Jugdeep Dhesi Dept of Ageing and Health Guy’s and St Thomas’ , London

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Jugdeep Dhesi Dept of Ageing and Health
Guy’s and St Thomas’ , London
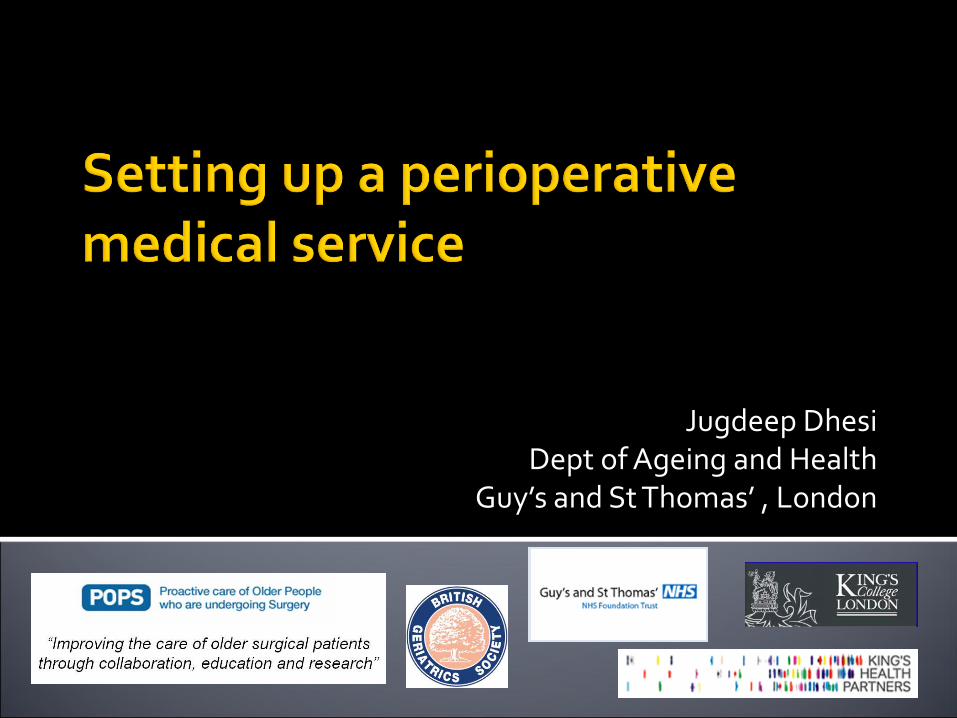
Perioperative medicine aims to Provide better care before, during & after surgery Reduce variation, improve outcomes
The RCoA programme The PSH programme
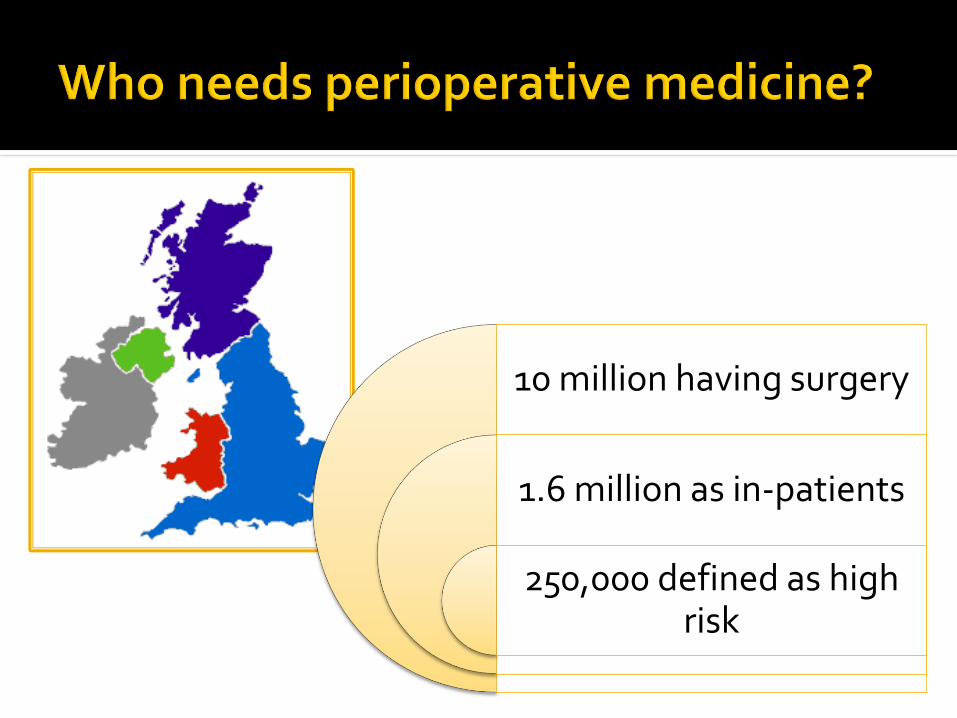
10 million having surgery
1.6 million as in-patients
250,000 defined as high risk
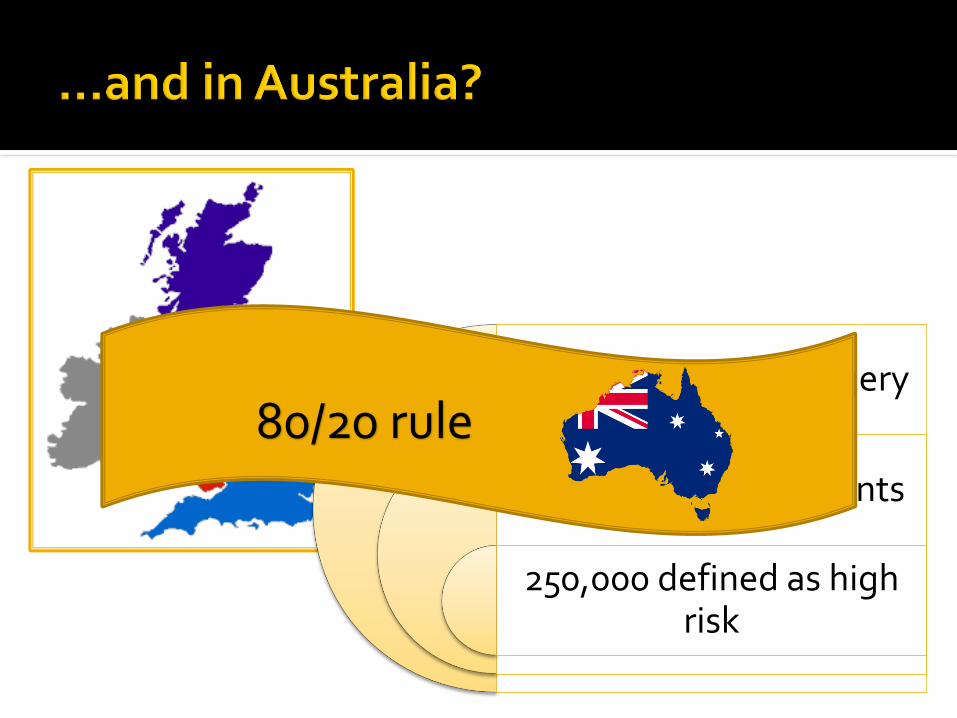
10 million having surgery
1.6 million as in-patients
250,000 defined as high risk
80/20 rule
Clinician reported outcomes Morbidity Mortality
Patient reported outcomes Recovery (change in trajectory of disease/disability) Experience, satisfaction
Process related outcomes Harm and complaints LOS, readmissions Cost (in-hospital, rehab, formal and informal )
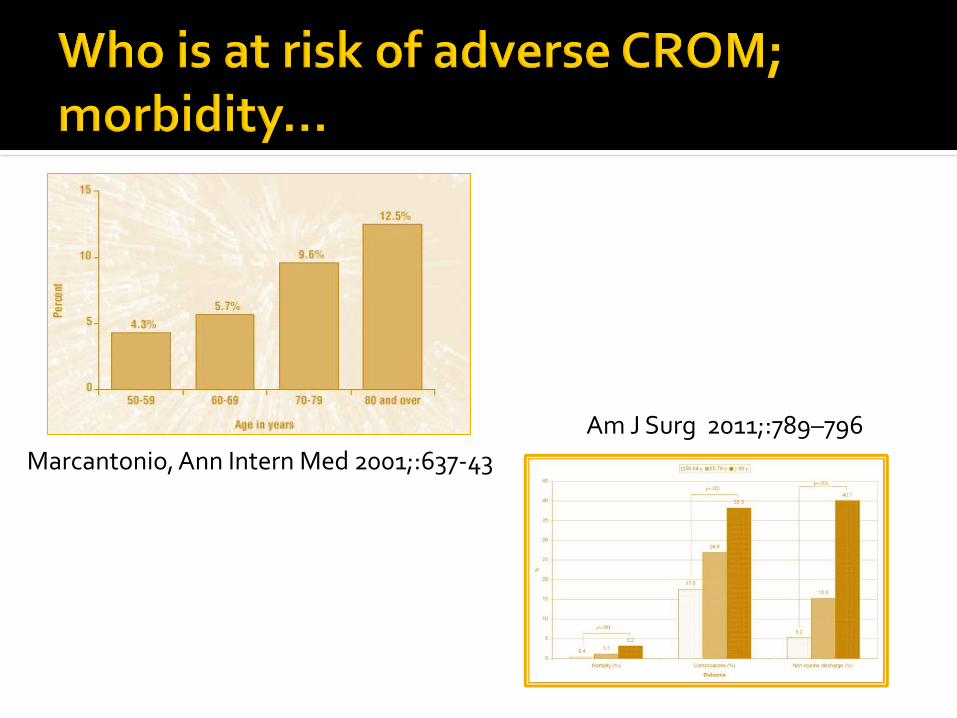
Marcantonio, Ann Intern Med 2001;:637-43
Am J Surg 2011;:789–796

