Journal of Bangladesh College of Physicians and Surgeons Vol. 28, No. 1, January 2010 Official Journal of the Bangladesh College of Physicians and Surgeons BCPS Bhaban, 67 Shaheed Tajuddin Ahmed Sarani Mohakhali, Dhaka-1212, Bangladesh EDITORIAL BOARD ADVISORY BOARD PUBLISHED BY Nazmun Nahar S.A.M. Golam Kibria Md. Sanawar Hossain Mohammod Shahidullah Mahmud Hasan Ava Hossain Kanak Kanti Barua Abdul Kader Khan Quazi Deen Mohammad Choudhury Ali Kawser Md. Ruhul Amin A.H..M. Towhidul Anowar Sayeba Akhter M.A. Majid T.I.M. Abdullah-Al-Faruq Mohammad Saiful Islam Md. Abul Kashem Khandaker A.K.M. Mahbubur Rahman Rashid-E-Mahbub A. K.M. Anowarul Azim Editorial Staff Afsana Huq Dilruba Pervin Professor Quazi Tarikul Islam on behalf of the Bangladesh College of Physicians and Surgeons PRINTED AT Asian Colour Printing 130 DIT Extension Road, Fakirerpool Dhaka-1000, Phone : 9357726, 8362258 ANNUAL SUBSCRIPTION Tk. 300/- for local and US$ 30 for overseas subscribers Chairperson A.K.M Mahbubur Rahamn Editor-in-Chief Quazi Tarikul Islam Editors K.M.H.S. Sirajul Haque Mahmud Hasan Md. Salehuddin M.A. Majid Abdus Salam Shafiqul Hoque Md. Abul Faiz Zafar Ahmed Latif Syed Kamaluddin Ahmed Projesh Kumar Roy A.K.M. Khorshed Alam Shafquat Hussain Khundkar Choudhury Ali Kawser Emran Bin Yunus U.H. Shahera Khatun Md. Abdul Masud Mohammed Abu Azhar Nazneen Kabir ( Brig.Gen.) Harunur Rashid T.I.M. Abdullah-Al-Faruq Md. Rajibul Alam Syed Azizul Haque Rezawana Quaderi Belayat Hossain Siddiquee Md. Habibur Rahman Dewan Saifuddin Ahmed Narayan Chandra Saha Md. Azharul Islam Md. Nazrul Islam Abdul Wadud Chowdhury Nishat Begum ( Col) Muhammad Saiful Islam Hasina Afroz Rezaul Karim Kazal Mohammad Khairuzzaman The Journal of Bangladesh College of Physicians and Surgeons is a peer reviewed Journal. It is published three times in a year, (January, May and September). It accepts original articles, review articles, and case reports. Complimentary copies of the journal are sent to libraries of all medical and other relevant academic institutions in the country and selected institutions abroad. While every effort is always made by the Editorial Board and the members of the Journal Committee to avoid inaccurate or misleading information appearing in the Journal of Bangladesh College of Physicians and Surgeons, information within the individual article are the responsibility of its author(s). The Journal of Bangladesh College of Physicians and Surgeons, its Editorial Board and Journal Committee accept no liability whatsoever for the consequences of any such inaccurate and misleading information, opinion or statement. ADDRESS OF CORRESPONDENCE Editor-in-Chief, Journal of Bangladesh College of Physicians and Surgeons, BCPS Bhaban, 67, Shaheed Tajuddin Ahmed Sarani, Mohakhali, Dhaka-1212, Tel : 8825005-6, 8856616-7, Fax : 880-2-8828928, E-mail : <[email protected]> Editor’s e-mail: [email protected]

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Journal of Bangladesh College ofPhysicians and Surgeons
Vol. 28, No. 1, January 2010Official Journal of the Bangladesh College of Physicians and Surgeons
BCPS Bhaban, 67 Shaheed Tajuddin Ahmed SaraniMohakhali, Dhaka-1212, Bangladesh
EDITORIAL BOARD ADVISORY BOARD
PUBLISHED BY
Nazmun NaharS.A.M. Golam KibriaMd. Sanawar HossainMohammod ShahidullahMahmud HasanAva HossainKanak Kanti BaruaAbdul Kader KhanQuazi Deen MohammadChoudhury Ali KawserMd. Ruhul AminA.H..M. Towhidul AnowarSayeba AkhterM.A. MajidT.I.M. Abdullah-Al-FaruqMohammad Saiful IslamMd. Abul Kashem KhandakerA.K.M. Mahbubur RahmanRashid-E-MahbubA. K.M. Anowarul Azim
Editorial StaffAfsana HuqDilruba Pervin
Professor Quazi Tarikul Islamon behalf of the Bangladesh Collegeof Physicians and Surgeons
PRINTED ATAsian Colour Printing130 DIT Extension Road, FakirerpoolDhaka-1000, Phone : 9357726, 8362258
ANNUAL SUBSCRIPTION
Tk. 300/- for local and US$ 30for overseas subscribers
ChairpersonA.K.M Mahbubur RahamnEditor-in-ChiefQuazi Tarikul IslamEditorsK.M.H.S. Sirajul HaqueMahmud HasanMd. SalehuddinM.A. MajidAbdus SalamShafiqul HoqueMd. Abul FaizZafar Ahmed LatifSyed Kamaluddin AhmedProjesh Kumar RoyA.K.M. Khorshed AlamShafquat Hussain KhundkarChoudhury Ali KawserEmran Bin YunusU.H. Shahera KhatunMd. Abdul MasudMohammed Abu AzharNazneen Kabir( Brig.Gen.) Harunur RashidT.I.M. Abdullah-Al-FaruqMd. Rajibul AlamSyed Azizul HaqueRezawana QuaderiBelayat Hossain SiddiqueeMd. Habibur RahmanDewan Saifuddin AhmedNarayan Chandra SahaMd. Azharul IslamMd. Nazrul IslamAbdul Wadud ChowdhuryNishat Begum( Col) Muhammad Saiful IslamHasina AfrozRezaul Karim KazalMohammad Khairuzzaman
The Journal of BangladeshCollege of Physicians andSurgeons is a peer reviewedJournal. It is published threetimes in a year, (January,May and September). Itaccepts original articles,review articles, and casereports. Complimentary copiesof the journal are sent tolibraries of all medical andother relevant academic institutionsin the country and selectedinstitutions abroad.
While every effort is alwaysmade by the Editorial Boardand the members of the JournalCommittee to avoid inaccurateor misleading informationappearing in the Journal ofBangladesh College of Physiciansand Surgeons, informationwithin the individual article arethe responsibility of its author(s).The Journal of BangladeshCollege of Physicians andSurgeons, its Editorial Boardand Journal Committee acceptno liability whatsoever for theconsequences of any suchinaccurate and misleadinginformation, opinion or statement.
ADDRESS OF CORRESPONDENCEEditor-in-Chief, Journal of Bangladesh College of Physicians and Surgeons, BCPS Bhaban, 67, Shaheed Tajuddin Ahmed Sarani, Mohakhali,
Dhaka-1212, Tel : 8825005-6, 8856616-7, Fax : 880-2-8828928, E-mail : <[email protected]> Editor’s e-mail: [email protected]
INFORMATION FOR AUTHORS
The Journal of Bangladesh College of Physicians andSurgeons agrees to accept manuscript prepared inaccordance with the 'Uniform Requirements Submitted tothe Biomedical Journals' published in the New EnglandJournal of Medicine 1991; 324 : 424-8.
Aims and scope:The Journal of Bangladesh College of Physicians andSurgeons is one of the premier clinical and laboratory basedresearch journals in Bangladesh. Its international readershipis increasing rapidly. It features the best clinical andlaboratory based research on various disciplines of medicalscience to provide a place for medical scientists to relateexperiences which will help others to render better patientcare.
Conditions for submission of manuscript:
� All manuscripts are subject to peer-review.
� Manuscripts are received with the explicit understandingthat they are not under simultaneous consideration by anyother publication.
� Submission of a manuscript for publication implies thetransfer of the copyright from the author to the publisherupon acceptance. Accepted manuscripts become thepermanent property of the Journal of Bangladesh Collegeof Physicians and Surgeons and may not be reproducedby any means in whole or in part without the writtenconsent of the publisher.
� It is the author's responsibility to obtain permission toreproduce illustrations, tables etc. from otherpublications.
Ethical aspects:� Ethical aspect of the study will be very carefully
considered at the time of assessment of the manuscript.
� Any manuscript that includes table, illustration orphotograph that have been published earlier shouldaccompany a letter of permission for re-publication fromthe author(s) of the publication and editor/publisher ofthe Journal where it was published earlier.
� Permission of the patients and/or their families toreproduce photographs of the patients where identity isnot disguised should be sent with the manuscript.Otherwise the identity will be blackened out.
Preparation of manuscript:Criteria:Information provided in the manuscript are important andlikely to be of interest to an international readership.
Preparation:a) Manuscript should be written in English and typed on
one side of A4 (290 x 210cm) size white paper.
b) Double spacing should be used throughout.
c) Margin should be 5 cm for the header and 2.5 cm for theremainder.
d) Style should be that of modified Vancouver.
e) Each of the following section should begin on separatepage :
� Title page
� Summary/abstract
� Text
� Acknowledgement
� References
� Tables and legends.
f) Pages should be numbered consecutively at the upperright hand corner of each page beginning with the titlepage.
Title Page :The title page should contain:� Title of the article (should be concise, informative and
self-explanatory).
� Name of each author with highest academic degree
� Name of the department and institute where the work wascarried out
� Name and address of the author to whom correspondenceregarding manuscript to be made
� Name and address of the author to whom request forreprint should be addressed
Summary/Abstract :The summary/abstract of the manuscript :� Should be informative
� Should be limited to less than 200 words
� Should be suitable for use by abstracting journals andinclude data on the problem, materials and method, resultsand conclusion.
� Should emphasize mainly on new and important aspectsof the study
� Should contain only approved abbreviations
Introduction:The introduction will acquaint the readers with the problemand it should include:
� Nature and purpose of the study
� Rationale of the study/observation
� Strictly pertinent references
� Brief review of the subject excepting data andconclusion
Materials and method :This section of the study should be very clear and describe:� The selection criteria of the study population including
controls (if any).
� The methods and the apparatus used in the research.
� The procedure of the study in such a detail so that otherworker can reproduce the results.
� Previously published methods (if applicable) withappropriate citations.
Results:The findings of the research should be described here and itshould be:
� Presented in logical sequence in the text, tables andillustrations.
� Described without comment.
� Supplemented by concise textual description of the datapresented in tables and figures where it is necessaery.
Tables:During preparation of tables following principles should befollowed
� Tables should be simple, self-explanatory andsupplement, not duplicate the text.
� Each table should have a tittle and typed in double spacein separate sheet.
� They should be numbered consecutively with romannumerical in order of text. Page number should be in theupper right corner.
� If abbreviations are to be used, they should be explainedin footnotes.
Illustrations:Only those illustrations that clarify and increase theunderstanding of the text should be used and:
� All illustrations must be numbered and cited in the text.
� Print photograph of each illustration should be submitted.
� Figure number, tittle of manuscript, name ofcorresponding author and arrow indicating the top shouldbe typed on a sticky label and affixed on the back of eachillustration.
� Original drawings, graphs, charts and lettering should beprepared on an illustration board or high-grade whitedrawing paper by an experienced medical illustrator.
Figures and photographs:The figures and photographs :
� Should be used only where data can not be expressed inany other form
� Should be unmounted glossy print in sharp focus, 12.7 x17.3 cms in size.
� Should bear number, tittle of manuscript, name ofcorresponding author and arrow indicating the top on asticky label and affixed on the back of each illustration.
Legend:The legend:� Must be typed in a separate sheet of paper.
� Photomicrographs should indicate the magnification,internal scale and the method of staining.
Units:� All scientific units should be expressed in System
International (SI) units.
� All drugs should be mentioned in their generic form. Thecommercial name may however be used within brackets.
Discussion:The discussion section should reflect:
� The authors' comment on the results and to relate themto those of other authors.
� The relevance to experimental research or clinicalpractice.
� Well founded arguments.
References:This section of the manuscript :
� Should be numbered consecutively in the order in whichthey are mentioned in the text.
� Should be identified in the text by superscript in Arabicnumerical.
� Should use the form of references adopted by US NationalLibrary of Medicine and used in Index Medicus.
Acknowledgements :Individuals, organizations or bodies may be acknowledgedin the article and may include:
� Name (or a list) of funding bodies.
� Name of the organization(s) and individual(s) with theirconsent.
Manuscript submission:Manuscript should be submitted to the Editor-in-Chief andmust be accompanied by a covering letter and followinginclusions:

a) A statement regarding the type of article beingsubmitted.
b) A statement that the work has not been published orsubmitted for publication elsewhere.
c) A statement of financial or other relationships thatmight lead to a conflict of interests.
d) A statement that the manuscript has been read,approved and signed by all authors.
e) A letter from the head of the institution where the workhas been carried out stating that the work has beencarried out in that institute and there is no objection toits publication in this journal.
f) If the article is a whole or part of the dissertation or thesissubmitted for diploma/degree, it should be mentioned indetail and in this case the name of the investigator andguide must be specifically mentioned.
Submissions must be in triplicates with four sets ofillustrations. Text must be additionally submitted in a CD.
Editing and peer review:All submitted manuscripts are subject to scrutiny by theEditor in-chief or any member of the Editorial Board.Manuscripts containing materials without sufficientscientific value and of a priority issue, or not fulfilling therequirement for publication may be rejected or it may besent back to the author(s) for resubmission with necessarymodifications to suit one of the submission categories.Manuscripts fulfilling the requirements and found suitablefor consideration are sent for peer review. Submissions,found suitable for publication by the reviewer, may needrevision/ modifications before being finally accepted.Editorial Board finally decides upon the publishability ofthe reviewed and revised/modified submission. Proof ofaccepted manuscript may be sent to the authors, and shouldbe corrected and returned to the editorial office within oneweek. No addition to the manuscript at this stage will beaccepted. All accepted manuscript are edited according tothe Journal's style.
Reprints for the author(s):Ten copies of each published article will be provided to thecorresponding author free of cost. Additional reprints maybe obtained by prior request and only on necessary payment.
Subscription information:Journal of Bangladesh College of Physicians and SurgeonsISSN 1015-0870
Published by the Editor-in-Chief three times a year inJanuary, May and September
Annual SubscriptionLocal BDT = 300.00Overseas $ = 30.00
Subscription request should be sent to:Editor-in-ChiefJournal of Bangladesh College of Physicians and Surgeons67, Shaheed Tajuddin Ahmed SaraniMohakhali, Dhaka-1212.
Any change in address of the subscriber should be notifiedat least 6-8 weeks before the subsequent issue is publishedmentioning both old and new addresses.
Communication for manuscript submission:Communication information for all correspondence isalways printed in the title page of the journal. Anyadditional information or any other inquiry relating tosubmission of the article the Editor-in-Chief or the Journaloffice may be contacted.
Copyright :No part of the materials published in this journal may bereproduced, stored in a retrieval system or transmitted inany form or by any means electronic, mechanical,photocopying, recording or otherwise without the priorwritten permission of the publisher.
Reprints of any article in the Journal will be available fromthe publisher.

JOURNAL OF BANGLADESH COLLEGE OFPHYSICIANS AND SURGEONS
Vol. 28, No. 1, Page 1-68 January 2010
CONTENTS
Climate Change and Health 1M A Faiz, Quazi Tarikul Islam
EDITORIAL
ORIGINAL ARTICLES
REVIEW ARTICLES
CASE REPORTS
COLLEGE NEWS
FROM THE DESK OF EDITOR IN CHIEF
Institutional Factors Affecting Maternal Mortality in a Teaching Hospital 5HA Baby, DR ShahaComparative Study of Ephedrine and Mephertermine in Treatment of Hypotension 10in Patients Undergoing Elective Trans Urethral Resection Prostate (TURP)N Puri, A TalwarPreterm Prelabour Rupture of the Membrane & Feto-Maternal out come: an Observational Study 17S Akter, R Akther, M RashidBurden of Heart Failure Patients in a Tertiary Level Cardiac HospitalM Kabiruzzaman, FN Malik, N Ahmed, M Badiuzzaman, SR Choudhury, T Haque, H Rahmana, 24MN Ahmed, D Banik, MAM Khan, AK Dutta, S Sayeed, RK Khandaker, A Malik
Medical Treatment of Rheumatoid Arthritis: A Review 30AHM FerozAromatase Inhibitors: New Drug of Choice for Induction of Ovulation 40M Siddiqui, N Mahmud, MR Begum, T A Chowdhury
SHORT COMMUNICATION
LETTER TO THE EDITOR
Experience of Pandemic Influenza A (H1N1) 2009 at Dhaka Medical College Hospital
Ruptured uterus in primiparous women 45IP Alam, H AfrozYellow Nail Syndrome- A Case Report 49NH Chowdhury, S Selim, R Yasmin, AHM Rowshan, MR RahmanIsolated Facial Nerve Palsy in Childhood Acute Myeloid Leukemia 53MG Hafiz, A Islam, MA Mannan, F RahmanLupus Nephritis in a 2.5 Year Old Girl- An Uncommon Presentation 59H Rahman, A Begum, RR Roy, R Siddique, K Alam, S Haque, S Jahan, GM Uddin, MM Hossain
64
63
66
67
NAME OF THE REVIEWERS OF ARTICLES IN THIS ISSUE 68
Global climate is changing as manifested by risingsurface temperature, melting ice and snow, rising sealevel, increasing climate variability. For more than acentury levels of CO2, methane and other green housegases are increasing, and it is now scientific realitythat the temperature will rise 1.8-4oC and sea levelwill rise by 0.18-0.59 m by 2100. It is nowappreciated that ‘Climate change is the biggest globalhealth threat of the 21st century’.1
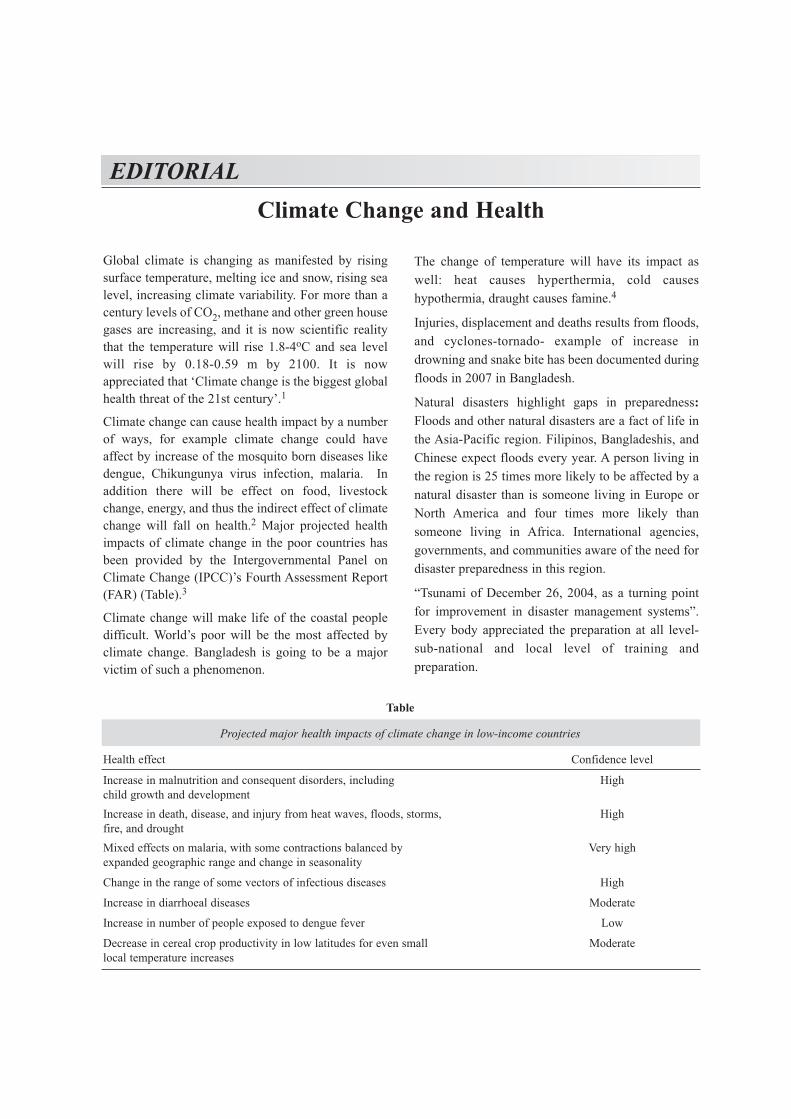
Climate change can cause health impact by a numberof ways, for example climate change could haveaffect by increase of the mosquito born diseases likedengue, Chikungunya virus infection, malaria. Inaddition there will be effect on food, livestockchange, energy, and thus the indirect effect of climatechange will fall on health.2 Major projected healthimpacts of climate change in the poor countries hasbeen provided by the Intergovernmental Panel onClimate Change (IPCC)’s Fourth Assessment Report(FAR) (Table).3
Climate change will make life of the coastal peopledifficult. World’s poor will be the most affected byclimate change. Bangladesh is going to be a majorvictim of such a phenomenon.
The change of temperature will have its impact aswell: heat causes hyperthermia, cold causeshypothermia, draught causes famine.4
Injuries, displacement and deaths results from floods,and cyclones-tornado- example of increase indrowning and snake bite has been documented duringfloods in 2007 in Bangladesh.
Natural disasters highlight gaps in preparedness:Floods and other natural disasters are a fact of life inthe Asia-Pacific region. Filipinos, Bangladeshis, andChinese expect floods every year. A person living inthe region is 25 times more likely to be affected by anatural disaster than is someone living in Europe orNorth America and four times more likely thansomeone living in Africa. International agencies,governments, and communities aware of the need fordisaster preparedness in this region.
“Tsunami of December 26, 2004, as a turning pointfor improvement in disaster management systems”.Every body appreciated the preparation at all level-sub-national and local level of training andpreparation.
Climate Change and HealthEDITORIAL
Table
Projected major health impacts of climate change in low-income countries
Health effect Confidence level
Increase in malnutrition and consequent disorders, including Highchild growth and developmentIncrease in death, disease, and injury from heat waves, floods, storms, Highfire, and droughtMixed effects on malaria, with some contractions balanced by Very highexpanded geographic range and change in seasonality
Change in the range of some vectors of infectious diseases High
Increase in diarrhoeal diseases Moderate
Increase in number of people exposed to dengue fever Low
Decrease in cereal crop productivity in low latitudes for even small Moderatelocal temperature increases
2
“Bangladesh has long been the leader in disaster riskmanagement and one of the key aspects of their workis the strong link between early warning,communication of that warning, and evacuationplans. There are cyclone shelters all over the country,which are built in consultation with communities. Therelay of cyclone and flood warnings is through acommunity channel as well.” Although 500 000people were killed by the 1972 cyclone, and another140 000 by the 1991 cyclone, Bangladesh hasmanaged to get their casualty numbers down to anestimated 4000–5000 in 2007’s cyclone SIDR. Thenumbers are still very high. “The country is stillembarking on building more of these double-purposecyclone shelters”. “The system can evacuate over 300000 people in 48 h-it is that well organized.”
World Health Assembly 2008 addressed theimportance of climate change and health:5
“The scientific evidence continues to mount,”, “theclimate is changing, the effects are already being felt,and human activities are a principal cause.”
There is an urgency of adapting health systems to dealwith the health risks of climate change-risks that willincrease in future, particularly in vulnerablegeographic regions and in poorly resourcedpopulations.
Weather-sensitive disease events give a clear previewof the health impacts of climate change. For example,major heat waves have exacted heavy tolls of extradeaths in many countries this decade.
Response of the health sector will need to beundertaken in wide collaboration with many othersectors of government and social action.The health sector, in general, has been slow toperceive the enormous significance of global climatechange, as a threat to Earth’s life-support systems,including the provision of water, food, clean air, andstable ecosystems-and, therefore, to humanwellbeing, health, and survival.
How climate change jeopardises the achievement ofthe Millennium Development Goals, especially thosethat relate directly to health outcomes: infectiousdiseases, hunger and under nutrition, and child andmaternal mortality.
The Assembly’s resolution lays out a five-pointagenda of research and action. First, fullerdocumentation of the risks to health and of
differences in vulnerability between and withinpopulations. Second, development of healthprotection strategies. Third, identification of thehealth co-benefits of actions taken to reducegreenhouse gas emissions or, in other sectors, to adaptto climate change. Fourth, development of decision-support tools and systems to predict the impact ofclimate change for member states. And fifth,estimation of the financial costs of actions andinactions in relation to health.
The health sector will be the source of much crucialinformation and understanding about the humanconsequences of climate change.
The different stakeholders in the health sector,doctors, nurses and other practitioners,administrators, public health personnel are toappreciate the importance of the issue and they haveto:6
� Promote recognition of the main health threatsfrom climate change.
� Find the win-win actions that promote health asthey reduce climate change – e.g. more activetransport in automobile-dependent cultures willimprove air quality, decrease greenhouse gasemissions and combat obesity.
� Stress the health sector’s direct responsibility torespond to the threats to health that climate changeis posing to the population.
� Provide an example of how the health sector candemonstrate carbon neutral practice.
� Point out that many of the most effectiveinterventions in protecting health from climatechange are basic public health interventions.
� Include issues of climate-related health threats ingeneral health training and continuing educationmodules.
It is now more and more appreciated that like manypublic health interventions prevention of healthimpact of climate change is possible.7 Primaryprevention of health impact of climate change ismitigation. Mitigation involves reduced productionand /or increased sequestration of green house gases.The responsibility of mitigation lies also with otherthan health ministry like ministry of communicationand transport, works (architecture) and energy.
Journal of Bangladesh College of Physicians and Surgeons Vol. 28, No. 1, January 2010

3
Secondary and tertiary prevention of the health effectof climate change is adaptation. Adaptation refers toactivities that preserves function and health in the faceof existing climate change and here the responsibilitylies with the Ministry of Health and Family Welfare.
The health sector in poor countries are already in stressto cope with existing health problems related tocommunicable and non communicable diseases. Inorder to adapt the new health threats of climate changelots to be done in different areas of health servicedelivery. Bangladesh is in a crucial position and wehave to act now to protect our population from thehealth impacts of climate change. In the first place as animportant member of the health professional we have toconvince ourselves that it is a reality and we have tocontinue to communicate in various ways of the healthbenefits of ‘low-carbon living’ which has far reachingimpact8. Health care professionals are in better positionto promote health benefit of clean cooking and walkingor bicycling which will lead to reduction of respiratoryillness and coronary heart disease.9 At the same time wehave to advocate and continually generate evidence onpriority basis by various studies related to impact ofclimate change on climate-sensitive diseases includingmonitoring and utilize the gathered knowledge inprotecting the community by a concerted effort.
(J Bangladesh Coll Phys Surg 2010; 28: 1-3)
M A Faiz1, Quazi Tarikul Islam2
Professor of Medicine,1 Sir Salimullah MedicalCollege, 2Dhaka Medical College Dhaka, Bangladesh.
References:1. Costello A, Abbas M, Allen A, et al. (2009) Lancet and
University College London Institute for Global HealthCommission: managing the health effects of climate change.Lancet; 373: 1693–733.
2. McMichael AJ, Haines A, Sloof R, Kovats S, eds. Climatechange and human health. Geneva: WHO/UNEP/WMO,1996.
3. Intergovernmental Panel on Climate Change. Climate change2007: impacts, adaptation and vulnerability. Contribution ofWorking Group II to the Fourth Assessment Report of theIntergovernmental Panel on Climate Change. Parry ML,Canziani OF, Palutikof JP, van der Linden PJ, Hanson CE,eds. Cambridge UK: Cambridge University Press, 2007.www.ipcc.ch/ipccreports/ar4-wg2.htm.
4. Haines A, Kovats R S, Campbell-Lendrum D, Corvalan C(2006). Climate change and human health: impacts,vulnerability, and mitigation, Lancet; 367: 2101–09.
5. WHO. The impact of climate change on human health. April7, 2008. http://www.who.int/ mediacentre/news/ statements/2008/s05/en/index.html.
6. WHO (2008) Protecting Health from Climate Change Atoolkit for event organizers. World Health Day 2008.
7. St. Louis M E, Hess J J, (2008). Climate Change: Impacts onand Implications for Global Health. Am J Prev Medicine; 35:527 – 538.
8. Lim V, Stubbs J W, Nahar N, Amarasena N, Chaudry Z U, etal. (2009). Politicians must heed health effects of climatechange. Lancet; 374: 973.
9. Wilks M (2010). “Greenwash” at the climate change summitin Copenhagen: Failure of leadership challenges doctors tolead by example. BMJ 340: 4-5.
Climate Change and Health M A Faiz & Quazi Tarikul Islam
Introduction:Maternal mortality is a major public health problem indeveloping countries like Bangladesh. Of theestimated total 536000 maternal death worldwide in2005, developing countries accounted for 99% of thesedeaths and in Bangladesh the number was 21000.1
A systematic review showed hemorrhage, hypertensivedisorders, abortion, sepsis and obstructed labor are themajor causes of maternal death world wide.2
The major causes of maternal mortality inBangladesh are hemorrhage, eclampsia, sepsis,induced abortions, and obstructed labor. 3, 4, 5, 6.
Eighty percent of these are preventable as theydepend strongly on quality of care.7
The three delays increase the risk to a woman’s lifeduring pregnancy, delay in deciding to seek care(First delay), delay in reaching a medical facility(Second delay) and delay in receiving quality care atthe facility (Third delay).8 The first and seconddelays are directly related to the factors in thefamily and community while third delay isconnected with factors related to health facility andquality of care.
Identification of institutional factors of third delayand their reduction can improve the quality of care atexisting medical facilities. This will have a greatestimpact in reducing maternal deaths.
Faridpur Medical College Hospital, a 250 beddedhospital, is a tertiary public health care centre inBangladesh situated in Faridpur district. In additionto provide clinical service this hospital is providingtraining to undergraduate medical students and
Institutional Factors Affecting Maternal Mortalityin a Teaching Hospital
HA BABYa, DR SHAHAb
Summary:Objective: To identify the institutional factors causingthird delay of maternal mortality in Faridpur MedicalCollege Hospital- a tertiary public health care centre inBangladesh.
Design: Cross-Sectional Study.
Study period: January 2001 to December 2005.
Methods and Materials: The case notes of all maternaldeaths were reviewed at the end of each month during thestudy period. Various factors causing delay in the propermanagement of the cases were identified and noted. The dataobtained from these reviews formed the basis of this study.
Results: During the study period total 202 mothers diedgiving the maternal mortality 2010.5 per 100,000deliveries. In 130(64.4%) cases one or more institutionalfactors were identified those contributed significantly tomaternal deaths. The identified factors were: delayed
blood transfusion or non availability of blood (40%);delayed or lack of operative interventions (37%); late ornonattendance by senior doctors (24.8%); operativeinterventions done by junior doctors (9.9%); nonavailability of ICU (intensive care unit) facility (29.7%)and of medicine (7.4%).
Conclusion: There is a steady fall in maternal mortalityratio (MMR) in Bangladesh since 1990. But to reach theMillennium Development Goal for maternal health(MDG-5), the MMR will need to decrease at a much fasterrate in the future. Improvement of the infrastructuralfacilities in the hospital can help to remove thepreventable institutional factors causing third delay ofmaternal mortality. This can be a short term strategy toreduce maternal mortality.
Key words: Maternal mortality, Institutional factor, Thirddelay.
(J Bangladesh Coll Phys Surg 2010; 28: 5-9)
ORIGINAL ARTICLES
a. Dr. Hosne Ara Baby, FCPS (Obs & Gyne), Professor(Obstetrics & Gynecology), Enam Medical College, Savar.
b. Dr. Dipti Rani Shaha, FCPS (Obs & Gyne), Junior Consultant(Obstetrics & Gynecology), Faridpur Medical CollegeHospital. Faridpur
Address of Correspondence: Dr. Hosne Ara Baby, ‘Alindo’Apartment, Flat No- 102, House No- 88, Road No- 8/A (New),Dhanmondi, Dhaka- 1209.
Received: 18 December, 2007 Accepted: 29 October, 2009
6
postgraduate medical specialists includingObstetricians and Gynecologists. The aim of thisstudy is to determine the magnitude of maternalmortality in this institution and to identify theinstitutional factors causing the third delay andthereby contributed significantly to maternal death.
Methods and Materials:This is a cross-sectional study. During the studyperiod analysis of maternal deaths were done at theend of each month. Information was collected fromcase records and from attending nurses, doctors,consultants and sometimes from relatives of thepatients when available. Information was collectedregarding number and causes of maternal deaths andvarious factors causing delay in the propermanagement of these patients. All collectedinformation was recorded.
Blood transfusion was regarded delayed when itcould not be transfused within 2 hours of necessity.Attendance by senior doctors is considered delayedwhen it was not possible within 2 hours of patient’sadmission or of development of emergency inadmitted patients. Operative interventions wereregarded delayed when it could not be done within 2hours of necessity. Eclamptic patients withcomplications, patients with septic shock, heartfailure, and anesthetic complications were regardedto need ICU facility. Non availability of medicineswas regarded as a contributing factor when thespecific drugs for the disease that cause maternaldeath were unavailable, as for example Inj.MgSO4 incase of eclampsia or oxytocic drugs in case ofpostpartum hemorrhage.
Limitations of the study: Data regarding total numberdeliveries were collected from record book whichmay not be strictly accurate. Some contributingfactors may be missed because of lack of information.Maternal mortality is expressed as total number ofmaternal death per 100,000 of deliveries instead oflive birth and case fatality ratio is not expressed.
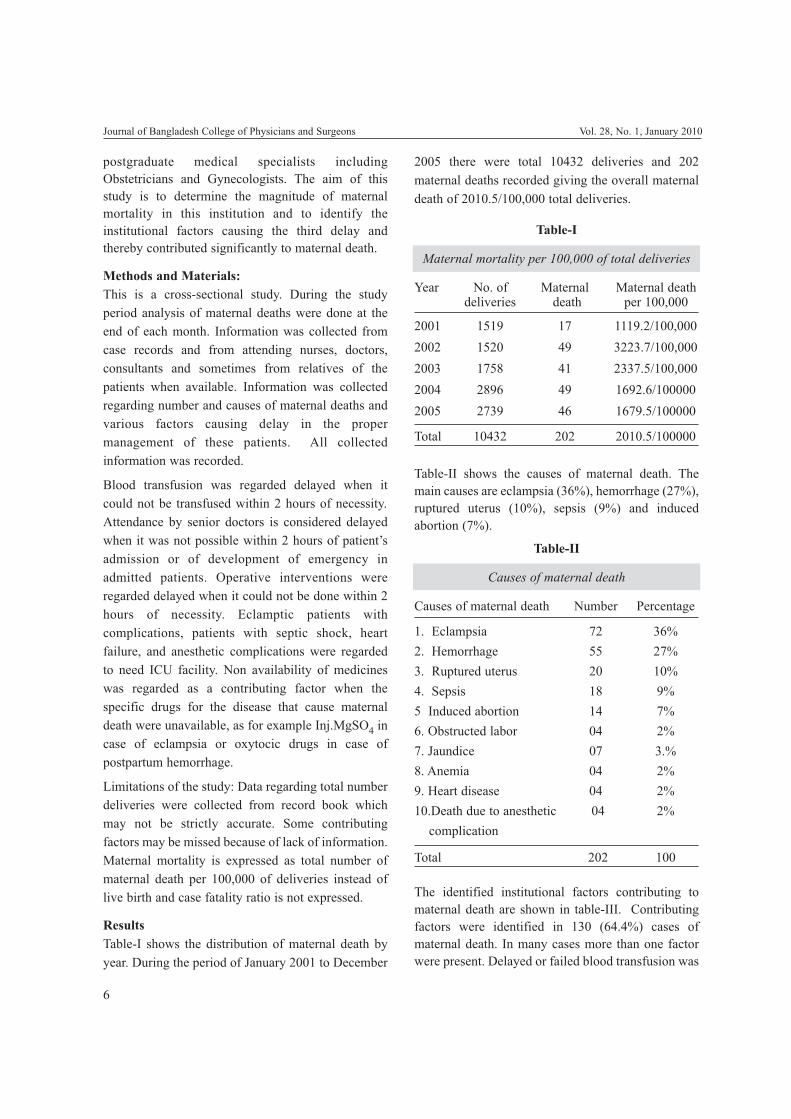
ResultsTable-I shows the distribution of maternal death byyear. During the period of January 2001 to December
2005 there were total 10432 deliveries and 202maternal deaths recorded giving the overall maternaldeath of 2010.5/100,000 total deliveries.
Table-I
Maternal mortality per 100,000 of total deliveries
Year No. of Maternal Maternal deathdeliveries death per 100,000
2001 1519 17 1119.2/100,0002002 1520 49 3223.7/100,0002003 1758 41 2337.5/100,0002004 2896 49 1692.6/1000002005 2739 46 1679.5/100000
Total 10432 202 2010.5/100000
Table-II shows the causes of maternal death. Themain causes are eclampsia (36%), hemorrhage (27%),ruptured uterus (10%), sepsis (9%) and inducedabortion (7%).
Table-II
Causes of maternal death
Causes of maternal death Number Percentage
1. Eclampsia 72 36%2. Hemorrhage 55 27%3. Ruptured uterus 20 10%4. Sepsis 18 9%5 Induced abortion 14 7%6. Obstructed labor 04 2%7. Jaundice 07 3.%8. Anemia 04 2%9. Heart disease 04 2%10.Death due to anesthetic 04 2%
complication
Total 202 100
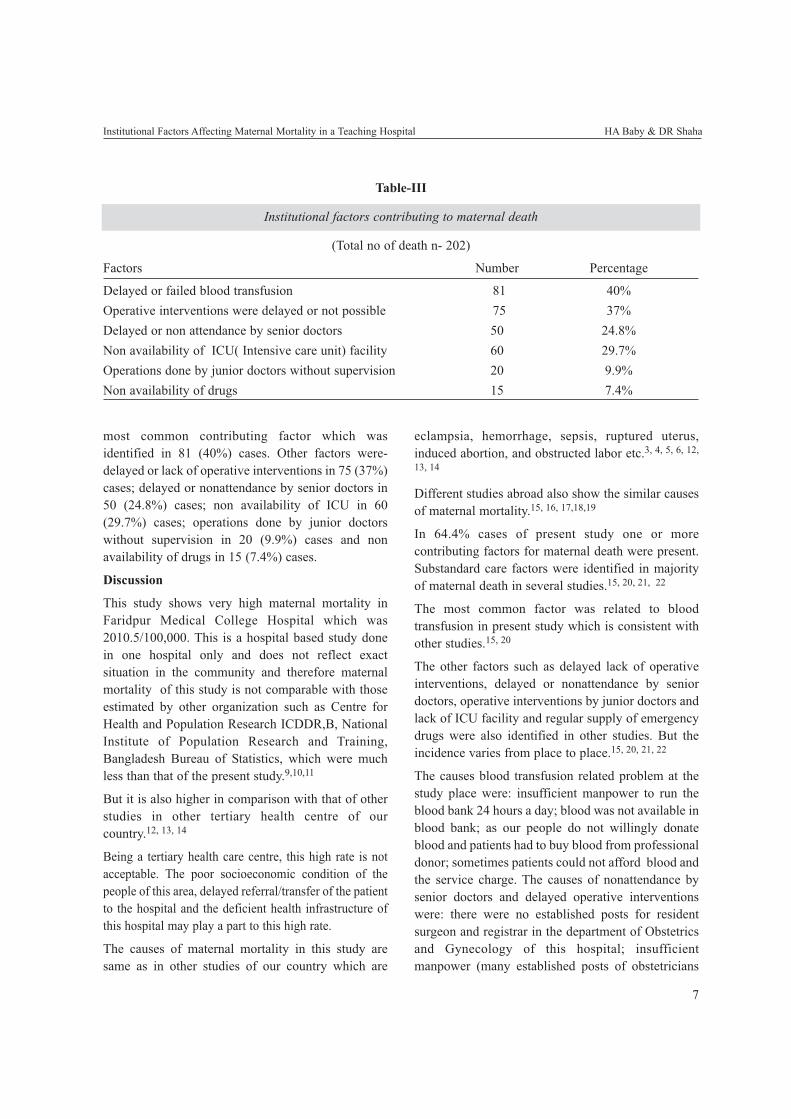
The identified institutional factors contributing tomaternal death are shown in table-III. Contributingfactors were identified in 130 (64.4%) cases ofmaternal death. In many cases more than one factorwere present. Delayed or failed blood transfusion was
Journal of Bangladesh College of Physicians and Surgeons Vol. 28, No. 1, January 2010
7
most common contributing factor which wasidentified in 81 (40%) cases. Other factors were-delayed or lack of operative interventions in 75 (37%)cases; delayed or nonattendance by senior doctors in50 (24.8%) cases; non availability of ICU in 60(29.7%) cases; operations done by junior doctorswithout supervision in 20 (9.9%) cases and nonavailability of drugs in 15 (7.4%) cases.
Discussion
This study shows very high maternal mortality inFaridpur Medical College Hospital which was2010.5/100,000. This is a hospital based study donein one hospital only and does not reflect exactsituation in the community and therefore maternalmortality of this study is not comparable with thoseestimated by other organization such as Centre forHealth and Population Research ICDDR,B, NationalInstitute of Population Research and Training,Bangladesh Bureau of Statistics, which were muchless than that of the present study.9,10,11
But it is also higher in comparison with that of otherstudies in other tertiary health centre of ourcountry.12, 13, 14
Being a tertiary health care centre, this high rate is notacceptable. The poor socioeconomic condition of thepeople of this area, delayed referral/transfer of the patientto the hospital and the deficient health infrastructure ofthis hospital may play a part to this high rate.
The causes of maternal mortality in this study aresame as in other studies of our country which are
eclampsia, hemorrhage, sepsis, ruptured uterus,induced abortion, and obstructed labor etc.3, 4, 5, 6, 12,
13, 14
Different studies abroad also show the similar causesof maternal mortality.15, 16, 17,18,19
In 64.4% cases of present study one or morecontributing factors for maternal death were present.Substandard care factors were identified in majorityof maternal death in several studies.15, 20, 21, 22
The most common factor was related to bloodtransfusion in present study which is consistent withother studies.15, 20
The other factors such as delayed lack of operativeinterventions, delayed or nonattendance by seniordoctors, operative interventions by junior doctors andlack of ICU facility and regular supply of emergencydrugs were also identified in other studies. But theincidence varies from place to place.15, 20, 21, 22
The causes blood transfusion related problem at thestudy place were: insufficient manpower to run theblood bank 24 hours a day; blood was not available inblood bank; as our people do not willingly donateblood and patients had to buy blood from professionaldonor; sometimes patients could not afford blood andthe service charge. The causes of nonattendance bysenior doctors and delayed operative interventionswere: there were no established posts for residentsurgeon and registrar in the department of Obstetricsand Gynecology of this hospital; insufficientmanpower (many established posts of obstetricians
Institutional Factors Affecting Maternal Mortality in a Teaching Hospital HA Baby & DR Shaha
Table-III
Institutional factors contributing to maternal death
(Total no of death n- 202)
Factors Number Percentage
Delayed or failed blood transfusion 81 40%Operative interventions were delayed or not possible 75 37%Delayed or non attendance by senior doctors 50 24.8%Non availability of ICU( Intensive care unit) facility 60 29.7%Operations done by junior doctors without supervision 20 9.9%Non availability of drugs 15 7.4%

