Original contribution Juxtaglomerular cell tumor: A morphological, immunohistochemical and genetic study of six cases ☆,☆☆,★ Naoto Kuroda MD a , Sperga Maris MD b , Federico A. Monzon MD c , Puay Hoon Tan MD, FRCPA d , Anjula Thomas MD e , Fredrik B. Petersson MD, PhD f , Zoran Gatalica MD, DSc g , Anatole Ghazalpour, PhD g , Ryan P. Bender, PhD g , Petr Grossmann MSc h , Michal Michal MD h , Marian Svajdler MD i , Zdenka Ovcak MD j , Milan Hora MD, PhD k , Ondrej Hes MD, PhD h, ⁎ a Department of Diagnostic Pathology, Kochi Red Cross Hospital, Kochi 780-8562, Japan b Department of Pathology, Riga East University, Riga LV-1038, Latvia c Department of Pathology and Genomic Medicine, The Methodist Hospital and The Methodist Hospital Research Institute, Houston, TX 77030, USA d Department of Pathology, Singapore General Hospital, Singapore 169608 e Parkway Laboratories, Mount Elizabeth Hospital, Singapore 228510 f Department of Pathology, National University Health System Hospital, Singapore 119074 g Caris Life Sciences, Phoenix, AZ 85040, USA h Sikl's Department of Pathology, Charles University, Medical Faculty Plzen, Plzen 30460, Czech Republic i Department of Pathology, Pasteur´s University Hospital, Kosice 04190, Slovakia j Department of Pathology, University Hospital Ljubljana, Ljubljana 1000, Slovenia k Department of Urology, Charles University, Medical Faculty Plzen, Plzen 30599, Czech Republic Received 9 February 2012; revised 11 April 2012; accepted 11 April 2012 Keywords: Juxtaglomerular cell tumor; Virtual karyotyping; Fluorescence in situ hybridization; Whole genome expression array Summary Juxtaglomerular cell tumors (JGCTs) are rare tumors characterized by renin synthesis, hyperaldosteronism and hypertension. A curious immunohistochemical overlap between JGCT and gastrointestinal stromal tumor (GIST) including the expression of vimentin, CD34, CD117, α-smooth muscle actin was previously reported, prompting us to further investigate JGCT and its phenotypic and molecular genetic characteristics. Virtual karyotyping showed gain of chromosomes 3, 4, 10, 13, 17 and 18 in one JGCT, and fluorescence in situ hybridization (FISH) study confirmed this multiple gain pattern. Additionally, loss of chromosome 9 was observed in four of six cases analyzed with FISH. A whole genome expression analysis revealed 415 up-regulated (including renin, and CD117) and 325 down-regulated genes between the 2 cases. The study confirmed earlier reports on the gain of ☆ The study was supported in part by Czech Government grant agency: IGA NT 12010-4. ☆☆ The authors declare that they have no conflict of interest. ★ This study was approved by the ethical committee (receipt No.89) on the clinicopathological research of Kochi Red Cross Hospital, Kochi, Japan. * Corresponding author. Department of Pathology, Charles University, Medical Faculty and Charles University Hospital Plzen, Alej Svobody 80, 304 60 Pilsen, Czech Republic. E-mail address: [email protected] (O. Hes). www.elsevier.com/locate/humpath 0046-8177/$ – see front matter © 2013 Elsevier Inc. All rights reserved. http://dx.doi.org/10.1016/j.humpath.2012.04.006 Human Pathology (2013) 44, 47–54

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
www.elsevier.com/locate/humpath
Human Pathology (2013) 44, 47–54
Original contribution
Juxtaglomerular cell tumor: A morphological,immunohistochemical and genetic study ofsix cases☆,☆☆,★
Naoto Kuroda MDa, Sperga Maris MDb, Federico A. Monzon MDc,Puay Hoon Tan MD, FRCPAd, Anjula Thomas MDe, Fredrik B. Petersson MD, PhD f,Zoran Gatalica MD, DSc g, Anatole Ghazalpour, PhDg, Ryan P. Bender, PhDg,Petr Grossmann MSch, Michal Michal MDh, Marian Svajdler MD i, Zdenka Ovcak MD j,Milan Hora MD, PhDk, Ondrej Hes MD, PhDh,⁎
aDepartment of Diagnostic Pathology, Kochi Red Cross Hospital, Kochi 780-8562, JapanbDepartment of Pathology, Riga East University, Riga LV-1038, LatviacDepartment of Pathology and Genomic Medicine, The Methodist Hospital and The Methodist Hospital Research Institute,Houston, TX 77030, USAdDepartment of Pathology, Singapore General Hospital, Singapore 169608eParkway Laboratories, Mount Elizabeth Hospital, Singapore 228510fDepartment of Pathology, National University Health System Hospital, Singapore 119074gCaris Life Sciences, Phoenix, AZ 85040, USAhSikl's Department of Pathology, Charles University, Medical Faculty Plzen, Plzen 30460, Czech RepubliciDepartment of Pathology, Pasteur´s University Hospital, Kosice 04190, SlovakiajDepartment of Pathology, University Hospital Ljubljana, Ljubljana 1000, SloveniakDepartment of Urology, Charles University, Medical Faculty Plzen, Plzen 30599, Czech Republic
