Klinikum Stuttgart – Medizin fürs Leben Osteosarkom Stefan Bielack Zentrum für Kinder- und Jugendmedizin - Olgahospital Cooperative Osteosarkom-Studiengruppe COSS Pädiatrie 5 (Onkologie, Hämatologie, Immunologie; Allgemeine Pädiatrie, Rheumatologie, Gastroenterologie)

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Klinikum Stuttgart – Medizin fürs Leben
Osteosarkom
Stefan Bielack Zentrum für Kinder- und Jugendmedizin - Olgahospital Cooperative Osteosarkom-Studiengruppe COSS Pädiatrie 5 (Onkologie, Hämatologie, Immunologie; Allgemeine Pädiatrie, Rheumatologie, Gastroenterologie)
Osteosarkom WHO classification 2002
Conventional - chondroblastic - fibroblastic - osteoblastic - various unusual subtypes
Teleangiectatic
Secondary Small cell High grade surface Parosteal Periosteal Low grade central
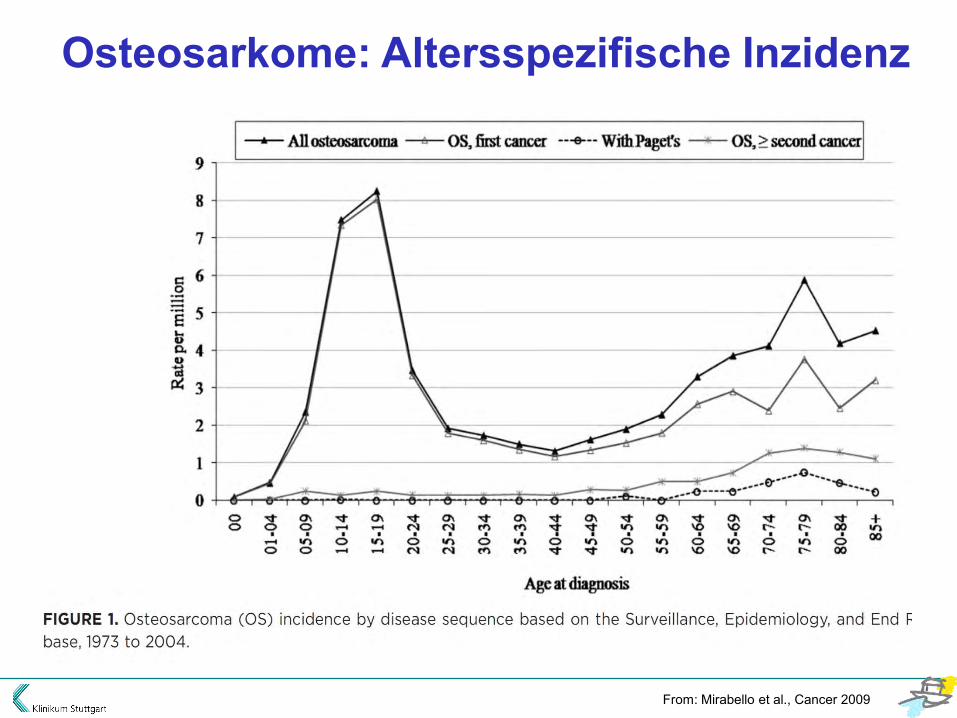
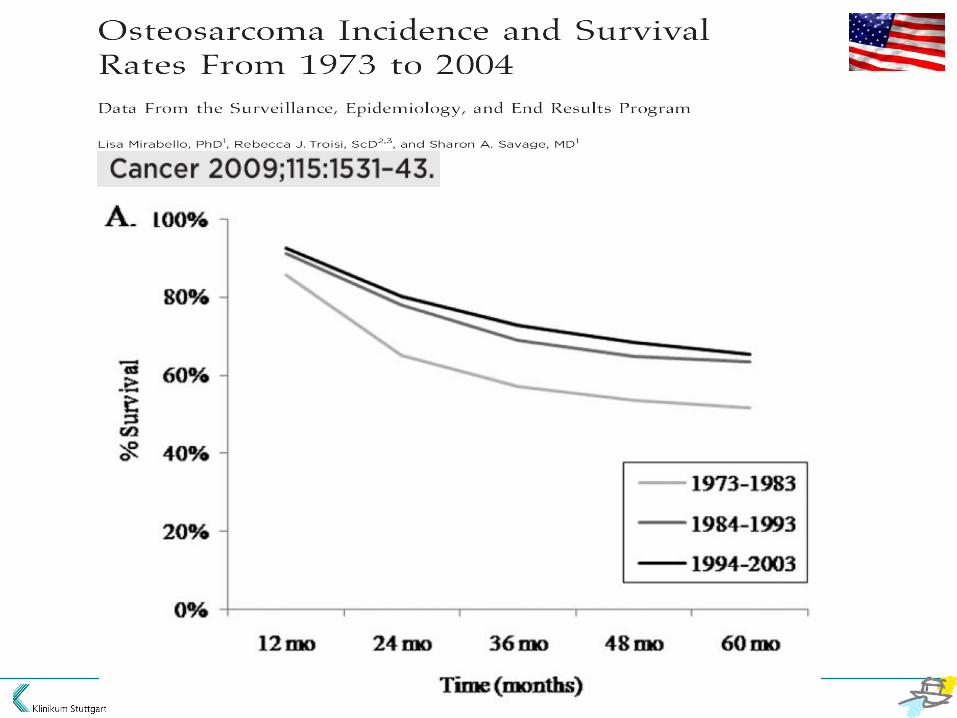
Osteosarkome: Altersspezifische Inzidenz
From: Mirabello et al., Cancer 2009
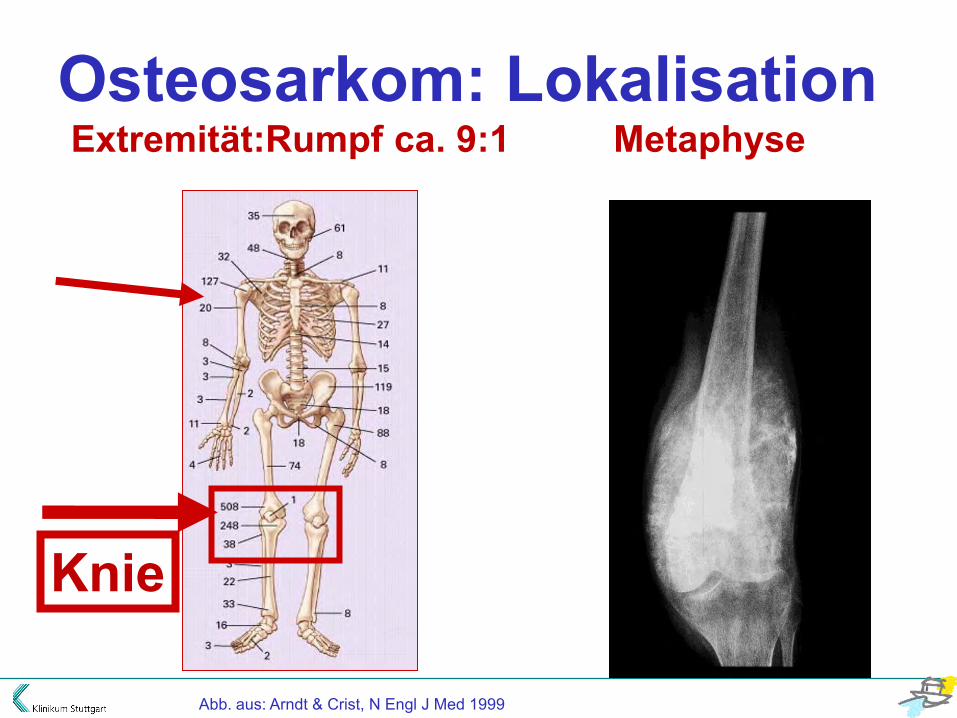
Abb. aus: Arndt & Crist, N Engl J Med 1999
Osteosarkom: Lokalisation Extremität:Rumpf ca. 9:1 Metaphyse
Knie

Osteosarkom Bildgebung: Röntgen
Methode der Wahl für ossäre
Veränderungen a Lyse/Sklerose b Codman-Dreieck c Spiculae

