KERATOCONUS DR TUSHYA OM PARKASH DR OM PARKASH EYE INSTITUTE

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

KERATOCONUS DR TUSHYA OM PARKASH
DR OM PARKASH EYE INSTITUTE
KERATOCONUS
• Keratoconus is a degenerative non inflammatory disease of the cornea were the central or paracentral cornea undergoes progressive thinning and steepening causing myopia and both regular and irregular astigmatism

ETIOLOGY• Etiology is unknown• The hereditary pattern is neither prominent nor
predictable,but positive family histories have been reported
• The most common presentation of keratoconus is as a sporadic disorder, in which only a significant minority of patients exhibit a family history with autosomal dominant or recessive transmission
• The incidence of keratoconus is often reported to be 1 in 2000 people

• Risk factors involved are eye rubbing,associated with atopy, sleep apnea, Floppy lid syndrome, contact lens wear
• Systemic and ocular associations
1. Systemic disorders: Down’s syndrome, Turner syndrome, Ehlers-Dunlos syndrome, Marfan syndrome,atopy, osteogenesis imperfecta, and mitral valve prolapse.
2. Ocular associations: Vernal disease, retinitis pigmentosa, blue sclera, aniridia, and ectopia lentis
• Onset is at puberty and progresses slowly thereafter, it
may become stationary

PATHOPHYSIOLOGY Increased levels of proteases&catabolic enzymes
Decreased levels of proteinase inhibitor Increased expression of IL-1 receptor
Decreased collagen & keratin sulphate Increased levels of non proteinaceous substance
Decreased stromal mass & apoptosis

PATHOLOGY• Classical Triad1. Stromal thinning2. Iron deposition in
epithelium 3. Breaks in Bowman's layer
(irregularity of basement membrane - earliest change)and fibrosis filling in the breaks that extend beneath the epithelium
• With hydrops,breaks at the layer of Descemets membrane are seen.
Classification• Based on severity of curvature
mild-less than 48D
moderate-48-54D
severe->54D• Based on shape
Nipple cone-<5 mmround shape; easiest to fit with contact lenses
oval cone-5-6mm and steep curvature often displaced inferiorly; more difficult to fit with lenses
globus cones-very large>6mm,75% of cornea affected; most difficult to fit with lenses

Clinical features• Symptoms are highly variable and, in part, depend on
the stage of the progression of the disorder. Early in the disease there may be no symptoms, and kera- toconus may be noted by the ophthalmologist simply because the patient cannot be refracted to a clear 20/20 corrected vision. In advanced disease there is significant distortion of vision accompanied by pro- found visual loss. Patients with keratoconus fortunately never become totally blind from their disease.
• Frequently changing spectacle Rx and axis of astigmatism
• Diplopia• Glare at night• Haloes around lights• Blurred/ distorted vision

The classical signs of keratoconus
External signs
• Munsons sign is a V-shaped conformation of the lower lid produced by the ectatic cornea in downgaze.

External signs
• Rizzuti sign-It is a sharply focused beam of light near the nasal limbus, produced by lateral illumination of the cornea in patients with advanced keratoconus.

Slit lamp findings
• Stromal thinning• Vogts striae-(Deep stromal
stress lines)-Small and brushlike lines, generally vertical but they can be oblique. -Found in the deep layers of the
stroma and form along the meridian of greatest curvature.
-Disappear when gentle pressure is exerted on the globe through the lid.

Slit lamp findings
• Iron ring-(fleischer ring)The Fleischer ring is a yellow-brown to olive-green ring of pigment which may or may not completely surround the base of the cone -Formed when hemosiderin (iron) pigment is deposited deep in the epithelium
-Fleischer’s ring often becomes thinner and more discrete with progression -Seen approximately 50% of all cases.
-Locating this ring initially may be made easier by using a cobalt filter and carefully focusing on the superior half of the cornea's epithelium.
Once located, the ring should be viewed in white light to assess its extent.

Slit lamp findings
• Scarring- epithelial and sub epithelial (epithelial nebulae, anterior stromal scars, enlarged corneal nerves).Sub-epithelial corneal scarring, not generally seen early, may occur as keratoconus progresses because of ruptures in Bowman's membrane which is then filled with connective tissue

Retroillumination signs
• Scissoring reflex on retinoscopy
• oil droplet reflex/Charleaux sign on distant direct ophthalmoscopy

• Other signs have been described such as pulsation of the mires on AT
• Videokeratography signs-
-Localized increased surface power-Inferior superior dioptric asymmetry-Relative skewing of the steepest radial axes above and below the horizontal meridian
• Photokeratoscopy signs--Compression of mires inferotemporally (“egg-shaped” mires)-Compression of mires inferiorly or centrally below the horizontal meridian

Acute hydropsIn some patients who have keratoconus, acute rupture of Descemet’s mem- brane may occur and result in acute overhydration of the cornea and ac- cumulation of lakes of fluid within the corneal stroma. The overlying corneal epithelium may become edematous, and fluid may leak through the corneal epithelium. The ruptured Descemet’s membrane curls in on itself, and over time endothelial cells spread over the posterior stromal defect to lay down new Descemet’s membrane and recompensate the cornea.

