ORIGINAL ARTIC LE Malaria detection with the Sysmex XE-2100 hematology analyzer using pseudoeosinophilia and abnormal WBC scattergram Hee Jin Huh & Gwi Young Oh & Jung Won Huh & Seok Lae Chae Received: 2 January 2008 /Accepted: 8 March 2008 /Published online: 22 April 2008 # Springer-V erlag 2008 Abstract Recent investigation using the Sysmex XE-2100 hema tology analy zer (Sys mex Cor pora tion, Japa n) has demonst rated erroneously high eosinophil counts and abnormal white blood cell (WBC) scattergrams in malaria cases. This study was conducted to assess the diagnostic effi cie ncy of the Sys mex XE- 2100 ana lyz er for mala ria . One hun dre d for ty-f our pat ients ini tial ly dia gno sed with Plasmodium vivax infe cti on, 319 pat ients with febril e illness, and 24 patients who underwent malaria treatment were analy zed . Aty pic al fea tures on Sysmex XE- 2100 analyzer were categorized as pseudoeosinophilia (a gap of more tha n 5% in eos inop hil count s bet ween the Sys mex XE-2100 anal yzer and microscopic examination) and abnormal WBC scattergram. Pseudoeosinophilia or abnor- mal WBC scattergram were detected in 100 of 144 malaria- positive samples (sensitivity 69.4%, specificity 100%). The samples with pseudoeosinophilia or abnormal WBC scatter- grams showed significantly higher parasite counts than the samples without pseudoeosinophilia or an abnormal WBC scatter gram ( P <0.05) . Al l 24 samples fr om pati ents for whom the mal aria smear was repeated after malar ia trea tme nt was ini tiat ed sho wed a nor mali zed eos inophi l count and a norma l WBC histogram. In conclus ion, atte nti on to dif fere ntial count and WBC scatter grams provided by the Sysmex XE-2100 would be a valuable tool in malaria detection. Keywords Malaria . Pseudoeosinophilia . Abnor mal WBC scattergram . Sysmex XE-210 0 hemato logy analyz er Introduction Malari a is dia gnosed usi ng a combination of cli nic al observations, case history, and diagnostic tests, principally microscopic examinati on of stained slides. However, classical micr osc opi c examination is labor int ensive and time consuming. Limitatio ns of malaria diagnos is using this method have led to the development of several new techniques that simplify and speed up diagnosis and increase sensitivity [ 1]. However, these all rely on clinical suspici on and, consequent ly , a clinic al request . Althou gh some methods lend themselves to automation (e.g., poly- merase chain reaction) [2], no technique can yet be used for routin e clinica l automa ted screeni ng. There is growing interest in the use of routine hemato- logical blood analysis as a component of measurement for the presumptive diagnosis of malaria infection [ 1, 3 ]. It has been reported that abnormal depolarizing patterns detected by a Cell-Dyn hematology analyzer (Abbott Diagnostics, Sant a, CA, USA) sho wed hi gh sensi tiv ity for malar ia Ann Hematol (2008) 87:755 – 759 DOI 10.1007/s00277-008-0486-8 H. J. Huh : S. L. Chae Department of Laboratory Medicine, College of Medicine, Dongguk University, Goyang, Republic of Korea G. Y. Oh Department of Laboratory Medicine, Eone Reference Laboratory, Seoul, Republic of Korea J. W. Huh Department of Laboratory Medicine, College of Medicine, Ewha Womans University, Seoul, Republic of Korea S. L. Chae (*) Department of Laboratory Medicine, Dongguk University International Hospital, Siksa-dong, Ilsandong-gu, Goyang-si, Gyeonggi-do 411-773, Republic of Korea e-mail: [email protected]

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

7/23/2019 Jurnal Malaria Tes
http://slidepdf.com/reader/full/jurnal-malaria-tes 1/5
ORIGINAL ARTICLE
Malaria detection with the Sysmex XE-2100 hematology
analyzer using pseudoeosinophilia and abnormal WBC
scattergram
Hee Jin Huh & Gwi Young Oh & Jung Won Huh &
Seok Lae Chae
Received: 2 January 2008 /Accepted: 8 March 2008 /Published online: 22 April 2008# Springer-Verlag 2008
Abstract Recent investigation using the Sysmex XE-2100
hematology analyzer (Sysmex Corporation, Japan) hasdemonstrated erroneously high eosinophil counts and
abnormal white blood cell (WBC) scattergrams in malaria
cases. This study was conducted to assess the diagnostic
efficiency of the Sysmex XE-2100 analyzer for malaria.