Received 9 February 2012; revised 11 April 2012; accepted 11 April 2012
P
0h
Keywords:Juxtaglomerular celltumor;Virtual karyotyping;Fluorescence in situhybridization;Whole genome expressionarray
Summary Juxtaglomerular cell tumors (JGCTs) are rare tumors characterized by renin synthesis,hyperaldosteronism and hypertension. A curious immunohistochemical overlap between JGCT andgastrointestinal stromal tumor (GIST) including the expression of vimentin, CD34, CD117, α-smoothmuscle actin was previously reported, prompting us to further investigate JGCT and its phenotypic andmolecular genetic characteristics. Virtual karyotyping showed gain of chromosomes 3, 4, 10, 13, 17 and18 in one JGCT, and fluorescence in situ hybridization (FISH) study confirmed this multiple gainpattern. Additionally, loss of chromosome 9 was observed in four of six cases analyzed with FISH. Awhole genome expression analysis revealed 415 up-regulated (including renin, and CD117) and 325down-regulated genes between the 2 cases. The study confirmed earlier reports on the gain of
☆ The study was supported in part by Czech Government grant agency: IGA NT 12010-4.☆☆ The authors declare that they have no conflict of interest.★ This study was approved by the ethical committee (receipt No.89) on the clinicopathological research of Kochi Red Cross Hospital, Kochi, Japan.* Corresponding author. Department of Pathology, Charles University, Medical Faculty and Charles University Hospital Plzen, Alej Svobody 80, 304 60
ilsen, Czech Republic.E-mail address: [email protected] (O. Hes).
046-8177/$ – see front matter © 2013 Elsevier Inc. All rights reserved.ttp://dx.doi.org/10.1016/j.humpath.2012.04.006
48 N. Kuroda et al.
chromosomes 4 and 10, and provided further evidence of up-regulation of the genes located on these 2chromosomes. For the first time our study indicated the importance of the loss of chromosome 9 andloss of expression of several tumor suppressor genes located on this chromosome as possiblepathogenetic events important in development of JGCT.© 2013 Elsevier Inc. All rights reserved.
1. Introduction
Juxtaglomerular cell tumor (JGCT) was first described byRobertson et al in 1967 and the present name was firstdesignated by Kihara et al in 1968 [1,2]. Approximately 100cases of JGCT have been reported to date [3-5], but only afew cases have been analyzed for chromosomal abnormal-ities [6-8]. Recently, virtual karyotyping using singlenucleotide polymorphisms (SNP) mapping array has beenapplied as a practical ancillary study for the classification ofrenal epithelial tumors [9-14]. Similarly, expression profilingwith microarrays has proven useful in elucidating the biologyof various tumors [15]. Curiously, an immunohistochemicaloverlap between JGCT and gastrointestinal stromal tumor(GIST) has been recently reported [16] including theexpression of CD34 and CD117 (c-Kit). In this article, wepresent new molecular genetic features of JGCT and discusstheir significance.
Table 1 Probes for aneuploidy detection of chromosomes 3,4, 6, 9, 10, 11, 13, 15, 17, 18, 21 and X
Chromosome Probe Locus
3 CEP 3 (D3Z1) 3p11.1-q11.1Alpha Satellite DNA
4 CEP 4 4p11-q11Alpha Satellite DNA
6 CEP 6 (D6Z1) 6p11.1-q11Alpha Satellite DNA
9 CEP 9 9p11-q11Alpha Satellite DNA
10 CEP 10 10p11.1-q11.1Alpha Satellite DNA
11 CEP 11 (D11Z1) 11p11.11-q11Alpha Satellite DNA
13 LSI 13 (RB1) 13q1415 CEP 15 (D15Z4) 15p11.1-q11.1
Alpha Satellite DNA17 CEP 17 (D17Z1) 17p11.1-q11.1
Alpha Satellite DNA18 CEP 18 (D18Z1) 18p11.1-q11.1
Alpha Satellite DNA21 LSI 21 21q22.13-22.2X CEP X (DXZ1) Xp11.1-q11.1
Alpha Satellite DNA
2. Materials and methods
2.1. Patients and specimen
Six archival samples of JGCT were collected from thepathological files of Riga East University, Singapore GeneralHospital and Charles University Hospital Plzen, including 2previously reported cases [4,17].
