LABORATORY AUDIT OF BENIGN OROFACIAL TUMOURS AT UNIVERSITY OF NAIROBI DENTAL HOSPITAL OVER A FIVE YEAR PERIOD, (2008-2012). INVESTIGATOR: KHANBHAI FATEMA JUZER V28/35908/2010 BDS LEVEL III A community dentistry research project report submitted in partial fulfillment of requirements for the award of the degree of Bachelor of Bachelor of Dental Surgery(BDS) at the University of Nairobi. 2013

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

LABORATORY AUDIT OF BENIGN OROFACIAL TUMOURS AT UNIVERSITY OF
NAIROBI DENTAL HOSPITAL OVER A FIVE YEAR PERIOD, (2008-2012).
INVESTIGATOR:
KHANBHAI FATEMA JUZER
V28/35908/2010
BDS LEVEL III
A community dentistry research project report submitted in partial fulfillment of
requirements for the award of the degree of Bachelor of Bachelor of Dental
Surgery(BDS) at the University of Nairobi.
2013
ii
DECLARATION
I, Fatema Khanbhai, declare that this research proposal is my own original work and has never
been submitted for any other degree or examination at this or any other University.
Signature…………………………………… Date………………………………
iii
APPROVAL
This project report has been submitted for examination with our approval as University of
Nairobi supervisors:
SUPERVISORS
PROF.FRANCIS G.MACIGO, BDS, MPH, PGD-STI (UON)
PUBLIC HEALTH SPECIALIST AND ASSOCIATE PROFESSOR OF COMMUNITY AND
PREVENTIVE DENTISTRY, DEPARTMENT OF PERIODONTOLOGY/ COMMUNITY
AND PREVENTIVE DENTISTRY, SCHOOL OF DENTAL SCIENCES, COLLEGE OF
HEALTH SCIENCES, UNIVERSITY OF NAIROBI.
Signature ……………………………….. Date ……………………
DR.ELIZABETH DIMBA (BDS –NBI, PHD-NORWAY)
SENIOR LECTURER,
DEPARTMENT OF ORAL AND MAXILLOFACIAL SURGERY ORAL PATHOLOGY AND
ORAL MEDICINE, SCHOOL OF DENTAL SCIENCES, COLLEGE OF HEALTH
SCIENCES,
UNIVERSITY OF NAIROBI
Signature ……………………………….. Date ……………………..

iv
DEDICATION
I dedicate this research to my grandparents, they will always be missed, my parents and my
brother for always giving me the support and strength to work hard.

v
ACKNOWLEDGEMENTS:
I wish to thank my supervisors Prof.Francis Macigo and Dr. Dimba for their assistance,
insightful comments and creating time for review meetings in the process of the completion of
this project.
Special thanks to Desmond for helping me during data analysis. To my dad Mr. Juzer Khanbhai,
mum Mrs. Naqiya. Juzer and brother Hussein Khanbhai, you have always been there for me.
Thank you.

vi
TABLE OF CONTENTS
Contents
DECLARATION ........................................................................................................................................................ ii
APPROVAL ............................................................................................................................................................ iii
DEDICATION ......................................................................................................................................................... iv
ACKNOWLEDGEMENTS: ......................................................................................................................................... v
TABLE OF CONTENTS ............................................................................................................................................. vi
LIST OF FIGURES .................................................................................................................................................. viii
LIST OF TABLES ................................................................................................................................................... viii
ABBREVIATIONS ................................................................................................................................................... ix
ABSTRACT .............................................................................................................................................................. 1
CHAPTER1: INTRODUCTION ................................................................................................................................... 3
CHAPTER 2: LITERATURE REVIEW ........................................................................................................................... 4
2.1: HISTOLOGICAL CLASSIFICATION OF BENIGN TUMOURS ............................................................. 4
2.2: ETIOLOGY AND EPIDEMIOLOGY .......................................................................................................... 7
2.3: MANAGEMENT AND TREATMENT MODALITIES; ............................................................................. 7
CHAPTER 3: STATEMENT OF THE PROBLEM, JUSTIFICATION AND OBJECTIVES....................................................... 9
3.1: Statement of the problem: ............................................................................................................................. 9
3.2: Study justification: ........................................................................................................................................ 9
3.3: Objectives: ..................................................................................................................................................... 9
3.3.1: General: ....................................................................................................................................................... 9
3.3.2: Specific: ........................................................................................................................................................ 9
3.4: Variables: ...................................................................................................................................................... 9
CHAPTER 4: STUDY METHODOLOGY .................................................................................................................... 11
vii
4.1: Study area: .................................................................................................................................................... 11
4.2: Study population: ........................................................................................................................................ 11
4.3: Study design: ............................................................................................................................................... 11
4.4: Sample size determination: ......................................................................................................................... 11
4.5: Sampling: ..................................................................................................................................................... 11
4.6: Inclusion and exclusion criteria: .................................................................................................................... 11
4.6.1: Inclusion criteria: ....................................................................................................................................... 11
4.6.2: Exclusion criteria: ....................................................................................................................................... 11
4.7: Data collection instruments and technique: ................................................................................................ 12
4.8: Problems anticipated ................................................................................................................................... 12
4.9: Data analyses and presentation: .................................................................................................................. 12
4.10: Ethical consideration: ................................................................................................................................ 12
4.11: Study benefits: ........................................................................................................................................... 13
CHAPTER 5: RESULTS ........................................................................................................................................... 14
CHAPTER 6: DISCUSSION, CONCLUSIONS AND RECOMMENDATION .................................................................... 23
6.1: DISCUSSIONS ................................................................................................................................................ 23
6.2: CONCLUSION: ............................................................................................................................................... 24
6.3: LIMITATION .................................................................................................................................................. 24
6.4: RECOMMENDATION ..................................................................................................................................... 24
REFERENCES:........................................................................................................................................................ 25
APPENDIX 1 ......................................................................................................................................................... 27
APPENDIX 2 ......................................................................................................................................................... 29
viii
LIST OF FIGURES
Figure 1: graph on age distribution
Figure 2 : Pie chart showing the gender distribution of benign tumors
Figure 3:pie showing histologic distribution of benign tumours
Figure 4: pie chart showing the distribution of odontogenic tumours
Figure 5: gross specimen of an ameloblast
Figure 6: pre-treatment duration
LIST OF TABLES
Table 1:gender and tumour distribution
Table 2: histologic subtypes of epithelial tumours
Table 3: mesenchymal odontogenic tumours
Table 4: mixed odontogenic tumours
Table 5: non-odontogenic tumours
Table 6: non-odontogenic subtypes
Table 7: site distribution
ix
ABBREVIATIONS
UON University of Nairobi
UONDH University of Nairobi Dental Hospital
KNH Kenyatta National Hospital
BOT Benign orofacial tumors

