HEALTH SOCIOLOGY REVIEW Volume 15, Issue 2, June 2006 156 Copyright © eContent Management Pty Ltd. Health Sociology Review (2006) 15: 156–168 ABSTRACT KEY WORDS Visibilising clinical work: Video ethnography in the contemporary hospital Received 16 March 2005 Accepted 30 March 2006 This paper discusses the role of video-based research methods in social research. The paper situates these methods in the context of rising levels of visibility of professionals in government-funded organisations. The paper argues that while visual research may appear to play an ambiguous role in these organisations, it can also enable practitioners to confront the encroaching demands of post- bureaucratic work. To ground its argument, the paper presents an account of a video-ethnographic project currently underway in a local metropolitan hospital. This project focuses on negotiating understandings about existing care practices among a team of multi-disciplinary clinicians. Visual data gathered as part of that project are presented to specify issues which have thus far arisen during the project. Against this empirical background, the paper turns to considering the ambiguous potential of video-based research. The argument developed here is that, besides potentially exacerbating the pressure already imposed on clinicians - thanks to audit, surveillance and risk minimisation - video-based research may provide staff with new resources and opportunities for shaping their increasingly public and visible work practices. Rick Iedema, Debbi Long and Rowena Forsyth Faculty of Medicine University of New South Wales Australia Video ethnography; post- bureaucracy; spinal care; reflexivity; health care; sociology Bonne Bonsan Lee Prince of Wales Hospital Australia Introduction D ecades ago, Strauss and colleagues noted that ‘no one knows what the hospital “is” on any given day unless he [sic] has a comprehensive grasp of what combination of rules and policies, along with agreements, understandings, pacts, contracts, and other working arrangements, currently obtains’ (Strauss et al 1963:163). As we move into the 21 st century, hospital work is unlikely to become any simpler. On the contrary, medical technological change (Gosling et al 2003), demands for organisational accountability (Degeling et al 2004), organisational restructuring, health reform and care improvement initiatives (Berwick and Nolan

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
HEALTH SOCIOLOGY REVIEW Volume 15, Issue 2, June 2006156
Copyright © eContent Management Pty Ltd. Health Sociology Review (2006) 15: 156–168
ABSTRACT
KEY WORDS
Visibilising clinical work: Videoethnography in the
contemporary hospital
Received 16 March 2005 Accepted 30 March 2006
This paper discusses the role of video-based research methods in social research.
The paper situates these methods in the context of rising levels of visibility of
professionals in government-funded organisations. The paper argues that while
visual research may appear to play an ambiguous role in these organisations, it
can also enable practitioners to confront the encroaching demands of post-
bureaucratic work. To ground its argument, the paper presents an account of a
video-ethnographic project currently underway in a local metropolitan hospital.
This project focuses on negotiating understandings about existing care practices
among a team of multi-disciplinary clinicians. Visual data gathered as part of
that project are presented to specify issues which have thus far arisen during
the project. Against this empirical background, the paper turns to considering
the ambiguous potential of video-based research. The argument developed here
is that, besides potentially exacerbating the pressure already imposed on
clinicians - thanks to audit, surveillance and risk minimisation - video-based
research may provide staff with new resources and opportunities for shaping
their increasingly public and visible work practices.
Rick Iedema, Debbi Long andRowena Forsyth
Faculty of MedicineUniversity of New South Wales
Australia
Video
ethnography;
post-
bureaucracy;
spinal care;
reflexivity; health
care; sociology
Bonne Bonsan Lee
Prince of Wales HospitalAustralia
Introduction
Decades ago, Strauss and colleagues noted
that ‘no one knows what the hospital “is”
on any given day unless he [sic] has a
comprehensive grasp of what combination of
rules and policies, along with agreements,
understandings, pacts, contracts, and other
working arrangements, currently obtains’ (Strauss
et al 1963:163). As we move into the 21st century,hospital work is unlikely to become any simpler.On the contrary, medical technological change(Gosling et al 2003), demands for organisationalaccountability (Degeling et al 2004),organisational restructuring, health reform andcare improvement initiatives (Berwick and Nolan

157Volume 15, Issue 2, June 2006 HEALTH SOCIOLOGY REVIEW
Visibilising clinical work: Video ethnography in the contemporary hospital
1998), increased stakeholder representation inhealth care decision-making (Gattellaria et al
2001), and the growing instability of professionaland occupational boundaries (US Institute ofMedicine 2001), are factors which suggesthospitals are significantly more complex now thanthey were in Strauss’ time.
Most prominent among these developmentsis that hospitals, l ike most other largeorganisations, are under increased pressure toaccount for what they do and ensure hospital-internal processes are ‘transparent’. Starting inthe 1970s, transparency was first sought byclarifying the kinds of medical work in hospitalswhich attract particular kinds of resourceexpenditure. Thus, economists began toappropriate medicine’s categorisation of itstreatments, referred to as Disease Related
Groups (DRG), and use these to devise DRG-cost maps for hospitals. These maps charted thevariety of medical treatments doctors provide ina particular organisation, and made it possibleto produce ‘casemix’ statements, which, in turn,enabled managers and policymakers to build apicture of the relationship (and potentialdivergence) between a particular hospital’sresource utilisation, its medical treatmentcategories, and specific costs (Degeling 1994).
At a time when reports about hospital-causedor ‘iatrogenic’ errors have appeared on the publicstage demonstrating how error seriously affectsapproximately 16% of hospital cases (Brennanet al 1991; Wilson et al 1995), and news ofmedical scandals regularly airs in the public media(Australian Broadcasting Corporation 2004;James 2002); policy makers have begun to searchfor ways of extending the scope of theirknowledge of hospital practices. Under thebanner of clinical quality and safety improvement,one recent example is the introduction of theImproved Incident Monitoring System (IIMS),an updated and web-based version of the systemused for the Australian Incident Monitoring
Study (Runciman et al 1993). IIMS is expectedto collect incident reports from around thecountry, facilitate their analysis and lead to bettertargeted strategies for minimising iatrogenic error.Another related technique is Root Cause
Analysis (RCA), with which clinicians investigatetheir colleagues’ incidents and deviserecommendations for improving their systems ofwork (Iedema et al 2006). Extending the originalreach of budgetary mechanisms, these latter twotechniques seek to broaden non-clinicians’ fieldof vision to cover the clinical-technical contentof health care provision.
