This article was downloaded by: [Near Eastern University] On: 07 July 2015, At: 01:04 Publisher: Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: 5 Howick Place, London, SW1P 1WG Click for updates Journal of Sports Sciences Publication details, including instructions for authors and subscription information: http://www.tandfonline.com/loi/rjsp20 Kinematic and EMG activities during front and back squat variations in maximum loads Hasan Ulas Yavuz a , Deniz Erdağ b , Arif Mithat Amca c & Serdar Aritan c a Sports Medicine, Near East University Hospital, Nicosia, Cyprus b School of Physical Education and Sports, Near East University, Nicosia, Cyprus c Faculty of Sports Sciences, Hacettepe University, Ankara, Turkey Published online: 29 Jan 2015. To cite this article: Hasan Ulas Yavuz, Deniz Erdağ, Arif Mithat Amca & Serdar Aritan (2015) Kinematic and EMG activities during front and back squat variations in maximum loads, Journal of Sports Sciences, 33:10, 1058-1066, DOI: 10.1080/02640414.2014.984240 To link to this article: http://dx.doi.org/10.1080/02640414.2014.984240 PLEASE SCROLL DOWN FOR ARTICLE Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) contained in the publications on our platform. However, Taylor & Francis, our agents, and our licensors make no representations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of the Content. Any opinions and views expressed in this publication are the opinions and views of the authors, and are not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be relied upon and should be independently verified with primary sources of information. Taylor and Francis shall not be liable for any losses, actions, claims, proceedings, demands, costs, expenses, damages, and other liabilities whatsoever or howsoever caused arising directly or indirectly in connection with, in relation to or arising out of the use of the Content. This article may be used for research, teaching, and private study purposes. Any substantial or systematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in any form to anyone is expressly forbidden. Terms & Conditions of access and use can be found at http:// www.tandfonline.com/page/terms-and-conditions

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

This article was downloaded by [Near Eastern University]On 07 July 2015 At 0104Publisher RoutledgeInforma Ltd Registered in England and Wales Registered Number 1072954 Registered office 5 Howick PlaceLondon SW1P 1WG
Click for updates
Journal of Sports SciencesPublication details including instructions for authors and subscription informationhttpwwwtandfonlinecomloirjsp20
Kinematic and EMG activities during front and backsquat variations in maximum loadsHasan Ulas Yavuza Deniz Erdağb Arif Mithat Amcac amp Serdar Aritanc
a Sports Medicine Near East University Hospital Nicosia Cyprusb School of Physical Education and Sports Near East University Nicosia Cyprusc Faculty of Sports Sciences Hacettepe University Ankara TurkeyPublished online 29 Jan 2015
To cite this article Hasan Ulas Yavuz Deniz Erdağ Arif Mithat Amca amp Serdar Aritan (2015) Kinematic and EMGactivities during front and back squat variations in maximum loads Journal of Sports Sciences 3310 1058-1066 DOI101080026404142014984240
To link to this article httpdxdoiorg101080026404142014984240
PLEASE SCROLL DOWN FOR ARTICLE
Taylor amp Francis makes every effort to ensure the accuracy of all the information (the ldquoContentrdquo) containedin the publications on our platform However Taylor amp Francis our agents and our licensors make norepresentations or warranties whatsoever as to the accuracy completeness or suitability for any purpose of theContent Any opinions and views expressed in this publication are the opinions and views of the authors andare not the views of or endorsed by Taylor amp Francis The accuracy of the Content should not be relied upon andshould be independently verified with primary sources of information Taylor and Francis shall not be liable forany losses actions claims proceedings demands costs expenses damages and other liabilities whatsoeveror howsoever caused arising directly or indirectly in connection with in relation to or arising out of the use ofthe Content
This article may be used for research teaching and private study purposes Any substantial or systematicreproduction redistribution reselling loan sub-licensing systematic supply or distribution in anyform to anyone is expressly forbidden Terms amp Conditions of access and use can be found at httpwwwtandfonlinecompageterms-and-conditions
Kinematic and EMG activities during front and back squat variations inmaximum loads
HASAN ULAS YAVUZ1 DENIZ ERDAĞ2 ARIF MITHAT AMCA3 amp SERDAR ARITAN3
1Sports Medicine Near East University Hospital Nicosia Cyprus 2School of Physical Education and Sports Near EastUniversity Nicosia Cyprus and 3Faculty of Sports Sciences Hacettepe University Ankara Turkey
(Accepted 1 November 2014)
AbstractThe aim of this study was to compare the musculature activity and kinematics of knee and hip joints during front and backsquat with maximal loading Two-dimensional kinematical data were collected and electromyographic activities of vastuslateralis vastus medialis rectus femoris semitendinosus biceps femoris gluteus maximus and erector spinae weremeasured while participants (n = 12 212 plusmn 19 years old) were completing front and back squat exercises with maximumloading Paired sample t-test was used for comparisons between two techniques Results showed that the electromyographicactivity of vastus medialis was found to be greater in the front squat compared to the back squat during the ascending phase(P lt 005 d = 062 95 CI minus150minus417) and the whole manoeuvre (P lt 005 d = 041 95 CI minus128minus043) whilesemitendinosus (P lt 005 d = minus079 95 CI 0622059) electromyographic activity was greater in the back squat duringthe ascending phase Compared to the front squat version back squat exhibited significantly greater trunk lean with nodifferences occurring in the knee joint kinematics throughout the movement Results may suggest that the front squat maybe preferred to the back squat for knee extensor development and for preventing possible lumbar injuries during maximumloading
Keywords strength training electromyography biomechanics two-dimensional maximal loading
Introduction
Progressive resistance training is an effective methodfor developing muscular strength for performance aswell as for injury prevention and rehabilitation(American College of Sports Medicine 1998)Choosing the right exercise is one of the most impor-tant factors for achieving the aims of the programme(Fleck 1999)
The squat is a staple multiple joint free weight resis-tance exercise that develops not only the quadriceps(rectus femoris vastus lateralis and vastus medialis)but also the hamstrings (biceps femoris and semitendi-nosus) and it also loads the erector spinae (ES)(McCaw amp Melrose 1999)
Increasing the power of these muscles can oftentranslate into improved performance in one or sev-eral athletic skills (sprinting jumping throwing andstriking) (Balshaw amp Hunter 2012 Channell ampBarfield 2008) Due to the popularity of the exer-cise many variations have been created by alteringthe placement of the squat bar back squat (barbellheld across the back slightly above or below the level
of the acromion) front squat (barbell held in front ofthe chest approximately at the level of the clavicles)(Donnelly Berg amp Fiske 2006) or overhead squat(barbell held over the head while elbows are fullyextended) (Hasegawa 2004) altering squat depthpartial squats (40deg knee angle) half squats (70deg to100deg) and deep squats (greater than 100deg)(Schoenfeld 2010) altering stance width narrow(87ndash118 shoulder width) medium (121ndash153shoulder width) or wide (158ndash196 shoulderwidth) (Escamilla 2000) altering foot rotationinternally or externally rotated feet or altering squat-ting surface stable or labile (power board BOSUball balance cone) However no standardised mea-sures of quantification have been universally recog-nised and terminology can differ betweenresearchers (Schoenfeld 2010)
Two common forms of the squat are the back squat(Figure 1(a)) and the front squat (Figure 1(b))Competitive or recreational athletes regularly performthe back squat while the front squat is much lesscommon Although both squats effectively work thelower back hip and leg muscles there are slight
Correspondence Hasan Ulas Yavuz Sports Medicine Near East University Hospital Dikmen Nicosia 99380 Cyprus E-mail ulasyavuzneuedutr
Journal of Sports Sciences 2015Vol 33 No 10 1058ndash1066 httpdxdoiorg101080026404142014984240
copy 2015 Taylor amp Francis
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015
variations in technique and muscular involvement(Gullett Tillman Gutierrez amp Chow 2009)
Several studies have described the patterns of thekinematics kinetics and muscle activities of the kneehip and ankle during the squat (Dionisio AlmeidaDuarte amp Hirata 2008 Escamilla Fleisig LowryBarrentine amp Andrews 2001 Escamilla et al 1998Flanagan Salem Wang Sanker amp Greendale 2003Hasegawa 2004 Isear Erickson amp Worrel 1997McCaw amp Melrose 1999 Stensdotter HodgesMellor Sundelin amp Hager 2003 Wretneberg FengampArborelius 1996)However only a few of themhavecompared front and back squat (Braidot BrusaLestussi amp Parera 2007 Diggin et al 2011 Gullettet al 2009) and even less have studied electromyogra-phy (EMG) and kinematics together in the same studyto see the interactions (Gullett et al 2009)
Braidot et al (2007) compared the kinematicsdynamics the power and the energy in the differentjoints during the complete cycle from the exercise inthe different variants of squat A better developmentof energy with the front bar is observed in the kneeallowing a better muscular exercise with the sameload In the study of Diggin et al (2011) back squatexhibited a significantly greater trunk lean than thefront squat (P lt 005) with no differences in theknee joint kinematics However these studies didnot quantify the electromyographic data and muscleactivity during the front and back squatFurthermore the load to evaluate the exercise iscalculated on the basis of 50 of one repetitionmaximum (1RM) for both variants
Gullett et al (2009) reported that the front squatwas as effective as the back squat in terms of overall
muscle recruitment with 70 of 1RM load for eachsquat technique Heavy loading in experienced indi-viduals is needed to recruit the high-threshold motorunits that may not be activated during light-to-moderate lifting (Kraemer amp Ratamess 2004)Besides during lower loading conditions strongermuscles may compensate the activation of weakerones and cause personal varieties But during max-imal loading all related muscles must be fully acti-vated in order to complete the manoeuvre That willform a normalisation in terms of muscle activity andnaturally EMG signalling Clark Lambert andHunter (2012) emphasised that the sub-maximalload used in Gulletrsquos study might have failed to elicitthe possible difference between back and front squatFurthermore an increase in trunk forward lean wasshown with higher loads by Hay Andrews Vaughanand Ueya (1983) and Kellis Arambatzi andPapadopoulos (2005) during squat Thereforeobviously squat kinematics and EMG signalisationpattern can change with maximal loading
We aimed to compare the musculature activity andkinematics of knee and hip joints during front and backsquat with maximal loading and investigate the possi-ble differences in these two common squat variations
Methods
Participants
Twelve healthy male individuals who were experi-enced at performing front and back squats partici-pated in this study All participants were right-handed and had no history of orthopaedic injury
Figure 1 (a) Bar positioning during the back squat (b) Bar positioning during the front squat
EMG Kinematic activities of back and front squat 1059
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015
or surgery that would have limited their ability toperform the squatting techniques Before participa-tion informed consent was obtained from eachparticipant The investigation was conductedaccording to the Declaration of Helsinki andapproved by the Near East University ScientificResearches Evaluation and Ethic Commission(YDUuml201211ndash60)
Instrumentation
An eight-channel dual-mode portable EMG andphysiological signal data acquisition system(Myomonitor IV Delsys Inc Boston MA USA)was used for data collection Data collections wereconducted using EMG Works Acquisition 405(Delsys Inc) The amplifier bandwidth frequencyranged from 20 to 450 Hz with an input voltage of9 VDC at 07 A and the common-mode rejectionratio was 80 dB Data were recorded at a samplingrate of 1000 Hz over a wireless local area network tothe host computer for real-time display and storage
Seven channels of this system were used to assessthe EMG activity of vastus lateralis vastus medialisrectus femoris semitendinosus biceps femoris glu-teus maximus and ES Recording sites were pre-pared by shaving the area and wiping with alcoholpads to decrease electrical impedance Electrodes(41 times 20 times 5 mm DE-23 Delsys Inc) were placedalong the longitudinal axis of each muscle tested onthe right side (dominant side) of the participantrsquosbody according to the procedures from Gullettet al (2009) (Table I) The sensor contacts aremade from 999 pure silver bars measuring10 mm in length 1 mm in diameter and spaced10 mm apart from optimal signal detection and con-sistency A 508 cm diameter oval-shaped commonreference electrode (Dermatrode HE-R AmericanImex Irvine CA USA) was placed on the iliaccrest of the right leg
At the same time the EMG system was synchro-nised with a Samsung (VP-D375 W) video camera
with a shutter speed of 1250 s by using NationalInstruments USB-6501 Digital IO trigger box(Delsys Inc) Video recordings were made withAMCap (Microsoft V 309) video capture softwareFor kinematical data reflective markers (3 cm dia-meter) were attached and positioned over the follow-ing bony landmarks (a) lateral malleolus of the rightfoot (b) upper edges of the lateral tibial plateau ofthe right knee (c) posterior aspect of the greatertrochanters of the right femur and (d) end of theright side of the Olympic bar A calibration planethat consists of eight control points was used for two-dimensional spatial reconstruction
A standard 205-kg Olympic barbell discs(Werksan Ankara Turkey) and a continental squatrack were used during the squat
Procedures
The participants were required to attend two ses-sions A pretest was given to each participant 1week before the actual testing session The experi-mental protocol was reviewed and the participantswere given the opportunity to ask questions Duringthe pretest the participantrsquos RM was determinedand recorded for the back squat and front squatThe procedure used for assessing 1RM wasdescribed by Kraemer and Fry (1995) The partici-pants were asked to perform initial preparation on astationary bike for 3ndash5 min at the beginning of thepretest session and then performed a warm-up set of8ndash10 repetitions at a light weight (approximately50 of assumed 1RM) A second initial preparationconsisting of a set of three to five repetitions withmoderate weight (approximately 75 of 1RM) and athird initial preparation including one to three repe-titions with a heavy weight (approximately 90 of1RM) followed
After the initial preparation the participants per-formed 1RM strength exercises by enhancing the loadduring consecutive trials until the participants wereunable to properly perform a proper lift complete
Table I A description of the positioning of each electrode in relation to the muscle being tested developed by Broer and Houtz (1967) anddescribed by Gullett et al (2009)
Muscle Electrode placement
Rectus femoris Approximately midway between the anterior inferior iliac spine and the patella on the anterior side of the thighVastus lateralis Approximately two-thirds of the thigh length from the greater trochanter on the lateral side of the thighVastus medialis Approximately three-fourths of the thigh length from the anterior inferior iliac spine on the medial side of the thighErector spinae Three centimetres lateral to the L3 spinous processGluteus maximus 50 on the line between the sacral vertebrae and the greater trochanter This position corresponds with the greatest
prominence of the middle of the buttocks well above the visible bulge of the greater trochanterBiceps femoris Midway between the ischial tuberosity and the lateral condyle of the femur on the posterior side of the thighSemitendinosus Midway between the ischial tuberosity and the medial condyle of the femur on the posterior side of the thighReference electrode Iliac crest of the right leg
1060 HU Yavuz et al
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015
range of motion and correct technique Each partici-pant was asked to lower the bar to the point where theknee angle was 90deg (Figure 2) which was marked byadjustable stoppers Adequate rest was allowedbetween trials (3ndash5 min) Subsequently 1 week afterthe pretest session the participants performed a sec-ond session for data collection For each participantall data collection was performed in one day session
After the EMG electrode placement maximumvoluntary isometric contraction (MVIC) data fromthe quadriceps hamstrings erector spine and glu-teus maximus were collected according to the pro-cedures described by Konrad (2005) Three 3-sMVIC trials were collected in a randomised mannerfor each muscle group Adequate rest was allowedbetween trials (1 min)
All participants performed two to three warm-upsets in preparation for testing For both lifting varia-tions each participant used their 1RM weights pre-viously established for the back squat and frontsquat Exercise began with a given verbal commandThe starting and ending positions for the back squatand front squat were with the knees in full extensionwhich was defined as 180deg knee angle From thestarting position the participant flexed their kneesto minimum knee angle (approximately 90deg) andthen extended their knees back to the startingposition
During the back squat the barbell positionedacross the shoulder on the trapezius slightly abovethe posterior aspect of the deltoids and the hips andknees flexed until the thighs are parallel to the floor(Baechle and Earle 2000 Delavier 2001) Thenthe participant extended the hips and knees untilthe starting position is reached keeping the backflat the heels on the floor and the knees alignedover the feet (Baechle and Earle 2000 Delavier2001) During the front squat the barbell positionedacross the anterior deltoids and clavicles and theelbows fully flexed to position the upper arms paral-lel to the floor (Baechle and Earle 2000 Delavier
2001) The descending and ascending motions aremuch the same as in the back squat (Gullett et al2009) Adequate rest was allowed between trials (3ndash5 min)
Data reduction
The sampling of EMG and video recordings wereinitiated simultaneously with the beginning of thefirst squat repetition For synchronisation a LEDconnected to the trigger box (National InstrumentsUSB-6501 Digital IO) outputted a digital signalwhen the Myomonitor started data acquisitionWith the data acquisition the LED lit and it wentoff as the data stopped The data obtained from thisprocedure were used to specify the start of therequired portion and the length of the requestedportion
Kinematical data were analysed by using thesaSuite two-dimensional kinematical analysis pro-gramme which was developed by HacettepeUniversity Faculty of Sports SciencesBiomechanics Research Group Ankara TurkeyFor each trail the required portion of the videorecordings was trimmed the anthropometric pointswere digitised and the two-dimensional positionaldata were obtained The raw position data of thejoints were smoothed using a moving average filterand the angular kinematics of the knee and hip jointswere calculated All EMG data were partitioned intoascending and descending phases Movement timewas normalised into 10 movement phases to controlinter-individual differences Knee and hip anglechanges were examined throughout the descendingand ascending phases
EMG data were analysed according to the proce-dures from International Society ofElectrophysiology and Kinesiology (Merletti 1999)by using the EMG Works Analysis 40 (Delsys IncBoston) To calculate the mean normalised EMGvalues the raw EMG signals were subsetted filtered(Passband 3 Response Bandpass Corner F110 Hz Corner F2 500 Hz) rectified integrated(root mean square (Window Length 0100Window Overlap 008 Remove Ofset)) and nor-malised to the participants highest correspondingMVIC trial
Statistical analysis
Kinematic and electromyographic data were ana-lysed and compared between the front and backsquad by using paired sample t-tests (P lt 005)Throughout the text data for all participants per-forming each type of exercise were averaged andpresented as means standard deviations P-valueeffect size (Cohenrsquos d Cohen 1988) and 95
Figure 2 Illustrations of measured joint angles during back squatand front squat (adapted from Starting Strength Basic BarbellTraining by permission of The Aasgaard Company Rippetoe ampKilgore 2007)
EMG Kinematic activities of back and front squat 1061
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015
confidence intervals Cohenrsquos categories were usedto evaluate the magnitude of these sizes (small if0 le [d] le 05 medium if 05 le [d] le 08 and large if[d] gt 08) (Cohen 1988)
Results
The mean 1RM loads that were employed duringtesting were 10917 plusmn 2551 kg for the back squatand 8500 plusmn 1567 kg for the front squat This was13883 plusmn 3262 of their body weight for back squatand 10587 plusmn 2434 for front squat Participantscould lift significantly higher loads with back squatcomparing to the front squat (P lt 005 d = minus12895 CI 16283204)
Normalised EMG values as a percentage of max-imal voluntary isometric contraction ( MVIC)P-values effect size (Cohenrsquos d Cohen 1988) and95 confidence intervals between back and frontsquats are shown in Table II Vastus medialisEMG activity was found to be greater during thefront squat compared to back squat (P lt 005
d = 041 95 CI minus128minus43) There were noother differences in any other muscles
Normalised average EMG values as a MVIC P-values effect size (Cohenrsquos d Cohen 1988) and 95confidence intervals between descending and ascend-ing phases performed with 1RM loads between backand front squats are shown in Table III EMG activ-ities of gluteus maximus (P lt 005 d = 078 95 CIminus2581minus1120) biceps femoris (P lt 005 d = 09795 CI minus1974minus1260) and semitendinosus(P lt 005 d = 105 95 CI minus2072minus728) duringback squat and EMG activities of gluteus maximus(P lt 005 d = 062 95 CI minus2209minus1118) bicepsfemoris (P lt 005 d = 038 95 CI minus1486minus471)and semitendinosus (P lt 005 d = 048 95 CIminus840minus34) during front squat were found to be sig-nificantly higher EMG activity of the vastus medialis(P lt 005 d = 032 95CI minus1103minus53) during theascending phase was higher only
The mean EMG activities as a percentage of max-imal voluntary isometric contraction ( MVIC)P-values effect size (Cohenrsquos d Cohen 1988) and
Table II Mean EMG activities as a percentage of maximal voluntary isometric contraction ( MVIC) P-values effect size(Cohenrsquos d Cohen 1988) and 95 confidence intervals for the back squats and front squats throughout entire movementsperformed with 1RM loads
Muscle Back squat (mean plusmn s) Front squat (mean plusmns) P d
95 CI
L U
Rectus femoris 367 plusmn 124 461 plusmn 217 0118 053 minus217 282Vastus medialis 488 plusmn 139 554 plusmn 180 0038 041 minus128 minus043Vastus lateralis 470 plusmn 151 512 plusmn 173 0149 026 minus102 minus175Erector spinae 432 plusmn 156 462 plusmn 121 0495 022 minus125 049Gluteus maximus 371 plusmn 235 372 plusmn 270 0959 0 minus55 523Biceps femoris 262 plusmn 161 241 plusmn 254 0611 minus0 minus65 106Semitendinosus 215 plusmn 117 160 plusmn 87 0115 minus053 minus16 126
Note Significantly higher EMG activities during the front squat compared to the back squat (P lt 005)
Table III Back squats and front squats mean EMG activities as a percentage of maximal voluntary isometric contraction ( MVIC)P-values effect size (Cohenrsquos d Cohen 1988) and 95 confidence intervals between descending and ascending phases performed with1RM loads
Back squat Front squat
Descendingphase
(mean plusmns)
Ascendingphase
(mean plusmn s) P d
95 CI Descendingphase
(mean plusmn s)
Ascendingphase
(mean plusmn s) P d
95 CI
Muscle L U L U
Rectus femoris 379 plusmn 121 360 plusmn 138 0455 minus015 minus3562 minus7432 464 plusmn 244 467 plusmn 194 0922 001 minus7122 6500Vastus medialis 483 plusmn 143 493 plusmn 139 0617 007 minus5293 3286 531 plusmn 193 589 plusmn 171 033 032 minus11036 minus533Vastus lateralis 459 plusmn 139 485 plusmn 172 0223 017 minus7005 1821 480 plusmn 158 562 plusmn 222 068 043 minus17190 07269Erector spinae 411 plusmn 140 460 plusmn 176 0124 031 minus11286 1564 451 plusmn 120 481 plusmn 168 0451 020 minus11276 5367Gluteus maximus 288 plusmn 189 473 plusmn 277 0000 078 minus25810 minus11200 300 plusmn 230 466 plusmn 301 0000 062 minus22098 minus11188Biceps femoris 187 plusmn 149 349 plusmn 182 0000 097 minus19740 minus12600 197 plusmn 233 295 plusmn 287 0001 038 minus14864 minus4711Semitendinosus 150 plusmn 69 290 plusmn 162 0001 105 minus20720 minus7280 140 plusmn 81 184 plusmn 101 0036 048 minus8404 minus0343
Note Significantly higher EMG activities during the ascending phase compared to the descending phase (P lt 005)
1062 HU Yavuz et al
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015
95 confidence intervals between back squats andfront squats during the descending and ascendingphases performed with 1RM loads are shownin Table IV There were no significant differencesobserved between back and front squats duringthe descending phase During the ascending phasethe EMG activity of the vastus medialis was foundto be significantly higher in the front squat comparedto the back squat (P lt 005 d = 062 95 CIminus1500minus417) while the EMG activity of the semi-tendinosus was higher in the back squat compared tothe front squat (P lt 05 d = minus079 95 CI 622059)
As can be seen from Figure 3 significant differ-ences were observed between minimum hip anglesreached during back squats and front squats Theaverage minimum hip angle was significantly higher(P lt 005 d = 108 95 CI minus2857minus428) duringthe front squat compared to the back squat
Figure 4 shows the mean changes in knee and hipangles throughout the ascending phases of bothsquatting movements No difference was observed
in knee angles during the whole movement whilehip angles were lower in 8 of 10 phases during theback squat compared to front squat showing anobvious forward trunk lean According to theangle-specific EMG changes semitendinosus(P lt 005 d = minus023 95 CI minus2421111) showeda sudden increase in the sixth phase and bicepsfemoris (P lt 005 d = minus014 95 CI minus10931911) and gluteus maximus (P lt 005 d = minus03795 CI minus4533089) showed a similar but smallerincrease in the eighth phase during the back squatcompared to the front squat
Discussion
Participants could lift significantly greater loads withback squat compared to the front squat(1388 plusmn 326 of their body weight1059 plusmn 243 of their body weight respectively)(Figure 1) and this finding is consistent with theprevious studies (Gullett et al 2009 Russell ampPhillips 1989)
Instead of the load the level of effort in voluntarymuscle actions determines the degree of motor unitactivity (Carpinelli 2008) consequently the level ofEMG signalling increases Furthermore higherloads may increase intradiscal pressure (11) com-pression on vertebral bodies (10) tibiofemoral (1213) and patellofemoral joints (14) which could pos-sibly increase the risk of injury while performingsquat Gullett et al (2009) emphasised that the mus-cles tested were equally active during the front squatwhile lifting less mass and it seems that the extraload lifted during the back squat is what accounts forthe increased tibiofemoral compressive forces andextensor moments observed during these lifts It is
Table IV Mean EMG activities as a percentage of maximal voluntary isometric contraction ( MVIC) P-values effect size (Cohenrsquos dCohen 1988) and 95 confidence intervals between back squats and front squats during the descending and ascending phases performedwith 1RM loads
Descending phase Ascending phase
Back squat(mean plusmn s)
Front squat(mean plusmn s) P d
95 CIBack squat(mean plusmn s)
Front squat(mean plusmn s) P d
95 CI
Muscle L U L U
Rectus femoris 379 plusmn 121 464 plusmn 244 0200 044 minus22011 5164 360 plusmn 138 467 plusmn 194 0061 064 minus21917 0578Vastus medialis 483 plusmn 143 531 plusmn 193 0204 028 minus12627 3020 493 plusmn 139 589 plusmn 171 0002 062 minus15001 minus4177Vastus lateralis 459 plusmn 139 480 plusmn 158 0396 014 minus7088 3028 485 plusmn 172 562 plusmn 222 0096 039 minus16932 1590Erector spinae 411 plusmn 140 451 plusmn 120 0438 031 minus14953 6940 460 plusmn 176 481 plusmn 168 0665 012 minus12493 8292Gluteus maximus 288 plusmn 189 300 plusmn 230 0573 006 minus5460 3181 473 plusmn 277 466 plusmn 301 0841 minus002 minus7001 8447Biceps femoris 187 plusmn 149 197 plusmn 233 0765 005 minus7883 5959 349 plusmn 182 295 plusmn 287 0329 minus022 minus6257 17099Semitendinosus 150 plusmn 69 140 plusmn 81 0676 minus013 minus4052 6019 290 plusmn 162 184 plusmn 101 0039 minus079 0624 20595
Notes Significantly higher EMG activities during the front squat compared to the back squat (P lt 005) Significantly higher EMGactivities during the back squat compared to the front squat (P lt 005)
Figure 3 Minimum hip angles reached during the back squat (BS)and front squat (FS) Significant differences (P lt 005) betweenthe back and front squats
EMG Kinematic activities of back and front squat 1063
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015
very important because excessive tibiofemoral com-pressive forces could be deleterious to the menisciand articular cartilage (Escamilla 2000)
During the squat the primary muscles actingaround the knee are the quadriceps femoris (vastuslateralis vastus medialis vastus intermedius and rec-tus femoris) which carry out concentric knee exten-sion as well as eccentrically resisting knee flexionFor both back and front squats vastus medialis andvastus lateralis produced more activity than the rec-tus femoris during the whole manoeuvre which is inagreement with the data from Escamilla et al (19971998) Escamilla (2000) Escamilla et al (2000)Hwang Kim and Kim (2009) Wretneberg Feng
Lindberg and Arborelius (1993) Wretneberg et al(1996) and Isear et al (1997)
Schoenfeld (2010) reported that this may be logi-cal because the rectus femoris is both a hip flexorand knee extensor and thus shortens at one endwhile lengthening at the other during the squatwith little if any net change in length throughoutmovement
Although the loads were heavier during the backsquat mean EMG activities in selected musclesshowed no difference with only one exceptionDespite the lighter loads during the front squatvastus medialis mean EMG activity was greaterthan the back squat during the whole manoeuvresGullett et al (2009) and Stuart Meglan LutzGrowney and An (1996) reported no differences inmuscle activities between front and back squats Thedifference in our study can be resulted from thehigher loads compared to Gullett et al (2009)(70 of 1RM) and Stuart et al (1996) (50 pounds)which may recruit more motor units during themovements
When we divided the manoeuvres into ascendingand descending phases all muscles tested were moreactive during the ascending phase than during thedescending phase These findings are in accordancewith those of several other studies (Escamilla et al1998 Escamilla et al 2000 Gullett et al 2009McCaw amp Melrose 1999 Stuart et al 1996)EMG activities were higher during the ascendingphase compared to the descending phase for allmuscles during both the front and the back squatBut statistically significant differences were seen forgluteus maximus semitendinosus and bicepsfemoris during both the front and the back squatand for vastus medialis during the front squat
