In order to simplify the enrollment process, the following items are required at the me of your registraon appointment: Your child’s original birth cerficate. The birth cerficate number will be recorded on your child’s school record. Your child must be five years of age prior to September 1, 2012. Your child’s immunizaon record. This will show up-to-date immunizaons, which are required by the Commonwealth of Penn- sylvania Secretary of Health to enter kindergarten. A record of these immunizaons must be kept on file in the school district, so please come prepared with this informaon. Your child will not be admied to school unless a current immunizaon record is on file with the school nurse. If you have your completed physical form, please bring it along at this me. If not, please return the physical form to your child’s school when it is completed. Proof of Residency (examples: driver’s license, lease agreement, home sales agreement, copy of ulity bill, etc.) Any child custody documentaon, if applicable Addionally, children should NOT aend this appointment. Later in the spring, you and your child will have an opportunity to meet some of the kindergarten teachers, tour a kindergarten classroom, and learn about the kindergarten curriculum. Those dates for each individual school will be announced at a later date. Kindergarten Registration 2012-2013 Academic Year Spring Grove Area School District Educaonal Service Center 100 East College Avenue Spring Grove, PA 17362 717.225.4731 www.sgasd.org

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
In order to simplify the enrollment process, the following items are required at the time of your registration appointment:
Your child’s original birth certificate. The birth certificate number will be recorded on your child’s school record. Your child must be five years of age prior to September 1, 2012.
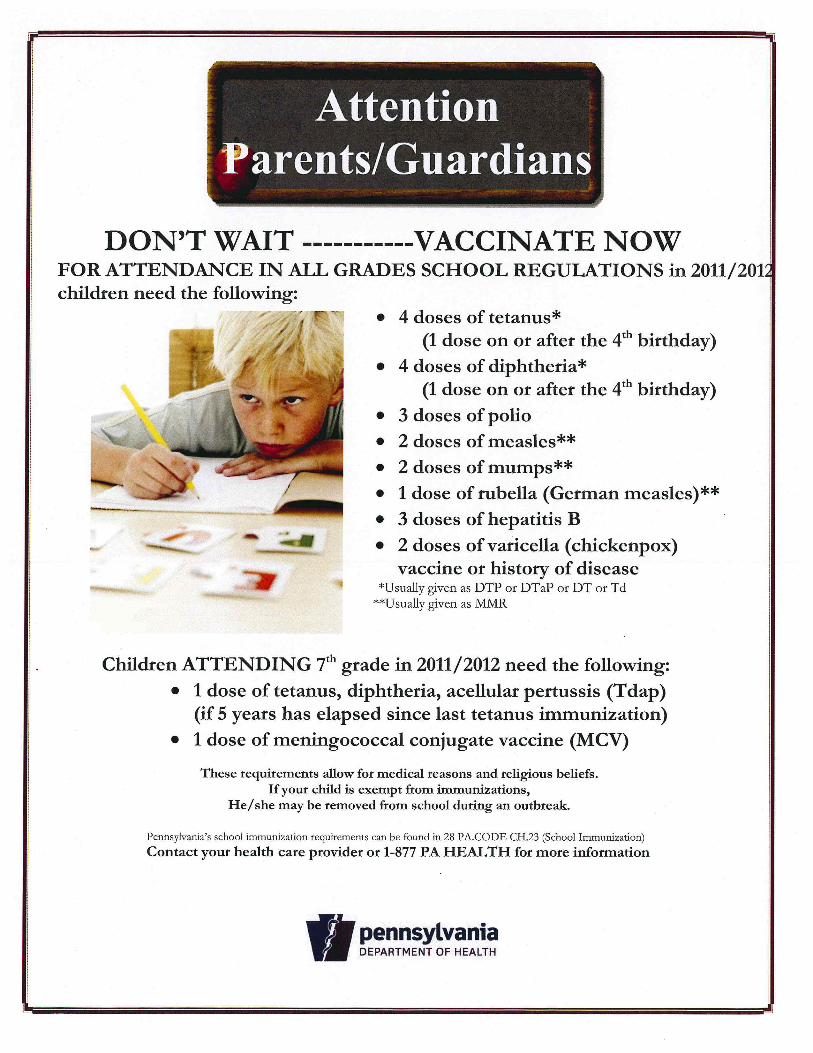
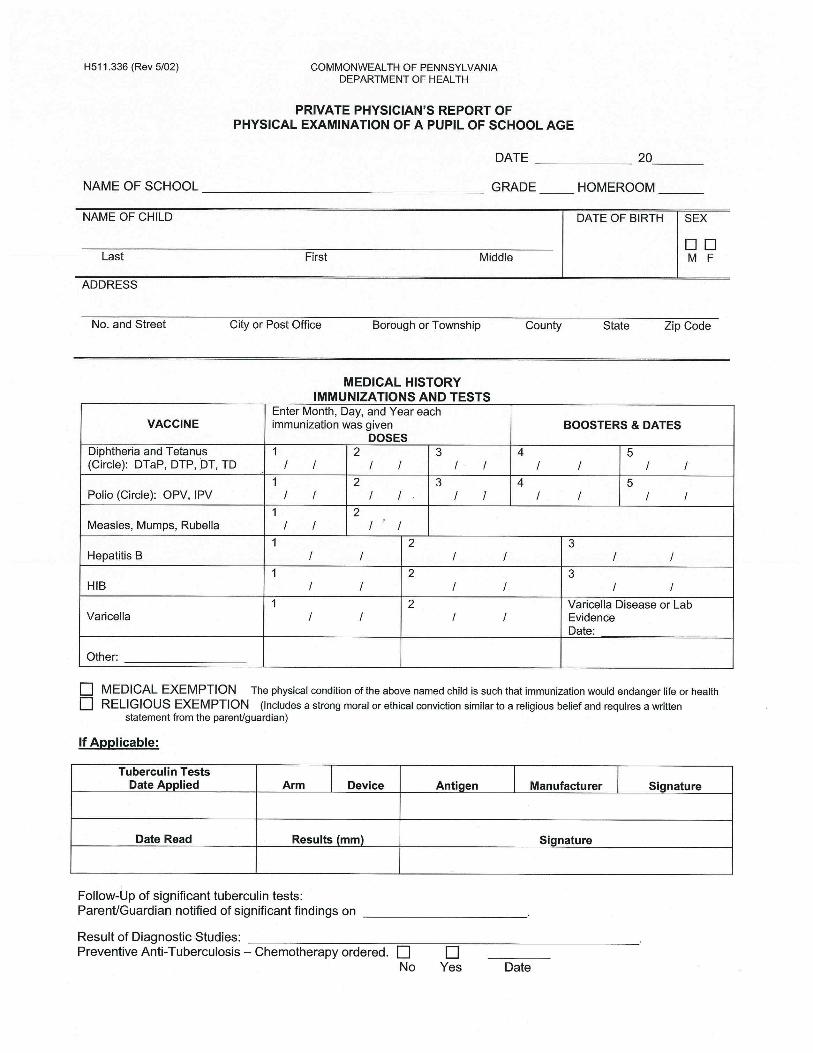
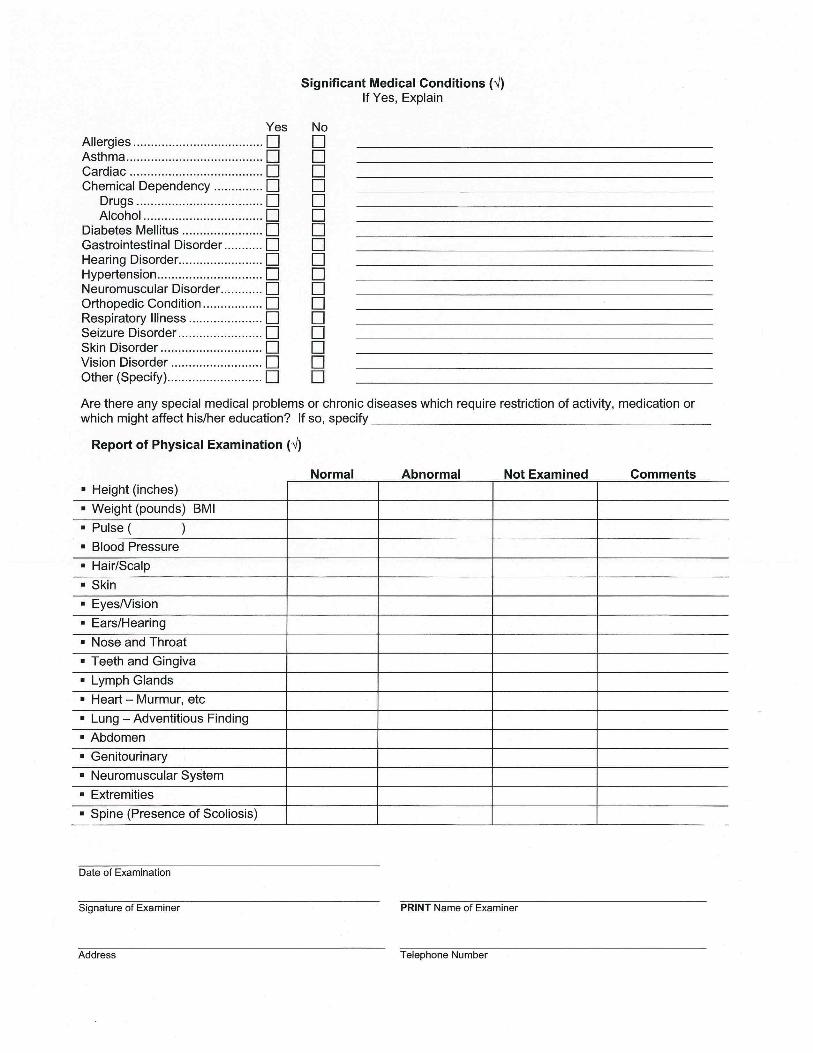
