Critical Limb Ischemia: Keeping a Leg Up on This Disease Ethan Korngold, MD Medical Director of Cardiovascular Research Providence Heart and Vascular Institute Co-Medical Director, Providence Valve Center June 7, 2015 © 2012 Abbott. All rights reserved. NPL03994 Rev. A (10/2012) CAUTION: Investigational device. Limited by Federal (U.S.) law to investigational use only. © 201 2012 Abbott. All rights reserv served. NPL03994 Rev. A (10/2012) CAUTION: Investigational de vice. Lim vice. Limited b ited by Federal (U.S.) law to investigatio ational use only. Disclosures • Abbott Vascular: medical advisory board, speakers bureau, education • Boston Scientific: medical advisory board • Edwards Lifesciences: proctoring • Medtronic: speakers bureau • Terumo: speakers bureau, education We will be discussing off-label uses of FDA approved devices. • 83 y/o M, CAD, CHF EF 45%, DM2, HTN • Lives independently with wife • 3 months of R foot ulcer and osteomyelitis • ABI noncompressible • Aggressive wound care, iv abx • Angiogram by vascular surgeon A Case…

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Critical Limb Ischemia:
Keeping a Leg Up on This Disease
Ethan Korngold, MD
Medical Director of Cardiovascular Research
Providence Heart and Vascular Institute
Co-Medical Director, Providence Valve Center
June 7, 2015
© 2012 Abbott. All rights reserved. NPL03994 Rev. A (10/2012) CAUTION: Investigational device. Limited by Federal (U.S.) law to investigational use only.© 2012 © 2012 Abbott. All rights reserved. eserved. NPL03994 Rev. A (10/2012) CAUTION: Investigational detional device. Limvice. Limited by Fited by Federal (U.S.) law to investigationaligational use only.
Disclosures
• Abbott Vascular: medical advisory board, speakers bureau, education
• Boston Scientific: medical advisory board
• Edwards Lifesciences: proctoring
• Medtronic: speakers bureau
• Terumo: speakers bureau, education
We will be discussing off-label uses of FDA approved devices.
• 83 y/o M, CAD, CHF EF 45%, DM2, HTN
• Lives independently with wife
• 3 months of R foot ulcer and osteomyelitis
• ABI noncompressible
• Aggressive wound care, iv abx
• Angiogram by vascular surgeon
A Case…

Angiogram
Procedure Note:
“Right LE Angiography
reveals patent arteries to
the right foot, with severe
small-vessel disease.
There is no option for
intervention.”
Occluded R tibioperoneal trunk
Subtotal occlusion R anterior tibial
• 3 months later, sees me for followup
• Wants any option to save his leg
A Case…
Angiogram
0.014” Command Wire 4x20mm Angiosculpt balloon

Angiogram
Final Images
• Ulcer heals 2-3 weeks later
• ABI at one month: 0.9 (mildly abnormal)
One Wire, One Balloon
• Common
• Systemic disease with high risk of
cardiovascular mortality and morbidity
• Requires systemic therapy
• Modern peripheral vascular interventions are
safe and effective
• There is no such thing as “small vessel
disease”
Peripheral Arterial Disease

0% 5% 10% 15% 20% 25% 30% 35%
29%PARTNERS5
Age >70, or between 50-69 with diabetes or smoking
11.7%San Diego2
Mean Age=66
19.8%Diehm4
Age ≥65
19.1%Rotterdam3
Age >55
14.5%NHANES1
Age ≥70
4.3%
Documented Presence of PAD
When common risk factors were included, the prevalence of PAD was ~1/3 of patients
1. Selvin E, Erlinger TP. NHANES. Circulation. 2004;110:738-743.2. Criqui MH, et al. Circulation. 1985;71:510-515.3. Diehm C, et al. Atherosclerosis. 2004;172:95–105. 4. Meijer WT, et al. Arterioscler Thromb Vasc Biol. 1998;18:185-192. 5. Hirsch AT, et al. JAMA. 2001;286:1317-1324.
NHANES1
Age >40
0
20
40
60
55-59 60-64 65-69 70-74 75-79 80-84 85-89
Rotterdam Study (ABI <0.9) San Diego Study (PAD by noninvasive tests)
Prevalence of PAD Increases With Age
Figure adapted from Creager M, ed. Management of Peripheral Arterial Disease. Medical, Surgical and Interventional Aspects. 2000.
Pati
en
ts w
ith
PA
D (
%)
Age Group (y)
Vascular Disease is a Systemic Disease
Bhatt DL, et al. REACH Investigation. Presented at: American College of Cardiology Annual Scientific Session; March 8, 2005; Orlando, FL. Abstract 1127-96.
PAD
36.9%
9.5%
39.4%
14.2%
CVD
CAD
N=7013