1
ABSTRACT
Background: Benign tumors can cause serious aesthetic disturbances, difficulty in chewing
organ damage and furthermore some have potential for malignant transformation. Due to the
morbidity caused by these tumors and challenges in management, particularly in developing
countries, understanding of sociodemographic and clinicopathological features is essential. In
Kenya there is very little information on these tumors.
Objective: To describe the socio-demographic and clinico-pathological features of benign
orofacial tumors among patients who visited University of Nairobi Dental Hospital from 2008-
2012.
Study design: This study was a descriptive cross sectional study.
Setting: The study was conducted at the University of Nairobi dental hospital histopathological
laboratory.
Data collection: Laboratory records of all patients diagnosed with oral tumors was retrieved and
examined. The data which was collected from each record included the prevalence, age, site of
lesion and the time taken before patient seeks treatment. The data was analyzed and results
presented in the form of text, tables, graphs and pie charts.
Results: Records were retrieved from the histopathology laboratory from the year 2008-
2012.These records were from many centers in Kenya, including from Machakos, Nakuru,
Nyeri, Meru, Kenyatta National hospital, Voi, Kericho and Homa Bay. The total number of
records retrieved and studied for the five year period was 755. The total number of benign
tumours were 325(43.1%) of the total while the rest 430 (56.9%) were malignant.
Of the 325 benign tumours reviewed, 184 (56.6%) were odontogenic while 141 (43.4%) were
non-odontogenic. Amongst the odontogenic, epithelial tumours (86.4%) were the most common,
while for the non-odontogenic, epithelial soft tissue tumours (44.0%) were the most common.
The commonest non-odontogenic tumour was the pleomorphic salivary adenoma (28.9%).
The mandible (44.3%) and the maxilla (12.5%) were the most common site of occurrence of
benign tumours. Patients sought treatment after 2 years.
Conclusion: From this study, it can be concluded that there is almost equal prevalence of benign
tumours in the orofacial area as the malignant tumours. They were more common in young
people from the 2nd
to 4th
decade and affected the females more than the males. The odontogenic
tumours(56.6%) were more common, while the non-odontogenic were (43.4%).Most patients
had the treatment done after 2 years and the most affected site was the mandible and maxillae.
Recommendation: Primary health workers should be better trained to diagnose and refer oral
tumours.

2
Communities should be educated on these lesions for them to seek treatment as early as possible,
so as to improve the prognosis

3
CHAPTER1: INTRODUCTION
A tumor is an abnormal mass of tissue growth of which is excessive and uncoordinated with that
of normal tissues (1).
Benign orofacial tumors are tumors that occur in the orofacial region, this includes the lip,
tongue, gingival, alveolus, floor of the mouth, palate, buccal mucosa, mandible and the maxilla
(2). It is a mass of cells that lacks the ability to invade neighboring tissue or metastasize, has a
slower growth rate and cells are well differentiated.
The growth of benign tumors produce a ‘mass effect’ that can compress tissue and may cause
nerve damage leading too parasthesia, reduction in blood supply to an area in the body leading to
tissue death (necrosis) and organ damage. When they are large enough they cause intraoral and
facial asymmetry affecting the aesthetics of the patient. They also cause displacement of teeth
and lead to malocclusion which causes chewing difficulties. Patients with extremely large
tumors may be at increased risk of secondary bone fractures due increased bone resorption and
subsequent bone thinning (3). Some have the capacity for malignant transformation.
Benign orofacial tumors are not well studied in Kenya and thus there is very little information on
it. The information on benign orofacial tumors is from research done in different parts of the
world and not in Kenya. This study will focus on the benign orofacial tumors that occur in
Kenyan population. It will also give baseline information on the tumors for advanced studies to
be conducted.

4
CHAPTER 2: LITERATURE REVIEW
Benign tumors are usually well differentiated and closely resemble the tissue of origin. They
grow slowly and do not metastasize. There are many harmful effects if their growth compresses
adjacent tissues. Radiographically they form well defined radioluscency.
2.1: HISTOLOGICAL CLASSIFICATION OF BENIGN TUMOURS
Classification of tumors in the orofacial region is cumbersome and complex because of varied
types of tissues in this region and their different growth characteristics. As a result, many have
emerged and simplest approach is to group them into:
Odontogenic tumors
Non-odontogenic tumors (4)
The classification is further sub classified according to World Health Organization as shown in
appendix 1(5).
The most frequently occurring tumours reported in various African countries include
ameloblastoma, adenomatoid odontogenic tumor, calcifying epithelial odontogenic tumor,
ameloblastic fibroma, odontogenic myxoma, odontoma, and giant cell granuloma and
pleomorphic adenoma (26,27,28).
AMELOBLASTOMA
This is a neoplasm of odontogenic epithelium. It is the most common and usually presents
between the third and fifth decades of life. Although it is a benign tumor, it exhibits aggressive
behavior, being locally invasive. It is capable of metastasis to the lungs. In its clinical behavior,
it is typically asymptomatic. Most cases appear as multilocular cysts radiographically. The most
common site is the posterior mandible. Ameloblastomas can be further classified into solid,
cystic or peripheral according to their clinical characteristics. The histological categorization is
as follows: desmoplastic, granular cell, basal cell, plexiform, follicular, and acanthomatous (6).
They are treated by excision with a wide margin of normal tissue. Maxillary ameloblastoma can
invade the cranial base and have the potential of being lethal (7).

5
ADENOMATOID ODONTOGENIC TUMOUR
It is an odontogenic tumor arising from the enamel organ or dental lamina (8).They are
uncommon, completely benign and probably a hamartoma. Clinically adenomatoid odontogenic
tumor is found either in late adolescence or young adulthood between ages 15-20. Females are
twice as frequently affected as males and it commonly occurs in the anterior maxilla.
Radiographically it appears as a unilocular dentigurous cyst (9). It is treated by enucleation (10).
CALCIFYING EPITHELIAL ODONTOGENIC TUMOUR
Rare neoplasm of odontogenic epithelium, which presents between ages 40-70. Histologically it
has many bizarre pleomorphic and hyperchromatic nuclei and formation of amyloid like
material. It’s a solid tumor, with mixed radioluscency (with both radioluscency and radio
opacity). Most commonly forms in posterior mandible. Locally invasive but does not
metastasize. It is treated by excision (11).
CALCIFYING ODONTOGENIC TUMOUR
This rare tumor mainly affects young adults and involves the alveolar process of either jaw, close
to the roots of erupted teeth. Radiographically it appears unilocular often undistinguishable from
non-neoplastic jaw cysts.
Calcification in the cysts wall may suggest the diagnosis forms at any site in alveolar ridge,
usually posteriorly, occasionally forms in soft tissues of the gingival. Histological presence of
ghost and ameloblastic like cells confirms the diagnosis. Usually responds to enucleation. (12).
AMELOBLASTIC FIBROMA
It is rare but very important as a relatively common and sometimes destructive odontogenic
tumor in the young. It’s a solid lesion but appears as unilocular or multilocular radioluscency. It
is treated by excising the tumor with a small soft tissue margin. It can undergo malignant change
(13).
ODONTOGENIC MYXOMA
The odontogenic myxoma is an uncommon benign odontogenic tumor arising from embryonic
connective tissue associated with tooth formation (14). As a myxoma, this tumor consists mainly
of spindle shaped cells and scattered collagen fibers distributed through a loose, mucoid material