Your child’s immunization record. This will show up-to-date immunizations, which are required by the Commonwealth of Penn-sylvania Secretary of Health to enter kindergarten. A record of these immunizations must be kept on file in the school district, so please come prepared with this information. Your child will not be admitted to school unless a current immunization record is on file with the school nurse. If you have your completed physical form, please bring it along at this time. If not, please return the physical form to your child’s school when it is completed.
Proof of Residency (examples: driver’s license, lease agreement, home sales agreement, copy of utility bill, etc.)
Any child custody documentation, if applicable
Additionally, children should NOT attend this appointment. Later in the spring, you and your child will have an opportunity to meet some of the kindergarten teachers, tour a kindergarten classroom, and learn about the kindergarten curriculum. Those dates for each individual school will be announced at a later date.
Kindergarten Registration
2012-2013 Academic Year
Spring Grove Area School District
Educational Service Center
100 East College Avenue
Spring Grove, PA 17362
717.225.4731 www.sgasd.org
STUDENT MASTER
GRADE: KINDERGARTEN PRE-REGISTRATION
Parent Signature:
STUDENT # SCHOOL: H/R:
STUDENT NAME: SEX:
First, Middle, Last
PARENT/GUARDIAN NAME:
COMPLETE INFORMATION BELOW - - ONLY IF CHANGED FROM A PREVIOUS COMPLETED REGISTRATION
ADDRESS: STREET/ROAD:_____________________________________________P.O. Box #:__________
CITY:____________________________________________________ STATE:______ ZIP:______________
TOWNSHIP OR MUNICIPALITY OF RESIDENCE:_____________________________________________
HOME TELEPHONE:__________________ UNLISTED:______ (X) CHILD’S BIRTHDATE:___________
BIRTH CITY: _________________ DATE FIRST ENTERED SCHOOL IN PENNSYLVANIA: __________
INITIAL UNITED STATES ENTRY DATE: ___________________
Circle all that apply: 1 = American Indian/Alaska Native; 3 = Black/African American; 4 = Hispanic/Latino; 5 = White; 9 = Asian; 10 = Native Hawaiian/Other Pacific Islander
EMERGENCY CONTACT NAME & PHONE:_________________________________________________
MOTHER’S NAME: EMPLOYER:
ADDRESS: EMPLOYER’S ADDRESS:
