Journa CALIFORNIA DENTAL ASSOCIATION Veneer Restorations Bleaching Systems Orthodontic Treatment Osteonecrosis Circadian Behaviors December 2019 Vol 47 N o 9 Spotlight on Dental Student Research Alice Goodwin, DDS, PhD, and Kyle Jones, DDS, PhD

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

JournaC A L I F O R N I A D E N T A L A S S O C I A T I O N
Veneer Restorations
Bleaching Systems
Orthodontic Treatment
Osteonecrosis
Circadian Behaviors
December 2019
Vo
l 47N
o9
Spotlight on Dental Student ResearchAlice Goodwin, DDS, PhD, and Kyle Jones, DDS, PhD
SAVE MOREON DENTAL SUPPLIESTHAN YOU PAY IN DUESThere’s no better time to be an association member!Your benefits now include negotiated discounts andfree shipping through The Dentists Supply Company.
See how tdsc.com can help you save more on dentalsupplies than you pay in annual association dues.
SHOP ONLINE ANDS TART SAVING TODAY
C DA J O U R N A L , V O L 4 7 , Nº 1 2
DECEMBER 2 0 1 9 755
Spotlight on Dental Student Research
An introduction to the issue.Alice Goodwin, DDS, PhD, and Kyle Jones, DDS, PhD
Minimally Invasive Veneer Restorations: Effect of Restorative Material on Traumatic Impact Strength
This article discusses how modern restorative materials and adhesive techniques are capable of restoring traumatized teeth to the impact strength of natural intact teeth.Michelle Yang, BS; Erik Balinghassay, BS; Johnny Huynh, BS; Xuehui Liu, DDS; Chunling Ge, DDS PhD; and Shane Newport White, BDentSc, MS, MA, PhD
Titanium-Oxide Nanoparticles and Nanofibers Used Alone or With UV Light Activation
This study evaluated the change in oxidation potential of synthesized TiO2 nanofibers (NFs) compared to commercial TiO2 nanoparticles (NPs).Christina Chi, BA, DDS; Brittney N. Springer, BS; Elvin Walemba, BSc, MRes, PhDc; Kevin E. Nick, PhD; Christopher C. Perry, PhD; and So Ran Kwon, DDS, MS, PhD, MS
Clinical and Microbial Changes in Orthodontic Patients Using Clear Aligners Vs. Fixed Appliances
This pilot study investigated the clinical and microbial changes that occur in patients undergoing orthodontic treatment using fixed appliances and clear aligners.Joseph Mullen, BS; Melissa Agnello, PhD; Edward Viloria, DDS; Kenneth Chang Chien, BS; Emily Duong, BS; Masuma Rizvi, BDS; Pega Hajian, BS; Huiying Li, PhD; Baochen Shi, PhD; Kang Ting, DMD, DMedSc; Wenyuan Shi, PhD; Renate Lux, PhD; and Tingxi Wu, DDS, PhD
10-Year Institutional Retrospective Case-Control Study of Medication-Related Osteonecrosis of the Jaw
This study looked at the association between ART and MRONJ for cancer therapy.Pardis Barati Mahvar, BSc; Amna Imran, DDS, MPhil, BDS; Reyes Enciso, PhD; Andrew Sanapanya, BS; Mohammad Khalifeh, DDS, MS; Parish P. Sedghizadeh, DDS, MS; and Laurel Henderson, DDS, MS
Circadian Behaviors of Oral and Skin Fibroblasts
This study reports fibroblasts derived from mouse palatal mucosa and dorsal skin and suggests that oral wound healing involving fibroblast repopulation and contraction may follow a diurnal cycle.John Ngo, BS; Hodaka Sasaki, DDS, PhD; and Ichiro Nishimura, DDS, DMSc, DMD
769
771
777
783
793
801
Dec. 2019
d e pa r tm e n t s
f e at u r e s
The Editor/Earworms and Merciful Acts
Letter to the Editor
Thank You to the 2019 Reviewers
Impressions
RM Matters/Reduce Risk, Increase Productivity With Cellphone Policies
Regulatory Compliance/HIPAA Myths Explained
Ethics/How To Handle a Difficult Situation
Tech Trends
757
761
763
765
811
815
819
822
765
First lineXXX

C DA J O U R N A L , V O L 4 7 , Nº 1 2
756 D E C E M B E R 2 01 9
Volume 47, Number 12 December 2019
JournaC A L I F O R N I A D E N T A L A S S O C I A T I O N
CDA classifieds work harder to
bring you results. Selling a practice
or a piece of equipment? Now you
can include photos to help buyers
see the potential.
And if you’re hiring, candidates
anywhere can apply right from
the site. Looking for a job? You can
post that, too. And the best part—
it’s free to all CDA members.
All of these features are designed to
help you get the results you need,
faster than ever. Check it out for
yourself at cda.org/classifieds.
CDA Classifieds. Free postings.Priceless results.
CDA OfficersR. Del Brunner, DDSpresident
Richard J. Nagy, DDSpresident-elect
Judee Tippett-Whyte, DDS vice president [email protected]
Ariane R. Terlet, DDS secretary [email protected]
Steven J. Kend, DDStreasurer
Debra S. Finney, MS, DDS, speaker of the house
Natasha A. Lee, DDSimmediate past president
ManagementPeter A. DuBoisexecutive director
Carrie E. Gordonchief strategy officer
Kristine Allingtonchief marketing officer
Alicia Malabycommunications director
Cris Webercreative and ux director
EditorialKerry K. Carney, DDS, CDEeditor-in-chief [email protected]
Ruchi K. Sahota, DDS, CDEassociate editor
Brian K. Shue, DDS, CDEassociate editor
Gayle Mathe, RDHsenior editor
Alice Goodwin, DDS, PhD Kyle Jones, DDS, PhDguest editors
Andrea LaMattina, CDEpublications manager
Kristi Parker Johnsonsenior communications specialist
Joie R. Harrisoncommunications and media relations specialist
Blake Ellingtontech trends editor
Jack F. Conley, DDSeditor emeritus
Robert E. Horseman, DDShumorist emeritus
ProductionRandi Taylorsenior graphic designer
Upcoming Topics January/Importance of Research in Dental EducationFebruary/AestheticsMarch/CDA’s 150th Anniversary
Advertising Sue Gardner advertising sales
Permission and ReprintsAndrea LaMattina, CDEpublications manager
Manuscript Submissionswww.editorialmanager.com/jcaldentassoc
Letters to the Editorwww.editorialmanager.com/jcaldentassoc
SubscriptionsAnnual subscriptions are available to association members at a rate of $36. To manage your printed Journal subscription online, log in to your cda.org account or email [email protected] for assistance. View the publication online at cda.org/journal.
published by the California Dental Association 1201 K St., 14th Floor Sacramento, CA 95814 800.232.7645 cda.org
Journal of the California Dental Association (issn 1043–2256) is published monthly by the California Dental Association, 1201 K St., 14th Floor, Sacramento, CA 95814, 916.554.5950. Periodicals postage paid at Sacramento, Calif. Postmaster: Send address changes to Journal of the California Dental Association, 1201 K St., 14th Floor, Sacramento, CA 95814.
The California Dental Association holds the copyright for all articles and artwork published herein. The Journal of the California Dental Association is published under the supervision of CDA’s editorial staff. Neither the editorial staff, the editor, nor the association are responsible for any expression of opinion or statement of fact, all of which are published solely on the authority of the author whose name is indicated. The association reserves the right to illustrate, reduce, revise or reject any manuscript submitted. Articles are considered for publication on condition that they are contributed solely to the Journal of the California Dental Association. The association does not assume liability for the content of advertisements, nor do advertisements constitute endorsement or approval of advertised products or services.
Copyright 2019 by the California Dental Association. All rights reserved.
@cdadentists
Connect to the CDA community by following and sharing on social channels
C DA J O U R N A L , V O L 4 7 , Nº 1 2
DECEMBER 2 0 1 9 757
Editor
Everyone has had it happen. You hear a tune and cannot get it out of your mind. This phenomenon has been described as a cognitive itch
or an earworm. Once ensconced in your thoughts, it is very difficult to drive out. It can wake you up at night. It can weave its way into every thought you have. The song can be in and of itself annoying, like a certain commercial about donating your cars to children, or, as in my case, the song can be simply cognitively sticky (like almost any song by Phil Collins).
Online, there are several suggestions for how to get rid of these earworms. My personal remedy involves either non-lexical vocables to the theme from “Bonanza” or the insistent refrain from Edwin Starr’s 1969 hit “War.”
The other day, I experienced a visual analog of this auditory tic. I was on my way to a meeting of dental editors in San Francisco. I was scanning the familiar urban scene through the car window when I marked a street vignette. A youngish woman with no visible means of support and a large backpack and a bedroll was leaning against a storefront wall. As I watched, she reached into her backpack, pulled out a toothbrush and toothpaste and proceeded to brush her teeth and spit over the curb into the street.
She was as discrete as possible under the circumstances. It made me wonder about her backstory. How did she get there? What vagaries of nature, nurture and fortune had led to this point? Since that moment, that scene has returned again and again to my thoughts.
There is no way to discern how that woman is living from day to
day. She was like a time-lapse video where she is crystal clear and the rest of the population is a blur. People walk past her on their way to a temporally structured day in a life with a reliable social structure. But she seemed disconnected, like a planet without an orbit.
When things break down so completely that you are living on the street, how does dental health still come to the fore? In a situation with no social backstop, how does the morning ritual of toothbrushing still endure?
When we are presented with a picture and no information, we have a tendency to fill in the backstory based on our own experience or fears. I kept thinking: What kind of little girl was she? Who showed her how to brush her teeth? Who instilled the importance of oral hygiene? Was it a hygienist, a dentist, a parent? Or was it just the continuing echo of Ipana’s Bucky Beaver ad campaign of the 1950s that directed the American population to “brush regularly and see your dentist every six months.”
Or maybe her oral hygiene ritual was an attempt to normalize her situation as much as possible. Maybe it helped bring a little order to a chaotic situation. Whatever the reason for her present circumstances, her image stayed with me like an earworm.
Singing the theme from “Bonanza” or the refrain from “War” did not eliminate the image from the recurring loop stuck in my head. However, I think I have discovered a possible antidote: CDA Cares. I started thinking about CDA Cares.
San Francisco has just over 8,000 homeless individuals. California as a whole has just under 130,000 homeless. That represents about a quarter of the national homeless population.1 This population makes up only a portion of the people that CDA Cares helps.
In 2012, the CDA Foundation held its first free dental clinic, CDA Cares, in Modesto, Calif. This original experiment was a collaboration with the national organization Missions of Mercy. The CDA Foundation has now held 16 CDA Cares events. The most recent was held in September in San Bernardino. CDA Cares was located twice in Modesto, Sacramento and Solano County. It has also been held in San Jose, San Diego, Pomona, Fresno, Ventura, Stockton, San Mateo, Bakersfield and Anaheim.
These events are amazing. They are like a military operation. The planning begins months in advance. Local connections are made to outreach organizations that get the word to folks who need help.
Earworms and Merciful ActsKerry K. Carney, DDS, CDE
When things break down so completely that you are living on the street, how does dental health still come to the fore?
C DA J O U R N A L , V O L 4 7 , Nº 1 2
758 D E C E M B E R 2 01 9
D E C . 2 0 1 9 E D I T O R
Before the first patient is seen, the location is a beehive of activity. Large exhibition halls are converted into a maze of specialized operations.
After a day of erecting privacy barriers, laying electrical cables, connecting pipes, setting up chairs and organizing the sterilization and supplies area, there is palpable excitement and expectation. The first patients show up the night before so they can be triaged and ready to be seen first thing in the morning. It is very moving to see people standing in line long before daybreak so they can be ready to receive care as soon as the event opens.
Once the gate opens, the operation runs smoothly, moving patients through intake, medical history and medical evaluation on to triage, radiographs and treatment. After the procedures are completed, the patient is guided to the pharmacy area, if necessary, and then on to an exit interview. Patients are provided with contacts to seek ongoing dental care, and often, community partners are on-site to provide information on additional local resources
Many times I have seen patients in their exit interview ask how they can volunteer to help with the next event. Heartwarming though that is, my favorite memory is of a crusty legislator whom I was guiding on a tour of the event. He was amazed at the donated service he witnessed. He was astounded that not only had dentists come from all over California to donate their time and expertise, but in many cases had closed their offices and brought their staff with them to the event. He was very appreciative, but the emotional moment came when he watched a
denture patient radiant with surprise and pleasure admiring his new smile in the mirror. The patient had not had teeth for years and that day he got his smile back. He beamed and the legislator got tears in his eyes.
It was at that moment that I reflected on how great it is to be a dentist and to be able to give someone the gift of their smile. It was a very touching moment that reminds me of the importance of every single merciful act.
CDA Cares has transformed the lives of more than 30,000 people. Through CDA Cares, California dentists have provided oral health services valued at more than $25 million to individuals who would otherwise go without. With tremendous attention from the media, policymakers and the public, organized dentistry has increased leveraging power for policymaking issues like adding adult Denti-Cal back into the state’s budget and bringing to light the importance of oral health for Californians.
Millions of Californians still experience barriers to care. With every CDA member’s support, the CDA Foundation continues to build on this momentum and create lasting change for our state’s most vulnerable citizens.
If you have never been involved with a CDA Cares event, you are missing out. As dentists, we have the immediate gratification of helping relieve pain and restore smiles every day. But the gratification that one feels at the end of a CDA Cares event is that feeling magnified a thousandfold. n
reference
1. Fagan K. SF homeless population swells by 17% in latest tally. www.sfchronicle.com/bayarea/article/SF-homeless-population-swells-by-17-in-latest-13851897.php.
The Journal welcomes lettersWe reserve the right to edit all
communications. Letters should discuss an item published in the Journal within the last two months or matters of general interest to our readership. Letters must be no more than 500 words and cite no more than five references. No illustrations will be accepted. Letters should be submitted at editorialmanager.com/jcaldentassoc. By sending the letter, the author certifies that neither the letter nor one with substantially similar content under the writer’s authorship has been published or is being considered for publication elsewhere, and the author acknowledges and agrees that the letter and all rights with regard to the letter become the property of CDA.
(855) 886-4824 | firstrepublic.com | New York Stock Exchange symbol: FRCMEMbER FDIC aND Equal HouSINg lENDER
“First Republic handles the banking side of our business, allowing us to focus on taking the best care of our patients.”
W e s t P o rta l o r a l & Fac i a l s u r g e ry c e n t e r
Dean L. Duncan, D.D.S. (left); Eric M. Scharf, D.D.S. (right)
CDAJour Dec_19 WestPortal ND2017.indd 1 10/7/19 7:42 PM
C DA J O U R N A L , V O L 4 7 , Nº 1 2
DECEMBER 2 0 1 9 761
medication identification, preparation and administration to essentially a layperson with no medical or nursing background. This is a duty that should only be done by individuals with an advanced professional degree and health care license such as a nurse, pharmacist or doctor.
Unfortunately, last year the California legislature passed and the governor signed SB 501. This law reinforced, continues and further codified the legality of this dangerous practice. This should be an affront to anybody who is invested in patient safety and seeks to reduce medical errors.
I wholeheartedly encourage any dental assistant, or for that matter anyone in dentistry, who takes on the task of additional training and education. The more that our assistants know and understand about the procedures we are doing, the better we are as doctors. But entrusting this important responsibility of sedation and anesthesia mediation administration to minimally trained dental assistants cannot replace the rigorous and accredited education that all licensed doctors and nurses have undergone.
It is high time that California dentists take patient safety seriously. This can start by abolishing a system in place in California that allows unqualified and unlicensed personnel to be responsible for the preparation, labeling and administration of potentially dangerous sedative medications. This would be a start that we take patient safety seriously.
l e n n y n a f ta l i n , d d s
Vice President, American Society of Dentist Anesthesiologists
President, California Society of Dentist Anesthesiologists
The Editor-in-Chief and Guest Editor Respond
Thank you for your letter Dr. Naftalin; we are pleased that you found Drs. Stevens and Sarasin’s article informative. Your letter expressed concerns regarding dental sedation assistants (DSAs), which provides an opportunity to describe for our readers the qualifications of this California dental team member.
The DSA, enacted in 2009 by the California Legislature, must complete a Dental Board of California approved course of instruction detailed in California Code of Regulations, Section 1070.8, and must pass a permitting examination to practice. A DSA’s education and training requires sedation-specific instruction of not less than 110 hours, and at a minimum must include 38 hours of clinical instruction and 20 supervised sedation cases.
The DSA’s primary role is to monitor the sedated patient and be a second pair of eyes, ears and hands for the dentist providing sedation services. The DSA’s duties, which are described in detail in the Dental Practice Act, Section 1750.5, require direct supervision as described further here (italics added):
JournaC A L I F O R N I A D E N T A L A S S O C I A T I O N
Patient Safety
Checklists
Legal Perspectives
Emergency Medications
July 2019
Perspectives and DirectionsDavid L. Rothman, DDS
Safety in DENTISTRY
Letter
I applaud the CDA and Dr. Rothman for the two journal editions dedicated to safety in dentistry. As an officer of the American Society of Dentist Anesthesiologists and the California Society of Dentist Anesthesiologists, we have long been dedicated to advocating for patient safety in the realm of anesthesia and sedation within dentistry.
Drs. Stevens and Sarasin’s article titled “Medication Safety: Reducing Errors and Adverse Drug Events in Dentistry” (September 2019) addresses medication errors in dentistry. Medical errors and, more specifically, medication errors are certainly problematic. These errors can lead to patient harm and even death. The exact numbers may be debatable, but every doctor should consider adopting every policy meant to prevent these errors from happening. Even one death or injury from a preventable medication error is one error too many.
However, Drs. Stevens and Sarasin’s article has a glaring omission of a systemic potential for medication errors permitted by law in California. Specifically in California, a “dental sedation assistant” can draw up, label and even administer irreversible sedative medications into an existing intravenous line in a patient. To become a dental sedation assistant, there is no need for any higher educational degree. This is on-the-job training in the office of approved oral surgeons. According to the Dental Board of California’s website, there are only 13 approved offices to obtain this training. Ten of these offices do not offer the course to other dental assistants outside of their practices. No other health care model would delegate such critical duties such as
Medication Safety and Dental Sedation Assistants
C DA J O U R N A L , V O L 4 7 , Nº 1 2
762 D E C E M B E R 2 01 9
■n (b) Monitor patients undergoing conscious sedation or general anesthesia utilizing data from noninvasive instrumentation … (b) Monitor patients undergoing conscious sedation or general anesthesia utilizing data from noninvasive instrumentation . . . evaluation of the condition of a sedated patient shall remain the responsibility of the dentist or other licensed health care professional authorized to administer [sedation], who shall be at the patient’s chairside while [sedation] is being administered.
■n (c) Drug identification and draw, limited to identification of appropriate medications,
D E C . 2 0 1 9 L E T T E R
ampule and vial preparation, and withdrawing drugs of correct amount as verified by the supervising dentist.
■n (d) Add drugs, medications and fluids to intravenous lines using a syringe, provided that a supervising licensed dentist is present at the patient’s chairside . . .The exception to this duty is the initial dose of a drug or medication shall be administered by the supervising licensed dentist.
Further, current law requires a DSA to be dedicated to monitoring and sedation assisting functions and cannot also be assisting the dentist for the dental treatment. Your assertion that California law allows “unqualified and unlicensed
personnel to be responsible for the preparation, labeling and administration of potentially dangerous sedative medications” is unfounded and not consistent with the requirements of the law.
We appreciate your continuing leadership and interest in patient safety and the series of articles on safety. Thank you again for taking time to participate in the forum of ideas that the Journal of the California Dental Association promotes. Discussions such as this can only bring more light on the subject and promote positive change.
k e r ry k . c a r n e y , d d s , c d e
Editor-in-Chiefdav i d l . r ot h m a n, d d s
Guest Editor
Insurance companies vary by region. Oscar coverage will be available starting January 1, 2020.
CoveredCA.com/ForSmallBusiness | 844.332.8384
Health coverage for practices of every type.
While you’re busy keeping your patients healthy, make sure your
employees are too. With Covered California for Small Business,
we help tailor health plan options so your employees can get
the coverage they want at a price that fits their budget and
yours. Give your employees financial protection and peace of
mind by offering them quality health insurance with access to
doctors and hospitals that fit their needs.
19CCM0015_D-CCP
10/22/19 11:31
1 of 1
M.Garrand J. Untalan
Healthcare
MG
edits
11249781
204015
2/0
CC/Print/2019/CCSB
Magazine - 4C
9.85”w x 6.625” h
Internal
7.375 in.
4.7
5 in
.
C DA J O U R N A L , V O L 4 7 , Nº 1 2
DECEMBER 2 0 1 9 763
Thank You to the 2019 ReviewersThe Journal of the California Dental Association is grateful for the many professionals who formally reviewed manuscripts in 2019 and offered their recommendations. We extend our thanks to those who are instrumental in helping us produce this award-winning scientific publication.
Ahmad Abdelkarim, DDS, MS, PhD, DMD, EdD
Marco M. Allard, PhDPamela Alston, DDS, MACraig W. Amundson, DDSElizabeth Andrews, DDS, MSHomayon Asadi, DDSKathryn Atchison, DDS, MPHDavid M. Avenetti, DDS, MPH, MSDLeif K. Bakland, DDSJeffrey Banas, PhDNicole Barkhordar, DDS, MEdDane Barlow, BBAJane R. Barrow, MSForrest Batz, PharmDKen Berley, DDS, JDJohn L. Blake, DDSAlan O. Blanton, DDS, MSGeorge Bogen, DDSRobert L. Boyd, DDSRonni Elise Brown, DDS, MPHMichael E. Cadra, DMD, MDBenjamin Chaffee, DDS, MPH, PhDDavid W. Chambers, EdM, MBA, PhDHubert Chan, DDSDavid Clark, DDSPaulo G. Coelho, DDS, PhDSusan E. Coldwell, PhDScott Conley, DDSLeopoldo P. Correa, BDS, MSSantos Cortez, DDSJean L. Creasey, DDSDavid R. Cummings, DDSEve Cuny, MSArthur Curley, JDMichael John Danford, DDSKaren K. Daw, MBA, CECMMartin Denbar, DDSRaymond Dionne, DDS, PhDSophie Domejean, DDS, PhDMark Donaldson, PharmDEvelyn Donate-Bartfield, PhDLori L. Doran-Garcia, DDSRena D’Souza, DDS, MS, PhDPiedad Suárez Durall, DDSChad Edwards, DDSSridhar Eswaran, BDS, MS, MSD Rhonda Everett, DDS, MPH
Ronald L. Ettinger, BDS, MDS, DDScLeticia Ferreira, DDS, MSJared Ira Fine, DDS, MPHBarry Freydberg, DDSYuwei Fan, PhDFariborz A. Farnad, DMDJames Fedusenko, DDS, RNAlan L. Felsenfeld, DDSLeticia Ferreira, DDS, MSJared Ira Fine, DDS, MPHTracy L. Finlayson, PhDSteven Friedrichsen, DDSBarry Freydberg, DDSSangeeta Gajendra, DDS, MPH, MSDesmond Gallagher, DDS, MASteven Ganzberg, DMD, MSClarisa Amarillas Gastelum, DDS, MSLawrence Gettleman, DMD, MSDJay Golinveaux, DDS, MSAnupama Grandhi, DDSMina Habibian, DMD, MS, PhDMagnus Hakeberg, DDS, PhDMarc Hayashi, DMDLisa Heaton, PhDReza Heshmati, DDS, MPH, MSEdmund Hewlett, DDSHelia Hooshangi, DDSMichelle Hurlbutt, RDH, MSDH, DHScNicola P.T. Innes, PhD, BDS, BSc, BMScRobert Isman, DDS, MPHLisa Itaya, DDSShankar Iyer, DDS, MDSPoonam Jain, BDS, MS, MPHDaniel Jenkins, DDSGinny Jorgensen, CDA, EFDAJohn R. Kalmar, DMD, PhDMathew Thomas Kattadiyil, BDS,
MDS, MSCristin E. Kearns, DDS, MBAChun K. Kim, DDSPerry Klokkevold, DDS, MSGregory Kolber, DDSJayanth Kumar, DDS, MPHSatish Kumar, DDS, MDSc, MSKevin Kwiecien, DMD, MSClarice S. Law, DMD, MSIrving Lebovics, DDSCindy Lebovics, RDH, DDS, EdD
Stuart E. Lieblich, DMDBrent Lin, DMDJeffrey W. Lineberry, DDSSanjay M Mallya, BDS, MDS, PhDDavid John Manton, BDSc, MDSc, PhDLeonardo Marchini, DDS, MSD, PhDMichael Marshall, DDS, HDSMichael Mashni, DDSMelanie E. Mayberry, DDS, MSKeith A. Mays, DDS, MS, PhDMaureen McAndrew, DDS, MSEdCarol J. McCutcheon, DDSDaniel W. McNeil, PhDEric P. Mediavilla, DDSMichael Meharry, DDSMike Meru, DDSDiana Messadi, DDS, MMSc, DMScMichael Monopoli, DMD, MPH, MSAlireza Moshaverinia, DDS, MS, PhDSherry A. Mostofi, Esq.Richard P. Mungo, DDS, MSD, MEdCarol Anne Murdoch-Kinch, DDS, PhD Theodore A. Murray Jr., DDSRichard J. Nagy, DDS Ichiro Nishimura, DDS, DMDNooshin Noghreian, DDSAdamo E. Notarantonio, DDSBrian Novy, DDSDennis P. Nutter, DDSGregory Olson, DDS, MSDaniel L. Orr, DDS, MS, PhD, JD, MDJoan Otomo-Corgel, DDS, MPHUdochukwu Oyoyo, MPHMariela Padilla, DDS, MEd Robert J. Palmer Jr., PhDDavid W. Paquette, DMD, MPH,
DMScSeena Patel, DMD, MPHTejas Patel, DMD, BDSSteven Perlman, DDS, MScD, DHLOve Peters, DMD, MS, PhDPeter J. Polverini, BS, DDS, DMScDoreen Pon, PharmDIain Pretty, BDS, MSc, PhDFred Quarnstrom, DDSChristine Quinn, DDSJack Ringer, DDSAlvin Rosenblum, DDS
Charles Rosson, DMDDavid Lawrence Rothman, DDSGary Sabbadini, DDSRoberto Savignano, MS, PhDKrunal Sherathiya, DDSWerner Shintaku, DDS, MS, MSCharles Shuler, BSc, DMD, PhDHarel Simon, DMDKrikor Simonian, DDS, DABPHarold C. Slavkin, DDS Rebecca L. Slayton, DDS, PhDColby Smith, DDSRichard D. Smith, DDSEric C. Sung, DDSRoy L. Stevens, DDSMontry Suprono, DDS, MSDMarlene Talley, DDSParihan Tamkin, DDSThomas Tanbonliong Jr., DDSScott L. Tomar, DMD, DrPHJanice A. Townsend, DDS, MSPhilip A. Trask, DDS, MSRichard D. Trushkowsky, DDSCynthia S. Valle-Oseguera, PharmDSuvendra Vijayan, BDS, MPH, MSMarisa K. Watanabe, DDS, MSDarien Weatherspoon, DDS, MPHMea A. Weinberg, MS, DDSJane A. Weintraub, DDS, MPHJohn F. Weston, DDSKyumin Whang, BS, MS, PhDKimberly G. Whippy, DMDTiril Willumsen, Dr OdontLukaz Witek, MSci, PhDCun-Yu Wong, DDS, PhDTim Wright, DDS, MSBenjamin M. Wu, DDS, PhDJuan Fernando Yepes, DDS, MD,
MPH, MS, DrPHSimon Young, DDS, MD, PhDLing Zhan, DDS, PhDAnthony J. Ziebert, DDS, MS
Every effort was made to ensure the accuracy of the list of contributors. If you discover an error or omission, please accept our apologies.
Reviewers
BE BOLD.BE BRIGHT.BELONG.
TOGETHERWE ARE
LIMITLESS
®
Be a part of what’s next as CDA celebrates 150 years.Explore new benefits and renew your membership for 2020 at cda.org/renew.

C DA J O U R N A L , V O L 4 7 , Nº 1 2
DECEMBER 2 0 1 9 765
Impressions
Anesthetic Approaches for Special Needs Patients
A recent study found that safe, successful dental treatments in special needs patients depend on choosing the right anesthetic methods and equipment and having a skilled staff. The study was published in the Journal of Dental Anesthesia and Pain Medicine in August.
Researchers found that the use of local anesthesia is sufficient for completing simple dental treatments, with 90% of patients in the study tolerating it. About 7% of patients needed additional analgesia and about 3% of patients were given narcotic analgesics in treatments that caused severe pain.
The study aimed to provide content about the different anesthetic approaches used in patients with special needs and included the medical records of 710 patients with special needs who were treated with general anesthesia or sedation. The patients ranged in age from 1 to 68.
For comparisons, the patients were evaluated according to the following groups: Down syndrome, other syndromes, psychiatric disorders, physical disabilities and complicated medical stories. Complicated medical stories included those patients who had conditions that affected their mental and motor abilities, such as cerebral palsy and spina bifida.
About 73% of patients were given general anesthesia and approximately 22% were sedated, according to the study. The mean duration of anesthesia was about 43 minutes.
Simple dental treatments were performed in patients in all groups, but the most common complications were found in those from the other-syndromes group.
The patients with other syndromes underwent maxillofacial procedures to correct facial deformities caused by self-injurious behaviors. Clinicians shortened anesthesia periods as much as possible for those in this group due to their life-threatening conditions.
Despite taking these steps, the author found that clinicians could not provide optimal treatments for these patients and only performed symptomatic and not restorative treatments.
Due to the difficult vascular access in other-syndrome patients, sevoflurane inhalation was used to extract teeth. Though very few patients were administered general anesthesia, this group experienced the highest complication rates, according to the author.
Patients with Down syndrome had specific diseases and conditions, such as respiratory system-related anomalies and severely low heart rates, that affected the types of anesthetic approaches used. Sedation was chosen for patients with Down syndrome due to intubation difficulties.
Although this is a complex subject, the common point was that all these patients required special care during dental procedures, according to the study.
Learn more about this study in the Journal of Dental Anesthesia and Pain Medicine (2019); doi.org/10.17245/jdapm.2019.19.4.191.■n■
BE BOLD.BE BRIGHT.BELONG.
TOGETHERWE ARE
LIMITLESS
®
Be a part of what’s next as CDA celebrates 150 years.Explore new benefits and renew your membership for 2020 at cda.org/renew.

C DA J O U R N A L , V O L 4 7 , Nº 1 2
766 D E C E M B E R 2 01 9
Periodontitis Associated With Hypertension Risk People with periodontitis have a greater likelihood of hypertension,
according to a study conducted by researchers from the UCL Eastman Dental Institute in the U.K. and published in Cardiovascular Research.
This study compiled the best available evidence to examine the odds of high blood pressure in patients with moderate and severe gum disease. A total of 81 studies from 26 countries were included in the meta-analysis.
Moderate-to-severe periodontitis was associated with a 22% raised risk for hypertension, while severe periodontitis was linked with 49% higher odds of hypertension, according to the study.
“We observed a positive linear relationship, with the hazard of high blood pressure rising as gum disease became more severe,” said lead author Eva Munoz Aguilera, MClinDent.
Average arterial blood pressure was higher in patients with periodontitis compared to those without. This amounted to 4.5 mmHg higher systolic and 2 mmHg higher diastolic blood pressures.
“The differences are not negligible,” said Dr. Munoz Aguilera. “An average 5 mmHg blood pressure rise would be linked to a 25% increased risk of death from heart attack or stroke.”
Hypertension, which affects 30% to 45% of adults and is the leading global cause of premature death, is the main preventable cause of cardiovascular disease. Periodontitis affects more than 50% of the world’s population and has been associated with increased risk of heart attack and stroke.
While the study investigated gum disease as a potential risk factor for hypertension, the reverse could also be true. Further research is needed to examine whether patients with high blood pressure have a raised likelihood of gum disease, but in the meantime, it would be prudent for health care professionals to provide oral health advice to those with hypertension, according to the authors.
Learn more about this study in Cardiovascular Research (2019); doi.org/10.1093/cvr/cvz201.
D E C . 2 0 1 9 I M P R E S S I O N S
research has shown that ultrasound can reliably evaluate soft tissues, bone surfaces and dental implants without ionizing radiation, according to the authors.
Researchers placed four dental implants in eight porcine bone samples. Each implant was scanned by a high-frequency ultrasound scanner (a prototype developed at RWTH Aachen University), a CBCT unit (Sirona Galileos, Dentsply
Sirona) and an extraoral optical scanner (D250, 3Shape) for comparison.
“Ultrasound showed a higher accuracy in comparison with CBCT, while its measurement error was closer to the optical scan values to a small degree,” the authors concluded.
Learn more about this study in the Journal of Clinical Medicine (2019); doi.org/10.3390/jcm8101539.
Ultrasound Tops CBCT in Peri-implant Bone Imaging
Cone beam CT (CBCT) is considered the gold standard for imaging peri-implant bone, but researchers from RWTH Aachen University Medical School in Aachen, Germany, wondered if another modality without the radiation dose might be more accurate. They tested CBCT against high-frequency ultrasound and reported a surprising conclusion.
Ultrasound had a lower mean measurement error compared with CBCT, while both modalities had the same maximum error, leading the researchers to conclude that high-frequency ultrasound may be useful clinically, according to the study published in the Journal of Clinical Medicine.
“Within the simulated limited conditions of this study, high-frequency ultrasound, with optical scanning used as a reference, presented higher accuracy in comparison to CBCT, and seems to be a promising tool for measuring peri-implant bone,” wrote the authors, led by Juliana Marotti, DDS, MSc, PhD.
CBCT is the gold standard for imaging peri-implant bone because it can provide cross-sectional images. However, any artifacts seen on images may jeopardize the viewing of the bone-implant interface and make it challenging to assess peri-implant bone. Researchers also noted that CBCT is not recommended for evaluating asymptomatic implants in periodic exams to avoid patient exposure to high levels of radiation.
Because of these limitations, researchers wanted to see if high-frequency ultrasound could measure bone thickness in the buccolingual region of dental implants with the same accuracy as CBCT. Previous
C DA J O U R N A L , V O L 4 7 , Nº 1 2
DECEMBER 2 0 1 9 767
Researchers in Japan have developed a removable dental appliance that can reduce vocal and motor tics in children and adults who have Tourette syndrome, according to a study published in Movement Disorders. The ability to ameliorate tics could positively impact
the everyday lives of individuals with Tourette syndrome, a neurological disorder characterized by vocal and motor tics.
While there is no cure for Tourette syndrome, several options are available to treat severe tics. These options include behavioral, pharmacological and more
intrusive surgical interventions. However, the efficacy of these treatments can vary, and patients still frequently suffer from physical, mental and social disabilities.
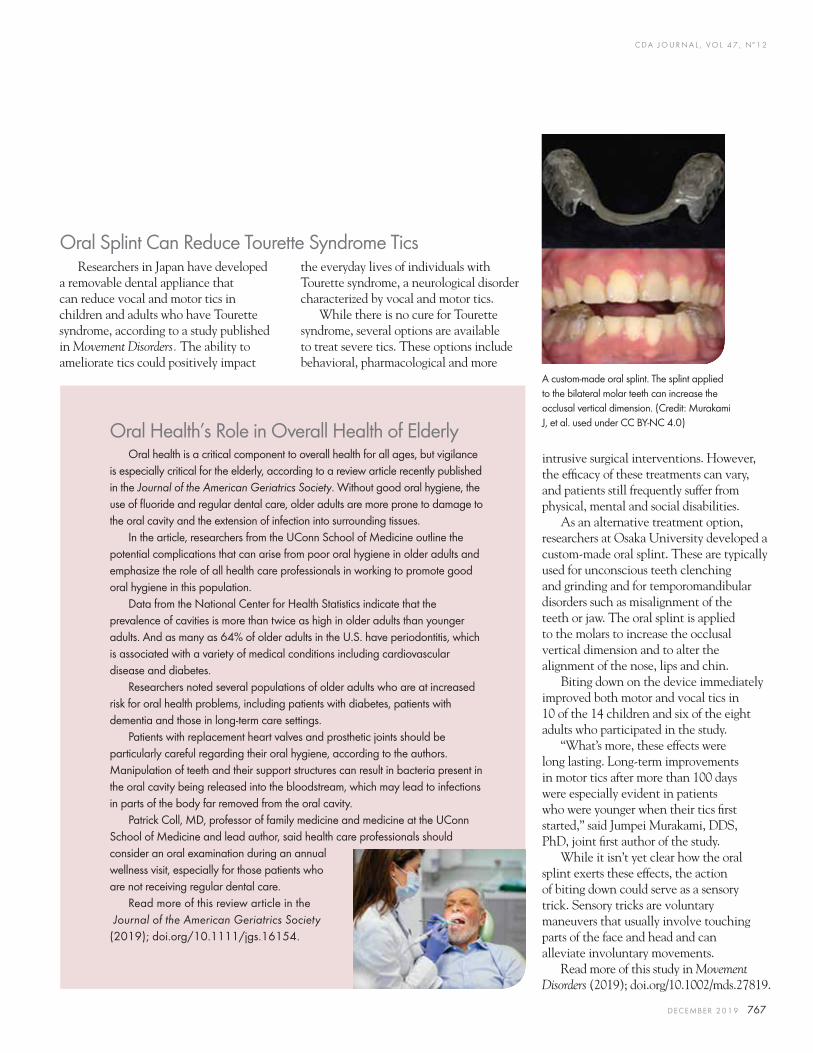
As an alternative treatment option, researchers at Osaka University developed a custom-made oral splint. These are typically used for unconscious teeth clenching and grinding and for temporomandibular disorders such as misalignment of the teeth or jaw. The oral splint is applied to the molars to increase the occlusal vertical dimension and to alter the alignment of the nose, lips and chin.
Biting down on the device immediately improved both motor and vocal tics in 10 of the 14 children and six of the eight adults who participated in the study.
“What’s more, these effects were long lasting. Long-term improvements in motor tics after more than 100 days were especially evident in patients who were younger when their tics first started,” said Jumpei Murakami, DDS, PhD, joint first author of the study.
While it isn’t yet clear how the oral splint exerts these effects, the action of biting down could serve as a sensory trick. Sensory tricks are voluntary maneuvers that usually involve touching parts of the face and head and can alleviate involuntary movements.
Read more of this study in Movement Disorders (2019); doi.org/10.1002/mds.27819.
Oral Health’s Role in Overall Health of ElderlyOral health is a critical component to overall health for all ages, but vigilance
is especially critical for the elderly, according to a review article recently published in the Journal of the American Geriatrics Society. Without good oral hygiene, the use of fluoride and regular dental care, older adults are more prone to damage to the oral cavity and the extension of infection into surrounding tissues.
In the article, researchers from the UConn School of Medicine outline the potential complications that can arise from poor oral hygiene in older adults and emphasize the role of all health care professionals in working to promote good oral hygiene in this population.
Data from the National Center for Health Statistics indicate that the prevalence of cavities is more than twice as high in older adults than younger adults. And as many as 64% of older adults in the U.S. have periodontitis, which is associated with a variety of medical conditions including cardiovascular disease and diabetes.
Researchers noted several populations of older adults who are at increased risk for oral health problems, including patients with diabetes, patients with dementia and those in long-term care settings.
Patients with replacement heart valves and prosthetic joints should be particularly careful regarding their oral hygiene, according to the authors. Manipulation of teeth and their support structures can result in bacteria present in the oral cavity being released into the bloodstream, which may lead to infections in parts of the body far removed from the oral cavity.
Patrick Coll, MD, professor of family medicine and medicine at the UConn School of Medicine and lead author, said health care professionals should consider an oral examination during an annual wellness visit, especially for those patients who are not receiving regular dental care.
Read more of this review article in the Journal of the American Geriatrics Society (2019); doi.org/10.1111/jgs.16154.
Oral Splint Can Reduce Tourette Syndrome Tics
A custom-made oral splint. The splint applied to the bilateral molar teeth can increase the occlusal vertical dimension. (Credit: Murakami J, et al. used under CC BY-NC 4.0)

C DA J O U R N A L , V O L 4 7 , Nº 1 2
DECEMBER 2 0 1 9 769
GUEST EDITORS
Alice Goodwin, DDS, PhD, is an assistant professor at the University of California, San Francisco, School of Dentistry. She is an American Board of Orthodontics certified orthodontist and researcher investigating the molecular biology underlying craniofacial anomalies, in particular clefting of the secondary palate and disorders of the temporomandibular joint.Conflict of Interest Disclosure: None reported.
Spotlight on Dental Student ResearchAlice Goodwin, DDS, PhD, and Kyle Jones, DDS, PhD
i n t r o d u c t i o n
As dental educators, we are sometimes asked by dental students and seasoned clinicians alike why research during dental school is
important, particularly for those who wish to pursue clinical careers outside of dental academia. While it is clear to most that dental research is critical for training the next generation of basic and clinical scientists who will move the dental profession forward, we strongly believe that it also imparts many important skills that are vital for clinical practice and continued professional and personal development. We believe exposure to research teaches dental students to think critically, evaluate scientific literature, critique their own work and collaborate with mentors and colleagues, which are all essential skills in clinical practice.
The ability to think critically is key to providing individualized patient care and improving clinical outcomes. Basic and clinical research
during dental school fosters this skill by exposing students to the scientific method. Dental student researchers learn to be curious, make thoughtful and quantifiable observations and develop questions and methods to answer them. These skills have wide-ranging practical applications in clinical practice, from treatment planning to quality assurance programs, all of which are important in an increasingly competitive business environment.
Lifelong learning founded on evidence-based dentistry is vital for clinicians to provide the safest, most effective treatments for their patients. Dental student researchers learn to seek out and critically evaluate information in an ever-evolving scientific literature. Whether looking up an optimal assay to run for an experiment or investigating which dental material is best for a particular clinical scenario, the ability to critically evaluate research studies is important and directly impacts decision-making in clinical practice.
Kyle Jones, DDS, PhD, is an assistant clinical professor at the University of California, San Francisco, School of Dentistry and is a diplomate of the American Board of Oral and Maxillofacial Pathology. His research focuses on how the immune system is altered in head and neck precancerous lesions and tumors, with the goal of improving current immunotherapies for these diseases.Conflict of Interest Disclosure: None reported.