It is clear from the instances of IIMS and RCAthat policy makers are not just operating fromwithin an inspectorial model, however, whose onlyaim is to intensify reporting requirements acrossincreasing tracts of clinical space. Important tonote here is that IIMS is a voluntary andanonymous reporting system: clinicians decidethemselves whether and when to report incidents;although there are guides as to what kinds oferrors should ideally be reported (NSW Health2005b). For its part, and in contrast with IIMS’anonymity, RCA engages frontline and middle-management clinicians in voluntary team-basedinvestigations of incidents. Here, clinicians partyto the incident may be asked to be involved asinterviewee, witness, or adviser. The central pointis that, like IIMS, RCA is a collaborative device:clinicians’ accountability and work processtransparency are contingent on the initiative andcommitment of clinicians from around theorganisation (Iedema et al in press).
In addition to IIMS and RCA, there are otherrisk management initiatives which intrude evenmore deeply into interpersonal-interactive clinicalspace: open disclosure (Safety and QualityCouncil 2003) and patient-centredness (UKDepartment of Health 2005). These initiativesprescribe conducts considered central tomaintaining trustful relationships with patients bydisclosing the details of errors as soon as theytranspire (in the case of open disclosure), and bystructuring care processes around the clinicalexpectations of patients rather than around thepreferences of units and departments (in the caseof patient-centredness). While the (policy)literature offers clear definitions of theseinitiatives, they confront frontline staff withdilemmas in the course of their everyday work,just as do IIMS and RCA. What these initiativeshave in common is a twofold development. On

158 HEALTH SOCIOLOGY REVIEW Volume 15, Issue 2, June 2006
Rick Iedema, Debbi Long, Rowena Forsyth and Bonne Bonsan Lee
the one hand, they push down to frontline staffthe responsibility to take decisions about whatto report, what to recommend, what to disclose,and what services to provide. On the other hand,all these decisions are subject to increasingorganisational and public visibility and feedback.
It is in that sense that these initiatives incur‘responsibilisation’ on the part of frontlineclinicians (du Gay 1996). This responsibilisationmanifests as downward pressure on employeesto engage with what used to be managerial-administrative concerns: a pressure whichHeckscher (1994) and others see as being ‘post-bureaucratic’ in nature, due to the onus it placeson frontline staff to be seen to self-manage andself-organise their work. Being trained as clinicalprofessionals, however, frontline clinicians arestruggling on a number of fronts. The mostprominent source of concern for theseprofessionals is that in addition to doing the workthey were trained to do, their new post-bureaucratic role means they are now increasinglyexpected to discuss, (re)design, report, andformally evaluate their work and the changes theyimpose on it (Degeling et al 2001; Iedema andScheeres 2003). While these tasks arechallenging enough in themselves, staff are awareof the burden of having to communicate with(and make themselves understood to) morepeople about a growing number of issues, notjust in formal written documentation and atformal forums, but also in a growing number ofad hoc and nonformal face-to-face situations. Thislatter point refers to staff finding they areincreasingly faced with having to deal with others’feelings and emotions, as they negotiate thesubstance of their priorities, norms and truths.This communicative work or ‘immaterial labour’(Hardt and Negri 2004; Iedema, Rhodes, andScheeres 2005) comes into play every time it isnecessary to confront and resolve differencesamong multi-disciplinary viewpoints andaccomplish workable ‘truces’.
It is this prominence of immaterial labourwhich countervails and complicates the rational-instrumental or scientific-bureaucratic dimensions(Harrison et al 2002) of contemporary hospitalpolicy initiatives (Iedema et al 2006). The new
kinds of team work produce interactions whichare not infrequently ‘volatile’: they require specialsocial, interpersonal and emotional skills on thepart of those present to ensure a workable andproductive outcome. Disconcertingly, particularlyfor clinicians used to autonomy (Degeling 2000),this pressure to enact immaterial labour in agrowing variety of organisational forums leadsto greater general visibility of clinicians’ social,interpersonal and emotional conducts.
The present paper engages with these trendsby describing the processes and outcomes of acurrently unfolding video-ethnographic hospital-based project. This project invites clinical staff toscrutinise themselves, each other, and how theydo their work together. In that sense, the projectseeks not to minimise but to simulate the intrusioninto the clinical work by outsiders (researchers),and familiarise clinicians with this emerging gaze.With this report on some of the empiricaloutcomes of this project as background, the paperturns to a discussion of the ambiguous role ofvideo-based research in social-organisationalresearch, to elaborate the tension between videoas method of surveillance and as a means toenvisage alternative kinds of workplace identity.In the next section we provide a brief overview ofvideo-based research to situate our work.
Video ethnography as researchmethodThe arrival of cheap and light cameras led to arapid spread of video-based enquiry (Harrison2002; Pink 2001; Raingruber 2003). During the1990s, video began to be deployed for qualitycontrol of technique-dependent hospitalprocesses as part of clinical education (Michaelsonand Levi 1997; Santora et al 1996), and whileexcellent and deeply probing hospitaldocumentaries have been produced from the1950s onwards (those by Frederick Wisemandeserve special mention here), video has onlymade tentative steps towards informing scholarlyresearch into hospital work. With hospitalethnography in its infancy (van der Geest andFinkler 2004), it is therefore not surprising thatvideo has not achieved more general academicapplication in hospitals.

