. states, the disease has assumed the characteristics of an emerging epidemic (4-9). The true incidence is almost certainly underestimated because of under-reporting (10, 11).
1.2 Most patients develop a distinctive rash, erythema migrans, that is accompanied by such flu-like symptoms as fatigue, headache, mild stiff neck, joint and muscle aches, and fever (12). Some weeks or months after the initial exposure, symptoms and signs of disseminated disease (particularly neurologic, cardiac, or articular disease) may develop in untreated patients (13, 14).
1.3 Case definitions of Lyme disease have been developed in the United States for national disease surveillance purposes. A positive serologic test result was initially required for patients who had erythema migrans alone and had not been exposed to Lyme disease in endemic areas (15), but the 1990 criteria established in the Centers for Disease Control and Prevention's (CDC's) U.S. Lyme disease national surveillance definition reduced this requirement to a recommendation (Table 1) (16). These criteria were developed for an epidemiologic case definition intended for surveillance purposes only. However, previous national disease surveillance criteria have been used in clinical studies (17, 18), and such definitions do provide standardization. Standardization allows comparisons of clinical studies and permits the performance of meta-analysis to facilitate development of clinically useful guidelines.
1.4 Requests for laboratory testing for Lyme disease have increased rapidly. In Wisconsin, for example, it was reported that more than 60 000 tests were being done annually (19); in New Jersey, 5000 tests were done in 1 week in 1989 (20). According to market projections for the United States, 2.79 million rapid tests were to have been done for Lyme disease in 1995 (21). Testing is often done in persons who have only nonspecific signs and symptoms of illness, such as headache, fatigue, myalgia, or arthralgia. Even in highly endemic areas, the pretest probability of Lyme disease in such patients is less
© 1997 American College of Physicians 1109

than 0.20 (usually much lower). Thus, even when highly experienced laboratories are used, the probability of a false-positive test result is higher than that of a true-positive result. This problem is compounded by the lack of standardized serologic tests for Lyme disease. Comparisons of the test results from different laboratories have shown poor reliability and accuracy; up to 21% of standardized positive samples are missed, and up to 7% of samples from persons with no known exposure are incorrectly identified as positive (22).
1.5 This background paper provides a quantitative and qualitative evaluation of the predictive value of the laboratory diagnosis of Lyme disease. This evaluation forms the basis for guidelines on clinical diagnosis. Practitioners have been confused by the lack of consensus on diagnostic criteria for Lyme disease. The causes of this controversy arise from a combination of factors: the use of different tests in different laboratories, the use of different criteria to set positive and negative cutoff values for the same tests, different degrees of quality control in different laboratories, and differences in the community prevalence of Lyme disease.
1.6 We address each of these factors and make recommendations for the diagnostic workup of patients suspected of having Lyme disease.
2. Methods
2.1 Data Sources
Relevant articles from the medical literature were identified by searching the MEDLINE database for English-language articles or articles with English-language abstracts published from 1982 (when the spirochetal cause of Lyme disease was established [23, 24]) to 1996. The keywords used were
Lyme disease, Borrelia burgdorferi, diagnosis, ELISA, Western blot, immunofluorescence assay, polymerase chain reaction, urinary antigen detection, and culture. The computerized literature search was complemented by citations from authorities in the field.
2.2 Study Selection
All identified articles were reviewed by using a modification of the methodologic criteria for evaluating diagnostic tests developed by Irwig and colleagues (25). The included studies had to provide the following material: a clear statement on the test of interest, a description of the study characteristics that used a design that permitted the calculation of sensitivity and specificity, reproducible information on the sampling and clinical details of patients with the disease of interest and on controls (that is, data on the presence or absence of the criteria for Lyme disease described in the U.S. Lyme disease national surveillance case definition) (Table 1), and reproducible information on the reference standard (that is, cases diagnosed by experts who were blinded to the results of the diagnostic tests being evaluated). Because there are systematic differences in the strains of B. burgdorferi in different parts of the world, studies were excluded if they described results in patients outside of North America. When the same cohort of patients was described in more than one report, the results for individual patients were included only once.
2.3 Data Extraction
Sensitivity, specificity, and likelihood ratios were calculated by using established methods (26); a random-effects model was used to combine the proportions from the eligible studies (27).
Table 1 . Criteria for Confirmed Lyme Disease
Clinical description A systemic, tick-borne disease with protean manifestations, including dermatologic, rheumatologic, neurologic, and cardiac abnormalities. The best clinical marker for the disease is the initial skin lesion, erythema migrans, which occurs in 60% to 80% of patients
Clinical case definition Erythema migrans or at least one late manifestation, as defined below, and laboratory confirmation of infection Laboratory criteria for diagnosis 1) Isolation of Borrelia burgdorferi from clinical specimen or 2) demonstration of diagnostic levels of IgM and IgG
antibodies to the spirochete in serum or cerebrospinal fluid or 3) significant change in IgM or IgG antibody response to B. burgdorferi in paired acute- and convalescent-phase serum samples
Late manifestations Musculoskeletal system Recurrent, brief attacks (lasting weeks or months) of objective joint swelling in one or a few joints, sometimes
followed by chronic arthritis in one or a few joints. Manifestations not considered criteria for diagnosis include chronic progressive arthritis not preceded by brief attacks and chronic symmetrical polyarthritis. Arthralagia, myalgia, or fibromyalgia syndromes alone are not criteria for musculoskeletal involvement
Nervous system Any of the following, alone or in combination: lymphocytic meningitis; cranial neuritis, particularly facial palsy (may be
bilateral); radiculoneuropathy; or, rarely, encephalomyelitis. Encephalomyelitis must be confirmed by showing antibody production against B. burgdorferi in the cerebrospinal fluid, demonstrated by a higher titer of antibody in cerebrospinal fluid than in serum. Headache, fatigue, paraesthesia, or mild stiff neck alone are not criteria for neurologic involvement
Cardiovascular system Acute-onset, high-grade (2 or 3) atrioventricular conduction defects that resolve in days to weeks and are sometimes
associated with myocarditis. Palpitations, bradycardia, bundle-branch block, or myocarditis alone are not criteria for cardiovascular involvement.
1110 15 December 1997 • Annals of Internal Medicine • Volume 127 • Number 12
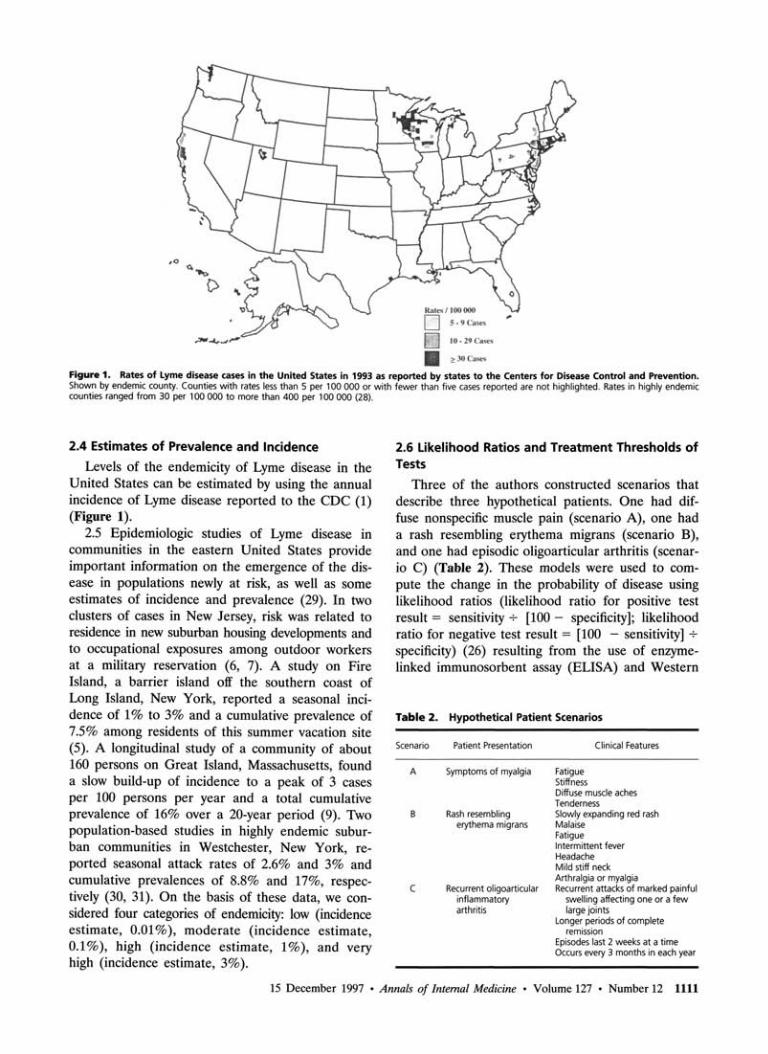
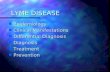
Figure 1. Rates of Lyme disease cases in the United States in 1993 as reported by states to the Centers for Disease Control and Prevention. Shown by endemic county. Counties with rates less than 5 per 100 000 or with fewer than five cases reported are not highlighted. Rates in highly endemic counties ranged from 30 per 100 000 to more than 400 per 100 000 (28).
2.4 Estimates of Prevalence and Incidence
Levels of the endemicity of Lyme disease in the United States can be estimated by using the annual incidence of Lyme disease reported to the CDC (1) (Figure 1).
