-
8/12/2019 Journal Wrist Ganglion[1]
1/31
GANGLION CYSTS
OF THE WRIST[BY PHIL MINOTTI, MD, AND JOHN S. TARAS, MD]
Pembimbing:dr. Wijiono, Sp.OT
Dipresentasikan oleh:
Naila Miskiyatun Nisa
-
8/12/2019 Journal Wrist Ganglion[1]
2/31
The ganglion cyst is he most common soft-tissue mass presenting in the hand and wristabout 50% to 70%.
Ganglion cysts occur at all ages but are mostprevalent during the second, third, and fourthdecades of life.
Women are affected 3 times as often as aremen.
-
8/12/2019 Journal Wrist Ganglion[1]
3/31
CLINIC L
CH R CTEISTIC
-
8/12/2019 Journal Wrist Ganglion[1]
4/31
-
8/12/2019 Journal Wrist Ganglion[1]
5/31
Less typical presenting symptoms includecarpal tunnel syndrome or trigger digitresulting from a volar carpal ganglioncysts interference with theflexor tendonsheaths.
-
8/12/2019 Journal Wrist Ganglion[1]
6/31
Diagnostic procedures includeaspiration of the mucinous, jelly-
like material, and radiographs,which will reveal any related
interosseous component.
-
8/12/2019 Journal Wrist Ganglion[1]
7/31
The differential diagnoses include solid
tumors and proliferative tenosynovitis.
A proliferative tenosynovitis
will move along with the
long extensors or flexors
A ganglion cyst will remain
stationary.
-
8/12/2019 Journal Wrist Ganglion[1]
8/31
P THOGENESIS
-
8/12/2019 Journal Wrist Ganglion[1]
9/31
There some theories about the etiology ofthe ganglion cyst, and confusion exists
about their origin.
Ganglion cysts were herniationsof synovial tissue from joints.
Eller (1746)Volkmann (1882)
Ganglion cysts arise de novo fromwithin the connective tissue.
Ledderhose (1893)
-
8/12/2019 Journal Wrist Ganglion[1]
10/31
Ganglion cysts resulted from mucinous
degeneration of connective tissue because of
chronic damage. The accumulation of collagen fibers, intra- and
extracellular mucin, and decreased collagen
fibers and stroma cells supported this theory.
Carp andStout (1928)
He reinforced this theory and postulated that a
constitutional factor may contribute to the
development of ganglion cysts because some
patients display multiple ganglion cysts on their
wrists and ankles.
Soren (1966)
-
8/12/2019 Journal Wrist Ganglion[1]
11/31
At present, most investigators agree that ganglion cystsarise from modified synovial or mesenchymal cells at the
synovial-capsular interface in response to repetitiveminor injury.
Repetitive stretching of the capsular and ligamentoussupporting joint structures appears to stimulate the
production of the tissue lubricant hyaluronic acid byfibroblasts at the synovial- capsule interface.
The resultant mucin accumulates in small channels,eventually pooling in the ganglion cyst.
There is currently no single theory that fully explains thepathogenesis of ganglion cysts.
-
8/12/2019 Journal Wrist Ganglion[1]
12/31
MICROSCOPIC
N TOMY
-
8/12/2019 Journal Wrist Ganglion[1]
13/31
Light microscopy reveals ganglion cysts to be single ormultiloculated, having a smooth, shiny lining.
Extensive studies by Psaila and Mansel by using scanningelectron microscopy showed that
The walls of ganglion cysts consist mainly of sheets ofcollagen fibers arranged in multidirectional strata.
The walls show sparse, flattened cells resemblingfibroblasts, but an epithelial or synovial lining is distinctlyabsent.
Most cysts contain a clear, highly viscous, jelly-like fluid,
significantly thicker than synovial fluid. This viscosity is attributed to its high concentration of
hyaluronic acid and other mucopolysaccharides.
-
8/12/2019 Journal Wrist Ganglion[1]
14/31
DORS L WRIST
G NGLION CYSTS
-
8/12/2019 Journal Wrist Ganglion[1]
15/31
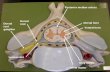
The dorsum of the wrist is the most commonlocation of ganglion formation for about 60% to70% of all hand and wrist ganglion cysts.
Ganglions in this region usually are directly over thescapholunate ligament, it appears anywhere
between the long thumb extensor laterally and thecommon finger extensors medially (Fig 1).
The main body of the cyst is tethered to the wristcapsule by a pedicle. This pedicle often penetrates
the capsule and enters the scapholunate ligament(Fig 2).
