b JOINT OVERVIEW AND SCRUTINY COMMITTTEE TO REVIEW 'HEALTHCARE FOR LONDON' Date and Time: Friday, 18 January 2008 10.30 am Venue : The Guildhall, Art Gallery, Basinghall Suite (Entrance E), City of London, EC2 Democratic Services Officer : Democratic Services Despatched: 10 January 2008 Craig Barney Tel/Voicemail: 020 7926 2183 Fax: 020 7926 2361 Email: [email protected] Website: www.lambeth.gov.uk

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
b
JOINT OVERVIEW AND SCRUTINY COMMITTTEE TO REVIEW 'HEALTHCARE FOR LONDON'
Date and Time: Friday, 18 January 2008 10.30 am
Venue: The Guildhall, Art Gallery, Basinghall Suite (Entrance E), City of
London, EC2
Democratic Services Officer: Democratic Services Despatched: 10 January 2008
Craig Barney Tel/Voicemail: 020 7926 2183 Fax: 020 7926 2361 Email: [email protected] Website: www.lambeth.gov.uk

AGENDA
Appendices to reports- bulky appendices are published on the Website www.lambeth.gov.uk and can be obtained from report authors or at the meeting. They are not circulated with the agenda.
PLEASE NOTE THAT THE ORDER OF THE AGENDA MAY BE CHANGED AT THE MEETING
Page
Nos. 1. Public Agenda
1 - 40
Attached
Note: Space for members of the public will be limited at this venue, and will need to be allocated on a 'first come, first served' basis: please contact Tracey Anderson (details below).
Notice of Meeting
Joint Overview & Scrutiny Committee to review
'Healthcare for London'
10.30am on Friday 18 January 2008 The Guildhall, Art Gallery, Basinghall Suite, (Entrance E) City of London, EC2. Issue date: 10 January 2008 Contact: Tracey Anderson (020 8356 3312 – [email protected])
Committee Membership: attached.
Public Agenda
Morning Session
1. Apologies for Absence 2. Declarations of Interest
Any Member of the Committee, or any other Member present in the
meeting room, having any personal or prejudicial interest in any item
before the meeting is reminded to make the appropriate oral declaration
at the start of proceedings. At meetings where the public are allowed to
be in attendance and with permission speak, any Member with a
prejudicial interest may also make representations, answer questions or
give evidence but must then withdraw from the meeting room before the
matter is discussed and before any vote is taken.
3. Chairman's Welcome and Introduction 4. Minutes (attached) To agree the minutes of the meetings held on 30 November and 7
December 2007. 5. Project Plan (attached) To receive a revised and updated version of the Project Plan. 6. Witness Session 1 : Steve Pennant, Chief Executive, London
Connects ICT implications of implementing 'Healthcare for London' proposals.
Agenda Item 1Page 1
7. Witness Session 2
David Walker, Editor, Guardian "Public" Magazine Commentary on the issues raised for local authorities by 'Healthcare for London'. John Appleby, Chief Economist, King's Fund Financial forecasts associated with 'Healthcare for London'.
A sandwich lunch will be served at the end of the morning session, at around 1.00 p.m. The afternoon session is scheduled to begin at 1.45 p.m. Afternoon Session 8. Witness Session 3 Councillor Merrick Cockell, Leader, London Councils and Mark
Brangwyn, Head of Health and Social Care, London Councils 'Healthcare for London': The view from London Councils on the implications for local authorities. Hannah Miller, Director of Social Services, London Borough of Croydon The broader social care implications for London Boroughs.
9. Any Other Oral or Written Items which the Chair considers urgent N.B. Business for the day's proceedings has been scheduled to allow the meeting to conclude by around 4.30 pm.
[Each written report on the public part of the Agenda as detailed above:
(i) was made available for public inspection from the date of the Agenda;
(ii) incorporates a list of the background papers which (i) disclose any facts or
matters on which that report, or any important part of it, is based; and (ii)
have been relied upon to a material extent in preparing it. (Relevant
documents which contain confidential or exempt information are not
listed.); and
(iii) may, with the consent of the Chairman and subject to specified reasons,
be supported at the meeting by way of oral statement or further written
report in the event of special circumstances arising after the despatch of
the Agenda.]
