Kaposi's Sarcoma: Relationship with Hematologic, Lymphoid, and Thymic Neoplasia THOMAS M. ULBRIGHT, MD,* AND DANIEL J. SANTA CRUZ, MDt Four cases of Kaposi's sarcoma (KS) are described; one each was associated with Hodgkin's disease, a thymoma, an atypical lymphoid proliferation resembling Castleman's disease, and a cutaneous reticulo- sis. The association of KS with lymphoproliferative, hematologic, and other neoplasms is thoroughly reviewed, with special attention to tissue diagnosis, relative order of development, and relationship to immunosuppressive treatment. Review of 65 accepted cases, including ours, showed that 85% of patients with KS and a known order of development appeared with KS either simultaneously or after the second neoplasm. There was a disproportionate tendency for hematologic malignancy to develop simultaneously with KS. Of the 22 patients who had KS subsequent to a second neoplasm, 18 (82%) had received some form of interval immunosuppression. This evidence and observations in renal allograft recipients, patients with pemphigus, and patients with other autoimmune disorders point to the frequency of a common background of deranged immune status in patients with KS. Therefore, either naturally occurring or iatrogenic immune deficiency likely predisposes patients to KS. Some possible mechanisms for this phenomenon are reviewed. Cancer 47:963-973, 1981. HE ASSOCIATION OF KAPOSI'S SARCOMA (KS) with jymphoma,2,13.23.~Z.~~.til .ti3 leukemia, 13,23,52,63 multi- and other malignanciesj4has been recognized for many years. Early reports date from the last century.I4 More recently several author^^.".'"*^^*- have collected substantial numbers of this concur- rence of KS and lymphoreticular neoplasia.$ In 1965, Reynolds et UI.~~ thoroughly reviewed the extant litera- ture. Statistically, there is no question that the associa- tion is highly ~ignificant,~.~.~~,~~,~~ at least in the non- African cases.5s Despite the well-documented association, no etio- logic relationship was clear, although some authors be- lieved the basis for concurrence of KS with lymphore- ticular neoplasia was a common progenitor ~ell.~~7~"."' Subsequently, several investigators noted the develop- ment of KS in patients who had undergone renal trans- plantation and long-term immunosuppressive ther- apy.3"-32-.i".6**72 Many felt that KS or other malignancies in allograft recipients resulted from failure of immuno- surveillance mechanisms secondary to immunosup- T ple mye10ma,35.51.54.fi.? 5".,;4.74 From the Department of Pathology. Division of Surgical Pathol- ogy, Washington University School of Medicine and Barnes Hospital, St. Louis, Missouri. * Chief Resident. t Assistant Professor of Pathology. Dr. Ulbright is presently at Department of Pathology, Indiana Address for reprints: Daniel J. Santa Cruz, MD, Division of Surgi- Accepted for publication March 17, 1980. University. cal Pathology. Barnes Hospital Plaza, St. Louis, MO 63110. pressive therapy and perhaps enhanced by chronic anti- genic stimulation53 and/or activation of latent oncogenic viruses by the allograft.6R In support of this view are cases of regression of KS with cessation or reduction of immunosuppression"*5" and progression with continua- tion.3n We have recently reviewed cases of KS at Barnes Hospital for concurrence with lymphoreticular disor- ders and have found four relevant cases. This discovery prompted us to review critically the medical literature in order to determine if a mechanism similar to the de- velopment of KS in transplant recipients could be applied to explain the concurrence of KS with these other diseases. Materials and Methods All cases of KS accessioned to the Barnes Hospital surgical pathology and autopsy files from 1950 to the present were reviewed. Thirty-four cases of KS were found, 17 of which were outside pathology consultation cases; the patients were never seen at Barnes Hospital, and these patients were not followed-up.The names of the remaining 17 patients were recorded, and the files were searched to see if a prior or subsequent diagnosis of a lymphoreticular disorder was present. (This method $ For the sake ofconvenience, the term "lymphoreticular" will be applied to all forms of leukemia, lymphoma, mycosis fungoides, and thymoma. We acknowledge the epithelial nature of thymorna. 0008-543X/81/0301/0963 $1.05 0 American Cancer Society 963

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Kaposi's Sarcoma:
Relationship with Hematologic, Lymphoid, and Thymic Neoplasia
THOMAS M. ULBRIGHT, MD,* AND DANIEL J. SANTA CRUZ, MDt
Four cases of Kaposi's sarcoma (KS) are described; one each was associated with Hodgkin's disease, a thymoma, an atypical lymphoid proliferation resembling Castleman's disease, and a cutaneous reticulo- sis. The association of KS with lymphoproliferative, hematologic, and other neoplasms is thoroughly reviewed, with special attention to tissue diagnosis, relative order of development, and relationship to immunosuppressive treatment. Review of 65 accepted cases, including ours, showed that 85% of patients with KS and a known order of development appeared with KS either simultaneously or after the second neoplasm. There was a disproportionate tendency for hematologic malignancy to develop simultaneously with KS. Of the 22 patients who had KS subsequent to a second neoplasm, 18 (82%) had received some form of interval immunosuppression. This evidence and observations in renal allograft recipients, patients with pemphigus, and patients with other autoimmune disorders point to the frequency of a common background of deranged immune status in patients with KS. Therefore, either naturally occurring or iatrogenic immune deficiency likely predisposes patients to KS. Some possible mechanisms for this phenomenon are reviewed.
Cancer 47:963-973, 1981.
H E ASSOCIATION OF KAPOSI'S SARCOMA (KS) with jymphoma,2 ,13 .23 .~Z.~~ . t i l .ti3 leukemia, 13,23,52,63 multi-
and other malignanciesj4 has been recognized for many years. Early reports date from the last century.I4 More recently several author^^.".'"*^^*-
have collected substantial numbers of this concur- rence of KS and lymphoreticular neoplasia.$ In 1965, Reynolds e t U I . ~ ~ thoroughly reviewed the extant litera- ture. Statistically, there is no question that the associa- tion is highly ~ignificant,~.~.~~,~~,~~ at least in the non- African cases.5s
Despite the well-documented association, no etio- logic relationship was clear, although some authors be- lieved the basis for concurrence of KS with lymphore- ticular neoplasia was a common progenitor ~ell.~~7~"."' Subsequently, several investigators noted the develop- ment of KS in patients who had undergone renal trans- plantation and long-term immunosuppressive ther- apy.3"-32-.i".6**72 Many felt that KS or other malignancies in allograft recipients resulted from failure of immuno- surveillance mechanisms secondary to immunosup-
T ple mye10ma,35.51.54.fi.?
5".,;4.74
From the Department of Pathology. Division of Surgical Pathol- ogy, Washington University School of Medicine and Barnes Hospital, St. Louis, Missouri.