2.5 Epidemiologic studies of Lyme disease in communities in the eastern United States provide important information on the emergence of the disease in populations newly at risk, as well as some estimates of incidence and prevalence (29). In two clusters of cases in New Jersey, risk was related to residence in new suburban housing developments and to occupational exposures among outdoor workers at a military reservation (6, 7). A study on Fire Island, a barrier island off the southern coast of Long Island, New York, reported a seasonal incidence of 1% to 3% and a cumulative prevalence of 7.5% among residents of this summer vacation site (5). A longitudinal study of a community of about 160 persons on Great Island, Massachusetts, found a slow build-up of incidence to a peak of 3 cases per 100 persons per year and a total cumulative prevalence of 16% over a 20-year period (9). Two population-based studies in highly endemic suburban communities in Westchester, New York, reported seasonal attack rates of 2.6% and 3% and cumulative prevalences of 8.8% and 17%, respectively (30, 31). On the basis of these data, we considered four categories of endemicity: low (incidence estimate, 0.01%), moderate (incidence estimate, 0.1%), high (incidence estimate, 1%), and very high (incidence estimate, 3%).
2.6 Likelihood Ratios and Treatment Thresholds of Tests
Three of the authors constructed scenarios that describe three hypothetical patients. One had diffuse nonspecific muscle pain (scenario A), one had a rash resembling erythema migrans (scenario B), and one had episodic oligoarticular arthritis (scenario C) (Table 2). These models were used to compute the change in the probability of disease using likelihood ratios (likelihood ratio for positive test result = sensitivity •*- [100 - specificity]; likelihood ratio for negative test result = [100 - sensitivity] -*• specificity) (26) resulting from the use of enzyme-linked immunosorbent assay (ELISA) and Western
Table 2. Hypothetical Patient Scenarios
Scenario Patient Presentation Clinical Features
A Symptoms of myalgia Fatigue Stiffness Diffuse muscle aches Tenderness
B Rash resembling Slowly expanding red rash erythema migrans Malaise
Fatigue Intermittent fever Headache Mild stiff neck Arthralgia or myalgia
C Recurrent oligoarticular Recurrent attacks of marked painful inflammatory swelling affecting one or a few arthritis large joints
Longer periods of complete remission
Episodes last 2 weeks at a time Occurs every 3 months in each year
15 December 1997 • Annals of Internal Medicine • Volume 127 • Number 12 1111

blotting. Decision analysis was used to assess the relative cost-effectiveness of the management options in these clinical situations when the clinician must decide whether to perform laboratory testing for Lyme disease (32). Incremental cost-effectiveness ratios were calculated as costs per quality-adjusted life-year for each scenario. This cost-effectiveness study is described in detail in a forthcoming paper (33).
3. Data Synthesis
3.1 Microbial Isolation
Cultural isolation of B. burgdorferi is the best diagnostic evidence of Lyme disease. Borrelia burgdorferi grows well in Barbour, Stoenner, Kelly (BSK) medium, but it is difficult to obtain isolates from clinical specimens other than biopsy samples from erythema migrans lesions.
3.2 Thirty-four papers were identified by the literature search. None met the criteria for formal analysis, but some case reports were worth noting. In the presence of erythema migrans, material has been collected from cutaneous lesions with various techniques, including direct aspiration of involved skin, aspiration after saline instillation, and skin biopsy. Wormser and colleagues (34) reported success rates of 29% with saline-lavage needle aspiration and 60% with 2-mm punch biopsies of the advancing edge of suspected primary erythema migrans lesions. Berger and colleagues (35) reported a success rate of more than 80% with biopsy specimens obtained from the leading edge of erythema migrans lesions.
3.3 Culture from sites other than the erythema migrans lesion is not usually successful. Borrelia burgdorferi has been recovered from a few specimens of patients' blood (24, 36, 37), cerebrospinal fluid (24), and joint fluid (38) and has been reported to be visible by silver staining of specimens obtained from cutaneous (39), myocardial (40), ret
inal (41), brain (42), and synovial (43) lesions. The specificity of these techniques is unknown because no studies used controls. In addition, no studies met the criteria for formal evaluation of the accuracy of culture or direct visualization techniques.
3.4 Serologic Testing with Enzyme-Linked Immunosorbent Assay and Western Blot
Enzyme-Linked Immunosorbent Assay We identified and reviewed 35 articles on this
topic (Appendix A). 3.5 Two large studies met the inclusion criteria:
Dressier and colleagues (44) described 155 patients with Lyme disease (57 cases of early disease and 98 cases of late disease) and 139 controls, and the CDC (45) studied 107 patients with Lyme disease (58 cases of early disease and 49 cases of late disease) and 113 controls. These studies allow the calculation of operating characteristics of ELISA when it is used in a dichotomous manner (that is, when the cut-off indicates a positive or negative result) or when three categories of results—negative, indeterminate, or positive—are used.
3.6 Dichotomous Test Results. According to Dressier and colleagues (44), the ELISA result should be classified as positive when the IgG optical density reading is at least 3 SDs above the mean reading for negative controls and at least 5 SDs above the mean IgM reading. The CDC used a positive cut-off at least 3 SDs above the mean of the values for negative controls when IgG and IgM values were combined. Table 3 shows the sensitivity, specificity, and likelihood ratios obtained by combining the data from these two studies.
3.7 Usefulness of ELISA in Different Clinical Situations. Scenario A (Table 2) describes a patient who seeks treatment for nonspecific symptoms that had lasted longer than 4 weeks, such as might occur in patients with fibromyalgia. In this scenario, the pretest probability that the patient is infected with B. burgdorferi is the same as the incidence of infection in the local population, and the results must be
Table 3. Sensitivity, Specificity, and Likelihood Ratios of Enzyme-Linked Immunosorbent Assay*
Variable Sensitivity Specificity Positive Likelihood Ratio
Negative Likelihood Ratio
0 /0
Early Lyme diseaset Study by Dressier et al. (44) (57 patients with Lyme disease; 139 controls) CDC study (45) (58 patients with Lyme disease; 113 controls) Random-effects combined estimate
Late Lyme disease* Study by Dressier et al. (44) (98 patients with Lyme disease; 139 controls) CDC study (45) (49 patients with Lyme disease; 113 controls) Random-effects combined estimate
40 78 59
89 100 95
94 89 93
72 89 81
8.42
5.01
0.44
0.06
* Indeterminate results were considered positive for these analyses. CDC = Centers for Disease Control and Prevention, t Serum samples were obtained from patients with erythema migrans. * Testing was done after the first weeks of infection.
1112 15 December 1997 • Annals of Internal Medicine • Volume 127 • Number 12
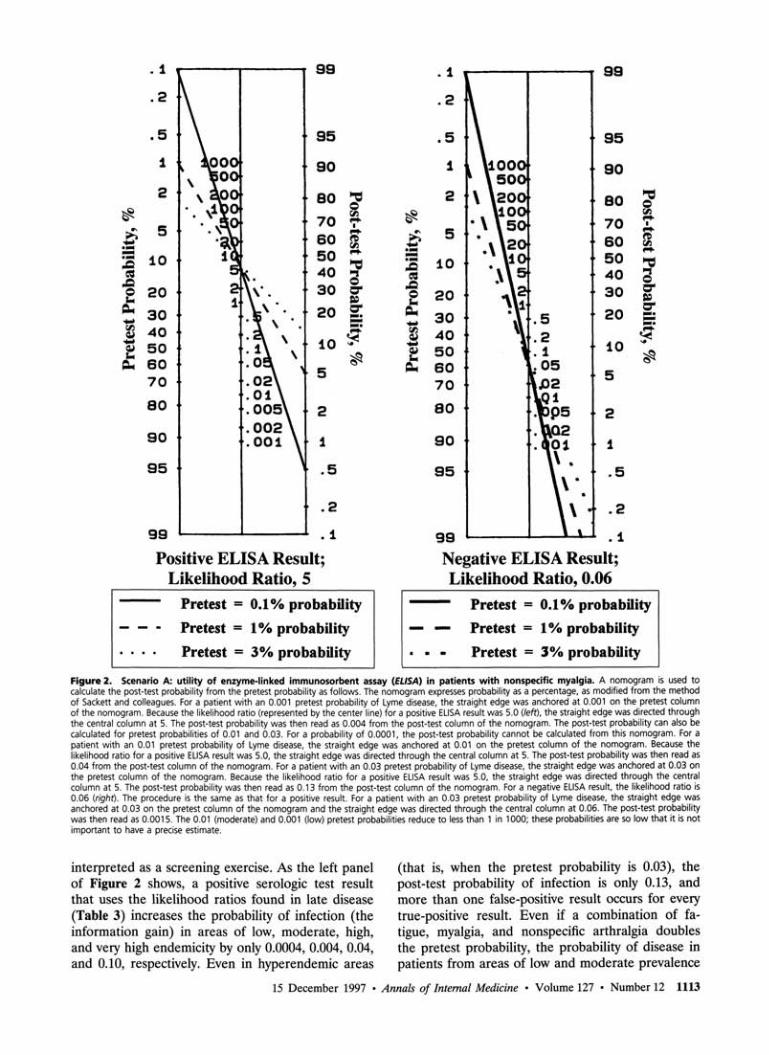
Figure 2. Scenario A: utility of enzyme-linked immunosorbent assay (ELISA) in patients with nonspecific myalgia. A nomogram is used to calculate the post-test probability from the pretest probability as follows. The nomogram expresses probability as a percentage, as modified from the method of Sackett and colleagues. For a patient with an 0.001 pretest probability of Lyme disease, the straight edge was anchored at 0.001 on the pretest column of the nomogram. Because the likelihood ratio (represented by the center line) for a positive ELISA result was 5.0 (left), the straight edge was directed through the central column at 5. The post-test probability was then read as 0.004 from the post-test column of the nomogram. The post-test probability can also be calculated for pretest probabilities of 0.01 and 0.03. For a probability of 0.0001, the post-test probability cannot be calculated from this nomogram. For a patient with an 0.01 pretest probability of Lyme disease, the straight edge was anchored at 0.01 on the pretest column of the nomogram. Because the likelihood ratio for a positive ELISA result was 5.0, the straight edge was directed through the central column at 5. The post-test probability was then read as 0.04 from the post-test column of the nomogram. For a patient with an 0.03 pretest probability of Lyme disease, the straight edge was anchored at 0.03 on the pretest column of the nomogram. Because the likelihood ratio for a positive ELISA result was 5.0, the straight edge was directed through the central column at 5. The post-test probability was then read as 0.13 from the post-test column of the nomogram. For a negative ELISA result, the likelihood ratio is 0.06 (right). The procedure is the same as that for a positive result. For a patient with an 0.03 pretest probability of Lyme disease, the straight edge was anchored at 0.03 on the pretest column of the nomogram and the straight edge was directed through the central column at 0.06. The post-test probability was then read as 0.0015. The 0.01 (moderate) and 0.001 (low) pretest probabilities reduce to less than 1 in 1000; these probabilities are so low that it is not important to have a precise estimate.