159Volume 15, Issue 2, June 2006 HEALTH SOCIOLOGY REVIEW
Visibilising clinical work: Video ethnography in the contemporary hospital
Outside the hospital context, video data havebeen used in three overarching ways: to objectifyin situ practices with the aim to describe theircomplexity; confront practitioners with video dataand thereby engender reflexivity; and model andtest specific kinds of practice intervention.Workplace studies (WS) is an example of the firstof these, in that its focus is on how practitionersinteract with each other and with and aroundcomputer technologies. WS has been deployedin general practitioner settings, undergroundrailway control centres and in museum contexts.The video data WS derives from these sites areused in combination with transcriptions of spokenlanguage to link physical movement not just totechnological constraint but also to linguisticinteraction (Heath and Luff 2000; Luff et al
2000). An important theme in WS analyses iswhether and how the logic of social interactionaccommodates the logic of the technologiesthrough which the work is done, illustratingexisting tensions and challenges with selectedvisual stills.
The activity theoretical (AT) work done by YrjöEngeström and colleagues initially used videoobjectively and reflexively, and more recently alsointerventionally. In an early project, they showedstaff in a General Practitioner’s clinic theiranalyses of existing consultation processes, andthey were able to elicit insight into work problemsand induce staff to adopt different work practices(Engeström 1999:85). As part of a more recentproject, Engeström and colleagues have soughtto bridge the divide in Finland between generalpractitioner and hospital care resulting frominadequate information transfer processes. Theybrought general practitioners, hospital specialists,community carers and patients together, and usedvideo data to capture discussions about obstaclesto ‘continuity of care’ (Engeström et al 2003).By making it possible for these clinicians andpatients to appreciate the extent to which theyfailed to communicate information appropriatelyto each other, the researchers were to someextent successful in exhorting physicians to adoptmethods which provided better informationcoordination and therefore a higher level of carecontinuity (Kerosuo forthcoming).
Along the lines of Engeström and colleagues’more recent work, the present paper reports ona study which uses video to depict selected facetsof clinicians’ practices; it involves ‘feeding back’edited video data to clinicians with the aim ofreflecting on the information thus produced, andit seeks to impact on the ways these practitionersdo their work by eliciting and institutingalternatives to deal with problematic aspects ofthe work. Against this backdrop, the presentpaper discusses the tension between video asexacerbation of organisational surveillance andthe apparent need on the part of (clinical)professionals to understand and preparethemselves for work in the post-bureaucratichospital (Iedema forthcoming).
The spinal pressure area clinicThis section of the paper presents data from acurrent video-ethnographic project sited (amongother places) in a spinal pressure area clinic.This clinic provides care for people with spinalcord injury who have developed pressure areas,also known as pressure ulcers, pressure soresor bed sores. The healing of pressure areasrequires complex clinical care, on occasionsnecessitating invasive surgery. Pressure areapatients who visit these clinics are highlysusceptible to hospital-based organisms and notinfrequently experience extended stays inhospital as a result of iatrogenic infection.
The research focuses on the relationshipsenacted between the spinal clinicians (includingmedical, nursing and allied health staff) and withtheir patients. It seeks to reveal the impact onthe redesign of the clinic on these relationshipsand their practices. This redesign meant theywere able to reduce expenditure per patient, duelargely to lower length of stay (Figure 1).
The impact of this intervention registerssignificantly on the expenses of the unit. Figure2 shows a decrease per patient admission from$198,000 to $42,000, and an overall reductionin spending of $600,000 over three years forpatients requiring surgery, in spite of almostdouble the number of patients treated.
What did clinicians do to bring this changeabout? To answer this question, the project began

160 HEALTH SOCIOLOGY REVIEW Volume 15, Issue 2, June 2006
Rick Iedema, Debbi Long, Rowena Forsyth and Bonne Bonsan Lee
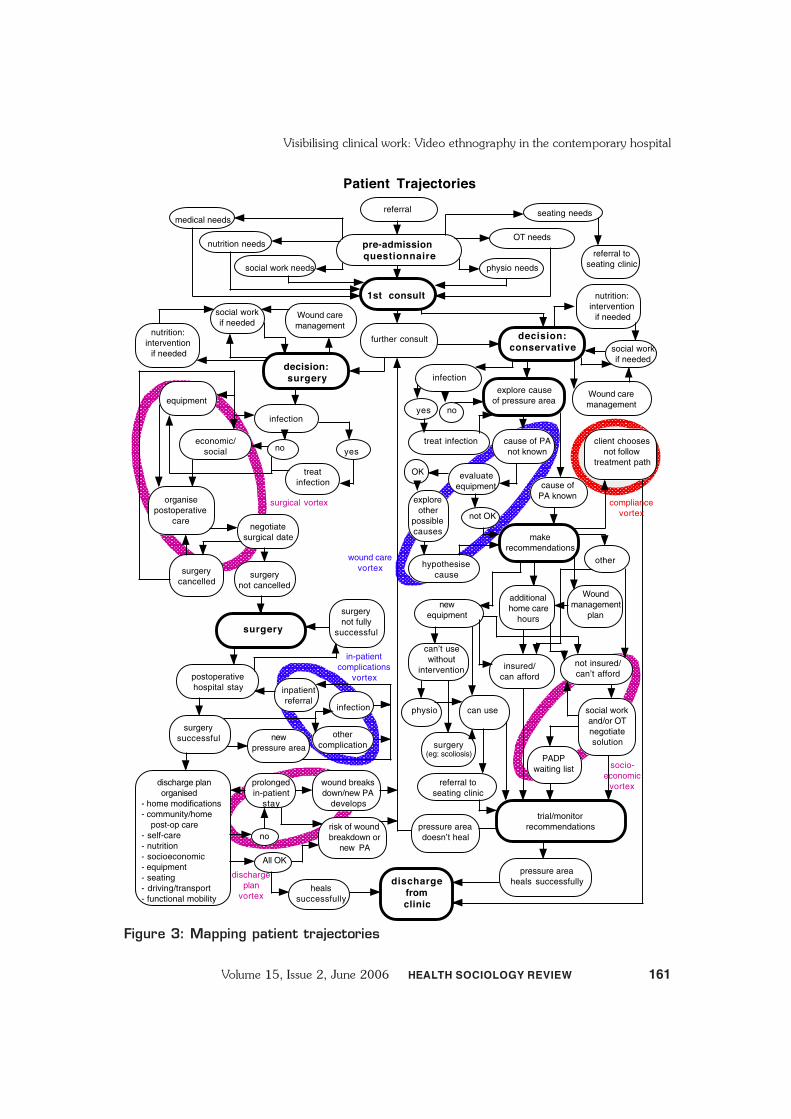
diagram is the discharge vortex: this is wheretrouble occurs due to a lack of coordination ofdischarge processes. Then there is the ‘woundcare vortex’ where wounds get badly infected,and the ‘socio-economic vortex’, where patientswith insufficient levels of insurance are unable toaccess adequate equipment support. As is in theirnature, these vortices multiply inter-professionaltensions and therefore raise the need for staff toengage in immaterial labour. Because the mapprovided an overview of these vortexes it servedto pinpoint the most common sources of teamtensions. It thereby provided a means forapprehending these problems from ‘under adifferent aspect’ (Wittgenstein 1953:193e),leading to understanding about the inevitabilityof some vortices (like non-concordance betweenclinical plans and patients’ wishes) and morestrategic approaches to resolve others.