* Chief Resident. t Assistant Professor of Pathology. Dr. Ulbright is presently at Department of Pathology, Indiana
Address for reprints: Daniel J. Santa Cruz, MD, Division of Surgi-
Accepted for publication March 17, 1980.
University.
cal Pathology. Barnes Hospital Plaza, St. Louis, MO 63110.
pressive therapy and perhaps enhanced by chronic anti- genic stimulation53 and/or activation of latent oncogenic viruses by the allograft.6R In support of this view are cases of regression of KS with cessation or reduction of immunosuppression"*5" and progression with continua- tion.3n
We have recently reviewed cases of KS at Barnes Hospital for concurrence with lymphoreticular disor- ders and have found four relevant cases. This discovery prompted us to review critically the medical literature in order to determine if a mechanism similar to the de- velopment of KS in transplant recipients could be applied to explain the concurrence of KS with these other diseases.
Materials and Methods
All cases of KS accessioned to the Barnes Hospital surgical pathology and autopsy files from 1950 to the present were reviewed. Thirty-four cases of KS were found, 17 of which were outside pathology consultation cases; the patients were never seen at Barnes Hospital, and these patients were not followed-up. The names of the remaining 17 patients were recorded, and the files were searched to see if a prior or subsequent diagnosis of a lymphoreticular disorder was present. (This method
$ For the sake ofconvenience, the term "lymphoreticular" will be applied to all forms of leukemia, lymphoma, mycosis fungoides, and thymoma. We acknowledge the epithelial nature of thymorna.
0008-543X/81/0301/0963 $1.05 0 American Cancer Society
963

964 CANCER March I 1981 Vol. 47
FIG. 1. Atypical mononuclear cells are scattered among lymphocytes and bundles of collagen in an effaced lymph node. Occasional Reed Sternberg cells ( i n s e t ) are present (W. U. Neg. #79-9891 and 80-1396, X 150. X 1200).
probably underestimated the concurrence of the two diseases.) Two cases of KS were found associated with Hodgkin’s disease and a thymoma. A third case was associated with an atypical lymphoid proliferation, which resembled angiofollicular lymphoid hyperplasia of the hyaline vascular A fourth patient with KS had a form of cutaneous reticulosis. All available slides were reviewed, and additional slides were cut from several blocks. The diagnoses were confirmed on review. Medical histories and follow-up were obtained from hospital charts or private physician’s records.
In reviewing the medical literature, all cases that did not have biopsy or autopsy diagnoses of both diseases were excluded. When it was not clear that tissue diag- noses existed, the cases were discarded for the purposes of this study. Consequently, many of the review arti- cles, which discussed the association of KS with leu- kemia and lymphoma, and which tabulated past and new cases, could not be included in our tabulations. This conservative approach explains the partial dis- crepancy between the number of cases we have con- sidered acceptable examples of the concurrence of KS
with these other diseases and those recorded by other authors. Clearly, from a review of the literature, dupli- cation of reported cases is a significant problem; all efforts to avoid this pitfall have been made, but it is still possible that some duplication is present in our review.
Another problem in this retrospective review con- cerns the recent significant reclassification of lympho- mas. For this reason, we have not attempted to sub- categorize lymphomas except into Hodgkin’s and non- Hodgkin’s types. We furthermore depend on the diagnostic accuracy of those reporting the cases.
One factor of particular interest was the order of presentation of the two diseases. The order was re- corded as preceding, simultaneous, or subsequent to KS. All cases of KS that appeared within one to two months of the second neoplasm, whether prior or sub- sequent, were regarded as actual simultaneous presen- tations.
Another factor evaluated was the presence or ab- sence of immunosuppressive therapy. For this study, the term “immunosuppression” was defined broadly to include all therapeutic modalities that had a potential to
No. 5 KAPosi's SARCOMA 1 Ulbright and Santa Cruz 965
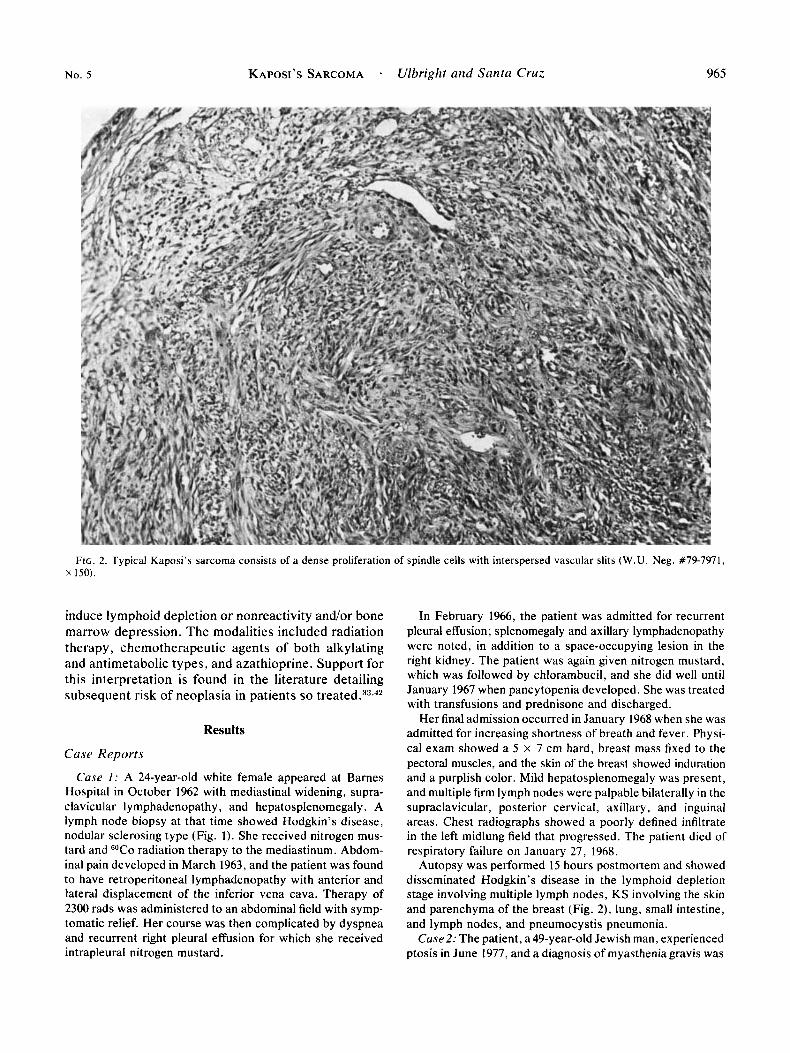
FIG. 2. Typical Kaposi's sarcoma consists of a dense proliferation of spindle cells with interspersed vascular slits ( W . U . Neg. #79-7971, x 150).
