Keratoconus

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Keratoconus
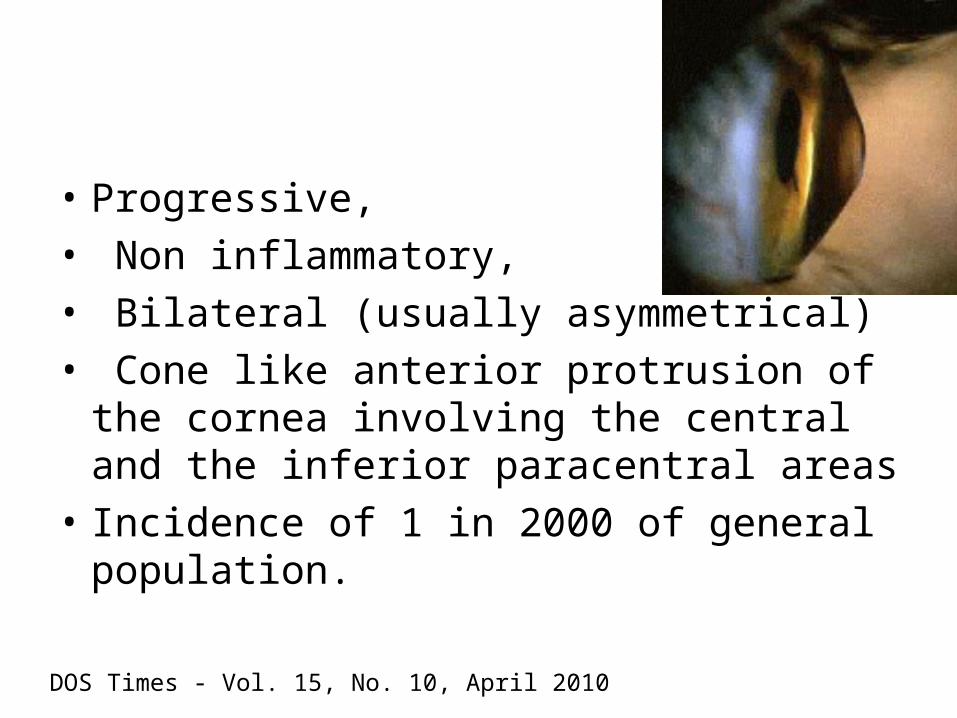
• Progressive,
• Non inflammatory,
• Bilateral (usually asymmetrical)
• Cone like anterior protrusion of the cornea involving the central and the inferior paracentral areas
• Incidence of 1 in 2000 of general population.
DOS Times - Vol. 15, No. 10, April 2010

• Usually seen after puberty
• No gender predominance
• No race predominance
• The patient becomes myopic but the error of refraction cannot be satisfactorily corrected with ordinary glasses owing to parabolic nature of the curvature which leads to irregular astigmatism.

• Abortive/forme fruste /sub clinical keratoconus is seen in family members or the fellow eye.
• No frank clinical sign
• The cornea is at risk of developing keratoconus at a later stage and can be diagnosed only by videokeratography.
DOS Times - Vol.10, No. 7 January 2005

Etiology
• Various theories:- • Thinning may be due to• Defective formation/destruction of extracellular
matrix• Abnormal collagenase activity.• Increased levels of proteases &catabolic
enzymes in the basal epithelial cells• Decreased levels of proteinase inhibitors alpha 1
proteinase inhibitor and alpha 2 macroglobulin

• Excessive eye rubbing or atopic disease-
• induces keratoconus by inducing epithelial damage-----epithelial stress----increased keratocyte apoptosis through interluekin 1 causing changes in stomal matrix
• Hard contact lens wear
• 6-15 % positive family history.

• The role of heredity :
not been clearly established. .
• In some cases, however, a sex-linked autosomal dominant mode of inheritance, particularly because of the predominance of familial females with keratoconus.