Routinely processed and stained sections (H&E) were usedin microscopic evaluation (by investigators N.K. and O.H).
2.2. Immunohistochemical examination
The immunohistochemical study was performed using aVentana Benchmark XT automated stainer (Ventana MedicalSystem, Inc., Tucson, AZ, USA). Antibodies against renin(AnaSpec, Inc., 1:100, San Jose, CA, USA), CD34 (My10,1:160, Beckton Dickinson, CA, USA), CD117(c-Kit)(poly-conal, 1:600, Dako, Glostrup, Denmark), PDGFR-α (poly-clonal, ;100, Spring Bioscience, Pleasanton, CA, USA), α-smooth muscle actin (ASMA)(1A4, 1:800, Dako), caldesmon(h-CD, 1:800, Dako), desmin (D33, prediluted, Dako), CD99(MIC2)(12E7, prediluted, Dako), bcl-2 oncoprotein (124,prediluted, Dako) and β-catenin (polyclonal, 1:1000, ThermoScientific, Fremont, CA) were applied.
2.3. Ultrastructural examination
Small pieces of the formaldehyde-fixed wet tissue of 3cases were postfixed in glutaraldehyde and routinelyprocessed by electron microscopy.
Table 2 Clinical information of six cases of juxtaglomerularcell tumor
Case Age Sex Tumorsize (cm)
Hypertension Outcome
1 22 F 2.3 + HT persistspostoperatively
2 32 F 3.2 + NA3 24 F 1.5 + NA4 24 F 2.5 + HT disappears
postoperatively5 24 F 4.5 + HT disappears
postoperatively6 33 M 2.5 + NA
Abbreviations: F, female; M, male; +, present; NA, not available; HT,hypertension.
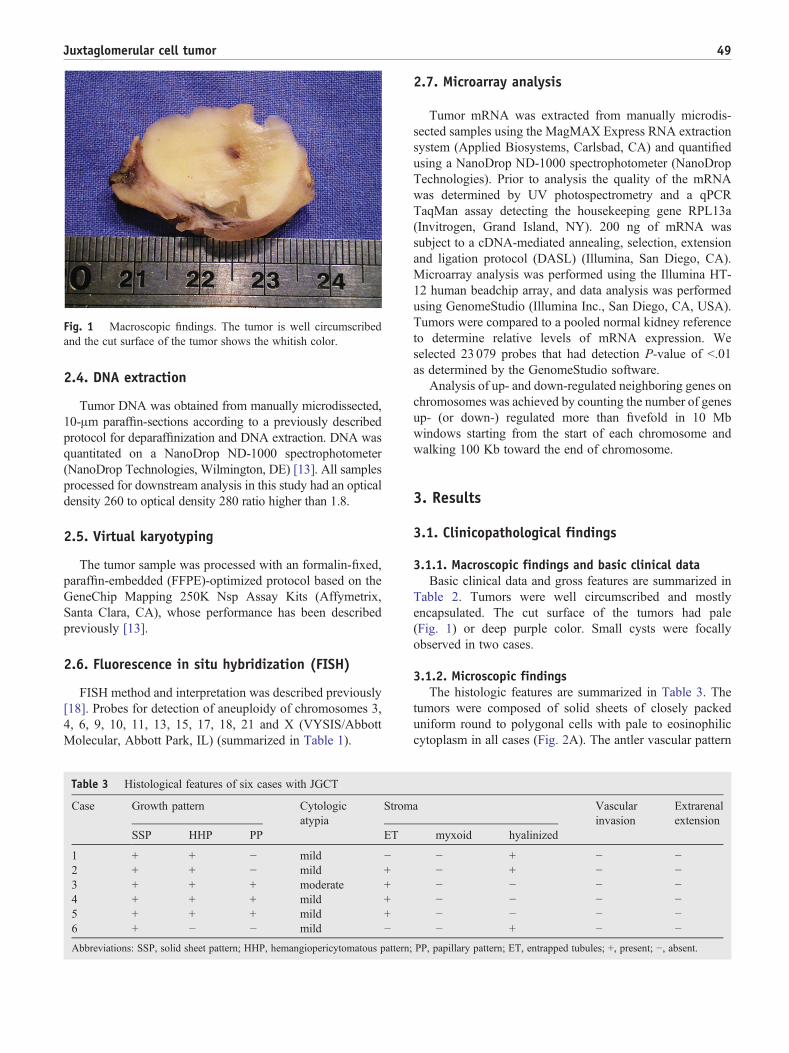
Fig. 1 Macroscopic findings. The tumor is well circumscribedand the cut surface of the tumor shows the whitish color.