C DA J O U R N A L , V O L 4 7 , Nº 1 2
770 D E C E M B E R 2 01 9
i n t r o d u c t i o n
Furthermore, research teaches students to critically evaluate their own work and to not give up when times are difficult. These important traits are directly applicable to clinical training and practice, especially when learning to master new clinical skills. Providers should continually strive for improvement through self-reflection and evaluation of their own work and business practices, which can improve the quality and efficiency of care provided to patients.
Finally, research teaches students the need to create strong collaborative working relationships.
Science is truly a team pursuit and often requires expertise from multiple people in order to answer challenging scientific questions. Similarly, dentists can utilize this spirit of collaboration in their own practices, whether consulting with a group of specialists on a complicated case or developing a strong and cohesive office team. For these and many other reasons, we feel strongly that research opportunities during dental school provide myriad learning experiences to dental students that are directly applicable to their futures in clinical practice and patient care.
We appreciate that research is not an undertaking for the faint of heart; it is often fraught with challenges, failures and frustrations. Therefore, we would like to acknowledge the hard work and determination of the dental student researchers who took on complex scientific questions and pursued challenging projects, which resulted in these peer-reviewed manuscripts. Additionally, we would like to thank the mentors of these students, because mentorship and guidance is essential at every step in one’s training, especially as a burgeoning scientist.
In this issue, we are excited to present scientific articles on a wide range of dental-related topics from students and mentors at multiple dental schools. We believe that the breadth of topics highlighted in this issue reflects the immense variety of topics in the broader field of dental research. Thank you again to all of the dental student researchers, mentors and their collaborators for the hard work that went into preparing these articles. We hope our readers enjoy this issue as much as we have. n
C DA J O U R N A L , V O L 4 7 , Nº 1 2
DECEMBER 2 0 1 9 771
v e n e e r r e s t o r a t i o n s
AUTHORS
Michelle Yang, BS, is a dental student at the University of California, Los Angeles, School of Dentistry.Conflict of Interest Disclosure: None reported.
Erik Balinghassay, BS, is a dental student at the University of California, Los Angeles, School of Dentistry.Conflict of Interest Disclosure: None reported.
Johnny Huynh, BS, is a dental student at the University of California, Los Angeles, School of Dentistry.Conflict of Interest Disclosure: None reported.
Minimally Invasive Veneer Restorations: Effect of Restorative Material on Traumatic Impact StrengthMichelle Yang, BS; Erik Balinghassay, BS; Johnny Huynh, BS; Xuehui Liu, DDS; Chunling Ge, DDS, PhD; and Shane Newport White, BDentSc, MS, MA, PhD
a b s t r ac t Traumatic tooth fracture is extremely common in adolescent patients and restorations need to be long-lasting, aesthetic and resistant to repeated trauma. Direct resin-composite restorations have generally been used, but minimally invasive veneers (MIV) now are a conservative and stable alternative. MIVs made of two different ceramic materials were compared to intact teeth and to resin-composite controls. Modern restorative materials and adhesive techniques were capable of restoring traumatized teeth to the impact strength of natural intact teeth.
Traumatic dental injury is one of the world’s most prevalent conditions.1–5 Traumatic tooth fracture is extremely common; incidence peaks at 4% at 12
years of age, dropping off slowly over the decades (FIGURE 1).2,6–8 Because fracture of anterior teeth is frequent in adolescent patients, restorations need to be particularly long-lasting and durable. Maxillary incisors are the most affected teeth because of their position and proclination. Traumatic fracture often affects enamel and dentin without disrupting the pulp and necessitating root canal treatment. Prior research on traumatic tooth fracture has generally focused on restorative approaches to crowned and posted teeth.9–15 Little attention has been given to refracture of restored teeth or to initial fracture of previously restored teeth.16–19 Patients generally retain the same anatomic,
behavioral and motor coordination risk factors to trauma; hence, repeated trauma is common throughout childhood, adolescence and beyond.5 For this reason, teeth and dental restorations placed to treat primary trauma are often subjected to additional trauma.5,18 Additionally, restorations placed to address carious lesions or aesthetic issues may later be subjected to trauma.
In the past, small to moderate defects on anterior teeth were almost exclusively treated using resin-composite materials, but resin composite is subject to wear, loss of detailed surface texture and discoloration over time. Large defects were generally treated using more stable ceramic materials in the form of full-facial veneers or full crowns. Recently, minimally invasive veneers, partial ceramic veneers or ultraconservative veneers have been used to restore a variety of anterior tooth defects
Xuehui Liu, DDS, is a visiting scholar at the University of California, Los Angeles, School of Dentistry and an assistant professor at the Peking University School of Stomatology, Third Dental Center.Conflict of Interest Disclosure: None reported.
Chunling Ge, DDS, PhD, is a visiting scholar at the University of California, Los Angeles, School of Dentistry and an associate professor at the Peking University School of Stomatology.Conflict of Interest Disclosure: None reported.
Shane Newport White, BDentSc, MS, MA, PhD, is a professor at the University of California, Los Angeles, School of Dentistry.Conflict of Interest Disclosure: None reported.
C DA J O U R N A L , V O L 4 7 , Nº 1 2
772 D E C E M B E R 2 01 9
v e n e e r r e s t o r a t i o n s
(F IGURE 1).20,21 Ceramic materials are inherently brittle, but no more brittle than human tooth enamel.22,23 Feldspathic porcelain has long been used for the fabrication of porcelain veneers because it is widely available, simple to use and allows layering and internal characterization for optimal aesthetics. More recently, monolithic glass ceramics have become widely used; these materials are stronger than porcelain or tooth enamel, but generally cannot be internally characterized.
Traumatic injury, such as falling off a bicycle or skateboard and hitting a tooth on a sidewalk, entails much higher forces, stresses and loading rates than chewing. So, the investigation of traumatic tooth fracture necessitates duplication of extreme conditions, quite different from the routine testing of restored teeth when simulating normal masticatory function. Impact testing of incisor teeth has only rarely been reported.9,12,14,15,24
We modeled individuals with a history of maxillary incisor trauma and a proclivity to repeated trauma, evaluating minimally invasive ceramic restorations through impact testing. We hypothesized that teeth restored using minimally invasive ceramic restorations would have equal impact strength compared to intact unrestored teeth and to teeth restored using a conventional direct resin-composite material.
MethodsSixty-four intact maxillary incisors
that had been kept wet since extraction were given simulated traumatic defects (FIGURE 2a). A high-speed diamond bur (TR-13, MANI, Utsunomiya, Japan) with copious water spray was used to make standardized Class IV preparations with a 60-degree facial bevel of 2 mm to 3 mm in length (TR-13, MANI) and a 45-degree lingual bevel of 1 mm in length (TR-13EF,
MANI) (fiGure 1B tooth No. 8 and fiGure 2a). Sixteen teeth were arbitrarily assigned to each of the four groups: intact control, direct resin-composite control, minimally invasive feldspathic porcelain veneer and minimally invasive glass-ceramic veneer. A power analysis based on pilot specimens suggested that 11 specimens per group would be sufficient to detect clinically meaningful differences among restoration materials. Restorations were made using direct resin-composite (Filtek Z350, 3M ESPE, St. Paul, Minn.), feldspathic porcelain (VMK Master, VITA, Bad Säckingen, Germany) or glass ceramic (IPS e.max, Ivoclar Vivadent, Schaan, Liechtenstein). An adhesive cement system bonding agent (Adper Single Bond Plus, 3M ESPE, St. Paul, Minn.) was used for the direct restorations, and the indirect restorations were adhesively cemented (Variolink N with Syntac and Heliobond, Ivoclar Vivadent). The restored teeth were stored in water for one month then artificially aged by thermal cycling from 5 degrees to 55 degrees Celsius for 1,500 cycles with 30-second dwell times.
A model for incisal trauma illustrated by Andreasen and Andreasen was followed.25 Teeth were mounted in acrylic resin to simulate bone support at an angle of 135 degrees ± 5 degrees to the horizontal. This angle was chosen so as to produce incisal fracture,25–27 whereas, prior impact studies had generally used an angle of 90 degrees to produce cervical or root fracture.9,12 An artificial periodontal ligament was not included because it would not have provided substantial dampening at the high-impact speed used.19,28
An impact tester, previously described by Trabert et al., was used to apply a hammer to the teeth 1 mm ± 0.2 mm below the incisal edge (fiGure 2c).9,18 The pendulum hammer, 800 g in weight, was lifted to an elevation of 64 degrees on a pivot point radius of 0.49 m. Acceleration due to gravity (9.81 m/sec−2) would provide the hammer with a certain amount of kinetic energy at the bottom of the swing. By securing the tooth specimen at the bottom, the pendulum would strike
FIGURE 1A .
FIGURE 1C .
FIGURE 1B .
FIGURE 1D.
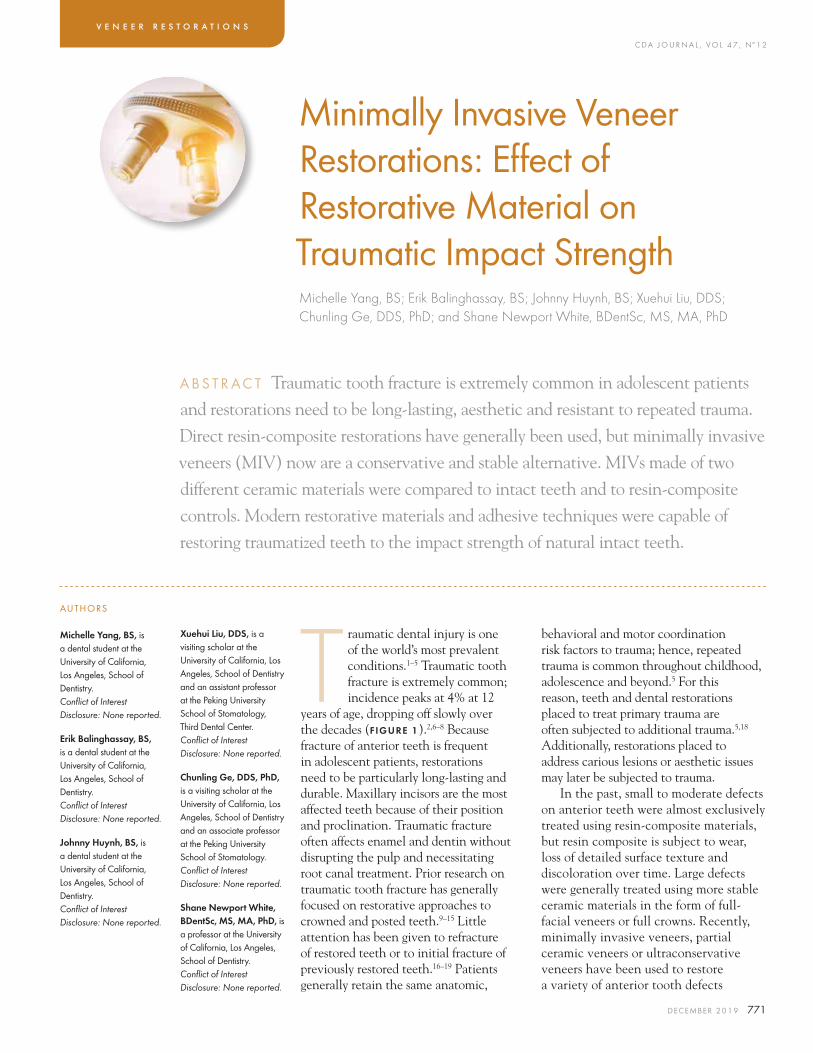
FIGURES 1. Impact trauma to the permanent incisors. Twelve-year-old boy has fallen on the asphalt playground (a). Two fractured central incisors with preparations for minimally invasive veneers; tooth No. 8 was used as a model for this study (B). Feldspathic porcelain veneers (c). Cemented minimally invasive veneers (d).
C DA J O U R N A L , V O L 4 7 , Nº 1 2
DECEMBER 2 0 1 9 773
and break the specimen’s incisal aspect. The pendulum would continue to swing onward and upward after the impact to an elevation somewhat lower than that of a free swing. Impact strengths in kJ/m−2 were determined by how much kinetic energy the hammer lost during impact as assessed by the difference in energy between the pendulum’s initial release angle and its maximum terminal angle divided by the area of the fracture.28 The energy absorbed at fracture is a reflection of the relative strength of the whole system enduring an impact force.14 This approach was verified in pilot testing to produce incisal fracture rather than cervical or root fracture (fiGure 2d). A priori, data from specimens with only minor injuries < 3.0 mm2 were to be censored because the traumatic injuries would be too small, just chips rather than fractures, to be considered clinically relevant to the aim of this study.9
Mean group impact strengths and their standard errors were calculated. All four groups were compared for impact strength using one-way analysis
of variance (ANOVA) (α < 0.05). The specimens were qualitatively evaluated for fracture patterns, whether the line of fracture involved tooth structure, restoration or both.
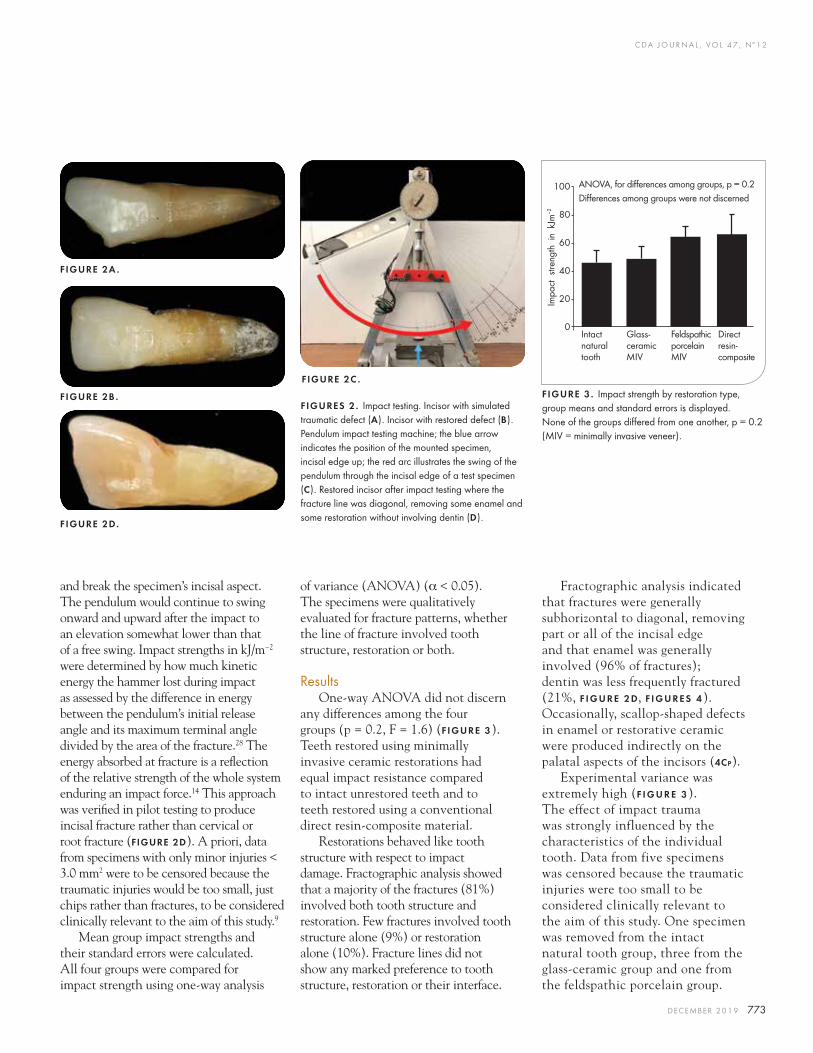
ResultsOne-way ANOVA did not discern
any differences among the four groups (p = 0.2, F = 1.6) (F IGURE 3). Teeth restored using minimally invasive ceramic restorations had equal impact resistance compared to intact unrestored teeth and to teeth restored using a conventional direct resin-composite material.
Restorations behaved like tooth structure with respect to impact damage. Fractographic analysis showed that a majority of the fractures (81%) involved both tooth structure and restoration. Few fractures involved tooth structure alone (9%) or restoration alone (10%). Fracture lines did not show any marked preference to tooth structure, restoration or their interface.
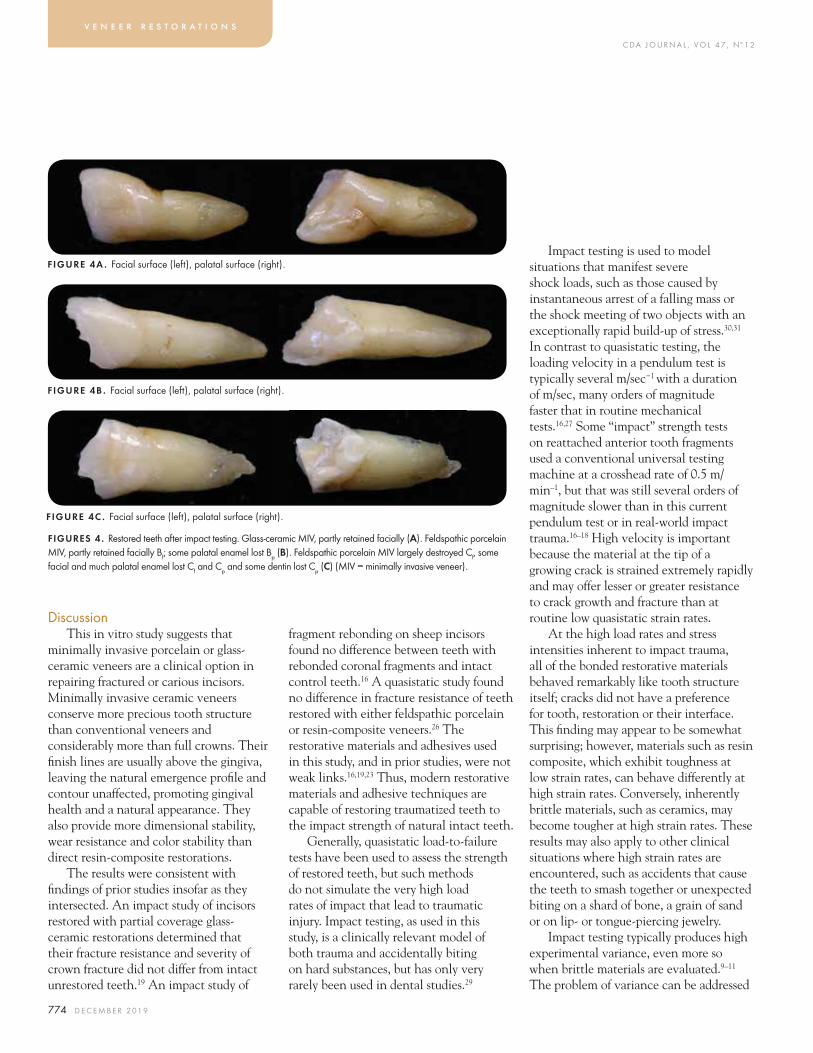
Fractographic analysis indicated that fractures were generally subhorizontal to diagonal, removing part or all of the incisal edge and that enamel was generally involved (96% of fractures); dentin was less frequently fractured (21%, F I G U R E 2 d, f i G u r e s 4). Occasionally, scallop-shaped defects in enamel or restorative ceramic were produced indirectly on the palatal aspects of the incisors (4cp).
Experimental variance was extremely high (f i G u r e 3). The effect of impact trauma was strongly influenced by the characteristics of the individual tooth. Data from five specimens was censored because the traumatic injuries were too small to be considered clinically relevant to the aim of this study. One specimen was removed from the intact natural tooth group, three from the glass-ceramic group and one from the feldspathic porcelain group.
FIGURE 2A .
FIGURE 2B .
FIGURE 2D.
FIGURE 2C .
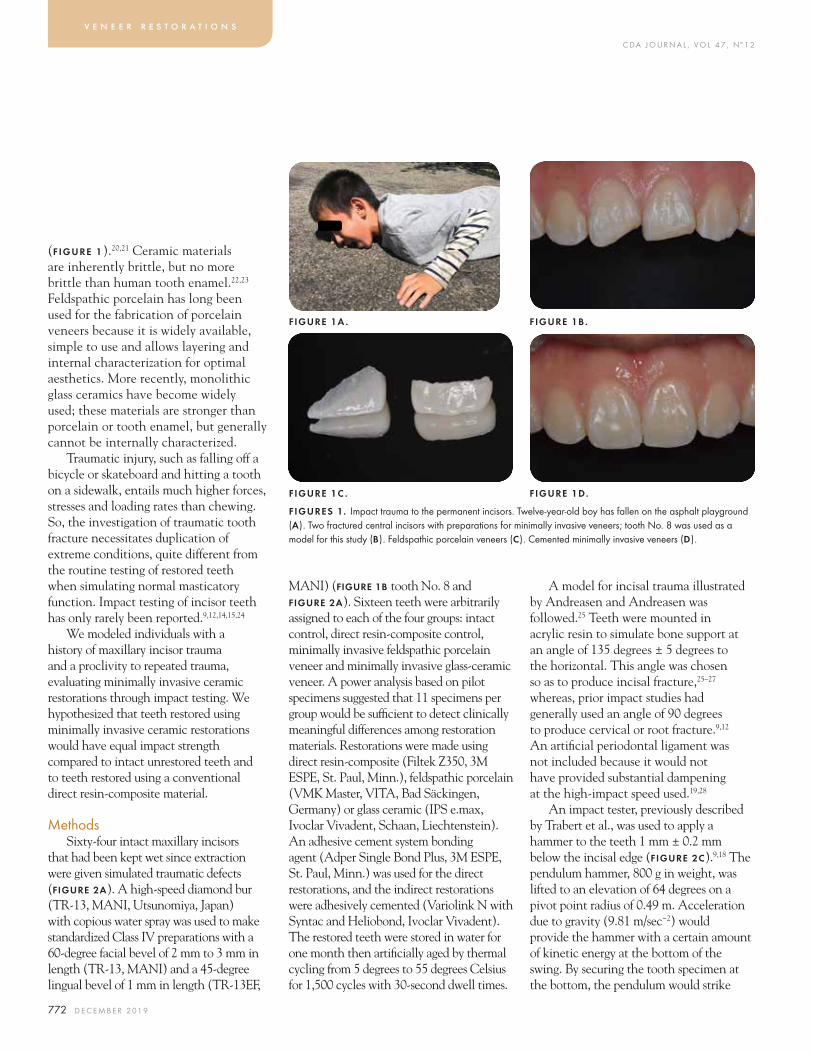
FIGURES 2. Impact testing. Incisor with simulated traumatic defect (a). Incisor with restored defect (B). Pendulum impact testing machine; the blue arrow indicates the position of the mounted specimen, incisal edge up; the red arc illustrates the swing of the pendulum through the incisal edge of a test specimen (c). Restored incisor after impact testing where the fracture line was diagonal, removing some enamel and some restoration without involving dentin (d).
100
80
60
40
20
0Intactnaturaltooth
Glass-ceramicMIV
FeldspathicporcelainMIV
Directresin-composite
FIGURE 3 . Impact strength by restoration type, group means and standard errors is displayed. None of the groups differed from one another, p = 0.2 (MIV = minimally invasive veneer).
Impa
ct s
treng
th i
n k
Jm–2
ANOVA, for differences among groups, p = 0.2Differences among groups were not discerned
C DA J O U R N A L , V O L 4 7 , Nº 1 2
774 D E C E M B E R 2 01 9
v e n e e r r e s t o r a t i o n s
DiscussionThis in vitro study suggests that
minimally invasive porcelain or glass-ceramic veneers are a clinical option in repairing fractured or carious incisors. Minimally invasive ceramic veneers conserve more precious tooth structure than conventional veneers and considerably more than full crowns. Their finish lines are usually above the gingiva, leaving the natural emergence profile and contour unaffected, promoting gingival health and a natural appearance. They also provide more dimensional stability, wear resistance and color stability than direct resin-composite restorations.
The results were consistent with findings of prior studies insofar as they intersected. An impact study of incisors restored with partial coverage glass-ceramic restorations determined that their fracture resistance and severity of crown fracture did not differ from intact unrestored teeth.19 An impact study of
FIGURES 4 . Restored teeth after impact testing. Glass-ceramic MIV, partly retained facially (A). Feldspathic porcelain MIV, partly retained facially Bf; some palatal enamel lost Bp (B). Feldspathic porcelain MIV largely destroyed Cf, some facial and much palatal enamel lost Cf and Cp and some dentin lost Cp (C) (MIV = minimally invasive veneer).
fragment rebonding on sheep incisors found no difference between teeth with rebonded coronal fragments and intact control teeth.16 A quasistatic study found no difference in fracture resistance of teeth restored with either feldspathic porcelain or resin-composite veneers.26 The restorative materials and adhesives used in this study, and in prior studies, were not weak links.16,19,23 Thus, modern restorative materials and adhesive techniques are capable of restoring traumatized teeth to the impact strength of natural intact teeth.
Generally, quasistatic load-to-failure tests have been used to assess the strength of restored teeth, but such methods do not simulate the very high load rates of impact that lead to traumatic injury. Impact testing, as used in this study, is a clinically relevant model of both trauma and accidentally biting on hard substances, but has only very rarely been used in dental studies.29
Impact testing is used to model situations that manifest severe shock loads, such as those caused by instantaneous arrest of a falling mass or the shock meeting of two objects with an exceptionally rapid build-up of stress.30,31 In contrast to quasistatic testing, the loading velocity in a pendulum test is typically several m/sec−1 with a duration of m/sec, many orders of magnitude faster that in routine mechanical tests.16,27 Some “impact” strength tests on reattached anterior tooth fragments used a conventional universal testing machine at a crosshead rate of 0.5 m/min–1, but that was still several orders of magnitude slower than in this current pendulum test or in real-world impact trauma.16–18 High velocity is important because the material at the tip of a growing crack is strained extremely rapidly and may offer lesser or greater resistance to crack growth and fracture than at routine low quasistatic strain rates.
At the high load rates and stress intensities inherent to impact trauma, all of the bonded restorative materials behaved remarkably like tooth structure itself; cracks did not have a preference for tooth, restoration or their interface. This finding may appear to be somewhat surprising; however, materials such as resin composite, which exhibit toughness at low strain rates, can behave differently at high strain rates. Conversely, inherently brittle materials, such as ceramics, may become tougher at high strain rates. These results may also apply to other clinical situations where high strain rates are encountered, such as accidents that cause the teeth to smash together or unexpected biting on a shard of bone, a grain of sand or on lip- or tongue-piercing jewelry.
Impact testing typically produces high experimental variance, even more so when brittle materials are evaluated.9–11 The problem of variance can be addressed
FIGURE 4C . Facial surface (left), palatal surface (right).
FIGURE 4A . Facial surface (left), palatal surface (right).
FIGURE 4B . Facial surface (left), palatal surface (right).

C DA J O U R N A L , V O L 4 7 , Nº 1 2
DECEMBER 2 0 1 9 775
by placing sharp notches in uniform test specimens to localize and standardize stresses when characterizing bulk material properties.29 However, natural and artificial crowns come in a wide variety of anatomic shapes and do not naturally contain notches; moreover, the presence of a notch substantially alters the measured impact strength. Hence, high variance was inherent to our test method, which simulated real-world incisal trauma. The considerable variability in within-group impact strength (fiGure 3) is typical of tooth impact studies; twentyfold to fiftyfold ranges of impact strengths within test groups have been reported.9,11,12,14,15,18,19,24 One study censored, or excluded, approximately 42% of its test specimens because those impacts did not produce the type of fracture being modeled.9 In this current study, 8% of the test specimens were censored because only minor chipping was produced. All other impact studies have been silent on the issue of data censoring even when disparate fracturing was reported.11,14,15,18 Clinical impact trauma produces considerable variability in fracture location and course.5
ConclusionsTeeth restored using minimally
invasive ceramic restorations had equal impact resistance compared to intact virgin teeth and to teeth restored using a conventional direct resin-composite material. Fracture lines did not show any marked preference to tooth structure, restoration or their interface; restorations behaved like tooth structure with respect to impact damage. Impact fracture was highly variable with respect to impact strength and damage produced. Modern restorative materials and adhesive techniques are capable of restoring traumatized teeth to the impact strength of natural intact teeth. n
references
1. Andersson L. Epidemiology of traumatic dental injuries. Pediatr Dent 2013 Mar–Apr;35(2):102–5.2. Lam R. Epidemiology and outcomes of traumatic dental injuries: A review of the literature. Aust Dent J 2016 Mar;61 Suppl 1:4–20. doi: 10.1111/adj.12395.3. Petti S, Andreasen JO, Glendor U, Andersson L. The fifth most prevalent disease is being neglected by public health organisations. Lancet Glob Health 2018 Oct;6:e1070–e1071. doi: doi.org/10.1016/S2214-109X(18)30380-2.4. Petti S, Glendor U, Andersson L. World traumatic dental injury prevalence and incidence, a meta-analysis — 1 billion living people have had traumatic dental injuries. Dent Traumatol 2018 Apr;34(2):71–86. doi: 10.1111/edt.12389.5. Andersson L, Petti S, Day P, Kenny K, Glendor U, Andreasen JO. Classification, Epidemiology and Etiology. In: Andreasen JO, Andreasen FM, Lars Andersson L, eds. Textbook and Color Atlas of Traumatic Injuries to the Teeth. 5th ed. Hoboken, N.J.: Wiley-Blackwell; 2018:252–94.6. Andreasen JO. Etiology and pathogenesis of traumatic dental injuries. A clinical study of 1,298 cases. Scand J Dent Res 1970 ;78(4):329–42.7. Andreasen JO, Ravn JJ. Epidemiology of traumatic dental injuries to primary and permanent teeth in a Danish population sample. Int J Oral Surg 1972;1(5):235–9. 8. Azami-Aghdash S, Ebadifard Azar F, Pournaghi Azar F, Rezapour A, Moradi-Joo M, Moosavi A, Ghertasi Oskouei S. Prevalence, etiology, and types of dental trauma in children and adolescents: Systematic review and meta-analysis. Med J Islam Repub Iran 2015 Jul 10;29(4):234. eCollection 2015.9. Trabert KC, Caputo AA, Abou Rass M. Tooth Fracture — A Comparison of Endodontic and Restorative Treatments. J Endod 1978 Nov;4(11):341–5.10. Salis SG, Hood JA, Stokes AN, Kirk EE. Patterns of indirect fracture in intact and restored human premolar teeth. Endod Dent Traumatol 1987 Feb;3(1):10–14.11. Salis SG, Hood JA, Kirk EE, Stokes AN. 1987. Impact-fracture energy of human premolar teeth. J Prosthet Dent 1987 Jul;58(1):43–8.12. McDonald AV, King PA, Setchell DJ. In vitro study to compare impact fracture resistance of intact root-treated teeth. Int Endod J 1990 Nov;23(6):304–12.13. Smith RL, Hood JA, Stokes AN. Influence of cavosurface configuration and composite resin type on impact fracture resistance of Class IV restorations. N Z Dent J 1990 Jul;86(385):58–61.14. Stokes AN, Hood JA. Impact fracture characteristics of intact and crowned human central incisors. J Oral Rehabil 1993 Jan;20(1):89–95.15. Cathro PR, Chandler NP, Hood JA. Impact resistance of crowned endodontically treated central incisors with internal composite cores. Endod Dent Traumatol 1996 Jun;12(3):124–8.16. Farik B, Munksgaard EC, Andreasen JO. Impact strength of teeth restored by fragment-bonding. Endod Dent Traumatol 2000 Aug;16(4):151–3.17. Farik B, Munksgaard EC, Andreasen JO, Kreiborg S. Fractured teeth bonded with dentin adhesives with and without unfilled resin. Dent Traumatol 2002 Apr;18(2):66–9.18. Bruschi Alonso RC, Alonso RC, Correr GM, Alves MC, Lewgoy HR, Sinhoreti MA, Puppin Rontani RM, Correr Sobrinho L. Reattachment of anterior fractured teeth: Effect
of materials and techniques on impact strength. Dental Traumatol 2010 Aug;26(4):315–22. doi: 10.1111/j.1600-9657.2010.00906.x.19. Vilaplana-Vivo J, Vilaplana-Vivo C, Miguel-Sánchez A, García-Ballesta C, Camacho-Alonso F. In vitro fracture resistance of mandibular incisors restored with modified partial-coverage ceramic restorations. Dent Traumatol 2014 Oct;30(5):356–61. doi: 10.1111/edt.12094. Epub 2014 Feb 6.20. Ge C, Green CC, Sederstrom D, McLaren EA, White SN. Effect of porcelain and enamel thickness on porcelain veneer failure loads in vitro. J Prosthet Dent 2014 May;111(5):380–7. doi: 10.1016/j.prosdent.2013.09.025. Epub 2014 Jan 14.21. Ge C, Green CC, Sederstrom DA, McLaren EA, Chalfant JA, White SN. Effect of tooth substrate and porcelain thickness on porcelain veneer failure loads in vitro. J Prosthet Dent 2018 Jul;120(1):85–91. doi: 10.1016/j.prosdent.2017.10.018. Epub 2017 Dec 19.22. White SN, Luo W, Paine ML, Fong H, Sarikaya M, Snead ML. Biological organization of hydroxyapatite crystallites into a fibrous continuum toughens and controls anisotropy in human enamel. J Dent Res 2001 Jan;80(1):321–6.23. Silva LHD, Lima E, Miranda RBP, Favero SS, Lohbauer U, Cesar PF. Dental ceramics: A review of new materials and processing methods. Braz Oral Res 2017 Aug 28;31(suppl 1):e58. doi: 10.1590/1807-3107BOR-2017.vol31.0058.24. Stokes AN, Hood JA. 1988. Impact fracture patterns of intact and restored human maxillary central incisors. Int J Prosthod 1988 1:208–10.25. Andreassen FM, Andreasen JO. Crown Fractures. In: Andreasen JO, Andreasen FM, Andersson L, eds. Textbook and Color Atlas of Traumatic Injuries to the Teeth. 4th ed. Hoboken, N.J.: Wiley-Blackwell; 2007:280–313.26. Batalocco G, Lee H, Ercoli C, Feng C, Malmstrom H. Fracture resistance of composite resin restorations and porcelain veneers in relation to residual tooth structure in fractured incisors. Dent Traumatol 2012 Feb;28(1):75–80. doi: 10.1111/j.1600-9657.2011.01037.x. Epub 2011 Jul 14.27. Jayasudha K1, Hemanth M, Baswa R, Raghuveer HP, Vedavathi B, Hegde C. Traumatic impact loading on human maxillary incisor: A dynamic finite element analysis. J Indian Soc Pedod Prev Dent 2015 Oct–Dec;33(4):302–6. doi: 10.4103/0970-4388.165680.28. Huang HM, Tsai CY, Lee HF, Lin CT, Yao WC, Chiu WT, Lee SY. Damping effects on the response of maxillary incisor subjected to a traumatic impact force: A nonlinear finite element analysis. J Dent 2006 Apr;34(4):261–8. Epub 2005 Sep 19.29. Charpy MG. Note sur l’essai des métaux à la flexion par choc de barreaux entaillés. Mémoires et Comptes rendus de la Société des Ingénieurs Civils de France. 1901 Jun;848–847.30. Farik B, Munksgaard EC. Fracture strength of intact and fragment-bonded teeth at various velocities of the applied force. Eur J Oral Sci 1999 Feb;107(1):70–3.31. Liaw PK. Impact Toughness Testing and Fracture Mechanics. In: Kuhn H, Medlin D, eds. ASM Handbook Volume 8: Mechanical Testing and Evaluation. Materials Park, Ohio: ASM International; 2000:561–678. doi.org/10.31399/asm.hb.v08.9781627081764.
the correspondinG author, Shane Newport White, BDentSc, MS, MA, PhD, can be reached at [email protected].
Exceptional protection from people who understand your profession. With a heritage of nearly 40 years, TDIC now delivers dentist-focused protection to more than 24,000 dentists in 15 states. Our success is due in no small part to the collective strength of our company, the trust of our policyholders and the focus of our board of directors.
It’s our privilege to serve a growing community of dentists who are engaged in the bright future of their profession.
unparalleled
Protecting dentists. It’s all we do.®
800.733.0633 | tdicinsurance.com | Insurance Lic. #0652783
@TDICinsurance
C DA J O U R N A L , V O L 4 7 , Nº 1 2
DECEMBER 2 0 1 9 777
AUTHORS
Christina Chi, BA, DDS, is a recent graduate of the Loma Linda University School of Dentistry. Conflict of Interest Disclosure: None reported.
Brittney N. Springer, BS, is a Master of Science student in the department of earth and biological sciences at Loma Linda University.Conflict of Interest Disclosure: None reported.
Elvin Walemba, BSc, MRes, PhDc, is a PhD candidate in the department of earth and biological sciences at Loma Linda University.Conflict of Interest Disclosure: None reported.
Titanium-Oxide Nanoparticles and Nanofibers Used Alone or With UV Light ActivationChristina Chi, BA, DDS; Brittney N. Springer, BS; Elvin Walemba, BSc, MRes, PhDc; Kevin E. Nick, PhD; Christopher C. Perry, PhD; and So Ran Kwon, DDS, MS, PhD, MS
a b s t r ac t Advances in nanotechnology are making a significant impact on dentistry. This study evaluated the change in oxidation potential of synthesized TiO2 nanofibers (NFs) compared to commercial TiO2 nanoparticles (NPs). TiO2 NFs had higher oxidation potential compared to TiO2 NPs when activated with ultraviolet (UV) light using a yellow tartrazine dye. Therefore, it is expected that replacement of TiO2 NPs to NFs as a photocatalyst in bleaching systems could enhance the efficacy and speed of the bleaching process.
Kevin E. Nick, PhD, is a professor in the department of earth and biological sciences at Loma Linda University.Conflict of Interest Disclosure: None reported.
Christopher C. Perry, PhD, is an assistant professor in the division of biochemistry at the Loma Linda University School of Medicine.Conflict of Interest Disclosure: None reported.
So Ran Kwon, DDS, MS, PhD, MS, is a professor and director of the student research program at the Loma Linda University School of Dentistry.Conflict of Interest Disclosure: None reported.
Advances in nanotechnology are making a significant impact on dentistry.1–3 It is now possible to have precise control over
the composition and morphology of nanomaterials, enabling the production of multifunctional devices with unique properties.4 Thus, novel features of nanotechnology have enabled a shift from the mechanistic restoration of tooth repair to an emphasis on diagnosis and disease prevention, revolutionizing the era of dentistry. Such innovations include diagnostic aids, treatment devices and therapeutic delivery systems. Innovative diagnostic tools have been developed to label specific caries-causing bacteria by immunofluorescence with nanotechnology using quantum dots and salivary markers to detect antibodies for autoimmune disorders.5
b l e a c h i n g s y s t e m s
Dental disease prevention systems, such as dentifrices and mouthwashes, incorporate nanosized calcium carbonate or hydroxyapatite crystals similar to the structure of enamel to remineralize early carious lesions and desensitize abraded surfaces.6,7 Bone regeneration can be accomplished using biocompatible composite bone graft scaffolds and calcium sulfate nanocrystals.7–9
Metal and metal oxide semiconductor nanomaterials are emerging as a new therapeutic strategy for the treatment of bacterial infections and the prevention of biofilm formation.9 Titanium dioxide (TiO2) is among the most investigated transition metal oxides. Titanium dioxide is a natural oxide of titanium with low toxicity and negligible biological effects and is found in food products, cosmetics and pharmaceutical products.10 The