induce lymphoid depletion or nonreactivity and/or bone marrow depression. The modalities included radiation therapy, chemotherapeutic agents of both alkylating and antimetabolic types, and azathioprine. Support for this interpretation is found in the literature detailing subsequent risk of neoplasia in patients so t ~ e a t e d . ~ ~ ' ~ *
Results
Case Reports
Case I : A 24-year-old white female appeared at Barnes Hospital in October 1962 with mediastinal widening, supra- clavicular lymphadenopathy, and hepatosplenomegaly. A lymph node biopsy at that time showed Hodgkin's disease, nodular sclerosing type (Fig. 1). She received nitrogen mus- tard and "CO radiation therapy to the mediastinum. Abdom- inal pain developed in March 1963, and the patient was found to have: retroperitoneal lymphadenopathy with anterior and lateral displacement of the inferior vena cava. Therapy of 2300 rads was administered to an abdominal field with symp- tomatic relief. Her course was then complicated by dyspnea and recurrent right pleural effusion for which she received intrapleural nitrogen mustard.
In February 1966, the patient was admitted for recurrent pleural effusion; splenomegaly and axillary lymphadenopathy were noted, in addition to a space-occupying lesion in the right kidney. The patient was again given nitrogen mustard, which was followed by chlorambucil, and she did well until January 1967 when pancytopenia developed. She was treated with transfusions and prednisone and discharged.
Her final admission occurred in January 1968 when she was admitted for increasing shortness of breath and fever. Physi- cal exam showed a S x 7 cm hard, breast mass fixed to the pectoral muscles, and the skin of the breast showed induration and a purplish color. Mild hepatosplenomegaly was present, and multiple firm lymph nodes were palpable bilaterally in the supraclavicular, posterior cervical, axillary, and inguinal areas. Chest radiographs showed a poorly defined infiltrate in the left midlung field that progressed. The patient died of respiratory failure on January 27, 1968.
Autopsy was performed IS hours postmortem and showed disseminated Hodgkin's disease in the lymphoid depletion stage involving multiple lymph nodes, KS involving the skin and parenchyma of the breast (Fig. 2), lung, small intestine, and lymph nodes, and pneumocystis pneumonia.
Case 2: The patient, a 49-year-old Jewish man, experienced ptosis in June 1977, and a diagnosis of myasthenia gravis was
966 CANCER Murch I 1981 Vol. 47
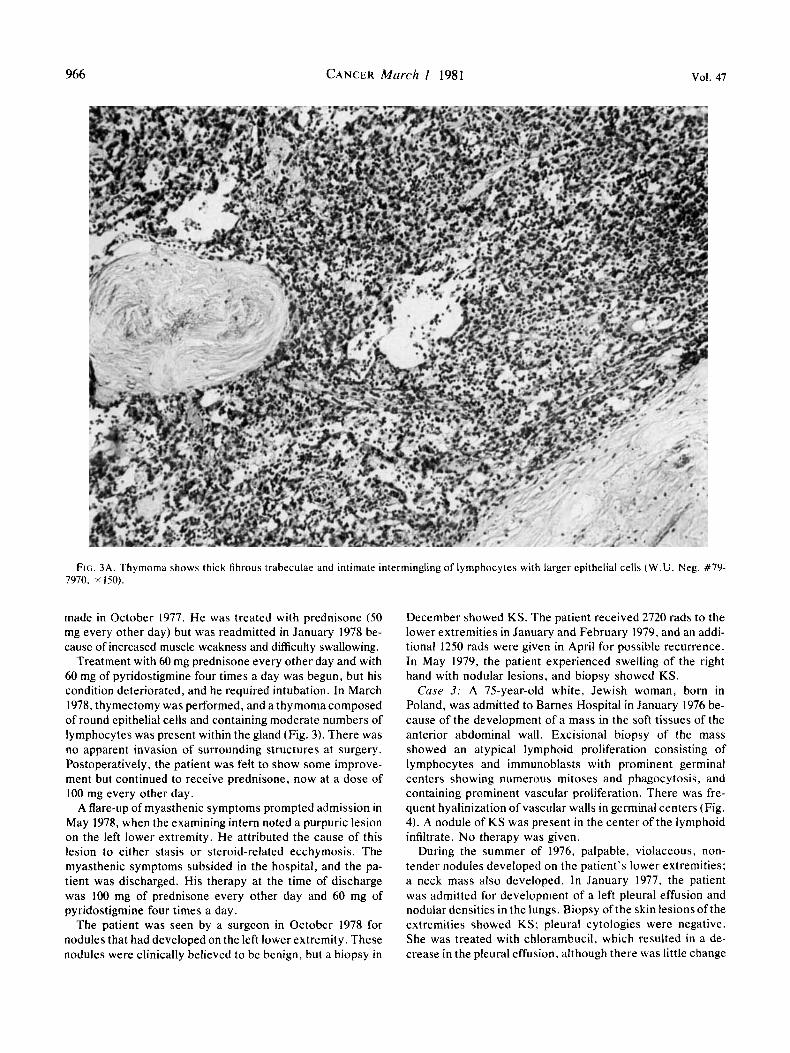
FIG. 3A. Thymoma shows thick fibrous trabeculae and intimate intermingling of lymphocytes with larger epithelial cells ( W . U . Neg. #79- 7970, x150).
made in October 1977. He was treated with prednisone ( S O mg every other day) but was readmitted in January 1978 be- cause of increased muscle weakness and difficulty swallowing.
Treatment with 60 mg prednisone every other day and with 60 mg of pyridostigmine four times a day was begun, but his condition deteriorated, and he required intubation. In March 1978, thymectomy was performed, and a thymoma composed of round epithelial cells and containing moderate numbers of lymphocytes was present within the gland (Fig. 3). There was no apparent invasion of surrounding structures at surgery. Postoperatively, the patient was felt to show some improve- ment but continued to receive prednisone, now at a dose of 100 mg every other day.
A flare-up of myasthenic symptoms prompted admission in May 1978, when the examining intern noted a purpuric lesion on the left lower extremity. He attributed the cause of this lesion to either stasis or steroid-related ecchymosis. The myasthenic symptoms subsided in the hospital, and the pa- tient was discharged. His therapy at the time of discharge was 100 mg of prednisone every other day and 60 mg of pyridostigmine four times a day.
The patient was seen by a surgeon in October 1978 for nodules that had developed on the left lower extremity. These nodules were clinically believed to be benign, but a biopsy in
December showed KS. The patient received 2720 rads to the lower extremities in January and February 1979, and an addi- tional 1250 rads were given in April for possible recurrence. In May 1979, the patient experienced swelling of the right hand with nodular lesions, and biopsy showed KS.
