Communications research conducted on behalf of the Robert Wood Johnson Foundation April 2011 Talking about Health Care Payment Reform with U.S. Consumers: Key Communications Findings from Focus Groups

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Communications research conducted on behalf of the Robert Wood Johnson Foundation
April 2011
Talking about Health Care Payment Reform with U.S. Consumers:Key Communications Findings from Focus Groups

1
Table of Contents
Talking About Health Care Payment Reform with U.S. Consumers ................................................................................................. 2
The Message Research Process ............................................................................. 4
Three Key Takeaways ............................................................................................ 5
Lessons Learned from Exploring Message Concepts ....................................... 6
Tested Messages for Use with Consumers ........................................................ 10
Tested Explanatory Narrative to Use with Consumers ................................... 11
Tested Answers to Five Common Questions ................................................... 12
Appendix A: Research Presentation Defending Payment Reform to Consumers .......................................................................... 13
Appendix B: Phase One Focus Group Questionnaire .............. 33
Appendix C: Phase Two Focus Group Questionnaire .............. 40
2
Talking About Health Care Payment Reform with U.S. Consumers: Key Communications Findings from Focus Groups
Finding effective language to talk to consumers about changing the way health care is paid for in the United States is extremely challenging. A series of intensive focus groups with consumers has shown that Americans are uncomfortable talking about the role money plays in delivering their health care to them, and insist that dollars should not be a part of the quality-care equation. When forced to have discussions about system reforms or controlling health care costs, emotions quickly escalate and fears that access to care may be limited dominate the conversation. But as difficult as conversations about new models for paying for health care may be, the nation still needs to have them, and soon. The Robert Wood Johnson Foundation (RWJF) is the largest foundation focused exclusively on health and health care in the United States. As a core part of its mission, RWJF is helping to lead a transformation in the quality of care provided to people in communities nationwide. Aligning Forces for Quality (AF4Q) is RWJF’s signature effort to lift the overall quality of health care in targeted communities, as well as reduce racial and ethnic disparities and provide real models of local reform to national leaders. In the regions where Aligning Forces operates, people who get care, give care and pay for care are working to rebuild health care systems, so they work better for everyone involved. The program intends to drive change in local health care markets that will result in measureable improvements by 2015.
Since AF4Q kicked off in 2006, it has helped define the field of regional quality improvement. When the program began, the idea of diverse local stakeholders linking approaches to enhance quality and increase the value of health care was novel. Since then, Aligning Forces’ emphasis on 1) engaging consumers, 2) measuring the performance of providers and reporting it publicly, and 3) improving the quality and equality of care being delivered has taken hold.
RWJF has long been committed to changing the current health care payment system to one that rewards value instead of volume. The foundation believes public and private payers should use common measures to assess provider performance, and that providers who deliver high-quality, cost-effective care or who improve significantly should be rewarded. RWJF also believes providers should be fairly compensated for preventive care, time spent coaching patients and coordinating care for those with chronic conditions.

3
As part of their commitment and beliefs, RWJF leadership has invested in considerable research and demonstration projects to explore different models for delivering care and for paying doctors and hospitals to deliver high-quality health care. The insights gained from this work are foundational to the work undertaken as part of the third phase of the Aligning Forces initiative, begun in 2011. From 2011 to 2013, communities involved in AF4Q will engage in their own exploratory efforts to improve the way providers are reimbursed. Each will implement – or set the stage to implement – a workable model for reforming a segment of the health care payment system in their community. They will develop and test small-scale models that incentivize providers to deliver high-quality, cost-effective care. As organizers in Aligning Forces communities begin their payment reform efforts, it is important that they have tested language and messages that best explain the need for payment reform in ways that consumers will understand and not fear their work. The AF4Q program has traditionally provided this type of message assistance. In the summer of 2007, RWJF began a process to develop messages for use by the Aligning Forces communities to begin conversations with consumers and patients about “quality” health care. The foundation recognized that educating the public about the importance of quality health care and making informed choices about one’s health is an instrumental part of health care transformation. Thus, RWJF sponsored research on how best to begin explaining the problems with health care quality, highlighting the types of solutions AF4Q is pursuing and calling people to action. Later, messages to use in beginning conversations with physicians about performance measurement and public reporting were developed and tested. The goal of this communications research project was to develop and test simple messages that explain the concepts of payment and delivery reform to consumers in ways they understand and support. IMPORTANT: The focus group results explained in this report were conducted for the sole purpose of identifying and testing messages for communications purposes. The groups were not conducted to determine – and the results do not explain – how to design different payment or reimbursement systems, or which types of systems consumers will support.
4
The Message Research Process RWJF staff and communications consultants from GYMR Public Relations and MSLGROUP worked with Lake Research Partners, a nationally respected message research and polling firm, to craft basic messages that explain the issues around health care payment, cost and value. These included concepts about delivery and payment reforms that coupled would improve the doctor-patient relationship and provide direct benefits to the patient. Dozens of words, phrases and message concepts were discussed in focus groups with people who are informed and engaged health care consumers and caregivers in their communities. Based on their reactions, initial messages were edited and some were refined for further exploration in a second round of focus groups, again with informed and engaged consumers. Based on the results, the team developed a final set of core messages. The four-step process for developing and testing messages included: 1. Brief analysis of existing research
Despite its importance, surprisingly little research had already been conducted into how consumers view the role money plays in delivering health care. A sampling of existing research on consumer views on health care costs, and payment and delivery reform were reviewed. Using the insight gained from this review, sample messages and a focus group guide were developed.
2. Initial round of six focus groups Six focus groups were conducted in December 2010 in Detroit, Kansas City, Mo. and Boston, all AF4Q communities. Groups were segmented by gender and included a mix of age, race, ethnicity, education and income. All participants were insured and half were managing at least one chronic condition. The initial groups tested concepts around payment reform and responses to negative reactions. The challenges encountered were used to refine message concepts.
3. Second round of four focus groups A second round of four focus groups took place in March of 2011 in Charlotte, N.C. and Philadelphia, neither of which are AF4Q communities. The participants were of the same profile as in the first round. The aim was to further test concepts and determine what language resonated most favorably with consumers.
4. Finalize messages Based on the results of the focus groups, final messages were selected and reviewed by RWJF staff and prepared for the AF4Q communities and related audiences.