C DA J O U R N A L , V O L 4 7 , Nº 1 2
778 D E C E M B E R 2 01 9
crystalline anatase phase of TiO2 is highly active photochemically. Moreover, TiO2 nanomaterials serve as ideal carriers and also exert enhanced photo-induced oxidation potentials from doping of other metals such as silver or gold.11,12 TiO2 nanomaterials are promising in the following applications: photocatalysis,13 solar cells,14 water purification15 and antimicrobial coatings.10,16,17 In dentistry, the photoctalytic property of TiO2 has been used in in-office bleaching materials to lower the hydrogen peroxide concentration without compromising bleaching efficacy. It is expected that the photosensitive TiO2 absorbs the energy from light activation units and speeds up the oxidation reaction of hydrogen peroxide, consequently enhancing the effectiveness and speed of the bleaching process.18
The two most investigated TiO2 morphologies are zero-dimensional (nanoparticles) and one-dimensional solids (nanofibers, nanotubes). One-dimensional nanostructures are good candidates for optimized titania because of their enhanced surface areas and porosities compared with commercially available TiO2 nanoparticles (NPs). Nanofibers (NFs) are made via hydrothermal, template-mediated, anodization and electrospinning approaches.14 Specifically, hydrothermally synthesized titania NFs are responsive to scale-up, have inherent low toxicity and are stable to moisture. We showed previously that hydrothermally synthesized TiO2 NFs result in approximately threefold higher adsorption to organophosphorus compounds, which comprise a class of environmental pollutants.19 This increase is attributed to morphological roughness, greater crystallographic nanoscale variation and active site competition between parent and daughter species.
We expected that hydrothermally synthesized TiO2 NFs would also have higher oxidation potential compared to TiO2 NPs because morphologically they may have more active surface oxidation sites.19 Therefore, the purpose of this study was to explore dental photobleaching applications of TiO2 NFs and evaluate its relative photocatalytic activity against anatase TiO2 NPs using a yellow tartrazine dye solution. We hypothesized that TiO2 NFs would degrade dye solutions at faster rates than the TiO2 NPs when activated with UV irradiation.
Materials and Methods
Synthesis of Titania NanofibersAnatase titanium(IV) oxide
(Sigma-Aldrich, St. Louis) anatase NPs (crystallite size ≈ 25 nm; surface area 45–55 m2 g−1) was the starting material. One gram of TiO2 anatase nanoparticle powder was suspended in 5 M NaOH (20 mL; using ultrapure water (18.2 MΩ cm−1 resistivity)) and placed in a stainless-steel enclosed Teflon autoclave (100 mL volume size) containing a Teflon-coated stir bar as previously described.18 The Teflon autoclave was ≈ 2/3 submerged in an oil bath at ~ 120–130 C (autoclave internal temperature ~ 170 C) on a magnetic hot plate with continuous stirring for approximately 48 to 72 hours. We used a base concentration range and temperature known to synthesize titanate nanofibers.21 Stirring with
a Teflon-coated stir bar is required to get fibers of several micrometers in length.22,23 Following heating, the autoclave in the oil bath was allowed to cool to room temperature over several hours. Excess base was separated by centrifugation then vacuum filtrated with acid (1 M HCl), followed by water to remove excess sodium and chloride. The washed precipitate was then oven dried at 110 C overnight (≈ 8 hours), followed by annealing at 400 C. Removal of Na and Cl from the hydrolysis product was verified by energy dispersive X-ray spectrometry (EDS) (NORAN System VI, Thermo Scientific, Waltham, Mass.) in a scanning electon microscope (SEM) (TESCAN Vega II, Brno-Kohoutovice, Czech Republic).
Characterization of Titania NanofibersPowder X-ray diffraction (XRD)
measurements were performed using a Bruker D8 Advance diffractometer irradiating Cu Kα X-rays (λ = 1.5418 Å) with an applied power of 1.5 kVA (30 kV x 50 mA). The scans were performed in continuous mode from 2 to 70 degrees (θ−2θ geometry). TiO2 products were characterized by digital transmission electron microscopy (TEM) (Philips Tecnai 12; 120 kV). Samples were prepared for TEM measurements by dropping 5 to 10 mL of a dilute nanofiber suspension onto a Formvar/carbon-coated Cu grid (Ted Pella 200 mesh) and allowing the samples to air dry.
b l e a c h i n g s y s t e m s
A B C D
FIGURE 1. Flowchart of experimental protocol. Tartrazine solutions with reagents are stirred in vials (a). Solution is transferred to microtubes and centrifuged (B). Supernatant is plated on a 96-well plate (c). Optical density is read with a microplate reader (d).
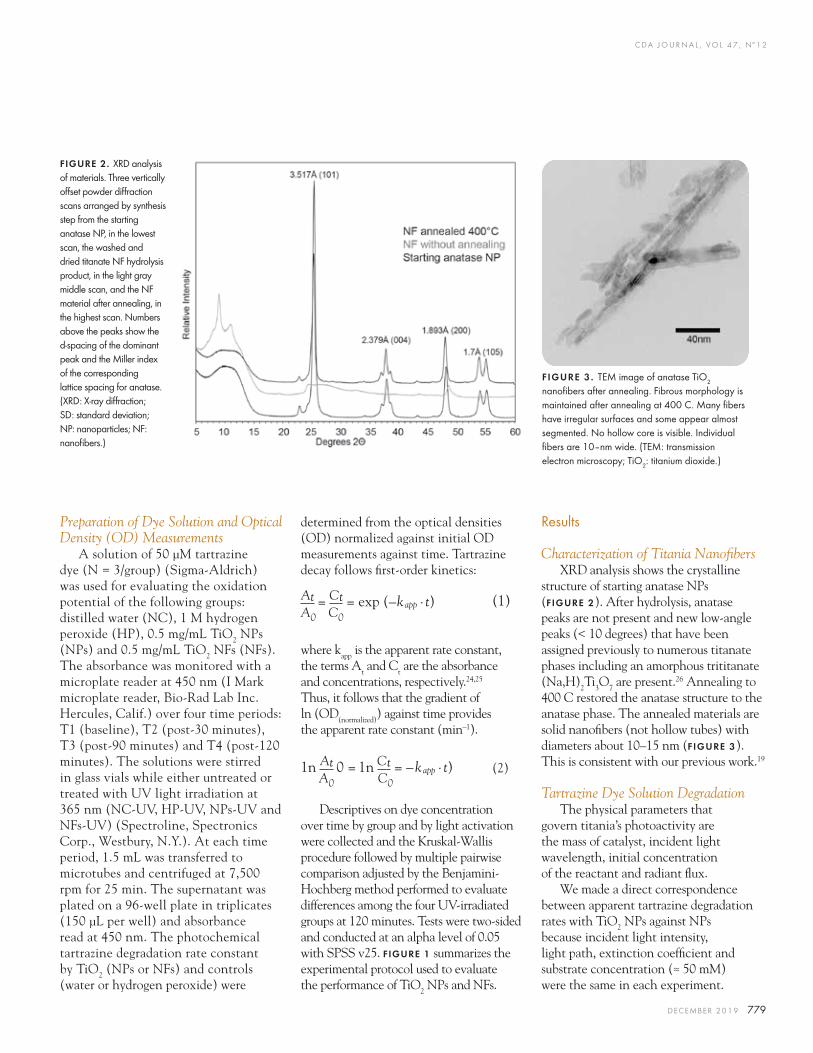
C DA J O U R N A L , V O L 4 7 , Nº 1 2
DECEMBER 2 0 1 9 779
Preparation of Dye Solution and Optical Density (OD) Measurements
A solution of 50 μM tartrazine dye (N = 3/group) (Sigma-Aldrich) was used for evaluating the oxidation potential of the following groups: distilled water (NC), 1 M hydrogen peroxide (HP), 0.5 mg/mL TiO2 NPs (NPs) and 0.5 mg/mL TiO2 NFs (NFs). The absorbance was monitored with a microplate reader at 450 nm (I Mark microplate reader, Bio-Rad Lab Inc. Hercules, Calif.) over four time periods: T1 (baseline), T2 (post-30 minutes), T3 (post-90 minutes) and T4 (post-120 minutes). The solutions were stirred in glass vials while either untreated or treated with UV light irradiation at 365 nm (NC-UV, HP-UV, NPs-UV and NFs-UV) (Spectroline, Spectronics Corp., Westbury, N.Y.). At each time period, 1.5 mL was transferred to microtubes and centrifuged at 7,500 rpm for 25 min. The supernatant was plated on a 96-well plate in triplicates (150 µL per well) and absorbance read at 450 nm. The photochemical tartrazine degradation rate constant by TiO2 (NPs or NFs) and controls (water or hydrogen peroxide) were
determined from the optical densities (OD) normalized against initial OD measurements against time. Tartrazine decay follows first-order kinetics:
(1)
where kapp is the apparent rate constant, the terms At and Ct are the absorbance and concentrations, respectively.24,25 Thus, it follows that the gradient of ln (OD(normalized)) against time provides the apparent rate constant (min–1).
(2)
Descriptives on dye concentration over time by group and by light activation were collected and the Kruskal-Wallis procedure followed by multiple pairwise comparison adjusted by the Benjamini-Hochberg method performed to evaluate differences among the four UV-irradiated groups at 120 minutes. Tests were two-sided and conducted at an alpha level of 0.05 with SPSS v25. fiGure 1 summarizes the experimental protocol used to evaluate the performance of TiO2 NPs and NFs.
At = Ct = exp (–kapp .t)A0 C0
1n At 0 = 1n Ct = –kapp .t) A0 C0
Results
Characterization of Titania NanofibersXRD analysis shows the crystalline
structure of starting anatase NPs (FIGURE 2). After hydrolysis, anatase peaks are not present and new low-angle peaks (< 10 degrees) that have been assigned previously to numerous titanate phases including an amorphous trititanate (Na,H)2Ti3O7 are present.26 Annealing to 400 C restored the anatase structure to the anatase phase. The annealed materials are solid nanofibers (not hollow tubes) with diameters about 10–15 nm (fiGure 3). This is consistent with our previous work.19
Tartrazine Dye Solution DegradationThe physical parameters that
govern titania’s photoactivity are the mass of catalyst, incident light wavelength, initial concentration of the reactant and radiant flux.
We made a direct correspondence between apparent tartrazine degradation rates with TiO2 NPs against NPs because incident light intensity, light path, extinction coefficient and substrate concentration (≈ 50 mM) were the same in each experiment.
FIGURE 2. XRD analysis of materials. Three vertically offset powder diffraction scans arranged by synthesis step from the starting anatase NP, in the lowest scan, the washed and dried titanate NF hydrolysis product, in the light gray middle scan, and the NF material after annealing, in the highest scan. Numbers above the peaks show the d-spacing of the dominant peak and the Miller index of the corresponding lattice spacing for anatase. (XRD: X-ray diffraction; SD: standard deviation; NP: nanoparticles; NF: nanofibers.)
FIGURE 3 . TEM image of anatase TiO2 nanofibers after annealing. Fibrous morphology is maintained after annealing at 400 C. Many fibers have irregular surfaces and some appear almost segmented. No hollow core is visible. Individual fibers are 10–nm wide. (TEM: transmission electron microscopy; TiO2: titanium dioxide.)
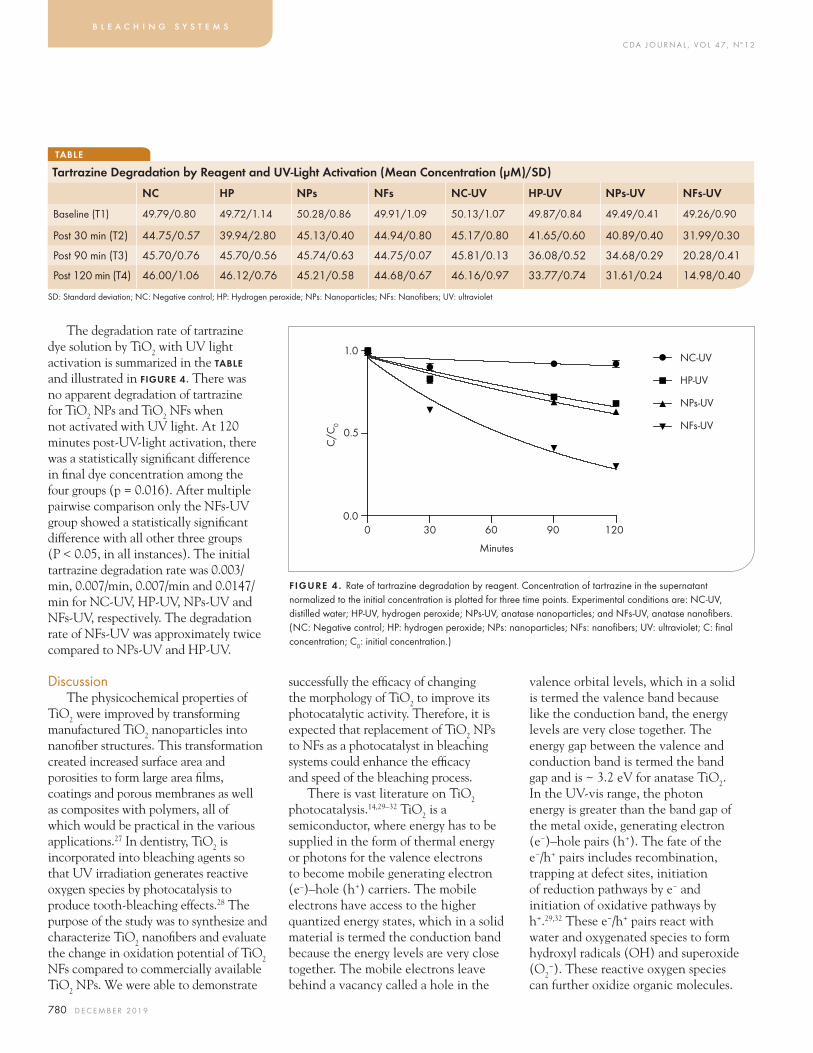
C DA J O U R N A L , V O L 4 7 , Nº 1 2
780 D E C E M B E R 2 01 9
The degradation rate of tartrazine dye solution by TiO2 with UV light activation is summarized in the taBle and illustrated in fiGure 4. There was no apparent degradation of tartrazine for TiO2 NPs and TiO2 NFs when not activated with UV light. At 120 minutes post-UV-light activation, there was a statistically significant difference in final dye concentration among the four groups (p = 0.016). After multiple pairwise comparison only the NFs-UV group showed a statistically significant difference with all other three groups (P < 0.05, in all instances). The initial tartrazine degradation rate was 0.003/min, 0.007/min, 0.007/min and 0.0147/min for NC-UV, HP-UV, NPs-UV and NFs-UV, respectively. The degradation rate of NFs-UV was approximately twice compared to NPs-UV and HP-UV.
DiscussionThe physicochemical properties of
TiO2 were improved by transforming manufactured TiO2 nanoparticles into nanofiber structures. This transformation created increased surface area and porosities to form large area films, coatings and porous membranes as well as composites with polymers, all of which would be practical in the various applications.27 In dentistry, TiO2 is incorporated into bleaching agents so that UV irradiation generates reactive oxygen species by photocatalysis to produce tooth-bleaching effects.28 The purpose of the study was to synthesize and characterize TiO2 nanofibers and evaluate the change in oxidation potential of TiO2 NFs compared to commercially available TiO2 NPs. We were able to demonstrate
successfully the efficacy of changing the morphology of TiO2 to improve its photocatalytic activity. Therefore, it is expected that replacement of TiO2 NPs to NFs as a photocatalyst in bleaching systems could enhance the efficacy and speed of the bleaching process.
There is vast literature on TiO2 photocatalysis.14,29–32 TiO2 is a semiconductor, where energy has to be supplied in the form of thermal energy or photons for the valence electrons to become mobile generating electron (e–)–hole (h+) carriers. The mobile electrons have access to the higher quantized energy states, which in a solid material is termed the conduction band because the energy levels are very close together. The mobile electrons leave behind a vacancy called a hole in the
valence orbital levels, which in a solid is termed the valence band because like the conduction band, the energy levels are very close together. The energy gap between the valence and conduction band is termed the band gap and is ~ 3.2 eV for anatase TiO2. In the UV-vis range, the photon energy is greater than the band gap of the metal oxide, generating electron (e−)–hole pairs (h+). The fate of the e−/h+ pairs includes recombination, trapping at defect sites, initiation of reduction pathways by e− and initiation of oxidative pathways by h+.29,32 These e−/h+ pairs react with water and oxygenated species to form hydroxyl radicals (OH) and superoxide (O2
−). These reactive oxygen species can further oxidize organic molecules.
b l e a c h i n g s y s t e m s
TABLE
Tartrazine Degradation by Reagent and UV-Light Activation (Mean Concentration (μM)/SD)
SD: Standard deviation; NC: Negative control; HP: Hydrogen peroxide; NPs: Nanoparticles; NFs: Nanofibers; UV: ultraviolet
NC HP NPs NFs NC-UV HP-UV NPs-UV NFs-UV
Baseline (T1) 49.79/0.80 49.72/1.14 50.28/0.86 49.91/1.09 50.13/1.07 49.87/0.84 49.49/0.41 49.26/0.90
Post 30 min (T2) 44.75/0.57 39.94/2.80 45.13/0.40 44.94/0.80 45.17/0.80 41.65/0.60 40.89/0.40 31.99/0.30
Post 90 min (T3) 45.70/0.76 45.70/0.56 45.74/0.63 44.75/0.07 45.81/0.13 36.08/0.52 34.68/0.29 20.28/0.41
Post 120 min (T4) 46.00/1.06 46.12/0.76 45.21/0.58 44.68/0.67 46.16/0.97 33.77/0.74 31.61/0.24 14.98/0.40
C/C
0
1.0
0.5
0.00 30 60 90 120
Minutes
NC-UV
HP-UV
NPs-UV
NFs-UV
FIGURE 4 . Rate of tartrazine degradation by reagent. Concentration of tartrazine in the supernatant normalized to the initial concentration is plotted for three time points. Experimental conditions are: NC-UV, distilled water; HP-UV, hydrogen peroxide; NPs-UV, anatase nanoparticles; and NFs-UV, anatase nanofibers. (NC: Negative control; HP: hydrogen peroxide; NPs: nanoparticles; NFs: nanofibers; UV: ultraviolet; C: final concentration; C0: initial concentration.)
C DA J O U R N A L , V O L 4 7 , Nº 1 2
DECEMBER 2 0 1 9 781
To evaluate the oxidation potential of different reagents, we used a tartrazine dye solution for several reasons. First, it is not subject to photo-bleaching as was demonstrated in the negative control group that was also irradiated with UV light. Second, tartrazine dye is a Food and Drug Administration approved dye that is commonly used to color food and drinks. Therefore, consumers are exposed to tartrazine that may directly affect tooth color and have strong clinical relevance. Third, it has been widely used to induce artificial staining on extracted teeth to evaluate the efficacy of bleaching products.33
We expected that UV illumination of the tartrazine dye solution mixed with TiO2 NFs would produce hole (h+) and electron (e−) charge carriers in TiO2 resulting in increased hydroxyl surface density and sequestration of hydronium ions (H3O
+) (TiO2 + H++ → TiO2:Hads; 2Hads → H2). These e−/h+pairs react with water and oxygenated species to form hydroxyl radicals (OH) and superoxide (O2
–). Furthermore, TiO2 degrades tartrazine under UV light,34,35 despite the fact that diffusion of e−/h+pairs was limited to the TiO2 interfacial region and that the photocatalytic efficiency of e–/h+ pairs is low at wavelengths above 360 nm. We observed that NFs have ≈ 2 times the degradation rate for tartrazine dye compared to NPs. This is in accordance with other studies that found photocatalytic organic dye oxidation performance is enhanced in nanofiber/nanotubular structures compared to NPs.20,36,37
It is noteworthy that our ultimate goal would be to enable electron/hole pair generation with optical photons preferable in the visible spectrum. In the case of TiO2, one drawback is the too-large band gap
that restricts applications mainly with UV irradiation.27 In the future, to even enhance the yield of electron/hole pairs at the TiO2 interface, the surface could be doped with noble metals to decrease the band gap and allow excitation with light in the visible spectrum (> 360 nm).12 This may promote increased oxidizing power to degrade organic compounds such as artificial dyes. Additionally, ion exchange and intercalation of other noble metals and organic molecules may lead to optimization and functionalization of nanofibers for diverse future applications in dentistry.
Conclusion Within the limitation of this
study, we conclude that the transition of TiO2 NPs into TiO2 NFs creates optimized structural changes that yield higher oxidation potential and results in faster degradation of an artificial dye solution. n
acknowledGment
This study earned first place in the scientific dental student category of the 2018 CDA Presents Table Clinic Competition. The study was supported by the Loma Linda University School of Dentistry Student Research Program Fund and Loma Linda University GRASP Grant No. 2170315.
references
1. Pokrowiecki R, Palka K, Mielczarek A. Nanomaterials in dentistry: A cornerstone or a black box? Nanomedicine (Lond) 2018 Mar 1;13(6):639–667. doi: 10.2217/nnm-2017-0329. Epub 2018 Feb 8.2. Maman P, Nagpal M, Gilhotra RM, Aggarwal G. Nano Era of Dentistry — An Update. Curr Drug Deliv 2018 Feb 14;15(2):186–204. doi: 10.2174/1567201814666170825155201.3. Padovani GC, Feitosa VP, Sauro S, Tay FR, Duran G, Paula AJ, et al. Advances in dental materials through nanotechnology: Facts, perspectives and toxicological aspects. Trends Biotechnol 2015 Nov;33(11):621–636. doi: 10.1016/j.tibtech.2015.09.005. Epub 2015 Oct 21.4. Liddle JA, Gallatin GM. Nanomanufacturing: A Perspective. ACS Nano 2016 Mar 22;10(3):2995–3014. doi: 10.1021/acsnano.5b03299. Epub 2016 Feb 22.5. Jan SM, Mir AM, Behal R, Shafi M, Kirmani M, Bhat MA. Role of nanotechnology in dentistry. Sch J App Med Sci 2014;14(2):785–9.
6. Chieruzzi M, Pagano S, Moretti S, Pinna R, Milia E, Torre L, et al. Nanomaterials for Tissue Engineering in Dentistry. Nanomaterials (Basel) 2016 Jul 21;6(7). pii: E134. doi: 10.3390/nano6070134.7. Bhavikatti SK, Bhardwaj S, Prabhuji ML. Current applications of nanotechnology in dentistry: A review. Gen Dent Jul–Aug 2014;62(4):72–7.8. Priyadarsini S, Mukherjee S, Mishra M. Nanoparticles used in dentistry: A review. J Oral Biol Craniofac Res 2018 Jan–Apr;8(1):58–67. doi: 10.1016/j.jobcr.2017.12.004. Epub 2017 Dec 7.9. Cheng L, Zhang K, Weir MD, Melo MA, Zhou X, Xu HH. Nanotechnology strategies for antibacterial and remineralizing composites and adhesives to tackle dental caries. Nanomedicine (Lond) 2015 Mar;10(4):627–41. doi: 10.2217/nnm.14.191.10. Tang ZS, Bolong N, Saad I, Ayog JL. The Morphology of Electrospun Titanium Dioxide Nanofibers and Its Influencing Factors. MATEC Web Conf 2016 Apr;47:01020.11. Santos LM, Machado WA, França MD, Borges KA, Paniago RM, Patrocinio AOT, et al. Structural characterization of Ag-doped TiO2 with enhanced photocatalytic activity. RSC Adv 2015 Nov;5(125):103752–9 doi:10.1039/C5RA22647C.12. Ayati A, Ahmadpour A, Bamoharram FF, Tanhaei B, Mänttäri M, Sillanpää M. A review on catalytic applications of Au/TiO2 nanoparticles in the removal of water pollutant. Chemosphere 2014 Jul;107:163–174. doi: 10.1016/j.chemosphere.2014.01.040. Epub 2014 Feb 18.13. Yang D, Liu H, Zheng Z, Yuan Y, Zhao J-c, Waclawik ER, et al. An efficient photocatalyst structure: TiO2(B) nanofibers with a shell of anatase nanocrystals. J Am Chem Soc 2009 Nov;131(49):17885–93. doi.org/10.1021/ja906774k.14. Lee K, Mazare A, Schmuki P. One-dimensional titanium dioxide nanomaterials: Nanotubes. Chem Rev 2014 Aug;114(19):9385–454. doi: 10.1021/cr500061m.15. Yang DJ, Zheng ZF, Liu HW, Zhu HY, Ke XB, Xu Y, et al. Layered titanate nanofibers as efficient adsorbents for removal of toxic radioactive and heavy metal ions from water. J Phys Chem C 2008 Oct;112(42):16275–80. doi.org/10.1021/jp803826g.16. Gregurec D, Wang G, Pires RH, Kosutic M, Lüdtke T, Delcea M, et al. Bioinspired titanium coatings: Self-assembly of collagen-alginate films for enhanced osseointegration. J Mater Chem B 2016 Feb;4(11):1978–86. doi: 10.1039/C6TB00204H.17. Yada M, Inoue Y, Noda I, Morita T, Torikai T, Watari T, et al. Antibacterial properties of titanate nanofiber thin films formed on a titanium plate. J Nanomater 2013 Jan;2013:1–9. doi: 10.1155/2013/476585.18. Kishi A, Otsuki M, Sadr A, Ikeda M, Tagami J. Effect of light units on tooth bleaching with visible-light activating titanium dioxide photocatalyst. Dent Mater J 2011;30(5):723–9. Epub 2011 Sep 23.19. Allard MM, Merlos SN, Springer BN, Cooper J, Zhang GY, Boskovic DS, et al. Role of TiO2 anatase surface morphology on organophosphorus interfacial chemistry. J Phys Chem C 2018 Dec;122(51):29237–48. doi.org/10.1021/acs.jpcc.8b08641.
C DA J O U R N A L , V O L 4 7 , Nº 1 2
782 D E C E M B E R 2 01 9
org/10.1021/cs200208a.25. Wunder S, Polzer F, Lu Y, Mei Y, Ballauff M. Kinetic Analysis of catalytic reduction of 4-nitrophenol by metallic nanoparticles immobilized in spherical polyelectrolyte brushes. J Phys Chem C 2010 Apr;114:8814–20. doi.org/10.1021/jp101125j.26. Bavykin DV, Kulak AN, Walsh FC. Metastable nature of titanate nanotubes in an alkaline environment. Cryst Growth Des 2010 Aug;10(10):4421–7. doi.org/10.1021/cg100529y.27. Wu MC, Hiltunen J, Sápi A, Avila A, Larsson W, Liao HC, et al. Nitrogen-doped anatase nanofibers decorated with noble metal nanoparticles for photocatalytic production of hydrogen. ACS Nano 2011;5(6):5025–30. 2011 Jun 28;5(6):5025–30. doi: 10.1021/nn201111j. Epub 2011 May 24.28. Saita M, Kobayashi K, Yoshino F, Hase H, Nonami T, Kimoto K, et al. ESR investigation of ROS generated by H2O2 bleaching with TiO2 coated HAp. Dent Mater J 2012;31(3):458–64. Epub 2012 May 14. doi.org/10.4012/dmj.2011-192.29. Schneider J, Matsuoka M, Takeuchi M, Zhang
20. Wu N, Wang J, Tafen de N, Wang H, Zheng JG, Lewis JP, et al. Shape-enhanced photocatalytic activity of single-crystalline anatase TiO(2) (101) nanobelts. J Am Chem Soc 2010 Apr;132(19):6679–85. doi.org/10.1021/ja909456f.21. Kasuga T, Hiramatsu M, Hoson A, Sekino T, Niihara K. Formation of titanium oxide nanotube. Langmuir 1998 May;14(12):3160–3. doi.org/10.1021/la9713816.22. Sallem F, Chassagnon R, Megriche A, El Maaoui M, Millot N. Effect of mechanical stirring and temperature on dynamic hydrothermal synthesis of titanate nanotubes. J Alloy Compd 2017 Jun;722:785–96. doi: 10.1016/j.jallcom.2017.06.172.23. Horvath E, Kukovecz A, Konya Z, Kiricsi I. Hydrothermal conversion of self-assembled titanate nanotubes into nanowires in a revolving autoclave. Chem Mater 2007 Jan;19(4):927–31. doi.org/10.1021/cm062413q.24. Wunder S, Lu Y, Albrecht M, Ballauff M. Catalytic activity of faceted gold nanoparticles studied by a model reaction: Evidence for substrate-induced surface restructuring. ACS Catal 2011 June;1(8):908–16. doi.
J, Horiuchi Y, Anpo M, et al. Understanding TiO2 photocatalysis: Mechanisms and materials. Chem Rev 2014 Sep;114(19):9919–86. doi.org/10.1021/cr5001892.30. Sang L, Zhao Y, Burda C. TiO2 nanoparticles as functional building blocks. Chem Rev 2014 May;114(19):9283–318. doi.org/10.1021/cr400629p.31. Kumar SG, Devi LG. Review on modified TiO2 photocatalysis under UV/visible light: Selected results and related mechanisms on interfacial charge carrier transfer dynamics. J Phys Chem A 2011 Sep;115(46):13211–41. doi.org/10.1021/jp204364a.32. Linsebigler AL, Lu G, John T. Yates J. Photocatalysis on TiO2 surfaces: Principles, mechanisms and selected results. Chem Rev 1995 May;95:735–58. doi.org/10.1021/cr00035a013.33. Kwon SR, Kurti SR, Jr., Oyoyo U, Li Y. Effect of light-activated tooth whitening on color change relative to color of artificially stained teeth. J Esthet Restor Dent 2015 Mar–Apr;27 Suppl 1:S10–7. doi: 10.1111/jerd.12142.34. Aoudjit L, Martins PM, Madjene F, Petrovykh DY, Lanceros-Mendez S. Photocatalytic reusable membranes for the effective degradation of tartrazine with a solar photoreactor. J Hazard Mater 2018 Feb 15;344:408–416. doi: 10.1016/j.jhazmat.2017.10.053. Epub 2017 Nov 6.35. Heredia CL, Sham dL, Farfán-Torres lM. Tartrazine degradation by supported TiO2 on magnetic particles. Matéria (Rio de Janeiro) 2015 Sep;20:668–75. doi: 10.1590/S1517-707620150003.0069.36. Kiatkittipong K, Scott J, Amal R. Hydrothermally synthesized titanate nanostructures: Impact of heat treatment on particle characteristics and photocatalytic properties. ACS Appl Mater Interfaces 2011 Sep;3(10):3988–96. doi.org/10.1021/am2008568.37. Lin J, Liu X, Zhu S, Liu Y, Chen X. Anatase TiO2 nanotube powder film with high crystallinity for enhanced photocatalytic performance. Nanoscale Res Lett 2015 Mar 4;10:110. doi: 10.1186/s11671-015-0814-6. eCollection 2015.
the correspondinG author, Christina Chi, BA, DDS, can be reached at [email protected].
b l e a c h i n g s y s t e m s
LDM_CDA_Journal_1.3_Square_LindaBrown_05_23_17.indd 1 5/24/2017 9:21:40 PM
C DA J O U R N A L , V O L 4 7 , Nº 1 2
DECEMBER 2 0 1 9 783
Clinical and Microbial Changes in Orthodontic Patients Using Clear Aligners Vs. Fixed AppliancesJoseph Mullen, BS; Melissa Agnello, PhD; Edward Viloria, DDS; Kenneth Chang Chien, BS; Emily Duong, BS; Masuma Rizvi, BDS; Pega Hajian, BS; Huiying Li, PhD; Baochen Shi, PhD; Kang Ting, DMD, DMedSc; Wenyuan Shi, PhD; Renate Lux, PhD; and Tingxi Wu, DDS, PhD
a b s t r ac t This pilot study investigated the clinical and microbial changes that occur in patients undergoing orthodontic treatment using fixed appliances and clear aligners. The clear aligner group had significantly less plaque accumulation than the fixed appliances group, but no significant differences in gingival health were found. Next-generation sequencing of the 16S rRNA encoding gene revealed a shift in the oral microbiome from baseline with a unique microbial community discovered on the inner surface of clear aligners.
AUTHORS
Joseph Mullen, BS, is a fourth-year dental student at the University of California, Los Angeles, School of Dentistry.
Melissa Agnello, PhD, received her PhD from the University of Southern California in clinical and experimental therapeutics. She is a former postdoctoral scholar in the UCLA School of Dentistry, section of oral biology, and works for uBiome in San Francisco.
Edward Viloria, DDS, is a third-year resident in the orthodontics and dentofacial orthopedics program at the UCLA School of Dentistry.
Orthodontic tooth movement has traditionally been achieved using fixed appliances. Although this treatment modality
has a long track record of success in treating malocclusion, it also has several disadvantages for patients, including poor aesthetics and a decrease in the patient’s ability to effectively brush and floss to remove oral biofilm.1,2 In the late 1990s, a computerized process of making casts with incremental changes was introduced that could be used to fabricate removable clear aligners to achieve orthodontic movement.1 With the advent of this new technology and treatment modality, orthodontic patients were then able to remove their orthodontic appliances to eat, brush and floss, thus allowing for excellent maintenance of oral hygiene.3–7
o r t h o d o n t i c t r e a t m e n t
Kenneth Chang Chien, BS, is a second-year dental student at the University of California, San Francisco School of Dentistry.
Emily Duong, BS, is a first-year dental student at the UCLA School of Dentistry.
Masuma Rizvi, BDS, is a third-year dental student at the UCLA School of Dentistry.
Pega Hajian, BS, is a third-year dental student at the UCLA School of Dentistry.
Huiying Li, PhD, is an associate professor in the department of molecular and medical pharmacology at the UCLA Geffen School of Medicine.
Baochen Shi, PhD, is a project scientist working in the department of molecular and medical pharmacology at the UCLA Geffen School of Medicine.
Kang Ting, DMD, DMedSc, is a professor in the division of growth and development at the UCLA School of Dentistry.
Wenyuan Shi, PhD, is the former chairman and professor of oral biology at the UCLA School of
Dentistry and serves as the chief executive officer and chief scientific officer of the Forsyth Institute in Cambridge, Mass.
Renate Lux, PhD, is a professor in the section of periodontics at the UCLA School of Dentistry.
Tingxi Wu, DDS, PhD, is the director of orthodontic and craniofacial development research and an assistant member of staff at the Forsyth Institute in Cambridge, Mass.
Conflict of Interest Disclosure for all authors: None reported.
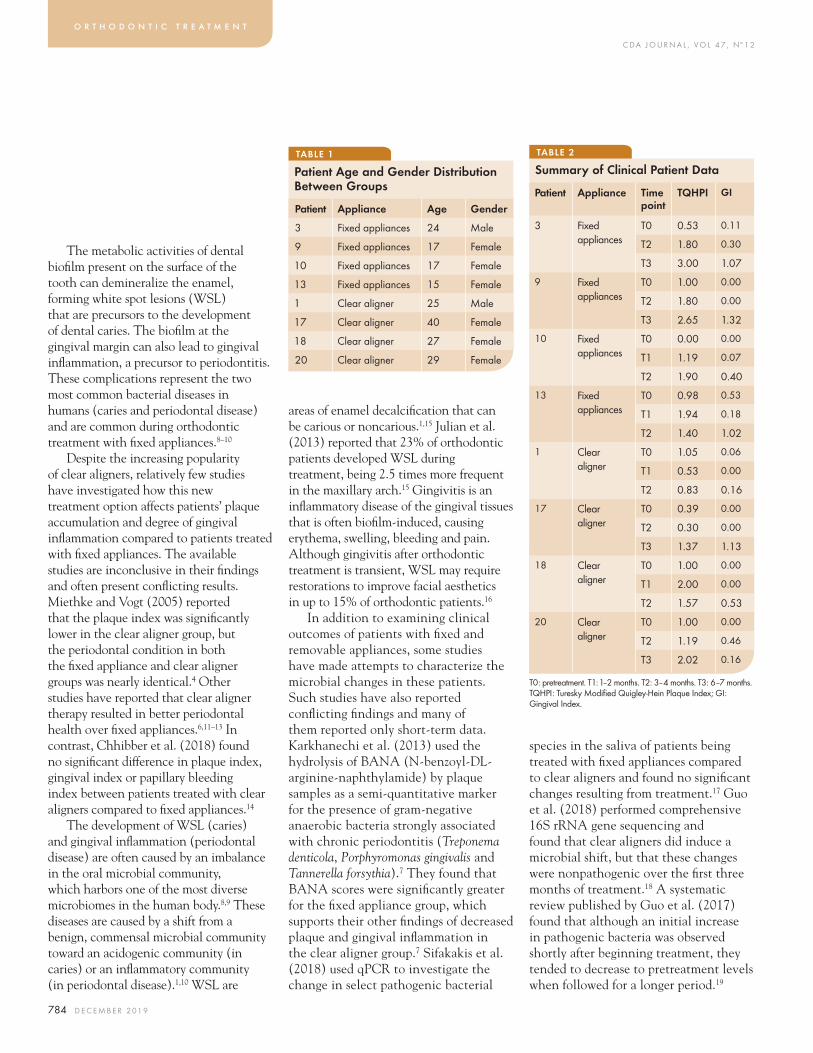
C DA J O U R N A L , V O L 4 7 , Nº 1 2
784 D E C E M B E R 2 01 9
species in the saliva of patients being treated with fixed appliances compared to clear aligners and found no significant changes resulting from treatment.17 Guo et al. (2018) performed comprehensive 16S rRNA gene sequencing and found that clear aligners did induce a microbial shift, but that these changes were nonpathogenic over the first three months of treatment.18 A systematic review published by Guo et al. (2017) found that although an initial increase in pathogenic bacteria was observed shortly after beginning treatment, they tended to decrease to pretreatment levels when followed for a longer period.19
areas of enamel decalcification that can be carious or noncarious.1,15 Julian et al. (2013) reported that 23% of orthodontic patients developed WSL during treatment, being 2.5 times more frequent in the maxillary arch.15 Gingivitis is an inflammatory disease of the gingival tissues that is often biofilm-induced, causing erythema, swelling, bleeding and pain. Although gingivitis after orthodontic treatment is transient, WSL may require restorations to improve facial aesthetics in up to 15% of orthodontic patients.16
In addition to examining clinical outcomes of patients with fixed and removable appliances, some studies have made attempts to characterize the microbial changes in these patients. Such studies have also reported conflicting findings and many of them reported only short-term data. Karkhanechi et al. (2013) used the hydrolysis of BANA (N-benzoyl-DL-arginine-naphthylamide) by plaque samples as a semi-quantitative marker for the presence of gram-negative anaerobic bacteria strongly associated with chronic periodontitis (Treponema denticola, Porphyromonas gingivalis and Tannerella forsythia).7 They found that BANA scores were significantly greater for the fixed appliance group, which supports their other findings of decreased plaque and gingival inflammation in the clear aligner group.7 Sifakakis et al. (2018) used qPCR to investigate the change in select pathogenic bacterial
The metabolic activities of dental biofilm present on the surface of the tooth can demineralize the enamel, forming white spot lesions (WSL) that are precursors to the development of dental caries. The biofilm at the gingival margin can also lead to gingival inflammation, a precursor to periodontitis. These complications represent the two most common bacterial diseases in humans (caries and periodontal disease) and are common during orthodontic treatment with fixed appliances.8–10
Despite the increasing popularity of clear aligners, relatively few studies have investigated how this new treatment option affects patients’ plaque accumulation and degree of gingival inflammation compared to patients treated with fixed appliances. The available studies are inconclusive in their findings and often present conflicting results. Miethke and Vogt (2005) reported that the plaque index was significantly lower in the clear aligner group, but the periodontal condition in both the fixed appliance and clear aligner groups was nearly identical.4 Other studies have reported that clear aligner therapy resulted in better periodontal health over fixed appliances.6,11–13 In contrast, Chhibber et al. (2018) found no significant difference in plaque index, gingival index or papillary bleeding index between patients treated with clear aligners compared to fixed appliances.14
The development of WSL (caries) and gingival inflammation (periodontal disease) are often caused by an imbalance in the oral microbial community, which harbors one of the most diverse microbiomes in the human body.8,9 These diseases are caused by a shift from a benign, commensal microbial community toward an acidogenic community (in caries) or an inflammatory community (in periodontal disease).1,10 WSL are
o r t h o d o n t i c t r e a t m e n t
TABLE 1
Patient Age and Gender Distribution Between Groups
Patient Appliance Age Gender
3 Fixed appliances 24 Male
9 Fixed appliances 17 Female
10 Fixed appliances 17 Female
13 Fixed appliances 15 Female
1 Clear aligner 25 Male
17 Clear aligner 40 Female
18 Clear aligner 27 Female
20 Clear aligner 29 Female
TABLE 2
Summary of Clinical Patient Data
T0: pretreatment. T1: 1–2 months. T2: 3–4 months. T3: 6–7 months. TQHPI: Turesky Modified Quigley-Hein Plaque Index; GI: Gingival Index.
Patient Appliance Time point
TQHPI GI
3 Fixed appliances
T0 0.53 0.11
T2 1.80 0.30
T3 3.00 1.07
9 Fixed appliances
T0 1.00 0.00
T2 1.80 0.00
T3 2.65 1.32
10 Fixed appliances
T0 0.00 0.00
T1 1.19 0.07
T2 1.90 0.40
13 Fixed appliances
T0 0.98 0.53
T1 1.94 0.18
T2 1.40 1.02
1 Clear aligner
T0 1.05 0.06
T1 0.53 0.00
T2 0.83 0.16
17 Clear aligner
T0 0.39 0.00
T2 0.30 0.00
T3 1.37 1.13
18 Clear aligner
T0 1.00 0.00
T1 2.00 0.00
T2 1.57 0.53
20 Clear aligner
T0 1.00 0.00
T2 1.19 0.46
T3 2.02 0.16
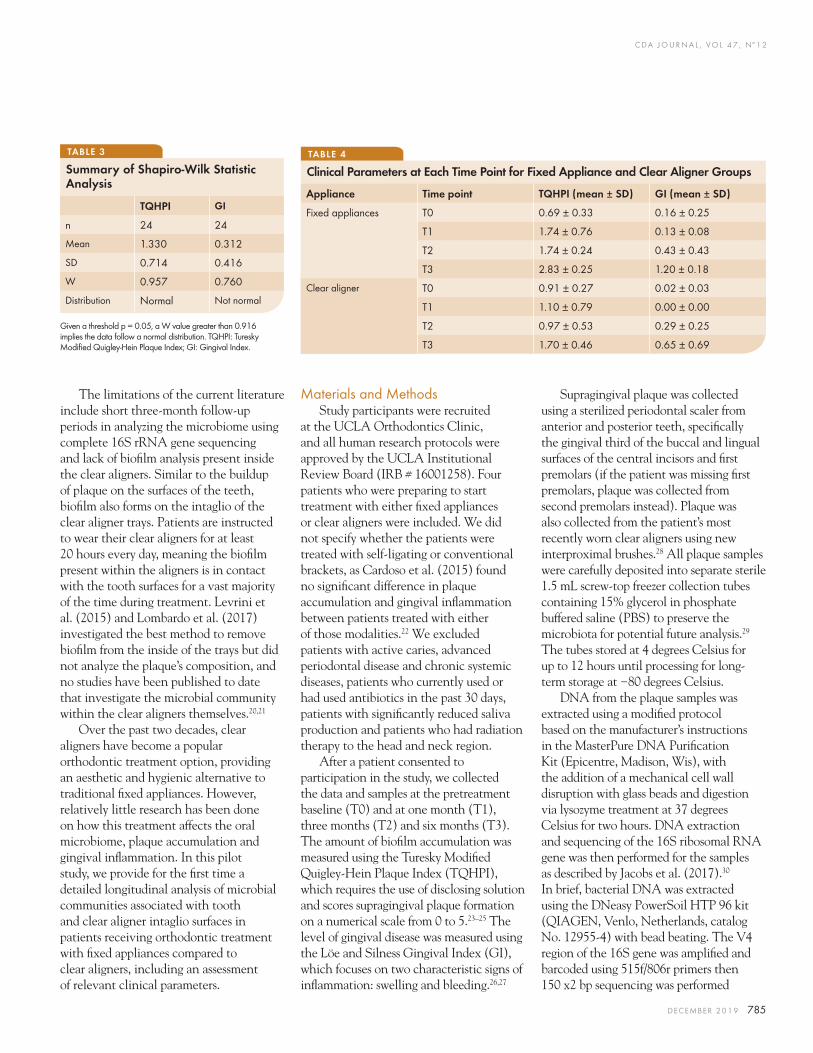
C DA J O U R N A L , V O L 4 7 , Nº 1 2
DECEMBER 2 0 1 9 785
Supragingival plaque was collected using a sterilized periodontal scaler from anterior and posterior teeth, specifically the gingival third of the buccal and lingual surfaces of the central incisors and first premolars (if the patient was missing first premolars, plaque was collected from second premolars instead). Plaque was also collected from the patient’s most recently worn clear aligners using new interproximal brushes.28 All plaque samples were carefully deposited into separate sterile 1.5 mL screw-top freezer collection tubes containing 15% glycerol in phosphate buffered saline (PBS) to preserve the microbiota for potential future analysis.29 The tubes stored at 4 degrees Celsius for up to 12 hours until processing for long-term storage at −80 degrees Celsius.
DNA from the plaque samples was extracted using a modified protocol based on the manufacturer’s instructions in the MasterPure DNA Purification Kit (Epicentre, Madison, Wis), with the addition of a mechanical cell wall disruption with glass beads and digestion via lysozyme treatment at 37 degrees Celsius for two hours. DNA extraction and sequencing of the 16S ribosomal RNA gene was then performed for the samples as described by Jacobs et al. (2017).30 In brief, bacterial DNA was extracted using the DNeasy PowerSoil HTP 96 kit (QIAGEN, Venlo, Netherlands, catalog No. 12955-4) with bead beating. The V4 region of the 16S gene was amplified and barcoded using 515f/806r primers then 150 x2 bp sequencing was performed
Materials and MethodsStudy participants were recruited
at the UCLA Orthodontics Clinic, and all human research protocols were approved by the UCLA Institutional Review Board (IRB # 16001258). Four patients who were preparing to start treatment with either fixed appliances or clear aligners were included. We did not specify whether the patients were treated with self-ligating or conventional brackets, as Cardoso et al. (2015) found no significant difference in plaque accumulation and gingival inflammation between patients treated with either of those modalities.22 We excluded patients with active caries, advanced periodontal disease and chronic systemic diseases, patients who currently used or had used antibiotics in the past 30 days, patients with significantly reduced saliva production and patients who had radiation therapy to the head and neck region.
After a patient consented to participation in the study, we collected the data and samples at the pretreatment baseline (T0) and at one month (T1), three months (T2) and six months (T3). The amount of biofilm accumulation was measured using the Turesky Modified Quigley-Hein Plaque Index (TQHPI), which requires the use of disclosing solution and scores supragingival plaque formation on a numerical scale from 0 to 5.23–25 The level of gingival disease was measured using the Löe and Silness Gingival Index (GI), which focuses on two characteristic signs of inflammation: swelling and bleeding.26,27
The limitations of the current literature include short three-month follow-up periods in analyzing the microbiome using complete 16S rRNA gene sequencing and lack of biofilm analysis present inside the clear aligners. Similar to the buildup of plaque on the surfaces of the teeth, biofilm also forms on the intaglio of the clear aligner trays. Patients are instructed to wear their clear aligners for at least 20 hours every day, meaning the biofilm present within the aligners is in contact with the tooth surfaces for a vast majority of the time during treatment. Levrini et al. (2015) and Lombardo et al. (2017) investigated the best method to remove biofilm from the inside of the trays but did not analyze the plaque’s composition, and no studies have been published to date that investigate the microbial community within the clear aligners themselves.20,21
Over the past two decades, clear aligners have become a popular orthodontic treatment option, providing an aesthetic and hygienic alternative to traditional fixed appliances. However, relatively little research has been done on how this treatment affects the oral microbiome, plaque accumulation and gingival inflammation. In this pilot study, we provide for the first time a detailed longitudinal analysis of microbial communities associated with tooth and clear aligner intaglio surfaces in patients receiving orthodontic treatment with fixed appliances compared to clear aligners, including an assessment of relevant clinical parameters.
TABLE 3
Summary of Shapiro-Wilk Statistic Analysis
Given a threshold p = 0.05, a W value greater than 0.916 implies the data follow a normal distribution. TQHPI: Turesky Modified Quigley-Hein Plaque Index; GI: Gingival Index.
TQHPI GI
n 24 24
Mean 1.330 0.312
SD 0.714 0.416
W 0.957 0.760
Distribution Normal Not normal
TABLE 4
Clinical Parameters at Each Time Point for Fixed Appliance and Clear Aligner Groups
Appliance Time point TQHPI (mean ± SD) GI (mean ± SD)
Fixed appliances T0 0.69 ± 0.33 0.16 ± 0.25
T1 1.74 ± 0.76 0.13 ± 0.08
T2 1.74 ± 0.24 0.43 ± 0.43
T3 2.83 ± 0.25 1.20 ± 0.18
Clear aligner T0 0.91 ± 0.27 0.02 ± 0.03
T1 1.10 ± 0.79 0.00 ± 0.00
T2 0.97 ± 0.53 0.29 ± 0.25
T3 1.70 ± 0.46 0.65 ± 0.69
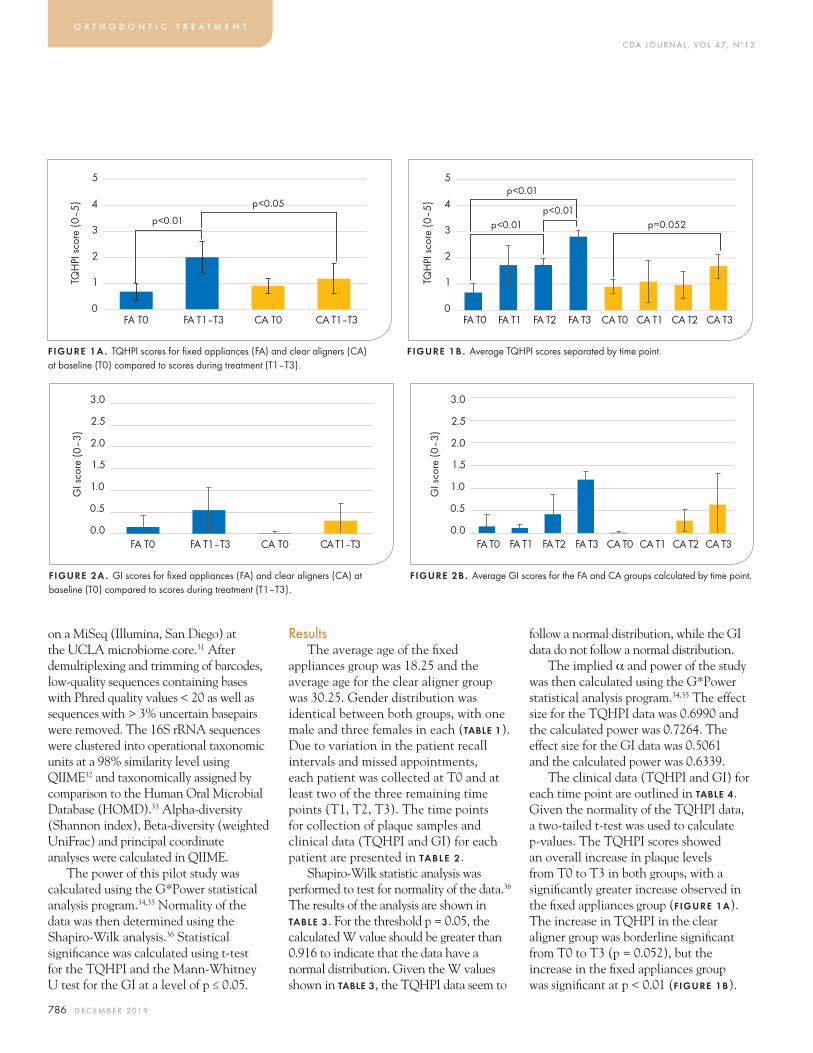
C DA J O U R N A L , V O L 4 7 , Nº 1 2
786 D E C E M B E R 2 01 9
on a MiSeq (Illumina, San Diego) at the UCLA microbiome core.31 After demultiplexing and trimming of barcodes, low-quality sequences containing bases with Phred quality values < 20 as well as sequences with > 3% uncertain basepairs were removed. The 16S rRNA sequences were clustered into operational taxonomic units at a 98% similarity level using QIIME32 and taxonomically assigned by comparison to the Human Oral Microbial Database (HOMD).33 Alpha-diversity (Shannon index), Beta-diversity (weighted UniFrac) and principal coordinate analyses were calculated in QIIME.
The power of this pilot study was calculated using the G*Power statistical analysis program.34,35 Normality of the data was then determined using the Shapiro-Wilk analysis.36 Statistical significance was calculated using t-test for the TQHPI and the Mann-Whitney U test for the GI at a level of p ≤ 0.05.
ResultsThe average age of the fixed
appliances group was 18.25 and the average age for the clear aligner group was 30.25. Gender distribution was identical between both groups, with one male and three females in each (taBle 1). Due to variation in the patient recall intervals and missed appointments, each patient was collected at T0 and at least two of the three remaining time points (T1, T2, T3). The time points for collection of plaque samples and clinical data (TQHPI and GI) for each patient are presented in TABLE 2 .
Shapiro-Wilk statistic analysis was performed to test for normality of the data.36 The results of the analysis are shown in TABLE 3. For the threshold p = 0.05, the calculated W value should be greater than 0.916 to indicate that the data have a normal distribution. Given the W values shown in taBle 3, the TQHPI data seem to
follow a normal distribution, while the GI data do not follow a normal distribution.
The implied α and power of the study was then calculated using the G*Power statistical analysis program.34,35 The effect size for the TQHPI data was 0.6990 and the calculated power was 0.7264. The effect size for the GI data was 0.5061 and the calculated power was 0.6339.
The clinical data (TQHPI and GI) for each time point are outlined in taBle 4. Given the normality of the TQHPI data, a two-tailed t-test was used to calculate p-values. The TQHPI scores showed an overall increase in plaque levels from T0 to T3 in both groups, with a significantly greater increase observed in the fixed appliances group (FIGURE 1a). The increase in TQHPI in the clear aligner group was borderline significant from T0 to T3 (p = 0.052), but the increase in the fixed appliances group was significant at p < 0.01 (fiGure 1B).
o r t h o d o n t i c t r e a t m e n t
0
5
4
3
2
1TQH
PI s
core
(0–5
)
FA T0 FA T1–T3 CA T0 CA T1–T3
p<0.01
p<0.05
FIGURE 1A . TQHPI scores for fixed appliances (FA) and clear aligners (CA) at baseline (T0) compared to scores during treatment (T1–T3).
0
5
4
3
2
1TQH
PI s
core
(0–5
)
FA T0 FA T1 FA T2 FA T3 CA T0 CA T1 CA T2 CA T3
p<0.01p<0.01 p=0.052
p<0.01
FIGURE 1B . Average TQHPI scores separated by time point.
0.0
3.0
2.5
2.0
1.5
1.0
0.5
FA T0 FA T1–T3 CA T0 CA T1–T3
GI s
core
(0–3
)
FIGURE 2A . GI scores for fixed appliances (FA) and clear aligners (CA) at baseline (T0) compared to scores during treatment (T1–T3).
0.0
3.0
2.5
2.0
1.5
1.0
0.5
FA T0 FA T1 FA T2 FA T3 CA T0 CA T1 CA T2 CA T3
GI s
core
(0–3
)
FIGURE 2B . Average GI scores for the FA and CA groups calculated by time point.
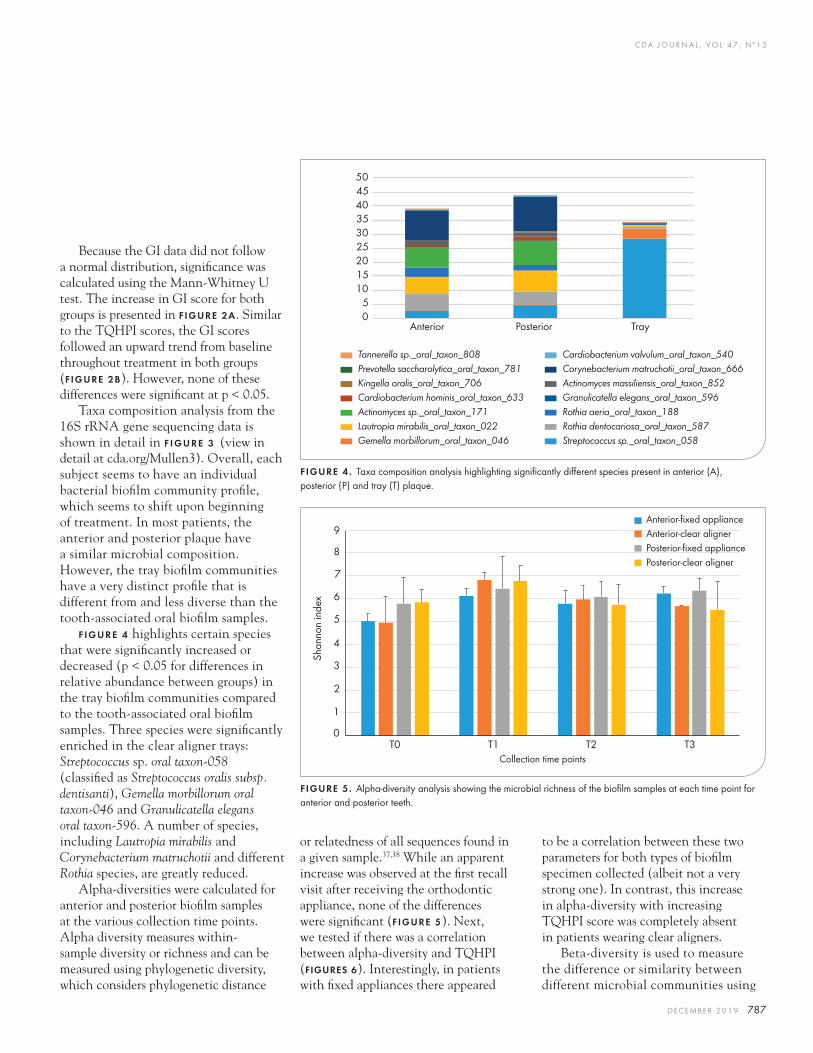
C DA J O U R N A L , V O L 4 7 , Nº 1 2
DECEMBER 2 0 1 9 787
Because the GI data did not follow a normal distribution, significance was calculated using the Mann-Whitney U test. The increase in GI score for both groups is presented in fiGure 2a. Similar to the TQHPI scores, the GI scores followed an upward trend from baseline throughout treatment in both groups (fiGure 2B). However, none of these differences were significant at p < 0.05.
Taxa composition analysis from the 16S rRNA gene sequencing data is shown in detail in F IGURE 3 (view in detail at cda.org/Mullen3). Overall, each subject seems to have an individual bacterial biofilm community profile, which seems to shift upon beginning of treatment. In most patients, the anterior and posterior plaque have a similar microbial composition. However, the tray biofilm communities have a very distinct profile that is different from and less diverse than the tooth-associated oral biofilm samples.
f iGure 4 highlights certain species that were significantly increased or decreased (p < 0.05 for differences in relative abundance between groups) in the tray biofilm communities compared to the tooth-associated oral biofilm samples. Three species were significantly enriched in the clear aligner trays: Streptococcus sp. oral taxon-058 (classified as Streptococcus oralis subsp. dentisanti), Gemella morbillorum oral taxon-046 and Granulicatella elegans oral taxon-596. A number of species, including Lautropia mirabilis and Corynebacterium matruchotii and different Rothia species, are greatly reduced.
Alpha-diversities were calculated for anterior and posterior biofilm samples at the various collection time points. Alpha diversity measures within-sample diversity or richness and can be measured using phylogenetic diversity, which considers phylogenetic distance
Shan
non
inde
x
0
1
2
3
4
5
6
7
8
9
T0 T1 T2 T3
Anterior-fixed applianceAnterior-clear alignerPosterior-fixed appliancePosterior-clear aligner
Collection time points
FIGURE 5. Alpha-diversity analysis showing the microbial richness of the biofilm samples at each time point for anterior and posterior teeth.
or relatedness of all sequences found in a given sample.37,38 While an apparent increase was observed at the first recall visit after receiving the orthodontic appliance, none of the differences were significant (fiGure 5). Next, we tested if there was a correlation between alpha-diversity and TQHPI (fiGures 6). Interestingly, in patients with fixed appliances there appeared
to be a correlation between these two parameters for both types of biofilm specimen collected (albeit not a very strong one). In contrast, this increase in alpha-diversity with increasing TQHPI score was completely absent in patients wearing clear aligners.
Beta-diversity is used to measure the difference or similarity between different microbial communities using
05
101520253035404550
Anterior Posterior Tray
FIGURE 4 . Taxa composition analysis highlighting significantly different species present in anterior (A), posterior (P) and tray (T) plaque.
Tannerella sp._oral_taxon_808Prevotella saccharolytica_oral_taxon_781Kingella oralis_oral_taxon_706Cardiobacterium hominis_oral_taxon_633Actinomyces sp._oral_taxon_171Lautropia mirabilis_oral_taxon_022Gemella morbillorum_oral_taxon_046
Cardiobacterium valvulum_oral_taxon_540Corynebacterium matruchotii_oral_taxon_666Actinomyces massiliensis_oral_taxon_852Granulicatella elegans_oral_taxon_596Rothia aeria_oral_taxon_188Rothia dentocariosa_oral_taxon_587Streptococcus sp._oral_taxon_058
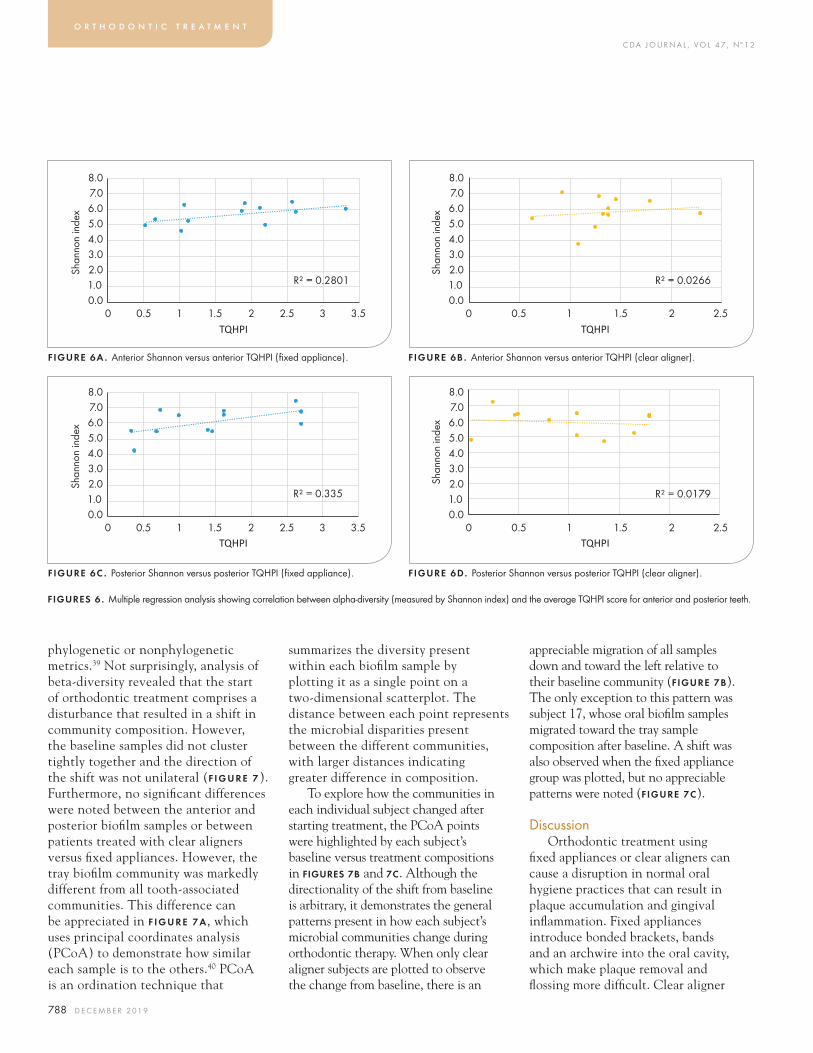
C DA J O U R N A L , V O L 4 7 , Nº 1 2
788 D E C E M B E R 2 01 9
phylogenetic or nonphylogenetic metrics.39 Not surprisingly, analysis of beta-diversity revealed that the start of orthodontic treatment comprises a disturbance that resulted in a shift in community composition. However, the baseline samples did not cluster tightly together and the direction of the shift was not unilateral (f i G u r e 7). Furthermore, no significant differences were noted between the anterior and posterior biofilm samples or between patients treated with clear aligners versus fixed appliances. However, the tray biofilm community was markedly different from all tooth-associated communities. This difference can be appreciated in f i G u r e 7 a, which uses principal coordinates analysis (PCoA) to demonstrate how similar each sample is to the others.40 PCoA is an ordination technique that
summarizes the diversity present within each biofilm sample by plotting it as a single point on a two-dimensional scatterplot. The distance between each point represents the microbial disparities present between the different communities, with larger distances indicating greater difference in composition.
To explore how the communities in each individual subject changed after starting treatment, the PCoA points were highlighted by each subject’s baseline versus treatment compositions in fiGures 7B and 7c. Although the directionality of the shift from baseline is arbitrary, it demonstrates the general patterns present in how each subject’s microbial communities change during orthodontic therapy. When only clear aligner subjects are plotted to observe the change from baseline, there is an
appreciable migration of all samples down and toward the left relative to their baseline community (fiGure 7B). The only exception to this pattern was subject 17, whose oral biofilm samples migrated toward the tray sample composition after baseline. A shift was also observed when the fixed appliance group was plotted, but no appreciable patterns were noted (fiGure 7c).
DiscussionOrthodontic treatment using
fixed appliances or clear aligners can cause a disruption in normal oral hygiene practices that can result in plaque accumulation and gingival inflammation. Fixed appliances introduce bonded brackets, bands and an archwire into the oral cavity, which make plaque removal and flossing more difficult. Clear aligner
o r t h o d o n t i c t r e a t m e n t
0.01.02.03.04.05.06.07.08.0
0 0.5 1 1.5 2 2.5 3 3.5
Shan
non
inde
x
TQHPI
R² = 0.2801
0.01.02.03.04.05.06.07.08.0
0 0.5 1 1.5 2 2.5 3 3.5
Shan
non
inde
x
TQHPI
R² = 0.335
0.01.02.03.04.05.06.07.08.0
0 0.5 1 1.5 2 2.5
Shan
non
inde
x
TQHPI
0.01.02.03.04.05.06.07.08.0
0 0.5 1 1.5 2 2.5
Shan
non
inde
x
TQHPI
FIGURE 6A . Anterior Shannon versus anterior TQHPI (fixed appliance).
FIGURE 6C . Posterior Shannon versus posterior TQHPI (fixed appliance).
FIGURE 6B . Anterior Shannon versus anterior TQHPI (clear aligner).
FIGURE 6D. Posterior Shannon versus posterior TQHPI (clear aligner).
FIGURES 6 . Multiple regression analysis showing correlation between alpha-diversity (measured by Shannon index) and the average TQHPI score for anterior and posterior teeth.
R² = 0.0179
R² = 0.0266
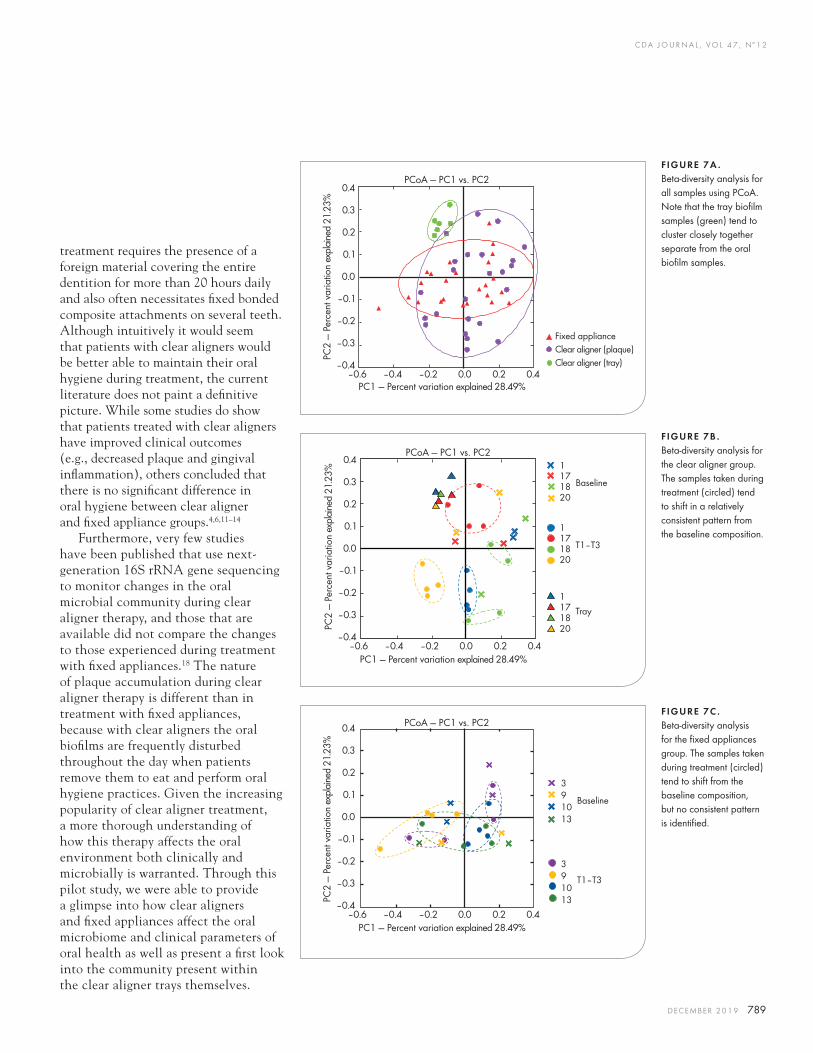
C DA J O U R N A L , V O L 4 7 , Nº 1 2
DECEMBER 2 0 1 9 789
treatment requires the presence of a foreign material covering the entire dentition for more than 20 hours daily and also often necessitates fixed bonded composite attachments on several teeth. Although intuitively it would seem that patients with clear aligners would be better able to maintain their oral hygiene during treatment, the current literature does not paint a definitive picture. While some studies do show that patients treated with clear aligners have improved clinical outcomes (e.g., decreased plaque and gingival inflammation), others concluded that there is no significant difference in oral hygiene between clear aligner and fixed appliance groups.4,6,11–14
Furthermore, very few studies have been published that use next-generation 16S rRNA gene sequencing to monitor changes in the oral microbial community during clear aligner therapy, and those that are available did not compare the changes to those experienced during treatment with fixed appliances.18 The nature of plaque accumulation during clear aligner therapy is different than in treatment with fixed appliances, because with clear aligners the oral biofilms are frequently disturbed throughout the day when patients remove them to eat and perform oral hygiene practices. Given the increasing popularity of clear aligner treatment, a more thorough understanding of how this therapy affects the oral environment both clinically and microbially is warranted. Through this pilot study, we were able to provide a glimpse into how clear aligners and fixed appliances affect the oral microbiome and clinical parameters of oral health as well as present a first look into the community present within the clear aligner trays themselves.
FIGURE 7A . Beta-diversity analysis for all samples using PCoA. Note that the tray biofilm samples (green) tend to cluster closely together separate from the oral biofilm samples.
FIGURE 7B . Beta-diversity analysis for the clear aligner group. The samples taken during treatment (circled) tend to shift in a relatively consistent pattern from the baseline composition.
FIGURE 7C . Beta-diversity analysis for the fixed appliances group. The samples taken during treatment (circled) tend to shift from the baseline composition, but no consistent pattern is identified.
0.4
0.3
0.2
0.1
0.0
–0.1
–0.2
–0.3
–0.4–0.6 –0.4 –0.2 0.0 0.2 0.4
PC2
— Pe
rcen
t var
iatio
n ex
plai
ned
21.2
3%
PC1 — Percent variation explained 28.49%
PCoA — PC1 vs. PC2
Fixed applianceClear aligner (plaque) Clear aligner (tray)
0.4
0.3
0.2
0.1
0.0
–0.1
–0.2
–0.3
–0.4–0.6 –0.4 –0.2 0.0 0.2 0.4
PC2
— Pe
rcen
t var
iatio
n ex
plai
ned
21.2
3%
PC1 — Percent variation explained 28.49%
PCoA — PC1 vs. PC211718 Baseline20
11718 T1–T320
11718
Tray
20
0.4
0.3
0.2
0.1
0.0
–0.1
–0.2
–0.3
–0.4–0.6 –0.4 –0.2 0.0 0.2 0.4
PC2
— Pe
rcen
t var
iatio
n ex
plai
ned
21.2
3%
PC1 — Percent variation explained 28.49%
PCoA — PC1 vs. PC2
3910
Baseline
13
3910
T1–T3
13