8
and anesthetists remained vacant); senior doctorslived far from the hospital; nonfunctioning of telecomsystem; nonfunctioning of ambulance; privatepractice of obstetricians and anesthetists; negativeattitude and lack of responsibilities of both junior andsenior doctors.
Other factors were lack ICU facility and absence ofregular supply of emergency lifesaving medicines inthis hospital and poor patients could not bought themedicine from outside. Absence of these facilitiesmakes the management of critically ill patientdifficult and increases the incidence of maternaldeath.
This is the scenario of public health services in manyplaces of our country.
Globally an annual decline of 5.5% in maternalmortality ratio is required to achieve MDG 5, whichaims to reduce the maternal death by 75% by 2015.But the maternal mortality ratio has decreased at anaverage of less than 1% annually between 1990 and2005.1
To achieve MDG 5, improving health care for womenand providing universal access to reproductive healthservices must be prioritized. This includes access tofamily planning, prevention of unplannedpregnancies and provision of high-quality pregnancyand delivery care, including emergency obstetriccare.
Improving the health care system is undoubtedly acritical component to reduce maternal morality. Oneof the most effective methods of bringing abouthealth changes is for governments to prioritize them.Political commitment is vital to the success of variousprograms for reduction of maternal death.23
Countries such as Bolivia, Brazil China, Egypt,Morocco and Peru have made good progress towardachieving MDG-5.24
This become possible as successful programmes arebeing implemented by their government.
Bangladesh has one of the highest rates of maternalmortality in the world, and despite substantialadvances over the last two decades, it remainscomparatively high. A simple extrapolation of recenttrends indicates that this MDG will not likely to bemet. One of the most significant impediments to
better maternal health outcomes is the current state ofpublic health services.25
The present study shows the present status of one ofthe tertiary public health centre in our country.
Conclusion:Improvement of infrastructure of health centre byimplementation of successful programme can providehigh quality emergency obstetric care services. Thisis an essential element of strategies to reduce thematernal mortality in our country.
References:1. Maternal Mortality in 2005. Estimates developed by WHO,
UNICEF, UNFPA, and The World Bank. 2007.
2. Khan KS, Wojdyla, Say L, Gulmezoqlu AM, Van Look PF.WHO analysis of causes of maternal death: a systematicreview. Lancet 2006; 367(9516):1066-74.
3. Fauveau V, Koenig MA, Chakrabarty, et al. Causes ofmaternal mortality in rural Bangladesh, 1976-85. BullWorld Health Organ. 1988; 66: 643-51.
4. Khan AR, Jahan FA, Begum SF. Maternal mortality in ruralBangladesh: the Jamalpur Distric. Stud Fam Plann. 1988Jan-Feb; 17(1):7-12.
5. Akhter HA, Situation analysis of maternal health inBangladesh. Paper presented at National Conference onSafe Motherhood, Dhaka, December 1994.
6. Rahman F, Whittaker M, Hossain MB. Maternal mortality inrural Bangladesh, 1982-1990: data from verbal autopsies.Dhaka: MCH-FP Extension Project, ICDDR, B, 1993.(Working paper no. 81).
7. de Bernis L d, Dumont A, Bouillin D, Gueye A, DompnierJP, Bouvier-Colle MH. Maternal morbidity and mortality intwo different populations of Senegal: a prospective study(MOMA survey). Br J Obstet Gynecol 2000; 107: 68-74.
8. Rai N K, Dali S M. Making pregnancies safer in South-EastAsia. Regional Health Forum WHO South-East Asia Region2002 (Volume 6, No.1)
9. Mahbub-ul-Alam, Kabir H, Nowsheruddin AH, SirajuddinAKM, Ashraf A. assessment of yearly geographicalreconnaissance of the Bangladesh health and populationsector programme. Dhaka: ICDDR,B: Centre for Health andPopulation Research, 2001:28-31. (ICDDR,B workingpaper no.149.).
10. National Institute of Population Research and Training.Bangladesh maternal health services and maternal mortalitysurvey 2001. Dhaka: National Institute of PopulationResearch and Training, 2003. 234 p.
11. Bangladesh Bureau of Statistics. Report of sample vitalregistration system 2002. Dhaka: Bangladesh Bureau ofStatistics, 2004. 291 p.
Journal of Bangladesh College of Physicians and Surgeons Vol. 28, No. 1, January 2010

9
12. S Tasnim et all. Maternal Death Audit: Experience from aPeriurban Hospital. J Bangladesh Coll Phys Surg 2006; 24:5-9.
13. Sayeba A. Presentation of workshop on facility basedmaternal death review at Dhaka Medical College Hospital,2005, Dhaka.
14. Begum N. Maternal mortality in Mymenshing MedicalCollege Hospital: 1984-1988. Bangladesh J Obs Gynecol1991;6: 14-21.
15. Shah N, Khan NH. Third delay of maternal mortality in atertiary hospital. Rawl Med J 2007;32: 163-167.
16. Jafarey SN Maternal Mortaliy in Pakistan- compilation ofavailable data. J Pak Med Assoc. 2002;52:539-44.
17. Onah HE, Okaro MJ, Umeh U, Chigbu CO. MaternalMortality in health institutions with emergency obstetriccare f acilities in Enugo State, Nigeria. J Obstet Gynecol2005;25:569-74.
18. Uzoigwe SA, John CT. Maternal Mortality in the Universityof Port Harcourt Teaching Hospital, Port Harcourt in the lastyear before the new millennium. Niger J Med. 2004;13: 32-5.
19. Thonneau F, Matsudai T, Alihonou E et al. Distribution ofcauses of maternal mortality during delivery and
postpartum: results of an African multicentre hospital-basedstudy. Eur J Obstet Gynecol Reprod Biol. 2004;114:150-4.
20. EJ Udoma et al. The role of institutional factors in maternalmortality from obstructed labour. Global J Med Sci. 2003;2(1): 13-17.
21. Samuel, Hailu. Delays in Maternal Morbidity and Mortalityat facility level. Retrieved November 07, 2009 fromhttp://hdl.handle.net/123456789/993.
22. Friday E. et al. Maternal Mortality in Ile-Ife,Nigeria: AStudy of Risk factors. Studies in Family Planning1992;23(5): 319-324.
23. Nawal M. Nour. An Introduction to Maternal Mortality. RevObstet Gynecol. 2008; 1(2): 77-81.
24. The United Nations Children’s Fund (UNICEF).Countdown to 2015: Maternal, Newborn and ChildSurvival. Executive summery: Tracking Progress inMaternal, Newborn and Child Survival. The 2008 report.New York: UNICEF; 2008.
25. To the MDGs and Beyond: Accountability and InstitutionalInnovation in Bangladesh. Bangladesh Development series.Paper No: 14. The World Bank Office. Dhaka. January2007.
Institutional Factors Affecting Maternal Mortality in a Teaching Hospital HA Baby & DR Shaha
14
IntroductionHypotension after spinal anaesthesia can be so severethat without prevention or treatment it can go beyondthe limit of physiologic trespass, leading tocomplications like nausea, bradycardia, vomiting,arrhythmias or even cardiac arrest1. The incidence ofhypotension during subarachnoid block in elderlypatients ranges from 25-69%.4 The elderly are at anincreased risk of developing long term complicationsfrom hypotension because they have a reducedphysiologic reserve and an increased incidence ofsystemic disease. In adults and obstetric patients, themanagement of hypotension after subarachnoid blockis well established but it is not so in elderly patients.The preloading used to correct hypotension in theelderly has not always been shown to be effective. Inaddition, in elderly patients preloading with large fluidvolumes may be poorly tolerated resulting in fluidoverload of the various vasopressors available,ephedrine is found to be the most effective in thetreatment of hypotension. It is speculated thatephedrine is incapable of correlating the decrease in
systemic vascular resistance and since the elderly havea reduced physiological reserve they are less capableof increasing their cardiac output in response toephedrine2,3. In addition, it causes a large increase inheart rate which is detrimental in elderly individuals4.An alpha agonist like metarminol is thought to act byincreasing both systemic vascular resistance and CVP.It is capable of maintaining the systemic pressure byvenoconstriction actions. Similarly, mephenterminehas also got sympathomimatic action. It causes a risein blood pressure due to a combination of ionotropicand vasoconstrictor actions. Similarly, mephenterminehas also got sympathomimetic action. It causes a risein B.P. due to a combination of ionotropic andvasoconstrictor actions. Moreover, it is the most freelyavailable vasopressors in our set up.
Material & MethodsIt was randomized conducted on 40 ASA I and IIpatients of more than 60 years undergoing urologic/surgical procedure for approximately 1 hour undersubarachnoid block. All the patients were clinicallyexamined for any other medical illness andinvestigated preoperatively. The purpose of the study,details regarding regional anaesthesia was explainedto the patients and informed consent for the procedurewas obtained. The patients were randomly dividedinto two groups.
Group I Received injection ephedrine 10 mg bolusintravenously ( 0.2 mg/kg) followed by infusion 0.6mg/kg/hr(30 mg/hr).
Journal of Bangladesh College of Physicians and SurgeonsVol. 28, No. 1, January 2010
Comparative Study of Ephedrine and Mephertermine inTreatment of Hypotension in Patients Undergoing
Elective Trans Urethral Resection Prostate (TURP)N PURIa, A TALWARb
Summary:The present study was carried out on forty ASA I and IIpatients undergoing elective trans urethral resection ofbladder tumour and ICA implant for carcinoma cervixunder subarachnoid block. The patients were randomlydivided into two groups each consisting of 20 patients.Vasopressors were used when the systolic blood pressuredecreased by 25% pressure of the baseline or less than 90mm Hg after subarachnoid block.Group I received
injection Ephedrine 10 mg bolus and immediately aninfusion was started at the rate of 30 mg/hr. group IIpatients received injection Mephentermine intravenous 10mg followed by an infusion of 60 mg/hr. The clinicalparameters observed during the procedure weremeasurement of heart rate, systolic/diastolic and meanblood pressure and CVP. The two groups were statisticallycompared with respect to the above parameters.
(J Bangladesh Coll Phys Surg 2010; 28: 10-16)
a. Dr Neerja Puri, Registrar Anaesthesia
b. Dr Ashutsoh Talwar, Assistant Professor Surgery
Department of Anaesthesia & Surgery, G.G.S. Medical College &Hospital, Faridkot. 151203. Punjab.
Address of Correspondence: Dr Neerja Puri, # 626, Phase II,Urban Estate, Dugri Road, Ludhiana, Punjab. India, Email : [email protected], Cell : 09814616427
Received: 16 July, 2008 Accepted: 7 September, 2009
11
Group II Received injection mephentermine 10 mgbolus followed by 1 mg/min or 60 mg/hr infusion.
Exclusion Criteria
The following patients were excluded from our study:
1. Patients with severe cardiac or respiratorydiseases like ILD and uncontrolled diabetesmellitus.
2. Patients with abnormal cardiac anatomy likevalvular heart disease , dilated cardiomyopathy.
3. Patients with heart rhythm other than sinusrhythm.
4. Patients receiving medication which have directcardiac effect eg Beta blockers, vasodilators,antihypertensives.
5. Patients with haemoglobin less than 10 gram%.
6. Patients having contraindication to subarachnoidblock.
All patients were fasting since twelve midnightbefore the day of surgery. For Premedication theyreceived tablet Daizepam 5 mg at bedtime and 5 mgon the morning of surgery. On the operating table acental venous pressure monitoring catheter waspassed through antecubital vein under localanaesthesia, taking all aseptic precautions. Beforegiving the block HR, BP (Systolic, diastolic andmean) and CVP were measured and they were takenas preblock values.
Subarachnoid block was given in the lateral positionat L2-3 or L3-4 space with a 25 G spinal needle using2.5 ml of 0.5% heavy bupivacaine. Soon after givingthe drug in suarachnoid space patients position waschanged from lateral to supine and patients stayed inthe position till the end of surgery. Fluids wereadministered as 4 ml/kg/hr of normal saline.thevasopressors were administered when systolic arterialpressure dropped to more than 25% of the baseline orless than 90 mm Hg systolic blood pressure. Thevasopressors were given first as intravenous bolusand then immediately an infusion of either ephedrineor mephenteramine was started. The variousparameters which were monitored during theprocedure were :
� ECG lead II for HR and rhythm.
� NIBP every 2 min for first 15 min and then every5 min for 30 min.
� CVP every 15 min.
� Level of block was determined by pin prickmethod every 2 min upto 15 min.
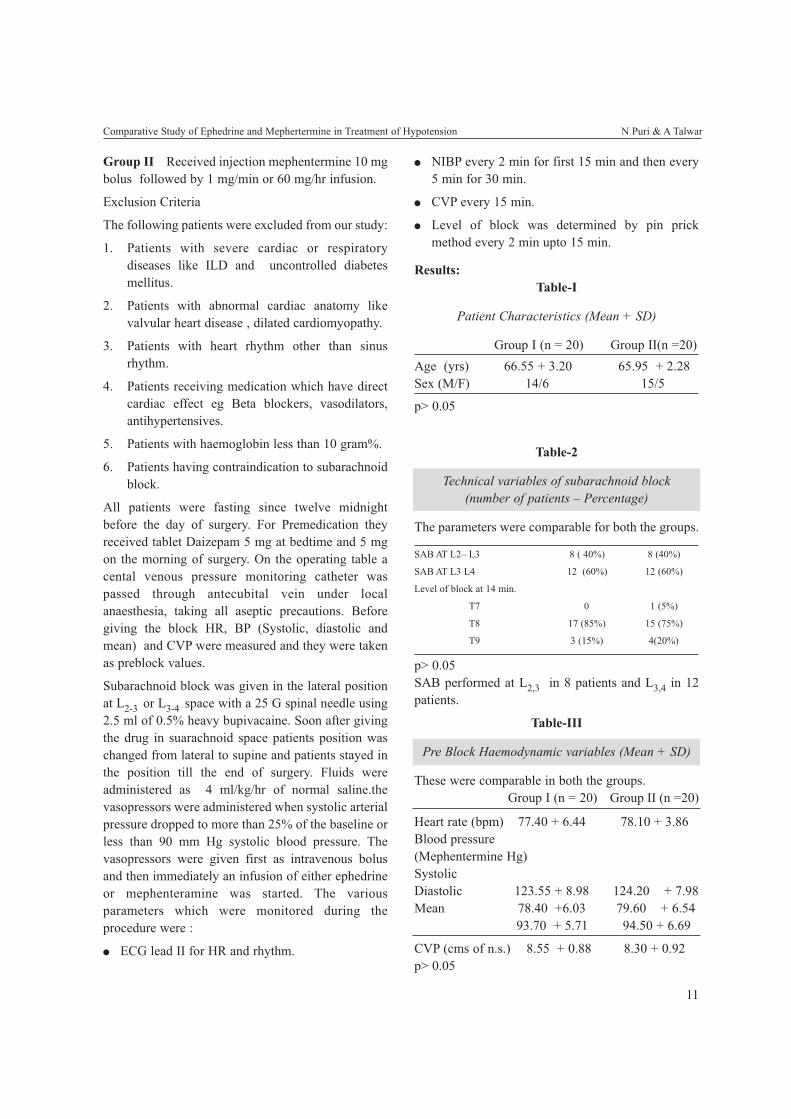
Results:Table-I
Patient Characteristics (Mean + SD)
Group I (n = 20) Group II(n =20)Age (yrs) 66.55 + 3.20 65.95 + 2.28Sex (M/F) 14/6 15/5
p> 0.05
Table-2
Technical variables of subarachnoid block(number of patients – Percentage)
The parameters were comparable for both the groups.
SAB AT L2– L3 8 ( 40%) 8 (40%)
SAB AT L3 L4 12 (60%) 12 (60%)
Level of block at 14 min.
T7 0 1 (5%)
T8 17 (85%) 15 (75%)
T9 3 (15%) 4(20%)
p> 0.05SAB performed at L2,3 in 8 patients and L3,4 in 12patients.
Table-III
Pre Block Haemodynamic variables (Mean + SD)
These were comparable in both the groups.Group I (n = 20) Group II (n =20)
Heart rate (bpm) 77.40 + 6.44 78.10 + 3.86Blood pressure(Mephentermine Hg)SystolicDiastolic 123.55 + 8.98 124.20 + 7.98Mean 78.40 +6.03 79.60 + 6.54
93.70 + 5.71 94.50 + 6.69
CVP (cms of n.s.) 8.55 + 0.88 8.30 + 0.92p> 0.05
Comparative Study of Ephedrine and Mephertermine in Treatment of Hypotension N Puri & A Talwar
12
Journal of Bangladesh College of Physicians and Surgeons Vol. 28, No. 1, January 2010
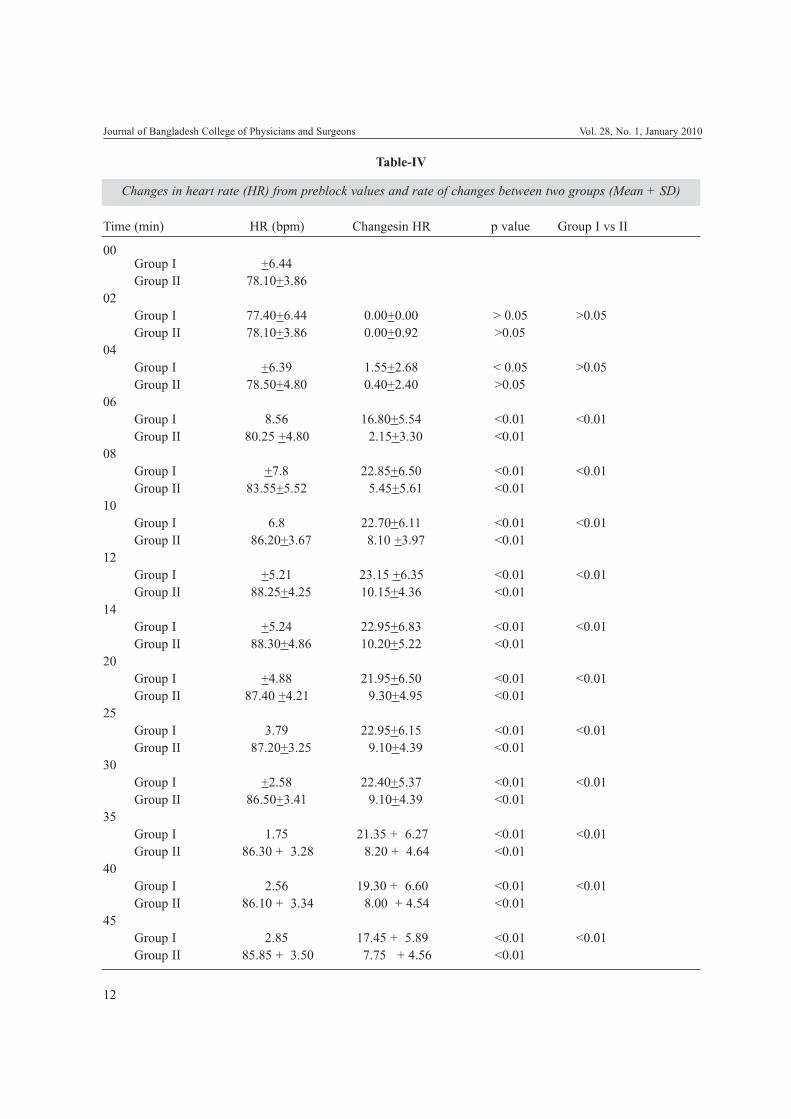
Table-IV
Changes in heart rate (HR) from preblock values and rate of changes between two groups (Mean + SD)
Time (min) HR (bpm) Changesin HR p value Group I vs II
00Group I +6.44Group II 78.10+3.86
02Group I 77.40+6.44 0.00+0.00 > 0.05 >0.05Group II 78.10+3.86 0.00+0.92 >0.05
04Group I +6.39 1.55+2.68 < 0.05 >0.05Group II 78.50+4.80 0.40+2.40 >0.05
06Group I 8.56 16.80+5.54 <0.01 <0.01Group II 80.25 +4.80 2.15+3.30 <0.01
08Group I +7.8 22.85+6.50 <0.01 <0.01Group II 83.55+5.52 5.45+5.61 <0.01
10Group I 6.8 22.70+6.11 <0.01 <0.01Group II 86.20+3.67 8.10 +3.97 <0.01
12Group I +5.21 23.15 +6.35 <0.01 <0.01Group II 88.25+4.25 10.15+4.36 <0.01
14Group I +5.24 22.95+6.83 <0.01 <0.01Group II 88.30+4.86 10.20+5.22 <0.01
20Group I +4.88 21.95+6.50 <0.01 <0.01Group II 87.40 +4.21 9.30+4.95 <0.01
25Group I 3.79 22.95+6.15 <0.01 <0.01Group II 87.20+3.25 9.10+4.39 <0.01
30Group I +2.58 22.40+5.37 <0.01 <0.01Group II 86.50+3.41 9.10+4.39 <0.01
35Group I 1.75 21.35 + 6.27 <0.01 <0.01Group II 86.30 + 3.28 8.20 + 4.64 <0.01
40Group I 2.56 19.30 + 6.60 <0.01 <0.01Group II 86.10 + 3.34 8.00 + 4.54 <0.01
45Group I 2.85 17.45 + 5.89 <0.01 <0.01Group II 85.85 + 3.50 7.75 + 4.56 <0.01
13
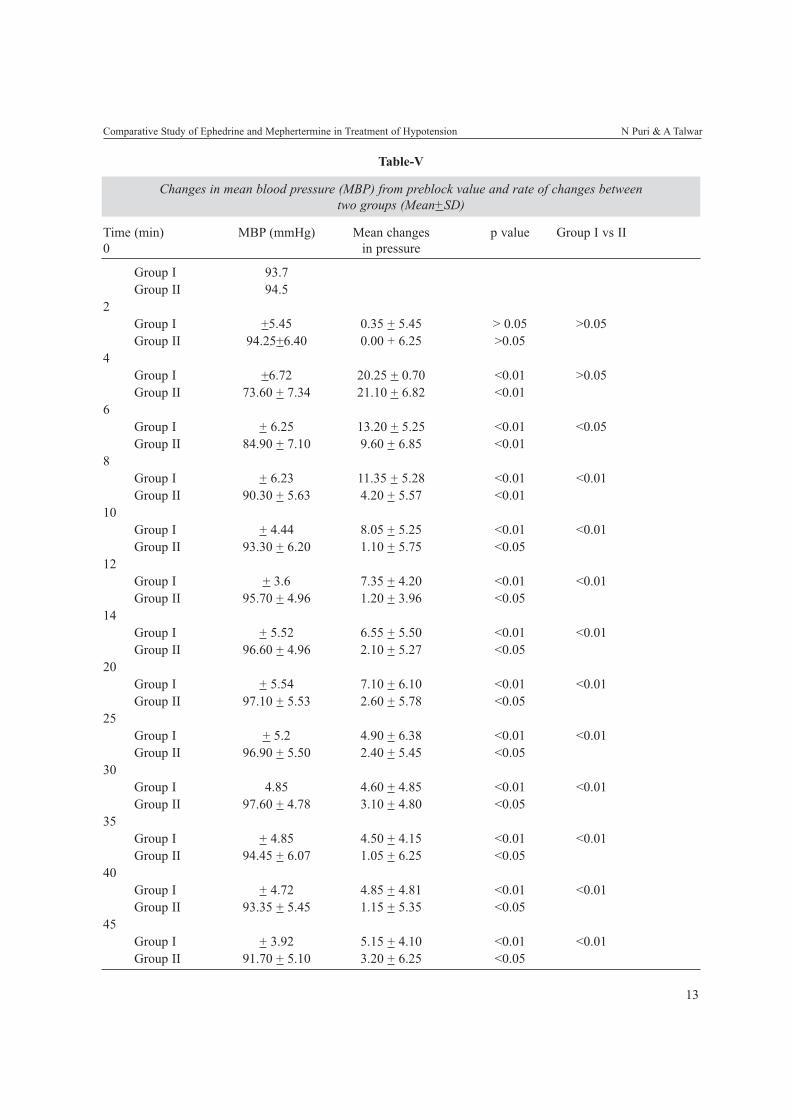
Table-V
Changes in mean blood pressure (MBP) from preblock value and rate of changes betweentwo groups (Mean+SD)
Time (min) MBP (mmHg) Mean changes p value Group I vs II0 in pressure
Group I 93.7Group II 94.5
2Group I +5.45 0.35 + 5.45 > 0.05 >0.05Group II 94.25+6.40 0.00 + 6.25 >0.05
4Group I +6.72 20.25 + 0.70 <0.01 >0.05Group II 73.60 + 7.34 21.10 + 6.82 <0.01
6Group I + 6.25 13.20 + 5.25 <0.01 <0.05Group II 84.90 + 7.10 9.60 + 6.85 <0.01
8Group I + 6.23 11.35 + 5.28 <0.01 <0.01Group II 90.30 + 5.63 4.20 + 5.57 <0.01
10Group I + 4.44 8.05 + 5.25 <0.01 <0.01Group II 93.30 + 6.20 1.10 + 5.75 <0.05
12Group I + 3.6 7.35 + 4.20 <0.01 <0.01Group II 95.70 + 4.96 1.20 + 3.96 <0.05
14Group I + 5.52 6.55 + 5.50 <0.01 <0.01Group II 96.60 + 4.96 2.10 + 5.27 <0.05
20Group I + 5.54 7.10 + 6.10 <0.01 <0.01Group II 97.10 + 5.53 2.60 + 5.78 <0.05
25Group I + 5.2 4.90 + 6.38 <0.01 <0.01Group II 96.90 + 5.50 2.40 + 5.45 <0.05
30Group I 4.85 4.60 + 4.85 <0.01 <0.01Group II 97.60 + 4.78 3.10 + 4.80 <0.05
35Group I + 4.85 4.50 + 4.15 <0.01 <0.01Group II 94.45 + 6.07 1.05 + 6.25 <0.05
40Group I + 4.72 4.85 + 4.81 <0.01 <0.01Group II 93.35 + 5.45 1.15 + 5.35 <0.05
45Group I + 3.92 5.15 + 4.10 <0.01 <0.01Group II 91.70 + 5.10 3.20 + 6.25 <0.05
Comparative Study of Ephedrine and Mephertermine in Treatment of Hypotension N Puri & A Talwar
14
DiscussionIt is seen that metarminol is better than ephedrine atmaintaining systolic arterial pressure in elderlypersons. Ephedrine is used in obstetric patients as ithas been found to be useful because it interferes verylittle with uterine blood flow 5,6.Ephedrine is analkaloid obtained from ephedra vulgaris.It resemblesephedrine except OH groups are missing frombenzene ring and methyl group is attached to thenitrogen atom. It is abase which forms salts withvarious acids most common sulphate. It is colourlessbut gradually decomposes on exposure to light. Itprimarily acts indirectly but has some direct actionson α and beta receptors. It stimulates the heart rateand cardiac output and variably increases theperipheral resistance. As a result ephedrine usuallyincreases the blood pressure. However, one of thedisadvantages of ephedrine is its failure to correct thedecreases in systemic vascular resistance. Stimulationof the alpha adrenergic receptors of smooth musclecell in the bladder base may increase the resistance tothe outflow of urine. Activation of beta adrenergicreceptors in the lungs promotes bronchodilatation. Itcrosses the blood brain barrier and has a stimulantaction on the brain. In the past ephedrine was used totreat stokes Adams attack with complete heart block
and as a central nervous system stimulant innarcolepsy and the depressive states. It has beenreplaced by alternate modes of treatment in each ofthese disorders. In addition its use as a bronchodilatorin patients with asthma has become less extensivewith the development of beta -2 agonists. Ephedrinehas been used to treat the hypotension that may occurwith spinal anaesthesia. Untoward effects ofephedrine include the risk of hypertension andcardiac arrythmias, particularly after parentraladministration7,8,9,10. Ephedrine is eliminated in urinelargely as unchanged drug with a half life of aboutthree to five hours. The various routes ofadministration of ephedrine are oral, subcutaneous,intramuscular and intravenous route.
Mephentermine has a weak alpha receptor activitybut strong beta receptor activity. It rises bloodpressure mainly by augmenting cardiac output. It alsodilates the coronary, cerebral, splanchnic and renalblood vessels. This effect of mephentermine has anadded advantage in the elderly individuals 11,12,13.Absence of bradycardia, absence of overshootresponse and sustained action were other advantagesof mephentermine14.
Mephentermine is a noncatecholamine sypathomimeticamine. It has 2 methyl groups on nitrogen bearing
Journal of Bangladesh College of Physicians and Surgeons Vol. 28, No. 1, January 2010
Table-VI
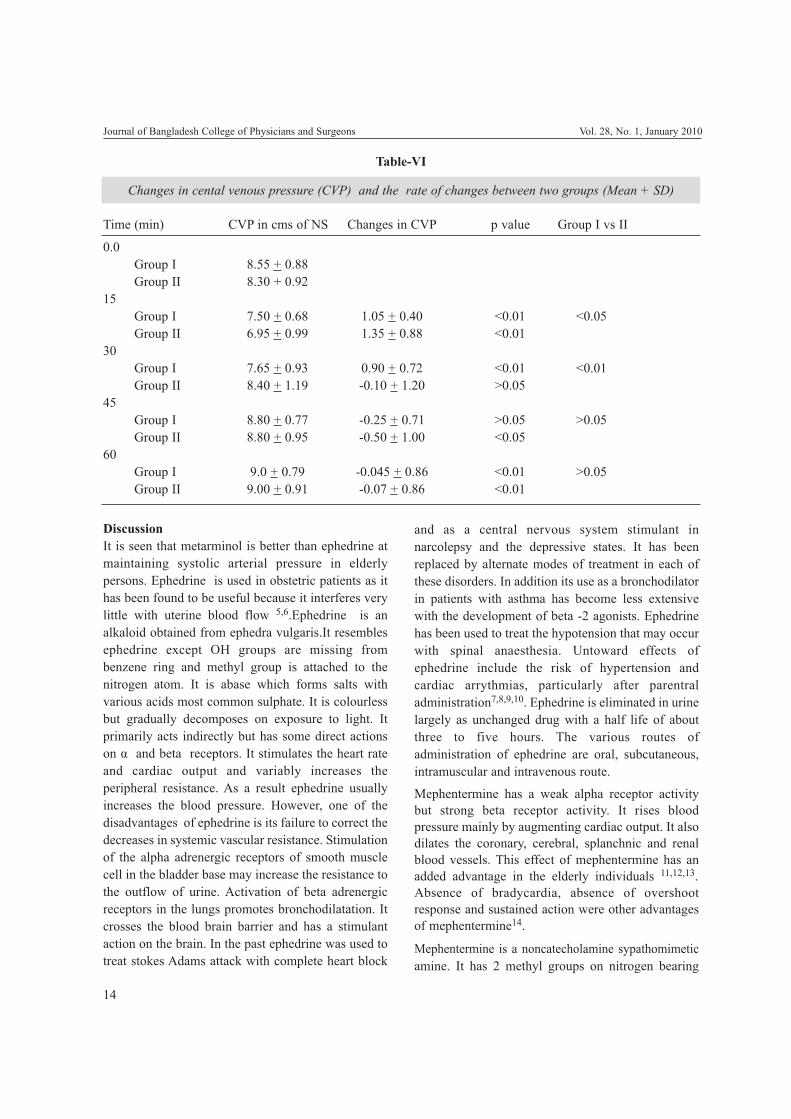
Changes in cental venous pressure (CVP) and the rate of changes between two groups (Mean + SD)
Time (min) CVP in cms of NS Changes in CVP p value Group I vs II
0.0Group I 8.55 + 0.88Group II 8.30 + 0.92
15Group I 7.50 + 0.68 1.05 + 0.40 <0.01 <0.05Group II 6.95 + 0.99 1.35 + 0.88 <0.01
30Group I 7.65 + 0.93 0.90 + 0.72 <0.01 <0.01Group II 8.40 + 1.19 -0.10 + 1.20 >0.05
45Group I 8.80 + 0.77 -0.25 + 0.71 >0.05 >0.05Group II 8.80 + 0.95 -0.50 + 1.00 <0.05
60Group I 9.0 + 0.79 -0.045 + 0.86 <0.01 >0.05Group II 9.00 + 0.91 -0.07 + 0.86 <0.01