5
Three Key Takeaways
1. This is not a conversation most consumers want to engage in. Beginning an aggressive public discussion about payment reform with consumers right now could raise more questions than answers, creating more problems than clearing paths toward solutions. The focus groups made it abundantly clear that consumers do not want to think or talk about how, when or why their health care providers are paid. They have little to no knowledge about how the current reimbursement process works, and linking money or payment to their health and health care makes them uncomfortable at best, very angry at worst. Especially in this economy, the notion that physicians should be paid differently to do high-quality work or go the extra mile to give their patients the care they need is a non-starter. The messages in this report therefore, are best used reactively rather than proactively.
2. There is a gender gap with this issue. In every focus group, men and women responded very differently to the topics of health care payment, earning more for higher performance and using adherence of established guidelines to measure quality of care. While both men and women expressed deep commitment to their doctor-patient relationship, men were far more ready to consider quantifying the relationship in terms of care-provided-for-dollars-earned. Women, in contrast, almost always spoke of the relationship in much more personal terms, and repeatedly expressed concerns that data alone do not provide information on the patient’s personal experience with the doctor. This is interesting, because while men seemed more ready to think about reforming the payment system, communications research has shown that women are typically a family’s gatekeeper to the health care system and choose doctors for family members. Closing this gender gap will be key to any broad changes to the system for paying doctors.
3. While consumers don’t want to discuss payment and reform, they do want
changes in care delivery – and these changes open the door to the conversation. Patients want to spend more time with their physicians, and they want the care they receive from different doctors to be better coordinated among them. While they are not keen to think about the role of money in their own personal health care, they are open to hearing about new methods of structuring the system if it would result in more of what they want without more cost to them.

6
Lessons Learned from Exploring Message Concepts “Reform” is not a popular word. Regardless of political ideology, there seemed to be fatigue, at best, and fear, at worst, about any concepts of further “reform” of American health care. Even when reform was seen as positive, there was little support from participants for it to be tested in their backyard. To reduce instant negative reactions by consumers, “payment and delivery reform” is best described as “improvements/changes to the payment and reimbursement system” rather than reform.
Focus on improving the doctor-patient relationship as the primary reason
to change the payment/reimbursement system. Consumers value the personal nature of the doctor-patient relationship, want to be involved in the decision-making process and want physicians to communicate with them more effectively. They support changes that would enable providers to spend enough time with them during appointments to address all of their questions, stay open late so they can see the doctor after the work day, or to at least answer their questions through a phone call, email or quick visit - even if they aren’t scheduled for an appointment, and can help them avoid a trip to the emergency room. Focus messages on PATIENTS not physicians. Consumers were ambivalent towards messages about changing the way health care is reimbursed to help physicians overcome barriers to practicing medicine the way they want to. The team tested initial messages focused on the plight of today’s primary care physicians under the current fee-for-service system, and consumers did not respond well. While they like their own doctors, they have little sympathy for the complaints of physicians. They see them as being among the best paid professionals. When told that physicians often do not get paid for doing the types of things necessary to effectively manage their patients’ care, many cite examples of “going above and beyond” what they are paid to do in their own jobs, having to stay late to do it and not getting a bonus for it. Most believe physicians did not go into health care for financial reasons and it unnerved them that doctors could be motivated by money. These feelings were especially strong when discussing incentivizing doctors for doing things they don’t currently get paid for, or “rewarding” them for providing high-quality care. They were shocked that physicians would need to be paid more to “provide good care.” Further discussion made them angrier, and many questioned whether physicians were “being greedy.”
I didn’t like this “easier” for your doctor. I am the patient and it may sound selfish but I am not worried about making it “easier” for the doctor. Female - Detroit, MI