Osteosarkom Bildgebung: MRT
Methode der Wahl für • Weichteilkomponente • intramedulläre Ausdehnung • Beziehung zu Nerven und Gefäßen
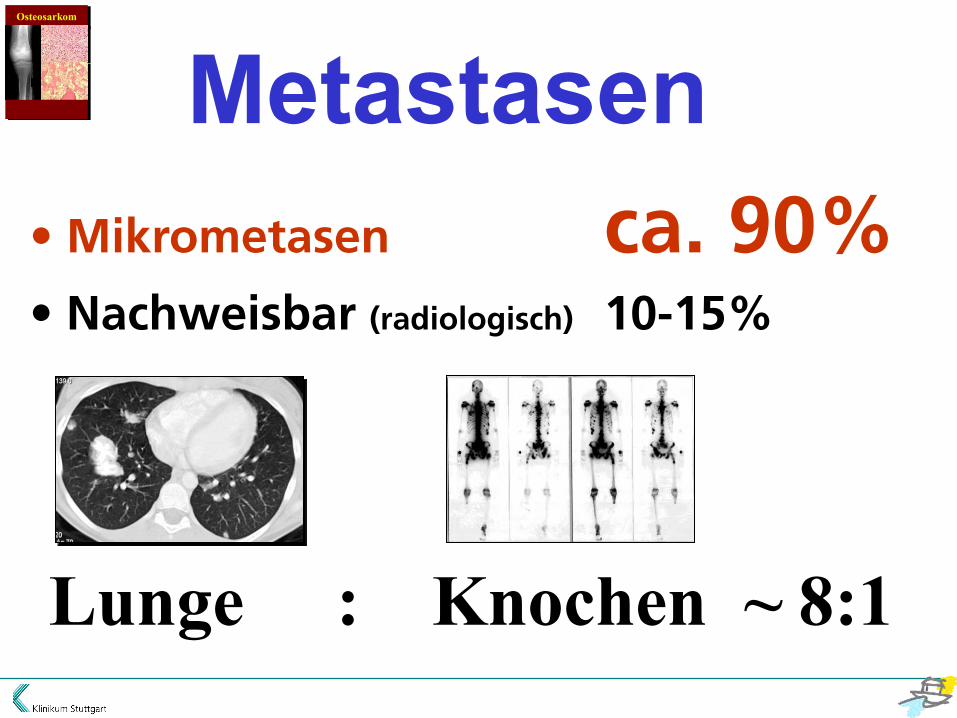
Metastasen • Mikrometasen ca. 90% • Nachweisbar (radiologisch) 10-15%
Lunge : Knochen ~ 8:1
Osteosarkom
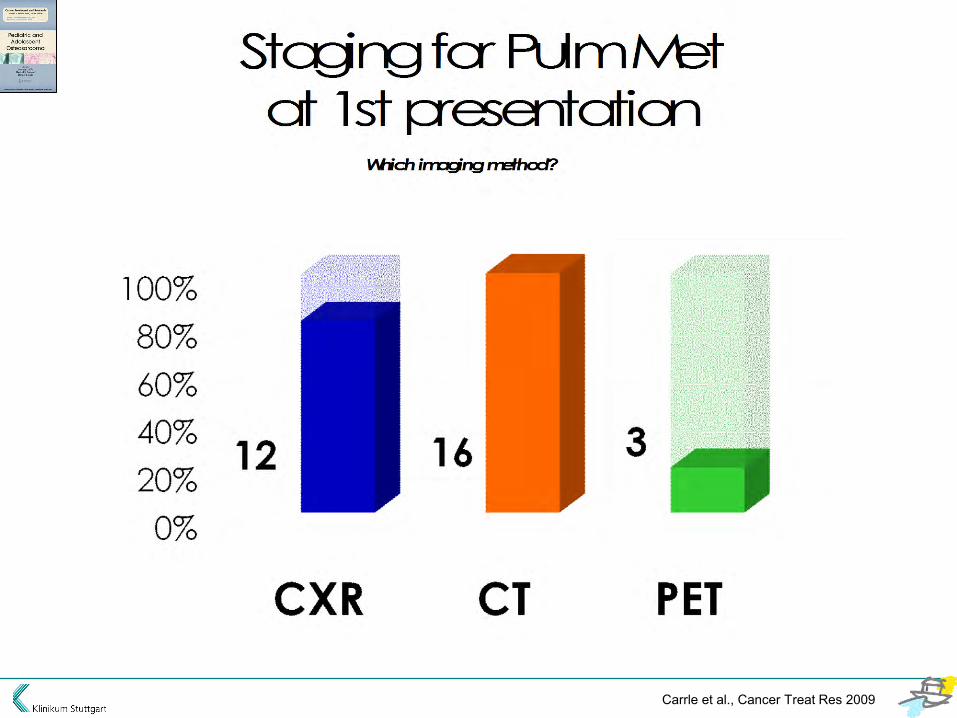
Staging for Pulm Met
at 1st presentation
Which imaging method?
Carrle et al., Cancer Treat Res 2009
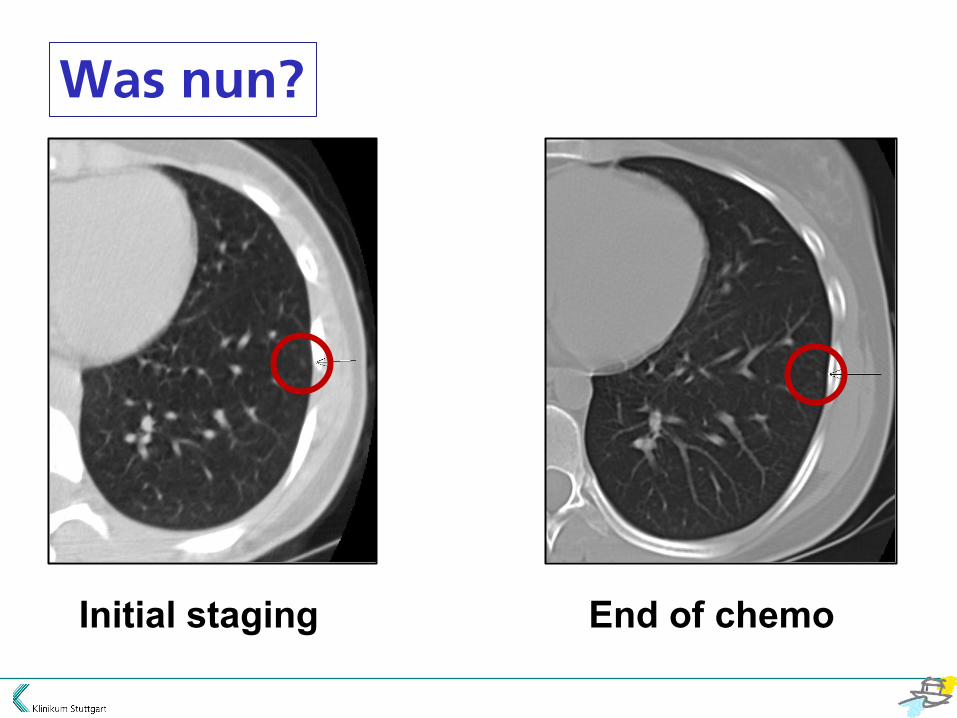
Initial staging End of chemo
Was nun?
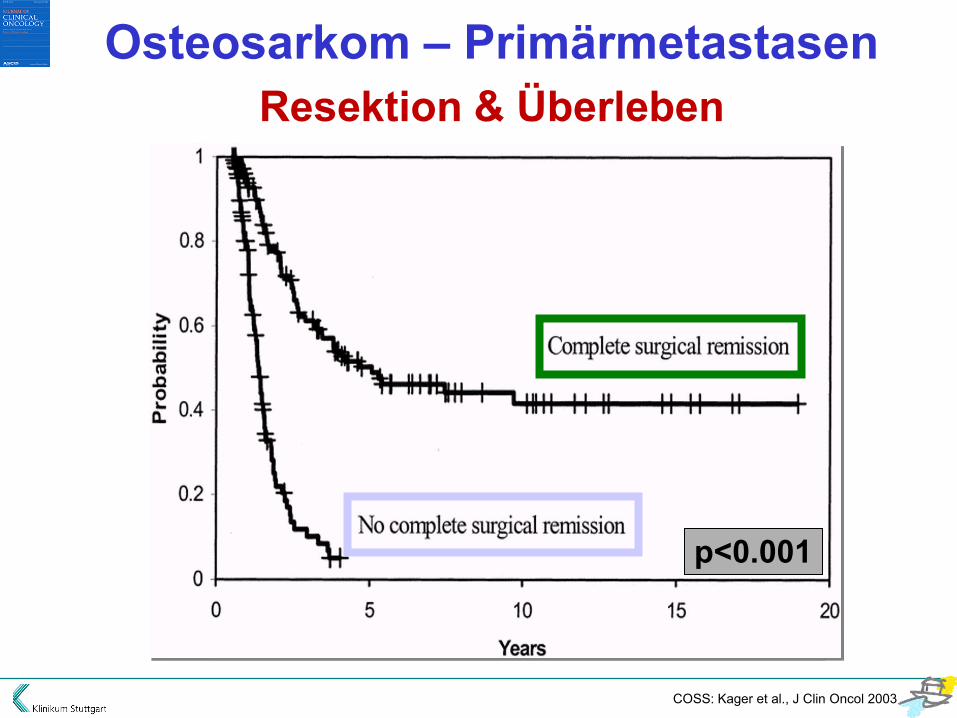
p<0.001
Osteosarkom – Primärmetastasen Resektion & Überleben
COSS: Kager et al., J Clin Oncol 2003

51 CT suspicion at surgery: 39 metastatic 22 no mets
Picci et al., Ann Oncol 12:1601-1604, 2001 Computed tomography of pulmonary metastases from osteosarcoma: the less poor technique. A study of 51 patients with histological correlation.
Nodules p
Size (</>5mm) .035* * however, 10/25 patients with nodules <5 mm had mets!
Variation in number ns
Variation in size ns

28 patients (1996-2004) 54 x thoracotomy preop. CT 183 nodules at surgery: 329 nodules / 209 osteosarcoma
Kayton et al., J Pediatr Surg. 2006 Jan;41(1):200-6 Computed tomographic scan of the chest underestimates the number of metastatic lesions in osteosarcoma.
CT vs. surgery CT overestimated 20/54 same number 15/54 CT underestimated 19/54

Osteosarcoma (lung) metastases
Take home messages
• no perfect imaging method
• often more than expected
• think bilateral
• get them out! - open thoracotomy (no VATS)
- manual palpation
- repeat if no CR
- repeat again if still no CR
Prognose?
„If you do not operate,
they die.
If you do operate, they die just the same.
Gentlemen, this meeting
should be concluded
with prayers.“
Sir Stanford Cade (1895–1973)