We observed no significant EMG activity differ-ences between the back and front squats during thedescending phases However during the ascendingphase EMG activity of the vastus medialis was higherin the front squat compared to the back squat whileEMG activity of the semitendinosus was higher inthe back squat compared to the front squat Thefront squat is believed to be a more isolated man-oeuvre for quadriceps (Grahammer 1986 Hatfield1983) and this result may support this idea Theheavier external resistance and more inclined torsoduring the back squat create a larger resistancemoment which requires greater muscular effort tocounterbalance (Swinton Aspe amp Keogh 2012) Itwas shown that increased forward trunk lean causesan increase in hamstring activity (Escamilla et al2000 Gullett et al 2009 Scotten 2010) Thismay explain the higher semitendinosus EMG activityduring the ascending phase of the back squats
When we divided the manoeuvres into 10 phasesfor being able to compare the movement patterns
Figure 4 Knee and hip angle-dependent EMG values of rectusfemoris (RF) vastus medialis (VM) vastus lateralis (VL) erectorspinae (ES) gluteus maximus (GM) biceps femoris (BF) andsemitendinosus (ST) throughout the phases of both backs squat(BS) and front squat (FS) movements Significant differences(P lt 005) between back and front squats
1064 HU Yavuz et al
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015
we did not observe any significant difference in kneeangles between the back and front squats Howeverwe observed significantly lower hip angles in 8 of 10phases during the back squat The lowest hip anglesreached during the manoeuvres were significantlylower in the back squat compared to the frontsquat These findings showed an increased forwardlean during the back squat compared to the frontsquat during maximum loading
When we check angle-specific EMG changes foreach muscle we saw that EMG activity patternswere quite parallel to each other for most of themuscles in both squat variants SemitendinosusEMG activity showed a sudden increase in thesixth phase which also shows the lowest hip angleand the starting of the ascending phase Gluteusmaximus and biceps femoris showed a similar butweaker change in pattern during the middle of theascending phase (eighth phase) This may probablybe due to the extra effort of the hip extensors tomaintain the balance by compensating the increasedforward lean during back squat
In both the squatting techniques as the perfor-mers lower throughout the eccentric phase they arerequired to lean forward in order to maintain bal-ance Centre of gravity moves further away from thelumbar spine increasing the moment arm and tor-que As a result the shear forces occurring withinthe lumbar spine would also increase (Comfort ampKasim 2007 Diggin et al 2011 Gullett et al2009) Increased forward lean reduces tolerance tocompressive load and results in a transfer of the loadfrom muscles to passive tissues heightening the riskof disc herniation (Matsumoto et al 2001)
As previously stated such an increase in shearforce under regular high loading conditions (eg1RM) may predispose an athlete to injury if theseforces continually exceed the strain capabilities ofthe joint connective tissues (Comfort amp Kasim2007) That is why it is beneficial to maintain aposture that is as close to upright as possible at alltimes for preventing the lumbar injuries (Schoenfeld2010)
Conclusion
We studied the musculature activity and kinematicsof knee and hip joints during front and back squatswith maximum loading (1RM) The front squat wasshown to be just as effective as the back squat undermaximum loading conditions in terms of overallmuscle activity with no difference in knee joint kine-matics and significantly less forward lean in hip jointwhich may probably show less lumbar injury riskWe also managed to show that the front squat cre-ated higher EMG activity in vastus medialis despitethe lighter loads compared to back squat that agrees
with the idea of ldquobeing a more isolated movementfor knee extensorsrdquo It is a known fact that the backsquat is used much more commonly compared to itsfront variation Results may suggest that the frontsquat may be a better choice for focusing on kneeextensor improvement andor for preventing lumbarinjuries under maximum loading conditions
References
American College of Sports Medicine (1998) Position standThe recommended quantity and quality of exercise for devel-oping and maintaining cardiorespiratory and muscular fitnessand flexibility in healthy adults Medicine and Science in Sportsand Exercise 975ndash991 doi101249MSS0b013e318213fefb
Baechle T R amp Earle R (2000) Essentials of strength trainingand conditioning (2nd ed) Champaign IL Human Kinetics
Balshaw T G amp Hunter A M (2012) Evaluation of electro-myography normalisation methods for the back squat Journalof Electromyography and Kinesiology 22 308ndash319
Braidot A A Brusa M H Lestussi F E amp Parera G P(2007) Biomechanics of front and back squat exercises Journalof Physics Conference Series 90 012009
Broer M R amp Houtz S J (1967) Patterns of muscular activity inselected sport skills (3rd ed) Springfield Charles C ThomasPublishing
Carpinelli R N (2008) The size principle and a critical analysisof the unsubstantiated heavier-is-better recommendation forresistance training Journal of Exercise Science and Fitness 667ndash86
Channell B T amp Barfield J P (2008) Effect of Olympic andtraditional resistance training on vertical jump improvement inhigh school boys Journal of Strength Conditioning and Research22 1522ndash1527
Clark D R Lambert M I amp Hunter A M (2012) Muscleactivation in the loaded free barbell squat A brief reviewJournal of Strength Conditioning and Research 26 1169ndash1178
Cohen J (1988) Statistical power analysis for the behavioral sciencesHillsdale NJ Lawrence Erlbaum
Comfort P amp Kasim P (2007) Optimizing squat techniqueStrength and Conditioning Journal 29 10ndash13
Delavier F (2001) Strength training anatomy Champaign ILHuman Kinetics
Diggin D OrsquoRegan C Whelan N Daly S McLoughlin VMcNamara L amp Reilly A (2011) A biomechanical ana-lysis of front vs back squat Injury implications PortugueseJournal of Sports Sciences 11(Suppl 2) Retrieved from httpwwwresearchgatenetpublication258363730_A_biomechanical_Analysis_of_front_and_back_squat_injury_implicationsfilee0b49528105693baa7pdf
Dionisio V C Almeida G L Duarte M amp Hirata R P(2008) Kinematic kinetic and EMG patterns during down-ward squatting Journal of Electromyography and Kinesiology 18134ndash143
Donnelly D V Berg W P amp Fiske D M (2006) The effectof the direction of gaze on the kinematics of the squat exerciseJournal of Strength Conditioning and Research 20 145ndash150Retrieved from httpwwwresearchgatenetpublication7273329_The_effect_of_the_direction_of_gaze_on_the_kinem-atics_of_the_squat_exerciselinks0c960523c48a69975c000000+ampcd=2amphl=trampct=clnk
Escamilla R F (2000) Knee biomechanics of the dynamic squatexercise Medicine amp Science in Sports amp Exercise 33 127ndash141
Escamilla R F Fleisig G S Lowry T M Barrentine S Wamp Andrews J R (2001) A three-dimensional biomechanicalanalysis of the squat during varying stance widths Medicine and
EMG Kinematic activities of back and front squat 1065
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015
Science in Sports and Exercise 33 984ndash998 Retrieved fromhttpwwwsweatpitcomforumstudiesSquattingA20three-dimensional20biomechanical20analysispdf
Escamilla R F Fleisig G S Zheng N Barrentine S WWilk K E amp Andrews J R (1998) Biomechanics of theknee during closed kinetic chain and open kinetic chain exer-cises Medicine and Science in Sports and Exercise 30 556ndash569doi10109700005768-199804000-00014
Escamilla R F Fleisig G S Zheng N Lander J EBarrentine S W Andrews J R Moorman C T(1997) The effects of technique variations on knee biomecha-nics during the squat and leg press Medicine and Science inSports and Exercise 29 156 doi10109700005768-200109000-00020
Escamilla R F Fleisig G S Zheng N Lander J EBarrentine S W Andrews J R hellip Moorman III C T(2000) Effects of technique variations on knee biomechanicsduring the squat and leg press Medicine amp Science in Sports ampExercise 33 1552ndash1566
Flanagan S Salem G J Wang M Y Sanker S ampGreendale G A (2003) Squatting exercises in older adultsKinematic and kinetic comparisons Medicine and Science inSports and Exercise 35 635ndash643 doi10124901MSS00000583644797306
Fleck S J (1999) Periodized strength training A critical reviewJournal of Strength Conditioning amp Research 13 82ndash89 Retrievedfrom httpjournalslwwcomnsca-jscrabstract199902000periodized_strength_training__a_critical_review15aspx
Grahammer J (1986) Sports illustrated strength training NewYork NY Harper amp Row
Gullett J C Tillman M D Gutierrez G M amp Chow J W(2009) A biomechanical comparison of back and front squatsin healthy trained individuals Journal of Strength andConditioning Research 23 284ndash292
Hasegawa I (2004) Using the overhead squat for core develop-ment NSCA Performance Training Journal 6 19ndash21
Hatfield F C (1983) Power A scientific approach Chicago ILContemporary Books Inc
Hay J G Andrews J G Vaughan C L amp Ueya K (1983)Load speed and equipment effects in strength-training exer-cises In H Matsui amp K Kobayashi (Eds) Biomechanics (3rded) Champaign IL Human Kinetics
Hwang S Kim Y amp Kim Y (2009) Lower extremity jointkinetics and lumbar curvature during squat and stoop liftingBMC Musculoskeletal Disorders 10 15 doi1011861471-2474-10-15
Isear J A Erickson Jr J C amp Worrel T W (1997) EMGanalysis of lower extremity muscle recruitment patterns duringan unloaded squat Medicine amp Science in Sports amp Exercise 29532ndash539
Kellis E Arambatzi F amp Papadopoulos C (2005) Effects ofload on ground reaction force and lower limb kinematics dur-ing concentric squats Journal of Sports Sciences 23 1045ndash1055
Konrad P (2005) ABC of EMG a practical introduction to kinesio-logical electromyography (1st ed) Scottsdale AZ Noraxon Inc
Kraemer W J amp Fry A C (1995) Strength testingDevelopment and evaluation of methodology In P Maud ampC Foster (Eds) Physiological assessment of human fitness(pp 115ndash138) Champaign IL Human Kinetics
Kraemer W J amp Ratamess N A (2004) Fundamentals ofresistance training Progression and exercise prescriptionMedicine amp Science in Sports amp Exercise 36 674ndash688
Matsumoto H Suda Y Otani T Niki Y Seedhom B B ampFujikawa K (2001) Roles of the anterior cruciate ligamentand the medial collateral ligament in preventing valgus instabil-ity Journal of Orthopaedic Science 6 28ndash32
McCaw S T amp Melrose D R (1999) Stance width and barload effects on leg muscle activity during the parallel squatMedicine and Science in Sports and Exercise 31 428ndash436
Merletti R (1999) Standards for reporting EMG data Journal ofElectromyography and Kinesiology 9 3ndash4 Retrieved from httpwwwisek onlineorgstandards_emghtml
Rippetoe M amp Kilgore L (2007) Starting strength Basic barbelltraining (2nd ed) Wichita Falls TX The Aasgaard Company
Russell P J amp Phillips S J (1989) A preliminary comparison offront and back squat exercises Research Quarterly for Exerciseand Sport 60 201ndash208
Schoenfeld B J (2010) Squatting kinematics and kinetics andtheir application to exercise performance Journal of Strengthand Conditioning Research 24 3497ndash3506
Scotten C M (2010) Differences in muscle activation in the lowerextremities while performing traditional squats and non-traditionalsquats (Master thesis) Boise State University Boise
Senter C amp Hame S L (2006) Biomechanical analysis of tibialtorque and knee flexion angle Implications for understandingknee injury Sports Medicine 36 635ndash641
Stensdotter A K Hodges P W Mellor R Sundelin G ampHager R C (2003) Quadriceps activation in closed and in openkinetic chain exercise Medicine and Science in Sports and Exercise35 2043ndash2047 doi10124901MSS000009910703704AE
Stuart M J Meglan D A Lutz G E Growney E S amp AnK N (1996) Comparison of intersegmental tibiofemoraljoint forces and muscle activity during various closed kineticchain exercises The American Journal of Sports Medicine 24792ndash799
Swinton P A Aspe R amp Keogh J (2012 July)Electromyographic comparison of The back squat and overheadsquat 30th Annual Conference of Biomechanics İn SportsMelbourne
Wretneberg P Feng Y amp Arborelius U P (1996) High- andlow-bar squatting techniques during weight-training Medicineand Science in Sports and Exercise 28 218ndash224
Wretneberg P Feng Y Lindberg F amp Arborelius U P(1993) Joint moments of force and quadriceps muscle activityduring squatting exercise Scandinavian Journal of Medicine ampScience in Sports 3 244ndash250
1066 HU Yavuz et al
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015

Kinematic and EMG activities during front and back squat variations inmaximum loads
HASAN ULAS YAVUZ1 DENIZ ERDAĞ2 ARIF MITHAT AMCA3 amp SERDAR ARITAN3
1Sports Medicine Near East University Hospital Nicosia Cyprus 2School of Physical Education and Sports Near EastUniversity Nicosia Cyprus and 3Faculty of Sports Sciences Hacettepe University Ankara Turkey
(Accepted 1 November 2014)
AbstractThe aim of this study was to compare the musculature activity and kinematics of knee and hip joints during front and backsquat with maximal loading Two-dimensional kinematical data were collected and electromyographic activities of vastuslateralis vastus medialis rectus femoris semitendinosus biceps femoris gluteus maximus and erector spinae weremeasured while participants (n = 12 212 plusmn 19 years old) were completing front and back squat exercises with maximumloading Paired sample t-test was used for comparisons between two techniques Results showed that the electromyographicactivity of vastus medialis was found to be greater in the front squat compared to the back squat during the ascending phase(P lt 005 d = 062 95 CI minus150minus417) and the whole manoeuvre (P lt 005 d = 041 95 CI minus128minus043) whilesemitendinosus (P lt 005 d = minus079 95 CI 0622059) electromyographic activity was greater in the back squat duringthe ascending phase Compared to the front squat version back squat exhibited significantly greater trunk lean with nodifferences occurring in the knee joint kinematics throughout the movement Results may suggest that the front squat maybe preferred to the back squat for knee extensor development and for preventing possible lumbar injuries during maximumloading
Keywords strength training electromyography biomechanics two-dimensional maximal loading
Introduction
Progressive resistance training is an effective methodfor developing muscular strength for performance aswell as for injury prevention and rehabilitation(American College of Sports Medicine 1998)Choosing the right exercise is one of the most impor-tant factors for achieving the aims of the programme(Fleck 1999)
The squat is a staple multiple joint free weight resis-tance exercise that develops not only the quadriceps(rectus femoris vastus lateralis and vastus medialis)but also the hamstrings (biceps femoris and semitendi-nosus) and it also loads the erector spinae (ES)(McCaw amp Melrose 1999)
Increasing the power of these muscles can oftentranslate into improved performance in one or sev-eral athletic skills (sprinting jumping throwing andstriking) (Balshaw amp Hunter 2012 Channell ampBarfield 2008) Due to the popularity of the exer-cise many variations have been created by alteringthe placement of the squat bar back squat (barbellheld across the back slightly above or below the level
of the acromion) front squat (barbell held in front ofthe chest approximately at the level of the clavicles)(Donnelly Berg amp Fiske 2006) or overhead squat(barbell held over the head while elbows are fullyextended) (Hasegawa 2004) altering squat depthpartial squats (40deg knee angle) half squats (70deg to100deg) and deep squats (greater than 100deg)(Schoenfeld 2010) altering stance width narrow(87ndash118 shoulder width) medium (121ndash153shoulder width) or wide (158ndash196 shoulderwidth) (Escamilla 2000) altering foot rotationinternally or externally rotated feet or altering squat-ting surface stable or labile (power board BOSUball balance cone) However no standardised mea-sures of quantification have been universally recog-nised and terminology can differ betweenresearchers (Schoenfeld 2010)
Two common forms of the squat are the back squat(Figure 1(a)) and the front squat (Figure 1(b))Competitive or recreational athletes regularly performthe back squat while the front squat is much lesscommon Although both squats effectively work thelower back hip and leg muscles there are slight
Correspondence Hasan Ulas Yavuz Sports Medicine Near East University Hospital Dikmen Nicosia 99380 Cyprus E-mail ulasyavuzneuedutr
Journal of Sports Sciences 2015Vol 33 No 10 1058ndash1066 httpdxdoiorg101080026404142014984240
copy 2015 Taylor amp Francis
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015
variations in technique and muscular involvement(Gullett Tillman Gutierrez amp Chow 2009)
Several studies have described the patterns of thekinematics kinetics and muscle activities of the kneehip and ankle during the squat (Dionisio AlmeidaDuarte amp Hirata 2008 Escamilla Fleisig LowryBarrentine amp Andrews 2001 Escamilla et al 1998Flanagan Salem Wang Sanker amp Greendale 2003Hasegawa 2004 Isear Erickson amp Worrel 1997McCaw amp Melrose 1999 Stensdotter HodgesMellor Sundelin amp Hager 2003 Wretneberg FengampArborelius 1996)However only a few of themhavecompared front and back squat (Braidot BrusaLestussi amp Parera 2007 Diggin et al 2011 Gullettet al 2009) and even less have studied electromyogra-phy (EMG) and kinematics together in the same studyto see the interactions (Gullett et al 2009)
Braidot et al (2007) compared the kinematicsdynamics the power and the energy in the differentjoints during the complete cycle from the exercise inthe different variants of squat A better developmentof energy with the front bar is observed in the kneeallowing a better muscular exercise with the sameload In the study of Diggin et al (2011) back squatexhibited a significantly greater trunk lean than thefront squat (P lt 005) with no differences in theknee joint kinematics However these studies didnot quantify the electromyographic data and muscleactivity during the front and back squatFurthermore the load to evaluate the exercise iscalculated on the basis of 50 of one repetitionmaximum (1RM) for both variants
Gullett et al (2009) reported that the front squatwas as effective as the back squat in terms of overall
muscle recruitment with 70 of 1RM load for eachsquat technique Heavy loading in experienced indi-viduals is needed to recruit the high-threshold motorunits that may not be activated during light-to-moderate lifting (Kraemer amp Ratamess 2004)Besides during lower loading conditions strongermuscles may compensate the activation of weakerones and cause personal varieties But during max-imal loading all related muscles must be fully acti-vated in order to complete the manoeuvre That willform a normalisation in terms of muscle activity andnaturally EMG signalling Clark Lambert andHunter (2012) emphasised that the sub-maximalload used in Gulletrsquos study might have failed to elicitthe possible difference between back and front squatFurthermore an increase in trunk forward lean wasshown with higher loads by Hay Andrews Vaughanand Ueya (1983) and Kellis Arambatzi andPapadopoulos (2005) during squat Thereforeobviously squat kinematics and EMG signalisationpattern can change with maximal loading
We aimed to compare the musculature activity andkinematics of knee and hip joints during front and backsquat with maximal loading and investigate the possi-ble differences in these two common squat variations
Methods
Participants
Twelve healthy male individuals who were experi-enced at performing front and back squats partici-pated in this study All participants were right-handed and had no history of orthopaedic injury
Figure 1 (a) Bar positioning during the back squat (b) Bar positioning during the front squat
EMG Kinematic activities of back and front squat 1059
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015
or surgery that would have limited their ability toperform the squatting techniques Before participa-tion informed consent was obtained from eachparticipant The investigation was conductedaccording to the Declaration of Helsinki andapproved by the Near East University ScientificResearches Evaluation and Ethic Commission(YDUuml201211ndash60)
Instrumentation
An eight-channel dual-mode portable EMG andphysiological signal data acquisition system(Myomonitor IV Delsys Inc Boston MA USA)was used for data collection Data collections wereconducted using EMG Works Acquisition 405(Delsys Inc) The amplifier bandwidth frequencyranged from 20 to 450 Hz with an input voltage of9 VDC at 07 A and the common-mode rejectionratio was 80 dB Data were recorded at a samplingrate of 1000 Hz over a wireless local area network tothe host computer for real-time display and storage
Seven channels of this system were used to assessthe EMG activity of vastus lateralis vastus medialisrectus femoris semitendinosus biceps femoris glu-teus maximus and ES Recording sites were pre-pared by shaving the area and wiping with alcoholpads to decrease electrical impedance Electrodes(41 times 20 times 5 mm DE-23 Delsys Inc) were placedalong the longitudinal axis of each muscle tested onthe right side (dominant side) of the participantrsquosbody according to the procedures from Gullettet al (2009) (Table I) The sensor contacts aremade from 999 pure silver bars measuring10 mm in length 1 mm in diameter and spaced10 mm apart from optimal signal detection and con-sistency A 508 cm diameter oval-shaped commonreference electrode (Dermatrode HE-R AmericanImex Irvine CA USA) was placed on the iliaccrest of the right leg
At the same time the EMG system was synchro-nised with a Samsung (VP-D375 W) video camera
with a shutter speed of 1250 s by using NationalInstruments USB-6501 Digital IO trigger box(Delsys Inc) Video recordings were made withAMCap (Microsoft V 309) video capture softwareFor kinematical data reflective markers (3 cm dia-meter) were attached and positioned over the follow-ing bony landmarks (a) lateral malleolus of the rightfoot (b) upper edges of the lateral tibial plateau ofthe right knee (c) posterior aspect of the greatertrochanters of the right femur and (d) end of theright side of the Olympic bar A calibration planethat consists of eight control points was used for two-dimensional spatial reconstruction
A standard 205-kg Olympic barbell discs(Werksan Ankara Turkey) and a continental squatrack were used during the squat
Procedures
The participants were required to attend two ses-sions A pretest was given to each participant 1week before the actual testing session The experi-mental protocol was reviewed and the participantswere given the opportunity to ask questions Duringthe pretest the participantrsquos RM was determinedand recorded for the back squat and front squatThe procedure used for assessing 1RM wasdescribed by Kraemer and Fry (1995) The partici-pants were asked to perform initial preparation on astationary bike for 3ndash5 min at the beginning of thepretest session and then performed a warm-up set of8ndash10 repetitions at a light weight (approximately50 of assumed 1RM) A second initial preparationconsisting of a set of three to five repetitions withmoderate weight (approximately 75 of 1RM) and athird initial preparation including one to three repe-titions with a heavy weight (approximately 90 of1RM) followed
After the initial preparation the participants per-formed 1RM strength exercises by enhancing the loadduring consecutive trials until the participants wereunable to properly perform a proper lift complete
Table I A description of the positioning of each electrode in relation to the muscle being tested developed by Broer and Houtz (1967) anddescribed by Gullett et al (2009)
Muscle Electrode placement
Rectus femoris Approximately midway between the anterior inferior iliac spine and the patella on the anterior side of the thighVastus lateralis Approximately two-thirds of the thigh length from the greater trochanter on the lateral side of the thighVastus medialis Approximately three-fourths of the thigh length from the anterior inferior iliac spine on the medial side of the thighErector spinae Three centimetres lateral to the L3 spinous processGluteus maximus 50 on the line between the sacral vertebrae and the greater trochanter This position corresponds with the greatest
prominence of the middle of the buttocks well above the visible bulge of the greater trochanterBiceps femoris Midway between the ischial tuberosity and the lateral condyle of the femur on the posterior side of the thighSemitendinosus Midway between the ischial tuberosity and the medial condyle of the femur on the posterior side of the thighReference electrode Iliac crest of the right leg
1060 HU Yavuz et al
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015
range of motion and correct technique Each partici-pant was asked to lower the bar to the point where theknee angle was 90deg (Figure 2) which was marked byadjustable stoppers Adequate rest was allowedbetween trials (3ndash5 min) Subsequently 1 week afterthe pretest session the participants performed a sec-ond session for data collection For each participantall data collection was performed in one day session
After the EMG electrode placement maximumvoluntary isometric contraction (MVIC) data fromthe quadriceps hamstrings erector spine and glu-teus maximus were collected according to the pro-cedures described by Konrad (2005) Three 3-sMVIC trials were collected in a randomised mannerfor each muscle group Adequate rest was allowedbetween trials (1 min)
All participants performed two to three warm-upsets in preparation for testing For both lifting varia-tions each participant used their 1RM weights pre-viously established for the back squat and frontsquat Exercise began with a given verbal commandThe starting and ending positions for the back squatand front squat were with the knees in full extensionwhich was defined as 180deg knee angle From thestarting position the participant flexed their kneesto minimum knee angle (approximately 90deg) andthen extended their knees back to the startingposition
During the back squat the barbell positionedacross the shoulder on the trapezius slightly abovethe posterior aspect of the deltoids and the hips andknees flexed until the thighs are parallel to the floor(Baechle and Earle 2000 Delavier 2001) Thenthe participant extended the hips and knees untilthe starting position is reached keeping the backflat the heels on the floor and the knees alignedover the feet (Baechle and Earle 2000 Delavier2001) During the front squat the barbell positionedacross the anterior deltoids and clavicles and theelbows fully flexed to position the upper arms paral-lel to the floor (Baechle and Earle 2000 Delavier
2001) The descending and ascending motions aremuch the same as in the back squat (Gullett et al2009) Adequate rest was allowed between trials (3ndash5 min)
Data reduction
The sampling of EMG and video recordings wereinitiated simultaneously with the beginning of thefirst squat repetition For synchronisation a LEDconnected to the trigger box (National InstrumentsUSB-6501 Digital IO) outputted a digital signalwhen the Myomonitor started data acquisitionWith the data acquisition the LED lit and it wentoff as the data stopped The data obtained from thisprocedure were used to specify the start of therequired portion and the length of the requestedportion
Kinematical data were analysed by using thesaSuite two-dimensional kinematical analysis pro-gramme which was developed by HacettepeUniversity Faculty of Sports SciencesBiomechanics Research Group Ankara TurkeyFor each trail the required portion of the videorecordings was trimmed the anthropometric pointswere digitised and the two-dimensional positionaldata were obtained The raw position data of thejoints were smoothed using a moving average filterand the angular kinematics of the knee and hip jointswere calculated All EMG data were partitioned intoascending and descending phases Movement timewas normalised into 10 movement phases to controlinter-individual differences Knee and hip anglechanges were examined throughout the descendingand ascending phases
EMG data were analysed according to the proce-dures from International Society ofElectrophysiology and Kinesiology (Merletti 1999)by using the EMG Works Analysis 40 (Delsys IncBoston) To calculate the mean normalised EMGvalues the raw EMG signals were subsetted filtered(Passband 3 Response Bandpass Corner F110 Hz Corner F2 500 Hz) rectified integrated(root mean square (Window Length 0100Window Overlap 008 Remove Ofset)) and nor-malised to the participants highest correspondingMVIC trial
Statistical analysis
Kinematic and electromyographic data were ana-lysed and compared between the front and backsquad by using paired sample t-tests (P lt 005)Throughout the text data for all participants per-forming each type of exercise were averaged andpresented as means standard deviations P-valueeffect size (Cohenrsquos d Cohen 1988) and 95
Figure 2 Illustrations of measured joint angles during back squatand front squat (adapted from Starting Strength Basic BarbellTraining by permission of The Aasgaard Company Rippetoe ampKilgore 2007)
EMG Kinematic activities of back and front squat 1061
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015
confidence intervals Cohenrsquos categories were usedto evaluate the magnitude of these sizes (small if0 le [d] le 05 medium if 05 le [d] le 08 and large if[d] gt 08) (Cohen 1988)
Results
The mean 1RM loads that were employed duringtesting were 10917 plusmn 2551 kg for the back squatand 8500 plusmn 1567 kg for the front squat This was13883 plusmn 3262 of their body weight for back squatand 10587 plusmn 2434 for front squat Participantscould lift significantly higher loads with back squatcomparing to the front squat (P lt 005 d = minus12895 CI 16283204)
Normalised EMG values as a percentage of max-imal voluntary isometric contraction ( MVIC)P-values effect size (Cohenrsquos d Cohen 1988) and95 confidence intervals between back and frontsquats are shown in Table II Vastus medialisEMG activity was found to be greater during thefront squat compared to back squat (P lt 005
d = 041 95 CI minus128minus43) There were noother differences in any other muscles
Normalised average EMG values as a MVIC P-values effect size (Cohenrsquos d Cohen 1988) and 95confidence intervals between descending and ascend-ing phases performed with 1RM loads between backand front squats are shown in Table III EMG activ-ities of gluteus maximus (P lt 005 d = 078 95 CIminus2581minus1120) biceps femoris (P lt 005 d = 09795 CI minus1974minus1260) and semitendinosus(P lt 005 d = 105 95 CI minus2072minus728) duringback squat and EMG activities of gluteus maximus(P lt 005 d = 062 95 CI minus2209minus1118) bicepsfemoris (P lt 005 d = 038 95 CI minus1486minus471)and semitendinosus (P lt 005 d = 048 95 CIminus840minus34) during front squat were found to be sig-nificantly higher EMG activity of the vastus medialis(P lt 005 d = 032 95CI minus1103minus53) during theascending phase was higher only
The mean EMG activities as a percentage of max-imal voluntary isometric contraction ( MVIC)P-values effect size (Cohenrsquos d Cohen 1988) and
Table II Mean EMG activities as a percentage of maximal voluntary isometric contraction ( MVIC) P-values effect size(Cohenrsquos d Cohen 1988) and 95 confidence intervals for the back squats and front squats throughout entire movementsperformed with 1RM loads
Muscle Back squat (mean plusmn s) Front squat (mean plusmns) P d
95 CI
L U
Rectus femoris 367 plusmn 124 461 plusmn 217 0118 053 minus217 282Vastus medialis 488 plusmn 139 554 plusmn 180 0038 041 minus128 minus043Vastus lateralis 470 plusmn 151 512 plusmn 173 0149 026 minus102 minus175Erector spinae 432 plusmn 156 462 plusmn 121 0495 022 minus125 049Gluteus maximus 371 plusmn 235 372 plusmn 270 0959 0 minus55 523Biceps femoris 262 plusmn 161 241 plusmn 254 0611 minus0 minus65 106Semitendinosus 215 plusmn 117 160 plusmn 87 0115 minus053 minus16 126