Management• Investigations-
-Pachymetry
-Keratometry
-Keratoscopy
-Videokeratography

Corneal PachymetrySlit lamp pachymetry shows thinning in the centre of the
apex. Ultrasonic pachymetry shows exact thickness of cornea at different places.
Thinning in the inferior quadrant can be diagnostic of keratoconus. Central or paracentral corneal thickness of less than 450 µm is abnormal.
If the reading decreases by nearly 20 µm towards the inferior periphery on successive pachymetric readings, it is suspicious of keratoconus. Increase in the progressive thinning of the cornea is a true index of keratoconus

KeratometerKeratometer is an invaluable tool for measuring corneal curvature. Inability to superimpose central keratometric rings suggests irregular corneal astigmatism, a hallmark of keratoconus. There is no keratometric value beyond which diagnosis of keratoconus is definite. There are patients with steep corneas and high astigmatic errors who do not have keratoconus and, conversely, patients with keratoconus who have central corneas of normal steepness

KeratometerInferior corneal steepening is also an early sign of keratoconus. By performing central keratometry, followed by keratometry with the patient in upward gaze, steepening in the inferior cornea can be identified . Keratoscopy or videokeratography, based on Placido disk, can show In early keratoconus, a focal area of increased corneal curvature as an isolated area of smaller ring spacing and distortion. ring spacing decreases overall and becomes increasingly irregular on progression
KeratoscopyKeratoscopy uses a pattern of concentric rings (mires) called a Placido disk with nine alternating bright and dark rings.
The rings are reflected off the anterior cornea surface via Purkinje image number one and viewed directly by the clinician.
The Placido disk is nothing more than a simple, inexpensive hand-held device with a central peep-hole for the clinician through which to look

Photokeratoscopy signsCompression of mires inferotemporally
(“egg-shaped” mires)Compression of mires inferiorly or centrally
The photokeratoscope or topographer placido disc can provide an overview of the cornea and can show the relative steepness of any corneal area.

Computerised videokeratography
• Commonly used ORBSAN• Elevation based maps with Placido disc capabilities
• Gives:• -true elevation maps• -posterior corneal surface• -anterior corneal surface• -pachymetry• -AC depth• -features ray tracing,IOL calculation and 3D
mapping software.

Forty images, 20 with slit beams projected from the left and 20 from the right, are acquired in two intervals, each 0.7 seconds in duration.
Simultaneously, a tracking system measures the involuntary movement of the eye during the exam.

COLOR CODED MAPGREEN- NormalYELLOW & RED- HOT (Steeper
areas).BLUE- COOL (Flatter areas

Keratoconus pattern
Keratoconus cornea-extreme asymmetrical and inferior steepening
Non keratoconus cornea-general symmetry overall withno excessive steepening

KeratoconusFeatures on topography [Rabinowitz et al]-Central corneal power > 47D-Diff. of 3D or more in corneal power of a point 3mm
superior to corneal vertex to that located 3mm inferior to it (sup./inf. Ratio).
-Asymmetry in central corneal power between two eyes > 1.4D.
-These findings have a sensitivity of 98% and a specificity of 99.5% for the diagnosis of keratoconus.

Normal Cornea

keratoconus suspect

Keratoconus

Treatment• Conservative
-Spectacles
-Contact lens
-Corneal Collagen cross linking• Surgical
-Intacs
-Corneal transplant
-Phakic IOLs
-Recent advances

Spectacles • Mild keratoconus can be corrected with spectacles.
• Retinoscopy is difficult; a normal subjective refraction is required.
• Monocular keratoconus is usually best dealt with using spectacle correction.
• In this group of patients, motivation for contact lens wear tends to be poor.
Contact lensesContact lenses are considered when vision is not correctible to
6/9 by spectacles and patients become symptomatic.
Rigid gas permeable (RGP) contact lenses are the lenses of first choice.
The aim is to provide the best vision possible with the maximum comfort so that the lenses can be worn for a long period of time.
Contact lenses• RGP contact lens-It resurfaces the irregular cornea & the intervening fluid and corrects the irregular astigmatism to provide good quality of vision-However the disadvantage with these lenses is that they have standard lens design with fixed optical zones and do not give an ideal fit in patients with keratoconus-Many patients find them uncomfortable and can tolerate only for short time,the reason is that cornea steepens and rubs against the lens causing n abrasion and light sensitivity-Dry eye is another problem with them