FATHER’S NAME: EMPLOYER:
ADDRESS: EMPLOYER’S ADDRESS:
GUARDIAN: EMPLOYER:
ADDRESS: EMPLOYER’S ADDRESS:
Please give a physical description of your house / dwelling:
Mileage from your home to nearest intersection:_____ Name of nearest intersection/crossroad:___________
BABYSITTER’S NAME, ADDRESS & PHONE:_______________________________________________
Please give a brief description of the babysitter’s home:
Mileage from home to nearest intersection:_______ Name of nearest intersection/crossroad:_____________
FOR OFFICE USE ONLY Administrator’s Signature___________________________
Date: ___________________________
Entry Code: _____________________
Re-Entry Code: __________________
Withdrawal Code: ________________
Bus #: __________________________
ATT-1
Register Date _____________________ Initials _____________
ss\AP200\Attachment ATT-1 (December /2010)
f:\Forms\Registration\Student Registration - rev. January, 2011
SPRING GROVE AREA SCHOOL DISTRICT Spring Grove, Pennsylvania 17362
Student Registration
This Registration Form is to be completed for the current school year by the parent/guardian of the new/transferring student. This information is intended to facilitate initial instructional placement prior to the receipt of official school records. Student Name _____________________________________________________ Grade _________ Date of Birth ______________ Starting Date ___________ Phone # ____________________ E-mail Address _________________________________________ Present Address ______________________________________________________________________________________________ Former Address ______________________________________________________________________________________________ Last School Attended _________________________________________________________________________________________ Previous School Address ______________________________________________________________________________________ PARENT MUST COMPLETE THE FOLLOWING: 1. Is the student in compliance with Pennsylvania immunization requirements? _________ Yes _________ No
Out of state students must submit immunization records prior to enrollment.
