KITLG Mutations Cause Familial Progressive Hyper- and Hypopigmentation Mustapha Amyere 1 , Thomas Vogt 2,5 , Joe Hoo 3 , Flemming Brandrup 4 , Anette Bygum 4 , Laurence Boon 1 and Miikka Vikkula 1 Familial progressive hyper- and hypopigmentation (FPHH) is thought to be an autosomal dominant disorder with reduced penetrance. Clinical signs consist of progressive diffuse, partly blotchy hyperpigmented lesions, multiple cafe ´ -au-lait spots, intermingled with scattered hypopigmented-appearing maculae, and lentigines. FPHH is distinct from familial progressive hyperpigmentation (FPH), in which no hypopigmented features are present, and which is phenotypically and histologically closer to Dyschromatosis Universalis Hereditaria 2 (DUH2). It also differs from the Legius syndrome, characterized by familial cafe ´ -au-lait spots and skin fold freckling, caused by mutations in SPRED1. We performed a genome-wide linkage analysis in seven families with FPHH, and identified linkage on 12q21.12-q22, which overlaps with the DUH2 locus. We investigated whether KITLG in the locus is mutated in FPHH. We discovered three different mutations in four families. A reported FPH substitution was observed in two FPHH families, and two, to our knowledge, previously unreported substitutions, p.Val33Ala and p.Thr34Pro, cosegregated with FPHH in two separate families. All three mutations were located in a conserved b-strand in KITLG, suggesting its important role in the activation of the KITLG receptor c-Kit. In aggregate, mutations in a single gene cause various pigmentation disorders: FPH, FPHH, and likely DUH2. Therefore, KITLG is an important modulator of skin pigmentation. Journal of Investigative Dermatology (2011) 131, 1234–1239; doi:10.1038/jid.2011.29; published online 3 March 2011 INTRODUCTION We have reported a distinct pigmentation disorder familial progressive hyper- and hypopigmentation (FPHH) associated with lentigines in three families from a small area in southeastern Germany, suggesting a founder effect (Zanardo et al., 2004). Transmission was compatible with autosomal dominant inheri- tance with variable expression (Figure 1). FPHH is characterized by diffuse hyperpigmentation with variable intensity. Cafe ´-au-lait macules and larger hypopigmented ash-leaf macules are also present. These features occur on the face, neck, trunk, and limbs, and they are present at birth or early in infancy. The lesions increase in size and number with age (Figure 2). Similar inherited hypomelanotic and hypermelanotic cutaneous macules associated with retarded growth and mental deficiency have been reported in one family (OMIM 154000; (Westerhof et al., 1978). Two additional reminiscent inherited phenotypes have been reported: autosomal dominant familial progressive hyperpigmentation (FPH, OMIM 145250), characterized by progressive hyperpigmen- tation similar to that seen in FPHH, but without hypopig- mented lesions, and autosomal recessive Dyschromatosis Universalis Hereditaria 2 (DUH2, OMIM 612715), charac- terized by depigmented and hyperpigmented features that appear during infancy. Histologically, hyperpigmented lesions display strong basal pigmentation of the epidermis with numerous melanin-filled melanophages. In contrast, the hypopigmented-appearing maculae show a slight basal hyperpigmentation of the epidermis, with virtually no melanophages in the upper dermis (Stuhrmann et al., 2008; Wang et al., 2009). Two loci have been identified for FPH: one on chromo- some 19p13-pter (Guo et al., 2006) and another on 12q21.31-q23.1 (Wang et al., 2009). DUH2 was subse- quently linked to the latter (Bukhari et al., 2006; Stuhrmann et al., 2008). In this locus, a single KITLG amino-acid substitution, p.Asn36Ser, cosegregating with FPH in one family, was reported (Wang et al., 2009). We studied seven families with progressive FPHH and lentigines. Whole-genome scan was performed with all avail- able family members (Figure 1). Multipoint linkage analyses See related commentary on pg 1182 ORIGINAL ARTICLE 1234 Journal of Investigative Dermatology (2011), Volume 131 & 2011 The Society for Investigative Dermatology Received 29 September 2010; revised 6 January 2011; accepted 13 January 2011; published online 3 March 2011 1 Laboratory of Human Molecular Genetics, de Duve Institute, Universite ´ Catholique de Louvain, Brussels, Belgium; 2 Department of Dermatology and Allergology, University of Regensburg, Hospital Munich Schwabing, Munich, Germany; 3 Department of Pediatrics, SUNY Upstate Medical University, Syracuse, New York, USA and 4 Department of Dermatology, Odense University Hospital, Odense, Denmark Correspondence: Miikka Vikkula, Laboratory of Human Molecular Genetics, de Duve Institute, Universite ´ Catholique de Louvain, 1200 Brussels, Belgium. E-mail: [email protected] 5 Current address: Department of Dermatology, Saarland University Hospital, Homburg/Saar, Germany Abbreviations: DUH2, Dyschromatosis Universalis Hereditaria 2; FPH, familial progressive hyperpigmentation; FPHH, familial progressive hyper- and hypopigmentation