Note Significantly higher EMG activities during the front squat compared to the back squat (P lt 005)
Table III Back squats and front squats mean EMG activities as a percentage of maximal voluntary isometric contraction ( MVIC)P-values effect size (Cohenrsquos d Cohen 1988) and 95 confidence intervals between descending and ascending phases performed with1RM loads
Back squat Front squat
Descendingphase
(mean plusmns)
Ascendingphase
(mean plusmn s) P d
95 CI Descendingphase
(mean plusmn s)
Ascendingphase
(mean plusmn s) P d
95 CI
Muscle L U L U
Rectus femoris 379 plusmn 121 360 plusmn 138 0455 minus015 minus3562 minus7432 464 plusmn 244 467 plusmn 194 0922 001 minus7122 6500Vastus medialis 483 plusmn 143 493 plusmn 139 0617 007 minus5293 3286 531 plusmn 193 589 plusmn 171 033 032 minus11036 minus533Vastus lateralis 459 plusmn 139 485 plusmn 172 0223 017 minus7005 1821 480 plusmn 158 562 plusmn 222 068 043 minus17190 07269Erector spinae 411 plusmn 140 460 plusmn 176 0124 031 minus11286 1564 451 plusmn 120 481 plusmn 168 0451 020 minus11276 5367Gluteus maximus 288 plusmn 189 473 plusmn 277 0000 078 minus25810 minus11200 300 plusmn 230 466 plusmn 301 0000 062 minus22098 minus11188Biceps femoris 187 plusmn 149 349 plusmn 182 0000 097 minus19740 minus12600 197 plusmn 233 295 plusmn 287 0001 038 minus14864 minus4711Semitendinosus 150 plusmn 69 290 plusmn 162 0001 105 minus20720 minus7280 140 plusmn 81 184 plusmn 101 0036 048 minus8404 minus0343
Note Significantly higher EMG activities during the ascending phase compared to the descending phase (P lt 005)
1062 HU Yavuz et al
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015
95 confidence intervals between back squats andfront squats during the descending and ascendingphases performed with 1RM loads are shownin Table IV There were no significant differencesobserved between back and front squats duringthe descending phase During the ascending phasethe EMG activity of the vastus medialis was foundto be significantly higher in the front squat comparedto the back squat (P lt 005 d = 062 95 CIminus1500minus417) while the EMG activity of the semi-tendinosus was higher in the back squat compared tothe front squat (P lt 05 d = minus079 95 CI 622059)
As can be seen from Figure 3 significant differ-ences were observed between minimum hip anglesreached during back squats and front squats Theaverage minimum hip angle was significantly higher(P lt 005 d = 108 95 CI minus2857minus428) duringthe front squat compared to the back squat
Figure 4 shows the mean changes in knee and hipangles throughout the ascending phases of bothsquatting movements No difference was observed
in knee angles during the whole movement whilehip angles were lower in 8 of 10 phases during theback squat compared to front squat showing anobvious forward trunk lean According to theangle-specific EMG changes semitendinosus(P lt 005 d = minus023 95 CI minus2421111) showeda sudden increase in the sixth phase and bicepsfemoris (P lt 005 d = minus014 95 CI minus10931911) and gluteus maximus (P lt 005 d = minus03795 CI minus4533089) showed a similar but smallerincrease in the eighth phase during the back squatcompared to the front squat
Discussion
Participants could lift significantly greater loads withback squat compared to the front squat(1388 plusmn 326 of their body weight1059 plusmn 243 of their body weight respectively)(Figure 1) and this finding is consistent with theprevious studies (Gullett et al 2009 Russell ampPhillips 1989)
Instead of the load the level of effort in voluntarymuscle actions determines the degree of motor unitactivity (Carpinelli 2008) consequently the level ofEMG signalling increases Furthermore higherloads may increase intradiscal pressure (11) com-pression on vertebral bodies (10) tibiofemoral (1213) and patellofemoral joints (14) which could pos-sibly increase the risk of injury while performingsquat Gullett et al (2009) emphasised that the mus-cles tested were equally active during the front squatwhile lifting less mass and it seems that the extraload lifted during the back squat is what accounts forthe increased tibiofemoral compressive forces andextensor moments observed during these lifts It is
Table IV Mean EMG activities as a percentage of maximal voluntary isometric contraction ( MVIC) P-values effect size (Cohenrsquos dCohen 1988) and 95 confidence intervals between back squats and front squats during the descending and ascending phases performedwith 1RM loads
Descending phase Ascending phase
Back squat(mean plusmn s)
Front squat(mean plusmn s) P d
95 CIBack squat(mean plusmn s)
Front squat(mean plusmn s) P d
95 CI
Muscle L U L U
Rectus femoris 379 plusmn 121 464 plusmn 244 0200 044 minus22011 5164 360 plusmn 138 467 plusmn 194 0061 064 minus21917 0578Vastus medialis 483 plusmn 143 531 plusmn 193 0204 028 minus12627 3020 493 plusmn 139 589 plusmn 171 0002 062 minus15001 minus4177Vastus lateralis 459 plusmn 139 480 plusmn 158 0396 014 minus7088 3028 485 plusmn 172 562 plusmn 222 0096 039 minus16932 1590Erector spinae 411 plusmn 140 451 plusmn 120 0438 031 minus14953 6940 460 plusmn 176 481 plusmn 168 0665 012 minus12493 8292Gluteus maximus 288 plusmn 189 300 plusmn 230 0573 006 minus5460 3181 473 plusmn 277 466 plusmn 301 0841 minus002 minus7001 8447Biceps femoris 187 plusmn 149 197 plusmn 233 0765 005 minus7883 5959 349 plusmn 182 295 plusmn 287 0329 minus022 minus6257 17099Semitendinosus 150 plusmn 69 140 plusmn 81 0676 minus013 minus4052 6019 290 plusmn 162 184 plusmn 101 0039 minus079 0624 20595
Notes Significantly higher EMG activities during the front squat compared to the back squat (P lt 005) Significantly higher EMGactivities during the back squat compared to the front squat (P lt 005)
Figure 3 Minimum hip angles reached during the back squat (BS)and front squat (FS) Significant differences (P lt 005) betweenthe back and front squats
EMG Kinematic activities of back and front squat 1063
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015
very important because excessive tibiofemoral com-pressive forces could be deleterious to the menisciand articular cartilage (Escamilla 2000)
During the squat the primary muscles actingaround the knee are the quadriceps femoris (vastuslateralis vastus medialis vastus intermedius and rec-tus femoris) which carry out concentric knee exten-sion as well as eccentrically resisting knee flexionFor both back and front squats vastus medialis andvastus lateralis produced more activity than the rec-tus femoris during the whole manoeuvre which is inagreement with the data from Escamilla et al (19971998) Escamilla (2000) Escamilla et al (2000)Hwang Kim and Kim (2009) Wretneberg Feng
Lindberg and Arborelius (1993) Wretneberg et al(1996) and Isear et al (1997)
Schoenfeld (2010) reported that this may be logi-cal because the rectus femoris is both a hip flexorand knee extensor and thus shortens at one endwhile lengthening at the other during the squatwith little if any net change in length throughoutmovement
Although the loads were heavier during the backsquat mean EMG activities in selected musclesshowed no difference with only one exceptionDespite the lighter loads during the front squatvastus medialis mean EMG activity was greaterthan the back squat during the whole manoeuvresGullett et al (2009) and Stuart Meglan LutzGrowney and An (1996) reported no differences inmuscle activities between front and back squats Thedifference in our study can be resulted from thehigher loads compared to Gullett et al (2009)(70 of 1RM) and Stuart et al (1996) (50 pounds)which may recruit more motor units during themovements
When we divided the manoeuvres into ascendingand descending phases all muscles tested were moreactive during the ascending phase than during thedescending phase These findings are in accordancewith those of several other studies (Escamilla et al1998 Escamilla et al 2000 Gullett et al 2009McCaw amp Melrose 1999 Stuart et al 1996)EMG activities were higher during the ascendingphase compared to the descending phase for allmuscles during both the front and the back squatBut statistically significant differences were seen forgluteus maximus semitendinosus and bicepsfemoris during both the front and the back squatand for vastus medialis during the front squat
We observed no significant EMG activity differ-ences between the back and front squats during thedescending phases However during the ascendingphase EMG activity of the vastus medialis was higherin the front squat compared to the back squat whileEMG activity of the semitendinosus was higher inthe back squat compared to the front squat Thefront squat is believed to be a more isolated man-oeuvre for quadriceps (Grahammer 1986 Hatfield1983) and this result may support this idea Theheavier external resistance and more inclined torsoduring the back squat create a larger resistancemoment which requires greater muscular effort tocounterbalance (Swinton Aspe amp Keogh 2012) Itwas shown that increased forward trunk lean causesan increase in hamstring activity (Escamilla et al2000 Gullett et al 2009 Scotten 2010) Thismay explain the higher semitendinosus EMG activityduring the ascending phase of the back squats
When we divided the manoeuvres into 10 phasesfor being able to compare the movement patterns
Figure 4 Knee and hip angle-dependent EMG values of rectusfemoris (RF) vastus medialis (VM) vastus lateralis (VL) erectorspinae (ES) gluteus maximus (GM) biceps femoris (BF) andsemitendinosus (ST) throughout the phases of both backs squat(BS) and front squat (FS) movements Significant differences(P lt 005) between back and front squats
1064 HU Yavuz et al
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015
we did not observe any significant difference in kneeangles between the back and front squats Howeverwe observed significantly lower hip angles in 8 of 10phases during the back squat The lowest hip anglesreached during the manoeuvres were significantlylower in the back squat compared to the frontsquat These findings showed an increased forwardlean during the back squat compared to the frontsquat during maximum loading
When we check angle-specific EMG changes foreach muscle we saw that EMG activity patternswere quite parallel to each other for most of themuscles in both squat variants SemitendinosusEMG activity showed a sudden increase in thesixth phase which also shows the lowest hip angleand the starting of the ascending phase Gluteusmaximus and biceps femoris showed a similar butweaker change in pattern during the middle of theascending phase (eighth phase) This may probablybe due to the extra effort of the hip extensors tomaintain the balance by compensating the increasedforward lean during back squat
In both the squatting techniques as the perfor-mers lower throughout the eccentric phase they arerequired to lean forward in order to maintain bal-ance Centre of gravity moves further away from thelumbar spine increasing the moment arm and tor-que As a result the shear forces occurring withinthe lumbar spine would also increase (Comfort ampKasim 2007 Diggin et al 2011 Gullett et al2009) Increased forward lean reduces tolerance tocompressive load and results in a transfer of the loadfrom muscles to passive tissues heightening the riskof disc herniation (Matsumoto et al 2001)
As previously stated such an increase in shearforce under regular high loading conditions (eg1RM) may predispose an athlete to injury if theseforces continually exceed the strain capabilities ofthe joint connective tissues (Comfort amp Kasim2007) That is why it is beneficial to maintain aposture that is as close to upright as possible at alltimes for preventing the lumbar injuries (Schoenfeld2010)
Conclusion
We studied the musculature activity and kinematicsof knee and hip joints during front and back squatswith maximum loading (1RM) The front squat wasshown to be just as effective as the back squat undermaximum loading conditions in terms of overallmuscle activity with no difference in knee joint kine-matics and significantly less forward lean in hip jointwhich may probably show less lumbar injury riskWe also managed to show that the front squat cre-ated higher EMG activity in vastus medialis despitethe lighter loads compared to back squat that agrees
with the idea of ldquobeing a more isolated movementfor knee extensorsrdquo It is a known fact that the backsquat is used much more commonly compared to itsfront variation Results may suggest that the frontsquat may be a better choice for focusing on kneeextensor improvement andor for preventing lumbarinjuries under maximum loading conditions
References
American College of Sports Medicine (1998) Position standThe recommended quantity and quality of exercise for devel-oping and maintaining cardiorespiratory and muscular fitnessand flexibility in healthy adults Medicine and Science in Sportsand Exercise 975ndash991 doi101249MSS0b013e318213fefb
Baechle T R amp Earle R (2000) Essentials of strength trainingand conditioning (2nd ed) Champaign IL Human Kinetics
Balshaw T G amp Hunter A M (2012) Evaluation of electro-myography normalisation methods for the back squat Journalof Electromyography and Kinesiology 22 308ndash319
Braidot A A Brusa M H Lestussi F E amp Parera G P(2007) Biomechanics of front and back squat exercises Journalof Physics Conference Series 90 012009
Broer M R amp Houtz S J (1967) Patterns of muscular activity inselected sport skills (3rd ed) Springfield Charles C ThomasPublishing
Carpinelli R N (2008) The size principle and a critical analysisof the unsubstantiated heavier-is-better recommendation forresistance training Journal of Exercise Science and Fitness 667ndash86
Channell B T amp Barfield J P (2008) Effect of Olympic andtraditional resistance training on vertical jump improvement inhigh school boys Journal of Strength Conditioning and Research22 1522ndash1527
Clark D R Lambert M I amp Hunter A M (2012) Muscleactivation in the loaded free barbell squat A brief reviewJournal of Strength Conditioning and Research 26 1169ndash1178
Cohen J (1988) Statistical power analysis for the behavioral sciencesHillsdale NJ Lawrence Erlbaum
Comfort P amp Kasim P (2007) Optimizing squat techniqueStrength and Conditioning Journal 29 10ndash13
Delavier F (2001) Strength training anatomy Champaign ILHuman Kinetics
Diggin D OrsquoRegan C Whelan N Daly S McLoughlin VMcNamara L amp Reilly A (2011) A biomechanical ana-lysis of front vs back squat Injury implications PortugueseJournal of Sports Sciences 11(Suppl 2) Retrieved from httpwwwresearchgatenetpublication258363730_A_biomechanical_Analysis_of_front_and_back_squat_injury_implicationsfilee0b49528105693baa7pdf
Dionisio V C Almeida G L Duarte M amp Hirata R P(2008) Kinematic kinetic and EMG patterns during down-ward squatting Journal of Electromyography and Kinesiology 18134ndash143
Donnelly D V Berg W P amp Fiske D M (2006) The effectof the direction of gaze on the kinematics of the squat exerciseJournal of Strength Conditioning and Research 20 145ndash150Retrieved from httpwwwresearchgatenetpublication7273329_The_effect_of_the_direction_of_gaze_on_the_kinem-atics_of_the_squat_exerciselinks0c960523c48a69975c000000+ampcd=2amphl=trampct=clnk
Escamilla R F (2000) Knee biomechanics of the dynamic squatexercise Medicine amp Science in Sports amp Exercise 33 127ndash141
Escamilla R F Fleisig G S Lowry T M Barrentine S Wamp Andrews J R (2001) A three-dimensional biomechanicalanalysis of the squat during varying stance widths Medicine and
EMG Kinematic activities of back and front squat 1065
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015
Science in Sports and Exercise 33 984ndash998 Retrieved fromhttpwwwsweatpitcomforumstudiesSquattingA20three-dimensional20biomechanical20analysispdf
Escamilla R F Fleisig G S Zheng N Barrentine S WWilk K E amp Andrews J R (1998) Biomechanics of theknee during closed kinetic chain and open kinetic chain exer-cises Medicine and Science in Sports and Exercise 30 556ndash569doi10109700005768-199804000-00014
Escamilla R F Fleisig G S Zheng N Lander J EBarrentine S W Andrews J R Moorman C T(1997) The effects of technique variations on knee biomecha-nics during the squat and leg press Medicine and Science inSports and Exercise 29 156 doi10109700005768-200109000-00020
Escamilla R F Fleisig G S Zheng N Lander J EBarrentine S W Andrews J R hellip Moorman III C T(2000) Effects of technique variations on knee biomechanicsduring the squat and leg press Medicine amp Science in Sports ampExercise 33 1552ndash1566
Flanagan S Salem G J Wang M Y Sanker S ampGreendale G A (2003) Squatting exercises in older adultsKinematic and kinetic comparisons Medicine and Science inSports and Exercise 35 635ndash643 doi10124901MSS00000583644797306
Fleck S J (1999) Periodized strength training A critical reviewJournal of Strength Conditioning amp Research 13 82ndash89 Retrievedfrom httpjournalslwwcomnsca-jscrabstract199902000periodized_strength_training__a_critical_review15aspx
Grahammer J (1986) Sports illustrated strength training NewYork NY Harper amp Row
Gullett J C Tillman M D Gutierrez G M amp Chow J W(2009) A biomechanical comparison of back and front squatsin healthy trained individuals Journal of Strength andConditioning Research 23 284ndash292
Hasegawa I (2004) Using the overhead squat for core develop-ment NSCA Performance Training Journal 6 19ndash21
Hatfield F C (1983) Power A scientific approach Chicago ILContemporary Books Inc
Hay J G Andrews J G Vaughan C L amp Ueya K (1983)Load speed and equipment effects in strength-training exer-cises In H Matsui amp K Kobayashi (Eds) Biomechanics (3rded) Champaign IL Human Kinetics
Hwang S Kim Y amp Kim Y (2009) Lower extremity jointkinetics and lumbar curvature during squat and stoop liftingBMC Musculoskeletal Disorders 10 15 doi1011861471-2474-10-15
Isear J A Erickson Jr J C amp Worrel T W (1997) EMGanalysis of lower extremity muscle recruitment patterns duringan unloaded squat Medicine amp Science in Sports amp Exercise 29532ndash539
Kellis E Arambatzi F amp Papadopoulos C (2005) Effects ofload on ground reaction force and lower limb kinematics dur-ing concentric squats Journal of Sports Sciences 23 1045ndash1055
Konrad P (2005) ABC of EMG a practical introduction to kinesio-logical electromyography (1st ed) Scottsdale AZ Noraxon Inc
Kraemer W J amp Fry A C (1995) Strength testingDevelopment and evaluation of methodology In P Maud ampC Foster (Eds) Physiological assessment of human fitness(pp 115ndash138) Champaign IL Human Kinetics
Kraemer W J amp Ratamess N A (2004) Fundamentals ofresistance training Progression and exercise prescriptionMedicine amp Science in Sports amp Exercise 36 674ndash688
Matsumoto H Suda Y Otani T Niki Y Seedhom B B ampFujikawa K (2001) Roles of the anterior cruciate ligamentand the medial collateral ligament in preventing valgus instabil-ity Journal of Orthopaedic Science 6 28ndash32
McCaw S T amp Melrose D R (1999) Stance width and barload effects on leg muscle activity during the parallel squatMedicine and Science in Sports and Exercise 31 428ndash436
Merletti R (1999) Standards for reporting EMG data Journal ofElectromyography and Kinesiology 9 3ndash4 Retrieved from httpwwwisek onlineorgstandards_emghtml
Rippetoe M amp Kilgore L (2007) Starting strength Basic barbelltraining (2nd ed) Wichita Falls TX The Aasgaard Company
Russell P J amp Phillips S J (1989) A preliminary comparison offront and back squat exercises Research Quarterly for Exerciseand Sport 60 201ndash208
Schoenfeld B J (2010) Squatting kinematics and kinetics andtheir application to exercise performance Journal of Strengthand Conditioning Research 24 3497ndash3506
Scotten C M (2010) Differences in muscle activation in the lowerextremities while performing traditional squats and non-traditionalsquats (Master thesis) Boise State University Boise
Senter C amp Hame S L (2006) Biomechanical analysis of tibialtorque and knee flexion angle Implications for understandingknee injury Sports Medicine 36 635ndash641
Stensdotter A K Hodges P W Mellor R Sundelin G ampHager R C (2003) Quadriceps activation in closed and in openkinetic chain exercise Medicine and Science in Sports and Exercise35 2043ndash2047 doi10124901MSS000009910703704AE
Stuart M J Meglan D A Lutz G E Growney E S amp AnK N (1996) Comparison of intersegmental tibiofemoraljoint forces and muscle activity during various closed kineticchain exercises The American Journal of Sports Medicine 24792ndash799
Swinton P A Aspe R amp Keogh J (2012 July)Electromyographic comparison of The back squat and overheadsquat 30th Annual Conference of Biomechanics İn SportsMelbourne
Wretneberg P Feng Y amp Arborelius U P (1996) High- andlow-bar squatting techniques during weight-training Medicineand Science in Sports and Exercise 28 218ndash224
Wretneberg P Feng Y Lindberg F amp Arborelius U P(1993) Joint moments of force and quadriceps muscle activityduring squatting exercise Scandinavian Journal of Medicine ampScience in Sports 3 244ndash250
1066 HU Yavuz et al
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015

variations in technique and muscular involvement(Gullett Tillman Gutierrez amp Chow 2009)
Several studies have described the patterns of thekinematics kinetics and muscle activities of the kneehip and ankle during the squat (Dionisio AlmeidaDuarte amp Hirata 2008 Escamilla Fleisig LowryBarrentine amp Andrews 2001 Escamilla et al 1998Flanagan Salem Wang Sanker amp Greendale 2003Hasegawa 2004 Isear Erickson amp Worrel 1997McCaw amp Melrose 1999 Stensdotter HodgesMellor Sundelin amp Hager 2003 Wretneberg FengampArborelius 1996)However only a few of themhavecompared front and back squat (Braidot BrusaLestussi amp Parera 2007 Diggin et al 2011 Gullettet al 2009) and even less have studied electromyogra-phy (EMG) and kinematics together in the same studyto see the interactions (Gullett et al 2009)
Braidot et al (2007) compared the kinematicsdynamics the power and the energy in the differentjoints during the complete cycle from the exercise inthe different variants of squat A better developmentof energy with the front bar is observed in the kneeallowing a better muscular exercise with the sameload In the study of Diggin et al (2011) back squatexhibited a significantly greater trunk lean than thefront squat (P lt 005) with no differences in theknee joint kinematics However these studies didnot quantify the electromyographic data and muscleactivity during the front and back squatFurthermore the load to evaluate the exercise iscalculated on the basis of 50 of one repetitionmaximum (1RM) for both variants
Gullett et al (2009) reported that the front squatwas as effective as the back squat in terms of overall
muscle recruitment with 70 of 1RM load for eachsquat technique Heavy loading in experienced indi-viduals is needed to recruit the high-threshold motorunits that may not be activated during light-to-moderate lifting (Kraemer amp Ratamess 2004)Besides during lower loading conditions strongermuscles may compensate the activation of weakerones and cause personal varieties But during max-imal loading all related muscles must be fully acti-vated in order to complete the manoeuvre That willform a normalisation in terms of muscle activity andnaturally EMG signalling Clark Lambert andHunter (2012) emphasised that the sub-maximalload used in Gulletrsquos study might have failed to elicitthe possible difference between back and front squatFurthermore an increase in trunk forward lean wasshown with higher loads by Hay Andrews Vaughanand Ueya (1983) and Kellis Arambatzi andPapadopoulos (2005) during squat Thereforeobviously squat kinematics and EMG signalisationpattern can change with maximal loading
We aimed to compare the musculature activity andkinematics of knee and hip joints during front and backsquat with maximal loading and investigate the possi-ble differences in these two common squat variations
Methods
Participants
Twelve healthy male individuals who were experi-enced at performing front and back squats partici-pated in this study All participants were right-handed and had no history of orthopaedic injury
Figure 1 (a) Bar positioning during the back squat (b) Bar positioning during the front squat
EMG Kinematic activities of back and front squat 1059
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015
or surgery that would have limited their ability toperform the squatting techniques Before participa-tion informed consent was obtained from eachparticipant The investigation was conductedaccording to the Declaration of Helsinki andapproved by the Near East University ScientificResearches Evaluation and Ethic Commission(YDUuml201211ndash60)
Instrumentation
An eight-channel dual-mode portable EMG andphysiological signal data acquisition system(Myomonitor IV Delsys Inc Boston MA USA)was used for data collection Data collections wereconducted using EMG Works Acquisition 405(Delsys Inc) The amplifier bandwidth frequencyranged from 20 to 450 Hz with an input voltage of9 VDC at 07 A and the common-mode rejectionratio was 80 dB Data were recorded at a samplingrate of 1000 Hz over a wireless local area network tothe host computer for real-time display and storage
Seven channels of this system were used to assessthe EMG activity of vastus lateralis vastus medialisrectus femoris semitendinosus biceps femoris glu-teus maximus and ES Recording sites were pre-pared by shaving the area and wiping with alcoholpads to decrease electrical impedance Electrodes(41 times 20 times 5 mm DE-23 Delsys Inc) were placedalong the longitudinal axis of each muscle tested onthe right side (dominant side) of the participantrsquosbody according to the procedures from Gullettet al (2009) (Table I) The sensor contacts aremade from 999 pure silver bars measuring10 mm in length 1 mm in diameter and spaced10 mm apart from optimal signal detection and con-sistency A 508 cm diameter oval-shaped commonreference electrode (Dermatrode HE-R AmericanImex Irvine CA USA) was placed on the iliaccrest of the right leg
At the same time the EMG system was synchro-nised with a Samsung (VP-D375 W) video camera
with a shutter speed of 1250 s by using NationalInstruments USB-6501 Digital IO trigger box(Delsys Inc) Video recordings were made withAMCap (Microsoft V 309) video capture softwareFor kinematical data reflective markers (3 cm dia-meter) were attached and positioned over the follow-ing bony landmarks (a) lateral malleolus of the rightfoot (b) upper edges of the lateral tibial plateau ofthe right knee (c) posterior aspect of the greatertrochanters of the right femur and (d) end of theright side of the Olympic bar A calibration planethat consists of eight control points was used for two-dimensional spatial reconstruction
A standard 205-kg Olympic barbell discs(Werksan Ankara Turkey) and a continental squatrack were used during the squat
Procedures
The participants were required to attend two ses-sions A pretest was given to each participant 1week before the actual testing session The experi-mental protocol was reviewed and the participantswere given the opportunity to ask questions Duringthe pretest the participantrsquos RM was determinedand recorded for the back squat and front squatThe procedure used for assessing 1RM wasdescribed by Kraemer and Fry (1995) The partici-pants were asked to perform initial preparation on astationary bike for 3ndash5 min at the beginning of thepretest session and then performed a warm-up set of8ndash10 repetitions at a light weight (approximately50 of assumed 1RM) A second initial preparationconsisting of a set of three to five repetitions withmoderate weight (approximately 75 of 1RM) and athird initial preparation including one to three repe-titions with a heavy weight (approximately 90 of1RM) followed
After the initial preparation the participants per-formed 1RM strength exercises by enhancing the loadduring consecutive trials until the participants wereunable to properly perform a proper lift complete
Table I A description of the positioning of each electrode in relation to the muscle being tested developed by Broer and Houtz (1967) anddescribed by Gullett et al (2009)
Muscle Electrode placement
Rectus femoris Approximately midway between the anterior inferior iliac spine and the patella on the anterior side of the thighVastus lateralis Approximately two-thirds of the thigh length from the greater trochanter on the lateral side of the thighVastus medialis Approximately three-fourths of the thigh length from the anterior inferior iliac spine on the medial side of the thighErector spinae Three centimetres lateral to the L3 spinous processGluteus maximus 50 on the line between the sacral vertebrae and the greater trochanter This position corresponds with the greatest
prominence of the middle of the buttocks well above the visible bulge of the greater trochanterBiceps femoris Midway between the ischial tuberosity and the lateral condyle of the femur on the posterior side of the thighSemitendinosus Midway between the ischial tuberosity and the medial condyle of the femur on the posterior side of the thighReference electrode Iliac crest of the right leg
1060 HU Yavuz et al
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015
range of motion and correct technique Each partici-pant was asked to lower the bar to the point where theknee angle was 90deg (Figure 2) which was marked byadjustable stoppers Adequate rest was allowedbetween trials (3ndash5 min) Subsequently 1 week afterthe pretest session the participants performed a sec-ond session for data collection For each participantall data collection was performed in one day session
After the EMG electrode placement maximumvoluntary isometric contraction (MVIC) data fromthe quadriceps hamstrings erector spine and glu-teus maximus were collected according to the pro-cedures described by Konrad (2005) Three 3-sMVIC trials were collected in a randomised mannerfor each muscle group Adequate rest was allowedbetween trials (1 min)
All participants performed two to three warm-upsets in preparation for testing For both lifting varia-tions each participant used their 1RM weights pre-viously established for the back squat and frontsquat Exercise began with a given verbal commandThe starting and ending positions for the back squatand front squat were with the knees in full extensionwhich was defined as 180deg knee angle From thestarting position the participant flexed their kneesto minimum knee angle (approximately 90deg) andthen extended their knees back to the startingposition
During the back squat the barbell positionedacross the shoulder on the trapezius slightly abovethe posterior aspect of the deltoids and the hips andknees flexed until the thighs are parallel to the floor(Baechle and Earle 2000 Delavier 2001) Thenthe participant extended the hips and knees untilthe starting position is reached keeping the backflat the heels on the floor and the knees alignedover the feet (Baechle and Earle 2000 Delavier2001) During the front squat the barbell positionedacross the anterior deltoids and clavicles and theelbows fully flexed to position the upper arms paral-lel to the floor (Baechle and Earle 2000 Delavier
2001) The descending and ascending motions aremuch the same as in the back squat (Gullett et al2009) Adequate rest was allowed between trials (3ndash5 min)
Data reduction
The sampling of EMG and video recordings wereinitiated simultaneously with the beginning of thefirst squat repetition For synchronisation a LEDconnected to the trigger box (National InstrumentsUSB-6501 Digital IO) outputted a digital signalwhen the Myomonitor started data acquisitionWith the data acquisition the LED lit and it wentoff as the data stopped The data obtained from thisprocedure were used to specify the start of therequired portion and the length of the requestedportion
Kinematical data were analysed by using thesaSuite two-dimensional kinematical analysis pro-gramme which was developed by HacettepeUniversity Faculty of Sports SciencesBiomechanics Research Group Ankara TurkeyFor each trail the required portion of the videorecordings was trimmed the anthropometric pointswere digitised and the two-dimensional positionaldata were obtained The raw position data of thejoints were smoothed using a moving average filterand the angular kinematics of the knee and hip jointswere calculated All EMG data were partitioned intoascending and descending phases Movement timewas normalised into 10 movement phases to controlinter-individual differences Knee and hip anglechanges were examined throughout the descendingand ascending phases