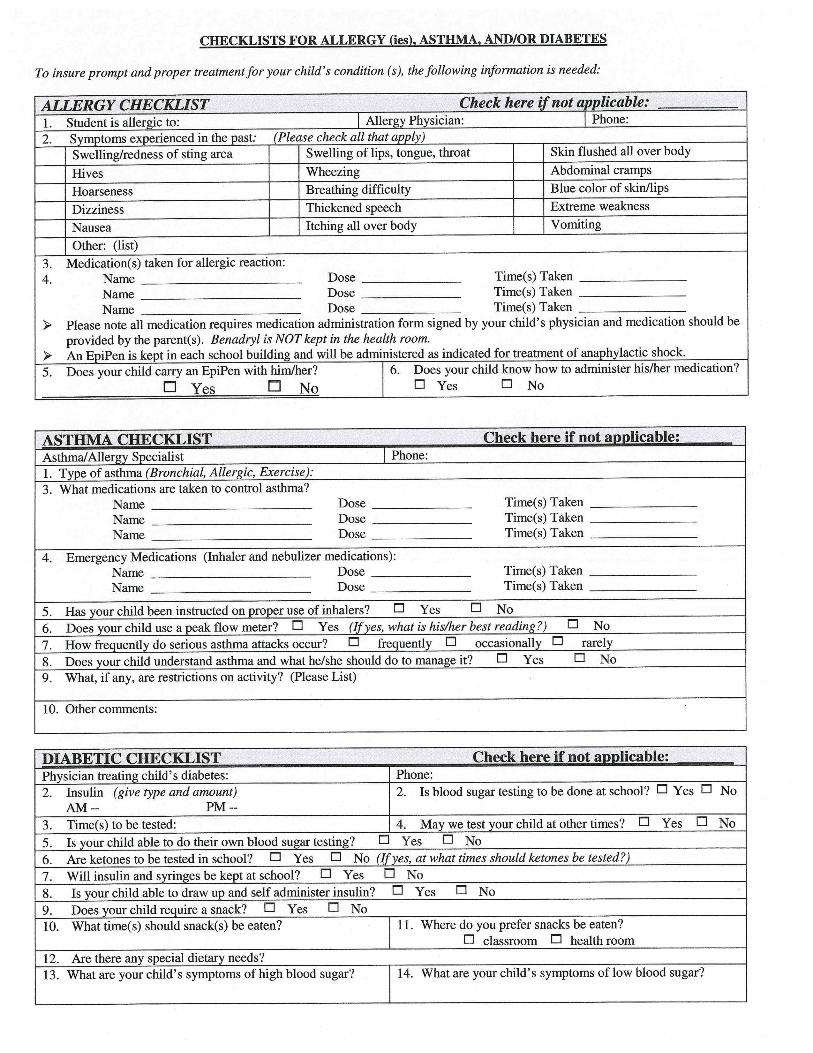
2. Does the student have any special health considerations? __________ Yes __________ No Please note allergies/health considerations _________________________________________________________________
3. Has the student been previously enrolled in the Spring Grove Area School District? _________ Yes _________ No
If YES, please list grades attended ________________________ 4. Is the student receiving special education services? __________ Yes _________ No
If YES, please indicate the exceptionality and sign the SE-602 form, which is the release of information statement.
____ Learning Support ____ Emotional Support ____ Hearing Impaired Support ____ Visually Impaired Support ____ Gifted/Talented Support ____ Speech / Language Support
5. Does your child receive: ____ ESL ____ Special Reading ____ Occupational Therapy ____ Physical Therapy 6. Is the student receiving free/reduced lunches? __________ Yes __________ No 7. Has the student been expelled from public school for violation of Act 26 (possession of weapons)? ______ Yes ______ No 8. Does the student live with his/her natural parent(s)? __________ Yes __________ No
If NO, with whom does the student reside (i.e., relationship to student)? __________________________________________ (NOTE: If the student resides with a guardian, a notarized 1302 statement may be a requirement prior to enrollment.)