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

KITLG Mutations Cause Familial ProgressiveHyper- and HypopigmentationMustapha Amyere1, Thomas Vogt2,5, Joe Hoo3, Flemming Brandrup4, Anette Bygum4, Laurence Boon1 andMiikka Vikkula1
Familial progressive hyper- and hypopigmentation (FPHH) is thought to be an autosomal dominant disorderwith reduced penetrance. Clinical signs consist of progressive diffuse, partly blotchy hyperpigmented lesions,multiple cafe-au-lait spots, intermingled with scattered hypopigmented-appearing maculae, and lentigines.FPHH is distinct from familial progressive hyperpigmentation (FPH), in which no hypopigmented features arepresent, and which is phenotypically and histologically closer to Dyschromatosis Universalis Hereditaria2 (DUH2). It also differs from the Legius syndrome, characterized by familial cafe-au-lait spots and skin foldfreckling, caused by mutations in SPRED1. We performed a genome-wide linkage analysis in seven families withFPHH, and identified linkage on 12q21.12-q22, which overlaps with the DUH2 locus. We investigated whetherKITLG in the locus is mutated in FPHH. We discovered three different mutations in four families. A reportedFPH substitution was observed in two FPHH families, and two, to our knowledge, previously unreportedsubstitutions, p.Val33Ala and p.Thr34Pro, cosegregated with FPHH in two separate families. All three mutationswere located in a conserved b-strand in KITLG, suggesting its important role in the activation of the KITLGreceptor c-Kit. In aggregate, mutations in a single gene cause various pigmentation disorders: FPH, FPHH, andlikely DUH2. Therefore, KITLG is an important modulator of skin pigmentation.
Journal of Investigative Dermatology (2011) 131, 1234–1239; doi:10.1038/jid.2011.29; published online 3 March 2011
INTRODUCTIONWe have reported a distinct pigmentation disorder familialprogressive hyper- and hypopigmentation (FPHH) associatedwith lentigines in three families from a small area in southeasternGermany, suggesting a founder effect (Zanardo et al., 2004).Transmission was compatible with autosomal dominant inheri-tance with variable expression (Figure 1). FPHH is characterizedby diffuse hyperpigmentation with variable intensity. Cafe-au-laitmacules and larger hypopigmented ash-leaf macules are alsopresent. These features occur on the face, neck, trunk, and limbs,and they are present at birth or early in infancy. The lesionsincrease in size and number with age (Figure 2).
Similar inherited hypomelanotic and hypermelanoticcutaneous macules associated with retarded growth andmental deficiency have been reported in one family (OMIM154000; (Westerhof et al., 1978). Two additional reminiscentinherited phenotypes have been reported: autosomaldominant familial progressive hyperpigmentation (FPH,OMIM 145250), characterized by progressive hyperpigmen-tation similar to that seen in FPHH, but without hypopig-mented lesions, and autosomal recessive DyschromatosisUniversalis Hereditaria 2 (DUH2, OMIM 612715), charac-terized by depigmented and hyperpigmented features thatappear during infancy. Histologically, hyperpigmentedlesions display strong basal pigmentation of the epidermiswith numerous melanin-filled melanophages. In contrast,the hypopigmented-appearing maculae show a slight basalhyperpigmentation of the epidermis, with virtually nomelanophages in the upper dermis (Stuhrmann et al., 2008;Wang et al., 2009).
Two loci have been identified for FPH: one on chromo-some 19p13-pter (Guo et al., 2006) and another on12q21.31-q23.1 (Wang et al., 2009). DUH2 was subse-quently linked to the latter (Bukhari et al., 2006; Stuhrmannet al., 2008). In this locus, a single KITLG amino-acidsubstitution, p.Asn36Ser, cosegregating with FPH in onefamily, was reported (Wang et al., 2009).
