J Gastroint Dig Syst Gastrointestinal Endoscopy ISSN: 2161-069X, an open access journal Journal of Gastrointestinal & Digestive System Yamabe et al,. J Gastroint Dig Syst 2013, S2 DOI: 10.4172/2161-069X.S2-005 Review Article Open Access Endosonographic Diagnosis of Chronic Pancreatitis Akane Yamabe, Athushi Irisawa*, Goro Shibukawa, Yoko Abe, Akiko Nikaido, Ko Inbe and Koki Hoshi Department of Gastroenterology, Fukushima Medical University Aizu Medical Center, Japan Abstract Chronic pancreatitis (CP) is characterized by irreversible damage that engenders fibrosis and necrosis of pancreatic tissue, with the consequent loss of endocrine and exocrine function of the pancreas. The clinical course of CP engenders a high rate of morbidity and mortality over a 20-25-year period. In view of this fact, current efforts emphasize the establishment of early diagnosis to commence intervention that can positively affect the natural course of the disease. Endoscopic ultrasonography (EUS) is a well-established and less-invasive modality for CP diagnosis. The higher imaging resolution provided by EUS enables detection of subtle pancreatic abnormalities, not only parenchymal but also ductal changes, that are undetectable using other modalities. This review presents an overview of the endosonographic diagnosis of chronic pancreatitis. *Corresponding author: Athushi Irisawa, Department of Gastroenterology, Fuku- shima Medical University Aizu Medical Center, 21-2, Maeda, Yazawa, Kawahigashi, Aizuwakamatsu, 969-3492, Japan, Tel: 81-0242-75-2100; E-mail: [email protected] Received May 09, 2013; Accepted May 30, 2013; Published June 01, 2013 Citation: Yamabe A, Irisawa A, Shibukawa G, Abe Y, Nikaido A, et al. (2013) Endosonographic Diagnosis of Chronic Pancreatitis. J Gastroint Dig Syst S2: 005. doi:10.4172/2161-069X.S2-005 Copyright: © 2013 Yamabe A, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Keywords: Chronic pancreatitis; EUS; Early chronic pancreatitis; ERP Introduction Chronic pancreatitis (CP) is characterized by irreversible damage that engenders fibrosis and necrosis of the pancreatic tissue [1], with the loss of endocrine and exocrine function of the pancreas [2]. Alcohol is the most common etiology of CP in 64.8% and idiopathy (unidentified) in 18.2%. Sarles et al. reported that 60-70% of patients with CP have a 6-12 year history of alcohol abuse [3]. In addition, regarding the relation between smoking and CP, smoking rates of CP patients are high (74.7% in men, 26.0% in women). Furthermore, lifestyles that include drinking and smoking are strongly associated with the onset and progress of CP. e clinical course of CP engenders a high rate of morbidity and mortality over a 20-25 year period. Moreover, CP is recognized as a risk factor of pancreatic cancer: patients with CP are 16 times more likely to develop pancreatic cancer than normal individuals are [4]. In view of these facts, current efforts emphasize establishment of early diagnosis to commence intervention that can positively affect the natural history of the disease: follow-up of CP in a rigorous manner is necessary using various modalities. Endoscopic ultrasonography (EUS) is a well-established and less-invasive modality for CP diagnosis [5-10]. Although endoscopic retrograde pancreatigraphy (ERP) has been regarded as the gold standard for CP diagnosis, ERP cannot investigate the parenchymal changes. In that respect, the higher imaging resolution provided by EUS enables detection of subtle pancreatic abnormalities, not only parenchymal, but also ductal changes that are undetectable using other modalities. In this review, the authors describe the role of EUS in CP diagnosis, especially in the early stage. Normal Pancreas on EUS An understanding of normal pancreas on EUS is extremely important for making EUS diagnosis of CP. e normal pancreatic parenchyma is uniformly depicted in equal or a slightly less hyperecho to the liver; it presents a so-called fine reticular pattern. e main duct dilation, duct irregularity and side branch ectasia are not visualized within the parenchyma [8]. Furthermore, the main ductal wall is observed as a uniform and slightly hyperlinear echo: 2.4 mm diameter in the head, 1.8 mm in the body, and 1.2 in the tail [6]. e EUS image of CP is defined based on these views. e EUS image of a normal pancreas is presented