One hundred forty-four patients initially diagnosed with
Plasmodium vivax infection, 319 patients with febrile
illness, and 24 patients who underwent malaria treatment
were analyzed. Atypical features on Sysmex XE-2100
analyzer were categorized as pseudoeosinophilia (a gap of
more than 5% in eosinophil counts between the Sysmex
XE-2100 analyzer and microscopic examination) and
abnormal WBC scattergram. Pseudoeosinophilia or abnor-
mal WBC scattergram were detected in 100 of 144 malaria-
positive samples (sensitivity 69.4%, specificity 100%). The
samples with pseudoeosinophilia or abnormal WBC scatter-
grams showed significantly higher parasite counts than thesamples without pseudoeosinophilia or an abnormal WBC
scattergram ( P <0.05). All 24 samples from patients for
whom the malaria smear was repeated after malaria
treatment was initiated showed a normalized eosinophil
count and a normal WBC histogram. In conclusion,
attention to differential count and WBC scattergrams
provided by the Sysmex XE-2100 would be a valuable
tool in malaria detection.
Keywords Malaria . Pseudoeosinophilia . Abnormal WBC
scattergram . Sysmex XE-2100 hematology analyzer
Introduction
Malaria is diagnosed using a combination of clinical
observations, case history, and diagnostic tests, principally
microscopic examination of stained slides. However,
classical microscopic examination is labor intensive and
time consuming. Limitations of malaria diagnosis using this
method have led to the development of several new
techniques that simplify and speed up diagnosis and
increase sensitivity [1]. However, these all rely on clinical
suspicion and, consequently, a clinical request. Although
some methods lend themselves to automation (e.g., poly-
merase chain reaction) [2], no technique can yet be used for
routine clinical automated screening.
There is growing interest in the use of routine hemato-
logical blood analysis as a component of measurement for
the presumptive diagnosis of malaria infection [1, 3]. It has
been reported that abnormal depolarizing patterns detected
by a Cell-Dyn hematology analyzer (Abbott Diagnostics,
Santa, CA, USA) showed high sensitivity for malaria
Ann Hematol (2008) 87:755 – 759
DOI 10.1007/s00277-008-0486-8
H. J. Huh : S. L. Chae
Department of Laboratory Medicine, College of Medicine,
Dongguk University,
Goyang, Republic of Korea
G. Y. Oh
Department of Laboratory Medicine, Eone Reference Laboratory,
Seoul, Republic of Korea
J. W. Huh
Department of Laboratory Medicine, College of Medicine,
Ewha Womans University,
Seoul, Republic of Korea
S. L. Chae (*)
Department of Laboratory Medicine,
Dongguk University International Hospital,
Siksa-dong, Ilsandong-gu, Goyang-si,
Gyeonggi-do 411-773, Republic of Korea
e-mail: [email protected]

7/23/2019 Jurnal Malaria Tes
http://slidepdf.com/reader/full/jurnal-malaria-tes 2/5
diagnosis [4]. One advantage of this method is its potential
to detect cases where clinical suspicion does not lead to a
request for a malaria test [5]. A few cases of malaria-
infected patients with pseudoeosinophilia on the Sysmex
XE-2100 hematology analyzer (Sysmex Corporation, Kobe,
Japan) were recently reported [6]. Moreover, abnormal
white blood cell (WBC) histograms were found in many
malaria-infected patients.The aim of this study was to determine the usefulness of
pseudoeosinophilia and abnormal WBC scattergrams, as
detected by the Sysmex XE-2100 analyzer, for the
diagnosis of malaria in a routine laboratory setting.
Materials and methods
The study group comprised a total of 487 samples from
patients for whom complete blood cell analysis and malaria
smears had been requested. Malaria patient group contained
144 patients that were initially diagnosed with Plasmodium
vivax infection (114 males and 30 females) and 24 patients
who underwent malaria treatment (18 males and six
females) at Dongguk University International Hospital and
Eone Reference Laboratory between June 2006 and
October 2007. Two hundred forty-two patients who
presented to the emergency department with a febrile
illness without malaria at Dongguk University International
Hospital between July 2007 and January 2008 and 77
patients diagnosed as bacteremia at Dongguk University
International Hospital November 2007 and January 2008
were included in control group. The diagnosis of 242
febrile patients were as followed: acute gastroenteritis 30
patients; respiratory tract infection 92 patients; urinary tract
infection 29 patients; other bacterial infection 36 patients;
fever due to other causes 55 patients. The diagnosis of
malaria was made by examining Wright-stained thick and
thin blood smears.
