Keratoameloblastoma: a tumor sui generis or a chimera? Joseph C. Whitt, DDS, MS, a Charles L. Dunlap, DDS, b John L. Sheets, DDS, c and Michael L. Thompson, DDS, d Kansas City, MO, Cape Girardeau, MO, and Jonesboro, AR UNIVERSITY OF MISSOURI KANSAS CITY AND PRIVATE PRACTICES The term keratoameloblastoma has been used to describe a histologically heterogeneous group of ameloblastoma variants which have in common the formation of keratin by the ameloblastomatous epithelium. The English language literature contains reports of only 12 cases of keratoameloblastoma, of which 4 cases exhibited a papilliferous component. We report a unique tumor that we believe falls within the broad histopathologic spectrum of keratoameloblastoma. We review the key clinical and histopathologic features of the previously reported cases of keratoameloblastoma and present an additional case that presented as an expansile, radiolucent lesion with internal opacification between the roots of teeth in the left anterior maxillary alveolar ridge of a 45-year-old white male. There is wide variation in the histopathologic appearance of cases reported under the appellation keratoameloblastoma. Our case exhibited a histopathologic feature shared by only 2 of the previously reported cases, notably islands and anastomosing cords of epithelium forming lamellated, pacinian-like stacks of parakeratin that extruded into the collagenous tumor stroma without eliciting a foreign body response. Due to the small number of reported cases, we are unable to accurately assess whether the biologic behavior of keratoameloblastoma differs from other histologic types of ameloblastoma. (Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007;104:368-76) The appellation keratoameloblastoma has been applied to ameloblastomas that exhibit evidence of keratin pro- duction to varying degrees. Keratin formation in amelo- blastomas may take various forms. Squamous metapla- sia within the stellate reticulum-like areas of ameloblastoma is a well-recognized feature that is the histologic hallmark of the acanthomatous variant of ameloblastoma. 1 It has long been recognized that kera- tinization in acanthomatous ameloblastomas may progress to keratin pearl formation in the central por- tion of the epithelial follicles. 2-4 The English language literature reports 12 lesions classified as keratoameloblastoma. A major distinction in these reports is whether or not the lesion exhibited a papilliferous component. Despite the similarity of names, keratoameloblastoma and papilliferous kera- toameloblastoma are distinct morphologically. Pind- borg 5 first proposed the term keratoameloblastoma for use as a diagnostic entity, although some 6-8 erroneously attribute this to his 1958 publication, 9 rather than to his 1970 publication. 5 In his report, Pindborg described a histologic variant of ameloblastoma, which he termed papilliferous ameloblastoma. 5 This lesion exhibited a growth pattern consisting of both epithelial follicles exhibiting central microcyst formation with keratiniza- tion and follicles exhibiting a papilliferous lining epi- thelium. Subsequently, 3 additional cases of ameloblas- toma with a papilliferous component were reported in 1991, 10 1994, 11 and 2002, 12 bringing the number of case reports of ameloblastoma with papilliferous fea- tures in the English language literature to 4 (Tables I and II). The remaining 8 cases without a papilliferous histologic component were reported under the terms This paper was presented at the 60th Annual Meeting of the Amer- ican Academy of Oral and Maxillofacial Pathology, San Antonio, TX, April 25, 2006. a Associate Professor, Oral and Maxillofacial Pathology, School of Dentistry, University of Missouri School of Dentistry. b Professor, Oral and Maxillofacial Pathology, School of Dentistry, University of Missouri School of Dentistry. c Oral and Maxillofacial Surgeon, Private Practice, Cape Girardeau, MO. d Periodontist, Private Practice, Jonesboro, AR. Received for publication Jul 6, 2006; returned for revision Jul 24, 2006; accepted for publication Jul 25, 2006. 1079-2104/$ - see front matter © 2007 Mosby, Inc. All rights reserved. doi:10.1016/j.tripleo.2006.07.025 368 Vol. 104 No. 3 September 2007 ORAL AND MAXILLOFACIAL PATHOLOGY Editor: Mark W. Lingen

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Vol. 104 No. 3 September 2007
ORAL AND MAXILLOFACIAL PATHOLOGY Editor: Mark W. Lingen
Keratoameloblastoma: a tumor sui generis or a chimera?Joseph C. Whitt, DDS, MS,a Charles L. Dunlap, DDS,b John L. Sheets, DDS,c andMichael L. Thompson, DDS,d Kansas City, MO, Cape Girardeau, MO, and Jonesboro, ARUNIVERSITY OF MISSOURI KANSAS CITY AND PRIVATE PRACTICES
The term keratoameloblastoma has been used to describe a histologically heterogeneous group ofameloblastoma variants which have in common the formation of keratin by the ameloblastomatous epithelium. TheEnglish language literature contains reports of only 12 cases of keratoameloblastoma, of which 4 cases exhibited apapilliferous component. We report a unique tumor that we believe falls within the broad histopathologic spectrum ofkeratoameloblastoma. We review the key clinical and histopathologic features of the previously reported cases ofkeratoameloblastoma and present an additional case that presented as an expansile, radiolucent lesion with internalopacification between the roots of teeth in the left anterior maxillary alveolar ridge of a 45-year-old white male. Thereis wide variation in the histopathologic appearance of cases reported under the appellation keratoameloblastoma. Ourcase exhibited a histopathologic feature shared by only 2 of the previously reported cases, notably islands andanastomosing cords of epithelium forming lamellated, pacinian-like stacks of parakeratin that extruded into thecollagenous tumor stroma without eliciting a foreign body response. Due to the small number of reported cases, weare unable to accurately assess whether the biologic behavior of keratoameloblastoma differs from other histologic
types of ameloblastoma. (Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007;104:368-76)The appellation keratoameloblastoma has been appliedto ameloblastomas that exhibit evidence of keratin pro-duction to varying degrees. Keratin formation in amelo-blastomas may take various forms. Squamous metapla-sia within the stellate reticulum-like areas ofameloblastoma is a well-recognized feature that is thehistologic hallmark of the acanthomatous variant ofameloblastoma.1 It has long been recognized that kera-tinization in acanthomatous ameloblastomas may
This paper was presented at the 60th Annual Meeting of the Amer-ican Academy of Oral and Maxillofacial Pathology, San Antonio,TX, April 25, 2006.aAssociate Professor, Oral and Maxillofacial Pathology, School ofDentistry, University of Missouri School of Dentistry.bProfessor, Oral and Maxillofacial Pathology, School of Dentistry,University of Missouri School of Dentistry.cOral and Maxillofacial Surgeon, Private Practice, Cape Girardeau,MO.dPeriodontist, Private Practice, Jonesboro, AR.Received for publication Jul 6, 2006; returned for revision Jul 24,2006; accepted for publication Jul 25, 2006.1079-2104/$ - see front matter© 2007 Mosby, Inc. All rights reserved.