6
(15). It usually occurs in young adults. They are benign but prone to recurrence. On radiographs
it forms as multilocular, sometimes soap bubble radioluscency. The most common site is
posterior mandible and it is treated by excision (16).
CEMENTOBLASTOMA
It is a relatively a rare benign neoplasm of the cementum of the teeth. It is derived from
ectomesenchyme of odontogenic origin (17). Less than 0.69%–8% of all odontogenic tumors that
usually is seen in young adults. Radiographically it appears radiopaque with narrow lucent rim.
Most commonly at the apex of a vital lower first molar. It is treated by surgical excision of the
lesion and depending upon the clinical circumstances; this may or may not involve removal of
the involved tooth. With incomplete removal, recurrence is common; some surgeons advocate
curettage after extraction to decrease the overall rate of recurrence (18).
ODONTOMA
The odontoma is a hamartoma (19) of odontogenic origin (20).Usually found between ages 10-
20 years. Develops like surrounding teeth with initial radiolucent phase, intermediate stage of
mixed radioluscency, finally densely radiopaque. May be compound (many small teeth) or
complex (disordered mass of dental hard tissue) (21). The most common sites are anterior
maxilla and posterior mandible. They are treated by enucleation (22).
PLEOMORPHIC ADENOMA
They account for about 75% of parotid gland tumors and arise mainly from duct epithelium or
myoepithelial cells. Histologically it has an incomplete capsule, sheets or strands of dark
staining epithelial cells. It presents with squamous metaplasia and foci of keratin myxoid tissue.
Growth of pleomorphic adenoma is slow and may take several years to reach an inch in
diameter. They form rubbery often lobulated swellings. It is treated by wide excision (23).
SQUAMOUS CELL PAPILLOMA
A Squamous cell papilloma is a generally benign papilloma that arises from the stratified
squamous epithelium of the skin, lip, oral cavity, tongue, pharynx, larynx, esophagus.Squamous
cell papillomas are a result of infection with human papillomavirus (HPV) (24,25).
Papillomas mainly affect adults and have a distinctive, clinically recognizable cauliflower like or
structure with finger like process.

7
Histologically the papillae consist of stratified squamous epithelium supported by a vascular
connective tissue core. Most keratinized and so appear white. While most cases require no
treatment, therapy options include cryotherapy, application of a topical salicylic acid compound,
surgical excision and laser ablation (26).
2.2: ETIOLOGY AND EPIDEMIOLOGY
Etiology of benign orofacial tumors include: environmental toxins such as exposure to radiation,
genetics, diet, tobacco, stress and local trauma or injury (2).
Benign orofacial tumors are not well studied in Kenya and thus there very little information on it.
However an audit of oral disease at Nairobi centre, 2000-2004 by Dr.Dimba et al found out that
benign tumors mean age(29.93- 18.27 years) peaked in the third decade and tended to affect men
at younger age. The most common benign tumor was the ameloblastoma (50.23%) which
predominantly affected the mandible and also occurred in male patients at younger age (27).
Another study was done in Libya that analyzed the incidence of benign tumors. Amongst the
total benign tumors the keratocystic odontogenic tumor (35%) was the most common
odontogenic tumor. Among the non-odontogenic tumors, fibrous and adipose origin was 33%,
bone tumors 20%, cases of vascular origin 14% and neurogenic 7.1% (28).
A 6 year prospective study on orofacial tumors in Ghana recorded benign tumors to be common
in men aged 40-70 years and 11-20 years in female patients. Results showed 15% as
odontogenic, 26 as non-odontogenic in relation to the total number of tumors and tumor like
lesions (29).
The annual incidence rates per million for ameloblastomas are 1.96, 1.20, 0.18 and 0.44 for black
males, black females, white males and white females respectively (30). Ameloblastomas account
for about one percent of all oral tumors (31) and about 18% of odontogenic tumors (32). Men
and women tend to be equally affected, although women tend to be 4 years younger than men
when tumors first occur and tumors appear to be larger in females (33).
2.3: MANAGEMENT AND TREATMENT MODALITIES;
Most BOT are managed by enucleation/excision and they tend to respond to treatment without
recurrence. Some of the tumors such as giant cell granulomas are treated by curettage and
requires second operation at times.
ENUCLEATION:
It is a general surgical technique that is done by surgical removal of a mass without cutting into
or dissecting it (34).
8
CURETTAGE:
It is a medical procedure that uses a curette to remove tissue by scraping or scooping (35).
There is scanty information on benign orofacial tumours in Kenya and hence this study.
9
CHAPTER 3: STATEMENT OF THE PROBLEM,
JUSTIFICATION AND OBJECTIVES
3.1: Statement of the problem:
Benign tumors contribute considerably to the disease burden in the orofacial region. Patients
tend to present late, with complications. They cause a mass effect that can compress tissue and
may cause nerve damage, reduction in blood supply to an area of the body and organ damage. It
also affects the aesthetic of a person, causes bone deposition and resorption at the tumor site and
lastly the benign tumor could metastasize to a malignant tumor. Thus this study on BOT is
important.
3.2: Study justification:
Benign orofacial tumors are a poorly studied are in Kenya. There is therefore the need to audit
and determine the clinicopathological and sociodemographic features of it, so as to facilitate the
development of management protocols and create awareness for early detection and treatment.
3.3: Objectives:
3.3.1: General:
To describe the sociodemographic and clinicopathological features of BOT in patients who
visited UONDH from 2008 to 2012
3.3.2: Specific:
1. To determine the percentage of benign oral tumors relative to all tumors diagnosed.
2. To determine the frequency of each type of benign oral tumor in relation to all benign tumors.
3. To describe the age and gender distribution of BOT
4. To determine the site of occurrence
5. To determine the time taken before patient seeks treatment.
3.4: Variables:
Dependant variables:
Benign oral tumors
10
Site of occurrence
Independent variables:
Age
Gender
Duration since the tumor was first observed
11
CHAPTER 4: STUDY METHODOLOGY
4.1: Study area:
The study will be carried out at the UONDH histopathology laboratory. The hospital is located
about 3 kilometers from the central business district of the capital city of Nairobi opposite
Nairobi hospital. UONDH is a university teaching hospital offering training to students taking
courses in the dental school of dental sciences and includes both under- and post- graduate
students. It has major and minor operating theatres and one surgical ward capable of hosting 9
patients at a time. It’s a major referral centre and it is currently the leading referral and training
dental hospital in Kenya. It therefore provides comprehensive dental services to the population
within Nairobi and its environs as well as serving as a referral hospital for many patients from
other parts of the country.
4.2: Study population:
The study will include all patients diagnosed with any type of benign oral tumor at UONDH
histopathology lab between 2008-2012.
4.3: Study design:
This is going to be a descriptive cross-sectional, done by reviewing of records of patients
samples examined at UONDH between 2008-2012.
4.4: Sample size determination:
Based on previous reports, it is estimated that around 184 records of patients with BOT will be
available for this study covering the 5 year period.
4.5: Sampling:
All the clinical records of patients seen at the oral pathology lab at the UONDH from 2008-2012,
will be included in the study.
4.6: Inclusion and exclusion criteria:
4.6.1: Inclusion criteria:
Patients diagnosed with benign orofacial tumors and treated at the UONDH between 2008-2012
4.6.2: Exclusion criteria:

12
Incomplete records
Unclear records
Records of cases not seen within specific time frame
4.7: Data collection instruments and technique:
The records were retrieved with the assistance of the laboratory technologist in charge of
histopathology laboratory. The investigator examined the records for the variables of interest of
the study and recorded them in a record form (appendix 1). The data collected included the age,
gender, type of tumor (whether benign or malignant), type of benign tumor, site of tumor and the
time taken before patient sought treatment.
4.8: Problems anticipated
Some patients who are diagnosed at the UONDH had their treatment at other hospitals.
The specimens received were from different doctors and different cities thus there was improper
history written in the records.
Lack of important information due to improper record keeping i.e. incomplete clinical notes and
missing files.
4.9: Data analyses and presentation:
The data collected was analyzed using computer aided using SPSS version 17. The data is
described in terms of percentages and frequencies and presented in the form of bar graphs and
pie charts.
4.10: Ethical consideration:
Permission will be sought from University of Nairobi dental hospital administration to carry out
the study. Research proposal will be submitted to the University of Nairobi/Kenyatta national
hospital research ethics and standard committee for approval. All information collected will be
treated with confidentiality and will be used for research purposes only.
13
4.11: Study benefits:
The study gave out information on BOT amongst the Kenyan population. The information on the
prevalence, age and gender distribution.
The findings of the study will be used as baseline data in any subsequent research on the same
topic in future on the etiology, genes involved etc.
The results of the study will be submitted as part of the fulfillment of a Bachelor of Dental
Surgery (BDS) degree of the University of Nairobi.
14
CHAPTER 5: RESULTS
Records were retrieved from the histopathology lab between the year 2008-2012.These records
were from many centers in Kenya, including Machakos, Nakuru, Nyeri, Meru, Kenyatta National
hospital, Voi, Kericho and Homa Bay.
The patients presented with pain, swelling, mobile teeth, tongue fixation, asymmetry, loss of
hearing, enlargement of tongue, altered speech, dysphagia, parasthesia and lymphadenopathy.
TYPE OF TUMOR:
The total number of tumours reported between 2008 and 2012 were 755.
Out of the 755: 382 (50.5%) were females and 373 (49.5%) were males.
The total number of benign tumours were 325(43.1%) while malignant were 430 (56.9%).
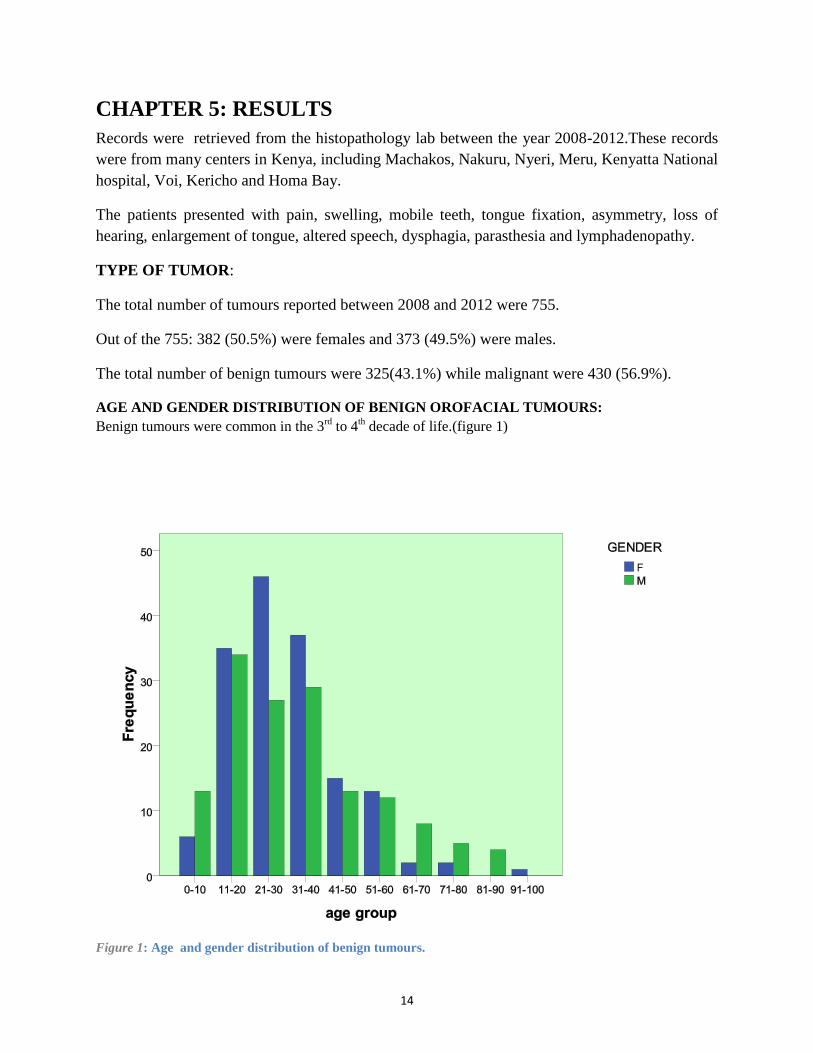
AGE AND GENDER DISTRIBUTION OF BENIGN OROFACIAL TUMOURS:
Benign tumours were common in the 3rd
to 4th decade of life.(figure 1)
Figure 1: Age and gender distribution of benign tumours.