The project also tracked the clinic’s practicesin more detail. It is here that the video-technologywas introduced and filming began of the clinic’spatient consults (but not the patient), the clinic’scase conferences where they discussed specificpatients’ histories, and team meetings where theyaddressed more general issues affecting the clinicand its management. It was particularly thepatient consults which drew attention. Theseconsults were highly significant for understandingthe logic of the clinic. Rather than the patientbeing asked to visit the different specialists bywheeling him or herself to their offices aroundthe hospital (and not infrequently being asked toappear for appointments on different days), thespinal clinic was structured so as to bring thevarious specialties involved or about to be involvedwith the patient together for the consult (Figures4 and 5).
In this clinic, then, multi-disciplinarity isinterpreted not just as ‘multiple professionalsattending meetings together’, but as involving thewhole team of clinicians in consults with patients.With an occupational therapist, a dietitian, awound-care nurse, a social worker, aphysiotherapist, at least one physician andregistrar converging on the patient, this approachcreates a busy, dialogic atmosphere in the consultroom due to multi-stranded, multi-party
Figure 1: Length of Stay (LOS) beforeand after the initiation of the spinalpressure area clinic.
Figure 2: Total cost of the clinic beforeand after its redesign
with an in-depth ethnography of the clinic to mapits practices in detail. Something resembling thisapproach has been labelled task analysis in recenthealth policy documentation (NSW Health2005a; UK Department of Health/DesignCouncil 2003). The difference between non-participant ethnography of clinical work andclinicians’ own task-analysis lies in the tendencyof staff to become accustomed to the hurly-burlyof their own work, while ‘naïve’ outsider observersare at times better able to describe its intricacies(Johnson 2001). Deploying a naïve observer, theproject was able to produce the following mapof the clinic’s practices and processes (Figure 3).
This map demonstrates not merely thecomplexity of the clinic’s care processes, but alsothe various ‘vortices’ where these processes failedand where staff regularly needed to intervene tofind alternative solutions. For instance, and withreference to Figure 3, the area in the top-left-hand corner (circled) is labelled ‘surgical vortex’:this is where delays occur due to cancelledsurgery. The circle at the left-hand bottom of the
Cost of clinic vs non-clinic mix 2003-2005
$1,200,000$1,000,000
$800,000$600,000$400,000$200,000
$ 0
$198,000
$1,000,000
$42,000
$400,000non-clinic (n = 5)
clinic (n = 9)
Cost per admission Total costs of cohort
LOS (days): Clinic vs non-clinic mix 2003-2005264
56
non-clinic (n = 5) clinic (n = 9)
LOS (days)
300200100
0
161Volume 15, Issue 2, June 2006 HEALTH SOCIOLOGY REVIEW
Visibilising clinical work: Video ethnography in the contemporary hospital
Figure 3: Mapping patient trajectories
Patient Trajectories
pre-admission
questionnaire
1st consult
physio needs
OT needs
further consult
decision:
surgery
decision:
conservative
yesno
equipment
nutrition: intervention
if needed
organise postoperative
carenegotiate
surgical date
surgery
postoperative hospital stay
discharge
from
clinic
surgery successful
heals successfully
economic/social
treat infection
surgery not fully
successful
infection
surgery not cancelled
surgery cancelled
wound breaks down/new PA
develops
new pressure area
pressure areadoesn’t heal
pressure area heals successfully
inpatientreferral
other complication
referral seating needs
referral to seating clinic
nutrition: intervention
if needed
infection
infection
treat infection
yes no
client chooses not follow
treatment path
evaluateequipment
OK
not OK
explore other
possible causes
make recommendations
can’t usewithout
intervention
can use
insured/can afford
not insured/can’t afford
PADP waiting list
social work and/or OT negotiate solution
trial/monitor recommendations
physio
surgery(eg: scoliosis)
cause of PA known
cause of PAnot known
explore causeof pressure area
hypothesisecause
new equipment
additional home care
hours
other
referral to seating clinic
Wound care management
Wound care management
Wound management
plan
compliance vortex
socio-economic
vortex
surgical vortex
wound care vortex
in-patient complications
vortex
risk of wound breakdown or
new PA
discharge plan organised- home modifications- community/home post-op care- self-care- nutrition- socioeconomic- equipment- seating- driving/transport- functional mobility
All OK
no
prolonged in-patient
stay
dischargeplan
vortex
social workif needed
social workif needed
nutrition needs
social work needs
medical needs

162 HEALTH SOCIOLOGY REVIEW Volume 15, Issue 2, June 2006
Rick Iedema, Debbi Long, Rowena Forsyth and Bonne Bonsan Lee
a patient who is not healing as expected. Theyhave just left a patient’s consult room where theywere consulting with other team members.During the consult, the doctor mentioneddepression to the patient. Now, in the corridor,he retraces that discussion with the CNC. Hisreason for doing so is that he has realised it mighthave been more appropriate not to raise thepatient’s depression in front of so many peoplein the consult room:
DR Once Liz gets out we need to pow-wow
about [patient F], I’m not convinced we
have a full [picture] ... And he’s had a
year of [treatment], and it’s still in this
situation ... so I think we need to look
at ... if there’s another way we can break
that ... there’s something going on here
that’s not allowing him to move forward.
