28 l Nursing2007Critical Care l Volume 2, Number 4 www.nursing2007criticalcare.com When laypersons hear the word “meningitis,” they may respond with fear, because the media often equate the condition with death. Meningitis is an inflamma- tion of the meninges of the brain, which is caused by various pathogens. Infections from other areas of the body can migrate into the cerebrospinal fluid (CSF), causing meningeal inflammation and infection. It’s important to revisit the anatomy, epidemiolo- gy, and types of meningitis, and prevention, nursing care, and treatment for this disease. The primary entrance of pathogens that cause meningitis is typically the nasopharynx. 1 Because the nasopharynx is in close proximity to the brain, the pathogens can pass through the nasopharyngeal membrane into blood circulation. Once in circula- tion, local pathogens can invade into the protective layers of the central nervous system, known as the meninges. The meningeal lay- ers are the dura mater, arachnoid, and pia mater. Cerebrospinal fluid originates within the ventricles of the brain, circulates through the subarachnoid space around the brain and spinal cord, and is absorbed by the arachnoid villi. 1 (See Cranial meninges .) The meninges help provide support against infection. Changes in the Meningitis the inflamed brain Critical care nurses are the first-line clinicians to observe these patients in the ICU, thus, they’re an integral part of preventing major complications. By Sophary Burnet, ACNP, Ann Huntley, RN, CCRN, MSN, APRN,BC, and Kelda M. Kemp, RN, BSN, BSEd Superior sagittal sinus Subarachnoid space Subdural space Skin Periosteum Bone Dura mater Arachnoid Pia mater Falx cerebri Arachnoid villi 2.0 ANCC /AACN CONTACT HOURS Cranial meninges

JRNL-Meningitis the Inflamed Brain
Dec 25, 2015
journal on meningitis
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

28 l Nursing2007CriticalCare l Volume 2, Number 4 www.nursing2007criticalcare.com
When laypersons hear the word“meningitis,” they may respondwith fear, because the mediaoften equate the condition withdeath. Meningitis is an inflamma-tion of the meninges of the brain,which is caused by variouspathogens. Infections from otherareas of the body can migrateinto the cerebrospinal fluid (CSF),causing meningeal inflammationand infection. It’s important torevisit the anatomy, epidemiolo-gy, and types of meningitis, andprevention, nursing care, andtreatment for this disease.
The primary entrance ofpathogens that cause meningitis istypically the nasopharynx.1
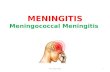
Because the nasopharynx is inclose proximity to the brain, thepathogens can pass through thenasopharyngeal membrane intoblood circulation. Once in circula-tion, local pathogens can invadeinto the protective layers of thecentral nervous system, known asthe meninges. The meningeal lay-ers are the dura mater, arachnoid,
and pia mater. Cerebrospinal fluidoriginates within the ventricles ofthe brain, circulates through thesubarachnoid space around thebrain and spinal cord, and isabsorbed by the arachnoid villi.1
(See Cranial meninges.) Themeninges help provide supportagainst infection. Changes in the
Meningitisthe inflamed brainCritical care nurses are the first-line cliniciansto observe these patients in the ICU, thus,they’re an integral part of preventing majorcomplications.By Sophary Burnet, ACNP, Ann Huntley, RN, CCRN, MSN, APRN,BC, and Kelda M. Kemp, RN, BSN, BSEd
Superior sagittal sinus
Subarachnoidspace
Subduralspace
Skin
Periosteum
Bone
Dura mater
Arachnoid
Pia mater
Falxcerebri
Arachnoid villi
2.0ANCC/AACN
CONTACT HOURS
Cranial meninges

www.nursing2007criticalcare.com July l Nursing2007CriticalCare l 29

blood-brain barrier (BBB) maylead to increased susceptibility forinfectious pathogens to passthrough the BBB and furtherinfect the meninges.1 Several fac-tors can increase permeability ofthe BBB, thereby allowing easierpassage of pathogens. Theseinclude alterations in the tightjunctions of the blood vessels orin glial cells of the membrane thatprevents most particles from pass-ing, and variations of hormonesthat create support for the plasmamembranes of the barrier itself.1
OrganismsOrganisms such as bacteria,viruses, and fungi can causemeningitis. In healthy individu-als, these organisms can be a partof the body’s normal flora.Pathogens can be endemic tospecific populations. Theseinclude persons living in closecontact, such as in a dormitoryor military barracks. Sub-SaharanAfrica is a hyperendemic area formeningitis and is known as the“meningitis belt.”2 Individualswith certain risk factors, such asyoung children, the elderly (age60 or older), or those with dia-betes, malignancy, immunosup-pression, or a ventriculoperi-toneal shunt (VPS), can becomemore susceptible to developingmeningitis. Neurosurgical proce-dures and basal skull fracturesalso predispose a person to con-tracting meningitis.