15
The oldest patient being 95years old while the youngest was 10 days old. (Figure 1)
Mean age 31.99±17.67
GENDER DISTRIBUTION OF BENIGN OROFACIAL TUMOURS:
Of the 325 benign tumours 157(48.4%) were males while 168 (51.6%) were female giving a male to
female ratio of 1:1.1 (figure 2).
Figure 2 : Pie chart showing the gender distribution of benign tumors
51.6%
48.4%
16
DISTRIBUTION OF BENIGN TUMOURS BY YEAR REPORTED:
Table 1:gender and tumour distribution
The highest numbers of the benign tumours were seen in 2011. This was due an increased number of
specimens received to the laboratory in that year and it was not so clear on why the increased number of
specimens.
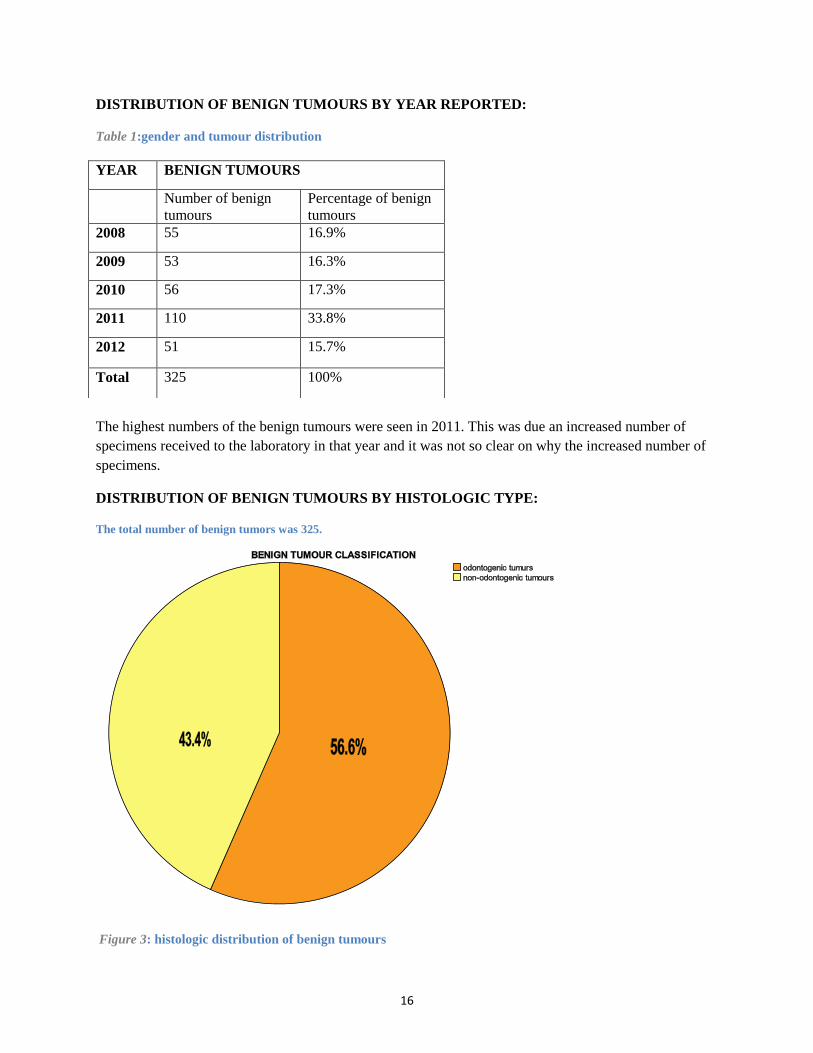
DISTRIBUTION OF BENIGN TUMOURS BY HISTOLOGIC TYPE:
The total number of benign tumors was 325.
Figure 3: histologic distribution of benign tumours
YEAR BENIGN TUMOURS
Number of benign
tumours
Percentage of benign
tumours
2008 55 16.9%
2009 53 16.3%
2010 56 17.3%
2011 110 33.8%
2012 51 15.7%
Total 325 100%
17
Of the 325 benign tumours reviewed 184 (56.6%) were odontogenic, 141 (43.4%) were non-
odontogenic.(figure 3)
DISTRIBUTION OF ODONTOGENIC TUMORS BY HISTOLOGIC TYPE:
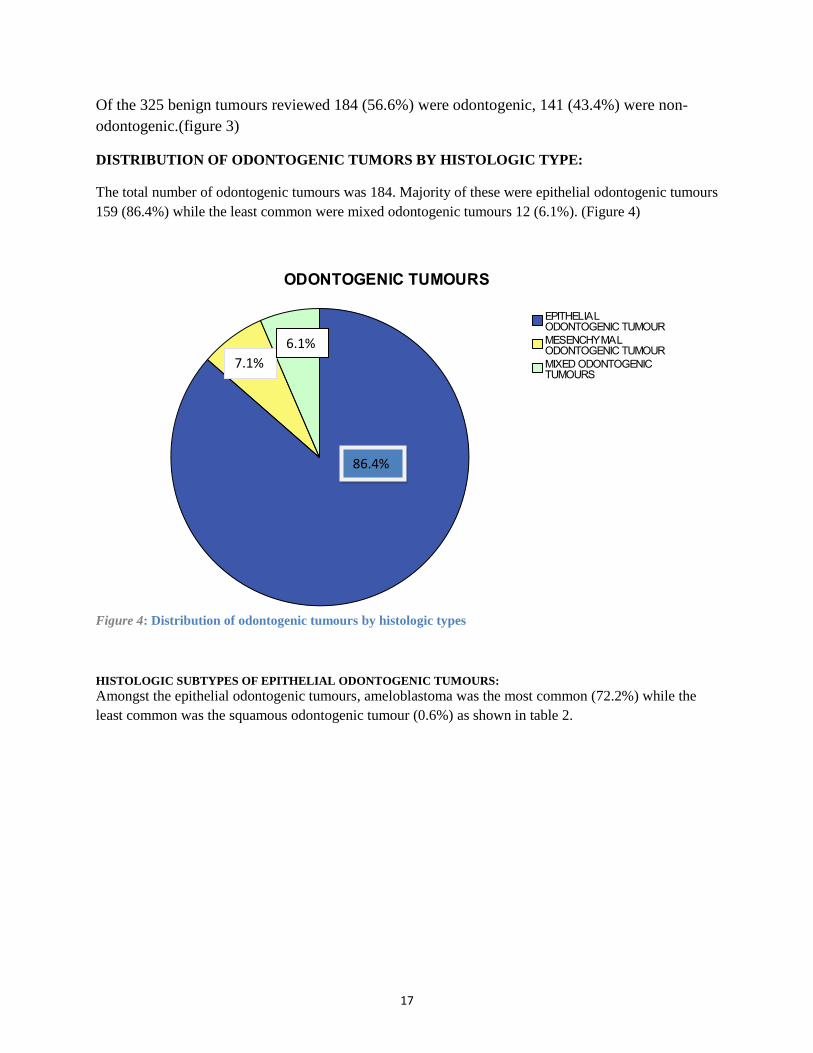
The total number of odontogenic tumours was 184. Majority of these were epithelial odontogenic tumours
159 (86.4%) while the least common were mixed odontogenic tumours 12 (6.1%). (Figure 4)
Figure 4: Distribution of odontogenic tumours by histologic types
HISTOLOGIC SUBTYPES OF EPITHELIAL ODONTOGENIC TUMOURS:
Amongst the epithelial odontogenic tumours, ameloblastoma was the most common (72.2%) while the
least common was the squamous odontogenic tumour (0.6%) as shown in table 2.
86.4%
7.1%
6.1%
18
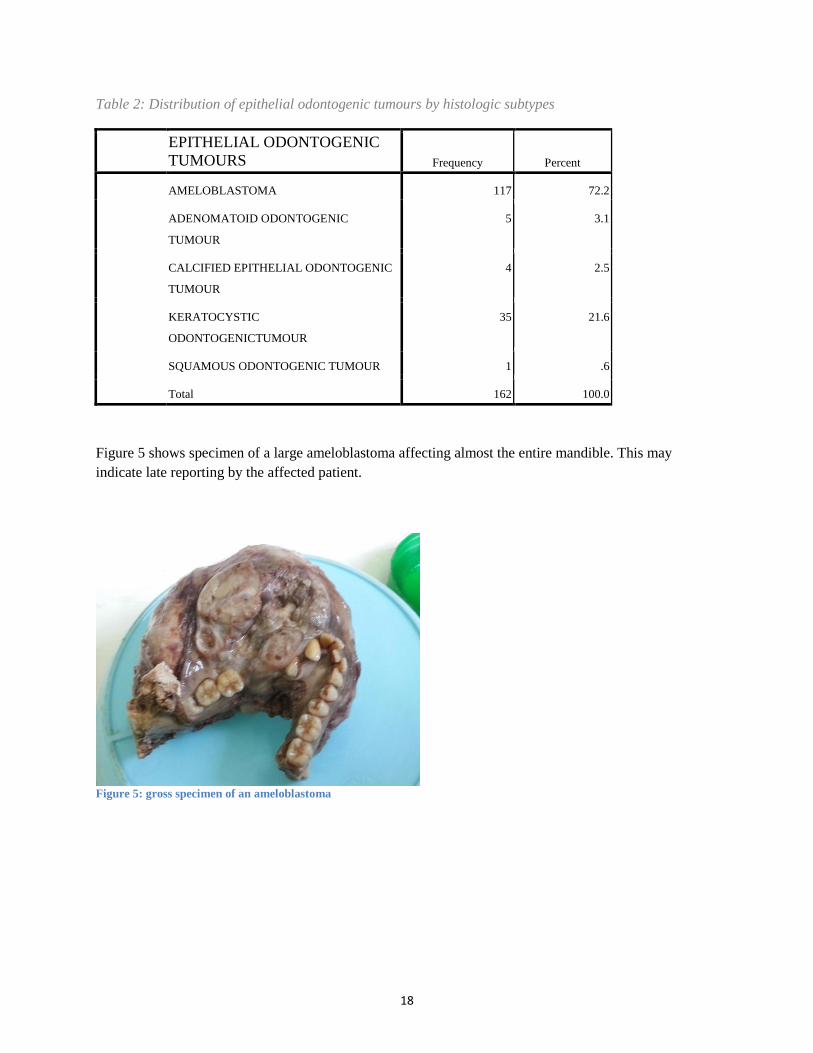
Table 2: Distribution of epithelial odontogenic tumours by histologic subtypes
EPITHELIAL ODONTOGENIC
TUMOURS Frequency Percent
AMELOBLASTOMA 117 72.2
ADENOMATOID ODONTOGENIC
TUMOUR
5 3.1
CALCIFIED EPITHELIAL ODONTOGENIC
TUMOUR
4 2.5
KERATOCYSTIC