9. Is there a custody agreement in place? ___________ Yes ___________ No
10. Did your child attend pre-school? (for kindergarten registrants only) ___________Yes ___________No
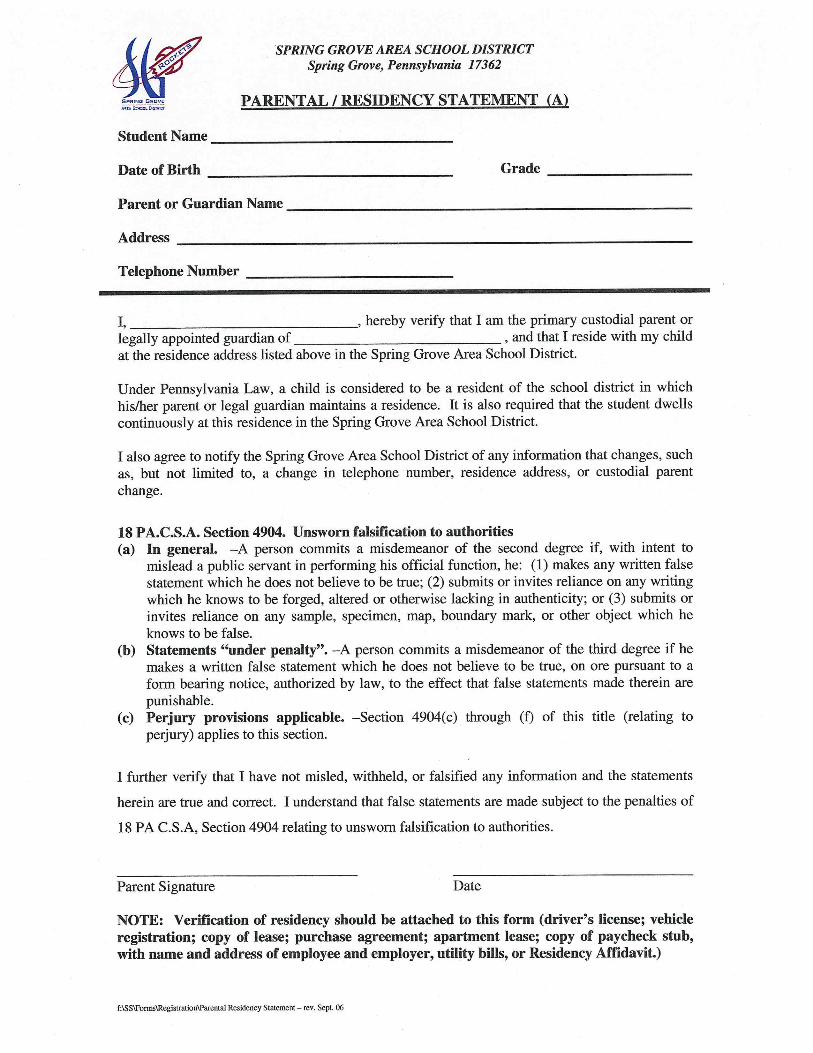
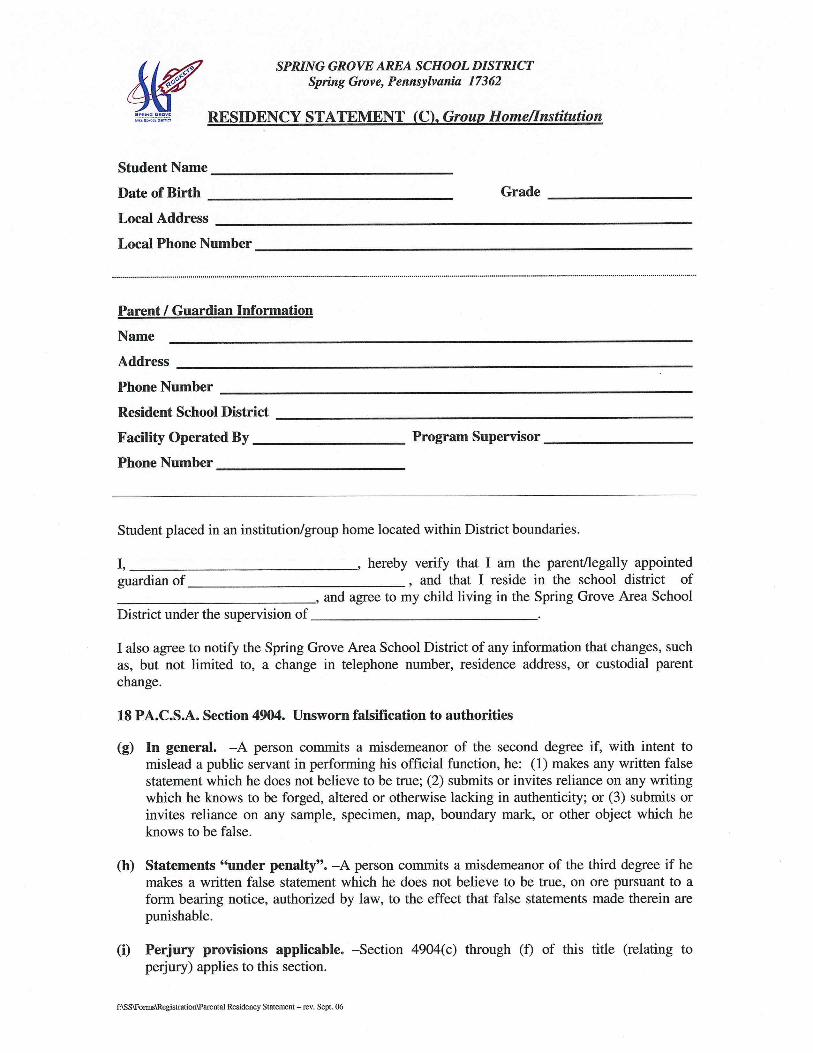
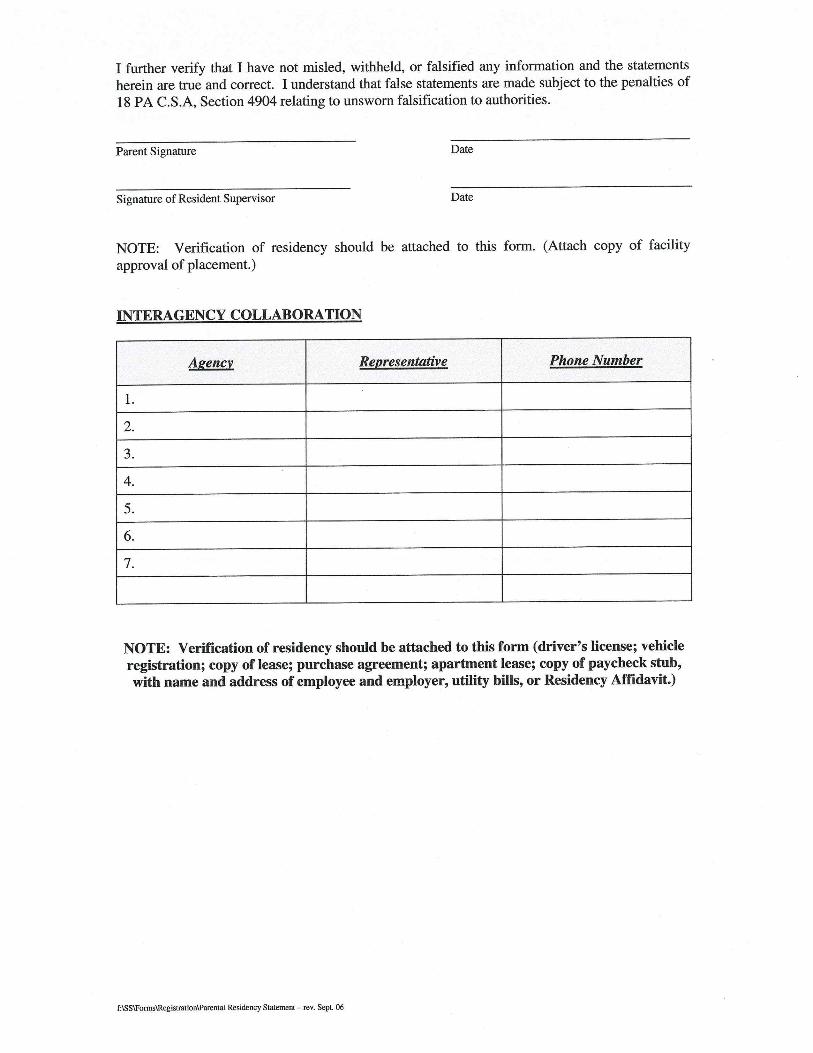
I verify that I am a resident of Spring Grove Area School District and have legal custody or guardianship of the student listed above. ___________________________________________________ ___________________________________________ (Parent/Guardian Signature) (Date)
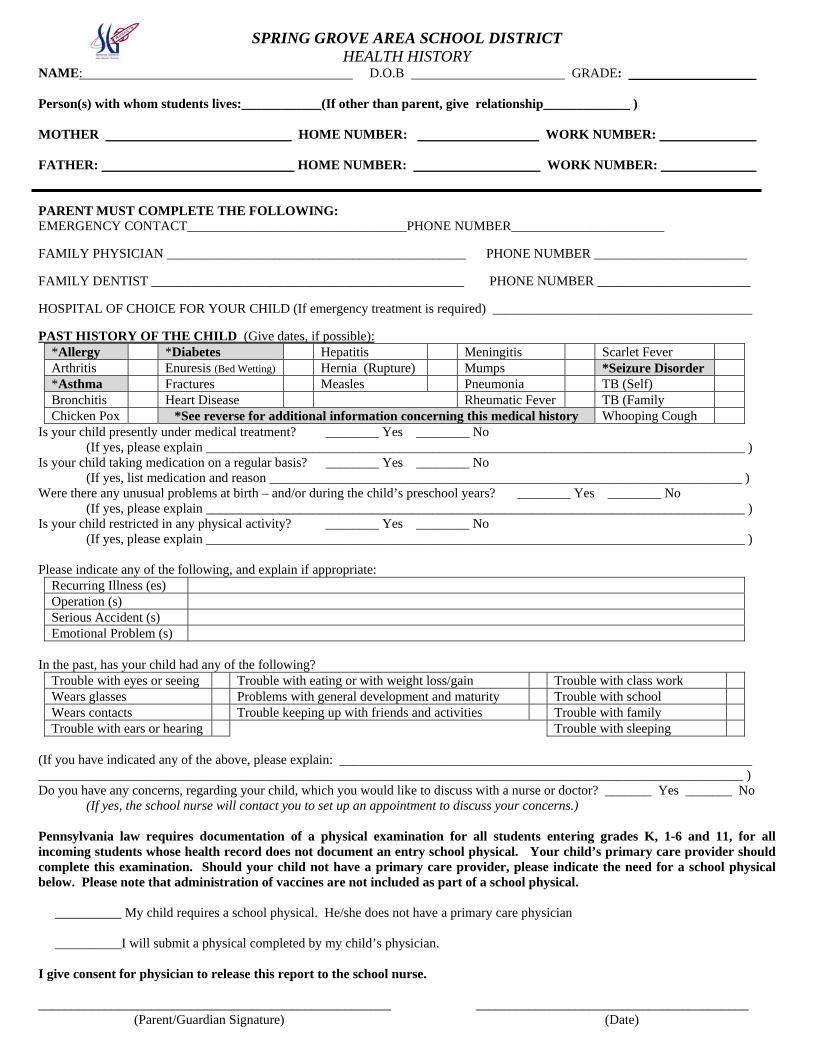
SPRING GROVE AREA SCHOOL DISTRICT HEALTH HISTORY
NAME: D.O.B GRADE: Person(s) with whom students lives:____________(If other than parent, give relationship_____________ ) MOTHER HOME NUMBER: WORK NUMBER: FATHER: HOME NUMBER: WORK NUMBER: PARENT MUST COMPLETE THE FOLLOWING: EMERGENCY CONTACT_________________________________PHONE NUMBER_______________________
FAMILY PHYSICIAN _____________________________________________ PHONE NUMBER _______________________