doi:10.1016/j.tripleo.2006.07.025368
progress to keratin pearl formation in the central por-tion of the epithelial follicles.2-4
The English language literature reports 12 lesionsclassified as keratoameloblastoma. A major distinctionin these reports is whether or not the lesion exhibited apapilliferous component. Despite the similarity ofnames, keratoameloblastoma and papilliferous kera-toameloblastoma are distinct morphologically. Pind-borg5 first proposed the term keratoameloblastoma foruse as a diagnostic entity, although some6-8 erroneouslyattribute this to his 1958 publication,9 rather than to his1970 publication.5 In his report, Pindborg described ahistologic variant of ameloblastoma, which he termedpapilliferous ameloblastoma.5 This lesion exhibited agrowth pattern consisting of both epithelial folliclesexhibiting central microcyst formation with keratiniza-tion and follicles exhibiting a papilliferous lining epi-thelium. Subsequently, 3 additional cases of ameloblas-toma with a papilliferous component were reported in1991,10 1994,11 and 2002,12 bringing the number ofcase reports of ameloblastoma with papilliferous fea-tures in the English language literature to 4 (Tables Iand II). The remaining 8 cases without a papilliferous
histologic component were reported under the terms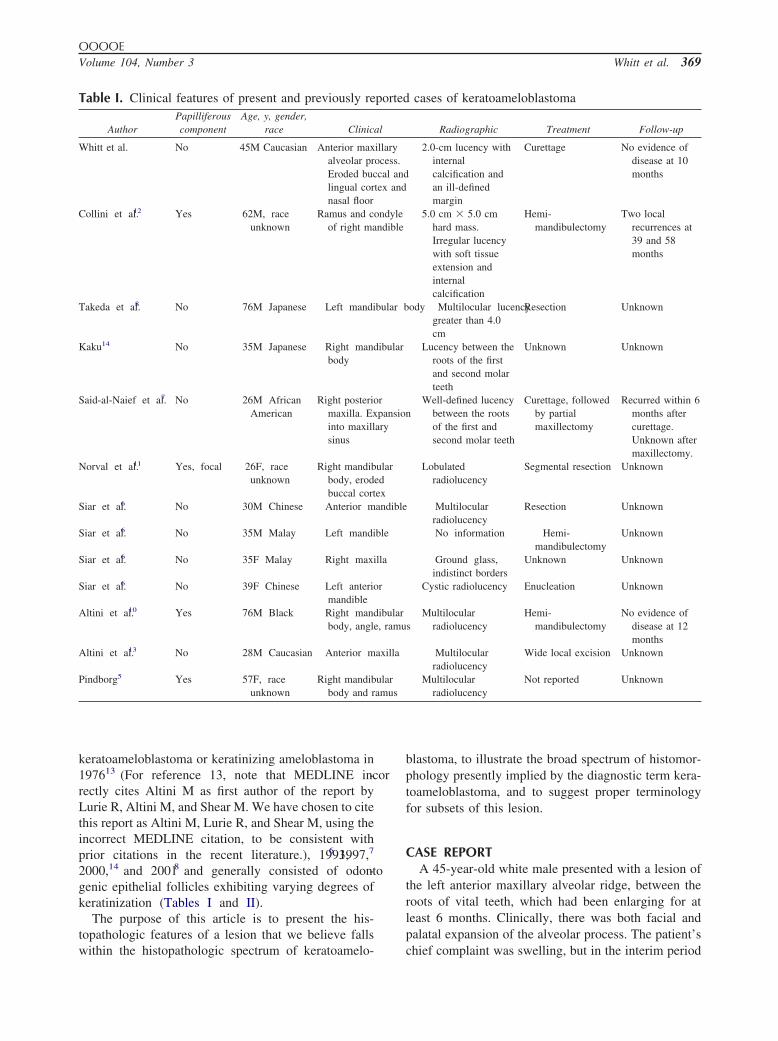
amus
OOOOEVolume 104, Number 3 Whitt et al. 369
keratoameloblastoma or keratinizing ameloblastoma in197613 (For reference 13, note that MEDLINE incor-rectly cites Altini M as first author of the report byLurie R, Altini M, and Shear M. We have chosen to citethis report as Altini M, Lurie R, and Shear M, using theincorrect MEDLINE citation, to be consistent withprior citations in the recent literature.), 1993,6 1997,7
2000,14 and 20018 and generally consisted of odonto-genic epithelial follicles exhibiting varying degrees ofkeratinization (Tables I and II).
The purpose of this article is to present the his-topathologic features of a lesion that we believe falls
Table I. Clinical features of present and previously re
AuthorPapilliferouscomponent
Age, y, gender,race Clinic
Whitt et al. No 45M Caucasian Anterior maxalveolar prEroded buclingual cornasal floor
Collini et al.12 Yes 62M, raceunknown
Ramus and cof right ma
Takeda et al.8 No 76M Japanese Left mandibu
Kaku14 No 35M Japanese Right mandibbody
Said-al-Naief et al.7 No 26M AfricanAmerican
Right posteriomaxilla. Exinto maxillsinus
Norval et al.11 Yes, focal 26F, raceunknown
Right mandibbody, erodbuccal cort
Siar et al.6 No 30M Chinese Anterior man
Siar et al.6 No 35M Malay Left mandible
Siar et al.6 No 35F Malay Right maxilla
Siar et al.6 No 39F Chinese Left anteriormandible
Altini et al.10 Yes 76M Black Right mandibbody, angle
Altini et al.13 No 28M Caucasian Anterior max
Pindborg5 Yes 57F, raceunknown
Right mandibbody and r
within the histopathologic spectrum of keratoamelo-
blastoma, to illustrate the broad spectrum of histomor-phology presently implied by the diagnostic term kera-toameloblastoma, and to suggest proper terminologyfor subsets of this lesion.