Chemotherapie
HD-MTX Jaffe, Cancer 1972
Doxorubicin Cortes et al., JAMA 1972 Gottlieb et al., Cancer 1972 (+DTIC) Tan et al., Cancer 1973
Cisplatin Ochs et al., Cancer Treat Rep 1978 Freeman et al., Cancer Treat Rep 1979
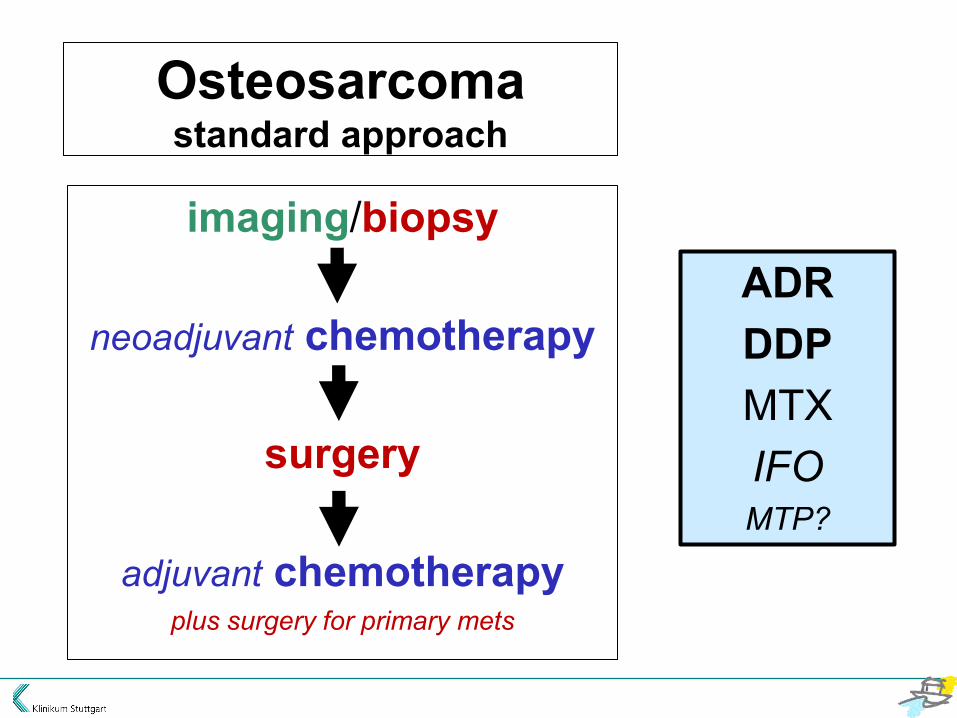
Osteosarcoma standard approach
imaging/biopsy
neoadjuvant chemotherapy
surgery
adjuvant chemotherapy plus surgery for primary mets
ADR DDP MTX IFO MTP?
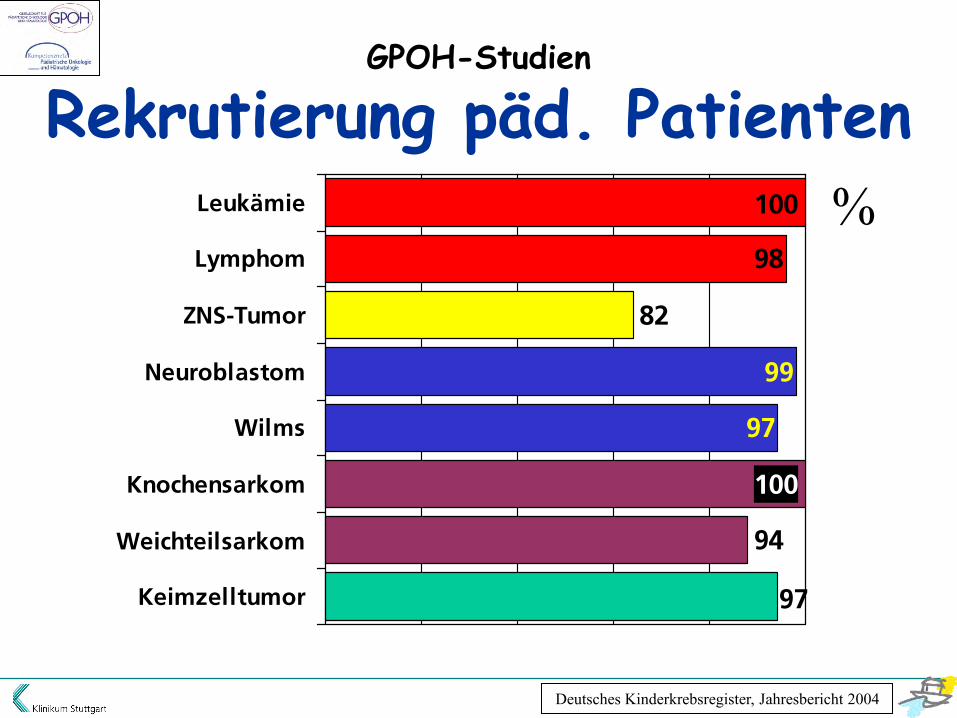
82
94
97
100
97
98
100
99
Leukämie
Lymphom
ZNS-Tumor
Neuroblastom
Wilms
Knochensarkom
Weichteilsarkom
Keimzelltumor
%
Deutsches Kinderkrebsregister, Jahresbericht 2004
GPOH-Studien
Rekrutierung päd. Patienten

GPOH-Studien
Qualitätssicherung • interdisziplinäre Therapieprotokolle (lokale & systemische Tumortherapie; Supportivtherapie)
• zentrale Referenzbeurteilung - Pathologie - Radiologie
• konsiliarische Beratung - Lokaltherapie (OP; Bestrahlung) - Chemotherapie

ICH Topic E6 Guideline for Good Clinical Practice

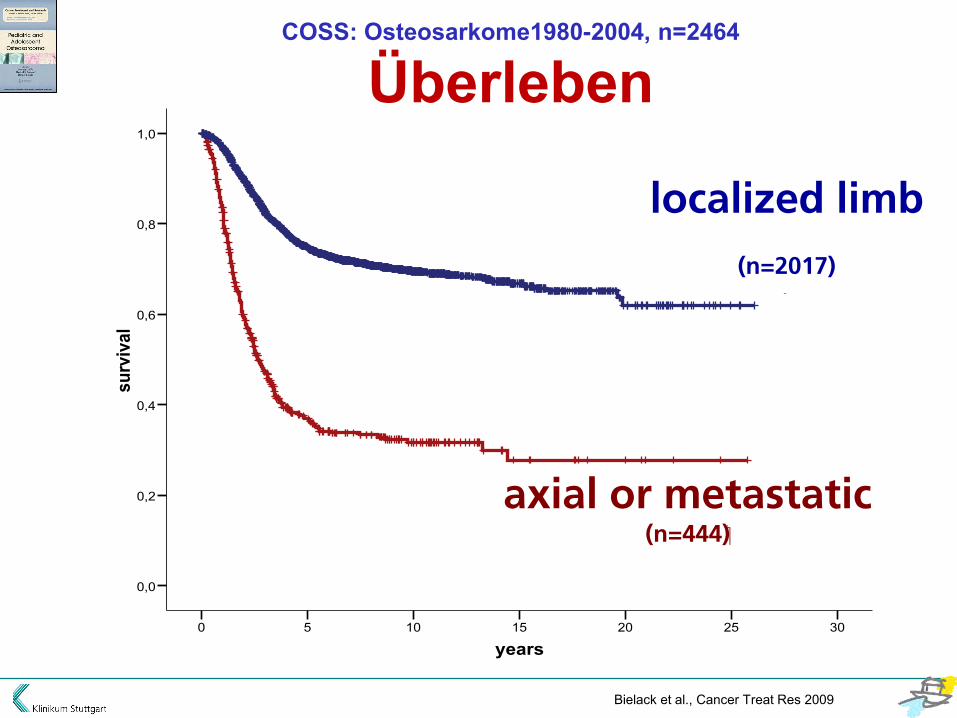
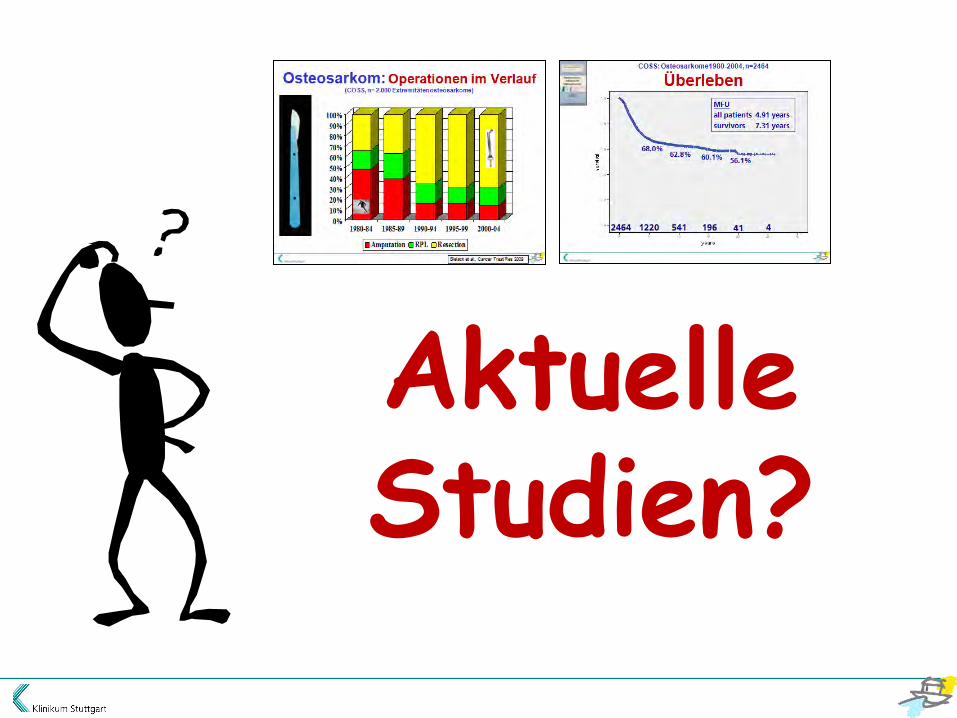
COSS: Osteosarkome1980-2004, n=2464
Überleben
years302520151050
surv
ival
1,0
0,8
0,6
0,4
0,2
0,0
68.0% 62.8% 60.1% 56.1%
MFU
all patients 4.91 years
survivors 7.31 years
41 1220 541 196 4 2464

37
58 59 61
0
10
20
30
40
50
60
70
1978-1982 1983-1987 1988-1992 1993-1997
Osteosarcoma in Europe 5-year survival rates
years302520151050
surv
ival
1,0
0,8
0,6
0,4
0,2
0,0
localized extremity
axial or / and primary metastatic
localized limb
(n=2017)
axial or metastatic (n=444)
COSS: Osteosarkome1980-2004, n=2464
Überleben
Bielack et al., Cancer Treat Res 2009

Pelvis-Osteosarkom: Lokalversagen
COSS: Ozaki et al., J Clin Oncol 2003

Lokaltherapie

0%10%20%30%40%50%60%70%80%90%
100%
1980-84 1985-89 1990-94 1995-99 2000-04
Amputation RPL Resection
Osteosarkom: Operationen im Verlauf (COSS, n= 2.000 Extremitätenosteosarkome)
Bielack et al., Cancer Treat Res 2009
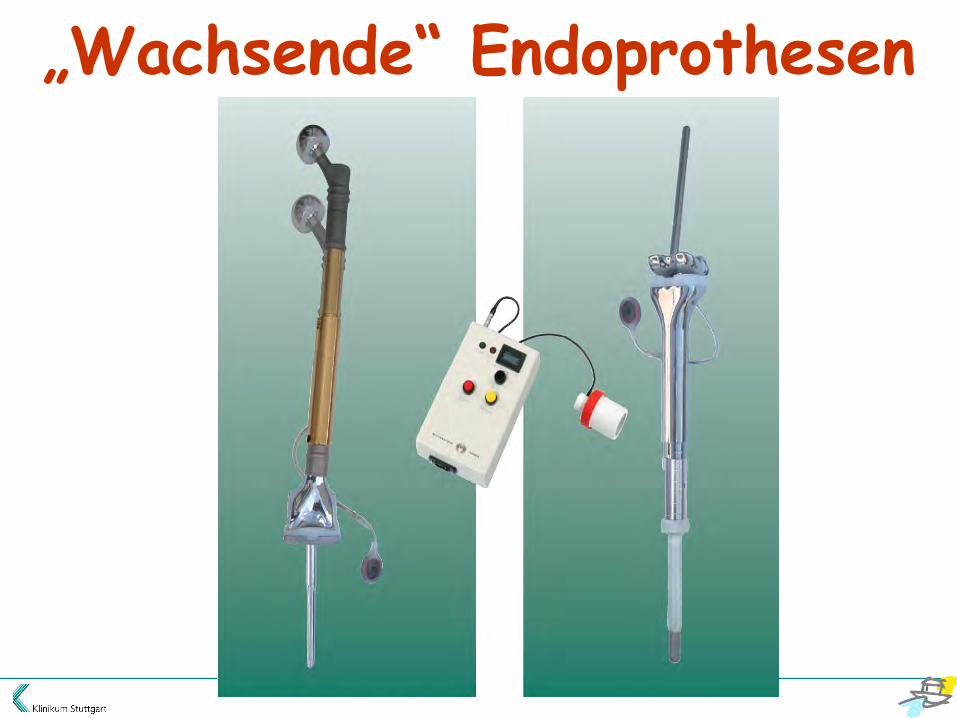
„Wachsende“ Endoprothesen