Natural History of PAD:
5-year Outcomes
Stable Claudication
70-80%
Worsening Claudication
10-20%
Critical Limb Ischemia
1-2 %
Limb MorbidityLimb Morbidity
Non-CV Causes 25%
CV Causes 75%
Mortality 15-30%
Nonfatal CV Events 15-30%
Cardiovascular Morbidity and Mortality
Weitz et al.
PAD Survival Curve
Criqui MH, et al. N Engl J Med. 1992;326:381–386.
Normal Subjects
Asymptomatic PAD
Symptomatic PAD
Severe Symptomatic PAD
100
75
50
25
0 2 4 6 8 10 12
Surv
ival (%
)
Year
Critical Limb Ischemia (CLI): Fate of Patients After Initial Treatment
Dormandy JA, et al. J Vasc Surg. 2000;31:S1-S296.
Summary of 19 studies on 6-month outcomes
tients After Initial Treatment
Summar6-m
Sumon 6-m
Dead
20%
Alive Without Amputation
45%
Alive with Amputation
35%

• History
• Physical exam
• Non-invasive assessments
• Invasive angiography
Establishing the diagnosis
of PAD
• Asymptomatic
• Intermittent claudication
– Discomfort, ache, cramping in leg with exercise
– Resolves with rest
• Critical limb ischemia
– Rest pain
• Pain or paresthesias in foot or toes, worsened by leg elevation and improved by dependency
– Ischemic ulceration and gangrene
Clinical Manifestations of
PAD
Elevation Pallor
Dependent Rubor

Critical Limb Ischemia (CLI)
Non-invasive assessments of CAD and PAD are similar
Peripheral Arterial Disease
- ABI
- PVR, Segmental Pressures
- Treadmill Test
- Duplex US, CTA, MRA
Coronary Artery Disease
- EKG
- Echo
- Stress Test
- Angiography
The Ankle-Brachial Index (EKG)
• Simple, painless, accurate, highly reproducible
• Clinical utility
–Diagnosis of PAD
–Prognosis: predictor of MACE

ACC/AHA 2006 PAD Management Guidelines Diagnostic Methods: Ankle-Brachial Index (ABI)
The resting ABI should be used to establish the lower extremity PAD
diagnosis in patients with suspected lower extremity PAD, defined as
individuals:
• with exertional leg symptoms,
• with nonhealing wounds,
• who are 70 years and older,
• or who are 50 years and older with a history of smoking or diabetes.
I IIa IIb III
C
Adapted from Hirsch AT, et al. J Am Coll Cardiol. 2006:47:1239-1312.
Ankle systolic pressure
Brachial systolic pressure
ABI =
• Ankle and brachial systolic pressures taken using a hand-held Doppler instrument
• The ABI is 95% sensitive, 99% specific for PAD
The Ankle-Brachial Index
Normal 0.90 -1.30
PAD < 0.90
Pain/Ulceration < 0.40
Non-Compressible > 1.30
ABI Limitations
• ABI may be elevated in patients with
noncompressible arteries, such as those who
are elderly or have diabetes
• Resting ABI is insensitive to mild aortoiliac
occlusive disease
• Some symptomatic patients have normal
resting ABI (like an EKG)