15
carbon. It is base which forms salts with variousacids. It is available as a solution of mephenteraminesulphate for parental administration15. Chemically, itresembles sympathomimatic amines such asamphetamine and desoxyephedrine. It has got asypathomimetic action. It has a combination ofionotropic and vasoconstrictor actions.Mephentermine has a weak alpha receptor activitybut strong beta receptor activity. It increases the bloodpressure by augmenting the cardiac output. It has adilating effect on the coronary, cerebral , splanchnicand renal blood vessels. Adverse effects are related tocentral nervous system stimulation, hypertension andarrythmias. The change in heart rate is variabledepending on the degree of vagal tone. It is used toprevent hypotension which accompanies spinalanaesthesia 16,17.
Studies on elderly individuals have shown that theyhave depleted catecholamine stores and ephedrinewhich acts mainly by release of noradrenaline couldnot be a better choice than mephentermine. so, weconducted a comparative study between these twovasopressors to decide which would be moreeffective, in treating hypotension after subarachnoidblock in elderly individuals.
Heart Rate:Patients in both the groups showed a statisticallysignificant rise in heart rate from 4th minute(p < 0.05)and 6th minute(p < 0.01) respectively and this risepersisted upto 45 minutes (p < 0.01). the rise in heartrate was significantly greater in group I as comparedto group II at all time intervals.
Mephentermine has been found to cause reflexslowing of heart rate when used in larger doses of 10to 20 mg. in our study, mephentermine group showeda rise in heart rate using a bolus of 10 mg followed byan infusion of 1 mg/ min. the probable reason forincreased heart rate by mephentermine in our studymay be related to the rise of bolus dose followed byinfusion since vagal slowing has been seen only withbolus doses.
Also the bolus dose of mephentermine used in ourstudy was on the lower side. Slowing of heart rate hasnot been documented by mephentermine in our studybecause the bolus dose of mephentermine was on thelower side.
Blood Pressure :There was significant fall in blood pressure frombaseline in both the groups. In our study, the delay thedelay in fall in blood pressure in fluid group is relatedto the initial rise in CVP which is sufficient tocounteract the venodilatation resulting fromsubarachnoid block. In the metarminol group systolicblood pressure was maintained in all patients and itwas greater than fluid group 15 minutes afterinduction. The systolic arterial pressure returned tobaseline by 15 minutes.
Central Venous Pressure (CVP) :In both groups I & II, the CVP dropped from baselinevalue 15 mins after subarachnoid block. After 30mins, the CVP was comparable to the baseline ingroup II whereas it was still low in group I. beyond 30mins the CVP was comparable to the baseline in boththe groups. The low CVP in group I upto 30 mins mayexplain the inability of ephedrine to maintain BPcomparable to baseline.
ConclusionsThe following conclusions were drawn from thepresent study.
1. There was a statistically significant rise in heartrate from the baseline at 4th minute in Group Iand at 6th minute inGroup II which persisted uptothe 45th minute of the study but the rise in heartrate in Group I was significantly grater thanGroup II at all time intervals.
2. There was arise in systolic blood pressure in bothGroup I and Group II after the start ofvasopressors but the rise in systolic blood pressurewas more in Group II as compared to Group I.similarly, it was observed that diastolic bloodpressure and mean blood pressure was bettercontrolled in Group II (Mephentermine group)and the blood pressure came close to the baselineearlier in Group II as compared to Group I.
3. The drop in CVP was significantly more in groupII than group I but it came closer to baselineearlier in group II patients as compared to thepatients of group I. Therefore, in conclusion,though both ephedrine and mephentermine areeffective in treatment of spinal hypertension ofelderly patients, but, mephentermine gives betterhaemodynamics and stability than ephedrine.
Comparative Study of Ephedrine and Mephertermine in Treatment of Hypotension N Puri & A Talwar

16
References1. Greene N.M. Physiology of Spinal anaesthesia. Fourth
edition. Baltimore : Williams & Wilkins, 1981 : VII –IX,134-200.
2. Bruch CJ, Harrison RT. The effect of spinal anaesthesia onthe cardiac output. Arch. Surg 1950 ; 21 : 330-32.
3. Smith HW, Rovenstine EA, Goldring, Chasis H, RangesHA. The effect of spinal anaesthesia on the circulation innormal, unoperated man with reference to the autonomy ofthe arterioles and especially those of the renal circulation.J.clin.invest 1959 : 18 : 319-339.
4. Critchley LAH. Hypotension subarachnoid block and theelderly. Br J anaesth 1996; 1139-43.
5. Kang VG, Caritis S. Prophylactic intravenous ephedrineinfusion during spinal anaesthesia for caesareansection.Anaesth Analg 1982; 61 : 839-42.
6. Critchley LAH, Stuart J, Conway F. Hypotension duringsubarachnoid anaesthesia: Haemodynamic effects ofephedrine. Br.J.Anaesth 1995,74 : 373-8.
7. Carpenter RL, Caplan RA, Brown DL, Slephenson RN,WuR. Incidence and risk factors for side effects of spinalanaesthesia.Anaesthesiology 1992 ; 76 : 906-916.
8. Owen H, Cousins MJ. Subarachnoid and extraduralanaesthesia. Anaesthesia, second volume, edited by WalterS. Nimino and Graham Smith. 1990 ; 2 : 1034-70.
9. Reynolds RJM Spinal and Epidural block. A practice ofanaesthesia, 5th edition ed by Wylie and Churchill
Davidson. HE PG publishing Pvt Ltd., New Delhi 1984,856-92.
10. Echenhoff JE, Hafkenshiel JH, Fultz. Influence ofhypotension on coronary blood flow, cardiac work andcardiac efficacy. AMJ Physiol 1984 ; 152 : 545-553.
11. McCrae AF Wild Smith J. Prevention and treatment ofhypotension during central neural block. Br. J. Anaesth1993, 70: 672-80.
12. Malmquist LA, Bengisson M. Sympathetic activity andHaemodynamic variables during spinal analgesia in man.Acta Anaesth Scand 1987 ; 31 : 467-73.
13. Coe AJ. Is crystalloid preloading useful in spinalanaesthesia in elderly ? Anaesthesia 1990 ; 45 : 241-3.
14. Buggy D, Higgins P. Prevention of spinal anaesthesiainduced hypotension in the elderly. Comparison betweenpreanaesthetic administration of cyrstalloids, colloids andnoprehydration. Anaesth Analg 1997 ; 84 : 106-10.
15. Critchley LAH, Short T, Gin T. Hypotension duringsubarachnoid anaesthesia. Haemodynamic analysis of threetreatments. Br J. Anaesth 1994 ; 72 . 151 -5.
16. Critchley LAH, Conway F. Hypotension duringsubarachnoid anaesthesia. Effects of colloids andmetarminol. Br J. Anaesth 1996 ; 76 . 734 -6.
17. Myres CR, Mathews TP, Jenicek JA. Clinical response toselected vasopressors during spinal anaesthesia. A. M.Pract, Dig. Treat, 1961; 12 : 828.
Journal of Bangladesh College of Physicians and Surgeons Vol. 28, No. 1, January 2010
Introduction:Premature rupture of the membrane (PROM) is acommon obstetric problem and the assessment ofwomen with possible membrane rupture is amanagement issue faced in every day practice. WhenPROM occurs, the fetus loses relative isolation &protection offered within the amniotic cavity. Ingeneral PROM refers to rupture of membranes withleakage of amniotic fluid in the absence of uterineactivity. The minimum latency for diagnosis of
PROM is 1 hour. PROM occurs in approximately 8%of term pregnancy 1. Under normal circumstances thefetal membrane ruptures during the active phase oflabor.2 When PROM occurs before 37 completedweeks, it is called preterm pre labor rupture of themembrane (PPROM). It is responsible forapproximately 35% of all preterm delivery 3. .PROMaffects 2.7% to 17% of all pregnancies and in mostcases happens spontaneously and without apparentcause 3. PPROM complicates approximately 2%-3%of all pregnancies below 37 weeks gestation1.Incidence of preterm PROM in Bangladesh is notknown but Incidence of PROM in Dhaka MedicalCollege Hospital is 8.12% 4 and 1.94% at HolyFamily Red Crescent Hospital 5. Epidemiologicalstudies have identified several risk factors associatedwith preterm PROM. Genital tract infection orcolonization with various microorganisms, lowsocioeconomic condition, poor nutrition, anemia,
Journal of Bangladesh College of Physicians and SurgeonsVol. 28, No. 1, January 2010
Preterm Prelabour Rupture of the Membrane &Feto-Maternal out come: an Observational Study
S AKTERa, R AKTHERb, M RASHIDa
Summary:Objective: The aim of this study was to see the maternaland fetal outcome of preterm pre labor rupture membraneand to identify the risk factors for preterm pre laborrupture membrane.
Methods and Material: This was a cross-sectionaldescriptive type study carried out in Dhaka MedicalCollege Hospital, Dhaka, during April to September, 2005(6months) in the Department of Obstetric andGynecology. 50 pregnant women with preterm prematurerupture of the membrane (gestational age 29-0 to 36-6weeks) were included in this study.
Results: The mean age of the women was 27.24±6.28yearsand 36% of them more than 30 years old. Sixty twopercent women were multi gravid .Socio-economiccondition, level of education and antenatal care of thewomen was low. Median gestational age of the patient was35weeks. Fifty six percent had previous history of PROM,preterm delivery, abortion, MR and dilatation andcurettage. Sixty two percent women had history of sexualactivity between 2 to 7days. Seventy two percent women
had UTI, anaemia, and lower genital tract infection.Mean duration of the latent period was 18.87 ±16.17hoursand time interval of rupture membrane and delivery was27.60 ± 21.127 hours. Eighty four percent patientdelivered by vaginal route and Fifty four percent deliveredwithin 24 hours of ruptured membrane .Forty two percentnewborn suffered from neonatal asphyxia, respiratorydistress syndrome, neonatal jaundice and neonatal sepsis.Thirty two percent women suffered fromchorioamnionitis, abruptio placent and endometritis.
Conclusion: PPROM is malnutrition and poverty relateddisease .Antenatal care is an important tool to preventPPROM by identifying the risk factors and itsmanagement. Steroid for fetal lung maturity, antibiotics toprevent fetal and maternal infection and induction and /or augmentation of labor will speeded delivery and reducehospital stay and infection.
Key wards: Premature rupture of the membrane,maternal and neonatal outcome, risk factors.
(J Bangladesh Coll Phys Surg 2010; 28: 17-23)
a. Dr. Shaida Akter, FCPS, Prof. Maliha Rashid, FCPS, DhakaMedical Collage Hospital, Dhaka, Bangladesh
b. Dr. Rabeya Akther, FCPS, Bangladesh Bank Medical Center,Dhaka, Bangladesh
Address of Correspondence: Address of Correspondence: Dr.Rabeya Akther Fellow no: 1996(Obstetric & Gynaecology),Assistant Chief Medical Officer, Bangladesh Bank Medical Center,Motijheel, Dhaka, Bangladesh, Email: [email protected]
Received: 6 November, 200 Accepted: 2 June, 2009

18
poor hygiene, stress, high parity, smoking and antepartum hemorrhage have all been linked to anincreased chance of preterm PROM. Education playsa significant role in reducing the risk of PROMespecially in developing countries 6. Pretermpremature rupture of the membrane is important forboth baby and mother. The survival rate of infants isdirectly related to their gestational age 1.There arenumerous possible fetal consequences of pretermdelivery due to PROM. There are respiratory distresssyndrome, hypothermia, hypoglycemia, jaundice,necrotizing enterocolitis, intraventricular hemorrhage,neurologic impairment, apnea, retrolentalfibroplasias, bronchopulmpnary dysplasia, patentductus arteriosus, fetal limb contracture formation,pulmonary hypoplasia and neonatal sepsis dependingupon gestational age. PROM causes 20% of allneonatal death 3. Probable maternal complicationsare chorioamnionitis (3-30%), endometritis, abruptioplacenta 1,2 .Recurrence of PROM may occur in20% cases.1
Aims and Objectives:PROM is very common in the obstetric wards. Weface problem in diagnosis, monitoring and adoptingtreatment policy. There were very limited studiesabout PROM in our country and no national statisticsis available about the incidence of PROM orincidence of maternal and perinatal mortality andmorbidity from PROM.
The aim of this study is to see the maternal and fetaloutcome of preterm premature rupture of themembrane in preterm labor and to identify the riskfactors for preterm PROM. It will give an opportunityto analyze the magnitude of problems caused byPROM.
Materials and Methods:This is a cross-sectional descriptive type study, donein the Department of Obstetrics and Gynecology inDhaka Medical College Hospital, Dhaka Bangladesh,from April 2005 to September 2005 (6months). Fiftypregnant women with preterm pre labor rupture of themembrane were recruited from the inpatient of thelabor ward of DMCH. Both primi and multi gravidwomen ,who consented to participate in this study,whose pregnancy duration 28 to 36 weeks 6 days
,with spontaneous rupture of the membrane ,not inactive labor were included in this study. Women withpregnancy 37completed weeks, with establishedlabor, with ante partum hemorrhage and withinfection were excluded from the study
After admission, full history including duration ofpregnancy, time and onset of rupture of membranes,past history of rupture of membranes, past obstetrichistory was taken. Rupture of the membrane wasdiagnosed by history of a gush of fluid from thevagina or continued leakage of fluid from the vaginaand demonstration of membranes rupture has to bemade by a sterile speculum examination visualizingflow of amniotic fluid from the cervical os and / or it’spooling in posterior vaginal fornix spontaneously orby fundal pressure and demonstrating alkaline PH ofvaginal fluid by litmus paper. During speculumexamination high vaginal swab was collected forculture and sensitivity and cervical dilatation andeffacement was assessed at the same time.Gestational age was determined from LMP and fromearly USG scan. Pregnancy of more than 28 weeksduration was included in this study to avoid theconflict of abortion.
Plan of management was decided on gestational age,cervical condition, latent period, presentation of thefetus, symptoms and signs of infection. All patientsreceived a single course of dexamethasone consistingof two 12.5 mg I/M injection 12 hourly afteradmission. Few patients who showed uterinecontraction short term tocolysis was given in order toallowed steroid therapy which can produce maximaleffect on pulmonary maturation. Fetal surveillancewas checked by daily fetal kick count andauscultation of fetal heart sound 4 hourly. All patientsreceived prophylactic antibiotic for 7 days afteradmission. Inj. Ampicillin / Cephradin 500mg I/V 6hourly for 48 hours, then this regimen was changed tooral form. This antibiotic was continued for sevendays if patient remain undelivered. Maternalmonitoring to detect the sign of chorioamnionitiswas done by recording of pulse, blood pressure,temperature, fundal height, abdominal tenderness,color and smell of liquor and fetal conditions fourhourly. Patients with features of chorioamnionitiswhich included maternal temperature above 1000F,maternal tachycardia, fetal tachycardia (fetal heartrate>160 beat/minute), uterine tenderness, foul
Journal of Bangladesh College of Physicians and Surgeons Vol. 28, No. 1, January 2010
19
smelled vaginal discharge and maternal leucocytosis(>16000/µL) was taken as the indication oftermination of pregnancy. Patients with features ofchorioamnionitis were given broad spectrumantibiotics in parental route during labor. Antibioticwas given to the baby after delivery in such cases. Allthe neonates were referred to neonatal ward forfurther management according to the hospitalprotocol. Without chorioamnionitis, a conservativeapproach was taken, advice for bed rest withbathroom facilities, to wear a sterile pad which wasinspected every four hourly to detect any change ofcolor of liquor and also to document amount of loss.If patient developed signs and symptoms of infectionor conservative approach failed then pregnancy wasterminated by induction, augmentation or caesariansection. The labor was induced with misoprostol oraugmented with oxytocin drip if there was no
contraindication or underwent caesarean section.Data were collected by standard questionnaire fromthe allocated patients. All data was checked andedited after collection. Then data was entered intocomputer and analyzed with the help of SPSS win12software programme.
Results:
The main objective of the study was to find out thematernal and fetal outcome in preterm prematurerupture of the membrane (PPROM) in respect of age,parity, antenatal care, educational background,nutrition, socio-economic condition, and occupation.The findings of the study are presented here.
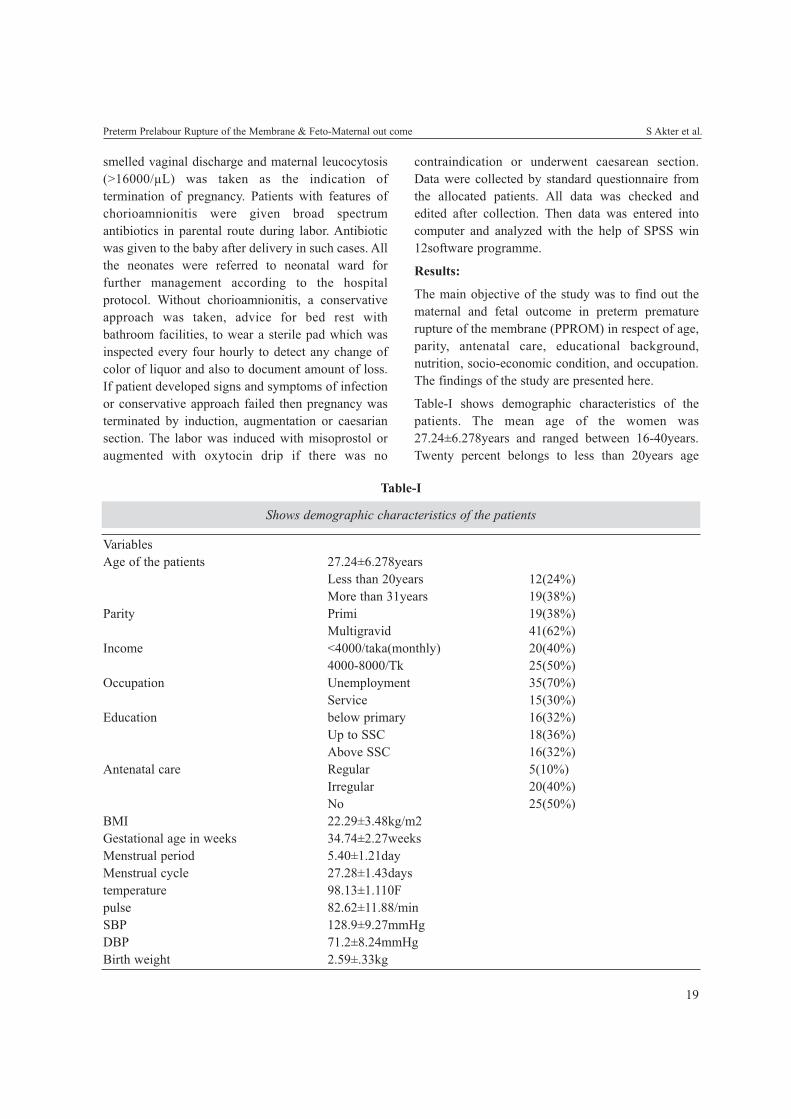
Table-I shows demographic characteristics of thepatients. The mean age of the women was27.24±6.278years and ranged between 16-40years.Twenty percent belongs to less than 20years age
Preterm Prelabour Rupture of the Membrane & Feto-Maternal out come S Akter et al.
Table-I
Shows demographic characteristics of the patients
VariablesAge of the patients 27.24±6.278years
Less than 20years 12(24%)More than 31years 19(38%)
Parity Primi 19(38%)Multigravid 41(62%)
Income <4000/taka(monthly) 20(40%)4000-8000/Tk 25(50%)
Occupation Unemployment 35(70%)Service 15(30%)
Education below primary 16(32%)Up to SSC 18(36%)Above SSC 16(32%)
Antenatal care Regular 5(10%)Irregular 20(40%)No 25(50%)
BMI 22.29±3.48kg/m2Gestational age in weeks 34.74±2.27weeksMenstrual period 5.40±1.21dayMenstrual cycle 27.28±1.43daystemperature 98.13±1.110Fpulse 82.62±11.88/minSBP 128.9±9.27mmHgDBP 71.2±8.24mmHgBirth weight 2.59±.33kg

20
group and 36% more than 31 years age group. Meanbody mass index is 22.29kg /m2. Sixty two percentwomen were multigravida where as 38% were primigravida. Ninty percent women had monthly income ≤4000-8000/ taka. Thirty four (68%) respondents wereeducated up to SSC level and remaining 16(32%)women educated up to degree level.Sixty two percent (31) patients were house wife and22% (11) were service holder. Fifty percent (25) ofthe patients had no antenatal care and 40% hadirregular and 10%had regular antenatal care. Meangestational age of the patient was 34.74weeks with astandard deviation of ±2.266weeks. Mediangestational age of the patient was 35weeks with arange from 29-0 to 36-6 weeks. This table also shownthe mean temperature, pulse and blood pressure were98.130F,82.62/min and 128/71mmHg respectively.Table-II shows distribution of women according totheir gestational age. 66% (33) respondents were nearterm, 24% (12) were between 32 to 34 gestationalweeks and 5(10%) were less than 33 weeks.
Table-II
Shows distribution of respondents accordingto their gestational age
Gestational age(week) Frequency29-0 to 31+6 5(10%)32-0 to 34+6 12(24%)35-0 to 36+6 33(66%)Total 50(100%)
Table-III shows, 20 %( 10) women had previoushistory of abortion, 14% (7) had previous history ofPROM, 10% (5) had previous history of pretermdelivery due to PROM, 8% (4) had history of MR and4% had history of D&C.
Table-III
Shows distribution of obstetric and gynecologichistory of the respondents
Variables FrequencyHistory of abortion 10(20%)History of PROM 7(14%)History of preterm delivery due to PROM 5(10%)History of MR 4(8%)History of D&C 2(4%)
Table-IV shows time of sexual activities beforePPROM. 62 % women had history of sexual activitiesbetween 2 to 7days.
Table-IV
Shows relation of preterm PROM with sexual behavior
Time of last coitus Frequency< 48 hours 6(12%)2 -7 days 30(60%)1week-1 month 10(20%)> 1month 04(08%)
Total 50(100%)
Table-V shows distribution of associated diseases.34% (17) had urinary tract infection, 26% (13) hadanaemia, 12 %( 6) had lower genital tract infection,10 %( 5) had hypertension, 4% (2) had diabetesmellitus and 2% (1) had renal disease.
Table-VShows distribution of associated disease
Variables Frequency
Urinary tract infection 17(34%)Anaemia 13(26%)Lower genital tract infection 6(12%)Hypertension 5(10%)Diabetes mellitus 2(4%)Renal disease 1(2%)
Table-6 shows cervical condition at the time ofadmission. Sixty eight percent women had cervicaleffacement 0 to50% and 32% had 51to100%.Cervicaldilatation was less than 2cm in 72% women and morethan 2cm in 28% women.
Table-VIShows cervical condition at the time of admission (n-50)Cervical condition FrequencyCervical effacement 0-51% 34(68%)
51-100% 16(32%)cervical dilatation <2cm 36(72%)
>2cm 14(28%)
In this study 78% women had cephalic, 16% hadbreech and 06% had shoulder presentation.
Table VII shows distribution of latent period.46%women start labor pain within 15hours, 26% womenwithin 16-30hours, 10% women within 31-45 hours,
Journal of Bangladesh College of Physicians and Surgeons Vol. 28, No. 1, January 2010
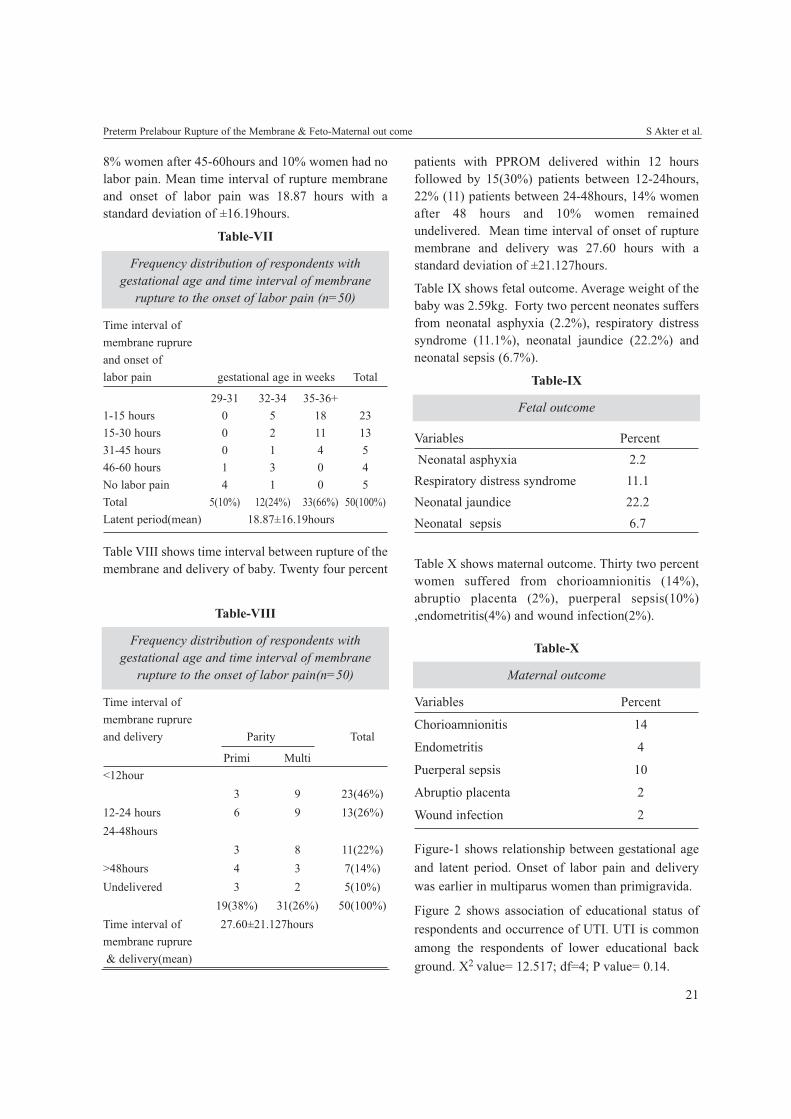
21
Preterm Prelabour Rupture of the Membrane & Feto-Maternal out come S Akter et al.
Table-VIII
Frequency distribution of respondents withgestational age and time interval of membrane
rupture to the onset of labor pain(n=50)
Time interval ofmembrane ruprureand delivery Parity Total
Primi Multi<12hour
3 9 23(46%)12-24 hours 6 9 13(26%)24-48hours
3 8 11(22%)>48hours 4 3 7(14%)Undelivered 3 2 5(10%)
19(38%) 31(26%) 50(100%)Time interval of 27.60±21.127hoursmembrane ruprure& delivery(mean)
8% women after 45-60hours and 10% women had nolabor pain. Mean time interval of rupture membraneand onset of labor pain was 18.87 hours with astandard deviation of ±16.19hours.
Table-VII
Frequency distribution of respondents withgestational age and time interval of membrane
rupture to the onset of labor pain (n=50)
Time interval ofmembrane ruprureand onset oflabor pain gestational age in weeks Total
29-31 32-34 35-36+1-15 hours 0 5 18 2315-30 hours 0 2 11 1331-45 hours 0 1 4 546-60 hours 1 3 0 4No labor pain 4 1 0 5Total 5(10%) 12(24%) 33(66%) 50(100%)Latent period(mean) 18.87±16.19hours
Table VIII shows time interval between rupture of themembrane and delivery of baby. Twenty four percent
patients with PPROM delivered within 12 hoursfollowed by 15(30%) patients between 12-24hours,22% (11) patients between 24-48hours, 14% womenafter 48 hours and 10% women remainedundelivered. Mean time interval of onset of rupturemembrane and delivery was 27.60 hours with astandard deviation of ±21.127hours.
Table IX shows fetal outcome. Average weight of thebaby was 2.59kg. Forty two percent neonates suffersfrom neonatal asphyxia (2.2%), respiratory distresssyndrome (11.1%), neonatal jaundice (22.2%) andneonatal sepsis (6.7%).
Table-IX
Fetal outcome
Variables PercentNeonatal asphyxia 2.2
Respiratory distress syndrome 11.1Neonatal jaundice 22.2Neonatal sepsis 6.7
Table X shows maternal outcome. Thirty two percentwomen suffered from chorioamnionitis (14%),abruptio placenta (2%), puerperal sepsis(10%),endometritis(4%) and wound infection(2%).
Table-X
Maternal outcome
Variables Percent
Chorioamnionitis 14
Endometritis 4
Puerperal sepsis 10
Abruptio placenta 2
Wound infection 2
Figure-1 shows relationship between gestational ageand latent period. Onset of labor pain and deliverywas earlier in multiparus women than primigravida.
Figure 2 shows association of educational status ofrespondents and occurrence of UTI. UTI is commonamong the respondents of lower educational background. X2 value= 12.517; df=4; P value= 0.14.
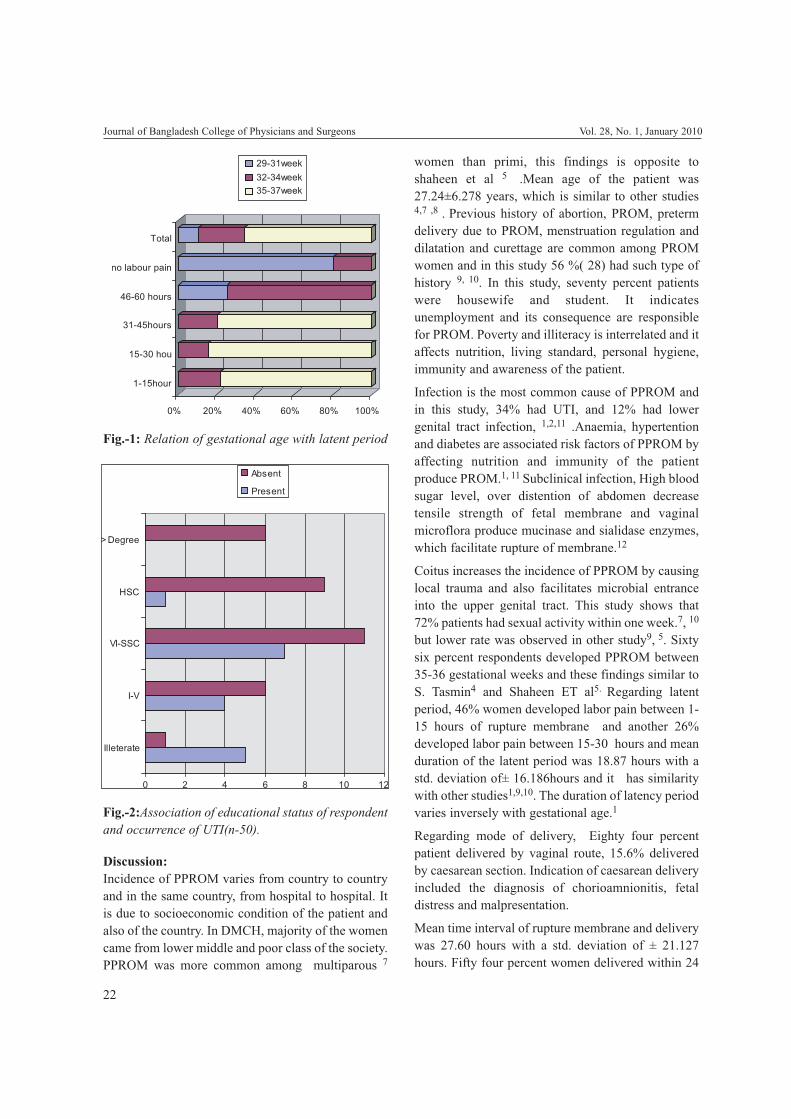
22
Discussion:Incidence of PPROM varies from country to countryand in the same country, from hospital to hospital. Itis due to socioeconomic condition of the patient andalso of the country. In DMCH, majority of the womencame from lower middle and poor class of the society.PPROM was more common among multiparous 7
women than primi, this findings is opposite toshaheen et al 5 .Mean age of the patient was27.24±6.278 years, which is similar to other studies4,7 ,8 . Previous history of abortion, PROM, pretermdelivery due to PROM, menstruation regulation anddilatation and curettage are common among PROMwomen and in this study 56 %( 28) had such type ofhistory 9, 10. In this study, seventy percent patientswere housewife and student. It indicatesunemployment and its consequence are responsiblefor PROM. Poverty and illiteracy is interrelated and itaffects nutrition, living standard, personal hygiene,immunity and awareness of the patient.
Infection is the most common cause of PPROM andin this study, 34% had UTI, and 12% had lowergenital tract infection, 1,2,11 .Anaemia, hypertentionand diabetes are associated risk factors of PPROM byaffecting nutrition and immunity of the patientproduce PROM.1, 11 Subclinical infection, High bloodsugar level, over distention of abdomen decreasetensile strength of fetal membrane and vaginalmicroflora produce mucinase and sialidase enzymes,which facilitate rupture of membrane.12
Coitus increases the incidence of PPROM by causinglocal trauma and also facilitates microbial entranceinto the upper genital tract. This study shows that72% patients had sexual activity within one week.7, 10
but lower rate was observed in other study9, 5. Sixtysix percent respondents developed PPROM between35-36 gestational weeks and these findings similar toS. Tasmin4 and Shaheen ET al5. Regarding latentperiod, 46% women developed labor pain between 1-15 hours of rupture membrane and another 26%developed labor pain between 15-30 hours and meanduration of the latent period was 18.87 hours with astd. deviation of± 16.186hours and it has similaritywith other studies1,9,10. The duration of latency periodvaries inversely with gestational age.1
Regarding mode of delivery, Eighty four percentpatient delivered by vaginal route, 15.6% deliveredby caesarean section. Indication of caesarean deliveryincluded the diagnosis of chorioamnionitis, fetaldistress and malpresentation.
Mean time interval of rupture membrane and deliverywas 27.60 hours with a std. deviation of ± 21.127hours. Fifty four percent women delivered within 24
Journal of Bangladesh College of Physicians and Surgeons Vol. 28, No. 1, January 2010
Fig.-2:Association of educational status of respondentand occurrence of UTI(n-50).
Fig.-1: Relation of gestational age with latent period