FAMILY DENTIST _______________________________________________ PHONE NUMBER _______________________
HOSPITAL OF CHOICE FOR YOUR CHILD (If emergency treatment is required) _______________________________________
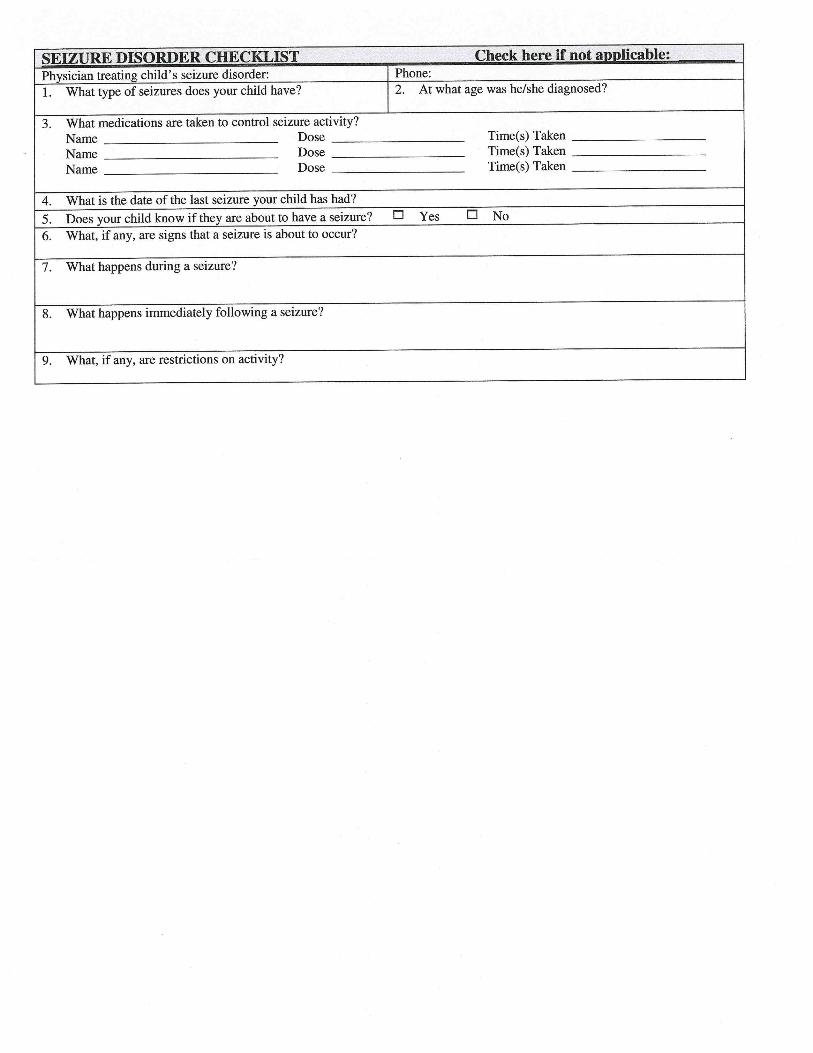
PAST HISTORY OF THE CHILD (Give dates, if possible): *Allergy *Diabetes Hepatitis Meningitis Scarlet Fever Arthritis Enuresis (Bed Wetting) Hernia (Rupture) Mumps *Seizure Disorder *Asthma Fractures Measles Pneumonia TB (Self) Bronchitis Heart Disease Rheumatic Fever TB (Family Chicken Pox *See reverse for additional information concerning this medical history Whooping Cough
Is your child presently under medical treatment? ________ Yes ________ No (If yes, please explain _________________________________________________________________________________ )
Is your child taking medication on a regular basis? ________ Yes ________ No (If yes, list medication and reason _______________________________________________________________________ )