Patel, Lancet 2000; 356;968-74
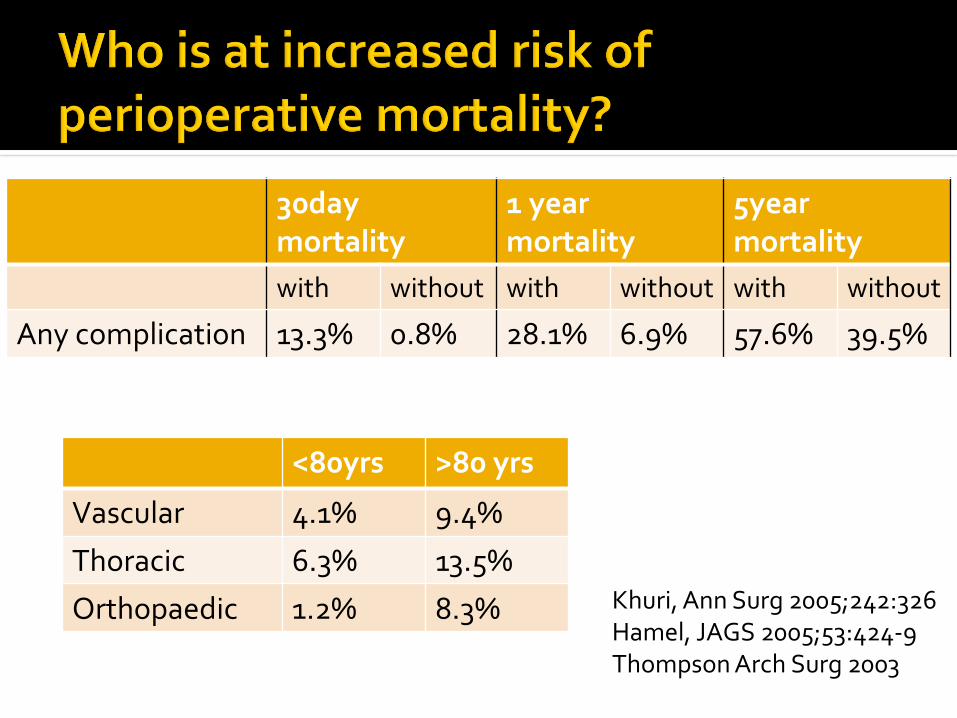
30day mortality
1 year mortality
5year mortality
with without with without with without
Any complication 13.3% 0.8% 28.1% 6.9% 57.6% 39.5%
Khuri, Ann Surg 2005;242:326Hamel, JAGS 2005;53:424-9Thompson Arch Surg 2003
<80yrs >80 yrs
Vascular 4.1% 9.4%
Thoracic 6.3% 13.5%
Orthopaedic 1.2% 8.3%
0
1,0
00
2,0
00
3,0
00
4,0
00
5,0
00
Patie
nts
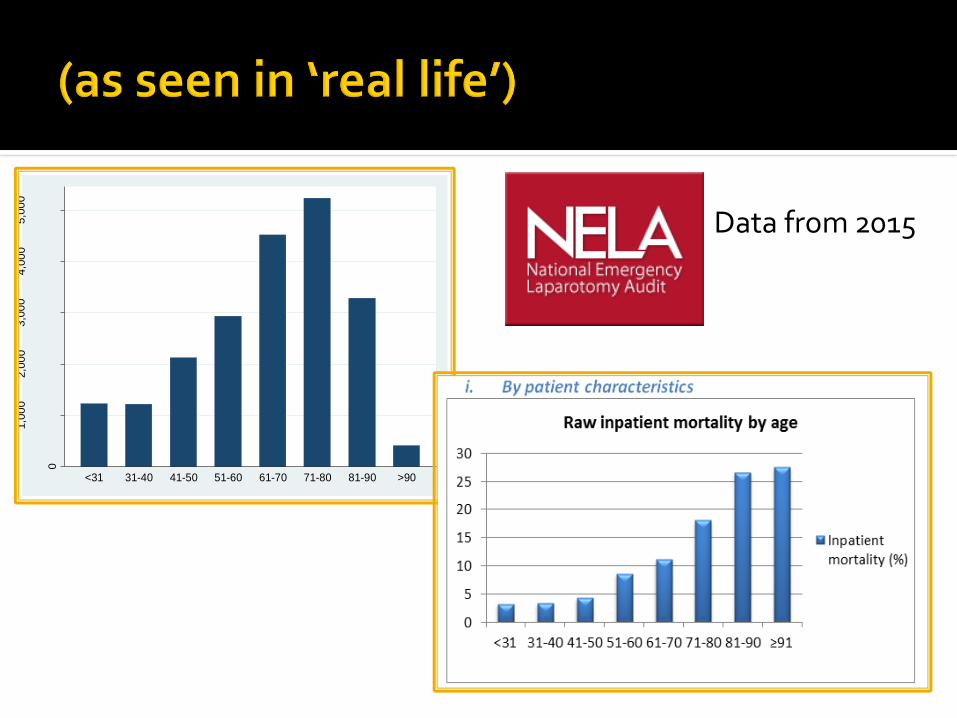
<31 31-40 41-50 51-60 61-70 71-80 81-90 >90
Data from 2015
Copyright © 2016 American Medical
Association. All rights reserved.
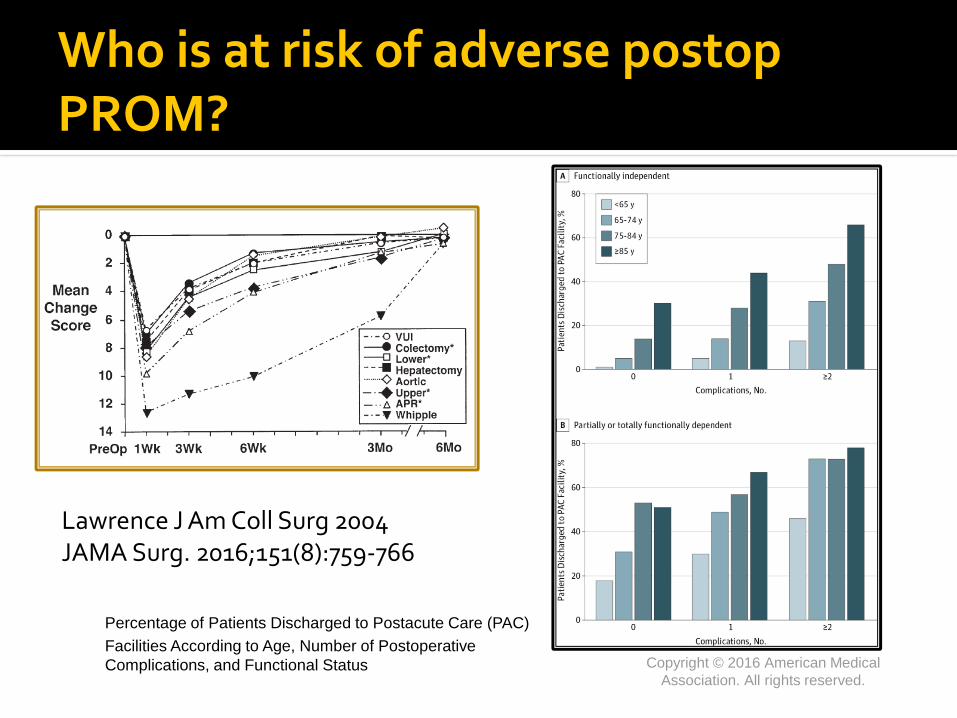
Percentage of Patients Discharged to Postacute Care (PAC)
Facilities According to Age, Number of Postoperative
Complications, and Functional Status
Who is at risk of adverse postop PROM?
Lawrence J Am Coll Surg 2004JAMA Surg. 2016;151(8):759-766

Poor cognitive recovery
Poor experienceNCEPOD An age old problemFrancis reportAIHW
Silverstein Br J Anaesth 2009, Partridge Int J Ger Psych 2014 Nadelson Br J Anaesth 2014
Most cost comes from
Late cancellations
Length of stay
Readmissions
Social care costs
Informal care costsCourtesy Sydney care home team
Shapter, Anaesthesia, 2012; 67:474-8
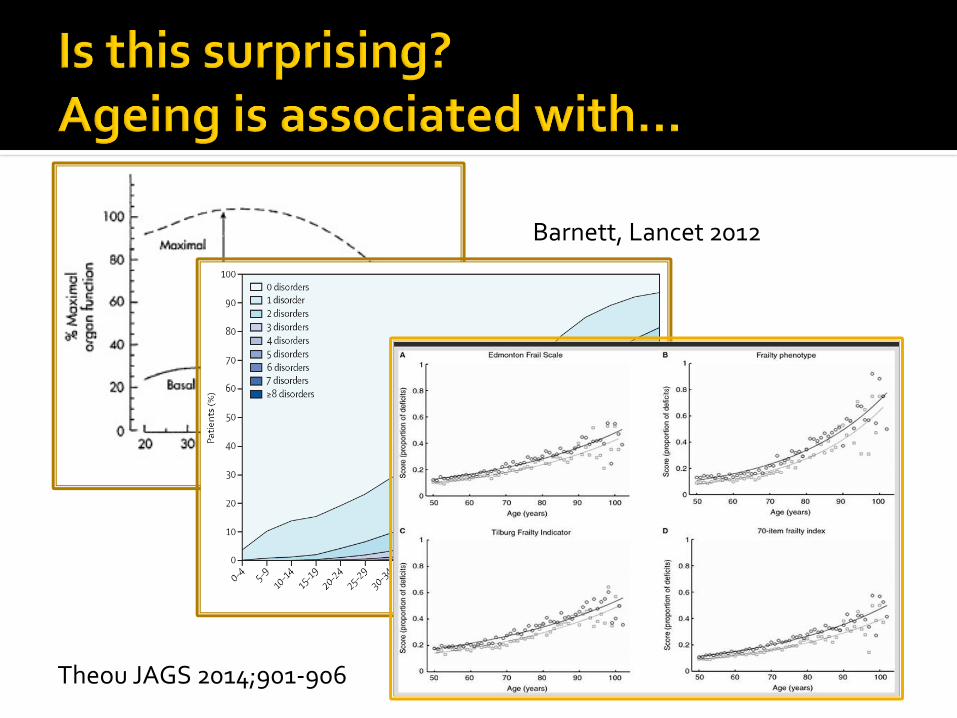
Theou JAGS 2014;901-906
Barnett, Lancet 2012

Wilson Br J Anaesth 2010;105:297, Pham ANZ J Surg 2014, Roche BMJ 2005;331:1374, Makary 2010, Partridge Age & Ageing 2012;41:142, Hubbard 2016