EMG data were analysed according to the proce-dures from International Society ofElectrophysiology and Kinesiology (Merletti 1999)by using the EMG Works Analysis 40 (Delsys IncBoston) To calculate the mean normalised EMGvalues the raw EMG signals were subsetted filtered(Passband 3 Response Bandpass Corner F110 Hz Corner F2 500 Hz) rectified integrated(root mean square (Window Length 0100Window Overlap 008 Remove Ofset)) and nor-malised to the participants highest correspondingMVIC trial
Statistical analysis
Kinematic and electromyographic data were ana-lysed and compared between the front and backsquad by using paired sample t-tests (P lt 005)Throughout the text data for all participants per-forming each type of exercise were averaged andpresented as means standard deviations P-valueeffect size (Cohenrsquos d Cohen 1988) and 95
Figure 2 Illustrations of measured joint angles during back squatand front squat (adapted from Starting Strength Basic BarbellTraining by permission of The Aasgaard Company Rippetoe ampKilgore 2007)
EMG Kinematic activities of back and front squat 1061
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015
confidence intervals Cohenrsquos categories were usedto evaluate the magnitude of these sizes (small if0 le [d] le 05 medium if 05 le [d] le 08 and large if[d] gt 08) (Cohen 1988)
Results
The mean 1RM loads that were employed duringtesting were 10917 plusmn 2551 kg for the back squatand 8500 plusmn 1567 kg for the front squat This was13883 plusmn 3262 of their body weight for back squatand 10587 plusmn 2434 for front squat Participantscould lift significantly higher loads with back squatcomparing to the front squat (P lt 005 d = minus12895 CI 16283204)
Normalised EMG values as a percentage of max-imal voluntary isometric contraction ( MVIC)P-values effect size (Cohenrsquos d Cohen 1988) and95 confidence intervals between back and frontsquats are shown in Table II Vastus medialisEMG activity was found to be greater during thefront squat compared to back squat (P lt 005
d = 041 95 CI minus128minus43) There were noother differences in any other muscles
Normalised average EMG values as a MVIC P-values effect size (Cohenrsquos d Cohen 1988) and 95confidence intervals between descending and ascend-ing phases performed with 1RM loads between backand front squats are shown in Table III EMG activ-ities of gluteus maximus (P lt 005 d = 078 95 CIminus2581minus1120) biceps femoris (P lt 005 d = 09795 CI minus1974minus1260) and semitendinosus(P lt 005 d = 105 95 CI minus2072minus728) duringback squat and EMG activities of gluteus maximus(P lt 005 d = 062 95 CI minus2209minus1118) bicepsfemoris (P lt 005 d = 038 95 CI minus1486minus471)and semitendinosus (P lt 005 d = 048 95 CIminus840minus34) during front squat were found to be sig-nificantly higher EMG activity of the vastus medialis(P lt 005 d = 032 95CI minus1103minus53) during theascending phase was higher only
The mean EMG activities as a percentage of max-imal voluntary isometric contraction ( MVIC)P-values effect size (Cohenrsquos d Cohen 1988) and
Table II Mean EMG activities as a percentage of maximal voluntary isometric contraction ( MVIC) P-values effect size(Cohenrsquos d Cohen 1988) and 95 confidence intervals for the back squats and front squats throughout entire movementsperformed with 1RM loads
Muscle Back squat (mean plusmn s) Front squat (mean plusmns) P d
95 CI
L U
Rectus femoris 367 plusmn 124 461 plusmn 217 0118 053 minus217 282Vastus medialis 488 plusmn 139 554 plusmn 180 0038 041 minus128 minus043Vastus lateralis 470 plusmn 151 512 plusmn 173 0149 026 minus102 minus175Erector spinae 432 plusmn 156 462 plusmn 121 0495 022 minus125 049Gluteus maximus 371 plusmn 235 372 plusmn 270 0959 0 minus55 523Biceps femoris 262 plusmn 161 241 plusmn 254 0611 minus0 minus65 106Semitendinosus 215 plusmn 117 160 plusmn 87 0115 minus053 minus16 126
Note Significantly higher EMG activities during the front squat compared to the back squat (P lt 005)
Table III Back squats and front squats mean EMG activities as a percentage of maximal voluntary isometric contraction ( MVIC)P-values effect size (Cohenrsquos d Cohen 1988) and 95 confidence intervals between descending and ascending phases performed with1RM loads
Back squat Front squat
Descendingphase
(mean plusmns)
Ascendingphase
(mean plusmn s) P d
95 CI Descendingphase
(mean plusmn s)
Ascendingphase
(mean plusmn s) P d
95 CI
Muscle L U L U
Rectus femoris 379 plusmn 121 360 plusmn 138 0455 minus015 minus3562 minus7432 464 plusmn 244 467 plusmn 194 0922 001 minus7122 6500Vastus medialis 483 plusmn 143 493 plusmn 139 0617 007 minus5293 3286 531 plusmn 193 589 plusmn 171 033 032 minus11036 minus533Vastus lateralis 459 plusmn 139 485 plusmn 172 0223 017 minus7005 1821 480 plusmn 158 562 plusmn 222 068 043 minus17190 07269Erector spinae 411 plusmn 140 460 plusmn 176 0124 031 minus11286 1564 451 plusmn 120 481 plusmn 168 0451 020 minus11276 5367Gluteus maximus 288 plusmn 189 473 plusmn 277 0000 078 minus25810 minus11200 300 plusmn 230 466 plusmn 301 0000 062 minus22098 minus11188Biceps femoris 187 plusmn 149 349 plusmn 182 0000 097 minus19740 minus12600 197 plusmn 233 295 plusmn 287 0001 038 minus14864 minus4711Semitendinosus 150 plusmn 69 290 plusmn 162 0001 105 minus20720 minus7280 140 plusmn 81 184 plusmn 101 0036 048 minus8404 minus0343
Note Significantly higher EMG activities during the ascending phase compared to the descending phase (P lt 005)
1062 HU Yavuz et al
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015
95 confidence intervals between back squats andfront squats during the descending and ascendingphases performed with 1RM loads are shownin Table IV There were no significant differencesobserved between back and front squats duringthe descending phase During the ascending phasethe EMG activity of the vastus medialis was foundto be significantly higher in the front squat comparedto the back squat (P lt 005 d = 062 95 CIminus1500minus417) while the EMG activity of the semi-tendinosus was higher in the back squat compared tothe front squat (P lt 05 d = minus079 95 CI 622059)
As can be seen from Figure 3 significant differ-ences were observed between minimum hip anglesreached during back squats and front squats Theaverage minimum hip angle was significantly higher(P lt 005 d = 108 95 CI minus2857minus428) duringthe front squat compared to the back squat
Figure 4 shows the mean changes in knee and hipangles throughout the ascending phases of bothsquatting movements No difference was observed
in knee angles during the whole movement whilehip angles were lower in 8 of 10 phases during theback squat compared to front squat showing anobvious forward trunk lean According to theangle-specific EMG changes semitendinosus(P lt 005 d = minus023 95 CI minus2421111) showeda sudden increase in the sixth phase and bicepsfemoris (P lt 005 d = minus014 95 CI minus10931911) and gluteus maximus (P lt 005 d = minus03795 CI minus4533089) showed a similar but smallerincrease in the eighth phase during the back squatcompared to the front squat
Discussion
Participants could lift significantly greater loads withback squat compared to the front squat(1388 plusmn 326 of their body weight1059 plusmn 243 of their body weight respectively)(Figure 1) and this finding is consistent with theprevious studies (Gullett et al 2009 Russell ampPhillips 1989)
Instead of the load the level of effort in voluntarymuscle actions determines the degree of motor unitactivity (Carpinelli 2008) consequently the level ofEMG signalling increases Furthermore higherloads may increase intradiscal pressure (11) com-pression on vertebral bodies (10) tibiofemoral (1213) and patellofemoral joints (14) which could pos-sibly increase the risk of injury while performingsquat Gullett et al (2009) emphasised that the mus-cles tested were equally active during the front squatwhile lifting less mass and it seems that the extraload lifted during the back squat is what accounts forthe increased tibiofemoral compressive forces andextensor moments observed during these lifts It is
Table IV Mean EMG activities as a percentage of maximal voluntary isometric contraction ( MVIC) P-values effect size (Cohenrsquos dCohen 1988) and 95 confidence intervals between back squats and front squats during the descending and ascending phases performedwith 1RM loads
Descending phase Ascending phase
Back squat(mean plusmn s)
Front squat(mean plusmn s) P d
95 CIBack squat(mean plusmn s)
Front squat(mean plusmn s) P d
95 CI
Muscle L U L U
Rectus femoris 379 plusmn 121 464 plusmn 244 0200 044 minus22011 5164 360 plusmn 138 467 plusmn 194 0061 064 minus21917 0578Vastus medialis 483 plusmn 143 531 plusmn 193 0204 028 minus12627 3020 493 plusmn 139 589 plusmn 171 0002 062 minus15001 minus4177Vastus lateralis 459 plusmn 139 480 plusmn 158 0396 014 minus7088 3028 485 plusmn 172 562 plusmn 222 0096 039 minus16932 1590Erector spinae 411 plusmn 140 451 plusmn 120 0438 031 minus14953 6940 460 plusmn 176 481 plusmn 168 0665 012 minus12493 8292Gluteus maximus 288 plusmn 189 300 plusmn 230 0573 006 minus5460 3181 473 plusmn 277 466 plusmn 301 0841 minus002 minus7001 8447Biceps femoris 187 plusmn 149 197 plusmn 233 0765 005 minus7883 5959 349 plusmn 182 295 plusmn 287 0329 minus022 minus6257 17099Semitendinosus 150 plusmn 69 140 plusmn 81 0676 minus013 minus4052 6019 290 plusmn 162 184 plusmn 101 0039 minus079 0624 20595
Notes Significantly higher EMG activities during the front squat compared to the back squat (P lt 005) Significantly higher EMGactivities during the back squat compared to the front squat (P lt 005)
Figure 3 Minimum hip angles reached during the back squat (BS)and front squat (FS) Significant differences (P lt 005) betweenthe back and front squats
EMG Kinematic activities of back and front squat 1063
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015
very important because excessive tibiofemoral com-pressive forces could be deleterious to the menisciand articular cartilage (Escamilla 2000)
During the squat the primary muscles actingaround the knee are the quadriceps femoris (vastuslateralis vastus medialis vastus intermedius and rec-tus femoris) which carry out concentric knee exten-sion as well as eccentrically resisting knee flexionFor both back and front squats vastus medialis andvastus lateralis produced more activity than the rec-tus femoris during the whole manoeuvre which is inagreement with the data from Escamilla et al (19971998) Escamilla (2000) Escamilla et al (2000)Hwang Kim and Kim (2009) Wretneberg Feng
Lindberg and Arborelius (1993) Wretneberg et al(1996) and Isear et al (1997)
Schoenfeld (2010) reported that this may be logi-cal because the rectus femoris is both a hip flexorand knee extensor and thus shortens at one endwhile lengthening at the other during the squatwith little if any net change in length throughoutmovement
Although the loads were heavier during the backsquat mean EMG activities in selected musclesshowed no difference with only one exceptionDespite the lighter loads during the front squatvastus medialis mean EMG activity was greaterthan the back squat during the whole manoeuvresGullett et al (2009) and Stuart Meglan LutzGrowney and An (1996) reported no differences inmuscle activities between front and back squats Thedifference in our study can be resulted from thehigher loads compared to Gullett et al (2009)(70 of 1RM) and Stuart et al (1996) (50 pounds)which may recruit more motor units during themovements
When we divided the manoeuvres into ascendingand descending phases all muscles tested were moreactive during the ascending phase than during thedescending phase These findings are in accordancewith those of several other studies (Escamilla et al1998 Escamilla et al 2000 Gullett et al 2009McCaw amp Melrose 1999 Stuart et al 1996)EMG activities were higher during the ascendingphase compared to the descending phase for allmuscles during both the front and the back squatBut statistically significant differences were seen forgluteus maximus semitendinosus and bicepsfemoris during both the front and the back squatand for vastus medialis during the front squat
We observed no significant EMG activity differ-ences between the back and front squats during thedescending phases However during the ascendingphase EMG activity of the vastus medialis was higherin the front squat compared to the back squat whileEMG activity of the semitendinosus was higher inthe back squat compared to the front squat Thefront squat is believed to be a more isolated man-oeuvre for quadriceps (Grahammer 1986 Hatfield1983) and this result may support this idea Theheavier external resistance and more inclined torsoduring the back squat create a larger resistancemoment which requires greater muscular effort tocounterbalance (Swinton Aspe amp Keogh 2012) Itwas shown that increased forward trunk lean causesan increase in hamstring activity (Escamilla et al2000 Gullett et al 2009 Scotten 2010) Thismay explain the higher semitendinosus EMG activityduring the ascending phase of the back squats
When we divided the manoeuvres into 10 phasesfor being able to compare the movement patterns
Figure 4 Knee and hip angle-dependent EMG values of rectusfemoris (RF) vastus medialis (VM) vastus lateralis (VL) erectorspinae (ES) gluteus maximus (GM) biceps femoris (BF) andsemitendinosus (ST) throughout the phases of both backs squat(BS) and front squat (FS) movements Significant differences(P lt 005) between back and front squats
1064 HU Yavuz et al
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015
we did not observe any significant difference in kneeangles between the back and front squats Howeverwe observed significantly lower hip angles in 8 of 10phases during the back squat The lowest hip anglesreached during the manoeuvres were significantlylower in the back squat compared to the frontsquat These findings showed an increased forwardlean during the back squat compared to the frontsquat during maximum loading
When we check angle-specific EMG changes foreach muscle we saw that EMG activity patternswere quite parallel to each other for most of themuscles in both squat variants SemitendinosusEMG activity showed a sudden increase in thesixth phase which also shows the lowest hip angleand the starting of the ascending phase Gluteusmaximus and biceps femoris showed a similar butweaker change in pattern during the middle of theascending phase (eighth phase) This may probablybe due to the extra effort of the hip extensors tomaintain the balance by compensating the increasedforward lean during back squat
In both the squatting techniques as the perfor-mers lower throughout the eccentric phase they arerequired to lean forward in order to maintain bal-ance Centre of gravity moves further away from thelumbar spine increasing the moment arm and tor-que As a result the shear forces occurring withinthe lumbar spine would also increase (Comfort ampKasim 2007 Diggin et al 2011 Gullett et al2009) Increased forward lean reduces tolerance tocompressive load and results in a transfer of the loadfrom muscles to passive tissues heightening the riskof disc herniation (Matsumoto et al 2001)
As previously stated such an increase in shearforce under regular high loading conditions (eg1RM) may predispose an athlete to injury if theseforces continually exceed the strain capabilities ofthe joint connective tissues (Comfort amp Kasim2007) That is why it is beneficial to maintain aposture that is as close to upright as possible at alltimes for preventing the lumbar injuries (Schoenfeld2010)
Conclusion
We studied the musculature activity and kinematicsof knee and hip joints during front and back squatswith maximum loading (1RM) The front squat wasshown to be just as effective as the back squat undermaximum loading conditions in terms of overallmuscle activity with no difference in knee joint kine-matics and significantly less forward lean in hip jointwhich may probably show less lumbar injury riskWe also managed to show that the front squat cre-ated higher EMG activity in vastus medialis despitethe lighter loads compared to back squat that agrees
with the idea of ldquobeing a more isolated movementfor knee extensorsrdquo It is a known fact that the backsquat is used much more commonly compared to itsfront variation Results may suggest that the frontsquat may be a better choice for focusing on kneeextensor improvement andor for preventing lumbarinjuries under maximum loading conditions
References
American College of Sports Medicine (1998) Position standThe recommended quantity and quality of exercise for devel-oping and maintaining cardiorespiratory and muscular fitnessand flexibility in healthy adults Medicine and Science in Sportsand Exercise 975ndash991 doi101249MSS0b013e318213fefb
Baechle T R amp Earle R (2000) Essentials of strength trainingand conditioning (2nd ed) Champaign IL Human Kinetics
Balshaw T G amp Hunter A M (2012) Evaluation of electro-myography normalisation methods for the back squat Journalof Electromyography and Kinesiology 22 308ndash319
Braidot A A Brusa M H Lestussi F E amp Parera G P(2007) Biomechanics of front and back squat exercises Journalof Physics Conference Series 90 012009
Broer M R amp Houtz S J (1967) Patterns of muscular activity inselected sport skills (3rd ed) Springfield Charles C ThomasPublishing
Carpinelli R N (2008) The size principle and a critical analysisof the unsubstantiated heavier-is-better recommendation forresistance training Journal of Exercise Science and Fitness 667ndash86
Channell B T amp Barfield J P (2008) Effect of Olympic andtraditional resistance training on vertical jump improvement inhigh school boys Journal of Strength Conditioning and Research22 1522ndash1527
Clark D R Lambert M I amp Hunter A M (2012) Muscleactivation in the loaded free barbell squat A brief reviewJournal of Strength Conditioning and Research 26 1169ndash1178
Cohen J (1988) Statistical power analysis for the behavioral sciencesHillsdale NJ Lawrence Erlbaum
Comfort P amp Kasim P (2007) Optimizing squat techniqueStrength and Conditioning Journal 29 10ndash13
Delavier F (2001) Strength training anatomy Champaign ILHuman Kinetics
Diggin D OrsquoRegan C Whelan N Daly S McLoughlin VMcNamara L amp Reilly A (2011) A biomechanical ana-lysis of front vs back squat Injury implications PortugueseJournal of Sports Sciences 11(Suppl 2) Retrieved from httpwwwresearchgatenetpublication258363730_A_biomechanical_Analysis_of_front_and_back_squat_injury_implicationsfilee0b49528105693baa7pdf
Dionisio V C Almeida G L Duarte M amp Hirata R P(2008) Kinematic kinetic and EMG patterns during down-ward squatting Journal of Electromyography and Kinesiology 18134ndash143
Donnelly D V Berg W P amp Fiske D M (2006) The effectof the direction of gaze on the kinematics of the squat exerciseJournal of Strength Conditioning and Research 20 145ndash150Retrieved from httpwwwresearchgatenetpublication7273329_The_effect_of_the_direction_of_gaze_on_the_kinem-atics_of_the_squat_exerciselinks0c960523c48a69975c000000+ampcd=2amphl=trampct=clnk
Escamilla R F (2000) Knee biomechanics of the dynamic squatexercise Medicine amp Science in Sports amp Exercise 33 127ndash141
Escamilla R F Fleisig G S Lowry T M Barrentine S Wamp Andrews J R (2001) A three-dimensional biomechanicalanalysis of the squat during varying stance widths Medicine and
EMG Kinematic activities of back and front squat 1065
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015
Science in Sports and Exercise 33 984ndash998 Retrieved fromhttpwwwsweatpitcomforumstudiesSquattingA20three-dimensional20biomechanical20analysispdf
Escamilla R F Fleisig G S Zheng N Barrentine S WWilk K E amp Andrews J R (1998) Biomechanics of theknee during closed kinetic chain and open kinetic chain exer-cises Medicine and Science in Sports and Exercise 30 556ndash569doi10109700005768-199804000-00014
Escamilla R F Fleisig G S Zheng N Lander J EBarrentine S W Andrews J R Moorman C T(1997) The effects of technique variations on knee biomecha-nics during the squat and leg press Medicine and Science inSports and Exercise 29 156 doi10109700005768-200109000-00020
Escamilla R F Fleisig G S Zheng N Lander J EBarrentine S W Andrews J R hellip Moorman III C T(2000) Effects of technique variations on knee biomechanicsduring the squat and leg press Medicine amp Science in Sports ampExercise 33 1552ndash1566
Flanagan S Salem G J Wang M Y Sanker S ampGreendale G A (2003) Squatting exercises in older adultsKinematic and kinetic comparisons Medicine and Science inSports and Exercise 35 635ndash643 doi10124901MSS00000583644797306
Fleck S J (1999) Periodized strength training A critical reviewJournal of Strength Conditioning amp Research 13 82ndash89 Retrievedfrom httpjournalslwwcomnsca-jscrabstract199902000periodized_strength_training__a_critical_review15aspx
Grahammer J (1986) Sports illustrated strength training NewYork NY Harper amp Row
Gullett J C Tillman M D Gutierrez G M amp Chow J W(2009) A biomechanical comparison of back and front squatsin healthy trained individuals Journal of Strength andConditioning Research 23 284ndash292
Hasegawa I (2004) Using the overhead squat for core develop-ment NSCA Performance Training Journal 6 19ndash21
Hatfield F C (1983) Power A scientific approach Chicago ILContemporary Books Inc
Hay J G Andrews J G Vaughan C L amp Ueya K (1983)Load speed and equipment effects in strength-training exer-cises In H Matsui amp K Kobayashi (Eds) Biomechanics (3rded) Champaign IL Human Kinetics
Hwang S Kim Y amp Kim Y (2009) Lower extremity jointkinetics and lumbar curvature during squat and stoop liftingBMC Musculoskeletal Disorders 10 15 doi1011861471-2474-10-15
Isear J A Erickson Jr J C amp Worrel T W (1997) EMGanalysis of lower extremity muscle recruitment patterns duringan unloaded squat Medicine amp Science in Sports amp Exercise 29532ndash539
Kellis E Arambatzi F amp Papadopoulos C (2005) Effects ofload on ground reaction force and lower limb kinematics dur-ing concentric squats Journal of Sports Sciences 23 1045ndash1055
Konrad P (2005) ABC of EMG a practical introduction to kinesio-logical electromyography (1st ed) Scottsdale AZ Noraxon Inc
Kraemer W J amp Fry A C (1995) Strength testingDevelopment and evaluation of methodology In P Maud ampC Foster (Eds) Physiological assessment of human fitness(pp 115ndash138) Champaign IL Human Kinetics
Kraemer W J amp Ratamess N A (2004) Fundamentals ofresistance training Progression and exercise prescriptionMedicine amp Science in Sports amp Exercise 36 674ndash688
Matsumoto H Suda Y Otani T Niki Y Seedhom B B ampFujikawa K (2001) Roles of the anterior cruciate ligamentand the medial collateral ligament in preventing valgus instabil-ity Journal of Orthopaedic Science 6 28ndash32
McCaw S T amp Melrose D R (1999) Stance width and barload effects on leg muscle activity during the parallel squatMedicine and Science in Sports and Exercise 31 428ndash436
Merletti R (1999) Standards for reporting EMG data Journal ofElectromyography and Kinesiology 9 3ndash4 Retrieved from httpwwwisek onlineorgstandards_emghtml
Rippetoe M amp Kilgore L (2007) Starting strength Basic barbelltraining (2nd ed) Wichita Falls TX The Aasgaard Company
Russell P J amp Phillips S J (1989) A preliminary comparison offront and back squat exercises Research Quarterly for Exerciseand Sport 60 201ndash208
Schoenfeld B J (2010) Squatting kinematics and kinetics andtheir application to exercise performance Journal of Strengthand Conditioning Research 24 3497ndash3506
Scotten C M (2010) Differences in muscle activation in the lowerextremities while performing traditional squats and non-traditionalsquats (Master thesis) Boise State University Boise
Senter C amp Hame S L (2006) Biomechanical analysis of tibialtorque and knee flexion angle Implications for understandingknee injury Sports Medicine 36 635ndash641
Stensdotter A K Hodges P W Mellor R Sundelin G ampHager R C (2003) Quadriceps activation in closed and in openkinetic chain exercise Medicine and Science in Sports and Exercise35 2043ndash2047 doi10124901MSS000009910703704AE
Stuart M J Meglan D A Lutz G E Growney E S amp AnK N (1996) Comparison of intersegmental tibiofemoraljoint forces and muscle activity during various closed kineticchain exercises The American Journal of Sports Medicine 24792ndash799
Swinton P A Aspe R amp Keogh J (2012 July)Electromyographic comparison of The back squat and overheadsquat 30th Annual Conference of Biomechanics İn SportsMelbourne
Wretneberg P Feng Y amp Arborelius U P (1996) High- andlow-bar squatting techniques during weight-training Medicineand Science in Sports and Exercise 28 218ndash224
Wretneberg P Feng Y Lindberg F amp Arborelius U P(1993) Joint moments of force and quadriceps muscle activityduring squatting exercise Scandinavian Journal of Medicine ampScience in Sports 3 244ndash250
1066 HU Yavuz et al
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015

or surgery that would have limited their ability toperform the squatting techniques Before participa-tion informed consent was obtained from eachparticipant The investigation was conductedaccording to the Declaration of Helsinki andapproved by the Near East University ScientificResearches Evaluation and Ethic Commission(YDUuml201211ndash60)
Instrumentation
An eight-channel dual-mode portable EMG andphysiological signal data acquisition system(Myomonitor IV Delsys Inc Boston MA USA)was used for data collection Data collections wereconducted using EMG Works Acquisition 405(Delsys Inc) The amplifier bandwidth frequencyranged from 20 to 450 Hz with an input voltage of9 VDC at 07 A and the common-mode rejectionratio was 80 dB Data were recorded at a samplingrate of 1000 Hz over a wireless local area network tothe host computer for real-time display and storage
Seven channels of this system were used to assessthe EMG activity of vastus lateralis vastus medialisrectus femoris semitendinosus biceps femoris glu-teus maximus and ES Recording sites were pre-pared by shaving the area and wiping with alcoholpads to decrease electrical impedance Electrodes(41 times 20 times 5 mm DE-23 Delsys Inc) were placedalong the longitudinal axis of each muscle tested onthe right side (dominant side) of the participantrsquosbody according to the procedures from Gullettet al (2009) (Table I) The sensor contacts aremade from 999 pure silver bars measuring10 mm in length 1 mm in diameter and spaced10 mm apart from optimal signal detection and con-sistency A 508 cm diameter oval-shaped commonreference electrode (Dermatrode HE-R AmericanImex Irvine CA USA) was placed on the iliaccrest of the right leg
At the same time the EMG system was synchro-nised with a Samsung (VP-D375 W) video camera
with a shutter speed of 1250 s by using NationalInstruments USB-6501 Digital IO trigger box(Delsys Inc) Video recordings were made withAMCap (Microsoft V 309) video capture softwareFor kinematical data reflective markers (3 cm dia-meter) were attached and positioned over the follow-ing bony landmarks (a) lateral malleolus of the rightfoot (b) upper edges of the lateral tibial plateau ofthe right knee (c) posterior aspect of the greatertrochanters of the right femur and (d) end of theright side of the Olympic bar A calibration planethat consists of eight control points was used for two-dimensional spatial reconstruction
A standard 205-kg Olympic barbell discs(Werksan Ankara Turkey) and a continental squatrack were used during the squat
Procedures
The participants were required to attend two ses-sions A pretest was given to each participant 1week before the actual testing session The experi-mental protocol was reviewed and the participantswere given the opportunity to ask questions Duringthe pretest the participantrsquos RM was determinedand recorded for the back squat and front squatThe procedure used for assessing 1RM wasdescribed by Kraemer and Fry (1995) The partici-pants were asked to perform initial preparation on astationary bike for 3ndash5 min at the beginning of thepretest session and then performed a warm-up set of8ndash10 repetitions at a light weight (approximately50 of assumed 1RM) A second initial preparationconsisting of a set of three to five repetitions withmoderate weight (approximately 75 of 1RM) and athird initial preparation including one to three repe-titions with a heavy weight (approximately 90 of1RM) followed
After the initial preparation the participants per-formed 1RM strength exercises by enhancing the loadduring consecutive trials until the participants wereunable to properly perform a proper lift complete
Table I A description of the positioning of each electrode in relation to the muscle being tested developed by Broer and Houtz (1967) anddescribed by Gullett et al (2009)
Muscle Electrode placement
Rectus femoris Approximately midway between the anterior inferior iliac spine and the patella on the anterior side of the thighVastus lateralis Approximately two-thirds of the thigh length from the greater trochanter on the lateral side of the thighVastus medialis Approximately three-fourths of the thigh length from the anterior inferior iliac spine on the medial side of the thighErector spinae Three centimetres lateral to the L3 spinous processGluteus maximus 50 on the line between the sacral vertebrae and the greater trochanter This position corresponds with the greatest
prominence of the middle of the buttocks well above the visible bulge of the greater trochanterBiceps femoris Midway between the ischial tuberosity and the lateral condyle of the femur on the posterior side of the thighSemitendinosus Midway between the ischial tuberosity and the medial condyle of the femur on the posterior side of the thighReference electrode Iliac crest of the right leg
1060 HU Yavuz et al
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015
range of motion and correct technique Each partici-pant was asked to lower the bar to the point where theknee angle was 90deg (Figure 2) which was marked byadjustable stoppers Adequate rest was allowedbetween trials (3ndash5 min) Subsequently 1 week afterthe pretest session the participants performed a sec-ond session for data collection For each participantall data collection was performed in one day session
After the EMG electrode placement maximumvoluntary isometric contraction (MVIC) data fromthe quadriceps hamstrings erector spine and glu-teus maximus were collected according to the pro-cedures described by Konrad (2005) Three 3-sMVIC trials were collected in a randomised mannerfor each muscle group Adequate rest was allowedbetween trials (1 min)
All participants performed two to three warm-upsets in preparation for testing For both lifting varia-tions each participant used their 1RM weights pre-viously established for the back squat and frontsquat Exercise began with a given verbal commandThe starting and ending positions for the back squatand front squat were with the knees in full extensionwhich was defined as 180deg knee angle From thestarting position the participant flexed their kneesto minimum knee angle (approximately 90deg) andthen extended their knees back to the startingposition
During the back squat the barbell positionedacross the shoulder on the trapezius slightly abovethe posterior aspect of the deltoids and the hips andknees flexed until the thighs are parallel to the floor(Baechle and Earle 2000 Delavier 2001) Thenthe participant extended the hips and knees untilthe starting position is reached keeping the backflat the heels on the floor and the knees alignedover the feet (Baechle and Earle 2000 Delavier2001) During the front squat the barbell positionedacross the anterior deltoids and clavicles and theelbows fully flexed to position the upper arms paral-lel to the floor (Baechle and Earle 2000 Delavier
2001) The descending and ascending motions aremuch the same as in the back squat (Gullett et al2009) Adequate rest was allowed between trials (3ndash5 min)
Data reduction