7
Position the benefits to consumers as “improving care coordination” and
“increasing preventive care.” Phrases like “improving care by having doctors and nurses and other medical professionals work together more” elicited positive reactions. People do not initially believe that doctors should be paid more to coordinate care, but certainly want coordination between their different doctors’ offices to be improved. By adding that better care coordination is a key to ensuring patients receive all the necessary preventive services and avoiding unnecessary hospital visits, participants’ positive reactions intensified.
I hate when the left hand doesn’t know what the right hand is doing. It’s so frustrating. Male – Philadelphia, PA
I like the idea of everyone communicating because I know that when I go to a new doctor or someone like a specialist that I don’t want to have to explain myself all over again. It is like retelling my story all over again and they say have you done this -- yes I have done that, my primary doctor has done that. Female – Charlotte, NC
Explain the need to improve the reimbursement system around benefits of
action, not risks of inaction. Consumers reacted poorly to messages that positioned this work as curtailing incidents of physicians performing the “wrong tests” or prescribing the “wrong medications.” They do not like the idea that they may receive the wrong care and this line of messaging caused them to shut down. They responded much more positively when the issue is framed as, “[making] sure you get the right
Do not discuss “efficiency” and “value.”
medications and tests.”
In initial focus groups, conversations about “eliminating waste,” “increasing efficiency” or even “saving money” sparked consumers to think this work could lead to rationing care that they want – and feel they need – but that may be expensive. The same holds true for the concept of increasing “value” in health care. They think of value as something they “go to a big box store for” – certainly not their doctor’s office. Anything that makes them feel that their care will be cheapened, time with their physician will be lessened, or – worst of all – that the care that they want will be curtailed, is a massive threat and not supported. People want to hear about actions taken, not ideas discussed. After failing with passive messages like, “our community is talking about how to improve care” that focus group participants said sounded unsubstantial and inconsequential, success was found with active phrases like, “our doctors and
8
hospitals are working with insurers, employers and everyday people to find
better ways to make sure people get the best care possible.” Focus group participants reacted positively to this line of messaging and noted that it sounded like real change was in the works, something they are eager to see (if described just right).
Frame conversation about costs as “spending dollars more wisely” – not cutting costs from the system.
Consumers think health care is expensive, and messages about “spending health care dollars more wisely” resonate with them. They know a lot of money flows through the health system and think some of it could be repurposed – not necessarily eliminated – with better results. They liked the concept of finding better ways to deliver health care without paying more
for it and without taking dollars away from it (which sparks fears of rationing). Consumers are aware that the U.S. spends more money than other countries on health care – but don’t know if that is a good or bad thing. They also know that examples of health care systems that provide quality, individually-tailored health care and use consumer dollars wisely already exist in the U.S., at places like the Mayo Clinic, and they want that kind of care. (Mentioning that a payment and delivery model - or type of care - was tried at the Mayo Clinic increased interest.)
Consumers want to see their doctor, not his/her nurse and not necessarily a “team.”
Talk about the concept of well-coordinated “teams” managing a patient’s care sparks concerns among consumers. They feel that it means they will see less of their primary provider, be cared for by others who are not necessarily physicians (e.g., nurses and other assistants) or that too many people will be involved in their care with no one in charge. Some worried about privacy if too many people were involved. Many focus group participants felt the “team” concept undermined the patient-doctor relationship by involving too many people and could limit the time a patient has with his/her provider. Others felt that a “team” setting would create confusion around who would be in charge of a person’s care. With further discussion and clearly explaining that a patient’s doctor would be in charge, or the “quarterback” of the health care team, and that it would not limit their time with their doctor, the participants had a more positive view of the health care “team.”
If you have ever been a part of the whole team concept at your job, all of this money they spent on this and all of this training … and it ended up not working. They hand off everything to each team member and something gets dropped, then it becomes a big bother and they spent thousands of dollars on the whole thing. Female – Detroit, MI

9
It’s tough to explain “measures,” “quality” and “guidelines.” Previous research has shown that consumers do not understand the concept of performance measures in health care, and references to measures and guidelines feel constraining to them. These terms speak to their fear that they will not be able to get whatever care they want whenever they want it in the future. They want to know who determines the guidelines and are concerned that using them will limit the care that they passionately feel they need to receive. Emphasizing that national medical experts/organizations created the guidelines, and that they are based on scientific evidence and are not binding on anyone helped defuse concerns.
10
Tested Messages for Use with Consumers Tested Statement that Effectively Describe the Overall Effort to Consumers
a. Right here in our community, XXXXX, a nonprofit group, is looking at ways to improve the health care that we all receive. We’re bringing together patients, doctors, business owners, insurers and others to find ways to get better outcomes and spend dollars more wisely. That includes making sure that doctors understand that we want to pay for the right care, not tests or procedures that we do not need.
Tested Statements that Effectively Explain Payment and Delivery Reform to Consumers
b. We want to make sure the way insurance pays for health care is consistent with the way you want to receive it. That means high-quality care that is tailored just for you, based on the best medical evidence, well-coordinated and communicated across your health care providers.
c. We have all heard about mistakes in health care – stories of people who did not get the care they should have gotten, or got care they never needed. Across America and right here at home, experts are looking at different ways of paying doctors – without any of us having to spend any more money – that would ensure patients are more likely to get high-quality care.
d. We want to test different ways insurance companies pay doctors to see what methods lead to physicians providing the highest-quality patient care most often.
Tested Statements that Effectively Link Payment to Quality/Guidelines
e. We are looking to see if paying physicians for providing care that is proven to work – like regularly checking the feet of people with diabetes in order to prevent complications like amputation later down the road – results in more physicians giving these check-ups.
f. There is an effort underway locally to look at ways to pay physicians based on whether they deliver care that is recommended by guidelines developed by national medical experts. Guidelines are just recommendations and do not need to be followed with every patient, but they indicate the type of care that generally works best for most patients, based on the evidence.