in figure 1. EUS Features of Chronic Pancreatitis CP is characterized by fibrosis of parenchyma along with ductal changes in the pancreas. ese changes of fibrosis have been characterized as hyperechoic using ultrasound [11-13]. e superiority of EUS is not so high in the case of advanced CP because typical CP findings such as atrophy, calcification, main duct dilation, duct irregularity, cyst are readily observed even using other modalities. However, it is difficult to observe minute changes of pancreatic parenchyma using means other than EUS. Among patients with chronic pancreatitis, EUS will reveal all pancreatic abnormalities. Typical EUS findings are shown in figures 2-6. Diagnosis of CP using EUS Traditional EUS criteria for diagnosis of CP Several studies have compared EUS findings with ERP (Cambridge classification) for CP evaluation [14]. Results of these studies suggest that ductal and parenchymal abnormalities detected using EUS correlate with the presence of CP. From these studies, the traditional EUS criteria Figure 1: Normal pancreatic parenchyma on EUS. Homogeneous and finely reticular patterns are visible in parenchyma without dilated ducts.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
-
J Gastroint Dig Syst Gastrointestinal Endoscopy ISSN: 2161-069X, an open access journal
Journal of Gastrointestinal & Digestive System
Yamabe et al,. J Gastroint Dig Syst 2013, S2 DOI: 10.4172/2161-069X.S2-005
Review Article Open Access
Endosonographic Diagnosis of Chronic PancreatitisAkane Yamabe, Athushi Irisawa*, Goro Shibukawa, Yoko Abe, Akiko Nikaido, Ko Inbe and Koki HoshiDepartment of Gastroenterology, Fukushima Medical University Aizu Medical Center, Japan
AbstractChronic pancreatitis (CP) is characterized by irreversible damage that engenders fibrosis and necrosis of
pancreatic tissue, with the consequent loss of endocrine and exocrine function of the pancreas. The clinical course of CP engenders a high rate of morbidity and mortality over a 20-25-year period. In view of this fact, current efforts emphasize the establishment of early diagnosis to commence intervention that can positively affect the natural course of the disease. Endoscopic ultrasonography (EUS) is a well-established and less-invasive modality for CP diagnosis. The higher imaging resolution provided by EUS enables detection of subtle pancreatic abnormalities, not only parenchymal but also ductal changes, that are undetectable using other modalities. This review presents an overview of the endosonographic diagnosis of chronic pancreatitis.
*Corresponding author: Athushi Irisawa, Department of Gastroenterology, Fuku-shima Medical University Aizu Medical Center, 21-2, Maeda, Yazawa, Kawahigashi, Aizuwakamatsu, 969-3492, Japan, Tel: 81-0242-75-2100; E-mail: [email protected]
Received May 09, 2013; Accepted May 30, 2013; Published June 01, 2013
Citation: Yamabe A, Irisawa A, Shibukawa G, Abe Y, Nikaido A, et al. (2013) Endosonographic Diagnosis of Chronic Pancreatitis. J Gastroint Dig Syst S2: 005. doi:10.4172/2161-069X.S2-005
Copyright: © 2013 Yamabe A, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Keywords: Chronic pancreatitis; EUS; Early chronic pancreatitis;ERP
IntroductionChronic pancreatitis (CP) is characterized by irreversible damage
that engenders fibrosis and necrosis of the pancreatic tissue [1], with the loss of endocrine and exocrine function of the pancreas [2]. Alcohol is the most common etiology of CP in 64.8% and idiopathy (unidentified) in 18.2%. Sarles et al. reported that 60-70% of patients with CP have a 6-12 year history of alcohol abuse [3]. In addition, regarding the relationbetween smoking and CP, smoking rates of CP patients are high (74.7%in men, 26.0% in women). Furthermore, lifestyles that include drinkingand smoking are strongly associated with the onset and progress ofCP. The clinical course of CP engenders a high rate of morbidity andmortality over a 20-25 year period. Moreover, CP is recognized as a riskfactor of pancreatic cancer: patients with CP are 16 times more likely todevelop pancreatic cancer than normal individuals are [4]. In view ofthese facts, current efforts emphasize establishment of early diagnosisto commence intervention that can positively affect the natural historyof the disease: follow-up of CP in a rigorous manner is necessary usingvarious modalities.