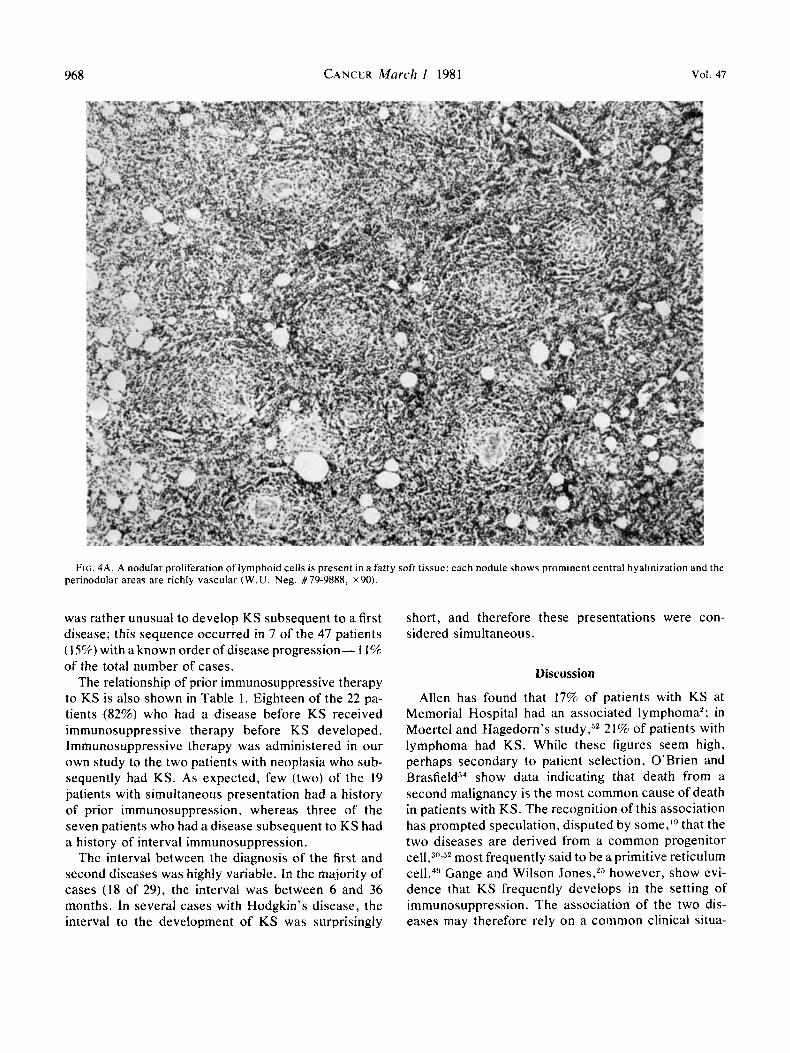
Case 3: A 75-year-old white, Jewish woman, born in Poland, was admitted to Barnes Hospital in January 1976 be- cause of the development of a mass in the soft tissues of the anterior abdominal wall. Excisional biopsy of the mass showed an atypical lymphoid proliferation consisting of lymphocytes and immunoblasts with prominent germinal centers showing numerous mitoses and phagocytosis, and containing prominent vascular proliferation. There was fre- quent hyalinization of vascular walls in germinal centers (Fig. 4). A nodule of KS was present in the center of the lymphoid infiltrate. No therapy was given.
During the summer of 1976, palpable, violaceous. non- tender nodules developed on the patient's lower extremities; a neck mass also developed. In January 1977, the patient was admitted for development of a left pleural effusion and nodular densities in the lungs. Biopsy of the skin lesions of the extremities showed KS; pleural cytologies were negative. She was treated with chlorambucil, which resulted in a de- crease in the pleural effusion, although there was little change

No. 5 KAPOSI’S SARCOMA Ulbright and Santa Crirz 967
Flc. 38. The neoplastic epithelial cells of the thymoma are round and proliferate in a cord-like arrangement; there is a moderate lymphocytic component (W.U. Neg. #80-1399, ~ 6 0 0 ) .
in size of the pulmonary nodules. In July 1977, the patient received 2500 rads to the neck and mediastinum for enlarged nodes. In October, a right pleural effusion developed, which was tapped twice; results of cytologic analysis of both taps were interpreted as positive for adenocarcinoma. Intrapleural nitrogen mustard was given, but the patient’s condition de- clined, and she died in November 1977. Permission for au- topsy was refused.
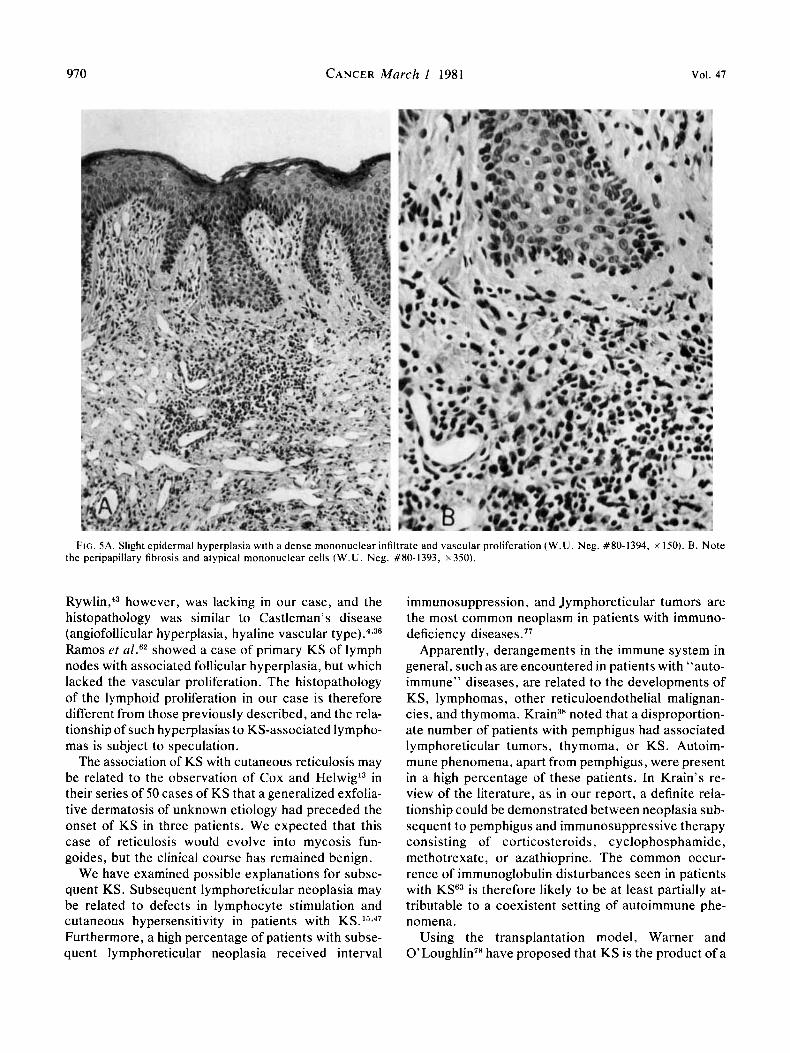
Crrsc 4: A 59-year-old white male had generalized exfolia- tive erythrodermain 1966. In 1968, purplish skin lesionsofthe lower extremities appeared. A biopsy of these purplish lesions showed KS; biopsies of the exfoliative lesions in 1970 and 1975 showed the findings of cutaneous reticulosis with foci suggestive of, but not diagnostic for, mycosis fungoides (Fig. 5 ) . The patient’s subsequent course has been indolent. Eryth- roderma persists, but there has been no progression to myco- sis fungoides. The lesions of KS have been treated with re- gression by localized radiation therapy. Recent skin biopsies show only nonspecific inflammatory changes and no evidence of either disease.