49Juxtaglomerular cell tumor
2.4. DNA extraction
Tumor DNA was obtained from manually microdissected,10-μm paraffin-sections according to a previously describedprotocol for deparaffinization and DNA extraction. DNA wasquantitated on a NanoDrop ND-1000 spectrophotometer(NanoDrop Technologies, Wilmington, DE) [13]. All samplesprocessed for downstream analysis in this study had an opticaldensity 260 to optical density 280 ratio higher than 1.8.
2.5. Virtual karyotyping
The tumor sample was processed with an formalin-fixed,paraffin-embedded (FFPE)-optimized protocol based on theGeneChip Mapping 250K Nsp Assay Kits (Affymetrix,Santa Clara, CA), whose performance has been describedpreviously [13].
2.6. Fluorescence in situ hybridization (FISH)
FISH method and interpretation was described previously[18]. Probes for detection of aneuploidy of chromosomes 3,4, 6, 9, 10, 11, 13, 15, 17, 18, 21 and X (VYSIS/AbbottMolecular, Abbott Park, IL) (summarized in Table 1).
Table 3 Histological features of six cases with JGCT
Case Growth pattern Cytologicatypia
Strom
SSP HHP PP ET
1 + + − mild −2 + + − mild +3 + + + moderate +4 + + + mild +5 + + + mild +6 + − − mild −
Abbreviations: SSP, solid sheet pattern; HHP, hemangiopericytomatous pattern;
2.7. Microarray analysis
Tumor mRNA was extracted from manually microdis-sected samples using the MagMAX Express RNA extractionsystem (Applied Biosystems, Carlsbad, CA) and quantifiedusing a NanoDrop ND-1000 spectrophotometer (NanoDropTechnologies). Prior to analysis the quality of the mRNAwas determined by UV photospectrometry and a qPCRTaqMan assay detecting the housekeeping gene RPL13a(Invitrogen, Grand Island, NY). 200 ng of mRNA wassubject to a cDNA-mediated annealing, selection, extensionand ligation protocol (DASL) (Illumina, San Diego, CA).Microarray analysis was performed using the Illumina HT-12 human beadchip array, and data analysis was performedusing GenomeStudio (Illumina Inc., San Diego, CA, USA).Tumors were compared to a pooled normal kidney referenceto determine relative levels of mRNA expression. Weselected 23 079 probes that had detection P-value of b.01as determined by the GenomeStudio software.
Analysis of up- and down-regulated neighboring genes onchromosomes was achieved by counting the number of genesup- (or down-) regulated more than fivefold in 10 Mbwindows starting from the start of each chromosome andwalking 100 Kb toward the end of chromosome.
3. Results
3.1. Clinicopathological findings
3.1.1. Macroscopic findings and basic clinical dataBasic clinical data and gross features are summarized in
Table 2. Tumors were well circumscribed and mostlyencapsulated. The cut surface of the tumors had pale(Fig. 1) or deep purple color. Small cysts were focallyobserved in two cases.
3.1.2. Microscopic findingsThe histologic features are summarized in Table 3. The
tumors were composed of solid sheets of closely packeduniform round to polygonal cells with pale to eosinophiliccytoplasm in all cases (Fig. 2A). The antler vascular pattern
a Vascularinvasion
Extrarenalextension
myxoid hyalinized
− + − −− + − −− − − −− − − −− − − −− + − −
PP, papillary pattern; ET, entrapped tubules; +, present; −, absent.

Fig. 2 Pathological findings, HE. A, The tumor consists of solid sheets of closely packed uniform round to polygonal cells with pale toeosinophilic cytoplasm, 100×. B, The hemangiopericytomatous vascular pattern is seen, 100×. C, Nuclei of tumor cells show oval to round andnucleoli are inconspicuous, 200×. D, Focal moderate nuclear atypia is seen, 400×.