Endoscopic ultrasonography (EUS) is a well-established and less-invasive modality for CP diagnosis [5-10]. Although endoscopic retrograde pancreatigraphy (ERP) has been regarded as the gold standard for CP diagnosis, ERP cannot investigate the parenchymal changes. In that respect, the higher imaging resolution provided by EUS enables detection of subtle pancreatic abnormalities, not only parenchymal, but also ductal changes that are undetectable using other
modalities. In this review, the authors describe the role of EUS in CP diagnosis, especially in the early stage.
Normal Pancreas on EUSAn understanding of normal pancreas on EUS is extremely
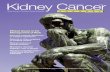
important for making EUS diagnosis of CP. The normal pancreatic parenchyma is uniformly depicted in equal or a slightly less hyperecho to the liver; it presents a so-called fine reticular pattern. The main duct dilation, duct irregularity and side branch ectasia are not visualized within the parenchyma [8]. Furthermore, the main ductal wall is observed as a uniform and slightly hyperlinear echo: 2.4 mm diameter in the head, 1.8 mm in the body, and 1.2 in the tail [6]. The EUS image of CP is defined based on these views. The EUS image of a normal pancreas is presented in figure 1.
EUS Features of Chronic PancreatitisCP is characterized by fibrosis of parenchyma along with ductal
changes in the pancreas. These changes of fibrosis have been characterized as hyperechoic using ultrasound [11-13]. The superiority of EUS is not so high in the case of advanced CP because typical CP findings such as atrophy, calcification, main duct dilation, duct irregularity, cyst are readily observed even using other modalities. However, it is difficult to observe minute changes of pancreatic parenchyma using means other than EUS. Among patients with chronic pancreatitis, EUS will reveal all pancreatic abnormalities. Typical EUS findings are shown in figures 2-6.
Diagnosis of CP using EUSTraditional EUS criteria for diagnosis of CP
Several studies have compared EUS findings with ERP (Cambridge classification) for CP evaluation [14]. Results of these studies suggest that ductal and parenchymal abnormalities detected using EUS correlate with the presence of CP. From these studies, the traditional EUS criteria
Figure 1: Normal pancreatic parenchyma on EUS. Homogeneous and finely reticular patterns are visible in parenchyma without dilated ducts.
-
Citation: Yamabe A, Irisawa A, Shibukawa G, Abe Y, Nikaido A, et al. (2013) Endosonographic Diagnosis of Chronic Pancreatitis. J Gastroint Dig Syst S2: 005. doi:10.4172/2161-069X.S2-005
Page 2 of 5
J Gastroint Dig Syst Gastrointestinal Endoscopy ISSN: 2161-069X, an open access journal
for CP are recognized as follows: hyperechoic foci, hyperechoic strands, parenchymal lobularity, irregular pancreatic duct margins, hyperechoic pancreatic duct margins, visible pancreatic side branches, pancreatic duct dilation, shadowing calcifications and cysts. Opinions vary among researchers, but the presence of CP was diagnosed when EUS revealed at least 2-3 of the features described above. Our investigation also showed the over 80% patient who showed changes over ‘equivocal’ in Cambridge classification had more than three EUS findings [12]. In addition, the EUS is able to evaluate the severity of CP depending on the number of criteria present with high sensitivity and specificity. The disease severity was classified as mild (2 or 3-4 features), moderate (5-6 features), and severe (more than 7 features), based on ERP findings as a gold standard [8-10].
New EUS criteria for CP diagnosis
Several investigators have reported the total number of EUS criteria, which is not only useful for diagnosis of CP but also for assessing severity. However, individual EUS criteria are considered
to have their own importance in each ERP grading. Consequently, to discriminate against EUS features in every stage of CP, each EUS criterion was made as a point of reference for comparison between normal and varying degrees of CP. Irisawa et al. [12] reported the important EUS features in each severity: hyperechoic foci in mild CP, hyperechoic foci/visible side-branches/duct dilatation in moderate CP, and visible side-branches/duct dilatation/duct irregularity/calcification in severe CP (p
-
Citation: Yamabe A, Irisawa A, Shibukawa G, Abe Y, Nikaido A, et al. (2013) Endosonographic Diagnosis of Chronic Pancreatitis. J Gastroint Dig Syst S2: 005. doi:10.4172/2161-069X.S2-005
Page 3 of 5
J Gastroint Dig Syst Gastrointestinal Endoscopy ISSN: 2161-069X, an open access journal
as ‘with shadowing’ or ‘without shadowing’; Lobularity is subclassified as ‘with honeycombing’ and ‘without honeycombing’. However, as pancreatic duct findings, Calcification/stone in main duct are added to findings proposed previously such as Duct irregularity and Side branch dilation and Main duct dilation and Hyperechoic duct margins. Including subclassification, diagnostic criteria are produced based on 12 items described above about EUS findings and its grade. Creation of the newer Rosemont classification carried the hope of accomplishing the following: higher accuracy, better interobserver agreement, more well-received descriptors used by referring doctors (‘consistent with’, ‘suggestive of ’, etc.) than the more conventional descriptors of ‘high probability’, ‘indeterminate’, or ‘intermediate probability’, etc.). However, it was reported that most patients had the same diagnosis irrespective of the criteria that had been used [16]. No clear conclusion has been provided yet for whether traditional criteria or Rosemont classification is superior for CP diagnosis.