Systemic associations• Atopy • Down syndrome• Turner syndrome• Ehlers –danlos syndrome• Marfans syndrome• Osteogenesis imperfecta• Floppy eyelid syndrome• Oculodentodigital syndrome• Rieger's syndrome • Focal dermal hypoplasia• Nail -patella syndrome• Apert's syndrome• craniofacial dysostosis (Crouzon's syndrome)
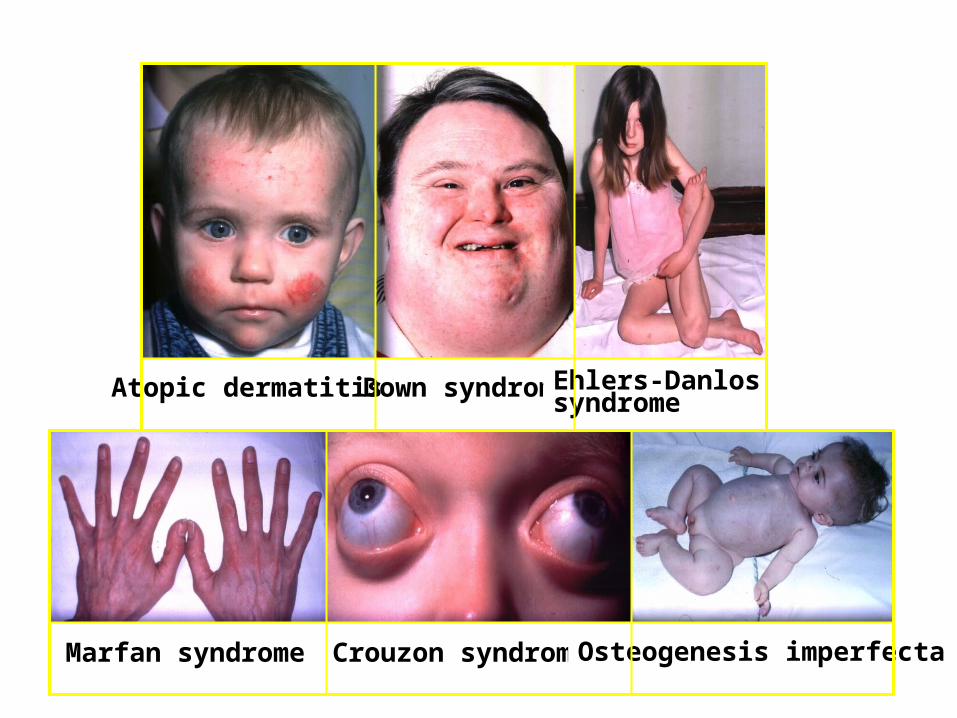
Crouzon syndromeMarfan syndrome Osteogenesis imperfecta
Atopic dermatitis Down syndrome Ehlers-Danlos syndrome