Contact lensesBased on shape of cone
Nipple cone : small diameter (5 mm.); round shape; easiest to fit with contact lenses
Oval large diameter(>5 mm.); often displaced inferiorly; more difficult to fit with lenses
Globus largest diameter (>6 mm.); 75% of cornea affected; most difficult to fit with lens
Contact lenses• Fitting methods-Three point touch technique-Apical clearance-Flat fitting
• Three-point-touch design-It actually refers to the area of apical central contact and two other areas of bearing or contact at the mid-periphery in the horizontal direction.
The three-point-touch design is the most popular and the most widely fitted design
The aim is to distribute the weight of the contact lens as evenly as possible between the cone and the peripheral cornea.
The ideal fit should show an apical contact area of 2-3mm with mid-peripheral contact.
Adequate edge clearance is required to ensure tear exchange.


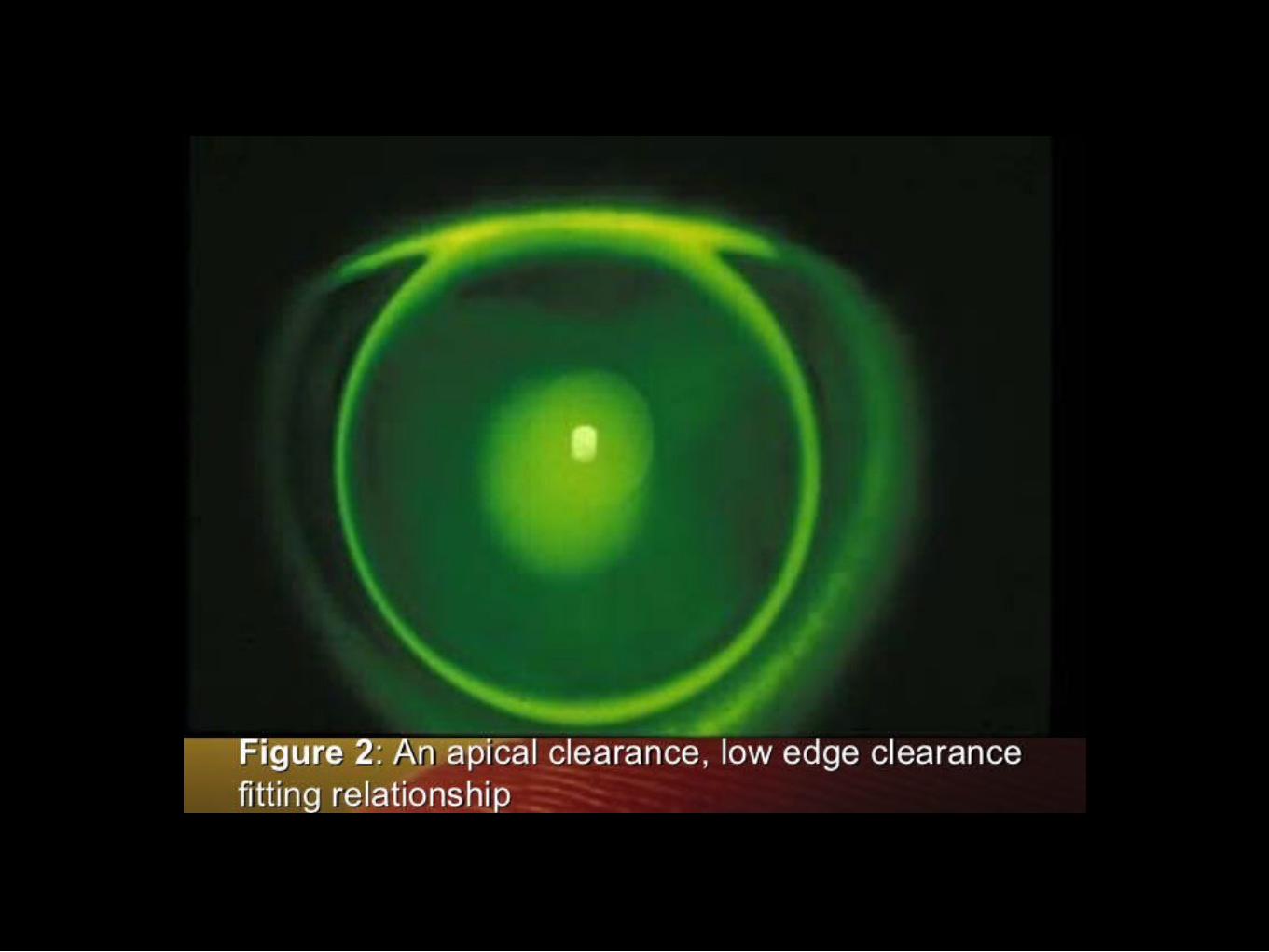
Contact lensesApical clearance
In this type of fitting technique, the lens vaults the cone and clears the central cornea, resting on the paracentral cornea.
These lenses tend to be small in diameter and have small optic zones
The potential advantages of reducing central corneal scarring are outweighed by the disadvantages like poor tear film, corneal oedema, and poor visual acuity as a result of bubbles becoming trapped under the lens.