Proposed diagnostic criteria for early stage CP
Since the establishment of the landmark classification of pancreatitis at the Marseille symposium in 1963 [17], many classifications and diagnostic criteria have been proposed for chronic pancreatitis. However, general diagnostic criteria for CP are set for diagnosing advanced CP. They are unlikely to improve patients’ prognoses. In 2009, the Research Committee on Intractable Pancreatic Diseases supported by the Ministry of Health, Labour and Welfare of Japan, the Japan Pancreas Society and the Japanese Society of Gastroenterology
revised the criteria, including through the standpoint of diagnosing early CP using EUS [18]. It is a challenge aimed at improvement of the long-term prognosis of CP patients by early diagnosis and therapeutic intervention in this disease.
This criteria comprise six items: (1) characteristic imaging findings, (2) characteristic histological findings, (3) repeated upper abdominal pain, (4) abnormal pancreatic enzyme levels in the serum or urine, (5) abnormal pancreatic exocrine function, and (6) continuous heavy drinking of alcohol equivalent to or more than 80 g/day of pure ethanol, as determined in accordance with criteria for alcoholic CP reported by Ammann [19]. According to these criteria, early CP is diagnosed by the presence of characteristic imaging findings for early CP together with more than two items among (3)-(6). The characteristic imaging findings for early CP were set as the following seven EUS features (five parenchymal and two ductal features): (1) lobularity with honeycombing, (2) lobularity without honeycombing, (3) hyperechoic foci without shadowing, (4) stranding, (5) cysts, (6) dilated side branches, and (7) hyperechoic main pancreatic duct (MPD) margin [15] (Table 3). More than two among the seven features including any of (1)-(4), which are most likely to reflect fibrous changes in pancreatic parenchyma, are judged to be sufficient for the EUS findings of early CP [9-12,20,21]. It remains as a challenge for future study to ascertain whether early CP diagnosed using these criteria progress to advanced CP.
Correlation between EUS and histological findings
Several researchers have investigated whether EUS features of CP
Rosemont criteriaParenchymal criteria Duct criteria
Major A Hyperechoic foci (>2 mm in length/width with shadowing) MPD calculi (echogenic structure[s] within the MPD with acoustic shadowing)
Major B Lobularity (≥ 13 contiguous lobules = 'honeycombing')
Minor Cyst (anechoic, round/elliptical with or without septations) Dilated duct (≥ 3.5 mm in body or >1.5 mm in tail)*Hyperechoic strands (≥ 3 mm in at least 2 different directions with respect to the imaged plane) Irregular MPD contour (uneven or irregular outline and ectatic course)
Hyperechoic foci (>2 mm in length/width with no shadowing) Dilated side branch (>3 tubular anechoic structures each measuring ≥1 mm in width, budding from the MPD)Hyperechoic MPD wall (echogenic, distinct structure >50% of entire MPD in the body and tail)
Table 1: Endoscopic ultrasound criteria for the diagnosis of pancreatitis.
Rosemont criteriaConsistent with CP Suggestive of CP Indeterminate for CP Normal
A 1 major A feature (+) ≥ 3 minor features 1 major A feature (+) < 3 minor features 3 to 4 minor features, no major features ≤2 minor features, no major features
B 1 major A feature (+) major B feature 1 major B feature (+) 3 ≥ minor features major B feature alone or with
-
Citation: Yamabe A, Irisawa A, Shibukawa G, Abe Y, Nikaido A, et al. (2013) Endosonographic Diagnosis of Chronic Pancreatitis. J Gastroint Dig Syst S2: 005. doi:10.4172/2161-069X.S2-005
Page 4 of 5
J Gastroint Dig Syst Gastrointestinal Endoscopy ISSN: 2161-069X, an open access journal
are correlated with histology. Specific criteria such as hyperechoic foci, hyperechoic strands, and lobularity, which are identified only by EUS, were estimated as correlated respectively with histological findings as follows: focal fibrosis, bridging fibrosis, and interlobular fibrosis (Table 4) [11].