It may be cognitive as well.
CNC I know, it may be related to the
depression.
DR Yeah, well, did you see what he did, what
his behaviour was when I mentioned
that? [CNC grimaces and covers eyes
with hand] I was thinking ‘I shouldn’t
have said this’].
CNC No. Maybe it would have been different
if it was just you there ... [the procedures
room had a large number of clinicians
with the patient at the time].
DR Let’s have a talk about it, and then we
can decide whether I go back in and talk
to him again. If we can feel strongly that
it’s worth pushing for an antidepressant,
then I’ll sit down in there with him for
as long as it takes and see if I can
convince him, because there’s something
that’s stopping this man moving forward
and I just don’t know what it is.
As a result of these interactions having beenvisualised and then reviewed during feedbackmeetings, researchers and staff were able to buildan explicit link between what was shown andthe modality of patient-centredness being enactedby the team. Clearly, the patient-centrednessmodel of the spinal clinic goes well beyond
Figure 4: The spinal pressure areaclinic’s patient consult
Figure 5: The spinal pressure areaclinic’s patient consult
conversations. This modality of multi-disciplinaryteam work means the patient does not have tomove to be seen by a whole array of clinicians,and the clinicians have the opportunity to sharetheir diagnosis and treatment plans with the otherclinicians present. This does not just obviateintricate kinds of information transfer, but alsogives team members the opportunity to monitorhow the plans of others relate to their own,creating ownership on the part of all cliniciansof the service and enhancing the chance of asafe outcome.
On the other hand, this intensity of clinicinteraction engenders significant burdens. In thefollowing excerpt, for example, the spinal doctorconsults with the CNC about a plan of action for

163Volume 15, Issue 2, June 2006 HEALTH SOCIOLOGY REVIEW
Visibilising clinical work: Video ethnography in the contemporary hospital
informing the patient of the available treatmentoptions and listening to their, and their families’,concerns (UK Department of Health 2005; vanDulmen 2003). More in line with recentformulations of ‘collaborative patient-centredpractice’, the clinic involves the patient andcolleagues in iterative, multi-disciplinarynegotiations over what is best and how toproceed. In that sense, the clinic’s practicesembody a patient-centredness which extends thenotion from a pre-determined, informationalprocedure to a dynamic form of collaborationgoverning everyday practices, relationships andcommunications (Health Canada 2004).
Having visualised individual patient consultsin this way, the project extended out to describehow the clinic structures consult days whichinvolve attending to three to four patients. Withpatients arriving around the same time in themorning, clinicians make choices about whichpatient to see based on what their priority patientsare (the surgeon does not need to speak topatients who are expected to get better with‘conservative healing’ rather than surgery, andso forth). As clinicians move to and fro betweenpatients and their consult rooms, they have adhoc encounters with each other in the small dead-end corridor around which the patient consultsrooms are arranged (Figures 6 and 7). Uponobserving and filming these ‘heterogeneous’ anddynamic interactions, it became evident that the‘liminal space’ of the corridor provided a crucialresource and site for exchanging knowledge anddecisions about patients, checking and confirmingthe significance of norms and rules, and engagingin immaterial labour to further people’sinterpersonal relationships, agendas andconcerns (Iedema, Long et al 2005).
During a discussion about hospital organization,an infection-control clinician commented:
Corridor conversations. God, the place runs
on them. We call them Corridor Conferences
- we have them just outside the ward, and in
the corridor outside the kiosk, you’re always
meeting people there and getting things sorted
out … You get more decisions made in
Corridor Conferences than you do in meetings
sometimes I reckon.
Upon viewing the corridor conversations onthe screen, the clinic’s infection-control clinicianbecame alerted to the infection risks theseconversations pose. Because the clinic deals withwounds and infections, and given the dangerousincrease in incidences of multi-resistantorganisms, infection control here is crucial. Thevideo data enabled the infection-control clinicianto identify previously unrecognised environmentalrisk factors, such as mobile phones and otherequipment handled and exchanged in the corridorand representing potential vectors of infectiontransmission. This led to the realisation thatclinicians’ heterogeneous corridor interactionscreate additional cross-infection risks, due toclinicians moving from patient room to patientroom, stopping to talk to each other, and touching
Figure 6: Corridor work in the spinalclinic
Figure 7: Corridor work in the spinalclinic

164 HEALTH SOCIOLOGY REVIEW Volume 15, Issue 2, June 2006
Rick Iedema, Debbi Long, Rowena Forsyth and Bonne Bonsan Lee
and exchanging objects in the corridor. Sheconcludes:
Whereas when I’ve observed and been in there,
there’s so much activity that it’s difficult to
focus on anything. Seeing the video you can
really focus and break things down. It’s great.
It’s much better than doing audits … And you
can make a really good risk assessment by
looking at what people are doing. Just viewing
this now, I can say definitely that [the social
worker] and [the occupational therapist]
definitely don’t need to wear PPE [personal
protective equipment such as gowns and
gloves]. The dietician, however, I would say,
yeah, you do.
DiscussionThe account presented in the previous section
describes a project which uses field-observationaland video-based methods to map the work ofselected hospital clinicians. Theoretically, theproject is designed to illuminate the contours of,and the pressures affecting, contemporary clinicalwork. Methodologically, the project involvesmaking visible what appears relevant andimportant from a research perspective, andnegotiating these understandings using visual dataas an empirical reference point. Embedded inthis research design is the notion thatcontemporary kinds of work require employeesto do their work as well as increasinglycommunicate about it (Iedema and Scheeres2003). This is not just a matter of devising adiscourse for what has thus far not been drawninto discourse, or making the ‘tacit’ explicit.Rather more challenging than that, contemporarywork involves constantly confronting newevidence, different viewpoints, diverging interestsand unpredictable emotions. This producesprocesses which are not linear and mechanical,and which therefore demand reflexive conduct.