11
Tested Explanatory Narrative to Use with Consumers:
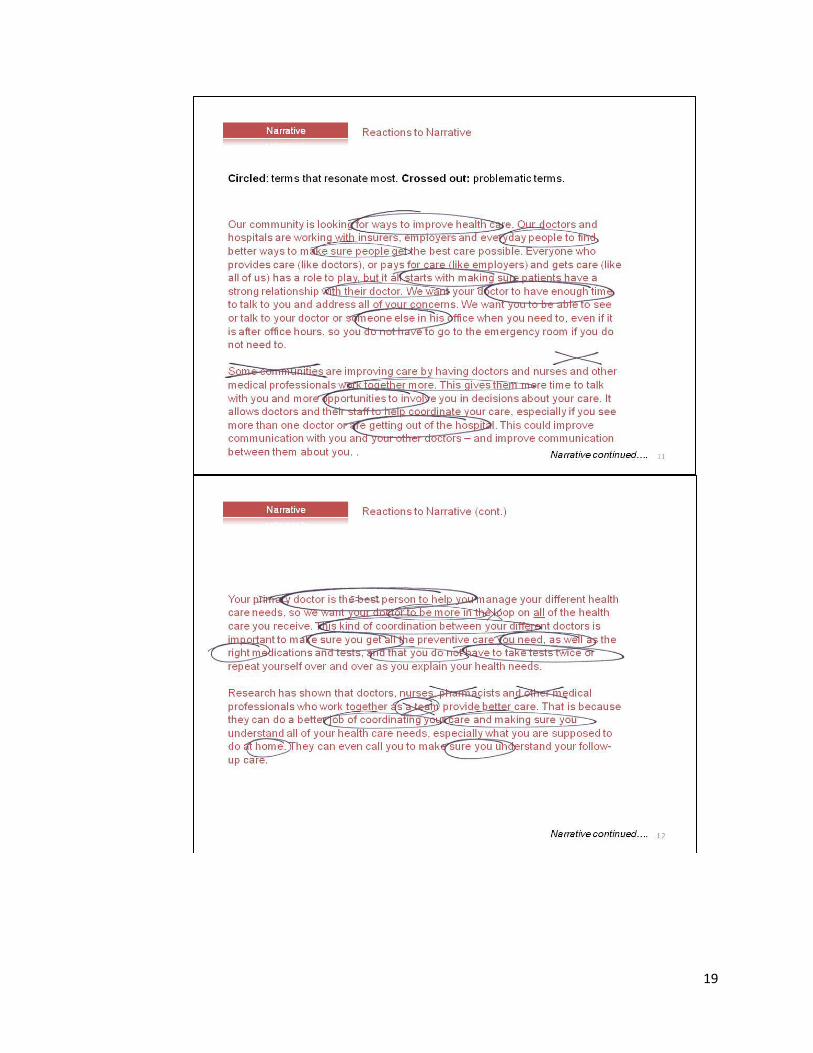
Our community is looking for ways to improve health care. Working with XXXXX, a nonprofit organization, our doctors and hospitals are working with insurers, employers and everyday people to find better ways to make sure people get the best care possible. Everyone who provides care (like doctors), pays for care (like employers) and gets care (like all of us) has a role to play, but it all starts with making sure patients have a strong relationship with their doctor. We want your doctor to have enough time to talk to you and address all of your concerns. We want you to be able to see or talk to your doctor or someone else in his office when you need to, even if it is after office hours, so you do not have to go to the emergency room if you do not need to. Some communities are improving care by having doctors and nurses work together more. This gives them more time to talk with you and more opportunities to involve you in decisions about your care. It allows doctors and their staff to help coordinate your care, especially if you see more than one doctor or are getting out of the hospital. This could improve communication with you and your other doctors – and improve communication between them about you. Your doctor is the best person to help you manage your different health care needs, so we want your doctor to be more in the loop on the health care you receive. Coordination between your different doctors is important for making sure you get all the preventive care you need, as well as the right medications and tests, and that you do not have to take tests twice or repeat yourself over and over as you explain your health needs. Research has shown that when doctors and nurses work closely together, they do a better job of coordinating your care and making sure you understand all of your health care needs, especially what you are supposed to do at home. They can even call you to make sure you understand your follow-up care. We are also working to find better ways to pay for health care. Right now, insurance companies pay most doctors based on the number of patients they see in a day, or how many different procedures they do. We want to make sure that the way insurance pays for health care is consistent with the way you want to receive it, which is high-quality care tailored just for you, based on the best medical evidence and your doctor’s recommendations, and well-coordinated. Health care is expensive, so it is important that we spend every dollar wisely. The goal is not to spend more money – it is to spend money in ways that best serve you, the patient. We are learning how to do this from some of the best health care systems in the country, like the Mayo Clinic, who have already found ways to improve care while using dollars more wisely. # # #