Diagnostic Algorithm for PAD
History, Physical Examination Suggestive of PAD?
No!Search for Alternate Diagnosis
Yes?
<0.9
PAD
>0.9
Still Suspicious?
>1.30
Vascular Lab Referral •segmental pressures, PVR •graded treadmill test
Anatomic Assessment: DUS, CTA, MRA
Ankle-Brachial Index
Therapies for PAD
Preventing Death, MI, Stroke
• Antiplatelets
• Cholesterol lowering – statins
• ACE Inhibitors
Pre
•••
Reducing Claudication Symptoms
• Exercise
• Cilostazol
• Endovascular interventions
• Surgery
Saving Limbs in CLI
• Endovascular interventions
• Surgery
Therapies for PAD
Preventing Death, MI, Stroke
• Antiplatelets
• Cholesterol lowering – statins
• ACE Inhibitors
Pre
•••

Risk of Occlusive Vascular Events in High-Risk Patients: Antithrombotic Trialists’ Collaboration
Antithrombotic Trialists’ Collaboration. BMJ. 2002;324:71-86.
APT=antiplatelet therapy with aspirin, clopidogrel,
dipyridamide, or a glycoprotein IIb/IIIa antagonist
N=9706
Intermittent
claudication (N=26)
Reduced Increased
Risk versus Control
1.0 1.5 2.00.50.0
6.4 7.9
Peripheral
grafting (N=12)5.4 6.5
Peripheral
angioplasty (N=4)2.5 3.6
All PAD trials (N=42) 5.8 7.1
Risk Category
(number of trials) APT Control
Patients with Event (%)
Intermittent
claudication (N=26)
Reduced IncreasedReduced Increased
6.4 7.9
Peripheral
grafting (N=12)5.4 6.5
Peripheral
angioplasty (N=4)2.5 3.6
All PAD trials (N=42) 5.8 7.1
Risk Category
(number of trials)
Efficacy of Clopidogrel vs Aspirin in MI, Ischemic Stroke, or Vascular Death
Months of Follow-Up
Cum
ula
tive
Event R
ate
(%
)
0
4
8
12
16
Clopidogrel
Aspirin
Overall Relative Risk
Reduction
8.7%*
0 3 6 9 12 15 18 21 24 27 30 33 36
Aspirin
5.83%
5.32%
Clopidogrel
*ITT analysis.CAPRIE Steering Committee. Lancet. 1996;348:1329-1339.
Mean Follow-up = 1.91 years
N=19,185
Heart Protection Study: Vascular Event by Prior Disease
Heart Protection Study Collaborative Group. Lancet. 2002;360:7-22.
MI - myocardial infarction; CHD - coronary heart disease; CVD - cerebrovascular disease; PAD - peripheral arterial disease; CI -
confidence interval; SE - standard error
Previous MI 23.5 29.4
Other CHD 18.9 24.2
No prior CHD or CVD 18.7 23.6
Peripheral arterial disease 24.7 30.5
Diabetes 13.8 18.6
All patients 19.8 25.2
1.0 1.2 1.40.80.60.4
24% Reduction
(p<0.0001)
Existing DiseaseStatin Control
Incidence of Events
(n=10,269)(n=10,267) Statin Favored Placebo
Risk versus Control

Statins Now Have Been Shown to Reduce Adverse Events After Revascularization
Lower MACCE
Better Long Term Patency After Infrapoplital Interventions
Westin GG et al., JACC 2014
HOPE Study Investigators. N Engl J Med. 2000;342:145-153.
HOPE Trial: Ramipril Benefits in
CV Risk Subgroups
NHANES database, 7458 patients, age >40
Pande et al., Circulation 2011
Prevalence of PAD: 5.9%
0%
25%
50%
75%
100%
ASA Statin ACE/ARB
24%30%
36%
PAD patients receiving therapy (%)
PAD Patients are Undertreated

PAD Patients are Common and Undertreated
0
1,000,000
2,000,000
3,000,000
4,000,000
5,000,000
6,000,000
ASA Statin ACE/ARB
5,400,0005,000,000
4,500,000
Number of patients not receiving therapy (US)
NHANES database, 7458 patients, age >40
Pande et al., Circulation 2011
CLI Patients are Undertreated
Westin GG et al., JACC 2014
Therapies for PAD
Reducing Claudication Symptoms
• Exercise
• Cilostazol
• Endovascular interventions
• Surgery