interpreted as a screening exercise. As the left panel of Figure 2 shows, a positive serologic test result that uses the likelihood ratios found in late disease (Table 3) increases the probability of infection (the information gain) in areas of low, moderate, high, and very high endemicity by only 0.0004, 0.004, 0.04, and 0.10, respectively. Even in hyperendemic areas
(that is, when the pretest probability is 0.03), the post-test probability of infection is only 0.13, and more than one false-positive result occurs for every true-positive result. Even if a combination of fatigue, myalgia, and nonspecific arthralgia doubles the pretest probability, the probability of disease in patients from areas of low and moderate prevalence
15 December 1997 • Annals of Internal Medicine • Volume 127 • Number 12 1113
who have a positive test result will still be less than 1%. Consequently, a positive test result in patients with a low prior probability of disease can safely be viewed as nondiagnostic. The same would be true for other situations in which pretest probability is very low, such as that of screening asymptomatic pregnant women; thus, testing would be inappropriate in these situations.
Although our key recommendation is not to routinely test such patients for the stated reasons, clinicians must frequently interpret negative test results in situations of low to moderate prevalence. As
Figure 3. Scenario B: utility of enzyme-linked immunosorbent assay (ELISA) in patients with possible erythema migrans. A nomogram is used to calculate the post-test probability from the pretest probability as follows. The nomogram expresses probability as a percentage, as modified from the method of Sackett and colleagues. For a patient with an 0.80 pretest probability of Lyme disease, the straight edge was anchored at 0.80 on the pretest column of the nomogram. Because the likelihood ratio (represented by the center line) for a positive ELISA result was 0.80, the straight edge was directed through the central column at 8. The post-test probability was then read as 0.98 from the post-test column of the nomogram. Conversely, because the likelihood ratio for a negative ELISA result was 0.44, the post-test probability was read as 0.63.
the right panel of Figure 2 shows, a negative test result in situations of low to moderate prevalence further reduces the probability of disease to less than 1 in 1000 and effectively rules out the disease.
Contrast this scenario with scenario B (Table 2), in which a patient with a rash that is not typical of erythema migrans. The panel estimated that the pretest probability with this clinical presentation was about 0.80. Figure 3 shows that although serologic testing has a relatively low sensitivity this early in the natural course of the disease (59% compared with 95% in late disease), the high, specificity of testing increases the probability of Lyme disease by 0.18 (from 0.80 to 0.98) (an example of SpIN—high Specificity resulting in the diagnosis being ruled IN [26]). However, the low sensitivity means that a negative ELISA result reduces the probability of true Lyme disease to only 0.63; thus, even with a negative test result, the patient is still more likely to have the disease (an example of SnOUT—high Sensitivity is needed to rule OUT the diagnosis [26]). In patients with symptoms of late disease, the sensitivity of the serologic tests improves; however, once again, the clinical history contributes more to the probability of Lyme disease than do the serologic results.
Contrast scenario A with scenario C (Table 2), in which a patient from an area of moderate endemic-ity (that is, an incidence of 0.1%) presents with no history of a tick bite, a vague history of a skin lesion that was not seen by a physician, and recurrent attacks of swelling in one knee. In this scenario, the panel estimated that the pretest probability was 0.50. As Figure 4 shows, a positive ELISA result increases the likelihood of disease to 80%, which is sufficiently high to justify antibiotic treatment. A negative test result is equally useful in this situation. For example, as shown in Figure 4, negative results on ELISA reduce the probability to 0.06, suggesting that another cause should be considered. The large change in the probability of disease with a negative test result demonstrates the SnOUT concept, namely, that the higher sensitivity of ELISA in late disease (0.95 compared with 0.59 in early disease) means that the high sensitivity is especially useful in ruling out the diagnosis (26).
3.8 Classification of ELISA Results into Three Levels. Grouping the results into multiple levels has been shown to improve the ability of many tests to differentiate disease from no disease (26). Dressier and colleagues (44) and the CDC (45) showed that the accuracy of diagnosis can be improved by classifying ELISA results as positive, indeterminate, or negative (Table 4). In Dressier and colleagues' study, an IgG titer of 1:800 or greater was defined as positive, IgG titers of 1:200 and 1:400 were defined as indeterminate, and IgG titers of 1:100 or
1114 15 December 1997 • Annals of Internal Medicine • Volume 127 • Number 12
less were defined as negative. An IgM titer of 1:200 or greater was defined as positive, an IgM titer of 1:100 was defined as indeterminate, and an IgM titer of less than 1:100 was defined as negative. The CDC uses an ELISA that measures combined IgG and IgM seroreactivity and has an indeterminate range of 1 to 3 SDs over the controls (45).
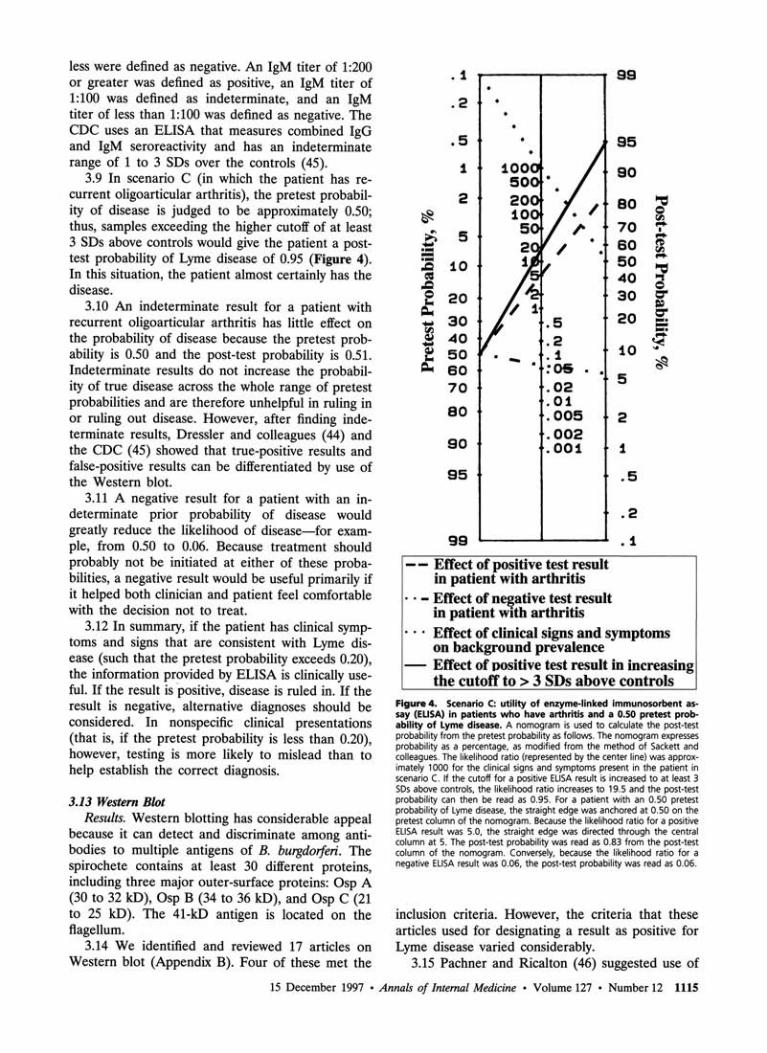
3.9 In scenario C (in which the patient has recurrent oligoarticular arthritis), the pretest probability of disease is judged to be approximately 0.50; thus, samples exceeding the higher cutoff of at least 3 SDs above controls would give the patient a post-test probability of Lyme disease of 0.95 (Figure 4). In this situation, the patient almost certainly has the disease.
3.10 An indeterminate result for a patient with recurrent oligoarticular arthritis has little effect on the probability of disease because the pretest probability is 0.50 and the post-test probability is 0.51. Indeterminate results do not increase the probability of true disease across the whole range of pretest probabilities and are therefore unhelpful in ruling in or ruling out disease. However, after finding indeterminate results, Dressier and colleagues (44) and the CDC (45) showed that true-positive results and false-positive results can be differentiated by use of the Western blot.
3.11 A negative result for a patient with an indeterminate prior probability of disease would greatly reduce the likelihood of disease—for example, from 0.50 to 0.06. Because treatment should probably not be initiated at either of these probabilities, a negative result would be useful primarily if it helped both clinician and patient feel comfortable with the decision not to treat.
3.12 In summary, if the patient has clinical symptoms and signs that are consistent with Lyme disease (such that the pretest probability exceeds 0.20), the information provided by ELISA is clinically useful. If the result is positive, disease is ruled in. If the result is negative, alternative diagnoses should be considered. In nonspecific clinical presentations (that is, if the pretest probability is less than 0.20), however, testing is more likely to mislead than to help establish the correct diagnosis.