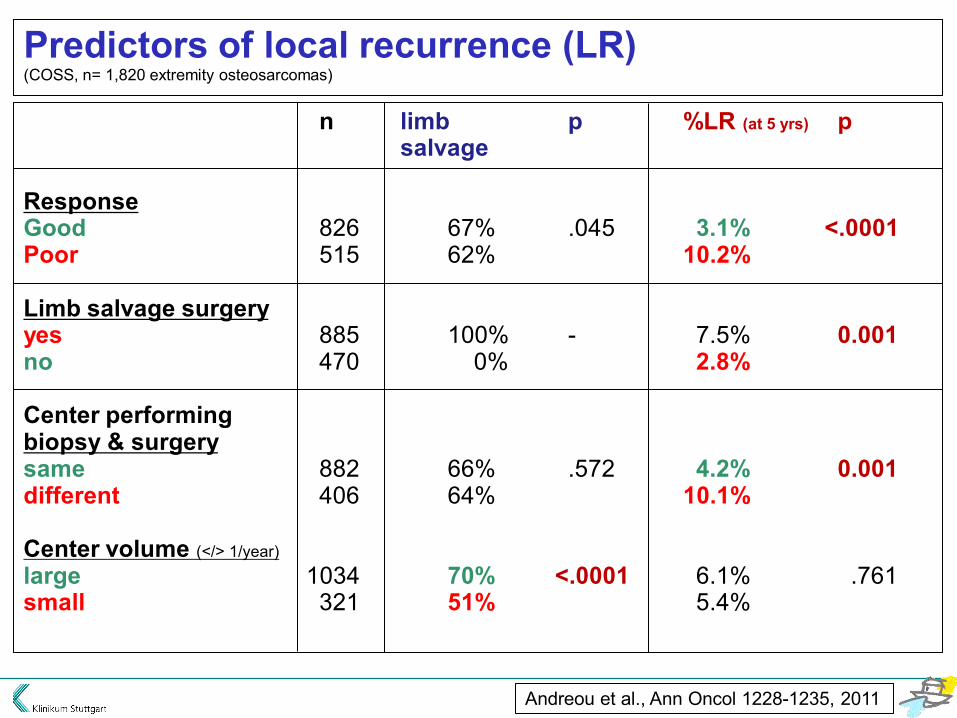
n limb p %LR (at 5 yrs) psalvage
ResponseGood 826 67% .045 3.1% <.0001Poor 515 62% 10.2%
Limb salvage surgeryyes 885 100% - 7.5% 0.001no 470 0% 2.8%
Center performingbiopsy & surgerysame 882 66% .572 4.2% 0.001different 406 64% 10.1%
Center volume (</> 1/year)
large 1034 70% <.0001 6.1% .761small 321 51% 5.4%
Andreou et al., Ann Oncol 1228-1235, 2011
Predictors of local recurrence (LR)(COSS, n= 1,820 extremity osteosarcomas)
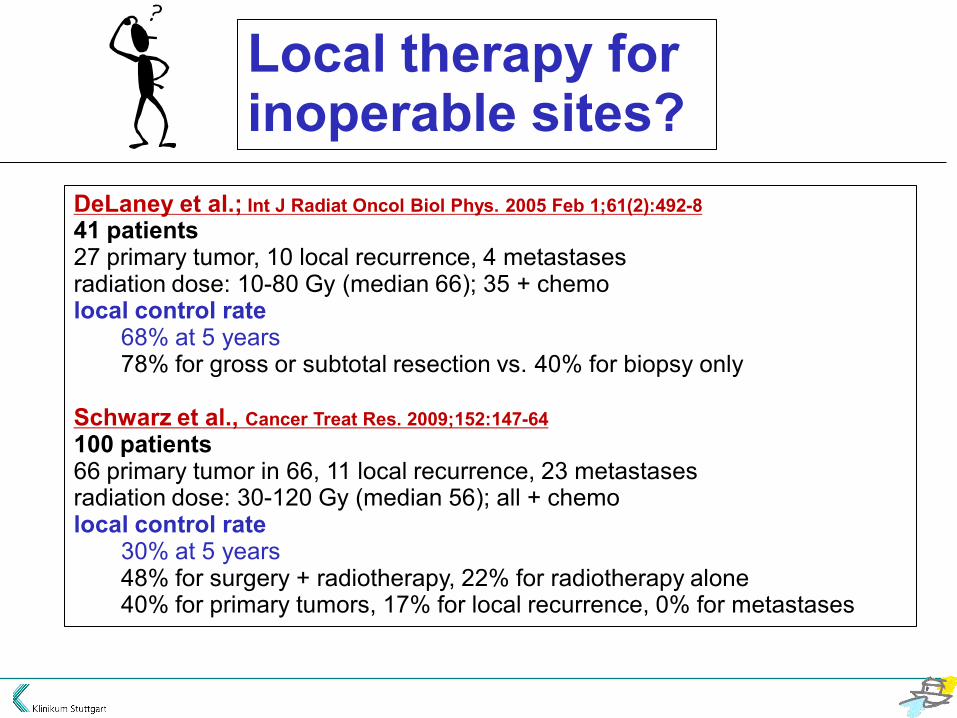
Local therapy for inoperable sites?
DeLaney et al.; Int J Radiat Oncol Biol Phys. 2005 Feb 1;61(2):492-841 patients27 primary tumor, 10 local recurrence, 4 metastasesradiation dose: 10-80 Gy (median 66); 35 + chemolocal control rate
68% at 5 years 78% for gross or subtotal resection vs. 40% for biopsy only
Schwarz et al., Cancer Treat Res. 2009;152:147-64100 patients 66 primary tumor in 66, 11 local recurrence, 23 metastasesradiation dose: 30-120 Gy (median 56); all + chemolocal control rate
30% at 5 years48% for surgery + radiotherapy, 22% for radiotherapy alone40% for primary tumors, 17% for local recurrence, 0% for metastases

Osteosarcoma local therapyTake home messages
• operate, operate, operate!• limb salvage is often feasible• local recurrence risk can be reduced
- by good imaging- by smart planning- by good chemo- by good surgery
• radiotherapy may be an option for selectedinoperable lesionsstudies with proton / heavy ion radiotherapy ongoing
Systemische Therapie

Osteosarcoma standard approach
imaging/biopsy
neoadjuvant chemotherapy
surgery
adjuvant chemotherapy plus surgery for primary mets
ADR DDP MTX IFO MTP?
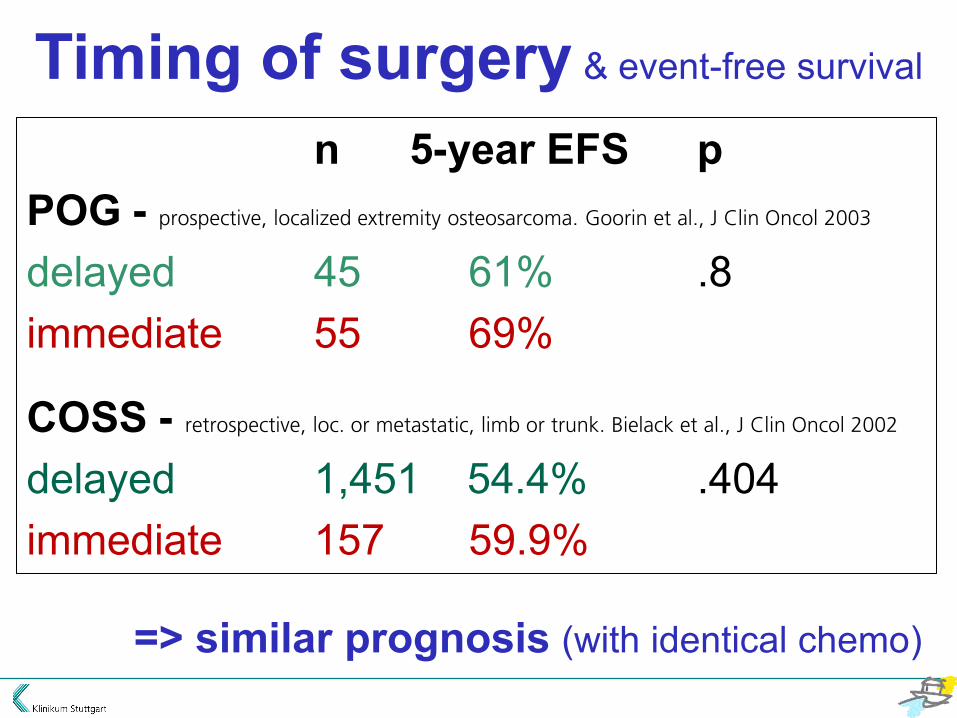
n 5-year EFS p POG - prospective, localized extremity osteosarcoma. Goorin et al., J Clin Oncol 2003
delayed 45 61% .8 immediate 55 69%
COSS - retrospective, loc. or metastatic, limb or trunk. Bielack et al., J Clin Oncol 2002
delayed 1,451 54.4% .404 immediate 157 59.9%
=> similar prognosis (with identical chemo)
Timing of surgery & event-free survival