Contact lensesFlat fitting
The flat fitting method places almost the entire weight of the lens on the cone.
The lens tends to be held in position by the top lid.
Good visual acuity is obtained as a result of apical touch.
Alignment can be obtained in early keratoconus; however, flat fitting lenses can lead to progression/ acceleration of apical changes and corneal abrasions.
This type of fitting is useful where the apex of the cone is displaced


Contact lensesPiggy back lenses - RGP-CL fitted on top of a SOFT CL
Can be used in pts who are uncomfortable with RGP wear, more so in pts prone to epithelial erosion at apex of cone
ROSE-K lenses -are specially designed for keratoconic eyes to fit any type of cone.The optical zone is reduced to snugly fit the cone & the peripheral curve is computer designed to fit the rest of the irregular cornea
Contact lensesScleral lensesThey are made of special polymer called itaflurocon.Scleral lenses play a very significant role in cases of advanced
keratoconus where corneal lenses do not work and corneal surgery is contra-indicated.
Scleral lenses completely neutralise any corneal irregularity and can help patients maintain a normal quality of life
Disadvantage is that they are difficult to use as they are large senses and cumbersome to the patients


Contact lenses• Soper lensesCustom made lens
Two zones in the peripheral posterior curvature
Central zone : to vault steep central cornea .It is of varying steepness depending of the patients cornea.
Peripheral zone is with a 45D curvature designed to vault the mid periphery and limbal cornea

Contact lenses• Boston scleral lens prosthetic device (BSLPD)The lenses are made of flurosilicone acrylate polymers with Dk
values of 87 and 130.-Fluid ventilated scleral lens
-Designed to enclose a bubble free reservoir of fluid over the corneal surface
-Series of breaches are created between haptic bearing surface of the lens and underlying sclera
-This will facilitate the aspiration of surface tears into the reservoir so that intrusion of air bubble during a blink is prevented.
-Shape of haptic confirms exactly to that of underlying sclera to maintain functionality and prevents intrusion of air bubbles.
-Very expensive