Exclusion of the Press and Public
There are no matters scheduled to be discussed at this meeting that would
appear to disclose confidential or exempt information under the provisions
Schedule 12A of the Local Government (Access to Information) Act 1985.
Should any such matters arise during the course of discussion of the above items
or should the Chairman agree to discuss any other such matters on the grounds
of urgency, the Committee will wish to resolve to exclude the press and public by
virtue of the private nature of the business to be transacted.
Page 2
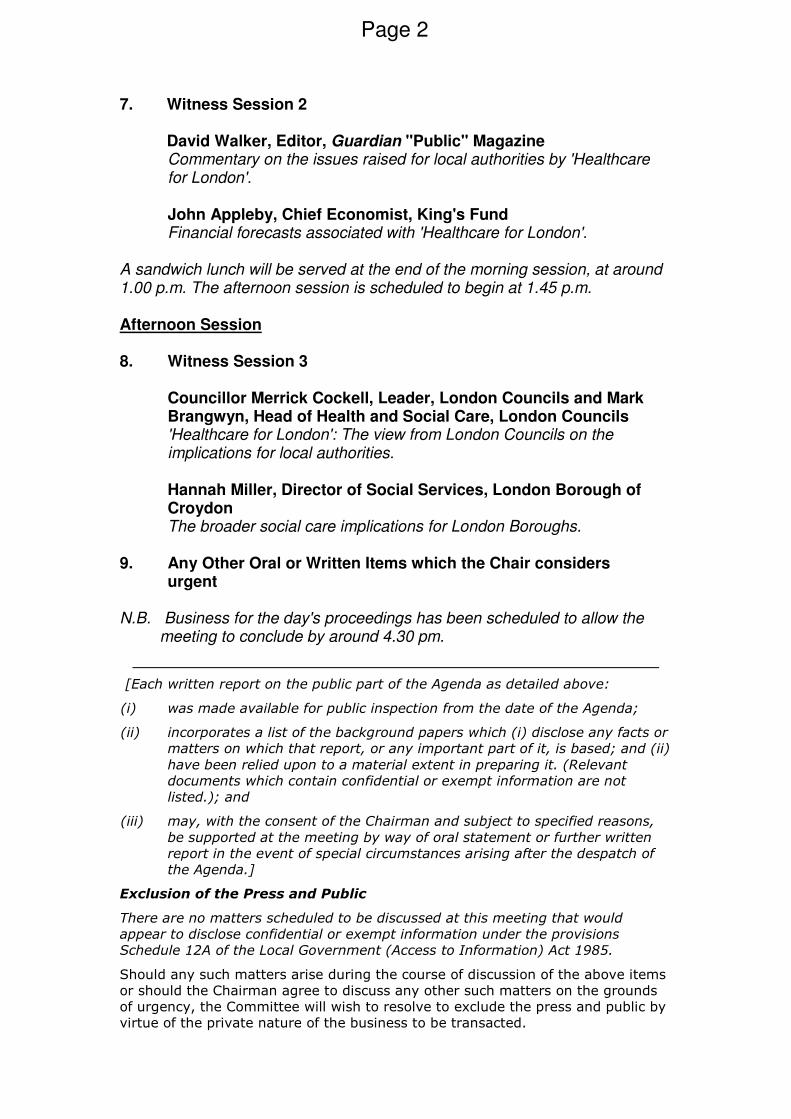
Key
A Main public entrance and access to GuildhallLibrary and Bookshop and Clockmakers’ Museum
B Guildhall Yard
C Vehicular goods delivery entrance
D Entrance to administrative departments
E Guildhall Art Gallery
F City Marketing Suite
G Guildhall Buildings
Entrances A, E and F are level. Entrance D is steppedwith handrails. Wheelchair accessible WC facilities areavailable and all major function rooms except the Crypthave inductions loops.