We studied seven families with progressive FPHH andlentigines. Whole-genome scan was performed with all avail-able family members (Figure 1). Multipoint linkage analyses
See related commentary on pg 1182ORIGINAL ARTICLE
1234 Journal of Investigative Dermatology (2011), Volume 131 & 2011 The Society for Investigative Dermatology
Received 29 September 2010; revised 6 January 2011; accepted 13 January2011; published online 3 March 2011
1Laboratory of Human Molecular Genetics, de Duve Institute, UniversiteCatholique de Louvain, Brussels, Belgium; 2Department of Dermatology andAllergology, University of Regensburg, Hospital Munich Schwabing, Munich,Germany; 3Department of Pediatrics, SUNY Upstate Medical University,Syracuse, New York, USA and 4Department of Dermatology, OdenseUniversity Hospital, Odense, Denmark
Correspondence: Miikka Vikkula, Laboratory of Human Molecular Genetics,de Duve Institute, Universite Catholique de Louvain, 1200 Brussels, Belgium.E-mail: [email protected]
5Current address: Department of Dermatology, Saarland University Hospital,Homburg/Saar, Germany
Abbreviations: DUH2, Dyschromatosis Universalis Hereditaria 2;FPH, familial progressive hyperpigmentation; FPHH, familial progressivehyper- and hypopigmentation

identified linkage to 12q21.12-q22, and in four families aKITLG mutation was identified.
RESULTSLoss of heterozygosity, copy number estimation,and linkage analysis
We could not detect any deletion, amplification, loss of hetero-zygosity, or uniparental isodisomy in the affected individualsusing single-nucleotide polymorphism chips (data not shown).However, significant linkage using multipoint analysis wasidentified in 12q with the more informative families: family F(z-scoremax¼1.536) and family G (z-scoremax¼ 2.449). Theoverlap between the two loci was about 70–100 Mb (Figure 3cand d). This locus was confirmed in both parametric and
nonparametric analyses. We had hypothesized that theGerman families A, B, C, D, and E might share a commonancestral haplotype and the same causative mutation. Yet,multipoint linkage analysis performed in several combina-tions of the pedigrees gave negative LOD scores for 12q.Only the combination of families A and B as one pedigree(AþB) showed linkage to this locus, with a z-scoremax¼1.103 (Figure 3a and b).
Mutation and cosegregation analysis
We screened KITLG in all affected family members. Threedistinct mutations, which cosegregated with the phenotype,were found in families A, B, F, and G (SupplementaryFigure S1 online). A c.107A4G mutation was identified intwo families (A and B). This is the gain-of-function mutationreported in a single Chinese family with FPH (Wanget al., 2009). The two other mutations, a c.98T4C and ac.100A4C substitution, which lead to p.Val33Ala andp.Thr34Pro changes, respectively, were identified in familiesF and G (Figure 4). No mutation was found in the codingregion of KITLG in families C, D, and E.
Families A and B shared the same mutation and live in thesame area, suggesting a common ancestry. This wasconfirmed by haplotype analysis (data not shown). The threeremaining German families, C, D, and E, without a KITLGcoding region mutation, did not share the same haplotype,rejecting the common ancestral origin of all five families(data not shown). Families C, D, and E are compatible withrecessive inheritance, dominant inheritance with reducedpenetrance, or X-linked inheritance (family D). The smallnumber of DNA samples available from these families limitedfurther analyses.
Secondary and three-dimensional structure of KITLGThe three identified mutations were located in the thirdb-strand of KITLG. They all altered a VTNN sequence, whichis conserved across species (Supplementary Figure S2a andS2b online). On the basis of the three-dimensional structure,the mutated domain may affect KITLG affinity to its receptorc-Kit (Supplementary Figure S2c online). Impact of aminoacid changes on the structure and function of KITLG usingtwo bioinformatic tools gave high scores for damage: PanthersubPSEC scores �3.03778, �4.16303, and �1.64518 andPolyphen PSIC scores 2.171, 1.795, and 1.259 for p.Val33Ala, p.Thr34Pro, and p.Asn36Ser, respectively.
DISCUSSIONMultiple factors influence melanoblast development, migra-tion from the neural crest to peripheral sites, differentiationinto melanocytes, survival, and finally, melanosome forma-tion and synthesis of melanin. Mutations affecting any ofthese steps can result in hereditary hypomelanoses, such asWaardenburg syndrome and vitiligo (Sulaimon and Kitchell,2003; Thomas and Erickson, 2008). Thus, several factors areinvolved. In mouse, roughly 80 alleles are implied to have aneffect on coat color are known. Causative mutations havebeen identified in 17 genes, 14 of which are also mutated inpatients with a pigmentation disorder (Jackson, 1997).
a b
Figure 2. Clinical features of family G. (a) Boy, 11 years of age, with general
hyperpigmentation, accentuated in the neck, with scattered cafe-au-lait
macules, lentigines, and small hypopigmented spots. (b) Male, 43 years of
age, with vitiligo as a rim in the periphery of a dark brown macule at the inner
aspect of left knee.