C DA J O U R N A L , V O L 4 7 , Nº 1 2
790 D E C E M B E R 2 01 9
The fixed appliances group experienced a significant mean increase in TQHPI score of 2.14 over the first six months of treatment, compared to the clear aligner mean increase of 0.79, which was borderline statistically significant (fiGure 1B). None of the increases in GI score were found to be statistically significant, although the fixed appliances group showed a higher mean increase in GI score compared to the clear aligner group (+1.04 versus +0.63, fiGure 2a). Thus, this pilot study concludes that clear aligner therapy results in less plaque buildup on teeth compared to treatment with fixed appliances. This observed lower level of plaque could be due to decreased plaque accumulation, greater ease of plaque removal or a combination of the two. However, the increased plaque levels in the fixed appliances group did not seem to affect gingival inflammation because the groups had similar GI scores.
Even though patients treated with fixed appliances had increased levels of plaque, this did not seem to have a major influence on the oral microbial community itself. Although an overall microbial shift was observed in the biofilm composition from baseline, there was noted variability from patient to patient in how much the community changed (fiGure 3). Given the small sample size in this limited pilot study, no clear or definitive pattern of how the oral community changes with these therapies was identified. The bacterial species that was most enriched in the clear aligner tray communities was Streptococcus sp_oral_taxon-058 (recently named Streptococcus oralis subsp. dentisanti), which is associated with caries-free individuals (fiGure 4).41 Gemella morbillorum oral taxon-046, a member of the normal oral microbiota, was also significantly enriched.42 The third species that was increased in the clear
aligner trays is Granulicatella elegans oral taxon-596, which is found in increased numbers in patients with active caries.43 This represents a mixture of benign and pathogenic bacteria, making it difficult at this time to draw any conclusions on whether the tray community should be considered pathogenic.
Alpha-diversity analysis showed an apparent increase in microbial diversity over the first month, which then seemed to plateau or slightly decrease back toward pretreatment levels (FIGURE 5). This finding was surprising because
decreased biofilm diversity tends to be associated with periodontal disease and increased diversity is generally a sign of periodontal health.44 However, this seemingly increased diversity may help explain in part the lack of a significant increase in GI scores in both groups.
Microbial sequencing from the anterior (central incisors) and posterior (first premolars) teeth showed no significant changes between the two communities (fiGure 3). This seems to indicate that the microbial makeup of biofilm at the gingival margin is relatively stable throughout the mouth, regardless of the tooth it is collected from. In future studies, it would be reasonable to choose one consistent location to collect plaque for sequencing, rather than multiple teeth.
Beta-diversity and taxa composition analysis revealed that the microbial makeup of the tray biofilm was significantly different from the oral biofilm communities (f iGure 7a). The microbiome present in the inner surface of the clear aligners was less diverse, which tends to be associated with periodontal disease.44 Because patients are instructed to wear the clear aligners for at least 20 hours per day, the biofilm present in the clear aligners is in contact with the teeth and gingival margin for a majority of the time during orthodontic treatment. As a whole, the tray biofilm did not seem to significantly alter the composition of the oral biofilms during the six-month treatment time period of this pilot study. However, in subject 17 the oral biofilm samples did show a shift in their composition toward the tray biofilm (f iGure 7B). The small sample size of this pilot study makes it difficult to determine whether this shift was an incidental finding or if such a shift may be observed more widely in the general patient population. A potential reason for this shift could be explained by the nature of plaque accumulation in clear aligner patients. For example, after receiving a professional dental cleaning (prophylaxis), patients place the same clear aligner into the mouth without cleaning it, which introduces the potential for re-inoculating the tooth surface with the tray community’s composition. A potential future direction for the research could be to explore whether cleaning/sterilizing clear aligner trays before reinsertion after prophylaxis affects that subject’s tooth-associated biofilm microbial composition. Further studies with a more robust sample size would provide greater insight to how the tray biofilm may affect the oral microbial community.
o r t h o d o n t i c t r e a t m e n t
There is no significant difference in the microbial communities found in biofilm collected from central incisors compared to first premolars.