Parking bays are located in Aldermanbury andBasinghall Street for National Orange Badge holders(after 10am Mon - Fri and all day Sat and Sun)
BUS Nearest Routes
Bank 11 23 26 388Moorgate 21 43 76 133 141Cheapside 8 25 242London Wall 100
RAIL Nearest rail stations
Liverpool Street Cannon StreetFenchurch Street MoorgateBlackfriars City Thames Link
UNDERGROUND Nearest underground stations
Moorgate Hammersmith and City, Metropolitan, Circle, and NorthernBank Northern, Central, Waterloo and City, and DLRMansion House District, CircleSt Paul's Central
PARKING Public car parks are available at
London Wall 24 hoursBarbican 8am - midnightAldersgate 24 hours
TO BARBICAN CENTRE
TO MUSEUM OF LONDON
TO ST PAUL'S
TO LIVERPOOL STREET
MOORGATE
LONDON WALL
GUILDHALL
BA
SS
ISH
AW
HIG
HW
ALK
LOVE LANE
ALD
ER
MA
NB
UR
Y
CO
LE
MA
NS
TR
EE
T
GRESHAM STREET
CHEAPSIDE
BA
SIN
GH
ALL
STR
EET
POULTRY BANK
MO
OR
GA
TE
DLR
D
C
B
EA
GF
How to get to GuildhallCity of London • PO Box 270 • Guildhall • London EC2P 2EJ • Tel: 020 7606 3030 • www.cityoflondon.gov.uk
Page 3

Page 4
This page is intentionally left blank
PARTICIPATING AUTHORITIES London Boroughs Barking and Dagenham - Cllr Marie West Barnet - Cllr Richard Cornelius Bexley - Cllr David Hurt Brent – Cllr Chris Leaman Bromley - Cllr Carole Hubbard Camden - Cllr David Abrahams City of London - Cllr Ken Ayers Croydon - Cllr Graham Bass Ealing - Cllr Mark Reen Enfield - Cllr Ann-Marie Pearce Greenwich - Cllr Janet Gillman Hackney - Cllr Jonathan McShane Hammersmith and Fulham - Cllr Peter Tobias Haringey - Cllr Gideon Bull Harrow - Cllr Vina Mithani Havering - Cllr Ted Eden Hillingdon - Cllr Mary O'Connor Hounslow - Cllr Jon Hardy Islington - Cllr Meral Ece Kensington and Chelsea - Cllr Christopher Buckmaster Kingston upon Thames - Cllr Don Jordan Lambeth - Cllr Helen O'Malley Lewisham - Cllr Alan Hall Merton - Cllr Gilli Lewis-Lavender Newham - Cllr Megan Harris Mitchell Redbridge - Cllr Allan Burgess Richmond upon Thames - Cllr Nicola Urquhart Southwark - Cllr Martin Seaton Sutton - Cllr Stuart Gordon-Bullock Tower Hamlets - Cllr Marc Francis Waltham Forest - Cllr Richard Sweden Wandsworth - Cllr Ian Hart Westminster - Cllr Barrie Taylor Health Scrutiny chairmen for social services authorities covering the areas of all the non-London PCTs to whom NHS London wrote in connection with 'Healthcare for London' were contacted (August 2007) concerning participation in the proposed JOSC. As of 30/11/07 (the first meeting of the JOSC) those authorities who have indicated a preference for participation are as follows:
Out-of-London Local Authorities Essex – Cllr Christopher Pond Surrey County Council – Cllr Chris Pitt
Page 5

Page 6
This page is intentionally left blank
MEETING OF THE JOINT OVERVIEW AND SCRUTINY COMMITTEE
TO REVIEW HEALTHCARE FOR LONDON FRIDAY 30TH NOVEMBER 2007
PRESENT: Councillors: Marie West – L.B.Barking and Dagenham