Ocular association• Vernal keratoconjunctivitis• RP• Leber’s congenital amaurosis• Retinopathy of prematurity• Progressive cone dystrophy• Aniridia • Iridoschisis • Iris atrophy• Fuchs' dystrophy• Posterior polymorphous dystrophy• Granular and lattice dystrophies
Symptoms
• Progressive visual blurring and/or distortion
• Rapidly changing spectacle prescription
• Eye rubbing
• Photophobia
• Glare
• Monocular diplopia
• Sudden onset of pain, redness, loss of vision, and photophobia suggests hydrops
• The onset of keratoconus occurs predominantly in the late teens.
• Symptoms usually appear bilaterally, but it is common to have an asymmetric presentation.
• During the first 5-7 years of onset, the condition generally worsens with intermittent periods of remissions
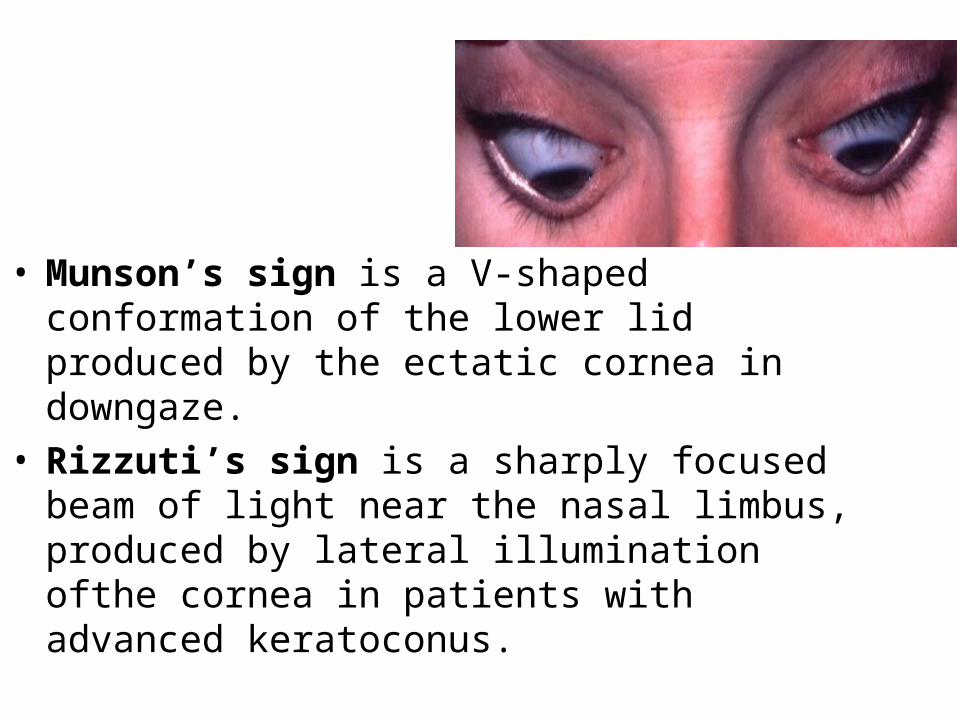
• Munson’s sign is a V-shaped conformation of the lower lid produced by the ectatic cornea in downgaze.
• Rizzuti’s sign is a sharply focused beam of light near the nasal limbus, produced by lateral illumination ofthe cornea in patients with advanced keratoconus.

Slit lamp examination
• Prominent corneal nerves

Slit lamp examination
• Fleischer's Ring – The Fleischer ring is a yellow-brown to
olive-green ring of pigment which may or may not completely surround the base of the cone
– Formed when hemosiderin (iron) pigment is deposited deep in the epithelium
– Fleischer's ring often becomes thinner and more discrete with progression
• seen approximately 50% of all cases.
• Locating this ring initially may be made easier by using a cobalt filter and carefully focusing on the superior half of the cornea's epithelium.
• Once located, the ring should be viewed in white light to assess its extent.


• Lines of Vogt:• small and brushlike lines, generally vertical but they can
be oblique. • Found in the deep layers of the stroma and form along
the meridian of greatest curvature.• Disappear when gentle pressure is exerted on the globe
through the lid.

• Corneal Thinning:
• Significant thinning (up to 1/5th cornea thickness) in the advanced stages of the disease and a diagnostic criterion based on comparison of central and peripheral corneal thickness has been proposed.
• Additionally, as the disease progresses, the cone is often displaced inferiorly. The steepest part of the cornea (apex) is generally the thinnest.

• Corneal Scarring:
• Sub-epithelial corneal scarring, not generally seen early, may occur as keratoconus progresses because of ruptures in Bowman's membrane which is then filled with connective tissue
• Deep opacity of the cornea are also common in keratoconus.