The sampling of EMG and video recordings wereinitiated simultaneously with the beginning of thefirst squat repetition For synchronisation a LEDconnected to the trigger box (National InstrumentsUSB-6501 Digital IO) outputted a digital signalwhen the Myomonitor started data acquisitionWith the data acquisition the LED lit and it wentoff as the data stopped The data obtained from thisprocedure were used to specify the start of therequired portion and the length of the requestedportion
Kinematical data were analysed by using thesaSuite two-dimensional kinematical analysis pro-gramme which was developed by HacettepeUniversity Faculty of Sports SciencesBiomechanics Research Group Ankara TurkeyFor each trail the required portion of the videorecordings was trimmed the anthropometric pointswere digitised and the two-dimensional positionaldata were obtained The raw position data of thejoints were smoothed using a moving average filterand the angular kinematics of the knee and hip jointswere calculated All EMG data were partitioned intoascending and descending phases Movement timewas normalised into 10 movement phases to controlinter-individual differences Knee and hip anglechanges were examined throughout the descendingand ascending phases
EMG data were analysed according to the proce-dures from International Society ofElectrophysiology and Kinesiology (Merletti 1999)by using the EMG Works Analysis 40 (Delsys IncBoston) To calculate the mean normalised EMGvalues the raw EMG signals were subsetted filtered(Passband 3 Response Bandpass Corner F110 Hz Corner F2 500 Hz) rectified integrated(root mean square (Window Length 0100Window Overlap 008 Remove Ofset)) and nor-malised to the participants highest correspondingMVIC trial
Statistical analysis
Kinematic and electromyographic data were ana-lysed and compared between the front and backsquad by using paired sample t-tests (P lt 005)Throughout the text data for all participants per-forming each type of exercise were averaged andpresented as means standard deviations P-valueeffect size (Cohenrsquos d Cohen 1988) and 95
Figure 2 Illustrations of measured joint angles during back squatand front squat (adapted from Starting Strength Basic BarbellTraining by permission of The Aasgaard Company Rippetoe ampKilgore 2007)
EMG Kinematic activities of back and front squat 1061
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015
confidence intervals Cohenrsquos categories were usedto evaluate the magnitude of these sizes (small if0 le [d] le 05 medium if 05 le [d] le 08 and large if[d] gt 08) (Cohen 1988)
Results
The mean 1RM loads that were employed duringtesting were 10917 plusmn 2551 kg for the back squatand 8500 plusmn 1567 kg for the front squat This was13883 plusmn 3262 of their body weight for back squatand 10587 plusmn 2434 for front squat Participantscould lift significantly higher loads with back squatcomparing to the front squat (P lt 005 d = minus12895 CI 16283204)
Normalised EMG values as a percentage of max-imal voluntary isometric contraction ( MVIC)P-values effect size (Cohenrsquos d Cohen 1988) and95 confidence intervals between back and frontsquats are shown in Table II Vastus medialisEMG activity was found to be greater during thefront squat compared to back squat (P lt 005
d = 041 95 CI minus128minus43) There were noother differences in any other muscles
Normalised average EMG values as a MVIC P-values effect size (Cohenrsquos d Cohen 1988) and 95confidence intervals between descending and ascend-ing phases performed with 1RM loads between backand front squats are shown in Table III EMG activ-ities of gluteus maximus (P lt 005 d = 078 95 CIminus2581minus1120) biceps femoris (P lt 005 d = 09795 CI minus1974minus1260) and semitendinosus(P lt 005 d = 105 95 CI minus2072minus728) duringback squat and EMG activities of gluteus maximus(P lt 005 d = 062 95 CI minus2209minus1118) bicepsfemoris (P lt 005 d = 038 95 CI minus1486minus471)and semitendinosus (P lt 005 d = 048 95 CIminus840minus34) during front squat were found to be sig-nificantly higher EMG activity of the vastus medialis(P lt 005 d = 032 95CI minus1103minus53) during theascending phase was higher only
The mean EMG activities as a percentage of max-imal voluntary isometric contraction ( MVIC)P-values effect size (Cohenrsquos d Cohen 1988) and
Table II Mean EMG activities as a percentage of maximal voluntary isometric contraction ( MVIC) P-values effect size(Cohenrsquos d Cohen 1988) and 95 confidence intervals for the back squats and front squats throughout entire movementsperformed with 1RM loads
Muscle Back squat (mean plusmn s) Front squat (mean plusmns) P d
95 CI
L U
Rectus femoris 367 plusmn 124 461 plusmn 217 0118 053 minus217 282Vastus medialis 488 plusmn 139 554 plusmn 180 0038 041 minus128 minus043Vastus lateralis 470 plusmn 151 512 plusmn 173 0149 026 minus102 minus175Erector spinae 432 plusmn 156 462 plusmn 121 0495 022 minus125 049Gluteus maximus 371 plusmn 235 372 plusmn 270 0959 0 minus55 523Biceps femoris 262 plusmn 161 241 plusmn 254 0611 minus0 minus65 106Semitendinosus 215 plusmn 117 160 plusmn 87 0115 minus053 minus16 126
Note Significantly higher EMG activities during the front squat compared to the back squat (P lt 005)
Table III Back squats and front squats mean EMG activities as a percentage of maximal voluntary isometric contraction ( MVIC)P-values effect size (Cohenrsquos d Cohen 1988) and 95 confidence intervals between descending and ascending phases performed with1RM loads
Back squat Front squat
Descendingphase
(mean plusmns)
Ascendingphase
(mean plusmn s) P d
95 CI Descendingphase
(mean plusmn s)
Ascendingphase
(mean plusmn s) P d
95 CI
Muscle L U L U
Rectus femoris 379 plusmn 121 360 plusmn 138 0455 minus015 minus3562 minus7432 464 plusmn 244 467 plusmn 194 0922 001 minus7122 6500Vastus medialis 483 plusmn 143 493 plusmn 139 0617 007 minus5293 3286 531 plusmn 193 589 plusmn 171 033 032 minus11036 minus533Vastus lateralis 459 plusmn 139 485 plusmn 172 0223 017 minus7005 1821 480 plusmn 158 562 plusmn 222 068 043 minus17190 07269Erector spinae 411 plusmn 140 460 plusmn 176 0124 031 minus11286 1564 451 plusmn 120 481 plusmn 168 0451 020 minus11276 5367Gluteus maximus 288 plusmn 189 473 plusmn 277 0000 078 minus25810 minus11200 300 plusmn 230 466 plusmn 301 0000 062 minus22098 minus11188Biceps femoris 187 plusmn 149 349 plusmn 182 0000 097 minus19740 minus12600 197 plusmn 233 295 plusmn 287 0001 038 minus14864 minus4711Semitendinosus 150 plusmn 69 290 plusmn 162 0001 105 minus20720 minus7280 140 plusmn 81 184 plusmn 101 0036 048 minus8404 minus0343
Note Significantly higher EMG activities during the ascending phase compared to the descending phase (P lt 005)
1062 HU Yavuz et al
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015
95 confidence intervals between back squats andfront squats during the descending and ascendingphases performed with 1RM loads are shownin Table IV There were no significant differencesobserved between back and front squats duringthe descending phase During the ascending phasethe EMG activity of the vastus medialis was foundto be significantly higher in the front squat comparedto the back squat (P lt 005 d = 062 95 CIminus1500minus417) while the EMG activity of the semi-tendinosus was higher in the back squat compared tothe front squat (P lt 05 d = minus079 95 CI 622059)
As can be seen from Figure 3 significant differ-ences were observed between minimum hip anglesreached during back squats and front squats Theaverage minimum hip angle was significantly higher(P lt 005 d = 108 95 CI minus2857minus428) duringthe front squat compared to the back squat
Figure 4 shows the mean changes in knee and hipangles throughout the ascending phases of bothsquatting movements No difference was observed
in knee angles during the whole movement whilehip angles were lower in 8 of 10 phases during theback squat compared to front squat showing anobvious forward trunk lean According to theangle-specific EMG changes semitendinosus(P lt 005 d = minus023 95 CI minus2421111) showeda sudden increase in the sixth phase and bicepsfemoris (P lt 005 d = minus014 95 CI minus10931911) and gluteus maximus (P lt 005 d = minus03795 CI minus4533089) showed a similar but smallerincrease in the eighth phase during the back squatcompared to the front squat
Discussion
Participants could lift significantly greater loads withback squat compared to the front squat(1388 plusmn 326 of their body weight1059 plusmn 243 of their body weight respectively)(Figure 1) and this finding is consistent with theprevious studies (Gullett et al 2009 Russell ampPhillips 1989)
Instead of the load the level of effort in voluntarymuscle actions determines the degree of motor unitactivity (Carpinelli 2008) consequently the level ofEMG signalling increases Furthermore higherloads may increase intradiscal pressure (11) com-pression on vertebral bodies (10) tibiofemoral (1213) and patellofemoral joints (14) which could pos-sibly increase the risk of injury while performingsquat Gullett et al (2009) emphasised that the mus-cles tested were equally active during the front squatwhile lifting less mass and it seems that the extraload lifted during the back squat is what accounts forthe increased tibiofemoral compressive forces andextensor moments observed during these lifts It is
Table IV Mean EMG activities as a percentage of maximal voluntary isometric contraction ( MVIC) P-values effect size (Cohenrsquos dCohen 1988) and 95 confidence intervals between back squats and front squats during the descending and ascending phases performedwith 1RM loads
Descending phase Ascending phase
Back squat(mean plusmn s)
Front squat(mean plusmn s) P d
95 CIBack squat(mean plusmn s)
Front squat(mean plusmn s) P d
95 CI
Muscle L U L U
Rectus femoris 379 plusmn 121 464 plusmn 244 0200 044 minus22011 5164 360 plusmn 138 467 plusmn 194 0061 064 minus21917 0578Vastus medialis 483 plusmn 143 531 plusmn 193 0204 028 minus12627 3020 493 plusmn 139 589 plusmn 171 0002 062 minus15001 minus4177Vastus lateralis 459 plusmn 139 480 plusmn 158 0396 014 minus7088 3028 485 plusmn 172 562 plusmn 222 0096 039 minus16932 1590Erector spinae 411 plusmn 140 451 plusmn 120 0438 031 minus14953 6940 460 plusmn 176 481 plusmn 168 0665 012 minus12493 8292Gluteus maximus 288 plusmn 189 300 plusmn 230 0573 006 minus5460 3181 473 plusmn 277 466 plusmn 301 0841 minus002 minus7001 8447Biceps femoris 187 plusmn 149 197 plusmn 233 0765 005 minus7883 5959 349 plusmn 182 295 plusmn 287 0329 minus022 minus6257 17099Semitendinosus 150 plusmn 69 140 plusmn 81 0676 minus013 minus4052 6019 290 plusmn 162 184 plusmn 101 0039 minus079 0624 20595
Notes Significantly higher EMG activities during the front squat compared to the back squat (P lt 005) Significantly higher EMGactivities during the back squat compared to the front squat (P lt 005)
Figure 3 Minimum hip angles reached during the back squat (BS)and front squat (FS) Significant differences (P lt 005) betweenthe back and front squats
EMG Kinematic activities of back and front squat 1063
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015
very important because excessive tibiofemoral com-pressive forces could be deleterious to the menisciand articular cartilage (Escamilla 2000)
During the squat the primary muscles actingaround the knee are the quadriceps femoris (vastuslateralis vastus medialis vastus intermedius and rec-tus femoris) which carry out concentric knee exten-sion as well as eccentrically resisting knee flexionFor both back and front squats vastus medialis andvastus lateralis produced more activity than the rec-tus femoris during the whole manoeuvre which is inagreement with the data from Escamilla et al (19971998) Escamilla (2000) Escamilla et al (2000)Hwang Kim and Kim (2009) Wretneberg Feng
Lindberg and Arborelius (1993) Wretneberg et al(1996) and Isear et al (1997)
Schoenfeld (2010) reported that this may be logi-cal because the rectus femoris is both a hip flexorand knee extensor and thus shortens at one endwhile lengthening at the other during the squatwith little if any net change in length throughoutmovement
Although the loads were heavier during the backsquat mean EMG activities in selected musclesshowed no difference with only one exceptionDespite the lighter loads during the front squatvastus medialis mean EMG activity was greaterthan the back squat during the whole manoeuvresGullett et al (2009) and Stuart Meglan LutzGrowney and An (1996) reported no differences inmuscle activities between front and back squats Thedifference in our study can be resulted from thehigher loads compared to Gullett et al (2009)(70 of 1RM) and Stuart et al (1996) (50 pounds)which may recruit more motor units during themovements
When we divided the manoeuvres into ascendingand descending phases all muscles tested were moreactive during the ascending phase than during thedescending phase These findings are in accordancewith those of several other studies (Escamilla et al1998 Escamilla et al 2000 Gullett et al 2009McCaw amp Melrose 1999 Stuart et al 1996)EMG activities were higher during the ascendingphase compared to the descending phase for allmuscles during both the front and the back squatBut statistically significant differences were seen forgluteus maximus semitendinosus and bicepsfemoris during both the front and the back squatand for vastus medialis during the front squat
We observed no significant EMG activity differ-ences between the back and front squats during thedescending phases However during the ascendingphase EMG activity of the vastus medialis was higherin the front squat compared to the back squat whileEMG activity of the semitendinosus was higher inthe back squat compared to the front squat Thefront squat is believed to be a more isolated man-oeuvre for quadriceps (Grahammer 1986 Hatfield1983) and this result may support this idea Theheavier external resistance and more inclined torsoduring the back squat create a larger resistancemoment which requires greater muscular effort tocounterbalance (Swinton Aspe amp Keogh 2012) Itwas shown that increased forward trunk lean causesan increase in hamstring activity (Escamilla et al2000 Gullett et al 2009 Scotten 2010) Thismay explain the higher semitendinosus EMG activityduring the ascending phase of the back squats
When we divided the manoeuvres into 10 phasesfor being able to compare the movement patterns
Figure 4 Knee and hip angle-dependent EMG values of rectusfemoris (RF) vastus medialis (VM) vastus lateralis (VL) erectorspinae (ES) gluteus maximus (GM) biceps femoris (BF) andsemitendinosus (ST) throughout the phases of both backs squat(BS) and front squat (FS) movements Significant differences(P lt 005) between back and front squats
1064 HU Yavuz et al
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015
we did not observe any significant difference in kneeangles between the back and front squats Howeverwe observed significantly lower hip angles in 8 of 10phases during the back squat The lowest hip anglesreached during the manoeuvres were significantlylower in the back squat compared to the frontsquat These findings showed an increased forwardlean during the back squat compared to the frontsquat during maximum loading
When we check angle-specific EMG changes foreach muscle we saw that EMG activity patternswere quite parallel to each other for most of themuscles in both squat variants SemitendinosusEMG activity showed a sudden increase in thesixth phase which also shows the lowest hip angleand the starting of the ascending phase Gluteusmaximus and biceps femoris showed a similar butweaker change in pattern during the middle of theascending phase (eighth phase) This may probablybe due to the extra effort of the hip extensors tomaintain the balance by compensating the increasedforward lean during back squat
In both the squatting techniques as the perfor-mers lower throughout the eccentric phase they arerequired to lean forward in order to maintain bal-ance Centre of gravity moves further away from thelumbar spine increasing the moment arm and tor-que As a result the shear forces occurring withinthe lumbar spine would also increase (Comfort ampKasim 2007 Diggin et al 2011 Gullett et al2009) Increased forward lean reduces tolerance tocompressive load and results in a transfer of the loadfrom muscles to passive tissues heightening the riskof disc herniation (Matsumoto et al 2001)
As previously stated such an increase in shearforce under regular high loading conditions (eg1RM) may predispose an athlete to injury if theseforces continually exceed the strain capabilities ofthe joint connective tissues (Comfort amp Kasim2007) That is why it is beneficial to maintain aposture that is as close to upright as possible at alltimes for preventing the lumbar injuries (Schoenfeld2010)
Conclusion
We studied the musculature activity and kinematicsof knee and hip joints during front and back squatswith maximum loading (1RM) The front squat wasshown to be just as effective as the back squat undermaximum loading conditions in terms of overallmuscle activity with no difference in knee joint kine-matics and significantly less forward lean in hip jointwhich may probably show less lumbar injury riskWe also managed to show that the front squat cre-ated higher EMG activity in vastus medialis despitethe lighter loads compared to back squat that agrees
with the idea of ldquobeing a more isolated movementfor knee extensorsrdquo It is a known fact that the backsquat is used much more commonly compared to itsfront variation Results may suggest that the frontsquat may be a better choice for focusing on kneeextensor improvement andor for preventing lumbarinjuries under maximum loading conditions
References
American College of Sports Medicine (1998) Position standThe recommended quantity and quality of exercise for devel-oping and maintaining cardiorespiratory and muscular fitnessand flexibility in healthy adults Medicine and Science in Sportsand Exercise 975ndash991 doi101249MSS0b013e318213fefb
Baechle T R amp Earle R (2000) Essentials of strength trainingand conditioning (2nd ed) Champaign IL Human Kinetics
Balshaw T G amp Hunter A M (2012) Evaluation of electro-myography normalisation methods for the back squat Journalof Electromyography and Kinesiology 22 308ndash319
Braidot A A Brusa M H Lestussi F E amp Parera G P(2007) Biomechanics of front and back squat exercises Journalof Physics Conference Series 90 012009
Broer M R amp Houtz S J (1967) Patterns of muscular activity inselected sport skills (3rd ed) Springfield Charles C ThomasPublishing
Carpinelli R N (2008) The size principle and a critical analysisof the unsubstantiated heavier-is-better recommendation forresistance training Journal of Exercise Science and Fitness 667ndash86
Channell B T amp Barfield J P (2008) Effect of Olympic andtraditional resistance training on vertical jump improvement inhigh school boys Journal of Strength Conditioning and Research22 1522ndash1527
Clark D R Lambert M I amp Hunter A M (2012) Muscleactivation in the loaded free barbell squat A brief reviewJournal of Strength Conditioning and Research 26 1169ndash1178
Cohen J (1988) Statistical power analysis for the behavioral sciencesHillsdale NJ Lawrence Erlbaum
Comfort P amp Kasim P (2007) Optimizing squat techniqueStrength and Conditioning Journal 29 10ndash13
Delavier F (2001) Strength training anatomy Champaign ILHuman Kinetics
Diggin D OrsquoRegan C Whelan N Daly S McLoughlin VMcNamara L amp Reilly A (2011) A biomechanical ana-lysis of front vs back squat Injury implications PortugueseJournal of Sports Sciences 11(Suppl 2) Retrieved from httpwwwresearchgatenetpublication258363730_A_biomechanical_Analysis_of_front_and_back_squat_injury_implicationsfilee0b49528105693baa7pdf
Dionisio V C Almeida G L Duarte M amp Hirata R P(2008) Kinematic kinetic and EMG patterns during down-ward squatting Journal of Electromyography and Kinesiology 18134ndash143
Donnelly D V Berg W P amp Fiske D M (2006) The effectof the direction of gaze on the kinematics of the squat exerciseJournal of Strength Conditioning and Research 20 145ndash150Retrieved from httpwwwresearchgatenetpublication7273329_The_effect_of_the_direction_of_gaze_on_the_kinem-atics_of_the_squat_exerciselinks0c960523c48a69975c000000+ampcd=2amphl=trampct=clnk
Escamilla R F (2000) Knee biomechanics of the dynamic squatexercise Medicine amp Science in Sports amp Exercise 33 127ndash141
Escamilla R F Fleisig G S Lowry T M Barrentine S Wamp Andrews J R (2001) A three-dimensional biomechanicalanalysis of the squat during varying stance widths Medicine and
EMG Kinematic activities of back and front squat 1065
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015
Science in Sports and Exercise 33 984ndash998 Retrieved fromhttpwwwsweatpitcomforumstudiesSquattingA20three-dimensional20biomechanical20analysispdf
Escamilla R F Fleisig G S Zheng N Barrentine S WWilk K E amp Andrews J R (1998) Biomechanics of theknee during closed kinetic chain and open kinetic chain exer-cises Medicine and Science in Sports and Exercise 30 556ndash569doi10109700005768-199804000-00014
Escamilla R F Fleisig G S Zheng N Lander J EBarrentine S W Andrews J R Moorman C T(1997) The effects of technique variations on knee biomecha-nics during the squat and leg press Medicine and Science inSports and Exercise 29 156 doi10109700005768-200109000-00020
Escamilla R F Fleisig G S Zheng N Lander J EBarrentine S W Andrews J R hellip Moorman III C T(2000) Effects of technique variations on knee biomechanicsduring the squat and leg press Medicine amp Science in Sports ampExercise 33 1552ndash1566
Flanagan S Salem G J Wang M Y Sanker S ampGreendale G A (2003) Squatting exercises in older adultsKinematic and kinetic comparisons Medicine and Science inSports and Exercise 35 635ndash643 doi10124901MSS00000583644797306
Fleck S J (1999) Periodized strength training A critical reviewJournal of Strength Conditioning amp Research 13 82ndash89 Retrievedfrom httpjournalslwwcomnsca-jscrabstract199902000periodized_strength_training__a_critical_review15aspx
Grahammer J (1986) Sports illustrated strength training NewYork NY Harper amp Row
Gullett J C Tillman M D Gutierrez G M amp Chow J W(2009) A biomechanical comparison of back and front squatsin healthy trained individuals Journal of Strength andConditioning Research 23 284ndash292
Hasegawa I (2004) Using the overhead squat for core develop-ment NSCA Performance Training Journal 6 19ndash21
Hatfield F C (1983) Power A scientific approach Chicago ILContemporary Books Inc
Hay J G Andrews J G Vaughan C L amp Ueya K (1983)Load speed and equipment effects in strength-training exer-cises In H Matsui amp K Kobayashi (Eds) Biomechanics (3rded) Champaign IL Human Kinetics
Hwang S Kim Y amp Kim Y (2009) Lower extremity jointkinetics and lumbar curvature during squat and stoop liftingBMC Musculoskeletal Disorders 10 15 doi1011861471-2474-10-15
Isear J A Erickson Jr J C amp Worrel T W (1997) EMGanalysis of lower extremity muscle recruitment patterns duringan unloaded squat Medicine amp Science in Sports amp Exercise 29532ndash539
Kellis E Arambatzi F amp Papadopoulos C (2005) Effects ofload on ground reaction force and lower limb kinematics dur-ing concentric squats Journal of Sports Sciences 23 1045ndash1055
Konrad P (2005) ABC of EMG a practical introduction to kinesio-logical electromyography (1st ed) Scottsdale AZ Noraxon Inc
Kraemer W J amp Fry A C (1995) Strength testingDevelopment and evaluation of methodology In P Maud ampC Foster (Eds) Physiological assessment of human fitness(pp 115ndash138) Champaign IL Human Kinetics
Kraemer W J amp Ratamess N A (2004) Fundamentals ofresistance training Progression and exercise prescriptionMedicine amp Science in Sports amp Exercise 36 674ndash688
Matsumoto H Suda Y Otani T Niki Y Seedhom B B ampFujikawa K (2001) Roles of the anterior cruciate ligamentand the medial collateral ligament in preventing valgus instabil-ity Journal of Orthopaedic Science 6 28ndash32
McCaw S T amp Melrose D R (1999) Stance width and barload effects on leg muscle activity during the parallel squatMedicine and Science in Sports and Exercise 31 428ndash436
Merletti R (1999) Standards for reporting EMG data Journal ofElectromyography and Kinesiology 9 3ndash4 Retrieved from httpwwwisek onlineorgstandards_emghtml
Rippetoe M amp Kilgore L (2007) Starting strength Basic barbelltraining (2nd ed) Wichita Falls TX The Aasgaard Company
Russell P J amp Phillips S J (1989) A preliminary comparison offront and back squat exercises Research Quarterly for Exerciseand Sport 60 201ndash208
Schoenfeld B J (2010) Squatting kinematics and kinetics andtheir application to exercise performance Journal of Strengthand Conditioning Research 24 3497ndash3506
Scotten C M (2010) Differences in muscle activation in the lowerextremities while performing traditional squats and non-traditionalsquats (Master thesis) Boise State University Boise
Senter C amp Hame S L (2006) Biomechanical analysis of tibialtorque and knee flexion angle Implications for understandingknee injury Sports Medicine 36 635ndash641
Stensdotter A K Hodges P W Mellor R Sundelin G ampHager R C (2003) Quadriceps activation in closed and in openkinetic chain exercise Medicine and Science in Sports and Exercise35 2043ndash2047 doi10124901MSS000009910703704AE
Stuart M J Meglan D A Lutz G E Growney E S amp AnK N (1996) Comparison of intersegmental tibiofemoraljoint forces and muscle activity during various closed kineticchain exercises The American Journal of Sports Medicine 24792ndash799
Swinton P A Aspe R amp Keogh J (2012 July)Electromyographic comparison of The back squat and overheadsquat 30th Annual Conference of Biomechanics İn SportsMelbourne
Wretneberg P Feng Y amp Arborelius U P (1996) High- andlow-bar squatting techniques during weight-training Medicineand Science in Sports and Exercise 28 218ndash224
Wretneberg P Feng Y Lindberg F amp Arborelius U P(1993) Joint moments of force and quadriceps muscle activityduring squatting exercise Scandinavian Journal of Medicine ampScience in Sports 3 244ndash250
1066 HU Yavuz et al
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015

range of motion and correct technique Each partici-pant was asked to lower the bar to the point where theknee angle was 90deg (Figure 2) which was marked byadjustable stoppers Adequate rest was allowedbetween trials (3ndash5 min) Subsequently 1 week afterthe pretest session the participants performed a sec-ond session for data collection For each participantall data collection was performed in one day session
After the EMG electrode placement maximumvoluntary isometric contraction (MVIC) data fromthe quadriceps hamstrings erector spine and glu-teus maximus were collected according to the pro-cedures described by Konrad (2005) Three 3-sMVIC trials were collected in a randomised mannerfor each muscle group Adequate rest was allowedbetween trials (1 min)
All participants performed two to three warm-upsets in preparation for testing For both lifting varia-tions each participant used their 1RM weights pre-viously established for the back squat and frontsquat Exercise began with a given verbal commandThe starting and ending positions for the back squatand front squat were with the knees in full extensionwhich was defined as 180deg knee angle From thestarting position the participant flexed their kneesto minimum knee angle (approximately 90deg) andthen extended their knees back to the startingposition
During the back squat the barbell positionedacross the shoulder on the trapezius slightly abovethe posterior aspect of the deltoids and the hips andknees flexed until the thighs are parallel to the floor(Baechle and Earle 2000 Delavier 2001) Thenthe participant extended the hips and knees untilthe starting position is reached keeping the backflat the heels on the floor and the knees alignedover the feet (Baechle and Earle 2000 Delavier2001) During the front squat the barbell positionedacross the anterior deltoids and clavicles and theelbows fully flexed to position the upper arms paral-lel to the floor (Baechle and Earle 2000 Delavier
2001) The descending and ascending motions aremuch the same as in the back squat (Gullett et al2009) Adequate rest was allowed between trials (3ndash5 min)
Data reduction
The sampling of EMG and video recordings wereinitiated simultaneously with the beginning of thefirst squat repetition For synchronisation a LEDconnected to the trigger box (National InstrumentsUSB-6501 Digital IO) outputted a digital signalwhen the Myomonitor started data acquisitionWith the data acquisition the LED lit and it wentoff as the data stopped The data obtained from thisprocedure were used to specify the start of therequired portion and the length of the requestedportion
Kinematical data were analysed by using thesaSuite two-dimensional kinematical analysis pro-gramme which was developed by HacettepeUniversity Faculty of Sports SciencesBiomechanics Research Group Ankara TurkeyFor each trail the required portion of the videorecordings was trimmed the anthropometric pointswere digitised and the two-dimensional positionaldata were obtained The raw position data of thejoints were smoothed using a moving average filterand the angular kinematics of the knee and hip jointswere calculated All EMG data were partitioned intoascending and descending phases Movement timewas normalised into 10 movement phases to controlinter-individual differences Knee and hip anglechanges were examined throughout the descendingand ascending phases
EMG data were analysed according to the proce-dures from International Society ofElectrophysiology and Kinesiology (Merletti 1999)by using the EMG Works Analysis 40 (Delsys IncBoston) To calculate the mean normalised EMGvalues the raw EMG signals were subsetted filtered(Passband 3 Response Bandpass Corner F110 Hz Corner F2 500 Hz) rectified integrated(root mean square (Window Length 0100Window Overlap 008 Remove Ofset)) and nor-malised to the participants highest correspondingMVIC trial
Statistical analysis
Kinematic and electromyographic data were ana-lysed and compared between the front and backsquad by using paired sample t-tests (P lt 005)Throughout the text data for all participants per-forming each type of exercise were averaged andpresented as means standard deviations P-valueeffect size (Cohenrsquos d Cohen 1988) and 95
Figure 2 Illustrations of measured joint angles during back squatand front squat (adapted from Starting Strength Basic BarbellTraining by permission of The Aasgaard Company Rippetoe ampKilgore 2007)
EMG Kinematic activities of back and front squat 1061
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015
confidence intervals Cohenrsquos categories were usedto evaluate the magnitude of these sizes (small if0 le [d] le 05 medium if 05 le [d] le 08 and large if[d] gt 08) (Cohen 1988)
Results
The mean 1RM loads that were employed duringtesting were 10917 plusmn 2551 kg for the back squatand 8500 plusmn 1567 kg for the front squat This was13883 plusmn 3262 of their body weight for back squatand 10587 plusmn 2434 for front squat Participantscould lift significantly higher loads with back squatcomparing to the front squat (P lt 005 d = minus12895 CI 16283204)
Normalised EMG values as a percentage of max-imal voluntary isometric contraction ( MVIC)P-values effect size (Cohenrsquos d Cohen 1988) and95 confidence intervals between back and frontsquats are shown in Table II Vastus medialisEMG activity was found to be greater during thefront squat compared to back squat (P lt 005
d = 041 95 CI minus128minus43) There were noother differences in any other muscles
Normalised average EMG values as a MVIC P-values effect size (Cohenrsquos d Cohen 1988) and 95confidence intervals between descending and ascend-ing phases performed with 1RM loads between backand front squats are shown in Table III EMG activ-ities of gluteus maximus (P lt 005 d = 078 95 CIminus2581minus1120) biceps femoris (P lt 005 d = 09795 CI minus1974minus1260) and semitendinosus(P lt 005 d = 105 95 CI minus2072minus728) duringback squat and EMG activities of gluteus maximus(P lt 005 d = 062 95 CI minus2209minus1118) bicepsfemoris (P lt 005 d = 038 95 CI minus1486minus471)and semitendinosus (P lt 005 d = 048 95 CIminus840minus34) during front squat were found to be sig-nificantly higher EMG activity of the vastus medialis(P lt 005 d = 032 95CI minus1103minus53) during theascending phase was higher only
The mean EMG activities as a percentage of max-imal voluntary isometric contraction ( MVIC)P-values effect size (Cohenrsquos d Cohen 1988) and