Richard Cornelius – L.B.Barnet David Hurt – L.B.Bexley Chris Leaman – L.B.Brent Carole Hubbard – L.B.Bromley Patricia Callaghan – L.B. Camden Graham Bass – L.B.Croydon Mark Reen – L.B.Ealing Mick Hayes – L.B.Greenwich Jonathan McShane – L.B. Hackney Peter Tobias – L.B.Hammersmith&Fulham Gideon Bull – L.B. Haringey Vina Mithani – L.B. Harrow Ted Eden – L.B.Havering Mary O’Connor – L.B.Hillingdon Jon Hardy – L.B.Hounslow Meral Ece – L.B.Islington Christopher Buckmaster – L.B.Kensington and Chelsea Don Jordan – Kingston upon Thames Helen O’Malley – L.B.Lambeth Alan Hall – L.B.Lewisham Gilli Lewis – Lavender – L.B.Merton Stuart Gordon-Bullock – L.B. Sutton Allan Burgess – L.B.Redbridge Nicola Urquhart – L.B.Richmond Stephanie Eaton – L.B. Tower Hamlets Marc Francis – L.B. Tower Hamlets Richard Sweden – L.B.Waltham Forest Ian Hart – L.B. Wansworth Barry Taylor – L.B.Westminster Chris Pond – Essex Chris Pitt - Surrey County Council
Officers: Tim Pearce – L.B.Barking & Dagenham
Graham Amita – L.B.Bexley Amanda Flower – L.B.Bexley Jacqueline Casson – L.B.Brent Graham Walton – L.B.Bromley
Page 7
Michael Carr – L.B. Camden Shama Smith – L.B.Camden Neal Hounsell – City of London Corporation Solomon Agutu – L.B. Croydon Trevor Harness – L.B. Croydon Nigel Spalding – L.B.Ealing Tracy Carpenter – L.B. Greenwich Alain Lodge – L.B.Greenwich Ben Vinter – L.B.Hackney Doreen Forester-Brown – L.B. Hackney Tracey Anderson – L.B.Hackney Sue Perrin – L.B. Hammersmith & Fulham Kevin Unwin – L.B. Hammersmith & Fulham
Lynne McAdam – L.B.Harrow Anthony Clements – L.B. Havering Guy Fiegehen – L.B.Hillingdon David Coombs – L.B.Hillingdon Sunita Sharma – L.B.Hounslow Deepa Patel – L.B.Hounslow Rachel Stern – L.B.Islington Gavin Wilson – R.B. Kensington & Chelsea Dave Burn – L.B.Lambeth Elaine Carter – L.B. Lambeth Barbara Jarvis – L.B.Merton Jeanette Phillips – L.B.Richmond Phil Williams – L.B.Waltham Forest Tasneem Mueen – L.B.Westminster Phillipa Stone – L.B. Westminster Derek Cunningham – Surrey County Council
1. WELCOME AND INTRODUCTIONS Councillor Peter Tobias stated that as the representative of the
hosting borough he would like to welcome Councillors and officers to the meeting and that joint scrutiny by some 31 boroughs was an historic occasion.
Councillor Tobias informed the meeting that the officer support group would conduct the procedure for the appointment of Chairman and Vice-Chairman’s. It was noted the JOSC wanted the elected members to the position of Chairman and Vice Chairmen to be from each of the three major political parties.
2. APPOINTMENT OF CHAIRMAN AND VICE-CHAIRMEN Councillors Mary O’Connor (Hillingdon) (Conservative) and
Barry Taylor (Westminster) (Labour) were nominated for Chairman. Councillor Taylor stated that he did not wish his name to go forward for appointment as Chairman.
Page 8
This being stated Councillor Mary O’Connor was appointed as
Chairman.
Councillors Christopher Buckmaster (Kensington & Chelsea) (Conservative), Allan Burgess (Redbridge) (Conservative), Meral Ece (Islington) (Liberal Democrat), Barrie Taylor (Westminster) (Labour), Peter Tobias (Hammersmith & Fulham) (Conservative) and McShane (Hackney) (Labour) were nominated for Vice-chair. Councillors Buckmaster, Burgess, and Tobias are from the same party as the Chairman and were therefore excluded from the next stage of the process.