3.13 Western Blot Results. Western blotting has considerable appeal
because it can detect and discriminate among antibodies to multiple antigens of B. burgdorferi. The spirochete contains at least 30 different proteins, including three major outer-surface proteins: Osp A (30 to 32 kD), Osp B (34 to 36 kD), and Osp C (21 to 25 kD). The 41-kD antigen is located on the flagellum.
3.14 We identified and reviewed 17 articles on Western blot (Appendix B). Four of these met the
Figure 4. Scenario C: utility of enzyme-linked immunosorbent assay (ELISA) in patients who have arthritis and a 0.50 pretest probability of Lyme disease. A nomogram is used to calculate the post-test probability from the pretest probability as follows. The nomogram expresses probability as a percentage, as modified from the method of Sackett and colleagues. The likelihood ratio (represented by the center line) was approximately 1000 for the clinical signs and symptoms present in the patient in scenario C. If the cutoff for a positive ELISA result is increased to at least 3 SDs above controls, the likelihood ratio increases to 19.5 and the post-test probability can then be read as 0.95. For a patient with an 0.50 pretest probability of Lyme disease, the straight edge was anchored at 0.50 on the pretest column of the nomogram. Because the likelihood ratio for a positive ELISA result was 5.0, the straight edge was directed through the central column at 5. The post-test probability was read as 0.83 from the post-test column of the nomogram. Conversely, because the likelihood ratio for a negative ELISA result was 0.06, the post-test probability was read as 0.06.
inclusion criteria. However, the criteria that these articles used for designating a result as positive for Lyme disease varied considerably.
3.15 Pachner and Ricalton (46) suggested use of
15 December 1997 • Annals of Internal Medicine • Volume 127 • Number 12 1115

Table 4. Additional Benefit of Western Blot for Indeterminate Enzyme-Linked Immunosorbent Assay Results*
Variable Study by Dressier et al. (44)t CDC Study (45)t Combined Study by Dressier et al. (44)t Likelihood
Case-Patients Controls Case-Patients Controls Ratio (n = 98)
< (n=139) (n = 49)
n
(n_ = 113)
>
ELISA alone Positive result 66 5 44 5 19.5 Indeterminate result 23 34 5 7 1.05 Negative result 9 100 0 101 0.06
ELISA and Western blot Positive ELISA result 66 5 44 5 19.5 Indeterminate ELISA result and positive Western blot result 17 2 5 1 11.7 Negative or indeterminate ELISA result and negative
Western blot result 15 132 0 107 0.08
* CDC = Centers for Disease Control and Prevention; ELISA = enzyme-linked immunosorbent assay, t Number in parentheses is reference number.
a quantitative gel densitometry assay (quantitative Western blot, or qWB) that compares bands of protein in serum samples of patients suspected of having Lyme disease to the density and width of the 41-kD band in a positive control serum sample. Fawcett and colleagues (47) proposed that to show positive serologic evidence of B. burgdorferi infection, an IgG Western blot must have four or more bands, of which one must correspond to the 41-kD antigen and one must correspond to a 60- to 69-kD antigen. Kowal and Weinstein (48) recommended that at least two bands of moderate to high intensity or at least five bands of lower intensity be present. Dressier and colleagues (44) proposed the following set of criteria: Two of the eight most common IgM bands must be present in early Lyme disease, and 5 of the 10 most common IgG bands must be present after the first 4 weeks of infection; the best discrimination was calculated by using receiver-operating characteristic curve (ROC) analyses on retrospective data and then prospectively testing these criteria on a new sample of patients.
3.16 Standardized Western blot criteria for Lyme disease, developed and presented at the recent Second National Conference on Serologic Diagnosis of Lyme Disease in Dearborn, Michigan (49), supersede previous recommendations and are closest to the approach taken by Dressier and colleagues (44).
3.17 Use of Western Blot for Indeterminate ELISA Results. Although no consistent evidence suggests that the Western blot adds additional information to the results of an ELISA or indirect immunofluorescence assay if used in all patients, Dressier and colleagues (44) and the CDC (45) suggest that a two-step testing strategy be used. This strategy consists of testing with ELISA and then using Western blot to test all cases whose ELISA results are indeterminate or positive. This is followed by treatment of patients with a positive Western blot result (47).
3.18 Consider again the patient described in scenario C, whose pretest probability was judged to be
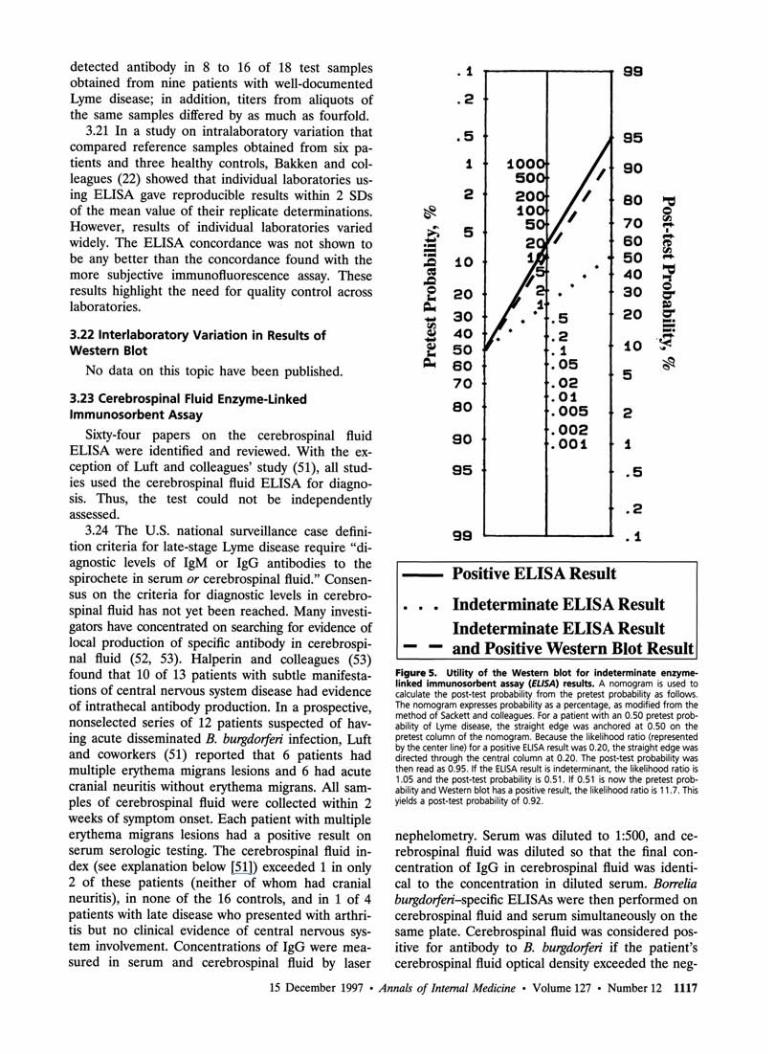
approximately 0.50. In the section on ELISA, we explained that a "positive" result was useful for ruling in disease and that a "negative" result was useful for ruling out disease. However, an indeterminate result is not helpful because the post-test probability (0.51) increased by only 0.01 from the pretest probability (0.50). Figure 5 shows what happens when the Western blot (using the criteria derived by Dressier and colleagues [44]) is used to test these indeterminate samples. A positive blot increases the probability of disease in these patients from 0.51 (the post-test probability after ELISA) to 0.92, a gain in information that would justify treatment.
3.19 Cost-Effectiveness of Enzyme-Linked Immunosorbent Assay and Western Blot
The cost-effectiveness analysis is detailed in a forthcoming paper (33). We considered four test-treatment strategies: 1) treatment of symptoms without testing or antibiotic therapy for Lyme disease, 2) testing with ELISA followed by treatment of patients with positive ELISA results, 3) two-step testing, and 4) antibiotic treatment of all patients suspected of having Lyme disease.
The analysis suggests that laboratory testing is not cost-effective for patients with low pretest probabilities (such as the patient with nonspecific myalgia in scenario A) or for patients with high pretest probabilities (such as the patient with possible erythema migrans in scenario B). In contrast, testing is economically attractive for patients in whom the pretest probability is 0.20 to 0.80 (as in scenario C), patients with oligoarticular arthritis, or patients with other possible late sequelae of Lyme disease.
3.20 Interlaboratory Variation in Results of Enzyme-Linked Immunosorbent Assay
Luger and Krauss (50) found high interlaboratory variability of serologic ELISA results among five laboratories in New Jersey. The five laboratories
1116 15 December 1997 • Annals of Internal Medicine • Volume 127 • Number 12
detected antibody in 8 to 16 of 18 test samples obtained from nine patients with well-documented Lyme disease; in addition, titers from aliquots of the same samples differed by as much as fourfold.
3.21 In a study on intralaboratory variation that compared reference samples obtained from six patients and three healthy controls, Bakken and colleagues (22) showed that individual laboratories using ELISA gave reproducible results within 2 SDs of the mean value of their replicate determinations. However, results of individual laboratories varied widely. The ELISA concordance was not shown to be any better than the concordance found with the more subjective immunofluorescence assay. These results highlight the need for quality control across laboratories.
3.22 Interlaboratory Variation in Results of Western Blot
No data on this topic have been published.
3.23 Cerebrospinal Fluid Enzyme-Linked Immunosorbent Assay
Sixty-four papers on the cerebrospinal fluid ELISA were identified and reviewed. With the exception of Luft and colleagues' study (51), all studies used the cerebrospinal fluid ELISA for diagnosis. Thus, the test could not be independently assessed.