ODONTOGENICTUMOUR
35 21.6
SQUAMOUS ODONTOGENIC TUMOUR 1 .6
Total 162 100.0
Figure 5 shows specimen of a large ameloblastoma affecting almost the entire mandible. This may
indicate late reporting by the affected patient.
Figure 5: gross specimen of an ameloblastoma
19
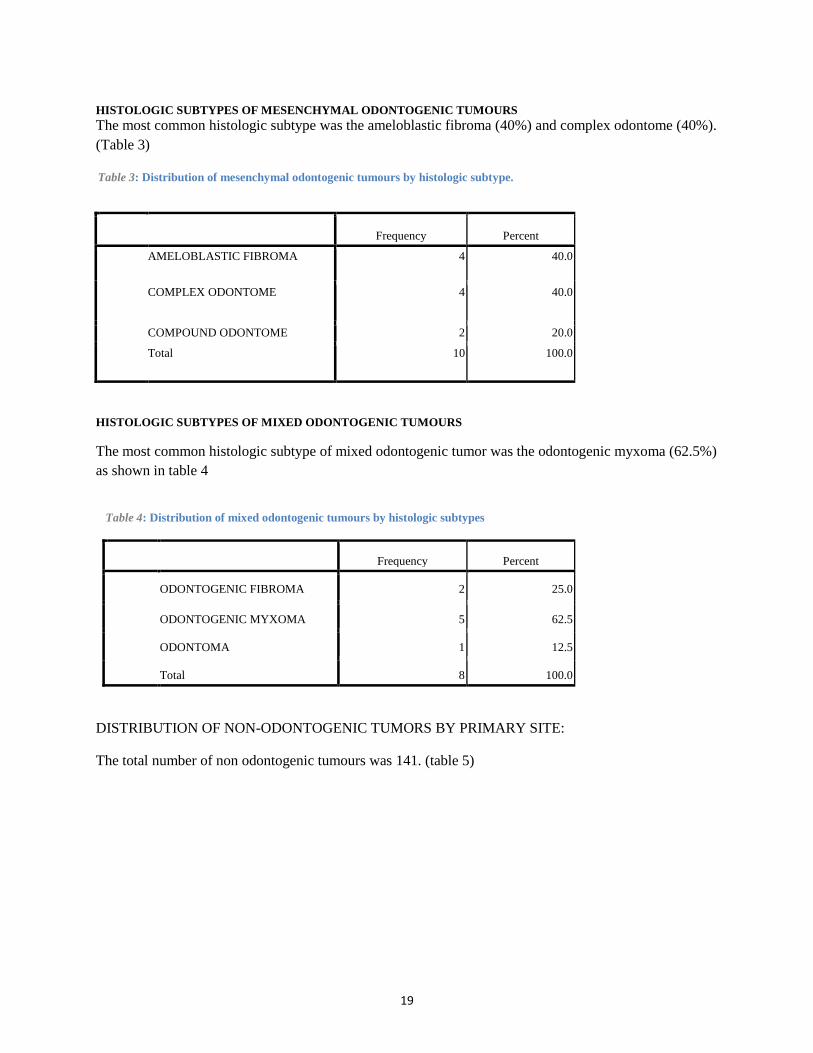
HISTOLOGIC SUBTYPES OF MESENCHYMAL ODONTOGENIC TUMOURS
The most common histologic subtype was the ameloblastic fibroma (40%) and complex odontome (40%).
(Table 3)
Table 3: Distribution of mesenchymal odontogenic tumours by histologic subtype.
Frequency Percent
AMELOBLASTIC FIBROMA 4 40.0
COMPLEX ODONTOME 4 40.0
COMPOUND ODONTOME 2 20.0
Total 10 100.0
HISTOLOGIC SUBTYPES OF MIXED ODONTOGENIC TUMOURS
The most common histologic subtype of mixed odontogenic tumor was the odontogenic myxoma (62.5%)
as shown in table 4
Table 4: Distribution of mixed odontogenic tumours by histologic subtypes
Frequency Percent
ODONTOGENIC FIBROMA 2 25.0
ODONTOGENIC MYXOMA 5 62.5
ODONTOMA 1 12.5
Total 8 100.0
DISTRIBUTION OF NON-ODONTOGENIC TUMORS BY PRIMARY SITE:
The total number of non odontogenic tumours was 141. (table 5)
20
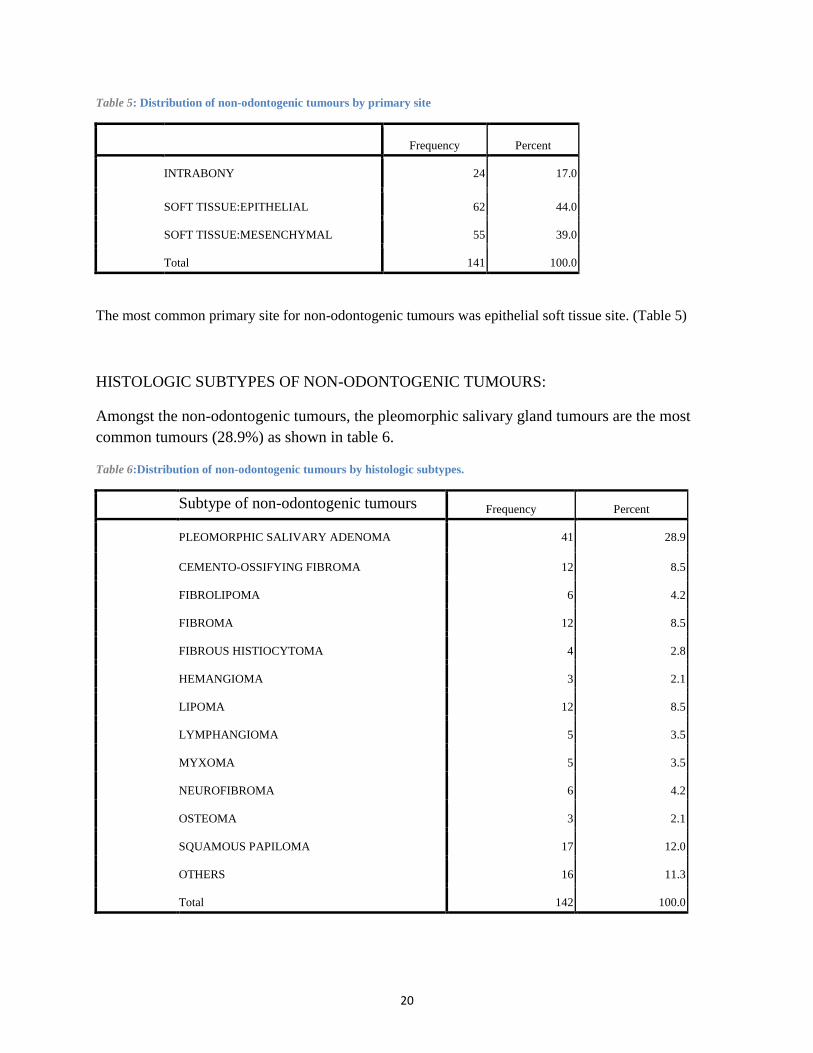
Table 5: Distribution of non-odontogenic tumours by primary site
Frequency Percent
INTRABONY 24 17.0
SOFT TISSUE:EPITHELIAL 62 44.0
SOFT TISSUE:MESENCHYMAL 55 39.0
Total 141 100.0
The most common primary site for non-odontogenic tumours was epithelial soft tissue site. (Table 5)
HISTOLOGIC SUBTYPES OF NON-ODONTOGENIC TUMOURS:
Amongst the non-odontogenic tumours, the pleomorphic salivary gland tumours are the most
common tumours (28.9%) as shown in table 6.
Table 6:Distribution of non-odontogenic tumours by histologic subtypes.
Subtype of non-odontogenic tumours Frequency Percent
PLEOMORPHIC SALIVARY ADENOMA 41 28.9
CEMENTO-OSSIFYING FIBROMA 12 8.5
FIBROLIPOMA 6 4.2
FIBROMA 12 8.5
FIBROUS HISTIOCYTOMA 4 2.8
HEMANGIOMA 3 2.1
LIPOMA 12 8.5
LYMPHANGIOMA 5 3.5
MYXOMA 5 3.5
NEUROFIBROMA 6 4.2
OSTEOMA 3 2.1
SQUAMOUS PAPILOMA 17 12.0
OTHERS 16 11.3
Total 142 100.0