140
Effects of Exercise Training on Claudication Meta-analysis of 21 Studies
Gardner AW, Poehlman ET. JAMA. 1995;274:975-980.
Exercise Training
Control
80
200
0
20
40
60
100
120
160
180
Onset of Claudication Pain
Maximal Claudication Pain
Ch
an
ge i
n T
read
mil
l
Walk
ing
Dis
tan
ce (
%)
Therapy of Intermittent Claudication:Magnitude of Functional Improvement
Pentoxifylline
Cilostazol
Supervised Exercise
Improvement Over Baseline After 90 to 180 Days (%)
Gardner AW, Poehlman ET. JAMA. 1995;274:975-980; Girolami B, et al. Arch Intern Med. 1999;159:337-345.Hiatt WR. N Engl J Med. 2001; 344;1608-1621.
0 50 100 150 200
Therapies for PAD
Reducing Claudication Symptoms
• Exercise
• Cilostazol
• Endovascular interventions
• Surgery
Saving Limbs in CLI
• Endovascular interventions
• Surgery
Sav

• Claudication – Disabling
– Lifestyle limiting
• Critical Limb Ischemia – Tissue loss/ulceration/ischemia
– Rest pain
– Refractory infection
PAD: Indications for Intervention
Analogy: Angina
Urgency: Whenever
Analogy: ACS
Urgency: Now!
Case: Critical Limb Ischemia
• 91 y/o F
–HTN, elevated cholesterol, CVA, CAD, CHF, COPD
• Two months of rest pain, ulceration of right foot,
despite supportive care
• ABI: non-compressible vessels
• PVR: flat
Physiologic Assessment
• ABI or Segmental Pressures
Anatomic Assessment
• Duplex ultrasound
• CTA or MRA
• Angiogram
CLI: What Evaluation is Needed

• Wound healing requires 6 times as much blood flow as baseline metabolic needs
• Typically multisegment infrainguinal disease
• Often chronic occlusions
• Goal: inline blood flow to foot to facilitate healing
• Safest possible way (high risk patients)
Critical Limb Ischemia: Goals
Tefera et al., JVS 2005
Is long term patency reallyneeded for healing in CLI?
Optimal Perfusion
Actual Perfusion
Metabolic Demand
Trauma
Revascularization
Patent
Restenosis
Time needed for healing
Adapted from: Vermassen F 2010 and S. McDonald 2011
Ulcer
Healing

Traditional Surgical Bypass Has Significant Morbidity and Mortality
• Mortality 2-5%
• Myocardial Infarction 1.9-3.4%
• Hemorrhage 2%
• Graft Thrombosis 2-7%
• Wound Infection 8-19%
• Surgical Revision >20%
TransAtlantic Inter-Society Consensus (TASC) JVS 2000; 31(1;2)
Femoral-Popliteal Bypass: 5 Year Primary Patency
JAMA 1995: 274: 71
0%
25%
50%
75%
100%
Claudication Critical Limb
47%
75%
66%
80%
Vein PTFE
5 year primary patency, pooled data, 1194 cases
Vein Bypass for SFA Disease: 2 year Patency
0%
25%
50%
75%
100%
Femoral-Popliteal Femoral-Tibial
55%
69%
51%
66%
Primary Patency Secondary Patency
24 month followup, 243 patients
Becquemin NEJM 1997: 337:1726

CryoVein Bypass for CLI:
Primary Patency
0%
25%
50%
75%
100%
Months
0 3 6 9 12 15 18
89%
63%
30%
17%9%
Zehr BP et al., Annals of Vascular Surgery, 2011
Cook Zilver PTX Drug Coated SFA Stent: 5 Year Data
0%
25%
50%
75%
100%
2 year 5 year
83%87%
66%
75%
Patency Freedom from TLR
Presented at VIVA 2014
Abbott Supera SFA Stent: 3 Year Data
0%
25%
50%
75%
100%
1 year 2 year 3 year
82%84%89%86%
PatencyFreedom from TLR
Presented at VIVA 2014
Non-Restenosis Rate by Lesion Length (12 months SUPERB TRIAL)