CASE REPORTA 45-year-old white male presented with a lesion of
the left anterior maxillary alveolar ridge, between theroots of vital teeth, which had been enlarging for atleast 6 months. Clinically, there was both facial andpalatal expansion of the alveolar process. The patient’s
cases of keratoameloblastoma
Radiographic Treatment Follow-up
2.0-cm lucency withinternalcalcification andan ill-definedmargin
Curettage No evidence ofdisease at 10months
5.0 cm � 5.0 cmhard mass.Irregular lucencywith soft tissueextension andinternalcalcification
Hemi-mandibulectomy
Two localrecurrences at39 and 58months
y Multilocular lucencygreater than 4.0cm
Resection Unknown
Lucency between theroots of the firstand second molarteeth
Unknown Unknown
Well-defined lucencybetween the rootsof the first andsecond molar teeth
Curettage, followedby partialmaxillectomy
Recurred within 6months aftercurettage.Unknown aftermaxillectomy.
Lobulatedradiolucency
Segmental resection Unknown
Multilocularradiolucency
Resection Unknown
No information Hemi-mandibulectomy
Unknown
Ground glass,indistinct borders
Unknown Unknown
Cystic radiolucency Enucleation Unknown
sMultilocular
radiolucencyHemi-
mandibulectomyNo evidence of
disease at 12months
Multilocularradiolucency
Wide local excision Unknown
Multilocularradiolucency
Not reported Unknown
ported
al
illaryocess.cal and
tex and
ondylendible
lar bod
ular
rpansionary
ularedexdible
ular, ramu
illa
ular
chief complaint was swelling, but in the interim period
OOOOE370 Whitt et al. September 2007
Table II. Histologic features of present and previously reported cases of keratoameloblastomaAuthor Histopathologic appearance*
Whitt et al. Complex histology- Two types of epithelial structures in a collagenous fibrous connective tissue stroma- Cystic follicles filled with parakeratin, orthokeratin, and necrotic material with calcification and lined by stratified
squamous epithelium exhibiting hyperchromatic, palisaded basal cells with focal reverse polarity and subnuclearvacuolation
- Curvilinear ribbons of similar-appearing odontogenic epithelium within the fibrous connective tissue extrudingpacinian-like stacks of lamellated parakeratin directly into the connective tissue without foreign body response
- Peripheral areas resembling odontogenic keratocystCollini et al.12 Papilliferous histology
- Cysts lined by monolayered epithelium forming micropapillary projections and true papillary projections- Cyst lumena containing necrotic debris- Cribiform and solid areas with squamous metaplasia- Tubular structures in a desmoplastic stroma- Focal areas resembling granular cell ameloblastoma- Poorly differentiated patterns and rare necrotic foci
Takeda et al.8 Complex histology- Multicystic spaces lined by papillary projections of odontogenic epithelium with connective tissue cores- Odontogenic epithelium with stellate reticulumlike areas and palisaded basal layer of tall, columnal ameloblastlike cells- Extensive surface parakeratinization with lamellar accumulation of keratin forming “hair-like” structures- Extrusion of keratin into connective tissue- Stromal hard tissue formation resembling cementum and woven bone
Kaku14 Simple histology- Histologic features based on description in published abstract- Cystic follicles filled with parakeratin and orthokeratin- Follicles lined by columnar cells with nuclear polarization
Said-al-Naief et al.7 Simple histology with OKC-like features- Epithelial follicles containing central solid masses of parakeratin and orthokeratin lined by edematous stratified
squamous epithelium with palisaded cuboidal basal cells with hyperchromatic nuclei exhibiting focal reversed polarity- Cystic areas resembling conventional odontogenic keratocyst
Norval et al.11 Complex histology- Two types of epithelial follicles in a scanty fibrous connective tissue stroma- Cystic follicles filled with parakeratin, orthokeratin and necrotic material with calcification- Basal cells with reverse polarity and subnuclear vacuolation- Microcysts lined by either a multilayered papilliferous or single-layered, hob-nailed epithelium- Extrusion of keratin into fibrous connective tissue with foreign body reaction (published photomicrograph does not
exhibit a foreign body response)Siar et al.6 Simple histology with OKC-like features. Four cases of similar histology consisting of the following:
- Solid and cystic epithelial tumor areas- Solid areas consisted of discrete and interconnecting islands of odontogenic epithelium with marked central
keratinization and peripheral palisading- Cystic areas lined by thin stratified squamous epithelium of uniform thickness with palisaded basal layer and an
orthokeratotic and/or parakeratotic surface- Collagenous fibrous connective tissue stroma- Tumor islands infiltrating cancellous bone
Altini et al.10 Papilliferous histology- Two types of epithelial follicles separated by bands of fibrous connective tissue- Predominately, a cystic type of epithelial follicle filled with necrotic debris and sometimes parakeratin, lined by
papilliferous epithelium with some true papillary projections.- A minority of epithelial follicles lined by parakeratinized stratified squamous epithelium.- Histomorphologic features of ameloblastoma absent
Altini et al.13 Simple histology- Epithelial follicles with central microcysts lined by parakeratin- Basal layer of follicles exhibiting palisaded cuboidal cells with nuclei oriented away from the basement membrane
Pindborg5 Papilliferous histology- Two types of epithelial follicles- One type forming keratinizing cysts- The other type forming tumor islands with a papilliferous appearance- The histomorphologic features of ameloblastoma were not described or illustrated
*The histologic types Papilliferous, Simple, Simple with odontogenic keratocyst (OKC)-like features, and Complex are defined in the Discussion
section.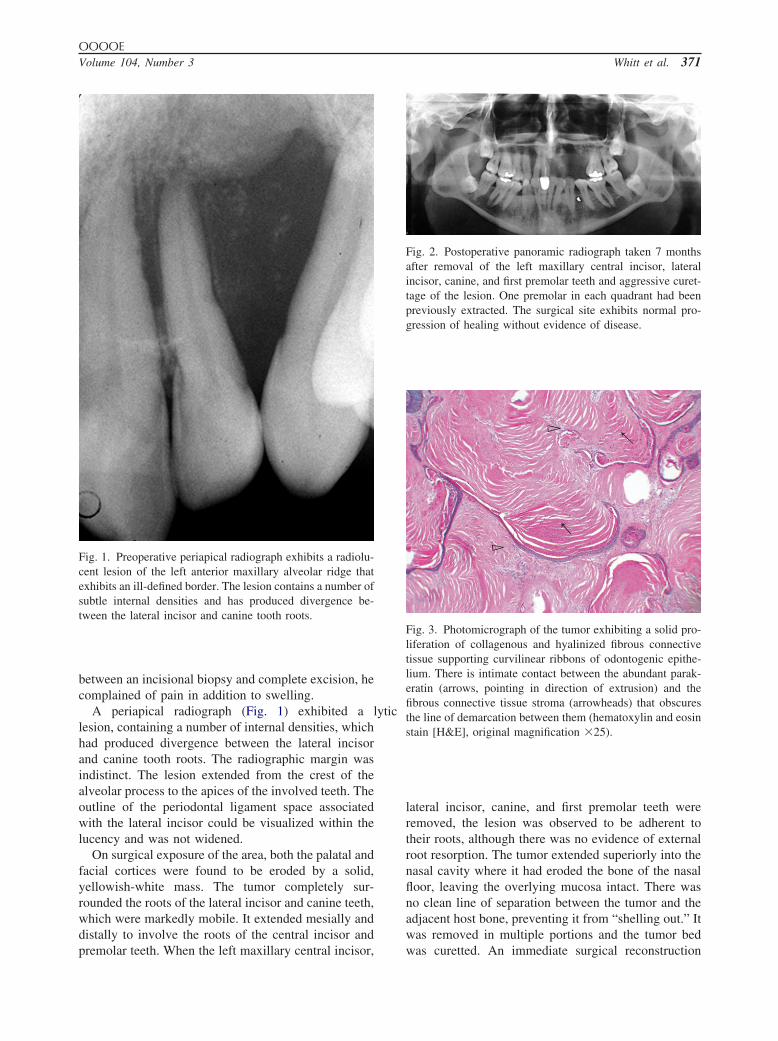
OOOOEVolume 104, Number 3 Whitt et al. 371
between an incisional biopsy and complete excision, hecomplained of pain in addition to swelling.
