Case Report Miniscrew implant-supported Frog Ò appliance for maxillary molar distalization Ankit H. Shah a, * , Darshit H. Shah b a Private Practice, Dallas, Texas b Orthodontic Resident, Center for Advanced Dental Education, Saint Louis University, Saint Louis, Missouri article info Article history: Received 8 August 2015 Accepted 4 February 2016 Keywords: Frog Ò appliance Miniscrew implants Molar distalization abstract Various appliances have been used for the correction of Class II malocclusion. The majority of these appliances depend on patient compliance for a successful treatment outcome. An 11-year-old girl was referred to our clinic for orthodontic treatment. She had a mild skeletal Class II malocclusion with Class II molar and canine relationship on both sides. The treatment plan included bilateral distalization of the maxillary first molars using a miniscrew implant-supported frog appliance along with comprehensive orthodontics. Successful correction of Class II malocclusion was achieved with the use of a relatively new intraoral distalization applianceethe Frog Ò Appliance. Proclination of maxillary incisors was minimal due to the use of miniscrew implants. This article presents an effective, noninvasive, and compliance-free intraoral distalization appliance for achieving maxillary molar distalization. Ó 2016 World Federation of Orthodontists. 1. Introduction Various distalization appliances have been developed to over- come compliance issues: the pendulum appliance [1], the distal jet [2], the Jones jig [3], the first-class appliance [4], the Carriere dis- talizer [5], appliances with nickel-titanium springs [6], and the simplified molar distalizer, also known as the Frog Ò Appliance (Forestadent, Pforzheim, Germany) [7]. Although all of these appliances achieve distalization of the maxillary molars, the reciprocal forces produce undesirable side effects, such as proclination of maxillary incisors, maxillary molar distal-crown tipping, and bite opening. Recently, miniscrew implants (MSIs) have been used clinically to reinforce anchorage during distalization and to avoid these side effects. Use of a skeletally anchored Frog Appliance was first reported in 2011 [8]. This appliance constitutes of an expansion screw and a removable distalizing spring that connects the expansion screw to the maxillary first molars (Fig. 1). The distalizing spring is fabricated from 0.032-in. TMA Ò (Ormco, Orange, CA) or stainless steel wire with adjustment loops. These adjustment loops are used to adjust the distalizing spring as needed. The ends of the distalizing spring have double back bends, which insert into the lingual sheaths of the maxillary first molar bands. The entire assembly is anchored to a pair of MSIs placed on either side of midline of the anterior palate. It is attached to the MSIs by using a modified acrylic Nance palatal button. This case report describes an 11-year-old girl who presented with a Class II malocclusion and maxillary crowding, including partially blocked-out canines (Figs. 2 and 3). The maxillary second molars were still in the tooth-bud stage when orthodontic appliances were placed, and an MSI-supported Frog Appliance was fitted. 2. Etiology and diagnosis The patient had a mesocephalic facial form with competent lips and no significant facial asymmetries (Fig. 2). Intraorally, she had Angle Class II molar relation on both sides (Figs. 2 and 3). She had mild mandibular crowding, a 3-mm overjet, 75% overbite, and coincident maxillary and mandibular midlines. Soft tissue analysis revealed that she had normal upper lip, retrusive lower lip, and retrusive chin (Table 1). No abnormalities were noted on the panoramic radiograph (Fig. 4). Clinical examination did not reveal any temporomandibular joint problems. Periodontal health was found to be within normal limits. All authors have completed and submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest, and none were reported. Authors have obtained and submitted the patient signed consent for images publication. * Corresponding author: 1001 Lake Carolyn Parkway, #452, Irving, TX 75039. E-mail address: [email protected] (A.H. Shah). Contents lists available at ScienceDirect Journal of the World Federation of Orthodontists journal homepage: www.jwfo.org 2212-4438/$ e see front matter Ó 2016 World Federation of Orthodontists. http://dx.doi.org/10.1016/j.ejwf.2016.02.003 Journal of the World Federation of Orthodontists 5 (2016) 35e43