3.24 The U.S. national surveillance case definition criteria for late-stage Lyme disease require "diagnostic levels of IgM or IgG antibodies to the spirochete in serum or cerebrospinal fluid." Consensus on the criteria for diagnostic levels in cerebrospinal fluid has not yet been reached. Many investigators have concentrated on searching for evidence of local production of specific antibody in cerebrospinal fluid (52, 53). Halperin and colleagues (53) found that 10 of 13 patients with subtle manifestations of central nervous system disease had evidence of intrathecal antibody production. In a prospective, nonselected series of 12 patients suspected of having acute disseminated B. burgdorferi infection, Luft and coworkers (51) reported that 6 patients had multiple erythema migrans lesions and 6 had acute cranial neuritis without erythema migrans. All samples of cerebrospinal fluid were collected within 2 weeks of symptom onset. Each patient with multiple erythema migrans lesions had a positive result on serum serologic testing. The cerebrospinal fluid index (see explanation below [51]) exceeded 1 in only 2 of these patients (neither of whom had cranial neuritis), in none of the 16 controls, and in 1 of 4 patients with late disease who presented with arthritis but no clinical evidence of central nervous system involvement. Concentrations of IgG were measured in serum and cerebrospinal fluid by laser
Figure 5. Utility of the Western blot for indeterminate enzyme-linked immunosorbent assay (ELISA) results. A nomogram is used to calculate the post-test probability from the pretest probability as follows. The nomogram expresses probability as a percentage, as modified from the method of Sackett and colleagues. For a patient with an 0.50 pretest probability of Lyme disease, the straight edge was anchored at 0.50 on the pretest column of the nomogram. Because the likelihood ratio (represented by the center line) for a positive ELISA result was 0.20, the straight edge was directed through the central column at 0.20. The post-test probability was then read as 0.95. If the ELISA result is indeterminant, the likelihood ratio is 1.05 and the post-test probability is 0.51. If 0.51 is now the pretest probability and Western blot has a positive result, the likelihood ratio is 11.7. This yields a post-test probability of 0.92.
nephelometry. Serum was diluted to 1:500, and cerebrospinal fluid was diluted so that the final concentration of IgG in cerebrospinal fluid was identical to the concentration in diluted serum. Borrelia burgdorferi-specific ELISAs were then performed on cerebrospinal fluid and serum simultaneously on the same plate. Cerebrospinal fluid was considered positive for antibody to B. burgdorferi if the patient's cerebrospinal fluid optical density exceeded the neg-
15 December 1997 • Annals of Internal Medicine • Volume 127 • Number 12 1117

ative serum cutoff; positivity was expressed as an antibody index (cerebrospinal fluid antibody index) that equals the ratio of the cerebrospinal fluid optical density to the negative serum cutoff. Intrathecal antibody production was considered present only when the antibody titer in cerebrospinal fluid exceeded the titer in serum (53). Steere and colleagues (54) found evidence of intrathecal antibody production in 12 of 13 patients with early meningitis and 5 of 12 patients with late central nervous system involvement. This study was a retrospective analysis of all patients who had been evaluated for early or late neurologic abnormalities of Lyme disease during the 10 years before the study and who had concomitant serum and cerebrospinal fluid samples available.
3.25 Although the inclusion criteria of many published series of neuroborreliosis (49) required the presence of positive results on serum serologic testing, few patients with Lyme disease have positive results on serologic testing of cerebrospinal fluid without positive results on serum serologic testing. Thus, the presence of antibodies in cerebrospinal fluid probably does not help in the basic diagnosis of Lyme disease. Determination of intrathecal antibody production may be useful in identifying meningeal involvement, although estimates of sensitivity and specificity await prospective series with adequate numbers.
3.26 Other Tests
Indirect Immunofluorescence Assay We identified and reviewed eight papers on in
direct immunofluorescence assay (Appendix C). Two papers met the inclusion criteria. The other studies did not provide sufficient evidence on the clinical definition of cases (that is, the application of reproducible clinical criteria without knowledge of laboratory results).
3.27 Two studies provided data on sensitivity and specificity based on appropriate clinical data (55, 56). These studies showed that sensitivity and specificity with indirect immunofluorescence assay are similar to those obtained with ELISA.
3.28 Interlaboratory variation studies, such as that by Bakken and colleagues (22), cannot be used to assess the sensitivity and specificity of the immunofluorescence assay because the patients were selected on the basis of the presence of immunofluorescence assay antibody titers. Similarly, the small sample size in Bakken and colleagues' study (six patients and three controls) precludes estimates of accuracy of the different laboratories in early compared with late disease. An interlaboratory variation study does not give sufficient information to allow cases of Lyme disease to be defined (20).
3.29 Several authors have noted that the immu
nofluorescence assay is more difficult to automate and that the readings are more subjective than those of ELISA (55, 56). Immunofluorescence assay results are difficult to interpret because variations in titer of ± 1 dilution factor are within the normal variability of the test.
3.30 Schwartz and colleagues (20) found moderate levels of agreement (K = 0.53) between the results of two laboratories in New Jersey that used the immunofluorescence assay. As mentioned earlier, Luger and Krauss (50) found a wide spectrum of sensitivity among four New Jersey laboratories that used the immunofluorescence assay. Hedberg and colleagues (57) studied the reproducibility in 17 specimens sent to four laboratories in Minnesota; the proportion of positive specimens ranged from 0% to 35%, and differences among three of the six interlaboratory comparisons of titers were significant (P < 0.05).
3.31 As described above, Bakken and coworkers (22) showed that the immunofluorescence assay and ELISA gave the same wide degree of interlaboratory variation in correctly identifying positive samples with immunofluorescence assay titers of 1:512 or greater (4% to 21%) and incorrectly identifying positive samples from healthy persons with no known exposure (2% to 7%). The authors ascribe this to use of different kits, cutoff schemes, antigen preparations, and control serum samples.
3.32 T-Cell Proliferative Assay for Partially Treated Patients
It has been suggested that the T-cell proliferative assay is useful for patients with Lyme disease whose diagnosis was based on the presence of erythema migrans and whose treatment is initially apparently successful but who then develop an attenuated picture of late Lyme disease, especially mild arthritic and neurologic signs and symptoms (58). Dattwyler and colleagues (59) reported an increased cellular response in 14 of 17 such patients. However, Zos-chke (60) found elevated B. burgdorferi-induced lymphoproliferative responses not only in 11 of 12 patients with Lyme disease but also in 8 of 12 healthy controls. In comparisons of inflammatory fluid (such as synovial fluid) with peripheral blood, T-cell proliferative responses have been found to be useful in confirming that B. burgdorferi is the cause of inflammation. Dressier and colleagues (58) found that the specificity was improved if the cutoff was increased to 3 SDs above the mean; using this cutoff reduces the sensitivity to 45% (19 of 42 cases) but increases the specificity to 95% (73 of 77 controls) if the stimulation index for a positive result is 10 or greater.
3.33 The operating characteristics of the T-cell proliferation assay need confirmation by other
1118 15 December 1997 • Annals of Internal Medicine • Volume 127 • Number 12
groups. Further comparisons with other tests, such as polymerase chain reaction (61), are needed before a recommendation can be made.
3.34 Polymerase Chain Reaction and Urinary Antigen Detection
Published experience with these techniques is insufficient to allow development of guidelines for their use. Polymerase chain reaction of joint fluid, cerebrospinal fluid, skin, and urine shows promise (53, 61-63). In a retrospective analysis of polymerase chain reaction of joint fluid, the sensitivity was 35% and the specificity was 100% (64). However, this test has not yet been evaluated in a consecutive series of patients with different clinical presentations that used appropriate controls.
4. Discussion
An accurate diagnosis is critical to making decisions about therapy, especially when therapy is expensive and not without risk. These guidelines for diagnosis are intended to help clinicians decide when to test and when to treat.
4.1 In patients who had an illness that met the 1990 American College of Rheumatology criteria for fibromyalgia (28), therapy for Lyme disease did not relieve fibromyalgia (17). Because such therapy can cost as much as $5000 for the standard 3- to 4-week course, the costs of the possible adverse effects of antibiotic use outweigh any benefit—even if up to 5% to 10% of untreated seropositive persons presenting with myalgia or fatigue develop neurologic symptoms or arthritis caused by Lyme disease (65).
4.2 The data reviewed in this paper confirm that ELISA or the immunofluorescence assay offers acceptable accuracy if the tests are standardized, have appropriate cut-offs, and are implemented with appropriate quality control that includes well-characterized reference samples. More important, however, the tests should be used only when the pretest probability of the clinical presentations is high enough (>0.20%) that the tests provide useful information. Such symptoms as arthralgia, myalgia, headache, fatigue, and palpitations alone are not sufficient to move the pretest likelihood into the range in which a positive test result will be clinically useful. This protects against the situations described in the section on ELISA (that is, laboratory tests being used in situations in which the pretest likelihood is too low for the laboratory tests to be clinically useful). Dressier and colleagues (44) and the CDC (45) showed that use of the Western blot is important for determining whether "indeterminate" results by ELISA are true positive. It is also critical
that laboratories testing for Lyme disease conform to a quality control standard and an improved proficiency program (as outlined in the U.S. Clinical Laboratory Improvement Act [CLIA]) (66). Serum samples used in proficiency testing should encompass the various stages and presentations of Lyme disease and should be representative of the target population. Each sample should be obtained from a single donor.
4.3 Although detection of clinically significant changes in antibody levels in paired acute-phase and convalescent-phase serum samples is cited as laboratory confirmation of Lyme disease in the U.S. national surveillance case definition and is of proven utility in other diseases, published data are not yet available on the clinical utility of this approach for Lyme disease.
4.4 Evaluating the usefulness of information on the sensitivity and specificity of diagnostic tests in clinical practice requires an understanding of the variables that should be considered in determining the pretest likelihood of disease. The clinician must appreciate that for diagnosing Lyme disease, the exposure history and clinical picture are critical in determining the predictive value of serologic test results.