Literrifirre Review
Sixty-five cases, including those reported here, were considered well-documented examples of the concur-
rence of KS with either leukemia, myeloma, lymphoma. mycosis fungoides, or thymoma. As shown in Table 1, the most frequent KS-associated conditions included Hodgkin’s disease, non-Hodgkin’s lymphomas, and lymphocytic leukemias. The KS-associated disease most frequently appeared before the development of KS; simultaneous presentation was next in frequency. In fact, 85% of patients had either a prior or simultane- ous disease with respect to K S among those patients in which the sequence was known. This pattern was most striking for the non-Hodgkin’s lymphomas; 92% of the patients with known sequence had lymphoma either before or simultaneous with KS. The same pattern was seen in all of the patients with myelogenous leukemia, multiple myeloma, mycosis fungoides, and thymoma; however the numbers of patients in each of these groups were small. Although lymphocytic leukemia, myelog- enous leukemia, and multiple myeloma accounted for only 29% of the total number of cases, these diseases accounted for 58% of the cases with a simultaneous development of KS. There was, therefore, a dispropor- tionate tendency for diseases, which primarily affected the bone marrow, to present simultaneously with KS. It
968 CANCER March I 1981 Vol. 47
FIG. 4A. A nodular proliferation of lymphoid cells is present in a fatty soft tissue: each nodule shows prominent central hyalinization and the perinodular areas are richly vascular ( W . U . Neg. #79-9888, ~ 9 0 ) .
was rather unusual to develop KS subsequent to a first disease; this sequence occurred in 7 of the 47 patients (15%) with a known order of disease progression- 1 1% of the total number of cases.
The relationship of prior immunosuppressive therapy to KS is also shown in Table 1. Eighteen of the 22 pa- tients (82%) who had a disease before KS received immunosuppressive therapy before KS developed. Immunosuppressive therapy was administered in our own study to the two patients with neoplasia who sub- sequently had KS. As expected, few (two) of the 19 patients with simultaneous presentation had a history of prior immunosuppression, whereas three of the seven patients who had a disease subsequent to KS had a history of interval immunosuppression.
The interval between the diagnosis of the first and second diseases was highly variable. In the majority of cases (18 of 29), the interval was between 6 and 36 months. In several cases with Hodgkin’s disease, the interval to the development of KS was surprisingly
short, and therefore these presentations were con- sidered simultaneous.
Discussion
Allen has found that 17% of patients with KS at Memorial Hospital had an associated lymphoma’; in Moertel and Hagedorn’s study,s2 21% of patients with lymphoma had KS. While these figures seem high, perhaps secondary to patient selection, O’Brien and Brasfie1d”l show data indicating that death from a second malignancy is the most common cause of death in patients with KS. The recognition of this association has prompted speculation, disputed by some,’9 that the two diseases are derived from a common progenitor
most frequently said to be a primitive reticulum cell.49 Gange and Wilson Jones,25 however, show evi- dence that KS frequently develops in the setting of immunosuppression. The association of the two dis- eases may therefore rely on a common clinical situa-

No. 5 KAPOSI’S SARCOMA . Ulbright and Santa Cruz 969
FIG. 4E1. The center of a nodule shows prominent vascular wall hyalinization. Phagocytotic and mitotic activity are prominent features else- where ( W . U . Neg. #80-989.5, ~ 3 . 5 0 ) .
tion instead of a common cell of origin, although these two possibilities are certainly not mutually exclusive. Hence, there is afairly high frequency of KS in patients who have had renal allografts with concomitant im- munosuppressive therapy.3‘)~32,53,6s,i‘
The belief that KS develops secondary to immuno- suppression is supported by our study. A critical review of the data indicates that KS develops either subse- quently or simultaneously in the majority of patients with KS and associated lymphoreticular neoplasia. Furthermore, the subsequent occurrence of KS usually followed immunosuppressive therapy for the initial disease:. “Simultaneous occurrence” may be related to the known immune deficiencies in patients with leu- kemia, myeloma, and lymphoma^.^^^""^^ Another ex- planation for simultaneous presentation is the possible presence of an undetected immunodeficiency di~order ,~’ which predisposes patients to both types of neoplasia.
The presence of an opportunistic infection (pneu- mocystis pneumonia) as the immediate cause of death
in our first patient lends credence to the belief that these associated disorders develop in a setting of im- munodeficiency. Added support is supplied by our second case in which thymic neoplasia with an auto- immune disorder was treated by immunosuppressive drugs. Kaposi’s sarcoma subsequently developed dur- ing exacerbations of myasthenic symptoms.
Two of our cases could not be regarded as acceptable examples of KS associated with neoplasia. One case had an exuberant associated follicular and vascular hyperplasia. Although Rywlin rt described the typical findings of KS involving lymph nodes as includ- ing a peculiar vascular, follicular hyperplasia, which lacked mitoses, phagocytosis, and nuclear debris, our case showed vascular hyperplasia but marked germinal center mitotic activity and phagocytosis, in addition to hyalinization of vessels. Lubin and R y w l W later de- scribed follicular hyperplasia with phagocytosis and mitoses in lymph nodal KS. The plasmacytosis noted by Rywlin et ~ 1 . ~ ~ and reemphasized by Lubin and
970 CANCER March 1 1981 Vol. 47
FIG. 5A. Slight epidermal hyperplasia with a dense mononuclear infiltrate and vascular proliferation ( W . U . Neg. #S0-1394, x 150). B . Note the peripapillary fibrosis and atypical mononuclear cells ( W . U . Neg. #SO-1393, ~350).