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Contents lists available at ScienceDirect
Journal of the World Federation of Orthodontists
journal homepage: www.jwfo.org
Journal of the World Federation of Orthodontists 5 (2016) 35e43
Case Report
Miniscrew implant-supported Frog� appliance for maxillary molardistalization
Ankit H. Shah a,*, Darshit H. Shah b
a Private Practice, Dallas, TexasbOrthodontic Resident, Center for Advanced Dental Education, Saint Louis University, Saint Louis, Missouri
a r t i c l e i n f o
Article history:Received 8 August 2015Accepted 4 February 2016
Keywords:Frog� applianceMiniscrew implantsMolar distalization
All authors have completed and submitted the ICPotential Conflicts of Interest, and none were reported
Authors have obtained and submitted the patienpublication.* Corresponding author: 1001 Lake Carolyn Parkwa
E-mail address: [email protected] (A.H. Sh
2212-4438/$ e see front matter � 2016 World Federahttp://dx.doi.org/10.1016/j.ejwf.2016.02.003
a b s t r a c t
Various appliances have been used for the correction of Class II malocclusion. The majority of theseappliances depend on patient compliance for a successful treatment outcome. An 11-year-old girl wasreferred to our clinic for orthodontic treatment. She had a mild skeletal Class II malocclusion with Class IImolar and canine relationship on both sides. The treatment plan included bilateral distalization of themaxillary first molars using a miniscrew implant-supported frog appliance along with comprehensiveorthodontics. Successful correction of Class II malocclusion was achieved with the use of a relatively newintraoral distalization applianceethe Frog� Appliance. Proclination of maxillary incisors was minimaldue to the use of miniscrew implants. This article presents an effective, noninvasive, and compliance-freeintraoral distalization appliance for achieving maxillary molar distalization.
� 2016 World Federation of Orthodontists.
1. Introduction
Various distalization appliances have been developed to over-come compliance issues: the pendulum appliance [1], the distal jet[2], the Jones jig [3], the first-class appliance [4], the Carriere dis-talizer [5], appliances with nickel-titanium springs [6], and thesimplified molar distalizer, also known as the Frog� Appliance(Forestadent, Pforzheim, Germany) [7]. Although all of theseappliances achieve distalization of the maxillary molars, thereciprocal forces produce undesirable side effects, such asproclination of maxillary incisors, maxillary molar distal-crowntipping, and bite opening. Recently, miniscrew implants (MSIs)have been used clinically to reinforce anchorage duringdistalization and to avoid these side effects.
Use of a skeletally anchored Frog Appliance was first reported in2011 [8]. This appliance constitutes of an expansion screw and aremovable distalizing spring that connects the expansion screw tothemaxillary first molars (Fig. 1). The distalizing spring is fabricatedfrom 0.032-in. TMA� (Ormco, Orange, CA) or stainless steel wirewith adjustment loops. These adjustment loops are used to adjust
MJE Form for Disclosure of.t signed consent for images
y, #452, Irving, TX 75039.ah).
tion of Orthodontists.
the distalizing spring as needed. The ends of the distalizing springhave double back bends, which insert into the lingual sheaths of themaxillary first molar bands. The entire assembly is anchored to apair of MSIs placed on either side of midline of the anterior palate. Itis attached to the MSIs by using a modified acrylic Nance palatalbutton.
This case report describes an 11-year-old girl who presentedwith a Class II malocclusion and maxillary crowding, includingpartially blocked-out canines (Figs. 2 and 3). The maxillarysecond molars were still in the tooth-bud stage when orthodonticappliances were placed, and an MSI-supported Frog Appliance wasfitted.