21
SITE DISTRIBUTION OF BENIGN TUMORS: The most common site where the benign tumours occurred was the mandible (44.3%) as shown in table
7.
The least common site was the floor of the mouth (0.9%).
Table 7: Distribution of the benign tumours by site.
Frequency Percent
LIP 13 3.8
TONGUE 22 6.4
GINGIVA/ALVEOLAR 7 2.0
FLOOR OF MOUTH 3 .9
PALATE 36 10.5
BUCCAL MUCOSA 20 5.8
MAJOR SALIVARY
GLANDS
14 4.1
CHEEK 4 1.2
MANDIBLE 152 44.3
MAXILLA 43 12.5
ILLDEFINED ORAL SITES 12 3.5
OTHERS 10 2.9
Total 336 98.0
Incomplete information 7 2.0
Total 343 100.0
Ill defined sites were due to lack of information in the records.
Others include rare sites such as the temporal bone, eye, eye lid, nasal space, peri-auricular and
supraorbital areas.

22
DURATION OF TIME BEFORE PATIENTS SOUGHT TREATMENT:
Figure 6 shows the duration (in months) before patients seek treatment.
44.3% patients sought treatment in less than 2yrs since the symptoms appearance while the rest
(55.7%) sought treatment after 2 yrs.
Figure 6: Duration before patient sought treatment.
For those who sought treatment after 2years, 69% got treatment within 6months, 47% within a
year, 7% within 13-18 months and 21% within 19-24 months (2 years).
Pre-treatment duration

23
CHAPTER 6: DISCUSSION, CONCLUSIONS AND
RECOMMENDATION
6.1: DISCUSSIONS The number of benign tumours to the total number seen between the year 2008-2012 was 325
(43.1%). Benign tumors are most common in the 2nd to the 4th decade of life with a peak in the
3rd
decade at a mean age of 31.99±17.67. These findings are similar to those of a study done by
Dimba et al (2000-2004) on an audit of oral diseases at Nairobi center, which found benign
tumours occurring at a mean age of 29.9-18.27 that peaked in the 3rd
decade (27).
The highest number of patients with benign tumors was seen in the year 2011 as shown in table 1
with a total of 110 (33.8%) cases due to increase number of biopsies brought to the laboratory
though the reason as to why the increased number was not clear.
Amongst the benign tumours the commonest were the odontogenic tumours as shown in figure
2.It contraindicates the results found in Ghana that recorded non-odontogenic to be more
common (29).
Epithelial odontogenic tumours were the most common odontogenic tumors. These included:
ameloblastoma, calcified epithelial odontogenic tumour, squamous odontogenic tumours,
keratocystic odontogenic tumour and adenomatoid odontogenic tumour. Ameloblastoma being
the most common compared to the study done in Libya which reported keratocystic odontogenic
tumour to be the most common (28).
Non–odonotogenic tumors constitute 34% of total benign orofacial tumours of which intrabony
19.6%, fibrous and adipose tissue 53.6% and vascular 26.8% while in Libya they reported 20%
intrabony, 32% fibrous and adipose and 14% vascular (28).
Benign tumours affected the women more than the man as shown in figure 1. This is different to
a study done in Ghana that recorded the benign tumours commonly occur in males (29).
The odontogenic tumours were the most common (56.6%). Amongst the odontogenic the
epithelial tumours were the most common accounting for 86.4%. The most common epithelial
tumour was ameloblastoma (72.2%) and the least was squamous odontogenic tumour
(0.6%).Amongst the mesenchymal odontogenic tumours ameloblastic fibroma(40%) and
complex odontome(40%) were the most common while for the mixed odontogenic tumours
odontogenic myxoma (62.5%) was the most common. Amongst the non-odontogenic the soft
tissue epithelial tumours are the most common (44.0%), of which pleomorphic salivary adenoma
was the most common accounting for 28.9%. However there is scanty information on these.
The most common sites at which benign tumours occur are the jaw bones, mandible and the
maxilla, mandible being 44.3% and maxilla 12.5%.