Family A
Family E Family F Family G
1
1
1
2
2
2
3 4 5 6
7 8
21 1
3 4 5
2
1 1
22 33 44
Family B Family C Family D
Figure 1. Familial progressive hyper- and hypopigmentation in seven
families. Five families (A–E) from southeastern Germany; family F, USA;
family G, Denmark. Numbered individuals included in whole-genome
mapping. Black symbols, familial progressive hyper- and hypopigmentation.
www.jidonline.org 1235
M Amyere et al.Familial Progressive Hyper- and Hypopigmentation

One of these factors is the c-Kit receptor (also known asCD117/p145 Kit). Mutations of which cause dominant whitespotting in pigs (Fontanesi et al., 2010), and white coat colorin horses (Haase et al., 2007) and in mice (Geissler, Ryan andHousman, 1988). In human, dominant c-Kit mutations causepiebaldism, typically characterized by a white forelock,triangular frontal, medioventral body and limb achromia(Fleischman, 1992; Spritz et al., 1992). Moreover, threesingle-nucleotide polymorphisms in KITLG, (also known asthe steel factor or mast cell growth factor/stem cell factor),
which encodes the ligand of c-Kit, were significantlyassociated with hair color in the Scottish population(Mengel-From et al., 2009). In one Chinese family with FPHwithout cafe-au-lait spots, a single amino-acid change inKITLG was reported. Here, we found two FPHH families withthe same substitution and two new substitutions in anothertwo FPHH families.
All the identified mutations in our study were located inthe third b-strand of KITLG. They were single amino-acidsubstitutions in an evolutionary conserved short amino-acidsequence VTNN, suggesting an important functional role forthis hotspot for mutations. Similar to the initially reportedp.Asn36Ser amino-acid change, the novel changes pVal33Ala and pThr34Pro likely cause gain-of-function of KITLGincreasing its affinity to its receptor and deregulating down-stream signalling. Interestingly, the p.Asn36Ser amino-acidchange causes both FPH and FPHH, suggesting additionalfactors to have a role in the development of the phenotype(Figure 5). As all four mutations affect the VTNN-motif, it maybe that the majority of KITLG mutations capable of causinghyperpigmentation alter this small motif. This should betested in FPH, FPHH, and DUH2 families.
After KITLG binds the c-Kit receptor, oligomerization istriggered. This initiates signal transduction via the RAS/MAPKpathway to upregulate melanoblast proliferation (Steel et al.,1992; Spritz, 1994). Mutations in proteins that regulatethis pathway also cause pigmentation disorders (Figure 5).Germline loss-of-function mutations in a RasGTPaseneurofibromin 1, NF1, cause neurofibromatosis type 1,characterized by multiple cafe-au-lait spots (De Schepperet al., 2008). Moreover, germline loss-of-function mutations
1.5
1
0.5
060 70 80 90 100
40
–1
0
0.5
1
1.5
2
2.5
32
1.5
1
0.5
0
–0.5
NP
L (z
-sco
re)
NP
L (z-score)
–1
–0.5
50 70 90 110 130
Mb
60 80 100 120
Mb
Mb
Families A and B
KTLG
KTLG KTLG
–0.5
NP
L (z
-sco
re)
–1Family A
1
1
2 2
Family B
Family GFamily F
a
c
b
d
Figure 3. Multipoint linkage analysis on three familial progressive hyper- and hypopigmentation families. (a) Combined pedigree for families AþB considering
closest possible common ancestor; (b) z-score plots for families AþB (locus: (66295754–94584860); (c, d) family F (locus: (70153597–114764214) and
family G (locus: (58300374–99949424). X axis, physical position on 12q in megabases (Mb); y axis, nonparametric z-score. Whole-genome scan using
Affymetrix 10K arrays (families AþB) and 250K arrays for families F and G.
Family F
Family G
Family A
Family B
98T>CV33A
100A>CT34P
107A>GN36S
Figure 4. Mutations found in KITLG. Mutations c.98T4C and c.100A4C,
resulting in substitutions of p.Val33Ala and p.Thr34Pro in families F and G,
respectively. In families A and B, c.107A4G substitution resulting in
p.Asn36Ser change. N, position of mutation.