Varadarajulu et al. [22] reported that EUS features were significantly associated with histologic abnormalities in a prospective study of 42 non-calcific CP (NCCP) patients. Parenchymal EUS features that were significantly associated with histopathologic NCCP were echogenic foci (p
-
Citation: Yamabe A, Irisawa A, Shibukawa G, Abe Y, Nikaido A, et al. (2013) Endosonographic Diagnosis of Chronic Pancreatitis. J Gastroint Dig Syst S2: 005. doi:10.4172/2161-069X.S2-005
Page 5 of 5
J Gastroint Dig Syst Gastrointestinal Endoscopy ISSN: 2161-069X, an open access journal
more likely to develop pancreatic cancer than normal individuals are. Strong evidence indicates the association of hereditary pancreatitis and pancreatic cancer [4]. Therefore, the physician is frequently faced with difficult decisions about how to manage the risk. Nevertheless, the identification of pancreatic cancer in advanced CP is extremely difficult. Some reports in the literature demonstrate that EUS detectability of pancreatic cancer in patients with CP is around 60% [32], and 54-74%, even if using combined EUS-FNA [33-36]. Therefore, the follow-up of CP from early stages, which is not detected using traditional modalities (e.g., CT, ERCP), will be important to detect smaller cancer nodes.
ConclusionEUS is a useful and safe technique for detecting pancreatic
parenchymal and ductal abnormalities, which are suggestive of CP. Medical intervention for CP in the early stage, can improve the CP prognosis.
References
1. Etemad B, Whitcomb DC (2001) Chronic pancreatitis: diagnosis, classification, and new genetic developments. Gastroenterology 120: 682-707.
2. Clain JE, Pearson RK (1999) Diagnosis of chronic pancreatitis. Is a gold standard necessary? Surg Clin North Am 79: 829-845.
3. Sarles H, Cros RC, Bidart JM (1979) A multicenter inquiry into the etiology of pancreatic diseases. Digestion 19: 110-125.
4. Simon B, Printz H (2001) Epidemiological trends in pancreatic neoplasias. Dig Dis 19: 6-14.
5. Dancygier H (1995) Endoscopic ultrasonography in chronic pancreatitis. Gastrointest Endosc Clin N Am 5: 795-804.
6. Catalano MF, Geenen JE (1998) Diagnosis of chronic pancreatitis by endoscopic ultrasonography. Endoscopy 30: 111-115.
7. Wiersema MJ, Hawes RH, Lehman GA, Kochman ML, Sherman S, et al. (1993) Prospective evaluation of endoscopic ultrasonography and endoscopic retrograde cholangiopancreatography in patients with chronic abdominal pain of suspected pancreatic origin. Endoscopy 25: 555-564.
8. Bhutani MS (1999) Endoscopic ultrasound in pancreatic diseases. Indications, limitations, and the future. Gastroenterol Clin North Am 28: 747-770.
9. Sahai AV, Zimmerman M, Aabakken L, Tarnasky PR, Cunningham JT, et al. (1998) Prospective assessment of the ability of endoscopic ultrasound to diagnose, exclude, or establish the severity of chronic pancreatitis found by endoscopic retrograde cholangiopancreatography. Gastrointest Endosc 48: 18-25.
10. Catalano MF, Lahoti S, Geenen JE, Hogan WJ (1998) Prospective evaluation of endoscopic ultrasonography, endoscopic retrograde pancreatography, and secretin test in the diagnosis of chronic pancreatitis. Gastrointest Endosc 48: 11-17.
11. Raimondo M, Wallace MB (2004) Diagnosis of early chronic pancreatitis by endoscopic ultrasound. Are we there yet? JOP 5: 1-7.
12. Irisawa A, Katakura K, Ohira H, Sato A, Bhutani MS, et al. (2007) Usefulness of endoscopic ultrasound to diagnose the severity of chronic pancreatitis. Journal of Gastroenterol 42: 90-94.