Councillor Meral Ece (Islington) (Liberal Democrat) was the only Liberal Democrat member nominated for Vice Chairman so therefore was appointed as Vice Chairman.
The two nominees for the second Vice Chairman (Labour): Councillors McShane and Taylor briefly explained why they believed they should hold the post.
A vote (by show of hands) followed: Councillor Taylor: 13 Councillor McShane 4
Councillor Taylor was nominated as Vice Chairman.
A vote (by show of hands) on the view that there should be three Vice Chairmen, the third to reflect independents, followed: In favour: 4 Against : 12
The Officer support handed over the meeting to the newly elected Chairman Cllr O’Connor.
Councillor O’Connor took the Chair.
3. DECLARATIONS OF INTEREST Cllr Carole Hubbard - London Borough of Bromley, declared
that she is an employee of Bromley PCT. Cllr Vina Mithani - London Borough of Harrow, declared that she is employed by the Health Protection Agency.
4. APOLOGIES FOR ABSENCE Apologies were received from Councillors David Hurt (Bexley),
Page 9
David Abrahams (Camden), Ken Ayres (City of London), Janet Gillman (Greenwich) and Alan Hall (Lewisham) and Councillor Gill Lewis-Lavender (Merton) for lateness.
5. PROPOSED TERMS OF REFERENCE The terms of reference were approved subject to the inclusion
of ‘people travelling across the GLA boundary with due regard to cross-border issues’ at the end of paragraph 2.
6. PROPOSED RULES OF PROCEDURE The rules of procedure were approved subject to the following
amendments: (i) to be made explicit that membership of JOSC is from elected members; and that, in the event of a vote, a substitute member would have the right to vote on the same way as the main member; should the member and nominated substitute be unable to attend, it was permissible to for another substitute to attend and have a right to vote; (ii)Voting, paragraphs 7-8 the final report to include both majority and minority recommendations; (iii) Local Overview and Scrutiny Committees, Havering proposed an amendment to the "Procedures" paper - specifically to paragraphs 17 -19, on Local OSCs.to: 1. The Joint Committee will invite local health overview and scrutiny committees (including any joint overview and scrutiny committees of two more boroughs) to make known their views on the proposals contained within the consultation.
2. The Joint Committee will consider those views in making its conclusions and comments on the proposals outlined in the consultation document.
3. Local health overview and scrutiny committees (including joint overview and scrutiny committees) will be encouraged to gather views from local NHS bodies and interested parties and advise the Joint Committee of instances where the Joint Committee should take evidence.
7. DRAFT PROJECT PLAN (i) Members wanted to have as much time as possible to hear
evidence on such a large and complex set of proposals, which would have far reaching consequences. However, the timescale was very tight. Timescale 1 had been planned by NHS London on the basis of getting views back before the start of the ‘purdah’ period for the GLA elections in May 2008, i.e. the process was being driven by the election of a body not involved in the consultation. Timescale 2 was the possible timescale should NHS London extend the deadline. The legal officer from the London Borough of Hackney, who
Page 10
was present at the meeting, advised she would need to see the legal advice NHS London received on Purdah to give the committee advice at the next meeting on the implications of purdah for the JOSC and reporting timescale. Officers were asked to seek advice on the proposal that the committee continued taking evidence up to the start of the purdah period, suspend member activity during purdah and meet again after the GLA elections to agree their response.
(ii) Clinicians who were not directly involved in the review would be invited to attend.
(iii) One meeting only had been scheduled for February 2008 to allow adequate time for the report to be written. The Chair and vice, in conjunction with officers, would schedule an additional witness session for early February 2008. It was agreed that the 2008 meetings would commence at 10.30am.
(iv) Clinical teams would look at particular aspects and proposals. It was agreed that the development of a two way dialogue would be facilitated by access to these teams and that observer status should be requested.