For complete blood cell analysis, we used the Sysmex
XE-2100 hematology analyzer. This instrument differen-
tiates WBCs using side fluorescence and side-scattered
light. An organic acid reagent binds specifically to the
granules of eosinophils and allows them to be discriminated
from neutrophils based on their higher side-scatter signal
intensities. WBC differential plots were examined for
abnormal WBC scattergrams. Manual WBC differential
counting was also performed by microscopic examination
of Wright-stained smears. Atypical features were catego-
rized as pseudoeosinophilia (a gap of more than 5% in
eosinophil counts between the Sysmex XE-2100 analyzer
and microscopic examination) and abnormal WBC scatter-
gram. The sensitivity and specificity of malaria detection
using pseudoeosinophilia and abnormal WBC scattergrams
were determined.
Parasitemia was indirectly calculated by assessing the
parasite numbers during the counting of 200 WBCs in the
thin blood film and, thereby, converting this to the number
of parasites per microliter of blood. Based on the parasite
number related with fever [7], samples from malaria
patients were subgrouped as a low parasitemia group
(<500 uL−1) and a high parasitemia group (≥500 uL−1).
Statistical analysis was performed using the StatisticalPackage for the Social Sciences (SPSS) program (version
11.0 for Windows; SPSS Inc., Chicago, IL, USA). Pearson
χ2 test and Fisher ’s exact test was used to compare
categorical variables. Student ’s t -test was used to compare
continuous variables between groups. P values of <0.05
were considered significant.
Results
Pseudoeosinophilia and abnormal WBC scattergrams
Of the 144 samples from malaria patients, 56 (38.9%)
showed pseudoeosinophilia. In samples with pseudoeosino-
philia, the mean (standard deviation (SD)) neutrophil count
by microscopic examination and Sysmex XE-2100 analyzer
were 67.1% (17.9) and 56.4% (15.1), respectively. The
mean (SD) eosinophil counts determined by microscopic
examination and Sysmex XE-2100 analyzer were 0.6%
(1.0) and 15.9% (9.5), respectively.
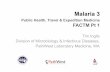
When compared to the normal WBC differential scatter-
gram (Fig. 1a), 75 samples from malaria patients showed
various abnormal features. The most strikingly noted
abnormal WBC scattergram was a nonclassified plot
extending from neutrophils toward the area of eosinophils
(n =33; Fig. 1 b). In these cases, neutrophils and eosinophil
counts are displayed as bars on the Sysmex XE-2100
analyzer. Other features encountered in malaria-positive
samples were two atypical eosinophil populations (n=31;
Fig. 1c), overlapping neutrophil and eosinophil populations
(n =7; Fig. 1d), and two neutrophil populations (n =4;
Fig. 1e). Among the 31 samples with two atypical
eosinophil populations, four samples simultaneously
showed two neutrophil populations (Fig. 1c).
Sensitivity and specificity
Using the abnormal WBC scattergrams for the initial
diagnosis, the sensitivity and specificity were 52.1% and
100%, respectively (Table 1). Using pseudoeosinophilia for
the initial diagnosis, the sensitivity and specificity were
38.9% and 100%, respectively. Overall, pseudoeosinophilia
or an abnormal WBC scattergram was detected in 100 of
144 malaria-positive samples (sensitivity 69.4%, specificity
100%).
756 Ann Hematol (2008) 87:755 – 759

7/23/2019 Jurnal Malaria Tes
http://slidepdf.com/reader/full/jurnal-malaria-tes 3/5
According to Fisher ’s exact test, there was a significant
difference in frequency of pseudoeosinophilia or abnormal
WBC scattergram between malaria-positive samples and
control samples ( P <0.05).
Correlation of parasite count with pseudoeosinophilia
and abnormal WBC scattergram
The samples without pseudoeosinophilia or abnormal WBC
scattergrams showed significantly lower parasite counts
(517.9±866.3 uL−1 vs. 4,003.3±6,530.2 uL−1) and higher
pl at el et co un t (8 0, 97 7 ± 42 ,9 14 uL−1 v s. 5 4 ,6 00 ±
31,079 uL−1) than the samples with pseudoeosinophilia or
an abnormal WBC scattergram ( P <0.05; Table 2). Age,
sex, and WBC count were not different between the
samples with pseudoeosinophilia or an abnormal WBC
scattergram and the samples without pseudoeosinophilia or
an abnormal WBC scattergram ( P >0.05).