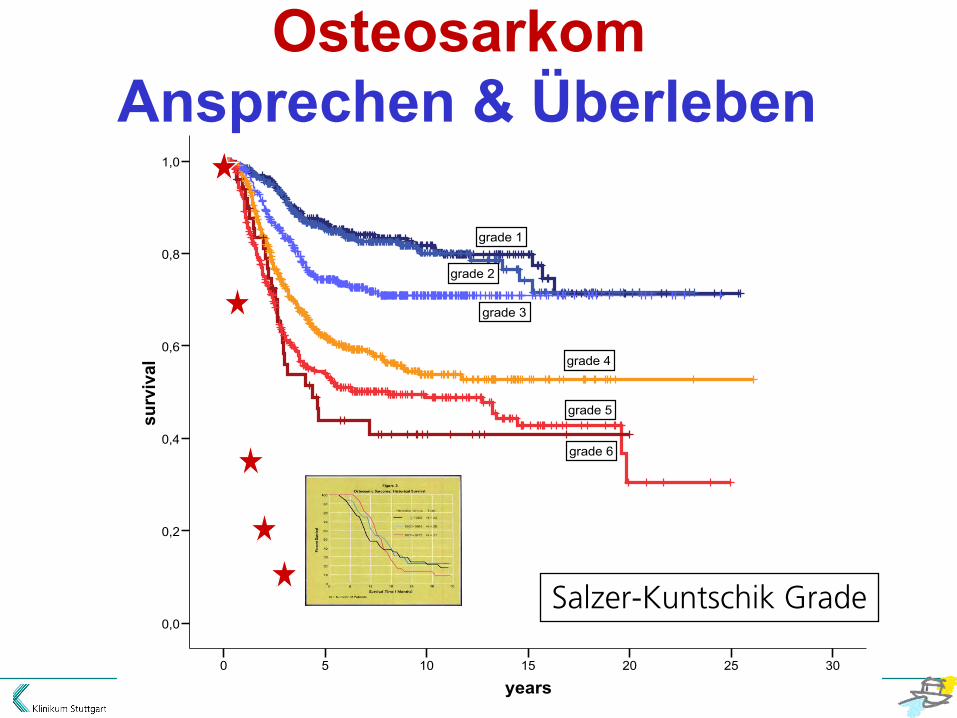
Ansprechen auf Therapie ist ein wichtiger
prognostischer Faktor
biopsy surgical specimen
years302520151050
surv
ival
1,0
0,8
0,6
0,4
0,2
0,0
grade 1
grade 2
grade 3
grade 4
grade 5
grade 6
Salzer-Kuntschik Grade
Osteosarkom Ansprechen & Überleben
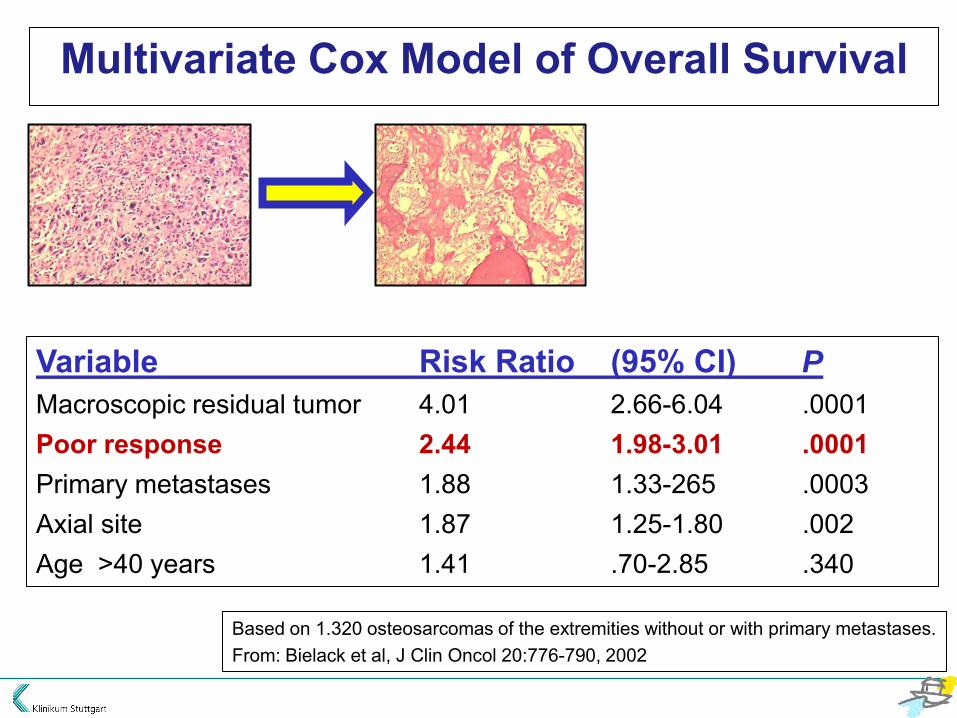
Variable Risk Ratio (95% CI) P
Macroscopic residual tumor 4.01 2.66-6.04 .0001 Poor response 2.44 1.98-3.01 .0001 Primary metastases 1.88 1.33-265 .0003 Axial site 1.87 1.25-1.80 .002 Age >40 years 1.41 .70-2.85 .340
Based on 1.320 osteosarcomas of the extremities without or with primary metastases. From: Bielack et al, J Clin Oncol 20:776-790, 2002
Multivariate Cox Model of Overall Survival
Dosis-Intensität?

Chemotherapy at standard or increased dose intensity in patients with operable osteosarcoma of the extremity – MRC BO06 EORTC 80931
Chart Title
4 cycles ofCDDP+DOX
Surgery (week 6)
2 cycles ofCDDP+DOX
Standard Arm
3 Cycles ofCDDP+DOX+G-CSF
Surgery (week 6)
3 Cycles ofCDDP+DOX+G-CSF
Intensified Arm
RANDOMISE
Biopsy-proven, non-metastaticosteosarcoma of the extremity
G-CSF?
EOI: Lewis et al., JNCI 2007
n(risk)Regimen 1245(64)169(46)112(17) 82 (2) 68 (5) 49 (1) 32 (0) 21Regimen 2252(55)185(56)117(15) 91 (5) 76 (4) 55 (1) 45 (0) 30
0.0
0.2
0.4
0.6
0.8
1.0
Ppn a
live a
nd pr
ogre
ssion
-free
0 12 24 36 48 60 72 84Time from randomisation (months)
Regimen 1 Regimen 2
All patients and timed from randomisation
KM plot of progression-free survival


Conclusion: Dose-Intensity • importance remains unproven G-CSF & interval compression • not useful in Osteosarcoma
Aktuelle Studien?
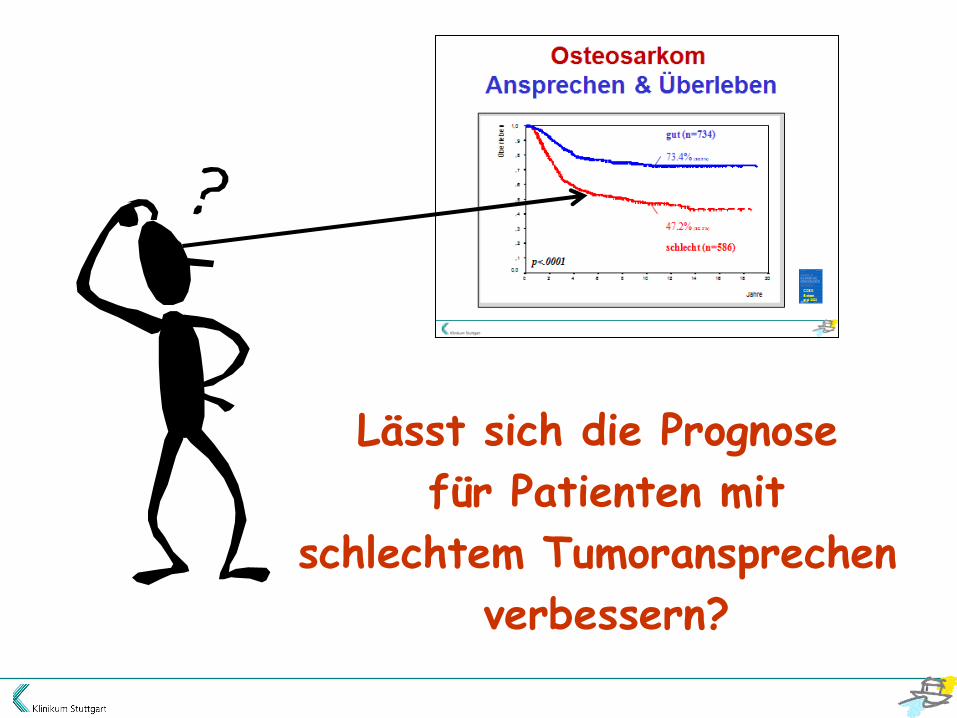
Lässt sich die Prognose
für Patienten mit
schlechtem Tumoransprechen
verbessern?
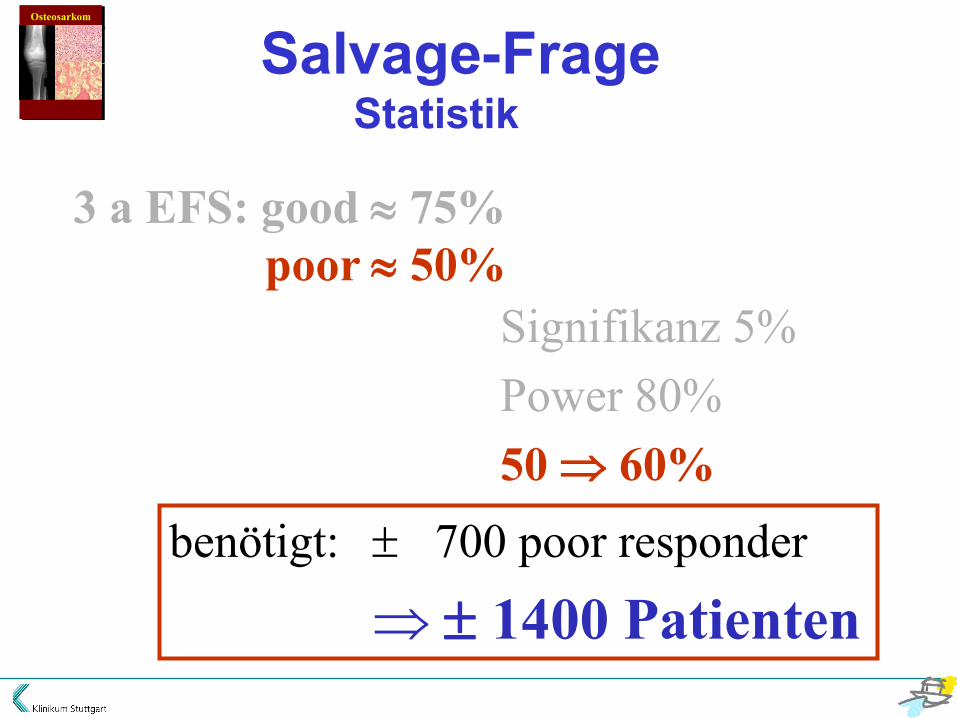
3 a EFS: good 75% poor 50%
Signifikanz 5% Power 80% 50 60%
Salvage-Frage Statistik
Osteosarkom
benötigt: 700 poor responder
1400 Patienten