50 N. Kuroda et al.
simulating hemangiopericytoma was seen in five cases(Fig. 2B). Papillary growth pattern was identified focally inthree cases. The cell borders were indistinct. Nuclei wereoval to round and nucleoli were generally inconspicuous(Fig. 2C). Significant mitotic activity or abnormal mitoticfigures were absent in all cases, but focal moderate nuclearatypia was seen in one tumor (Fig. 2D). Entrapped tubulesand stromal hyalinization were identified in four and three
Table 4 Immunohistochemical results of six cases of JGCT
Case Renin CD34 CD117 ASMA h-caldesmon
1 d,++ d, ++ f, + f, + f, +2 d,++ d, ++ − − −3 d,++ d, ++ − f, + −4 d,++ d, ++ f, + − −5 d,++ d, ++ f, + − −6 d,++ − − − f, +
Abbreviations: ASMA, a-smooth muscle actin; d, diffuse; f, focal; ++, strongly
cases, respectively. No myxoid stroma was identified in anyof the tumors. No tumor showed penetration of the fibrouscapsule, necrosis or vascular invasion.
3.2. Immunohistochemical findings
The immunohistochemical results are summarized inTable 4. Neoplastic cells showed diffuse and strong
PDGFR-α Desmin CD99 bcl-2 β-catenin
f, + f, + − − +f, + − − − ++d, + f, + − − NAd, + − − − NAd, + − − − +f, + − − − ++
positive; +, positive; −, negative; NA, not anayzable.

51Juxtaglomerular cell tumor
immunoreactivity for renin (Fig. 3A) and CD34 in 6/6 and 5/6 cases, respectively. Focal immunoreactivity for CD117(Fig. 3B), α-smooth muscle actin and h-caldesmon wasidentified in 3/6, 2/6 and 2/6 cases, respectively. PDGFR-α
Fig. 3 Immunohistochemical findings. A, Renin is diffuselydistributed in the tumor cytoplasm, 40×. B, CD117 demonstrates afocal immunolabeling in the cytoplasm, 200×. C, Tumorous cellsshow diffuse nuclear labeling for β-catenin, 40×.
was expressed in all cases (focally in three and diffuselypositive in three cases). Desmin was focally positive in 2/6cases. JGCT cells were negative for CD99 or bcl-2. Nuclearexpression of β-catenin was identified in 4/4 cases analyzed(Fig. 3C).
3.3. Ultrastructural findings
Ultrastructural examination of three cases (cases # 3,4,6)revealed rhomboid-shaped renin protogranules within cyto-plasm of tumorous cells (Fig. 4).
3.4. Virtual karyotyping findings
Only one tumor (case #4) gave adequate results on thevirtual karyotyping assay. Two other tumors analyzed failedthe assay due to low DNA quality. The chromosomalabnormalities of the successful tumor were: +3, +4, +10,+13, +17 and +18 (Fig. 5).
3.5. FISH findings
FISH results are summarized in Table 5. Monosomy ofchromosome 9 was identified in 4/6 cases. Monosomyof chromosome 15 was found in 2/6 cases, and monosomy ofchromosome 11 was seen in 1/6 case. In case # 4, polysomyof chromosomes 3, 4, 10, 13, 17 and 18 was observed, andthese results agreed with results from virtual karyotype.Polysomy of chromosome 3 was also present in case # 3.
3.6. Tumor mRNA expression array
Two tumors were analyzed using whole transcriptomeexpression profiling. We arbitrarily set the threshold of 5-fold change to identify 415 genes that were up-regulated and325 genes that were down-regulated between bothcases. Table 6 shows the number of neighboring genes that
Fig. 4 Rhomboid-shaped protogranules of renin within cyto-plasm of tumorous cells.

Fig. 5 Finding of virtual karyotyping in case # 4. The gain of chromosomes 3, 4, 10, 13, 17 and 18 was identified.
52 N. Kuroda et al.
were up- and down- regulated and their location onchromosomes (1-22 and X-chromosome). Renin was up-regulated in both cases, 36 and 84 times, respectively.Table 6 lists some of the genes (based on their function suchas tumor suppressors, or location on chromosome 9, whichwas commonly deleted in our series) whose mRNAtranscripts were fivefold or more down regulated. Analysisof fivefold or more over-expressed genes (Table 7) locatedon chromosomes 4 and 10 revealed 43 individual genes andalso identified 2 oncogenes: BMI1, a component of aPolycomb group (PcG) multiprotein PRC1-like complex,and KIT.
4. Discussion
JGCT is a rare renal neoplasm clinically characterized byrenin production, hyperaldosteronism and hypertension.Therefore, these clinical features are very important for anaccurate diagnosis. However, the non-functioning varianthas also been reported [1-5]. Although JGCTs are generallyconsidered as benign lesions, at least one metastatic tumorwas reported [19].