2. Etiology and diagnosis
The patient had a mesocephalic facial form with competent lipsand no significant facial asymmetries (Fig. 2). Intraorally, she hadAngle Class II molar relation on both sides (Figs. 2 and 3). She hadmild mandibular crowding, a 3-mm overjet, 75% overbite, andcoincident maxillary and mandibular midlines. Soft tissue analysisrevealed that she had normal upper lip, retrusive lower lip, andretrusive chin (Table 1).
No abnormalities were noted on the panoramic radiograph(Fig. 4). Clinical examination did not reveal any temporomandibularjoint problems. Periodontal health was found to be within normallimits.
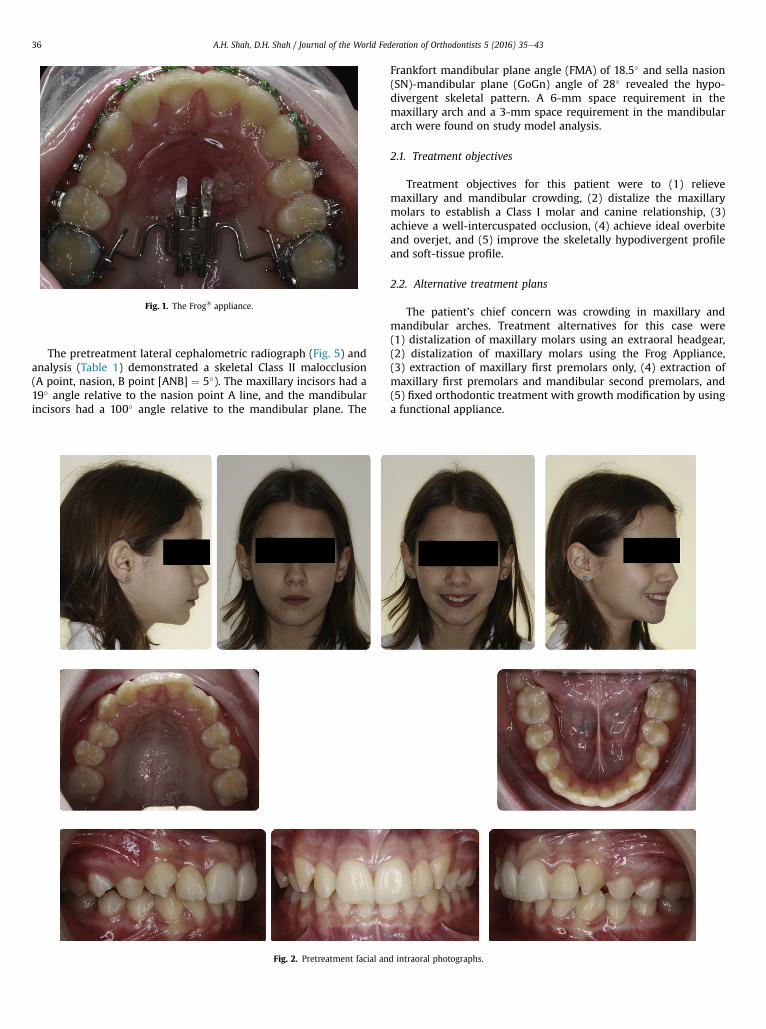
Fig. 1. The Frog� appliance.
A.H. Shah, D.H. Shah / Journal of the World Federation of Orthodontists 5 (2016) 35e4336
The pretreatment lateral cephalometric radiograph (Fig. 5) andanalysis (Table 1) demonstrated a skeletal Class II malocclusion(A point, nasion, B point [ANB] ¼ 5�). The maxillary incisors had a19� angle relative to the nasion point A line, and the mandibularincisors had a 100� angle relative to the mandibular plane. The
Fig. 2. Pretreatment facial an
Frankfort mandibular plane angle (FMA) of 18.5� and sella nasion(SN)-mandibular plane (GoGn) angle of 28� revealed the hypo-divergent skeletal pattern. A 6-mm space requirement in themaxillary arch and a 3-mm space requirement in the mandibulararch were found on study model analysis.