Table II Mean EMG activities as a percentage of maximal voluntary isometric contraction ( MVIC) P-values effect size(Cohenrsquos d Cohen 1988) and 95 confidence intervals for the back squats and front squats throughout entire movementsperformed with 1RM loads
Muscle Back squat (mean plusmn s) Front squat (mean plusmns) P d
95 CI
L U
Rectus femoris 367 plusmn 124 461 plusmn 217 0118 053 minus217 282Vastus medialis 488 plusmn 139 554 plusmn 180 0038 041 minus128 minus043Vastus lateralis 470 plusmn 151 512 plusmn 173 0149 026 minus102 minus175Erector spinae 432 plusmn 156 462 plusmn 121 0495 022 minus125 049Gluteus maximus 371 plusmn 235 372 plusmn 270 0959 0 minus55 523Biceps femoris 262 plusmn 161 241 plusmn 254 0611 minus0 minus65 106Semitendinosus 215 plusmn 117 160 plusmn 87 0115 minus053 minus16 126
Note Significantly higher EMG activities during the front squat compared to the back squat (P lt 005)
Table III Back squats and front squats mean EMG activities as a percentage of maximal voluntary isometric contraction ( MVIC)P-values effect size (Cohenrsquos d Cohen 1988) and 95 confidence intervals between descending and ascending phases performed with1RM loads
Back squat Front squat
Descendingphase
(mean plusmns)
Ascendingphase
(mean plusmn s) P d
95 CI Descendingphase
(mean plusmn s)
Ascendingphase
(mean plusmn s) P d
95 CI
Muscle L U L U
Rectus femoris 379 plusmn 121 360 plusmn 138 0455 minus015 minus3562 minus7432 464 plusmn 244 467 plusmn 194 0922 001 minus7122 6500Vastus medialis 483 plusmn 143 493 plusmn 139 0617 007 minus5293 3286 531 plusmn 193 589 plusmn 171 033 032 minus11036 minus533Vastus lateralis 459 plusmn 139 485 plusmn 172 0223 017 minus7005 1821 480 plusmn 158 562 plusmn 222 068 043 minus17190 07269Erector spinae 411 plusmn 140 460 plusmn 176 0124 031 minus11286 1564 451 plusmn 120 481 plusmn 168 0451 020 minus11276 5367Gluteus maximus 288 plusmn 189 473 plusmn 277 0000 078 minus25810 minus11200 300 plusmn 230 466 plusmn 301 0000 062 minus22098 minus11188Biceps femoris 187 plusmn 149 349 plusmn 182 0000 097 minus19740 minus12600 197 plusmn 233 295 plusmn 287 0001 038 minus14864 minus4711Semitendinosus 150 plusmn 69 290 plusmn 162 0001 105 minus20720 minus7280 140 plusmn 81 184 plusmn 101 0036 048 minus8404 minus0343
Note Significantly higher EMG activities during the ascending phase compared to the descending phase (P lt 005)
1062 HU Yavuz et al
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015
95 confidence intervals between back squats andfront squats during the descending and ascendingphases performed with 1RM loads are shownin Table IV There were no significant differencesobserved between back and front squats duringthe descending phase During the ascending phasethe EMG activity of the vastus medialis was foundto be significantly higher in the front squat comparedto the back squat (P lt 005 d = 062 95 CIminus1500minus417) while the EMG activity of the semi-tendinosus was higher in the back squat compared tothe front squat (P lt 05 d = minus079 95 CI 622059)
As can be seen from Figure 3 significant differ-ences were observed between minimum hip anglesreached during back squats and front squats Theaverage minimum hip angle was significantly higher(P lt 005 d = 108 95 CI minus2857minus428) duringthe front squat compared to the back squat
Figure 4 shows the mean changes in knee and hipangles throughout the ascending phases of bothsquatting movements No difference was observed
in knee angles during the whole movement whilehip angles were lower in 8 of 10 phases during theback squat compared to front squat showing anobvious forward trunk lean According to theangle-specific EMG changes semitendinosus(P lt 005 d = minus023 95 CI minus2421111) showeda sudden increase in the sixth phase and bicepsfemoris (P lt 005 d = minus014 95 CI minus10931911) and gluteus maximus (P lt 005 d = minus03795 CI minus4533089) showed a similar but smallerincrease in the eighth phase during the back squatcompared to the front squat
Discussion
Participants could lift significantly greater loads withback squat compared to the front squat(1388 plusmn 326 of their body weight1059 plusmn 243 of their body weight respectively)(Figure 1) and this finding is consistent with theprevious studies (Gullett et al 2009 Russell ampPhillips 1989)
Instead of the load the level of effort in voluntarymuscle actions determines the degree of motor unitactivity (Carpinelli 2008) consequently the level ofEMG signalling increases Furthermore higherloads may increase intradiscal pressure (11) com-pression on vertebral bodies (10) tibiofemoral (1213) and patellofemoral joints (14) which could pos-sibly increase the risk of injury while performingsquat Gullett et al (2009) emphasised that the mus-cles tested were equally active during the front squatwhile lifting less mass and it seems that the extraload lifted during the back squat is what accounts forthe increased tibiofemoral compressive forces andextensor moments observed during these lifts It is
Table IV Mean EMG activities as a percentage of maximal voluntary isometric contraction ( MVIC) P-values effect size (Cohenrsquos dCohen 1988) and 95 confidence intervals between back squats and front squats during the descending and ascending phases performedwith 1RM loads
Descending phase Ascending phase
Back squat(mean plusmn s)
Front squat(mean plusmn s) P d
95 CIBack squat(mean plusmn s)
Front squat(mean plusmn s) P d
95 CI
Muscle L U L U
Rectus femoris 379 plusmn 121 464 plusmn 244 0200 044 minus22011 5164 360 plusmn 138 467 plusmn 194 0061 064 minus21917 0578Vastus medialis 483 plusmn 143 531 plusmn 193 0204 028 minus12627 3020 493 plusmn 139 589 plusmn 171 0002 062 minus15001 minus4177Vastus lateralis 459 plusmn 139 480 plusmn 158 0396 014 minus7088 3028 485 plusmn 172 562 plusmn 222 0096 039 minus16932 1590Erector spinae 411 plusmn 140 451 plusmn 120 0438 031 minus14953 6940 460 plusmn 176 481 plusmn 168 0665 012 minus12493 8292Gluteus maximus 288 plusmn 189 300 plusmn 230 0573 006 minus5460 3181 473 plusmn 277 466 plusmn 301 0841 minus002 minus7001 8447Biceps femoris 187 plusmn 149 197 plusmn 233 0765 005 minus7883 5959 349 plusmn 182 295 plusmn 287 0329 minus022 minus6257 17099Semitendinosus 150 plusmn 69 140 plusmn 81 0676 minus013 minus4052 6019 290 plusmn 162 184 plusmn 101 0039 minus079 0624 20595
Notes Significantly higher EMG activities during the front squat compared to the back squat (P lt 005) Significantly higher EMGactivities during the back squat compared to the front squat (P lt 005)
Figure 3 Minimum hip angles reached during the back squat (BS)and front squat (FS) Significant differences (P lt 005) betweenthe back and front squats
EMG Kinematic activities of back and front squat 1063
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015
very important because excessive tibiofemoral com-pressive forces could be deleterious to the menisciand articular cartilage (Escamilla 2000)
During the squat the primary muscles actingaround the knee are the quadriceps femoris (vastuslateralis vastus medialis vastus intermedius and rec-tus femoris) which carry out concentric knee exten-sion as well as eccentrically resisting knee flexionFor both back and front squats vastus medialis andvastus lateralis produced more activity than the rec-tus femoris during the whole manoeuvre which is inagreement with the data from Escamilla et al (19971998) Escamilla (2000) Escamilla et al (2000)Hwang Kim and Kim (2009) Wretneberg Feng
Lindberg and Arborelius (1993) Wretneberg et al(1996) and Isear et al (1997)
Schoenfeld (2010) reported that this may be logi-cal because the rectus femoris is both a hip flexorand knee extensor and thus shortens at one endwhile lengthening at the other during the squatwith little if any net change in length throughoutmovement
Although the loads were heavier during the backsquat mean EMG activities in selected musclesshowed no difference with only one exceptionDespite the lighter loads during the front squatvastus medialis mean EMG activity was greaterthan the back squat during the whole manoeuvresGullett et al (2009) and Stuart Meglan LutzGrowney and An (1996) reported no differences inmuscle activities between front and back squats Thedifference in our study can be resulted from thehigher loads compared to Gullett et al (2009)(70 of 1RM) and Stuart et al (1996) (50 pounds)which may recruit more motor units during themovements
When we divided the manoeuvres into ascendingand descending phases all muscles tested were moreactive during the ascending phase than during thedescending phase These findings are in accordancewith those of several other studies (Escamilla et al1998 Escamilla et al 2000 Gullett et al 2009McCaw amp Melrose 1999 Stuart et al 1996)EMG activities were higher during the ascendingphase compared to the descending phase for allmuscles during both the front and the back squatBut statistically significant differences were seen forgluteus maximus semitendinosus and bicepsfemoris during both the front and the back squatand for vastus medialis during the front squat
We observed no significant EMG activity differ-ences between the back and front squats during thedescending phases However during the ascendingphase EMG activity of the vastus medialis was higherin the front squat compared to the back squat whileEMG activity of the semitendinosus was higher inthe back squat compared to the front squat Thefront squat is believed to be a more isolated man-oeuvre for quadriceps (Grahammer 1986 Hatfield1983) and this result may support this idea Theheavier external resistance and more inclined torsoduring the back squat create a larger resistancemoment which requires greater muscular effort tocounterbalance (Swinton Aspe amp Keogh 2012) Itwas shown that increased forward trunk lean causesan increase in hamstring activity (Escamilla et al2000 Gullett et al 2009 Scotten 2010) Thismay explain the higher semitendinosus EMG activityduring the ascending phase of the back squats
When we divided the manoeuvres into 10 phasesfor being able to compare the movement patterns
Figure 4 Knee and hip angle-dependent EMG values of rectusfemoris (RF) vastus medialis (VM) vastus lateralis (VL) erectorspinae (ES) gluteus maximus (GM) biceps femoris (BF) andsemitendinosus (ST) throughout the phases of both backs squat(BS) and front squat (FS) movements Significant differences(P lt 005) between back and front squats
1064 HU Yavuz et al
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015
we did not observe any significant difference in kneeangles between the back and front squats Howeverwe observed significantly lower hip angles in 8 of 10phases during the back squat The lowest hip anglesreached during the manoeuvres were significantlylower in the back squat compared to the frontsquat These findings showed an increased forwardlean during the back squat compared to the frontsquat during maximum loading
When we check angle-specific EMG changes foreach muscle we saw that EMG activity patternswere quite parallel to each other for most of themuscles in both squat variants SemitendinosusEMG activity showed a sudden increase in thesixth phase which also shows the lowest hip angleand the starting of the ascending phase Gluteusmaximus and biceps femoris showed a similar butweaker change in pattern during the middle of theascending phase (eighth phase) This may probablybe due to the extra effort of the hip extensors tomaintain the balance by compensating the increasedforward lean during back squat
In both the squatting techniques as the perfor-mers lower throughout the eccentric phase they arerequired to lean forward in order to maintain bal-ance Centre of gravity moves further away from thelumbar spine increasing the moment arm and tor-que As a result the shear forces occurring withinthe lumbar spine would also increase (Comfort ampKasim 2007 Diggin et al 2011 Gullett et al2009) Increased forward lean reduces tolerance tocompressive load and results in a transfer of the loadfrom muscles to passive tissues heightening the riskof disc herniation (Matsumoto et al 2001)
As previously stated such an increase in shearforce under regular high loading conditions (eg1RM) may predispose an athlete to injury if theseforces continually exceed the strain capabilities ofthe joint connective tissues (Comfort amp Kasim2007) That is why it is beneficial to maintain aposture that is as close to upright as possible at alltimes for preventing the lumbar injuries (Schoenfeld2010)
Conclusion
We studied the musculature activity and kinematicsof knee and hip joints during front and back squatswith maximum loading (1RM) The front squat wasshown to be just as effective as the back squat undermaximum loading conditions in terms of overallmuscle activity with no difference in knee joint kine-matics and significantly less forward lean in hip jointwhich may probably show less lumbar injury riskWe also managed to show that the front squat cre-ated higher EMG activity in vastus medialis despitethe lighter loads compared to back squat that agrees
with the idea of ldquobeing a more isolated movementfor knee extensorsrdquo It is a known fact that the backsquat is used much more commonly compared to itsfront variation Results may suggest that the frontsquat may be a better choice for focusing on kneeextensor improvement andor for preventing lumbarinjuries under maximum loading conditions
References
American College of Sports Medicine (1998) Position standThe recommended quantity and quality of exercise for devel-oping and maintaining cardiorespiratory and muscular fitnessand flexibility in healthy adults Medicine and Science in Sportsand Exercise 975ndash991 doi101249MSS0b013e318213fefb
Baechle T R amp Earle R (2000) Essentials of strength trainingand conditioning (2nd ed) Champaign IL Human Kinetics
Balshaw T G amp Hunter A M (2012) Evaluation of electro-myography normalisation methods for the back squat Journalof Electromyography and Kinesiology 22 308ndash319
Braidot A A Brusa M H Lestussi F E amp Parera G P(2007) Biomechanics of front and back squat exercises Journalof Physics Conference Series 90 012009
Broer M R amp Houtz S J (1967) Patterns of muscular activity inselected sport skills (3rd ed) Springfield Charles C ThomasPublishing
Carpinelli R N (2008) The size principle and a critical analysisof the unsubstantiated heavier-is-better recommendation forresistance training Journal of Exercise Science and Fitness 667ndash86
Channell B T amp Barfield J P (2008) Effect of Olympic andtraditional resistance training on vertical jump improvement inhigh school boys Journal of Strength Conditioning and Research22 1522ndash1527
Clark D R Lambert M I amp Hunter A M (2012) Muscleactivation in the loaded free barbell squat A brief reviewJournal of Strength Conditioning and Research 26 1169ndash1178
Cohen J (1988) Statistical power analysis for the behavioral sciencesHillsdale NJ Lawrence Erlbaum
Comfort P amp Kasim P (2007) Optimizing squat techniqueStrength and Conditioning Journal 29 10ndash13
Delavier F (2001) Strength training anatomy Champaign ILHuman Kinetics
Diggin D OrsquoRegan C Whelan N Daly S McLoughlin VMcNamara L amp Reilly A (2011) A biomechanical ana-lysis of front vs back squat Injury implications PortugueseJournal of Sports Sciences 11(Suppl 2) Retrieved from httpwwwresearchgatenetpublication258363730_A_biomechanical_Analysis_of_front_and_back_squat_injury_implicationsfilee0b49528105693baa7pdf
Dionisio V C Almeida G L Duarte M amp Hirata R P(2008) Kinematic kinetic and EMG patterns during down-ward squatting Journal of Electromyography and Kinesiology 18134ndash143
Donnelly D V Berg W P amp Fiske D M (2006) The effectof the direction of gaze on the kinematics of the squat exerciseJournal of Strength Conditioning and Research 20 145ndash150Retrieved from httpwwwresearchgatenetpublication7273329_The_effect_of_the_direction_of_gaze_on_the_kinem-atics_of_the_squat_exerciselinks0c960523c48a69975c000000+ampcd=2amphl=trampct=clnk
Escamilla R F (2000) Knee biomechanics of the dynamic squatexercise Medicine amp Science in Sports amp Exercise 33 127ndash141
Escamilla R F Fleisig G S Lowry T M Barrentine S Wamp Andrews J R (2001) A three-dimensional biomechanicalanalysis of the squat during varying stance widths Medicine and
EMG Kinematic activities of back and front squat 1065
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015
Science in Sports and Exercise 33 984ndash998 Retrieved fromhttpwwwsweatpitcomforumstudiesSquattingA20three-dimensional20biomechanical20analysispdf
Escamilla R F Fleisig G S Zheng N Barrentine S WWilk K E amp Andrews J R (1998) Biomechanics of theknee during closed kinetic chain and open kinetic chain exer-cises Medicine and Science in Sports and Exercise 30 556ndash569doi10109700005768-199804000-00014
Escamilla R F Fleisig G S Zheng N Lander J EBarrentine S W Andrews J R Moorman C T(1997) The effects of technique variations on knee biomecha-nics during the squat and leg press Medicine and Science inSports and Exercise 29 156 doi10109700005768-200109000-00020
Escamilla R F Fleisig G S Zheng N Lander J EBarrentine S W Andrews J R hellip Moorman III C T(2000) Effects of technique variations on knee biomechanicsduring the squat and leg press Medicine amp Science in Sports ampExercise 33 1552ndash1566
Flanagan S Salem G J Wang M Y Sanker S ampGreendale G A (2003) Squatting exercises in older adultsKinematic and kinetic comparisons Medicine and Science inSports and Exercise 35 635ndash643 doi10124901MSS00000583644797306
Fleck S J (1999) Periodized strength training A critical reviewJournal of Strength Conditioning amp Research 13 82ndash89 Retrievedfrom httpjournalslwwcomnsca-jscrabstract199902000periodized_strength_training__a_critical_review15aspx
Grahammer J (1986) Sports illustrated strength training NewYork NY Harper amp Row
Gullett J C Tillman M D Gutierrez G M amp Chow J W(2009) A biomechanical comparison of back and front squatsin healthy trained individuals Journal of Strength andConditioning Research 23 284ndash292
Hasegawa I (2004) Using the overhead squat for core develop-ment NSCA Performance Training Journal 6 19ndash21
Hatfield F C (1983) Power A scientific approach Chicago ILContemporary Books Inc
Hay J G Andrews J G Vaughan C L amp Ueya K (1983)Load speed and equipment effects in strength-training exer-cises In H Matsui amp K Kobayashi (Eds) Biomechanics (3rded) Champaign IL Human Kinetics
Hwang S Kim Y amp Kim Y (2009) Lower extremity jointkinetics and lumbar curvature during squat and stoop liftingBMC Musculoskeletal Disorders 10 15 doi1011861471-2474-10-15
Isear J A Erickson Jr J C amp Worrel T W (1997) EMGanalysis of lower extremity muscle recruitment patterns duringan unloaded squat Medicine amp Science in Sports amp Exercise 29532ndash539
Kellis E Arambatzi F amp Papadopoulos C (2005) Effects ofload on ground reaction force and lower limb kinematics dur-ing concentric squats Journal of Sports Sciences 23 1045ndash1055
Konrad P (2005) ABC of EMG a practical introduction to kinesio-logical electromyography (1st ed) Scottsdale AZ Noraxon Inc
Kraemer W J amp Fry A C (1995) Strength testingDevelopment and evaluation of methodology In P Maud ampC Foster (Eds) Physiological assessment of human fitness(pp 115ndash138) Champaign IL Human Kinetics
Kraemer W J amp Ratamess N A (2004) Fundamentals ofresistance training Progression and exercise prescriptionMedicine amp Science in Sports amp Exercise 36 674ndash688
Matsumoto H Suda Y Otani T Niki Y Seedhom B B ampFujikawa K (2001) Roles of the anterior cruciate ligamentand the medial collateral ligament in preventing valgus instabil-ity Journal of Orthopaedic Science 6 28ndash32
McCaw S T amp Melrose D R (1999) Stance width and barload effects on leg muscle activity during the parallel squatMedicine and Science in Sports and Exercise 31 428ndash436
Merletti R (1999) Standards for reporting EMG data Journal ofElectromyography and Kinesiology 9 3ndash4 Retrieved from httpwwwisek onlineorgstandards_emghtml
Rippetoe M amp Kilgore L (2007) Starting strength Basic barbelltraining (2nd ed) Wichita Falls TX The Aasgaard Company
Russell P J amp Phillips S J (1989) A preliminary comparison offront and back squat exercises Research Quarterly for Exerciseand Sport 60 201ndash208
Schoenfeld B J (2010) Squatting kinematics and kinetics andtheir application to exercise performance Journal of Strengthand Conditioning Research 24 3497ndash3506
Scotten C M (2010) Differences in muscle activation in the lowerextremities while performing traditional squats and non-traditionalsquats (Master thesis) Boise State University Boise
Senter C amp Hame S L (2006) Biomechanical analysis of tibialtorque and knee flexion angle Implications for understandingknee injury Sports Medicine 36 635ndash641
Stensdotter A K Hodges P W Mellor R Sundelin G ampHager R C (2003) Quadriceps activation in closed and in openkinetic chain exercise Medicine and Science in Sports and Exercise35 2043ndash2047 doi10124901MSS000009910703704AE
Stuart M J Meglan D A Lutz G E Growney E S amp AnK N (1996) Comparison of intersegmental tibiofemoraljoint forces and muscle activity during various closed kineticchain exercises The American Journal of Sports Medicine 24792ndash799
Swinton P A Aspe R amp Keogh J (2012 July)Electromyographic comparison of The back squat and overheadsquat 30th Annual Conference of Biomechanics İn SportsMelbourne
Wretneberg P Feng Y amp Arborelius U P (1996) High- andlow-bar squatting techniques during weight-training Medicineand Science in Sports and Exercise 28 218ndash224
Wretneberg P Feng Y Lindberg F amp Arborelius U P(1993) Joint moments of force and quadriceps muscle activityduring squatting exercise Scandinavian Journal of Medicine ampScience in Sports 3 244ndash250
1066 HU Yavuz et al
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015

confidence intervals Cohenrsquos categories were usedto evaluate the magnitude of these sizes (small if0 le [d] le 05 medium if 05 le [d] le 08 and large if[d] gt 08) (Cohen 1988)
Results
The mean 1RM loads that were employed duringtesting were 10917 plusmn 2551 kg for the back squatand 8500 plusmn 1567 kg for the front squat This was13883 plusmn 3262 of their body weight for back squatand 10587 plusmn 2434 for front squat Participantscould lift significantly higher loads with back squatcomparing to the front squat (P lt 005 d = minus12895 CI 16283204)
Normalised EMG values as a percentage of max-imal voluntary isometric contraction ( MVIC)P-values effect size (Cohenrsquos d Cohen 1988) and95 confidence intervals between back and frontsquats are shown in Table II Vastus medialisEMG activity was found to be greater during thefront squat compared to back squat (P lt 005
d = 041 95 CI minus128minus43) There were noother differences in any other muscles
Normalised average EMG values as a MVIC P-values effect size (Cohenrsquos d Cohen 1988) and 95confidence intervals between descending and ascend-ing phases performed with 1RM loads between backand front squats are shown in Table III EMG activ-ities of gluteus maximus (P lt 005 d = 078 95 CIminus2581minus1120) biceps femoris (P lt 005 d = 09795 CI minus1974minus1260) and semitendinosus(P lt 005 d = 105 95 CI minus2072minus728) duringback squat and EMG activities of gluteus maximus(P lt 005 d = 062 95 CI minus2209minus1118) bicepsfemoris (P lt 005 d = 038 95 CI minus1486minus471)and semitendinosus (P lt 005 d = 048 95 CIminus840minus34) during front squat were found to be sig-nificantly higher EMG activity of the vastus medialis(P lt 005 d = 032 95CI minus1103minus53) during theascending phase was higher only
The mean EMG activities as a percentage of max-imal voluntary isometric contraction ( MVIC)P-values effect size (Cohenrsquos d Cohen 1988) and
Table II Mean EMG activities as a percentage of maximal voluntary isometric contraction ( MVIC) P-values effect size(Cohenrsquos d Cohen 1988) and 95 confidence intervals for the back squats and front squats throughout entire movementsperformed with 1RM loads
Muscle Back squat (mean plusmn s) Front squat (mean plusmns) P d
95 CI
L U
Rectus femoris 367 plusmn 124 461 plusmn 217 0118 053 minus217 282Vastus medialis 488 plusmn 139 554 plusmn 180 0038 041 minus128 minus043Vastus lateralis 470 plusmn 151 512 plusmn 173 0149 026 minus102 minus175Erector spinae 432 plusmn 156 462 plusmn 121 0495 022 minus125 049Gluteus maximus 371 plusmn 235 372 plusmn 270 0959 0 minus55 523Biceps femoris 262 plusmn 161 241 plusmn 254 0611 minus0 minus65 106Semitendinosus 215 plusmn 117 160 plusmn 87 0115 minus053 minus16 126
Note Significantly higher EMG activities during the front squat compared to the back squat (P lt 005)
Table III Back squats and front squats mean EMG activities as a percentage of maximal voluntary isometric contraction ( MVIC)P-values effect size (Cohenrsquos d Cohen 1988) and 95 confidence intervals between descending and ascending phases performed with1RM loads
Back squat Front squat
Descendingphase
(mean plusmns)
Ascendingphase
(mean plusmn s) P d
95 CI Descendingphase
(mean plusmn s)
Ascendingphase
(mean plusmn s) P d
95 CI
Muscle L U L U
Rectus femoris 379 plusmn 121 360 plusmn 138 0455 minus015 minus3562 minus7432 464 plusmn 244 467 plusmn 194 0922 001 minus7122 6500Vastus medialis 483 plusmn 143 493 plusmn 139 0617 007 minus5293 3286 531 plusmn 193 589 plusmn 171 033 032 minus11036 minus533Vastus lateralis 459 plusmn 139 485 plusmn 172 0223 017 minus7005 1821 480 plusmn 158 562 plusmn 222 068 043 minus17190 07269Erector spinae 411 plusmn 140 460 plusmn 176 0124 031 minus11286 1564 451 plusmn 120 481 plusmn 168 0451 020 minus11276 5367Gluteus maximus 288 plusmn 189 473 plusmn 277 0000 078 minus25810 minus11200 300 plusmn 230 466 plusmn 301 0000 062 minus22098 minus11188Biceps femoris 187 plusmn 149 349 plusmn 182 0000 097 minus19740 minus12600 197 plusmn 233 295 plusmn 287 0001 038 minus14864 minus4711Semitendinosus 150 plusmn 69 290 plusmn 162 0001 105 minus20720 minus7280 140 plusmn 81 184 plusmn 101 0036 048 minus8404 minus0343
Note Significantly higher EMG activities during the ascending phase compared to the descending phase (P lt 005)
1062 HU Yavuz et al
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015
95 confidence intervals between back squats andfront squats during the descending and ascendingphases performed with 1RM loads are shownin Table IV There were no significant differencesobserved between back and front squats duringthe descending phase During the ascending phasethe EMG activity of the vastus medialis was foundto be significantly higher in the front squat comparedto the back squat (P lt 005 d = 062 95 CIminus1500minus417) while the EMG activity of the semi-tendinosus was higher in the back squat compared tothe front squat (P lt 05 d = minus079 95 CI 622059)
As can be seen from Figure 3 significant differ-ences were observed between minimum hip anglesreached during back squats and front squats Theaverage minimum hip angle was significantly higher(P lt 005 d = 108 95 CI minus2857minus428) duringthe front squat compared to the back squat
Figure 4 shows the mean changes in knee and hipangles throughout the ascending phases of bothsquatting movements No difference was observed
in knee angles during the whole movement whilehip angles were lower in 8 of 10 phases during theback squat compared to front squat showing anobvious forward trunk lean According to theangle-specific EMG changes semitendinosus(P lt 005 d = minus023 95 CI minus2421111) showeda sudden increase in the sixth phase and bicepsfemoris (P lt 005 d = minus014 95 CI minus10931911) and gluteus maximus (P lt 005 d = minus03795 CI minus4533089) showed a similar but smallerincrease in the eighth phase during the back squatcompared to the front squat
Discussion
Participants could lift significantly greater loads withback squat compared to the front squat(1388 plusmn 326 of their body weight1059 plusmn 243 of their body weight respectively)(Figure 1) and this finding is consistent with theprevious studies (Gullett et al 2009 Russell ampPhillips 1989)
Instead of the load the level of effort in voluntarymuscle actions determines the degree of motor unitactivity (Carpinelli 2008) consequently the level ofEMG signalling increases Furthermore higherloads may increase intradiscal pressure (11) com-pression on vertebral bodies (10) tibiofemoral (1213) and patellofemoral joints (14) which could pos-sibly increase the risk of injury while performingsquat Gullett et al (2009) emphasised that the mus-cles tested were equally active during the front squatwhile lifting less mass and it seems that the extraload lifted during the back squat is what accounts forthe increased tibiofemoral compressive forces andextensor moments observed during these lifts It is
Table IV Mean EMG activities as a percentage of maximal voluntary isometric contraction ( MVIC) P-values effect size (Cohenrsquos dCohen 1988) and 95 confidence intervals between back squats and front squats during the descending and ascending phases performedwith 1RM loads
Descending phase Ascending phase
Back squat(mean plusmn s)
Front squat(mean plusmn s) P d
95 CIBack squat(mean plusmn s)
Front squat(mean plusmn s) P d
95 CI
Muscle L U L U
Rectus femoris 379 plusmn 121 464 plusmn 244 0200 044 minus22011 5164 360 plusmn 138 467 plusmn 194 0061 064 minus21917 0578Vastus medialis 483 plusmn 143 531 plusmn 193 0204 028 minus12627 3020 493 plusmn 139 589 plusmn 171 0002 062 minus15001 minus4177Vastus lateralis 459 plusmn 139 480 plusmn 158 0396 014 minus7088 3028 485 plusmn 172 562 plusmn 222 0096 039 minus16932 1590Erector spinae 411 plusmn 140 451 plusmn 120 0438 031 minus14953 6940 460 plusmn 176 481 plusmn 168 0665 012 minus12493 8292Gluteus maximus 288 plusmn 189 300 plusmn 230 0573 006 minus5460 3181 473 plusmn 277 466 plusmn 301 0841 minus002 minus7001 8447Biceps femoris 187 plusmn 149 197 plusmn 233 0765 005 minus7883 5959 349 plusmn 182 295 plusmn 287 0329 minus022 minus6257 17099Semitendinosus 150 plusmn 69 140 plusmn 81 0676 minus013 minus4052 6019 290 plusmn 162 184 plusmn 101 0039 minus079 0624 20595
Notes Significantly higher EMG activities during the front squat compared to the back squat (P lt 005) Significantly higher EMGactivities during the back squat compared to the front squat (P lt 005)
Figure 3 Minimum hip angles reached during the back squat (BS)and front squat (FS) Significant differences (P lt 005) betweenthe back and front squats
EMG Kinematic activities of back and front squat 1063
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015
very important because excessive tibiofemoral com-pressive forces could be deleterious to the menisciand articular cartilage (Escamilla 2000)
During the squat the primary muscles actingaround the knee are the quadriceps femoris (vastuslateralis vastus medialis vastus intermedius and rec-tus femoris) which carry out concentric knee exten-sion as well as eccentrically resisting knee flexionFor both back and front squats vastus medialis andvastus lateralis produced more activity than the rec-tus femoris during the whole manoeuvre which is inagreement with the data from Escamilla et al (19971998) Escamilla (2000) Escamilla et al (2000)Hwang Kim and Kim (2009) Wretneberg Feng
Lindberg and Arborelius (1993) Wretneberg et al(1996) and Isear et al (1997)
Schoenfeld (2010) reported that this may be logi-cal because the rectus femoris is both a hip flexorand knee extensor and thus shortens at one endwhile lengthening at the other during the squatwith little if any net change in length throughoutmovement
Although the loads were heavier during the backsquat mean EMG activities in selected musclesshowed no difference with only one exceptionDespite the lighter loads during the front squatvastus medialis mean EMG activity was greaterthan the back squat during the whole manoeuvresGullett et al (2009) and Stuart Meglan LutzGrowney and An (1996) reported no differences inmuscle activities between front and back squats Thedifference in our study can be resulted from thehigher loads compared to Gullett et al (2009)(70 of 1RM) and Stuart et al (1996) (50 pounds)which may recruit more motor units during themovements