4.5 For patients with low pretest probability of Lyme disease, such as those with nonspecific symptoms of myalgia, either no testing and no treatment or two-step testing avoids many unnecessary treatments compared with empirical treatment of all such patients (33). Conversely, positive test results in such patients do not increase the probability of Lyme disease enough to justify treatment. However, these patients should not receive empirical antibiotic therapy (antibiotic therapy without previous serologic testing). It is not generally recommended that ELISA be done in patients with a very low pretest probability; however, in cases in which such tests have been done, the test does lead to a greatly reduced probability of disease.
4.6 Rare manifestations of Lyme disease include myositis or neurophthalmology conditions. Because these features were not assessed in our analysis and data with which to evaluate test-treatment strategies in such patients are insufficient, two-step testing should be performed until additional studies are available.
4.7 The relation between the incidence and prevalence of Lyme disease in the community is unclear. Our analysis used the annual incidence in the community as the pretest probability of Lyme disease. Because acute illness with Lyme disease lasts about 3 months, our analysis overestimates the pretest probability of Lyme disease in such patients. Conversely, because the cumulative prevalence of Lyme disease is about three times the annual incidence,
15 December 1997 • Annals of Internal Medicine • Volume 127 • Number 12 1119
our analysis underestimates the pretest probability of Lyme disease in patients with possible late manifestations of disease. However, the results of our cost-effectiveness analysis did not change when reasonable values for community incidence were considered. Therefore, clinicians considering whether to test or treat should emphasize the presence or absence of features suggestive of Lyme disease rather than the community incidence of disease.
4.8 The pretest probability of Lyme disease depends on the presence or absence of clinical features suggestive of Lyme disease and on the incidence of disease in the community. For the purposes of this analysis, an expert panel simplified the range of pretest probabilities to low (0.01), medium (0.50), and high (0.80).
4.9 The CDC has adopted criteria recommending that ELISA-positive and ELISA-indeterminate samples be tested with Western blot (67). We choose not to adopt this recommendation until appropriately conducted studies have assessed its effectiveness. However, it is important that laboratories use stringent cut-off criteria for designating indeterminate and positive ELISA results. If patients are to be treated appropriately, the designation of samples as indeterminate must be rigorously defined.
Appendix A: Bibliography for Enzyme-Linked Immunosorbent Assay
Carlsson B, Hanson HS, Wasserman J, Brauner A. Evaluation of the fluorescent treponemal antibody-absorption (FTA-Abs) test specificity. Acta Derm Venereol. 1991;71: 306-11.
Christenson VD, White DH. Evaluation of four commercially available ELISA assays for the serologic diagnosis of Lyme disease. J Clin Lab Anal. 1991;5:340-3.
Coleman JL, Benach JL. Isolation of antigenic components from the Lyme disease spirochete: their role in early diagnosis. J Infect Dis. 1987;155:756-65.
Craft JE, Grodzicki RL, Shrestha M, Fischer DK, Gar-cia-Blanco M, Steere AC. The antibody response in Lyme disease. Yale J Biol Med. 1984;57:561-5.
Cutler SJ, Wright DJ. Evaluation of three commercial tests for Lyme disease. Diagn Microbiol Infect Dis. 1990; 13:271-2.
Dressier F, Yoshinari NH, Steere AC. The T-cell proliferative assay in the diagnosis of Lyme disease. Ann Intern Med. 1991;115:533-9.
Eiffert H, Lotter H, Thomssen R. Use of peroxidase-labelled antigen for the detection of antibodies to Borrelia burgdorferi in human and animal sera. Scand J Infect Dis. 1991;23:79-87.
Enders G, Biber M, Baier R, Hlobil H, Wellensiek HJ.
[Suspected syphilis during pregnancy due to cross reactions in Borrelia infection.] Dtsche Med Wochenschr. 1988;113:1511-4.
Fawcett PT, Gibney KM, Rose CD, Klein JD, Doughty RA. Adsorption with a soluble E. coli antigen fraction improves the specificity of ELISA tests for Lyme disease. J Rheumatol. 1991;18:705-8.
Fikrig E, Huguenel ED, Berland R, Rahn DW, Hardin JA, Flavell RA. Serologic diagnosis of Lyme disease using recombinant outer surface proteins A and B and flagellin. J Infect Dis. 1992;165:1127-32.
Guerrero A, Quereda C, Escudero R, Cobo J, Mor-cillo R, Marti-Belda P. [Serologic diagnosis of Lyme disease. A pending problem.] Enferm Infec Microbiol Clin. 1991;9:335-8.
Guy EC, Bateman DE, Martyn CN, Heckels JE, Law-ton NF. Lyme disease: prevalence and clinical importance of Borrelia burgdorferi specific IgG in forestry workers. Lancet. 1989;1:484-6.
Hansen K, Asbrink E. Serodiagnosis of erythema migrans and acrodermatitis chronica atrophicans by the Borrelia burgdorferi flagellum enzyme-linked immunosorbent assay. J Clin Microbiol. 1989;27:545-51.
Hansen K, Hindersson P, Pedersen NS. Measurement of antibodies to the Borrelia burgdorferi flagellum improves serodiagnosis in Lyme disease. J Clin Microbiol. 1988;26:338-46.
Hansen K, Pii K, Lebech AM. Improved immunoglobulin M serodiagnosis in Lyme borreliosis by using a mu-capture enzyme-linked immunosorbent assay with biotin-ylated Borrelia burgdorferi flagella. J Clin Microbiol. 1991; 29:166-73.
Heller J, Holzer G, Schimrigk K. Immunological differentiation between neuroborreliosis and multiple sclerosis. J Neurol. 1990;237:465-70.
Karlsson M. Aspects of the diagnosis of Lyme borreliosis. Scand J Infect Dis Suppl. 1990;67:1-59.
Karlsson M, Mollegard I, Stiernstedt G, Wretlind B. Comparison of Western blot and enzyme-linked immunosorbent assay for diagnosis of Lyme borreliosis. Eur J Clin Microbiol Infect Dis. 1989;8:871-7.
Kawabata M, Kubo N, Arashima Y, Yoshida M, Kawano K. [Serodiagnosis of Lyme disease by ELISA using Borrelia burgdorferi flagellum antigen.] Rinsho Byori. 1991;39:891-4.
Kruger H, Pulz M, Martin R, Sticht-Groh V. Long-term persistence of specific T- and B-lymphocyte responses to Borrelia burgdorferi following untreated neuroborreliosis. Infection. 1990;18:263-7.
Kujala GA, Steere AC, Davis JS 4th. IgM rheumatoid factor in Lyme disease: correlation with disease activity, total serum IgM, and IgM antibody to Borrelia burgdorferi. J Rheumatol. 1987;14:772-6.
Magnarelli LA. Laboratory diagnosis of Lyme disease. Rheum Dis Clin North Am. 1989;15:735-45.
1120 15 December 1997 • Annals of Internal Medicine • Volume 127 • Number 12
Magnarelli LA, Anderson JF. Adsorption and biotin-streptavidin amplification in serologic tests for diagnosis of Lyme borreliosis. J Clin Microbiol. 1991;29:1761-4.
Magnarelli LA, Anderson JF. Early detection and persistence of antibodies to Borrelia burgdorferi in persons with Lyme disease. Zentralbl Bakteriol Mikrobiol Hyg [A]. 1987;263:392-9.
Magnarelli LA, Anderson JF, Barbour AG. Enzyme-linked immunosorbent assays for Lyme disease: reactivity of subunits of Borrelia burgdorferi. J Infect Dis. 1989;159:43-9.
Magnarelli LA, Anderson JF, Johnson RC. Cross-reactivity in serological tests for Lyme disease and other spirochetal infections. J Infect Dis. 1987;156:183-8.
Mauch E, Vogel P, Kornhuber HH, Hahnel A. [Clinical value of antibody titers to Borrelia burgdorferi and titer course in neurologic disease pictures.] Nervenarzt. 1990;61:98-104.
Rose CD, Fawcett PT, Singsen BH, Dubbs SB, Doughty RA. Use of western blot and enzyme-linked immunosorbent assays to assist in the diagnosis of Lyme disease. Pediatrics. 1991;88:465-70.
Ross AH, Benach JL. The significance of controls in Lyme arthritis of children. Zentralbl Bakteriol Mikrobiol Hyg [A]. 1987;263:400-6.
Smith JL, Crumpton BC, Hummer J. The Bascom Palmer Eye Institute Lyme/syphilis survey. J Clin Neuro-ophthalmol. 1990;10:255-60.
Smith JL. Neuro-ocular Lyme borreliosis. Neurol Clin. 1991;9:35-53.
Stanek G. Laboratory diagnosis and seroepidemiology of Lyme borreliosis. Infection. 1991;19:263-7.
Stiernstedt G, Granstrom M. Borrelia arthritis in Sweden. Zentralbl Bakteriol Mikrobiol Hyg [A]. 1986;263:285-7.
Suchanek G, Kristoferitsch W, Stanek G, Bernheimer H. Anti-myelin antibodies in cerebrospinal fluid and serum of patients with meningopolyneuritis Garin-Bujadoux-Bannwarth and other neurological diseases. Zentralbl Bakteriol Mikrobiol Hyg [A]. 1986;263:160-8.
Wilkinson HW. Immunodiagnostic tests for Lyme disease. Yale J Biol Med. 1984;57:567-72.
Appendix B: Bibliography for Western Blot
Carlsson B, Hanson HS, Wasserman J, Brauner A. Evaluation of the fluorescent treponemal antibody-absorption (FTA-Abs) test specificity. Acta Derm Venereol. 1991;71: 306-11.