The sensitivity was 39.3% for the low parasitemia group
when pseudoeosinophilia or an abnormal WBC scattergram
was used for malaria detection, but this sensitivity increased
significantly, to 88.6%, for the high parasitemia group
(Table 3).
Follow-up results of malaria patients
During the treatment periods of 24 malaria patients, all cases
with an initial abnormal WBC scattergram and pseudoeosi-
nophilia were changed to normal. Among 24 samples, all
nine samples from patients who underwent treatment for less
than 3 days and had atypical features at initial diagnosis had a
normalized eosinophil count and WBC histogram.
a b c
ed
DIFF DIFF
DIFF DIFF
DIFF
Fig. 1 Abnormal WBC scatter-
grams generated by the Sysmex
XE-2100 hematology analyzer.
a Normal WBC differential
plots (blue neutrophil plots and
red eosinophil plots). b Non-
classified neutrophils and eosi-
nophils with the plot extending
from neutrophils toward the area
of eosinophils. c Two atypicaleosinophil populations and two
neutrophil populations. d Over-
lapping neutrophil and eosino-
phil populations. e Two
neutrophil populations
Table 1 Diagnostic efficiency
of the Sysmex-2100 analyzer
in malaria
Malaria Sensitivity
(%)
Specificity
(%) Negative
(n=319)
Positive
(n=144)
Pseudoeosinophilia 38.9 100
Positive 0 56
Negative 319 88
Abnormal WBC scattergram 52.1 100
Positive 0 75
Negative 319 69
Pseudoeosinophilia or abnormal WBC scattergram 69.4 100
Positive 0 100
Negative 319 44
Ann Hematol (2008) 87:755 – 759 757

7/23/2019 Jurnal Malaria Tes
http://slidepdf.com/reader/full/jurnal-malaria-tes 4/5
Discussion
Automated blood cell analyzers can detect cases of malaria
in the absence of clinical suspicion [1, 8]. Suspicious plots
should be checked by stained blood film. The Cell-Dyn
3500 was the first autoanalyzer that allowed the detection
of malaria during routine investigation by complete bloodcell analysis [5]. The Cell-Dyn 3500 appears to detect
hemozoin-containing leukocytes according to their depola-
rizing properties [3]. It is believed that hemozoin-laden
monocytes, which have ingested parasites, are the major
component of the defining abnormal population identified
using the Cell-Dyn method [8, 9]. Hemozoin-containing
neutrophils seemed to be misidentified as eosinophils [9].
Moreover, it was suggested that the Cell-Dyn 3500 could
detect intraerythrocytic pigmented malarial parasites in rare
circumstances, such as relatively high parasitemia or
osmotic resistance [3].
Pseudoeosinophilia was detected in samples from ma-
laria patients using the Sysmex XE-2100 analyzer [6, 10].
The Sysmex XE-2100 analyzer cannot differentiate hemo-
zoin-containing monocytes from normal monocytes. How-
ever, the instrument detects hemozoin-containing
neutrophils and classifies them incorrectly as eosinophils
due to considerable side light scattering, which causes a
diagnosis of pseudoeosinophilia [6]. In this study, the mean
difference in neutrophil counts between microscopic exam-
ination and the Sysmex XE-2100 analyzer was 11%, and
the mean difference in eosinophil counts was 15%. This
difference could be explained by the incorrect classification
of neutrophils as eosinophils. Eleven samples with a normal
eosinophil count and an abnormal WBC scattergram
showed two atypical eosinophil populations or two neutro-
phil populations. This suggests that the instrument also
shows hemozoin-containing neutrophils to be abnormally
scattered eosinophil or neutrophil populations without
pseudoeosinophilia. The number of hemozoin-containing
neutrophils has been identified as an adverse prognosticindicator [11, 12]. This raises the possibility that the use of
the Sysmex XE-2100 analyzer for malaria diagnosis in our
study could also be useful prognostically.
The sensitivity of Cell-Dyn for the diagnosis of malaria
was variable, ranging from 43 – 95% [4, 8, 13, 14], and the
specificity was reported to be as high as 96 – 100%. This
study is the first evaluation of the sensitivity and specificity
of the Sysmex SE 2100 analyzer for malaria diagnosis. The
overall sensitivity and specificity were 69.4% (100/144)
and 100% (319/319), respectively, in our study. It has been
suggested that the kinetics of pigment-containing WBCs
may vary between different populations and could be
related to the severity of infection and host immunity
factors [4, 8, 13, 15]. In agreement with this, not all patients
in our study showed pseudoeosinophilia or abnormal WBC
scattergrams.