When we divided the manoeuvres into ascendingand descending phases all muscles tested were moreactive during the ascending phase than during thedescending phase These findings are in accordancewith those of several other studies (Escamilla et al1998 Escamilla et al 2000 Gullett et al 2009McCaw amp Melrose 1999 Stuart et al 1996)EMG activities were higher during the ascendingphase compared to the descending phase for allmuscles during both the front and the back squatBut statistically significant differences were seen forgluteus maximus semitendinosus and bicepsfemoris during both the front and the back squatand for vastus medialis during the front squat
We observed no significant EMG activity differ-ences between the back and front squats during thedescending phases However during the ascendingphase EMG activity of the vastus medialis was higherin the front squat compared to the back squat whileEMG activity of the semitendinosus was higher inthe back squat compared to the front squat Thefront squat is believed to be a more isolated man-oeuvre for quadriceps (Grahammer 1986 Hatfield1983) and this result may support this idea Theheavier external resistance and more inclined torsoduring the back squat create a larger resistancemoment which requires greater muscular effort tocounterbalance (Swinton Aspe amp Keogh 2012) Itwas shown that increased forward trunk lean causesan increase in hamstring activity (Escamilla et al2000 Gullett et al 2009 Scotten 2010) Thismay explain the higher semitendinosus EMG activityduring the ascending phase of the back squats
When we divided the manoeuvres into 10 phasesfor being able to compare the movement patterns
Figure 4 Knee and hip angle-dependent EMG values of rectusfemoris (RF) vastus medialis (VM) vastus lateralis (VL) erectorspinae (ES) gluteus maximus (GM) biceps femoris (BF) andsemitendinosus (ST) throughout the phases of both backs squat(BS) and front squat (FS) movements Significant differences(P lt 005) between back and front squats
1064 HU Yavuz et al
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015
we did not observe any significant difference in kneeangles between the back and front squats Howeverwe observed significantly lower hip angles in 8 of 10phases during the back squat The lowest hip anglesreached during the manoeuvres were significantlylower in the back squat compared to the frontsquat These findings showed an increased forwardlean during the back squat compared to the frontsquat during maximum loading
When we check angle-specific EMG changes foreach muscle we saw that EMG activity patternswere quite parallel to each other for most of themuscles in both squat variants SemitendinosusEMG activity showed a sudden increase in thesixth phase which also shows the lowest hip angleand the starting of the ascending phase Gluteusmaximus and biceps femoris showed a similar butweaker change in pattern during the middle of theascending phase (eighth phase) This may probablybe due to the extra effort of the hip extensors tomaintain the balance by compensating the increasedforward lean during back squat
In both the squatting techniques as the perfor-mers lower throughout the eccentric phase they arerequired to lean forward in order to maintain bal-ance Centre of gravity moves further away from thelumbar spine increasing the moment arm and tor-que As a result the shear forces occurring withinthe lumbar spine would also increase (Comfort ampKasim 2007 Diggin et al 2011 Gullett et al2009) Increased forward lean reduces tolerance tocompressive load and results in a transfer of the loadfrom muscles to passive tissues heightening the riskof disc herniation (Matsumoto et al 2001)
As previously stated such an increase in shearforce under regular high loading conditions (eg1RM) may predispose an athlete to injury if theseforces continually exceed the strain capabilities ofthe joint connective tissues (Comfort amp Kasim2007) That is why it is beneficial to maintain aposture that is as close to upright as possible at alltimes for preventing the lumbar injuries (Schoenfeld2010)
Conclusion
We studied the musculature activity and kinematicsof knee and hip joints during front and back squatswith maximum loading (1RM) The front squat wasshown to be just as effective as the back squat undermaximum loading conditions in terms of overallmuscle activity with no difference in knee joint kine-matics and significantly less forward lean in hip jointwhich may probably show less lumbar injury riskWe also managed to show that the front squat cre-ated higher EMG activity in vastus medialis despitethe lighter loads compared to back squat that agrees
with the idea of ldquobeing a more isolated movementfor knee extensorsrdquo It is a known fact that the backsquat is used much more commonly compared to itsfront variation Results may suggest that the frontsquat may be a better choice for focusing on kneeextensor improvement andor for preventing lumbarinjuries under maximum loading conditions
References
American College of Sports Medicine (1998) Position standThe recommended quantity and quality of exercise for devel-oping and maintaining cardiorespiratory and muscular fitnessand flexibility in healthy adults Medicine and Science in Sportsand Exercise 975ndash991 doi101249MSS0b013e318213fefb
Baechle T R amp Earle R (2000) Essentials of strength trainingand conditioning (2nd ed) Champaign IL Human Kinetics
Balshaw T G amp Hunter A M (2012) Evaluation of electro-myography normalisation methods for the back squat Journalof Electromyography and Kinesiology 22 308ndash319
Braidot A A Brusa M H Lestussi F E amp Parera G P(2007) Biomechanics of front and back squat exercises Journalof Physics Conference Series 90 012009
Broer M R amp Houtz S J (1967) Patterns of muscular activity inselected sport skills (3rd ed) Springfield Charles C ThomasPublishing
Carpinelli R N (2008) The size principle and a critical analysisof the unsubstantiated heavier-is-better recommendation forresistance training Journal of Exercise Science and Fitness 667ndash86
Channell B T amp Barfield J P (2008) Effect of Olympic andtraditional resistance training on vertical jump improvement inhigh school boys Journal of Strength Conditioning and Research22 1522ndash1527
Clark D R Lambert M I amp Hunter A M (2012) Muscleactivation in the loaded free barbell squat A brief reviewJournal of Strength Conditioning and Research 26 1169ndash1178
Cohen J (1988) Statistical power analysis for the behavioral sciencesHillsdale NJ Lawrence Erlbaum
Comfort P amp Kasim P (2007) Optimizing squat techniqueStrength and Conditioning Journal 29 10ndash13
Delavier F (2001) Strength training anatomy Champaign ILHuman Kinetics
Diggin D OrsquoRegan C Whelan N Daly S McLoughlin VMcNamara L amp Reilly A (2011) A biomechanical ana-lysis of front vs back squat Injury implications PortugueseJournal of Sports Sciences 11(Suppl 2) Retrieved from httpwwwresearchgatenetpublication258363730_A_biomechanical_Analysis_of_front_and_back_squat_injury_implicationsfilee0b49528105693baa7pdf
Dionisio V C Almeida G L Duarte M amp Hirata R P(2008) Kinematic kinetic and EMG patterns during down-ward squatting Journal of Electromyography and Kinesiology 18134ndash143
Donnelly D V Berg W P amp Fiske D M (2006) The effectof the direction of gaze on the kinematics of the squat exerciseJournal of Strength Conditioning and Research 20 145ndash150Retrieved from httpwwwresearchgatenetpublication7273329_The_effect_of_the_direction_of_gaze_on_the_kinem-atics_of_the_squat_exerciselinks0c960523c48a69975c000000+ampcd=2amphl=trampct=clnk
Escamilla R F (2000) Knee biomechanics of the dynamic squatexercise Medicine amp Science in Sports amp Exercise 33 127ndash141
Escamilla R F Fleisig G S Lowry T M Barrentine S Wamp Andrews J R (2001) A three-dimensional biomechanicalanalysis of the squat during varying stance widths Medicine and
EMG Kinematic activities of back and front squat 1065
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015
Science in Sports and Exercise 33 984ndash998 Retrieved fromhttpwwwsweatpitcomforumstudiesSquattingA20three-dimensional20biomechanical20analysispdf
Escamilla R F Fleisig G S Zheng N Barrentine S WWilk K E amp Andrews J R (1998) Biomechanics of theknee during closed kinetic chain and open kinetic chain exer-cises Medicine and Science in Sports and Exercise 30 556ndash569doi10109700005768-199804000-00014
Escamilla R F Fleisig G S Zheng N Lander J EBarrentine S W Andrews J R Moorman C T(1997) The effects of technique variations on knee biomecha-nics during the squat and leg press Medicine and Science inSports and Exercise 29 156 doi10109700005768-200109000-00020
Escamilla R F Fleisig G S Zheng N Lander J EBarrentine S W Andrews J R hellip Moorman III C T(2000) Effects of technique variations on knee biomechanicsduring the squat and leg press Medicine amp Science in Sports ampExercise 33 1552ndash1566
Flanagan S Salem G J Wang M Y Sanker S ampGreendale G A (2003) Squatting exercises in older adultsKinematic and kinetic comparisons Medicine and Science inSports and Exercise 35 635ndash643 doi10124901MSS00000583644797306
Fleck S J (1999) Periodized strength training A critical reviewJournal of Strength Conditioning amp Research 13 82ndash89 Retrievedfrom httpjournalslwwcomnsca-jscrabstract199902000periodized_strength_training__a_critical_review15aspx
Grahammer J (1986) Sports illustrated strength training NewYork NY Harper amp Row
Gullett J C Tillman M D Gutierrez G M amp Chow J W(2009) A biomechanical comparison of back and front squatsin healthy trained individuals Journal of Strength andConditioning Research 23 284ndash292
Hasegawa I (2004) Using the overhead squat for core develop-ment NSCA Performance Training Journal 6 19ndash21
Hatfield F C (1983) Power A scientific approach Chicago ILContemporary Books Inc
Hay J G Andrews J G Vaughan C L amp Ueya K (1983)Load speed and equipment effects in strength-training exer-cises In H Matsui amp K Kobayashi (Eds) Biomechanics (3rded) Champaign IL Human Kinetics
Hwang S Kim Y amp Kim Y (2009) Lower extremity jointkinetics and lumbar curvature during squat and stoop liftingBMC Musculoskeletal Disorders 10 15 doi1011861471-2474-10-15
Isear J A Erickson Jr J C amp Worrel T W (1997) EMGanalysis of lower extremity muscle recruitment patterns duringan unloaded squat Medicine amp Science in Sports amp Exercise 29532ndash539
Kellis E Arambatzi F amp Papadopoulos C (2005) Effects ofload on ground reaction force and lower limb kinematics dur-ing concentric squats Journal of Sports Sciences 23 1045ndash1055
Konrad P (2005) ABC of EMG a practical introduction to kinesio-logical electromyography (1st ed) Scottsdale AZ Noraxon Inc
Kraemer W J amp Fry A C (1995) Strength testingDevelopment and evaluation of methodology In P Maud ampC Foster (Eds) Physiological assessment of human fitness(pp 115ndash138) Champaign IL Human Kinetics
Kraemer W J amp Ratamess N A (2004) Fundamentals ofresistance training Progression and exercise prescriptionMedicine amp Science in Sports amp Exercise 36 674ndash688
Matsumoto H Suda Y Otani T Niki Y Seedhom B B ampFujikawa K (2001) Roles of the anterior cruciate ligamentand the medial collateral ligament in preventing valgus instabil-ity Journal of Orthopaedic Science 6 28ndash32
McCaw S T amp Melrose D R (1999) Stance width and barload effects on leg muscle activity during the parallel squatMedicine and Science in Sports and Exercise 31 428ndash436
Merletti R (1999) Standards for reporting EMG data Journal ofElectromyography and Kinesiology 9 3ndash4 Retrieved from httpwwwisek onlineorgstandards_emghtml
Rippetoe M amp Kilgore L (2007) Starting strength Basic barbelltraining (2nd ed) Wichita Falls TX The Aasgaard Company
Russell P J amp Phillips S J (1989) A preliminary comparison offront and back squat exercises Research Quarterly for Exerciseand Sport 60 201ndash208
Schoenfeld B J (2010) Squatting kinematics and kinetics andtheir application to exercise performance Journal of Strengthand Conditioning Research 24 3497ndash3506
Scotten C M (2010) Differences in muscle activation in the lowerextremities while performing traditional squats and non-traditionalsquats (Master thesis) Boise State University Boise
Senter C amp Hame S L (2006) Biomechanical analysis of tibialtorque and knee flexion angle Implications for understandingknee injury Sports Medicine 36 635ndash641
Stensdotter A K Hodges P W Mellor R Sundelin G ampHager R C (2003) Quadriceps activation in closed and in openkinetic chain exercise Medicine and Science in Sports and Exercise35 2043ndash2047 doi10124901MSS000009910703704AE
Stuart M J Meglan D A Lutz G E Growney E S amp AnK N (1996) Comparison of intersegmental tibiofemoraljoint forces and muscle activity during various closed kineticchain exercises The American Journal of Sports Medicine 24792ndash799
Swinton P A Aspe R amp Keogh J (2012 July)Electromyographic comparison of The back squat and overheadsquat 30th Annual Conference of Biomechanics İn SportsMelbourne
Wretneberg P Feng Y amp Arborelius U P (1996) High- andlow-bar squatting techniques during weight-training Medicineand Science in Sports and Exercise 28 218ndash224
Wretneberg P Feng Y Lindberg F amp Arborelius U P(1993) Joint moments of force and quadriceps muscle activityduring squatting exercise Scandinavian Journal of Medicine ampScience in Sports 3 244ndash250
1066 HU Yavuz et al
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015
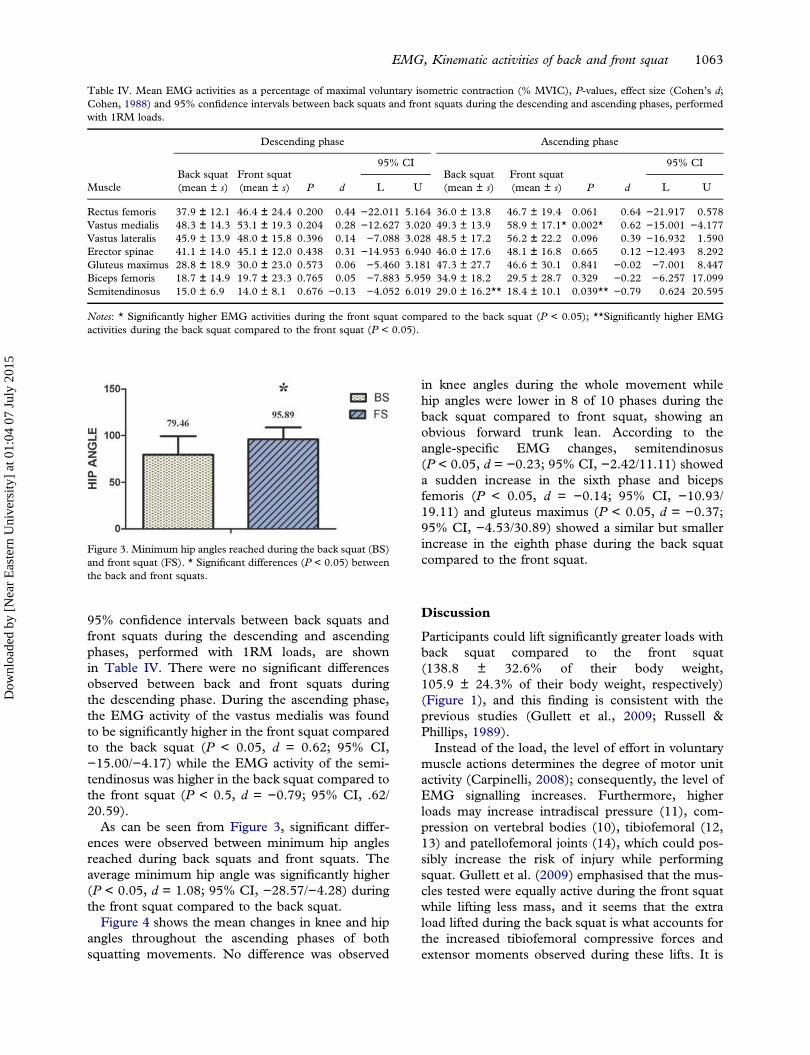
95 confidence intervals between back squats andfront squats during the descending and ascendingphases performed with 1RM loads are shownin Table IV There were no significant differencesobserved between back and front squats duringthe descending phase During the ascending phasethe EMG activity of the vastus medialis was foundto be significantly higher in the front squat comparedto the back squat (P lt 005 d = 062 95 CIminus1500minus417) while the EMG activity of the semi-tendinosus was higher in the back squat compared tothe front squat (P lt 05 d = minus079 95 CI 622059)
As can be seen from Figure 3 significant differ-ences were observed between minimum hip anglesreached during back squats and front squats Theaverage minimum hip angle was significantly higher(P lt 005 d = 108 95 CI minus2857minus428) duringthe front squat compared to the back squat
Figure 4 shows the mean changes in knee and hipangles throughout the ascending phases of bothsquatting movements No difference was observed
in knee angles during the whole movement whilehip angles were lower in 8 of 10 phases during theback squat compared to front squat showing anobvious forward trunk lean According to theangle-specific EMG changes semitendinosus(P lt 005 d = minus023 95 CI minus2421111) showeda sudden increase in the sixth phase and bicepsfemoris (P lt 005 d = minus014 95 CI minus10931911) and gluteus maximus (P lt 005 d = minus03795 CI minus4533089) showed a similar but smallerincrease in the eighth phase during the back squatcompared to the front squat
Discussion
Participants could lift significantly greater loads withback squat compared to the front squat(1388 plusmn 326 of their body weight1059 plusmn 243 of their body weight respectively)(Figure 1) and this finding is consistent with theprevious studies (Gullett et al 2009 Russell ampPhillips 1989)
Instead of the load the level of effort in voluntarymuscle actions determines the degree of motor unitactivity (Carpinelli 2008) consequently the level ofEMG signalling increases Furthermore higherloads may increase intradiscal pressure (11) com-pression on vertebral bodies (10) tibiofemoral (1213) and patellofemoral joints (14) which could pos-sibly increase the risk of injury while performingsquat Gullett et al (2009) emphasised that the mus-cles tested were equally active during the front squatwhile lifting less mass and it seems that the extraload lifted during the back squat is what accounts forthe increased tibiofemoral compressive forces andextensor moments observed during these lifts It is
Table IV Mean EMG activities as a percentage of maximal voluntary isometric contraction ( MVIC) P-values effect size (Cohenrsquos dCohen 1988) and 95 confidence intervals between back squats and front squats during the descending and ascending phases performedwith 1RM loads
Descending phase Ascending phase
Back squat(mean plusmn s)
Front squat(mean plusmn s) P d
95 CIBack squat(mean plusmn s)
Front squat(mean plusmn s) P d
95 CI
Muscle L U L U
Rectus femoris 379 plusmn 121 464 plusmn 244 0200 044 minus22011 5164 360 plusmn 138 467 plusmn 194 0061 064 minus21917 0578Vastus medialis 483 plusmn 143 531 plusmn 193 0204 028 minus12627 3020 493 plusmn 139 589 plusmn 171 0002 062 minus15001 minus4177Vastus lateralis 459 plusmn 139 480 plusmn 158 0396 014 minus7088 3028 485 plusmn 172 562 plusmn 222 0096 039 minus16932 1590Erector spinae 411 plusmn 140 451 plusmn 120 0438 031 minus14953 6940 460 plusmn 176 481 plusmn 168 0665 012 minus12493 8292Gluteus maximus 288 plusmn 189 300 plusmn 230 0573 006 minus5460 3181 473 plusmn 277 466 plusmn 301 0841 minus002 minus7001 8447Biceps femoris 187 plusmn 149 197 plusmn 233 0765 005 minus7883 5959 349 plusmn 182 295 plusmn 287 0329 minus022 minus6257 17099Semitendinosus 150 plusmn 69 140 plusmn 81 0676 minus013 minus4052 6019 290 plusmn 162 184 plusmn 101 0039 minus079 0624 20595
Notes Significantly higher EMG activities during the front squat compared to the back squat (P lt 005) Significantly higher EMGactivities during the back squat compared to the front squat (P lt 005)
Figure 3 Minimum hip angles reached during the back squat (BS)and front squat (FS) Significant differences (P lt 005) betweenthe back and front squats
EMG Kinematic activities of back and front squat 1063
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015
very important because excessive tibiofemoral com-pressive forces could be deleterious to the menisciand articular cartilage (Escamilla 2000)
During the squat the primary muscles actingaround the knee are the quadriceps femoris (vastuslateralis vastus medialis vastus intermedius and rec-tus femoris) which carry out concentric knee exten-sion as well as eccentrically resisting knee flexionFor both back and front squats vastus medialis andvastus lateralis produced more activity than the rec-tus femoris during the whole manoeuvre which is inagreement with the data from Escamilla et al (19971998) Escamilla (2000) Escamilla et al (2000)Hwang Kim and Kim (2009) Wretneberg Feng
Lindberg and Arborelius (1993) Wretneberg et al(1996) and Isear et al (1997)
Schoenfeld (2010) reported that this may be logi-cal because the rectus femoris is both a hip flexorand knee extensor and thus shortens at one endwhile lengthening at the other during the squatwith little if any net change in length throughoutmovement
Although the loads were heavier during the backsquat mean EMG activities in selected musclesshowed no difference with only one exceptionDespite the lighter loads during the front squatvastus medialis mean EMG activity was greaterthan the back squat during the whole manoeuvresGullett et al (2009) and Stuart Meglan LutzGrowney and An (1996) reported no differences inmuscle activities between front and back squats Thedifference in our study can be resulted from thehigher loads compared to Gullett et al (2009)(70 of 1RM) and Stuart et al (1996) (50 pounds)which may recruit more motor units during themovements
When we divided the manoeuvres into ascendingand descending phases all muscles tested were moreactive during the ascending phase than during thedescending phase These findings are in accordancewith those of several other studies (Escamilla et al1998 Escamilla et al 2000 Gullett et al 2009McCaw amp Melrose 1999 Stuart et al 1996)EMG activities were higher during the ascendingphase compared to the descending phase for allmuscles during both the front and the back squatBut statistically significant differences were seen forgluteus maximus semitendinosus and bicepsfemoris during both the front and the back squatand for vastus medialis during the front squat
We observed no significant EMG activity differ-ences between the back and front squats during thedescending phases However during the ascendingphase EMG activity of the vastus medialis was higherin the front squat compared to the back squat whileEMG activity of the semitendinosus was higher inthe back squat compared to the front squat Thefront squat is believed to be a more isolated man-oeuvre for quadriceps (Grahammer 1986 Hatfield1983) and this result may support this idea Theheavier external resistance and more inclined torsoduring the back squat create a larger resistancemoment which requires greater muscular effort tocounterbalance (Swinton Aspe amp Keogh 2012) Itwas shown that increased forward trunk lean causesan increase in hamstring activity (Escamilla et al2000 Gullett et al 2009 Scotten 2010) Thismay explain the higher semitendinosus EMG activityduring the ascending phase of the back squats
When we divided the manoeuvres into 10 phasesfor being able to compare the movement patterns
Figure 4 Knee and hip angle-dependent EMG values of rectusfemoris (RF) vastus medialis (VM) vastus lateralis (VL) erectorspinae (ES) gluteus maximus (GM) biceps femoris (BF) andsemitendinosus (ST) throughout the phases of both backs squat(BS) and front squat (FS) movements Significant differences(P lt 005) between back and front squats
1064 HU Yavuz et al
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015
we did not observe any significant difference in kneeangles between the back and front squats Howeverwe observed significantly lower hip angles in 8 of 10phases during the back squat The lowest hip anglesreached during the manoeuvres were significantlylower in the back squat compared to the frontsquat These findings showed an increased forwardlean during the back squat compared to the frontsquat during maximum loading
When we check angle-specific EMG changes foreach muscle we saw that EMG activity patternswere quite parallel to each other for most of themuscles in both squat variants SemitendinosusEMG activity showed a sudden increase in thesixth phase which also shows the lowest hip angleand the starting of the ascending phase Gluteusmaximus and biceps femoris showed a similar butweaker change in pattern during the middle of theascending phase (eighth phase) This may probablybe due to the extra effort of the hip extensors tomaintain the balance by compensating the increasedforward lean during back squat
In both the squatting techniques as the perfor-mers lower throughout the eccentric phase they arerequired to lean forward in order to maintain bal-ance Centre of gravity moves further away from thelumbar spine increasing the moment arm and tor-que As a result the shear forces occurring withinthe lumbar spine would also increase (Comfort ampKasim 2007 Diggin et al 2011 Gullett et al2009) Increased forward lean reduces tolerance tocompressive load and results in a transfer of the loadfrom muscles to passive tissues heightening the riskof disc herniation (Matsumoto et al 2001)
As previously stated such an increase in shearforce under regular high loading conditions (eg1RM) may predispose an athlete to injury if theseforces continually exceed the strain capabilities ofthe joint connective tissues (Comfort amp Kasim2007) That is why it is beneficial to maintain aposture that is as close to upright as possible at alltimes for preventing the lumbar injuries (Schoenfeld2010)
Conclusion
We studied the musculature activity and kinematicsof knee and hip joints during front and back squatswith maximum loading (1RM) The front squat wasshown to be just as effective as the back squat undermaximum loading conditions in terms of overallmuscle activity with no difference in knee joint kine-matics and significantly less forward lean in hip jointwhich may probably show less lumbar injury riskWe also managed to show that the front squat cre-ated higher EMG activity in vastus medialis despitethe lighter loads compared to back squat that agrees
with the idea of ldquobeing a more isolated movementfor knee extensorsrdquo It is a known fact that the backsquat is used much more commonly compared to itsfront variation Results may suggest that the frontsquat may be a better choice for focusing on kneeextensor improvement andor for preventing lumbarinjuries under maximum loading conditions
References
American College of Sports Medicine (1998) Position standThe recommended quantity and quality of exercise for devel-oping and maintaining cardiorespiratory and muscular fitnessand flexibility in healthy adults Medicine and Science in Sportsand Exercise 975ndash991 doi101249MSS0b013e318213fefb
Baechle T R amp Earle R (2000) Essentials of strength trainingand conditioning (2nd ed) Champaign IL Human Kinetics
Balshaw T G amp Hunter A M (2012) Evaluation of electro-myography normalisation methods for the back squat Journalof Electromyography and Kinesiology 22 308ndash319
Braidot A A Brusa M H Lestussi F E amp Parera G P(2007) Biomechanics of front and back squat exercises Journalof Physics Conference Series 90 012009
Broer M R amp Houtz S J (1967) Patterns of muscular activity inselected sport skills (3rd ed) Springfield Charles C ThomasPublishing
Carpinelli R N (2008) The size principle and a critical analysisof the unsubstantiated heavier-is-better recommendation forresistance training Journal of Exercise Science and Fitness 667ndash86
Channell B T amp Barfield J P (2008) Effect of Olympic andtraditional resistance training on vertical jump improvement inhigh school boys Journal of Strength Conditioning and Research22 1522ndash1527
Clark D R Lambert M I amp Hunter A M (2012) Muscleactivation in the loaded free barbell squat A brief reviewJournal of Strength Conditioning and Research 26 1169ndash1178
Cohen J (1988) Statistical power analysis for the behavioral sciencesHillsdale NJ Lawrence Erlbaum
Comfort P amp Kasim P (2007) Optimizing squat techniqueStrength and Conditioning Journal 29 10ndash13
Delavier F (2001) Strength training anatomy Champaign ILHuman Kinetics
Diggin D OrsquoRegan C Whelan N Daly S McLoughlin VMcNamara L amp Reilly A (2011) A biomechanical ana-lysis of front vs back squat Injury implications PortugueseJournal of Sports Sciences 11(Suppl 2) Retrieved from httpwwwresearchgatenetpublication258363730_A_biomechanical_Analysis_of_front_and_back_squat_injury_implicationsfilee0b49528105693baa7pdf
Dionisio V C Almeida G L Duarte M amp Hirata R P(2008) Kinematic kinetic and EMG patterns during down-ward squatting Journal of Electromyography and Kinesiology 18134ndash143
Donnelly D V Berg W P amp Fiske D M (2006) The effectof the direction of gaze on the kinematics of the squat exerciseJournal of Strength Conditioning and Research 20 145ndash150Retrieved from httpwwwresearchgatenetpublication7273329_The_effect_of_the_direction_of_gaze_on_the_kinem-atics_of_the_squat_exerciselinks0c960523c48a69975c000000+ampcd=2amphl=trampct=clnk
Escamilla R F (2000) Knee biomechanics of the dynamic squatexercise Medicine amp Science in Sports amp Exercise 33 127ndash141
Escamilla R F Fleisig G S Lowry T M Barrentine S Wamp Andrews J R (2001) A three-dimensional biomechanicalanalysis of the squat during varying stance widths Medicine and
EMG Kinematic activities of back and front squat 1065
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015
Science in Sports and Exercise 33 984ndash998 Retrieved fromhttpwwwsweatpitcomforumstudiesSquattingA20three-dimensional20biomechanical20analysispdf
Escamilla R F Fleisig G S Zheng N Barrentine S WWilk K E amp Andrews J R (1998) Biomechanics of theknee during closed kinetic chain and open kinetic chain exer-cises Medicine and Science in Sports and Exercise 30 556ndash569doi10109700005768-199804000-00014
Escamilla R F Fleisig G S Zheng N Lander J EBarrentine S W Andrews J R Moorman C T(1997) The effects of technique variations on knee biomecha-nics during the squat and leg press Medicine and Science inSports and Exercise 29 156 doi10109700005768-200109000-00020
Escamilla R F Fleisig G S Zheng N Lander J EBarrentine S W Andrews J R hellip Moorman III C T(2000) Effects of technique variations on knee biomechanicsduring the squat and leg press Medicine amp Science in Sports ampExercise 33 1552ndash1566
Flanagan S Salem G J Wang M Y Sanker S ampGreendale G A (2003) Squatting exercises in older adultsKinematic and kinetic comparisons Medicine and Science inSports and Exercise 35 635ndash643 doi10124901MSS00000583644797306
Fleck S J (1999) Periodized strength training A critical reviewJournal of Strength Conditioning amp Research 13 82ndash89 Retrievedfrom httpjournalslwwcomnsca-jscrabstract199902000periodized_strength_training__a_critical_review15aspx
Grahammer J (1986) Sports illustrated strength training NewYork NY Harper amp Row
Gullett J C Tillman M D Gutierrez G M amp Chow J W(2009) A biomechanical comparison of back and front squatsin healthy trained individuals Journal of Strength andConditioning Research 23 284ndash292
Hasegawa I (2004) Using the overhead squat for core develop-ment NSCA Performance Training Journal 6 19ndash21
Hatfield F C (1983) Power A scientific approach Chicago ILContemporary Books Inc
Hay J G Andrews J G Vaughan C L amp Ueya K (1983)Load speed and equipment effects in strength-training exer-cises In H Matsui amp K Kobayashi (Eds) Biomechanics (3rded) Champaign IL Human Kinetics
Hwang S Kim Y amp Kim Y (2009) Lower extremity jointkinetics and lumbar curvature during squat and stoop liftingBMC Musculoskeletal Disorders 10 15 doi1011861471-2474-10-15
Isear J A Erickson Jr J C amp Worrel T W (1997) EMGanalysis of lower extremity muscle recruitment patterns duringan unloaded squat Medicine amp Science in Sports amp Exercise 29532ndash539
Kellis E Arambatzi F amp Papadopoulos C (2005) Effects ofload on ground reaction force and lower limb kinematics dur-ing concentric squats Journal of Sports Sciences 23 1045ndash1055
Konrad P (2005) ABC of EMG a practical introduction to kinesio-logical electromyography (1st ed) Scottsdale AZ Noraxon Inc
Kraemer W J amp Fry A C (1995) Strength testingDevelopment and evaluation of methodology In P Maud ampC Foster (Eds) Physiological assessment of human fitness(pp 115ndash138) Champaign IL Human Kinetics
Kraemer W J amp Ratamess N A (2004) Fundamentals ofresistance training Progression and exercise prescriptionMedicine amp Science in Sports amp Exercise 36 674ndash688
Matsumoto H Suda Y Otani T Niki Y Seedhom B B ampFujikawa K (2001) Roles of the anterior cruciate ligamentand the medial collateral ligament in preventing valgus instabil-ity Journal of Orthopaedic Science 6 28ndash32
McCaw S T amp Melrose D R (1999) Stance width and barload effects on leg muscle activity during the parallel squatMedicine and Science in Sports and Exercise 31 428ndash436
Merletti R (1999) Standards for reporting EMG data Journal ofElectromyography and Kinesiology 9 3ndash4 Retrieved from httpwwwisek onlineorgstandards_emghtml
Rippetoe M amp Kilgore L (2007) Starting strength Basic barbelltraining (2nd ed) Wichita Falls TX The Aasgaard Company
Russell P J amp Phillips S J (1989) A preliminary comparison offront and back squat exercises Research Quarterly for Exerciseand Sport 60 201ndash208
Schoenfeld B J (2010) Squatting kinematics and kinetics andtheir application to exercise performance Journal of Strengthand Conditioning Research 24 3497ndash3506
Scotten C M (2010) Differences in muscle activation in the lowerextremities while performing traditional squats and non-traditionalsquats (Master thesis) Boise State University Boise
Senter C amp Hame S L (2006) Biomechanical analysis of tibialtorque and knee flexion angle Implications for understandingknee injury Sports Medicine 36 635ndash641
Stensdotter A K Hodges P W Mellor R Sundelin G ampHager R C (2003) Quadriceps activation in closed and in openkinetic chain exercise Medicine and Science in Sports and Exercise35 2043ndash2047 doi10124901MSS000009910703704AE
Stuart M J Meglan D A Lutz G E Growney E S amp AnK N (1996) Comparison of intersegmental tibiofemoraljoint forces and muscle activity during various closed kineticchain exercises The American Journal of Sports Medicine 24792ndash799
Swinton P A Aspe R amp Keogh J (2012 July)Electromyographic comparison of The back squat and overheadsquat 30th Annual Conference of Biomechanics İn SportsMelbourne