Older people are the most likely to need the specialty of perioperative
medicine
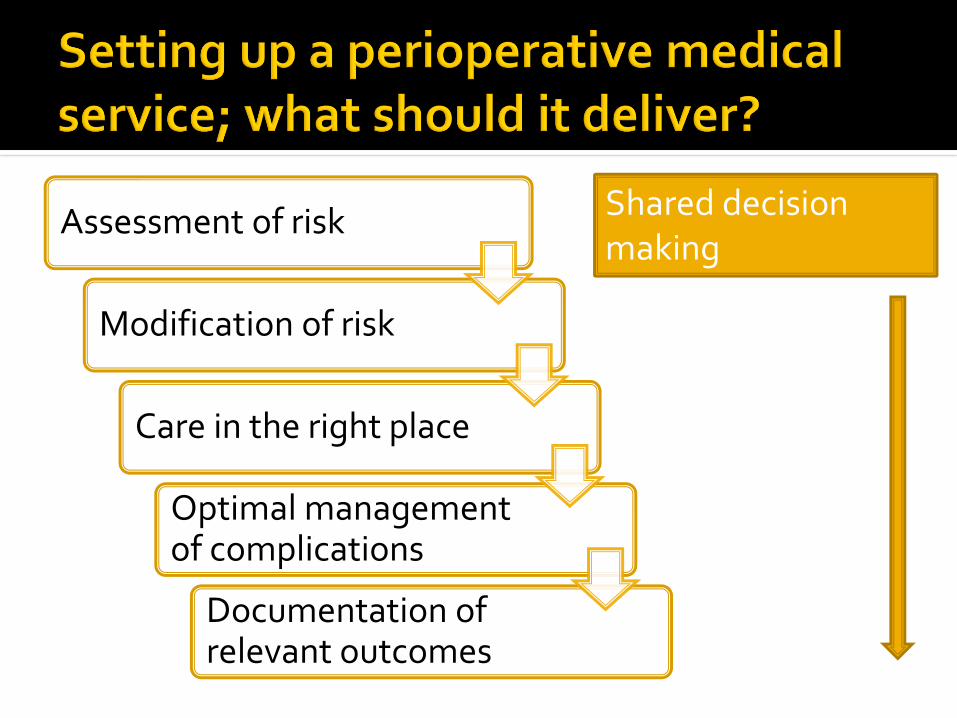
Assessment of risk
Modification of risk
Care in the right place
Optimal management of complications
Documentation of relevant outcomes
Shared decision making

Clinical pathway
Skeletal muscle
conditioning Cardiopul fitness
Frailty
Anaemia
Manage comorbidity
Nutrition
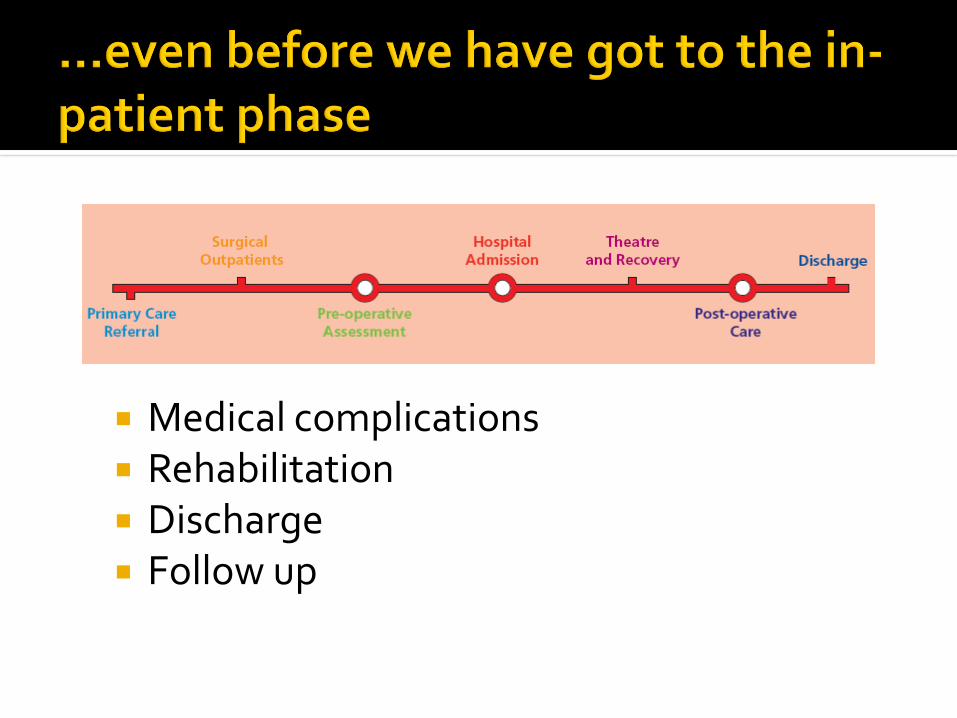
Medical complications Rehabilitation Discharge Follow up
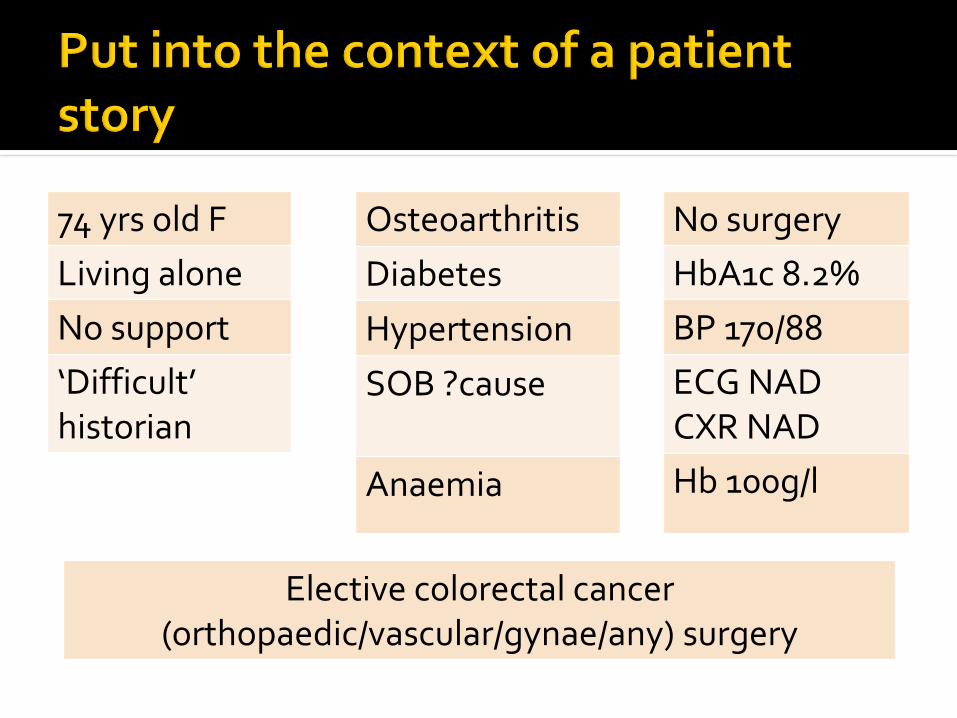
74 yrs old F
Living alone
No support
‘Difficult’ historian
Osteoarthritis
Diabetes
Hypertension
SOB ?cause
Anaemia
No surgery
HbA1c 8.2%
BP 170/88
ECG NADCXR NAD
Hb 100g/l
Elective colorectal cancer (orthopaedic/vascular/gynae/any) surgery

Declines surgery
• Understanding - Info poorly communicated
• Understanding –Sensory/cognitive impairm’t
• Health literacy – life expectancy, impact of ca/stoma
• Burden of intervention
Referred for medical opinion
• Anaemia
• Diabetes
• Shortness of breath
Cancelled on day of surgery
• Not followed fasting or medicines instructions
• Concern about medical status (anaemia, SOB)

Day of surgery
admission
Surgery with
consultant sx/anaesth
management
GDFT
HDU post op
Ward at 48 hours
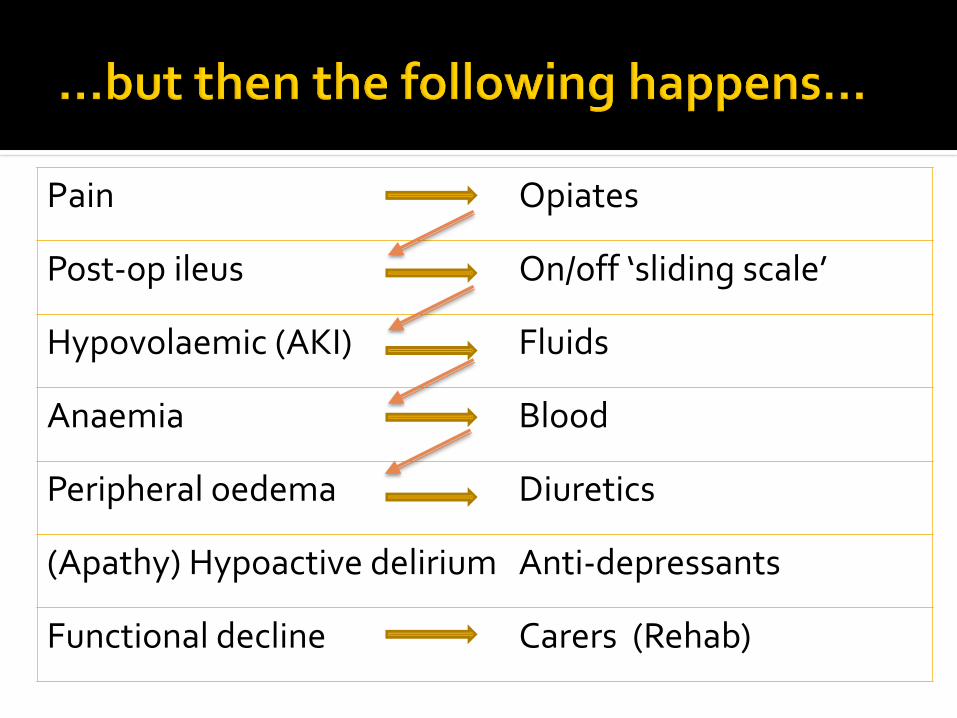
Pain Opiates
Post-op ileus On/off ‘sliding scale’
Hypovolaemic (AKI) Fluids
Anaemia Blood
Peripheral oedema Diuretics
(Apathy) Hypoactive delirium Anti-depressants
Functional decline Carers (Rehab)

• 4 in 5 high risk patients to general ward
• Management on wards by junior staff
• Poor recognition of medical problems
• Reliance on on-call staff
• Multiple medical team involvement

Jan 2009-2012111 public, 61 private 11,000 patients>40% >80 years>80% emergency
Duke University, US
Holistic, multidimensional, interdisciplinary assessment of an individual
Formulation of
a list of needs and issues to tackle
an individualised care and support plan
tailored to an individual’s needs, wants and priorities
= Comprehensive Geriatric Assessment