1236 Journal of Investigative Dermatology (2011), Volume 131
M Amyere et al.Familial Progressive Hyper- and Hypopigmentation
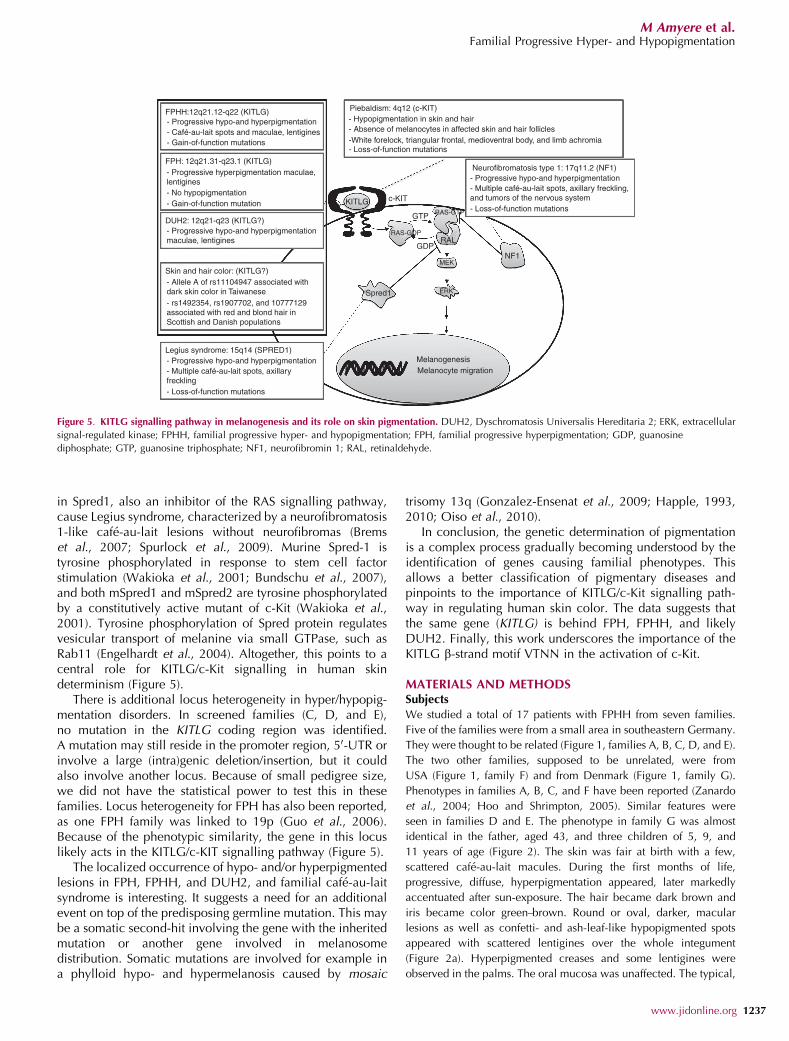
in Spred1, also an inhibitor of the RAS signalling pathway,cause Legius syndrome, characterized by a neurofibromatosis1-like cafe-au-lait lesions without neurofibromas (Bremset al., 2007; Spurlock et al., 2009). Murine Spred-1 istyrosine phosphorylated in response to stem cell factorstimulation (Wakioka et al., 2001; Bundschu et al., 2007),and both mSpred1 and mSpred2 are tyrosine phosphorylatedby a constitutively active mutant of c-Kit (Wakioka et al.,2001). Tyrosine phosphorylation of Spred protein regulatesvesicular transport of melanine via small GTPase, such asRab11 (Engelhardt et al., 2004). Altogether, this points to acentral role for KITLG/c-Kit signalling in human skindeterminism (Figure 5).
There is additional locus heterogeneity in hyper/hypopig-mentation disorders. In screened families (C, D, and E),no mutation in the KITLG coding region was identified.A mutation may still reside in the promoter region, 50-UTR orinvolve a large (intra)genic deletion/insertion, but it couldalso involve another locus. Because of small pedigree size,we did not have the statistical power to test this in thesefamilies. Locus heterogeneity for FPH has also been reported,as one FPH family was linked to 19p (Guo et al., 2006).Because of the phenotypic similarity, the gene in this locuslikely acts in the KITLG/c-KIT signalling pathway (Figure 5).
The localized occurrence of hypo- and/or hyperpigmentedlesions in FPH, FPHH, and DUH2, and familial cafe-au-laitsyndrome is interesting. It suggests a need for an additionalevent on top of the predisposing germline mutation. This maybe a somatic second-hit involving the gene with the inheritedmutation or another gene involved in melanosomedistribution. Somatic mutations are involved for example ina phylloid hypo- and hypermelanosis caused by mosaic
trisomy 13q (Gonzalez-Ensenat et al., 2009; Happle, 1993,2010; Oiso et al., 2010).
In conclusion, the genetic determination of pigmentationis a complex process gradually becoming understood by theidentification of genes causing familial phenotypes. Thisallows a better classification of pigmentary diseases andpinpoints to the importance of KITLG/c-Kit signalling path-way in regulating human skin color. The data suggests thatthe same gene (KITLG) is behind FPH, FPHH, and likelyDUH2. Finally, this work underscores the importance of theKITLG b-strand motif VTNN in the activation of c-Kit.