Wretneberg P Feng Y amp Arborelius U P (1996) High- andlow-bar squatting techniques during weight-training Medicineand Science in Sports and Exercise 28 218ndash224
Wretneberg P Feng Y Lindberg F amp Arborelius U P(1993) Joint moments of force and quadriceps muscle activityduring squatting exercise Scandinavian Journal of Medicine ampScience in Sports 3 244ndash250
1066 HU Yavuz et al
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015
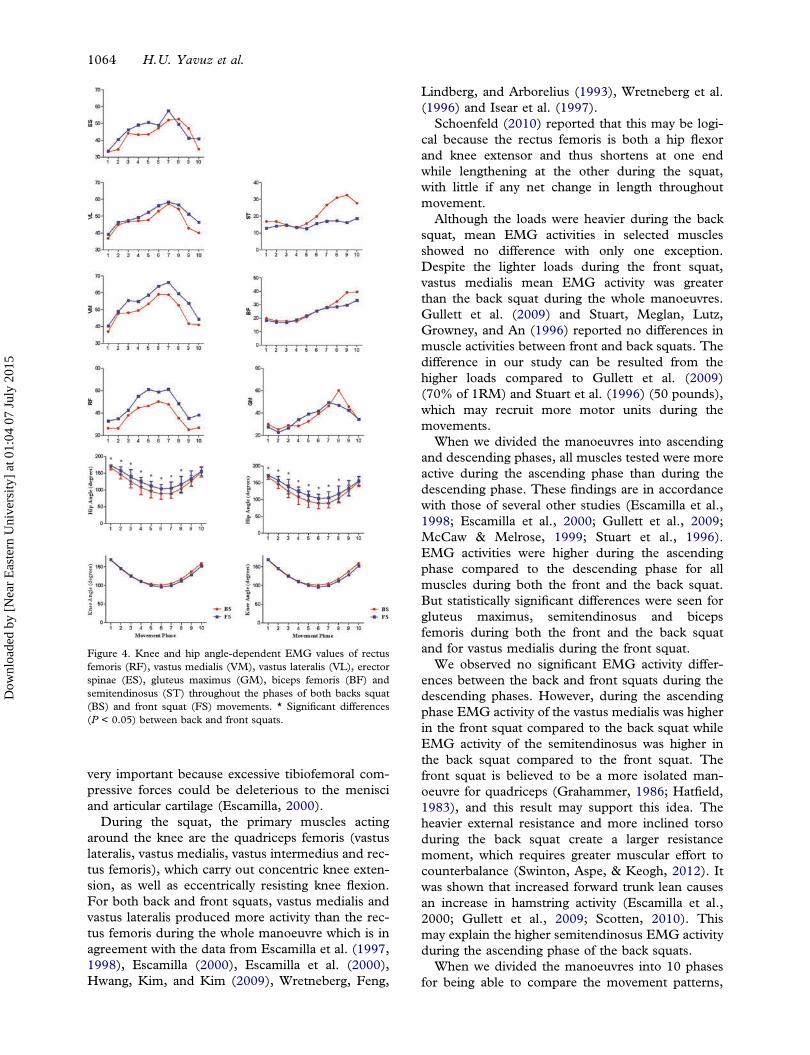
very important because excessive tibiofemoral com-pressive forces could be deleterious to the menisciand articular cartilage (Escamilla 2000)
During the squat the primary muscles actingaround the knee are the quadriceps femoris (vastuslateralis vastus medialis vastus intermedius and rec-tus femoris) which carry out concentric knee exten-sion as well as eccentrically resisting knee flexionFor both back and front squats vastus medialis andvastus lateralis produced more activity than the rec-tus femoris during the whole manoeuvre which is inagreement with the data from Escamilla et al (19971998) Escamilla (2000) Escamilla et al (2000)Hwang Kim and Kim (2009) Wretneberg Feng
Lindberg and Arborelius (1993) Wretneberg et al(1996) and Isear et al (1997)
Schoenfeld (2010) reported that this may be logi-cal because the rectus femoris is both a hip flexorand knee extensor and thus shortens at one endwhile lengthening at the other during the squatwith little if any net change in length throughoutmovement
Although the loads were heavier during the backsquat mean EMG activities in selected musclesshowed no difference with only one exceptionDespite the lighter loads during the front squatvastus medialis mean EMG activity was greaterthan the back squat during the whole manoeuvresGullett et al (2009) and Stuart Meglan LutzGrowney and An (1996) reported no differences inmuscle activities between front and back squats Thedifference in our study can be resulted from thehigher loads compared to Gullett et al (2009)(70 of 1RM) and Stuart et al (1996) (50 pounds)which may recruit more motor units during themovements
When we divided the manoeuvres into ascendingand descending phases all muscles tested were moreactive during the ascending phase than during thedescending phase These findings are in accordancewith those of several other studies (Escamilla et al1998 Escamilla et al 2000 Gullett et al 2009McCaw amp Melrose 1999 Stuart et al 1996)EMG activities were higher during the ascendingphase compared to the descending phase for allmuscles during both the front and the back squatBut statistically significant differences were seen forgluteus maximus semitendinosus and bicepsfemoris during both the front and the back squatand for vastus medialis during the front squat
We observed no significant EMG activity differ-ences between the back and front squats during thedescending phases However during the ascendingphase EMG activity of the vastus medialis was higherin the front squat compared to the back squat whileEMG activity of the semitendinosus was higher inthe back squat compared to the front squat Thefront squat is believed to be a more isolated man-oeuvre for quadriceps (Grahammer 1986 Hatfield1983) and this result may support this idea Theheavier external resistance and more inclined torsoduring the back squat create a larger resistancemoment which requires greater muscular effort tocounterbalance (Swinton Aspe amp Keogh 2012) Itwas shown that increased forward trunk lean causesan increase in hamstring activity (Escamilla et al2000 Gullett et al 2009 Scotten 2010) Thismay explain the higher semitendinosus EMG activityduring the ascending phase of the back squats
When we divided the manoeuvres into 10 phasesfor being able to compare the movement patterns
Figure 4 Knee and hip angle-dependent EMG values of rectusfemoris (RF) vastus medialis (VM) vastus lateralis (VL) erectorspinae (ES) gluteus maximus (GM) biceps femoris (BF) andsemitendinosus (ST) throughout the phases of both backs squat(BS) and front squat (FS) movements Significant differences(P lt 005) between back and front squats
1064 HU Yavuz et al
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015
we did not observe any significant difference in kneeangles between the back and front squats Howeverwe observed significantly lower hip angles in 8 of 10phases during the back squat The lowest hip anglesreached during the manoeuvres were significantlylower in the back squat compared to the frontsquat These findings showed an increased forwardlean during the back squat compared to the frontsquat during maximum loading
When we check angle-specific EMG changes foreach muscle we saw that EMG activity patternswere quite parallel to each other for most of themuscles in both squat variants SemitendinosusEMG activity showed a sudden increase in thesixth phase which also shows the lowest hip angleand the starting of the ascending phase Gluteusmaximus and biceps femoris showed a similar butweaker change in pattern during the middle of theascending phase (eighth phase) This may probablybe due to the extra effort of the hip extensors tomaintain the balance by compensating the increasedforward lean during back squat
In both the squatting techniques as the perfor-mers lower throughout the eccentric phase they arerequired to lean forward in order to maintain bal-ance Centre of gravity moves further away from thelumbar spine increasing the moment arm and tor-que As a result the shear forces occurring withinthe lumbar spine would also increase (Comfort ampKasim 2007 Diggin et al 2011 Gullett et al2009) Increased forward lean reduces tolerance tocompressive load and results in a transfer of the loadfrom muscles to passive tissues heightening the riskof disc herniation (Matsumoto et al 2001)
As previously stated such an increase in shearforce under regular high loading conditions (eg1RM) may predispose an athlete to injury if theseforces continually exceed the strain capabilities ofthe joint connective tissues (Comfort amp Kasim2007) That is why it is beneficial to maintain aposture that is as close to upright as possible at alltimes for preventing the lumbar injuries (Schoenfeld2010)
Conclusion
We studied the musculature activity and kinematicsof knee and hip joints during front and back squatswith maximum loading (1RM) The front squat wasshown to be just as effective as the back squat undermaximum loading conditions in terms of overallmuscle activity with no difference in knee joint kine-matics and significantly less forward lean in hip jointwhich may probably show less lumbar injury riskWe also managed to show that the front squat cre-ated higher EMG activity in vastus medialis despitethe lighter loads compared to back squat that agrees
with the idea of ldquobeing a more isolated movementfor knee extensorsrdquo It is a known fact that the backsquat is used much more commonly compared to itsfront variation Results may suggest that the frontsquat may be a better choice for focusing on kneeextensor improvement andor for preventing lumbarinjuries under maximum loading conditions
References
American College of Sports Medicine (1998) Position standThe recommended quantity and quality of exercise for devel-oping and maintaining cardiorespiratory and muscular fitnessand flexibility in healthy adults Medicine and Science in Sportsand Exercise 975ndash991 doi101249MSS0b013e318213fefb
Baechle T R amp Earle R (2000) Essentials of strength trainingand conditioning (2nd ed) Champaign IL Human Kinetics
Balshaw T G amp Hunter A M (2012) Evaluation of electro-myography normalisation methods for the back squat Journalof Electromyography and Kinesiology 22 308ndash319
Braidot A A Brusa M H Lestussi F E amp Parera G P(2007) Biomechanics of front and back squat exercises Journalof Physics Conference Series 90 012009
Broer M R amp Houtz S J (1967) Patterns of muscular activity inselected sport skills (3rd ed) Springfield Charles C ThomasPublishing
Carpinelli R N (2008) The size principle and a critical analysisof the unsubstantiated heavier-is-better recommendation forresistance training Journal of Exercise Science and Fitness 667ndash86
Channell B T amp Barfield J P (2008) Effect of Olympic andtraditional resistance training on vertical jump improvement inhigh school boys Journal of Strength Conditioning and Research22 1522ndash1527
Clark D R Lambert M I amp Hunter A M (2012) Muscleactivation in the loaded free barbell squat A brief reviewJournal of Strength Conditioning and Research 26 1169ndash1178
Cohen J (1988) Statistical power analysis for the behavioral sciencesHillsdale NJ Lawrence Erlbaum
Comfort P amp Kasim P (2007) Optimizing squat techniqueStrength and Conditioning Journal 29 10ndash13
Delavier F (2001) Strength training anatomy Champaign ILHuman Kinetics
Diggin D OrsquoRegan C Whelan N Daly S McLoughlin VMcNamara L amp Reilly A (2011) A biomechanical ana-lysis of front vs back squat Injury implications PortugueseJournal of Sports Sciences 11(Suppl 2) Retrieved from httpwwwresearchgatenetpublication258363730_A_biomechanical_Analysis_of_front_and_back_squat_injury_implicationsfilee0b49528105693baa7pdf
Dionisio V C Almeida G L Duarte M amp Hirata R P(2008) Kinematic kinetic and EMG patterns during down-ward squatting Journal of Electromyography and Kinesiology 18134ndash143
Donnelly D V Berg W P amp Fiske D M (2006) The effectof the direction of gaze on the kinematics of the squat exerciseJournal of Strength Conditioning and Research 20 145ndash150Retrieved from httpwwwresearchgatenetpublication7273329_The_effect_of_the_direction_of_gaze_on_the_kinem-atics_of_the_squat_exerciselinks0c960523c48a69975c000000+ampcd=2amphl=trampct=clnk
Escamilla R F (2000) Knee biomechanics of the dynamic squatexercise Medicine amp Science in Sports amp Exercise 33 127ndash141
Escamilla R F Fleisig G S Lowry T M Barrentine S Wamp Andrews J R (2001) A three-dimensional biomechanicalanalysis of the squat during varying stance widths Medicine and
EMG Kinematic activities of back and front squat 1065
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015
Science in Sports and Exercise 33 984ndash998 Retrieved fromhttpwwwsweatpitcomforumstudiesSquattingA20three-dimensional20biomechanical20analysispdf
Escamilla R F Fleisig G S Zheng N Barrentine S WWilk K E amp Andrews J R (1998) Biomechanics of theknee during closed kinetic chain and open kinetic chain exer-cises Medicine and Science in Sports and Exercise 30 556ndash569doi10109700005768-199804000-00014
Escamilla R F Fleisig G S Zheng N Lander J EBarrentine S W Andrews J R Moorman C T(1997) The effects of technique variations on knee biomecha-nics during the squat and leg press Medicine and Science inSports and Exercise 29 156 doi10109700005768-200109000-00020
Escamilla R F Fleisig G S Zheng N Lander J EBarrentine S W Andrews J R hellip Moorman III C T(2000) Effects of technique variations on knee biomechanicsduring the squat and leg press Medicine amp Science in Sports ampExercise 33 1552ndash1566
Flanagan S Salem G J Wang M Y Sanker S ampGreendale G A (2003) Squatting exercises in older adultsKinematic and kinetic comparisons Medicine and Science inSports and Exercise 35 635ndash643 doi10124901MSS00000583644797306
Fleck S J (1999) Periodized strength training A critical reviewJournal of Strength Conditioning amp Research 13 82ndash89 Retrievedfrom httpjournalslwwcomnsca-jscrabstract199902000periodized_strength_training__a_critical_review15aspx
Grahammer J (1986) Sports illustrated strength training NewYork NY Harper amp Row
Gullett J C Tillman M D Gutierrez G M amp Chow J W(2009) A biomechanical comparison of back and front squatsin healthy trained individuals Journal of Strength andConditioning Research 23 284ndash292
Hasegawa I (2004) Using the overhead squat for core develop-ment NSCA Performance Training Journal 6 19ndash21
Hatfield F C (1983) Power A scientific approach Chicago ILContemporary Books Inc
Hay J G Andrews J G Vaughan C L amp Ueya K (1983)Load speed and equipment effects in strength-training exer-cises In H Matsui amp K Kobayashi (Eds) Biomechanics (3rded) Champaign IL Human Kinetics
Hwang S Kim Y amp Kim Y (2009) Lower extremity jointkinetics and lumbar curvature during squat and stoop liftingBMC Musculoskeletal Disorders 10 15 doi1011861471-2474-10-15
Isear J A Erickson Jr J C amp Worrel T W (1997) EMGanalysis of lower extremity muscle recruitment patterns duringan unloaded squat Medicine amp Science in Sports amp Exercise 29532ndash539
Kellis E Arambatzi F amp Papadopoulos C (2005) Effects ofload on ground reaction force and lower limb kinematics dur-ing concentric squats Journal of Sports Sciences 23 1045ndash1055
Konrad P (2005) ABC of EMG a practical introduction to kinesio-logical electromyography (1st ed) Scottsdale AZ Noraxon Inc
Kraemer W J amp Fry A C (1995) Strength testingDevelopment and evaluation of methodology In P Maud ampC Foster (Eds) Physiological assessment of human fitness(pp 115ndash138) Champaign IL Human Kinetics
Kraemer W J amp Ratamess N A (2004) Fundamentals ofresistance training Progression and exercise prescriptionMedicine amp Science in Sports amp Exercise 36 674ndash688
Matsumoto H Suda Y Otani T Niki Y Seedhom B B ampFujikawa K (2001) Roles of the anterior cruciate ligamentand the medial collateral ligament in preventing valgus instabil-ity Journal of Orthopaedic Science 6 28ndash32
McCaw S T amp Melrose D R (1999) Stance width and barload effects on leg muscle activity during the parallel squatMedicine and Science in Sports and Exercise 31 428ndash436
Merletti R (1999) Standards for reporting EMG data Journal ofElectromyography and Kinesiology 9 3ndash4 Retrieved from httpwwwisek onlineorgstandards_emghtml
Rippetoe M amp Kilgore L (2007) Starting strength Basic barbelltraining (2nd ed) Wichita Falls TX The Aasgaard Company
Russell P J amp Phillips S J (1989) A preliminary comparison offront and back squat exercises Research Quarterly for Exerciseand Sport 60 201ndash208
Schoenfeld B J (2010) Squatting kinematics and kinetics andtheir application to exercise performance Journal of Strengthand Conditioning Research 24 3497ndash3506
Scotten C M (2010) Differences in muscle activation in the lowerextremities while performing traditional squats and non-traditionalsquats (Master thesis) Boise State University Boise
Senter C amp Hame S L (2006) Biomechanical analysis of tibialtorque and knee flexion angle Implications for understandingknee injury Sports Medicine 36 635ndash641
Stensdotter A K Hodges P W Mellor R Sundelin G ampHager R C (2003) Quadriceps activation in closed and in openkinetic chain exercise Medicine and Science in Sports and Exercise35 2043ndash2047 doi10124901MSS000009910703704AE
Stuart M J Meglan D A Lutz G E Growney E S amp AnK N (1996) Comparison of intersegmental tibiofemoraljoint forces and muscle activity during various closed kineticchain exercises The American Journal of Sports Medicine 24792ndash799
Swinton P A Aspe R amp Keogh J (2012 July)Electromyographic comparison of The back squat and overheadsquat 30th Annual Conference of Biomechanics İn SportsMelbourne
Wretneberg P Feng Y amp Arborelius U P (1996) High- andlow-bar squatting techniques during weight-training Medicineand Science in Sports and Exercise 28 218ndash224
Wretneberg P Feng Y Lindberg F amp Arborelius U P(1993) Joint moments of force and quadriceps muscle activityduring squatting exercise Scandinavian Journal of Medicine ampScience in Sports 3 244ndash250
1066 HU Yavuz et al
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015

we did not observe any significant difference in kneeangles between the back and front squats Howeverwe observed significantly lower hip angles in 8 of 10phases during the back squat The lowest hip anglesreached during the manoeuvres were significantlylower in the back squat compared to the frontsquat These findings showed an increased forwardlean during the back squat compared to the frontsquat during maximum loading
When we check angle-specific EMG changes foreach muscle we saw that EMG activity patternswere quite parallel to each other for most of themuscles in both squat variants SemitendinosusEMG activity showed a sudden increase in thesixth phase which also shows the lowest hip angleand the starting of the ascending phase Gluteusmaximus and biceps femoris showed a similar butweaker change in pattern during the middle of theascending phase (eighth phase) This may probablybe due to the extra effort of the hip extensors tomaintain the balance by compensating the increasedforward lean during back squat
In both the squatting techniques as the perfor-mers lower throughout the eccentric phase they arerequired to lean forward in order to maintain bal-ance Centre of gravity moves further away from thelumbar spine increasing the moment arm and tor-que As a result the shear forces occurring withinthe lumbar spine would also increase (Comfort ampKasim 2007 Diggin et al 2011 Gullett et al2009) Increased forward lean reduces tolerance tocompressive load and results in a transfer of the loadfrom muscles to passive tissues heightening the riskof disc herniation (Matsumoto et al 2001)
As previously stated such an increase in shearforce under regular high loading conditions (eg1RM) may predispose an athlete to injury if theseforces continually exceed the strain capabilities ofthe joint connective tissues (Comfort amp Kasim2007) That is why it is beneficial to maintain aposture that is as close to upright as possible at alltimes for preventing the lumbar injuries (Schoenfeld2010)
Conclusion
We studied the musculature activity and kinematicsof knee and hip joints during front and back squatswith maximum loading (1RM) The front squat wasshown to be just as effective as the back squat undermaximum loading conditions in terms of overallmuscle activity with no difference in knee joint kine-matics and significantly less forward lean in hip jointwhich may probably show less lumbar injury riskWe also managed to show that the front squat cre-ated higher EMG activity in vastus medialis despitethe lighter loads compared to back squat that agrees
with the idea of ldquobeing a more isolated movementfor knee extensorsrdquo It is a known fact that the backsquat is used much more commonly compared to itsfront variation Results may suggest that the frontsquat may be a better choice for focusing on kneeextensor improvement andor for preventing lumbarinjuries under maximum loading conditions
References
American College of Sports Medicine (1998) Position standThe recommended quantity and quality of exercise for devel-oping and maintaining cardiorespiratory and muscular fitnessand flexibility in healthy adults Medicine and Science in Sportsand Exercise 975ndash991 doi101249MSS0b013e318213fefb
Baechle T R amp Earle R (2000) Essentials of strength trainingand conditioning (2nd ed) Champaign IL Human Kinetics
Balshaw T G amp Hunter A M (2012) Evaluation of electro-myography normalisation methods for the back squat Journalof Electromyography and Kinesiology 22 308ndash319
Braidot A A Brusa M H Lestussi F E amp Parera G P(2007) Biomechanics of front and back squat exercises Journalof Physics Conference Series 90 012009
Broer M R amp Houtz S J (1967) Patterns of muscular activity inselected sport skills (3rd ed) Springfield Charles C ThomasPublishing
Carpinelli R N (2008) The size principle and a critical analysisof the unsubstantiated heavier-is-better recommendation forresistance training Journal of Exercise Science and Fitness 667ndash86
Channell B T amp Barfield J P (2008) Effect of Olympic andtraditional resistance training on vertical jump improvement inhigh school boys Journal of Strength Conditioning and Research22 1522ndash1527
Clark D R Lambert M I amp Hunter A M (2012) Muscleactivation in the loaded free barbell squat A brief reviewJournal of Strength Conditioning and Research 26 1169ndash1178
Cohen J (1988) Statistical power analysis for the behavioral sciencesHillsdale NJ Lawrence Erlbaum
Comfort P amp Kasim P (2007) Optimizing squat techniqueStrength and Conditioning Journal 29 10ndash13
Delavier F (2001) Strength training anatomy Champaign ILHuman Kinetics
Diggin D OrsquoRegan C Whelan N Daly S McLoughlin VMcNamara L amp Reilly A (2011) A biomechanical ana-lysis of front vs back squat Injury implications PortugueseJournal of Sports Sciences 11(Suppl 2) Retrieved from httpwwwresearchgatenetpublication258363730_A_biomechanical_Analysis_of_front_and_back_squat_injury_implicationsfilee0b49528105693baa7pdf
Dionisio V C Almeida G L Duarte M amp Hirata R P(2008) Kinematic kinetic and EMG patterns during down-ward squatting Journal of Electromyography and Kinesiology 18134ndash143
Donnelly D V Berg W P amp Fiske D M (2006) The effectof the direction of gaze on the kinematics of the squat exerciseJournal of Strength Conditioning and Research 20 145ndash150Retrieved from httpwwwresearchgatenetpublication7273329_The_effect_of_the_direction_of_gaze_on_the_kinem-atics_of_the_squat_exerciselinks0c960523c48a69975c000000+ampcd=2amphl=trampct=clnk
Escamilla R F (2000) Knee biomechanics of the dynamic squatexercise Medicine amp Science in Sports amp Exercise 33 127ndash141
Escamilla R F Fleisig G S Lowry T M Barrentine S Wamp Andrews J R (2001) A three-dimensional biomechanicalanalysis of the squat during varying stance widths Medicine and
EMG Kinematic activities of back and front squat 1065
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015
Science in Sports and Exercise 33 984ndash998 Retrieved fromhttpwwwsweatpitcomforumstudiesSquattingA20three-dimensional20biomechanical20analysispdf
Escamilla R F Fleisig G S Zheng N Barrentine S WWilk K E amp Andrews J R (1998) Biomechanics of theknee during closed kinetic chain and open kinetic chain exer-cises Medicine and Science in Sports and Exercise 30 556ndash569doi10109700005768-199804000-00014
Escamilla R F Fleisig G S Zheng N Lander J EBarrentine S W Andrews J R Moorman C T(1997) The effects of technique variations on knee biomecha-nics during the squat and leg press Medicine and Science inSports and Exercise 29 156 doi10109700005768-200109000-00020
Escamilla R F Fleisig G S Zheng N Lander J EBarrentine S W Andrews J R hellip Moorman III C T(2000) Effects of technique variations on knee biomechanicsduring the squat and leg press Medicine amp Science in Sports ampExercise 33 1552ndash1566
Flanagan S Salem G J Wang M Y Sanker S ampGreendale G A (2003) Squatting exercises in older adultsKinematic and kinetic comparisons Medicine and Science inSports and Exercise 35 635ndash643 doi10124901MSS00000583644797306
Fleck S J (1999) Periodized strength training A critical reviewJournal of Strength Conditioning amp Research 13 82ndash89 Retrievedfrom httpjournalslwwcomnsca-jscrabstract199902000periodized_strength_training__a_critical_review15aspx
Grahammer J (1986) Sports illustrated strength training NewYork NY Harper amp Row
Gullett J C Tillman M D Gutierrez G M amp Chow J W(2009) A biomechanical comparison of back and front squatsin healthy trained individuals Journal of Strength andConditioning Research 23 284ndash292
Hasegawa I (2004) Using the overhead squat for core develop-ment NSCA Performance Training Journal 6 19ndash21
Hatfield F C (1983) Power A scientific approach Chicago ILContemporary Books Inc
Hay J G Andrews J G Vaughan C L amp Ueya K (1983)Load speed and equipment effects in strength-training exer-cises In H Matsui amp K Kobayashi (Eds) Biomechanics (3rded) Champaign IL Human Kinetics
Hwang S Kim Y amp Kim Y (2009) Lower extremity jointkinetics and lumbar curvature during squat and stoop liftingBMC Musculoskeletal Disorders 10 15 doi1011861471-2474-10-15
Isear J A Erickson Jr J C amp Worrel T W (1997) EMGanalysis of lower extremity muscle recruitment patterns duringan unloaded squat Medicine amp Science in Sports amp Exercise 29532ndash539
Kellis E Arambatzi F amp Papadopoulos C (2005) Effects ofload on ground reaction force and lower limb kinematics dur-ing concentric squats Journal of Sports Sciences 23 1045ndash1055
Konrad P (2005) ABC of EMG a practical introduction to kinesio-logical electromyography (1st ed) Scottsdale AZ Noraxon Inc
Kraemer W J amp Fry A C (1995) Strength testingDevelopment and evaluation of methodology In P Maud ampC Foster (Eds) Physiological assessment of human fitness(pp 115ndash138) Champaign IL Human Kinetics
Kraemer W J amp Ratamess N A (2004) Fundamentals ofresistance training Progression and exercise prescriptionMedicine amp Science in Sports amp Exercise 36 674ndash688
Matsumoto H Suda Y Otani T Niki Y Seedhom B B ampFujikawa K (2001) Roles of the anterior cruciate ligamentand the medial collateral ligament in preventing valgus instabil-ity Journal of Orthopaedic Science 6 28ndash32
McCaw S T amp Melrose D R (1999) Stance width and barload effects on leg muscle activity during the parallel squatMedicine and Science in Sports and Exercise 31 428ndash436
Merletti R (1999) Standards for reporting EMG data Journal ofElectromyography and Kinesiology 9 3ndash4 Retrieved from httpwwwisek onlineorgstandards_emghtml
Rippetoe M amp Kilgore L (2007) Starting strength Basic barbelltraining (2nd ed) Wichita Falls TX The Aasgaard Company
Russell P J amp Phillips S J (1989) A preliminary comparison offront and back squat exercises Research Quarterly for Exerciseand Sport 60 201ndash208
Schoenfeld B J (2010) Squatting kinematics and kinetics andtheir application to exercise performance Journal of Strengthand Conditioning Research 24 3497ndash3506
Scotten C M (2010) Differences in muscle activation in the lowerextremities while performing traditional squats and non-traditionalsquats (Master thesis) Boise State University Boise
Senter C amp Hame S L (2006) Biomechanical analysis of tibialtorque and knee flexion angle Implications for understandingknee injury Sports Medicine 36 635ndash641
Stensdotter A K Hodges P W Mellor R Sundelin G ampHager R C (2003) Quadriceps activation in closed and in openkinetic chain exercise Medicine and Science in Sports and Exercise35 2043ndash2047 doi10124901MSS000009910703704AE
Stuart M J Meglan D A Lutz G E Growney E S amp AnK N (1996) Comparison of intersegmental tibiofemoraljoint forces and muscle activity during various closed kineticchain exercises The American Journal of Sports Medicine 24792ndash799
Swinton P A Aspe R amp Keogh J (2012 July)Electromyographic comparison of The back squat and overheadsquat 30th Annual Conference of Biomechanics İn SportsMelbourne
Wretneberg P Feng Y amp Arborelius U P (1996) High- andlow-bar squatting techniques during weight-training Medicineand Science in Sports and Exercise 28 218ndash224
Wretneberg P Feng Y Lindberg F amp Arborelius U P(1993) Joint moments of force and quadriceps muscle activityduring squatting exercise Scandinavian Journal of Medicine ampScience in Sports 3 244ndash250
1066 HU Yavuz et al
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015

Science in Sports and Exercise 33 984ndash998 Retrieved fromhttpwwwsweatpitcomforumstudiesSquattingA20three-dimensional20biomechanical20analysispdf
Escamilla R F Fleisig G S Zheng N Barrentine S WWilk K E amp Andrews J R (1998) Biomechanics of theknee during closed kinetic chain and open kinetic chain exer-cises Medicine and Science in Sports and Exercise 30 556ndash569doi10109700005768-199804000-00014
Escamilla R F Fleisig G S Zheng N Lander J EBarrentine S W Andrews J R Moorman C T(1997) The effects of technique variations on knee biomecha-nics during the squat and leg press Medicine and Science inSports and Exercise 29 156 doi10109700005768-200109000-00020
Escamilla R F Fleisig G S Zheng N Lander J EBarrentine S W Andrews J R hellip Moorman III C T(2000) Effects of technique variations on knee biomechanicsduring the squat and leg press Medicine amp Science in Sports ampExercise 33 1552ndash1566
Flanagan S Salem G J Wang M Y Sanker S ampGreendale G A (2003) Squatting exercises in older adultsKinematic and kinetic comparisons Medicine and Science inSports and Exercise 35 635ndash643 doi10124901MSS00000583644797306
Fleck S J (1999) Periodized strength training A critical reviewJournal of Strength Conditioning amp Research 13 82ndash89 Retrievedfrom httpjournalslwwcomnsca-jscrabstract199902000periodized_strength_training__a_critical_review15aspx
Grahammer J (1986) Sports illustrated strength training NewYork NY Harper amp Row
Gullett J C Tillman M D Gutierrez G M amp Chow J W(2009) A biomechanical comparison of back and front squatsin healthy trained individuals Journal of Strength andConditioning Research 23 284ndash292
Hasegawa I (2004) Using the overhead squat for core develop-ment NSCA Performance Training Journal 6 19ndash21
Hatfield F C (1983) Power A scientific approach Chicago ILContemporary Books Inc
Hay J G Andrews J G Vaughan C L amp Ueya K (1983)Load speed and equipment effects in strength-training exer-cises In H Matsui amp K Kobayashi (Eds) Biomechanics (3rded) Champaign IL Human Kinetics
Hwang S Kim Y amp Kim Y (2009) Lower extremity jointkinetics and lumbar curvature during squat and stoop liftingBMC Musculoskeletal Disorders 10 15 doi1011861471-2474-10-15
Isear J A Erickson Jr J C amp Worrel T W (1997) EMGanalysis of lower extremity muscle recruitment patterns duringan unloaded squat Medicine amp Science in Sports amp Exercise 29532ndash539
Kellis E Arambatzi F amp Papadopoulos C (2005) Effects ofload on ground reaction force and lower limb kinematics dur-ing concentric squats Journal of Sports Sciences 23 1045ndash1055
Konrad P (2005) ABC of EMG a practical introduction to kinesio-logical electromyography (1st ed) Scottsdale AZ Noraxon Inc
Kraemer W J amp Fry A C (1995) Strength testingDevelopment and evaluation of methodology In P Maud ampC Foster (Eds) Physiological assessment of human fitness(pp 115ndash138) Champaign IL Human Kinetics
Kraemer W J amp Ratamess N A (2004) Fundamentals ofresistance training Progression and exercise prescriptionMedicine amp Science in Sports amp Exercise 36 674ndash688
Matsumoto H Suda Y Otani T Niki Y Seedhom B B ampFujikawa K (2001) Roles of the anterior cruciate ligamentand the medial collateral ligament in preventing valgus instabil-ity Journal of Orthopaedic Science 6 28ndash32
McCaw S T amp Melrose D R (1999) Stance width and barload effects on leg muscle activity during the parallel squatMedicine and Science in Sports and Exercise 31 428ndash436
Merletti R (1999) Standards for reporting EMG data Journal ofElectromyography and Kinesiology 9 3ndash4 Retrieved from httpwwwisek onlineorgstandards_emghtml
Rippetoe M amp Kilgore L (2007) Starting strength Basic barbelltraining (2nd ed) Wichita Falls TX The Aasgaard Company
Russell P J amp Phillips S J (1989) A preliminary comparison offront and back squat exercises Research Quarterly for Exerciseand Sport 60 201ndash208
Schoenfeld B J (2010) Squatting kinematics and kinetics andtheir application to exercise performance Journal of Strengthand Conditioning Research 24 3497ndash3506
Scotten C M (2010) Differences in muscle activation in the lowerextremities while performing traditional squats and non-traditionalsquats (Master thesis) Boise State University Boise
Senter C amp Hame S L (2006) Biomechanical analysis of tibialtorque and knee flexion angle Implications for understandingknee injury Sports Medicine 36 635ndash641
Stensdotter A K Hodges P W Mellor R Sundelin G ampHager R C (2003) Quadriceps activation in closed and in openkinetic chain exercise Medicine and Science in Sports and Exercise35 2043ndash2047 doi10124901MSS000009910703704AE
Stuart M J Meglan D A Lutz G E Growney E S amp AnK N (1996) Comparison of intersegmental tibiofemoraljoint forces and muscle activity during various closed kineticchain exercises The American Journal of Sports Medicine 24792ndash799
Swinton P A Aspe R amp Keogh J (2012 July)Electromyographic comparison of The back squat and overheadsquat 30th Annual Conference of Biomechanics İn SportsMelbourne
Wretneberg P Feng Y amp Arborelius U P (1996) High- andlow-bar squatting techniques during weight-training Medicineand Science in Sports and Exercise 28 218ndash224
Wretneberg P Feng Y Lindberg F amp Arborelius U P(1993) Joint moments of force and quadriceps muscle activityduring squatting exercise Scandinavian Journal of Medicine ampScience in Sports 3 244ndash250
1066 HU Yavuz et al
Dow
nloa
ded
by [
Nea
r E
aste
rn U
nive
rsity
] at
01
04 0
7 Ju
ly 2
015
Related Documents