Although an abnormal WBC scattergram on the Sysmex
XE-2100 analyzer is specific for malaria diagnosis, it is
impossible to pay attention to all WBC histograms to detect
malaria in the laboratory. Among 100 samples with
pseudoeosinophilia or an abnormal WBC scattergram, 56
samples showed pseudoeosinophilia and 33 samples
showed blank eosinophil counts. Among the other 11
samples with a normal eosinophil count and an abnormal
Table 3 Comparison of pseudoeosinophilia and abnormal WBC scattergram between the low parasitemia group and the high parasitemia group
Low parasitemia group (n=56) High parasitemia group (n=88) P value
Pseudoeosinophilia (%) 17.8 (15/56) 34.1 (30/88) 0.5
Abnormal WBC scattergram (%) 17.8 (15/56) 68.2 (60/88) 0.000
Pseudoeosinophilia or abnormal WBC scattergram (%) 39.3 (22/56) 88.6 (78/88) 0.000
Table 2 Comparison of
parasite counts between
samples with and without
atypical features on the
Sysmex XE-2100 analyzer
Parasite count (Mean ± SD (uL−1)) P value
Pseudoeosinophilia
Positive (n=56) 2437.4±3452.2 0.002
Negative (n =88) 376.7±1378.6
Abnormal WBC scattergram
Positive (n=75) 4659.5±7246.5 0.000
Negative (n =69) 1067.5±2013.2
Pseudoeosinophilia or abnormal WBC scattergram
Positive (n=100) 4003.3±6530.2 0.000
Negative (n =44) 517.9±866.3
758 Ann Hematol (2008) 87:755 – 759

7/23/2019 Jurnal Malaria Tes
http://slidepdf.com/reader/full/jurnal-malaria-tes 5/5
WBC scattergram, ten samples showed thrombocytopenia.
High incidence of thrombocytopenia has been reported in
malaria patients [16]. Disadvantage of detecting malaria
parasite by microscopic examination of stained slides is that
expertise and continuous training are required. Therefore,
the advantage of the Sysmex XE-2100 rather than micro-
scopic examination and Cell-Dyn is possible to suspect
malaria infection using high eosinophil count or uncountedeosinophil before review of slide or WBC scattergram.
After suspecting malaria infection in febrile patients due to
eosinophilia or a blank eosinophil count, careful review of
WBC histograms could be helpful in the diagnosis of
malaria. Interestingly, using pseudoeosinophilia and abnor-
mal WBC histograms, we detected several cases of malaria
during the recent 2 years without clinical suspicion.
This study demonstrated that samples with pseudoeosi-
nophilia or abnormal WBC scattergrams showed signifi-
cantly higher parasite counts than the samples without
pseudoeosinophilia or an abnormal WBC scattergram ( P <
0.05). Furthermore, the high parasitemia group showedhigher sensitivity for malaria diagnosis than the low
parasitemia group. These results are different from previous
studies using Cell-Dyn, which showed no correlation
between the amo unt of parasites and the abnormal
depolarizing pattern [4, 8, 13]. This difference could be
explained by the short half-life (6 – 7 hours) of neutrophils
compared with that of monocytes (2 – 3 weeks) [17].
Therefore, it is possible that recent parasites counts could
be reflected by the Sysmex XE-2100 abnormal WBC
scattergram.
In previous reports related to follow-up evaluation with
Cell-Dyn, samples of treated malaria with no residual
parasitemia showed abnormal depolarization [14, 18]. In
this study, pseudoeosinophilia and abnormal WBC scatter-
grams became normal within 3 days after the initiation of
treatment. The normalized eosinophil count and WBC
scattergram within a few days could be also explained by
the kinetics of hemozoin clearance, as the removal of
hemoglobin-containing neutrophils is faster than that of
hemoglobin-containing monocytes. If Sysmex XE-2100
analyzer is used as a clinical follow-up parameter for
eradication of malaria after treatment, further evaluation to
be applied to a larger cohort of patients is needed.
In conclusion, the Sysmex XE-2100 analyzer has an
advantage in that it is able to detect unexpected malaria
cases. Considering its low sensitivity, hematological anal-
ysis performed with this instrument should not be consid-
ered an alternative to existing methods for the diagnosis of
malaria. However, attention to differential counts and WBC
scattergrams provided by Sysmex XE-2100 may be
valuable in the diagnosis of malaria.