Microscopic differential diagnosis of JGCT includesglomus tumor (GT), hemangiopericytoma (HP) and solitaryfibrous tumor (SFT) [4,5,20]. GT commonly display, amyxoid-edematous stroma and contains no epithelial com-ponent. GTs are most often immunohistochemically reactivefor α-smooth muscle actin and/or h-caldesmon [21,22], andare negative for CD34 and renin [23]. HP/SFT lackspolygonal cells and thick-walled vessels. SFTs often containa hemangiopericytomatous (“stag-horn”) vascular patternand are frequently located in close proximity to the renal
Table 5 Fluorescence in situ hybridization results
Case CEP3 CEP4 CEP6 CEP9 CEP10 CEP11
1 NA D NA M D NA2 D D D M D M3 P D D M* D D4 P P D D P D5 D D D M D D6 X NA NA NA NA NA
Abbreviations: D, disomy; M, monosomy; M*, borderline monosomy (45.2%);
pelvis or renal capsule. SFT is also positive for CD99 andbcl-2 [24,25]. In a study by Kim et al [16], an interesting andunexpected immunohistochemical overlap between JGCTand GIST was observed, including strong expression ofCD34 and c-Kit. Using the same immunohistiochemicalmethods, we confirmed these findings and also demonstratedincreased mRNA expression of KIT in 2 cases analyzed bythe gene expression profiling. We further observed addition-al overlap in the immunohistochemical features betweenJGCT and GIST demonstrating expression of PDGFR-α inall of our cases.
The studies on genetic abnormalities of JGCT are few.Brandal et al reported the study of three JGCTs usingconventional cytogenetics, comparative genomic hybridiza-tion (CGH) and interphase FISH [6]. They suggested that gainof chromosome 10 as well as losses of chromosomes 9 and Xand most of chromosome 11q may be important events in thepathogenesis of JGCT. In another reported case, the tumorexhibited loss of chromosomes X, 6, 9, 11, 15 and 21 usingFISH analysis [7]. Another study using CGH reported lossesof chromosomes 9 and 11 in two JGCT tumors [8]. In thepresent study, gain of chromosomes 3, 4, 10, 13, 17 and 18were observed in one JGCT with virtual karyotype andconfirmed by FISH analyses. Additionally, loss of chromo-some 9 was observed in the majority of cases using FISHanalysis. Of these abnormalities, gains of chromosomes 4 and10 are consistent with the observations of Brandal et al. [6].These results raise the possibility that the oncogene(s) ortumor suppressor gene(s) responsible for the pathogenesis ofJGCT may be localized on chromosome 4 and 10, orchromosome 9 and 11, respectively. The chromosomalabnormalities found on JGCT show that this tumor has adistinct genomic profile when compared to other renal tumors[9,11,14]. Despite the overlap in immunohistochemical
LSI13 CEP15 CEP17 CEP18 LSI21 CEPX
NA NA D D NA NAD M D D D DD D D D D DP NA P P D DD M D D D DX NA X X NA NA
P, polysomy; NA, not analyzable.
Table 7 Selected up-regulated (fivefold or more) genes(symbols), chromosomal sublocation and functionaldescription (as provided by Gene Cards, http://www.genecards.org/) in 2 cases of JGCT analyzed by the wholegenome expression microarray
Genesymbol
Chromosomallocation
Functional description
BM1 10p12.2 Polycomb ring finger oncogeneKIT 4q12 type 3 transmembrane receptor for
MGF (mast cell growth factor, alsoknown as stem cell factor)
PIP4K2A 10p12.2 Phosphatidylinositol-5-phosphate 4-kinase, type II, alpha;Phosphatidylinositol-5,4-bisphosphate is the precursor tosecond messengers involved in theregulation of secretion, cellproliferation, differentiation, andmotility
TLX1 10q24.31 A nuclear transcription factor that
53Juxtaglomerular cell tumor
profiles, we found little if any overlap in chromosomalchanges between JGCT and GIST [26].
The gene expression profiling of the cases reported in ourstudy was done using whole-genome DASL assay (IlluminaInc., San Diego, CA) which has been shown to provide ahighly reliable and reproducible platform for genome-wideexpression profiling in archived materials [27].
Gene expression profiling confirmed renin over-expression in the 2 cases analyzed. The cause of highrenin expression in JGCT is not known. It is known thatTNF-α inhibits renin transcription [28] and we observedoverexpression of TNIP3, a negative regulator of TNF-α inboth tumors, analyzed. Overexpression of KIT mRNA inthese two tumors was consistent with IHC findings. Severalnovel observations were made utilizing the whole genomeexpression approach. Two types of protein phosphatases(PTPRT and PPP2R3B) were found down-regulated inJGCT (Table 6). Protein tyrosine phosphatases (PTPs)constitute a large family of enzymes that can exert both
Table 6 Selected down-regulated (fivefold or more) genes(symbols), chromosomal sublocation and functionaldescription (as provided by Gene Cards, http://www.genecards.org/) in 2 cases of JGCT analyzed by the wholegenome expression microarray
Genesymbol
Chromosomallocation
Functional description
LRSAM1 9q33.3 A multifunctional RING fingerprotein that selectively regulates celladhesion molecules, has ubiquitinligase activity, and plays a role inreceptor endocytosis
PTPRT 20q12-q13 Protein tyrosine phosphatase (PTP),receptor type; PTPs are knownsignaling molecules that regulate avariety of cellular processesincluding cell growth,differentiation, mitotic cycle, andoncogenic transformation.