Medical therapy• For acute corneal hydrops involves
-A cycloplegic agent
-Sodium chloride 5% ointment or eye drop
-Lubricating eye drop
-Steroid drops can be used if the eye is congested
-A pressure patch
-After the pressure patch is removed patients may still need to continue sodium chloride drops or ointment for several weeks to months.
-Patients are advised to avoid vigorous eye rubbing
Collagen cross linking
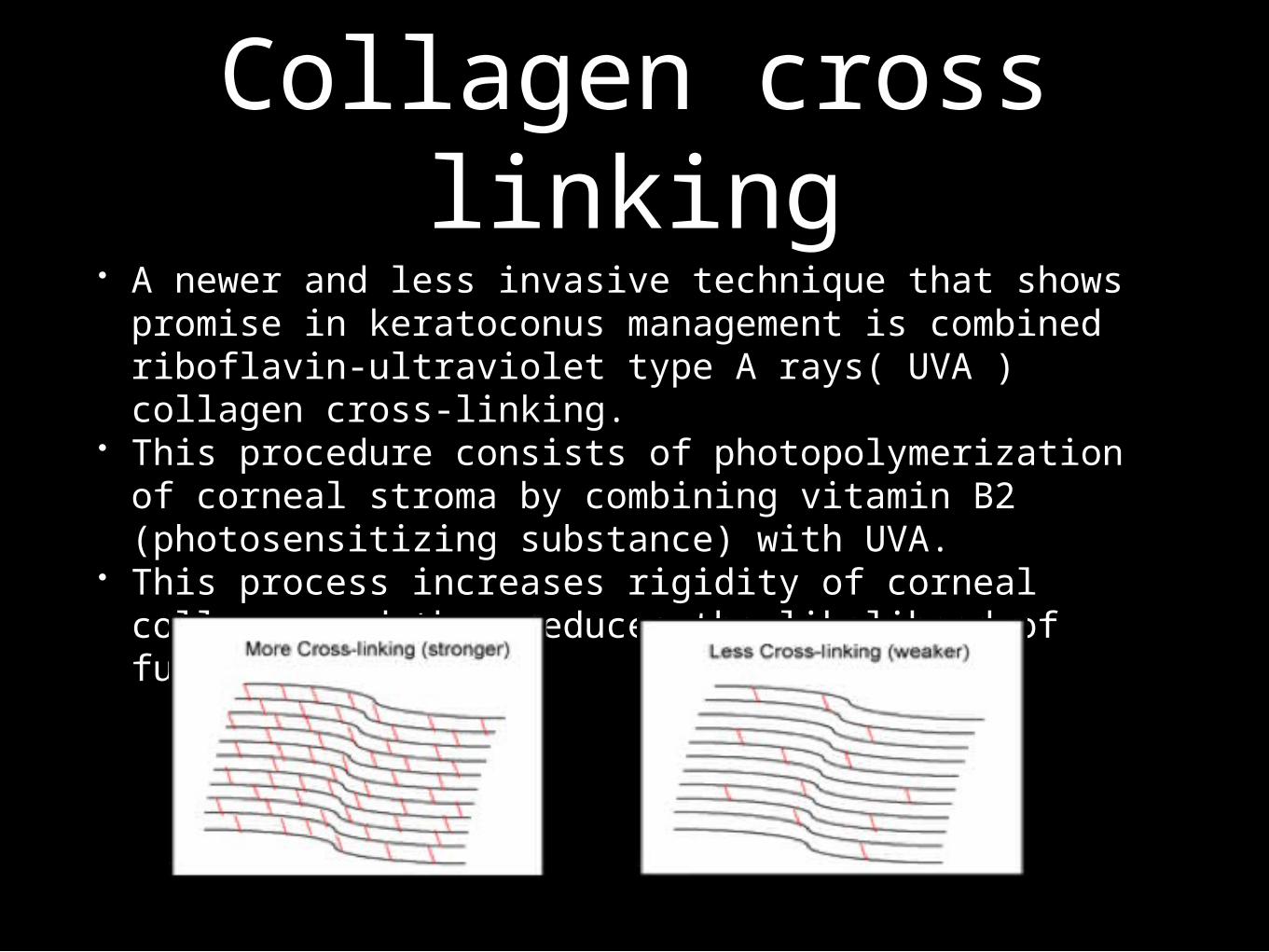
• A newer and less invasive technique that shows promise in keratoconus management is combined riboflavin-ultraviolet type A rays( UVA ) collagen cross-linking.
• This procedure consists of photopolymerization of corneal stroma by combining vitamin B2 (photosensitizing substance) with UVA.
• This process increases rigidity of corneal collagen and thus reduces the likelihood of further ectasia.

Corneal collagen crosslinking
• Technique
-Using topical anaesthesia, 7mm circle is marked on the cornea using a marker.
-Epithelium of the marked area is scraped off using a blunt spatula.
-A corneal abrasion is created to facilitate riboflavin diffusion into the cornea.
-One drop of riboflavin 0.1% and 20% dextran ophthalmic solution is instilled topically in the eye every 2 minutes for 30 minutes.
-At the end of the 30-minute pretreatment period, the eye is examined with blue light for the presence of a yellow flare in the anterior chamber, indicating adequate riboflavin saturation of the corneal tissue.
Corneal collagen cross linking
-When the yellow flare in the anterior chamber is confirmed, the eye is aligned under the UV-A light
-The correct aperture setting is selected for the size of the eye; the eye is irradiated at 3Mw/cm2 for 30 minutes at wavelength of 370nm, during which time instillation of riboflavin is continued (one drop every 5 minutes).

-After completion of the procedure,eye is washed with BSS , an antibiotic drop is instilled and a bandage contact lens is applied.
-The contact lens is removed once the abrasion has healed.
-Postoperative medications include an antibiotic and a steroid(controversial) for 2 weeks postoperatively.
-Complications of C3R
Corneal hazeDiffuse lamellar keratitisReactivation of viral keratitis and iritisInfective keratitisCorneal scarringPersistent corneal edemaCorneal melt

-mild to moderate keratoconus-post refractive ectasia-PMD Contraindications-A minimum stromal thickness of 400 μm after epithelial removal is required for safe CXL.
-In patients with corneas thinner than this, conventional CXL cannot be performed. For such patients, either contact lens–assisted CXL (CACXL) or hypotonic CXL is performed.
-CXL is also not performed in patients with stable, nonprogressive keratoconus. Keratoconus is generally likely to be nonprogressive in patients older than 35 years because of naturally occurring cross-linking occurring with age.
Indications