A periapical radiograph (Fig. 1) exhibited a lyticlesion, containing a number of internal densities, whichhad produced divergence between the lateral incisorand canine tooth roots. The radiographic margin wasindistinct. The lesion extended from the crest of thealveolar process to the apices of the involved teeth. Theoutline of the periodontal ligament space associatedwith the lateral incisor could be visualized within thelucency and was not widened.
On surgical exposure of the area, both the palatal andfacial cortices were found to be eroded by a solid,yellowish-white mass. The tumor completely sur-rounded the roots of the lateral incisor and canine teeth,which were markedly mobile. It extended mesially anddistally to involve the roots of the central incisor and
Fig. 1. Preoperative periapical radiograph exhibits a radiolu-cent lesion of the left anterior maxillary alveolar ridge thatexhibits an ill-defined border. The lesion contains a number ofsubtle internal densities and has produced divergence be-tween the lateral incisor and canine tooth roots.
premolar teeth. When the left maxillary central incisor,
lateral incisor, canine, and first premolar teeth wereremoved, the lesion was observed to be adherent totheir roots, although there was no evidence of externalroot resorption. The tumor extended superiorly into thenasal cavity where it had eroded the bone of the nasalfloor, leaving the overlying mucosa intact. There wasno clean line of separation between the tumor and theadjacent host bone, preventing it from “shelling out.” Itwas removed in multiple portions and the tumor bed
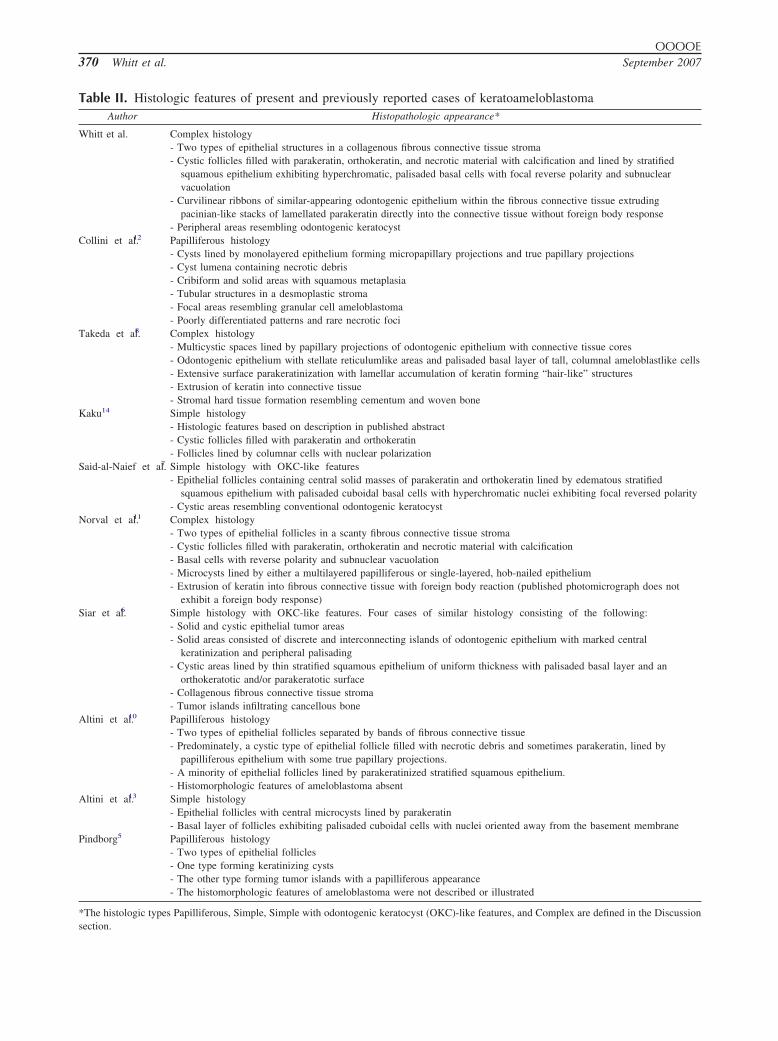
Fig. 2. Postoperative panoramic radiograph taken 7 monthsafter removal of the left maxillary central incisor, lateralincisor, canine, and first premolar teeth and aggressive curet-tage of the lesion. One premolar in each quadrant had beenpreviously extracted. The surgical site exhibits normal pro-gression of healing without evidence of disease.
Fig. 3. Photomicrograph of the tumor exhibiting a solid pro-liferation of collagenous and hyalinized fibrous connectivetissue supporting curvilinear ribbons of odontogenic epithe-lium. There is intimate contact between the abundant parak-eratin (arrows, pointing in direction of extrusion) and thefibrous connective tissue stroma (arrowheads) that obscuresthe line of demarcation between them (hematoxylin and eosinstain [H&E], original magnification �25).
was curetted. An immediate surgical reconstruction
OOOOE372 Whitt et al. September 2007
was not performed and function was restored with aremovable appliance. Healing progressed normally andthere was no evidence of recurrence of the lesion after10 months (Fig. 2).