12
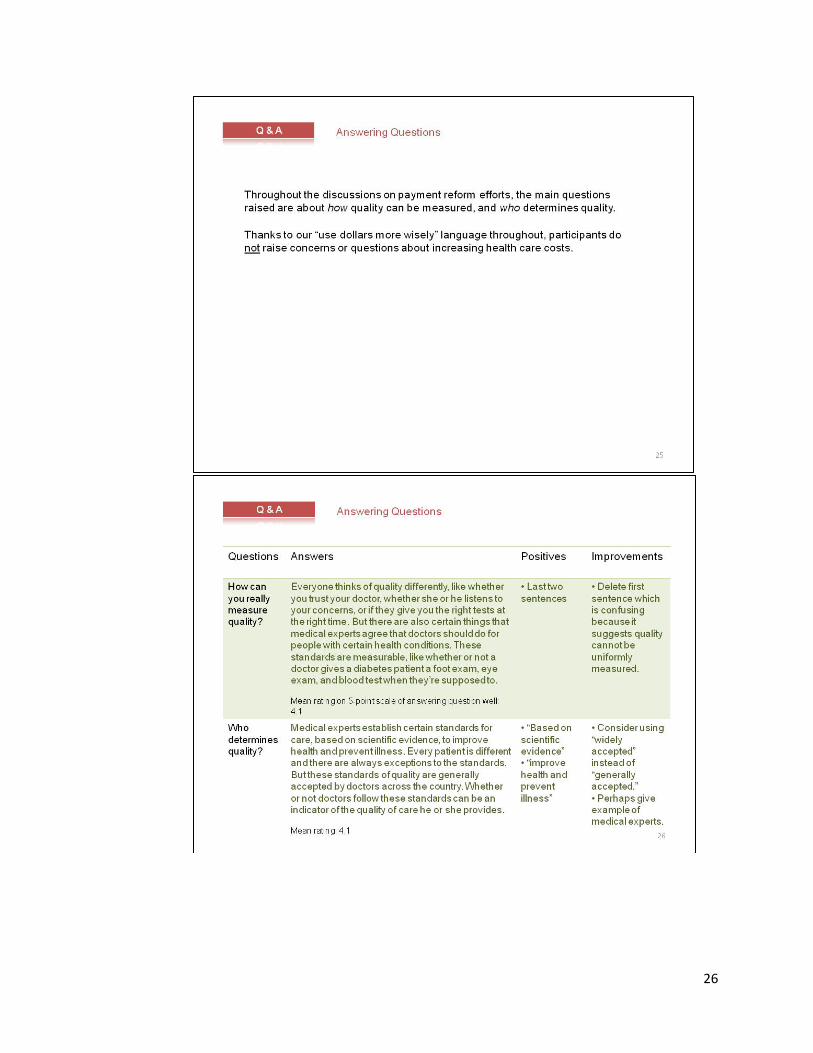
Tested Answers to Five Common Questions 1. How can you measure quality? There are also certain things that medical experts agree that doctors should
do for people with certain health conditions. When you get these things it indicates you’re getting high-quality care. These standards are measurable, like whether or not a doctor gives a diabetes patient a foot exam, eye exam and blood test when they’re supposed to.
2. Who determines quality/standards? Medical organizations establish certain standards for care, based on scientific
evidence, to improve health and prevent illness. Every patient is different and there are always exceptions to the standards. But these standards of quality are widely accepted by doctors across the country. Whether or not doctors follow these standards can indicate the quality of care he or she provides.
3. How would payment changes affect my doctor and my care? Your doctor’s pay could depend in part on providing consistently high-
quality care, based on standards. He or she would not get less payment under any circumstances. You would not pay any differently than you currently do.
4. I’m skeptical of changing the way doctors are paid. Won’t they just follow the money? We hope so. Instead of just getting paid for seeing as many patients as
possible, doctors would be paid, in part, to provide high-quality care, based on standards. That’s the care that medical experts agree should usually be provided and that you should expect.
5. Wouldn’t this make health care more expensive? This would not cost you more. Right now doctors are paid for a lot of things
that are not related to making sure your care is the absolute best care or making sure your condition is well-managed. For example, a lot of the costs that come from serious complications from diabetes – like losing a foot – could be avoided if we paid doctors specifically for giving you the care that we know results in fewer complications. We are trying to use existing health care dollars more wisely.
###

13
Appendix A: Research Presentation
Defending Payment Reform to
Consumers

14
15

16

17
18
19

20

21

22

23

24

25
26

27

28

29
30

31

32

33
Appendix B: Phase One Focus Group
Questionnaire
Detroit, Kansas City, Mo. and Boston

34
Messaging on Payment Reform
Focus Groups for AF4Q/RWJF/GYMR
Consumer Guide
December 7, 2010
Six focus groups (Detroit, Kansas City, Boston)
90 minute groups
I. Introduction/Welcome 10 mins
Moderator Introduction
Description of the Project
Ground Rules
• We are audio and video taping • There are colleagues behind the one way mirror • Please speak one at a time since we are being taped • You do not need to be an expert on this topic – we just want your feelings and
impressions • There are no wrong answers in this discussion so please speak up
Participant Introductions
• Name • Family situation • Length of time lived in the area
Let’s get started.
II. Starting with Benefit of Payment Reform 15 mins

35
1. What do you think is the biggest problem with health care right now? KEEP ANSWERS BRIEF.
2. Okay now I want to focus now on the type of care you get. I’d like you to think
about your doctor visits or any recent stays in a hospital. What are some things that could be improved?
3. Have you or someone in your family ever experienced a situation where you
didn’t understand what you needed to do to follow up on a medical treatment, or your doctor didn’t have enough time to discuss it with you? PROBE: Did you ever feel that you weren’t getting all the right tests from your doctor at the right time? Or you had to fill out the same forms every time you see a doctor?
4. Has anyone heard of a new effort in CITY working to improve the quality of
health care here? What have you heard? 5. HANDOUT. Turn to the first page in your handout. This is a description of what
an effort in CITY might do. I’d like you to read it and then rate on a scale of 1 to 10 whether you think this is important or not. I’d also like you to circle words that really stand out to you positively and cross out anything you don’t like.
GENERAL DESCRIPTION: BENEFITS Our community is talking about how to improve care. One way is to have doctors, nurses, and others work together more. This could make it easier for your doctor to spend quality time with you during appointments, to give you the right tests and treatments at the right time, and to give you more help to make sure you get the care you need, even if you see several different doctors. This could improve communication with you and other doctors – and communication between them about you. The goal would be to make sure you get the best care possible.
a. Discuss ratings. Would you support this? b. What did you circle? What is most important to you? c. Did you cross out anything? d. Is there anything else you would like to see improved?
6. HANDOUT. Turn the page again. Here’s a description of how the initiative is
trying to help doctors, nurses and others make sure you get the best care possible. Do the same thing – give it a rating and then circle and cross out words you like and don’t like.