23
hours 9, 10 and among them 36% are multi and 18%are primi. Progress of labor are speeded amongwomen with higher gestational age and gravidity .1
Regarding neonatal outcome, we assess neonatalweight which was 2.59kg. Forty two percent neonatessuffered from neonatal asphyxia (2.2%), respiratorydistress syndrome (11.1%), neonatal jaundice(22.2%) and neonatal sepsis (6.7%) and admitted tospecial baby care unit. This result is accord with someother studies.4 5 In DMCH, intensive neonatal carefacilities are limited .We didn’t check fetal lungmaturity. Gestational age and birth weight at the timeof delivery both affect neonatal survival. More theGestational age and birth weight, more the rate ofsurival.2
Thirty two percent women suffered fromchorioamnionitis (14%), abruptio placenta(2%),puerperal sepsis(10%) ,endometritis(4%) and woundinfection(2%). 9,10 Studies shows that bacterialvaginosis group of organism( Gardnerella vaginalisand bacteroid species) and a group ofenteropharyngeal organisms were associated withPPROM.12. These organisms are normal commenselof vagina. We used ampicillin / cephradin in all cases(hospital supply), while other use erythromycin4, 13
and cephradin& metronidazole5 .The occurrence ofchorioamnionitis (14%) was more 9, 10. But nochorioamnionitis5 among cephradin andmetronidazole user. Standard of hospital andmanagement strategy also have some influences ondevelopment of chorioamnionitis. We were unableto do C-reactive protein and ultrasonography topredict infection earlier.
Conclusion:From the above study, we found that majority of thepatients were poor, their access to antenatal care waspoor. It might be due to lack of awareness and/ orknowledge. It was presumptive that PPROM wasmalnutrition and poverty related disease .Antenatalcare is an important tool to prevent PPROM byidentifying risk factors and its management .Pretermprelabor rupture of membranes has significant impacton perinatal out come. But our main target washealthy mother and healthy baby. In managingPPROM, timely use of proper antibiotics, steroid and
induction or augmentation of labor speeded labor,reduce hospital stay and ultimately reduce perinataland maternal complications.
Reference:1. Griff Jones; Pre labour rupture of the membrane; Obstetrics
&Gynaecology-An evidenced based text for MRCOG;Arnold, Member of the hodder headline group.www.arnoldpublishers.com; 1st edition; Oxford University press; 2004;p297.
2. Andrea CScharfe, Jude P Crino: Pre term labor and Pre laborrupture of the membranes; The Johns Hopkins Manual ofGynecology Obstetrics; 2nd edition, 2000; LippincotWilliams & Wilkins, USA, p123.
3. Willium’s Obstetric Gynaecologic: Pre term labor, Pre laborrupture of the membranes, 19th edition, 1993; Appleton &Lange, California,USA; p361.
4. Tasnim S, A B Bhuiyan: Outcome of premature rupture ofmembranes; Bangladesh Journal of Obstetrics&Gynaecology , 1998;13(1),16-20.
5. Shaheen Rhaman Chowdhury et al; Incidence and outcome ofpreterm pre mature rupture of membranes and pre term laborat Holy Family Red Crescent Medical College Hospital,Bangladesh Journal of Obstetrics& Gynaecology ,2005;20(1),19-24.
6. Bhide AG: Premature rupture of membranes. In: Krishna U,Tank DK, Daftary S. editors; Pregnancy at risk, Currentconcepts; 3rd edition; Jaypee Brothers publishers, India;1997, 360.
7. Begum A, Choudhury: A clinical evaluation of 60 cases; JInst Postgra Med res 1991; 6:11-15.
8. Moretti M, Sibai BM: Maternal and perinatal outcome ofexpectant management of premature rupture of membranes inthe mid trimester; Am J Obstet Gynecol 1988; 159:390-96.
9. J Sultana,T A Chowdhury, M H Khan,K Begum: Amnioticfluid index values after preterm premature rupture of themembranes and subsequent prenatal infections ; BangladeshJournal of Obstetrics& Gynaecology , 2005;20(2),51-55.
10. Ahmed Nazneen. Maternal and fetal outcome in prematurerupture of membrane [dissertation] Dhaka BangladeshCollege of Physician and Surgeon (BCPS); 2002.
11. Ashley S. Roman,MD,MPH&Martin L .Pernoll,MD. Latepregnancy complication, Current obstetric GynaecologicDiagnosis and treatment. 8th edition. Appleton & Lange.1994; 286-87.
12. Mcdonald HM, O’Loughlin JA, Jolley P, Vigneswaren R,McDonald PJ; Vaginal infection and preterm labor; Br. JObstet Gynecol;1991May, 98(5):427-35.
13. kenyon S,Boulvain M, Neilson J :Antibiotics for preterm premature rupture of membranes; ORACLE Clinical Co-ordinating Centre,Leicester Royal Infirmary, Department ofObstetrics,Clinical Science Building,[email protected]
Preterm Prelabour Rupture of the Membrane & Feto-Maternal out come S Akter et al.

28
Introduction:Bangladesh is passing through an epidemiologicaltransition. Burden of infectious diseases are comingdown while with increased life expectancy and widespread change of lifestyle, non-communicable diseasesare on the rise 1 . Cardiovascular diseases are one of
the main causes of morbidity and mortality in thiscountry now. Heart failure (HF) is a significant andgrowing health problem as the population ages.Despite improvements in therapy, mortality andmorbidity remain high 2 . In the United Kingdom, mostpatients admitted to hospital with HF are more than 65years old and remain inpatients for a week or more .Prevalence of heart failure rises from around 1% in theage group 50-59 years to between 5 and 10% of thoseaged 80-89 years 3. Heart failure is frequently due tocoronary artery disease, tends to affect elderly peopleand often leads to prolonged disability. Although theoutlook depends to some extent on the underlyingcause of the problem, heart failure carries a very poorprognosis, approximately 50% of patients with severeHF due to severe left ventricular dysfunction will diewithin 2years 3. Hospitalized heart failure is regardedas prognostically more adverse with a high mortalityand readmission rate .However, there is a paucity ofdata on outcomes of heart failure in particular in Indo-Asians 4.
There is an ever increasing number of hospitaladmissions due to heart failure in different hospitals
Burden of Heart Failure Patients in a Tertiary LevelCardiac Hospital
M KABIRUZZAMANa, FN MALIKb, N AHMEDc, M BADIUZZAMANc, SR CHOUDHURYd, T HAQUEe,H RAHMANa, MN AHMEDa, D BANIKa, MAM KHANa, AK DUTTAa, S SAYEEDf,
RK KHANDAKERb, A MALIKb
Summary:Objective: Heart failure (HF) has become an increasinglyfrequent cause of hospital admission and carries a poorprognosis. There is a paucity of data in Indo-Asiansparticularly in Bangladesh on characteristics of heartfailure patients. The purpose of this study was todetermine the etiological factors and co-morbidity ofhospitalized heart failure patients.
Method: A hospital based cross sectional study was doneat a tertiary cardiac hospital in Dhaka city. Hospitalmedical records of 14009 patients admitted betweenJanuary 2005 and August 2006 were reviewed and 1970patients with the diagnosis of HF were identified.Relevant etiological information and socio demographicdata were abstracted from the hospital record files.
Result: About one-seventh of total hospital admittedpatient had HF. Mean age (SD) was 54.1 (15.3) years.
Majority (35.79%) had ischaemic heart disease (IHD) asthe principal etiological factor but this frequently co-existed with a history of hypertension (46.8%).Hypertension was considered the primary risk factor ofHF in 29.14% of cases. Hypertension alone and in co-existence with other etiology was found in 48.07% (947)cases. Diabetes Mellitus (DM) co-existed with IHD in41.4% (292) and it (32.64%) was found more prevalentin Dilated Cardiomyopathy (DCM) patient with HF.
Conclusions: The mean age of hospitalized HF patients isremarkably lower than other related studies done abroad.The single most common etiology for HF is ischemicheart disease in this population. Hypertension is the mostcommon risk factor. Measures to prevent ischaemic heartdisease and control of risk factors are essential to preventpremature onset of HF.
(J Bangladesh Coll Phys Surg 2010; 28: 24-29)
Journal of Bangladesh College of Physicians and Surgeons Vol. 28, No. 1, January 2010
a Dr. Mohammad Kabiruzzaman MD, a Dr. Habibur RahmanMD, Dr. M Nesar Ahmed MD, Dr. Dhiman Banik MD, Dr. MA Majid Khan D-Card, Dr. Asok K Dutta MD, Assistantprofessor, Department of Cardiology, NHFH&RI
b Professor Fazila-Tun-Nessa Malik MRCP, Professor R KKhandaker FRCP, Professor Abdul Malik FRCP, Professor,Department of Cardiology, NHFH&RI
c Dr. Nazir Ahmed MD, Dr. Mohammad Badiuzzaman MD,Associate professor, Department of Cardiology, NHFH&RI
d Dr. Sohel R Choudhury PhD, Associate Professor,Department of Epidemiology & Research, NHFH&RI
e Dr.Tuhin Haque PhD, Associate Professor, Department ofEchocardiography, NHFH&RI
f Dr. Sadia Sayeed MPH, Epidemiologist, Department ofEpidemiology & Research, NHFH&RI
Address of Correspondence: Dr M Kabiruzzaman, AssistantProfessor, Department of Cardiology, National Heart FoundationHospital & Research Institute, Plot no. 7/2, Section 2, MirpurDhaka 1216, Tel: 8061314-6, 8053939-6, E-mail:[email protected]: 22 April, 2009 Accepted: 11 September, 2009

25
in Bangladesh, however there is a paucity of data oncharacteristics of the patients in terms ofdemographic and etiological information. It isimportant to identify the etiological factors associatedwith HF in this population to determine strategy forprevention and early detection. In this study wesought to determine the disease burden of heartfailure patients and the age and sex specificprevalence of heart failure among patients admittedinto NHFH&RI and to identify the etiological patternof diseases leading to heart failure with associated co-morbid factors.
Materials & Method:Settings: This was a single center cross sectional studycarried out at National Heart Foundation Hospital &Research Institute (NHFH&RI), a tertiary teachinghospital in Dhaka, Bangladesh. This centre receives amixture of affluent and low-middle income patientsand serves the entire country as a referral center forpatients requiring high-intensity tertiary care.
The hospital medical records from January 2005 toAugust 2006 were searched & all patients sufferingfrom heart failure were included in this study.Variables recorded includes age, sex, history ofDiabetes Mellitus (DM) (defined as a fasting glucose≥ 126 mg/dl or on treatment), Hyperlipidemia (fastingcholesterol ≥ 200mg/dl or on treatment),hypertension (blood pressure ≥140/90mmHg or ontreatment). Associated co-morbidity were classifiedinto some major group of heart diseases: oldmyocardial infarction (OMI), acute coronarysyndrome (ACS), dilated cardiomyopathy (includingischaemic and other causes), valvular heart diseases,hypertensive heart disease, congenital heart diseases.Among the ACS were acute myocardial infarction(AMI), recent myocardial infarction (RMI), andunstable angina (UA).
Coronary artery disease was considered the primaryaetiology if the patient had a documented history ofmyocardial infarction (acute or in the past); unstableangina pectoris; a history of stable angina ; orcoronary artery disease confirmed at coronaryangiography. Such cases were subdivided into thosewith acute cardiac ischaemic syndromes (acutemyocardial infarction or unstable angina pectoris),and those without. Hypertension was considered the
aetiology if there was a history of hypertension fromthe general practice records or sustained hypertension(blood pressure greater than 140/90 mmHg) duringhospital admission and there was no documentedhistory of myocardial infarction or angina, and noevidence of other cardiac pathology. The presenceand severity of underlying valvular heart disease wasassessed from the history, clinical examination andechocardiographic findings. The presence of cardiacarrhythmias was noted and the temporal relationshipof these to the development of heart failureascertained. Data were checked for completeness andconsistencies. The descriptive statistics were analysedwith SPSS for windows version 12.5.
Results:Among 14,009 total admitted patients throughout thisperiod 1970 patients were found to have a diagnosis ofheart failure ie 14.1% of totally admitted patients hadheart failure. The mean age of these patients were 54.1± 15.3 years ranging from 1 to 95 years with a highpreponderance of males. The majority of the patientpopulation was in the age group of 51- 60 years(30.7%) (Table I). 71.7% of the cases were male &28.3% female by gender specification. Chronic heartfailure patients were more prevalent among the patientpopulation (71.3% chronic Vs 28.7% acute). Coronaryartery disease was found to be the common cause ofheart failure in adult population (n=705, 35.79%).
Majority of the ACS patients were diagnosed as AMI(n=400, 20.3%). Among total study population,49.4% (n=974) patients were hypertensive and 18.8%(n=371) patients were diabetic. 29.14% (n=574)patients had hypertensive heart disease leading toheart failure. The patients with heart failure havingcoronary artery disease (n=705) had hypertension(n=330, 46.8%) as the most prevalent major riskfactor; diabetes was found to be second common co-morbid factor. Patients with dilated cardiomyopathy(n=242) had DM (n=79; 32.64%) as most prevalentcomorbid factor. Among the congenital heartdiseases, ventricular septal defect (VSD) and patentductus arteriosus (PDA) were most common cause ofheart failure needing hospitalization (Table 2).
Mortality rate of the study population were 9.7% andwas higher among males (10.6% vs. 7.7%) thanfemales.
Burden of Heart Failure Patients in a Tertiary Level Cardiac Hospital M Kabiruzzaman et al.
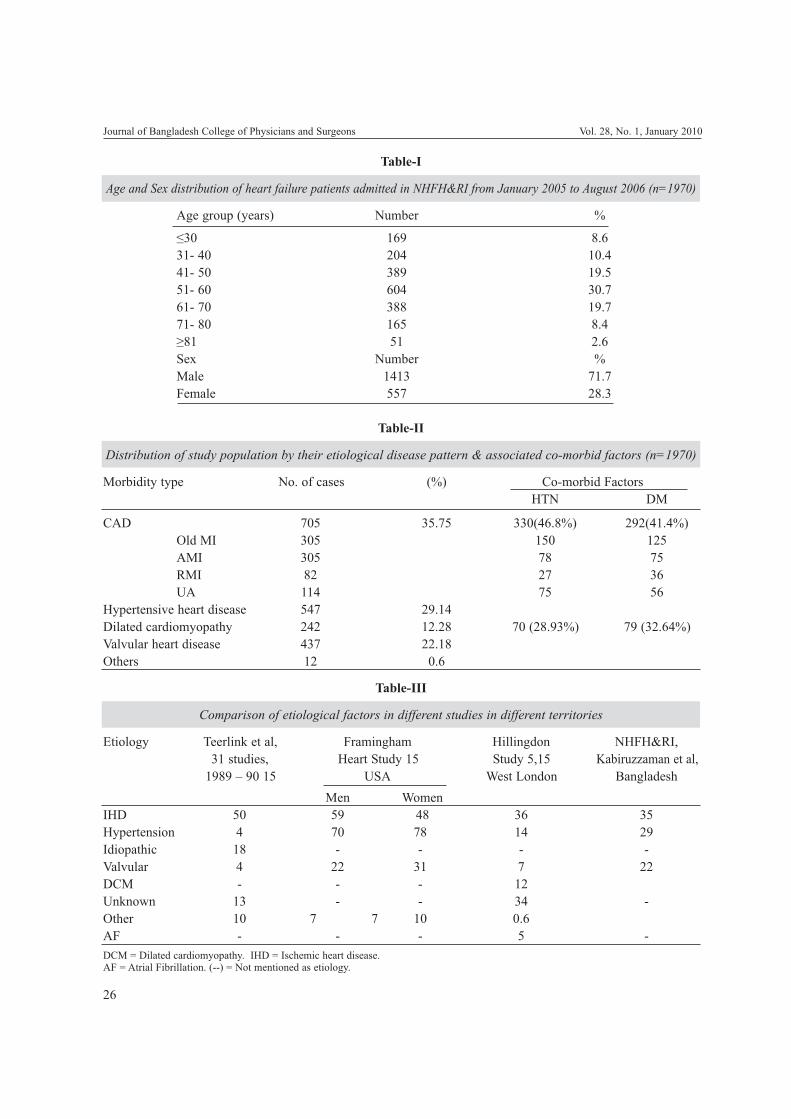
26
Journal of Bangladesh College of Physicians and Surgeons Vol. 28, No. 1, January 2010
Table-I
Age and Sex distribution of heart failure patients admitted in NHFH&RI from January 2005 to August 2006 (n=1970)
Age group (years) Number %
≤30 169 8.631- 40 204 10.441- 50 389 19.551- 60 604 30.761- 70 388 19.771- 80 165 8.4≥81 51 2.6Sex Number %Male 1413 71.7Female 557 28.3
Table-II
Distribution of study population by their etiological disease pattern & associated co-morbid factors (n=1970)
Morbidity type No. of cases (%) Co-morbid FactorsHTN DM
CAD 705 35.75 330(46.8%) 292(41.4%)Old MI 305 150 125AMI 305 78 75RMI 82 27 36UA 114 75 56
Hypertensive heart disease 547 29.14Dilated cardiomyopathy 242 12.28 70 (28.93%) 79 (32.64%)Valvular heart disease 437 22.18Others 12 0.6
Table-III
Comparison of etiological factors in different studies in different territories
Etiology Teerlink et al, Framingham Hillingdon NHFH&RI,31 studies, Heart Study 15 Study 5,15 Kabiruzzaman et al,
1989 – 90 15 USA West London BangladeshMen Women
IHD 50 59 48 36 35Hypertension 4 70 78 14 29Idiopathic 18 - - - -Valvular 4 22 31 7 22DCM - - - 12Unknown 13 - - 34 -Other 10 7 7 10 0.6AF - - - 5 -DCM = Dilated cardiomyopathy. IHD = Ischemic heart disease.AF = Atrial Fibrillation. (--) = Not mentioned as etiology.
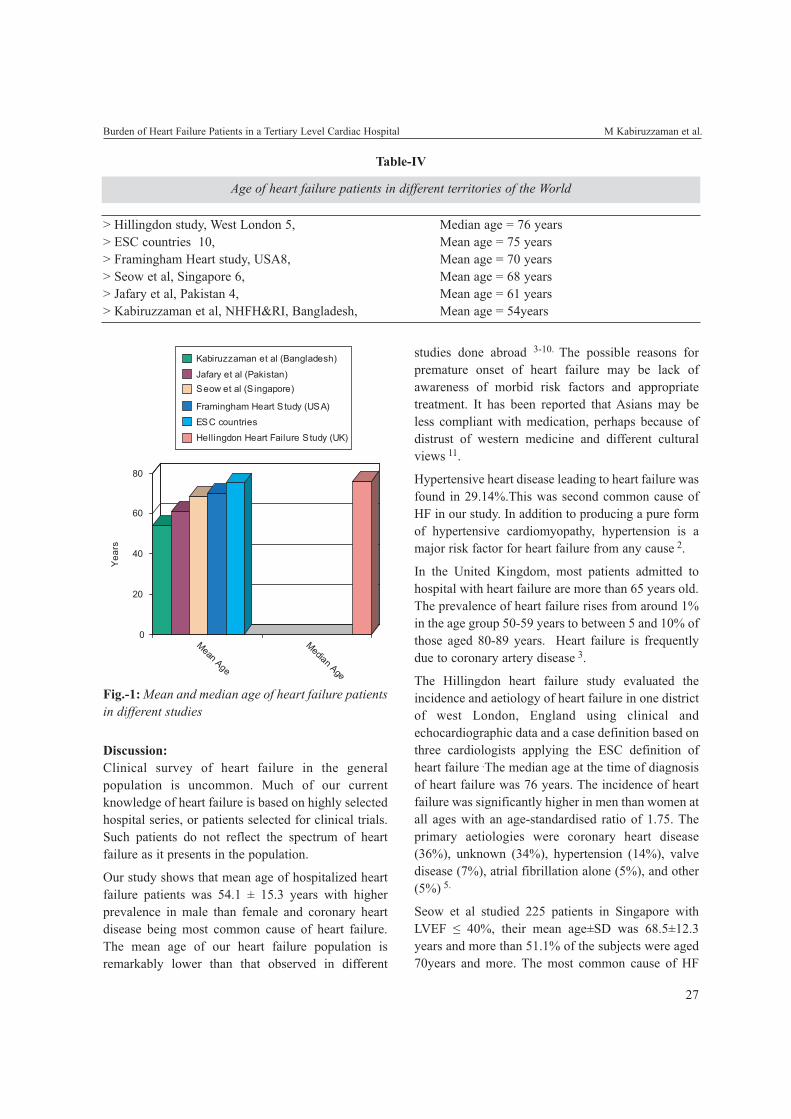
27
Discussion:Clinical survey of heart failure in the generalpopulation is uncommon. Much of our currentknowledge of heart failure is based on highly selectedhospital series, or patients selected for clinical trials.Such patients do not reflect the spectrum of heartfailure as it presents in the population.
Our study shows that mean age of hospitalized heartfailure patients was 54.1 ± 15.3 years with higherprevalence in male than female and coronary heartdisease being most common cause of heart failure.The mean age of our heart failure population isremarkably lower than that observed in different
studies done abroad 3-10. The possible reasons forpremature onset of heart failure may be lack ofawareness of morbid risk factors and appropriatetreatment. It has been reported that Asians may beless compliant with medication, perhaps because ofdistrust of western medicine and different culturalviews 11.
Hypertensive heart disease leading to heart failure wasfound in 29.14%.This was second common cause ofHF in our study. In addition to producing a pure formof hypertensive cardiomyopathy, hypertension is amajor risk factor for heart failure from any cause 2.
In the United Kingdom, most patients admitted tohospital with heart failure are more than 65 years old.The prevalence of heart failure rises from around 1%in the age group 50-59 years to between 5 and 10% ofthose aged 80-89 years. Heart failure is frequentlydue to coronary artery disease 3.
The Hillingdon heart failure study evaluated theincidence and aetiology of heart failure in one districtof west London, England using clinical andechocardiographic data and a case definition based onthree cardiologists applying the ESC definition ofheart failure .The median age at the time of diagnosisof heart failure was 76 years. The incidence of heartfailure was significantly higher in men than women atall ages with an age-standardised ratio of 1.75. Theprimary aetiologies were coronary heart disease(36%), unknown (34%), hypertension (14%), valvedisease (7%), atrial fibrillation alone (5%), and other(5%) 5.
Seow et al studied 225 patients in Singapore withLVEF ≤ 40%, their mean age±SD was 68.5±12.3years and more than 51.1% of the subjects were aged70years and more. The most common cause of HF
Burden of Heart Failure Patients in a Tertiary Level Cardiac Hospital M Kabiruzzaman et al.
Table-IV
Age of heart failure patients in different territories of the World
> Hillingdon study, West London 5, Median age = 76 years> ESC countries 10, Mean age = 75 years> Framingham Heart study, USA8, Mean age = 70 years> Seow et al, Singapore 6, Mean age = 68 years> Jafary et al, Pakistan 4, Mean age = 61 years> Kabiruzzaman et al, NHFH&RI, Bangladesh, Mean age = 54years
Fig.-1: Mean and median age of heart failure patientsin different studies

28
was coronary heart disease (85.5%). Co morbidmedical conditions were prevalent in this cohort, with83.5% having at least one co-morbid condition.Hypertension was the most prevalent co-morbidcondition; affecting 60% of the patients; followed bydiabetes mellitus (56.9%) 6.
In Pakistan, Jafary et al studied 196 patients withmean age ± SD 61.2 ± 12.8 years with a highpreponderance of males. All of them were sufferingfrom systolic heart failure with LVEF ≤ 40%,requiring hospital admission with more than 60%suffering from hypertension (67.3%) and diabetesmellitus (60.7%) and more than three-fourths havinga history of coronary artery disease in the past 4.
In the United States, it is primarily a disease ofageing, with over 75% of existing and new casesoccurring in individuals over 65 years of age7. In theUSA, the Framingham heart study has reported themean age at the time of diagnosis of heart failure was70 years. The incidence of heart failure to be 0.3% perannum in men and 0.2% per annum in women aged50-59 years; rising by a factor of 10 to 2.7% perannum in men and 2.2% per annum in women aged80-90 years. The incidence of heart failure wassignificantly higher in men than women at all ageswith an age-standardized incidence ratio of 1.67 8
Mcmurray et al studied trends in hospitalization forheart failure in Scotland 1980-1990. They foundseventy-eight percent of discharges were in personsaged ≥ 65years and 48% of discharges were male 9.
Remes et al studied incidence of heart failure in 45-74 year old inhabitant in four rural communities inEastern Finland. The incidence rates of heart failureincreased with age in both sexes. Coronary heartdisease or hypertension was evident in 80% cases 12.
This is a single centre retrospective cohort study andour results may not be extrapolated to the entireBangladeshi population. However, our hospitalprovides services to a wide mix of patients, rangingfrom affluent to poor, somewhat reflective of thepopulation at large throughout Bangladesh. Becauseof the retrospective nature of the study severalimportant variable are missing in our study includingreliable documentation of sign and symptoms as wellas anthropometric values. We could not determine co-
morbid illness like COPD, renal functionalimpairment, obesity.
Heart failure is a significant and growing healthproblem as the population ages. About one-seventh oftotal hospital admitted patients had heart failure. Themean age (54.1±15.3) of our heart failure patientswas significantly lower than the other studies doneabroad (Table-4). Coronary heart disease (with orwithout hypertension) should be the dominantaetiology of heart failure in the Bangladesh. In thisstudy the single most common aetiology wasischaemic heart disease (35.79%) and past history ofhypertension was common (48.07%). This is verysimilar to the findings in the heart failure study donein Hillingdon (West London) 5, Finland 12 andSweden 13 and is not dissimilar to that reported fromFramingham study 14 (Table-3). The number ofpatients with heart failure is bound to rise at thepremature age if appropriate measurement is nottaken to manage risk factors and to increase publicawareness. Clinical and Epidemiological study isneeded to explore further details.
References:1. Ministry of Health and Family Welfare, Government of
People’s Republic of Bangladesh. Strategic plan forSurveillance and Prevention of Noncomunicable Disease inBangladesh 2007-2010. 2007, Dhaka
2. Dar O, Cowie MR. 2008. The Epidemiology and Diagnosisof Heart Failure. In: Fuster V, Walsh RA, O’Rourke RA,Poole-Wilson P (eds). Hurst’s The Heart. 12th ed. McGraw-Hill, New York, pp. 713-721.
3. Bloomfield P, Bradbury A, Grubb NR, Newby DE. 2006.Cardiovascular disease. In: Boon NA, Colledge NR, WalkerBR, Hunter JAA (eds). Davidson’s Principles and Practiceof Medicine, 20th ed. Churchill Livingstone, Edinburgh,pp. 519-644.
4. Jafary FH, Kumar M, Chandna IE. Prognosis of hospitalizednew- onset systolic heart failure in Indo-Asians- A lethalproblem. J Cardiac Fail 2007; 13:855-860.
5. Cowie MR, Wood DA, Coats AJ, et al. Incidence andaetiology of heart failure: a Population-based study. EurHeart J 1999; 20:421-8.
6. Seow SC, Lee YP, Chan YH, et al. Heart Failure Mortalityin South Asian Patients With Left Ventricular SystolicDysfunction. J Cardiac Fail 2007; 13:476-481.
7. Bashore TM, Granger CB, Hranitzky P. 2007. Heart. In:McPhee SJ, Papadakis MA, Tierney LM (eds). CurrentMedical Diagnosis and Treatment, 46th ed. McGraw Hill,New York, pp. 316-428.
Journal of Bangladesh College of Physicians and Surgeons Vol. 28, No. 1, January 2010

29
8. Ho KK, Pinsky JL, Kannel WB, et al. The epidemiology ofheart failure: the Framingham study. J Am Coll Cardiol1993; 22(4 suppl A):6A-13A.
9. McMurray J, McDonagh T, Morrison CE, Dargie HJ.Trends in hospitalization for heart failure in Scotland 1980-1990. Eur Heart J 1993; 14:1158-62.
10. The Task Force for the Diagnosis and Treatment of Acuteand Chronic Heart Failure 2008 of the European Society ofCardiology. ESC Guidelines for the diagnosis and treatmentof acute and chronic heart failure 2008. European Journal ofHeart Failure dol:10.1016/j.ejheat.2008.08.005
11. Sung CL. Asian patients’ distrust of western medical care:one perspective. M Sinai J Med 1999; 66:259-61.
12. Remes J, Reunanen A, Aromaa A, Pyorala K. Incidence ofheart failure in Eastern Finland: a population-basedsurveillance study. Eur Heart J 1992; 13: 588-93.
13. Eriksson H, Svarsudd K, Larsson B et al. Risk factors forheart failure in the general population: the study of menborn in 1913. Eur Heart J 1989; 10: 647-56.
14. Kannel WB, Pinsky J, Trends in cardiac failure- incidenceand causes over three decades in the Framingham study(Abstr). J Am Coll Cardiol 1991; 17: 87A.
15. Lip GYH, Gibbs CR, Beevers DG. ABC of heart failure,Aetiology. BMJ Volume 320 8 January 2000. www.bmj.com
Burden of Heart Failure Patients in a Tertiary Level Cardiac Hospital M Kabiruzzaman et al.
Introduction:Rheumatoid arthritis is a chronic systemicinflammatory disease whose major manifestation issynovitis of multiple joints. The hallmark ofrheumatoid arthritis is symmetrical synovialproliferation and tenderness of multiple joints,particularly the small joints of hands and feet. Whenthe disease is unchecked, it leads to substantialdisability and premature death1. It affectsapproximately 0.8 percent of adults worldwide 2 andis more common in women (by a ratio of 3 to 1) andhas an earlier onset in women, frequently beginningin the childbearing years.3 Recent advances inunderstanding the cytokine networks that areresponsible for the ongoing inflammatory response inrheumatoid arthritis4 have led to the successful use oftherapies that target tumor necrosis factor α (TNF- α)and interleukin-14. During the past 10 years,improved understanding of the pathophysiology ofrheumatoid arthritis has led to several key changes inthe approach to therapy. First, early diagnosis andtreatment are important; second the use of diseasemodifying anti rheumatic drugs (DMARDs) incombination is highly effective. Third, the use ofagents that target cytokines, such as (TNF- α) andinterleukin-1 is an effective strategy. And fourth,recognition is growing that the assessment oftreatment outcomes should include an analysis ofimportant coexisting illnesses (particularlycardiovascular disease and osteoporosis). In thisarticle, I will discuss the clinical application of theseprinciples, which has resulted in markedimprovement in clinical outcomes.
Early Diagnosis and TreatmentJoint damage occurs early in the course of rheumatoidarthritis; 30 percent of patients have radiographic
evidence of bony erosions at the time of diagnosis,and this proportion increases to 60 percent by twoyears5. Unfortunately, bony erosions and deformitiesare largely irreversible. Initiation of therapy withDMARDs within three months after the diagnosis ofrheumatoid arthritis is crucial; a delay of as little asthree months in the introduction of these medicationsresults in substantially more radiographic damage atfive years6. Therefore, early diagnosis, althoughchallenging, is critical7. The diagnosis of rheumatoidarthritis cannot be established by a single laboratorytest or procedure but is made with four or more of thediagnostic criteria8. The diagnostic criteria are thepresence of morning stiffness (more than 1 hour),arthritis of three or more joint areas, arthritis of thehand joints, symmetrical arthritis, rheumatoidnodules, elevated levels of serum rheumatoid factor,radiographic changes and duration of 6 weeks ormore. Many other syndromes, including self-limitingviral conditions lasting several weeks, mimicrheumatoid arthritis. Antibodies to cyclic citrulinatedpeptides (CCPs) appear to have a high specificity (90to 98 percent) and thus may prove useful in earlydiagnosis even though the sensitivity of the test forthem is approximately 50 to 60 percentages atpresentation9 .Interestingly, these antibodies mayappear in the serum years before the onset of clinicaldisease10.
Gemeral Therapeutic PrinciplesGuidelines concerning therapy for rheumatoidarthritis have been published recently by theAmerican college of Rheumatology (Fig-1)11. Notreatment cures rheumatoid arthritis; therefore, thetherapeutic goals are a remission of joint symptoms, areturn of full function, and the maintenance ofremission with DMARD therapy. A usefulintermediate goal is to have all patients evaluated bya rheumatologist within three months after the onsetof symptoms, So that essentially all patients will bereceiving DMARDs by the time they have hadsymptoms for three months.
Medical Treatment of Rheumatoid Arthritis: A ReviewAHM FEROZ
(J Bangladesh Coll Phys Surg 2010; 28: 30-39)
REVIEW ARTICLES
Address of Correspondence: Dr. A.H.M. Feroz, FCPS, MD(Internal Medicine), Senior Consultant of Medicine, Department ofMedicine, 200 bedded Hospital, Narayangonj
Received: 4 May, 2008 Accepted: 25 January, 2009