13. Irisawa A, Mishra G, Hernandez LV, Bhutani MS (2004) Quantitative analysis of endosonographic parenchymal echogenicity in patients with chronic pancreatitis. J Gastroenterol Hepatol 19: 1199-1205.
14. Sarner M, Cotton PB (1984) Classification of pancreatitis. Gut 25: 756-759.
15. Catalano MF, Sahai A, Levy M, Romagnuolo J, Wiersema M, et al. (2009) EUS-based criteria for the diagnosis of chronic pancreatitis: The Rosemont classification. Gastrointest Endosc 69: 1251-1261.
16. Kalmin B, Hoffman B, Hawes R, Romagnuolo J (2011) Conventional versus Rosemont endoscopic ultrasound criteria for chronic pancreatitis: comparing interobserver reliability and intertest agreement. Can J Gastroenterol 25: 261-264.
17. Sarles H (1963) Pancreatitis: Symposium of Marseille. Karger: 1965.
18. Shimosegawa T, Kataoka K, Kamisawa T, Miyakawa H, Ohara H, et al. (2010) The revised Japanese clinical diagnostic criteria for chronic pancreatitis. J Gastroenterol 45: 584-591.
19. Ammann RW (1997) A clinically based classification system for alcoholic chronic pancreatitis: summary of an international workshop on chronic pancreatitis. Pancreas 14: 215-221.
20. Chong AK, Hawes RH, Hoffman BJ, Adams DB, Lewin DN, et al (2007) Diagnostic performance of EUS for chronic pancreatitis: a comparison with histopathology. Gastrointest Endosc 65: 808-814.
21. Gleeson FC, Topazian M (2009) Endoscopic retrograde chlangiopancreatography and endoscopic ultrasound for diagnosis of chronic pancreatitis. Curr Gastroenterol Rep 9: 123-129.
22. Varadarajulu S, Eltoum I, Tamhane A, Eloubeidi MA (2007) Histopathologic correlates of noncalcific chronic pancreatitis by EUS: a prospective tissue characterization study. Gastrointest Endosc 66: 501-509.
23. Albashir S, Bronner MP, Parsi MA, Walsh RM, Stevens T (2010) Endoscopic ultrasound, secretin endoscopic pancreatic function test, and histology: correlation in chronic pancreatitis. Am J Gastroenterol 105: 2498-2503.
24. Bhutani MS, Ahmed I, Verma D, Xiao SY, Brining D (2009) An animal model for studying endoscopic ultrasound changes of early chronic pancreatitis with histologic correlation: a pilot study. Endoscopy 41: 352-356.
25. Bhutani MS (1999) Endoscopic ultrasonography: changes of chronic pancreatitis in asymptomatic and symptomatic alcoholic patients. J Ultrasound Med 18: 455-462.
26. Wallace MB, Hawes RH, Durkalski V, Chak A, Mallery S (2001) The reliability of EUS for the diagnosis of chronic pancreatitis: interobserver agreement among experienced endosonographers. Gastrointest Endosc 53: 294-299.
27. Nattermann C, Goldschmidt AJ, Dancygier H (1993) Endosonography in chronic pancreatitis: A comparison between endoscopic retrograde pancreatography and endoscopic ultrasonography. Endoscopy 25: 565.
28. Rajan E, Clain JE, Levy MJ, Norton ID, Wang KK, (2005) Age-related changes in the pancreas identified by EUS: a prospective evaluation. Gastrointest Endosc 61: 401-406.
29. Yusoff IF, Sahai AV (2004) A prospective, quantitative assessment of the effect of ethanol and other variables on the endosonographic appearance of the pancreas. Clin Gastroenterol Hepatol 2: 405-409.
30. Al-Haddad M, Khashab M, Zyromski N, Pungpapong S, Wallace MB, et al. (2009) Risk factors for hyperechogenic pancreas on endoscopic ultrasound: a case-control study. Pancreas 38: 672-675.
31. Chang KJ, Erickson RA, Chak A, Lightdale C, Chen YK, et al. (2010) EUS compared with endoscopy plus transabdominal US in the initial diagnostic evaluation of patients with upper abdominal pain. Gastrointest Endosc 72: 967-974.
32. Fritscher-Ravens A, Brand L, Knöfel WT, Bobrowski C, Topalidis T, et al. (2002) Comparison of endoscopic ultrasound-guided fine needle aspiration for focal pancreatic lesions in patients with normal parenchyma and chronic pancreatitis. Am J Gastroenterol 97: 2768-2775.