36
HOW THINGS WILL CHANGE: CARE COORDINATION Some communities are improving care by having doctors, nurses, and other medical professionals spend more time working in teams. In a team, that they can help you better manage your different health care needs and get all the tests and treatments you need, and none that you do not need. A team approach can improve coordination between your different doctors and make sure that you do not receive the wrong medications, the wrong tests, or have to repeat yourself over and over as you explain your health needs.
a. Discuss. Would you support this? b. What did you circle? c. Did you cross out anything? d. Is there anything else you would like to see improved? Think about your
own experiences.
7. Who do you think would benefit from these improvements, such as working more in a team? Probe:
a. Would doctors? How might doctors benefit? b. Would hospitals? How might hospitals benefit? c. Would insurance companies? Is that good/bad?
III. Rationale 10 mins
8. HANDOUT. Turn the page again. This is one reason why the initiative is trying to
improve care here.
Many doctors in our community are frustrated with the current system of care because they no longer have time to provide the type of care you really want: involving you more in decisions about your care, making sure you understand all of your health needs, calling you to follow-up, and helping you coordinate your care by talking more with your other doctors. Right now, doctors and their staff have to do these types of things on their own time and without getting paid, or they do not do them at all. That’s because doctors are paid for how much care they provide – like the number of patients they can see in a day – and not for taking the time to coordinate care or talk to patients about how to follow a treatment properly. If doctors were paid for these types of services, it would be easier for them to provide the high quality care they want to give, and patients would see the benefits.
a. Reactions? What do you think about this? b. Is it believable or not? Which part is not believable? c. Any questions?

37
d. What do you think about that last part – the way the system pays doctors right now? Do you think we should change this?
IV. Describing Payment Reform 15 mins
9. Now I’d like you to read more details of how this initiative is going to work to
make these improvements. Circle words or phrases you like, cross out anything you do not like. HANDOUT This local effort could work toward better ways to pay doctors and their staff for health care. The issue is not that we need more money to pay for care; the issue is that we could use the money more wisely. For example, instead of paying for the number of services that doctors and hospitals provide to you, maybe we should pay for the overall quality of care that you receive.
a. Discuss. b. What did you circle/cross out? c. What are your concerns about this? d. What are advantages? e. Would you support this if you knew your local doctors wanted this
improvement?
10. HANDOUT. Here are more specific ways that doctors could be paid. Let’s read each one and give it a 1 to 10 rating. 1 means you strongly oppose, 10 means you would strong support.
Doctors could be paid for coaching patients and coordinating your care among your multiple doctors. This would mean your main doctor would be more in the loop on all of the health care you receive and help you make sense of it.
Doctors and hospitals could be paid for caring for the total package of treatments needed for an entire “episode of care” for a certain medical condition. Bundling these payments would make it easier for doctors to talk and work together instead of being paid separately for each step in your care.
Groups of doctors and hospitals could be paid for the overall outcomes that all of their patients receive, so to they would be paid based on the quality of care they provide. When physicians improve the quality of care their patients receive and people are healthier – and costs are saved – they would share in the success.

38
a. Discuss each. b. How would you feel if you knew local doctors supported these changes?
V. Challenges and Responses
11. HANDOUT. Now I’d like us to go over some questions and answers about these changes. Let’s read the first one. DISCUSS EACH INDIVIDUALLY.
Q. Won’t this make health care more expensive? This would not cost you more. Right now doctors are paid for a lot of things that are not related to making sure your care is the absolute best care or making sure your condition is well managed. For example, a lot of the costs that come from serious complications from diabetes – like losing a foot – could be avoided if we pay doctors specifically for giving you the care that we know results in fewer complications. If those complications occur, they are not only horrible to live with, but expensive to treat. We are trying to use existing health care dollars more wisely. Q. If doctors aren’t paid for the number of tests and treatments they give, won’t that lead to rationing care? Does that mean I won’t be able to get a test if I need it? You will always be able to get the care you need – like tests and treatments when you need them – and that your doctor recommends. This is about making it easier for doctors to give you the best care possible, not less, and giving you and your doctor more information about what works in care. Q. Is this part of the health reform law that passed? No. This is something a local group of doctors, hospitals, patients, and insurance plans are working on to improve care in CITY. Q. I’m skeptical of changing the way doctors are paid. Won’t they just follow the money? In a way, yes. And that is why some people are working to change things. Instead of getting paid for seeing as many patients as possible, Doctors would be paid to provide the high quality care they want to provide.
VI. Costs
12. Another reason to change the way doctors are paid is to try to use health care dollars more wisely. Experts say many health care dollars are wasted because doctors are not paid for time spent doing many things that would help improve