Infrapopliteal Angioplasty: Meta-analysis
0%
25%
50%
75%
100%
1 month 6 months 1 year 2 years 3 years
82%85%89%91%95%
63%64%68%
74%
83%
49%51%58%
65%
77%
Patency Secondary Patency Limb Salvage
Romiti M, et al., JVS 2008
Disconnect Between Patency and Salvage
Romiti M, et al., JVS 2008
Endovascular First Approach for Critical Limb Ischemia is Effective for Limb Salvage
• Dorros, Jaff, et al., Circ 2001
• Feiring et al., JACC 2004
• Tefera et al., JVS 2005
• Kudo et al., JVS 2005
• May KK, VES 2014
0%
25%
50%
75%
100%
Dorros Feiring Tefera Kudo May
78%
89%84%
90%91%
Limb Salvage at 1-5y
813813 Total Limbs

Infrapopliteal Intervention: Low Complication Rates
0%
2%
4%
6%
8%
10%
Gro
in h
emat
oma
Thom
bosis
Embo
lism
Perfo
ratio
n
Diss
ectio
n
PSA
GIB
Oth
erEm
erge
ncy
Surg
ery
1.3%
0.2%0.2%0.3%0.1%0.7%1.0%
2.1%
3.2%
Emer
g
Emer
g
Little “clinical penalty” in starting with an endovascular approach
Romiti M, et al., JVS 2008
1743 Interventions Analyzed
BASIL Trial: Infrainguinal Critical Limb Ischemia
• 452 patients with CLI, randomized 1:1 to bypass or angioplasty first
• Primary Outcome
–Amputation free survival
–Death
Adam et al., Lancet 2005: 366; 1925
BASIL Trial: Primary Outcomes
Adam et al., Lancet 2005: 366; 1925
BAP
BSX
Surv
ival
(%
)
100
80
40
20
60
0
0 1 2
Time after randomisation (years)
3 4 5
Number at risk
Angioplasty
Surgery224
228
149
148
51
64
100
108
19
23
2
7
Amputation Free Survival
BAP
BSX
Surv
ival
(%
)
100
80
40
20
60
0
0 1 2
Time after randomisation (years)
3 4 5
Number at risk
Angioplasty
Surgery224
228
173
169
63
71
116
120
25
26
6
7
All-Cause Mortality

BASIL Trial: Conclusions
• No difference in primary endpoint: amputation-free
survival at 6 months
• No difference in health-related QOL
• Higher early morbidity with surgery
• Hospital costs one-third higher with bypass first
– Increased LOS, intensive therapy, wound infection
• Endovascular therapy first is considered a
reasonable approach for critical limb ischemia
Adam et al., Lancet 2005: 366; 1925
Meta-Analysis of Open versus Endovascular Approach to CLI
Hinchliffe RJ et al., Diabetes/Metabolism Research and Reviews 2012
0%
25%
50%
75%
100%
Limb Salvage at 1 Year
78%85%
Open Endovascular
49 Reports, 1980-2010
Comparison of Open Versus Endovascular Approach in CLI Patients: 5 Year Followup
Garg K et al., JVS 2014
0%
25%
50%
75%
100%
Mortality Repeat Procedures Limb Salvage
85%
55%
42%
83%
68%
48%
Open Endovascular

Trends in Revascularization 1996-2011
Goodney PP et al., JAMA Surgery 2015
Trends in Amputation 1996-2011
Goodney PP et al., JAMA Surgery 2015

How Do We Achieve Success in CLI?
Revascularization
Wound Care Medical Therapy
• What is the safest way of achieving a good result for this anatomy in this patient?
• Which vessels need to be opened?
• How durable of a result is needed?
• If different options: safest, least invasive approach first
• Don’t burn bridges to future options
CLI Management in Practice

Modern Limb Salvage Intervention
Angiosome Guided 0.014” and 0.018” Wires
Tibial/pedal Access
CTO and Re-Entry Devices