C DA J O U R N A L , V O L 4 7 , Nº 1 2
DECEMBER 2 0 1 9 791
ConclusionThis study concludes that patients
treated with clear aligners experience significantly less plaque accumulation (measured by the TQHPI) on the surfaces of the teeth compared to patients treated with fixed appliances over the first six months of orthodontic therapy. There is no significant difference in the microbial communities found in biofilm collected from central incisors compared to first premolars. Orthodontic treatment with clear aligners and fixed appliances caused a shift in the oral microbial community from baseline, although the nature of this shift seems to be largely patient specific. The inner surfaces of clear aligners harbor a unique microbial community that is less diverse compared to the communities found in tooth-associated biofilms. Further studies with a larger sample size are needed to better understand the clinical and microbial changes that are induced by fixed appliances and clear aligner therapy. n
acknowledGments
This study was partially funded by the Orthodontic Faculty Development Fellowship Award from the American Association of Orthodontists Foundation to Dr. Tingxi Wu.
references
1. Proffit WR, Fields HW, Sarver DM. Contemporary Orthodontics. 5th ed. St. Louis: Mosby; 2012.2. Naranjo AA, et al. Changes in the subgingival microbiota and periodontal parameters before and three months after bracket placement. 2006 Sep;130(3):275.e17–22.3. Chenin DA, et al. Orthodontic treatment with a series of removable appliances. 2003 Sep;134(9):1232–9.4. Miethke RR, Vogt S. A comparison of the periodontal health of patients during treatment with the Invisalign system and with fixed orthodontic appliances. 2005 May;66(3):219–29.5. Levrini L, et al. Periodontal health status in patients treated with the Invisalign system and fixed orthodontic appliances: A three months clinical and microbiological evaluation. 2015 Jul–Sep;9(3):404–410. doi: 10.4103/1305-7456.163218.6. Azaripour A, et al. Braces versus Invisalign: Gingival parameters and patients’ satisfaction during treatment: A cross-sectional study. 15. doi.org/10.1186/s12903-015-0060-4.7. Karkhanechi M. et al. Periodontal status of adult patients treated with fixed buccal appliances and removable aligners over one year of active orthodontic therapy. 2013 Jan;83(1):146–51. doi: 10.2319/031212-217.1. Epub 2012 Jun 22.8. Wade WG. The oral microbiome in health and disease. 2013 Mar;69(1):137–43. doi: 10.1016/j.phrs.2012.11.006. Epub 2012 Nov 28.
9. Dewhirst FE, et al. The Human Oral Microbiome. 2010 Oct;192(19):5002–17. doi: 10.1128/JB.00542-10. Epub 2010 Jul 23.10. Kilian M, et al. The oral microbiome — an update for oral healthcare professionals. 2016 Nov 18;221(10):657–666. doi: 10.1038/sj.bdj.2016.865.11. Jiang Q, et al. Periodontal health during orthodontic treatment with clear aligners and fixed appliances. 2018 Aug;149(8):712–720.e12. doi: 10.1016/j.adaj.2018.04.010. Epub 2018 Jun 18.12. Lu H, et al. Assessment of the periodontal health status in patients undergoing orthodontic treatment with fixed appliances and Invisalign system: A meta-analysis. 2018 Mar;97(13):e0248. doi: 10.1097/MD.0000000000010248.13. Rossini G, et al. Periodontal health during clear aligners treatment: A systematic review. 2015 Oct;37(5):539–43. doi: 10.1093/ejo/cju083. Epub 2014 Dec 29.14. Chhibber A, et al. Which orthodontic appliance is best for oral hygiene? A randomized clinical trial. 2018 Feb;153(2):175–183. doi: 10.1016/j.ajodo.2017.10.009.15. Julien KC, Buschang PH, Campbell PM. Prevalence of white spot lesion formation during orthodontic treatment. 2013 Jul;83(4):641–7. doi: 10.2319/071712-584.1. Epub 2013 Jan 4.16. Ren Y, et al. Orthodontic treatment with fixed appliances and biofilm formation — a potential public health threat? 2014 Sep;18(7):1711–8. doi: 10.1007/s00784-014-1240-3. Epub 2014 Apr 13.17. Sifakakis I, et al. Salivary levels of cariogenic bacterial species during orthodontic treatment with thermoplastic aligners or fixed appliances: A prospective cohort study. 2018 Aug 1;19(1):25. doi: 10.1186/s40510-018-0230-4.18. Guo R, et al. Profiling of subgingival plaque biofilm microbiota in female adult patients with clear aligners: A three-month prospective study. 2018 Jan 2;6:e4207. doi: 10.7717/peerj.4207. eCollection 2018.19. Guo R, et al. The microbial changes in subgingival plaques of orthodontic patients: A systematic review and meta-analysis of clinical trials. 2017 Jun 2;17(1):90. doi: 10.1186/s12903-017-0378-1.20. Luca L, et al. Scanning electron microscopy analysis of the growth of dental plaque on the surfaces of removable orthodontic aligners after the use of different cleaning methods. 2015 Dec 15;7:125–31. doi: 10.2147/CCIDE.S95814. eCollection 2015.21. Lombardo L, et al. Comparative SEM analysis of nine F22 aligner cleaning strategies. 2017 Dec;18(1):26. doi: 10.1186/s40510-017-0178-9. Epub 2017 Sep 11.22. de Almeida Cardoso M, et al. Alterations in plaque accumulation and gingival inflammation promoted by treatment with self-ligating and conventional orthodontic brackets. 2015 Mar–Apr;20(2):35–41. doi: 10.1590/2176-9451.20.2.035-041.oar.23. Panagakos FS, et al. Advanced oral antibacterial/anti-inflammatory technology: A comprehensive review of the clinical benefits of a triclosan/copolymer/fluoride dentifrice. 2005;16 Suppl:S1–19.24. Turesky S, Gilmore ND, Glickman I. Reduced plaque formation by the chloromethyl analogue of victamine C. 1970 Jan;41(1):41–3.25. Cugini M, Thompson M, Warren PR. Correlations between two plaque indices in assessment of toothbrush effectiveness. 2006 Nov 1;7(5):1–9.26. Loe H, Silness J. Periodontal disease in pregnancy. I. Prevalence and severity. 1963 Dec;21:533–51.27. Benamghar L, et al. Comparison of gingival index and sulcus bleeding index as indicators of periodontal status. 1982 60(1):147–51.28. Low B, et al. Ultrastructure and morphology of biofilms on
thermoplastic orthodontic appliances in ‘fast’ and ‘slow’ plaque formers. 2011 Oct;33(5):577–83. doi: 10.1093/ejo/cjq126. Epub 2010 Dec 27.29. Addgene. Protocol — How to Create a Bacterial Glycerol Stock, 2018. www.addgene.org/protocols/create-glycerol-stock.30. Jacobs JP, et al. Microbial, metabolomic and immunologic dynamics in a relapsing genetic mouse model of colitis induced by T-synthase deficiency. 2017 Jan 2;8(1):1–16. doi: 10.1080/19490976.2016.1257469. Epub 2016 Nov 22.31. Tran Q, Pham DT, Phan V. Using 16S rRNA gene as marker to detect unknown bacteria in microbial communities. 2017 18(Suppl 14):499. doi: 10.1186/s12859-017-1901-8.32. Caporaso J, Kuczynski J, Stombaugh J, et al. QIIME allows analysis of high-throughput community sequencing data. 2010 May;7(5):335–6. doi: 10.1038/nmeth.f.303. Epub 2010 Apr 11.33. Chen T, Yu WH, Izard J, et al. The Human Oral Microbiome Database: A web accessible resource for investigating oral microbe taxonomic and genomic information. 2010 Jul 6;2010:baq013. doi: 10.1093/database/baq013.34. Faul F, et al. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. 2009 Nov;41(4):1149–60. doi: 10.3758/BRM.41.4.1149. 35. Faul F, Erdfelder E, Lang A, Buchner A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. 2007 May;39(2):175–91.36. Shapiro SS, Wilk MB. Analysis of variance test for normality (complete samples). 1965 Dec;52:591–611.37. Whittaker RJ, Willis KJ, Field R. Scale and species richness: Towards a general, hierarchical theory of species diversity. 2001 Apr;28:453–70.38. Chao A, Chiu CH, Jost L. Phylogenetic diversity measures and their decomposition: A framework based on Hill numbers. In: Pellens R, Grandcolas P, eds. Biodiversity Conservation and Phylogenetic Systematics, 14. Springer, Cham; 2016:141–72.39. Ricotta C. Of beta diversity, variance, evenness and dissimilarity. 2017 Jul(13): 7:4835–43. doi: 10.1002/ece3.2980.40. Zuur AF, Ieno EN, Smith BM. Principal coordinate analysis and non-metric multidimensional scaling. In: Analyzing Ecological Data. Springer, N.Y.: SpringerLink; 2007:259–264.41. Jensen A, Scholz CF, Kilian M. Re-evaluation of the taxonomy of the Mitis group of the genus Streptococcus based on whole genome phylogenetic analyses and proposed reclassification of Streptococcus dentisani as Streptococcus oralis subsp. dentisani comb. nov., Streptococcus tigurinus. Int J Syst Evol Microbiol 2016 Nov;66(11):4803–4820. doi: 10.1099/ijsem.0.001433. Epub 2016 Aug 17.42. Human Oral Microbiome Taxon Description: Gemella morbillorum. 2007 5/13/2009. www.homd.org/index.php?name=HOMD&view=dynamic&oraltaxonid=46.43. Peterson SN, et al. The Dental Plaque Microbiome in Health and Disease. 2013;8(3):e58487. doi: 10.1371/journal.pone.0058487. Epub 2013 Mar 8.44. Camelo-Castillo A, Novoa L, Balsa-Castro C, Blanco J, Mira A, Tomás I. Relationship between periodontitis-associated subgingival microbiota and clinical inflammation by 16S pyrosequencing. 2015 Dec;42(12):1074–82. doi: 10.1111/jcpe.12470. Epub 2015 Nov 29.
the correspondinG authors, Tingxi Wu, DMD, DMedSc, and Renate Lux, PhD, can be reached at [email protected] and [email protected].
®
ENDORSEDPROGRAMS
CDA has leveraged the strength of our large membership to deliver even more value, including resources to support you in the business side of practice. Endorsed Programs provide money-saving solutions from vendors that have been vetted by CDA.
cda.org/endorsedprograms
STRENGTH.SAVINGS.CONFIDENCE.
Grow your patient base, sustain your current base and manage your practice’s reputation with expert consulting and a broad range of marketing services. As a CDA member, you benefit from free assessments and discounted start-up costs from WEO Media.
WEO’s consultants apply the unique needs and goals of practicesof every size in developing custom marketing plans. Services include responsive websites, premium SEO, PPC, reviewgeneration, social media, video and more.
F E AT U R E D E N D O R S E D P R O G R A M
C DA J O U R N A L , V O L 4 7 , Nº 1 2
DECEMBER 2 0 1 9 793
10-Year Institutional Retrospective Case-Control Study of Medication-Related Osteonecrosis of the JawPardis Barati Mahvar, BSc; Amna Imran, DDS, MPhil, BDS; Reyes Enciso, PhD; Andrew Sanapanya, BS; Mohammad Khalifeh, DDS, MS; Parish P. Sedghizadeh, DDS, MS; and Laurel Henderson, DDS, MS
a b s t r ac t The connection between antiresorptive therapy (ART) and medication-related osteonecrosis of the jaw (MRONJ) has been studied extensively in the literature but limited by methodological challenges. This retrospective case-control study evaluates the connection between ART and MRONJ over a 10-year period. We identified 223 MRONJ patients and compared them to 615 non-MRONJ patients taking ART. Observational population studies can help inform dental practitioners of risk assessment and aid in preventing morbidity in the dental setting.
AUTHORS
Pardis Barati Mahvar, BS, is a fourth-year dental student at the Herman Ostrow School of Dentistry of USC.Conflict of Interest Disclosure: None reported.
Amna Imran, DDS, MPhil, BDS, is a graduate of the Herman Ostrow School of Dentistry of USC.Conflict of Interest Disclosure: None reported.
Reyes Enciso, PhD, is a full-time associate professor (instructional) at the division of dental public health and pediatric dentistry of USC. Conflict of Interest Disclosure: None reported.
o s t e o n e c r o s i s
Andrew Sanapanya, BS, is a business data analyst at the Herman Ostrow School of Dentistry of USC.Conflict of Interest Disclosure: None reported.
Mohammad Khalifeh, DDS, MS, is part-time faculty at the Herman Ostrow School of Dentistry of USC.Conflict of Interest Disclosure: None reported.
Bisphosphonate (BP) and denosumab (Dmab) medications are used as antiresorptive therapy (ART) to treat specific bone conditions including osteoporosis,
metastatic bony lesions and multiple myeloma. Prescriptions for ART, specifically oral BPs, have increased steadily since 1988. According to a 2004 review of medical office visits for osteoporosis, out of 6.3 million office visits, nearly 73% included a prescription written for BP.1 Long-term use of ART is associated with several potential adverse effects including medication-related osteonecrosis of the jaw (MRONJ), atrial fibrillation, esophageal cancer, musculoskeletal pain and atypical femoral fractures without clear causal relationship.2 MRONJ is a condition defined as exposed or unexposed necrotic bone in the
Parish P. Sedghizadeh, DDS, MS, is an associate professor of clinical dentistry at the Herman Ostrow School of Dentistry of USC and director of the USC Center for Biofilms research laboratory. He serves as the section chair for diagnostic sciences and is the director of the hybrid oral pathology and radiology program.Conflict of Interest Disclosure: None reported.
Laurel Henderson, DDS, MS, is a recent graduate of the USC orofacial pain and oral medicine advanced specialty program and is currently training in oral and maxillofacial pathology at the Northwell Health Long Island Jewish Medical Center.Conflict of Interest Disclosure: None reported.
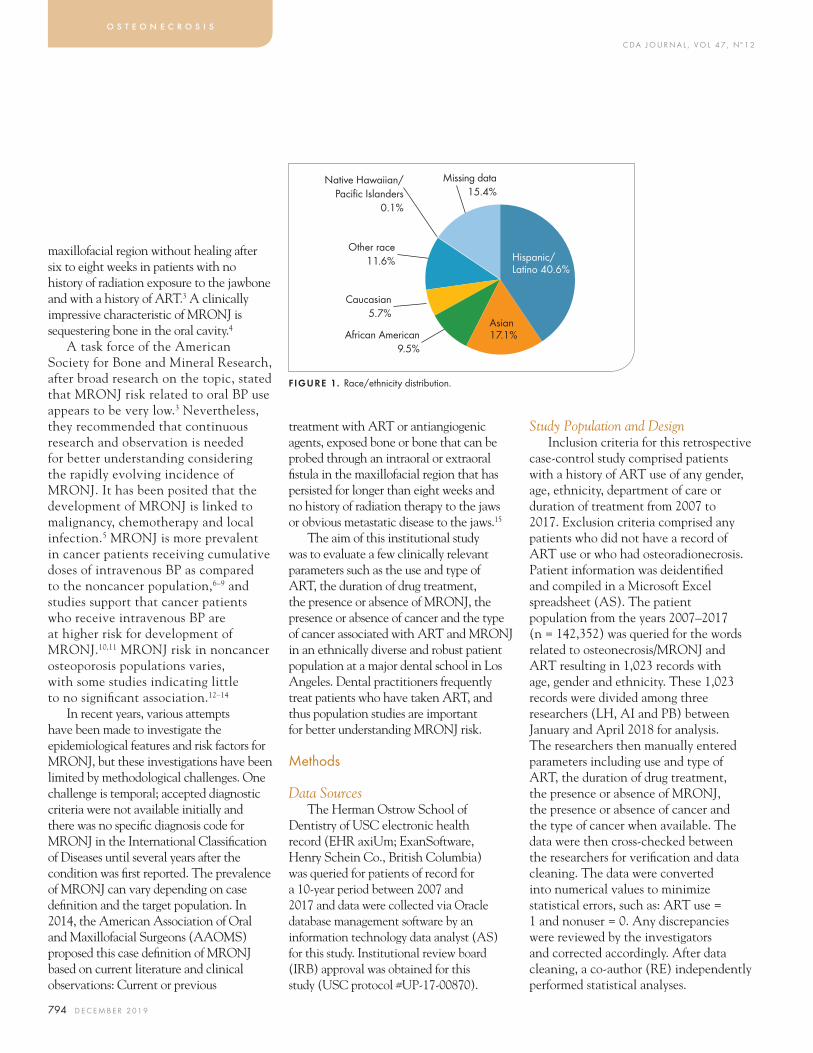
C DA J O U R N A L , V O L 4 7 , Nº 1 2
794 D E C E M B E R 2 01 9
maxillofacial region without healing after six to eight weeks in patients with no history of radiation exposure to the jawbone and with a history of ART.3 A clinically impressive characteristic of MRONJ is sequestering bone in the oral cavity.4
A task force of the American Society for Bone and Mineral Research, after broad research on the topic, stated that MRONJ risk related to oral BP use appears to be very low.3 Nevertheless, they recommended that continuous research and observation is needed for better understanding considering the rapidly evolving incidence of MRONJ. It has been posited that the development of MRONJ is linked to malignancy, chemotherapy and local infection.5 MRONJ is more prevalent in cancer patients receiving cumulative doses of intravenous BP as compared to the noncancer population,6–9 and studies support that cancer patients who receive intravenous BP are at higher risk for development of MRONJ.10,11 MRONJ risk in noncancer osteoporosis populations varies, with some studies indicating little to no significant association.12–14
In recent years, various attempts have been made to investigate the epidemiological features and risk factors for MRONJ, but these investigations have been limited by methodological challenges. One challenge is temporal; accepted diagnostic criteria were not available initially and there was no specific diagnosis code for MRONJ in the International Classification of Diseases until several years after the condition was first reported. The prevalence of MRONJ can vary depending on case definition and the target population. In 2014, the American Association of Oral and Maxillofacial Surgeons (AAOMS) proposed this case definition of MRONJ based on current literature and clinical observations: Current or previous
treatment with ART or antiangiogenic agents, exposed bone or bone that can be probed through an intraoral or extraoral fistula in the maxillofacial region that has persisted for longer than eight weeks and no history of radiation therapy to the jaws or obvious metastatic disease to the jaws.15
The aim of this institutional study was to evaluate a few clinically relevant parameters such as the use and type of ART, the duration of drug treatment, the presence or absence of MRONJ, the presence or absence of cancer and the type of cancer associated with ART and MRONJ in an ethnically diverse and robust patient population at a major dental school in Los Angeles. Dental practitioners frequently treat patients who have taken ART, and thus population studies are important for better understanding MRONJ risk.
Methods
Data SourcesThe Herman Ostrow School of
Dentistry of USC electronic health record (EHR axiUm; ExanSoftware, Henry Schein Co., British Columbia) was queried for patients of record for a 10-year period between 2007 and 2017 and data were collected via Oracle database management software by an information technology data analyst (AS) for this study. Institutional review board (IRB) approval was obtained for this study (USC protocol #UP-17-00870).
Study Population and DesignInclusion criteria for this retrospective
case-control study comprised patients with a history of ART use of any gender, age, ethnicity, department of care or duration of treatment from 2007 to 2017. Exclusion criteria comprised any patients who did not have a record of ART use or who had osteoradionecrosis. Patient information was deidentified and compiled in a Microsoft Excel spreadsheet (AS). The patient population from the years 2007–2017 (n = 142,352) was queried for the words related to osteonecrosis/MRONJ and ART resulting in 1,023 records with age, gender and ethnicity. These 1,023 records were divided among three researchers (LH, AI and PB) between January and April 2018 for analysis. The researchers then manually entered parameters including use and type of ART, the duration of drug treatment, the presence or absence of MRONJ, the presence or absence of cancer and the type of cancer when available. The data were then cross-checked between the researchers for verification and data cleaning. The data were converted into numerical values to minimize statistical errors, such as: ART use = 1 and nonuser = 0. Any discrepancies were reviewed by the investigators and corrected accordingly. After data cleaning, a co-author (RE) independently performed statistical analyses.
o s t e o n e c r o s i s
FIGURE 1. Race/ethnicity distribution.
African American 9.5%
Caucasian5.7%
Other race 11.6%
Missing data 15.4%
Native Hawaiian/Pacific Islanders
0.1%
Hispanic/ Latino 40.6%
Asian 17.1%
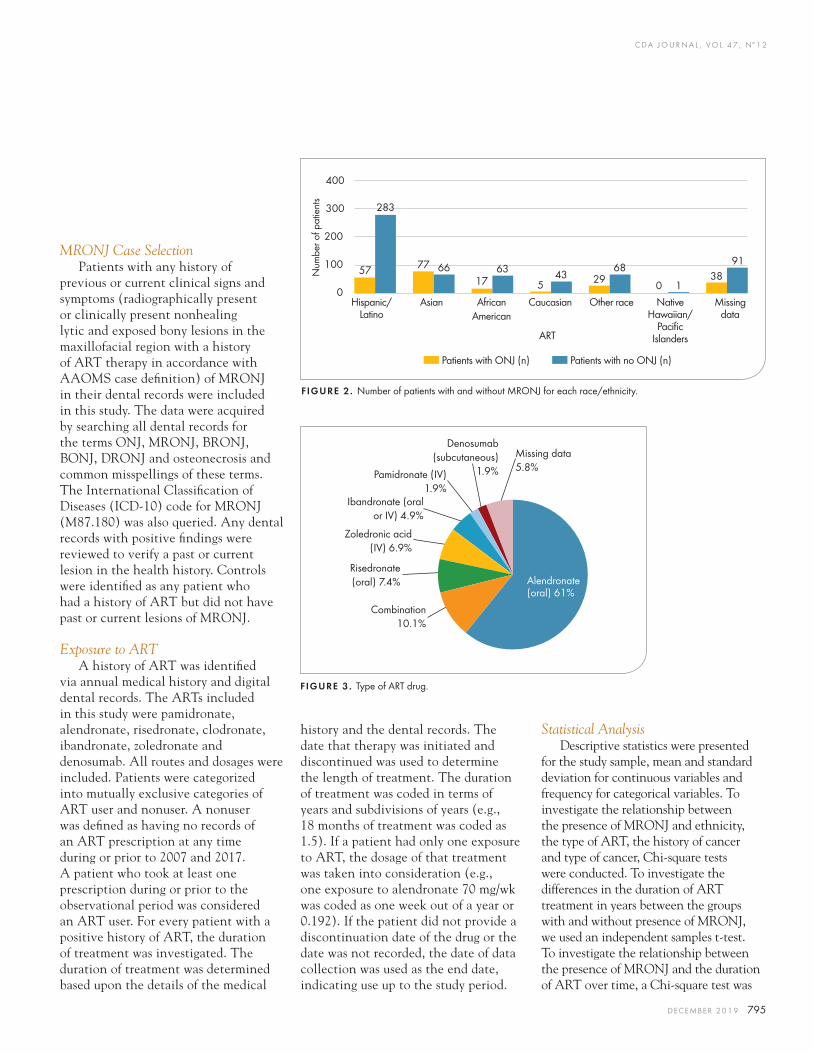
C DA J O U R N A L , V O L 4 7 , Nº 1 2
DECEMBER 2 0 1 9 795
MRONJ Case SelectionPatients with any history of
previous or current clinical signs and symptoms (radiographically present or clinically present nonhealing lytic and exposed bony lesions in the maxillofacial region with a history of ART therapy in accordance with AAOMS case definition) of MRONJ in their dental records were included in this study. The data were acquired by searching all dental records for the terms ONJ, MRONJ, BRONJ, BONJ, DRONJ and osteonecrosis and common misspellings of these terms. The International Classification of Diseases (ICD-10) code for MRONJ (M87.180) was also queried. Any dental records with positive findings were reviewed to verify a past or current lesion in the health history. Controls were identified as any patient who had a history of ART but did not have past or current lesions of MRONJ.
Exposure to ARTA history of ART was identified
via annual medical history and digital dental records. The ARTs included in this study were pamidronate, alendronate, risedronate, clodronate, ibandronate, zoledronate and denosumab. All routes and dosages were included. Patients were categorized into mutually exclusive categories of ART user and nonuser. A nonuser was defined as having no records of an ART prescription at any time during or prior to 2007 and 2017. A patient who took at least one prescription during or prior to the observational period was considered an ART user. For every patient with a positive history of ART, the duration of treatment was investigated. The duration of treatment was determined based upon the details of the medical
history and the dental records. The date that therapy was initiated and discontinued was used to determine the length of treatment. The duration of treatment was coded in terms of years and subdivisions of years (e.g., 18 months of treatment was coded as 1.5). If a patient had only one exposure to ART, the dosage of that treatment was taken into consideration (e.g., one exposure to alendronate 70 mg/wk was coded as one week out of a year or 0.192). If the patient did not provide a discontinuation date of the drug or the date was not recorded, the date of data collection was used as the end date, indicating use up to the study period.
Statistical AnalysisDescriptive statistics were presented
for the study sample, mean and standard deviation for continuous variables and frequency for categorical variables. To investigate the relationship between the presence of MRONJ and ethnicity, the type of ART, the history of cancer and type of cancer, Chi-square tests were conducted. To investigate the differences in the duration of ART treatment in years between the groups with and without presence of MRONJ, we used an independent samples t-test. To investigate the relationship between the presence of MRONJ and the duration of ART over time, a Chi-square test was
FIGURE 3 . Type of ART drug.
Alendronate (oral) 61%
Combination10.1%
Risedronate (oral) 7.4%
Zoledronic acid (IV) 6.9%
Ibandronate (oral or IV) 4.9%
Pamidronate (IV) 1.9%
Denosumab (subcutaneous)
1.9%
Missing data 5.8%
400
300
200
100
0
Num
ber o
f pat
ient
s
57 77 6617
635
43 2968
138
91
0
283
Hispanic/Latino
Asian African American
Caucasian Other race Native Hawaiian/
Pacific Islanders
Missing data
ART
nn Patients with ONJ (n) nn Patients with no ONJ (n)
FIGURE 2. Number of patients with and without MRONJ for each race/ethnicity.
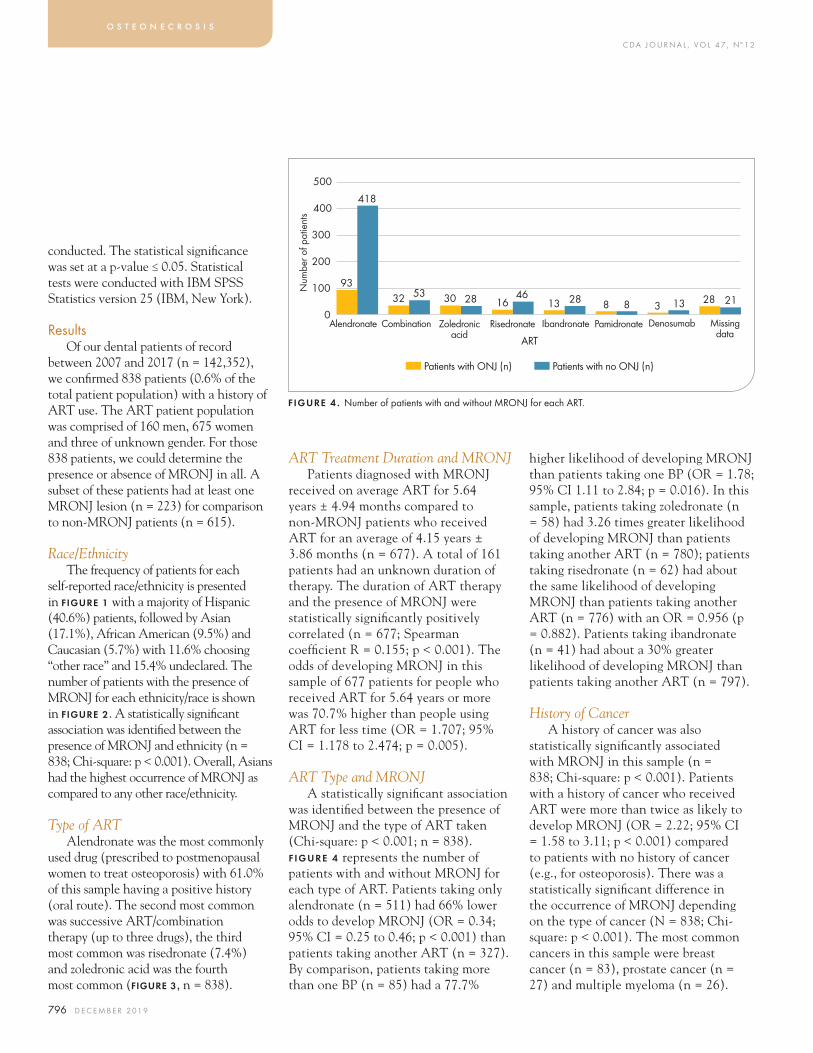
C DA J O U R N A L , V O L 4 7 , Nº 1 2
796 D E C E M B E R 2 01 9
conducted. The statistical significance was set at a p-value ≤ 0.05. Statistical tests were conducted with IBM SPSS Statistics version 25 (IBM, New York).
ResultsOf our dental patients of record
between 2007 and 2017 (n = 142,352), we confirmed 838 patients (0.6% of the total patient population) with a history of ART use. The ART patient population was comprised of 160 men, 675 women and three of unknown gender. For those 838 patients, we could determine the presence or absence of MRONJ in all. A subset of these patients had at least one MRONJ lesion (n = 223) for comparison to non-MRONJ patients (n = 615).
Race/EthnicityThe frequency of patients for each
self-reported race/ethnicity is presented in fiGure 1 with a majority of Hispanic (40.6%) patients, followed by Asian (17.1%), African American (9.5%) and Caucasian (5.7%) with 11.6% choosing “other race” and 15.4% undeclared. The number of patients with the presence of MRONJ for each ethnicity/race is shown in fiGure 2. A statistically significant association was identified between the presence of MRONJ and ethnicity (n = 838; Chi-square: p < 0.001). Overall, Asians had the highest occurrence of MRONJ as compared to any other race/ethnicity.
Type of ARTAlendronate was the most commonly
used drug (prescribed to postmenopausal women to treat osteoporosis) with 61.0% of this sample having a positive history (oral route). The second most common was successive ART/combination therapy (up to three drugs), the third most common was risedronate (7.4%) and zoledronic acid was the fourth most common (fiGure 3, n = 838).
ART Treatment Duration and MRONJPatients diagnosed with MRONJ
received on average ART for 5.64 years ± 4.94 months compared to non-MRONJ patients who received ART for an average of 4.15 years ± 3.86 months (n = 677). A total of 161 patients had an unknown duration of therapy. The duration of ART therapy and the presence of MRONJ were statistically significantly positively correlated (n = 677; Spearman coefficient R = 0.155; p < 0.001). The odds of developing MRONJ in this sample of 677 patients for people who received ART for 5.64 years or more was 70.7% higher than people using ART for less time (OR = 1.707; 95% CI = 1.178 to 2.474; p = 0.005).
ART Type and MRONJA statistically significant association
was identified between the presence of MRONJ and the type of ART taken (Chi-square: p < 0.001; n = 838). F IGURE 4 represents the number of patients with and without MRONJ for each type of ART. Patients taking only alendronate (n = 511) had 66% lower odds to develop MRONJ (OR = 0.34; 95% CI = 0.25 to 0.46; p < 0.001) than patients taking another ART (n = 327). By comparison, patients taking more than one BP (n = 85) had a 77.7%
higher likelihood of developing MRONJ than patients taking one BP (OR = 1.78; 95% CI 1.11 to 2.84; p = 0.016). In this sample, patients taking zoledronate (n = 58) had 3.26 times greater likelihood of developing MRONJ than patients taking another ART (n = 780); patients taking risedronate (n = 62) had about the same likelihood of developing MRONJ than patients taking another ART (n = 776) with an OR = 0.956 (p = 0.882). Patients taking ibandronate (n = 41) had about a 30% greater likelihood of developing MRONJ than patients taking another ART (n = 797).
History of CancerA history of cancer was also
statistically significantly associated with MRONJ in this sample (n = 838; Chi-square: p < 0.001). Patients with a history of cancer who received ART were more than twice as likely to develop MRONJ (OR = 2.22; 95% CI = 1.58 to 3.11; p < 0.001) compared to patients with no history of cancer (e.g., for osteoporosis). There was a statistically significant difference in the occurrence of MRONJ depending on the type of cancer (N = 838; Chi-square: p < 0.001). The most common cancers in this sample were breast cancer (n = 83), prostate cancer (n = 27) and multiple myeloma (n = 26).
o s t e o n e c r o s i s
FIGURE 4 . Number of patients with and without MRONJ for each ART.
500
400
300
200
100
0N
umbe
r of p
atie
nts
RisedronateAlendronate Ibandronate Pamidronate Denosumab Missing data
Combination Zoledronic acid ART
nn Patients with ONJ (n) nn Patients with no ONJ (n)
93
418
32 53 30 28 1646
13 28 8 8 3 13 28 21
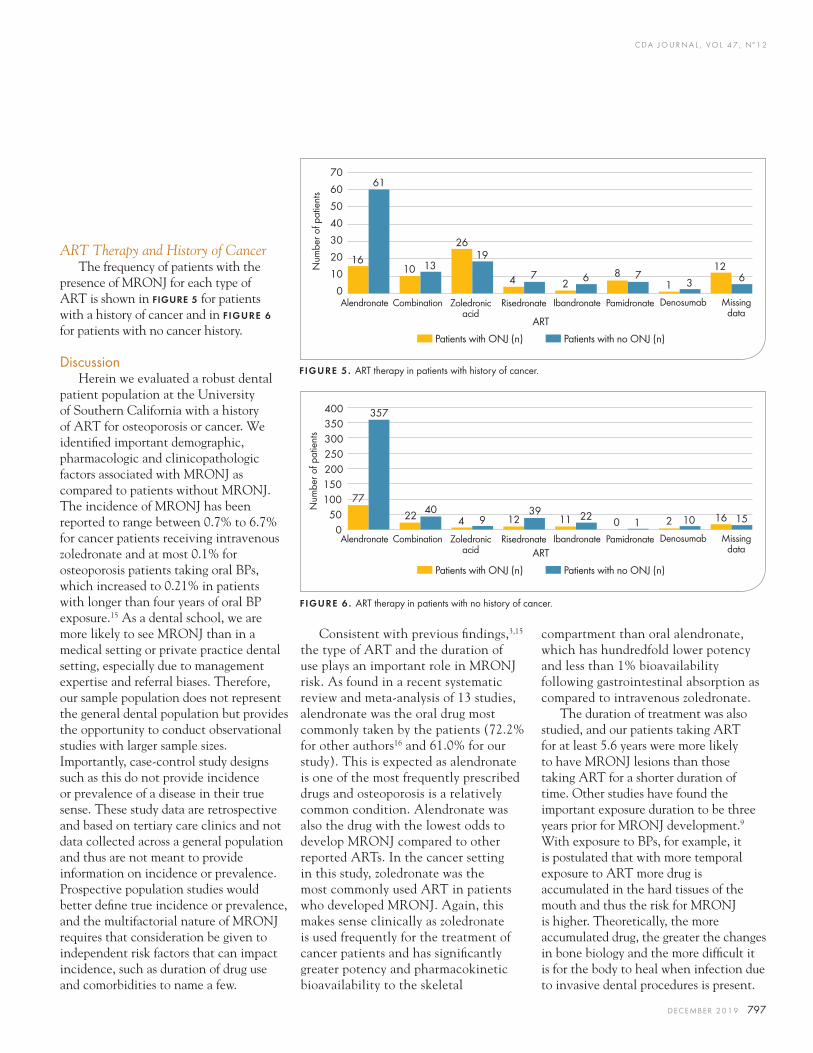
C DA J O U R N A L , V O L 4 7 , Nº 1 2
DECEMBER 2 0 1 9 797
ART Therapy and History of CancerThe frequency of patients with the
presence of MRONJ for each type of ART is shown in fiGure 5 for patients with a history of cancer and in FIGURE 6 for patients with no cancer history.
DiscussionHerein we evaluated a robust dental
patient population at the University of Southern California with a history of ART for osteoporosis or cancer. We identified important demographic, pharmacologic and clinicopathologic factors associated with MRONJ as compared to patients without MRONJ. The incidence of MRONJ has been reported to range between 0.7% to 6.7% for cancer patients receiving intravenous zoledronate and at most 0.1% for osteoporosis patients taking oral BPs, which increased to 0.21% in patients with longer than four years of oral BP exposure.15 As a dental school, we are more likely to see MRONJ than in a medical setting or private practice dental setting, especially due to management expertise and referral biases. Therefore, our sample population does not represent the general dental population but provides the opportunity to conduct observational studies with larger sample sizes. Importantly, case-control study designs such as this do not provide incidence or prevalence of a disease in their true sense. These study data are retrospective and based on tertiary care clinics and not data collected across a general population and thus are not meant to provide information on incidence or prevalence. Prospective population studies would better define true incidence or prevalence, and the multifactorial nature of MRONJ requires that consideration be given to independent risk factors that can impact incidence, such as duration of drug use and comorbidities to name a few.
Consistent with previous findings,3,15 the type of ART and the duration of use plays an important role in MRONJ risk. As found in a recent systematic review and meta-analysis of 13 studies, alendronate was the oral drug most commonly taken by the patients (72.2% for other authors16 and 61.0% for our study). This is expected as alendronate is one of the most frequently prescribed drugs and osteoporosis is a relatively common condition. Alendronate was also the drug with the lowest odds to develop MRONJ compared to other reported ARTs. In the cancer setting in this study, zoledronate was the most commonly used ART in patients who developed MRONJ. Again, this makes sense clinically as zoledronate is used frequently for the treatment of cancer patients and has significantly greater potency and pharmacokinetic bioavailability to the skeletal
compartment than oral alendronate, which has hundredfold lower potency and less than 1% bioavailability following gastrointestinal absorption as compared to intravenous zoledronate.
The duration of treatment was also studied, and our patients taking ART for at least 5.6 years were more likely to have MRONJ lesions than those taking ART for a shorter duration of time. Other studies have found the important exposure duration to be three years prior for MRONJ development.9 With exposure to BPs, for example, it is postulated that with more temporal exposure to ART more drug is accumulated in the hard tissues of the mouth and thus the risk for MRONJ is higher. Theoretically, the more accumulated drug, the greater the changes in bone biology and the more difficult it is for the body to heal when infection due to invasive dental procedures is present.
FIGURE 5. ART therapy in patients with history of cancer.
FIGURE 6 . ART therapy in patients with no history of cancer.
0
10
20
30
40
50
60
70
Num
ber o
f pat
ient
sRisedronateAlendronate Ibandronate Pamidronate Denosumab Missing
dataCombination Zoledronic
acid ART
nn Patients with ONJ (n) nn Patients with no ONJ (n)
1610
26
4 28
1
12
61
1319
7 6 73 6
400350300250200150100
500
Num
ber o
f pat
ient
s
RisedronateAlendronate Ibandronate Pamidronate Denosumab Missing data
Combination Zoledronic acid ART
nn Patients with ONJ (n) nn Patients with no ONJ (n)
77
22 4 12 11 0 2 16
357
409
39 22 1 10 15

C DA J O U R N A L , V O L 4 7 , Nº 1 2
798 D E C E M B E R 2 01 9
This study found an association between the use of ART for cancer therapy and MRONJ lesions. Cancer has been shown to be an independent risk factor for MRONJ.17–19 This connection could be due to the immunocompromised state associated with cancer, which makes resisting oral infections and maintaining ideal oral hygiene a challenge. Our study found that breast cancer, prostate cancer and multiple myeloma were the types of cancers most commonly presenting at our university dental school.
A significant limitation of this study, like many retrospective studies, is the heterogeneity of the reporting of the data by clinical practitioners. There were a number of patient records with no specific cancer name or no duration of treatment entered in the chart. Also, we are a major referral center for MRONJ cases in the Los Angeles area, thus we have sampling and referral bias. This makes for inflated values of MRONJ occurrence that are not generalizable to other populations. Further, certain Asian populations have greater risk for MRONJ for yet unknown reasons that may include genetic factors or ART overtreatment. Accordingly, we have a large Asian population in Los Angeles and in our study, thus further inflating MRONJ occurrence. Overall, our MRONJ occurrence and target population may not be representative of the overall occurrence in different populations at large and so our results should not be generalized to other populations. Finally, not all patients taking ART will report this in a health or dental record. This will lead to underestimated numbers of controls, again relatively inflating the number of disease cases. There are many reasons for this, including patients not remembering
that they are taking one of these medications given the weekly or monthly dosing, for example, in the osteoporosis setting. In other cases, patients do not know what a BP or ART is even if they are taking it, particularly with the different ethnicities and languages represented here, and thus they do not always self-report taking such a medication. Additionally, the duration of therapy varied from 0.3 to 10 years, explaining the large standard deviation of our results in this context.
In this study, we did not report the average age of patients because we found these values to be higher than previous reports due to the nature of our study query and our electronic health record, axiUm. This increased age variable could intrinsically make sense, as those of more advanced age could have greater cumulative exposure to ART and thus potentially more adverse effects associated with therapy. Unfortunately, this variable is inaccurate in our study due to a common confounding factor associated with retrospective studies utilizing databases like axiUm. The axiUm software keeps patient records that are not updated with the vitality of the patient; thus, there are likely some patients who are deceased who have been included in this study but their death date is not included in axiUm charting, creating a bias for older age. This type of variable and discrepancy could be overcome if medical records are merged with dental records. Finally, retrospective studies such as this naturally suffer some degree of observational bias and confounders given the multifactorial nature of MRONJ development. These aforementioned factors highlight study limitations, some of which are relatively common and inherent to MRONJ investigations in this context.
ConclusionsThe findings in this study
characterize some of the factors associated with MRONJ in our patient population at the Herman Ostrow School of Dentistry of USC. Those at highest risk are oncologic as compared to osteoporotic patients and Asians, and long-term use increases risk for MRONJ in the ART population. The data are important for clinicians in order for them to better understand what factors are associated with MRONJ development in this patient population and also to identify which patients could benefit from risk reduction and prevention protocols prior to invasive oral surgical procedures, as one example. n
references
1. Stafford RS, Drieling RL, Hersh AL. National trends in osteoporosis visits and osteoporosis treatment, 1988–2003. Arch Intern Med 2004 Jul 26;164:1525–30.2. Watts NB, Diab DL. Long-term use of bisphosphonates in osteoporosis. J Clin Endocrinol Metab 2010 Apr;95(4):1555–65. doi: 10.1210/jc.2009-1947. Epub 2010 Feb 19.3. Khosla S, Burr D, Cauley J, Dempster DW, Ebeling PR, Felsenberg D, Gagel RF, Gilsanz V, Guise T, Koka S, et al. Bisphosphonate-associated osteonecrosis of the jaw: Report of a task force of the American Society for Bone and Mineral Research. J Bone Miner Res 2007 Oct;22:1479–91.4. Silverman SL, Landesberg R. Osteonecrosis of the jaw and the role of bisphosphonates: A critical review. Am J Med 2009 Feb;122(2 Suppl):S33–45. doi: 10.1016/j.amjmed.2008.12.005.5. Khan AA, Sandor GK, Dore E, Morrison AD, Alsahli M, Amin F, et al. Bisphosphonate associated osteonecrosis of the jaw. J Rheumatol 2008 Jul;35(7):1391–7. Epub 2008 Jun 1.6. Marx RE. Pamidronate (Aredia) and zoledronate (Zometa) induced avascular necrosis of the jaws: A growing epidemic. J Oral Maxillofac Surg 2003 Sep;61(9):1115–17.7. Woo SB, Hellstein JW, Kalmar JR. Systematic review: Bisphosphonates and osteonecrosis of the jaws. Ann Intern Med 2006 May 16;144 (10):753–61.8. Ruggiero SL, Mehrotra B, Rosenberg TJ, Engroff SL. Osteonecrosis of the jaws associated with the use of bisphosphonates: A review of 63 cases. J Oral Maxillofac Surg 2004 May;62:527–34.9. Marx RE, Sawatari Y, Fortin M, Broumand V. Bisphosphonate-induced exposed bone (osteonecrosis/osteopetrosis) of the jaws: Risk factors, recognition, prevention and treatment. J Oral Maxillofac Surg 2005 Nov;63(11):1567–75.
o s t e o n e c r o s i s
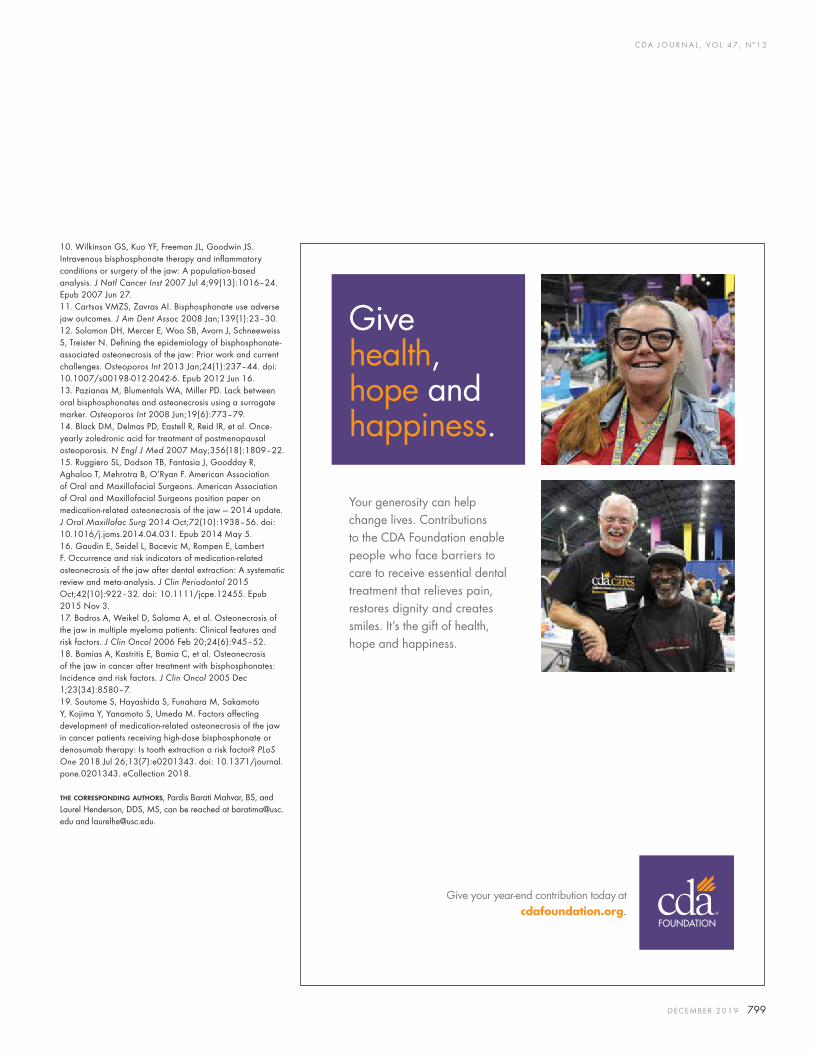
C DA J O U R N A L , V O L 4 7 , Nº 1 2
DECEMBER 2 0 1 9 799
10. Wilkinson GS, Kuo YF, Freeman JL, Goodwin JS. Intravenous bisphosphonate therapy and inflammatory conditions or surgery of the jaw: A population-based analysis. J Natl Cancer Inst 2007 Jul 4;99(13):1016–24. Epub 2007 Jun 27.11. Cartsos VMZS, Zavras AI. Bisphosphonate use adverse jaw outcomes. J Am Dent Assoc 2008 Jan;139(1):23–30.12. Solomon DH, Mercer E, Woo SB, Avorn J, Schneeweiss S, Treister N. Defining the epidemiology of bisphosphonate-associated osteonecrosis of the jaw: Prior work and current challenges. Osteoporos Int 2013 Jan;24(1):237–44. doi: 10.1007/s00198-012-2042-6. Epub 2012 Jun 16.13. Pazianas M, Blumentals WA, Miller PD. Lack between oral bisphosphonates and osteonecrosis using a surrogate marker. Osteoporos Int 2008 Jun;19(6):773–79.14. Black DM, Delmas PD, Eastell R, Reid IR, et al. Once-yearly zoledronic acid for treatment of postmenopausal osteoporosis. N Engl J Med 2007 May;356(18):1809–22.15. Ruggiero SL, Dodson TB, Fantasia J, Goodday R, Aghaloo T, Mehrotra B, O’Ryan F. American Association of Oral and Maxillofacial Surgeons. American Association of Oral and Maxillofacial Surgeons position paper on medication-related osteonecrosis of the jaw — 2014 update. J Oral Maxillofac Surg 2014 Oct;72(10):1938–56. doi: 10.1016/j.joms.2014.04.031. Epub 2014 May 5.16. Gaudin E, Seidel L, Bacevic M, Rompen E, Lambert F. Occurrence and risk indicators of medication-related osteonecrosis of the jaw after dental extraction: A systematic review and meta-analysis. J Clin Periodontol 2015 Oct;42(10):922–32. doi: 10.1111/jcpe.12455. Epub 2015 Nov 3.17. Badros A, Weikel D, Salama A, et al. Osteonecrosis of the jaw in multiple myeloma patients: Clinical features and risk factors. J Clin Oncol 2006 Feb 20;24(6):945–52.18. Bamias A, Kastritis E, Bamia C, et al. Osteonecrosis of the jaw in cancer after treatment with bisphosphonates: Incidence and risk factors. J Clin Oncol 2005 Dec 1;23(34):8580–7.19. Soutome S, Hayashida S, Funahara M, Sakamoto Y, Kojima Y, Yanamoto S, Umeda M. Factors affecting development of medication-related osteonecrosis of the jaw in cancer patients receiving high-dose bisphosphonate or denosumab therapy: Is tooth extraction a risk factor? PLoS One 2018 Jul 26;13(7):e0201343. doi: 10.1371/journal.pone.0201343. eCollection 2018.
the correspondinG authors, Pardis Barati Mahvar, BS, and Laurel Henderson, DDS, MS, can be reached at [email protected] and [email protected].
Your generosity can help change lives. Contributions to the CDA Foundation enable people who face barriers to care to receive essential dental treatment that relieves pain, restores dignity and creates smiles. It’s the gift of health, hope and happiness.
Give health, hope and happiness.
Give your year-end contribution today at cdafoundation.org.