Grossly, the surgical specimen was solid, with auniform, tan surface that cut with a gritty consistency.Histopathologic examination revealed a generally solid,unencapsulated lesion composed of a prominent collag-
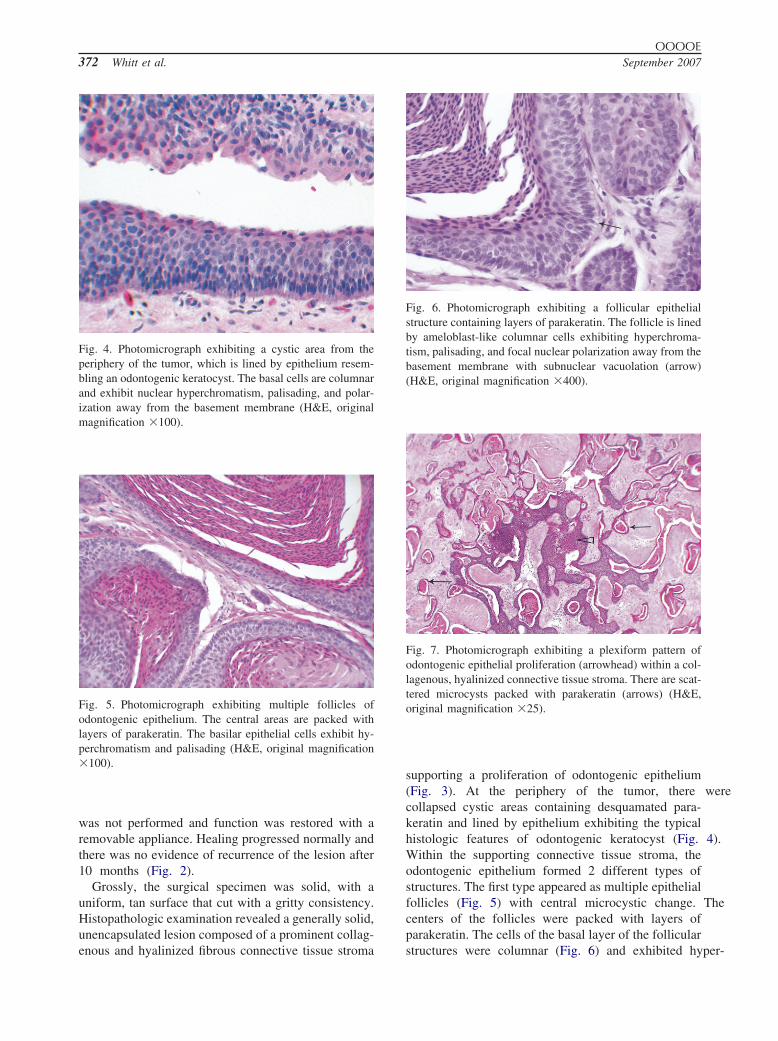
Fig. 4. Photomicrograph exhibiting a cystic area from theperiphery of the tumor, which is lined by epithelium resem-bling an odontogenic keratocyst. The basal cells are columnarand exhibit nuclear hyperchromatism, palisading, and polar-ization away from the basement membrane (H&E, originalmagnification �100).
Fig. 5. Photomicrograph exhibiting multiple follicles ofodontogenic epithelium. The central areas are packed withlayers of parakeratin. The basilar epithelial cells exhibit hy-perchromatism and palisading (H&E, original magnification�100).
enous and hyalinized fibrous connective tissue stroma
supporting a proliferation of odontogenic epithelium(Fig. 3). At the periphery of the tumor, there werecollapsed cystic areas containing desquamated para-keratin and lined by epithelium exhibiting the typicalhistologic features of odontogenic keratocyst (Fig. 4).Within the supporting connective tissue stroma, theodontogenic epithelium formed 2 different types ofstructures. The first type appeared as multiple epithelialfollicles (Fig. 5) with central microcystic change. Thecenters of the follicles were packed with layers ofparakeratin. The cells of the basal layer of the follicular
Fig. 6. Photomicrograph exhibiting a follicular epithelialstructure containing layers of parakeratin. The follicle is linedby ameloblast-like columnar cells exhibiting hyperchroma-tism, palisading, and focal nuclear polarization away from thebasement membrane with subnuclear vacuolation (arrow)(H&E, original magnification �400).
Fig. 7. Photomicrograph exhibiting a plexiform pattern ofodontogenic epithelial proliferation (arrowhead) within a col-lagenous, hyalinized connective tissue stroma. There are scat-tered microcysts packed with parakeratin (arrows) (H&E,original magnification �25).