Guys and St Thomas’ NHS Foundation Trust
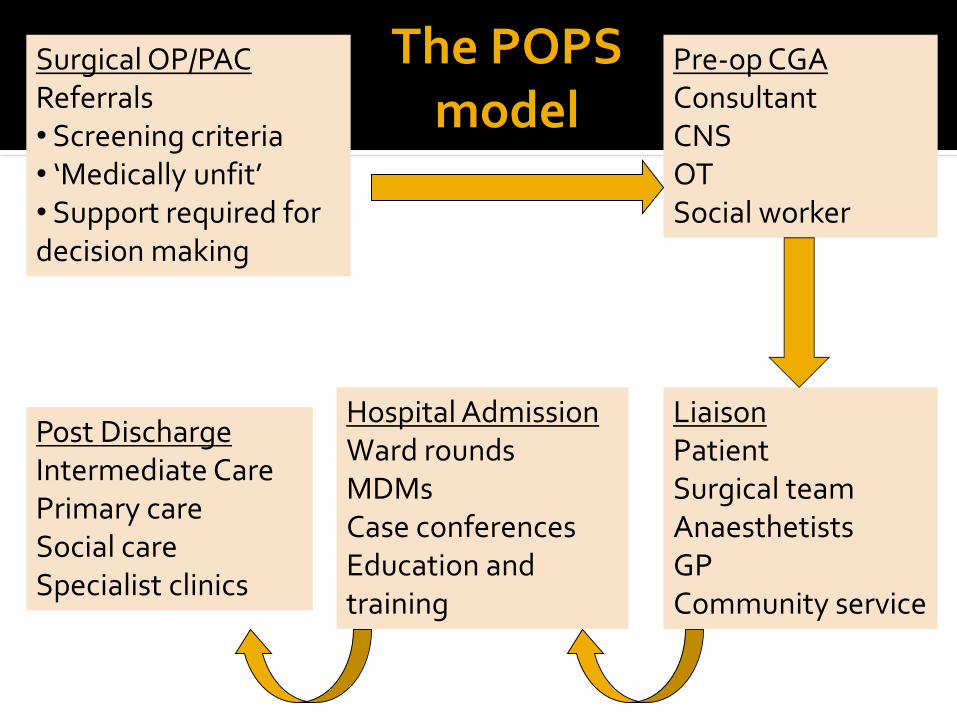
Surgical OP/PACReferrals• Screening criteria• ‘Medically unfit’ • Support required for decision making
Pre-op CGAConsultantCNSOTSocial worker
Hospital AdmissionWard roundsMDMsCase conferencesEducation and training
Post DischargeIntermediate CarePrimary careSocial careSpecialist clinics
LiaisonPatientSurgical teamAnaesthetistsGPCommunity service
The POPS model
Risk assessment
Recognition of known comorbidity
Identification of unrecognised disease, disability, frailty
Assessment of functional reserve
Optimisation
Medical, functional, psychological & social condition
Application of organ specific guidelines
Use of multidisciplinary interventions

Collaborative decision making Risk/harm versus benefit Consent, capacity, advance directives Communication
Risk management Prediction of post operative complications Planning of postoperative care promting
Early identification of medical complications Standardised mx of medical complications
Prediction of support required on discharge
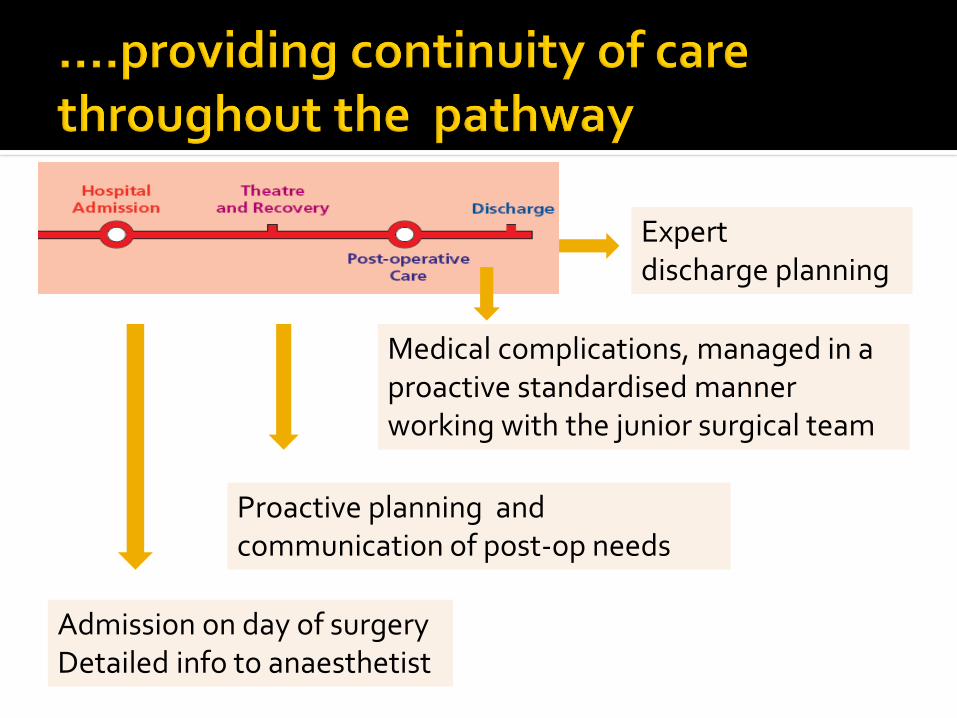
Admission on day of surgeryDetailed info to anaesthetist
Proactive planning and communication of post-op needs
Medical complications, managed in a proactive standardised manner working with the junior surgical team
Expertdischarge planning

Pain Opiates
Post-op ileus On/off ‘sliding scale’
Hypovolaemic (AKI) Fluids
Anaemia Blood
Peripheral oedema Diuretics
‘Not engaging, apathetic’ Anti-depressants
Functional decline POC
Refuses surgery Referred for medical opinion
Cancelled on day of surgery
Unrecognised disease/syndromes
Suboptimal control of comorbidity
Unrecognised complications
Poor coordination of care
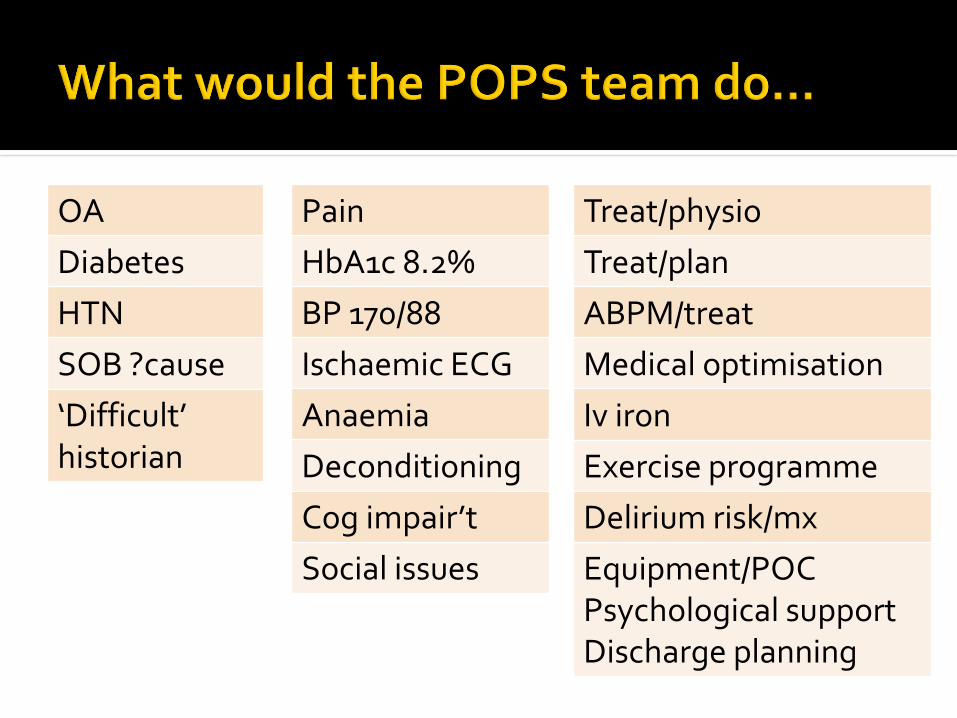
OA
Diabetes
HTN
SOB ?cause
‘Difficult’ historian
Pain
HbA1c 8.2%
BP 170/88
Ischaemic ECG
Anaemia
Deconditioning
Cog impair’t
Social issues
Treat/physio
Treat/plan
ABPM/treat
Medical optimisation
Iv iron
Exercise programme
Delirium risk/mx
Equipment/POCPsychological supportDischarge planning
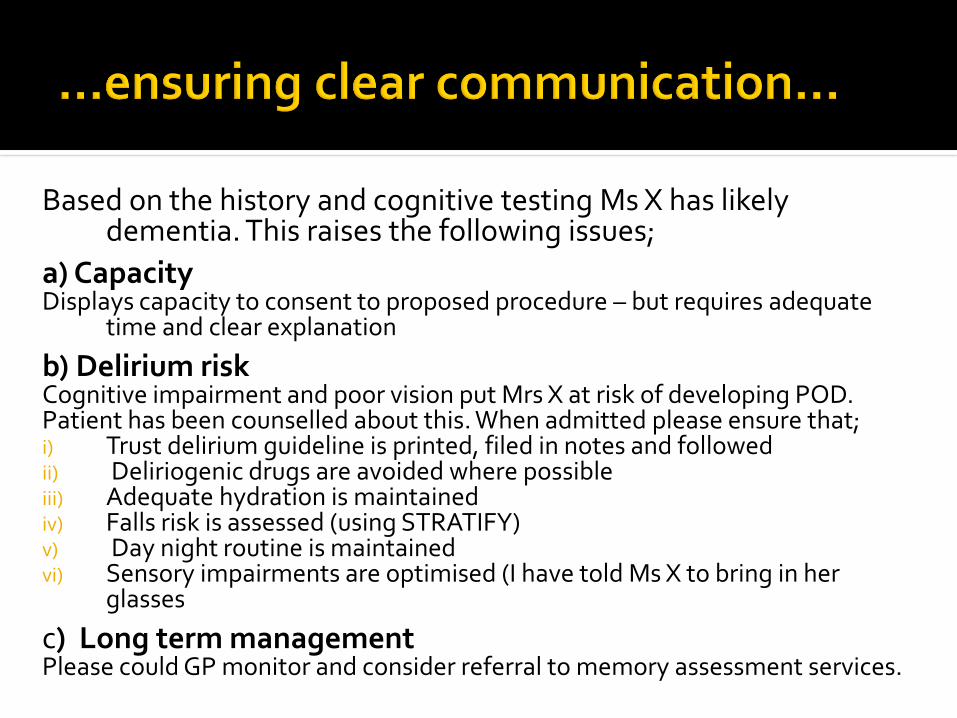
Based on the history and cognitive testing Ms X has likely dementia. This raises the following issues;
a) CapacityDisplays capacity to consent to proposed procedure – but requires adequate
time and clear explanation
b) Delirium riskCognitive impairment and poor vision put Mrs X at risk of developing POD. Patient has been counselled about this. When admitted please ensure that; i) Trust delirium guideline is printed, filed in notes and followedii) Deliriogenic drugs are avoided where possible iii) Adequate hydration is maintainediv) Falls risk is assessed (using STRATIFY)v) Day night routine is maintainedvi) Sensory impairments are optimised (I have told Ms X to bring in her
glasses
c) Long term managementPlease could GP monitor and consider referral to memory assessment services.
Risk of complications
Delirium, change in trajectory
Falls, functional decline
What carers can do to support the patient?
In hospital
At discharge
Where and how carers can seek support for themselves?
Admit day of surgery
Advocate same day admission / day surgery
Minimise unnecessary unit / ward moves
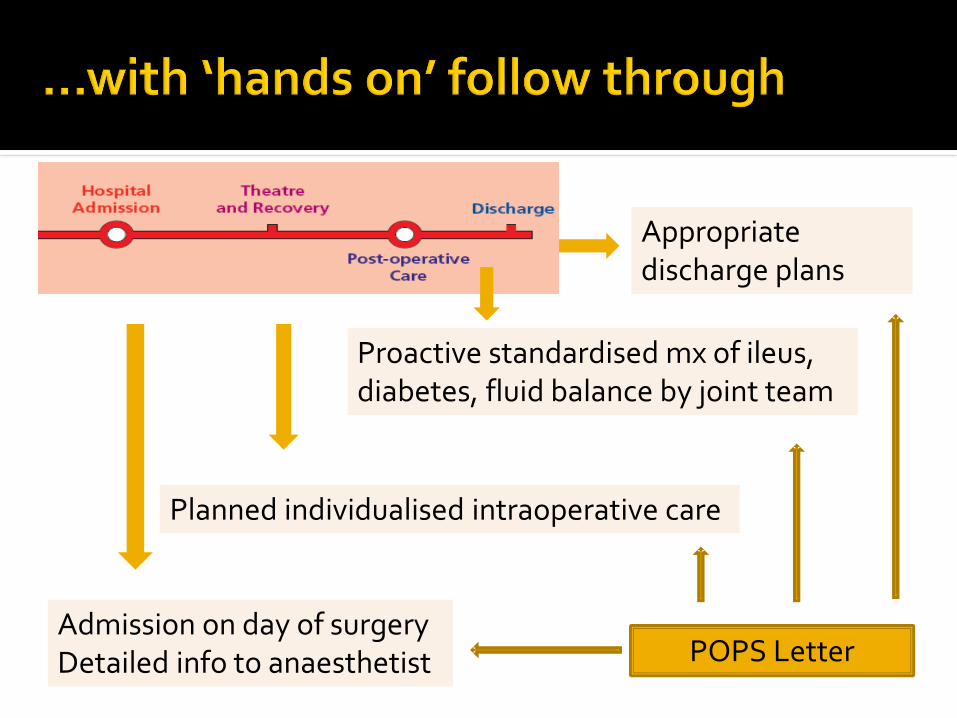
Admission on day of surgeryDetailed info to anaesthetist
Planned individualised intraoperative care
Proactive standardised mx of ileus, diabetes, fluid balance by joint team
Appropriate discharge plans
POPS Letter