(v) Suggestions were made for the following additions to ‘themes and witnesses’:
(a) Themes Cross boundary issues Finance Learning disabilities Maternity services Older peoples services Polyclinics (look at the experience of the United States and the John Hopkins model and visit facilities in the United Kingdom, as several models had already been adopted although not always called polyclinics) Social care Transport
(b) Witnesses BMA/Royal Colleges Health Protection Agency Healthlink, patients’ parliament Journalists (Times if possible) Kings Fund (respected in the field of health economics) Local Medical Committee London Councils Mental Health organisation such as MIND or the
Page 11

PCT representative from periphery of London (cross boundary issues) Sainsbury’s centre for mental health Patients and Public Involvement Forums (hospitals, PCTs and London Ambulance Services)
It was the role of this committee to take a strategic approach. Active local organisations such as the Lambeth users’ group would be consulted by their local health scrutiny committee as the consultation process was rolled out.
(vi) The South West region officer network was asked to re-consider the appointment of a member to the officer support group.
(vii) The order of implementation of the recommendations was very important and a timescale for the process had not been given.
(viii) The report did not give a convincing answer as to how services would be provided for London’s rising population.
(ix) It was agreed that at the beginning of each meeting there would be a resume of what had been covered to date.
Action: 1. The legal officer, London Borough of Hackney to advise the committee, at its next meeting, of the implications of purdah for the timescale or clarification be sought from NHS London. 2. Officers to seek advice on the proposal that the committee continue to take evidence throughout the purdah period, suspend member activity during purdah and meet again after the GLA elections to agree their response. 3. NHS London to be asked for observer status for the JOSC on the clinical teams. 4. Briefing notes given to future speakers would be copied to the committee.
The meeting adjourned at 11.30pm and reconvened at 1.30pm. Copies of the final version of the JCPCT consultation document were received and distributed.
8. RICHARD SUMRAY, CHAIR OF JOINT COMMITTEE OF LONDON PCTs
Councillor O’Connor introduced Richard Sumray, Chair of Joint Committee of London PCTs (JPCT) and Chas Hollwey of
Page 12

Barnet PCT.
During the presentation and discussion with the Chairman of the JPCT the following main points were made –
• The decision making process would be flexible with as many decisions as possible being made at local level by individual PCTs. Decisions would be made a higher level only if imperative to do so.
• The first stage consultation had been delegated to PCTs, which would involve as many people as possible, including ‘hard to reach groups’. The consultation was not about specifics, but the direction of travel and the different strands of the report. At the end of the process all information would be gathered and analysed. There would be various stage 2 consultations to discuss local implementation, with key decisions being made during this phase.
• The JCPCT, which had been set up specifically for the purpose of the first stage consultation, would meet monthly, and would meet in public when decisions were being made; i.e. at the end of the consultation. The JCPCT would seek to ensure that all PCTs gave the same message and same level of consultation, but there would be some local variations to meet the needs of boroughs.
• The consultation would be focus on public health; how inequalities in health would be dealt with, improved and changed. Whilst the proposals were medically centred, extension to social care would give added value.
• Funding had been allocated for the consultation. There had been a broad financial appraisal of the end costs, and the proposals were believed to be affordable in line with the increased funding (significantly above inflation) for healthcare in London. NHS finances overall had been turned around in the last 18 months, although there remained a few trusts with deficits.
• Implications for social services had not been integrated into the document and it was anticipated that these would be identified through consultation with local authorities.
• There were no plans for re-organisation of PCTs in the short to medium term, although it was likely that the joint commissioning role with local authorities would be strengthened, and that the provider role would be lessened.
• Consultation currently underway tended to be compatible
Page 13

with Healthcare for London.
9. RUTH CARNALL, CHIEF EXECUTIVE, NHS LONDON
Cllr O’Connor introduced Ruth Carnall, Chief Executive, NHS London and Bill Gillespie, Interim Communications Director of NHS London.