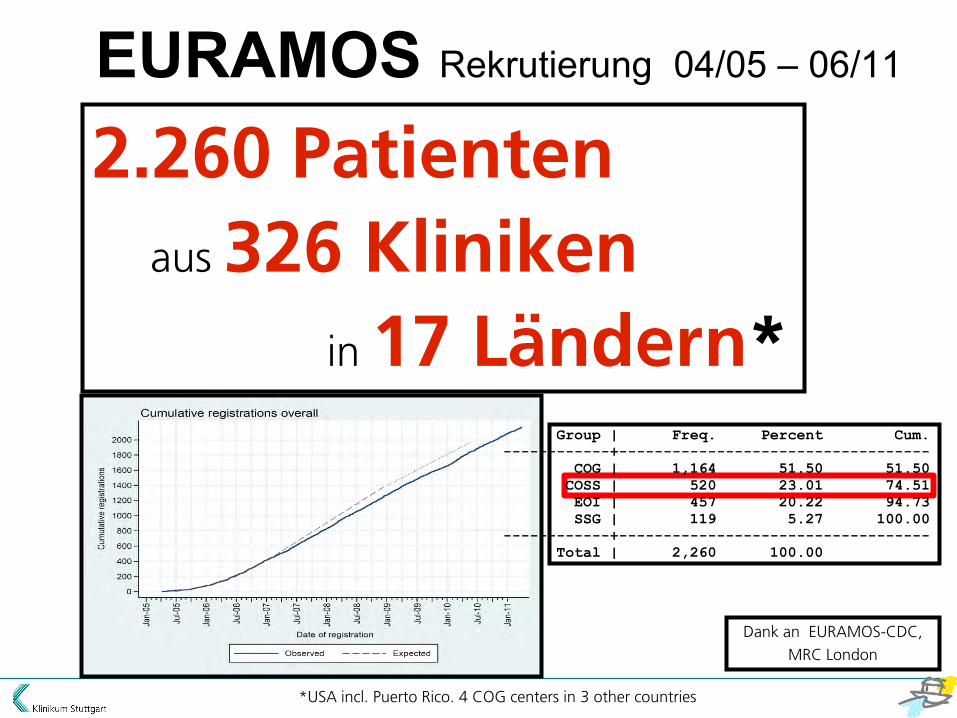
EURAMOS Rekrutierung 04/05 – 06/11
Dank an EURAMOS-CDC,
MRC London
2.260 Patienten
aus 326 Kliniken
in 17 Ländern*
*USA incl. Puerto Rico. 4 COG centers in 3 other countries
Group | Freq. Percent Cum.
------------+-----------------------------------
COG | 1,164 51.50 51.50
COSS | 520 23.01 74.51
EOI | 457 20.22 94.73
SSG | 119 5.27 100.00
------------+-----------------------------------
Total | 2,260 100.00

Sum 346/2,260 = 15.3% of total recruitment
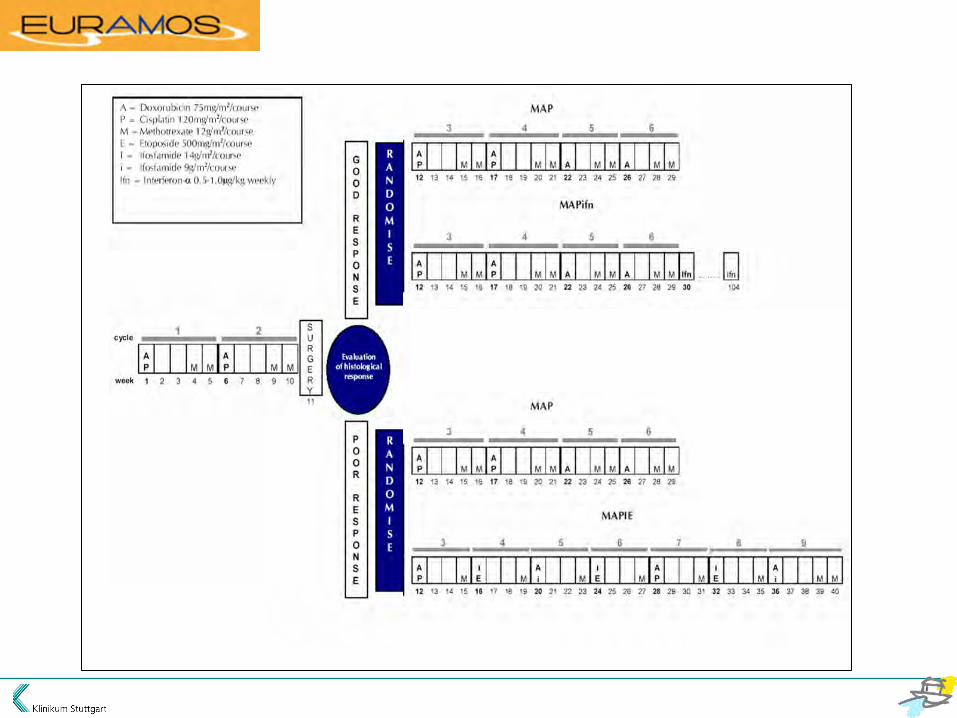
EURAMOS1
Top 10 Recruiters

EURAMOS Patients per center per year
>5 n = 3 (0.9%)
4-<5 n = 2 (0.6%)
3-<4 n = 14 (4.3%)
2-<3 n = 34 (10.4%)
1-<2 n = 90 (27.4%)
<1 n= 185 (56.4%)
(spring 2011 estimates)

ISG
Italian Sarcoma Group
COSS
Cooperative OSteosarcoma Study
SSG
Scandinavian Sarcoma Group
EURO-B.O.S.S. EUROpean Bone Over 40 Sarcoma Study A European treatment protocol for bone sarcomas in patients older than 40 years
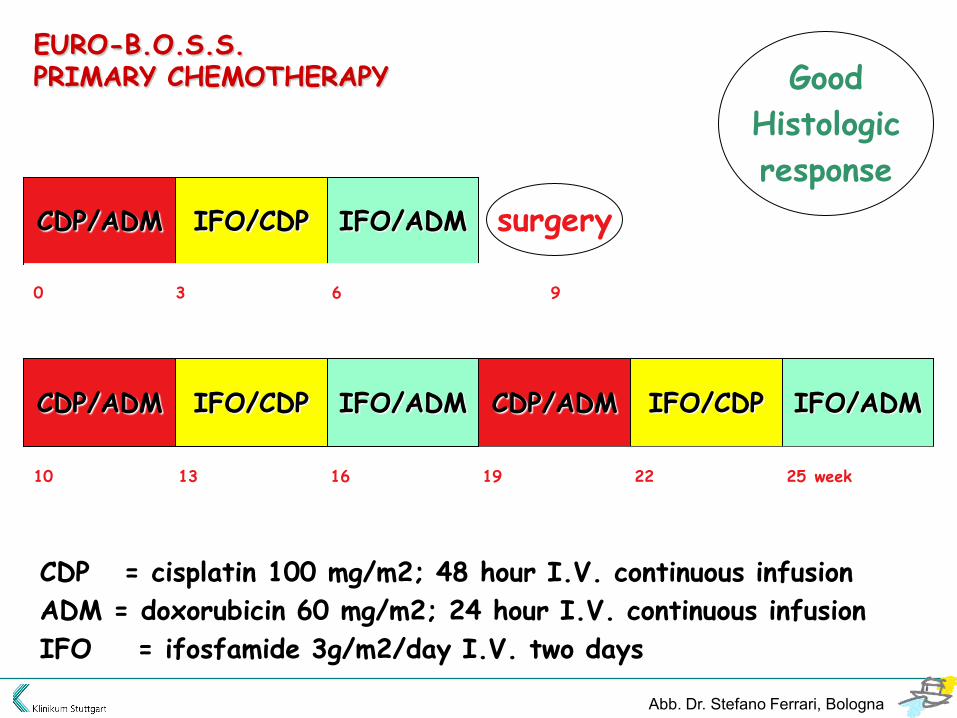
CDP/ADM
IFO/ADM IFO/CDP CDP/ADM
IFO/CDP IFO/ADM
0 3 6 9
10 13 16 19 22 25 week
CDP = cisplatin 100 mg/m2; 48 hour I.V. continuous infusion
ADM = doxorubicin 60 mg/m2; 24 hour I.V. continuous infusion
IFO = ifosfamide 3g/m2/day I.V. two days
EURO-B.O.S.S. PRIMARY CHEMOTHERAPY
CDP/ADM IFO/CDP IFO/ADM
surgery
Good
Histologic
response
Abb. Dr. Stefano Ferrari, Bologna

CDP/ADM
MTX IFO/ADM MTX
IFO/CDP IFO/ADM
0 3 6 9
10 13 14 17 18 21
CDP = cisplatin 100 mg/m2; 48 hour I.V. continuous infusion ADM = doxorubicin 60 mg/m2; 24 hour I.V. continuous infusion IFO = ifosfamide 3g/m2/day I.V. two days MTX = Methotrexate 8 g/m2; 4 hours I.V
EURO-B.O.S.S. PRIMARY CHEMOTHERAPY
CDP/ADM MTX IFO/CDP
surgery
Very Poor
Histologic
response
IFO/ADM MTX CDP/ADM MTX IFO/CDP
22 25 26 29 30 week
Abb. Dr. Stefano Ferrari, Bologna
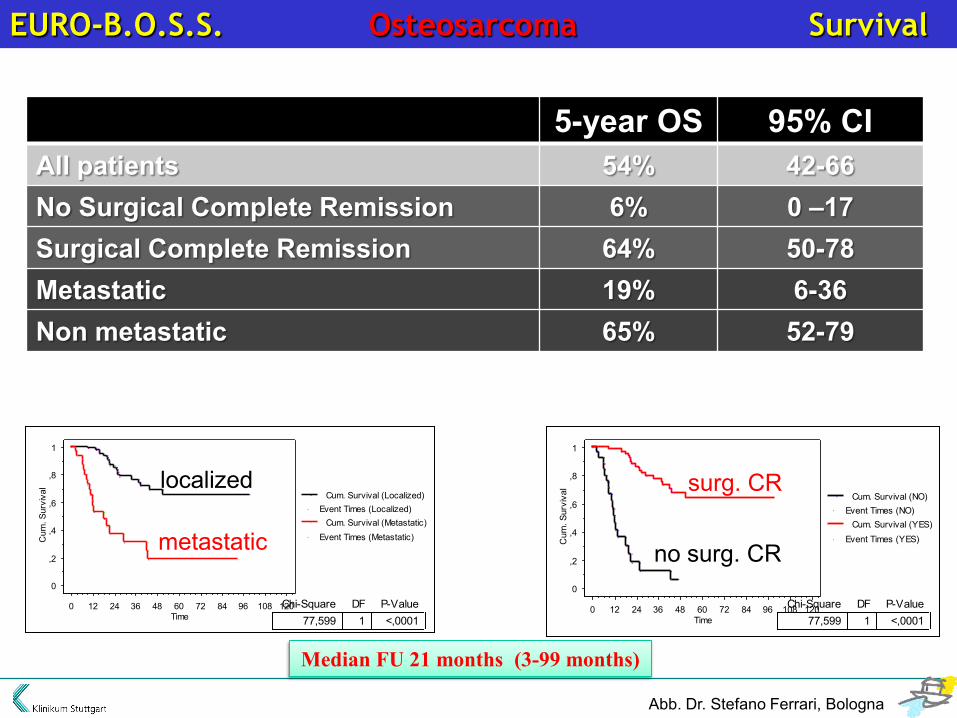
EURO-B.O.S.S. Osteosarcoma Survival
5-year OS 95% CI All patients 54% 42-66 No Surgical Complete Remission 6% 0 –17 Surgical Complete Remission 64% 50-78 Metastatic 19% 6-36 Non metastatic 65% 52-79
Median FU 21 months (3-99 months)
0
,2
,4
,6
,8
1
Cum
. Sur
viva
l
0 12 24 36 48 60 72 84 96 108 120Time
Event Times (Metastatic)Cum. Survival (Metastatic)
Event Times (Localized)Cum. Survival (Localized)
0
,2
,4
,6
,8
1
Cum
. Sur
viva
l
0 12 24 36 48 60 72 84 96 108 120Time
Event Times (YES)Cum. Survival (YES)
Event Times (NO)Cum. Survival (NO)
77,599 1 <,0001Chi-Square DF P-Value
77,599 1 <,0001Chi-Square DF P-Value
localized
metastatic
surg. CR
no surg. CR
Abb. Dr. Stefano Ferrari, Bologna