Cimmino MA, Accardo S, Sambri V. Western blotting for the diagnosis of Borrelia burgdorferi infection in patients with sacroiliitis [Letter]. J Rheumatol. 1992;19:833-4.
Corpuz M, Hilton E, Lardis MP, Singer C, Zolan J. Problems in the use of serologic tests for the diagnosis of Lyme disease. Arch Intern Med. 1991;151:1837-40.
Dattwyler RJ, Volkman DJ, Luft BJ, Halperin JJ, Thomas J, Golightly MG. Seronegative Lyme disease. Dissociation of specific T- and B-lymphocyte responses to Borrelia burgdorferi. N Engl J Med. 1988;319:1441-6.
Dressier F, Whalen JA, Reinhardt BN, Steere AC. Western blotting in the serodiagnosis of Lyme disease. J Infect Dis. 1993;167:392-400.
Fister RD, Weymouth LA, McLaughlin JC, Ryan RW, Tilton RC. Comparative evaluation of three products for the detection of Borrelia burgdorferi antibody in human serum. J Clin Microbiol. 1989;27:2834-7.
Grellner W, Erbguth F, Brade V. [Serodiagnosis of Lyme borreliosis: antibody titer and specificity in the IFT and western blot.] Immun Infekt. 1989;17:189-94.
Guy EC, Bateman DE, Martyn CN, Heckels JE, Law-ton NF. Lyme disease: prevalence and clinical importance of Borrelia burgdorferi specific IgG in forestry workers. Lancet. 1989;1:484-6.
Karlsson M. Aspects of the diagnosis of Lyme borreliosis. Scand J Infect Dis Suppl. 1990;67:1-59.
Karlsson M, Mollegard I, Stiernstedt G, Wretlind B. Comparison of Western blot and enzyme-linked immunosorbent assay for diagnosis of Lyme borreliosis. Eur J Clin Microbiol Infect Dis. 1989;8:871-7.
Kowal K, Weinstein A. Western blot band intensity analysis. Application to the diagnosis of Lyme arthritis. Arthritis Rheum. 1994;37:1206-11.
Kruger H, Pulz M, Martin R, Sticht-Groh V. Long-term persistence of specific T- and B-lymphocyte responses to Borrelia burgdorferi following untreated neu-roborreliosis. Infection. 1990;18:263-7.
Ma B, Christen B, Leung D, Vigo-Pelfrey C. Serodiagnosis of Lyme borreliosis by western immunoblot: reactivity of various significant antibodies against Borrelia burgdorferi. J Clin Microbiol. 1992;30:370-6.
Pachner A, Ricalton NS. Western blotting in evaluating Lyme seropositivity and the utility of a gel densiomet-ric approach. Neurology. 1992;42:2185-92.
Rose CD, Fawcett PT, Singsen BH, Dubbs SB, Doughty RA. Use of western blot and enzyme-linked immunosorbent assays to assist in the diagnosis of Lyme disease. Pediatrics. 1991;88:465-70.
Smith JL. Neuro-ocular Lyme borreliosis. Neurol Clin. 1991;9:35-53.
Stanek G. Laboratory diagnosis and seroepidemiology of Lyme borreliosis. Infection. 1991;19:263-7.
Appendix C: Bibliography for Immunofluorescence Assay
Cutler SJ, Wright DJ. Evaluation of three commercial tests for Lyme disease. Diagn Microbiol Infect Dis. 1990; 13:271-2.
15 December 1997 • Annals of Internal Medicine • Volume 127 • Number 12 1121
Lane RS, Lennette ET, Madigan JE. Interlaboratory and intralaboratory comparisons of indirect immunofluorescence assays for serodiagnosis of Lyme disease. J Clin Microbiol. 1990;28:1774-9.
Magnarelli LA, Anderson JF. Early detection and persistence of antibodies to Borrelia burgdorferi in persons with Lyme disease. Zentralbl Bakteriol Mikrobiol Hyg [A]. 1987;263:392-9.
Magnarelli LA, Anderson JF, Johnson RC. Cross-reactivity in serological tests for Lyme disease and other spirochetal infections. J Infect Dis. 1987;156:183-8.
Ross AH, Benach JL. The significance of controls in Lyme arthritis of children. Zentralbl Bakteriol Mikrobiol Hyg [A]. 1987;263:400-6.
Smith JL. Neuro-ocular Lyme borreliosis. Neurol Clin. 1991;9:35-53.
Smith JL, Crumpton BC, Hummer J. The Bascom Palmer Eye Institute Lyme/syphilis survey. J Clin Neuro-ophthalmol. 1990;10:255-60.
Wilkinson HW. Immunodiagnostic tests for Lyme disease. Yale J Biol Med. 1984;57:567-72.
Acknowledgment: The authors thank Diane Gagnon for support in preparing this manuscript.
Requests for Reprints: Peter Tugwell, MD, Department of Medicine, Ottawa General Hospital, 501 Smyth Road, Ottawa, Ontario K1H 8L6, Canada.
Current Author Addresses: Dr. Tugwell: Department of Medicine, University of Ottawa and Ottawa General Hospital, 501 Smyth Road, Ottawa, Ontario K1H 8L6, Canada. Dr. Dennis: Centers for Disease Control and Prevention, PO Box 2087, Fort Collins, CO 80521. Dr. Weinstein: Division of Rheumatic Diseases and Immunology, New York Medical College, Munger Pavilion, Valhalla, NY 10595. Drs. Wells and Nichol and Ms. Shea: Clinical Epidemiology Unit, Ottawa Civic Hospital, 1053 Carling Avenue, Ottawa, Ontario K1Y 4E9, Canada. Dr. Hayward: Department of Clinical Epidemiology and Biosta-tistics, McMaster University Medical Centre, 1200 Main Street, Hamilton, Ontario L8N 3Z5, Canada. Dr. Lightfoot: Division of Rheumatology, University of Kentucky, Kentucky Clinic J511, Lexington, KY 40536-0284. Mr. Baker: Menzies School of Health Research, University of Sydney, PO Box 41096, Casuarina NT 0811, Australia. Dr. Steere: Rheumatology/Immunology, New England Medical Center #406, 750 Washington Street, Boston, MA 02111.
References
1. Lyme disease—United States, 1994. MMWR Morb Mortal Wkly Rep. 1995; 44:459-62.
2. Malawista SE, Steere AC. Lyme disease: infectious in origin, rheumatic in expression. Adv Intern Med. 1986;31:147-66.
3. Steere AC, Malawista SE, Snydman DR, Shope RE, Andiman WA, Ross MR, et al. Lyme arthritis: an epidemic of oligoarticular arthritis in children and adults in three Connecticut communities. Arthritis Rheum. 1977;20:7-17.
4. Dennis DT. Epidemiology. In: Coyle PK, ed. Lyme Disease. St. Louis: Mosby-Year Book; 1993:27-37.
5. Hanrahan JP, Benach JL, Coleman JL, Bosler EM, Morse DL, Cameron DJ, et al. Incidence and cumulative frequency of Lyme disease in a community. J Infect Dis. 1984;150:489-96.
6. Bowen GS, Schulze TL, Hayne C, Parkin WE. A focus of Lyme disease in Monmouth County, New Jersey. Am J Epidemiol. 1984;120:387-94.
7. Schulze TL, Shisler JK, Bosler EM, Lakat MF, Parkin WE. Evolution of a focus of Lyme disease. Zentralblatt Bakteriol Mikrobiol Hyg [A]. 1986;263:65-71.
8. Lastavica CC, Wilson ML, Berardi VP, Spielman A, Deblinger RD. Rapid emergence of a focal epidemic of Lyme disease in coastal Massachusetts. N Engl J Med. 1989;320:133-7.
9. Steere AC, Taylor E, Wilson ML, Levine JF, Spielman A. Longitudinal assessment of the clinical and epidemiological features of Lyme disease in a defined population. J Infect Dis. 1986;154:295-300.
10. Weinstein A, Bujak Dl. Lyme disease: a review of its clinical features. N Y State J Med. 1989;89:566-71.
11. Coyle BS, Strickland GT, Liang YY, Pena C, McCarter R, Israel E. The public health impact of lyme disease in Maryland. J Infect Dis. 1996; 173: 1260-2.
12. Steere AC, Malawista SE, Hardin JA, Ruddy S, Askenase PW, Andiman WA. Erythema chronicum migrans and Lyme arthritis. The enlarging clinical spectrum. Ann Intern Med. 1977;86:685-98.
13. Pachner AR, Steere AC. The triad of neurologic manifestations of Lyme disease: meningitis, cranial neuritis, and radiculoneuritis. Neurology. 1985;35: 47-53.
14. Steere AC. Lyme disease. N Engl J Med. 1989;321:586-96. 15. Ciesielski CA, Markowitz LE, Horsley R, Hightower AW, Russell H,
Broome CV. The geographic distribution of lyme disease in the United States. Ann N Y Acad Sci. 1988;539:283-8.
16. Wharton M, Chorba TL, Vogt RL, Morse DL, Buehler JW. Case definitions for public health surveillance. MMWR Morb Mortal Wkly Rep. 1990; 39(RR-13):1-43.
17. Dinerman H, Steere AC. Lyme disease associated with fibromyalgia. Ann Intern Med. 1992;117:281-5.
18. Wormser GP, Forseter G, Cooper D, Nowakowski J, Nadelman RB, Horowitz H, et al. Use of a novel technique of cutaneous lavage for diagnosis of Lyme disease associated with erythema migrans. JAMA. 1992;268: 1311-3.
19. Jones JM. Serodiagnosis of Lyme disease [Letter]. Ann Intern Med. 1991 ;114: 1064.
20. Schwartz BS, Goldstein MD, Ribeiro JM, Schulze TL, Shahied SI. Antibody testing in Lyme disease. A comparison of results in four laboratories. JAMA. 1989;262:3431-4.