R y ~ l i n , ~ ~ however, was lacking in our case, and the histopathology was similar to Castleman’s disease (angiofollicular hyperplasia, hyaline vascular t ~ p e ) . ~ , ~ ~ Ramos et al.6z showed a case of primary KS of lymph nodes with associated follicular hyperplasia, but which lacked the vascular proliferation. The histopathology of the lymphoid proliferation in our case is therefore different from those previously described, and the rela- tionship of such hyperplasias to KS-associated lympho- mas is subject to speculation.
The association of KS with cutaneous reticulosis may be related to the observation of Cox and HelwigL3 in their series of 50 cases of KS that a generalized exfolia- tive dermatosis of unknown etiology had preceded the onset of KS in three patients. We expected that this case of reticulosis would evolve into mycosis fun- goides, but the clinical course has remained benign.
We have examined possible explanations for subse- quent KS. Subsequent lymphoreticular neoplasia may be related to defects in lymphocyte stimulation and cutaneous hypersensitivity in patients with KS. 1s*47
Furthermore, a high percentage of patients with subse- quent lymphoreticular neoplasia received interval
immunosuppression, and Jymphoreticular tumors are the most common neoplasm in patients with immuno- deficiency diseases.77
Apparently, derangements in the immune system in general, such as are encountered in patients with “auto- immune” diseases, are related to the developments of KS, lymphomas, other reticuloendothelial malignan- cies, and thymoma. noted that a disproportion- ate number of patients with pemphigus had associated lymphoreticular tumors, thymoma, or KS. Autoim- mune phenomena, apart from pemphigus, were present in a high percentage of these patients. In Krain’s re- view of the literature, as in our report, a definite rela- tionship could be demonstrated between neoplasia sub- sequent to pemphigus and immunosuppressive therapy consisting of corticosteroids, cyclophosphamide, methotrexate, or azathioprine. The common occur- rence of immunoglobulin disturbances seen in patients with KSG3 is therefore likely to be at least partially at- tributable to a coexistent setting of autoimmune phe- nomena.
Using the transplantation model, Warner and O ’ L ~ u g h l i n ~ ~ have proposed that KS is the product of a

No. 5 KAPOSI'S SARCOMA . Ulbright and Santa Cruz
TABLE 1. Association of Kaposi's Sarcoma With Other Types of Neoplasia
97 1
Prior immuno- No. of suppression
patients (96) Sequence* Timet (months) (+ ) ( - ) (?) References
Lymphocytic leukemnas
Myelogenous leukemia
Multiple myeloma
Hodgkin's disease
Non-Hodgkin's lymphornas
Mycosis fungoides
Thymoma
TOTAI.
12 (18)
2 (3)
5 (8)
19 (29)
17 (26)
6 (9)
4 (6)
65
2 prior 7 simultaneous 2 subsequent 1 unknown
2 simultaneous
3 prior 2 simultaneous
5 prior 3 simultaneous 4 subsequent 7 unknown
7 prior 4 simultaneous 1 subsequent 5 unknown
3 prior 1 simultaneous 2 unknown
2 prior 2 unknown
22 prior 19 simultaneous 7 subsequent 17 unknown
96, 48
60. 300 -
-
35, 19, 3.5 -
21, 5, 8, 360, 63
6, 29, 42, 9 -
-
>7, 16, 36, 23, 18, 9. 21
72
12, >36, 15
-
-
- -
12, 9 -
- 7 I 1
2
- 2
1 1 2 2
- 4
I -
- 1 -
1 1
27
10.81 11, 14, 34, 58, 64, 75, 79 24, 65 11
I , 74
35, 46, 48 22, 40
7, 27. 28. 51$ 4, 17. 63 56, 60, 63, 76 2, 21, 41
6. 16, 30, 37, 45, 63, 65 20, 53. 57, 70 2 2. 52. 57. 63
5. 13, 39 82 2
63$ 26. 44
Sequence refers to the time the second disease was diagnosed
t Time is the number of months in the interval between the diag- with respect to KS.
defective graft-versus-host reaction, as transformed lymphocytes activate latent RNA tumor viruses during reaction against renal allografts.fiR The early KS there- fore shows lymphoma characteristics, followed by an intense vascular proliferation as the "transformed-neo- plastic" lymphocytes release angiogenesic factor. The finding of an intensely vascular follicular hyperplasia with numerous immunoblasts in our third case is con- sistent with this concept.
KS appears to be causally related to immunode- ficiency , iatrogenic or secondary to preexisting neo- plasia and/or immunodeficiency (including autoimmune diseases). Less commonly, KS preexists, but similar arguments apply to the development of the second tumor. Kaposi's sarcoma appears to result from both immunodeficiency and antigenic stimulation and is therefore particularly prone to develop in transplant recipients.53 to occur in Africa where malaria causes both prerequisite conditions,29 and to be associated with the common tumor type of immunodeficiency, i.e., lymphoreticular neoplasia. Kaposi's sarcoma indeed appears to be what CairnsX has described as an oppor-
noses of the two diseases for those cases with available data. $ This paper.
tunistic malignancy. The place of those few cases that claim to demonstrate a histopathologic transition from KS to lymphoma (usually Hodgkin's d i s e a ~ e ) ~ . ~ " ~ " in this scheme is not clear. The demonstration that treat- ment induces Reed-Sternberg-like cells in lymphocytic neoplasia'j7 makes careful assessment of similar cases mandatory.
REFERENCES
1 . Abrahmsen AM, Wetteland P. Kaposi sarkom og myelogen
2. Allen AC. The Skin: A Clinicopathologic Treatise. St. Louis:
3. Berg JW. The incidence of multiple primary cancers: I. Devel- opment of further cancers in patients with lymphomas, leukemias, and myeloma. J Narl Cancer Insr 1967; 38:741-752.
4. Beurey J , Weber Mazet J , de Ren G, Vaillant G. Association maladie de Kaposi-maladie de Hodgkin. Ann Dermafol Syphilol (Paris) 1976; 103:151-159.
5. Beylot C, Beylot J, Veyret V. et a / . Maladie de Kaposi et lymphome malin: discussion de cette association. Ann Drrmatol VetiereoI 1977: 104:817-823.
6. Bluefarb SM, Webster JR. Kaposi's sarcoma associated with lymphosarcoma. Arch Ititern Med 1953: 91:97- 105.
7. Brunning RD, Foley JF, Fortuny IE. Hodgkin's disease and Kaposi's sarcoma. Arch Intern Med 1963; 112:363-369.
leukemia. Nord Med 1959; 62:1811- 1813.
C. V. Mosby CO.. 1954:996-1000.
972 CANCER March I 1981 VOl. 47
8. Cairns RJ. “Opportunistic” auto-immune disease and “oppor- tunistic” malignancy from impaired cell mediated immunity? Br J Dermatol 1974; 91:601-602.