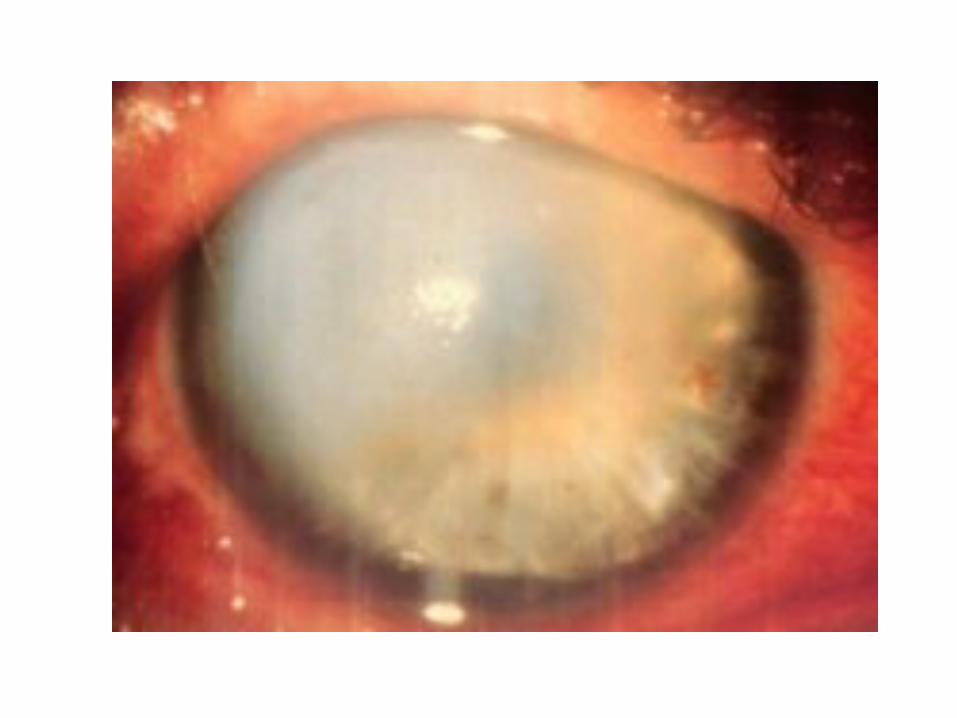
Corneal Hydrops:
• Corneal hydrops occurs in advanced cases, when Descemet's membrane ruptures, aqueous flows into the cornea and reseals
• Keratoconus patients who are having an acute episode of corneal hydrops report a sudden loss of vision and a visible white spot on the cornea.
• Corneal hydrops causes edema and opacification.

• As Descemet's regenerates, edema and opacification diminish. Occasionally, hydrops can benefit keratoconus patients who have extremely steep corneas. If the cornea scars, a flatter cornea often results, making it easier to fit with a contact lens.
• An increased incidence of hydrops has also been reported in keratoconus patients with Down's syndrome.

Diagnosis
• Early keratoconus usually manifests as a small island of irregular astigmatism in the inferior paracentral cornea.
• As the cornea bulges outward, the amount of astigmatism increases due to the progressive distortion of the corneal surface.
• These changes can easily be seen as irregular mires on keratometry readings and on corneal topography, a test used to map the topographical surface area of the cornea

• Many objective signs are present in keratoconus.
• Retinoscopy shows a scissoring reflex.• Direct ophthalmoscopy may show a
shadow If the pupil is dilated and a +6.00 D lens is in the ophthalmoscopic system, the cone may appear as an oil or honey droplet when the red reflex is observed-Charleux” oil droplet sign

• The photokeratoscope or topographer placido disc can provide an overview of the cornea and can show the relative steepness of any corneal area.
• The even separation of the rings in the spherical cornea ".

