KOK SIU YAN AMY United Christian Hospital 1

KOK SIU YAN AMY United Christian Hospital 1. Introduction Classification Investigation Indication for resection Methods of resection Follow-up.
Dec 24, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
KOK SIU YAN AMY
United Christian Hospital
1

Introduction Classification Investigation Indication for resection Methods of resection Follow-up Prognosis
2

History: 1982Described by Ohashi and his colleagues
Incidence ~2.04 per 100 000 Autopsy studies 25% of cystic
pancreatic lesions 30-50% may become invasive Accounts for 5-7% of all pancreatic
neoplasm
3
Dtsch Arztebl Int. 2011 Nov;108(46):788-94.Intraductal papillary mucinous neoplasia (IPMN) of the pancreas: its diagnosis, treatment, and prognosis.Grützmann R, Post S, Saeger HD, Niedergethmann

4
Dtsch Arztebl Int. 2011 Nov;108(46):788-94..Intraductal papillary mucinous neoplasia (IPMN) of the pancreas: its diagnosis, treatment, and prognosis.Grützmann R, Post S, Saeger HD, Niedergethmann M.

First international consensus guideline in 2006 and was revised in 2012
5
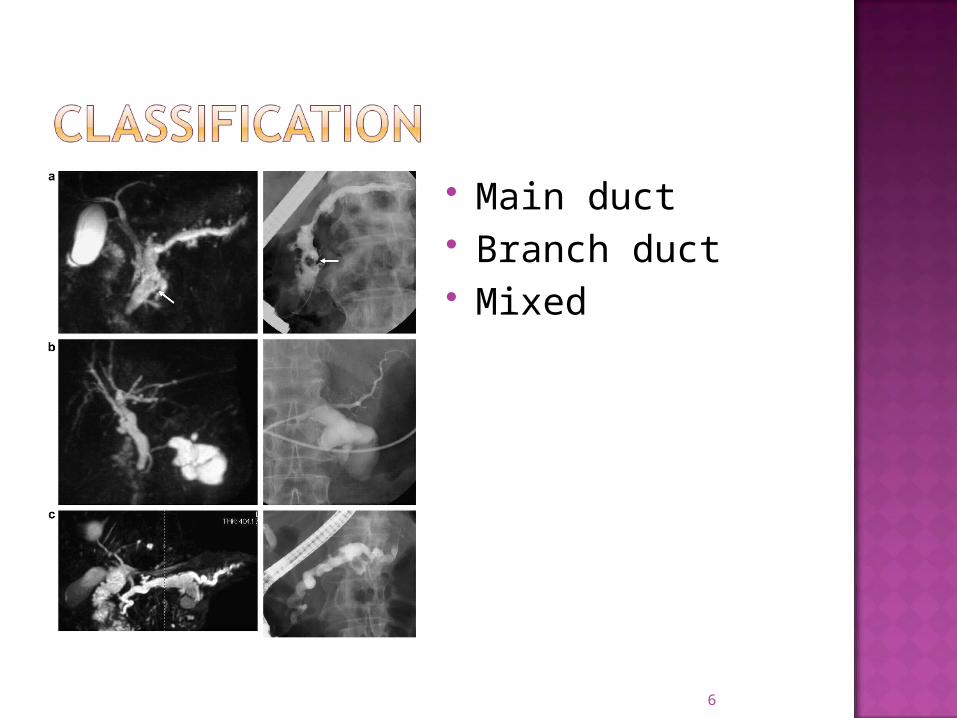
Main duct Branch duct Mixed
6

7

USG CT MRI + MRCP EUS +/- FNAC ERCP Intraductal USG or pancreatoscopy
8

USGSize and extent
CTDiffusely distended pancreatic duct with
mucinous filling defects and cystic space occupying lesions
Sensitivity 42%
9

MRI with MRCPEntire pancreatic parenchyma and the intra-
abdominal organsMore sensitive to detect mural nodulesSensitivity 88%
10
Br J Surg. 2009 Jan;96(1):5-20.Preoperative tissue diagnosis for tumours of the pancreas.Hartwig W, Schneider L, Diener MK, Bergmann F, Büchler MW, Werner J.