2.1. Treatment objectives
Treatment objectives for this patient were to (1) relievemaxillary and mandibular crowding, (2) distalize the maxillarymolars to establish a Class I molar and canine relationship, (3)achieve a well-intercuspated occlusion, (4) achieve ideal overbiteand overjet, and (5) improve the skeletally hypodivergent profileand soft-tissue profile.
2.2. Alternative treatment plans
The patient’s chief concern was crowding in maxillary andmandibular arches. Treatment alternatives for this case were(1) distalization of maxillary molars using an extraoral headgear,(2) distalization of maxillary molars using the Frog Appliance,(3) extraction of maxillary first premolars only, (4) extraction ofmaxillary first premolars and mandibular second premolars, and(5) fixed orthodontic treatment with growth modification by usinga functional appliance.
d intraoral photographs.

Fig. 3. Pretreatment dental casts.
A.H. Shah, D.H. Shah / Journal of the World Federation of Orthodontists 5 (2016) 35e43 37
Due to the patient’s parents’ opposition to the extraction ofhealthy teeth for orthodontic purposes and the patient’s reluctanceto wear headgear, intermaxillary elastics, or a functional appliance,the distalization of maxillary molars was evaluated as a treatmentplan option. This treatment planwas selected by the patient and herparents.
2.3. Treatment progress
Preadjusted fixed appliances (0.022 � 0.028-inch, MBT system�
3M Unitek, Monrovia, CA) were placed in both arches for initialleveling and alignment. After 4 months of initial leveling andalignment, two MSIs were placed in the anterior palate. One MSIwas placed on either side of the midline approximately 1 to 2 mmfrom the midpalatal suture and 5 to 6 mm behind the incisalpapillae. A maxillary impression was taken for fabrication of theFrog Appliance. The Frog Appliance was cemented in the oral cavity1 week later (Fig. 1). This appliance was activated by performingthree rotations each at 4-week intervals. Then 5� to 10� of “toe-in”bends were placed in the double back bends of the springs asneeded to prevent the undesirable rotation of maxillary molarsduring distalization.
Table 1Pretreatment and posttreatment lateral cephalometric analysis data
Measurement Pretreatment Posttreatment
SNA angle (�) 80 81SNB angle (�) 75 77ANB angle (�) 5 4Wits appraisal (mm) 3 1FMA (�) 18.5 24SN-Go Gn (�) 28 28Upper incisor to NA (mm) 0 2Upper incisor to NA (�) 19 20Lower incisor NB (mm) 3 6Lower incisor to NB (�) 25 29IMPA (�) 100 101Interincisal angle (�) 132 127Upper lip to E line (mm) �1 �1Lower lip to E line (mm) �1 0
ANB, A point, nasion, B point; FMA, Frankfort mandibular plane angle; Gn, gnathion;Go, gonial; IMPA, incisor to mandibular plane angle; NA, nasion point A; NB, nasionpoint B; SN, sella nasion; SNA, sella nasion point A; SNB, sella nasion point B.
Appliance stability and distalization progress were evaluated ateach appointment. Themaxillary first molars were distalized until aClass I molar relationship was achieved on both sides (Fig. 6). Thiswas completed within 5 months of appliance cementation. Theappliance was left in place for an additional period of 4 months toprevent any mesial movement of molars. Pull from the transseptalfibers helped in the distal drifting of maxillary canines andpremolars during this period. Complete distalization of maxillarycanines and premolars was achieved by using continuous archwiresand power chains. The Frog Appliance was removed after13 months of overall treatment. MSIs were removed 1 week afterthe removal of the Frog Appliance.