The nature and orientation of this modality ofreflexivity differs from the processes which thesociological literature describes as the meansthrough which reflexivity is demanded from andimposed on citizens and employees. The latter‘reflexive modernisation’ (Beck 2000; Giddens1990) relies on techniques such as audit (Power
1997), surveillance (Lyon 1994; Lyon 2001) andrisk minimisation (Beck 1992). These techniquesproduce feedback whose form and substance aregenerally structured by the authorities andorganisations who seek it and whose agendas itconfirms. For example, the audit reports whichconstitute hospitals’ casemix summarieslegitimate specific norms, values, interests andperspectives that can be at odds with those ofmedicine (Degeling 1994). Audit, surveillanceand risk minimisation represent techniqueswhich, one might say, are likely to be ‘exogenous’to the in situ work these devices seek to categoriseand measure.
Video-based research can contribute to theseincreasingly rapid, generalising and intensefeedback processes which define reflexivemodernisation. Particularly its approach to visualdata editing (‘diegesis’; Metz 1974:98) can serveto give prominence to some details of practice atthe expense of others (Iedema 2001). Such useof video data may impose exogenous criteria onthe representation of practice, and mayexacerbate the subjugation of workers to thelogics which inform those criteria. That risknotwithstanding, the present paper suggests thatthis particular project’s governance of its videoresearch neutralises this potential.
First, the project’s methodological governanceproceeds from the following triumvirate ofprinciples: the research is participative, dynamic(as in ongoing and iterative) and protective ofindividuals. Endogenous in approach, the video-based research described here relies oncooperation and negotiation among practitioner-clinicians and hospital researchers as the basesupon which meaning and significance are co-constructed. Second, video-based research wasnot deployed with the aim to reduce thecomplexity of situated clinical work to a limitedand unchangeable set of proto-typical,measurable features. On the contrary, it wasnoted above that video data served to enhanceparticipants’ appreciation of the complexity ofclinical work, and perturbed prevailing descriptorsand existing categories.
Third, in using video data as a means forindividuals to observe themselves interacting with

165Volume 15, Issue 2, June 2006 HEALTH SOCIOLOGY REVIEW
Visibilising clinical work: Video ethnography in the contemporary hospital
others, the video research takes in situ specificsas its point of departure. Commenting on theirgeneral involvement in this research, clinicianshave noted on several occasions (in addition tothose captured in the excerpts cited above) howsurprised and fascinated they were by footage oftheir own in situ practices and interactions. Thiswas clearly not because they did not recogniseor understand what they were doing on thescreen. Rather, the footage enabled clinicians toaccess a field of vision commonly buried underthe hurly-burly of everyday tasks. The footageputs them in touch not just with aspects of theirwork which have been ‘settled’ and ‘filed away’upon socialisation into their specialty, but alsowith facets commonly treated as marginal to thework; principally, the immaterial dimensions oftheir everyday work inflated by the risingcomplexity of hospital work and the attendantneed to communicate with others.
That said, it is undeniable that video-ethnographic research walks a fine line betweensurveillance and self-produced observance(Iedema, Rhodes and Scheeres in press). Whilethe project operated with a clearly defined set ofprinciples for its governance, a dispute amongteam members was enough to reveal its potentialto be experienced as threatening, and to pointto the power of those who control the visual data.This became evident when a disagreement aroseover the scope and responsibilities of a particularclinical function. With the inception of thisdisagreement, the role, meaning and purpose ofvisual data collection and interpretation becamecontested and research meetings weresuspended. There was little doubt that, for thoseentangled in the dispute, the power of the visualevidence had transformed from being catharticto being disturbing.
ConclusionThis paper has presented an argument about
the changing nature of contemporary work, andabout the role played in this by video-basedresearch. The paper noted that in hospitals, asin other organisations, work is becomingincreasingly sensit ive to feedback fromconsumers, colleagues, policy makers and other
stakeholders, and it therefore becomes more andmore communication-based. This shift meansthe principles determining how work isorganised become more tentative and temporal,because dependent on the direction, content andtenor of communicat ion. In this post-bureaucratic climate, frontline staff find theyhave been responsibilised: they are put in chargeof working out how to design their work andintervene in it in light of the (public) knowledgethey are increasingly asked to produce about it.In this regard, video-based methods canexacerbate the pressure on clinicians to reformtheir work and themselves down to the moleculardetails of their conduct to suit the prevailingethos of work and the generalised standards ofperformance.
But if the hallmarks of audit, surveillance andrisk management are pre-determinedcategorisations and standards produced at aremove from the work, and with limitedinvolvement by those who enact the work(Bowker and Star 1999), the project reportedon here engages with new social-organisationalgovernmentalities by seeking to test clinicians’ability to confront these emerging visibilities withalternative conducts, measurement criteria andprocess descriptions. In doing so, the projectcapitalises on rather than suppresses the camera’sheteroglossic potential (Bakhtin 1981; Benjamin1973). It deploys video footage not with a pre-determined agenda, but as a means to negotiatethe multiple meanings and possibilities inherentin what professional practitioners do and whatthey understand themselves as doing. Also crucialfor the argument of this paper was that thisheteroglossic potential extends to the meaningsand possibilities of video itself as instrument ofresearch. Besides capturing what observation hadshown to be important for understanding the logicof the work, the visual data provided a meanswith which the clinicians could articulate whatneeded to be filmed, avoided, kept or destroyed.The progress of the project was thereforecontingent on how the clinicians responded tothe data and what it meant to them.
By describing a number of empirical issuesemerging from the video research, the paper

166 HEALTH SOCIOLOGY REVIEW Volume 15, Issue 2, June 2006
Rick Iedema, Debbi Long, Rowena Forsyth and Bonne Bonsan Lee
sought to explain how the project’s governanceinvolves those who are video-ed in directing andorienting this technology as well as in interpretingand processing the resulting data. This was putforward to support the argument that the intentof this project diverges from the agendas whichcharacterise managerial audit, top-downsurveillance and organisational risk minimisation.In a sense, the project hands frontline staff thetools usually associated with reflexivemodernisation, rather than subjecting staff tothem and their pre-determined criteria ofjudgment. The project does so not just tofamiliarise staff with the discourses and practiceswhich increasingly seek to define and describethem (such as casemix, incident reporting andpatient centredness), but to enable them toproduce alternative clusters of meaning andsignificance.