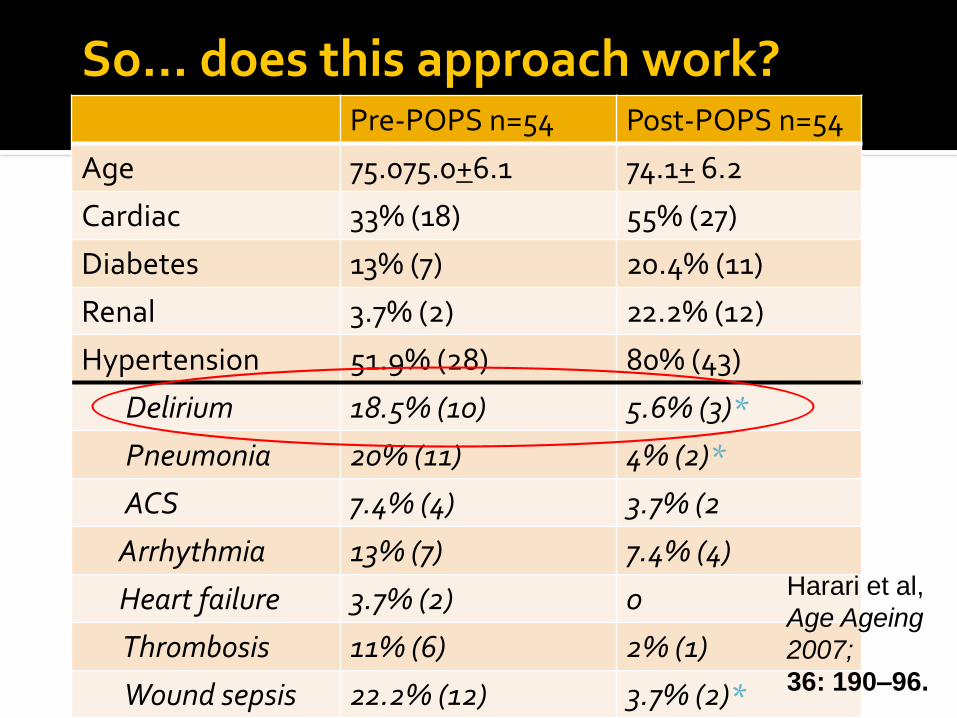
Pre-POPS n=54 Post-POPS n=54
Age 75.075.0+6.1 74.1+ 6.2
Cardiac 33% (18) 55% (27)
Diabetes 13% (7) 20.4% (11)
Renal 3.7% (2) 22.2% (12)
Hypertension 51.9% (28) 80% (43)
Delirium 18.5% (10) 5.6% (3)*
Pneumonia 20% (11) 4% (2)*
ACS 7.4% (4) 3.7% (2
Arrhythmia 13% (7) 7.4% (4)
Heart failure 3.7% (2) 0
Thrombosis 11% (6) 2% (1)
Wound sepsis 22.2% (12) 3.7% (2)*
Harari et al,
Age Ageing
2007;
36: 190–96.
So… does this approach work?