39
quality of care. If they were paid for these services, they would spend their time doing them.
HANDOUT. Here are some examples of why we should use health care dollars more wisely.
a. More than half of seniors who are hospitalized end up back in the hospital within three months for the same problem. This is often because the hospital does not work with their doctor to make sure they get follow up care.
b. Two-thirds of all costs associated with diabetes complications could be avoided if we make it easier for doctors to provide better care.
c. $700 billion dollars per year is spent on tests and procedures that do not actually improve health outcomes. Costs could be greatly reduced if doctors had more time to provide the best care possible to every patient.
d. We spend more money for health care, per person, in American that anywhere else on Earth – but we do not have the best health outcomes.
13. What do you think of these? 14. Which is most surprising to you? 15. Which do you think is the strongest reason why things need to change?
VII. Making It Personal
16. Now that you’ve heard more about changing the way doctors and hospitals are paid– do you think it is important?
17. At the beginning of the group, many of you said [costs, uninsured, gov’t
involvement] were the biggest problems in health care. So why do you think changing the way doctors are paid is important?
18. Some health plans and providers in CITY will make these changes over the next
couple years – paying doctors differently – and some will not. So this could affect your health plan and your doctors. If you had the choice, would you want your current plan or doctor to be part of these changes? Why/why not?
19. IN YES: Would you switch doctors
to be a part of it? Why/why not?
20. IF NO: Would you switch doctors
so that you wouldn’t have to be a part of it? Why/why not?
21. WRITE. Let’s say you had to convince a friend to switch doctors so that he or she would be part of this new effort. Write down the three things you would tell him or her.
Thank and dismiss.

40
Appendix C: Phase Two Focus Group
Questionnaire
Charlotte, N.C. and Philadelphia

41
Messaging on Payment Reform – Round 2
Focus Groups for AF4Q/RWJF/GYMR
Consumer Guide
February 15, 2011
Four focus groups (Charlotte, Philadelphia)
90 minute groups
I. Introduction/Welcome 10 mins
Moderator Introduction
Description of the Project
Ground Rules
• We are audio and video taping • There are colleagues behind the one way mirror • Please speak one at a time since we are being taped • You do not need to be an expert on this topic – we just want your feelings and
impressions • There are no wrong answers in this discussion so please speak up
Participant Introductions
• Name • Family situation • Length of time lived in the area
Let’s get started.
42
II. Warm Up 5 mins
22. What do you think is the biggest problem with health care right now? KEEP
ANSWERS BRIEF. 23. I want to focus now on the type of care you get. I would like you to think about
your doctor visits or any recent stays in a hospital. What are some things that could be improved?
III. Narrative 30 mins
In communities across the country, health systems, non-profits, foundations, and other groups are working to improve the quality of health care at the local level. I want to talk about these efforts and get your reactions. HANDOUT. So turn to page two of your hand out. This is a description of what a local group in another community is doing to improve care. I would like you to read this and do two things. Circle any words or phrases that stand out to you in a positive way, and cross out any words or phrases that stand out to you in a negative way. So read this with your pen - I want to talk about those words and phrases after we are done.
Our community is looking for ways to improve health care. Our doctors and hospitals are working with insurers, employers and everyday people to find better ways to make sure people get the best care possible. Everyone who provides care (like doctors), or pays for care (like employers) and gets care (like all of us) has a role to play, but it all starts with making sure patients have a strong relationship with their doctor. We want your doctor to have enough time to talk to you and address all of your concerns. We want you to be able to see or talk to your doctor or someone else in his office when you need to, even if it is after office hours, so you do not have to go to the emergency room if you do not need to.
Some communities are improving care by having doctors and nurses and other medical professionals work together more. This gives them more time to talk with you and more opportunities to involve you in decisions about your care. It allows doctors and their staff to help coordinate your care, especially if you see more than one doctor or are getting out of the hospital. This could improve communication with you and your other doctors – and improve communication between them about you.
Your primary doctor is the best person to help you manage your different health care needs, so we want your doctor to be more in the loop on all of the health care you receive. This kind of coordination between your different doctors is important to make sure you get all the preventive care you need, as well as the right medications and tests,