Bacterial Bacterial meningitis may becomefatal if left untreated. There arecommon forms of bacterialmeningitis:
1. Streptococcus pneumoniae(pneumococcus) is the most com-mon cause of bacterial meningitis,
and also causes pneumonia, sinusinfection, and otitis media in allage groups except neonates.3
2. Neisseria meningitidis(meningococcus), which oftenresides in the nose and throat,causes bacterial meningitis that’sassociated with areas havingincreased communal living, suchas college dormitories and daycare centers.4 Primary modes oftransmission include direct con-tact or inhalation of respiratorydroplets through coughing orsneezing from infected carriers.According to researchers,although 5% to 10% of adults areasymptomatic carriers, the inci-dence of infection increases 60%to 80% within members of aclosed population.4 Meningo-coccus is highly contagious andcan cause devastating neurologi-cal consequences and death.
3. Haemophilus influenzaeserotype B (Hib) is transmitted viadirect contact with respiratorydroplets from the nasopharynx, isformerly the leading cause of bac-terial meningitis, and is account-able for upper respiratory infec-tions and otitis media in children.Administration of the Hib vaccineas part of childhood immuniza-tions has dramatically reducedthe incidence of H. influenzaemeningitis.3
4. Listeria monocytogenes infec-tion, transmitted via ingestion ofcontaminated foods, is prevalentin pregnant women, the elderly,neonates, and patients withimmunosuppression.5
5. Staphylococcus aureus is asso-ciated with head trauma, cran-iotomies, VPS, and other neuro-surgical procedures.3 The modeof transmission is throughhematogenous spread from aninfected site.
ViralEnteroviruses, which includepolioviruses, coxsackieviruses,and echoviruses, are responsiblefor 85% to 95% of all cases ofviral meningitis.5 Viral meningitisusually clears on its own and isoften responsible for gastroin-testinal viral infections. Entero-viruses are commonly transmit-ted via direct contact with conta-minated respiratory secretion,including saliva, sputum, and thedirect transmission via hands tonose or mouth. They are alsotransmitted via direct contactwith feces. Other common virus-es include adenovirus and para-myxovirus (mumps), and the her-pes family viruses: HSV-1, HSV-2, varicella-zoster virus, Epstein-Barr virus, and cytomegalovirus.6
FungalA common nonbacterial, nonviralcause of meningitis is the fungusCryptococcus neoformans, anencapsulated yeast, which isresponsible for cryptococcalmeningitis. Commonly associatedwith aged pigeon droppings orbird feces, C. neoformans is themost common variety in theUnited States and is most associ-ated with cryptococcal infectionsworldwide.7
IncidenceAccording to data, statistics of theincidence of major bacterialpathogens (per 100,000) in theUnited States in 1995 are as fol-lows: • Streptococcus pneumoniae (13)had a mortality rate of 14% inpatients hospitalized8
• Neisseria meningitidis (0.6) usual-ly increased in late winter andearly spring, with a 10% to 14%mortality3,8
30 l Nursing2007CriticalCare l Volume 2, Number 4 www.nursing2007criticalcare.com
Meningitis

• Haemophilus influenzae serotypeb (0.2) in unvaccinated childrenand adults, with a 3% to 6% mor-tality.3,8
Signs and symptomsPatients with all forms of menin-gitis present with signs andsymptoms of meningeal inflam-mation/irritation and systemicinfection. Common complaintsusually include headache, fever,chills, nuchal rigidity, vomiting,photophobia, and seizures.Depending on age, virulence ofthe strain, and defense system ofthe host, patients can becomecritically ill if not promptly diag-
nosed and treated.3
Infection with bacterial menin-gitis carries high mortality andmorbidity rates with an overallfatality of 25% reported inadults.4 These patients can havean acute onset of commonmeningeal symptoms, as listedabove, which can progress rapid-ly to neurological deterioration.As the disease advances, macularskin rash progressing to purpuricand ecchymotic lesions may bepresent due to petechial hemor-rhage, seen specifically inmeningococcal disease.9 As theinfection ensues, circulatoryshock and death can transpire,even if treated. Therefore, antibi-otic therapy should be initiatedwithin 30 minutes of emergencydepartment presentation forthose suspected of bacterialmeningitis.3
Viral meningitis is more preva-
lent, but causes less serious com-plications than bacterial meningi-tis. Patients with viral meningitiscommonly present with similarmeningeal symptoms, which maybe less severe and appear flu-likein nature. They may complain ofa history of an upper respiratoryinfection that is accompanied byheadache, stiff neck, anorexia, orgeneralized malaise.9 Dependingon the infecting organism, thesesymptoms may dissipate withouttreatment.