structures were columnar (Fig. 6) and exhibited hyper-
OOOOEVolume 104, Number 3 Whitt et al. 373
chromatism and palisading, with focal reversed polarityand subnuclear vacuolation. The second type of epithe-lial structure consisted of curvilinear, sometimes anas-tomosing and plexiform ribbons of odontogenic epithe-lium within a collagenous, hyalinized connective tissuestroma (Fig. 7). The basal cells of the ribbons of odon-
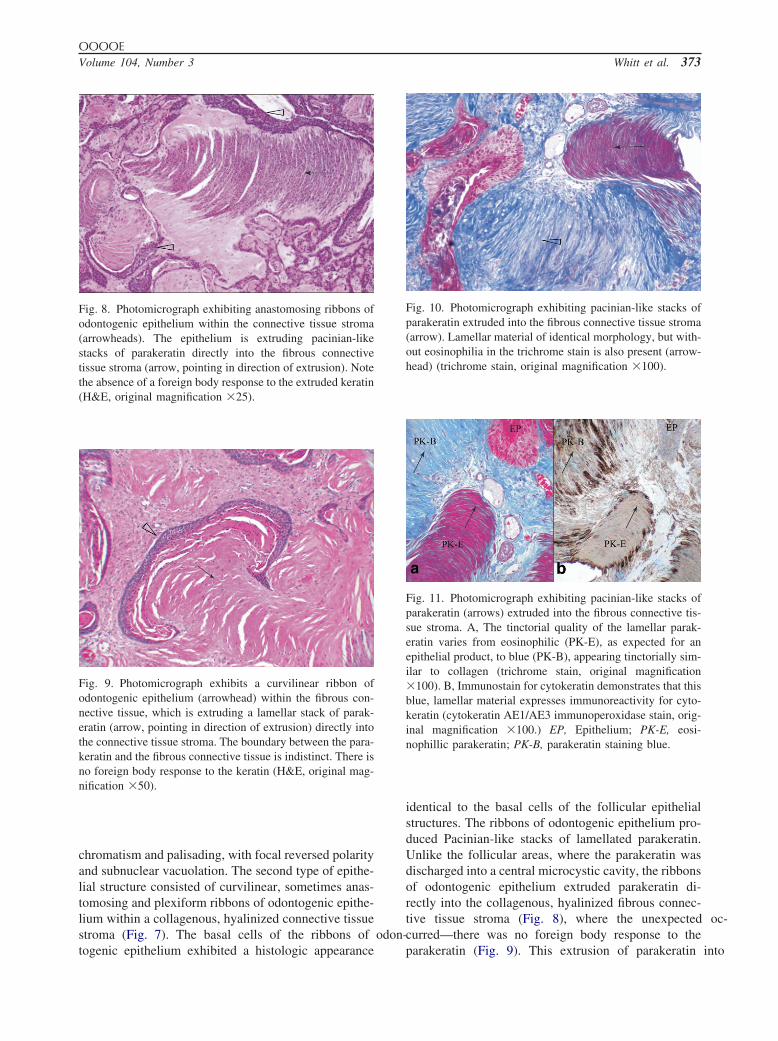
Fig. 8. Photomicrograph exhibiting anastomosing ribbons ofodontogenic epithelium within the connective tissue stroma(arrowheads). The epithelium is extruding pacinian-likestacks of parakeratin directly into the fibrous connectivetissue stroma (arrow, pointing in direction of extrusion). Notethe absence of a foreign body response to the extruded keratin(H&E, original magnification �25).
Fig. 9. Photomicrograph exhibits a curvilinear ribbon ofodontogenic epithelium (arrowhead) within the fibrous con-nective tissue, which is extruding a lamellar stack of parak-eratin (arrow, pointing in direction of extrusion) directly intothe connective tissue stroma. The boundary between the para-keratin and the fibrous connective tissue is indistinct. There isno foreign body response to the keratin (H&E, original mag-nification �50).
togenic epithelium exhibited a histologic appearance
identical to the basal cells of the follicular epithelialstructures. The ribbons of odontogenic epithelium pro-duced Pacinian-like stacks of lamellated parakeratin.Unlike the follicular areas, where the parakeratin wasdischarged into a central microcystic cavity, the ribbonsof odontogenic epithelium extruded parakeratin di-rectly into the collagenous, hyalinized fibrous connec-tive tissue stroma (Fig. 8), where the unexpected oc-curred—there was no foreign body response to the
Fig. 10. Photomicrograph exhibiting pacinian-like stacks ofparakeratin extruded into the fibrous connective tissue stroma(arrow). Lamellar material of identical morphology, but with-out eosinophilia in the trichrome stain is also present (arrow-head) (trichrome stain, original magnification �100).
Fig. 11. Photomicrograph exhibiting pacinian-like stacks ofparakeratin (arrows) extruded into the fibrous connective tis-sue stroma. A, The tinctorial quality of the lamellar parak-eratin varies from eosinophilic (PK-E), as expected for anepithelial product, to blue (PK-B), appearing tinctorially sim-ilar to collagen (trichrome stain, original magnification�100). B, Immunostain for cytokeratin demonstrates that thisblue, lamellar material expresses immunoreactivity for cyto-keratin (cytokeratin AE1/AE3 immunoperoxidase stain, orig-inal magnification �100.) EP, Epithelium; PK-E, eosi-nophillic parakeratin; PK-B, parakeratin staining blue.
parakeratin (Fig. 9). This extrusion of parakeratin into

OOOOE374 Whitt et al. September 2007
the stroma of the tumor was a frequent, widespread, anddefining feature of this neoplasm, present throughoutthe lesion, rather than a focal, isolated finding. Many ofthe lamellated stacks of parakeratin exhibited foci ofdystrophic calcification that contributed to the internalcalcification present on the preoperative intraoral radio-graph of the lesion. In hematoxylin and eosin sections,parakeratin and collagen blended. It was not possible toidentify the interface where one ended and the otherbegan, but Masson trichrome (Fig. 10) and cytokeratin(AE1/AE3) (Fig. 11) stains were helpful. A peculiarpicture emerged where the red stacks of parakeratingradually changed to the blue hue of collagen, produc-ing a “no man’s land,” a kerato-collagen mélange, andyet, no foreign body response. On cursory examinationof the tumor at scanning levels, mitotic activity did notappear striking. However, when formal counts of mi-totic activity were performed at a magnification of�400, the lesion exhibited a surprising number ofnormal-appearing mitotic figures. The mitotic rate was2.5 mitoses per 10 high-power fields, based on theaverage of the counts observed in 100 high-powerfields. Over two thirds of the basal and parabasal cellswere immunoreactive for Ki-67 with rare positive cellsabove this zone (Fig. 12). The Ki-67 proliferative indexwas 22.8%.
REVIEW OF THE LITERATUREThe clinical and histopathologic features of the 12
previously reported cases of keratoameloblastoma in
Fig. 12. Photomicrograph exhibiting nuclear localization ofKi-67 immunoreactivity. More than two thirds of the basaland parabasal cells are immunoreactive for Ki-67. There arerare positive cells above the basal and parabasal zone. Theproliferative fraction was 22.5% (Ki-67 immunoperoxidasestain, original magnification �100).
the English language literature and the present case are
summarized in Tables I and II. The aggregate averageage is 44 years with a range of 26 to 76 years. Theaverage age of cases with a papillary component is 55years with a range of 26 to 76 years. The average ageof cases without a papillary component is 40 years witha range of 26 to 76 years. There was a male predilectionwith a male-to-female ratio of 3:1. With regard to race,there was predominance for Asians.
Overall, the most commonly affected location wasthe posterior mandible (n � 7), with the posteriormaxilla, anterior maxilla, and anterior mandible equallyrepresented with 2 cases each. The cases with a papil-lary architecture were all located in the posterior man-dible. There was no site predilection for cases withouta papillary component. Three cases arose within thealveolar process between the roots of the teeth. The sizeof the lesion was available for only 3 cases and rangedfrom 2 cm to 5 cm in maximum dimension.