31
To evaluate the success of intervention, investigatorshave used a number of clinical measures. Theyinclude the number of joints that are tender andswollen, markers of inflammation (including theerythrocyte sedimentation rate and c- reactive proteinlevel), and patients’ responses to questions about theirpain, their global assessment of disease activity, andtheir physical function. The American College ofRheumatology criteria for improvement can be usedby clinicians to quantify patients’ improvement aftertreatment (Table1) 12. Most clinical studies haverequired a benchmark of 20 percent improvement inthese criteria, a result that is known as ACR 20; nowthat better treatments are being initiated earlier in thecourse of the disease, 50 percent improvement (ACR50) is becoming a more frequent target.
MedicationsMedications that are used to treat rheumatoid arthritisare divided into three main classes: nonsteroidal anti-inflammatory drugs (NSAIDs), corticosteroids andDMARDs (both synthetic and biologic).
NSAIDSNSAIDs are particularly helpful during the first fewweeks in which a patient has symptoms, because thedrugs provide partial relief of pain and stiffness untila definitive diagnosis of rheumatoid arthritis can beestablished. NSAIDs have not been shown to slow theprogression of the disease; therefore, in long-termcare, NSAIDs should be used together with
DMARDs 11. Although both these classes ofmedications are well tolerated for short periods, longterm administration may result in gastrointestinalulcer, perforation, and hemorrhage. Every year 1.5percent of patients with rheumatoid arthritis arehospitalized with gastrointestinal problems13. Therisk of these complications increases with older age,corticosteroid use, and a history of peptic ulcerdisease.
Recently cyclooxygenase-2 (COX-2) inhibitors,which decrease the incidence of gastric andduodenal ulcers by approximately 50 percent ascompared with traditional NSAIDs, have beenintroduced14, 15. To a similar degree, the addition ofproton-pump inhibitors to therapy with NSAIDsalso decreases the incidence of bleeding ulcersassociated with traditional NSAIDs15. The efficacyof the COX-2 inhibitors is no better than of theolder and less expensive NSAIDs14. Bothtraditional NSAIDs and COX-2 inhibitors haveassociated with increased fluid retention,exacerbation of hypertension, and impairment ofrenal function in susceptible patients14. Thromboticevents have been reported in patients who aretaking COX-2 inhibitors and may occur morefrequently than with traditional NSAIDs16.
CorticosteroidsCorticosteroids are potent suppressors of theinflammatory response in rheumatoid arthritis and in
Medical Treatment of Rheumatoid Arthritis: A Review AHM Feroz
Table-I
American College of Rheumatology preliminary Definition of 20 percent Improvementin Rheumatoid Arthritis (ACR 20).
Measure of Disease Activity RequirementTender-joint count >20% ImprovementSwollen- joint count >20% ImprovementPatient’s assessment of painPatient’s global assessment of disease activityPhysician’s global assessment of disease activity >20% Improvement inPatient’s assessment of physical function three of the fiveMarkers of inflammation measures

32
many other diseases. Unfortunately, their dose-dependent side effects are familiar to all clinicians.
Studies conducted more recently 17,18 havecorroborated findings from older trials by clearlyestablishing that corticosteroids decrease theprogression of rheumatoid arthritis as detected radiographically. Corticosteroids in low doses (e.g. <10mgof prednisone per day) are used to treat 30 to 60percent of patients 17. Table ІІ presents some usefulguidelines for corticosteroid use in patients withrheumatoid arthritis. Predictable side effects ofcorticosteroid drugs include thinning of the skin,cataracts, osteoporosis, hypertension, andhyperlipidemia18. The latter three conditions may bepreventable with aggressive management ofosteoporosis and cardiovascular risk factors.Essentially, all patients taking corticosteroids shouldreceive supplemental calcium (1to 1.5g per day) andvitamin D (800 IU per day) 19. Bisphosphonatesappear to be very effective in reducing vertebralfractures is patients taking corticosteroids 19 (offeringa reported 70 percent reduction in incidence) andshould be prescribed for patients who have low bonedensity (e.g. a T score of -2 or lower). Recentevidence suggests that inflammation plays a majorrole in atherosclerosis20; the ability of corticosteroidsto decrease inflammation rapidly may offset some ofthe potentially detrimental effects of the drugs on thevascular endothelium20.
Synthetic DmardsOptimal management of rheumatoid arthritis requiresrapid and sustained suppression
of inflammation with DMARDs, which are definedas medications that retard or halt the progression ofdisease. Disease modification is most convincinglydemonstrated by the ability of the medications todecrease radiographic progression. A metaanalysisof blinded clinical trials has suggested that therelative efficacy of methotrexate, sulfasalazine,intramusculat gold and penicillamine is similar21.
Antimalarial drugs (e.g. chloroquine andhydroxychloroquine) are less effective.Penicillamine, because of concern about its
toxicity, and oral gold, because of its marginalefficacy are rarely used today21.
Table-ІІ
Keys to Optimizing the Outcome of Treatment
Make an early diagnosis
Start DMARD therapy as early as possible (withinthree months after onset of symptoms)
Strive for remission (no joint symptoms) in allpatients Use corticosteroids as bridge to effectiveDMARD therapy
Prednisone at doses >10mg/day is rarely indicated forjoint disease
Avoid using corticosteroids without DMARDs
Minimize duration and dose by tapering to the lowestdose that controls the disease
Always consider prophylaxis to avert osteoporosis
Recognize and treat coexisting illnesses
Facilitate communication between primary carephysician and rheumatologist
Since observational trials have clearly identifiedmethotrexate as the synthetic DMARD that is mostlikely to induce a long-term response, it is most oftenselected for initial therapy21. It has demonstratedefficacy and durability, a long-term track record ofacceptable toxicity, and low cost22. An importantobservational study has shown that patients withrheumatoid arthritis who have been treated withmethotrexate have significantly lower mortality (oddsratio for death, 0.4) than patients who have not beentreated with methotrexate23. Due to its markedefficacy, safety, tolerability and sustainable effect,most clinical trials have listed active disease despitemethotrexate therapy as an inclusion criterion andhave tested the safety and efficacy of new drugs incomparison with methotrexate 22. Concomitantadministration of folic acid (1 to 3 mg per day) orfolinic acid (2.5 to 5 mg given 12 to 24 hours aftermethotrexate) significantly decreases many toxiceffects without a measurable decrease in efficacy andhas improved the tolerability of methotrexate24, a
Journal of Bangladesh College of Physicians and Surgeons Vol. 28, No. 1, January 2010

33
finding that has permitted clinicians to administer 20to 30 mg of methotrexate per week when necessary.Most data suggest that methotrexate is most effectiveat a dose of 7.5 to 30 mg per week25 but that oraladsorption may be highly variable. Therefore, if oralmethotrexate produces a suboptimal response, a trialof subcutaneous or intramuscular methotrexate isindicated11.
Leflunomide, a new synthetic DMARD, has anefficacy similar to that of sulfasalazine or moderatedose methotrexate26, 27. Leflunomide is given orallyas a loading dose of 100 mg daily for 3 days followedby a daily dose of 20 mg. Leflunomide is analternative to MTX as a first-line DMARD in patientsintolerant of MTX or with renal insufficiency.
Hydroxychloroquine (200-400 mg/day),considered the least potent but best tolerated of theDMARDs 21 is the DMARD that is mostcommonly combined with methotrexate.Hydroxychloroquine may be used by itself in anearly and mild RA. Sulfasalazine was the firstDMARD that was developed specifically to treatrheumatoid arthritis and has an efficacy similar tothat of methotrexate21. It is often a first-choiceagent for rheumatoid arthritis; starting with onetablet (500mg) daily and building up to the fulldose of 2-3 gm daily over two weeks. Sulfasalazineis most commonly used in the United States as partof combination DMARD therapy21. Intramusculargold (500mg/month) provide significant clinicalimprovement in up to 30% of patients withrheumatoid arthritis and prolonged completeremission have been observed28. Its cumbersomeadministration and toxicity have limited itsuse.21.Safe administration of DMARDs requirescritical and careful monitoring (table ІІІ) 29.
Detailed monitoring guidelines have beenpublished to help avert damage to the liver30,
which was a major concern when use of the drugfor rheumatoid arthritis became popular in the mid-1980s. These guidelines include measuring serumalbumin and aminotransferase levels every four toeight weeks. Doses of methotrexate should be
decreased when aminotransterase levels ateelevated above the upper limit of normal, andtreatment should be stopped if the elevationpersists. Obtaining complete blood counts andmeasuring serum creatinine are alsorecommended29, since a decrease in renal functionmay precipitate toxic effects in a patient inpreviously stable condition who is takingmethotrexate.
Both methotrexate and leflunomide have asubstantial potential for teratogenesis30. So womenof childbearing potential who require thesemedications should be using reliable birth control.Subacute pneumonitis is rare with methotrexate(51 cases have been reported worldwide) but maybe life-threatening32. If pneumonitis is suspectedon the basis of clinical findings or a chestradiograph, methortexate should be promptlydiscontinued and not reintroduced. As the besttolerated of all the DMARDs, hydroxychloroquineis used at doses below 6.5 mg per kilogram of leanbody mass per day, requires only yearly visits tothe opththalmologist to prevent the rare occurrenceof retinal toxic effects33.
Four double blind, controlled trials have nowshown that minocycline is effective in treatingrheumatoid arthritis34, 35. Minocycline that wasused as initial therapy in patients who testedpositive for rheumatoid factor was superior toplacebo (response rate 65 percent, as comparedwith 13 percent for placebo)34 and superior tohydroxy-chloroquine (60 percent vs. 33 percent)35
when measuring ACR 50. The mechanism bywhich minocycline works is incompletelyunderstood but probably involvesinnunomodulation, suppression of matrixmetalloproteinases and suppression of nonspecificinfections that would otherwise stimulateinflammatory cytokine production35. Reversiblehyper pigmentation is seen in up to 30 percent ofpatients who are receiving long-term minocyclinetherapy.
Medical Treatment of Rheumatoid Arthritis: A Review AHM Feroz

34
Three biologic products that inhibit the actions ofTNF-α (infliximab, etanercept, and adalimumab), onethat inhibits the action of interleukin-1 (anakinra) andan anti CD20 monoclonal antibody are now availableto treat rheumatoid 36. Infliximab is a chimerichuman-murine anti TNF-α monoclonal antibody,which is administered by intravenous infusion,3mg/kg at 0, 2 and 6 weeks and then every 1-2 month.Etanercept is a synthetic human TNF receptor-Fcprotein, administered subcutaneously 25mg twiceweekly or 50 mg weekly. Adalimumab is a humanmonoclonal antibody to TNF-α administeredsubcutaneously 40 mg every 1-2 week. Anakinra, arecombinant form of human interleukin-1 receptorantagonist, 100mg daily by subcutaneous injectionmay be useful in patients who have no response to or
unable to tolerate methotrexate, leflunomide or TNF-α antagonist.
Rituximab is a chimeric (humanized mouse) antiCD20 monoclonal antibody that depletes CD20positive B cells. It has been approved by the FDA in2006 and has demonstrated clinical efficacy and safetyin of rheumatoid arthritis with incomplete response tomethotrexate.In a randomized, double-blind controlledclinical study of 161 patients who had activerheumatoid arthritis despite methotrexate treatment, asingle course of two infusions of rituximab (1000mgon days 1 and 15) alone or in combination with eithercyclophosphamide(750 mg on days 3 and 17) orcontinued methotrexate(≥10mg/week),providedsignificant improvement in disease symptoms at bothweeks 24 and 48.42
Journal of Bangladesh College of Physicians and Surgeons Vol. 28, No. 1, January 2010
Biologic DMARDS
Table-III
Guidelines for Monitoring the Traatment of Rheumatoid Arthritis

35
These drugs are more effective than standardDMARDs (with faster onset of action, greater clinicalefficacy and sustained benefit) but because of theircost many countries have set restrictive guidelines fortheir use. Current UK recommendations are that theyshould be initiated only in active RA when anadequate trial of at least two other DMARDs(including methotrexate) has failed.
Combination Therapy with DMARDSOne of the first randomized studies that directlycompared combination DMARD therapy withmethotrexate was a two-year, double-blind trial inwhich patients were assigned to three groups: thosewho took methotrexate alone (at 17.5 mg per week),those who took a combination of sulfasalazine (at 1g per day) and hydroxychloroquine (at 400 mg perday), and those who took all three medications37. Attwo years, the end point of 50 percent improvement incomposite symptoms of arthritis was reached by 77percent of patients who were treated with all threedrugs but by only 33 percent of patients who weretreated with methotrexate alone. Patients whoreceived combination therapy did not have more sideeffects than those who received methotrexate alone.In another study, the triple combination ofmethotrexate (at 17.5 mg per week), sulfasalazine (at2 g per day), and hydroxy-chloroquine (at 400 mg perday) was superior to either the combination ofmethotrexate and sulfasalazine or the combination ofmethotrexate and hydroxychloroquine38.
In patients who have early disease, three critical trialshave all shown that initial combination therapy issuperior to therapy with a single DMARD39, 40. TheCombination therapy Bij Rheumatoid Arthritis(COBRA)39 trial compared sulfasalazine alone withthe combination of sulfasalazine, low-dosemethotrexate (which was stopped at 40 weeks), andpredinisolone (which was given initially at 60 mg perday but tapered off by 28 weeks). Patients in thecombination group had a more rapid response totreatment, fewer withdrawals from the study becauseof toxicity, and most important, less radiographicevidence of progression at five years41. Other trialsinvolving patients with early disease havedemonstrated the superiority of triple therapy(methotrexate, sulfasalazine, and hydroxychloroquine)over sulfasalazine alone40, double therapy
(methotrexate and sulfasalazine or methotrexate andhydroxychloroquine), and monotherapy42.
Initial TreatmentEstablishing a diagnosis as early as possible and thenstarting DMARD therapy is the foundation forsuccessful treatment of patients with rheumatoidarthritis. Most rheumatologists select methotrexate asthe initial therapy for most patients43. Thecharacteristics and personal choices of patientsinfluence this decision11. Methotrexate should not beused in patients who have underlying liver or renaldisease, who consume alcohol, who plan to becomepregnant in the near future, or who do not want toundergo regular laboratory monitoring. Whether tostart a course of low-dose corticosteroids initiallyalong with the chosen DMARD is controversial,many clinicians start treatment with prednisone at 5to 7.5 mg per day as bridge therapy until the slower-acting DMARDs have a chance to work. Once theDMARD begins working, corticosteroids should betapered (Table-ІІ).
Methotrexate is started at a dose of 10 mg, givenorally once weekly. If patients continue to have activedisease (as indicated by swollen and tender joints), asmost do, the dose should be increased in 5mgincrements after two weeks interval up to 30mg perweek. If patients continue to have active disease,consideration should be given to switching tosubcutaneous administration of equivalent dose ofmethotrexate 11. If active disease persists despiteoptimal methotrexate therapy for 2-3 months, otherDMARDs should be added21. The Early RheumatoidArthritis (ERA) trial 44 is an important study thatcompared methotrexate (at a dose that escalated to 20mg per week) with etanercept in patients with diseasediagnosed within the preceding three years. Bothtreatments were very effective in controlling thedisease at one year, but etanercept (administered at 25mg subcutaneously twice a week) was more effectivein rapidly suppressing disease activity. In both theERA and COBRA trials, markers of inflammation(including the erythrocyte sedimentation rate and theC-reactive protein level) were dramatically reducedafter two weeks of therapy. If, in fact, it is importantto control disease in days, rather than in weeks ormonths, then corticosteroids and TNF inhibitors (both
Medical Treatment of Rheumatoid Arthritis: A Review AHM Feroz

36
of which appear to be capable of stopping activedisease) should be examined in trials to test theconcept of induction therapy (i.e., medication that isadministered initially and then withdrawn).
Therapy for Established Rheumatoid ArthritisIf patients continue to have active disease after two tothree months of methotrexate at a dose of 20 to 30 mgper week, or if they cannot tolerate higher doses ofmethotrexate despite folate replacement, the currentstandard practice is to add another DMARD tomethotrexate11. The most economical initial choice44
for the patient who has active disease despite takingmethotrexate is the addition of sulfasalazine,hydroxychloroquine, or both. If active disease(manifested by swollen and tender joints) persistsafter three months of these DMARD combinations,leflunomide or a TNF inhibitor should be added tomethotrexate.
If DMARD therapy is started within three monthsafter the onset of symptoms and escalated with thegoal of achieving remission, the majority of patientswill have their disease well controlled within a yearwhile taking conventional single or combinationDMARD therapy45 .If inflammatory disease isinadequately controlled, therapy with TNF inhibitorsshould be started.
Coexisting IllnessesThe long-term prognosis for patients with rheumatoidarthritis depends not only on how well their jointdisease is treated but also on how well theircoexisting illnesses are addressed46. The threecoexisting conditions that have the greatest effect onmorbidity and mortality in rheumatoid arthritis areinfection (particularly pulmonary infection),osteoporosis, and cardiovascular disease.
Rheumatoid arthritis is associated with approximatelya doubling of the risk of infection, as compared withthe risk in age-matched controls47, and the degree ofincrease in the risk correlates with the severity of thedisease48. Although some studies suggest thatcorticosteroids may increase the risk of infection49,
controversy exists about whether such an increase isdue to the use of corticosteroids itself or to the factthat patients who are at higher risk are more likely touse corticosteroids. Whether the new TNF inhibitorsincrease the risk of infection is a matter for debate
since the drugs have been associated with a change inthe spectrum of infections50 specifically, increasetuberculosis, histoplasmosis, and listeria.6
The clinician who is caring for patients withrheumatoid arthritis should be aware of the risk ofinfection. All patients should have yearly influenzavaccinations and should receive the pneumococcalvaccine at appropriate intervals. Since patients mayhave a better immunologic response to vaccinationbefore taking methotrexate51, it seems prudent tovaccinate before starting DMARD treatment, whenpossible. Live vaccines should be avoided in patientswho are receiving immunosuppressive medications.When considering TNF inhibitors, clinicians shouldrecommend that all patients be tested for priorexposure to tuberculosis. Both clinicians and patientswith rheumatoid arthritis should be vigilant withregard to avoiding infections and treating them earlyand aggressively. Stopping or withdrawing drugtreatment during infections is critical50.
The incidence of osteoporosis is doubled in patientswith rheumatoid arthritis52and baseline bone-densitystudies should be performed in all patients,particularly those who will receive corticosteroids. Ifosteoporosis is present, bisphosphonate therapy,which is reported to decrease the risk of fracture by70 percent despite the co administration ofcorticosteroids should be used19.
Cardiovascular disease accounts for most of theexcess mortality associated with rheumatoiddisease20. The newer concepts of the pathogenesis ofatherosclerosis suggest that inflammation is a keyfactor in causing vascular endothelial damage20. Ithas been hypothesized that the systemic inflammationthat characterizes rheumatoid arthritis may play a keyrole in the excess artherosclerosis seen in patientswith this disease20. Risk factors for atherosclerosisshould be aggressively soughted and addressed. Inparticular, smoking cessation may be fruitful, sincesmoking has been associated with increased severityof arthritis53. Current trials of statin therapy inpatients with rheumatoid arthritis may address therisk of cardiovascular disease, since statins shoulddecrease atherosclerosis and inflammation54.
Many of the new therapies are expensive, with initialcosts that may exceed $1,500 per month. However,
Journal of Bangladesh College of Physicians and Surgeons Vol. 28, No. 1, January 2010

37
these upfront costs may be justified in the long termby savings that result from an improved quality of lifeand enhanced productivity.
The treatment of rheumatoid arthritis has improveddramatically in the past decade7, 8. Thanks to earlydiagnosis and the availability of DMARDs.Physicians can now have the goal of eradicatingactive disease and aggressively intervening to addresscoexisting illnesses. Remission in patients who arereceiving therapy is now a realistic goal.
Summary and Conclusion:The treatment of rheumatoid arthritis has changeddramatically in the past decade due to improvedunderstanding of its pathophysiology and theavailability of DMARDS. Initiation of treatment veryearly in the disease (within three months), the use ofcombinations of DMARDs and emergences of anumber of new drugs (TNF-α antagonists, IL-1antagonist, anti CD20 antibody) that have novelmechanism of action have made it possible to achievecontrol of synovitis and improvement in the quality oflife in the majority of rheumatoid arthritis patients.Many of the new therapy are expensive, with initialcosts that may exceed £1500 per month. However,these upfront costs may be justified in the long termby savings that results from an improved quality oflife and enhanced productivity. Indeed, emergingclinical and epidemiological data suggest thatexcellent long term control of synovitis will result insignificant reduction in rate of unemployment, jointsurgeries, disability and mortality in rheumatoidarthritis patients. Complete remission of disease (ontherapy) should be the goal of treatment, even if notachievable, in all RA patients
Reference:1. Scott DL, Symmons DPM, Coulton BL, Popert AJ. Long-
term outcome of treating rheumatoid arthritis: results after20 years. Lancet 1987; 1:1108-11.
2. Gabriel SE. The epidemiology of rheumatoid arthritis.Rheum Dis Clin North Am 2001; 27: 269-81.
3. Symmons DP, Barrett EM, Bankhead CR, Scoott DG,Silman AJ. The incidence of rheumatoid arthritis in theUnited Kingdom: Results from the Norfolk ArthritisRegister. Br.J Rheumatol 1994; 33; 735-9.
4. Choy EHS, Panayi GS. Cytokine pathways and jointinflammation in rheumatoid arthritis. N Engl J Med 2001;344:907-16
5. Van der Heijde DM. Joint erosions and patients with earlyrheumatoid arthritis. Br J Rheumatol 1995; 34Suppl 2:74
6. Lard LR, Visser H, Speyer I. Early versus delayed treatmentin patients with recent onset rheumatoid arthritis:comparison of two cohorts who received different treatmentstrategies. AM J Med 2001; 11:445-51.
7. O’Dell JR. Treating rheumatoid arthritis early: a window ofopportunity. Arthritis Rheum 2002; 46:283-5.
8. Arnett FC, Edworthy SM, Bloch DA, Mc Shane DJ, FriesJF, Cooper NS et al. The American Rheumatism Association1988 revised criteria for the classification of rheumatoidarthritis. Arthritis Rheum 1988; 31:315-24.
9. Jansen ALMA, van der Horst-Bruinsma IE, vanSchaardenburg D, van de Stadt RJ, de Koning MHMT,Bijkmans BAC. Rheumatoid factor and antibodies to cycliccitrucllinated peptide differentiate rheumatoid arthritis fromundifferentiated polyarthritis in patients with early arthritis.J Rheumatol 2002; 29:2074-6.
10. Nielen MM, van Schaardenburg D, Reesink HW. Specificauto antibodies precede the symptoms of rheumatoidarthritis: a study of serial measurements in blood donors.Arthritis Rheum 2004, 50,380-6.
11. American College of Rheumatology Sub-committee onRheumatoid Arthritis Guidelines. Guidelines for themanagement of rheumatoid arthritis: 2002 update. ArthritisRheum 2002; 46:328-42.
12. Felson DT, Anderson JJ, Boers M. Preliminary definition ofimprovement in rheumatoid arthritis. Arthritis Rheum1995;38:727-35.
13. Singh G. Recent considerations in non-steroidal anti-inflammatory drug gastropathy. Am J Med 1998; 105: Suppl1B: 31S-38S.
14. Silverstein FE, Faich G, Goldstein. Gastrointestinal toxicitywith celecoxib vs nosteroidal anti-inflammatory drugs forosteoarthritis and rheumatoid arthritis: the CLASS study: arandomized controlled trial. JAMA 2000:284:1247-55.
15. Chan FKI, Hung LCT, Suen BY. Celecoxib versusdiclofenac and omeprazole in reducing the risk of recurrentulcer bleeding in patients with arthritis. N Engl J Med 2002;347:2104-10.
16. Stand V, Hochberg MC. The risk of cardiovascularthrombosis events with selective cyclooxygenase-2inhibitors. Arthritis Rheum 2002; 47:349-55.
17. Kirwan JR, Arthritis and Rheumatism Council Low-DoseGlucocorticoids on joint destruction in rheumatoid arthritis.N Engl J Med 1995; 333:142-6.
18. Van Everdingen AA, Jacobs JWG, Siewertsz van ResemaDR, Bijlsma WJ. Low dose prednisone therapy for patientswith early active rheumatoid arthritis; clinical efficacy,disease-modifying properties, and side effects: arandomized, double blind, placebo-controlled clinical trial.Ann Intern Med 2002; 135:1-12.
Medical Treatment of Rheumatoid Arthritis: A Review AHM Feroz
38
19. American College of Rheumatology Ad Hoc Committee onGlucocorticoid-Induced Osteoporosis. Recommendationsfor the prevention and treatment of Glucocorticoid inducedosteoporosis: 2001 update. Arthritis Rheum 2001; 44:1496-503.
20. Van Doorrnum S, McColl G, Wicks IP. Acceleratedatherosclerosis: an extraarticular feature of rheumatoidarthritis? Arthritis Rheum 2002; 46:862-73.
21. Felson DT, Anderson JJ, Meenan RF. The comparativeefficacy and toxicity of second-line drugs in rheumatoidarthritis; results of two metaanlyses. Arthritis Rheum 1990;33:1449-61.
22. Ortendahl M, Holmes T, Schettler JD, Fries JF. Themethotrexate therapeutic response in rheumatoid arthritis. JRheumatol 2002; 29:2084-91.
23. Choi HK, Hernán MA, Seeger JD, Robins JM, Wolfe F.Methotrexate and mortality in patients with rheumatoidarthritis: a prospective study. Lancet 2002; 359:1173-7.
24. Van Ede AE, Laan RF, Rood MJ. Effect of folic or folinicacid supplementation on the toxicity and efficacy ofmethotrexate in rheumatoid arthritis: a forty-eight week,multiceneter, randomized, doubleblind, placebo-controlledstudy. Arthritis Rheum 2001; 44:1515-24.
25. Genovese M, Keystone EC, Tesser JRP, Finck BK, Spencer-Green GT. High dose oral methotrexate (MTX) in early RAis needed for maximum efficacy. Arthritis Rheum 2000; 43:Suppl: S382.abstract.
26. Smolen JS, Kalden JR, Scott DL. Efficacy and safety ofleflunomide compared with placebo and sulphasalzine inactive rheumatoid arthritis: a double-blind randomizedmulticentre trial. Lancet 1999; 353:259-66.
27. Strand V, Cohen S, Schiff M. Treatment of activerheumatoid arthritis with leflunomide compared withplacebo and methotrexate. Arch Intern Med 1999;159:2542-250.
28. Rau R, Herborn G, Menninger H, Blechschmidt J.Comparison of intramuscular methotrexate and gold sodiumthiomalate in the treatment of early erosive rheumatoidarthritis: 12 month data of double-blind parallel study of174 patients. Br J Rheumatol 1997; 36:345-52.
29. American College of Rheumatology Adhoc Committee onClinical Guidelines. Guidelines for monitoring drug therapyin rheumatoid arthritis. Arthritis Rheum 1995; 39:723-31.
30. Kremer JM, Alarcon GS, Lightfoot RW Jr. Methotrexate forrheumatoid arthritis: suggested guidelines for monitoringliver toxicity. Arthritis Rheum 1994; 37:316-28.
31. Janssen NM, Genta MS. The effects of immunosuppressiveand anti-inflammatory medications on fertility, pregnancy,and lactation. Arch Intern Med 2000; 160:610-9.
32. Kremer JM, Alarcon GS, Weinblatt ME. Clinical,laboratory, radiographic, and histopathologic features ofmethotrexate- associated lung injury in patients with
rheumatoid arthritis: a multicenter study with literaturereview. Arthritis Rheum 1997; 40:1829-37.
33. Marmor MF, Carr RE, Easterbrook M, Farjo AA, MielerWF. Recommendations on screening for chloroquine andhydroxy-chloroquine retinopathy: a report by the AmericanAcademy of Ophthalmology. Ophthalmology 2002;109:1377-82.
34. Kloppenburg M, Breedveld FC, Terwiel JP, Mallee C,Kijkmans B.A. Minocycline in active rheumatoid arthritis:a double blind, placebo-controlled trial. Arthritis Rheum1994; 37:629-36.
35. O’Dell JR, Blakely KW, Mallek. Treatment of earlyseropositive rheumatoid arthritis: a two-year, double-blindcomparison of minocycline and hydroxychloroquine,Arthritis Rheum 2001; 44:2235-41.
36. Olsen NJ, Stein CM. New drugs for rheumatoid arthritis. NEngl J Med 2004; 350:2167-79.
37. O’Dell JR, Haire CE, Erikson N. Treatment of rheumatoidarthritis with methotrexate alone, sulfasalazine andhydroxychloropuine, or combination of all threemedications. N Engl J Med 1996; 334:1287-91.
38. O’Dell JR, Leff R, Paulsen G. Treatment of rheumatoidarthritis with methotrexate and hydroxychloropuine,methotrexate and sulfasalazine, or a combination of thethree medications: results of a two year, randomized, doubleblind, and placebocotrolled trial. Arthritis Rheum 2002;46:1164-70.
39. Boers M, Verhoeven AC, Markusse HM. Randomizedcomparison of combined step-down prednisolone,methotrexate and sulphasalazine with sulphasalazine alonein early rheumatoid arthritis. Lancet 1997; 350:309-18.[Erratum, Lancet 1998; 351:220.]
40. Mottonen T, Hannonen P, Leirisalo- Repo M. Comparisonof combination therapy with single-drug therapy in earlyrheumatoid arthritis: a randomized trial. Lancet 1999;3531568-73.
41. Landewe RBM, Boers M, Verhoever AC, Westhovens R,Vande Laar MA, Murkusse HM et al. COBRA combinationtherapy in patients with early rheumatoid arthritis:long-term structural benefits of a brief intervention. ArthritisRheum 2002; 46:347-56.
42. Edwards JCW, Szczepanski L, Szechin ski J, SosnowskaAF, Emery P, Close DR et al. Efficacy of B-cell-targetedtherapy with rituoximab in patients with rheumatoidarthritis. N Engl J Med 2004; 350:2572-81.
43. Mikuls TR, O’Dell JR. The changing face of rheumatoidarthritis therapy: results of serial surveys. Arthritis Rheum2002; 43: 464-5.
44. Bathon JM,Martin RW,Fleichmann RM. A comparison ofetanercept and methotrexate in patients with earlyrheumatoid arthritis. N Engl J Med 2000; 343:1586-1593.
Journal of Bangladesh College of Physicians and Surgeons Vol. 28, No. 1, January 2010
39
45. Sokka T, Pincus T. Eligibility of patients in routine care formajor clinical trials of anti-tumour necrosis factor alpha agentsin rheumatoid arthritis. Arthritis Rheum 2003;48:313-8
46. Mikuls TR, Saag KG. Comorbidity in rheumatoid arthritis.Rheum Dis Clin North AM 2001; 27: :283-303.
47. Doran MF, Crowson CS, Pond GR, O’Fallon WM, GabrielSE. Frequency of infection in patients with rheumatoidarthritis compared with controls: a population-based study.Arthritis Rheum 2002; 46:2287-93.
48. Wolfe F, Mitchell DM, Sibley JT. The mortality ofrheumatoid arthritis. Arthritis Rheum 1994; 37:481-94.
49. Doran MF, Crowson CS, Pond GR, O’ Fallon WM, GabrielSE. Predictors of infection in rheumatoid arthritis. ArthritisRheum 2002; 46:2294-300
50. Ellerin T, Rubin RH, Weinblatt ME. Infections and anti-tumor necrosis factor α therapy. Arthritis Rheum2003:48:3013-22.
51. O’Dell JR. Gilg J, Palmer W, Haire C, Klassen L, Moore G.Pneumococcal vaccine in rheumatoid arthritis: decreasedresponse while taking methotrexate. J Clin Rheumatol 1996;2:59-63.
52. Haugeberg G, Orstavik Re, Uhlig T, Falch JA, Halse JI,Kvien TK. Bone loss in patients with rheumatoid arthritis:results from a populations-based cohort of 366 patientsfollowed up for two years. Arthritis Rheum 2002; 46:1720-8.
53. Mattey DL, Hutchinson D, Dawes PT. Smoking and diseaseseverity in rheumatoid arthritis: association withpolymorphism at the glutathione S-transferase M 1 locus.Arthritis Rheum 2002; 46:640-6.
54. Leung BP, Sattar N, Crilly A. A novel anti-inflammatoryrole for simvastatin in inflammatory arthritis. J Immunol2003; 170: 1524-30.
Medical Treatment of Rheumatoid Arthritis: A Review AHM Feroz
Introduction:Infertility is thought to affect 10 to 15% of couplesbut this percentage may be an underestimate1,2. Theinability to conceive carries a hidden stigma of shameand secrecy for some couples, whereas others arenever enumerated because they cannot afford to seekmedical treatment3. Failure to seek management,investigation and treatment compounds the tragedy ofinfertility because simple, inexpensive therapeuticoptions may be appropriate for anovulatory infertilityor even in expectant management of unexplainedinfertility. In a study on rural population of
Bangladesh, 3.2% of married women of reproductiveage have primary infertility and 3% have secondaryinfertility4. Majority of infertile women (40%)believed this to be their fate and 33% accusedthemselves for infertility4.
In a review, Homberg and Insler5 concluded thattaking into account efficacy, complication rates andcost of infertility treatment, women withhypogonadotrophic hypogonadism or polycysticovary syndrome(PCOS) should be offered acceptablemethods of ovulation induction and that couples with‘unexplained’ or ‘multifactorial subfertility’ shouldbe exposed to controlled ovarian hyperstimulationwith intrauterine insemination and only after thefailure of these therapies should be offered in vitrofertilization(IVF).
Ovulatory dysfunction is one of the most commoncauses for reproductive difficulty in otherwise fertilecouples. Once successful ovulation is achieved,fertility is often restored. Ovarian stimulation duringinfertility treatment is used either alone or inconjunction with intrauterine insemination andassisted reproductive technologies. At present, thetwo main medications used for induction of ovulationinclude an oral antiestrogen, such as clomiphenecitrate (CC), and an injectable gonadotropins,
Journal of Bangladesh College of Physicians and SurgeonsVol. 28, No. 1, January 2010
Aromatase Inhibitors: New Drug of Choicefor Induction of Ovulation
M SIDDIQUIa, N MAHMUDb, MR BEGUMc, T A CHOWDHURYd
Summary:Anovulation accounts for around 20% cases of infertilityeven when other fertility factors are normal. ClomipheneCitrate (CC), the oral anti-estrogen has long been used asthe first line drug for induction of ovulation. Clomipheneis associated with a high ovulation (60-80%) but relativelypoor pregnancy rate (30-40%). CC leads to long lastingestrogen receptor depletion. Because of its long half-life(2 weeks), CC possibly exerts a negative feedback effect onthe cervical mucous and endometrial development withsubsequent implantation failure. The aromatase inhibitorletrozole (originally approved for use in postmenopausalwomen with breast cancer to suppress estrogen
production) is now increasingly being used by fertilityspecialists worldwide for ovulation induction. With a half-life of around 45 hours, letrozole possibly avoids theadverse effects of CC on endometrium. Preliminary trialshave shown impressive prospects of aromatase inhibitorletrozole for induction of ovulation (even in CC resistantcases) with satisfactory pregnancy rates. Letrozole is nowbeing marketed by our local pharmaceutical companies.Though large scale randomized controlled trials are notyet available, letrozole holds a very promising chance ofreplacing CC in near future.
(J Bangladesh Coll Phys Surg 2010; 28: 40-44)
a. Dr.Maruf Siddiqui, FCPS, Junior Consultant (Obstetrics &Gynaecology), OSD, DGHS, Deputed to MS, BIRDEM
b. Dr.Nusrat Mahmud, MSc(Singapore), Junior Consultant(Infertility), Centre for Assisted Reproduction (CARE),BIRDEM
c. Dr.Mosammat Rashida Begum, FCPS, MS, MSc(ART,UK),Assistant Professor of Obstetrics & Gynaecology, DMCH
d. Professor T A Chowdhury, FRCS, FRCOG, FRCP, FCPS(B),FCPS(P), Professor & Head of the Department of Obstetrics& Gynaecology, BIRDEM
Address of Correspondence: Dr.Maruf Siddiqui, JuniorConsultant (OBGYN), OSD, DGHS, Deputed to MS, BIRDEM,Apt # A1, Oriental Tower-1, 1/G/1, Paribagh, Dhaka-1000, Tel:9675555, Cell: 01711 593978, E-mail: [email protected]
Received: 19 September, 2008 Accepted: 12 January, 2009

41
predominantly recombinant follicle stimulatinghormone (FSH)6-9. In specific situations, there areother less frequently used treatments to induce orrestore ovulation, such as pulsatile administration ofgonadotropin-releasing hormone (GnRH) for womenwith hypothalamic anovulation10, dopaminargicagonists for women with hyperprolactinemicanovulation11,12 and insulin sensitizers for womenwith PCOS13.
Both clomiphene citrate(CC) and gonadotropins areassociated with various disadvantages that includerisk of life threatening ovarian hyperstimulationsyndrome, high order multiple pregnancy, lowerpregnancy rate despite high ovulatory rate (especiallyfor clomiphene citrate) and high expenses withparenteral administration requiring intensivemonitoring (FSH treatment)14.
Clomiphene citrate (CC) is the most commonly useddrug for the induction and augmentation of ovulation.However 20-25% women are resistant to clomiphenecitrate14. In addition, clinical data reveal adiscrepancy between ovulation and conception ratesbetween CC treatment, and a higher than expectedincidence of miscarriage in conception cycles. Theseobservations have been attributed to the peripheralanti-estrogenic mechanism of action of CC thatinvolves long lasting estrogen receptor depletion inthe endometrium and cervix14.
In spite of high ovulation rate, clomiphene isassociated with low pregnancy rate with resistance to20-25% 0f women. In CC failures, expensivegonadotropin injections are the next treatment optionbut, especially in polycystic ovary syndrome, areassociated with increased risk of ovarianhyperstimulation requiring intensive monitoring. So,obviously a cheap oral agent is preferred that caninduce ovulation in resistant cases without extensivemonitoring and having less side effects on theendometrium.
Letrozole : The aromatase inhibitorMode of Action
Letrozole belongs to a new group of very potent, non-steroidal, selective reversible third generationaromatase inhibitor developed for postmenopausalbreast cancer therapy14. Letrozole inhibits the
conversion of adrenally generated androstenedione toestrone or estradiol by aromatase enzyme inperipheral tissues. It acts by competitive binding tothe haem of cytochrome P450 subunit of thearomatase enzyme and interrupts the metabolism ofestrogen resulting in a decrease level of estrogen inthe body. As a negative feedback mechanism, thepituitary gland produces follicle stimulating hormone(FSH) leading to ovulation or superovulation.Therefore, letrozole generally mimics the action ofCC without depletion of estrogen receptors whenadministered early in the menstrual cycle14. Becauseof the much shorter life span (2 days) and absence ofestrogen receptor binding, it possibly avoids theantiestrogenic effects associated with CC14.
Metabolism and side effects
Letrozole has no significant active metabolites. It iscompletely absorbed after oral administration and hasa mean terminal half-life of 45 hours (range 30-60hours). It is cleared from the systemic circulationmainly by the liver.
Letrozole generally is well tolerated; the mostcommon treatment-related adverse effects are hotflushes, nausea, and hair thinning. In the trial ofextended adjuvant therapy, adverse events reportedmore frequently with letrozole than placebo were hotflushes, arthralgia, myalgia and arthritis, butcessation of letrozole was no more frequent thanplacebo in this double-blind trial. A greater number ofnew diagnosis of osteoporosis occurred amongwomen receiving letrozole, but the long term effectson bone mineral density or lipid metabolism are yet tobe determined.
Is it teratogenic?
Over the recent years, letrozole has been studied atthe University of Toronto as a fertility drug withsatisfying results15. Their studies found that the drugappears to be completely eliminated from the bodywithin a few days of the last tablet. So far there is noevidence that this drug has any harmful effects on thedeveloping fetus. It therefore appears to be safe as afertility drug.
In 2005, some concern was raised as a result of anabstract of a study that compared 150 babies born towomen who had used letrozole with 36,005 babies
Aromatase Inhibitors: New Drug of Choice for Induction of Ovulation M Siddiqui et al.