After a Class I canine relationship was achieved on both sides,0.019 � 0.025-in. TMA� (Ormco, Orange, CA) archwire with “tear-drop” loops was used in the maxillary arch to retract the anteriorteeth. Detailing bends were placed in 0.016-in. stainless steel wiresto improve alignment of the teeth. Coordinated archwires andsettling elastics were used to gain maximum intercuspation of theteeth. The orthodontic appliances were removed after 21 months oftreatment. Hawley retainers were fabricated for retention in botharches.
3. Results
The patient’s chief concern of crowding was resolvedwhile idealoverbite and overjet were achieved. Posterior occlusion wasimproved to a bilateral Class I molar relationship. Class I caninerelationship was also achieved on both sides (Figs. 7 and 8).
Satisfactory root parallelism was achieved as noted on theposttreatment panoramic radiograph (Fig. 9). No temporomandib-ular joint problems were noted. Improvement in soft-tissue profilewas noted. Lower lip position improved by 1 mm, and the upper lipposition was maintained with respect to the E line (Figs. 10 and 11and Table 1).
Maxillary growth was noted to be in a forward directionpredominantly (Fig. 11). Significant mandibular growth wasobserved in an anteroinferior direction. Bodily distal movementand simultaneous uprighting of maxillary first molars was alsonoted. Mandibular first molars demonstrated significantcompensatory mesial and occlusal movement as a response toskeletal mandibular growth [9]. The maxillary incisors proclinedminimally in a bodily fashion compared with their pretreatment

Fig. 4. Pretreatment panoramic radiograph.
A.H. Shah, D.H. Shah / Journal of the World Federation of Orthodontists 5 (2016) 35e4338
position. The mandibular incisors also showed slight labialmovement (Fig. 11).
3.1. Case retention
The patient received Hawley retainers for maxillary andmandibular arches. The occlusion and treatment changes werestable at 1 year of posttreatment follow-up (Fig. 12).
4. Discussion
Distalization is one of the treatment modalities used byclinicians and practitioners for correction of Class II malocclusionswithout any major skeletal discrepancies. Use of various
Fig. 5. Pretreatment lateral c
noncompliance intraoral molar distalization appliances [1e8] hasbeen described in literature.
Several studies have reported that obtaining a bodily distalmovement of the maxillary first molars with minimal rotation andminimal distal-crown tipping remains a significant challenge ofmaxillary molar distalization [10e12]. In our patient, the FrogAppliance was oriented parallel to the occlusal plane andpositioned approximately 10 to 12mm apical to the occlusal surfaceof the maxillary first molar. This position is close to the trifurcationof roots of maxillary first molar and is considered its approximatecenter of resistance [13]. Positioning the appliance in this mannerallows the effective distalizing force vector to pass through thecenter of resistance of the maxillary first molars, thereby producingbodily distal movement. In our case, the maxillary first molarsmoved distally in a bodily fashion and also exhibited distal-root
ephalogram and tracing.

Fig. 6. Progress facial and intraoral photographs.
A.H. Shah, D.H. Shah / Journal of the World Federation of Orthodontists 5 (2016) 35e43 39
tipping (Fig. 11). This distal-root tipping is very critical in achievinga well-intercuspated posterior occlusion [14].
Another significant challenge is prevention of bodily mesialmovement, mesial tipping, and extrusion of maxillary firstpremolars during distalization [15,16]. A meta-analysis wasperformed to compare intraoral distalizer effects with conventionaland skeletal anchorage [17]. The analysis showed an average molardistalization amount of 3.34 mmwith conventional anchorage and5.10 mm with skeletal anchorage. This analysis also showedmesialization of premolars by 2.3 mm in studies with conventionalanchorage compared with �4.01 mm of premolar distalization instudies with skeletal anchorage [17]. This is a major drawback oftooth- and/or palate-borne distalization appliances. MSIs have beenshown to act as efficient anchorage units and help overcomethese limitations [18,19]. For our patient, mesial movement and/ormesial tipping of maxillary first premolars was avoided as theanchorage was obtained from MSIs instead of maxillary firstpremolars.