GRIN1 9q34.3 Critical subunit of N-methyl-D-aspartate receptors, members of theglutamate receptor channelsuperfamily
GNG10 9q31.3 Guanine nucleotide-binding proteingamma 10
DNM1 9q34.11 A member of the dynaminsubfamily of GTP-binding proteins;Involved in receptor-mediatedendocytosis
CTSL1 9q21.33 Lysosomal cysteine proteinase thatplays a major role in intracellularprotein catabolism
PPP2R3B Xp22.33 Protein phosphatase 2 (formerlynamed type 2A) is one of the fourmajor Ser/Thr phosphatases and isimplicated in the negative control ofcell growth and division.
belongs to the NK-linked or NK-like(NKL) subfamily of homeoboxgenes. Ectopic expression of thisgene due to chromosomaltranslocations is associated withcertain T-cell acute lymphoblasticleukemias.
TNIP3 4q27 Inhibits NF-kappa-B activationinduced by tumor necrosis factor
positive and negative effects on signaling pathways. Theyplay dominant roles in setting the levels of intracellularphosphorylation downstream of many receptors includingreceptor tyrosine kinases and G protein-coupled receptors.As observed with kinases, deregulation of PTP activity canalso contribute to cancer [29]. Over-expression of BMI1mRNA was observed in 2 cases analyzed (Table 7), whichis a component of Polycomb Repressive Complex 1(PRC1), required to maintain the transcriptionally repres-sive state of many genes. The expression of BMI1 mRNAin human colon cancers is significantly associated withnuclear β-catenin, a hallmark for the activated Wntsignaling [30]. Similarly, we found that in the majority ofJGCT analyzed, β-catenin showed abnormal, nuclearlocalization. These data indicate that deregulation of theWnt signaling pathway may be important in pathogenesisof JGCT, and additional focused research in the mutationsof the Wnt pathway genes (eg, APC), as well as KIT andPDGFRA, may prove useful in elucidating the pathophys-iology of this rare neoplasm.
References
[1] Robertson PW, Klidijan A, Harding LK, Walters G, Lee MR, Robb-Smith AHT. Hypertension due to a renin-secreting renal tumor. Am JMed 1967;43:963-76.

54 N. Kuroda et al.
[2] Kihara I, Kitamura S, Hoshino T, Sieda H, Watanabe T. A hithertounreported vascular tumor of the kidney: A proposal of “juxtaglo-merular cell tumor”. Acta Pathol Jpn 1968;18:197-206.
[3] Kodet R, Taylor M, Vachalova H, Pycha K. Juxtaglomerular celltumor. An immunohistochemical, electron-microscopic, and in situhybridization study. Am J Surg Pathol 1994;18:837-42.
[4] Ng SB, Tan PH, Chuah KL, Cheng C, Tan J. A case of juxtaglomerularcell tumor associated with membranous glomerulonephritis. AnnDiagn Pathol 2003;7:314-20.
[5] Kuroda N, Gotoda H, Ohe C, et al. Review of juxtaglomerular celltumor with focus on pathobiological aspect. Diagn Pathol 2011;6:80.
[6] Brandal P, Busund L-T, Heim S. Chromosome abnormalities injuxtaglomerular cell tumors. Cancer 2005;104:504-10.
[7] Shao L, Manalang M, Cooley L. Juxtaglomerular cell tumor in an8-year-old girl. Pediatr Blood Cancer 2008;50:406-9.
[8] Capovilla M, Couturier J, Molinie V, et al. Loss of chromosomes 9 and11 may be recurrent chromosomal imbalances in juxtaglomerular celltumors. HUM PATHOL 2008;39:459-62.
[9] Monzon FA, Hagnekord JM, Lyons-Weiler MA, et al. Whole genomeSNP arrays as a potential diagnostic tool for the detection ofcharacteristic chromosomal aberrations in renal epithelial tumors.Mod Pathol 2008;21:599-608.
[10] Hagenkord JM, Parwani AV, Lyons-Weiler MA, et al. Virtualkaryotyping with SNP microarrays reduces uncertainty in thediagnosis of renal epithelial tumors. Diagn Pathol 2008;3:44.