Clinical manifestation of fungalmeningitis may be mild initially.Due to the encapsulated natureof the organism, the body may
not exhibit signs of infection untilextensive neurological involve-ment has occurred. Headache,low-grade fever, vomiting, andlethargy are primary symptomsthat can occur and may fluctuatethroughout the course of illness.3
Once a patient becomes infected,a characteristic feature of fungalinfection is its tendency to recur,especially for patients who areimmunosuppressed.7 Therefore,devastating outcomes can occur ifpatients aren’t adequately treatedwith antifungal medications.
Nursing assessmentInitial nursing assessmentincludes a thorough history, neu-rological exam, review of sys-tems, and vital signs. The nursingassessment must also focus onhistory of travel, previous infec-tions, medications, and sources ofimmunosuppression. The neuro-
logical exam consists of cranialnerve assessment, level of con-sciousness, motor strength, sen-sory exam and evaluation ofheadache. Other signs of menin-geal irritation may include posi-tive Kernig’s sign, which is painand hamstring resistance that iselicited upon passive knee exten-sion while patient is supine.9
Brudzinski’s sign is positive ifthere’s an involuntary flexion ofhips due to passive neck flexionwhile patient is supine.9 (SeeTesting for meningeal irritation.)Findings from a neurologicalexam may include altered mentalstatus, confusion and irritability,
vision disturbances such as pho-tophobia, cranial nerve deficits,and changes in level of conscious-ness.9
The gastrointestinal systemmay be affected if the patientpresents with nausea and vomit-ing that can typically be relatedto meningeal irritation. All othermajor body systems may be nor-mal depending on the severity ofthe initial infection.
Diagnostic testsDiagnostic tests include comput-ed tomography (CT) scan andmagnetic resonance imaging(MRI) to rule out other sourcesfor neurological changes, assessfor hydrocephalus, and showmeningeal enhancement. Achest x-ray may be done to iden-tify pneumonia or secondaryfungal infection. Laboratorytests include complete blood cell
www.nursing2007criticalcare.com July l Nursing2007CriticalCare l 31
Devastating outcomes can occur if patients aren’t adequately treated with antifungal medications.

count with differential, whichmay show leukocytosis, serumglucose, which may be drawn asa baseline determination fornormal CSF glucose, BUN, crea-tinine, and liver function studiesto assess renal and hepatic func-tion and adjust antibioticdosages.3 Serology is needed toidentify specific antigens corre-lated with specific pathogens.Cultures are also required of thefollowing: CSF, blood, urine,nasal passages, and drainagefrom wounds, for diagnosis of aspecific organism and the sourceof infection.10 Further investiga-tion of the CSF helps determinethe specific type of meningitisand the degree of infiltration. Alumbar puncture is performedto obtain CSF and assess initialopening pressures, which canindicate hydrocephalus. (SeeComparison of CSF findingsamong organisms.)
Nursing careNursing care needs to focus onpatient’s symptoms as they arepresented. The primary treat-ment is the timely administrationof empiric antibiotics, even if anorganism hasn’t been initiallyidentified.3 Antibiotics may bestarted, especially if meningealsymptoms are present, prior toCSF culture results.6,9 Basic carewhile in the intensive care unit(ICU) includes reducing theamount of stimulation, maintain-ing proper body alignment withhead straight and elevated to atleast 30 degrees, frequent painand neurological assessment,close monitoring of vital signs,ensuring adequate cerebral perfu-sion pressure (CPP), assessingand treating fever, maintainingstandard precautions, and provid-ing adequate skin care, nutrition,and hydration throughout thehospital stay.9 Minimal noise lev-
els and dim lights create a morecalming environment and canprevent agitation in the patientwith meningitis. All these factorscan help prevent the devastatingoutcomes of organism invasionsuch as shock and increasingintracranial pressure (ICP).
If meningococcal meningitis issuspected, droplet precautionsare recommended until 24 hoursafter initiation of effective thera-py.11 Any close contacts, includ-ing family members, healthcareproviders who did not wearmasks, and anyone in close prox-imity to the patient, need admin-istration of prophylactic antibi-otics within 24 hours after pa-tient diagnosis.8
TreatmentMedical interventions depend onwhether the meningitis is bacteri-al, viral, or fungal in nature.Bacterial treatment: Empiric
32 l Nursing2007CriticalCare l Volume 2, Number 4 www.nursing2007criticalcare.com
Meningitis
Testing for meningeal irritationPositive Brudzinski’s and Kernig’s signs indicate meningeal irritation, a sign of meningitis.
Brudzinski’s signHave your patient lie in the supine position. Thenplace your hand under his neck and flex it forward,chin to chest. The test is positive if he flexes hisknees and hips bilaterally. The patient will typicallycomplain of pain when his neck is flexed.