Finally, prevention of anchorage loss during distalization, whichis expressed as either proclination of the maxillary incisors withincreased overjet or maxillary anterior crowding, is equallyimportant [15,16]. The anterior teeth cannot resist the opposingforces of distalization without moving in the anterior direction.Satisfactory distalization results without anchorage loss have beenachieved in molar distalization studies using skeletal anchorage[18,19]. We were able to control the undesired proclination of
maxillary incisors due to the direct anchorage from MSIs (Fig. 11and Table 1).
5. Conclusion
The Frog Appliance is an effective, noninvasive, and compliance-free intraoral distalization appliance for achieving maxillary molardistalization. This case report should help other clinicians andpractitioners to consider adding this appliance as another tool intheir armamentarium for their Class II patients.
Acknowledgment
The authors would like to thank Dr. Khamir Patel for histechnical assistance.
Source of financial support: The authors have no financialrelationship to disclose.
References
[1] Hilgers JJ. The pendulum appliance for Class II non-compliance therapy. J ClinOrthod 1992;26:706e14.
[2] Carano A, Testa M. The distal jet for upper molar distalization. J Clin Orthod1996;30:374e80.
[3] Brickman CD, Sinha PK, Nanda RS. Evaluation of the Jones jig appliance fordistal molar movement. Am J Orthod Dentofacial Orthop 2000;118:526e34.

A.H. Shah, D.H. Shah / Journal of the World Federation of Orthodontists 5 (2016) 35e4340
[4] Fortini A, Lupoli M, Parri M. The first class appliance for rapid molardistalization. J Clin Orthod 1999;33:322e8.
[5] Carrière LA. New Class II distalizer. J Clin Orthod 2004;38:224e31.[6] Gianelly AA, Bednar J, Dietz VS. Japanese NiTi coils used to move molars
distally. Am J Orthod Dentofacial Orthop 1991;99:564e6.[7] Walde KC. The simplified molar distalizer. J Clin Orthod 2003;37:616e9.[8] Ludwig B, Glasl B, Kinzinger GS, Walde KC. The skeletal Frog Appliance for
maxillary molar distalization. J Clin Orthod 2011;45:77e84.[9] Proffit WR, editor. Contemporary orthodontics. 3rd ed. St. Louis, MO: Mosby;
2000. p. 171.[10] Ghosh J, Nanda RS. Evaluation of an intraoral maxillary molar distalization
technique. Am J Orthod Dentofacial Orthop 1996;110:639e46.[11] Byloff FK, Darendeliler MA. Distal molar movement using the pendulum
appliance. Part 1. Clinical and radiological evaluation. Angle Orthod1997;67:249e60.
[12] Kinzinger GS, Eren M, Diedrich PR. Treatment effects of intraoral applianceswith conventional anchorage designs for non-compliance maxillary molardistalization: a literature review. Eur J Orthod 2008;30:558e71.
[13] Dermaut LR, Kleutghen JP, De Clerck HJ. Experimental determination of thecenter of resistance of the upper first molar in a macerated, dry human skull
Fig. 7. Posttreatment facial an
submitted to horizontal headgear traction. Am J Orthod Dentofacial Orthop1986;90:29e36.
[14] Andrews LF. The six keys to normal occlusion. Am J Orthod 1972;62:296e309.
[15] Bussick TJ, McNamara Jr JA. Dentoalveolar and skeletal changes associatedwith the pendulum appliance. Am J Orthod Dentofacial Orthop 2000;117:333e43.
[16] Antonarakis GS, Kiliaridis S. Maxillary molar distalization with noncomplianceintramaxillary appliances in Class II malocclusion. A systematic review. AngleOrthod 2008;78:1133e40.
[17] Grec RH, Janson G, Branco NC, Moura-Grec PG, Patel MP, CastanhaHenriques JF. Intraoral distalizer effects with conventional and skeletalanchorage: a meta-analysis. Am J Orthod Dentofacial Orthop 2013;143:602e15.