References
1. Hanscheid T (1999) Diagnosis of malaria: a review of alternatives
to conventional microscopy. Clin Lab Haematol 21:235 – 245
2. Zalis MG, Ferreira-da-Cruz MF, Balthazar-Guedes HC, Banic
DM, Alecrim W, Souza JM, Druilhe P, Daniel-Ribeiro CT (1996)
Malaria diagnosis: standardization of a polymerase chain reaction
for the detection of Plasmodium falciparum parasites in individ-
uals with low-grade parasitemia. Parasitol Res 82:612 – 6163. Hanscheid T, Pinto BG, Cristino JM, Grobusch MP (2000)
Malaria diagnosis with the haematology analyser Cell-Dyn
3500: what does the instrument detect. Clin Lab Haematol
22:259 – 261
4. Hanscheid T, Melo-Cristino J, Pinto BG (2001) Automated
detection of malaria pigment in white blood cells for the diagnosis
of malaria in Portugal. Am J Trop Med Hyg 64:290 – 292
5. Hanscheid T, Pinto BG, Pereira I, Cristino JM, Valadas E (1999)
Avoiding misdiagnosis of malaria: a novel automated method
allows specific diagnosis, even in the absence of clinical
suspicion. Emerg Infect Dis 5:836 – 838
6. Huh J, Jung J, Yoon H, Chung W (2005) Pseudoeosinophilia
associated with malaria infection determined in the Sysmex XE-
2100 hematology analyzer. Ann Hematol 84:400 – 402
7. Boisier P, Jambou R, Raharimalala L, Roux J (2002) Relationship between parasite density and fever risk in a community exposed to
a low level of malaria transmission in Madagascar highlands. Am
J Trop Med Hyg 67:137 – 140
8. Mendelow BV, Lyons C, Nhlangothi P, Tana M, Munster M,
Wypkema E, Liebowitz L, Marshall L, Scott S, Coetzer TL (1999)
Automated malaria detection by depolarization of laser light. Br J
Haematol 104:499 – 503
9. Hanscheid T, Valadas E, Grobusch MP (2000) Automated malaria
diagnosis using pigment detection. Parasitol Today 16:549 – 551
10. Park GB, Cha YJ (2006) Three cases of pseudoeosinophilia
associated with malaria determined in the Sysmex XE-2100
Automated Hematology Analyzer. Korean J Lab Med 26:77 – 80
11. Nguyen PH, Day N, Pram TD, Ferguson DJ, White NJ (1995)
Intraleucocytic malaria pigment and prognosis in severe malaria.
Trans R Soc Trop Med Hyg 89:200 – 20412. Hanscheid T, Egan TJ, Grobusch MP (2007) Haemozoin: from
melatonin pigment to drug target, diagnostic tool, and immune
modulator. Lancet Infect Dis 7:675 – 685
13. Grobusch MP, Hanscheid T, Kramer B, Neukammer J, May J,
Seybold J, Kun JF, Suttorp N (2003) Sensitivity of hemozoin
detection by automated flow cytometry in non- and semi-immune
malaria patients. Cytometry B Clin Cytom 55:46 – 51
14. Suh IB, Kim HJ, Kim JY, Lee SW, An SS, Kim WJ, Lim CS
(2003) Evaluation of the Abbott Cell-Dyn 4000 hematology
analyzer for detection and therapeutic monitoring of Plasmodium
vivax in the Republic of Korea. Trop Med Int Health 8:1074 –
1081
15. Padial MM, Subirats M, Puente S, Lago M, Crespo S, Palacios G,
Baquero M (2005) Sensitivity of laser light depolarization analysis
for detection of malaria in blood samples. J Med Microbiol54:449 – 452
16. Chai JY (1999) Re-emerging Plasmodium vivax malaria in the
Republic of Korea. Korean J Parasitol 37:129 – 143
17. Day NP, Pham TD, Phan TL, Dinh XS, Pham PL, Ly VC, Tran
TH, Nguyen TH, Bethell DB, Nguyan HP, White NJ (1996)
Clearance kinetics of parasites and pigment-containing leukocytes
in severe malaria. Blood 88:4694 – 4700
18. Metzger WG, Mordmuller BG, Kremsner PG (1995) Malaria
pigment in leucocytes. Trans R Soc Trop Med Hyg 89:637 – 638
Ann Hematol (2008) 87:755 – 759 759
Related Documents