Accepted BJS Partridge Oct 2016

02
04
06
08
0
Pe
rcen
tage
Medical complications (p=0.002) Surgical complications (p=0.04) Delayed discharge (p=0.05)
Control Intervention Control Intervention Control Intervention
Percentage of patients with complications and delayed discharge by trial arm
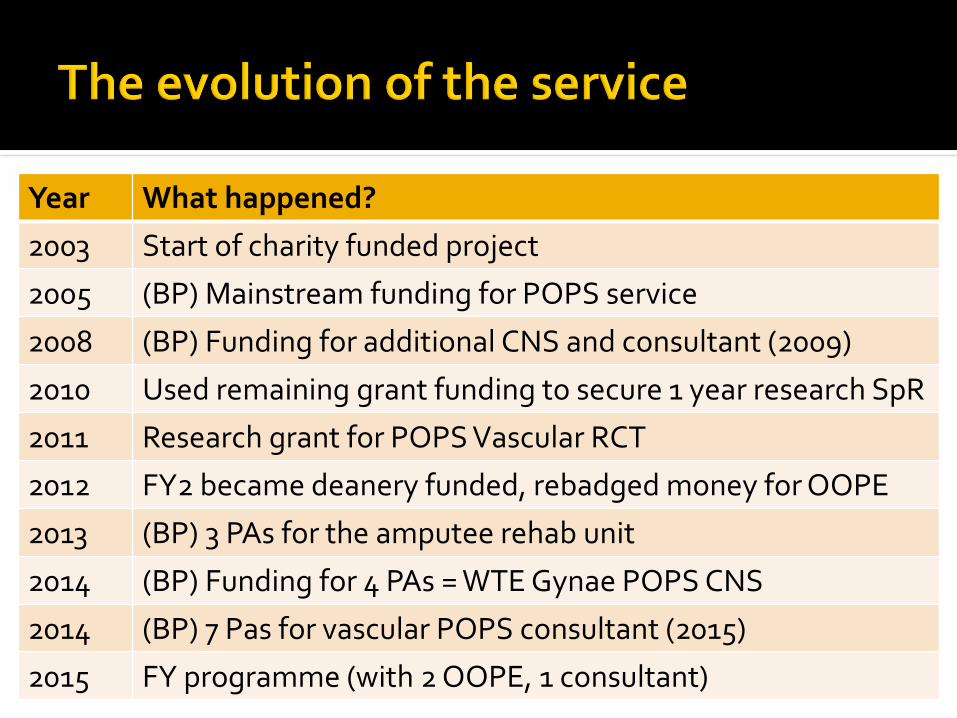
Year What happened?
2003 Start of charity funded project
2005 (BP) Mainstream funding for POPS service
2008 (BP) Funding for additional CNS and consultant (2009)
2010 Used remaining grant funding to secure 1 year research SpR
2011 Research grant for POPS Vascular RCT
2012 FY2 became deanery funded, rebadged money for OOPE
2013 (BP) 3 PAs for the amputee rehab unit
2014 (BP) Funding for 4 PAs = WTE Gynae POPS CNS
2014 (BP) 7 Pas for vascular POPS consultant (2015)
2015 FY programme (with 2 OOPE, 1 consultant)
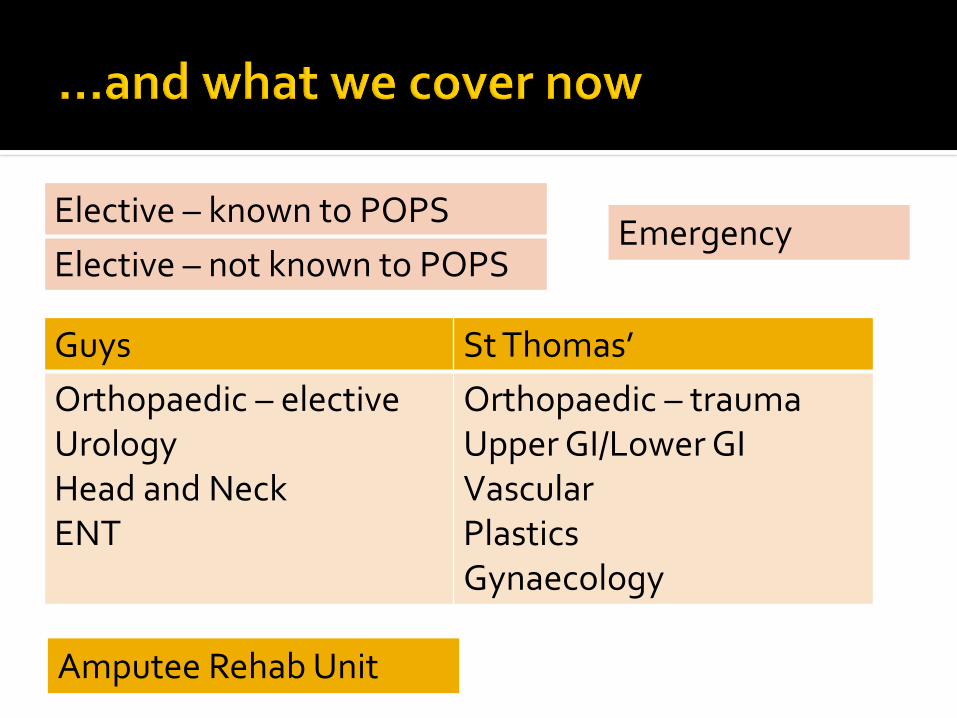
Guys St Thomas’
Orthopaedic – electiveUrologyHead and NeckENT
Orthopaedic – traumaUpper GI/Lower GIVascularPlasticsGynaecology
Elective – known to POPS
Elective – not known to POPS
Amputee Rehab Unit
Emergency
Medical specialties
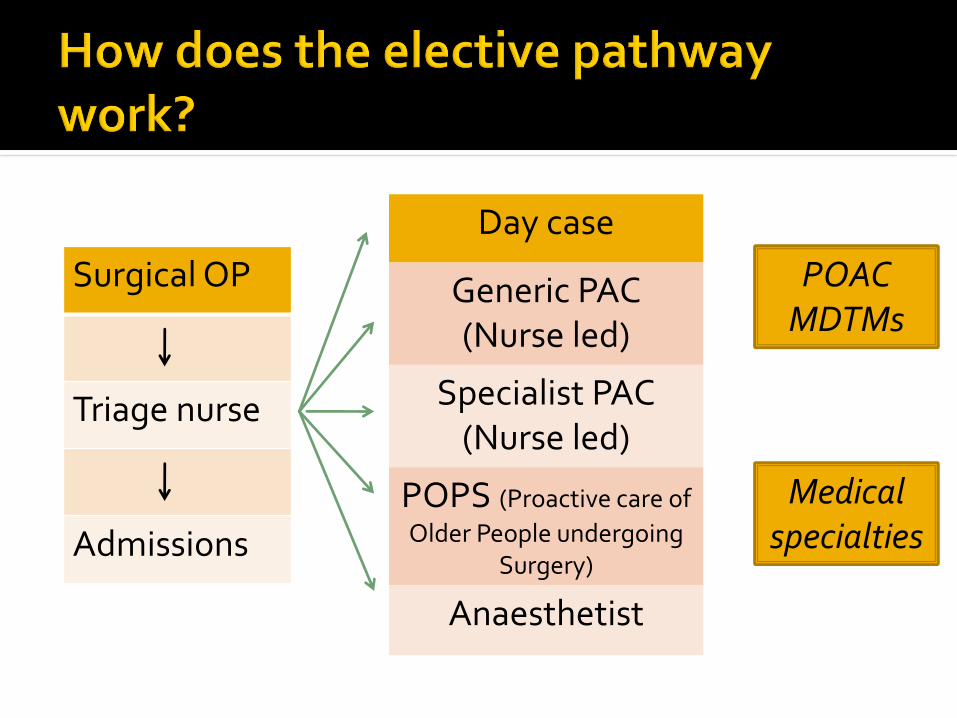
Day case
Generic PAC (Nurse led)
Specialist PAC (Nurse led)
POPS (Proactive care of
Older People undergoing Surgery)
Anaesthetist
Surgical OP
Triage nurse
Admissions
POAC MDTMs
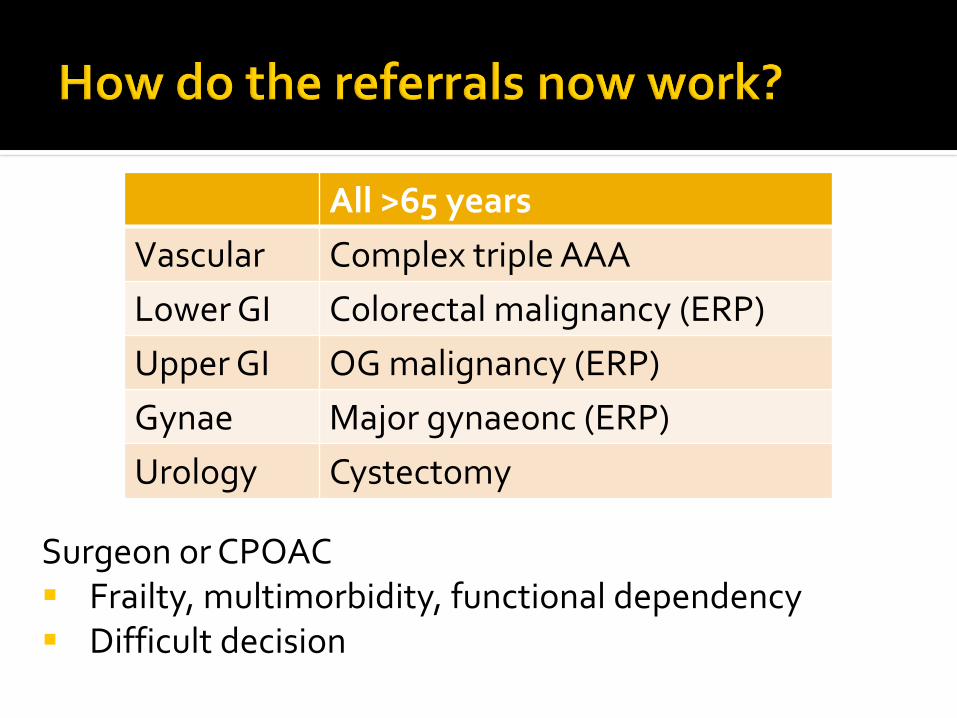
All >65 years
Vascular Complex triple AAA
Lower GI Colorectal malignancy (ERP)
Upper GI OG malignancy (ERP)
Gynae Major gynaeonc (ERP)
Urology Cystectomy
Surgeon or CPOAC Frailty, multimorbidity, functional dependency Difficult decision
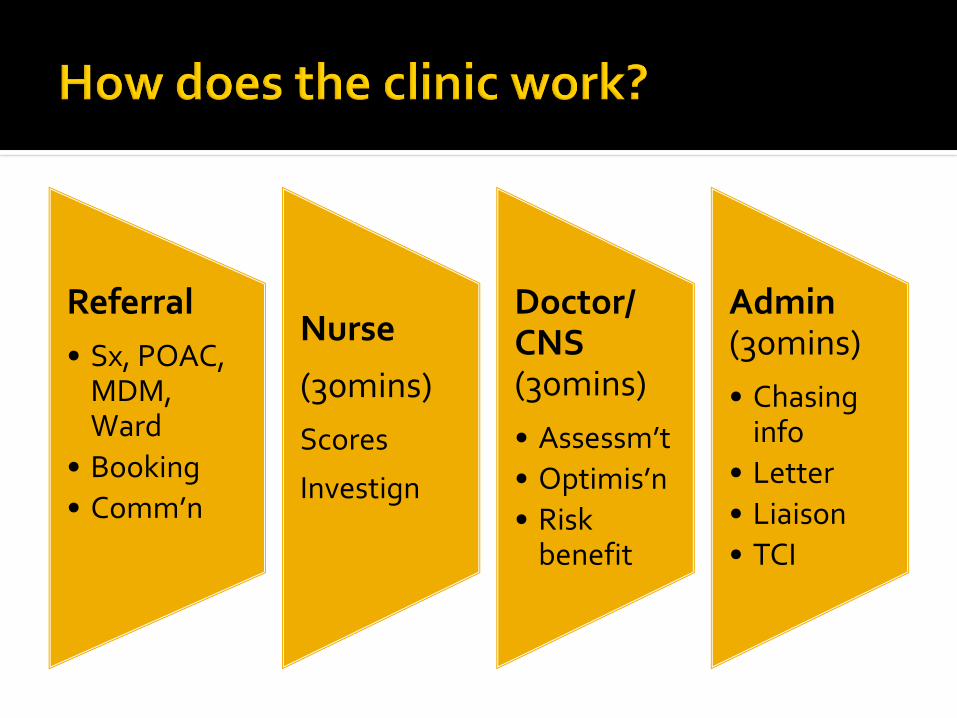
Referral
• Sx, POAC, MDM, Ward
• Booking
• Comm’n
Nurse
(30mins)
Scores
Investign
Doctor/ CNS(30mins)
• Assessm’t
• Optimis’n
• Risk benefit
Admin(30mins)
• Chasing info
• Letter
• Liaison
• TCI

POPS Clinic 4x week
One stop assessment and optimisation clinic
1000-1200 new out patients per year
MDM
In patient work
1200 elective and 1000 emergency
Joint surgeon-geriatrician ward rounds
Mon-Fri presence on wards 8-4pm
Board rounds/MDTMs, Prn reviews, telephone, email advice
Case conferences/family meetings