42
born to low-risk pregnant women16. The results ofthis study, which had several gross methodologicaldrawbacks, suggested that letrozole might increasethe risk of cardiac and bone anomalies16. Since thatinitial report, however, several full-length studieshave not shown an increased risk for congenitalmalformations following the use of letrozole toinduce ovulation. A study published in 2006examined 514 babies born to mother who had usedletrozole to conceive, and compared them with 397babies born to mothers who had conceived usingclomiphene citrate17. There were no increased ratesof major and minor malformations beyond whatwould be expected in the general population (1-3%)17. Additionally, the number of cardiac anomaliesin the letrozole group (0.2%) was slightly lower thanthat of the general population17.
Letrozole is approved by the United States Food andDrug Administration (FDA) for the treatment of localor metastatic breast cancer that is hormone receptorpositive in postmenopausal women. Infertilityspecialists have been using this drug for ovulationinduction since 2001. However, like many otherdrugs (eg.misoprostol), induction of ovulation byletrozole is an ‘off-label’ indication because it is notmarketed for use as a fertility drug15.
Recent Studies on letrozoleOver the last few years, several published studies,both controlled and noncontrolled, comparedclomiphene citrate and letrozole, either alone or incombination with gonadotropins, for ovulationinduction or augmentation18.These studies foundletrozole as effective as clomiphene in inducingovulation, with the major advantage of absence of anyanti-estrogenic adverse effects. Patients treated withletrozole demonstrated low estrogen production perdeveloping follicle resulting in more physiologicalestrogen levels around the time of ovulation and goodpregnancy rates with a lower incidence of multiplepregnancies than with clomiphene18. When combinedwith gonadotropins, letrozole reduces the dose ofgonadotropins required for optimal follicularrecruirment and improve the response togonadotropin stimulation in poor responders19.However, a recent study involving 438 PCOS patientsdid not show any advantage of letrozole over CC as a
first line treatment for induction of ovulation inPCOS patients20. A group of Turkish researchersconcluded that letrozole and CC have comparableeffectiveness in ovulatory patients with unexplainedinfertility21. A small study involving 22 patients fromthe University of Toronto showed the supremacy ofletrozole in ovulation induction in patients with aninadequate response to Clomiphene citrate22. Thishypothesis is supported by another study in a tertiatyreferral infertility clinic at Dhaka involving 35infertile patients non responsive to CC which showeda high success rate (77.77%) for folliculardevelopment using letrozole23. Another survey alsoreported a successful induction (62%) in PCOSpatients using letrozole previously treated withClomiphene citrate24. Researchers from a universityhospital in Greece concluded that ovulation inductionwith letrozole is associated with acceptable successrate compared with gonadotropin with significant lesscost, risks and patient inconvenience25. In patientswho failed to conceive with CC, gonadotrophins havea higher pregnancy rate for ovulation induction thanletrozole26. However, pregnancy rates were highenough with letrozole to justify its use26. Comparedto CC in gonadotrophin combined IntrauterineInsemination (IUI) cycles, number of mature folliclesand serum estradiol levels on the day of hCG weresignificantly lower in the letrozole group. Nosignificant differences were found in endometrialthickness measured on the day of hCG but thepregnancy rate was higher in letrozole group27.Comparing the endocrinological environment,significantly lower estradiol concentrations and fewerfollicles were observed in cycles stimulated with 2.5mg letrozole compared to 100 mg of CC from day 3to day 7 of the cycle28. However, the administrationof 50 mg CC was found superior to 2.5 mg letrozolefor superovulation induction in Asian women withnormal ovulation29. Similar to CC, aromataseinhibition by letrozole reduces FSH dose required forcontrolled ovarian hyperstimulation (COH) withoutthe undesirable antiestrogenic effects sometimes seenwith CC29. Letrozole appears to constitute a goodalternative to CC in patients with unexplainedinfertility undergoing gonadotrophin stimulated COHcycles combined with IUI therapy30. It also seems tobe an acceptable alternative to CC as an ovulation
Journal of Bangladesh College of Physicians and Surgeons Vol. 28, No. 1, January 2010

43
inducing agent in patients with PCOS31. The thirdgeneration aromatase inhibitor letrozole is aseffective as or superior to CC in ovulation inductionand in superovulation32. Unlike CC, they do not carryan antiestrogenic effect on the endometrium32.Letrozole blocks estrogen production, not estrogenreceptors, and would therefore be expected toproduce superior conception rates and less multiplepregnancies33. Letrozole has got better ovulation andpregnancy rate in comparison to clomiphene citrate inpatients with PCOS34. It also seems to be an effectivealternative as a low-cost IVF protocol in women withpoor response to gonadotrophins35. Letrozole is yet toundergo further large, robust clinical trials in order tofulfill these promises as a feasible alternative to CC inthis role, but some preliminary trials have shown atleast equality and some superiority.
ConclusionClinical utilization of ovarian stimulation to facilitatethe ability of a couple to conceive has not onlyprovided a valuable therapeutic approach, but hasalso yielded extensive information on the physiologyof ovarian follicular recruitment, endometrialreceptivity and early embryo competency. For the last40 years, the first line of treatment for induction ofovulation has been clomiphene citrate. It is a safe,cheap oral agent but is known to have relativelycommon antiestrogenic endometrial and cervicalmucous side effects that could prevent pregnancy inthe face of successful ovulation. Infertility specialistshave been increasingly using letrozole for induction.Because of the recent acceptance of the concept ofusing aromatase inhibitors for ovulation induction, afew small controlled studies were identified, and therest were pilot or preliminary comparisons. Based onthese studies, it appears that aromatase inhibitorletrozole is as effective as clomiphene in inducingovulation, results in lower serum estrogenconcentrations, and is associated with a goodpregnancy rate with a lower incidence of multiplepregnancies than clomiphene citrate. Letrozolereduces the dose of FSH required for optimalfollicular recruitment and improves the response toFSH in poor responders. So, preliminary evidence issuggesting that letrozole may replace clomiphenecitrate in the future because of similar efficacy with a
reduced side effect profile. Although worldwideexperience with letrozole for ovulation induction isincreasing, at present, definitive large scale studies inthe form of randomized controlled trials comparingclomiphene citrate with letrozole are lacking.
References:1. Whiteford LM, Gonzalez L. Stigma: the hidden burden of
infertility. Soc Sci Med 1995;40:27-36
2. Downey J, Yingling S, McKinney M, Husami N. Mooddisorders, psychistric symptoms and distress in womenpresenting for infertility evaluation. Fertil Steril1989;52:425-432
3. Schroeder P. Infertility and the world outside. Fertil Steril1988;49:765-767
4. Bangladesh Institute of Research in Promotion of Essentialand Reproductive Health & Technologies (BIRPERHT).Assessment of Reproductive Health Care and ReviewServices provided at the level of Thana, Union and Villages.August 1997 issue, vol-5
5. Hommburg R, Insler V. Ovulation Induction in perspective.Hum Reprod Update 2002;8:449-462
6. Melis GB, Paoletti AM, Strigini F, et al. Pharmacologicinduction of Multiple follicular development improves thesuccess rate of IUI in inexplained infertility. Fertil Steril1987;47:441-445
7. Serhal PF, Katz M, Little V, Woronowski H. Uuexplainedinfertility: the value of pergonal superovulation combinedwith intrauterine insemination. Fertil Steril 1988;49:602-606
8. Melis GB, Strigini F, Meis V, et al. Critical reappraisal of theclinical effectiveness of different methods of assistedfertilization. J Endocrinol Invest 1990;13:263-274
9. Franks S. Polycystic ovary syndrome. N Engl J Med1995;333:853-861
10. Gomped A, Mauvais Jervis P. Induction of ovulation withpulsatile GnRH in hypothalamic amennorhoea. HumReprod 1988;3:473-477
11. Lin SG, Gu CX, Xu L, et al. Experience with bromocriptinefor the treatment of female infertility due tohyperprolactinemia. Chin Med J (Eng) 1991;104:679-684
12. The ESHRE Capri workshop. Female infertility: treatmentoptions for complicated cases. Hum Reprod 1997;12:1191-1196
13. Nestler JE, Stovall D, Akhter N, et al. Strategies for the useof insulin sensitizing drug to treat infertility in women withpolycystic ovary syndrome. Fertil Steril 2002;77:209-215
14. Casper RF. Aromatase inhibitors: New experiments or newvalue. Updates in Infertility treatment 2004 Seminar inFlorida 22-24 January
Aromatase Inhibitors: New Drug of Choice for Induction of Ovulation M Siddiqui et al.
44
15. Hudson Stephen. Infosheet: Letrozole . Victoria FertilityCentre. #207-4400 Chatterton way Victoria BC.www.victoriafertility.com
16. Biljan MM, Hemmings R, Brassand N. The outcome of 150babies following the treatment with letrozole or letrozoleand gonadotropins. Fertil Steril 2005;84:S95
17. Tulandi T, Martin J, Al-Fadhli R, Kabli N, Forman R,Hitkari J, et al. Fetal safety of letrozole and clomiphenecitrate for ovulation induction. J Obstet Gynaecol Can2007;29(8):668-71
18. Mitwally MF, Casper RF. Potential of aromatase inhibitorsfor ovulation and superovulation induction in infertilewomen. Drugs 2006;66(17):2149-60
19. Mitwally MF, Casper RF. Aromatase inhibition improvesovarian response to follicle-stimulating hormone in poorresponders. Fertil Steril 2002 April; 77(4):776-80
20. Badawy A, Abdel Aal I, Abulatta M. Clomiphene citrate orletrozol for ovulation induction in women with polycysticovary syndrome: a prospective randomized trial. Fertil Steril2007 Jun 18
21. Bayar U, Tanriverdi HA, Barut A, Ayoglu F, Ozcan O, KayaE. Letrozole vs clomiphene citrate in patients with ovulatoryinfertility. Fertil Steril 2006 Apr; 85(4):1045-48
22. Mitwally MF, Casper RF. Use of an aromatase inhibitor forinduction of ovulation in patients with an inadequateresponse to clomiphene citrate. Fertil Steril 2001Feb;75(2):305-309
23. Begum MR, Quadir E, Begum A, Begum RA, Begum M.Role of aromatase inhibitor in ovulation induction inpatients with poor response to clomiphene citrate. J ObstetGynaecol Res 2006 Oct;32(5):502-506
24. Badawy A, Mosbah A, Shady M. Anastrozole or letrozolefor ovulation induction in clomiphene resistant women withpolycystic ovary syndrome: a prospective randomized trial.Fertil Steril 2007 Aug 7
25. Gregoriou O, Viahos NF, Konidaris S, Papadis K, Botsis D,Creatsas GK. Randomized controlled trial comparingsuperovulation with letrozole versus recombinant follicle-stimulating hormone combined to intrauterine inseminationfor couples with unexplained infertility who had failedclomiphene citrate stimulation and intrauterine stimulation.Fertile Steril 2007 Oct 23
26. Quintero RB, Urban R, Lathi RB, Westphal LM, DahanMH. A comparison of letrozole to gonadotrophins forovulation induction, in subjects who failed to conceive withclomiphene citrate. Fertil steril 2007 Oct;88(4):879-85
27. Jee BC, Ku SY, Suh CS, Kim KC, Lee WD, Kim SH. Useof letrozole versus clomiphene citrate combined with
gonadotropins in intrauterine insemination cycles: a pilotstudy. Fertil Steril 2006 Jun;85(6):1774-7
28. Fatemi HM, Kolibianakis E, tournaye H, Camus m,Steirtegham Van AC, Devroy P. Clomiphene citrate versusletrozole for ovarian stimulation: a pilot study. ReprodBiomed Online 2003 Nov;7(5):543-546
29. Topipat C, Choktanasiri W, Jultanmas R, Weerakiet S,Wongkularb A, Rojanasakul A. A comparison of the effectsof clomiphene citrate and the aromatase inhibitor letrozoleon superovulation in Asian women with normal ovulatorycycles. Gynecol Endocrinol 2008 Mar;24(3):145-50
30. Noriega-Portella L, Noriega-Hoces L, Delgado A, Rubio J,Gonzales GF. Effect of letrozole at 2.5mg or 5.0mg/day onovarian stimulation with gonadotropins in womenundergoing intrauterine insemination. Fertil Steril 2007 Dec14
31. Bayar U, Basaran M, Kiran S, Coskun A, Gezwe S: Use ofan aromatase inhibitor in patients with polycystic ovarysyndrome: a prospective randomized trial. Fertil Steril 2006Nov;86(5):1447-51
32. Holzer H, Casper R, Tulandi T. A new era in ovulationinduction. Fertil Steril 2006 Feb;85(2):277-84
33. Homburg R. Oral agents for ovulation induction-clomiphene citrate vs aromatase inhibitors. Hum Fertil(Camb) 2008 Mar;11(1): 17-22
34. Begum MR, Begum A, Quadir E. Comparison of efficacy ofaromatase inhibitor and clomiphene citrate in induction ofovulation in polycystic ovary syndrome. Fertil SterilJanuary 2008
35. Chakravarty BN, Goswami SK, Das T, Chattopadhyay R,Sawhney V, Kumar J, Chaudhury K, Kabir SN. Arandomized single-blind controlled trial of letrozole as alow-cost IVF protocol in women with poor ovarianresponse: a preliminary report. Human Reproduction 200419(9):2031-35
36. Casper RF, Mitwally MF. Review: aromatase inhibitors forovulation induction. J Clin Endocrinol Metab 2006Mar;91(3):760-71
37. Mitwally MF, Casper RF. Aromatase inhibitors in ovulationinduction. Semin Reprod Med 2004 Feb;22(1):61-78
38. Al-Fozan H, Al-Khadouri M, Tan SL, Tulandi T. Arandomized trial of letrozole versus clomiphene citrate inwomen undergoing superovulation. Fertil Steril 2004Dec;82(6):1561-3
39. Mitwally MF, Casper RF. Aromatase inhibitors for thetreatment of infertility. Expert Opin Investig Drugs 2003Mar;12(3);353-71
Journal of Bangladesh College of Physicians and Surgeons Vol. 28, No. 1, January 2010
IntroductionRuptured uterus is an unexpected, relativelyuncommon occurrence in the general obstetricpopulation and rare in developed country, butunfortunately it is common in a developing countrylike Bangladesh. It is one of the major obstetricemergencies, it carries high incidence of maternal andfoetal mortality and morbidity1.
According to UNFPA (2002), the estimated lifetimerisk of dying from pregnancy and childbirth relatedcauses in Bangladesh is 1 in 21, compared to 1 in over4,000 in industrialized countries2. The World Bank,however, currently estimates the national MMR at440 per 100,000 live births3. Bangladesh is one of thepoorest countries in the world, with a maternalmortality ratio of 320/100,000 live births (NIPORT2001) 4 . One of the causes of maternal mortality isruptured uterus. Rupture uterus and obstructed labour(indirectly causes rupture in neglected cases)constituted about 19% of maternal death1.
Most of the labours in our country are conducted byuntrained dais (traditional birth attendants). They do
not have enough knowledge and background tounderstand the presentation, lie, and position of thefoetus. Also they can not asses state of maternalcondition such as uterine contraction and progress oflabour. Above all, due to illiteracy and low socio-economic condition and conservative religious belief,most of our pregnant mothers are deprived of properantenatal care that is available. Majority of poorwomen deliver at home unattended by doctor andattended by dais. They seek medical help only whena woman fails to deliver after a long time at home orwhen there is serious deterioration in her condition.Often there is delay in every step from decisionmaking to final hospital management.
Rupture of uterus in multigravidae during labour iswell-documented complication but rupture ofunscarred uterus is uncommon event and in theprimigravidae it extremely rare. But in a tertiaryreferral hospital it is sometime seen. Here four casesof ruptured uterus in primiparous patients describedall of these cases were admitted in Obstetrics unit ofDhaka Medical College hospital (DMCH) which isone of the biggest tertiary referral hospital located inDhaka city. These cases are due to injudicious use ofoxytocin, obstructed labour due to hydrocephalus,cephalopelvic disproportion due to maternalkyphoscoliosis and road traffic accident in a patient inthird trimester of pregnancy.
Case-1:A 22year primigravid lady married for two years atfull term pregnancy was admitted in labour ward withsevere abdominal pain and per vaginal blood stained
Ruptured Uterus in Primiparous WomenIP ALAMa, H AFROZb
Summary:Ruptured uterus is rare in developed country, butunfortunately it is common in a developing country likeBangladesh. It is one of the major obstetric emergencies.Rupture of unscarred uterus is uncommon event. Majority ofthe patients are multigravidae and in primipara it extremelyrare. But in a tertiary referral hospital it is sometime seen.Four cases of ruptured uterus in primiparous patients are
described. These patients were admitted as emergency casesin obstetrics and gynaecology department of Dhaka MedicalCollege Hospital during the period 2000 –2001. These aredue to injudicious use of oxytocin, obstructed labour due tohydrocephalus,cephalopelvic disproportion due to maternalkyphoscoliosis and road traffic accident in third trimester ofpregnancy.
(J Bangladesh Coll Phys Surg 2010; 28: 45-48)
CASE REPORTS
a. Dr. Irin Parveen Alam. FCPS (Obst&Gynae), Juniorconsultant (Obst and Gynae)
b. Dr. Hasina Afroz.MS, FCPS,MCPS (Obst&Gynae) ,Assistant Professor (Obst&Gynae) Dhaka Medical CollegeHospital .
Dhaka Medical College Hospital .
Address of Correspondence : Dr.Irin Parveen Alam. 64/AHossaini Dalan Road, Johora Bhavan, Dhaka. E- [email protected].
Received: 22 August, 2007 Accepted: 6 August, 2009

46
discharge for two hours. She was in regular antenatalcheckup by a renowned gynaecologist in Dhaka cityin her antenatal period and she was immunized. Butat the onset of labour pain in the absence of patient’shusband her mother in law instead of transferring herto hospital called a dai and she gave one ampoule ofintramuscular injection of oxytocin directly. Patientspain increased but delivery not occurred, shecounseled the patients attendant that they often dosuch and delivery usually occur then again anotheroxytocin injection was given intramuscularly. Butdelivery not occurred in spite of presence of severeabdominal pain. Patient’s condition was deterioratingand decided to transfer her to hospital. Patient wastransferred to a nearby clinic but they referred her toDhaka Medical college Hospital. Patient was pale andanxious. On examination she was severely anaemicher pulse rate was 100/min and blood pressure was90/60mmof Hg. she could not lie down and sheprefers to sit in bed. Patient did not allow touchingher abdomen due to pain. So per-abdominal andpervaginal examination could not performedproperly, and the patient was diagnosed clinically as acase of rupture uterus. Resuscitation was done byopening two intravenous channels, giving oxygen byfacemask. Urgent laparotomy was done afterarrangement of blood transfusion. After openingabdomen there was haemoperitoneum of about 4liters and the foetus was dead and found outside theuterus, the rupture was on the posterior wall and veryirregular in type, it was repaired with difficulty.Subsequent postoperative period was uneventful andpatient discharged.
Case-2:A 24years old primiparos woman admitted withlabour pain. She was never in antenatal check up andnot immunized and could not mention duration ofpregnancy. On examination her pulsewas110/minutes blood pressure was 90/60mmof hgrespiratory rate was 26per minute and she wasmoderately anaemic. Per abdominal examinationrevealed fundal height about 36weeks with alongitudinal lie and contour of uterus was normal,foetal heart sound could not detect. Pervaginalexamination revealed a full-dilated cervix with a bigsoft caput with station high up. Clinical diagnosis ofobstructed labour was made with suspected ruptured
uterus. Only blood grouping and Rh typing was donefor emergency blood transfusion. Emergencylaparotomy was done and found that there washaemoperitoneum and rupture of anterior wall ofuterus, which extended downwards up to vaginalvault. Foetus was in utero and a big hydrocephalusfoetus was delivered, which was not diagnosedpreviously. Uterus was repaired in two layersabdomen was close after keeping a drain. Subsequentpostoperative period was uneventful and patientdischarged at 8th postoperative day.
Case-3:A 25year old poor woman short stature emaciatedpatient at her term pregnancy admitted in labour wardwith abdominal pain and parvaginal bleeding. Shewas married for 4 years with no issue. She was neverin antenatal check up. She had kyphoscoliosis ofthorax her pelvis was deformed and scoliotic in type,fundal height was of 36 weeks, abdomen was tenderand rigid foetal heart sound was absent andpervaginal examination shows irregular cervix ofabout of 4cm, cephalic presentation with high uphead. pervaginl bleeding was present. Her skeletaldeformity was such that she could not lie downproperly even after anaesthesia and her knee jointspersist always in flexed position. Emergencycaesarian section was done due to contracted pelvisand found that uterus was ruptured irregularly inanterior wall. Uterine bleeding continued and thepatient ultimately required a subtotal hysterectomydue to postpartum haemorrhage. Postoperative periodwas uneventful, the patient discharged home at 9th
postoperative day.
Case: 4A 25 years old primigravidae patient at her 37weekspregnancy was traveling in rickshaw and suddenlyroad traffic accident occurred and she was brought inlabour emergency room. She had severe abdominalpain; she was restless and developed shock withinshort time. She was diagnosed as a case of internalhaemorrhage. Resuscitation and arrangement ofemergency laparotomy was done under generalanesthesia. Operative findings revealed a largehaemoperitoneum (about 4000ml bloody ascitis inperitoneal cavity) and the foetus was floating in theperitoneal cavity. After urgent delivery of the foetus
Journal of Bangladesh College of Physicians and Surgeons Vol. 28, No. 1, January 2010

47
from the abdominal cavity about 8cm irregularlaceration was found on the posterior uterine wallextending from upper to lower segment. Placenta wasin fundal area and delivered. Foetus was freshstillborn. Primary repair of uterus was done. Afterappropriate treatment mother was discharged on 10th
postoperative day.
Discussion:It is well known that women who have previousgynaecological operations resulting in scarred uterusare at high risk for uterine in pregnancy; theoccurance is often intrapartum. Therefore closeobservation and followup during the labour areemphasized in these patients5. Uterine ruptureaccounts for significant number of maternal death indeveloping countries but it is also increasing indeveloped countries due to vaginal birth aftercaesarian delivery. The incidence of rupture of graviduterus in DMCH is 0.85% of total admission 6. In astudy in Sir Salimullah Medical College and MitfordHospital (SSMC&H) was 1 in 104.4 deliveries1,another study performed in SSMC between 1986-1988 showed that there was one ruptured uterus per102 hospital deliveries7. But in those studies therewas no rupture in primiparous patient. In literaturereview shows an oxytocin associated rupture inunscarred uterus in second stage of labour8. In a casereport there was a spontaneous fundal rupturesecondary to placenta percreta that necessitatedperforming a total abdominal hysterectomy 9,10.Another case report describes a rupture in aprimigravid patient who was at 38weeks’ gestationundergoing labour induction under epiduralanalgesia. The patient was diagnosed as a rupturecase in the post delivery period subsequentlydeveloped dissiminated intravascular coagulation andultimately required a hysterectomy8. However therehave been a few case reports of spontaneous uterinerupture, without significant risk factors 11,12 . In thepresented 4case reports two cases were diagnosed asobstructed labour. Obstructed labour for a prolongedperiod caused rupture in these cases. The patientswere primigravidae and had no congenital anomaly ofuterus or placental abnormality. The placenta waseasily removed from the fundal area; the placenta didnot invade the rupture site as established after carefulexamination of the uterus and the observation that it
was grossly normal. In the reported case,histopathology was not done, so any possibility ofunderlying pathological changes could not exclude.
The incidence of ruptured uterus is reflection of thelevel of health care delivery service available in acommunity. Now a day’s rupture of uterus in labourin women with history of previous caesarian sectionrecognized as an important factor. Multiparity withobstructed labour also recognized as importantcommon factor. In this case report all of the ruptureduterus patient came in hospital in the terminal stage,all of the cases occurred during labour, there wasintrauterine death of all the foetus before admission.All the patients except the patient with road trafficaccident, never sought antenatal advice, they are alsosocioeconomically deprived.
Conclusion:It is obvious that lack of adequate antenatal care, lackof community awareness, illiteracy, poor referralsystem and poverty are predisposing factors foruterine rupture. Spontaneous rupture of theprimigravid uterus can occur in the absence of ahistory of uterine trauma or infection rarely. If agravid woman presents with hypotension, abdominalpain and fetal distress, the differential diagnosisshould include rupture of the uterus. Rapid diagnosis,blood product replacement and emergencylaparotomy are the key steps in successfulmanagement. By reviewing the case reports, weshould keep in mind that prompt response to everywoman during labour is of paramount importance toavoid repeating the occurrence of uterine rupture.
Acknowledgement :I acknowledge Professor Sayeba Akhter, ProfessorAtika Begum, Dr. Salma Rouf ,Assistant Professor(Obst &Gynae).
References:1. A Begum. Ruptured Uterus-A Study of 32 Cases.
Bangladesh J Obstet Gynaecol, 1997; Vol 12 (1):29-35.
2. Maternal Mortality Statistics by Region and by Country.UNFPA Website,`accessed15/08/2002:http://www.unfpa.org/rh/mothers/statsbycountry.htmUNFPA (2002).
3. Attacking Poverty. Oxford: Oxford University Press for theWorld Bank. World Development Report 2000/2001.
Ruptured Uterus in Primiparous Women IP Alam & H Afroz

48
4. “Bangladesh Maternal Health Services and MaternalMortality Survey.” Final report. Calverton, Md.: ORCMacro Calverton. NIPORT (National Institute ofPopulations Research and Training). 2001.
5. Wang P H, Yuan C C, Taichao H, Yang M and Ng H T. Casereport. Posterior uterine wall rupture during labour.Human Reproduction Volm.15 no.5pp.1198-1199,2000.
6. S Rouf, N Nasrin, J Begum, MR Begum, S nahar, A Begum.Emergency Peripartum Hysterectomy- in a DevelopingCountry. J Bangladesh Coll Phys Surg 2002; 20:68-75.
7. Nessa A(1990) Rupture uterus: A study of 46 casesObstetrics and Gynaecological case records andcommentaries for MRCOG examination 1990;276.
8. Catanzarite V, Cousins L, Dowling D, and Daneshmand S,Case report Oxytocin-Associated Rupture of an Unscarred
Uterus in a Primigravida. Obstetrics & Gynecology2006;108:723-725
9. Imseis HM, Murtha AP, Alexander KA, Barnett BDSpontaneous rupture of a primigravid uterus secondary toplacenta percreta. A case report. J Reprod Med. 1998Mar;43(3):233-6.
10. Nagy, P.S. (1989) Placenta Percreta induced uterine ruptureand resulted in intraabdominal abortion. Am J. Obstet.Gynecol.,161, 1185-1186.
11. Langton J, Fishwick K. Kumar B.and Norosu,E.C.(1997)Spontaneous rupture of Unscarred gravid uterus at 32 weeksgestation. Hum Reprod. 12.2066-2067.
12. Wang P H,Chao H.T, L.L.and Yuan, C.C,(1999). Primaryrepair for corneal rupture occurred in a 21-gestational weekspregnant woman. Hum. Reprod. 14, 1894-1895.
Journal of Bangladesh College of Physicians and Surgeons Vol. 28, No. 1, January 2010
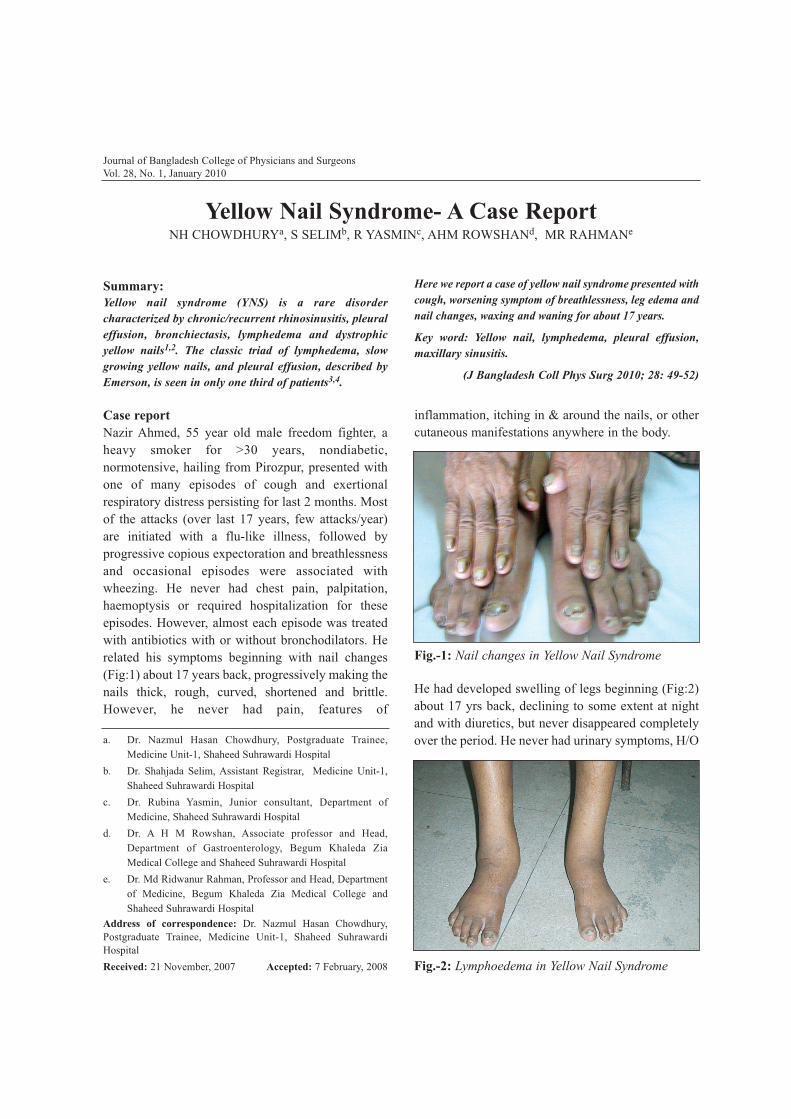
Case reportNazir Ahmed, 55 year old male freedom fighter, aheavy smoker for >30 years, nondiabetic,normotensive, hailing from Pirozpur, presented withone of many episodes of cough and exertionalrespiratory distress persisting for last 2 months. Mostof the attacks (over last 17 years, few attacks/year)are initiated with a flu-like illness, followed byprogressive copious expectoration and breathlessnessand occasional episodes were associated withwheezing. He never had chest pain, palpitation,haemoptysis or required hospitalization for theseepisodes. However, almost each episode was treatedwith antibiotics with or without bronchodilators. Herelated his symptoms beginning with nail changes(Fig:1) about 17 years back, progressively making thenails thick, rough, curved, shortened and brittle.However, he never had pain, features of
inflammation, itching in & around the nails, or othercutaneous manifestations anywhere in the body.
Journal of Bangladesh College of Physicians and SurgeonsVol. 28, No. 1, January 2010
Yellow Nail Syndrome- A Case ReportNH CHOWDHURYa, S SELIMb, R YASMINc, AHM ROWSHANd, MR RAHMANe
Summary:Yellow nail syndrome (YNS) is a rare disordercharacterized by chronic/recurrent rhinosinusitis, pleuraleffusion, bronchiectasis, lymphedema and dystrophicyellow nails1,2. The classic triad of lymphedema, slowgrowing yellow nails, and pleural effusion, described byEmerson, is seen in only one third of patients3,4.
Here we report a case of yellow nail syndrome presented withcough, worsening symptom of breathlessness, leg edema andnail changes, waxing and waning for about 17 years.
Key word: Yellow nail, lymphedema, pleural effusion,maxillary sinusitis.
(J Bangladesh Coll Phys Surg 2010; 28: 49-52)
a. Dr. Nazmul Hasan Chowdhury, Postgraduate Trainee,Medicine Unit-1, Shaheed Suhrawardi Hospital
b. Dr. Shahjada Selim, Assistant Registrar, Medicine Unit-1,Shaheed Suhrawardi Hospital
c. Dr. Rubina Yasmin, Junior consultant, Department ofMedicine, Shaheed Suhrawardi Hospital
d. Dr. A H M Rowshan, Associate professor and Head,Department of Gastroenterology, Begum Khaleda ZiaMedical College and Shaheed Suhrawardi Hospital
e. Dr. Md Ridwanur Rahman, Professor and Head, Departmentof Medicine, Begum Khaleda Zia Medical College andShaheed Suhrawardi Hospital
Address of correspondence: Dr. Nazmul Hasan Chowdhury,Postgraduate Trainee, Medicine Unit-1, Shaheed SuhrawardiHospitalReceived: 21 November, 2007 Accepted: 7 February, 2008 Fig.-2: Lymphoedema in Yellow Nail Syndrome
Fig.-1: Nail changes in Yellow Nail Syndrome
He had developed swelling of legs beginning (Fig:2)about 17 yrs back, declining to some extent at nightand with diuretics, but never disappeared completelyover the period. He never had urinary symptoms, H/O