Enroll at 4MInstitute.com OR contact us at 562-294-5200 or [email protected] to request to be enrolled.
3918 Long Beach Blvd • Suite 200 • Long Beach • CA • 90807
Specialized Training Designed to Give DENTISTS Cutting-Edge Skills TRANSFORM
YOUR PRACTICE
Inquire about SCHOLARSHIPS up to $5,000 at [email protected] OR SAVE $500 off any course
with CODE SALES500 Expires 12/31/19
THE WOW EXPERIENCE - SALES PROCESS AND MARKETING FOR DENTISTS $995 and $495 for 2nd Team Member
Learn the art, science, and steps to attracting, selling, and keeping new patients from customer service guru Dr. James Roman, digital marketing architect Todd Whitaker, and social media maven Julieanne O’Connor. This fun, transformative day will revolutionize how you approach marketing your practice, training your team, and delivering a “Wow!” experience your patients will love.
February 8, 2020 • Delighting Your Patients from First Contact to Treatment Acceptance
ALL-ON-4® IMPLANT SOLUTION COURSE I$9995 ($2500 deposit required to hold spot)
Three days of hands on/live surgery. You will acquire the skills necessary to execute $20,000 – $50,000 cases. In addition to the clinical, you will learn powerful marketing strategies.
Choose your preferred dates: January 24 – 26, 2020, OR July 31 – August 2, 2020
PRF/PHLEBOTOMY TRAINING - $1299 (Ask about early bird enrollment specials)
Incorporating PRF (CGF) & Phlebotomy into your practice. 1 Day Blood Drawing Certification.
February 29, 2020 OR August 29, 2020 • with Dr. Kayvon Javid DDS, DICOI, FCII, AFWCLI, CPT 1

C DA J O U R N A L , V O L 4 7 , Nº 1 2
DECEMBER 2 0 1 9 801
AUTHORS
John Ngo, BS, is a third-year dental student at the University of California, Los Angeles, School of Dentistry. He received his undergraduate degree in biological sciences from UC Irvine. His research in the Nishimura Lab at the Weintraub Center for Reconstructive Biotechnology focuses on the circadian rhythm and its effect on wound healing.Conflict of Interest Disclosure: None reported.
Circadian Behaviors of Oral and Skin FibroblastsJohn Ngo, BS; Hodaka Sasaki, DDS, PhD; and Ichiro Nishimura, DDS, DMSc, DMD
a b s t r ac t One of the key factors in oral and skin wound healing is fibroblast behaviors. This study reports fibroblasts derived from mouse palatal mucosa and dorsal skin. Oral fibroblasts exhibited robust expression of core clock genes as compared to skin fibroblasts and a clear circadian pattern in the cell migration and floating collagen gel contraction in vitro. Our study suggests that oral wound healing involving fibroblast repopulation and contraction may follow a diurnal cycle.
Hodaka Sasaki, DDS, PhD, is a lecturer in the department of oral and maxillofacial implantology at Tokyo Dental College. He previously performed research as a visiting assistant project scientist in the Nishimura Lab at the Weintraub Center for Reconstructive Biotechnology.Conflict of Interest Disclosure: None reported.
Ichiro Nishimura, DDS, DMSc, DMD, is a professor of dentistry and bioengineering at the University of California, Los Angeles, and the founding director of the Weintraub Center for Reconstructive Biotechnology at the UCLA School of Dentistry.Conflict of Interest Disclosure: None reported.
The skin and oral barriers in humans are comprised of an overlying epithelial layer and an underlying connective tissue. In response to injury,
however, oral mucosa presents better wound healing than skin, resulting in minimal or practically no scarring.1,2 One of the key differentiating factors in the environment that account for the accelerated healing observed in the oral mucosa is the presence of saliva. Saliva contains multiple key growth factors and cytokines, including epidermal growth factor (EGF) and transforming growth factor (TGF-a).3,4 Cell migration and proliferation of oral epithelial cells are increased in the presence of EGF-containing saliva and are decreased upon exposure to EGF-inhibiting factors.3 Moisture balance provided by saliva is also a critical facilitator of the wound healing process.5 While environmental factors of the oral cavity contribute to better wound healing, it must be noted that skin transplanted into the oral cavity retains its original behaviors such
c i r c a d i a n b e h a v i o r s
as keratin production and proliferation patterns.6 Therefore, intrinsic factors of oral barrier tissue and, in particular, oral fibroblasts may affect wound healing.
We propose that the intrinsic factors regulating oral fibroblast behavior may include the molecular clock mechanism, which has been shown to control wound healing.7,8 The central circadian rhythm is maintained in the suprachiasmatic nucleus (SCN), a region in the hypothalamus responsible for regulating physiological homeostasis.9 The molecular clock mechanism consists of a transcriptional/translational feedback loop orchestrated by clock genes10 (fiGure 1). Circadian Locomotor Output Cycles Kaput (Clock) and Brain and Muscle Arnt-Like protein-1 (Bmal1) perform as positive feedback signals. The heterodimeric transcriptional factors CLOCK and BMAL1 activate transcription of Period (Per) and Cryptochrome (Cry) genes.11,12 Their protein products form PER-CRY heterodimers, which in turn inhibit the transcriptional activation by CLOCK and BMAL1.13 These circadian rhythm genes
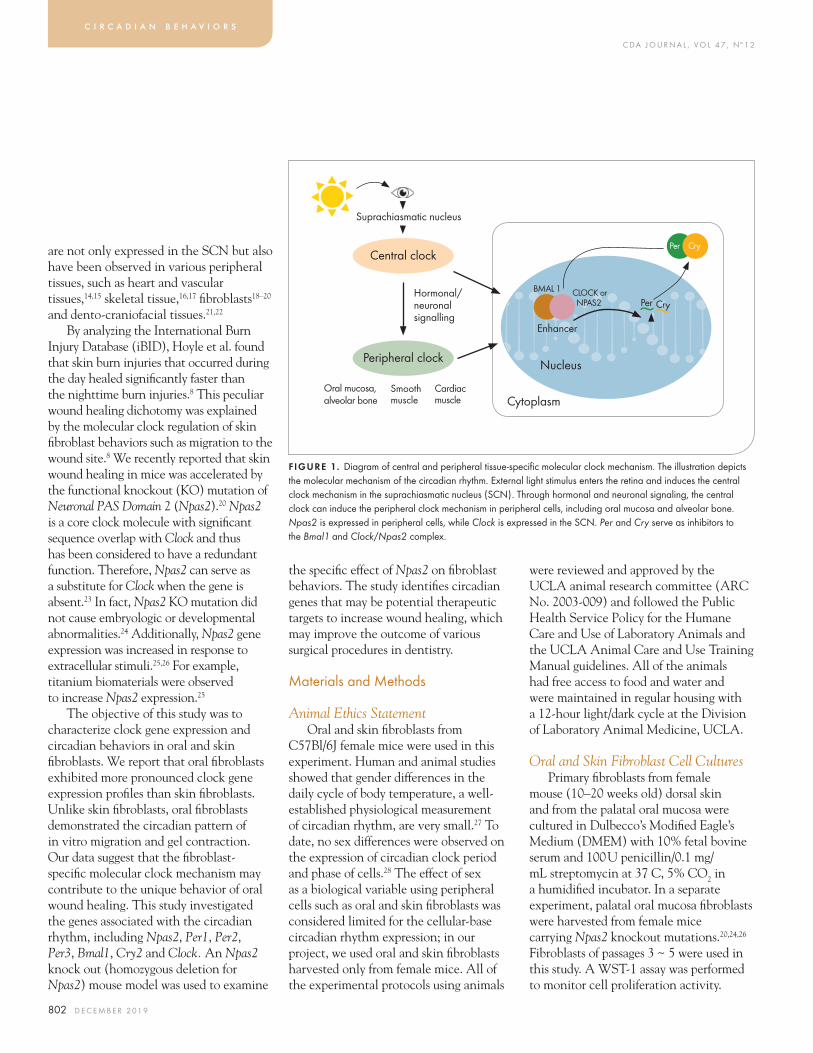
C DA J O U R N A L , V O L 4 7 , Nº 1 2
802 D E C E M B E R 2 01 9
are not only expressed in the SCN but also have been observed in various peripheral tissues, such as heart and vascular tissues,14,15 skeletal tissue,16,17 fibroblasts18–20 and dento-craniofacial tissues.21,22
By analyzing the International Burn Injury Database (iBID), Hoyle et al. found that skin burn injuries that occurred during the day healed significantly faster than the nighttime burn injuries.8 This peculiar wound healing dichotomy was explained by the molecular clock regulation of skin fibroblast behaviors such as migration to the wound site.8 We recently reported that skin wound healing in mice was accelerated by the functional knockout (KO) mutation of Neuronal PAS Domain 2 (Npas2).20 Npas2 is a core clock molecule with significant sequence overlap with Clock and thus has been considered to have a redundant function. Therefore, Npas2 can serve as a substitute for Clock when the gene is absent.23 In fact, Npas2 KO mutation did not cause embryologic or developmental abnormalities.24 Additionally, Npas2 gene expression was increased in response to extracellular stimuli.25,26 For example, titanium biomaterials were observed to increase Npas2 expression.25
The objective of this study was to characterize clock gene expression and circadian behaviors in oral and skin fibroblasts. We report that oral fibroblasts exhibited more pronounced clock gene expression profiles than skin fibroblasts. Unlike skin fibroblasts, oral fibroblasts demonstrated the circadian pattern of in vitro migration and gel contraction. Our data suggest that the fibroblast-specific molecular clock mechanism may contribute to the unique behavior of oral wound healing. This study investigated the genes associated with the circadian rhythm, including Npas2, Per1, Per2, Per3, Bmal1, Cry2 and Clock. An Npas2 knock out (homozygous deletion for Npas2) mouse model was used to examine
the specific effect of Npas2 on fibroblast behaviors. The study identifies circadian genes that may be potential therapeutic targets to increase wound healing, which may improve the outcome of various surgical procedures in dentistry.
Materials and Methods
Animal Ethics StatementOral and skin fibroblasts from
C57Bl/6J female mice were used in this experiment. Human and animal studies showed that gender differences in the daily cycle of body temperature, a well-established physiological measurement of circadian rhythm, are very small.27 To date, no sex differences were observed on the expression of circadian clock period and phase of cells.28 The effect of sex as a biological variable using peripheral cells such as oral and skin fibroblasts was considered limited for the cellular-base circadian rhythm expression; in our project, we used oral and skin fibroblasts harvested only from female mice. All of the experimental protocols using animals
were reviewed and approved by the UCLA animal research committee (ARC No. 2003-009) and followed the Public Health Service Policy for the Humane Care and Use of Laboratory Animals and the UCLA Animal Care and Use Training Manual guidelines. All of the animals had free access to food and water and were maintained in regular housing with a 12-hour light/dark cycle at the Division of Laboratory Animal Medicine, UCLA.
Oral and Skin Fibroblast Cell CulturesPrimary fibroblasts from female
mouse (10–20 weeks old) dorsal skin and from the palatal oral mucosa were cultured in Dulbecco’s Modified Eagle’s Medium (DMEM) with 10% fetal bovine serum and 100 U penicillin/0.1 mg/mL streptomycin at 37 C, 5% CO2 in a humidified incubator. In a separate experiment, palatal oral mucosa fibroblasts were harvested from female mice carrying Npas2 knockout mutations.20,24,26 Fibroblasts of passages 3 ~ 5 were used in this study. A WST-1 assay was performed to monitor cell proliferation activity.
c i r c a d i a n b e h a v i o r s
FIGURE 1. Diagram of central and peripheral tissue-specific molecular clock mechanism. The illustration depicts the molecular mechanism of the circadian rhythm. External light stimulus enters the retina and induces the central clock mechanism in the suprachiasmatic nucleus (SCN). Through hormonal and neuronal signaling, the central clock can induce the peripheral clock mechanism in peripheral cells, including oral mucosa and alveolar bone. Npas2 is expressed in peripheral cells, while Clock is expressed in the SCN. Per and Cry serve as inhibitors to the Bmal1 and Clock/Npas2 complex.
Suprachiasmatic nucleus
Central clock
Peripheral clock
Hormonal/ neuronal signalling
Oral mucosa, alveolar bone
Smooth muscle
Cardiac muscle
Per Cry
Cytoplasm
Nucleus
BMAL 1
Enhancer
Per Cry
CLOCK or NPAS2

C DA J O U R N A L , V O L 4 7 , Nº 1 2
DECEMBER 2 0 1 9 803
Circadian Gene Expression in Skin and Oral Fibroblasts
Messenger RNA expression of seven circadian genes in oral and skin fibroblasts, as well as in Npas2 KO oral fibroblasts, was determined by quantitative real-time polymerase chain reaction (RT-PCR) using TaqMan MGB probes (Thermo Fisher Scientific Inc., Waltham, Mass.). Fibroblasts were cultured in 24-well plates and synchronized at 80% confluency via addition of 100 nM dexamethasone to the medium and incubated for two hours, followed by washing with DMEM.29 Dexamethasone is known to exert a synchronizing effect on circadian rhythms.30 Total RNA was extracted (RNeasy kit, Qiagen, Valencia, Calif.) every six hours for 48 hours (n = 4 per time point) after the synchronization. After quantity and quality of the RNA were examined, RT-PCR was performed to quantify RNA expression using commercially available RNA primers for each gene. Glyceraldehyde 3-phosphate dehydrogenase (GAPDH) was used as the housekeeping control. The circadian expression pattern of clock genes was compared between skin and oral fibroblasts by two-way analysis of variance (ANOVA). The interaction between time and fibroblast origin was used to assess the circadian expression pattern of core clock genes. P-values < 0.01 were considered statistically significant.
In Vitro Wound Healing Scratch Plate Assay
Fibroblasts were seeded into a 6-well plate and synchronized as described above. After two hours, scratch lines were created with a plastic pipette and wells were washed with medium (n = 5 per group). These scratched areas were examined by photomicrography every hour from zero to 24 hours. The number of cells that migrated into the scratched
area was counted at three, six, nine, 12, 15, 18 and 24 hours. The increased number of cells from the previous time point (CNt) determined the cell migration rate (Rmagt) that was standardized by the total cells in the scratch area at 24 hours.
Rmagt = CN
t – CN
t–3 / |CN
t24 – CN
t0|
The cell migration rate of oral and skin fibroblasts was compared by two-way ANOVA. P-values <0.01 were considered statistically significant. When the significance by two-way ANOVA was reached, a Student’s t-test was performed for each time point.
Floating Collagen Gel Contraction AssayThe floating collagen gel contraction
assay was performed following the published protocol.31 A 500 μL collagen type 1 gel mixture containing 50,000 oral or skin fibroblasts was placed in a 24-well plate (n = 5 in each group) and incubated at room temperature for 20 minutes. In a separate experiment, oral fibroblasts isolated from palatal gingiva of Npas2+/– and Npas2–/– mutant mice were used. The solidified gels were transferred to a 100 mm diameter dish and cultured (37 C, 5% CO2 in a humidified incubator). The gel images were scanned by a desktop scanner at zero, six, 12, 18, 24 and 48 hours. The area of each gel (GAt) was determined in the scanned images. The gel contraction percent (Rgel) was determined by the gel area difference between the time point of interest and the initial time point standardized by the gel contraction rate at 48 hours.
Rgelt = GA
t – GA
t0/ |GA
t48 – GA
t0|
Two-way ANOVA was performed and p-values < 0.01 were considered statistically significant. When the significance by two-way ANOVA was reached, a Student’s t-test was performed for each time point.
Results
Circadian Clock Gene Expression in Oral and Skin Fibroblasts
Oral and skin fibroblasts were successfully synchronized in their circadian rhythms and harvested. A WST-1 assay was used to evaluate cell proliferation and indicated that there was no significant difference in proliferation activity between oral fibroblasts and skin fibroblasts (data not shown). RT-PCR was performed after synchronization in order to examine the peak time points when the fibroblasts expressed the highest amount of the assayed RNA. RT-PCR of the oral and skin fibroblasts depicted cyclical pattern of the circadian rhythm gene expression (fiGure 2). Over the 48-hour period, the circadian expression patterns of Per1, Bmal1 and Npas2 were found more prominent in oral fibroblasts, indicating clearer diurnal peaks than those of skin fibroblasts (two-way ANOVA, p < 0.01). The circadian expression timing of Per3 and Cry2 differed significantly between oral and skin fibroblasts. These experiments revealed that the clock gene expression pattern of fibroblasts was tissue-source specific.
Different Circadian Pattern of Oral and Skin Fibroblast Migration
Scratch tests were performed in order to quantify the rate of fibroblast migration. Time-lapse photomicrographic recording of the in vitro wound healing scratch test demonstrated that oral and skin fibroblasts migrated into the created void area (fiGure 3a). The total number of oral fibroblasts that migrated into the created void area was less than that of skin fibroblasts at 24 hours. There was no observable difference in fibroblast migration at the 48-hour mark. Interestingly, the rate of oral fibroblast migration was minimal at the early time period. The oral fibroblast migration
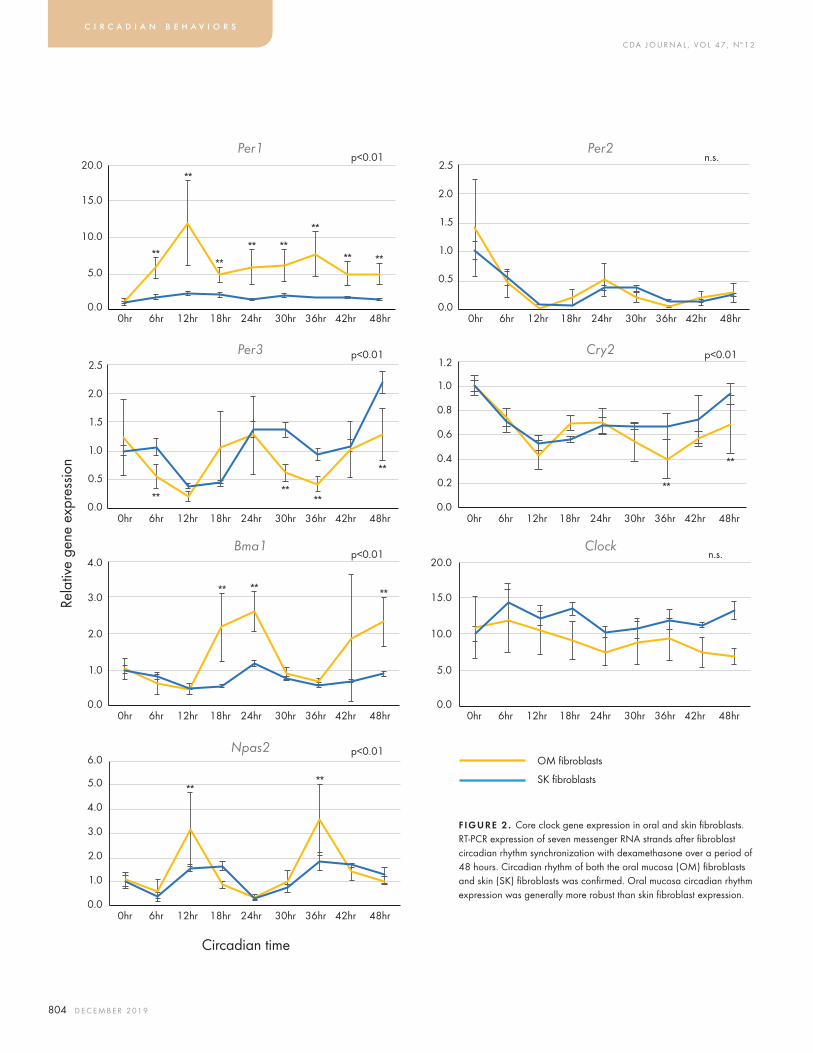
C DA J O U R N A L , V O L 4 7 , Nº 1 2
804 D E C E M B E R 2 01 9
c i r c a d i a n b e h a v i o r s
2.5
2.0
1.5
1.0
0.5
0.00hr 6hr 12hr 18hr 24hr 30hr 36hr 42hr 48hr
FIGURE 2 . Core clock gene expression in oral and skin fibroblasts. RT-PCR expression of seven messenger RNA strands after fibroblast circadian rhythm synchronization with dexamethasone over a period of 48 hours. Circadian rhythm of both the oral mucosa (OM) fibroblasts and skin (SK) fibroblasts was confirmed. Oral mucosa circadian rhythm expression was generally more robust than skin fibroblast expression.
20.0
15.0
10.0
5.0
0.00hr 6hr 12hr 18hr 24hr 30hr 36hr 42hr 48hr
OM fibroblasts
SK fibroblasts
Circadian time
n.s.
n.s.Per2
Clock
p<0.0120.0
15.0
10.0
5.0
0.00hr 6hr 12hr 18hr 24hr 30hr 36hr 42hr 48hr
Per1
2.5
2.0
1.5
1.0
0.5
0.00hr 6hr 12hr 18hr 24hr 30hr 36hr 42hr 48hr
p<0.01Per31.2
0.8
1.0
0.6
0.4
0.2
0.00hr 6hr 12hr 18hr 24hr 30hr 36hr 42hr 48hr
p<0.01Cry2
4.0
3.0
2.0
1.0
0.00hr 6hr 12hr 18hr 24hr 30hr 36hr 42hr 48hr
p<0.01Bma1
6.0
4.0
5.0
3.0
2.0
1.0
0.00hr 6hr 12hr 18hr 24hr 30hr 36hr 42hr 48hr
p<0.01Npas2
Rela
tive
gene
exp
ress
ion
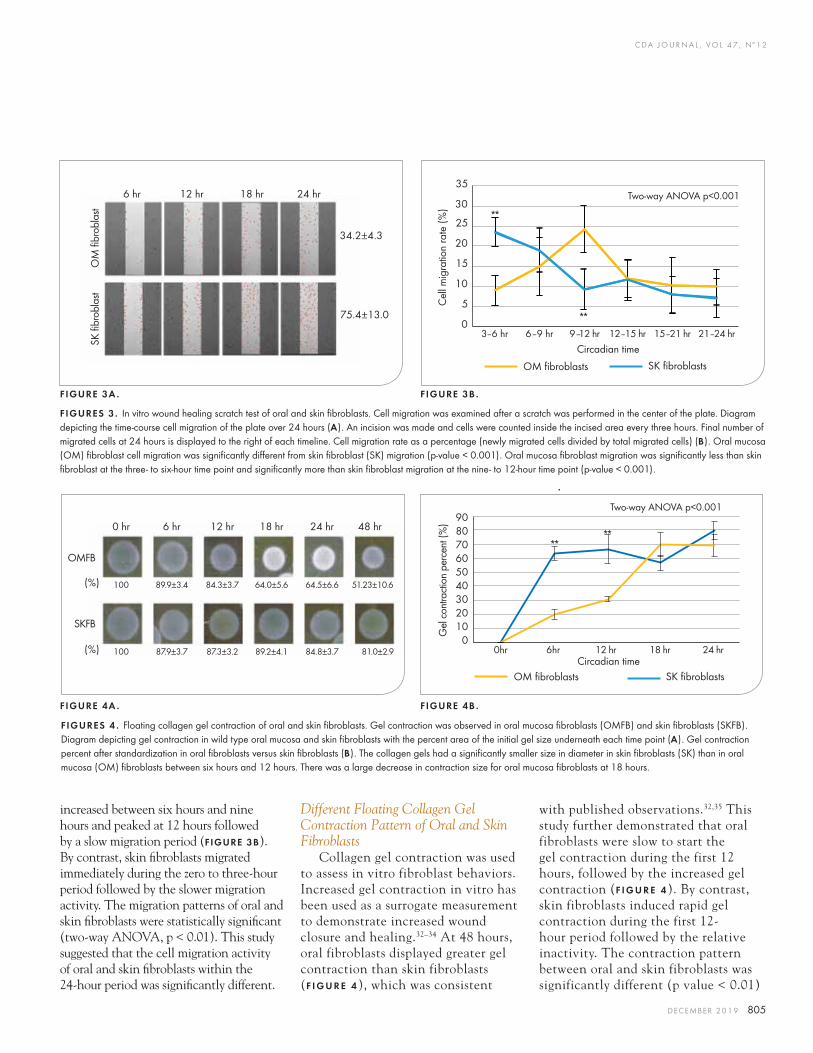
C DA J O U R N A L , V O L 4 7 , Nº 1 2
DECEMBER 2 0 1 9 805
increased between six hours and nine hours and peaked at 12 hours followed by a slow migration period (fiGure 3B). By contrast, skin fibroblasts migrated immediately during the zero to three-hour period followed by the slower migration activity. The migration patterns of oral and skin fibroblasts were statistically significant (two-way ANOVA, p < 0.01). This study suggested that the cell migration activity of oral and skin fibroblasts within the 24-hour period was significantly different.
Different Floating Collagen Gel Contraction Pattern of Oral and Skin Fibroblasts
Collagen gel contraction was used to assess in vitro fibroblast behaviors. Increased gel contraction in vitro has been used as a surrogate measurement to demonstrate increased wound closure and healing.32–34 At 48 hours, oral fibroblasts displayed greater gel contraction than skin fibroblasts (f i G u r e 4), which was consistent
with published observations.32,35 This study further demonstrated that oral fibroblasts were slow to start the gel contraction during the first 12 hours, followed by the increased gel contraction (f i G u r e 4). By contrast, skin fibroblasts induced rapid gel contraction during the first 12-hour period followed by the relative inactivity. The contraction pattern between oral and skin fibroblasts was significantly different (p value < 0.01)
FIGURES 3 . In vitro wound healing scratch test of oral and skin fibroblasts. Cell migration was examined after a scratch was performed in the center of the plate. Diagram depicting the time-course cell migration of the plate over 24 hours (a). An incision was made and cells were counted inside the incised area every three hours. Final number of migrated cells at 24 hours is displayed to the right of each timeline. Cell migration rate as a percentage (newly migrated cells divided by total migrated cells) (B). Oral mucosa (OM) fibroblast cell migration was significantly different from skin fibroblast (SK) migration (p-value < 0.001). Oral mucosa fibroblast migration was significantly less than skin fibroblast at the three- to six-hour time point and significantly more than skin fibroblast migration at the nine- to 12-hour time point (p-value < 0.001).
6 hr 12 hr 18 hr 24 hr
34.2±4.3
75.4±13.0
OM
fibr
obla
stSK
fibr
obla
st
FIGURE 3A . FIGURE 3B .
FIGURE 4A . FIGURE 4B .
SK fibroblasts
8090
70
30
50
100
Gel
con
tract
ion
perc
ent (
%)
0hr 6hr 12 hr 18 hr 24 hrCircadian time
OM fibroblasts
Two-way ANOVA p<0.001
20
40
60
0 hr 6 hr 12 hr 18 hr 24 hr 48 hr
100 89.9±3.4 84.3±3.7 64.0±5.6 64.5±6.6 51.23±10.6
OMFB
SKFB
(%)
100 87.9±3.7 87.3±3.2 89.2±4.1 84.8±3.7 81.0±2.9 (%)
FIGURES 4 . Floating collagen gel contraction of oral and skin fibroblasts. Gel contraction was observed in oral mucosa fibroblasts (OMFB) and skin fibroblasts (SKFB). Diagram depicting gel contraction in wild type oral mucosa and skin fibroblasts with the percent area of the initial gel size underneath each time point (a). Gel contraction percent after standardization in oral fibroblasts versus skin fibroblasts (B). The collagen gels had a significantly smaller size in diameter in skin fibroblasts (SK) than in oral mucosa (OM) fibroblasts between six hours and 12 hours. There was a large decrease in contraction size for oral mucosa fibroblasts at 18 hours.
SK fibroblasts
Two-way ANOVA p<0.00135
25
30
20
10
15
5
0
Cel
l mig
ratio
n ra
te (%
)
3–6 hr 6–9 hr 9–12 hr 12–15 hr 15–21 hr 21–24 hrCircadian time
OM fibroblasts
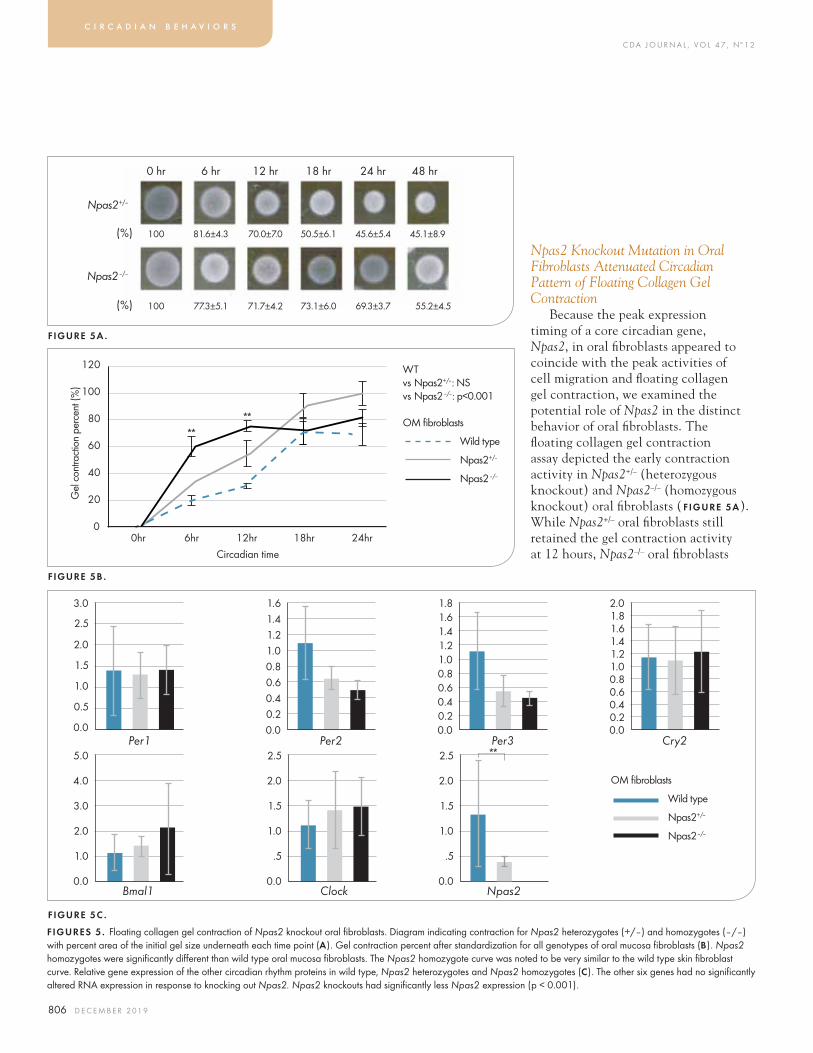
C DA J O U R N A L , V O L 4 7 , Nº 1 2
806 D E C E M B E R 2 01 9
Npas2 Knockout Mutation in Oral Fibroblasts Attenuated Circadian Pattern of Floating Collagen Gel Contraction
Because the peak expression timing of a core circadian gene, Npas2, in oral fibroblasts appeared to coincide with the peak activities of cell migration and floating collagen gel contraction, we examined the potential role of Npas2 in the distinct behavior of oral fibroblasts. The floating collagen gel contraction assay depicted the early contraction activity in Npas2+/– (heterozygous knockout) and Npas2–/– (homozygous knockout) oral fibroblasts (fiGure 5a). While Npas2+/– oral fibroblasts still retained the gel contraction activity at 12 hours, Npas2–/– oral fibroblasts
c i r c a d i a n b e h a v i o r s
0 hr 6 hr 12 hr 18 hr 24 hr 48 hr
100 81.6±4.3 70.0±7.0 50.5±6.1 45.6±5.4 45.1±8.9
Npas2+/–
Npas2–/–
(%)
100 77.3±5.1 71.7±4.2 73.1±6.0 69.3±3.7 55.2±4.5 (%)
FIGURES 5. Floating collagen gel contraction of Npas2 knockout oral fibroblasts. Diagram indicating contraction for Npas2 heterozygotes (+/–) and homozygotes (–/–) with percent area of the initial gel size underneath each time point (a). Gel contraction percent after standardization for all genotypes of oral mucosa fibroblasts (B). Npas2 homozygotes were significantly different than wild type oral mucosa fibroblasts. The Npas2 homozygote curve was noted to be very similar to the wild type skin fibroblast curve. Relative gene expression of the other circadian rhythm proteins in wild type, Npas2 heterozygotes and Npas2 homozygotes (c). The other six genes had no significantly altered RNA expression in response to knocking out Npas2. Npas2 knockouts had significantly less Npas2 expression (p < 0.001).
3.0
2.5
2.0
1.0
1.5
0.5
0.0Per1
1.61.41.21.00.8
0.40.6
0.20.0
Per2
1.81.61.41.21.00.8
0.40.6
0.20.0
Per3
OM fibroblasts
Wild type
Npas2+/–
Npas2–/–
FIGURE 5C .
WTvs Npas2+/–: NSvs Npas2–/–: p<0.001
OM fibroblasts
Wild type
Npas2+/–
Npas2–/–
Circadian time
100
120
80
60
40
20
00hr 6hr 12hr 24hr18hr
Gel
con
tract
ion
perc
ent (
%)
FIGURE 5B .
FIGURE 5A .
5.0
4.0
2.0
3.0
1.0
0.0Bmal1
2.5
2.0
1.0
1.5
.5
0.0
2.5
2.0
1.0
1.5
.5
0.0Clock Npas2
2.0
1.61.8
1.41.21.00.8
0.40.6
0.20.0
Cry2