EURO-B.O.S.S.
EUROpean Bone Over 40 Sarcoma Study
INCLUSION CRITERIA
Histologically proven diagnosis of high grade sarcoma of bone.
Histologic types:
Osteosarcoma (central primary and secondary, high
grade surface), Fibrosarcoma, Malignant Fibrous
Histiocytoma, Leiomyosarcoma, Dedifferentiated
Chondrosarcoma.
Age: ≥ 41 - 65
Normal Bone marrow, hepatic and renal function;
Absence of contraindications to the use of cisplatin, adriamycin,
ifosfamide and methotrexate
Informed consent
Abb. Dr. Stefano Ferrari, Bologna
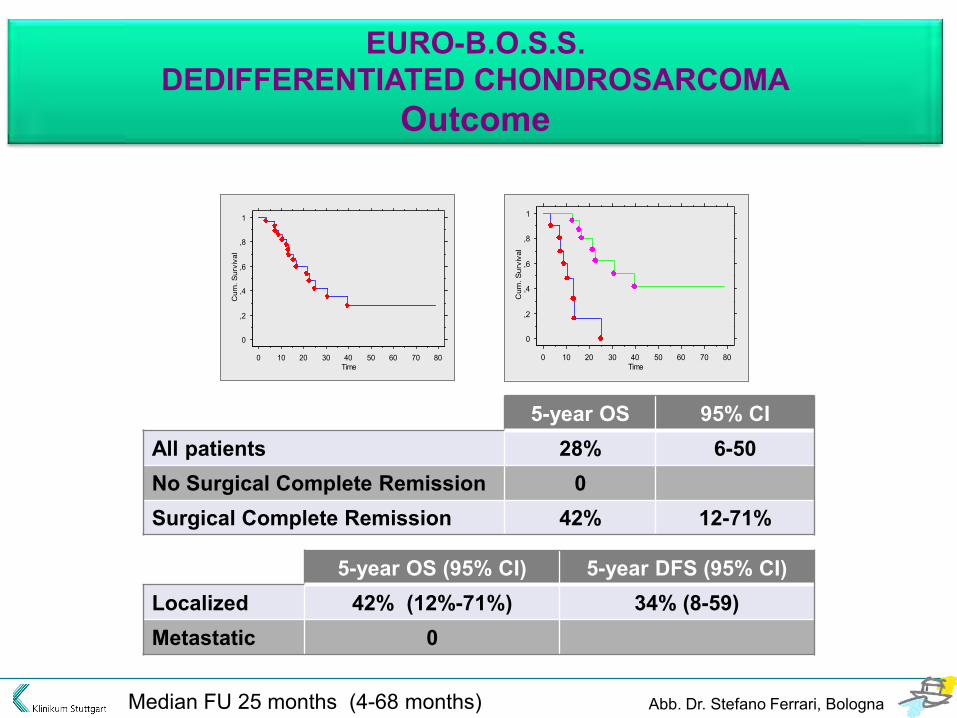
EURO-B.O.S.S. DEDIFFERENTIATED CHONDROSARCOMA
Outcome
5-year OS 95% CI All patients 28% 6-50 No Surgical Complete Remission 0 Surgical Complete Remission 42% 12-71%
5-year OS (95% CI) 5-year DFS (95% CI) Localized 42% (12%-71%) 34% (8-59) Metastatic 0
Median FU 25 months (4-68 months)
0
,2
,4
,6
,8
1
Cum
. Sur
viva
l
0 10 20 30 40 50 60 70 80Time
0
,2
,4
,6
,8
1
Cum
. Sur
viva
l
0 10 20 30 40 50 60 70 80Time
Abb. Dr. Stefano Ferrari, Bologna

EURO-B.O.S.S.
Largest prospective study on osteosarcoma patients >40 Chemotherapy intensive, about 30% of patients require dose-reductions High incidence of peripheral neurotoxicity, not described in younger populations Use of MTX feasible, but rate of delayed excretion higher than in younger patients Pathological response rate lower than reported in younger patients In patients with SCR a 64% 5-year probability of survival can be expected Similar probability of survival in case of primary chemotherapy or upfront surgery Poor probability of survival in metastatic patients and in patients with pelvic tumors
Nichts Neues
beim Osteosarkom?
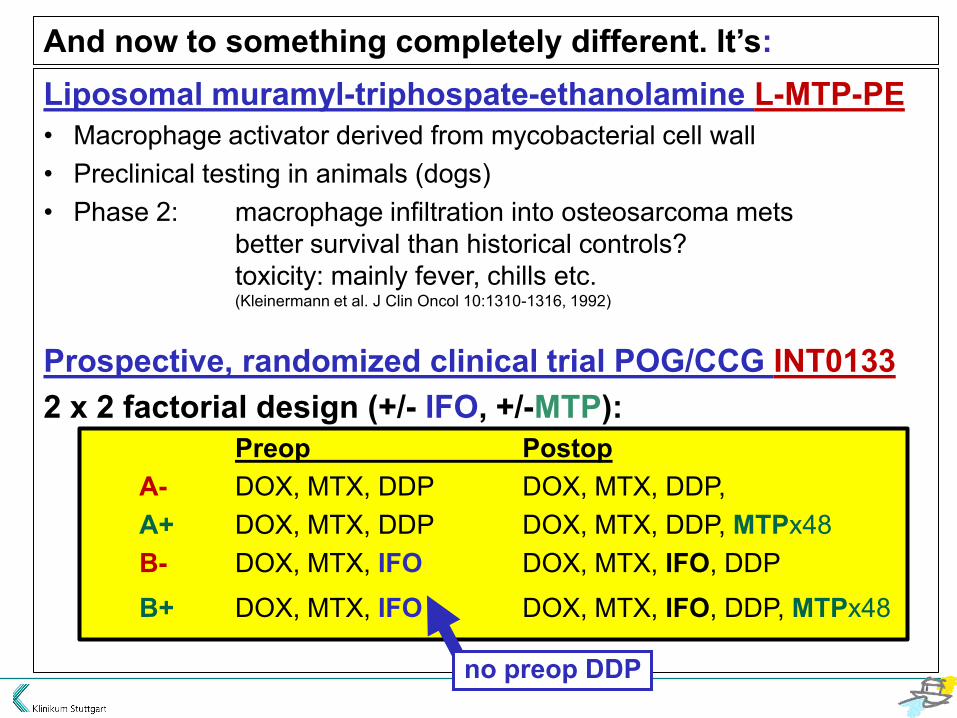
Liposomal muramyl-triphospate-ethanolamine L-MTP-PE • Macrophage activator derived from mycobacterial cell wall • Preclinical testing in animals (dogs) • Phase 2: macrophage infiltration into osteosarcoma mets
better survival than historical controls? toxicity: mainly fever, chills etc. (Kleinermann et al. J Clin Oncol 10:1310-1316, 1992)
Prospective, randomized clinical trial POG/CCG INT0133 2 x 2 factorial design (+/- IFO, +/-MTP): Preop Postop A- DOX, MTX, DDP DOX, MTX, DDP, A+ DOX, MTX, DDP DOX, MTX, DDP, MTPx48 B- DOX, MTX, IFO DOX, MTX, IFO, DDP
B+ DOX, MTX, IFO DOX, MTX, IFO, DDP, MTPx48
no preop DDP
And now to something completely different. It’s:

INT 0133 Meyers et al., J Clin Oncol 23:2004-2011, 2005
n = 667 localized osteosarcomas; primary end point EFS
EFSregimen n 3-year 5-yearA- - 172 71% 64%A+ MTP 168 68% ca. 65%
B- IFO 167 61% 53%B+ IFO, MTP 170 78% 72%
addition of IFO to standard chemotherapy did not enhance EFS
addition of MTP to chemotherapy might improve EFS, but interaction between IFO and MTP
“Apossible biologic explanation for the observed outcome involves the interaction between fas and fas ligand. Lafleur et al showed that 4-hydroperoxy-cyclophosphamide, an active metabolite of oxazaphosphorine chemotherapy, enhances fas ligand expression in an OS cell line. This upregulation was not observed with doxorubicin, cisplatin, or methotrexate. They found that MTP stimulates multiple cytokines, including interleukin (IL) -12, and that IL-12 upregulates expression of fas in an OS cell line selected for high probability to metastasize. Administration of ifosfamide and MTP could activate the fas/fas-ligand pathway that initiates apoptosis. This hypothesis suggests that we should investigate other agents with the potential to affect IL-12 and the fas/fas-ligand pathway.”