MATERIALS AND METHODSSubjects
We studied a total of 17 patients with FPHH from seven families.
Five of the families were from a small area in southeastern Germany.
They were thought to be related (Figure 1, families A, B, C, D, and E).
The two other families, supposed to be unrelated, were from
USA (Figure 1, family F) and from Denmark (Figure 1, family G).
Phenotypes in families A, B, C, and F have been reported (Zanardo
et al., 2004; Hoo and Shrimpton, 2005). Similar features were
seen in families D and E. The phenotype in family G was almost
identical in the father, aged 43, and three children of 5, 9, and
11 years of age (Figure 2). The skin was fair at birth with a few,
scattered cafe-au-lait macules. During the first months of life,
progressive, diffuse, hyperpigmentation appeared, later markedly
accentuated after sun-exposure. The hair became dark brown and
iris became color green–brown. Round or oval, darker, macular
lesions as well as confetti- and ash-leaf-like hypopigmented spots
appeared with scattered lentigines over the whole integument
(Figure 2a). Hyperpigmented creases and some lentigines were
observed in the palms. The oral mucosa was unaffected. The typical,
FPHH:12q21.12-q22 (KITLG)
FPH: 12q21.31-q23.1 (KITLG)
- Progressive hypo-and hyperpigmentation
Piebaldism: 4q12 (c-KIT)
Neurofibromatosis type 1: 17q11.2 (NF1)- Progressive hypo-and hyperpigmentation- Multiple café-au-lait spots, axillary freckling,and tumors of the nervous system- Loss-of-function mutations
- Hypopigmentation in skin and hair- Absence of melanocytes in affected skin and hair follicles-White forelock, triangular frontal, medioventral body, and limb achromia- Loss-of-function mutations
KITLG c-KIT
RAS-GDP
Spred1
GDP
GTP RAS-GTP
RAL
MEK
ERK
MelanogenesisMelanocyte migration
NF1
- Progressive hyperpigmentation maculae,lentigines
- Progressive hypo-and hyperpigmentationmaculae, lentigines
Skin and hair color: (KITLG?)- Allele A of rs11104947 associated withdark skin color in Taiwanese- rs1492354, rs1907702, and 10777129associated with red and blond hair inScottish and Danish populations
Legius syndrome: 15q14 (SPRED1)- Progressive hypo-and hyperpigmentation- Multiple café-au-lait spots, axillaryfreckling- Loss-of-function mutations
- No hypopigmentation- Gain-of-function mutation
DUH2: 12q21-q23 (KITLG?)
- Café-au-lait spots and maculae, lentigines- Gain-of-function mutations
Figure 5. KITLG signalling pathway in melanogenesis and its role on skin pigmentation. DUH2, Dyschromatosis Universalis Hereditaria 2; ERK, extracellular
signal-regulated kinase; FPHH, familial progressive hyper- and hypopigmentation; FPH, familial progressive hyperpigmentation; GDP, guanosine
diphosphate; GTP, guanosine triphosphate; NF1, neurofibromin 1; RAL, retinaldehyde.
www.jidonline.org 1237
M Amyere et al.Familial Progressive Hyper- and Hypopigmentation

progressive vitiligo had been present in the father since 40 years of
age. This has not been reported for FPHH. The symmetric,
vitiliginous macules were seen at the volar aspects of the wrists, at
the elbows and dorsum of the feet. A rim of progressive vitiligo was
also observed in a large hyperpigmented macule at the inner aspect
of the left knee (Figure 2b).
All protocols were approved by national and/or local institutional
review boards, informed written consent was obtained from all
subjects, and the study was conducted according to the Declaration
of Helsinki Principles.
Venous blood samples (10 ml) were collected and DNA was
extracted using the Puregene DNA extraction kit (Gentra, Qiagen
Benelux BV, Belgium).
Microarray analyses
Molecular karyotyping was performed in all seven families using
Affymetrix Human Mapping 10K or 250K SNP chips (Affymetrix,
Santa Clara, CA) according to the manufacturer’s instructions.
Briefly, total genomic DNA was digested with XbaI for the 10K
and with NspI for the 250K chips. Generated fragments were ligated
to adaptors, and amplified with a single primer. After purification of
the PCR products, amplicons were quantified, fragmented, labeled,
and hybridized on the array. Signal intensities were measured with
Affymetrix GeneChip Scanner 3000 7G (Affymetrix). Genotypes
were generated using the Dynamic model for 10K or the Improved
Genotype Calling Method (BRLMM) for 250K.