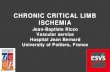
Angiosomes of the Foot and Ankle
Attinger, et al. Plast Reconstr Surg. 2006;117 (suppl): 261S–293S. Images courtesy of Dr. Mehdi H. Shishehbor
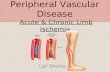
• Retrospective analysis, 203 limbs (177 patients) with ischemic ulcerations who underwent endovascular therapy
• Patients were classified into direct and indirect revascularization based on the angiosome concept
• Limb salvage was 86% when patients were directly revascularized versus 69% when indirectly revascularized (P = 0.03) for up to 4 years post-procedure
0
20
40
60
80
100
120
0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45 48 51
Fre
ed
om
fro
m A
mp
uta
tio
n (
%)
Months
Direct
Indirect
Months 0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45 48 51
At Risk D 118 82 62 53 48 39 31 23 22 13 11 8 6 3 3 2 2
I 85 59 44 31 27 19 14 11 9 9 4 4 2 2 2 2 2 1
% D 100 91.2 87.6 87.6 85.9 81.9 81.9 81.9 81.9 81.9 81.9 81.9 81.9 81.9 81.9 81.9 81.9
I 100 88.3 80.4 74.4 69.3 64.1 64.1 64.1 64.1 64.1 64.1 64.1 64.1 64.1 64.1 64.1 64.1 64.1
SE D 0.000 0.028 0.034 0.034 0.038 0.045 0.045 0.045 0.045 0.045 0.045 0.045 0.045 0.045 0.045 0.045 0.045
I 0.000 0.037 0.048 0.055 0.062 0.067 0.067 0.067 0.067 0.067 0.067 0.067 0.067 0.067 0.067 0.067 0.067
P value 0.03 0.029 0.029 0.029
Iida , et al. Catheter Cardiovasc Interv .2010; 75:830–836.
Endovascular Therapy for CLI
Based on the Angiosome Principle
Downsize Wires!
Iliac: 0.035”
Femoral/Popliteal:
0.018” or 0.035”
Tibial/Peroneal:
0.014” or 0.018”

Slippery
Intraluminal Crossing DevicesIntraluminal Crossing Devices
TruePath™ TruePath™ CTO Device
CROSSER™ CROSSCROSSER™Catheter
Frontrunner™ XP CTO
Catheter
Wildcat™ WildcWildcat™ Catheter
ces
Viance™ Crossing CrossCrossing ing Catheter

Occluded Anterior Tibial and Posterior Tibial Arteries
Antegrade R Leg Angiogram
CTO Crossing with Avinger KittyCat
Final
Baseline
Final Angiography:
After AT and PT CTO Crossing and Angioplasty

Re-Entry Devices
OffRoad™ Re-Entry ntryntryCatheter
Pioneer™ LTD Catheter
Outback™ Catheter
Enteer™ Catheter
Case: SFA Occlusive Disease
• Antegrade L femoral artery
stick
• Mid SFA total occlusion
with reconstitution in
popliteal
• Two vessel runoff
Subintimal Tracking and Re-entry (STAR)
Crossed the occluded segment, but difficulty re-entering lumen

Potential Solution:
Re-enter true lumen by utilizing a re-entry device
Scenario: Guidewire enters
subintimal space but subisubintimntimal spacepace but fails to re-enter true
lumen
Pioneer Used to Facilitate Reentry Into Distal Lumen
True lumen with Chroma Flo feature
Needle trajectory indicator
Pioneer catheter tip in subintimal space
Intima
Adventitia
> Enhanced ImagingIVUS transducer
> PositioningDual-wire system
> TargetingCurved-needle housing
> AccuracyAdjustable needle depth (1–7)
> ControlDouble-braided shaft
Pioneer adjacent toreconstituted vessel
Wire into true lumen of reconstituted vessel
Intervention with PTA/Stent
True lumen2-vessel runoff
Angioplasty5x150mm balloon
2 overlapping SE stents6x150mm x2

Final Angiography
Baseline Final
Options for CTO Access
The Front Door (antegrade)
The Side Door (subintimal & collateral)
The Back Door (retrograde)
Extensive Collateral Network