Placido disc
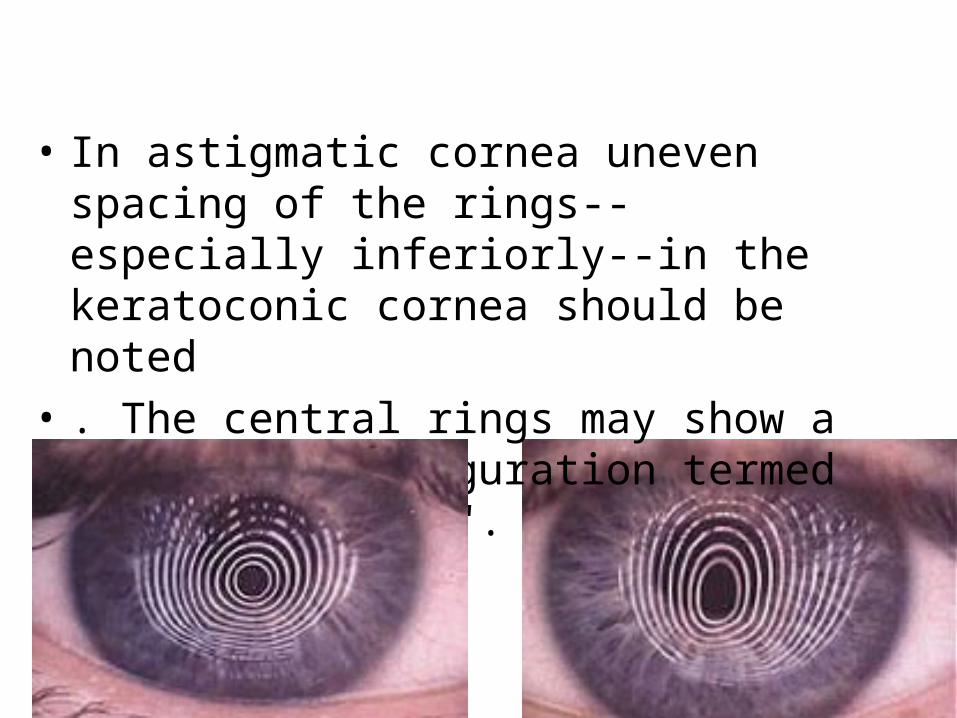
• In astigmatic cornea uneven spacing of the rings--especially inferiorly--in the keratoconic cornea should be noted
• . The central rings may show a tear-drop configuration termed "keratokyphosis".
DOS Times - Vol.10, No. 7 January 2005
• With the handheldkeratoscopes, such as the Klein keratoscope,early keratoconus is characterized by a downward deviation of the horizontal axis of the Placido disk reflection
• The keratometer also aids diagnosis.
• The initial keratometric sign of keratoconus is absence of parallelism and inclination of the mires. These can easily be missed in mild or early cases.

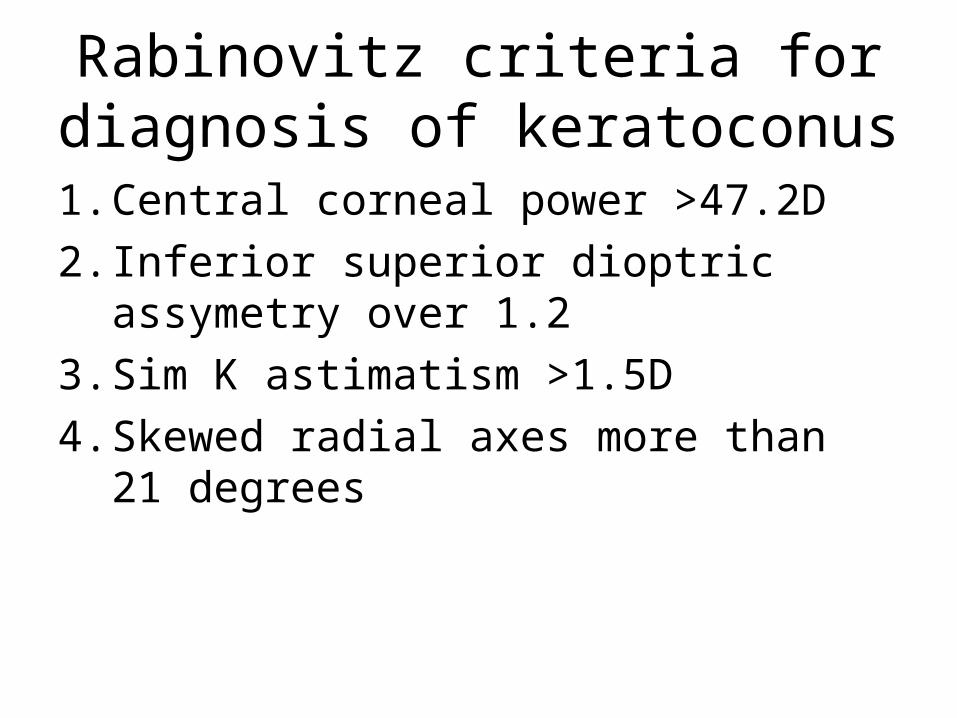
Rabinovitz criteria for diagnosis of keratoconus
1. Central corneal power >47.2D
2. Inferior superior dioptric assymetry over 1.2
3. Sim K astimatism >1.5D
4. Skewed radial axes more than 21 degrees
Corneal topography
• Provides a color coded map of the corneal surface.
• The power in diopters of the steepest and flattest meridians and their axes are calculated and displayed
• Steep curvatures are marked orange or red
• Flat curvature in blue or violet• Normal curvatures in green or yellow