INT 0133 Meyers et al., J Clin Oncol 26:633-638, 2008
n = 662 localized resectable osteosarcoma; end points EFS & overall survival
EFS overall survivalregimen 4-year 6-year 4-year 6-yearA- - 66% 64% 78% 71%A+ MTP 65% 63% 82% 75%B- IFO 60% 58% 77% 70%B+ IFO, MTP 74% 71% 86% 81%
EFS overall survivalregimen 4-year 6-year 4-year 6-yearA-/B- no MTP 63% 61% 78% 70%A+/B+ MTP 69% 67% 84% 78%
no statistical evidence of interactionproportional hazards regression analysis P =.102 (EFS), .60 (overall survival)
p=.08 p=.03
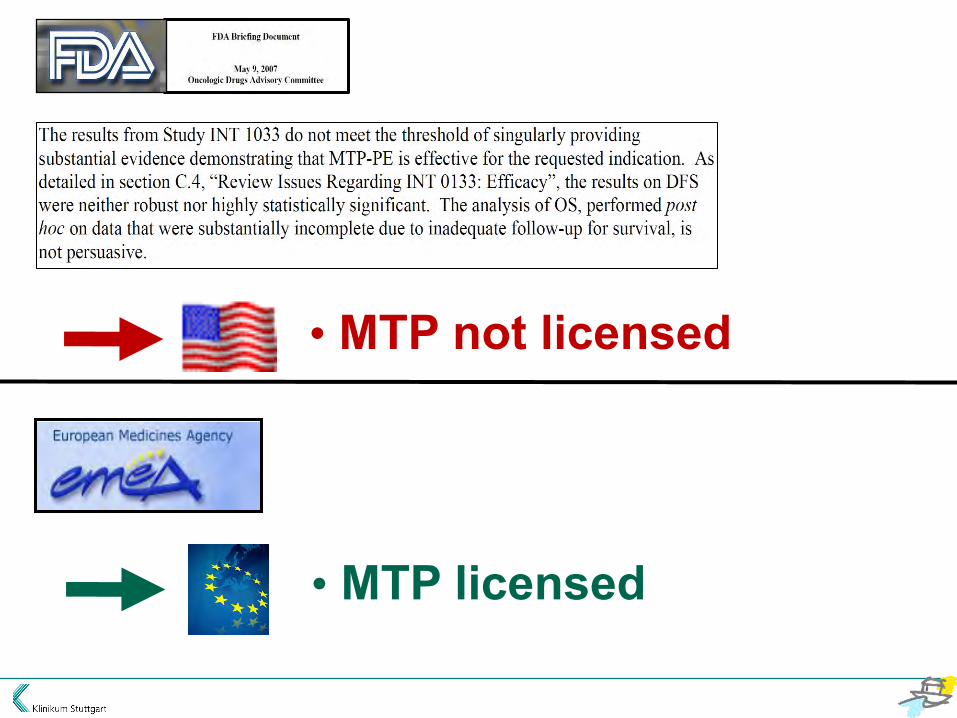

• Europe: licensed by EMEA• congratulations to Dr. Meyers and the
Children’s Oncology Group for the successful completion of the phase III study and the high quality data that provide the basis for seeking marketing approval of the first drug ever developed specifically for osteosarcoma(Romet-Lemonne, Mills, Fridman, Munsell, J Clin Oncol 2005)
• - first treatment to improve survival in 20 years- reduces the risk of death by almost one third compared with chemotherapy alone(Takeda press release, Feb. 1, 2010)
• robust evidence of young adult survival advantage(Davies, Neidle, Taylor, Br J Cancer 2012)
• USA: license refused by FDAnot sufficient evidence of a survival advantage (US Food and Drug Administration, 2007)
• does not meet generally accepted standards for practice-changing conclusions (Hunsberger, Freidlin, Smith, J Clin Oncol 2008)
• additional clinical evaluations are required before the agent can be considered for routine use (Bielack, Marina, Ferrari, Helman, Smeland, Whelan, Reaman, J Clin Oncol 2008)
• ineffective and harmful (Prescrire International, 2011)
• should patients and health care systems be subjected to the additional burdens associated with therapies that have not been evaluated as thoroughly as one would like? (Bielack, Eur J Cancer 2010)
L-MTP-PE (mifamurtide)
Price in Germany: 3.223€ inkl. VAT, x 48 = 154.700€

„… it could have been feared that the viability of the EURAMOS trial of established therapies would be impaired if more osteosarcoma patients were able to access MTP (Bielack*, 2010). But this would be a perverse reason for delaying marketing approval for MTP, given the robust evidence of young adult survival advantage available.” Davies JE, Neidle S, Taylor DG (2012) Minireview: Developing and paying for medicines for orphan indications in oncology: utilitarian regulation vs equitable care? Br J Cancer 106: 14 – 17
* misquoted from: Eur J Cancer 46:1942– 1945, 2010
„… it could have been feared that the viability of the EURAMOS trial of established therapies would be impaired if more osteosarcoma patients were able to access MTP (Bielack*, 2010). But this would be a perverse reason for delaying marketing approval for MTP, given the robust evidence of young adult survival advantage available.” Davies JE, Neidle S, Taylor DG (2012) Minireview: Developing and paying for medicines for orphan indications in oncology: utilitarian regulation vs equitable care? Br J Cancer 106: 14 – 17
* misquoted from: Eur J Cancer 46:1942– 1945, 2010
• ASSG • COG • COSS • EOI • GEIS • ISG • JCOG • SARC • SFCE • SSG
Osteosarcoma Meeting London, March 2010
• Intergroup infrastructure • Study question(s): first choice: chemo +/- MTP
Europäisches „FP7“ Forschungsnetzwerk
Knochentumor-“Work Package“: Leitung Klinikum Stuttgart - Olgahospital

Klinikum Stuttgart – Medizin fürs Leben
Danke für Ihre Aufmerksamkeit!
Danke an M. Paulussen, H. Jürgens für Dias!

COSS-Background • upfront treatment intensity important
• intensive 4-drug chemo (DOX, MTX, DDP, IFO)
• COSS-86:
72% overall & 66% event-free survival risk factors tumor volume & response

Questions • long-term toxic treatment necessary for all?
• salvage therapy effective for high-risk patients?
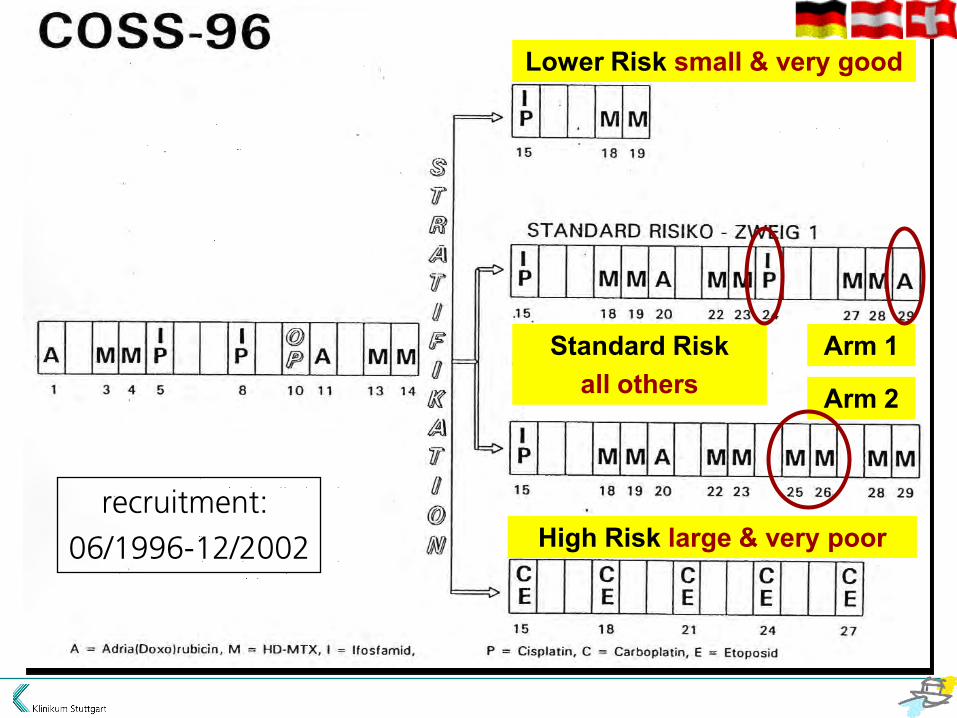
recruitment:
06/1996-12/2002
Lower Risk small & very good
High Risk large & very poor
Arm 1
Arm 2
Standard Risk all others

COSS-96 (all 443 patients): Survival 5a: 82.5% (SE: 1.9)
5a: 70.8% (SE: 2.2)
Overall
Event-Free
Is “salvage” with carboplatin/etoposide
beneficial for “high-risk”
patients?
COSS-96: „high risk“ (large, very poor reponse: carbo/eto salvage)
A 1
2
M 3
M 4
IP 5
6
7
IP 8
9
surg. 10
A 11
12
M 13
M 14
CE 15
16
17
CE 18
19
20
CE 21
22
23
CE 24
25
26
CE 27

COSS-96 High-Risk: Survival
55.6% (SE13.6) Overall
43.1% (SE 13.2) Event free
COSS-96: Conclusion high risk“
• outcome not worse than expected <-> 17% 5y.-overall survival
• inclusion criteria too rigid (15 patients/6 years)
• too few patients to draw definitive conclusions
Can therapy be abbreviated for
“lower-risk” patients?
COSS-96 „lower risk“: Survival expected EFS 97%

COSS-96: EFS by risk group
Lower 77.7% (SE: 5.3)
Standard
High

Even patients with favorable prognostic indicators seem to require „full“ treatment to achieve optimal results
COSS-96: Conclusion “lower risk“

Is it safe to replace DOX, DDP and IFO
by MTX during late phase of
chemotherapy?
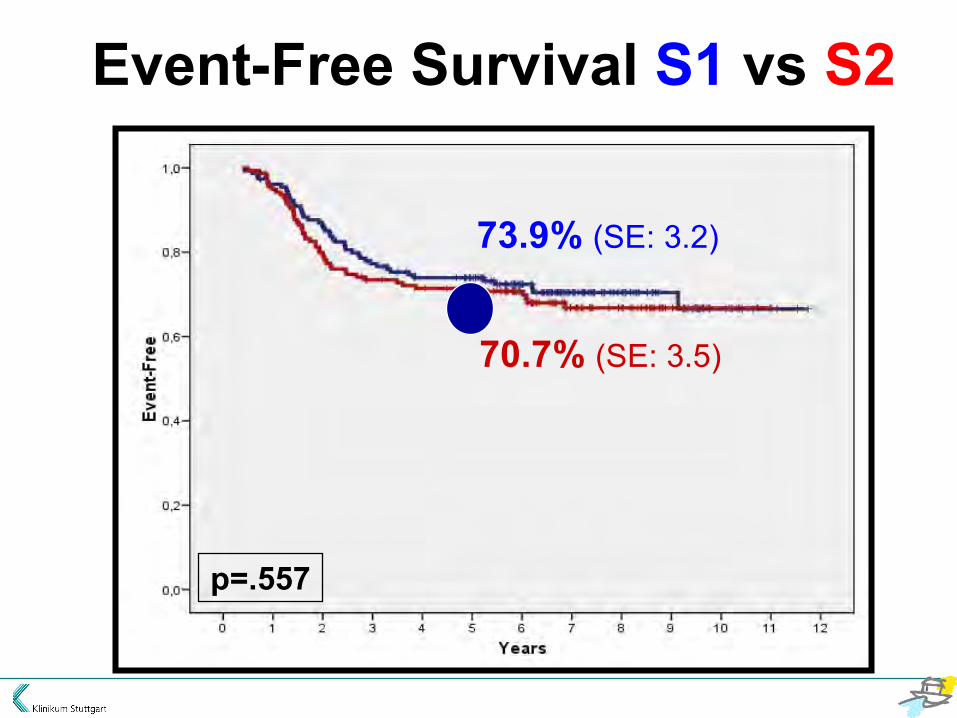
70.7% (SE: 3.5)
73.9% (SE: 3.2)
p=.557
Event-Free Survival S1 vs S2

COSS-96 Conclusion „Standard Risk“
• no significant difference between SR treatment arms
• „late“ MTX plausible alternative in case of toxicity
Related Documents