11
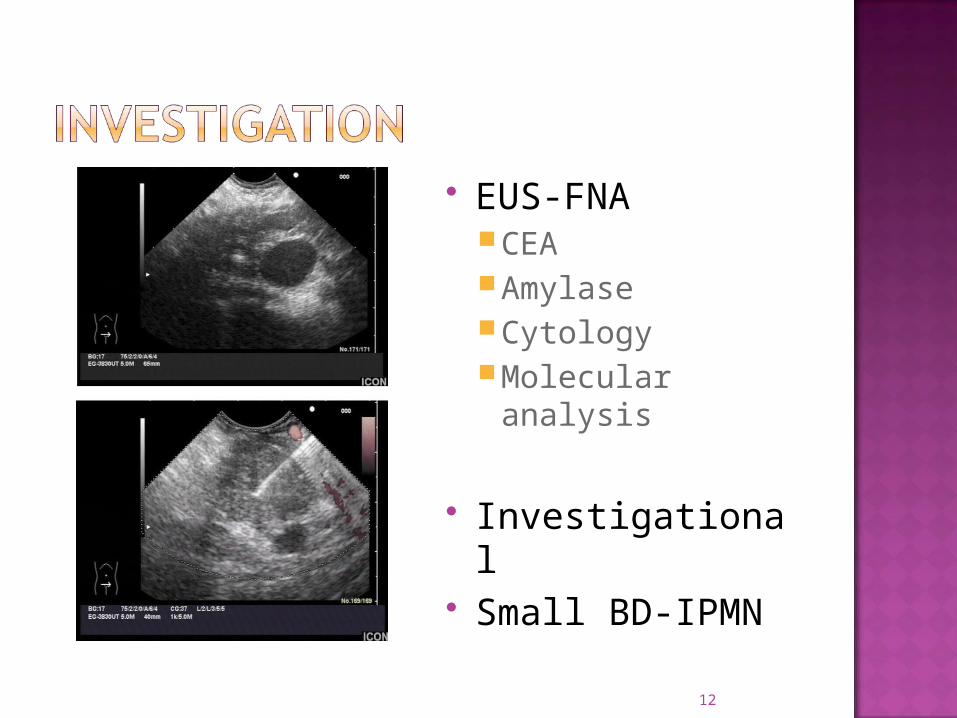
EUS-FNACEAAmylaseCytologyMolecular analysis
Investigational Small BD-IPMN
12

13
MD-IPMN BD-IPMN
14

Main duct dilatation≥1cm Frequency of malignancy: 60-92% No clinical parameters accurately
discriminate malignant and non-malignant lesion
RESECT ALL MAIN DUCT AND MIXED VARIANT IPMN
IF SURGICALLY FIT
15

16

17

18

High-risk stigmata Obstructive jaundice in patient with cystic
lesion of the head of pancreasEnhancing solid component within cystMain pancreatic duct ≥10mm in size
CONSIDER SURGERY IF CLINICALLY APPROPRIATE
19
Worrisome featuresClinical: pancreatitis Imaging:
cyst≥3cm Thickened/enhancing cyst walls Main duct size 5-9mm Non-enhancing mural nodule Abrupt change in calibre of pancreatic duct with
distal pancreatic atrophy
PERFORM ENDOSCOPIC ULTRASOUND
20

EUS features:Definite mural noduleMain duct features suspicious for
involvementCytology: suspicious or positive for
malignancy
CONSIDER SURGERY IF CLINICALLY APPROPRIATE
21

22

MD-IPMNMain duct dilatation≥5mm5-9mm worrisom features
Evaluation No immediate resection
23

According to site and extend of diseasePancreatoduodenectomyDistal pancreatectomyTotal pancreatectomy
Limited resection ExcisionEnucleationUncinatectomy
Laparoscopy
+/- lymph node dissection
24
25
Non-resected IPMN Surgically resected IPMN

26

Benign:Yearly CT/MRI
Malignant6 monthly CT/MRICEA & CA19.9 no value
27

28
Surgical margin statusnormal pancreatic tissuenon-dysplastic changes low grade dysplasiamoderate grade dysplasia invasive carcinoma
29
Repeat exam 2-5 years
Hx/PE/MRCP half-yearly
Identical to PDAC

Complete resection of noninvasive IPMN5 year survival rate 95%
Complete resection of early stage tumors(T1N0)5 year survival rate 60%
Advanced or nodal positive tumors5 year survival rate 36%
30

31

32
High-risk stigmata surgery Smaller cyst + worrisome features
EUS Cyst >3cm + NO worrisome features
EUS if elderly Cyst ≤3cm + NO worrisome features
surveillance
33

High incidence of malignant/invasive lesions (61.6%/43.1%)
Segmental ectatic type/Diffuse type with focal lesions
Diffuse type without focal lesions Frozen section Intraductal USG/pancreatoscopy
34

Mean frequency of malignancy/invasive cancer (25.5/17.7%)
Elderly Annual malignancy risk 2-3%
High risk factors:Mural nodulesHigh grade dysplasia/Positive cytology Rapidly increasing size
Individual decision
35

One 1st degree relative with PDAC 2.3-fold increased risk
high-quality MRI/MRCP or CT and EUSMalignant stigmata/worrisome features
resectionNo malignant stigmata/worrisome features
MRI/MRCP or CT at 3-month intervals EUS annually for first 2 years
36
Combination of clinical & imaging characteristics can provide preoperative diagnosis of cyst type
Multidetector CT (MDCT) & MRCP are useful for defining morphology, location, multiplicity, and communication with the MPD
Distinguishing features: multiplicity & visualisation of a connection to MPD
EUS: delineate malignant characteristics eg mural nodules & invasion but operator dependent
Cyst fluid x CEA, amylase & cytology cannot distinguish MCN & IPMN
Molecular analysis for GNAS mutations can distinguish MCN from BD-IPMN
37