Kernig’s signHave your patient lie in the supine position. Flexhis hip and knee to form a 90-degree angle. Thenattempt to extend his leg. If he exhibits pain orresistance to extension and spasm of the ham-string, the test is positive.

intravenous antibiotics must begiven for the specific organismendemic to the region. When spe-cific organisms are isolated, theappropriate antibiotic may thenbe started intravenously.12 Initialempiric antibiotics include thirdgeneration cephalosporins suchas ceftriaxone (Rocephin), or fluo-roquinolones such as ciprofloxa-cin (Cipro).8 According to re-searchers, the use of glucocorti-coids, such as dexamethasone(Decadron), with the initiation ofthe first antibiotic dose has beenshown to decrease unfavorableoutcomes and mortality frombacterial meningitis with adults.11
However, there’s limited data ondexamethasone use in adults, andif given should be initiated withthe first dose of antibiotics for alimited number of days.3 Steroiduse is controversial, and researchis ongoing.13 In a systemicreview, experts suggest, “…rou-tine steroid therapy with the firstdose of antibiotics is justified inmost adult patients in whomacute community acquired bacte-rial meningitis is suspected.”14
The major effect of dexametha-sone is a decrease in the inflam-
matory response.14
Viral treatment: Medical man-agement for viral meningitis ismostly supportive based onsymptoms. Bed rest, adequatehydration, antipyretics, antiemet-ics, and analgesics are recom-mended. Antiviral medicationsmay be administered and areusually reserved for severe casesof infection caused by herpesviruses.15
Fungal treatment: Patients withfungal meningitis should beaggressively treated with antifun-gal medications such as ampho-tericin B and fluconazole (Diflu-can) given intravenously for sev-eral weeks.7
Possible complicationsComplications of meningitis areexclusive to the presenting symp-toms of the individual. The crani-um is an isolated vault that can-not sustain much change.Infection within the meningesleads to the inflammatory cas-cade, producing many dynamicevents in the brain from mildheadache to herniation anddeath. Because of the inflamma-tory response and the result of
increased blood flow, severalmajor complications developfrom meningitis:• Compromised respiratory status isa possible complication. The res-piratory center is located in thebrain stem, and additional pres-sure on this area causes changesin respiratory status. Vigilantassessment of respiratory statusshould focus on maintaining apatent airway. Changes in statusmay require noninvasive ventila-tor support or full ventilator sup-port as indicated by the patient’sdecline.11
• Circulatory collapse and shockcan occur during sepsis, whichcan mount an excessive immuneresponse, specifically the releaseof cytokines such as tumor necro-sis factor alpha. This event thenstimulates endothelial damageand a systemic inflammatoryresponse.13 Nurses should moni-tor volume status, while payingclose attention to vital signs,especially changes in blood pres-sure. Intravenous crystalloid flu-ids, volume expanders, andinotropic agents may be neces-sary to maintain adequate perfu-sion of organs.10 A pulmonary
www.nursing2007criticalcare.com July l Nursing2007CriticalCare l 33
Comparison of CSF findings among organisms
Source: Bader M, Littlejohns L. AANN Core Curriculum for Neuroscience Nursing. Philadelphia, Pa: Saunders; 2004:632.
Normal parameters
Open pressure(mm H2O)
Leukocyte countWBC/mm3
Neutrophils (%)
Protein (mg/dL)
Glucose (mg/dL)
Normal CSF
100 to 180
0 to 5
0
18 to 45
45 to 80; 0.6 timesblood glucose level
Bacterial meningitis
200 to 500
Increased 1,000 to5,000
Greater than or equalto 80
Elevated 100 to 500
Five to 40; less than0.3 times blood glucose level
Viral meningitis
Less than or equal to250
Increased 50 to 1,000
Less than 40
Elevated less than200
Greater than 45
Fungal meningitis
Greater than 200
Increased greaterthan 20
—
Elevated greater than45
Less than 40

artery catheter may become nec-essary for more detailed monitor-ing of hemodynamic status.11
• Cerebral edema is swelling ofthe cerebral tissue that can alsolead to increased ICP, thus affect-ing neurological status. Methodsto control cerebral edema includethe administration of hypertonicsaline solutions and osmoticdiuretics. In extreme cases,craniectomy, or bone flap re-moval via surgery, can also al-leviate pressure.9
• Hydrocephalus is secondary todecreased CSF absorption, andincreases CSF in the central ner-vous system. This leads toincreased ICP and must berelieved to prevent severe neuro-logic decompensation. A ven-triculostomy placed into the ven-tricles of the brain can help tomonitor ICP and drain excessCSF.11 It also creates a simpleavenue to obtain CSF specimensfor cultures. • Seizure activity is triggered byalteration in the electrical activi-ty of the brain.6 There can beseveral causes of seizure in ameningitis patient includingfever, edema, inflammation, andincreased pressure. Electroen-cephalogram (EEG) monitoringis needed to further investigatethe location, length, and severityof seizure activity. Corticalinflammation, a definitive causeof seizures in patients withmeningitis, may be visible onEEG.11 Antiepileptic medica-tions should be administered inmeningitis patients who have a clinical suspicion or priorseizure.11 Witnessed seizures canbe treated emergently with ben-zodiazepines. Protection fromself injury, maintaining adequateoxygenation, and airway patency