[11] Kim HJ, Shen SS, Ayala AG, et al. Virtual-karyotype with SNPmicroarrays in morphologically challenging renal cell neoplasms: Apractical and useful diagnostic modality. Am J Surg Pathol 2009;33:1276-86.
[12] Monzon FA, Alvarez K, Gatalica Z, et al. Detection of chromosomalaberrations in renal tumors: A comparative study of conventionalcytogenetics and virtual karyotyping with single-nucleotide polymor-phism microarrays. Arch Pathol Lab Med 2009;133:1917-22.
[13] Alvarez K, Kash SF, Lyons-Weiler MA, et al. Reproducibility andperformance of virtual karyotyping with SNP microarrays for thedetection of chromosomal imbalances in formalin-fixed paraffin-embedded tissues. Diagn Mol Pathol 2010;19:127-34.
[14] Powers MP, Alvarez K, Kim HJ, Monzon FA. Molecular classificationof adult renal epithelial neoplasms using microRNA expression andvirtual karyotype. Diagn Mol Pathol 2011;20:63-70.
[15] Golub TR, Slonim DK, Tamayo P, et al. Molecular classification ofcancer: class discovery and class prediction by gene expressionmonitoring. Science 1999;286:531-7.
[16] Kim HJ, Kim CH, Choi YJ, Ayala AG, Amirikachi M, Ro JY.Juxtaglomerular cell tumor of kidney with CD34 and CD117immunoreactivity. Report of 5 cases. Arch Pathol Lab Med 2006;130:707-11.
[17] Lachvac L, Svajdler M, Valansky L, et al. Juxtaglomerular cell tumor,causing fetal demise. Int Urol Nephrol 2011;43:365-70.
[18] Petersson F, Gatalica Z, Grossmann P, et al. Sporadic hybridoncocytic/chromophobe tumor of the kidney: a clinicopathologic,histomorphologic, immunohistochemical, ultrastructural, and molec-ular genetic study of 14 cases. Virchows Arch 2010;456:355-66.
[19] Duan X, Bruneval P, Hammadeh R, et al. Metastatic juxtaglomerularcell tumor in a 52-year-old man. Am J Surg Pathol 2004;28:1098-102.
[20] Martin SA, Mynderse LA, Lager DJ, Cheville JC. Juxtaglomerular celltumor. A clinicopathologic study of four cases and review of theliterature. Am J Clin Pathol 2001;116:854-63.
[21] Al-Ahmadie HA, Yilmaz A, Olgac S, Reuter VE. Glomus tumor of thekidney: A report of 3 cases involving renal parenchyma and review ofthe literature. Am J Surg Pathol 2007;31:585-91.
[22] Siddiqui NH, Rogalska A, Basil LS. Glomangiomyoma (glomustumor) of the kidney. Arch Pathol Lab Med 2005;129:1172-4.
[23] Kuroda N. Glomus tumor of the kidney. Int J Urol 2011;18:871,http://dx.doi.org/10.1111/j.1442-2042.2011.02853.x Epub 2011Oct 11.
[24] Gelb AB, Simmons ML, Weidner N. Solitary fibrous tumor involvingthe renal capsule. Am J Surg Pathol 1996;20:1288-95.
[25] Hasegawa T, Matsuno Y, Shimoda T, Hasegawa F, Sano T,Hirohashi S. Extrathoracic solitary fibrous tumors: their histologicalvariability and potentially aggressive behavior. HUM PATHOL 1999;30:1464-73.
[26] Antonescu CR, Wu K, Xing GL, et al. DNA copy number analysis ingastrointestinal stromal tumors using gene expression microarrays.Cancer Inform 2008;6:59-75.
[27] April C, Klotzle B, Royce T, et al. Whole-genome gene expressionprofiling of formalin-fixed, paraffin-embedded tissue samples. PLoSOne 2009;4:e8162.
[28] Todorov VT, Völkl S, Müller M, et al. Tumor necrosis factor-alphaactivates NF(kappa)B-p65 to inhibit renin transcription by targetingcAMP-responsive element. J Biol Chem 2005;280:24356-62.
[29] Tonks NK. Protein tyrosine phosphatases: from genes, to function, todisease. Nat Rev Mol Cell Biol 2006;7:833-46.
[30] Yu T, Chen X, Zhang W, et al. Regulation of the Potential markerfor intestinal cells, Bmi1, by beta-catenin and the zinc finger proteinKLF4: implications for colon cancer. J Biol Chem 2012;287:3760-8.
Related Documents