43
and that you do not have to take tests twice or repeat yourself over and over as you explain your health needs.
Research has shown that doctors, nurses, pharmacists and other medical professionals who work together as a team provide better care. That is because they can do a better job of coordinating your care and making sure you understand all of your health care needs, especially what you are supposed to do at home. They can even call you to make sure you understand your follow-up care.
We are also working to find better ways to pay for health care. Right now, insurance companies pay most doctors based on the number of patients they can see in a day or how many different procedures they do. We want to make sure the way insurance pays for health care is consistent with the way you want to receive it, which is high-quality care tailored just for you, based on the best medical evidence and your doctor’s recommendations, and well-coordinated. Health care is expensive, so it is important that we spend every dollar wisely. The goal is not to spend more money – it is to spend money in ways that best serve you, the patient. We are learning how to do this from some of the best health care systems in the country, like the Mayo Clinic, who have already found ways to improve care while using dollars more wisely.
24. Would you support this in your community or not? 25. Why would you want this?
26. What worries you about this?
27. Let’s go paragraph by paragraph. READ EACH OUTLOUD
a. What is positive here? What did you circle? Why? b. What did you cross out? Why? c. Any questions or doubts? Explain
IV. Statements 30 mins
Now I would like to get your reaction to some statements. Let’s say a local group is going to take this on here in your community. This is a group of health systems, doctors, employers, and community members.
HANDOUT. Let’s say a spokesperson from this group is talking about what they want to do. I want you to read each statement, again with your pen. Circle words that stand out positively and cross out words that stand out negatively to you.
44
Then rate each statement on whether it makes you more likely or less likely to support the group. Finally, put a star next to the statement you think is BEST – that is most likely to earn your support. [1 to 10 scale less likely to support, more likely to support, 5 is no affect]
General Statements
a. There is a lot of waste in the health care system – we can certainly spend money more wisely. Here in our community, we are looking at ways to pay for the type of high-quality care we all want and not pay for unnecessary care or care that does not work.
b. There is a lot of talk in Washington about different ways to pay for health care,
but one size does not fit all. What works for Baltimore is not necessarily best for Boston. That is why a local nonprofit group is exploring ways to improve health care. They are looking at our health care from every angle to figure out what will work best for us.
c. Right here in our community, a nonprofit group is bringing together patients,
doctors, business owners, insurers and others to talk about how we can get better outcomes for all the money that is being spent on health care.
d. Here in our community, we are looking at ways to improve the health care that
we all receive, so that we get more for the money we spend. That includes making sure that doctors understand that we want to pay for the right care, not tests that we do not need or other unnecessary procedures.
28. Get ratings, discuss. 29. Get stars, discuss. 30. What words did you circle? Why? 31. What words did you cross out? Why?
Specific Statements about Paying MDs
Here are a few more statements. Again, these are statements that a spokesperson from the local group might say. I want you to read each statement with your pen. Circle words that stand out positively and cross out words that stand out negatively to you.
Then rate each statement on whether it makes you more likely or less likely to support the group. Finally, put a star next to the statement you think is BEST – that is most likely to earn your support. [1 to 10 scale less likely to support, more likely to support, 5 is no affect]
45
e. We are exploring different ways to recognize and reward doctors in our community who consistently provide the highest-quality of health care possible. The idea is that other doctors can learn from their example and follow them, so all of us get the benefit of better care.
f. We want to make sure the way insurance pays for health care is consistent with
the way you want to receive it, which is high-quality care tailored just for you, based on the best medical evidence, well-coordinated and communicated across your health care providers.
g. We all know that people are more eager to do things that they get paid for.
Here in our community, a local nonprofit organization is looking to see if paying physicians for when they provide care that is proven to work results in better care for you.
h. We want to test different ways of paying doctors to see what method leads to
physicians providing the highest-quality patient care most often.
i. We are looking at ways to reward doctors who constantly provide the highest-quality care, with the hope that other doctors will follow their example.
j. We have all heard about mistakes in health care – stories of people who did not
get the care they should have gotten, or got care they never needed. Across America and right here at home, experts are looking at different ways of paying doctors –without any of us having to spend any more money – that would ensure patients are more likely to get high-quality care that is free of mistakes.
32. What do you think about this concept, of paying doctors differently, rewarding them for high-quality care, etc? Positives? Negatives?
33. Get ratings, discuss. 34. Get stars, discuss. 35. What words did you circle? Why? 36. What words did you cross out? Why?
Specific Statements about Guidelines
Let’s do the same thing one more time for three final statements. Read it with your pen, rate each statement, and then put a star next to the best one.
k. There is an effort locally to look at ways to pay physicians based on whether they deliver care that is recommended by guidelines that are developed by national medical experts.
l. Maybe we should pay doctors more when they provide care that is proven to
work, and pay them less when they ignore these recommendations.

46
m. We are looking to see if rewarding physicians for providing care that is proven to work – like regularly checking the feet of people with diabetes in order to prevent complications like amputation later down the road – results in more physicians giving these check-ups.
37. Get ratings, discuss. 38. Get stars, discuss. 39. What words did you circle? Why? 40. What words did you cross out? Why?
V. Q & A 15 mins
41. What are the main questions you have on what we have been talking about – paying doctors differently?
42. HANDOUT. Now I would like us to go over some questions and answers about these potential changes. Read each question and then rate the answer on a scale of 1 to 5 on how well it answers the question for you personally.
Q. How can you really measure quality? Everyone thinks of quality differently, like whether you trust your doctor, whether she or he listens to your concerns, or if they give you the right tests at the right time. But there are also certain things that medical experts agree that doctors should do for people with certain health conditions. These standards are measurable, like whether or not a doctor gives a diabetes patient a foot exam, eye exam, and blood test when they’re supposed to. Q. Who determines quality? Medical experts establish certain standards for care, based on scientific evidence, to improve health and prevent illness. Every patient is different and there are always exceptions to the standards. But these standards of quality are generally accepted by doctors across the country. Whether or not doctors follow these standards can be an indicator of the quality of care he or she provides. Q. How would payment changes affect my doctor and my care? Your doctor could be rewarded for providing consistently high-quality care, based on standards. He or she would not get less payment under any circumstances and you would not pay any differently than you currently do.

47
Q. I’m skeptical of changing the way doctors are paid. Won’t they just follow the money? We hope so. Instead of just getting paid for seeing as many patients as possible, doctors would be paid to provide high-quality care , based on the standards. That’s the care that medical experts agree should always be provided and that you should expect. Q. Wouldn’t this make health care more expensive? This would not cost you more. Right now doctors are paid for a lot of things that are not related to making sure your care is the absolute best care or making sure your condition is well managed. For example, a lot of the costs that come from serious complications from diabetes – like losing a foot – could be avoided if we pay doctors specifically for giving you the care that we know results in fewer complications. We are trying to use existing health care dollars more wisely.
43. Discuss ratings.
VI. Wrap-Up 5 mins
44. If this were to happen in your community, who would you want involved?
Thank and dismiss.

Copyright © 2011
For more information:Alexis LevyCommunications OfficerRobert Wood Johnson Foundation(877) [email protected]
www.rwjf.org www.forces4quality.org
Related Documents