C DA J O U R N A L , V O L 4 7 , Nº 1 2
DECEMBER 2 0 1 9 807
appeared to have lost the contraction activity during this period, resulting in a plateau in the gel contraction (f iGure 5B). As a result, the gel contraction behavior of Npas2–/– oral fibroblasts, resembling skin fibroblasts, was statistically different from that of wild type oral fibroblasts. The Npas2 knockout mutation did not affect the expression of other clock genes although Per2 and Per3 expressions were slightly decreased (f iGure 5c).
DiscussionConnective tissue fibroblasts present
a wide range of phenotypic diversities.36 A large number of studies have reported that oral fibroblasts increase the floating collagen gel contraction in vitro37–39 and synthesize growth factors,37,40 collagens and remodeling enzymes.36,41,42 Overall, oral fibroblasts are proposed to contribute to faster oral wound healing and less scarring than their dermal counterparts.32,43 The present study further revealed that oral and skin fibroblasts significantly differed in their circadian behaviors.
The role of the molecular clock mechanism during dento-cranial tissue embryogenesis and development has been researched. For example, Lacruz et al. reported circadian expression of Per1, Per2 and Bmal1 in ameloblast-like LS8 cells.44 Zheng et al. also reported circadian expression of core clock genes in an ameloblast cell line.45 These studies further demonstrated the circadian expression of amelogenin (Amelx), a critical enamel-specific protein,44,45 suggesting that enamel development is regulated by a circadian clock mechanism. In fact, the enamel rods show transverse lines called cross-striations, and enamel development has been suggested to have a circadian pattern.46
In order to regenerate lost tissue, wound healing reiterates, at least in part, tissue-specific embryogenesis and development processes. It has been suggested that the circadian clock genes regulate cell migration of mesenchymal stromal cells,47 hematopoietic immune progenitor cells48,49 and fibroblasts,8,20 all of which participate in wound healing. Oral fibroblasts were able to complete the wound healing process faster than their skin counterparts with minimal scarring in the oral cavity. The expression of
circadian clock genes (Per1, Cry1, Bmal1 and Clock) has been postulated to be responsible for physiological variations in cell proliferation of human oral mucosa.50 Therefore, this study investigated the tissue-specific molecular clock mechanism and circadian behavior of oral fibroblasts.
The scratch test (f iGure 3) and the floating collagen gel contraction assay (f iGure 4) revealed that oral fibroblasts behaved differently from skin fibroblasts and the peak oral mucosa fibroblast activity is observed to occur at 12 hours. However, skin fibroblasts are observed to contract the gels slowly, with no further substantial contraction after six hours. Furthermore, both cell migration and the collagen gel contraction assays indicated that oral
fibroblast behavior was most substantial at the same time point when Npas2 expression in oral mucosa fibroblasts peaked (f iGure 2). An experiment involving Npas2 knockdown in human colorectal cancer cells demonstrated an increased cell migration and cell proliferation activities.51 Therefore, we examined if a complete Npas2 knockout mutation affected their behavior. The Npas2 knockout mutation in oral fibroblasts significantly decreased the midday activity of collagen gel contraction (f iGure 5), and thus, Npas2–/– oral fibroblasts mimicked the skin fibroblast behavior (f iGures 4
and 5). In conclusion, our observations suggest that Npas2 gene expression plays an essential role in oral wound healing. An increase in Npas2 gene expression would increase the speed of oral mucosal wound healing by promoting fibroblast behavior. Npas2 knockout fibroblasts display fibroblast behaviors that are similar to skin fibroblasts. Furthermore, increased Npas2 expression has been linked with enhanced osseointegration with rough surface implants.24 These findings suggest that Npas2 expression may become a future therapeutic target to hasten implant and implant-supported crown delivery time.
Recently, Janjic and Agis proposed “chronodentistry,”22 in which therapeutic application in dentistry might consider circadian rhythm for more effective outcome. For example, swelling after oral surgery does not reduce progressively but follows a circaseptan (approximately seven days) rhythm.52,53 Furthermore, environmentally induced “jet lag” in mice affects the corneal epithelium renewal and repair.54 These studies, in addition to the findings presented here, highlight the potential role molecular clock genes could play in wound healing. For this reason, clock genes
Overall, oral fibroblasts are proposed to contribute to faster oral wound healing and less scarring than their dermal counterparts.
C DA J O U R N A L , V O L 4 7 , Nº 1 2
808 D E C E M B E R 2 01 9
could be a potential therapeutic target. It is possible that manipulation of these genes could decrease healing times following surgical procedures in dentistry, including implants, apicoectomies, free gingival grafts and crown-lengthening procedures, which would all benefit from a decreased recovery time. The exact process of wound healing is currently unknown; however, the outcome of this study suggests that further investigation of circadian clock gene regulation may provide an important clue in accelerating oral mucosa wound healing following dental surgical procedures. n
acknowledGments
The authors thank Dr. Akishige Hokugo, David Geffen School of Medicine, UCLA, and Dr. Hiroko Okawa, Weintraub Center for Reconstructive Biotechnology, UCLA School of Dentistry for their technical support and discussion on data interpretation. This study was conducted in part as the Pilot Study of UCLA School of Dentistry.
references
1. Wong JW, et al. Wound healing in oral mucosa results in reduced scar formation as compared with skin: Evidence from the red Duroc pig model and humans. Wound Repair Regen 2009 Sep–Oct;17(5):717–29. doi: 10.1111/j.1524-475X.2009.00531.x.2. Glim JE, van Egmond M, Niessen FB, Everts V, Beelen RH. Detrimental dermal wound healing: What can we learn from the oral mucosa? Wound Repair Regen 2013 Sep–Oct;21(5):648–60. doi: 10.1111/wrr.12072. Epub 2013 Aug 8.3. Yang J, et al. Salivary EGF regulates eosinophil-derived TGF-alpha expression in hamster oral wounds. Am J Physiol 1996 Jan;270(1 Pt 1):G191–202.4. Ohshima M, Sato M, Ishikawa M, Maeno M, Otsuka K. Physiologic levels of epidermal growth factor in saliva stimulate cell migration of an oral epithelial cell line, HO-1-N-1. Eur J Oral Sci 2002 Apr;110(2):130–6.5. Okan D, Woo K, Ayello EA, Sibbald G. The role of moisture balance in wound healing. Adv Skin Wound Care 2007 Jan;20(1):39–53; quiz 53–5.6. Bussi M, Valente G, Curato MP, Carlevato MT, Cortesina G. Is transposed skin transformed in major head and neck mucosal reconstruction? Acta Otolaryngol 1995 Mar;115(2):348–51.7. Cable EJ, Onishi KG, Prendergast BJ. Circadian rhythms accelerate wound healing in female Siberian hamsters. Physiol Behav 2017 Mar 15;171:165–174. doi: 10.1016/j.physbeh.2016.12.019. Epub 2016 Dec 18.8. Hoyle NP, et al. Circadian actin dynamics drive rhythmic fibroblast mobilization during wound healing. Sci Transl Med 2017 Nov 8;9(415). pii: eaal2774. doi: 10.1126/scitranslmed.aal2774.9. Buijs RM, Guzmán Ruiz MA, Méndez Hernández
R, Rodríguez Cortés B. The suprachiasmatic nucleus; a responsive clock regulating homeostasis by daily changing the set points of physiological parameters. Auton Neurosci 2019 May;218:43–50. doi: 10.1016/j.autneu.2019.02.001. Epub 2019 Feb 13.10. Dunlap JC. Molecular bases for circadian clocks. Cell 1999 Jan 22;96(2):271–90.11. Gekakis N, et al. Role of the CLOCK protein in the mammalian circadian mechanism. Science 1998 Jun 5;280(5369):1564–9.12. Shearman LP, et al. Interacting molecular loops in the mammalian circadian clock. Science 2000 May 12;288(5468):1013–9.13. Brown SA, Kowalska E, Dallmann R. (Re)inventing the circadian feedback loop. Dev Cell 2012 Mar 13;22(3):477–87. doi: 10.1016/j.devcel.2012.02.007.14. Takeda N, Maemura K. The role of clock genes and circadian rhythm in the development of cardiovascular diseases. Cell Mol Life Sci 2015 Sep;72(17):3225–34. doi: 10.1007/s00018-015-1923-1. Epub 2015 May 14.15. Crnko S, Cour M, Van Laake LW, Lecour S. Vasculature on the clock: Circadian rhythm and vascular dysfunction. Vascul Pharmacol 2018 Sep;108:1–7. doi: 10.1016/j.vph.2018.05.003. Epub 2018 May 17.16. Wu QY, et al. Emerging role of circadian rhythm in bone remodeling. J Mol Med (Berl) 2019 Jan;97(1):19–24. doi: 10.1007/s00109-018-1723-9. Epub 2018 Nov 16.17. Song C, et al. Insights into the role of circadian rhythms in bone metabolism: A promising intervention target? Biomed Res Int 2018 Sep 27;2018:9156478. doi: 10.1155/2018/9156478. eCollection 2018.18. Hida A, et al. Evaluation of circadian phenotypes utilizing fibroblasts from patients with circadian rhythm sleep disorders. Transl Psychiatry 2017 Apr 25;7(4):e1106. doi: 10.1038/tp.2017.75.19. Streuli CH, Meng QJ. Influence of the extracellular matrix on cell-intrinsic circadian clocks. J Cell Sci 2019 132:jcs207498. doi: 10.1242/jcs.207498.20. Sasaki H, et al. Neuronal PAS Domain 2 (Npas2)-Deficient Fibroblasts Accelerate Skin Wound Healing and Dermal Collagen Reconstruction. Anat Rec (Hoboken) 2019 Mar 9. doi: 10.1002/ar.24109. [Epub ahead of print] .21. Janjić K, Kurzmann C, Moritz A, Agis H. Core circadian clock gene expression in human dental pulp-derived cells in response to L-mimosine, hypoxia and echinomycin. Eur J Oral Sci 2018 Aug;126(4):263–271. doi: 10.1111/eos.12535.22. Janjić K, Agis H. Chronodentistry: The role and potential of molecular clocks in oral medicine. BMC Oral Health 2019 Feb 13;19(1):32. doi: 10.1186/s12903-019-0720-x.23. DeBruyne JP, Weaver DR, Reppert SM. CLOCK and NPAS2 have overlapping roles in the suprachiasmatic circadian clock. Nat Neurosci 2007 May;10(5):543–5. Epub 2007 Apr 8.24. Morinaga K, et al. Neuronal PAS domain 2 (Npas2) facilitated osseointegration of titanium implant with rough surface through a neuroskeletal mechanism. Biomaterials 2019 Feb;192:62–74. doi: 10.1016/j.biomaterials.2018.11.003. Epub 2018 Nov 3.25. Matsumura R, Matsubara C, Node K, Takumi T, Akashi M. Nuclear receptor-mediated cell-autonomous
oscillatory expression of the circadian transcription factor, neuronal PAS domain protein 2 (NPAS2). J Biol Chem 2013 Dec 20;288(51):36548–53. doi: 10.1074/jbc.M113.517235. Epub 2013 Nov 6.26. Hassan N, et al. Titanium biomaterials with complex surfaces induced aberrant peripheral circadian rhythms in bone marrow mesenchymal stromal cells. PLoS One 2017 Aug 17;12(8):e0183359. doi: 10.1371/journal.pone.0183359. eCollection 2017.27. Mortola JP. Gender and the circadian pattern of body temperature in normoxia and hypoxia. Respir Physiol Neurobiol 2017 Nov;245:4–12. doi: 10.1016/j.resp.2016.11.002. Epub 2016 Nov 17.28. Okubo N, et al. Prolonged bioluminescence monitoring in mouse ex vivo bone culture revealed persistent circadian rhythms in articular cartilages and growth plates. PLoS One 2013 Nov 4;8(11):e78306. doi: 10.1371/journal.pone.0078306. eCollection 2013.29. Nagoshi E, et al. Circadian gene expression in individual fibroblasts: Cell-autonomous and self-sustained oscillators pass time to daughter cells. Cell 2004 Nov 24;119(5):693–705.30. Balsalobre A, Marcacci L, Schibler U. Multiple signaling pathways elicit circadian gene expression in cultured Rat-1 fibroblasts. Curr Biol 2000 Oct 19;10(20):1291–4.31. Ngo P, Ramalingam P, Phillips JA, Furuta GT. Collagen gel contraction assay. Methods Mol Biol 2006;341:103–109.32. Lin A, Hokugo A, Choi J, Nishimura I. Small cytoskeleton-associated molecule, fibroblast growth factor receptor 1 oncogene partner 2/wound inducible transcript-3.0 (FGFR1OP2/wit3.0), facilitates fibroblast-driven wound closure. Am J Pathol 2010 Jan;176(1):108–21. doi: 10.2353/ajpath.2010.090256. Epub 2009 Dec 3.33. Sukotjo C, Abanmy AA, Ogawa T, Nishimura I. Molecular cloning of wound inducible transcript (wit 3.0) differentially expressed in edentulous oral mucosa undergoing tooth extraction wound-healing. J Dent Res 2002 Apr;81(4):229–35.34. Romero A, et al. Cigarette smoke condensate inhibits collagen gel contraction and prostaglandin E2 production in human gingival fibroblasts. J Periodontal Res 2015 Jun;50(3):371–9. doi: 10.1111/jre.12216. Epub 2014 Jul 29.35. Lygoe KA, Wall I, Stephens P, Lewis MP. Role of vitronectin and fibronectin receptors in oral mucosal and dermal myofibroblast differentiation. Biol Cell 2007 Nov;99(11):601–14.36. Stephens P, et al. Skin and oral fibroblasts exhibit phenotypic differences in extracellular matrix reorganization and matrix metalloproteinase activity. Br J Dermatol 2001 Feb;144(2):229–37.37. Shannon DB, McKeown ST, Lundy FT, Irwin CR. Phenotypic differences between oral and skin fibroblasts in wound contraction and growth factor expression. Wound Repair Regen 2006 Mar–Apr;14(2):172–8.38. Lee HG, Eun HC. Differences between fibroblasts cultured from oral mucosa and normal skin: Implication to wound healing. J Dermatol Sci 1999 Nov;21(3):176–82.39. Sukotjo C, et al. Oral fibroblast expression of wound-inducible transcript 3.0 (wit3.0) accelerates the
c i r c a d i a n b e h a v i o r s
C DA J O U R N A L , V O L 4 7 , Nº 1 2
DECEMBER 2 0 1 9 809
collagen gel contraction in vitro. J Biol Chem 2003 Dec 19;278(51):51527–34. Epub 2003 Oct 3.40. Schrementi ME, Ferreira AM, Zender C, DiPietro LA. Site-specific production of TGF-beta in oral mucosal and cutaneous wounds. Wound Repair Regen 2008 Jan–Feb;16(1):80–6. Epub 2007 Dec 13.41. McKeown ST, et al. Matrix metalloproteinase-3 differences in oral and skin fibroblasts. J Dent Res 2007 May;86(5):457–62.42. Ambrosini P, Cherene S, Miller N, Weissenbach M, Penaud J. A laser Doppler study of gingival blood flow variations following periosteal stimulation. J Clin Periodontol 2002 Feb;29(2):103–7.43. Lin A, Hokugo A, Nishimura I. Wound closure and wound management: A new therapeutic molecular target. Cell Adh Migr 2010 Jul–Sep;4(3):396–9. Epub 2010 Jul 31.44. Lacruz RS, et al. The circadian clock modulates enamel development. J Biol Rhythms 2012 Jun;27(3):237–45. doi: 10.1177/0748730412442830.45. Zheng L, et al. Circadian rhythms regulate amelogenesis. Bone 2013 Jul;55(1):158–65. doi:
10.1016/j.bone.2013.02.011. Epub 2013 Feb 26.46. Antoine D, Hillson S, Dean MC. The developmental clock of dental enamel: A test for the periodicity of prism cross-striations in modern humans and an evaluation of the most likely sources of error in histological studies of this kind. J Anat 2009 Jan;214(1):45–55. doi: 10.1111/j.1469-7580.2008.01010.x.47. Boucher H, Vanneaux V, Domet T, Parouchev A, Larghero J. Circadian Clock genes modulate human bone marrow mesenchymal stem cell differentiation, migration and cell cycle. PLoS One 2016 Jan 7;11(1):e0146674. doi: 10.1371/journal.pone.0146674. eCollection 2016.48. Weger M, Diotel N, Dorsemans AC, Dickmeis T, Weger BD. Stem cells and the circadian clock. Dev Biol 2017 Nov 15;431(2):111–123. doi: 10.1016/j.ydbio.2017.09.012. Epub 2017 Sep 9.49. Brown SA. Circadian clock-mediated control of stem cell division and differentiation: Beyond night and day. Development 2014 Aug;141(16):3105–11. doi: 10.1242/dev.104851.50. Bjarnason GA, et al. Circadian expression of clock
genes in human oral mucosa and skin: Association with specific cell-cycle phases. Am J Pathol 2001 May;158(5):1793–1801.51. Xue X, et al. Silencing NPAS2 promotes cell growth and invasion in DLD-1 cells and correlated with poor prognosis of colorectal cancer. Biochem Biophys Res Commun 2014 Jul 25;450(2):1058–62. doi: 10.1016/j.bbrc.2014.06.104. Epub 2014 Jun 27.52. Pollmann L. Long-term follow-up of postoperative swelling. Int J Oral Surg 1983 Apr;12(2):90–94.53. Bertolami CN, Cohen CH, Chrzanowski RR. Quantitation of experimental postsurgical edema. J Oral Maxillofac Surg 1982 Aug;40(8):473–6.54. Xue Y, et al. Modulation of circadian rhythms affects corneal epithelium renewal and repair in mice. Invest Ophthalmol Vis Sci 2017 Mar 1;58(3):1865–1874. doi: 10.1167/iovs.16-21154.
the correspondinG author, Ichiro Nishimura, DDS, DMSc, DMD, can be reached at [email protected].
Specializing in selling and appraising dental practices for over 40 years!
CONTACT US FOR A FREE CONSULTATION Phone: (800) 697 -5656
WWW.CALPRACTICESALES.COM CA BRE #00283209
youtube.com/mycpsteam faceboook.com/mycpsteam Happy Holidays!
LOS ANGELES & VENTURA COUNTY
CANOGA PARK— 25+ years of goodwill GP w/ 4 eq ops and 1 plmbd not eq op. Located in a single story bldg. Proj. approx. $369K for 2019. Property ID #5241.
CERRITOS— GP with 40 yrs of goodwill in shopping plaza. Grossed $1.4M in 2018. NET $328K. Property ID #5295.
CENTURY CITY—GP in 11 story prof med bldg. Has 5 eq in a 1,955 sq ft. Grossed approx. $715K. Buyer’s net of $184K. Prop-erty ID 4509.
DUARTE— GP established in1964 located in a 2 story mixed bldg. Grossed $404K in 2018. NET $73K. Property ID #5183.
GRANDA HILLS— With 50 yrs of goodwill this general practice grossed approx. $328K in 2018. NET $177K. Property #5276.
LONG BEACH —GP w/ 35 yrs goodwill. Has 3 eq ops in a 1,698 sq ft suite. Grossed $336K in 2018. NET $115K. Property ID #5282.
LYNWOOD— GP in single story busy shop-ping center. Absentee owner. Grossed $570K in 2018. NET $255K. Property ID #5264.
ROWLAND HEIGHTS— Estab. in 2009, this GP is located in a 1 story free standing bldg. Grossed $772K in 2018. NET $237K. Proper-ty ID 5278.
SIMI VALLEY— GP w/ 54 years of goodwill in free standing building. Projecting approx. $621K for 2019. NET $200K. ID #5294
VENTURA - GP w/ 4 eq ops . PPO & Cash only. 40 years goodwill. Grossed $496K in 2018. Property ID #5288.
ORANGE COUNTY
ANAHEIM— GP located in a small shopping center. Has 4 eq ops w/ digital x-ray. Ap-prox. 40-45 new patients/mo. Projecting approx. $1.3M for 2019. Net $800K. Prop-erty ID #5296
CORONA DEL MAR— Well established GP with 3 eq ops. Grossed $898K in 2018. Net $214K. Property ID #5285.
FOUNTAIN VALLEY— GP in strip shopping center w/ great street visibility. Grossed $287K in 2018. Has 4 eq ops and 1 plmbd not eq. Great staff. Property ID #5293
LAGUNA HILLS — With 16 yrs of gdwll this GP is in a single story shopping center. Has 4 eq ops in a 1,200 sq ft suite. Property ID #5290.
SAN CLEMENTE—GP w/ 15 yrs gdwll. Pro-jecting approx. $1M. Property ID #5297.
WESTMINSTER/FOUNTAIN VALLEY— Es-tablished in 1978 GP in 2 story free stand-ing bldg. Grossed $737K in 2018. Has rea-sonable rent. Property ID #5291.
OCEANSIDE— Established in 1990 with 4 eq ops in a one story busy shopping center. PPO and Cash Only. Grossed approx. $560K in 2018. NET $181K. Property ID #5267.
RIVERSIDE COUNTY
RANCHO MIRAGE— Beautiful Fee for ser-vice General / Implant practice located in free standing bldg. Has 4 eq ops. . Grossed $1M in 2018. NET $333K. Property ID #5284.
TEMECULA - Pedo and Ortho Practice! It’s located in a duplex single story building. Grossed $1.7M with a Buyer’ net of $947K. PPO/Cash/Denti-cal. Has 8 eq ops in a 3,500 sq ft office. Property ID # 5243.
LA QUINTA— Price Reduced!! Well estab-lished GP with over 8 years of goodwill. This modern designed practice has 8 eq ops. On a the busiest major intersection. Grossed $1.5M for 2018. NET $568K. Property ID #5130.
SAN BERNARDINO — General practice located in single story free standing bldg w/ 4 eq ops. Seller owns building. Grossed $401K in 2019. Property ID #5289.
UPLAND—Beautiful general practice locat-ed in 2 story building with 4 equipped oper-atories. Grossed $943K in 2018. Buyer’s net of $221K. Property ID #5237.
COMING SOON
Bakersfield, Encino, Laguna Niguel, La Habra, Long Beach, San Bernardi-no, San Diego / Escondido, Ventura,
and Yorba Linda
SAN DIEGO COUNTY
CARLSBAD— This beautiful practice has over 22 yrs of goodwill. Has 4 eq ops in a 1,800 sq ft suite. Fee for service office. Grossed ap-prox. $440K for 2018. Property ID # 5256.
CARMEL VALLEY — Price Reduced! Turn key practice with 3 eq ops and 1 plumbed not eq on an approx. 1,815 sq ft suite. PPO and Cash only. Grossed approx. $325K in 2018. ID # 5274.
EL CAJON - GP + Real State. Price Re-duced !!!Consists of 5 eq ops and equipped with 3D Sirona CBCT Digital X-ray. Grossed over $1M in the past 10 years. NET $244K. Property ID # 5265.
SOLD
C DA J O U R N A L , V O L 4 7 , Nº 1 2
DECEMBER 2 0 1 9 811
RM Matters
There is little doubt that cellphones have dramatically changed our lives. In fact, “phone” is a bit of a misnomer, as it does so much more than make and receive calls.
These mobile devices are now computers, cameras, media players, e-readers and GPS trackers all rolled into one.
It’s not surprising then that few of us can go a day without our cellphone by our side. They have become ubiquitous, accompanying us in the car, in meetings, in restaurants and in the workplace. But this puts employers in a difficult spot. Not only does cellphone use bring up questions of productivity and professionalism, it also brings up questions of privacy when used in a dental office setting.
According to a survey conducted by CareerBuilder, more than half the respondents identified cellphone use as the biggest productivity killer in the workplace. The consequences of lost productivity are direct and indirect, causing reduced employee morale, strain on employer-employee relationships, a lower quality of work and negative impact on client interactions.
The Dentists Insurance Company reminds dentists that cellphone use during work hours can send the message that patients are not the practice’s priority. It can also lead to distractions, which can result in errors in documentation and lack of attention to detail, opening the practice to a liability claim.
TDIC’s Risk Management Advice Line has received several calls regarding cellphone use in the office. In one case, a practice owner called about a dental assistant who was repeatedly on her phone. At a performance review six months prior, she was instructed to put her phone away during the workday. After that time, her restroom breaks increased, suggesting she was using her phone in the restroom.
Reduce Risk, Increase Productivity With Cellphone PoliciesTDIC Risk Management Staff
The Risk Management analyst informed the dentist that it is within an employer’s right to require employees to keep their phones in a drawer and to limit their use to designated break periods. The analyst suggested the office create a universal cellphone-use policy and distribute it to all employees. Violation of this policy would be grounds for disciplinary action, including termination.
In another situation, a dentist reported that her head assistant, who had been with the practice for 14 years, was “addicted” to her phone. The employee would read (and send) text messages during morning huddles
and would have her phone in her hand while greeting patients. She would even leave her phone out during treatments. The employee manual stated that cellphone use was not allowed during work hours and was only allowed during breaks and lunch periods. The dentist relied on this employee heavily and didn’t want to lose her.
The Risk Management analyst guided the dentist to apply policies consistently with all employees. She advised the dentist that in addition to addressing the matter with the employee directly to hold an office meeting to remind staff of the office’s cellphone policy
From one-on-one risk management advice by phone to informed consent forms to expert-led seminars, we’re here to help you practice with confidence.We are The Dentists Insurance Company.
Learn more at tdicinsurance.com/rm
answers
Protecting dentists. It’s all we do.®
800.733.0633 | tdicinsurance.com | Insurance Lic. #0652783