[18] Fudalej P, Antoszewska J. Are orthodontic distalizers reinforced with thetemporary skeletal anchorage devices effective? Am J Orthod DentofacialOrthop 2011;139:722e9.
[19] Kyung SH, Lee JY, Shin JW, Hong C, Dietz V, Gianelly AA. Distalization of theentire maxillary arch in an adult. Am J Orthod Dentofacial Orthop2009;135:S123e32.
d intraoral photographs.

Fig. 8. Posttreatment dental casts.
Fig. 9. Posttreatment panoramic radiograph.
A.H. Shah, D.H. Shah / Journal of the World Federation of Orthodontists 5 (2016) 35e43 41
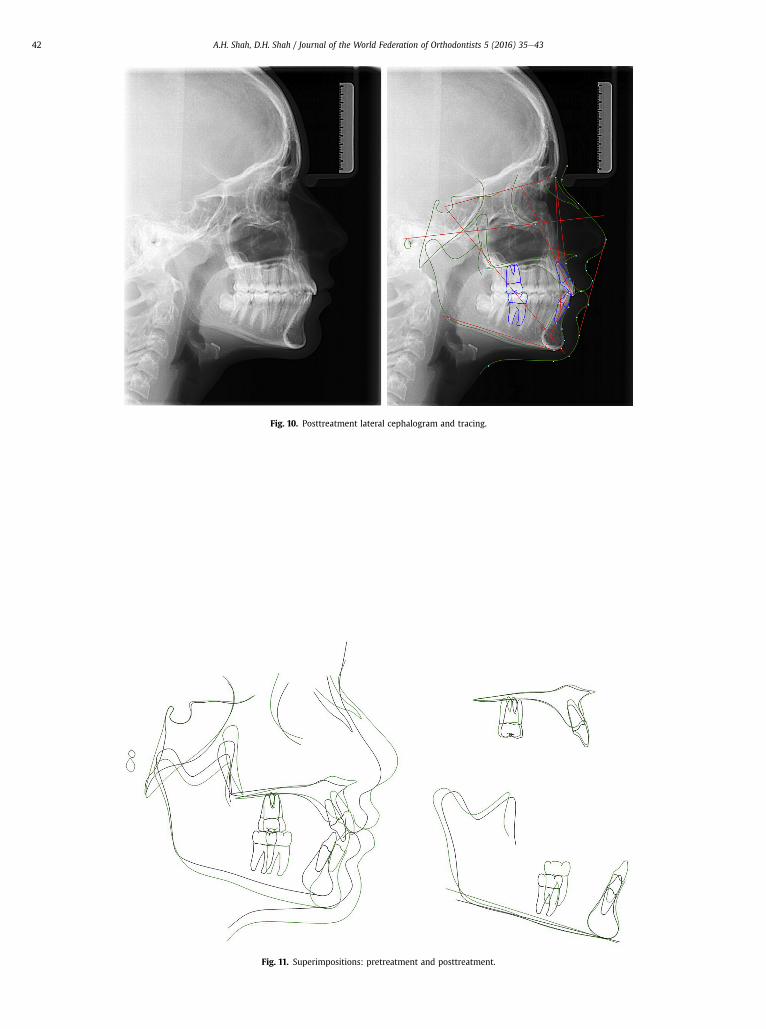
Fig. 10. Posttreatment lateral cephalogram and tracing.
Fig. 11. Superimpositions: pretreatment and posttreatment.
A.H. Shah, D.H. Shah / Journal of the World Federation of Orthodontists 5 (2016) 35e4342

Fig. 12. Facial and intraoral photographs at 1-year follow-up.
A.H. Shah, D.H. Shah / Journal of the World Federation of Orthodontists 5 (2016) 35e43 43
Related Documents