Copy number, loss of heterozygosity, and uniparentalisodisomy analysis
Intensity of hybridization was quantified to estimate relative copy
numbers for each chromosome. The signal intensity ratios of tested
samples were divided by the mean of a set of 264 internal reference
samples to calculate copy number status, using the CNAG software
version 3 (Nannya et al., 2005; Yamamoto et al., 2007). Intensity of
hybridization was estimated using the Hidden Markov model.
Linkage analysis and haplotype analysis
Genome-wide parametric and nonparametric multipoint linkage
analyses were performed in all families using Dchip software (http://
biosun1.harvard.edu/complab/dchip/) and haplotypes were inferred
using Genehunter software package (http://linkage.rockefeller.edu/
soft/gh/). The parametric analyses were run under an autosomal
dominant model. The penetrance for homozygous and heterozygous
disease-causing gene carriers was set to 90% and the phenocopy
rate for non-gene carriers to 1%.
Mutation screening and cosegregation
Patients were screened for the eight known coding exons of the
KITLG, including 50 base pairs (bp) of flanking intronic sequences
around each exon. PCR primers were designed using CLC Main
Workbench 5 software (http://www.clcbio.com/). All amplicons
were resolved on agarose gels, and sequenced on a CEQ2000
fluorescent capillary sequencer (Beckman Coulter, Brea, CA).
Cosegregation analyses were performed by direct sequencing in
families A and B. Presence of mutations (c.98T4C or c.100A4C)
were detected by restriction-enzyme analysis using MaeIII. Both
mutations destroy a restriction-enzyme cutting site that normally
splits the 430 bp fragment into two fragments of 300 and 130 bp.
Bioinformatic analysisProbability for an amino-acid change to have an impact on the structure
and/or function of a KITLG was studied using two bioinformatic tools:
PANTHER (Protein ANalysis THrough Evolutionary Relation-
ships; (http://www.pantherdb.org/) and PolyPhen (POLYmorphism
PHENotyping; http://genetics.bwh.harvard.edu/pph/).
PANTHER: scores sequence variants on the basis of the degree of
evolutionary conservation of amino acid residues in between
species. The result is indicated as a ‘‘potential deleterious effect’’
of a missense change, with a continuous value from 0 (neutral) to
approximately –10 (most likely deleterious).
PolyPhen: calculates the probability of an amino acid replace-
ment being incompatible with function of the protein on the basis of
spectrum of substitutions observed at the corresponding position in
the family of homologous proteins. The result is given as a PISIC
score: damaging score 41 and benign¼ 0.5.
Predictive secondary structure was viewed with CLC Main
Workbench 5.
The crystal structure of KITLG was uploaded from Protein
Data Bank (http://www.rcsb.org/pdb/explore.do?structureId=2O27)
and visualized with CLC Main Workbench 5.
CONFLICT OF INTERESTThe authors state no conflict of interest.
ACKNOWLEDGMENTSWe are grateful to all the family members for their participation. These studies werepartially supported by the FRS-FNRS (Fonds de la Recherche Scientifique); andla Lotterie Nationale, Belgium (to MV). MA is a ‘‘Scientific Logistics Manager’’ of theFonds de la Recherche Scientifique-FNRS. The authors thank the Genomics/Transcriptomics Platform of Universite Catholique de Louvain for Affymetrix chipanalyses. The authors thank Stephane Messe for his help in sequencing experiments.