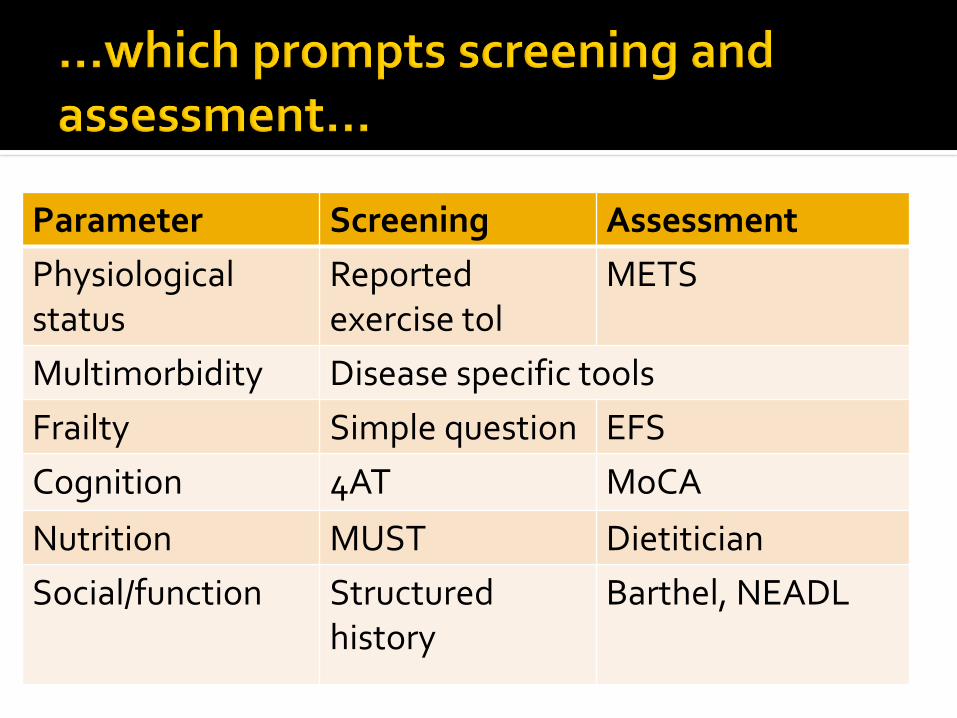
Parameter Screening Assessment
Physiologicalstatus
Reported exercise tol
METS
Multimorbidity Disease specific tools
Frailty Simple question EFS
Cognition 4AT MoCA
Nutrition MUST Dietitician
Social/function Structured history
Barthel, NEADL