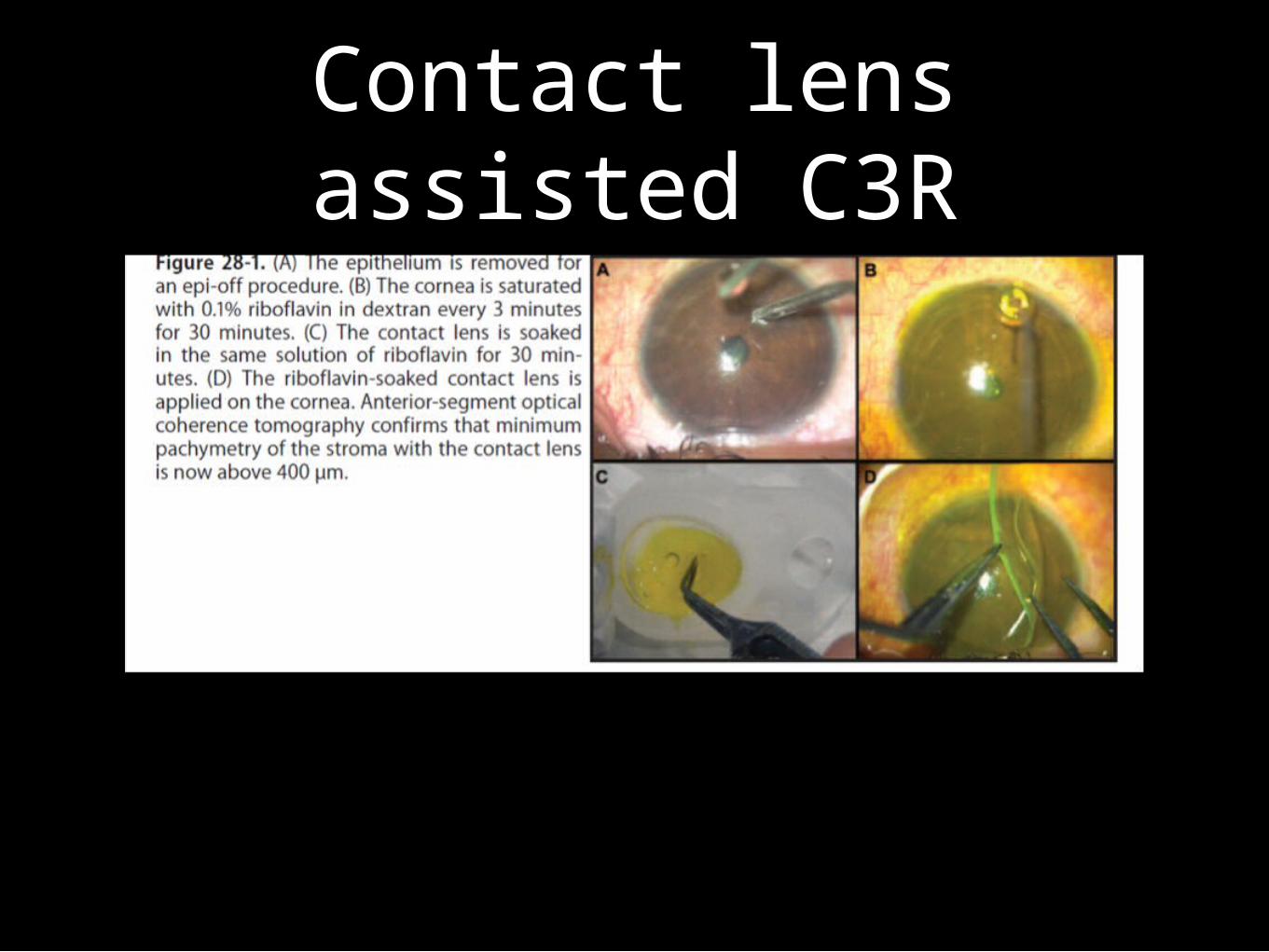
Contact lens-Assisted collagen cross-linking
It is possible that some corneas do not swell enough to make hypo-osmolar CXL possible.
CACXL has advantage of not being dependent on swelling properties of the cornea . In CACXL, thickness of cornea is artificially increased by increasing amount of riboflavin-containing substance anterior to the stroma, increasing functional corneal thickness. using precorneal riboflavin film, a riboflavin-soaked soft contact lens , and a pre–contact lens riboflavin film
Contact lens assisted C3R

Contact lens associated C3R

Accelerated C3RAs an alternative to riboflavin formulations containing dextran,
the KXL uses riboflavin 0.1% in hydroxypropyl methylcellulose (Vibex Rapid™, Avedro, Inc.). initial procedure is similar to conventional CXL of epithelial debridement. Vibex is then administered topically for 10 minutes. The cornea is then exposed to 365 nm UVA light with the CXL system for three minutes at an irradiance level of 30 mW/cm2 (accelerated CXL).