Classification scheme of normal videokeratographsin the absolute scale devised as a baseline to monitortopographic progression to keratoconus A, round:B, oval: C, superior steepening; D, inferior steepening; E,irregular; F, symmetric bow tie; G, symmetric bow tie withskewed radial axes; H, asymmetric bow tie with inferiorsteepening (AB/IS); I, asymmetric bow tie with superiorsteepening; J, asymmetric bow tie with skewed radial axes(AB/SRAX
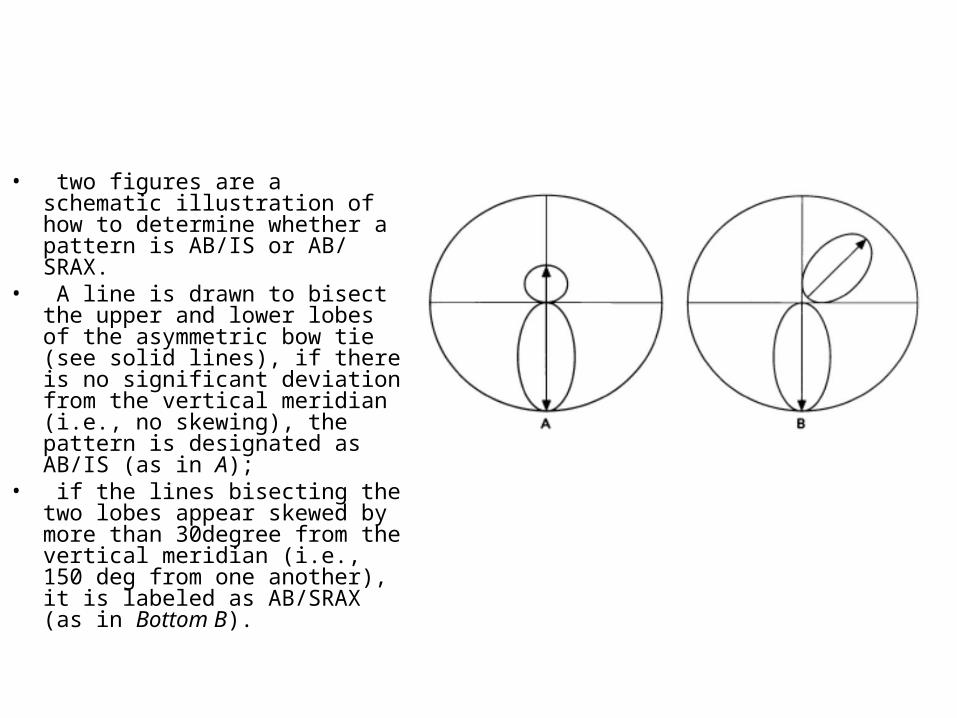
• two figures are a schematic illustration of how to determine whether a pattern is AB/IS or AB/ SRAX.
• A line is drawn to bisect the upper and lower lobes of the asymmetric bow tie (see solid lines), if there is no significant deviation from the vertical meridian (i.e., no skewing), the pattern is designated as AB/IS (as in A);
• if the lines bisecting the two lobes appear skewed by more than 30degree from the vertical meridian (i.e., 150 deg from one another), it is labeled as AB/SRAX (as in Bottom B).

Management of Keratoconus
• Spectacles• Mild keratoconus can be corrected with
spectacles.• Retinoscopy is difficult;• a normal subjective refraction is required. • Monocular keratoconus is usually best
dealt with using spectacle correction. • In this group of patients, motivation for
contact lens wear tends to be poor.
Related Documents