50
jaundice and history suggestive of recurrent attacks oflymphangitis / thrombophlebitis or inguinal swelling.He was repeated evaluated for oedema at home and inthe neighbouring country and was negative for anyspecific disease and received multiple courses (atleast three) of full course antifilarial treatment. Healso received repeated courses of anti-fungaltreatment for the nail changes.
On examination at hospital, patient was mildlydyspnoeic, afebrile, pulse 72 beats/min, BP 120/70mm of Hg, moderate non-pitting leg oedema, neckvein not visible, normal general skin. There wasclubbing, and the nails had broken cuticle, thicksubungual tissue, onycholysis, longitudinally ridgedand had a yellow tint to its colour. Chest examinationrevealed vesicular breath sound with prolongedexpiration, few scattered crepitations and polyphonicrhonchi, and evidence of left sided pleural effusion.Abdominal examination was unremarkable withabsence of ascitis and organomegaly. Other systemicexamination findings were normal.
On Investigation, the haemoglobin was 12.6 gm%,ESR-30 mm in 1st hr, total count of WBC- 6000 / cumm and the differential count was Neutrophil-60%,Eosinophil-02%, Lymphocytes-36%. The Fastingblood sugar was 85 mg/dl & blood sugar 2 hr afterbreakfast was 90 mg/dl. The serum total protein was6.13 gm/dl and serum Albumin was 3.16 gm/dl.Tuberculin test was negative, 3 sample Sputum forAFB was negative, blood test for microfilaria andImmuno-chromatrographic test for filarial wasnegative. The renal, hepatic and cardiac function testswere normal. The thyroid function was normal (TSH- 2.25 mIU/ ml). Urinary examination revealed noprotein and microscopic examination was normal.Chest X-ray cheat PA view revealed ill defined faintopacities (Fig:3) distributed bilaterally suggestive ofinflammatory lung lesions with small left pleuraleffusion. X-ray of the paranasal sinuses weresuggestive of bilateral maxillary sinusitis.Audiometric evaluation revealed mild to moderateconductive type hearing loss in right ear and mildconductive type hearing loss in left ear. Colourdoppler flow study of lower limb circulation reveledno evidence of venous hypertension. Nail scrappingfor fungus was negative.
Ultrasonographic evaluation of abdomen revealednormal findings except for bilateral pleural effusion(left more than right). Diagnostic Pleural fluidanalysis revealed deep straw coloured exudativeeffusion (protein 6.9 gm/dl), raised triglyceride (29mg/dl) and polymorph pleocytosis (plenty per highpower field), Few RBC was also found. Two repeatexaminations of pleural fluid from both sides reveledsimilar findings.
DiscussionThe whole team of more than 20 trainee doctors andthe consultants were puzzled to find a singlediagnosis for the presented clinical syndrome. He wasthought to have Bronchiectasis, Allergic Rhinitis anda component of bronchial hyper-responsiveness toexplain his respiratory symptoms. He was consideredto have long standing Chronic Venous Insufficiency(CVI) to explain his hard pitting oedema, thoughpost-lymphangitic lymphoedema was also on thesuspicion. His nail changes was not explainable,thought to be due to fungal infection of the nails. Thediagnosis was further complicated by the finding ofbilateral exudative pleural effusion and at one point oftime, he was a candidate for receiving a therapeutictrial of anti-TB drugs. The dermatologist’s opinionregarding the nail changes were inconclusive andsuggested twenty nail syndrome (non-infective) asthe possible diagnosis. The trainee doctors came upwith the literature search to find the Yellow NailSyndrome to match all the components of thesyndrome in our patient. Lymphangiogram could notbe done to confirm lymphoedema because of non-availability of the facility in our set up or anywhere inthe city. However, by exclusion we could arrive at a
Journal of Bangladesh College of Physicians and Surgeons Vol. 28, No. 1, January 2010
Fig.-3: Pleural effusion in Yellow Nail Syndrome

51
diagnosis of the lymphoedema. The subsequentsection will now make a brief literature review of theYellow Nail Syndrome.
Since the original description by Samman & White3
many associated findings have been described.Yellow nails result from slow growth, possiblysecondary to defective lymphatic drainage. The nailsbecome dystrophic and dysmorphic with longitudinalor transverse ridging and loss of lonula & cuticle16.Airway manifestations include rhinosinusitis &bronchiectasis. Pleural effusion appear to be a latermanifestation of the syndrome secondary toinadequate drainage by overstressed hypoplasticlymphatics rather than increased fluid production15.The cause of bronchiectasis is unclear but again thedysfunctional lymphatics are thought to play animportant role with compromised drainage ofsecretion & local immune function14.
Yellow nail syndrome is classified as a dominantlyinherited lymphedema with variable expression1.Over 100 cases have been published, most of whichhave been sporadic. There have been only a fewpublished report where a positive family history hasbeen documented in cases of yellow nail syndrome.
The three main features of yellow nail syndrome aredescribed in the following table2.
Feature Characteristics
Nail changes (Fig:1) All nails are usually affected(though few may be spared)
Nails are slow growing orappear to have stoppedgrowing
Nails become thicker and turna pale yellow or greenish-yellow colour with edgesslightly darker
Nails mainly remain smoothbut may be cross-ridging andnail humped with loss ofcuticles
Onycholysis (separation ofnail from the nail bed) mayaffect one or more nails
Lymphoedema (Fig:2) Swelling occurs in about 80%
of patients and mostfrequently affects the legs
Signs of swelling usuallyoccur after nail changesappear and may not been seenfor some months later
Swelling less often affects thehands, face or genitals
Respiratory signs Pleural effusions occur inabout 36% of patients
In about 30% of patients, theinitial symptom is related topleural effusions
Patients often give a historyof recurrent attack ofbronchitis, chronic sinusitis,and pneumonia
Individual manifestations of the syndrome can appearat different times and clinical onset varies from birthto late adult life5.Yellow nail syndrome has beenassociated with autoimmune disorders, such asthyroiditis, systemic lupus erythematosus andrheumatoid arthritis5. There are also isolated casereports of YNS associated with cancer of breast5 ,larynx6, lung7, endometrium8, gall bladder9,metastatic sarcoma10, metastatic melanoma3,Hodgkin’s disease11 and mycosis fungoidis12. It hasalso been described in AIDS and otherimmunodeficiency states and with the use of certaindrugs13.
ConclusionThe cause of yellow nail syndrome is unknown.However, it is seen in patients with chronicbronchiectasis or sinusitis, pleural effusions, internalmalignancies, immunodeficiency syndromes, andrheumatoid arthritis. In some cases the lymphaticabnormality may be congenital (occur duringdevelopment) but in most it is probably related to theother associated conditions. No specific treatment isdescribed for the whole syndrome. Patients shouldreceive appropriate medical treatment for theirrespiratory symptoms and oedema. Nail changes onceestablished are usually permanent, although completereversion to normal nails has been described in someof the case reports. Treatment of nails includes topical
Yellow Nail Syndrome- A Case Report NH Chowdhury et al.

52
vitamin E solution and oral itraconazole. Somestudies have shown that nutritional supplementationwith vitamin E appears to be effective in controllingyellow nail syndrome, for unknown reasons. Zincsupplements have also been used but it is unclearwhether they are effective.
References:1. Norkild P, Kroman-Anderson H, Struve-Christensen E,
Yellow nail Syndrome; the triad of yellow nails,lymphedema and pleural effusion. Acta Med Scand1986;219:221-227.
2. Varney Va, Cumberworth V, Sudderic R. et al. Rhinitis,sinusitis and the yellow nail syndrome: a review ofsymptoms and response to treatment in 17 patients. ClinOtolaryngol 1994;19:237-240
3. Samman PD,White WF. The “yellow nail” syndrome.Br JDermatol 1964;76:153-157
4. Pavlidakey G P, Hashimoto K, Blum D. Yellow nailsyndrome. J Am Acad Dermatol 1984; 11:509-512
5. Gupta A K. Davies G M, Haberman H F. Yellow nailsyndrome. Cuttis 1986; 37:371-374
6. Guin J D, Elleman J H. Yellow nail syndrome; Possibleassociation with malignancy. Arch Dermatol 1979;115:734-735
7. Thomas P S, Sidhu B. Yellow nail syndrome and bronchialcarcinoma [letter]. Chest 1987;92:191
8. Mambretti-Zumwalt J, Seidman , Higano N. Yellow nailsyndrome: Complete triad with pleural protein tern overstudies. South Med J 1980; 73: 995-997
9. Barrows N P, jones R R. Yellow nail syndrome inassociation with carcinoma of gall bladder. Clin ExpDermatol 1991; 16: 471-473
10. Hiller E, Rosenow E C, Olsen A M. Pulmonarymenifestations of the yellow nail syndrome. Chest 1972; 61:452-458
11. Siegelman S S, Heckman BH, Hasson J. Lymphedema,pleural effusions and Yellow nails: associated immunologicdeficiency. Dis Chest 1969;56:114-117
12. Stosick N, Peters K P, Hiller D, et al. Yellow nail syndromein a patient with mycosis fungoides. J Am Acad Dermatol1993;28:792-794
13. Hershko A, Hirsh Berg B, Nahir M, et al. Yellow nailsyndrome. Post Grad Med J 1997;73:466-468
14. Wiggins J, Strickland B, Chung K F. Detection ofbronchiectasis by high resolution computed tomograghy inthe yellow nail syndrome. Clin Radiol 1991;43:377-379
15. Runyon BA,Forker EL,Sopko G A. Pleural – fluid kineticsin a patient with primary lymphedema, pleural effusions,and yellow nails. Am Rev Respir Dis 1979;119:821-825
16. Ilchyshyna, Vickers C H. Yellow nail syndrome associatedwith penicillamine therapy. Acta Derm Venereol 1983;63:554-555
Journal of Bangladesh College of Physicians and Surgeons Vol. 28, No. 1, January 2010

Introduction:Granulocytic sarcoma (GS) is an extramedullarytumor of granulocytic lineage that has a longrecognized association with acute myeloid leukemia(AML).1 It usually occurs in patients with AML,myeloproliferative disorders or myelodysplasia butcan develop in patients with no known hematologicdisorder.2,3 GS, describes extramedullary collectionsof leukemic cells. These collections can occur, alebeit
rarely, as the sole evidence of leukemia. In a reviewof 3 AML, studies conducted by the former ChildrenCancer Group, <1% of patients had isolated GS and11% had GS along with marrow disease at the time ofdiagnosis.4
GS is a localized extramedullary tumor composed ofimmature cells of the granulocytic series. Most casesof GS occur associated with acute or chronicleukemia or myeloproliferative disorders.5 Rarely thetumor may be observed before the diagnosis of anyhematological malignancy3,6 and most of them areharbingers of existing or impending AML. GS mayoccur in almost every part of the body5,7 but thespinal cord invasion and symptomatic facial nervepalsy are relatively uncommon.8,9,10 It may be due toleukemic cell infiltration at any site of facial nerve oroccurrence of GS in the temporal bone or auditorycanal and may be accompanied by hearing loss.9
Symptomatic facial nerve involvement in AMLpatients is rare.9,10
Journal of Bangladesh College of Physicians and SurgeonsVol. 28, No. 1, January 2010
Isolated Facial Nerve Palsy in ChildhoodAcute Myeloid Leukemia
MG HAFIZa, A ISLAMb, MA MANNANc , F RAHMANd
Summary:Case report-1: Sabarna, a female baby of fifteen monthsold was admitted in Pediatric Hematology and Oncology,Bangabandhu Sheikh Mujib Medical University(BSMMU), Dhaka, Bangladesh with the complaints ofdeviation of the angle of mouth to right side and inabilityto close the left eye for five days. Systemic examinationrevealed an incision scar mark on the left mastoid region.Facial asymmetry as evidenced by smooth forehead,absence of nasolabial fold, drooping of the angle of mouthand nonclosure of eyelid on left side. She was mildly pale,mild hepatomegaly, no lymphadenopathy, bone pain orbleeding manifestation. Physical, hematological andhistopathological investigations the features weresuggestive of facial nerve palsy due to granulocyticsarcoma (GS) with acute myeloid leukemia (AML).Following second day of chemotherapy her vital signssuddenly deteriorated and succumbed probably due to theleukostasis or intracranial hemorrhage.
Case report-2: Chayon, another nine month old femalebaby was admitted in the same unit with the history offever, proptosis of both eye balls, deviation of the angle ofmouth to the right side and unable to close the left eye forone month. Physical examination revealed facialasymmetry with the features of left sided facial nervepalsy along with proptosis of eyeballs. She wasmoderately pale, moderate hepatosplenomegaly, nobleeding manifestation or bone pain. Physical,hematological and cerebrospinal fluid (CSF)examination the features were suggestive of facial nervepalsy due to leukemic cell infiltration with AML.Following induction and consolidation the baby is oncontinuation phase with regular follow up for last 9month having significant improvement of her facialnerve palsy along with hematological remission.
(J Bangladesh Coll Phys Surg 2010; 28: 53-58)
a. Dr. Md. Golam Hafiz, MD, Assistant Professor, PaediatricHaematology and Oncology, Dept. of Paediatrics, BSMMU, Dhaka.
b. Dr. Afiqul Islam, FCPS, MD, Professor of Paediatric Haematologyand Oncology, Dept. of Paediatrics, BSMMU, Dhaka.
c. Dr. MA Mannan, M.Phil (Edin), FCPS (BD), FCPS (Pak), FRCP(Edin), Professor of Paediatric Haematology and Oncology,Chairman, Dept. of Paediatrics, BSMMU, Dhaka.
d. Dr. Fazlur Rahman, MCPS, D-Card, MD, Associate Professor, Dept.of Cardiology, BSMMU, Dhaka.
Address of Correspondence: Dr. Md. Golam Hafiz, MD, AssistantProfessor, Paediatric Haematology and Oncology, Dept. of Paediatrics,BSMMU, Dhaka.
Received: 18 December, 2007 Accepted: 12 February, 2008

54
The clinical picture of central nervous system (CNS)leukemia is usually one of the meningeal irritationswith headache, vomiting, photophobia and the signssimply of raised intracranial pressure. Occasionally,fits can be the presenting feature or cranial nerveinvolvement, particularly isolated VII nerve palsies.There is also well recognized syndrome ofhyperphagia, pathological weight gain andsomnolence thought to be due to involvement of thehypothalamus.11
To the best of our knowledge no account of facialnerve palsy due to GS or leukemic cell infiltration hasearlier been reported in Bangladesh with childhoodAML. To highlight this issue, here we are reportingtwo cases of childhood AML with isolated facialnerve palsy.
Case Report-1:Sabarna, a fifteen month old female child weighing10kg hailing from Bagerhat, Bangladesh was admittedin Pediatric Neurology, BSMMU on 3rd September,2007 with the complaints of deviation of the angle ofmouth to right side and inability to close the left eyefor five days (Fig-I). Before admission, she was seenby an otorhinolaryngologist because of a small mass in
the auditory canal of the left ear. The mass lesion wasexcised totally to obtain decompression but there wasno significant improvement of her complaints. Thepatient came of an average socioeconomicbackground, completely immunized and her generalcondition was good. There was no history of fever,vomiting, bone pain, cough, respiratory distress,bleeding manifestation, neck swelling, ear discharge,jaw pain, any trauma to head or blood transfusion. Shewas delivered at home at term without anycomplication. Milestone of development up to thistime was appropriate for her age.On systemic examination, there was an incision scarmark on the left mastoid region. The child wasconscious, afebrile, restless, facial asymmetry asevidenced by smooth forehead, absence of nasolabialfold, drooping of the angle of mouth and non-closure ofeyelid on left side. She was a mildly pale, skin surveyrevealed normal, no lymphadenopathy but mildhepatomegaly was present. Pupillary examinationfindings were normal. She was then treated withdexamethasone and facial massage having no significantimprovement. Histopathological examination of thetumor mass showed various mature and immaturegranular cells with large mononuclear cells which hadlobulated nucleus and immature loose structure ofchromatin which was consistent with GS (Fig-2). Then,she was transferred to Pediatric Hematology andOncology, BSMMU for further evaluation.
Journal of Bangladesh College of Physicians and Surgeons Vol. 28, No. 1, January 2010
Fig.-2: Histopathologically the tumor is composed ofa relatively uniform population of immature cells.There are some immature eosinophils (E) andneutrophils(N)
Fig.-1: Photograph (facial palsy) at presentation
Hematological investigations showed the followings:hemoglobin level 8.2 gm/dl, ESR 35 mm after firsthour (westergren method), total leukocyte count 300x 109/L, platelet count 40 x 109/L, differential count:
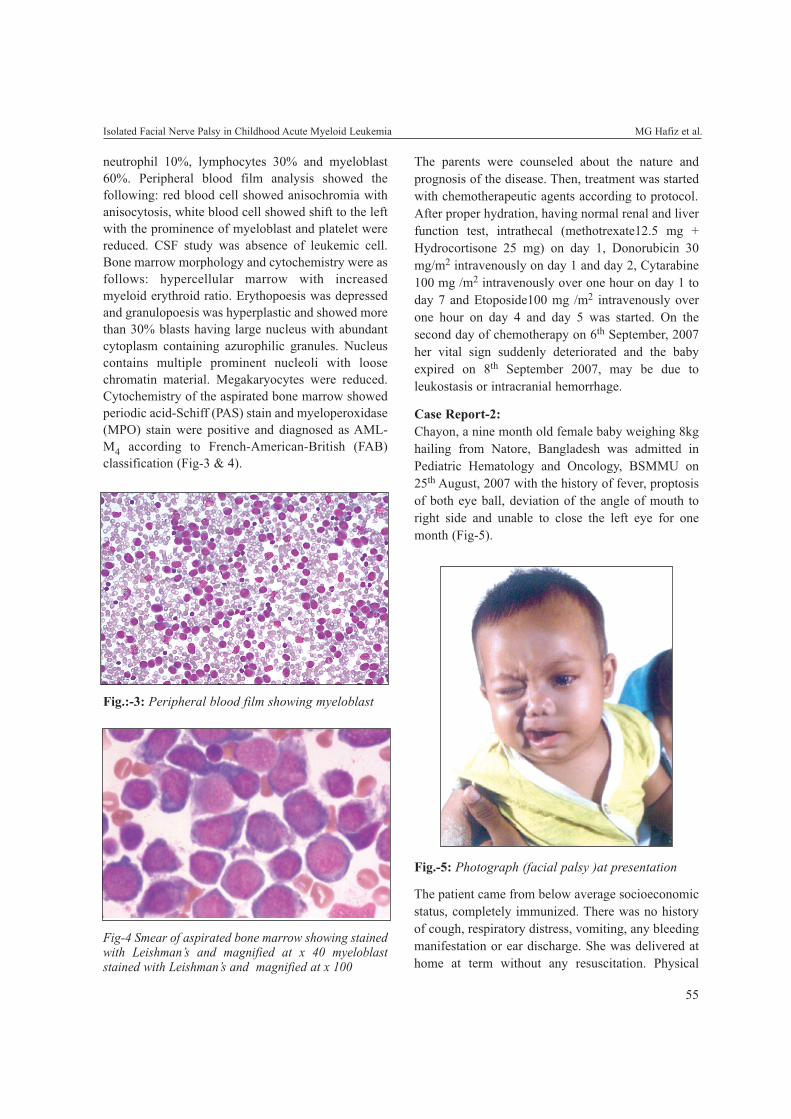
55
neutrophil 10%, lymphocytes 30% and myeloblast60%. Peripheral blood film analysis showed thefollowing: red blood cell showed anisochromia withanisocytosis, white blood cell showed shift to the leftwith the prominence of myeloblast and platelet werereduced. CSF study was absence of leukemic cell.Bone marrow morphology and cytochemistry were asfollows: hypercellular marrow with increasedmyeloid erythroid ratio. Erythopoesis was depressedand granulopoesis was hyperplastic and showed morethan 30% blasts having large nucleus with abundantcytoplasm containing azurophilic granules. Nucleuscontains multiple prominent nucleoli with loosechromatin material. Megakaryocytes were reduced.Cytochemistry of the aspirated bone marrow showedperiodic acid-Schiff (PAS) stain and myeloperoxidase(MPO) stain were positive and diagnosed as AML-M4 according to French-American-British (FAB)classification (Fig-3 & 4).
The parents were counseled about the nature andprognosis of the disease. Then, treatment was startedwith chemotherapeutic agents according to protocol.After proper hydration, having normal renal and liverfunction test, intrathecal (methotrexate12.5 mg +Hydrocortisone 25 mg) on day 1, Donorubicin 30mg/m2 intravenously on day 1 and day 2, Cytarabine100 mg /m2 intravenously over one hour on day 1 today 7 and Etoposide100 mg /m2 intravenously overone hour on day 4 and day 5 was started. On thesecond day of chemotherapy on 6th September, 2007her vital sign suddenly deteriorated and the babyexpired on 8th September 2007, may be due toleukostasis or intracranial hemorrhage.
Case Report-2:Chayon, a nine month old female baby weighing 8kghailing from Natore, Bangladesh was admitted inPediatric Hematology and Oncology, BSMMU on25th August, 2007 with the history of fever, proptosisof both eye ball, deviation of the angle of mouth toright side and unable to close the left eye for onemonth (Fig-5).
Isolated Facial Nerve Palsy in Childhood Acute Myeloid Leukemia MG Hafiz et al.
Fig.-5: Photograph (facial palsy )at presentation
Fig.:-3: Peripheral blood film showing myeloblast
Fig-4 Smear of aspirated bone marrow showing stainedwith Leishman’s and magnified at x 40 myeloblaststained with Leishman’s and magnified at x 100
The patient came from below average socioeconomicstatus, completely immunized. There was no historyof cough, respiratory distress, vomiting, any bleedingmanifestation or ear discharge. She was delivered athome at term without any resuscitation. Physical
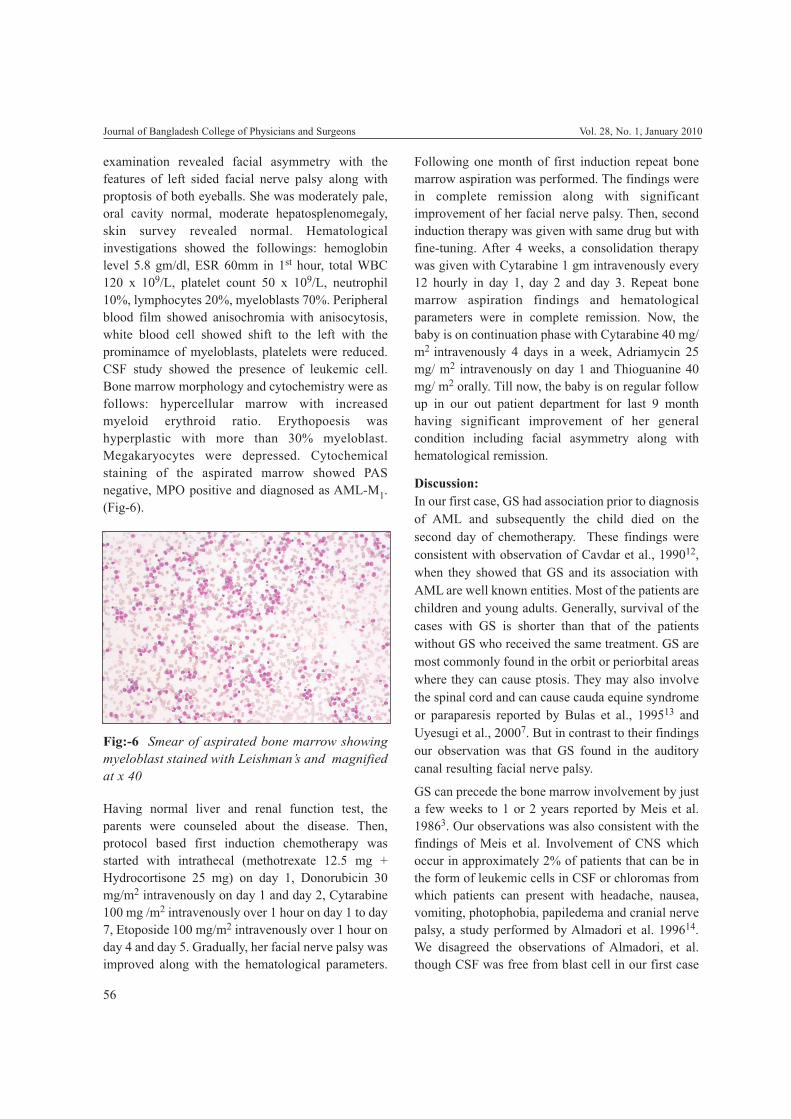
56
examination revealed facial asymmetry with thefeatures of left sided facial nerve palsy along withproptosis of both eyeballs. She was moderately pale,oral cavity normal, moderate hepatosplenomegaly,skin survey revealed normal. Hematologicalinvestigations showed the followings: hemoglobinlevel 5.8 gm/dl, ESR 60mm in 1st hour, total WBC120 x 109/L, platelet count 50 x 109/L, neutrophil10%, lymphocytes 20%, myeloblasts 70%. Peripheralblood film showed anisochromia with anisocytosis,white blood cell showed shift to the left with theprominamce of myeloblasts, platelets were reduced.CSF study showed the presence of leukemic cell.Bone marrow morphology and cytochemistry were asfollows: hypercellular marrow with increasedmyeloid erythroid ratio. Erythopoesis washyperplastic with more than 30% myeloblast.Megakaryocytes were depressed. Cytochemicalstaining of the aspirated marrow showed PASnegative, MPO positive and diagnosed as AML-M1.(Fig-6).
Following one month of first induction repeat bonemarrow aspiration was performed. The findings werein complete remission along with significantimprovement of her facial nerve palsy. Then, secondinduction therapy was given with same drug but withfine-tuning. After 4 weeks, a consolidation therapywas given with Cytarabine 1 gm intravenously every12 hourly in day 1, day 2 and day 3. Repeat bonemarrow aspiration findings and hematologicalparameters were in complete remission. Now, thebaby is on continuation phase with Cytarabine 40 mg/m2 intravenously 4 days in a week, Adriamycin 25mg/ m2 intravenously on day 1 and Thioguanine 40mg/ m2 orally. Till now, the baby is on regular followup in our out patient department for last 9 monthhaving significant improvement of her generalcondition including facial asymmetry along withhematological remission.
Discussion:In our first case, GS had association prior to diagnosisof AML and subsequently the child died on thesecond day of chemotherapy. These findings wereconsistent with observation of Cavdar et al., 199012,when they showed that GS and its association withAML are well known entities. Most of the patients arechildren and young adults. Generally, survival of thecases with GS is shorter than that of the patientswithout GS who received the same treatment. GS aremost commonly found in the orbit or periorbital areaswhere they can cause ptosis. They may also involvethe spinal cord and can cause cauda equine syndromeor paraparesis reported by Bulas et al., 199513 andUyesugi et al., 20007. But in contrast to their findingsour observation was that GS found in the auditorycanal resulting facial nerve palsy.
GS can precede the bone marrow involvement by justa few weeks to 1 or 2 years reported by Meis et al.19863. Our observations was also consistent with thefindings of Meis et al. Involvement of CNS whichoccur in approximately 2% of patients that can be inthe form of leukemic cells in CSF or chloromas fromwhich patients can present with headache, nausea,vomiting, photophobia, papiledema and cranial nervepalsy, a study performed by Almadori et al. 199614.We disagreed the observations of Almadori, et al.though CSF was free from blast cell in our first case
Journal of Bangladesh College of Physicians and Surgeons Vol. 28, No. 1, January 2010
Fig:-6 Smear of aspirated bone marrow showingmyeloblast stained with Leishman’s and magnifiedat x 40
Having normal liver and renal function test, theparents were counseled about the disease. Then,protocol based first induction chemotherapy wasstarted with intrathecal (methotrexate 12.5 mg +Hydrocortisone 25 mg) on day 1, Donorubicin 30mg/m2 intravenously on day 1 and day 2, Cytarabine100 mg /m2 intravenously over 1 hour on day 1 to day7, Etoposide 100 mg/m2 intravenously over 1 hour onday 4 and day 5. Gradually, her facial nerve palsy wasimproved along with the hematological parameters.

57
but there was GS in the auditory canal subsequentlydeveloped facial nerve palsy. In both of our patients,facial nerve palsy preceded the diagnosis of AMLnearly one month earlier and tumor mass in theauditory canal causing facial nerve palsy one weekearlier. After the detection of GS, peripheral bloodsmear and bone marrow aspiration findings revealedthe diagnosis of AML. It could not be establishedwhether there was AML initially, because theevaluation of peripheral blood smear and bonemarrow aspiration were not performed earlier in bothcases. These findings were consistent with theobservations of Chen et al. 199615, when they showedthat CNS symptoms may occur due to GS in patientswith AML. In our first case, CSF study was absenceof leukemic cell at presentation but blast cell waspresent in CSF in second case. After the detection offacial nerve palsy, peripheral blood smear and bonemarrow aspiration findings revealed the diagnosis ofAML.
AML has a strong association with GS. Rarely, thetumor may be seen before the diagnosis of leukemia.Symptomatic facial nerve palsy by GS is alsorelatively uncommon, a study performed by Bulent etal,. 2001.16 But in our first case, the GS was seenbefore the diagnosis of AML.
Symptomatic facial nerve involvement in AMLpatient is rare reported by Kurabayashi et al, 1989. 7
and Chapman et al., 1980.10 It may be due toleukemic cell infiltration at any site of the facial nerveor occurrence of GS in temporal bone or auditorycanal and may be accompanied by hearing loss anobservation of Kurabayashi et al,. 1989.9 But in oursecond case had only facial nerve palsy due toleukemic cell infiltration without any association ofhearing loss.
The treatment of AML patients with facial nervepalsy is chemotherapy/or radiotherapy, anobservation of Chapman et al.,1980.10 Thoughunfortunately we could not treat withchemotherapeutic agents with proper duration in ourfirst case, as she succumbed after the second day ofchemotherapy may be due to suspected intracranialhemorrhage or leukostasis.
But in our second case we have given a protocolbased induction of remission with chemotherapeutic
agents having leukemic cells infiltration in CSF.Second bone marrow aspiration and otherhematological investigations were done subsequently.Her physical condition along with the facial nervepalsy was improved gradually and bone marrowaspiration findings were in complete remission. Tillnow, the baby is on maintenance therapy for last ninemonth with regular follow up in our out patientdepartment with significant improvement of herfacial nerve palsy including hematological remission.
Conclusion:So, an awareness of varied clinical manifestation ofchildhood AML is needed in order to establish thecorrect diagnosis when the presenting signs andsymptoms are enigmatic. As in these cases, patientsmay get admitted in the hospital with isolated facialnerve palsy before the diagnosis of childhood AML.GS and leukemic cell infiltration should beconsidered in the differential diagnosis, particularly,in the pediatric patients presenting with isolated facialnerve palsy. Complete blood count along withperipheral blood film examination should be doneroutinely and if atypical cell are found then bonemarrow aspiration and morphological examinationshould be done to establish the diagnosis. In patientswith GS and facial nerve palsy, chemotherapy and/orradiotherapy should be tried prior to surgery becauseof the good response.
References:1. Dock G. Chloroma and its relation to leukemia. Am J Med
Sci 1893; 106: 152-57.
2. Wiernik PH, Serpick AA. Granulocytic sarcoma(chloroma). Blood 1970; 35: 361-69.
3. Meis JM, Butler JJ, Osborne BM, Manning JT. Granulocyticsarcoma in nonleukemic patients. Cancer 1986; 58: 2697-709.
4. Dusenbery KE, Howells WB, Arthur DC, et al. Extramedullary leukemia in children with newly diagnosed acutemyeloid leukemia: a report from the Children CancerGroup. J Pediatr Hematol Oncol 2003; 25 : 760-68.
5. Neiman RS, Barcos M, Berard C, Mann R, Rydell RE,Bennet JM. Granulocytic sarcoma: a clinicopathologicstudy of 61 biopsied cases. Cancer 1981; 48: 1426-137.
6. Krause JR. Granulocytic sarcoma preceding acute leukemia:a report of six cases. Cancer 1979; 44: 1017-21.
7. Uyesugi WY, Watabe J, Petermann G. Orbital and facialgranulocytic sarcoma (chloroma): a case report. PediatrRadiol 2000; 30: 276-78.
Isolated Facial Nerve Palsy in Childhood Acute Myeloid Leukemia MG Hafiz et al.