-
8/12/2019 Journal Wrist Ganglion[1]
16/31
-
8/12/2019 Journal Wrist Ganglion[1]
17/31
-
8/12/2019 Journal Wrist Ganglion[1]
18/31
VOL R WRIST
G NGLION CYSTS
-
8/12/2019 Journal Wrist Ganglion[1]
19/31
Volar wrist ganglion cysts account for 18% to 20%
of all ganglion cysts of the hand and wrist. They generally occur under the volar wrist crease,
just radial to the flexor carpi radialis tendon (Fig 3).
Volar ganglion cysts arise most frequently from theradiocarpal joint or the scaphotrapezial joint.
Volar wrist ganglion cysts can be quite extensive,tracking under the thenar muscles, into the carpal
canal, or along the flexor carpi radialis tendon.
-
8/12/2019 Journal Wrist Ganglion[1]
20/31
-
8/12/2019 Journal Wrist Ganglion[1]
21/31
NON SURGIC L
TRE TMENT
-
8/12/2019 Journal Wrist Ganglion[1]
22/31
The indications for treatmentinclude pain, weakness, anddisfigurement.
Nonsurgical treatments that
have come and gone includeheat, radiation, and injectionwith sclerosing agents.
These methodshavebeen shownto be ineffective,
or in the case ofsclerotherapy,dangerous.
-
8/12/2019 Journal Wrist Ganglion[1]
23/31
The mainstay of conservative
treatment is aspiration of the cystwith a large bore needle followed
by injection of lidocaine and a
corticosteroid.
In the case of dorsal wrist
ganglion cyst, up to 80% ofpatients can expect at least a
temporary resolution of their
symptoms, but recurrence is
common.
Volar wrist ganglion cysts
generally respond poorly tononsurgical treatment.
Wright et al noted recurrence in
20 of 24 (83%) patients after
aspiration and injection and a100% recurrence rate in patients
who required multiple injections.
-
8/12/2019 Journal Wrist Ganglion[1]
24/31
SURGIC L
TRE TMENT
-
8/12/2019 Journal Wrist Ganglion[1]
25/31
Dorsal ganglion cysts are approached
through a transverse incision centered
directly over the ganglion cyst
Extensive skin incisions are rarely necessary
because the dorsal skin is freely mobile
The main cyst is mobilized from the
surrounding tissues by using tenotomy
scissors
Avoid rupturing the cyst because this makes
identification and full excision of the pedicle
and capsular attachments more difficult
-
8/12/2019 Journal Wrist Ganglion[1]
26/31
-
8/12/2019 Journal Wrist Ganglion[1]
27/31
A wide swath of
dorsal capsule is
excised with the cyst,
greatly reducing the
chance of recurrence.
Maintaining the
integrity of the
scapholunate ligament
will eliminate the
possibility of iatrogenicscapholunate instability.
Do not close the capsule
primarily or with a flap
because such closures
only serve to delay early
mobilization.
-
8/12/2019 Journal Wrist Ganglion[1]
28/31
Volar wrist ganglion cysts are approached a
longitudinally incision curving around the radial
side of the ganglion cyst.
The incision is placed in such a way as to allow
proximal and distal extension in pursuit of remotecapsular attachments.
The palmar cutaneous branch of the median nerve
arises 5 cm proximal to the wrist joint and runs
distally along the ulnar side of the flexor carpi
radialis tendon.
Wh h i
-
8/12/2019 Journal Wrist Ganglion[1]
29/31
The ganglion is freed from all surrounding connective tissue and the radial
artery is mobilized proximally and distally.
As the ganglion is separated from the artery, a 1- to 2-mm cuff of cyst wall
is left with the artery to prevent vessel injury.
Once the artery is separated and protected, the pedicle can be traced to its
capsular attachments to the scaphotrapezial or radiocarpal ligament and
excised (Fig 4).
When the cyst is
intimately adherent to the
vessel wall
Lister and Smiths
technique
-
8/12/2019 Journal Wrist Ganglion[1]
30/31
-
8/12/2019 Journal Wrist Ganglion[1]
31/31
TERIMA KASIH
![Ultrasound -WC 2017-KW.pptx [Read-Only]€¦ · Joint‐Elbow effusion, wrist ganglion cyst ... Microsoft PowerPoint - Ultrasound -WC 2017-KW.pptx [Read-Only] Author: akeeney Created](https://static.cupdf.com/doc/110x72/5ac89e287f8b9aa3298c441e/ultrasound-wc-2017-kwpptx-read-only-jointelbow-effusion-wrist-ganglion.jpg)