Intracorneal ring segments in keratoconus
• A method for flattening the cornea that is too steep and making a patient more contact lens tolerant is the insertion of INTACS into the cornea
• This procedure is good for patients who are contact lens intolerant and who want to avoid a corneal transplant and whose k reading are not in excess of 58 diopters
• INTACS have been approved for the treatment of mild to moderate keratinous in patients who are contact lens intolerant

Intracorneal ring segments
• In these cases, patients must have a clear central cornea and a corneal thickness of >450 microns where the segments are inserted,approximately at 7mm optical zone
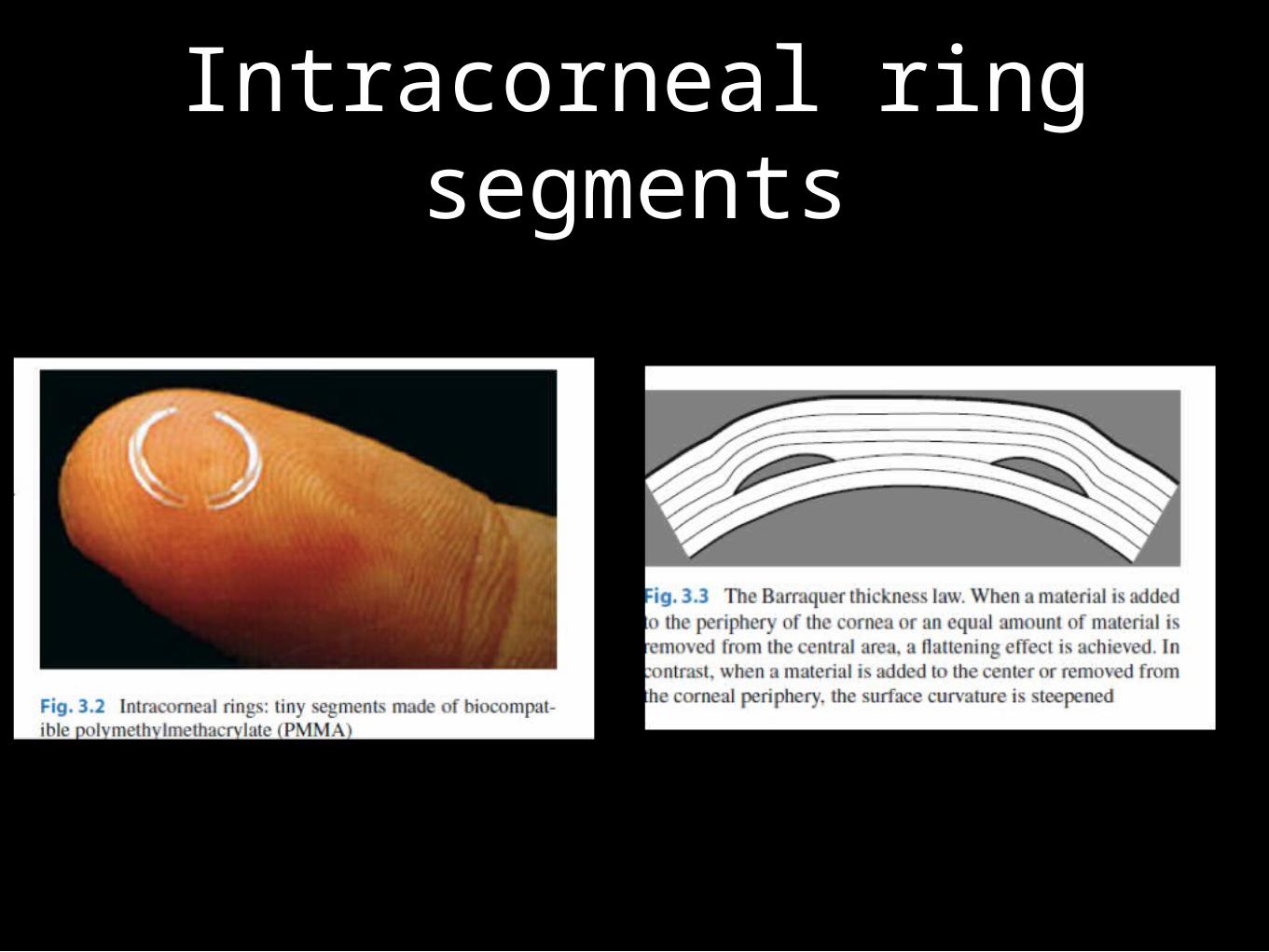
• INTACS have crescent shaped two 150-degree PMMA segments that are surgically placed in the peripheral cornea at two-thirds corneal depth
• INTACS comes in thickness from 0.25 to 0.45 mm in 0.05mm increments
• INTACS correct the myopia and irregular astigmatism by producing a mechanical flattening of the central cone