Although a description of the clinical symptoms wasnot available for most of the case reports, when de-scribed, they consisted of swelling and pain. The ra-diographic appearance was radiolucent. Three tumors,including the current case, exhibited densities withinthe lesion. Six cases were described as multilocularradiolucencies. Two cases were described as exhibitingindistinct margins and 1 case was described as havinga ground glass appearance.
Follow-up information is limited and is available foronly 3 cases. One patient with a lesion exhibiting apapilliferous component10 was free of disease at 12months. Our patient, whose lesion does not include apapilliferous component, was free of disease at 10months. The remaining patient for which follow-up isavailable, had a tumor that exhibited a papilliferouscomponent.12 He experienced local recurrences at 39months and at 58 months. The authors concluded thatthe histologic features, including a mitotic rate of 3mitoses per 10 high-power fields, the presence of ne-crosis, and the recurrent behavior of this lesion justifiedclassification as a carcinoma and asserted that the pap-illiferous ketatoameloblastoma represents a papillaryameloblastic carcinoma. One of the recurrences exhib-ited features of granular cell ameloblastoma. Local ordistant metastasis or death from disease was not re-ported in any of the cases.
DISCUSSIONIn 1992, the World Health Organization (WHO)
loosely defined keratoameloblastoma as an ameloblas-toma with extensive keratinization,15 although the cur-rent WHO Classification of Odontogenic Tumors1
makes no mention of the term. We believe this omis-
sion most likely reflects an editorial decision to limit
OOOOEVolume 104, Number 3 Whitt et al. 375
the classification to well-defined entities, rather than aretraction of prior nosology.
The WHO1 accepts focal keratinization, includingkeratin pearl formation, as within the histologic spec-trum of acanthomatous ameloblastoma, while O’Delland Morgan4 define an ameloblastoma with unequivo-cal keratinization occurring in the center of the epithe-lial follicles at the expense of the stellate reticulum-likeareas as a keratoameloblastoma. It is not clear howO’Dell and Morgan’s definition of keratoameloblas-toma differs from acanthomatous ameloblastoma, sincethe degree of keratin formation separating the two is notquantified. Norval et al.11 suggested that keratoamelo-blastoma should be considered a variant of acanthoma-tous ameloblastoma.
The histopathologic features of the group of 13 le-sions (Table II), including ours, reported under thediagnosis of keratoameloblastoma fall into 4 broadgroups: (1) papilliferous histology, (2) simple histol-ogy, (3) simple histology with odontogenic keratocyst(OKC)-like features, and (4) complex histology.
Four of the cases5,10-12 exhibited a papilliferous com-ponent. While Pindborg’s5 initial description of thepapilliferous ameloblastoma was spartan, Altini et al.10
thoroughly illustrate of the histomorphology of thislesion. The histomorphologic features of ameloblas-toma were absent in their lesion, as they were in Pind-borg’s.5 Since only 1 of the 411 showed convincingevidence of ameloblastoma, there is minimal evidencethat they are ameloblastomas and may represent a sep-arate entity.
Disregarding the presence or absence of a papilliferouscomponent, there is considerable variation in the histo-morphology of the remaining nonpapilliferous cases(Table II). Two of the lesions13,14 exhibited follicularameloblastoma with extensive keratinization (simple his-tology). This is the most straightforward group of lesionssince it meets the general criteria for keratoameloblastomaas set forth by the WHO15 and by O’Dell and Morgan.4
Five lesions6,7 exhibited follicular ameloblastoma withextensive keratinization and OKC-like areas (simple his-tology with OKC-like features). Said-al-Naief et al.7 sug-gested broadening the criteria for keratoameloblastoma toinclude this group of lesions. Three lesions, includingours,8,11 exhibited a more complex histomorphology, withepithelial follicles packed with parakeratin and ribbons ofepithelium forming lamellar stacks of parakeratin ex-truded into the stroma to varying degrees (complex his-tology). Although both reports of the lesions with com-plex histology described and illustrated parakeratinlocated in the stroma, they did not comment on the degreeto which it was present.
Active production of parakeratin in our tumor and
the presence of this material in the connective tissue isa most intriguing histopathologic feature. It raises thequestion of how such a unique morphology might de-velop. It is likely that the continuing active accumula-tion of keratin caused follicular rupture, followed byongoing extrusion of parakeratin directly into the con-nective tissue. Continued accumulation of parakeratincaused separation of the epithelial fragments, leading tothe histologic appearance of anastomosing ribbons ofepithelium.
The surprising lack of a foreign body response to theparakeratin raises the question of the subtypes of ker-atin proteins present. Although cytokeratin-10 has beenreported as specific for OKC,16 we were unable toinvestigate the keratin composition of our lesion be-yond a simple cytokeratin cocktail (AE1/AE3) and areunable to further comment on the molecular profile ofthe parakeratin.
The WHO Classification of Odontogenic Tumors re-cently recognized the neoplastic nature of the OKCwith the designation keratocystic odontogenic tumor(KCOT),1 based on its aggressive behavior, high recur-rence rate, and molecular genetic features.17 The basicarchitecture of the KCOT is, as always, that of a cyst,including the lesions reported as solid variants ofOKC.18,19 While the complex histology and growthpattern of our lesion clearly identify it as an odonto-genic neoplasm, it exhibits the strongest resemblance toOKC, with only focal areas exhibiting the pattern ofameloblastoma. We are uncertain whether this tumorrepresents a KCOT with foci that resemble ameloblas-toma or an ameloblastoma that resembles a KCOT, orperhaps, a chimera. Others have expressed similar frus-tration.6
The presence of the brisk mitotic rate of 2.5 mitoticfigures per 10 high-power fields is of interest withregard to the biologic potential of this tumor. In fact, 2of our colleagues, who studied this material in consul-tation, expressed concern that this lesion might repre-sent a keratinizing ameloblastic carcinoma. Corio etal.20 noted the typical histologic features of malignancyin their series of ameloblastic carcinomas, which in-cluded pleomorphism, increased nuclear/cytoplastic ra-tio, nuclear hyperchromatism, increased numbers ofmitotic figures, abnormal mitotic figures, and necrosis.Gardner21 observed that the diagnosis of ameloblasticcarcinoma is clear if there are obvious dysplasticchanges present, but that the prognostic significance ofmitotic figures in ameloblastoma is not well under-stood, particularly the level of mitotic activity to justifythe interpretation of a lesion as ameloblastic carcinoma.Our lesion exhibits an elevated level of mitotic activityrelative to typical ameloblastoma in which mitotic fig-ures are quite rare. The Ki-67 proliferative index of
22.8% does not seem alarming when viewed in the
OOOOE376 Whitt et al. September 2007
context of other Ki-67 proliferative indices determinedfor histologically benign ameloblastomas of 16.6%22
and 16.9%.23 Based on the absence of the cytologicfeatures of malignancy, even with a brisk rate of normalmitoses, we were reluctant to interpret this lesion as akeratinizing ameloblastic carcinoma. We believe thislesion has the potential to act in a locally aggressive,but benign manner, with potential for local recurrenceif inadequately excised.