Were there any unusual problems at birth – and/or during the child’s preschool years? ________ Yes ________ No (If yes, please explain _________________________________________________________________________________ )
Is your child restricted in any physical activity? ________ Yes ________ No (If yes, please explain _________________________________________________________________________________ )
Please indicate any of the following, and explain if appropriate:
Recurring Illness (es) Operation (s) Serious Accident (s) Emotional Problem (s)
In the past, has your child had any of the following?
Trouble with eyes or seeing Trouble with eating or with weight loss/gain Trouble with class work Wears glasses Problems with general development and maturity Trouble with school Wears contacts Trouble keeping up with friends and activities Trouble with family Trouble with ears or hearing Trouble with sleeping
(If you have indicated any of the above, please explain: ______________________________________________________________ __________________________________________________________________________________________________________ ) Do you have any concerns, regarding your child, which you would like to discuss with a nurse or doctor? _______ Yes _______ No (If yes, the school nurse will contact you to set up an appointment to discuss your concerns.) Pennsylvania law requires documentation of a physical examination for all students entering grades K, 1-6 and 11, for all incoming students whose health record does not document an entry school physical. Your child’s primary care provider should complete this examination. Should your child not have a primary care provider, please indicate the need for a school physical below. Please note that administration of vaccines are not included as part of a school physical. __________ My child requires a school physical. He/she does not have a primary care physician __________I will submit a physical completed by my child’s physician. I give consent for physician to release this report to the school nurse. _____________________________________________________ _________________________________________
(Parent/Guardian Signature) (Date)

Related Documents