C DA J O U R N A L , V O L 4 7 , Nº 1 2
812 D E C E M B E R 2 01 9
D E C . 2 0 1 9 R M M A T T E R S
and to make it clear that they could be subject to termination if they are caught violating the policy repeatedly.
Written policies are an employer’s best protection against excessive cellphone use during work hours. While banning cellphone use entirely isn’t feasible, it is appropriate to limit when employees can use phones, such as during meal and rest periods. It is also recommended that cellphones be kept with an employee’s personal belongings or in a drawer to avoid distraction.
It’s not enough to simply have a policy. Following through with disciplinary action demonstrates that you are committed to your policy. Employees will be less likely to break cellphone rules if they know that the policy is more than an empty threat.
Other cellphone-use considerations include:
■n Restricting locations where cellphone use is permitted. For example, it is reasonable to prohibit their use in operatories, in the front office or in the presence of patients.
■n Outlining what type of use is allowed. For example, texts and brief phone calls are fine, but downloading music or videos is not.
■n Minimizing disruptions. Employers can request that ringers are set to silent or vibrate, calls are kept brief and free from offensive language and employees speak quietly when on the phone.
■n Protecting privacy. Policies should prohibit taking photos or videos within the practice to protect patient privacy, unless preapproved by the dentist.
■n Employee safety. Employees should not use a cellphone while driving on company business or when engaged in physical activities such as carrying an instrument tray.
■n Infectious disease control. Cellphones are believed to harbor as much as 10 times the bacteria as toilet seats. But unlike toilets, people rarely disinfect their phones. A 2014 study showed cellphones are frequent contributors to hospital-acquired infections in the dental setting.
TDIC’s Risk Management team also warns dentists of the inherent risks of texting patients with regards to protecting privacy. It is recommended that dental practices avoid texting patients altogether, but if you must text a patient, be sure to avoid sending any protected health information and make sure the communication is documented in the patient’s chart. Text messaging is only considered HIPAA compliant under certain circumstances. If your practice intends to text patients regularly, seek a secure, HIPAA-compliant third-party vendor that offers the needed encryption.
It is also recommended that dental practices develop a policy regarding communication expectations between employees and their employer. For example, it is a best practice to call in sick, rather than send a text. If an employee is unable to report to work, it is advised they speak to the dentist or office manager directly by phone.
In a case reported to the Risk Management Advice Line, a dentist stated he received a text from an employee at 4 a.m. on a Saturday that conveyed she would not be able to make it to work that day. The dentist called the employee back immediately after receiving the text. When the employee answered, the dentist heard “what sounded like Vegas in the background.” He later found photos of a bridal shower at a local casino posted on the employee’s Facebook page. Had the employee called in, it would have been clear that she was
not, in fact, sick. But the office did not have such a policy in place at the time.
The issue in the above case was the informality of the communication. Texting reduces an employee’s accountability as well as the likelihood that these interactions will be documented in the employee’s file. Additionally, there are often cases in which an employee is texting nonmanagement staff members rather than those to whom they should be reporting. This should not be allowed. Following up with a phone call is not intended to catch employees doing something they shouldn’t be doing; rather, it is to have a conversation about the behavior and to inquire whether the employee has available sick time or PTO.
Cellphone-use policies should be documented in writing, signed by the employee and kept within the employee file. It’s important to note that dentists should model acceptable cellphone use in the office. Setting the tone means avoiding the impression of being distracted by a call and limiting phone use to appropriate times that do not interfere with patient care.
Cellphones are an integral part of our daily lives. It’s hard to imagine a time when we weren’t reachable every moment of every day or when we didn’t have access to information at our fingertips. In the workplace, smart cellphone policies as part of a comprehensive employee manual can help your office maintain productivity, increase professionalism and ensure patient privacy is protected. n
TDIC’s Risk Management Advice Line is a benefit of CDA membership. If you need to schedule a no-cost consultation with an experienced risk management analyst, visit tdicinsurance.com/RMconsult or call 800.733.0633.
4381 SOUTH SAN FRANCISCO GP Retiring dentist offering 23 yearpractice close to Kaiser Hospital. 4 op facility with new & recentlyupgraded equipment. Asking price to be determined.
4359 SANTA CRUZ GP offering 30+ years of goodwill within walkingdistance to the beach! Located in a well-established, attractive, singlestory professional building complex w/ample parking, good visibility andeasy access. 2 doctor days/week, 2 hygiene days/week, 380 activepatients with approx. 10 new patients/mo. 3 fully equipped ops in 850sq. ft. Average GR $250K with Average adj net of $135K. Asking price$150K.
4368 SANTA CLARA GP 25 year practice in community retail centernear Levi Stadium. Nice fully-equipped 2,100 sq. ft. facility with 5 ops.Average Gross Receipts base on 5 years is $583K. Asking $350K.
4380 SAN MATEO GP Unique opportunity to own a San Mateo GP.This location generates significant foot traffic. 1,498 square foot facilitywith 4 ops, reception area, business office, private office, staff lounge,lab area, sterilization area, bathroom, storage & dedicated parkingspaces. Current Gross Receipts annualizing at $431K with an adjustednet of $192K. Seller will help for smooth transition. Asking $292K.
4351 SEBASTOPOL AREA GP & BLDG. Charming practice situatedamidst rolling hills, soaring redwood trees and lush vineyards. Offering70+ years of goodwill. Beautiful, modern facility with 3 fully-equippedops (room for a 4th op) and digital x-ray. Equipment in pristine condition,most purchased 2016-2018. 2019 GR annualized at $679K+ with adj.net of $210K. Average 3.5 doctor days/week and 4 hygiene days/week. 800 active patients, all fee-for-service. Seller owns the building, itis available for purchase. Asking $305K for practice, $425K for building.Owner/doctor willing to help for smooth transition.
4370 SAN JOSE PROSTHODONTIC PRACTICE Cosmetic andprosthodontic practice established 40+ years. Located in a busycommercial/residential area of San Jose, close to several amenities,referral sources. 4 fully equipped ops in 1,074 sq. ft. facility. Lots of on-site parking and EZ freeway access. 3 yr. average GR $554K+ withaverage adjusted net of $180K. Approx 700 active patients, allcompletely fee-for-service (Seller is not contracted with any insurancecompanies or Delta). 2 days of hygiene/week. Owner transitioning intoretirement, will help for smooth transition. Asking $299K.
4338 PENINSULA PROSTHODONTIC PRACTICE Preeminent 45year Prosthodontic practice located in mid peninsula neighborhood. State-of-the-art 1,242 square foot facility with 5 operatories. Seller willing to helpin the transition. Outstanding referral sources. Average Gross Receipts$1.3M with 4 doctor-days per week. Asking $884K.
4382 MONTEREY COUNTY GP Gorgeous practice in scenicMonterey Bay peninsula in ample seller owned building with state-of-the-art equipment. $900K+ average annual gross receipts with 4 doctordays. Asking $678K.
4343 CAPITOLA GP Gorgeous, state-of-the-art practice offering 33+years of goodwill. Beautifully appointed office environment and building,located within minutes of charming downtown Capitola, known for itscolorful, seaside shops and restaurants tucked into a hillside alongSoquel Creek. Must see this office to appreciate its splendor. Asking$643K for practice. Seller owns building, it is available for purchase, orto lease.
4366 SONOMA COUNTY GP Fabulous practice and location withinone of the North Bay’s gems of a town. Classically beautiful and wellappointed office with 4 ops in 1,425 sq. ft. Fantastic storefront locationon a well traveled road, walking distance to the pedestrian-friendly centerof downtown. 900+ active patients, all fee-for-service. No Delta DentalPatients. 4 doctor days/week and 4 hygiene days/week. Last two yearsaverage GR $865K with average adj. net of $407K. Seller will help forsmooth transition. Asking $650K..
4375 LOS GATOS FACILITY Seller offering fully equipped, state-of-the-art, modern, 2 operatory facility including furniture, fixtures andleasehold assets in medical office building adjacent to Los GatosCommunity Hospital. Asking $250K.
4362 MARIN COUNTY GP Seller owned 1,550 square foot facility with5 fully-equipped ops. Owner/Doctor transitioning into retirement andoffering 36 years of goodwill in desirable area. Located on a well traveledroad in a charming town with temperate weather, easy, outdoor livingand natural beauty. Enjoy California living at its best. No Delta Premierpatients. Excellent reputation and word-of-mouth referrals. Seller willhelp for smooth transition. Average Gross Receipts last 2 yrs is $450K.Asking $248K for the practice. Bldg condo is available for purchase.
4355 SAN FRANCISCO ENDO Endodontic practice in signaturebuilding with wealth of referral sources. State-of-the-Art, modern, 1,027square foot office with 2 fully equipped ops. Well established, seller withsterling reputation willing to help for smooth transition.
4216 SIERRA NEVADA FOOTHILLS 23 year practice located in theheart of the Sierra Nevada foothills in modern building close to downtownarea. 1,024 square foot office with 4 fully- equipped ops., upgraded majorequipment and digital radiography. Average Gross Receipts $890K+ with56% average overhead. Asking price for practice $604K.
UPCOMING:Santa Cruz County GP, San Francisco GP, Redwood ShoresGP, & Fairfield GP
carroll.company [email protected] (650) 362-7004 (650) 362-7007
CARROLL& C O M P A N Y
“Matching the Right Dentist to the Right Practice”
Mike Carroll Pamela Carroll-Gardiner Mary McEvoy Carroll
Carroll & Company2055 Woodside Road, Suite 160Redwood City, CA 94061DRE #00777682
PENDING
SOLD
PENDING
PENDING
WE HAVE ANSWERS.When it comes to managing your practice, you’re not alone. Our smart analysts have dentistry-focused expertise in leadership, ownership, patient management, practice systems and transitions. Tap into one-on-one guidance by phone or explore an online library of tools and guides.
OVERWHELMED BY PRACTICE
MANAGEMENT?
800.232.7645cda.org/practicesupport
®
Practice ManagementEmployment PracticesDental Benefit PlansRegulatory Compliance
PRACTICE SUPPORT
C DA J O U R N A L , V O L 4 7 , Nº 1 2
DECEMBER 2 0 1 9 815
Aspects of the Health Insurance Portability and Accountability Act (HIPAA), which became law in 1996, continue to be misinterpreted by health care
providers who are covered entities. Dentists who do not understand basic elements of the law risk paying more for compliance efforts and can fail to meet the law’s standards. This article explains common misunderstandings heard by CDA Practice Support staff from dentists and their staff.
Every health care provider must comply with HIPAA rules.
Only health care providers that conduct certain transactions electronically are required to comply with HIPAA.1 The covered transactions include but are not limited to:
■n Submitting a claim for payment (even if it is submitted on paper to a claims clearinghouse that electronically submits the claims to the payer).
■n Checking patient eligibility for benefits and coverage under a plan.
■n Requesting authorization for treatment.
■n Requesting status of a claim.These health care providers,
along with claims clearinghouses and health plans, are generally referred to as HIPAA-covered entities.
Therefore, it is possible for a dental practice to maintain patient information electronically and to not have to comply with HIPAA because the practice does not conduct the covered transactions electronically. Regardless of HIPAA, all state health care providers must comply with California’s Confidentiality of Medical Information Act that is similar to HIPAA and is in some aspects more stringent.
HIPAA Myths ExplainedCDA Practice Support
Regulatory Compliance
HIPAA requires a written patient authorization in order to share patient information with family and friends.
Not in every situation. The law permits a HIPAA-covered entity to infer, based on professional judgment, that a patient does not object to the entity sharing information with family or individuals involved in the care of the patient.2 For example, a dental practice with a family as long-time patients may not need written authorization to share an adult child’s treatment information with a parent because the practice knows the parent coordinates every family member’s treatment. An example of when a dental practice may want to obtain written authorization is when an individual contacts the practice requesting information about proposed treatment for her elderly mother. The practice has never before seen or talked to the individual in the years the practice has treated the patient, so it should contact the patient to obtain authorization to disclose information. If this situation is altered a bit, for example if the individual accompanies her mother to an appointment for the first time, the dentist or staff can seek the patient’s
verbal consent before discussing her treatment in front of the individual. The practice can then presume the patient does not object to sharing her information with the individual.
The practice’s privacy officer should assess each unique request for patient information to determine if written authorization is necessary or required. A dental practice may elect to require written authorization in all requests for patient information but should consider that policy’s impact on patient care.
Providing patient information to another health care provider requires patient authorization.
This type of disclosure for the purpose of treating the patient is permitted without patient authorization, for example, when a general dentist forwards patient information to a specialist to whom they are referring a patient. In other circumstances, such as when a patient moves out of the area, a dental practice may require a patient’s written authorization to confirm the patient’s desire to share information with a new dentist.
It is a legal requirement to provide annual HIPAA training to employees.
HIPAA requires covered entities to train their workforce but its occurrence is not calendar dependent. Training at a small dental practice could be as simple as providing employees with the practice’s privacy and security policies and documenting their review.3 After initial training, employees should be trained again after a material change in office policy or in the law. An employee who has failed to follow the dental practice’s policies and procedure should be retrained.
Regardless of HIPAA, all state health care providers must comply with California’s Confidentiality of Medical Information Act that is similar to HIPAA and is in some aspects more stringent.
C DA J O U R N A L , V O L 4 7 , Nº 1 2
816 D E C E M B E R 2 01 9
D E C . 2 0 1 9 REGUL ATORY COMPL IANCE
The designated privacy officer and security officer should have a higher level of training because they are ultimately responsible for inventorying where the dental practice’s patient information is stored and how it moves, assessing risks to that information, implementing a risk management plan that includes required safeguards and developing the dental practice’s written policies and procedures. They are responsible for documenting the practice’s compliance efforts.
Patient information cannot be taken out of the facility.
Patient information can be taken out of the facility as long as there is a legitimate need to do so and the dental practice has taken reasonable safeguards to protect the information. For example, an associate dentist may need to follow up with patients in the evening after treatment. The practice should have a policy that describes the business reasons for which patient information may be taken out of the facility and that the information should be limited to the minimum necessary to accomplish the task. The policy can include details and options such as electronic communication of patient information and destruction or return of information after use.
Sharing treatment details without patient identifiers with a study club does not require patient authorization.
Has everything shared with a study club been stripped of patient identifiers? Does the context of the presentation provide clues about the patient? Just because information is not visible to the eye does not mean a digital image cannot be linked to an
individual. Digital images have metadata that can be linked to an individual if the image is posted online. It is best to obtain patient authorization to use their information for nontreatment purposes.
A covered entity must ensure electronic patient information is received securely.
A covered entity is responsible for the secure communication of patient information unless the patient has given informed consent to receiving the information via unsecure email. A covered entity should verify the recipient’s email address is correct but is not required to verify the recipient’s email inbox is secure. If the recipient is a HIPAA-covered entity, then the recipient is required to ensure stored electronic patient information is secure.
The Notice of Privacy Practices and business associate agreements are the only HIPAA documents required.
A covered entity investigated by the U.S. Department of Health and Human Services Office for Civil Rights for a patient complaint or security incident will be requested to produce myriad documentation. A description of required documents will be the subject of this column in January 2020. n
references
1. Centers for Medicare and Medicaid. Covered entity guidance. www.cms.gov/Regulations-and-Guidance/Administrative-Simplification/HIPAA-ACA/Downloads/CoveredEntitiesChart20160617.pdf.2. U.S. Department of Health and Human Services. Does the HIPAA Privacy Rule permit a doctor to discuss a patient’s health status, treatment or payment arrangements with the patient’s family and friends? www.hhs.gov/hipaa/for-professionals/faq/488/does-hipaa-permit-a-doctor-to-discuss-a-patients-health-status-with-the-patients-family-and-friends/index.html.3. U.S. Department of Health and Human Services. Generally, what does the HIPAA Privacy Rule require the average provider or health plan to do? www.hhs.gov/hipaa/for-professionals/faq/189/what-does-the-hipaa-privacy-rule-require-the-average-provider-to-do/index.html.
Regulatory Compliance appears monthly and features resources about laws that impact dental practices. Visit cda.org/practicesupport for more than 600 practice support resources, including practice management, employment practices, dental benefits plans and regulatory compliance.
Offices: 805.777.7707 818.991.6552 800.752.7461
LEE S
KARI
N&
ASSO
CIAT
ES IN
C.With scores of Buyers, profiles of their practice interests and financial ability, Lee Skarin & Associates is able to find the right buyer for your practice.
Experience the difference. Call Lee Skarin and Associates for responses to all of your questions - No obligation!
Visit our website for current listings: www.LeeSkarinandAssociates.comDental Practice Brokers CA DRE #00863149
EXPERIENCE THE DIFFERENCE • Lee Skarin and Associates has been serving the dental profession since 1959.• Kurt Skarin has over 30 years experience in dental practice sales.• We have sold more practices than any broker in the state within the last 12 months.• Our experienced practice appraisals are backed with credentials unequaled among dental practice brokers.• We provide in-house legal counsel to advise you in all aspects of the sale and purchase, including the tax consequences of the sale.• Excellent financing is available, in most cases for 100% of the purchase price.• With a reputation for experienced, conscientious, and ethical performance, we give our clients personal attention in all aspects of the purchase.
6170 SONOMA Long established practice anchored by 6-days of Hygiene. Great location in this desirable valley community. 2019 trending $745,000 in collections reflecting growth over 2018 which collected $705,000. Excellent staff available to continue with New Doc. Successor shall be able to grow practice as he / she appeals to younger demographic while retaining loyal patients.6169 VACAVILLE Long established Delta PPO practice. 5-days of hygiene. 2019 trending $700,000+ with Available Profits of $280,000. Great north side location. Full Price $300,000. 6168 SACRAMENTO’S CAMPUS COMMONS “Bread & butter” Delta PPO practice averages $480,000 in collections per year. Well liked Dentist. 10+ weeks off a year. 4-days of Hygiene. 3-D Cone Beam. Great implant upside as retirees in area require this service. Full Price $200,000.6167 NORTH SANTA CLARA COUNTY - “OUT-OF-NETWORK” Perfect for Skilled Dentist who seeks strong patient relationships and wants to be insurance independent! 2019 trending $840,000+ on Owner’s 3-day week. Office has been upgraded and charting is paperless.6166 TRI-VALLEY’S PLEASANTON 2019 trending $850,000+ in collections. Averages 20 new patients per month. Attractive 4-op office, Digital Pan and Fabrication Center. Available Profits of $465,000.6165 ROSEVILLE ORTHO – “OUT-OF-NETWORK” Stanford Ranch. Great satellite office. $455,000 invested in build-out, furnishings, computers and equipment. 3-chair Bay. Digital Pan with Ceph. 51 active patients and averages 3 New Patients per month. Full Price $150,000.6164 SAN FRANCISCO BAY AREA - “OUT-OF-NETWORK” Highly regarded as evidenced by 25+ new patients per month. Collections have topped $2 Million in each of the last 3-years with Profits averaging $1 Million. Paperless. 3D Cone Beam. Great location. Seller shall work-back to affect orderly transition. Rare opportunity for Dentist seeking Superior Platform to practice their craft at highest level.6163 LAKEPORT Attractive option to practicing in ultra-competitive settings in expensive housing markets. Appeal of practicing here is ability live a less hectic life. Decompress, have more time for yourself. Beautiful 6-op facility with high-end technology and completely networked. 2018 collected $956,000 with Profits of $360,000. 2019 trending $1.1+ Million in collections. Building optional purchase. Full Price $240,000.6158 FORTUNA Relaxed lifestyle in Humboldt County’s Banana Belt. Adjacent to Ferndale. Perfect for Dentist seeking small town living. 2018 Collected $395,000 with $156,000 in Profits. 2019 trending$400,000+. 6-weeks off. Lots of work referred. Full Price $75,000.6157 SACRAMENTO’S ELK GROVE AREA - “SOLD” 2018 collected $909,000 on Owner’s 3-day week. Successor can increase to 4-days as practice is rich in patients. 25+ new patients per month. 5-ops, digital Pan, strong Recall, great staff.6152 SAN RAFAEL - “SOLD” 2018 collected $520,000. Stand-alone building optional purchase. Nearby DDS who desires their own building should relocate their practice and have instant $1+ Million practice in superior location.6147 SAN FRANCISCO BAY AREA - “OUT-OF-NETWORK” - “SOLD” 2018 collected $2.2 Million. Hygiene produced $1+ Million.$700,000+ in profits. Seller available for long transition.
NORTHERN CALIFORNIA(415) 899-8580 – (800) 422-2818
Raymond and Edna [email protected]
California DRE License 1422122
SOUTHERN CALIFORNIA(714) 832-0230 – (800) 695-2732Thomas Fitterer and Dean George
California DRE License 324962
4003 PEDO CHINESE / HISPANIC 3,000+ Charts. Move to your office. Full Price $150,000. 4006 ALTA LOMA High identity Center. Absentee. Grossing $700,000. 5-ops, 3 equipped.4009 IRVINE Lady DDS Grossing $1 Million. 5-ops. Partnership.4011 DIAMOND BAR This is a Dream Million Dollar location to be. 5-ops. Several Restaurants bring in droves of customers on a daily basis, FP $150,000.4013 ORANGE COUNTY BEACH CITY Grossed $70,000 last month. 4-ops with room for more. Full Price $800,000. 4015 HEMET Easy way to Gross $500,000. Grossing $240,000 on 1-day per week. Full Price $110,000.4019 $1 MILLION NET PROFIT Opportunity of a lifetime.APPLE VALLEY Grosses $500,000 to $600,000. 3 ops. Low overhead. BAKERSFIELD AREA Grossing $40,000/month on 2 day week. DIAMOND BAR 5-ops with digital Pan. Very busy future here. Full Price $150,000IRVINE Lady DDS grossing $1 Million. Will share office.LA HABRA Huge Shopping Center. Well maintained. PT Seller will stay. LADERA RANCH 4-ops. Grossing $500,000. High Growth area. LAGUNA WOODS Grossed $800,000 during Renovation. Renovation done. Should gross $1 Million.LOS ALAMITOS Established 4-ops with real estate. MIRACLE MILE NEAR FAIRFAX Beautiful corner suite with Wilshire view. 3-ops recently remodeled.ORANGE Grossing $1.2 Million. State-of-art beautiful!ORANGE COUNTY High profile shopping center. Grossing $1.5 Million. ORANGE COUNTY Near Chapman / Tustin Streets. Gross $400,000. Merge or grow.ORANGE COUNTY BEACH 5-ops. Gross $1.2 Million first year. Area growing. ORANGE COUNTY BEACH CITY Absentee. Grossing $900,000+. 4-ops, room for 5th. Hands-on Owner will do $1 Million first year. ORANGE COUNTY BEACH CITY Grossing $800,000 part-time. Valuable Real Estate may be available.PALM SPRINGS AREA Grossing $1.5 Million. 8-ops. REDLANDS 5-ops. Grossing $500,000. Low overhead. Part Time Seller. Full Price $450,000.RIVERSIDE Lady DDS grossing $300,000. 3-ops. Full Price $250,000. SAN JUAN CAPISTRANO BEACH Grossing $200,000 on 16 hour week. SANTA CLARITA 70,000 Autos pass daily. Tremendous upside. Full Price $250,000.SOUTH ORANGE COUNTY Crown Valley Shopping Center. 4 ops. Grossing near $800,000. Lots of new home development. UNION PRACTICE - INLAND EMPIRE Grossing $650,000 on 2.5 day week. Nets close to $400,000.UPLAND 3-ops, low overhead. Seller will transition. Full Price $360,000. WANTED: IRVINE - NEWPORT BEACH - COSTA MESA - TUSTIN “High Fee-for-Service” Dentist lost lease. Seller will merge his 40-year practice doing $800,000 into yoursWEST LOS ANGELES Prestigious Medical Building. Grossing $800,000. WESTMINISTER Starter in busy strip center. One side Hispanic, other side Vietnamese. Full Price $85,000.
PracticesWanted
Specialists in the Sale and Appraisal of Dental PracticesServing California Dentists since 1966
How much is your practice worth??PPS extends Our Wishes for a
Wonderful Holiday and Happy New Year
C DA J O U R N A L , V O L 4 7 , Nº 1 2
DECEMBER 2 0 1 9 819
The call came from another office in town just before Christmas asking if we could see one of their patients because their dentists were gone for the
holidays. I must admit I was surprised at how upset the patient was at his dentist and how willing he was to share the tale. Seems he broke a cusp on tooth No. 31 a few weeks prior. Other than a sharp edge, the tooth was without any symptoms. He was informed by his dentist that he needed a crown on No. 31. And because tooth No. 30 had a large previously placed amalgam and the patient hadn’t used his calendar maximum, his dentist also recommended preventing future fracture by placing a crown on No. 30 at the same time. This sounded reasonable, so the patient agreed. As soon as the anesthetic wore off after the procedure, the patient’s lower right side was very painful and extremely cold sensitive. To make matters worse, the temporaries came off within a week and the sensitivity got much more intense. They were recemented and promptly came off again. The next time they came off was when I got the call. I made custom temporaries to get him through the holidays with the hopes the sensitivity would lessen.
The patient returned a couple of days later and happily told me the temporaries were doing just fine. He asked if he should keep his appointment with his previous dentist to have the final restorations cemented. I told him there is a world of difference between temporaries and permanent crowns and that he absolutely should keep that appointment.
A few weeks later the patient returned mad as a hornet. Since the crowns were cemented, the teeth had been hurting. From his description of the discomfort, it didn’t sound like
How To Handle a Difficult SituationHenrik Hansen, DDS
Ethics
irreversible pulpitis, just severe pulpal inflammation. I checked the occlusion, which was OK. The PA showed no evident apical pathology, but the BW had significant mesial and distal open margins on Nos. 30 and 31. I informed the patient of the open margins and that they needed to be redone. The CDA Code of Ethics supports informing patients of the status of their oral health if the comments are justifiable and not based on opinion (section 1F, Obligation to Inform). The patient said he felt something wasn’t quite right when he could put his fingernail under the crowns on the facial. I tried to get him to agree to return to his dentist and said I would gladly forward the films to their office. He adamantly refused to consider this. I then told him of a wonderful program that CDA has called Peer Review and how fair and impartial it is. His comment was that he’s been in constant pain for months, except during the time he was wearing my temps, and that he wanted this fixed now. He then asked if I would call his dentist.
As I prepared myself to make the call, I couldn’t help but reflect on a call I had received many years ago from a dentist who informed me that one of my previous patients, who I had done a deep composite restoration on, was having severe pain in the tooth. He told me that on his films, which he emailed to me, there appeared to be decay that was not completely removed. Other than the fact that it was a heart-stopping experience, I remember clearly the kind and compassionate way he delivered the bad news. Therefore, when I called this dentist, I not only told him of the open margins and the patient’s refusal to return or consider peer review, I
also said that from my many years of peer review I had learned that even in the hands of the finest dentist, not everything turns out as we would hope. Crowns that don’t fully seat happen. I also said the patient was very angry and that I feared there might be a potential lawsuit. The dentist’s office manager called back within the hour and asked if we would replace the crowns, which we did. I believe that, being human, we all make mistakes. What matters is what we learn from them and what we do about it when mistakes happen. I believe the dentist made a wise decision and avoided a potential nightmare.
This type of situation is not easy to handle and brings up the ethical principles of veracity (being truthful) and professionalism. If done well, a hostile situation can be defused and respect for the profession enhanced. n
Henrik Hansen, DDS, is a general dentist practicing in Fairfield, Calif. He currently serves on the CDA Judicial Council and is a past chair of the Council on Peer Review as well as a past member of the ADA Council on Dental Benefit Programs.
Have an ethical question you’d like to have addressed by the Judicial Council? Email [email protected].
BAY AREA CONTINUED CC-979 NOVATO: Seller Retiring. 803 sf w/ 3 ops near downtown and Old Town Novato. $195K (Real Estate $215k) CC-1030 SANTA ROSA: Condo office in modern bldg w/ ample parking & adjoining Ortho prac-tice! 1683 sf w 5 ops $325k CC-1049 SANTA ROSA: Fully Remodeled, Amazing Location. 2000 sf w/ 5 ops $685k Real Estate Also Available CC-1074 SANTA ROSA: Unbelievable Buildouts! 1200 sf 3 ops $300k CG-616 NAPA COUNTY: State-of-the-Art office! ~850 sf w/ 2 Ops. $250k CG-995 VALLEJO: Live, play and practice here where your lifestyle can’t be beat! ~2035 sf w/ 7 ops $1.175M CG-1048 SONOMA: This highly successful family-oriented practice has it ALL! ~1500 sf w/ 4 ops Reduced $630k CN-911 SANTA ROSA: Want a change in life-style? This fabulous practice is the heart of the Wine Country! 2250 sf w/4 ops + 1add’l. $499k DG-862 MID-PENINSULA: Rare gem with up to 7 operatories in the Bay Area! ~2274 sf w/ 6ops + 1 add’l. $475k DG-986 CAMPBELL: The ideal opportunity to practice in this community! ~988 sf w/ 3 ops $288k DG-1006 MONTEREY AREA: This practice is one which every dentist aspires to! ~3400 sf w/ 8 ops Reduced $1.325M DG-1009 CARMEL: Amazing fee-for-service practice w/ no contracts! ~1150 sf w/ 4 ops $625K DG-1014 MONTEREY: Don’t miss your opportuni-ty to live and practice in beautiful Monterey! ~1125 sf w/ 4 Ops. Reduced $750k DG-1034 BELMONT: Med Prof Bldg on bustling commercial corridor. ~2000 sf w/ 5 ops $425k DG-1035 LOS GATOS: Over 40 years Goodwill in this charming community! ~1010 sf w/ 4 ops. $790k DG-1042 MOUNTAIN VIEW: Amazing opportunity providing quality, high-end dentistry! ~ 890 sf w/ 3 Ops $895K DG-1078 SARATOGA Ortho: One-of-a-kind, mod-ern, high-tech orthodontic boutique practice! ~ 1400 sf w/ 5 Ops $980K DN-1031 CUPERTINO: This remarkable practice awaits only your talent and skill! 1500sf w 3 ops + 1 add’l. $1.25M
BAY AREA AC-989 SAN FRANCISCO (Facility): Busy Retail Shop-ping Plaza w/ major anchor tenants! 3 ops $125k AC-1059 DALY CITY: Amazing practice w/ seasoned staff in highly desirable neighborhood. 1500 sf w/ 4 ops $345k AC-1072 DALY CITY: Seller to work back until May 2022! 1045 sf w/ 3 ops. Plumbed for 1 add’l $450k AG-871 SAN FRANCISCO: Seller Motivated! ~600 sf w/ 2 ops Price Reduced $65k AG-944 SAN FRANCISCO: An opportunity like this does not come along very often! ~998 sf w/ 3 ops Reduced $540k AG-945 SOUTH SAN FRANCISCO: ~1800 sf w/ 4 ops $495k AG-993 WEST PORTAL AREA: Desirable area w/ easy commute to downtown San Francisco. ~1000sf w/ 3 ops Reduced Price: $395k BC-741 DANVILLE (FACILITY): ~ 1600 sf w/ 3 ops. PRICED TO SELL! $10k BC-949 ALBANY: Desirable commercial/residential area. Medical Prof Bldg w/ good frontage. 3200sf w/ 4 ops $695k Real Estate: $1.8 BC-1010 ANTIOCH: Health Prof. Complex 2118 sf w/ 2 equipped ops + 3 add’l $250k BC-1022 OAKLAND: “Pill Hill” Area near hospital! 1064 sf & 2 ops. Plumbed for 1 add’l $150k BC-1056 SAN RAMON (Facility): Move-in ready facility in well maintained professional complex. 1698 sf w/ 4 ops $80k BG-1025 WALNUT CREEK: You won’t find a more outstanding opportunity than this extraordinary practice! ~2138 sf w/ 6 ops. $750k Real Estate: $995k BN-952 BERKELEY: Don’t hesitate on this incredible opportunity! ~835 sf w/ 3 Ops. Seller Motivated $200k BN-1023 RICHMOND: This is a rich opportunity for the astute dentist! 1450sf w/2 ops + 2 add’l. $50k/ Real Estate $750k BN-1038 BERKELEY: A perfect opportunity to own a practice in one the Bay Area’s most popular cities! 1000sf w/ 3ops. $385k BN-1060 LAYAFETTE: Imagine living, practicing & raising your family here in this community! 1400sf w/ 3op. Seller Motivated $225k CC-846 SAN RAFAEL: Prof/Retail Building Complex. 3 ops 640 sf Collections $433k in 2017 $275k CC-927 SAN RAFAEL: Build the practice of your dreams by increasing this 2-day work week! 800 sf w/ 3 ops $175k
Jon B. Noble, MBA Mona Chang, DDS John M. Cahill, MBA
BAY AREA CONTINUED DN-1032 PLEASANTON Facility: The perfect place to live, practice & raise a family! 1400sf w/4ops. Includes CT Scan! $185k DN-1041 SAN JOSE: This stunning practice is an excellent opportunity for new grads! 1207sf w 2ops + 1 add’l. Reduced! $175k DN-1003 PLEASANTON Facility: This is an excellent opportunity for a gradu-ate or a dentist seeking a Satellite location. 1000sf w/ 3ops. $68k DN-1046 SANTA CRUZ AREA: Opportunities like this does not come along, except once in a lifetime! Office 2050 sf w/ 5 ops. Total sq ft 3880. $595k /Real Estate: $1.1mil DN-1067 CASTRO VALLEY: Conservative treatment & compassionate philos-ophy delivered in a warm environment. 1498sf w/ 5ops. $650k/Real Estate: $675k
NORTHERN CALIFORNIA EC-1018 WEST SACRAMENTO: All new leaseholds & top of the line PC EQ in 5 ops! 6 ops currently in use. 10 ops total available! $795k EG-910 MIDTOWN SACRAMENTO: A thriving practice does not come along very often! ~1107 sf w/ 2 + 1 add’l. Reduced $210k EG-968 SACRAMENTO: Desirable, mid-town neighborhood, w/ ample parking in garage! ~1527 sf w/ 5 Ops. Reduced $480k EG-972 ELK GROVE: Prime location! Real Estate available to purchase in the future! ~ 3500 sf w/ 8 ops+. Reduced $495k EG-1012 EAST SACRAMENTO: A practice like this one does not come available very often! ~ 2900 sf w/ 8 ops. $2.5M EG-1016 LINCOLN: Look no further than this growing community to springboard into your success! ~1800 sf w/ 4 Ops Reduced $560k EG-1039 EL DORADO HILLS VICINITY: The ideal opportunity to practice in this community! ~1100 sf w/ 4 Ops. $350k EG-1061 SOUTH AUBURN VICINITY: Come live, play and practice in the heart of this pristine town! ~1100 sf w/ 4 Ops. $350k EN-1051 SACRAMENTO: Location, Accessibility and Quality Relationships! 1,671sf w/ 5ops. $395k EN-1052 EAST SACRAMENTO: Remarkable, long-established opportunity, loaded w/ goodwill! 1100 sf w/ 4 ops. $950k EN-1055 ROCKLIN Facility: Build your own success here in this family-oriented community! 1650 sf w/ 4 ops +1 add’l. $95k EN-1077 DAVIS: Imagine living and practicing here! Hesitate and you may miss out on your dream! 1100sf. w/ 5 ops. $575k FC-650 FORT BRAGG: Family-oriented practice. 5 ops in 2000 sf $350k for the Practice & $400k for the Real Estate FG-841 ARCATA: Great demographics w/ very little competition! ~1114 sf w/3 ops Reduced Price: $200k/ Real Estate Available FN-961 EUREKA: Where the quality of life can’t be beat! 1400sf w. 4 ops. Practice Reduced: $395k/ Real Estate Available $395k! FN-855 NO. HUMBOLDT: Seller relocating! Long-established, 100% FFS practice! 1600 sf w/ 3ops + 1 add’l. $190k/ Real Estate Available GN-953 CHICO: Established for 34 years and the seller is passing their good-will on to you! 1067sf w/ 3ops. Now Only $220k! GN-1071 REDDING: Streamlined policies & loyal patient base, this quality practice is your springboard to success! 2264sf w/ 4 ops. $525k
NORTHERN CALIFORNIA CONTINUED HG-1053 GRASS VALLEY: Well-established practice of 40+ years, known for its quality dentistry! ~1200 sf w/ 3 ops $420K HG-1068 LAKE TAHOE AREA: ~2500 sf w/ 3 Ops. Reduced $315k /Real Es-tate Available HG-815 TRUCKEE AREA: Amazingly priced at 50% of Collections! ~1000 sf w/ 3 ops $165k/ Real Estate Available HG-983 GRASS VALLEY: Newly remodeled office in highly desirable neighbor-hood! ~1250 sf w/ 3 ops. Reduced Price $195k/Real Estate Available HG-987 LAKE TAHOE AREA: State-of-the-Art Practice located in picturesque mountain setting! ~ 3,400 sf w/ 6 Ops $785K HN-879 SONORA: Great Cash-Flow for Only 3 Days a Week! 2950 sf w/ 3 ops Reduced Price: $265k HG-934 GRASS VALLEY: Underworked PT base should support larger pro-duction numbers! ~1200 sf w/ 3 Ops Reduced $168,750/Real Estate Availa-ble HN-999 CALAVERAS Co. (Facility/Real Estate): 1,500 sf w/ 2 equipped Ops + 1 fully plumbed & 3 partially plumbed. $500k HN-991 PLACERVILLE: Quality, conservative and compassionate practice! Will consider work back. 1,654 + 473 sf w 5 ops. $675k
CENTRAL VALLEY IG-881 TURLOCK: Long established has unsurpassed quality care. ~3500 sf w/ 10 Ops (shared). Reduced: $295k IG-1007 GREATER MODESTO AREA: Combines a quality learning environ-ment with relaxed rural living. ~3000sf w/ 6 ops. $645k IG-1009 TRACY: This opportunity is waiting for you to sink your roots down and invest your future here! ~1200sf w/ 4 ops. $745k IN-1069 STOCKTON: Well-established & fully equipped w/ modern equip-ment, this is an excellent opportunity! 1450sf w/ 3ops +1 add’l. $260k JC-811 FRESNO COUNTY: Seller willing to consider Associateship for qualified DDS w. intention to Buy In! Considerable Goodwill in Community! 3,000 sf w/ 6 ops $350k JC-823 LOS BANOS: Heavy emphasis on hygiene. 1000 sf w/ 3 ops $80k JC-1054 VISALIA: Practice AND REAL ESTATE! Prof Bldg on major thorough-fare. 2,260 sf w/ 6 ops $275k/ Real Estate $517k
SPECIALTY PRACTICES BC-784 CENTRAL CONTRA COSTA CO Perio: Seasoned Staff. 3 ops $295k BG-843 WALNUT CREEK Perio: Priced at 50% of collections! 4 ops $390k BG-1024 WALNUT CREEK Prosth:~2138 sf w/ 6 ops. $750k Real Estate: $995k BN-998 WALNUT CREEK/SAN RAMON AREA Ortho: Looking for your dream Orthodontic practice! 1450 sf w/ 5 Open bays/Chairs. $1.150M DN-1044 FOSTER CITY Pedo: Shared Space Situation. Conveniently located within walking distance of major corporations. 830sf w/ 3 ops. $195k GG-940 NORTH OF SACRAMENTO Pedo: Practice is on track to collect more than $1,000,000 in revenues this year! ~4300 sf w/ 5 ops. Reduced $555k JG-757 VISALIA Perio: Incredible Giveaway at this price! Collections over $800k! ~2000 sf w/ 5 ops Steal at $150k
Edmond P. Cahill, JD Timothy Giroux, DDS
800.641.4179 [email protected] “ASK THE BROKER” can now be found at WWW.WESTERNPRACTICESALES.COM
Your Life’s Work Comes Down To
This Decision
What separates us from other brokerage firms?
Western Practice Sales is locally owned by dentists and has been proudly serving dentists in California for over 45 years. Our personal attention to our sellers and reputation of integrity and honesty has made us Northern California’s Preferred Dental Practice Broker.
Our extensive buyer database
allows us to offer you…
Better Exposure Better Fit
Better Price!
Call or email today for a free copy of Dr Giroux’s book
Top Ten Issues for
Dentists Contemplating Retirement in Ten
Years or Less
BAY AREA CONTINUED CC-979 NOVATO: Seller Retiring. 803 sf w/ 3 ops near downtown and Old Town Novato. $195K (Real Estate $215k) CC-1030 SANTA ROSA: Condo office in modern bldg w/ ample parking & adjoining Ortho prac-tice! 1683 sf w 5 ops $325k CC-1049 SANTA ROSA: Fully Remodeled, Amazing Location. 2000 sf w/ 5 ops $685k Real Estate Also Available CC-1074 SANTA ROSA: Unbelievable Buildouts! 1200 sf 3 ops $300k CG-616 NAPA COUNTY: State-of-the-Art office! ~850 sf w/ 2 Ops. $250k CG-995 VALLEJO: Live, play and practice here where your lifestyle can’t be beat! ~2035 sf w/ 7 ops $1.175M CG-1048 SONOMA: This highly successful family-oriented practice has it ALL! ~1500 sf w/ 4 ops Reduced $630k CN-911 SANTA ROSA: Want a change in life-style? This fabulous practice is the heart of the Wine Country! 2250 sf w/4 ops + 1add’l. $499k DG-862 MID-PENINSULA: Rare gem with up to 7 operatories in the Bay Area! ~2274 sf w/ 6ops + 1 add’l. $475k DG-986 CAMPBELL: The ideal opportunity to practice in this community! ~988 sf w/ 3 ops $288k DG-1006 MONTEREY AREA: This practice is one which every dentist aspires to! ~3400 sf w/ 8 ops Reduced $1.325M DG-1009 CARMEL: Amazing fee-for-service practice w/ no contracts! ~1150 sf w/ 4 ops $625K DG-1014 MONTEREY: Don’t miss your opportuni-ty to live and practice in beautiful Monterey! ~1125 sf w/ 4 Ops. Reduced $750k DG-1034 BELMONT: Med Prof Bldg on bustling commercial corridor. ~2000 sf w/ 5 ops $425k DG-1035 LOS GATOS: Over 40 years Goodwill in this charming community! ~1010 sf w/ 4 ops. $790k DG-1042 MOUNTAIN VIEW: Amazing opportunity providing quality, high-end dentistry! ~ 890 sf w/ 3 Ops $895K DG-1078 SARATOGA Ortho: One-of-a-kind, mod-ern, high-tech orthodontic boutique practice! ~ 1400 sf w/ 5 Ops $980K DN-1031 CUPERTINO: This remarkable practice awaits only your talent and skill! 1500sf w 3 ops + 1 add’l. $1.25M
BAY AREA AC-989 SAN FRANCISCO (Facility): Busy Retail Shop-ping Plaza w/ major anchor tenants! 3 ops $125k AC-1059 DALY CITY: Amazing practice w/ seasoned staff in highly desirable neighborhood. 1500 sf w/ 4 ops $345k AC-1072 DALY CITY: Seller to work back until May 2022! 1045 sf w/ 3 ops. Plumbed for 1 add’l $450k AG-871 SAN FRANCISCO: Seller Motivated! ~600 sf w/ 2 ops Price Reduced $65k AG-944 SAN FRANCISCO: An opportunity like this does not come along very often! ~998 sf w/ 3 ops Reduced $540k AG-945 SOUTH SAN FRANCISCO: ~1800 sf w/ 4 ops $495k AG-993 WEST PORTAL AREA: Desirable area w/ easy commute to downtown San Francisco. ~1000sf w/ 3 ops Reduced Price: $395k BC-741 DANVILLE (FACILITY): ~ 1600 sf w/ 3 ops. PRICED TO SELL! $10k BC-949 ALBANY: Desirable commercial/residential area. Medical Prof Bldg w/ good frontage. 3200sf w/ 4 ops $695k Real Estate: $1.8 BC-1010 ANTIOCH: Health Prof. Complex 2118 sf w/ 2 equipped ops + 3 add’l $250k BC-1022 OAKLAND: “Pill Hill” Area near hospital! 1064 sf & 2 ops. Plumbed for 1 add’l $150k BC-1056 SAN RAMON (Facility): Move-in ready facility in well maintained professional complex. 1698 sf w/ 4 ops $80k BG-1025 WALNUT CREEK: You won’t find a more outstanding opportunity than this extraordinary practice! ~2138 sf w/ 6 ops. $750k Real Estate: $995k BN-952 BERKELEY: Don’t hesitate on this incredible opportunity! ~835 sf w/ 3 Ops. Seller Motivated $200k BN-1023 RICHMOND: This is a rich opportunity for the astute dentist! 1450sf w/2 ops + 2 add’l. $50k/ Real Estate $750k BN-1038 BERKELEY: A perfect opportunity to own a practice in one the Bay Area’s most popular cities! 1000sf w/ 3ops. $385k BN-1060 LAYAFETTE: Imagine living, practicing & raising your family here in this community! 1400sf w/ 3op. Seller Motivated $225k CC-846 SAN RAFAEL: Prof/Retail Building Complex. 3 ops 640 sf Collections $433k in 2017 $275k CC-927 SAN RAFAEL: Build the practice of your dreams by increasing this 2-day work week! 800 sf w/ 3 ops $175k
Jon B. Noble, MBA Mona Chang, DDS John M. Cahill, MBA
BAY AREA CONTINUED DN-1032 PLEASANTON Facility: The perfect place to live, practice & raise a family! 1400sf w/4ops. Includes CT Scan! $185k DN-1041 SAN JOSE: This stunning practice is an excellent opportunity for new grads! 1207sf w 2ops + 1 add’l. Reduced! $175k DN-1003 PLEASANTON Facility: This is an excellent opportunity for a gradu-ate or a dentist seeking a Satellite location. 1000sf w/ 3ops. $68k DN-1046 SANTA CRUZ AREA: Opportunities like this does not come along, except once in a lifetime! Office 2050 sf w/ 5 ops. Total sq ft 3880. $595k /Real Estate: $1.1mil DN-1067 CASTRO VALLEY: Conservative treatment & compassionate philos-ophy delivered in a warm environment. 1498sf w/ 5ops. $650k/Real Estate: $675k
NORTHERN CALIFORNIA EC-1018 WEST SACRAMENTO: All new leaseholds & top of the line PC EQ in 5 ops! 6 ops currently in use. 10 ops total available! $795k EG-910 MIDTOWN SACRAMENTO: A thriving practice does not come along very often! ~1107 sf w/ 2 + 1 add’l. Reduced $210k EG-968 SACRAMENTO: Desirable, mid-town neighborhood, w/ ample parking in garage! ~1527 sf w/ 5 Ops. Reduced $480k EG-972 ELK GROVE: Prime location! Real Estate available to purchase in the future! ~ 3500 sf w/ 8 ops+. Reduced $495k EG-1012 EAST SACRAMENTO: A practice like this one does not come available very often! ~ 2900 sf w/ 8 ops. $2.5M EG-1016 LINCOLN: Look no further than this growing community to springboard into your success! ~1800 sf w/ 4 Ops Reduced $560k EG-1039 EL DORADO HILLS VICINITY: The ideal opportunity to practice in this community! ~1100 sf w/ 4 Ops. $350k EG-1061 SOUTH AUBURN VICINITY: Come live, play and practice in the heart of this pristine town! ~1100 sf w/ 4 Ops. $350k EN-1051 SACRAMENTO: Location, Accessibility and Quality Relationships! 1,671sf w/ 5ops. $395k EN-1052 EAST SACRAMENTO: Remarkable, long-established opportunity, loaded w/ goodwill! 1100 sf w/ 4 ops. $950k EN-1055 ROCKLIN Facility: Build your own success here in this family-oriented community! 1650 sf w/ 4 ops +1 add’l. $95k EN-1077 DAVIS: Imagine living and practicing here! Hesitate and you may miss out on your dream! 1100sf. w/ 5 ops. $575k FC-650 FORT BRAGG: Family-oriented practice. 5 ops in 2000 sf $350k for the Practice & $400k for the Real Estate FG-841 ARCATA: Great demographics w/ very little competition! ~1114 sf w/3 ops Reduced Price: $200k/ Real Estate Available FN-961 EUREKA: Where the quality of life can’t be beat! 1400sf w. 4 ops. Practice Reduced: $395k/ Real Estate Available $395k! FN-855 NO. HUMBOLDT: Seller relocating! Long-established, 100% FFS practice! 1600 sf w/ 3ops + 1 add’l. $190k/ Real Estate Available GN-953 CHICO: Established for 34 years and the seller is passing their good-will on to you! 1067sf w/ 3ops. Now Only $220k! GN-1071 REDDING: Streamlined policies & loyal patient base, this quality practice is your springboard to success! 2264sf w/ 4 ops. $525k
NORTHERN CALIFORNIA CONTINUED HG-1053 GRASS VALLEY: Well-established practice of 40+ years, known for its quality dentistry! ~1200 sf w/ 3 ops $420K HG-1068 LAKE TAHOE AREA: ~2500 sf w/ 3 Ops. Reduced $315k /Real Es-tate Available HG-815 TRUCKEE AREA: Amazingly priced at 50% of Collections! ~1000 sf w/ 3 ops $165k/ Real Estate Available HG-983 GRASS VALLEY: Newly remodeled office in highly desirable neighbor-hood! ~1250 sf w/ 3 ops. Reduced Price $195k/Real Estate Available HG-987 LAKE TAHOE AREA: State-of-the-Art Practice located in picturesque mountain setting! ~ 3,400 sf w/ 6 Ops $785K HN-879 SONORA: Great Cash-Flow for Only 3 Days a Week! 2950 sf w/ 3 ops Reduced Price: $265k HG-934 GRASS VALLEY: Underworked PT base should support larger pro-duction numbers! ~1200 sf w/ 3 Ops Reduced $168,750/Real Estate Availa-ble HN-999 CALAVERAS Co. (Facility/Real Estate): 1,500 sf w/ 2 equipped Ops + 1 fully plumbed & 3 partially plumbed. $500k HN-991 PLACERVILLE: Quality, conservative and compassionate practice! Will consider work back. 1,654 + 473 sf w 5 ops. $675k
CENTRAL VALLEY IG-881 TURLOCK: Long established has unsurpassed quality care. ~3500 sf w/ 10 Ops (shared). Reduced: $295k IG-1007 GREATER MODESTO AREA: Combines a quality learning environ-ment with relaxed rural living. ~3000sf w/ 6 ops. $645k IG-1009 TRACY: This opportunity is waiting for you to sink your roots down and invest your future here! ~1200sf w/ 4 ops. $745k IN-1069 STOCKTON: Well-established & fully equipped w/ modern equip-ment, this is an excellent opportunity! 1450sf w/ 3ops +1 add’l. $260k JC-811 FRESNO COUNTY: Seller willing to consider Associateship for qualified DDS w. intention to Buy In! Considerable Goodwill in Community! 3,000 sf w/ 6 ops $350k JC-823 LOS BANOS: Heavy emphasis on hygiene. 1000 sf w/ 3 ops $80k JC-1054 VISALIA: Practice AND REAL ESTATE! Prof Bldg on major thorough-fare. 2,260 sf w/ 6 ops $275k/ Real Estate $517k
SPECIALTY PRACTICES BC-784 CENTRAL CONTRA COSTA CO Perio: Seasoned Staff. 3 ops $295k BG-843 WALNUT CREEK Perio: Priced at 50% of collections! 4 ops $390k BG-1024 WALNUT CREEK Prosth:~2138 sf w/ 6 ops. $750k Real Estate: $995k BN-998 WALNUT CREEK/SAN RAMON AREA Ortho: Looking for your dream Orthodontic practice! 1450 sf w/ 5 Open bays/Chairs. $1.150M DN-1044 FOSTER CITY Pedo: Shared Space Situation. Conveniently located within walking distance of major corporations. 830sf w/ 3 ops. $195k GG-940 NORTH OF SACRAMENTO Pedo: Practice is on track to collect more than $1,000,000 in revenues this year! ~4300 sf w/ 5 ops. Reduced $555k JG-757 VISALIA Perio: Incredible Giveaway at this price! Collections over $800k! ~2000 sf w/ 5 ops Steal at $150k
Edmond P. Cahill, JD Timothy Giroux, DDS
800.641.4179 [email protected] “ASK THE BROKER” can now be found at WWW.WESTERNPRACTICESALES.COM
Your Life’s Work Comes Down To
This Decision
What separates us from other brokerage firms?
Western Practice Sales is locally owned by dentists and has been proudly serving dentists in California for over 45 years. Our personal attention to our sellers and reputation of integrity and honesty has made us Northern California’s Preferred Dental Practice Broker.
Our extensive buyer database
allows us to offer you…
Better Exposure Better Fit
Better Price!
Call or email today for a free copy of Dr Giroux’s book
Top Ten Issues for
Dentists Contemplating Retirement in Ten
Years or Less
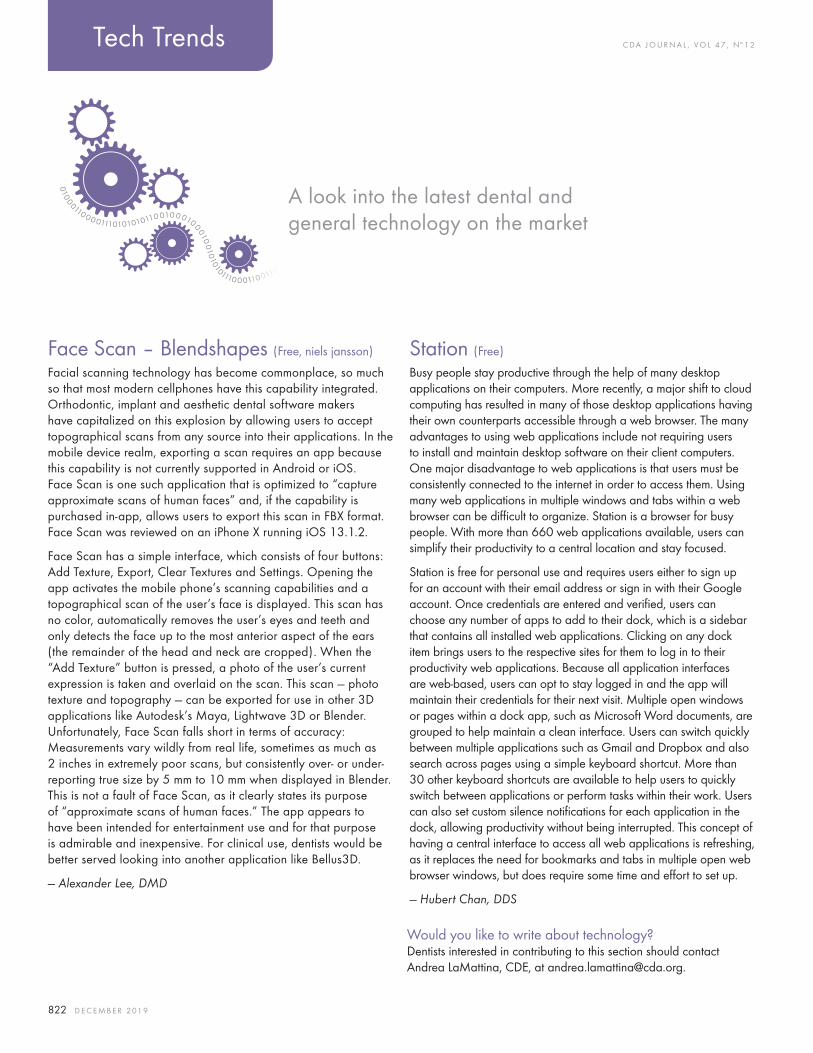
C DA J O U R N A L , V O L 4 7 , Nº 1 2
822 D E C E M B E R 2 01 9
A look into the latest dental and general technology on the market
Tech Trends
Face Scan – Blendshapes (Free, niels jansson)
Facial scanning technology has become commonplace, so much so that most modern cellphones have this capability integrated. Orthodontic, implant and aesthetic dental software makers have capitalized on this explosion by allowing users to accept topographical scans from any source into their applications. In the mobile device realm, exporting a scan requires an app because this capability is not currently supported in Android or iOS. Face Scan is one such application that is optimized to “capture approximate scans of human faces” and, if the capability is purchased in-app, allows users to export this scan in FBX format. Face Scan was reviewed on an iPhone X running iOS 13.1.2.
Face Scan has a simple interface, which consists of four buttons: Add Texture, Export, Clear Textures and Settings. Opening the app activates the mobile phone’s scanning capabilities and a topographical scan of the user’s face is displayed. This scan has no color, automatically removes the user’s eyes and teeth and only detects the face up to the most anterior aspect of the ears (the remainder of the head and neck are cropped). When the “Add Texture” button is pressed, a photo of the user’s current expression is taken and overlaid on the scan. This scan — photo texture and topography — can be exported for use in other 3D applications like Autodesk’s Maya, Lightwave 3D or Blender. Unfortunately, Face Scan falls short in terms of accuracy: Measurements vary wildly from real life, sometimes as much as 2 inches in extremely poor scans, but consistently over- or under- reporting true size by 5 mm to 10 mm when displayed in Blender. This is not a fault of Face Scan, as it clearly states its purpose of “approximate scans of human faces.” The app appears to have been intended for entertainment use and for that purpose is admirable and inexpensive. For clinical use, dentists would be better served looking into another application like Bellus3D.
— Alexander Lee, DMD
Station (Free)
Busy people stay productive through the help of many desktop applications on their computers. More recently, a major shift to cloud computing has resulted in many of those desktop applications having their own counterparts accessible through a web browser. The many advantages to using web applications include not requiring users to install and maintain desktop software on their client computers. One major disadvantage to web applications is that users must be consistently connected to the internet in order to access them. Using many web applications in multiple windows and tabs within a web browser can be difficult to organize. Station is a browser for busy people. With more than 660 web applications available, users can simplify their productivity to a central location and stay focused.
Station is free for personal use and requires users either to sign up for an account with their email address or sign in with their Google account. Once credentials are entered and verified, users can choose any number of apps to add to their dock, which is a sidebar that contains all installed web applications. Clicking on any dock item brings users to the respective sites for them to log in to their productivity web applications. Because all application interfaces are web-based, users can opt to stay logged in and the app will maintain their credentials for their next visit. Multiple open windows or pages within a dock app, such as Microsoft Word documents, are grouped to help maintain a clean interface. Users can switch quickly between multiple applications such as Gmail and Dropbox and also search across pages using a simple keyboard shortcut. More than 30 other keyboard shortcuts are available to help users to quickly switch between applications or perform tasks within their work. Users can also set custom silence notifications for each application in the dock, allowing productivity without being interrupted. This concept of having a central interface to access all web applications is refreshing, as it replaces the need for bookmarks and tabs in multiple open web browser windows, but does require some time and effort to set up.
— Hubert Chan, DDS
Would you like to write about technology?Dentists interested in contributing to this section should contact Andrea LaMattina, CDE, at [email protected].

“AN AMAZING EXPERIENCE!”
CDA Presents The Art and Science of DentistryJoin us in California for cutting-edge workshops, inspiring speakers, innovative exhibitors and after-hours adventure.
New events and opportunities await you. Take a peek at cdapresents.com.
Save the date for the nation’s most brilliant dental convention.
Anaheim #cdaANA San Francisco #cdaSF May 14–16, 2020 Sept. 10–12, 2020May 13–15, 2021 Sept. 9–11, 2021
Follow us@cdadentists
Connect with usCalifornia Dental Association
Like us@cdadentists
Follow us@cdadentists
The Art and Science of Dentistry
© 2019 Ultradent Products, Inc. All rights reserved.
#MYSM I L E I S P OWER FU L
CheerfulM Y S M I L E I S
Augustina, from China—a data analyst, painter, and kickboxer—travels the
world with a smile. Opalescence™ Boost™ in-office whitening quickly whitens her smile
to keep up with her jet-setting lifestyle. A brighter, whiter smile will help each of your
patients live their best life. That’s the power of a smile. Find out more at
ultradent.com/mysmileispowerful.
Related Documents