3 morphological patterns:Polycystic Honeycomb Oligocystic
Distinguished from SCN with a polycystic or honeycomb pattern by CT or MRCP
Differentiation between a small oligocystic SCN & a BD-IPMN may require EUS-FNA with cyst fluid CEA determination
38
Neoplastic cysts:Non-mucinous
Serous cystic neoplasm (SCN) Solid pseudopapillary neoplasm (SPN)
Mucinous Mucinous cystic neoplasm (MCN) Intraductal papillary mucinous neoplasm
(IPMN)
39
40

Low prevalence of invasive carcinoma (<15%)
Resection is recommendedYoung Risk of progression Locations in body and tail High cost of long-term FU
Distal pancreatectomy Parenchymal-sparing resection (middle
pancreatectomy) Laparoscopic
41
Apart from imaging, elevated cyst fluid CEA is a marker that distinguishes mucinous from non mucinous cysts, but NOT benign from malignant cysts
A cut off of >/=192-200ng/ml is ~80% accurate for diagnosis of mucinous cyst
Cyst fluid amylase is shown to be not uniformly elevated in IPMN
Fluid cytology may add value especially for evaluation of a small BD-IPMN without “worrisome features”.
High grade epithelial atypia recognised in cyst fluid predicted malignancy in a mucinous cyst with 72% sensitivity in one study and detected 30% more cancers in small IPMN without worrisome features in another study
Some studies showed molecular analysis of cyst fluid may be helpful in distinguishing significant mucinous cysts from indolent cysts that can be conservatively managed
However, in view of the inconclusive evidence, this guideline suggests cyst fluid analysis is still investigational, but is recommended for evaluation of small BD-IPMN without worrisome features only in centres with expertise in EUS-FNA and cytological interpretation
42
Synchronous/metachronous malignant diseases in extra-pancreatic organs 20-30%
Frequency and location of extra-pancreatic malignancies differsGI cancer is common in AsiaSkin/breast/prostatic cancers common in US
43

This comprehensive guideline has lowered the criterion for characterising MD-IPMN to MPD dilatation of >5mm without losing specificity for radiologic diagnosis
-high risk stigmata and worrisome features have been defined to stratify risk of malignancy in BD-IPMN and consider resection or increased freq of surveillance
-resection is recommended for all surgically fit patients with MD-IPMN or MCN
Indications for resection of BD-IPMN are more conservative
BD IPMN >3cm without high risk stigmata can be observed without immediate resection
44
A previous history of diabetes, especially with insulin use, CP, and family history of PDAC are all relevant risk factors for the development of IPMN.
Am J Gastroenterol. 2013 Jun;108(6):1003-9. doi: 10.1038/ajg.2013.42. Epub 2013 Mar 5.
Risk factors for intraductal papillary mucinous neoplasm (IPMN) of the pancreas: a multicentre case-control study.
45

Good past health No history of pancreatitis No family history of pancreatic cancer Physical examination: unremarkable
46

47

Differential diagnosis
Benign– Pseudocyst– Serous cystic neoplasm (SCN)– Simple cyst, retention cyst, congential, lymphoepithelial
cyst
Potentially malignant– Intraductal papillary mucinous neoplasm (IPMN)– Mucinous cystic neoplasm (MCN)– Solid pseudopapillary neoplasm (SPN)– Neuroendocrine tumor
Malignant– Ductal adenocarcinoma
48

Pathological diagnosis (n = 212)
Fernandez-del Castillo et al. Arch Surg 2003
Intraductal papillary mucinous neoplasm (IPMN)
75 (35%)
Mucinous cystic neoplasm (MCN)
43 (19%)
Serous cystadenoma 23 (11%)
Pseudocyst 29 (14%)
Ductal adenocarcinoma 14 (7%)
Others 28 (13%)
49

WHO classification of digestive system 2010 IPMN with low or
intermediate grade dysplasia
IPMN with high grade dysplasia
IPMN with invasive cancer
50

Criterion for characterising MD-IPMN >5mm
MD-IPMN: resection BD-IPMN:
high-risk stigmata & worrisome featuresConservative
51

EUS-guided mucosal ablation by ethanol injection
Indication:Cyst >2cmUnilocular/oligolocularNo communication with MPDRefuse surgeryHigh risk surgical candidates
52

CT-defined cyst resolution rates 33-79% Variable histopathologic degrees of
epithelial ablation
Complication:Acute pancreatitis (4.5-10%)Abdominal pain (<20%)Splenic vein obliteration
53

ERCP Washing or brushing for cytology Not recommended
54

55
Related Documents