9. Castleman B, Iverson L, Menendez V. Localized mediastinal lymph node hyperplasia resembling thymoma. Cancer 1956; 9:822- 830.
10. Caulet T, Hibbon E, Roth A, et a / . Sarcome de Kaposi visceral associe a une carcinome medullaire throidien chez une enfant en tres longue remission de leucemie lymphoblastique. N O N I ~ Presse Med 1977; 6: 2673- 2676.
1 1 . Cole HN, Crump ES. Report of two cases of idiopathic hemor- rhagic sarcoma (Kaposi), the first complicated with lymphatic leu- kemia. Arch Dermatol Syph 1920; 1:283-295.
12. Cone L, Uhr JW. Immunological deficiency disorders asso- ciated with chronic lymphocytic leukemia and multiple myeloma. J Clin Invest 1964; 43:2241-2248.
13. Cox FH, Helwig EB. Kaposi’s sarcoma. Cancer 1959;
14. Dieballa G. Ueber eihen mit Lymphocytose einhergehenden Fall von Sarcoma multiplex cutis. Wien Klin Wchschr 1897;
15. Dobozy A, Husz S, Hunyadi J, Berko G, Simon N. Immune deficiencies and Kaposi’s sarcoma. Lancet 1973; 2:625.
16. Dollinger MR, Foye LV Jr. Kaposi’s sarcoma and coexistent giant follicular lymphoblastoma. Yale J Biol Med 1966; 38:449-455.
17. Donnelly WJ. Clinicopathologic conference: Hodgkin’s dis- ease and mucocutaneous lesions. Postgrad Med 1963; 33:301-306.
18. Dutz W, Stout AP. Kaposi’s sarcoma in infants and children. Cancer 1960; 13:684-694.
19. Ecklund RE, Valaitus J. Kaposi’s sarcoma of lymph nodes. Arch Path01 1962; 74:224-229.
20. El-Arini AF. Idiopathic multiple hemorrhagic sarcoma of Kaposi. Alexundrin Mrd J 1958; 4:35-42.
21. Epstein E. Extracutaneous manifestations of Kaposi’s sar- coma: a systemic lymphoblastoma. Calif Med 1957; 87:98- 103.
22. Ettinger DS, Humphrey RL, Skinner MD. Kaposi’s sarcoma associated with multiple myeloma. Johns Hopkins Med J 1975;
23. Feurerman EJ, Potruch-Eisenkraft S. Kaposi’s sarcoma: a fol- low-up of 38 patients. Dermatologica 1973; 146: 115- 122.
24. Fischer JW, Cohen DM. Simultaneous occurrence of Kaposi’s sarcoma, leukemia, and diabetes mellitus. Am J CIin Path01 1951;
25. Gange RW, Wilson Jones E. Kaposi’s sarcoma and immuno- suppressive therapy: an appraisal. Clin Exp Dermarol 1978; 3:135- 146.
26. Gellin G. Kaposi’s sarcoma: three cases of which two have unusual findings in association. Arch Derrnatol 1969; 99:92-94.
27. Gilbert TT, Evjy JT, Edelstein L. Hodgkin’s disease associated with Kaposi’s sarcoma and malignant melanoma: case report of mul- tiple primary malignancies. Cancer 1971; 28:293-299.
28. Greenstein RH, Conston AS. Coexistent Hodgkin’s disease and Kaposi’s sarcoma: report of a case with unusual histologic fea- tures. Am J Med Sci 1949; 218:384-388.
29. Greenwood BM, Bradley-Moore AM, Palit A, Bryceson ADM. Lancet 1972; 1: 169-172.
30. Haim S. Shafrir A, Better OS, Robinson E , Chaimowitz C, Erlik D. Kaposi’s sarcoma in association with immunosuppressive therapy: report of two cases. I s r J Med Sci 1972; 8: 1993- 1997.
3 I . Haim S, Friedman-Birnbaum R, Better OS, Tuma S. Skin com- plications in immunosuppressed patients: follow-up of kidney recipi- ents. Br J Dermatol 1973; 89:169- 173.
32. Hardy MA, Goldfarb P, Levine S, et a / . De novo Kaposi’s sarcoma in renal transplantation: case report and a brief review. Cancer 1976; 38:144- 148.
33. Hams CC. Malignancy during methotrexate and steroid ther- apy for psoriasis. Arch Dermatol 1971; 103:501-504.
34. Hufnagel L, Dupont A. Sarcomatose idiopathique de Kaposi et leucemie lymphoide. Bull Snc Franc Drrmnrol Svph 1931; 38:656-664.
12:289-298.
10:523-525.
1 37: 88-90.
21 ~586-589.
35. Kapadia SB, Krause JR. Kaposi’s sarcoma after long-term alkylating agent therapy for multiple myeloma. South Med J 1977; 70: 101 1- 1013.
36. Keller AR, Hochholzer L, Castleman B. Hyaline-vascular and plasma cell types of giant lymph node hyperplasia of the mediastinum and other locations. Cancer 1972; 29670-683.
37. Klepp 0, Dahl 0, Stenwig JT. Association of Kaposi’s sar- coma and prior immunosuppressive therapy: a 5-year material of Kaposi’s sarcoma in Norway. Cancer 1978; 42:2626-2630.
38. Krain LS. The association of pemphigus with thymoma or malignancy: a critical review. Br J Dermatol 1974; 90:397-405.
39. Lane CG, Greenwood AM. Lymphoblastoma (mycosis fun- goides) and hemorrhagic sarcoma of Kaposi in the same person. Arch Dermatol Syph 1936; 27:643-657.
40. Law IP. Kaposi sarcoma and plasma cell dyscrasia. JAMA 1974; 229:1329-1331.
41. Lothe F, Murray JF. Kaposi’s sarcoma: autopsy findings in the African. Acta Unio Int Cont Cancer 1962; 18:429-452.
42. Lowney ED. Anti-mitotic drugs and aggressive squamous cell tumors. Arch Dermatol 1972; 105:924.
43. Lubin J, Rywlin AM. Lymphoma-like lymph node changes in Kaposi’s sarcoma: two additional cases. Arch Pathol 1971; 92:338-341.
44. Maberry JD, Stone DJ. Kaposi’s sarcoma with thymoma. Arch Dermatol 1967; 95:210-2 17.
45. Malkinson FD, Stone BS. Kaposi’s sarcoma, lymphoblastoma, and Herpes zoster. Arch Dermatol 1955; 72:79.
46. Mandel EM, Lask D, Gafter U, Weiss S, Kende L, Djaldetti M. Multiple myeloma associated with Kaposi’s sarcoma. Acra Haematol 1977; 58:120-128.