Intracorneal ring segments
• The advantage INTACS is that they require no removal of corneal tissue.no intraocular incision,and leave the central cornea untouched
• Most patients will need spectacles/contact lens postoperatively for best vision,but will have flatter corneas and easier use of lenses
• If a patient does not gain the expected results, the INTACS can be removed and then other surgical options can be considered
Intracorneal ring segments

Intracorneal ring segments
• Types
1.Ferrara ring
2.Keraring
3.INTACS

Intracorneal ring segments
Implantation of intracorneal ring segments with support from the femtosecond laser• Femtosecond laser technology allows realization with very high accuracy of individualised shape and size of corneal tunnel depending on the surgical
need• During surgery stress on the cornea is minimal, because only moderate pressure is exerted on the eye• The risk of infection is significantly reduced

Intracorneal ring segments
ComplicationsUndercorrection
Overcorrection
Migration of rings
Extrusion or progressive thinning
New vessel formation
glare /halos
Lamellar keratoplasty
-LKP has been shown to result in less endothelial cell loss, less IOP problems than PKP , a reduction in rejection episodes, &, in some cases, a reduction of induced astigmatism.
-This technique requires less recovery time, and poses less chance for corneal graft rejection or failure.
-However, while some series have achieved comparable visual outcomes, others have demonstrated that penetrating techniques
slightly outperform deep lamellar procedure.

LK• Indications of DALK regarding KC: Anterior corneal scars Advanced disease with stress lines and clear cornea K-max > 65 dptThinnest location < 350 m Very high refractive error (sphere > −6 and/or cylinder > −6)

Penetrating keratoplasty
Between 10% & 25% of cases of KC progress to point where visual rehabilitation is no longer possible, especially in those who present at a young age (younger than 20) and with keratometry measurements > 60 dpt & corneal thickness < 400 m at the thinnest location. In the past, such patients have had only one option: a full thickness corneal transplant . KC is one of the most common
indications for penetrating keratoplasty accounting for 15–25% of such surgeries
Penetrating keratoplasty
As the cornea is avascular, the donor and host do not have to be tissue matched and eye banks – after checking for communicable diseases and tissue quality – can provide
suitable tissue within a few days or weeks. Following surgery, visual recovery takes several weeks/ months, with full stabilization often taking up to a year after which time the sutures can be removed.
PKPCorneal transplantation in KC is considered relatively low risk, in terms of graft rejection and other postoperative complications, as these eyes do not typically exhibit corneal neovascularization.
Despite these facts, there are reportedcomplications such as allograft rejection, iatrogenic astigmatism, significant endothelial cell loss .

PKPWhen the life expectancy is long, side effects caused by long-term use of topical steroids (e.g., secondary glaucoma and cataract), and recurrence of KC on the graft itself. Clear grafts are obtained in 95% of cases but optical outcomes may be unsatisfactory
because of the iatrogenic astigmatism and anisometropia. Between 30% and 50% of grafted eyes still require contact lens correction for best acuity or further keratorefractive surgical procedures

Phakic IOLSUsed to correct high myopia and associated
astigmatism of selected keratoconus patients.
Anterior chamber phakic intraocular lens have also been combined with intacs with good results.
The Intacs implantation is followed by toric phakic intraocular lens implantation to correct the residual myopic and astigmatic refractive error

Recent Advances• Keraflex KXL-It is the newest procedure under investigation for the treatment of keratinous -It is non incisional and reshapes the cornea without removing any tissue-It is currently under clinical investigation in Europe for treating myopia and keratoconus-It involves the delivery of a single low energy microwave pulse lasting less than one second to the cornea-Energy is applied to the cornea using a dielectrically shielded microwave emitter which contacts the epithelial surface-Through capacitive coupling, the single pulse raises the temperature of the selected region of corneal stroma to approximately 65 degree celsius, forming a doughnut shaped area of collagen shrinkage in the upper 150 microns of the stroma

• The lesion created during keraflex is intended to flatten the central cornea both to decrease the cone in keratoconus and to achieve myopic correction
• In order to improve the stability of the cornea with keraflex, Keraflex KXL includes focal corneal collagen cross linking
• After the actual Keraflex procedure, riboflavin drops are administered over the treatment area, a mask is applied to protect the central and peripheral areas of the cornea, and uv light is administered to crosslink the collagen.

Final Summary-Anyone with progressive ectasia should undergo CXL no matter what age or level of vision (assuming the eye was an appropriate candidate).
not to proceed with surgery (other than CXL) -If patients were satisfied with their vision with glasses or contact lenses. ICRS may be considered. phakic IOLs should be used less often
Final summary-A strong preference for DALK when a corneal transplant was needed, unless eye had previous compromise of Descemet membrane (most commonly from acute hydrops), at which point the preference is for a PK.
- pdDALK may be considered even in the presence of previous hydrops.
Related Documents