Balloon From Above, Withdraw Loop
Final Images, after PTA and Supera Stent

• Ultrasound or fluoro guidance
• Distal 1/3 of leg
• Access to tibials is easier than peroneal
• Start with micropuncture kit
• 0.014” or 0.018” wire
• Remove access as soon as feasible
• Nitro 100-300mcg per sheath
Tibial/Pedal Access
Technical Success and Safety
of Tibiopedal Access
Bazan H et al., JVS 2014; Mustapha JA et al., CCI 2014
Technic
al S
uccess
0%
25%
50%
75%
100%
Bazan H et al., 2014 Mustapha JA et al., 2014
95%
69%
13 Patients
23 Patients
No Major Access Complications
Fluoro Access
Works well with
• Suboptimal ultrasound images
• Calcified lesions
• Disease near entry site
Spectranetics Quick-Access Needle Holder

Ultrasound
Access
No radiation
Easy to distinguish arteries
from veins
Learning curve
Mustapha JA, et al, EV Today 2014
4F Cook Micropuncture
+/- Tuohy
Wire crossing
4F Terumo
Pinnacle Precision
Supportive wire crossing
Intervention: 0.014” balloon
1.25mm Diamondback
Not Sheathless!
Draping

Hemostasis: External
Courtesy of of Dr. J. Wang
Hemostasis: Internal
Courtesy of of Dr. J. Wang
Balloon inflation
3-5 minutes
Techniques for Retrograde Crossing and ConnectingRetrograde CART Reverse CART Double Balloon
FacilitatedReentry

Occluded Anterior Tibial, Posterior Tibial, and Peroneal Arteries
Crossover R Leg Angiogram: 83 y/o M with Ulcers
CTO Crossing from Posterior Tibial Retrograde Access
Angioplasty of Posterior Tibial
• Vascutrak 3x250mm scoring balloon

FinalBaseline
Final Angiography
Reverse CART Technique
Long SFA Total Occlusion Reverse CARTFinal ImagesPost Stents
85 y/o F
Not diabetic
R foot ulcer x 2y

Retrograde AT access
Unable to pass into Unable to pass into
popliteal true lumen
Double Balloon:
5x20mm and
4x30mm Fox SV
Wired from above
with Steelcore
4.5 x 60mm Supera stent in popliteal
4 x 40mm Chocolate in popliteal-AT 4 x 40mm Chocolate in popliteal-AT
3 x 40mm Armada 0.014” PTA in AT
Heavily Calcified SFA Complex Lesion

Subintimal with Wire…
Subintimal with Wire…Outback Re-entry…Failed…
Retrograde AT Access, Unable to Connect Wires

Retrograde PTA to Facilitate Outback Re-entry
Antegrade PTA and Supera Stent
Final Angiogram

Modern Limb Salvage Intervention: ATK Treatment
Atherectomy
Drug Coated Balloons
Newer SFA Stents
Specialty Balloons
Atherectomy Devices
Silverhawk
Jetstream
Diamondback
LASER
12-Month Primary Patency (K-M) for Superficial Femoral Artery Endovascular Therapies

Modern Limb Salvage Intervention: BTK Treatment
Long 0.014” Balloons/Long Inflation Times
Atherectomy
Coronary DES (as Bailout)
Specialty Balloons
Atherectomy
93 y/o F
R foot ulcer x 4 mos
Not diabetic
ABI non-comp
Orbital Atherectomy
1.25mm solid crown
Adjunctive PTA
Angiosculpt Balloon: Recalcitrant Lesions

Chocolate Balloon: Popliteal
Modern Limb Salvage Intervention: Treatment
Specialty BalloonsSpecSpecSpecSpecSpecSpecSpecSpecSpecSpecSpecSpecSpecSpecSpecialtialtialtialtialtialtialtialtialty Bay Bay Bay Bay Bay Bay Bay Bay Bay Bay Bay Bay Bay Bay Balloolloolloolloolloolloolloolloolloolloolloolloolloonsnsnsnsns
Multiple options
Little comparative data
Tailor to anatomy
• Be vigilant for PAD
• Systemic disease requires systemic treatment
• Medical therapy
• Wound care
• Cardiovascular risk assessment
• Consider revascularization early
• There is no such thing as “small vessel
disease”
Critical Limb Ischemia:
Conclusions
Related Documents