The video research described in this paperoccurs rarely in hospitals. In spite of its ability tomake visible the extraordinary efforts andachievements of clinicians, there are numerousbarriers to its deployment in these sites. Positingthe privacy of patients and the legal burden ofhaving to publicise evidence of iatrogenic erroras insurmountable obstacles, human researchethics committees are hesitant in our experiencewhen it comes to approving video-based research.One could argue that their stance contravenesthe basis of these committees’ own constitution:to create public visibility into and a negotiatedjudgement about what clinicians do with and topatients (National Health and Medical ResearchCouncil, Australian Research Council, andAustralian Vice-Chancellors’ Committee 2006).If one takes the rise in public accountability andorganisational visibility as points of departure for21st century professionalism and scholarship,integrating the methods and technologies of thesetrends into research can only lead to ademocratisation of their access, meaning andapplication.
AcknowledgementThe video study is one part of a three-yearAustralian Research Council funded Discoveryproject. Ethics for the project were obtained from
our university (UNSW; HREC 03271) as well asthe hospital site, and consent from allparticipating staff was obtained in writing.
ReferencesAustralian Broadcasting Corporation (2004) The
Law Report: Medical Mistakes ABC: Sydney,Australia.
Bakhtin, M.M. (1981) The Dialogic ImaginationUniversity of Texas Press: Austin.
Beck, U. (1992) Risk Society: Towards A NewModernity Sage: London.
Beck, U. (2000) The Brave New World Of WorkPolity: Cambridge.
Benjamin, W. (1973) ‘The work of art in the ageof mechanical reproduction’ in Benjamin, W.(ed) Illuminations Fontana Press: London:211-244.
Berwick, D. and Nolan, T.W. (1998) ‘Physiciansas leaders in improving health care: A newseries of annals of internal medicine’ Annalsof Internal Medicine 128(4):289-292.
Bowker, G. and Star, S.L. (1999) Sorting ThingsOut MIT Press: Massachusetts.
Brennan, T.A.; Leape, L.L.; Laird, M.M.; Nan,M.; Hebert, L.; Localio, A.R.; Lawthers, A.G.;Newhouse, J.P.; Weiler, P.C. and Hiatt, H.H.(1991) ‘Incidence of adverse events andnegligence in hospitalized patients: Results ofthe Harvard Medical Practice Study’ NewEngland Journal of Medicine 324:370-376.
Degeling, P. (1994) ‘Unrecognised structuralimplications of casemix management’ HealthServices Management Research 7(1):9-21.
Degeling, P. (2000) ‘Reconsidering clinicalaccountability: An examination of somedilemmas inherent in efforts to bolster clinicianaccountability’ International Journal ofHealth Planning and Management 15(1):3-16.
Degeling, P.; Hill, M. and Kennedy, J. (2001)‘Mediating the cultural boundaries betweenmedicine, nursing and management - thecentral challenge in hospital reform’ HealthServices Management Research 14(1):36-48.
Degeling, P.; Maxwell, S. and Iedema, R. (2004)‘Restructuring clinical governance to maximizeits development potential’ in Gray, A. andHarrison, S. (eds) Governing Medicine:Theory and Practice Open University Press:Maidenhead: 163-179.

167Volume 15, Issue 2, June 2006 HEALTH SOCIOLOGY REVIEW
Visibilising clinical work: Video ethnography in the contemporary hospital
du Gay, P. (1996) ‘Organizing identity:Entrepreneurial governance and publicmanagement’ in Hall, S. and du Gay, P. (eds)Questions of Cultural Identity Sage: London:151-169.
Engeström, Y. (1999) ‘Expansive visibilization ofwork: An activity-theoretical perspective’ TheJournal of Collaborative Computing 8(1):63-93.
Engeström, Y.; Engeström, R. and Kerosuo, H.(2003) ‘The discursive construction ofcollaborative care’ Applied Linguistics24(3):286-315.
Gattellaria, M.; Butow, P. and Tattersall, M.(2001) ‘Sharing decisions in cancer care’Social Science and Medicine 52:1865-1878.
Giddens, A. (1990) The Consequences ofModernity Polity Press: Cambridge.
Gosling, A.S.; Westbrook, J.I. and Braithwaite, J.(2003) ‘Clinical team functioning and ITinnovation: A study of the diffusion of a point-of-care online evidence system’ Journal of theAmerican Medical Informatics Association10:246-253.
Hardt, M. and Negri, A. (2004) Multitude: WarAnd Democracy In The Age Of Empire ThePenguin Press: New York.
Harrison, B. (2002) ‘Seeing health and illnessworlds - using visual methodologies in asociology of health and illness: Amethodological review’ Sociology of Healthand Illness 24(6):856-872.
Harrison, S.; Moran, M. and Wood, B. (2002)‘Policy emergence and policy convergence:The case of “scientific-bureaucratic medicine”in the United States and United Kingdom’British Journal of Politics and InternationalRelations 4(1):1-24.
Health Canada (2004) InterdisciplinaryEducation For Collaborative Patient-Centredness: Research And Findings ReportHealth Canada: Toronto.
Heath, C. and Luff, P. (2000) Technology inAction Cambridge University Press:Cambridge.
Heckscher, C. (1994) ‘Defining the post-bureaucratic type’ in Heckscher, C. andDonnellon, A. (eds) The Post-BureaucraticOrganization Sage: Thousand Oaks: 14-62.
Iedema, R. (2001) ‘Analysing film and television:A social semiotic account of “hospital: an
unhealthy business”’ in van Leeuwen, T. andJewitt, C. (eds) Handbook of Visual AnalysisSage: London: 183-204.
Iedema, R. and Scheeres, H. (2003) ‘From doingwork to talking work: Renegotiating knowing,doing and identity’ Applied Linguistics24(3):316-337.