21 . Lyme disease—United States, 1995. MMWR Morb Mortal Wkly Rep. 1996; 45:481-4.
22. Bakken LL, Case KL, Callister SM, Bourdeau NJ, Schell RF. Performance of 45 laboratories participating in a proficiency testing program for Lyme disease serology. JAMA. 1992;268:891-5.
23. Burgdorfer W, Barbour AG, Hayes SF, Benach JL, Grunwaldt E, Davis JP. Lyme disease—a tick-borne spirochetosis? Science. 1982;216:1317-9.
24. Steere AC, Grodzicki RL, Kornblatt AN, Craft JE, Barbour AG, Burgdorfer W, et al. The spirochaetal etiology of Lyme disease. N Engl J Med. 1983;308:733-40.
25. Irwig L, Tosteson AN, Gatsonis C, Lau J, Colditz G, Chalmers T, et al. Guidelines for meta-analyses evaluating diagnostic tests. Ann Intern Med. 1994;120:667-76.
26. Sackett DL, Haynes RB, Guyatt GH, et al. Clinical Epidemiology: A Basic Science for Clinical Medicine. 2d ed. Boston: Little, Brown; 1991.
27. Hedges LV, Olkin I. Statistical Methods for Meta-Analysis. Orlando, FL: Academic Pr; 1985.
28. Wolfe F, Smythe HA, Yunus MB, Bennett RM, Bombardier C, Golden-berg DL, et al. The American College of Rheumatology 1990 Criteria for the Classification of Fibromyalgia. Report of the Multicenter Criteria Committee. Arthritis Rheum. 1990;33:160-72.
29. Dennis DT. Lyme disease. Tracking an epidemic [Editorial]. JAMA. 1991;266: 1269-70.
30. Alpert B, Esin J, Sivak SL, Wormser GP. Incidence and prevalence of Lyme disease in a suburban Westchester County community. N Y State J Med. 1992;92:5-8.
31. Miller GL, Bailey RE, Morse DL. 1990 prevalence and incidence of Lyme disease in two New York communities [Abstract]. Proceedings of V International Conference on Lyme Disease. Arlington, VA; 1992.
32. Sox HC, Blatt MA, Higgens MC, et al. Medical Decision Making. Toronto: Butterworths; 1997.
33. Nichol G, Dennis DT, Steere AC, Lightfoot R, Wells G, Shea B, et al. Test-treatment strategies for patients suspected of having Lyme disease. A cost-effectiveness analysis. Ann Intern Med. [In press].
34. Wormser GP, Forseter G, Cooper D, Nowakowski J, Nadelman RB, Horowitz H, et al. Use of a novel technique of cutaneous lavage for diagnosis of Lyme disease associated with erythema migrans. JAMA. 1992;268: 1311-3.
35. Berger BW, Johnson RC, Kodner C, Coleman L. Cultivation of Borrelia burgdorferi from erythema migrans lesions and perilesional skin. J Clin Microbiol. 1992;30:359-61.
36. Benach JL, Bosler EM, Hanrahan JP, Coleman JL, Habicht GS, Bast TF, et al. Spirochetes isolated from the blood of two patients with Lyme disease. N Engl J Med. 1983;308:740-2.
37. Nadelman RB, Pavia CS, Magnarelli LA, Wormser GP. Isolation of Borrelia burgdorferi from blood of seven patients with Lyme disease. Am J Med. 1990;88:21-6.
38. Snydman DR, Schenkein DP, Berardi VP, Lastavica CC, Pariser KM. Borrelia burgdorferi in joint fluid in chronic Lyme arthritis. Ann Intern Med. 1986;104:798-800.
1122 15 December 1997 • Annals of Internal Medicine • Volume 127 • Number 12

39. Berger BW, Clemmensen OJ, Ackerman AB. Lyme disease is a spirochetosis. A review of the disease and evidence for its cause. Am J Dermatopathol. 1983;5:111-24.
40. Marcus LC, Steere AC, Duray PH, Anderson AE, Mahoney EB. Fatal pancarditis in a patient with coexistent Lyme disease and babesiosis. Demonstration of spirochetes in the myocardium. Ann Intern Med. 1985;103:374-6.
41. Kramer N, Rickert RR, Brodkin RH, Rosenstein ED. Septal panniculitis as a manifestation of Lyme disease. Am J Med. 1986;81:149-52.
42. Pachner AR, Duray P, Steere AC. Central nervous system manifestations of Lyme disease. Arch Neurol. 1989;46:790-5.
43. Johnston YE, Duray PH, Steere AC, Kashgarian M, Buza J, Malawista SE, et al. Lyme arthritis. Spirochetes found in synovial microangiopathic lesions. Am J Pathol. 1985;118:26-34.
44. Dressier F, Whalen JA, Reinhardt BN, Steere AC. Western blotting in the serodiagnosis of Lyme disease. J Infect Dis. 1993;167:392-400.
45. Johnson BJ, Robbins KE, Bailey RE, Cao BL, Sviat SL, Craven RB, et al. Serodiagnosis of Lyme disease: accuracy of a two-step approach using a flagella-based ELISA and immunoblotting. J Infect Dis. 1996;174:346-53.
46. Pachner A, Ricalton NS. Western blotting in evaluating Lyme seropositivity and the utility of a gel densiometric approach. Neurology. 1992;42:2185-92.
47. Fawcett PT, Gibney KM, Rose CD, Doughty RA. Frequency and specificity of antibodies that crossreact with Borrelia burgdorferi antigens. J Rheumatol. 1992;19:582-7.
48. Kowal K, Weinstein A. Western blot band intensity analysis. Application to the diagnosis of Lyme arthritis. Arthritis Rheum. 1994;37:1206-11.
49. Recommendations for test performance and interpretation from the Second National Conference on Serologic Diagnosis of Lyme Disease. MMWR Morb Mortal Wkly Rep. 1995;44:590-1.
50. Luger SW, Krauss E. Serologic tests for Lyme disease. Interlaboratory variability. Arch Intern Med. 1990;150:761-3.
51. Luft BJ, Steinman CR, Neimark HC, Muralidhar B, Rush T, Finkel MF, et al. Invasion of the central nervous system by Borrelia burgdorferi in acute disseminated infection. JAMA. 1992;267:1364-7.
52. Hansen K, Hindersson P, Pedersen NS. Measurement of antibodies to the Borrelia burgdorferi flagellum improves serodiagnosis in Lyme disease. J Clin Microbiol. 1988;26:338-46.
53. Halperin JJ, Volkman DJ, Wu P. Central nervous system abnormalities in Lyme neuroborreliosis. Neurology. 1991;41:1571-82.
54. Steere AC, Berardi VP, Weeks KE, Logigian EL, Ackermann R. Evaluation of the intrathecal antibody response to Borrelia burgdorferi as a diagnostic test for Lyme neuroborreliosis. J Infect Dis. 1990;161:1203-9.
55. Russell H, Sampson JS, Schmid GP» Wilkinson HW, Plikaytis B. Enzyme-linked immunosorbent assay and indirect immunofluorescence assay for Lyme disease. J Infect Dis. 1984;149:465-70.
56. Magnarelli LA, Meegan JM, Anderson JF, Chappell WA. Comparison of an indirect fluorescent-antibody test with an enzyme-linked immunosorbent assay for serological studies of Lyme disease. J Clin Microbiol. 1984;20:181-4.
57. Hedberg CW, Osterholm MT, MacDonald KL, White KE. An interlaboratory study of antibody to Borrelia burgdorferi. J Infect Dis. 1987;155:1325-7.
58. Dressier F, Yoshinari NH, Steere AC. The T-cell proliferative assay in the diagnosis of Lyme disease. Ann Intern Med. 1991;115:533-9.
59. Dattwyler RJ, Volkman DJ, Luft BJ, Halperin JJ, Thomas J, Golightly MG. Seronegative Lyme disease. Dissociation of specific T- and B-lymphocyte responses to Borrelia burgdorferi. N Engl J Med. 1988;319:1441-6.
60. Zoschke DC. Is it Lyme disease? How to interpret results of laboratory testing. Postgrad Med. 1992;91:46-8.
61. Keller TL, Halperin JJ, Whitman M. PCR detection of Borrelia burgdorferi DNA in cerebrospinal fluid of Lyme neuroborreliosis patients. Neurology. 1992;42:32-42.
62. Melchers W, Meis J, Rosa P, Claas E, Nohlmans L, Koopman R, et al. Amplification of Borrelia burgdorferi DNA in skin biopsies from patients with Lyme disease. J Clin Microbiol. 1991;29:2401-6.
63. Goodman JL, Jurkovich P, Kramber JM, Johnson RC. Molecular detection of persistent Borrelia burgdorferi in the urine of patients with active Lyme disease. Infect Immun. 1991;59:269-78.
64. Nocton JJ, Dressier F, Rutledge BJ, Rys PN, Persing DH, Steere AC. Detection of Borrelia burgdorferi DNA by polymerase chain reaction in synovial fluid from patients with Lyme arthritis. N Engl J Med. 1994;330:229-34.
65. Lightfoot RW Jr, Luft BJ, Rahn DW, Steere AC, Sigal LH, Zoschke DC, et al. Empiric parenteral antibiotic treatment of patients with fibromyalgia and fatigue and a positive serologic result for Lyme disease. A cost-effectiveness analysis. Ann Intern Med. 1993;119:503-9.
66. Federal Register. 28 February 1992; vol. 57, no. 40. 67. Lyme disease—United States, 1993. MMWR Morb Mortal Wkly Rep. 1994;
43:564-71.
15 December 1997 • Annals of Internal Medicine • Volume 127 • Number 12 1123
Related Documents