34 l Nursing2007CriticalCare l Volume 2, Number 4 www.nursing2007criticalcare.com
Meningitis
Case studyJ.T. is a 28-year-old Caucasian female who presented to the emer-gency department with complaints of headache, vomiting, andchanges in level of consciousness. A computed tomography scan ofthe head was done and showed enlarged ventricles, indicatinghydrocephalus. She was admitted to the neuroscience intensive careunit. A ventriculostomy was inserted to alleviate ventricular pres-sure, and samples of cerebrospinal fluid (CSF) were sent for analy-sis, including cultures. The initial CSF specimen isolated an organ-ism, and indicated protein and glucose levels consistent withmeningitis. Collective assessment of laboratory tests, diagnostics,signs and symptoms, and personal history of bird handling has ledto her diagnosis. She was diagnosed with infection by Cryptococcusneoformans, an infectious diseases physician was consulted, andamphotericin B was initiated intravenously. From admission to day5 of hospitalization, CSF results showed significant improvements.(See Results of CSF analysis over 5 days.) Once the infectioncleared, J.T. received a ventriculoperitoneal shunt (VPS).
In addition to the multiple shunt revisions during this admission,J.T. dealt with numerous complications in the ICU. Her residualneurological effects included memory deficiencies, slow speech,and flat affect. She developed a deep vein thrombosis, pulmonaryembolism, recurrent urinary tract infections, and multiple cardiacevents such as hypertension and tachycardia. During her ICUcourse, a brain biopsy was also done to rule out any malignant diag-nosis. She was eventually discharged to the neuroscience floor 4months after admission, only to return to ICU with respiratory fail-ure requiring ventilator support. This admission was the first ofmany admissions to the ICU from the neuroscience floor. J.T. spentapproximately 6 months in the hospital before she was finally dis-charged home. In the last month prior to discharge, she received apercutaneous endogastrostomy tube to help maintain caloric intake.Although her recovery was slow, she had ample family supportthroughout her lengthy hospitalization. Due to her prolonged hospi-talization, she also required the assistance of physical therapy, occu-pational therapy, and speech therapy in her long transition to nor-mal functionality. She eventually went to a rehabilitation facilityclose to home to finish her recovery.
Although this case may not be a typical patient seen in the neuro-science ICU, it demonstrates the damaging and long-term sequelaof fungal meningitis.
Results of CSF analysis over 5 daysAdmission Day 2 Day 5
Protein (mg/dL) 730 1,111 190
Glucose (mg/dL) 38 45 55

are important during seizures. • Diabetes insipidus (DI) and syn-drome of inappropriate antidiuretichormone (SIADH) are also compli-cations that may occur. Altera-tions in the pituitary gland leadto electrolyte disturbances andfluid imbalances. The posteriorpituitary secretes antidiuretichormone, and excess amountswill produce SIADH, whiledecreased amounts will produceDI. Serum sodium and osmolali-ty, body weight, and urine specif-ic gravity must be monitored fortrends. SIADH, which result inincreased water retention and alow serum sodium, is treated
with fluid restriction and insevere cases judicious replace-ment of sodium using hypertonicsaline intravenously.6 Diuretictherapy with furosemide (Lasix)may be initiated if fluid restric-tion is not sufficient.9 Diabetesinsipidus can increase waterexcretion and can be treated withfluid replacement and use ofvasopressin if deemed necessaryby the medical team, to facilitatewater reabsorption.6
• Immobility is caused by defi-ciencies in neurological status.Nursing measures include turn-ing the patient every 2 hours, per-forming range-of-motion exercis-es, and meticulous skin care.Deep vein thrombosis prophylax-is should also be implemented byuse of sequential compressiondevices and prophylactic antico-agulation if not contraindicated.• Gastrointestinal issues are anoth-
er complication. Decrease in gas-trointestinal motility for meningi-tis patient can result in complica-tion such as constipation. Stoolsofteners are given to encouragenormal bowel regimen. Increasedgastric secretions can cause pep-tic ulcers, so prophylaxis can beaccomplished by administeringproton pump inhibitors.11
• Herniation, one of the mostsevere complications, will leadto brain death. Herniation is theresult of many factors includingcerebral edema and increasedICP. Frequent neurologicalassessments with special atten-tion to pupillary response to
light are vital to predicting animpending herniation. A positiveassessment of pressure on thethird cranial nerve (oculomotornerve) is a clear indicator ofimpending downward pressureonto the brainstem. Ipsilateralpupillary dilatation may be anearly indicative sign of uncalherniation. Treatment to preventherniation consists of adminis-tration of diuretics, hypertonicsaline, osmotic diuretics, andmaintaining ICP less than 15mm Hg and CPP greater than 60mm Hg.11 (For more on manag-ing complications, see Casestudy.)