SUPPLEMENTARY MATERIAL
Supplementary material is linked to the online version of the paper at http://www.nature.com/jid
REFERENCES
Brems H, Chmara M, Sahbatou M et al. (2007) Germline loss-of-functionmutations in SPRED1 cause a neurofibromatosis 1-like phenotype.Nat Genet 39:1120
Bukhari IA, El-Harith EA, Stuhrmann M (2006) Dyschromatosis universalishereditaria as an autosomal recessive disease in five members of onefamily. J Eur Acad Dermatol Venereol 20:628
Bundschu K, Walter U, Schuh K (2007) Getting a first clue about SPREDfunctions. Bioessays 29:897
De Schepper S, Maertens O, Callens T et al. (2008) Somatic mutation analysisin NF1 cafe au lait spots reveals two NF1 hits in the melanocytes.J Invest Dermatol 128:1050
Engelhardt CM, Bundschu K, Messerschmitt M et al. (2004) Expression andsubcellular localization of Spred proteins in mouse and human tissues.Histochem Cell Biol 122:527
Fleischman RA (1992) Effect of the c-kit codon 584 Phe——Leu substitutiondemonstrated in human piebaldism. Am J Hum Genet 51:677
Fontanesi L, D’Alessandro E, Scotti E et al. (2010) Genetic heterogeneity andselection signature at the KIT gene in pigs showing different coat coloursand patterns. Anim Genet 41:478
Geissler EN, Ryan MA, Housman DE (1988) The dominant-white spotting (W)locus of the mouse encodes the c-kit proto-oncogene. Cell 55:185
Gonzalez-Ensenat MA, Vicente A, Poo P et al. (2009) Phylloid hypomelanosisand mosaic partial trisomy 13: two cases that provide further evidence ofa distinct clinicogenetic entity. Arch Dermatol 145:576
1238 Journal of Investigative Dermatology (2011), Volume 131
M Amyere et al.Familial Progressive Hyper- and Hypopigmentation

Guo X, Shen H, Xiao X et al. (2006) Cataracts, ataxia, short stature,and mental retardation in a Chinese family mapped to Xpter-q13.1.J Hum Genet 51:695
Haase B, Brooks SA, Schlumbaum A et al. (2007) Allelic heterogeneityat the equine KIT locus in dominant white (W) horses. PLoS Genet3:e195
Happle R (1993) Mosaicism in human skin. Understanding the patterns andmechanisms. Arch Dermatol 129:1460
Happle R (2010) Phylloid hypermelanosis: an unusual form of pigmentarymosaicism. Dermatology 220:183
Hoo JJ, Shrimpton AE (2005) Familial hyper- and hypopigmentation withage-related pattern change. Am J Med Genet A 132A:215
Jackson IJ (1997) Homologous pigmentation mutations in human, mouse andother model organisms. Hum Mol Genet 6:1613
Mengel-From J, Wong TH, Morling N et al. (2009) Genetic determinants ofhair and eye colours in the Scottish and Danish populations. BMC Genet10:88
Nannya Y, Sanada M, Nakazaki K et al. (2005) A robust algorithm for copynumber detection using high-density oligonucleotide single nucleotidepolymorphism genotyping arrays. Cancer Res 65:6071
Oiso N, Tsuruta D, Imanishi H et al. (2010) Phylloid hypermelanosis andmelanocytic nevi with aggregated and disfigured melanosomes: causalrelationship between phylloid pigment distribution and chromosome13 abnormalities. Dermatology 220:169
Spritz RA (1994) Molecular basis of human piebaldism. J Invest Dermatol103:137S
Spritz RA, Giebel LB, Holmes SA (1992) Dominant negative and loss offunction mutations of the c-kit (mast/stem cell growth factor receptor)proto-oncogene in human piebaldism. Am J Hum Genet 50:261
Spurlock G, Bennett E, Chuzhanova N et al. (2009) SPRED1 mutations(Legius syndrome): another clinically useful genotype for dissectingthe neurofibromatosis type 1 phenotype. J Med Genet 46:431
Steel KP, Davidson DR, Jackson IJ (1992) TRP-2/DT, a new early melanoblastmarker, shows that steel growth factor (c-kit ligand) is a survival factor.Development 115:1111
Stuhrmann M, Hennies HC, Bukhari IA et al. (2008) Dyschromatosisuniversalis hereditaria: evidence for autosomal recessive inheritanceand identification of a new locus on chromosome 12q21-q23.Clin Genet 73:566
Sulaimon SS, Kitchell BE (2003) The biology of melanocytes. Vet Dermatol14:57
Thomas AJ, Erickson CA (2008) The making of a melanocyte: the specification ofmelanoblasts from the neural crest. Pigment Cell Melanoma Res 21:598
Wakioka T, Sasaki A, Kato R et al. (2001) Spred is a Sprouty-related suppressorof Ras signalling. Nature 412:647
Wang ZQ, Si L, Tang Q et al. (2009) Gain-of-function mutation of KIT ligandon melanin synthesis causes familial progressive hyperpigmentation.Am J Hum Genet 84:672
Westerhof W, Beemer FA, Cormane RH et al. (1978) Hereditary congenitalhypopigmented and hyperpigmented macules. Arch Dermatol 114:931
Yamamoto G, Nannya Y, Kato M et al. (2007) Highly sensitive method forgenomewide detection of allelic composition in nonpaired, primarytumor specimens by use of affymetrix single-nucleotide-polymorphismgenotyping microarrays. Am J Hum Genet 81:114
Zanardo L, Stolz W, Schmitz G et al. (2004) Progressive hyperpigmentationand generalized lentiginosis without associated systemic symptoms: arare hereditary pigmentation disorder in south-east Germany. Acta DermVenereol 84:57
www.jidonline.org 1239
M Amyere et al.Familial Progressive Hyper- and Hypopigmentation
Related Documents