Iedema, R.; Long, D.; Carroll, K.; Stenglin, M.and Braithwaite, J. (2005) ‘Corridor work:How liminal space becomes a resource forhandling complexity in health care’ inMuetzelfeld, M. (ed) Australian-PacificResearchers in Organization StudiesConference University of Victoria: Melbourne.
Iedema, R.; Rhodes, C. and Scheeres, H. (2005)‘Presenting identity: Organizational changeand immaterial labour’ Journal ofOrganizational Change Management18(4):327-337.
Iedema, R.; Jorm, C.M.; Long, D.; Braithwaite,J.; Travaglia, J. and Westbrook, M. (2006)‘Turning the medical gaze in upon itself: Rootcause analysis and the investigation of clinicalerror’ Social Science and Medicine62(7):1605-1615.
Iedema, R. (forthcoming) ‘Postbureaucratizingmedicine’ in Meyer, F. and Gotti, M. (eds)Medical Language Peter Lang: Frankfurt.
Iedema, R.; Jorm, C.M.; Braithwaite, J.;Travaglia, J. and Lum, M. (in press) ‘Rootcause analysis: Confronting the disjunctionbetween formal rules and situated clinicalactivity’ Social Science and Medicine.
Iedema, R.; Rhodes, C. and Scheeres, H. (inpress) ‘Surveillance, resistance, observance:Exploring the teleo-affective intensity ofidentity (at) work’ Organization Studies.
James, B. (2002) Minimising Harm To PatientsIn Hospital Australian BroadcastingCorporation: Sydney Australia.
Johnson, S. (2001) Emergence Penguin Books:London.
Kerosuo, H. (forthcoming) ‘Renegotiatingdisjunctions in inter-organizationally providedcare’ in Iedema, R. (ed) CommunicatingHospital Work Palgrave-Macmillan:Basingstoke.
Luff, P.; Hindmarsh, J. and Heath, C. (2000)Workplace Studies: Recovering WorkPractice And Informing System DesignCambridge University Press: Cambridge.
168 HEALTH SOCIOLOGY REVIEW Volume 15, Issue 2, June 2006
Rick Iedema, Debbi Long, Rowena Forsyth and Bonne Bonsan Lee
Lyon, D. (1994) The Electronic Eye: The RiseOf The Surveillance Society Polity Press:Oxford.
Lyon, D. (2001) Surveillance Society:Monitoring Everyday Life Open UniversityPress: Buckingham.
Metz, C. (1974) Film Language: A Semiotics ofCinema Oxford University Press: New York.
Michaelson, M. and Levi, L. (1997) ‘Video-tapingin the admitting area: A most useful tool forthe quality improvement of the trauma care’European Journal of Emergency Medicine4:94-96.
National Health and Medical Research Council,Australian Research Council, and AustralianVice-Chancellors’ Committee (2006)National Statement On Ethical Conduct InHuman Research (Draft Report) NationalHealth and Medical Research Council:Canberra.
NSW Health (2005a) Clinical Services RedesignProgram: Redesigning A Better PatientJourney NSW Health: Sydney.
NSW Health (2005b) Policy Directive: IncidentManagement Policy (PD2005_604) NSWHealth: Sydney.
Pink, S. (2001) Doing Visual Ethnography:Images, Media And Representation InResearch Sage: London.
Power, M. (1997) The Audit Society: Rituals ofVerification Oxford University Press: Oxford.
Raingruber, B. (2003) ‘Video-cued narrativereflection: A research approach for articulatingtacit, relational and embodied understandings’Qualitative Health Research 13(8):1155-1169.
Runciman, W.B.; Webb, R.K.; Lee, R. andHolland, R. (1993) ‘The Australian IncidentMonitoring study: System failure - an analysisof 2000 incident reports’ AnaestheticIntensive Care 21(5):684-695.
Safety and Quality Council (2003) OpenDisclosure Standard: A National StandardFor Open Communication In Public AndPrivate Hospitals Following An AdverseEvent In Health Care Commonwealth ofAustralia: Canberra.
Santora, T.A.; Trooskin, S.Z.; Blank, C.A.;Clarke, J.R. and Schinco, M.A. (1996) ‘Videoassessment of trauma response’ AmericanJournal of Emergency Medicine 14(6):564-569.
Strauss, A.; Schatzman, L.; Ehrlich, D.; Bucher,R. and Sabshin, M. (1963) ‘The hospital andits negotiated order’ in Freidson, E. (ed) TheHospital In Modern Society Free Press ofGlencoe: New York: 147-169.
UK Department of Health (2005) Creating APatient-Led NHS - Delivering The NHSImprovement Plan UK Department of Health:London.
UK Department of Health/Design Council (2003)Design For Patient Safety: A System-WideDesign-Led Approach To Tackling PatientSafety In The NHS Department of Health:London.
US Institute of Medicine (2001) Crossing TheQuality Chasm: A New Health System ForThe 21st Century National Academy Press:Washington.
van der Geest, S. and Finkler, K. (2004) ‘Hospitalethnography: Introduction’ Social Science andMedicine 59(10):1995-2001.
van Dulmen, S. (2003) ‘Patient-centredness’Patient Education and Counseling51(3):195-196.
Wilson, R.; Runciman, W.B.; Gibberd, R.W.;Harrison, B.; Newby, L. and Hamilton, J.(1995) ‘The Quality in Australian Health CareStudy’ The Medical Journal of Australia163(9):458-471.
Wittgenstein, L. (1953) PhilosophicalInvestigations Blackwell: Oxford.
Published by eContent Management Pty Ltd (SAN 902-4964), PO Box 1027, Maleny, QLD 4552, Australia.Tel.: +61-7-5435 2900; Fax: +61-7-5435 2911;
[email protected]; www.e-contentmanagement.com
CHILDBIRTH, RISK & TECHNOLOGY — OCTOBER 2006
A special issue of Health Sociology Review – Vol 15/4Edited by Kerreen Reiger
ISBN 0-9775242-5-6 iv + 92 pages Soft cover
Related Documents