VaccinationAn important factor to considerin meningitis is disease preven-tion strategies. For example,there are several serotypes ofinfectious meningococci. Certain
types are specific to an endemicarea. Common serotypes ofmeningococci include A, B, C, Y,and W-135. The most commongroups found in the UnitedStates are groups B and C.8,12
There are two types of vaccinesavailable to prevent meningitis:the conjugate and the polysac-charide. Both of these vaccinesprevent infection from serotypesA, C, Y, and W-135, but not fromgroup B. The Centers for DiseaseControl and Prevention (CDC)recommends meningococcal vac-cination for specific groups: per-sons living in close quartersincluding military and first-year
college students, techniciansexposed to the bacteria, and per-sons traveling to sub-SaharanAfrican countries during themonths of December to June.16
It’s also recommended for trav-el to Mecca during the Hajj(Islamic pilgrimage to SaudiArabia). The CDC also recom-mends that those who have hada splenectomy also receive thevaccine.16 Pneumococcal, Hib,and influenza vaccines have alsoassisted in the decline of menin-gitis related to these infections.8
First line of defenseMeningitis is a universal phe-nomenon and can be devastatingto any patient. Specifically,meningococcal infection must bediagnosed and treated promptlywith antibiotics to prevent an epi-demic. The medical team mustbe diligent in its effort to over-
www.nursing2007criticalcare.com July l Nursing2007CriticalCare l 35
Meningococcal infection must be diagnosed and treatedpromptly with antibiotics to prevent an epidemic.

come the complex side effects ofbrain injury secondary to organ-ism invasion. Careful neurologi-cal examination by trained care-givers, interpretation of intracra-nial monitoring must be foremostin all nursing care. The criticalcare nurse is the first-line clini-cian to observe these patients inthe ICU, and thus is in an inte-gral part of the prevention ofmajor complications. The nursemust have a thorough under-standing of the anatomy of thebrain and understanding of theinflammatory cascade and itssequela. Adequate managementof respiratory infections andpneumonia can prevent meningi-tis. Such management includesappropriate vaccinations, espe-cially to high-risk populations,which may lessen the risk ofmeningitis. Prompt antibioticadministration for basal skullfractures and CSF leaks may alsolessen the risk of meningitis.9
Community education is alsoessential to disease prevention.
Vaccination as indicated by theCDC is essential in the preven-tion and spread of bacterialmeningitis. Research continues,and with the emergence of genet-ic factors in healthcare, new ther-apies and diagnostics may also beemerging. v
REFERENCES 1. Sherwood L. Human Physiology: FromCells to Systems. 5th ed. Belmont, Calif:BrooksCole/Thomson Learning; 2004.
2. World Health Organization. Meningococcalmeningitis. Available at: http://www.who.int/.Accessed May 30, 2007.
3. Lazoff M, Slabinski MS, Talavera F, et al.Meningitis. Available at: http://www.emedicine.com/EMERG/topic309.htm. AccessedMay 30, 2007.
4. de Assis Aquino Gondim F, Singh MK,Croul SE. Meningococcal meningitis. Avail-able at: http://www.emedicine.com/NEURO/topic210.htm. Accessed May 30, 2007.
5. Beaman MH, Wesselingh SL. Acute com-munity-acquired meningitis and encephalitis.Available at: http://www.mja.com.au/public/issues/177_05_020902/saltman_020902.html. Accessed May 30, 2007.
6. Bader K, Littlejohns L. AANN Core Cur-riculum for Neuroscience Nursing. St Louis,Mo: Saunders Elsevier; 2004:619-680.
7. King J, Markanday A, Khan A. Cryptococ-cosis. Available at: http://www.emedicine.com/med/topic482.htm. Accessed May 30, 2007.
8. Centers for Disease Control and Preven-
tion. Prevention and control of meningococ-cal disease: recommendations of the Advi-sory Committee on Immunization Practices(ACIP). MMWR Recommendations and Reports2005. Available at: http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5407a1.htm.Accessed May 30, 2007.
9. Hickey JV. The Clinical Practice of Neuro-logical and Neurosurgical Nursing. Philadel-phia, Pa: Lippincott Williams and Wilkins;2003:645.