Diagnosis
Management decision
Surgery (40%)Procedure Medical
As IP
(25%)
<48 hrs
(15%) Trauma Acute Care Surg 2013JAMA 2016, BJS 2013
Risk assessment CROM
PROMShared decision making
Process
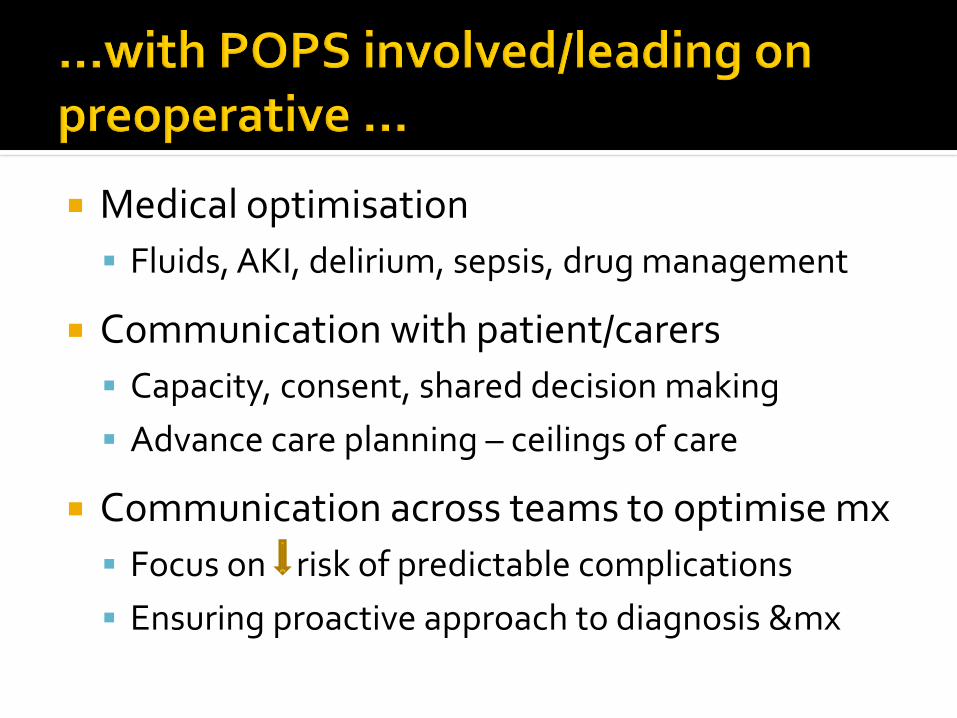
Medical optimisation
Fluids, AKI, delirium, sepsis, drug management
Communication with patient/carers
Capacity, consent, shared decision making
Advance care planning – ceilings of care
Communication across teams to optimise mx
Focus on risk of predictable complications
Ensuring proactive approach to diagnosis &mx
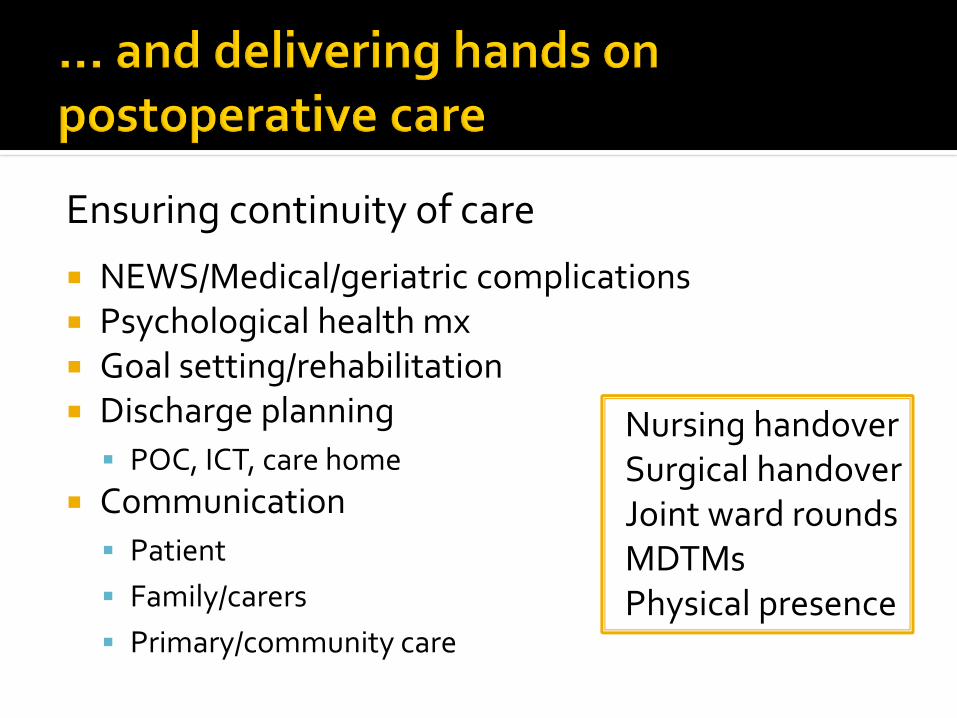
Ensuring continuity of care
NEWS/Medical/geriatric complications Psychological health mx Goal setting/rehabilitation Discharge planning
POC, ICT, care home
Communication
Patient
Family/carers
Primary/community care
Nursing handoverSurgical handoverJoint ward roundsMDTMsPhysical presence
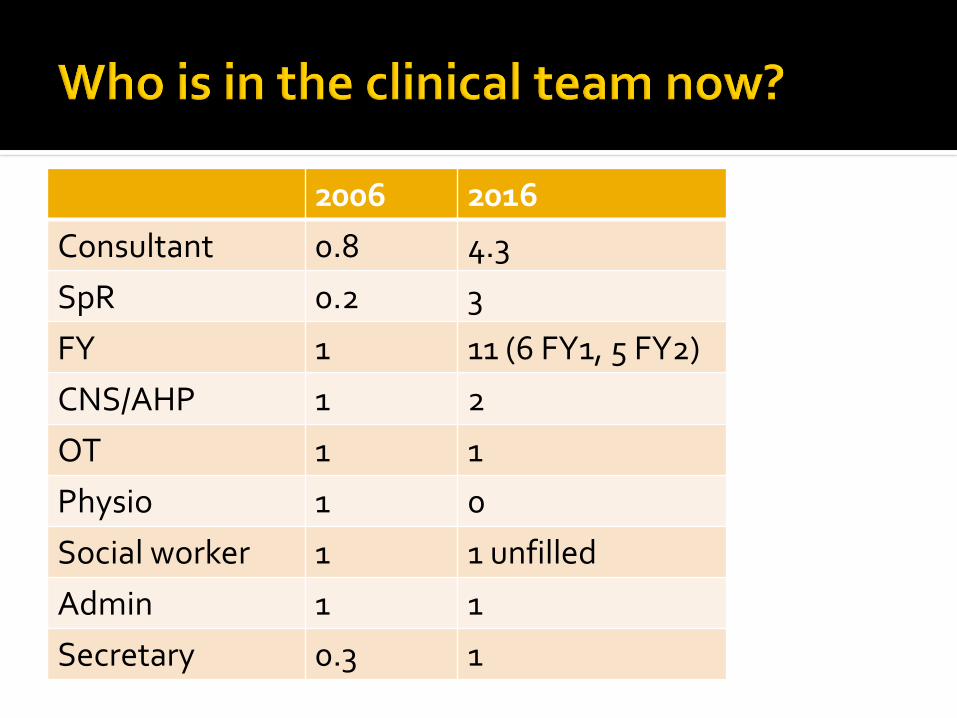
2006 2016
Consultant 0.8 4.3
SpR 0.2 3
FY 1 11 (6 FY1, 5 FY2)
CNS/AHP 1 2
OT 1 1
Physio 1 0
Social worker 1 1 unfilled
Admin 1 1
Secretary 0.3 1
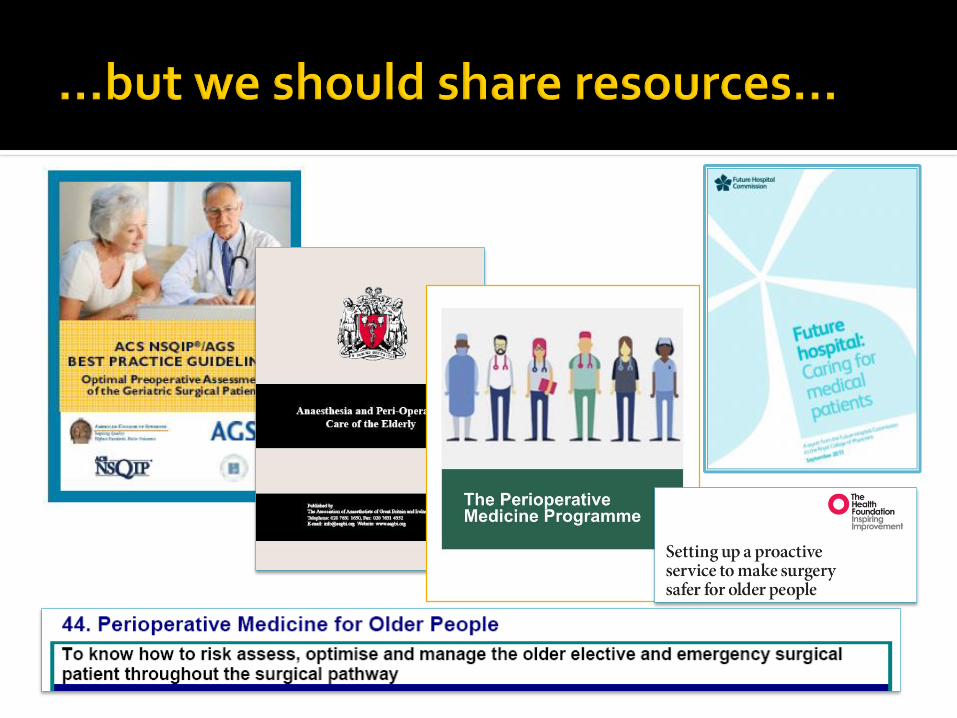
Delivering evidence based clinical practice
Do we have the evidence to inform practice ?
How do we translate into routine care? (behaviours, attitudes)
How do we change culture and when should we not?
Education and training (knowledge)
Is our workforce ready? Which workforce?
How do we ensure they are?
Research and QIP
Making it relevant to the ‘messy’ patient, the context and the workforce
Understanding service and trust priorities
Top three for a service delivery manager
Trust core values
Collecting ‘relevant’ data Engagement with and embedding within
established teams
Eg Transformation team, Delirium and dementia team, End of life care team
Using the available workforce Ensuring visibility
Annual report, Audit meetings, Grand rounds
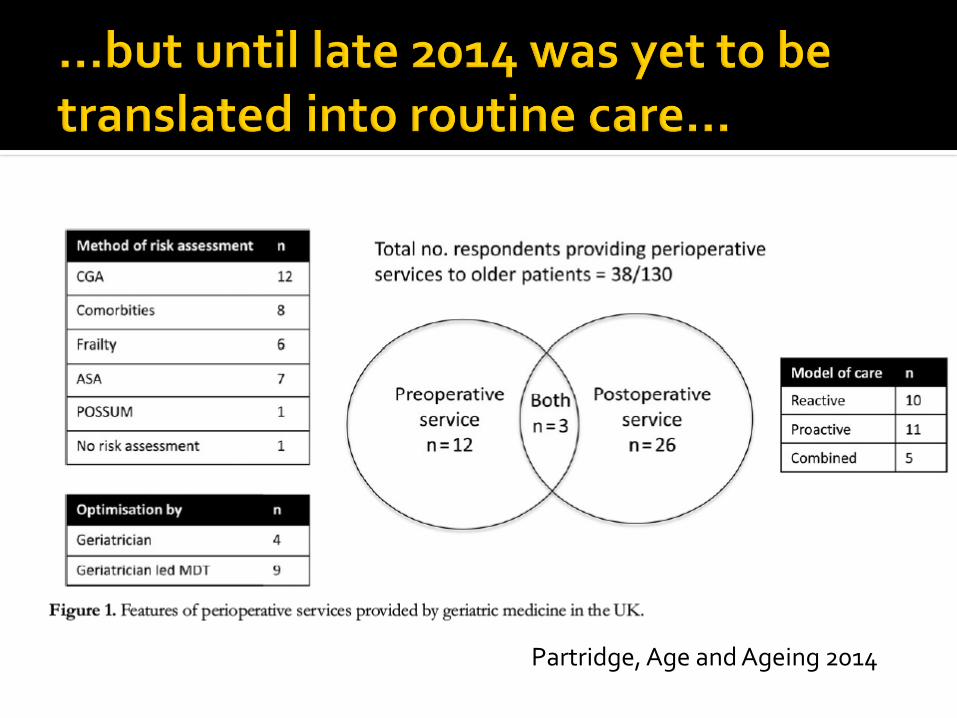
Partridge, Age and Ageing 2014
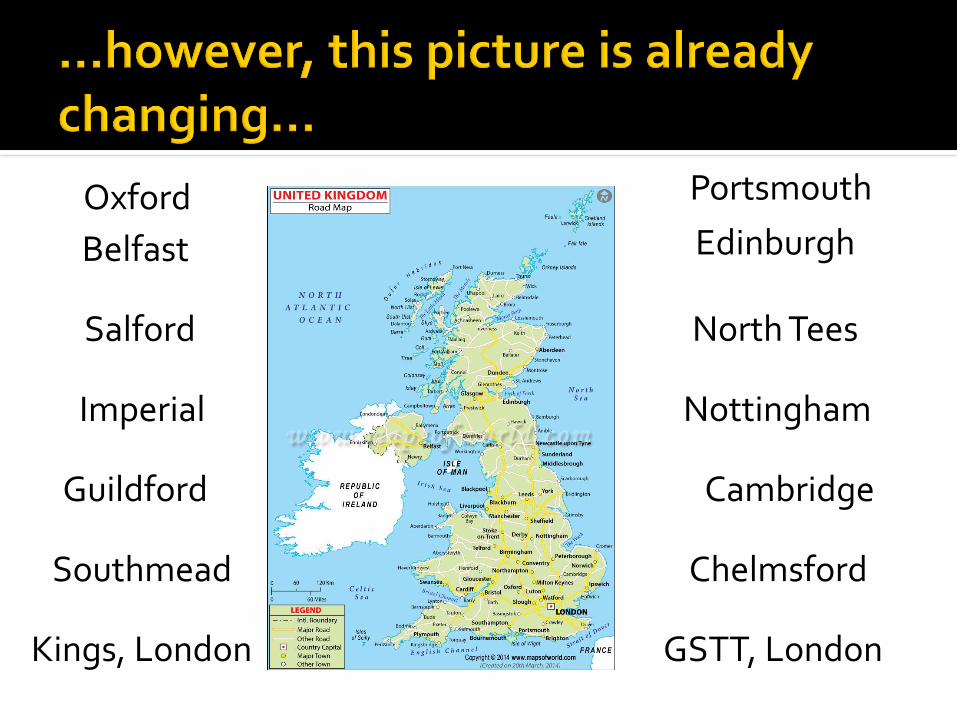
Chelmsford
Imperial
Belfast Edinburgh
Nottingham
Guildford
Southmead
North TeesSalford
GSTT, London
Cambridge
Kings, London
Oxford Portsmouth
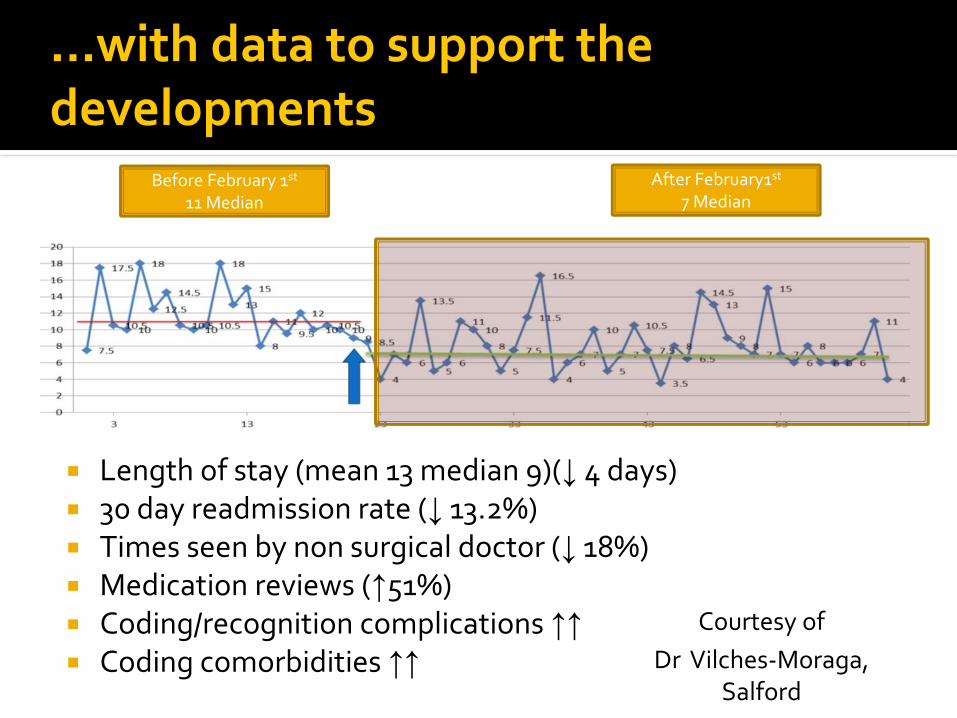
…with data to support the developments
Before February 1st
11 MedianAfter February1st
7 Median
Length of stay (mean 13 median 9)(↓ 4 days) 30 day readmission rate (↓ 13.2%) Times seen by non surgical doctor (↓ 18%) Medication reviews (↑51%) Coding/recognition complications ↑↑ Coding comorbidities ↑↑
Courtesy of
Dr Vilches-Moraga, Salford


…is a complex undertaking requiring ….
collaboration across specialties and disciplines
whole system reorganisation (cultural change)
upfront funding
…which raises many questions
Are surgical liaison services generic or subspecialised?
Is this primary care, anaesthetics, organ specific medicine, general medicine or geriatric medicine?
Can we embed specialist knowledge or do we have to embed the specialist?

www.popsteam.co.uk British Geriatrics Society POPS SIG POPS annual education conf (register via BGS) POPS OOPE/Fellow posts (advertised March/April) Research posts
RCoA Perioperative medicine programme UCL Perioperative Medicine MSc EBPOM, NELA Age Anaesthesia Association (May)
Related Documents