It would be of interest to learn of the presence ofspecific DNA mutations, for example of tumor suppres-sor genes or tumor oncogenes. Unfortunately, we werenot able to perform these studies and are unable tofurther comment on the molecular genetics of this tu-mor.
The group of lesions reported as keratoameloblas-toma includes a broad spectrum of histopathologic ap-pearance. Based on the small number of cases and lackof follow-up we are unable to accurately assess whetherthe biologic behavior of keratoameloblastoma differsfrom other histologic types of ameloblastoma. Therewas wide variation in the treatment of the reportedcases, ranging from enucleation to hemi-mandibulec-tomy and partial maxillectomy. Given the nonencapsu-lated and locally infiltrative growth pattern, it appearsthat wide excision accompanied by close clinical fol-low-up is appropriate treatment. These interesting neo-plasms should continue to be reported to enable assess-ment of their histologic features and behavior.
REFERENCES1. Gardner DG, Heikinheimo K, Shear M, Philipsen HP, Coleman
H. Ameloblastomas. In: Barnes L, Eveson JW, Reichart P,Sidransky D, editors. World Health Organization classification oftumors: pathology and genetics of head and neck tumors. Lyon:International Agency for Research on Cancer (IARC) Press;2005. p. 296-300.
2. Cahn LR, Tiecke RW. Odontogenic tumors. In: Tiecke RW,editor. Oral pathology. New York: McGraw-Hill Book Com-pany; 1965. p. 215-6.
3. Shafer WG, Hine MK, Levy B, M. A textbook of oral pathology.4th ed. Philadelphia (PA): W.B. Saunders Company; 1983. p.284.
4. O’Dell EW, Morgan PR. Biopsy pathology of the oral tissues.London: Chapman & Hall; 1998. p. 381-2.
5. Pindborg JJ. Pathology of the dental hard tissues. Philadelphia(PA): W.B. Saunders; 1970. p. 371-6.
6. Siar CH, Ng KH. “Combined ameloblastoma and odontogenickeratocyst” or “keratinising ameloblastoma.” Br J Oral Maxillo-fac Surg 1993;31(3):183-6.
7. Said-al-Naief NA, Lumerman H, Ramer M, et al. Keratoamelo-blastoma of the maxilla. A case report and review of the litera-ture. Oral Surg Oral Med Oral Pathol Oral Radiol Endod1997;84(5):535-9.
8. Takeda Y, Satoh M, Nakamura S, Ohya T. Keratoameloblastoma
with unique histological architecture: an undescribed variation ofameloblastoma. Virchows Arch 2001;439(4):593-6.
9. Pindborg JJ, Weinmann JP. Squamous cell metaplasia with cal-cification in ameloblastomas. Acta Pathol Microbiol Scand1958;44:247-52.
10. Altini M, Slabbert HD, Johnston T. Papilliferous keratoamelo-blastoma. J Oral Pathol Med 1991;20(1):46-8.
11. Norval EJ, Thompson IO, van Wyk CW. An unusual variant ofkeratoameloblastoma. J Oral Pathol Med 1994;23(10):465-7.
12. Collini P, Zucchini N, Vessecchia G, Guzzo M. Papilliferouskeratoameloblastoma of mandible: a papillary ameloblastic car-cinoma: report of a case with a 6-year follow-up and review ofthe literature. Int J Surg Pathol 2002;10(2):149-55.
13. Altini M, Lurie R, Shear M. A case report of keratoameloblas-toma. Int J Oral Surg 1976;5(5):245-9.
14. Kaku T. Keratoameloblastoma of the mandible [abstract]. J OralPathol Med 2000;29:350.
15. Kramer IRH, Pindborg JJ, Shear M. World Health Organizationinternational histological classification of tumors: histologicaltyping of odontogenic tumors. 2nd ed. New York: Springer-Verlag; 1992. p. 13, 55.
16. August M, Faquin WC, Troulis M, Kaban LB. Differentiation ofodontogenic keratocysts from nonkeratinizing cysts by use offine-needle aspiration biopsy and cytokeratin-10 staining. J OralMaxillofac Surg 2000;58(9):935-40.; discussion 40-1.
17. Agaram NP, Collins BM, Barnes L, Lomago D, Aldeeb D,Swalsky P, et al. Molecular analysis to demonstrate that odon-togenic keratocysts are neoplastic. Arch Pathol Lab Med2004;128(3):313-7.
18. Vered M, Buchner A, Dayan D, Shteif M, Laurian A. Solidvariant of odontogenic keratocyst. J Oral Pathol Med2004;33(2):125-8.
19. Ide F, Mishima K, Saito I. Solid-cystic tumor variant of odon-togenic keratocyst: an aggressive but benign lesion simulatingkeratoameloblastoma. Virchows Arch 2003;442(5):501-3.
20. Corio RL, Goldblatt LI, Edwards PA, Hartman KS. Ameloblasticcarcinoma: a clinicopathologic study and assessment of eightcases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod1987;64(5):570-6.
21. Gardner DG. Some current concepts on the pathology of amelo-blastomas. Oral Surg Oral Med Oral Pathol Oral Radiol Endod1996;82(6):660-9.
22. Piattelli A, Lezzi G, Fioroni M, Santinelli A, Rubini C. Ki-67expression in dentigerous cysts, unicystic ameloblastomas, andameloblastomas arising from dental cysts. J Endod 2002;28(2):55-8.
23. Meer S, Galpin JS, Altini M, Coleman H, Ali H. Proliferatingcell nuclear antigen and Ki67 immunoreactivity in ameloblasto-mas. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2003;95(2):213-21.
Reprint requests:
Joseph C. Whitt, DDS, MSAssociate ProfessorOral and Maxillofacial PathologySchool of DentistryUniversity of Missouri Kansas City650 E. 25th StreetKansas City, MO 64108-6489
[email protected]; [email protected]
Related Documents