10. Alspach J. Core Curriculum for CriticalCare Nursing. St Louis, Mo: Saunders Else-vier; 2006:500-505.
11. van de Beek D, de Gans J, Tunkel AR,Wijdicks EF. Community-acquired bacterialmeningitis in adults. N Engl J Med. 2006;354(1):44-53.
12. Rosenstein NE, Perkins BA, Stephens DS,et al. Meningococcal disease. N Engl J Med.2001;344(18):1378-1388.
13. Estep M. Meningococcal meningitis incritical care: an overview, new treatments/preventions, and a case study. Neurologicalinjury. Crit Care Nurs Q. 2005;28(2):111-121.
14. van de Beek D, de Gans J, McIntyre P,Prasad K. Steroids in adults with acute bacte-rial meningitis: a systematic review. LancetInfect Dis. 2004;4(3):139-143.
15. Vokshoor A, Moore L. Viral meningitis.Available at: http://www.emedicine.com/NEURO/topic607.htm. Accessed May 30, 2007.
16. Centers for Disease Control and Preven-tion. National Immunization Program. Avail-able at: http://www.cdc.gov/nip. AccessedMay 30, 2007.
At Emory University Hospital, Atlanta, Ga., neuro-science ICU, Sophary Burnet is a clinical nursemanager, Ann Huntley is a clinical nurse specialist,and Kelda M. Kemp is a Registered Nurse II.
36 l Nursing2007CriticalCare l Volume 2, Number 4 www.nursing2007criticalcare.com
Meningitis
INSTRUCTIONS
Meningitis: the inflamed brain
Earn CE credit online:Go to http://www.nursingcenter.com/NCC andreceive a certificate within minutes.
DISCOUNTS and CUSTOMER SERVICE• Send two or more tests in any nursing journal published by LippincottWilliiams and Wilkins together and deduct $0.95 from the price of each test.• We also offer CE accounts for hospitals and other health care facilities onnursingcenter.com. Call 1-800-787-8985 for details.
PROVIDER ACCREDITATION:Lippincot Williams & Wilkins, publisher of Nursing2007 Critical Care, willaward 2.0 contact hours for this continuing nursing education activity.
LWW is accredited as a provider of continuing nursing education by theAmerican Nurses Credentialing Center’s Commission on Accreditation.
LWW is also an approved provider of continuing nursing education by theAmerican Association of Critical-Care Nurses #00012278 (CERP Category A),District of Columbia, Florida #FBN2454, and Iowa #75. LWW home studyactivities are classified for Texas nursing continuing education requirementsas Type 1. This activity is also provider approved by the California Board ofRegistered Nursing, Provider Number CEP 11749, for 2.0 contact hours.Your certificate is valid in all states.
TEST INSTRUCTIONS• To take the test online, go to our secure Web site athttp://www.nursingcenter.com/NCC.• On the print form, record your answers in the testanswer section of the CE enrollment form on page 37.Each question has only one correct answer. You maymake copies of these forms.• Complete the registration information and courseevaluation. Mail the completed form and registrationfee of $19.95 to: Lippincott Williams & Wilkins, CE Group,2710 Yorktowne Blvd., Brick, NJ 08723. We will mail yourcertificate in 4 to 6 weeks. For faster service, include afax number and we will fax your certificate within 2business days of receiving your enrollment form. • You will receive your CE certificate of earned contacthours and an answer key to review your results. Thereis no minimum passing grade.• Registration deadline is August 31, 2009.

ENROLLMENT FORM Nursing2007 Critical Care, July, Meningitis: the inflamed brain
B. Test Answers: Darken one circle for your answer to each question.a b c d
1. m m m m2. m m m m3. m m m m4. m m m m
a b c d5. m m m m6. m m m m7. m m m m8. m m m m
a b c d9. m m m m
10. m m m m11. m m m m12. m m m m
a b c d13. m m m m14. m m m m15. m m m m16. m m m m
a b c d17. m m m m
C. Course Evaluation*1. Did this CE activity's learning objectives relate to its general purpose? q Yes q No2. Was the journal home study format an effective way to present the material? q Yes q No3. Was the content relevant to your nursing practice? q Yes q No4. How long did it take you to complete this CE activity?___ hours___minutes5. Suggestion for future topics _________________________________________________________
D. Two Easy Ways to Pay:q Check or money order enclosed (Payable to Lippincott Williams & Wilkins)q Charge my q Mastercard q Visa q American Express
Card # ____________________________________________ Exp. date __________________
Signature _____________________________________________________________________
*In accordance with the Iowa Board of Nursing administrative rules governing grievances, a copy of your evaluation of the CE offering may be submitted directly to the Iowa Board of Nursing. CCN0407
Meningitis: the inflamed brainGENERAL PURPOSE: To provide the registered professional nurse with an overview of meningitis, including causes, treatment, and nursing care.LEARNING OBJECTIVES: After reading this article and taking this test, you should be able to: 1. Describe the causative organisms and signs and symptomsof meningitis. 2. Discuss current treatment and potential complications of meningitis.