47. Master SP, Taylor JF, Kyalwazi SK, Ziegler JL. Immunologi- cal studies in Kaposi’s sarcoma in Uganda. Br MedJ 1970; 1:600-602.
48. Mazzaferri EL, Penn GM. Kaposi’s sarcoma associated with multiple myeloma: report of a patient and review of the literature. Arch Intern Med 1968; 122:521-525.
49. McCarthy WD, Pack GT. Malignant blood vessel tumors: a re- port of 56 cases of angiosarcoma and Kaposi’s sarcoma. S w g Gyne- col Obstet 1950; 91:465-482.
50. Miller DG, Lizard0 JG, Snyderman RK. Homologous and heterologous skin transplantation in patients with lymphomatous disease. J Nat l Cancer Inst 1961; 26:569-579.
51. Moe N. Hodgkin’s disease and Kaposi’s sarcoma: report of a case. Acta Path01 Microbiol Scand 1966; 68: 189- 193.
52. Moertel CG, Hagedorn AB. Leukemia or lymphoma and co- existent primary malignant lesions: a review of the literature and a study of 120 cases. Blood 1957; 12:788-803.
53. Myers BD, Kessler E, Levi J, Pick A, Rosenfeld JB. Kaposi’s sarcoma in kidney recipients. Arch Intern Med 1974; 133:307-311.
54. O’Brien PH, Brasfield RD. Kaposi’s sarcoma. Cancer 1966; 19: 1497- 1502.
5 5 . Oettle AG. Geographical and racial differences in the fre- quency of Kaposi’s sarcoma as evidence of environmental or genetic causes. Acta Unio Int Cont Cancer 1962; 18:330-363.
56. Osbome ED, Jordan JW, Hoak FC, Pschierer FJ. Nitrogen mustard therapy in cutaneous blastomatous disease. JA MA 1947;
57. Pack GT, Davis J. Concomitant occurrence of Kaposi’s sar- coma and lymphoblastoma. Arch Dermatol 1954; 69:604-611.
58. Pannacciulli I, Bottino G, Lapertosa G, Maiello M. Associazone tra leucemia linfatica cronica e morbo di Kaposi a local- izzazione cutanea, linfonodale e splenica. Pathologica 1975; 67:205-2 15.
59. Penn I , Halgrimson GC, Starzl TE. De Novo malignant tumors in organ transplant recipients. Transplant Proc 1971; 3:773-778.
60. Pohle EA, Clark EA. Kaposi’s sarcoma or lymphogranulo- matosis cutis: report of a case treated with roentgen rays. Urol Cutan Rev 1947; 51:382-385.
61. Rajka G. Kaposi‘s sarcoma associated with Hodgkin’s disease. Actn Derrnntol Venereol 1965; 45:40-43.
62. Ramos CV, Taylor HB, Hernandez BA, Tucker EF. Primary
135:1123- 1128.

No. 5 KAPOSI'S SARCOMA . Ulbright and Santa Cruz 973
Kaposi's sarcoma of lymph nodes. Am J Clin Pathol 1976: 66:998- 1003.
63. Reynolds WA, Winkelmann RK, Soule EH. Kaposi's sarcoma: a clinicopathologic study with particular reference to its relationship to the reticuloendothelial system. Medicine 1965: 44:4 19-443.
64. Rosen I . Idiopathic hemorrhagic sarcoma and lymphatic leu- kemia. Ard7 Dertnatol S.vph 1943: 48:566.
65. Rothman S. Some clinical aspects of Kaposi's sarcoma in the European and North American population. Acfa Unio In! Con/ Crrr7ccr 1962: 18:364-371.
66. Rywlin A , Recher L, Hoffman EP. Lymphoma-like presenta- tion of Kaposi's sarcoma. Arch Dermcrtol 1966: 9 3 3 4 - 5 6 1 .
67. Schnitzer B. Reed-Sternberg-like cells in lymphocytic lymphoma and chronic lymphocytic leukemia. Lancet 1970; 1: 1399- 1400.
68. Schwartz RS. Immunoregulation, oncogenic viruses, and malignant lymphomas. Lancet 1972; 1: 1266-1269.
69. Siegels JH. Janis R, Alper JC. Schutte H, Robins L, Blaufox D. Disseminated visceral Kaposi's sarcoma: appearance after human renal homograft operation. JAMA 1969: 207: 1493- 1496.
70. Simpson CL, Regelson W, Lessman F. Clinicopathologic con- ference. N Y Sttrtr Mrrl J 1959; 59:4589-4597.
7 1 . Starzl TE. Iatrogenic alterations of immunologic surveillance in man and their influence on malignancy. Trcrnsplant Rev 1971; 7: I I ? - 145.
72. Strachy CJ 111, Santos J I , Downey DM, Lewin KJ. Kaposi's
sarcoma in a renal transplant recipient. Arch Pothol 1975: 99:611- 613.
73. Tavida HB, Goudu RB, Nicoll WB. Inhibition of normal lymphocyte transformation by plasma and lymphocyte factors in CLL. Clin Exp Immunol 1974: 16: 177- 182.
74. Tedeschi CG, Folsom HF, Carnicelli TJ. Visceral Kaposi's disease. Arch Pathol 1947; 43:335-357.
75. Thijs A. L'angiosarcomatose de Kaposi au Congo belge et au Ruanda-Urundi. Ann Soc Belg Med Trop 1957: 37:295-308.
76. Uys CJ, Bennett MB. Kaposi's sarcoma: a neoplasm of reticu- lar origin. S Afr J Lab Clin Med 1959; 5:39-48.
77. Waldmann TA, Strober W, Blaese RM. Immunodeficiency dis- ease and malignancy: various immunological deficiencies of man and the role of immune process in the control of malignant disease. Ann Intern Mcd 1972; 77:605-628.
78. Warner TFCS, O'Loughlin S. Kaposi's sarcoma: a byproduct of tumor rejection. Lancet 1975; 2:687-689.
79. Weshler 2, Leviatan A, Krasnokuki D, Kopolovitch J. Primary Kaposi's sarcoma in lymph nodes concurrent with chronic lymphocytic leukemia. A m J Clin Pathol 1979: 71:234-237.
80. Willis RA. Pathology of Tumors. St. Louis: C. V. Mosby, 1948:780.
81. Wilson PR, Nishiyama RH. Lymph nodal Kaposi's sarcoma and chronic lymphocytic leukemia associated with a hepatic nodule simulating Hodgkin's disease. Concer 1971 ; 27: 1419- 1425.
82. Winer LH. Mycosis fungoides: benign and malignant reticu- lum cell dysplasia. Arch Dermatol Syph 1947; 56:480-498.
Related Documents