33. Barthet M, Portal I, Boujaoude J, Bernard JP, Sahel J (1996) Endoscopic ultrasonographic diagnosis of pancreatic cancer complicating chronic pancreatitis. Endoscopy 28: 487-491.
34. Ardengh JC, Lopes CV, Campos AD, Pereira de Lima LF, Venco F, et al. (2007) Endoscopic ultrasound and fine needle aspiration in chronic pancreatitis: differential diagnosis between pseudotumoral masses and pancreatic cancer. JOP 8: 413-421.
35. Varadarajulu S, Tamhane A, Eloubeidi MA (2005) Yield of EUS-guided FNA of pancreatic masses in the presence or the absence of chronic pancreatitis. Gastrointest Endosc 62: 728-736.
36. Krishna NB, Mehra M, Reddy AV, Agarwal B (2009) EUS/EUS-FNA for suspected pancreatic cancer: influence of chronic pancreatitis and clinical presentation with or without obstructive jaundice on performance characteristics. Gastrointest Endosc 70: 70-79.
This article was originally published in a special issue, Gastrointestinal Endoscopy handled by Editor(s). Dr. Rohan R. Walvekar, LSU Health Sciences Center, New Orleans, USA
http://www.ncbi.nlm.nih.gov/pubmed/11179244http://www.ncbi.nlm.nih.gov/pubmed/11179244http://www.ncbi.nlm.nih.gov/pubmed/10470330http://www.ncbi.nlm.nih.gov/pubmed/10470330http://www.ncbi.nlm.nih.gov/pubmed/478188http://www.ncbi.nlm.nih.gov/pubmed/478188http://www.ncbi.nlm.nih.gov/pubmed/11385246http://www.ncbi.nlm.nih.gov/pubmed/11385246http://europepmc.org/abstract/MED/8535628/reload=0;jsessionid=eoyGPPwwh5LPwprQoOXd.4http://europepmc.org/abstract/MED/8535628/reload=0;jsessionid=eoyGPPwwh5LPwprQoOXd.4http://www.ncbi.nlm.nih.gov/pubmed/8119204http://www.ncbi.nlm.nih.gov/pubmed/8119204http://www.ncbi.nlm.nih.gov/pubmed/8119204http://www.ncbi.nlm.nih.gov/pubmed/8119204http://www.ncbi.nlm.nih.gov/pubmed/10503148http://www.ncbi.nlm.nih.gov/pubmed/10503148http://www.ncbi.nlm.nih.gov/pubmed/9684659http://www.ncbi.nlm.nih.gov/pubmed/9684659http://www.ncbi.nlm.nih.gov/pubmed/9684659http://www.ncbi.nlm.nih.gov/pubmed/9684659http://www.ncbi.nlm.nih.gov/pubmed/9684659http://www.ncbi.nlm.nih.gov/pubmed/9684658http://www.ncbi.nlm.nih.gov/pubmed/9684658http://www.ncbi.nlm.nih.gov/pubmed/9684658http://www.ncbi.nlm.nih.gov/pubmed/9684658http://www.ncbi.nlm.nih.gov/pubmed/14730117http://www.ncbi.nlm.nih.gov/pubmed/14730117http://www.ncbi.nlm.nih.gov/pubmed/17238035http://www.ncbi.nlm.nih.gov/pubmed/17238035http://www.ncbi.nlm.nih.gov/pubmed/17238035http://www.ncbi.nlm.nih.gov/pubmed/15377300http://www.ncbi.nlm.nih.gov/pubmed/15377300http://www.ncbi.nlm.nih.gov/pubmed/15377300http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1432589/http://www.ncbi.nlm.nih.gov/pubmed/19243769http://www.ncbi.nlm.nih.gov/pubmed/19243769http://www.ncbi.nlm.nih.gov/pubmed/19243769http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3115006/http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3115006/http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3115006/http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3115006/http://books.google.co.in/books/about/Pancreatitis.html?id=pf_oPgAACAAJ&redir_esc=yhttp://www.ncbi.nlm.nih.gov/pubmed/20422433http://www.ncbi.nlm.nih.gov/pubmed/20422433http://www.ncbi.nlm.nih.gov/pubmed/20422433http://www.ncbi.nlm.nih.gov/pubmed/9094150http://www.ncbi.nlm.nih.gov/pubmed/9094150http://www.ncbi.nlm.nih.gov/pubmed/9094150http://www.ncbi.nlm.nih.gov/pubmed/17466199http://www.ncbi.nlm.nih.gov/pubmed/17466199http://www.ncbi.nlm.nih.gov/pubmed/17466199http://www.ncbi.nlm.nih.gov/pubmed/17418057http://www.ncbi.nlm.nih.gov/pubmed/17418057http://www.ncbi.nlm.nih.gov/pubmed/17418057http://www.ncbi.nlm.nih.gov/pubmed/17640639http://www.ncbi.nlm.nih.gov/pubmed/17640639http://www.ncbi.nlm.nih.gov/pubmed/17640639http://www.ncbi.nlm.nih.gov/pubmed/20606675http://www.ncbi.nlm.nih.gov/pubmed/20606675http://www.ncbi.nlm.nih.gov/pubmed/20606675http://www.ncbi.nlm.nih.gov/pubmed/19340741http://www.ncbi.nlm.nih.gov/pubmed/19340741http://www.ncbi.nlm.nih.gov/pubmed/19340741http://www.ncbi.nlm.nih.gov/pubmed/10400047http://www.ncbi.nlm.nih.gov/pubmed/10400047http://www.ncbi.nlm.nih.gov/pubmed/10400047http://www.ncbi.nlm.nih.gov/pubmed/11231386http://www.ncbi.nlm.nih.gov/pubmed/11231386http://www.ncbi.nlm.nih.gov/pubmed/11231386http://www.ncbi.nlm.nih.gov/pubmed/8119205http://www.ncbi.nlm.nih.gov/pubmed/8119205http://www.ncbi.nlm.nih.gov/pubmed/8119205http://www.ncbi.nlm.nih.gov/pubmed/15758911http://www.ncbi.nlm.nih.gov/pubmed/15758911http://www.ncbi.nlm.nih.gov/pubmed/15758911http://www.ncbi.nlm.nih.gov/pubmed/15118979http://www.ncbi.nlm.nih.gov/pubmed/15118979http://www.ncbi.nlm.nih.gov/pubmed/15118979http://www.ncbi.nlm.nih.gov/pubmed/19506531http://www.ncbi.nlm.nih.gov/pubmed/19506531http://www.ncbi.nlm.nih.gov/pubmed/19506531http://www.ncbi.nlm.nih.gov/pubmed/20650452http://www.ncbi.nlm.nih.gov/pubmed/20650452http://www.ncbi.nlm.nih.gov/pubmed/20650452http://www.ncbi.nlm.nih.gov/pubmed/20650452http://www.ncbi.nlm.nih.gov/pubmed/12425546http://www.ncbi.nlm.nih.gov/pubmed/12425546http://www.ncbi.nlm.nih.gov/pubmed/12425546http://www.ncbi.nlm.nih.gov/pubmed/12425546http://www.ncbi.nlm.nih.gov/pubmed/8886634http://www.ncbi.nlm.nih.gov/pubmed/8886634http://www.ncbi.nlm.nih.gov/pubmed/8886634http://www.ncbi.nlm.nih.gov/pubmed/17625292http://www.ncbi.nlm.nih.gov/pubmed/17625292http://www.ncbi.nlm.nih.gov/pubmed/17625292http://www.ncbi.nlm.nih.gov/pubmed/17625292http://www.ncbi.nlm.nih.gov/pubmed/16246688http://www.ncbi.nlm.nih.gov/pubmed/16246688http://www.ncbi.nlm.nih.gov/pubmed/16246688http://www.ncbi.nlm.nih.gov/pubmed/19249774http://www.ncbi.nlm.nih.gov/pubmed/19249774http://www.ncbi.nlm.nih.gov/pubmed/19249774http://www.ncbi.nlm.nih.gov/pubmed/19249774
TitleCorresponding authorAbstractKeywordsIntroductionNormal Pancreas on EUS EUS Features of Chronic Pancreatitis Diagnosis of CP using EUS Traditional EUS criteria for diagnosis of CP New EUS criteria for CP diagnosis Proposed diagnostic criteria for early stage CP Correlation between EUS and histological findings Issues of CP diagnosis by EUS
Role and Future Development of EUS in CP Diagnosis ConclusionFigure 1Figure 2Figure 3Figure 4Figure 5Figure 6Table 1Table 2Table 3Table 4References
Related Documents