$
2.0ANCC/AACN CONTACT HOURS
A. Registration Information:
Last name ____________________________ First name ________________________ MI _____
Address _______________________________________________________________________________
City _______________________________________ State _________________ ZIP ______________
Telephone ___________________ Fax ___________________ E-mail ______________________
Registration Deadline: August 31, 2009Contact hours: 2.0 Pharmacology hours: 0.0 Fee: $19.95
q LPN q RN q CNS q NP q CRNA q CNM q other _________________
Job title _______________________________ Specialty _________________________________
Type of facility _______________________________ Are you certified? q Yes q No
Certified by _________________________________________________________________________
State of license (1) __________________________ License # _________________________
State of license (2) __________________________ License # _________________________
q Please fax my certificate to me.q From time to time, we make our mailing list available to outside organizations to announce spe-
cial offers. Please check here if you do not wish us to release your name and address.
1. The primary entrance for pathogens causingmeningitis isa. basal skull fracture. c. ears.b. nasopharynx. d. ventricles.
2. The protective layers of the central nervous sys-tem are known as thea. meninges.b. glial cells.c. cerebrospinal fluid (CSF).d. arachnoid villi.
3. Which causative organism for meningitis is mostcommon in communal living situations?a. Cryptococcus neoformansb. Streptococcus pneumoniaec. Neisseria meningitidisd. Cytomegalovirus
4. Which type of meningitis has a reduced inci-dence due to an effective childhood vaccine?a. Staphylococcus aureusb. echovirusc. Listeria monocytogenesd. Haemophilus influenzae
5. Which type of virus is responsible for 85% to95% of all viral meningitis cases?a. varicella-zoster virusb. Cytomegalovirusc. Enterovirusd. adenovirus
6. Which statement is true regarding fungalmeningeal infections?a. They have a sudden and severe onset of symp-
toms.b. They are a less dangerous infection because the
organisms are encapsulated. c. They exhibit a macular skin rash.d. They have a tendency to recur.
7. A positive Brudzinski’s sign isa. an elevated opening pressure when obtaining CSF.
b. the involuntary flexion of the hips with passiveneck flexion in a supine position.
c. neck pain and hamstring resistance with passiveknee extension.
d. confusion, irritability, and photophobia on theneurologic exam.
8. Explain to the patient and family that a computedtomography scan is needed a. to assess fluid accumulation and swelling in the
brain.b. on everybody presenting to the emergency
department with a headache.c. to determine the organism causing meningitis.d. to measure the pressure on the brain.
9. Which of the following statements is trueregarding initial nursing care?a. Begin antibiotics once CSF cultures are obtained.b. Begin antibiotics even if the organism has not
been identified.c. Keep the patient flat; do not elevate the head of
the bed.d. Maintain a stimulating environment to minimize
neurologic loss.
10. Which nursing measure is most appropriate forsuspected meningococcal meningitis?a. droplet precautions for 24 hours after initiation of
therapyb. strict isolation for 24 hoursc. universal precautionsd. prophylactic antibiotics for close contacts within
1 week of diagnosis
11. Which statement best reflects current researchon dexamethasone use with bacterial meningitisin adults?a. It is ineffective and not recommended.b. If given with the first dose of antibiotics, it may
decrease the inflammatory response.c. It should be administered with every dose of a
full course of antibiotics.d. Dexamethasone use has been widely studied and
is universally recommended.
12. Which of the following is indicated for fungalmeningitis?a. dexamethasone c. amphotericin Bb. ceftriaxone d. ciprofloxacin
13. Ventriculostomy is used for all of the followingexcepta. administering hypertonic saline.b. monitoring intracranial pressure. c. draining excess CSF.d. obtaining CSF culture specimens.
14. Witnessed seizures in patients with meningitisare emergently treated witha. antiepileptic medications.b. placement of a ventriculostomy.c. administration of high-dose glucocorticoids.d. administration of benzodiazepines.
15. A low serum sodium and increasing bodyweight are suspicious of which complication?a. diabetes insipidusb. circulatory collapsec. syndrome of inappropriate antidiuretic hormoned. tumor necrosis factor alpha
16. In patients with meningitis, testing of the pupil-lary response to light is used to determinea. presence of photophobia.b. impending brain herniation.c. seizure potential. d. oversedation with opioids.
17. Which group should receive meningococcalvaccination?a. all infants b. children in grade schoolc. first-year college studentsd. all persons traveling to China
$
Related Documents