58
8. Doshi HM, Schochet SS, Gold M, Nugent GR. Granulocyticsarcoma presenting as an epidural mass with acuteparapareses in an aleukemic patient. Am J Clin Pathol 1991;95: 228-32.
9. Kurabayashi H, Miyawaki S, Naruse T, Kubota K. Bilateraltympanic cavity infiltrtation with effusion in a patient withacute myeloblastic leukemia. Blut 1989; 58: 45-46.
10. Chapman P, Johnson SA. Mastoid chloroma as relapse inacute myeloid leukemia. J Laryngol Otol 1980; 94: 1423-27.
11. Lilleyman JS. Neurological complications of acutechildhood leukemia. J Royal Soc Med 1993; 86: 252-53.
12. Cavdar AO, Babacan E, Gozdasoglu S, Kilicturgay K,Arcasoy A, Cin S, et al. High risk subgroup of acutemyelomonocytic leukemia (AMML) with orbito-oculargranulocytic sarcoma (OOGS) in Turkish Children:retrospective analysis of clinical, hematological,
ultrastructral and therapeutic findings of thirty three OOGS.Acta Haematol 1990; 83: 89-93.
13. Bulas RB, Laine FJ, Das NL. Bilateral orbital granulocyticsarcoma (chloroma) preceding the blast phase of acutemyelogenons leukemia: CT findings. Pediatr Radiol 1995;25: 488-89.
14. Almadori G, Del NM, Cadoni G, et al. Facial nerve paralysisin acute otomastoidits as presenting symptoms of FABM2,T8, 21 leukemic relapse. Case report and review ofliteratures. Int J Pedi Orthinolargyngol. 1996; 36: 45-52.
15. Chen CY, Zimmerman RA, Faro S, Bilaniuk LT, Chou TY,Molloy PT. Childhood leukemia: central nervous systemabnormalities during and after treatment. Am J Neuroradiol1996; 17: 295-310.
16. Bulent E, Mustafa C, Olgum K, Ali U, Ozlem Er, Hasan SCand Mustafa A. Facial nerve palsy and paraplegia aspresenting symptoms of acute myeloid leukemia. Jpn J ClinOncol 2001; 31:86-88.
Journal of Bangladesh College of Physicians and Surgeons Vol. 28, No. 1, January 2010
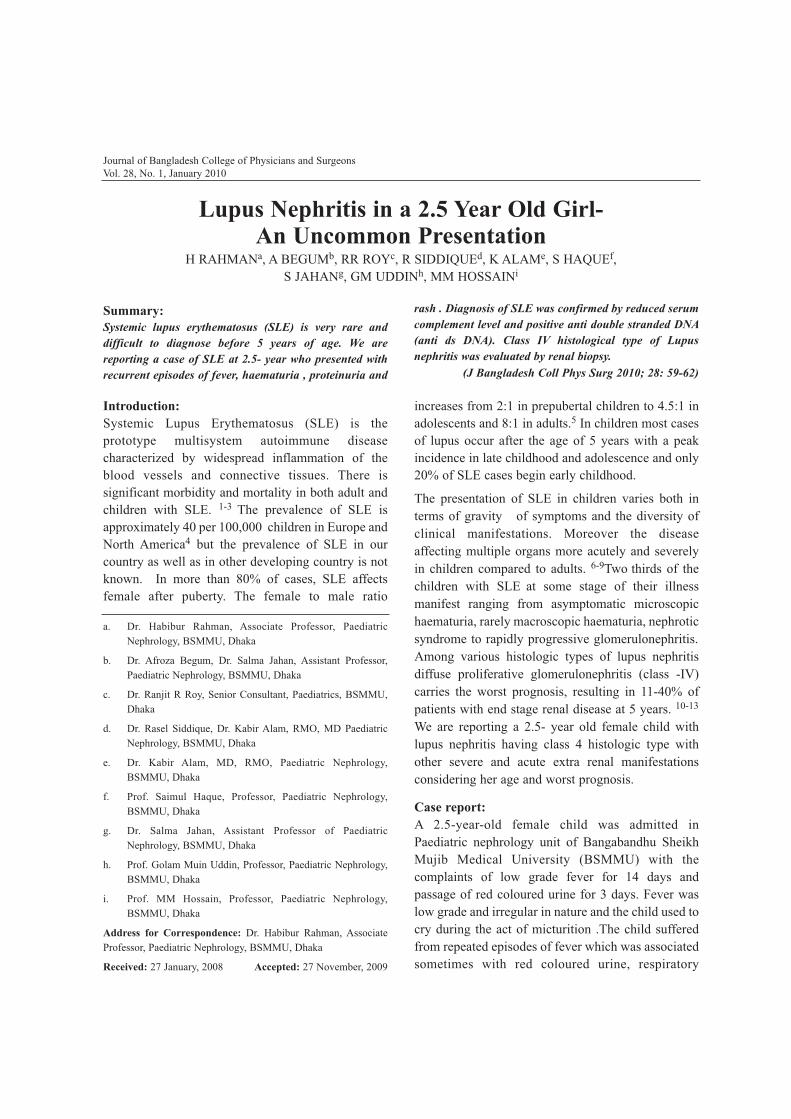
Introduction:Systemic Lupus Erythematosus (SLE) is theprototype multisystem autoimmune diseasecharacterized by widespread inflammation of theblood vessels and connective tissues. There issignificant morbidity and mortality in both adult andchildren with SLE. 1-3 The prevalence of SLE isapproximately 40 per 100,000 children in Europe andNorth America4 but the prevalence of SLE in ourcountry as well as in other developing country is notknown. In more than 80% of cases, SLE affectsfemale after puberty. The female to male ratio
increases from 2:1 in prepubertal children to 4.5:1 inadolescents and 8:1 in adults.5 In children most casesof lupus occur after the age of 5 years with a peakincidence in late childhood and adolescence and only20% of SLE cases begin early childhood.
The presentation of SLE in children varies both interms of gravity of symptoms and the diversity ofclinical manifestations. Moreover the diseaseaffecting multiple organs more acutely and severelyin children compared to adults. 6-9Two thirds of thechildren with SLE at some stage of their illnessmanifest ranging from asymptomatic microscopichaematuria, rarely macroscopic haematuria, nephroticsyndrome to rapidly progressive glomerulonephritis.Among various histologic types of lupus nephritisdiffuse proliferative glomerulonephritis (class -IV)carries the worst prognosis, resulting in 11-40% ofpatients with end stage renal disease at 5 years. 10-13
We are reporting a 2.5- year old female child withlupus nephritis having class 4 histologic type withother severe and acute extra renal manifestationsconsidering her age and worst prognosis.
Case report:A 2.5-year-old female child was admitted inPaediatric nephrology unit of Bangabandhu SheikhMujib Medical University (BSMMU) with thecomplaints of low grade fever for 14 days andpassage of red coloured urine for 3 days. Fever waslow grade and irregular in nature and the child used tocry during the act of micturition .The child sufferedfrom repeated episodes of fever which was associatedsometimes with red coloured urine, respiratory
Journal of Bangladesh College of Physicians and SurgeonsVol. 28, No. 1, January 2010
Lupus Nephritis in a 2.5 Year Old Girl-An Uncommon Presentation
H RAHMANa, A BEGUMb, RR ROYc, R SIDDIQUEd, K ALAMe, S HAQUEf,S JAHANg, GM UDDINh, MM HOSSAINi
Summary:Systemic lupus erythematosus (SLE) is very rare anddifficult to diagnose before 5 years of age. We arereporting a case of SLE at 2.5- year who presented withrecurrent episodes of fever, haematuria , proteinuria and
rash . Diagnosis of SLE was confirmed by reduced serumcomplement level and positive anti double stranded DNA(anti ds DNA). Class IV histological type of Lupusnephritis was evaluated by renal biopsy.
(J Bangladesh Coll Phys Surg 2010; 28: 59-62)
a. Dr. Habibur Rahman, Associate Professor, PaediatricNephrology, BSMMU, Dhaka
b. Dr. Afroza Begum, Dr. Salma Jahan, Assistant Professor,Paediatric Nephrology, BSMMU, Dhaka
c. Dr. Ranjit R Roy, Senior Consultant, Paediatrics, BSMMU,Dhaka
d. Dr. Rasel Siddique, Dr. Kabir Alam, RMO, MD PaediatricNephrology, BSMMU, Dhaka
e. Dr. Kabir Alam, MD, RMO, Paediatric Nephrology,BSMMU, Dhaka
f. Prof. Saimul Haque, Professor, Paediatric Nephrology,BSMMU, Dhaka
g. Dr. Salma Jahan, Assistant Professor of PaediatricNephrology, BSMMU, Dhaka
h. Prof. Golam Muin Uddin, Professor, Paediatric Nephrology,BSMMU, Dhaka
i. Prof. MM Hossain, Professor, Paediatric Nephrology,BSMMU, Dhaka
Address for Correspondence: Dr. Habibur Rahman, AssociateProfessor, Paediatric Nephrology, BSMMU, Dhaka
Received: 27 January, 2008 Accepted: 27 November, 2009
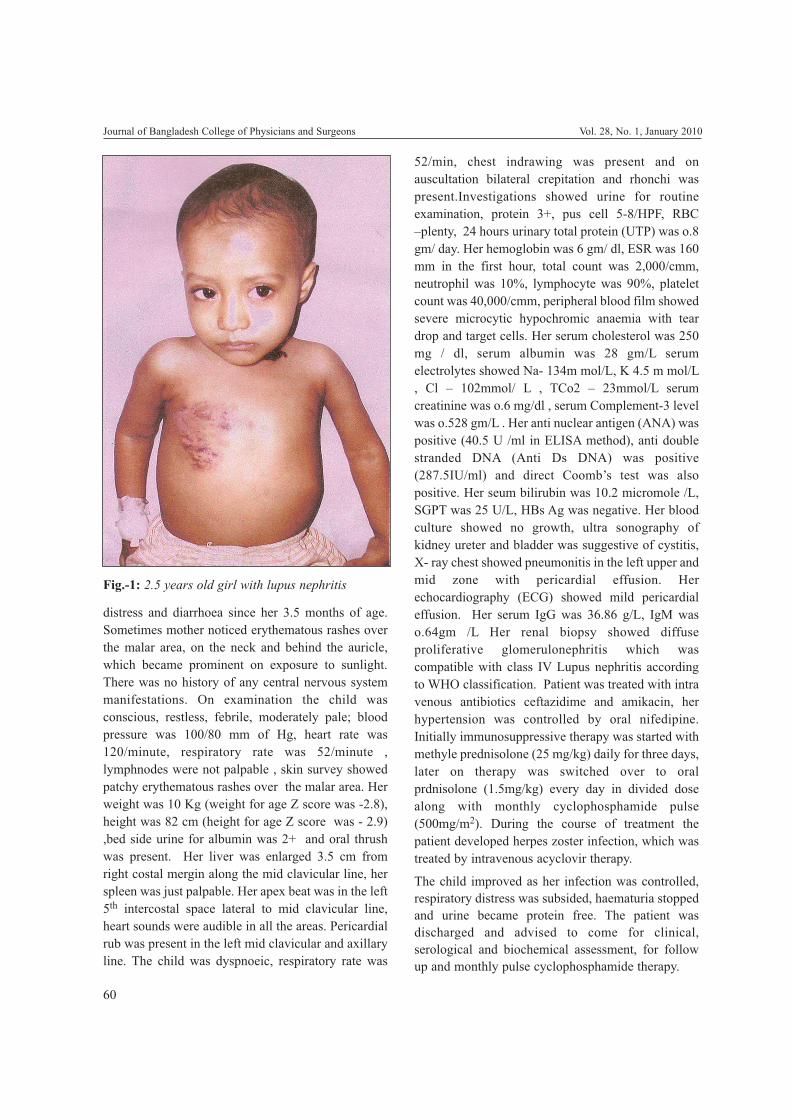
60
distress and diarrhoea since her 3.5 months of age.Sometimes mother noticed erythematous rashes overthe malar area, on the neck and behind the auricle,which became prominent on exposure to sunlight.There was no history of any central nervous systemmanifestations. On examination the child wasconscious, restless, febrile, moderately pale; bloodpressure was 100/80 mm of Hg, heart rate was120/minute, respiratory rate was 52/minute ,lymphnodes were not palpable , skin survey showedpatchy erythematous rashes over the malar area. Herweight was 10 Kg (weight for age Z score was -2.8),height was 82 cm (height for age Z score was - 2.9),bed side urine for albumin was 2+ and oral thrushwas present. Her liver was enlarged 3.5 cm fromright costal mergin along the mid clavicular line, herspleen was just palpable. Her apex beat was in the left5th intercostal space lateral to mid clavicular line,heart sounds were audible in all the areas. Pericardialrub was present in the left mid clavicular and axillaryline. The child was dyspnoeic, respiratory rate was
52/min, chest indrawing was present and onauscultation bilateral crepitation and rhonchi waspresent.Investigations showed urine for routineexamination, protein 3+, pus cell 5-8/HPF, RBC–plenty, 24 hours urinary total protein (UTP) was o.8gm/ day. Her hemoglobin was 6 gm/ dl, ESR was 160mm in the first hour, total count was 2,000/cmm,neutrophil was 10%, lymphocyte was 90%, plateletcount was 40,000/cmm, peripheral blood film showedsevere microcytic hypochromic anaemia with teardrop and target cells. Her serum cholesterol was 250mg / dl, serum albumin was 28 gm/L serumelectrolytes showed Na- 134m mol/L, K 4.5 m mol/L, Cl – 102mmol/ L , TCo2 – 23mmol/L serumcreatinine was o.6 mg/dl , serum Complement-3 levelwas o.528 gm/L . Her anti nuclear antigen (ANA) waspositive (40.5 U /ml in ELISA method), anti doublestranded DNA (Anti Ds DNA) was positive(287.5IU/ml) and direct Coomb’s test was alsopositive. Her seum bilirubin was 10.2 micromole /L,SGPT was 25 U/L, HBs Ag was negative. Her bloodculture showed no growth, ultra sonography ofkidney ureter and bladder was suggestive of cystitis,X- ray chest showed pneumonitis in the left upper andmid zone with pericardial effusion. Herechocardiography (ECG) showed mild pericardialeffusion. Her serum IgG was 36.86 g/L, IgM waso.64gm /L Her renal biopsy showed diffuseproliferative glomerulonephritis which wascompatible with class IV Lupus nephritis accordingto WHO classification. Patient was treated with intravenous antibiotics ceftazidime and amikacin, herhypertension was controlled by oral nifedipine.Initially immunosuppressive therapy was started withmethyle prednisolone (25 mg/kg) daily for three days,later on therapy was switched over to oralprdnisolone (1.5mg/kg) every day in divided dosealong with monthly cyclophosphamide pulse(500mg/m2). During the course of treatment thepatient developed herpes zoster infection, which wastreated by intravenous acyclovir therapy.
The child improved as her infection was controlled,respiratory distress was subsided, haematuria stoppedand urine became protein free. The patient wasdischarged and advised to come for clinical,serological and biochemical assessment, for followup and monthly pulse cyclophosphamide therapy.
Journal of Bangladesh College of Physicians and Surgeons Vol. 28, No. 1, January 2010
Fig.-1: 2.5 years old girl with lupus nephritis

61
Discussion:Paediatric and adult SLE patients with class IV LNhave worse renal and overall survival rate, thoughboth morbidity and mortality rates are improving withbetter supportive and medical care.14,15 Besidehistological class of lupus nephritis risk ofprogression also depends on other factors like age ,gender , race, hypertension , initial serum creatinineconcentration , delay between onset of renal diseaseand treatment and the response to therapy after thefirst year.16 Our patient a girl of 2.5 years old withclass IV histological type lupus nephritis, initiallypresented with typical manifestations of SLE withboth renal and extra renal manifestations which is notas common at this age like older children andadolescents. We treated the patient with propernutritional support, intravenous broad spectrumantibiotics to combat infections and patients generalwellbeing was improved after 7 days of treatment. Westarted anti inflammatory and immunsuppressivetreatment after controlling infection with intravenouspulse methyle prednisolone for three days which wasmaintained with oral corticosteroid at a dose of 1.5mg/ kg/day in three divided doses and intravenousmonthly pulse cyclophosphamide. Thereby ourpatient showed signs of both clinical and serologicalimprovement after one month of therapy. It has beenobserved by different authors in their study that bothpulse methyleprednisolone and cyclophosphamidehave synergistic and superior effects in inducingremission.17,18 Austin et al 19 and Bounepas et al 20
observed that intravenous pulse cyclophosphamidewith higher cumulative dose was superior over oralcylophosphamide both in the context of fewer sideeffects and preservation of renal function and alsorate of relapse of nephritis beyond 5 years. Most ofthe authors concluded that corticosteroid pulse and anextended course of pulse cyclophosphamide over 30months becomes the standard protocol for the initialtreatment of aggressive LN in many centers, whichwas followed in our case also. Herpes zoster is a verycommon viral infection in SLE 18 occurred in ourpatient during the course of treatment, which wastreated by I/V acyclovir. Even after aggressivetreatment in advanced LN 10 to 20% patient maydevelop end stage renal failure after a mean period of5 years.21,22 So it is obligatory to closely supervise
the patient both clinically, serologically and byevaluation of renal function at close intervalthroughout the life.
References :1. Moss KE, Ioannou Y , Sultan SM , Haq I , Iseaberg DA .
Oucome of a cohort of 300 patients with systemic lupuserythematosus attending a dedicated clinic for over twodecades. Ann Rheum Dis 2002; 61:407-413.
2. Lehan TJ , Mecurly DK , Bermstein BH , King KK, HansonV. Systemic lupus erythematosus in the first decade of life.Paediatric 1989; 83: 235-39.
3. Marini R, Costallat LT. Young age at onset, renalinvolvement and arterial hypertension of adverse prognosticsignificance in Juvenile systemic lupus erythematosus. RevRheum Engl Ed 199; 66: 303-309.
4. Hockberg MC. Systmic lupus eythematosus. Rheum DisClin North Am 1990; 16: 617 -639.
5. Cameron JS. Lupus nephritis. J Am Soc Nephrol 1999; ID:413-424.
6. Tucker LB, Menon S, Schauer JG et al. Adult and childhoodonset Systemic lupus erythematosus: a comparison of onset,clinical feature and outcome. Br J Rheumatol 1995; 34:866-872.
7. Hood MJ, Tencate R, Vansulekom Smith LWA et al.Childhood onset systemic lupus erythematosus- clinicalpresentation and prognosis in 31 patients. Scan J Rheumatol1999; 28: 222-226.
8. Correno L, Lopes – Lango FJ, Montagudol et al.Immunological and clinical difference between juvenile andadult onset systemic lupus erythematosus. Lupus 1999; 8:287-292.
9. Font J, Cervera R , Espinosa G et al . SLE in childhood:analysis of clinical and immunological findings in 34patients and comparison with SLE characteristic in adults.Ann Rheum Dis 1998; 57: 456-459.
10. Mok CC, Wong RWS, Lou CS. Lupus nephritis in SouthernChinese patients: clinicopatholoical findings and long termoutcome. Am J Kidney Dis 1999; 34: 315-23.
11. Young LY, Chen Wap, Lin CY. Lupus nephritis in children –A review of 167 patients. Paediatrics 1994; 94: 335-40.
12. Bakir AA , Ley PS , Dunea G. The prognosis of lupusnephritis in African – Americans: A retrospective analysis.Am J Kidney Dis 1994; 24: 159 -71.
13. Bogdanovic R, Nikolic V, Pasic S, Dimitrijevic J, LipnovskaMarkovic J, Eric Marinkovic J et al. Lupus nephritis inchildhood: a review of 53 patient s followed at a singlecentre . Pediatr Nephrol 2000; 19: 36-44.
14. Emre S, Bilge I, Sirin A, Kilicaslan I , Nayir A, Oktem F etal. Lupus nephritis in children : prognostic significance of
Lupus Nephritis In A 2.5 – Year Old Girl- An Uncommon Presentation H Rahman et al.
62
clinicopathological findings. Nephron 2001; 87 : 118-126..
15. Iseki K, Miyasato F, Okra T. An epidemiological analysis ofend stage lupus nephritis. Am J Kidney Dis 1994; 23: 547-554.
16. Gourley MF, Austin HA, Scott D, Yarboro CH, VaughanEM, Muir J et al. Methyl prednisolone andcyclophosphamide alone in combination in patients withlupus nephritis. A randomized control trial. Ann Intern Med1996, 125; 549-57.
17. Illei CG, Austin HA, Crane M, Collins L, Courley MF,Yarbo CH et al. Combination therapy with pulsecyclophosphamide plus methyl prednisolone improve longterm renal outcome without adding toxicity in patients withLN . Ann Intern Med 2001; 135: 248-57.
18. Austin HA , Klippel JH , Balone JE , Riche NGH, SteinbergAD , Plotz PH et al. Therapy of lupus nephritis: controlledtrial of prednisolone and cytotoxic drugs. N Eng J Med1986; 314: 614-19.
19. Boumpus DT, Austin HA, Vaughan EM , Klippel JH, SteinbergAD, Yarboro CH et al. Controlled trial of pulse methyleprednisolone versus two regimens of pulse cyclophosphamidein severe lupus nephritis. Lancet 1992; 304: 741-5.
20. Boro L, Cameron JS, Hicks JA. The very long termprognosis and complications of lupus nephritis and itstreatment. QJM 1999; 92: 211-218.
21. Cheigh JS, Stenzl KH. End stage renal disease in SLE. AmJ Kidney Dis 1993; 21: 2-8.
22. Berden JHM. Lupus nephritis. Kidney Int 1997; 52: 538-558.
Journal of Bangladesh College of Physicians and Surgeons Vol. 28, No. 1, January 2010
(J Bangladesh Coll Phys Surg 2010; 28: 63)
Influenza pandemic is not a new phenomenon to theworld. The recent outbreak of Pandemic InfluenzaH1N1 2009, is a newly packaged from of the goodold Influenza A virus (H3N2) swept across the world!It's a triple reassortment virus: Which means that it isa combination of the classical Swine HIN2, HumanH3N2 and Avian influenza viruses known as theNorth American Swine H3N2 and H1N2 that laterconverted into the 2009 Human H1N1 virus. TheWorld Health Organization has stopped using theterm "swine flu" to avoid confusion over the dangerposed by pigs. The proper name is "Pandemic (HIN1)2009 Influenza".The first case of 2009 pandemic influenza A (H1N1)virus infection in Bangladesh was documented onJune 184 Subsequently, persons with suspected casesof infection and contacts of those with suspectedinfection were tested. Individuals in whom infectionwas confirmed were hospitalized and quarantined,and some of them were closely pbserved for thepurpose of investigating the nature and duration ofthe disease. In Dhaka Medical College Hospital therewere 28 admitted patients in flu ward and 2335registered suspected H1N1 influenza cases wereattended in flue corner but 833 highly suspected caseswere recorded in case record form. We describe theclinical and epidemiological characteristics of 28indoor (flu ward) and 833 outdoor (flu corner)patients. Most of them were in between 20 to 30 yearsage group. Among 833 outdoor patients 611(73.34%)were male and 222(26.65%) were female. 354(42.49%) patients were student, 195 (23.40%) wereservice holder. No patients (indoor) had any seriousunderlying medical conditions. Indoor patientspresented with mostly fever (92.85%), Rhinorrhea
(71.42%), shortness of breath (89.28%) and cough(64.28%). Where Out of the 833 outdoor patients59b(71.54%) patients had fever, 585(70.229b) hadcough, 410(49.21%) had Rhinorrhea and 314 (37.69%)had sore throat. Antiviral (Oseltamivir) was given to100% of indoor patients and 6.45% of outdoorpatients. Out of 28 patients admitted, 09 cases werePCR positive and one patient died in hospital whowas immunocompromised another one patient diedwhose PCR test would not done. Early antiviraltreatment may have shortened the duration ofsymptoms and produced better outcome.
Prof. Quazi Tarikul Islam,FCPS, FRCP, FACPProfessor, Department of MedicineDhaka Medical College, Dhaka.andCoordinator Swine Flu preparedness teamDhaka Medical College Hospital
References:1. Cumming N,lacobs A, Otterman S. WHO Raises Alert
Level as Flu Spreads to 74 Countries. The New York Times.June 11, 2009. Available at: http://www.nytimes.com/2009/06/12/worfd/12who.html?_r=2. Accessed 18th December,2009.
2. Ahasan HAMN. Pandemic (H1N1) 2009 influenza:Bangladesh Perspective. Editorial, J Bangladesh Coll PhysSurg 2009;27;129-131.
3. Islam QT. Swine Flu. Editorial. l 0 Med July 2009;10;2:38-39.
4. Institute of Epidemiology, Disease Control and Research.Situation of Influenza A H1N1 (Swine Flu). IEDCR;15December 2009.
Experience of Pandemic Influenza A (H1N1) 2009 atDhaka Medical College Hospital
SHORT COMMUNICATION

(1). A comprehensive and time honored review on“Epidemiology of Hepatitis C Virus infection” ofthe journal of Bangladesh College of Physicians andSurgeons of September 2009, Vol 27, No 3.To the Editor in chief: We have gone through the reviewand we have few important comments on this review.
Acute HCV is asymptomatic in approximately 84%of cases and is usually not recognized clinically.1Approximately 85% of those infected with HCV willdevelop chronic infection and 15% will spontaneouslyclear virus, which is higher in children (45%). 20-30% of chronic HCV patient develop cirrhosis over10-20 years of infection.1 HCV cirrhosis increasesthe risk of Hepatocellular carcinoma (HCC)dramatically. It is estimated that between 2 and 6.7%of all patients with HCV cirrhosis will develop HCCover 10 years and annual risk is 1-4%.1 It is rare thatHCC will develop in patients without cirrhosis oradvanced fibrosis (unlike HBV infection). Globalprevalence of chronic hepatitis C is estimated toaverage 3% (ranging from 0.1-5% in differentcountries). 2 Intravenous drug uses remains the mainmode of transmission, sexual and intra-familialspread is believed to be very low (unlike HIV). 2 Thecost of investigation, treatment and monitoringtherapy out of reach at the millions of sufferer’sworldwide.2
We should pay more attention to prevent infection ofHCV. Currently there is no vaccine available.Efficacy of standard immunoglobulin after needleprick, sexual or perinatal exposure to HCV has notbeen determined and is not recommended.1 Allprecautions to prevent infection of HCV shouldtarget reduction of transmission of the virus, screenof blood donors, treatments of blood products, safeinjection practice and strongly discourage illegaldrug use will minimize the spread of lethal infectionin future.
References:1. Current medical diagnosis and treatment Gastroenterology,
2nd edition McGraw Hill, 2003, 554-559.
2. Disease of the Liver and Biliary System 11th edition, SheilaSherlock and James Dooley 2002 Blackwell;305-316.
3. Sultan MT, Rahman MM, Begum S. Epidemiology ofHepatitis C virus infection, J Bangladesh Coll Phy Surg2009;27;3:160-162.
Maj. Gen. (Dr.) M. A. Moyeed Siddiqui (Retd.)MCPS, FCPS(BD), FCPS(Pak), FRCP (Ireland),FRCP(Edin), FACP(USA)Ex. Director General Armed Forces MedicalServices, Ex. Consultant Physician General &Professor of Medicine. e-mail:[email protected]
Dr. Md. Mahmudur Rahman SiddiquiPostgraduate trainee, Department of Medicine,Dhaka Medical College Hospital, Dhaka.
Author's ReplyWe thank Maj. Gen. (Dr.) M A Moyeed Siddiqui andDr. Md. Mahmudur Rahman Siddiqui for their interestin our article. We were highly delighted to read theirletter with few important comments on "Epidemiologyof Hepatitis C Virus Infection". Since we onlyreviewed the prevalence, genotype data, transmissionrisk and prevention, we did not mention the elaboratedata regarding percentage of asymptomatic infection,virus clearance, cirrhosis of liver and development ofhepatocellular carcinoma. However we gladly acceptthe additional information, they had provided butregarding prevalence, transmission and prevention, allthe information discussed in our article are consistentwith their comments.
Dr Md Tipu SultanAssistant Professor, Virology Department ofMicrobiology Chittagong Medical College
Ref:Siddiqui MAM, Siddiqui MMR. Letter to the Editor-Epidemiology of Hepatitis C Virus Infection, J Bangladesh CollPhy Surg 2010
(J Bangladesh Coll Phys Surg 2010; 28: 64-65)
LETTER TO THE EDITOR

65
(2). About “Familial Hypokalaemic Periodic Paralysis–A Case Report” of the journal of BangladeshCollege of Physicians and Surgeons of September2009, Vol-27, No-3.To the Editor in Chief: I have gone through this casereport and have few comments. It is the clinicalfeature and serum electrolyte report which are usuallysufficient for the diagnosis of Hypokalaemic PeriodicParalysis (HypoKPP). Though it mimics GuillainBarre Syndrome (GBS), lumber puncture for CSFstudy is usually not necessary to differentiateHypoKPP from GBS. The CSF findings suggestive ofGBS usually appear at the end of first week of illnessand by this time patients of HypoKPP improves withthe treatment with potassium1.In this case report there is a mistake in thearrangement of the ECG tracings in fig: 1(b) and fig:2(b) as the descriptions mentioned below the figuresare opposite to each other2.References :1. Hauser SL, Asbury AK. Guillain Barre syndrome and other
immune mediated neuropathies. In Fauci AS, KasperDL,Longo DL,Braunwald E, Hauser SL,Jameson JL,LoscalzoJ. Harrison’s Principles of Internal Medicine 17th ed. NewYork.McGraw-hill Companies Inc. 2008: Vol-2, p 2691-2.
2. Majumder MSH. Familial Hypokalaemic PeriodicParalysis– A case report. J Bangladesh Col Phy Surg2009:27; 3:166-168
Dr. Ahmed HossainAssistant Professor, Department of MedicineDhaka Medical College, Dhaka.
Author's ReplyI thank Dr. Ahmed Hossain for his comments. I agreethat CSF protein level may not rise until the end of thefirst week in case of Guillain Barre syndrome (GBS).Regarding CSF protein in GBS, it may be mentionedhere that tau protein may be elevated within first fewdays of symptoms; a predictor of residual deficits1.However, the reported case, being familialhypokalaemic periodic paralysis, I emphasized onclinical course, electrolytic balance and ECGchanges.
I do apologies to you and all other readers on behalfof editorial staff/ press staff regarding the interchangeof two ECG tracing scans (a gross mistake) whichhave been misled the readers by this error2.
Reference:1. Hauser SL, Asbury AK. Guillain-Barre syndrome and other
immune mediated neuropathies. In Fauci AS, Kasper DL,Longo DL, Braunwald E, Hauser SL, Jameson IL, LoscalzoJ. Harrison's Principles of Internal Medicine 17th ed. NewYork. McGraw-Hill Companies Inc. 2008: Vol-2, p 2669-70.
2. Majumder MSH. Familial Hypokalaemic Periodic Paralysis -A case report. 3 Bangladesh Col Phy Surg 2009:27; 3:166-168.
Dr. Md. Shafayet Hasan MajumderAssociate Professor of MedicineMedical College for Women & Hospital Uttara,Dhaka.
Letter to the Editor
Date Time Topic Speaker Chairperson / Moderator
13-10-09Tuesday
12-10 pm to1-00 pm
Guideline of Managementand its Effect on SubsequentPregnancy Outcome
Dr. Asma HabibFCPS (Gynae & Obst.)Register, BMCH
Professor Sameena Chowdhury(Chair.P), Professor of Obst. & GynaeDr. Iffat Ara (Chair.P)Associate Professor of Obst. & GynaeDr. Salma Rouf(Moderator)
27-10-09Tuesday
11-00 am to11-50 am
11-50 am to12-10pm
12-10 pm to1-00 pm
Spesis in Cardiac Surgery
TEA
The Role of Mirena (LNGIUS),other than contraceptive benefits
Dr. Bhabesh MondolJr. Consultant, CardiacAnaesthesiology & SurgicalICU, BIRDEM
Dr. Ismatara BinaFCPS (O&B), MRCOG(London)Khulna
Professor Ahsanul Habib(Chair.P), ConsultantCardiac Anaesthesia
Professor Abu Yousur Fazle ElahiChowdhury (Chair.P)Professor of AnaesthesiologyDr. Mohammad Abdur Rahman(Moderator)
Professor Rowshan Ara Begum(Chair.P)Prof. & Head, Dept. of Obst. & Gynae
Dr. Ferdousi Begum (Chair.P)Assoc. Professor of Obst. & Gynae
Dr. Tabassum Parveen(Moderator)
10-11-09Tuesday
12-00 am to12-50 am
12-50 am to01-10pm
01-10 pm to02-00 pm
Percutaneous Intervention forPain REvascularization
TEA
Laparoscopic OvarianCystectomy Experience ofRemote District Town
Dr. A.P.M. SohrabuzzamanSenior Consultant inInterventional Cardiology
Dr. Samar Kumar GhoshAssistant Professor (Gynae)
Professor Abduz Zaher (Chair.P)Professor of Cardiology
Professor Md. Nazrul Islam (Chair.P)Professor of Interventional Cardiology
Dr. Sarder Mokaddas Hossain (Sadi)(Moderator)
Professor Sultana Razia Begum (Chair.P),Chairman & Prof., Dept. of Obs & Gynae
Dr. Nazneen Kabir (Ch.P)Assoc. Prof. of Obs & GynaeDr. Habiba Khatoon(Moderator)
24-10-09Tuesday
11.00 pm to11-30 pm
Advancement of Orthopaedic &Trauma Management -Bangladesh Perspective
Dr. Md. Shah AlamAssociate ProfessorNITOR, Dhaka
Professor Shamsuddin Ahmed(Chair.P), Professor of OrthopaedicSurgery (Retd.)
Professor A.K.M. MahbuburRahman (Chair.P)Professor of Surgery
Professor A.H.M. Towhidul Alam(Moderator)
The following were Continuing Professionals Development (CPD) Lectures heldduring October to November, 2009
COLLEGE NEWS(J Bangladesh Coll Phys Surg 2010; 28: 66)

This corner of the journal has been introduced fromthis issue to communicate news regarding journal andits new development. In the meeting of the board ofeditors chaired by Professor AKM MahbuburRahman few decisions have been taken which will beimplemented in the forth coming journals.
Already we have started printing the names of theReviewers of the articles of that issue .Informationabout the national and international scientificseminars of different societies & subjects will bepublished in due course of time.
Fellows are requested to submit any medical miraclethat they have come across during their professionalpractice which is exciting and reportable.
Publication of an article may take long time in JBCPSso, short communication of professional and nationalinterestng topics are invited for Publications onpriority basis.
Fellows are requested to submit letters to the editor forcomments and criticism on any article and editorial.We are trying to disseminate the Journal to manydifferent web sites. www.banglajol.info has beenupdated upto 2009.Directory of Open Access Journal (DOAJ) [email protected] have agreed to include JBCPS intheir website very soon.Hope to give more new information and furtherdevelopment in the coming days. Best wishes for allthe fellows.A new email address has been activated for the editorof the Journal: [email protected] the fellowsare requested to communicate to the above mail address& can submit their articles fulfilling the requirment
Prof. Quazi Tarikul IslamEditor-in-Chief
FROM THE DESK OF EDITOR IN CHIEF(J Bangladesh Coll Phys Surg 2010; 28: 67)

Dr. Ferdousi Begum & Dr. Fahmida Zabin
Professor U.H. Shahera Khatun & Professor M.A. Salam
Prof. Sabera Khatun & Dr. Fahmida Zabin
Dr. Mizanur Ragman & Dr. Abdul Waded Chowdhury
Prof. Md. Moyeenuzzaman, Prof. Md. Ismail Patwary & Dr. Minhaj R Chowdhery
Prof. Mst. Sabera KHaitian & Dr. Laila Parveen Banu
Prof. Farhana Dewan & Dr. Fatema
Prof Md. Ismail Patary & Dr. (Lt. Col.) Mamun Mostafi
Prof. Nazmul Alan & Dr. Ahmed Murtuza
Prof. Ekhlasur Rahman & Prof. Choudhury Ali Kawser
NAME OF THE REVIEWERS OF ARTICLES IN THIS ISSUE(J Bangladesh Coll Phys Surg 2010; 28: 68)
Related Documents