24
Most patients did not seek treatment at an earlier stage. Most got the treatment after 2years when
the sign and symptoms are severe. The tumour tends to have increased in size and the
management becomes more difficult when the tumour involves vital structures and increased
destruction of bone and normal tissue (3).
6.2: CONCLUSION:
From this study, it can be concluded that there is almost equal prevalence of benign tumours in
the orofacial area as the malignant tumours. The benign tumours affected females more than the
male. Benign tumours are more common in young people from the 2nd
to 4th
decade. The
odontogenic tumours were the most common (56.6%). Amongst the odontogenic, the epithelial
tumours were the most common accounting for 86.4%. The most common epithelial tumour was
ameloblastoma (72.2%). Amongst the non-odontogenic the soft tissue epithelial tumours are the
most common (44.0%), of which pleomorphic salivary adenoma was the most common
accounting for 28.9%. Most patients had the treatment done after 2 years and the most affected
site was the mandible and maxillae.
6.3: LIMITATION
It was difficult to access to clinical files. The study was retrospective and was dependant on
laboratory records.
6.4: RECOMMENDATION
1. Primary health workers should be better trained to diagnose and refer tumours.
2. There should be more pathologists trained in the head and neck area and distributed in
many centers in Kenya for faster results and better prognosis.
3. Communities should be educated on these lesions for them to seek treatment as early as
possible, within 6 months so as to improve the prognosis.
4. More studies to be carried out on larger samples for definitive trend among the tumours
and to develop evidence based strategies for treatment of benign orofacial tumours in
Kenya.
5. Widespread of pathology laboratory with specialized personnel would lead to faster
diagnosis and earlier treatment for better prognosis.
6. An investigation on why an increased number of benign tumours in 2011.
25
REFERENCES:
1. Robbins and Cotran, (Saunders 1991). Pathologic basis of disease 8th
edition, page 75.
2. JOSEPH A REGEZI, (Saunders 1990) Clinical pathology correlations 4th
edition, Pgs 267-
290.
3. Philip A Szanto, Lippincott Williams and Wilkins, 1991, Pathology board review series,
2nd
Ed pg 95-96.
4. 4 July-December 2003, The Nigerian Journal of Surgical Research, volume 5, number 3-4,
page 134.
5. Barnes L, Eveson JW, Reichont P, Sidransky D, IARC Press, Lyon 2005. World health
Organization classification of tumours, Pathology and Genetics of head and necktumours, pg 5-
7.
6. Madhup, R; Kirti, S; Bhatt, M; Srivastava, M; Sudhir, S; Srivastava A , January 2006,
"Giant ameloblastoma of jaw successfully treated by radiotherapy". Oral Oncology Extra 42 (1):
22–25.
7. Ackerman GL, Altini M Shear , The unicystic ameloblastoma: a clinicopathological study
57 cases. J oral patho med 1988 17: pg 541- 546.
8. Nigam S, Gupta SK, Chaturvedi KU (2005). "Adenomatoid odontogenic tumor - a rare
cause of jaw swelling". Braz Dent J 16 (3): 251–3
9. Baden E Doyle, Mesa M, Fabie M, Lederman D, Eichen M, 1993, squamous odontogenic
tumor. Report of three cases. Oral surg med oral patho volume 75; pg 733-738.
10. Vasconcelos BC, Frota R, Cardoso AB, Porto GG, Carneiro SC (2008). "Adenomatoid
odontogenic tumor". Braz J Otorhinolaryngol 74 (2): pg 315.
11. Buchner A Merrel PW, Hansen LS Leider AS, 1991, Peripheral calcifying odontogenic
tumour. A review of 45 cases. Oral surg oral patho, vol 72:pg 65-70.
12. Cawson RA, Binnie WH,barrett AW, Speight P, Wright JM luca’s (1998), pathology of
tumors of the oral tissues. Churchill Livingstone, Edinburgh pg 131-132.
13. Kahn, Michael A, (2001), Basic Oral and Maxillofacial Pathology. Volume 1 pg 3
26
14. Sapp, J. Philip., Lewis R. Eversole, and George P. Wysocki, (2002) , Contemporary Oral
and Maxillofacial Pathology, 2nd ed. St. Louis, MO: Mosby, pg 152-53.
15. Cawson, R. A., and E. W. Odell, (2008), Cawson's Essentials of Oral Pathology and Oral
Medicine. 8th ed. Edinburgh: Churchill Livingstone, pg 145-46.
16. Cawson RA,(1972), Myxoma of the mandible within a 35 year follow-up. Br oral surg vol
10: pg 59-63.
17. Leena S Sankari and K Ramakrishnan, 2011 Sep-Dec , Journal of Oral and Maxillofacial
Pathology, Benign cementoblastoma, vol 15(3):pg 358-360, at
http://www.ncbi.nlm.nih.gov/pmc/articles
18. Huber AR, Folk GS. (20009), Cementoblastoma. Head Neck Pathol. Volume 3:133–5
19. Junquera L, de Vicente JC, Roig P, Olay S, Rodríguez-Recio O (2005). "Intraosseous
odontoma erupted into the oral cavity: an unusual pathology". Med Oral Patol Oral Cir Bucal 10
(3): 248–51.
20. "Oral Pathology Glossary O". Retrieved 2009-01-04.
21. Amado Cuesta S, Gargallo Albiol J, Berini Aytés L, Gay Escoda C (2003). "Review of 61
cases of odontoma. Presentation of an erupted complex odontoma". Med Oral 8 (5): 366–73
22. Cawson RA Binnie WH,barrett AW, Speight P, Wright JM oral disease,3ed. Mosby-
Wolfe, London.2001.
23. Brookstone M, Huvos AG, (1992), Central salivary gland tumors of the maxilla and the
mandible: a clinicopathological study of 11 cases with an analysis of the literature. J oral
maxillofacial surg , vol 50:pg 229-236.
24. New Zealand Dermatological Society (2007). "Squamous cell papilloma". New Zealand
Dermatological Society, Retrieved December 19, 2007.
25. Nikon Microscopy (2007). "Squamous Cell Papilloma". Nikon Microscopy. Retrieved
December 19, 2007.
26. National Library for Health (2007). "Squamous cell papilloma". National Library for
Health. Retrieved December 19, 2007.
27. Dimba E.A.O et al IDJ December 2000-2004, An audit of oral diseases at a Nairobi centre,
vol 6, pgs 1-2
28. El-ghani r, Orafi m, Elarabi m and Subhash raj k.(2007), Study on benign tumors of
orofacial region, Benghazi, Libya pg 3-5.
29. Parkins GE, Armh, Tetty Y, (1998-2003), study on orofacial tumors and tumor like lesions,
University of Ghana Dental School, College of Health Sciences, Korle –Bu, Ghana.pg 4
30. Shear M, Singh S (July 1978). "Age-standardized incidence rates of ameloblastoma and
dentigerous cyst on the Witwatersrand, South Africa". Community Dent Oral Epidemiol 6 (4):
195–9.
31. Randall S. Zane, M.D. (3 January 2009). "Maxillary Ameloblastoma, pg 19-20.
32. Jonathan Gordon, M.D., Ph.D. (30 December 2008). "Clinical Quiz: Painless Mass". Appl
Radiol Online 3, pg 8.
33. Reichart PA, Philipsen HP, Sonner S. (Mar; 1995). "Ameloblastoma: biological profile of
3677 cases". Eur J Cancer B Oral Oncol. 31B (2): 86–99.
34. Robert E Stern Diane(2003) oral and maxillofacial pathology; a rationale for diagnosis and
treatment
35. Science and technology: www.encyclopaedia Britannia.com, January 2010.
27
APPENDIX 1
WHO CLASSIFICATION OF TUMOURS 2005
These are sub classified into:
1. EPITHELIAL TUMOURS : They composed of odontogenic epithelium but without
odontogenic ectomesenchyme
Ameloblastoma
Squamous odontogenic tumor
Calcifying epithelial odontogenic tumor
Adenomatoid odontogenic tumor
Keratocystic odontogenic tumor
2. MESENCHYMAL TUMOURS: These are composed of odontogenic epithelium with
odontogenic ectomesenchyme with r without hard tissue formation)
ameloblastic fibroma
ameloblastic fibro-odontoma
ameloblastic fibro-dentinoma
odontma, complex and compound
odonoameloblastoma
calcifying cystic odontogenic tumor
dentinogenic ghost cell tumor
3. MIXED TUMOURS
They are composed of odontogenic mesenchyme and/ or ectomesenchyme with or
without epithelium.
Odontogenic fibroma
Odontogenic myxoma and myxofibroma
28
NON-ODONTOGENIC TUMOURS
These are sub classified into:
1. Intra-bony/jaw tumors
2. Soft tissue tumors
INTRA-BONY
osteoma
osteochondroma
cement-ossifying fibroma
central giant cell granuloma
hemangioma
melanotic neuroectodermal tumor
SOFT TISSUE
Soft tissue tumors are further classified into:
I. Epithelial:
Pleomorphic adenoma
Myoepithelioma
Basal cell adenoma
Warthin’s tumor
Oncocytoma
Canalicular adenoma
Sebaceous adenoma
Cystaadenoma
Ductal papillomas
Squamous cell papilloma
II. Mesenchymal :
Myxoma
Fibroma
Angiofibroma
Nodular fasciitis
Fibromatosis
29
APPENDIX 2
Data collection form:
Serial
no:
Patient
file no:
Gender Age Type of
tumor(B=benig
n,
M=malignant)
Type of benign
tumor
Site Duration
before
patient seeks
treatment

30
Related Documents