During the presentation and discussion with the Chief Executive from NHS London the following main points were made –
• A ‘big bang’ approach was not possible; some changes would require more in depth work/investment. Changes would be implemented by PCTs at local level.
• The quality of hospital food was an important issue for the Chief Nurse, and it was believed that it was improving, but there would be continued vigilance.
• Implementation would primarily be at local and there were already incentives within the system to ensure change. Hospitals were responsible to PCTs and could be held to account through contracts.
• The outcomes of other reviews, such as the North West London Strategy, and the Imperial College Healthcare NHS Trust would have to be balanced with the consultation and some local issues go ahead, for example if the changes were in line with Framework for London or if there were issues of patient safety.
• There were no proposals in respect of PCTs and foundation trust status. The organisational form would be derived from the consultation strategy: a partnership agenda between them would need to work at sector level to bring about effective commissioning of services. There were already a number of joint appointments between local authorities and PCTs and it was likely that there would be a range of different models.
• With respect to pathology services, the development of a larger facility would bring about cost efficiencies, but local x-ray facilities for example could be provided at a polyclinic to meet access criteria.
• NHS London did not plan to top slice PCT budgets again and some £135million had already been returned. Additionally, PCTs would be allowed to retain surpluses. Through the commissioning process, PCTs were able to
Page 14
direct resources where best services can be delivered to patients. NHS London would challenge the use of resources without interfering and would allow more freedom to good performing PCTs.
• NHS London would welcome any advice from the JOSC as
to the success or otherwise of the project. Similarly, local authorities are keen to be proactive and to have broader engagement, without compromising their ability to critic. This could be achieved by the JOSC network aligned to the clinical networks. Chief Executive for NHS London stated that JOSC involvement would be very helpful and that NHS London would provide project resources for these proposals.
• Diabetes had been selected as an example of a care pathway, which would provide an opportunity to work through the care settings for people with complex needs. Care should not revolve through a local hospital, but with complex multi-disciplinary needs being balanced with attendance at a specialist centre.
• Mental health providers had been enthusiastic about polyclinics and integration with primary care services. There had been significant progress in the provision of care outside of hospitals.
• There would be a further review of mental health and childrens’ services as these had not been covered in adequate depth.
• Benchmarking was currently fairly insular, but it was planned to extend the boundaries and to look at good practice in the rest of the world, as well as drawing on the national review of good practice.
• The multiple care needs of patients would be assessed on the basis on what could be provided in their own home in a more integrated way; what could be provided in a polyclinic; and what could be provided in a more integrated way.
• NHS London did not want foundation trusts to sell land and other assets to balance their books. However, there were costs associated with owning assets which were not used. An estates plan was being developed, which would stipulate what trust could do with their assets before foundation trust status.
Councillor O’Connor thanked Ruth Carnall and Bill Gillespie for attending.
Page 15
10. DATE OF NEXT MEETING
7th December 2007 at 10.00am, Council Chamber Camden Town Hall
Page 16
Appendix One – Amended Terms of Reference for JOSC JOINT OVERVIEW & SCRUTINY COMMITTEE TO REVIEW 'HEALTHCARE FOR
LONDON'
TERMS OF REFERENCE
1. Consider and respond to the proposals set out in the PCT consultation document 'Healthcare for London: A Framework for Action';
2. Consider whether the 'Healthcare for London' proposals are in the interests of
the health of local people and will deliver better healthcare for the people of London noting people travelling across the GLA boundary with due regard to cross-border issues
3. Consider the PCT consultation arrangements - including the formulation of
options for change, and whether the formal consultation process is inclusive and comprehensive.
Page 17

Page 18
This page is intentionally left blank

1
MEETING OF THE JOINT OVERVIEW AND SCRUTINY COMMITTEE
TO REVIEW HEALTHCARE FOR LONDON FRIDAY 7TH DECEMBER 2007
PRESENT: Cllr Mrs. Marie West - London Borough of Barking and Dagenham Cllr Richard Cornelius - London Borough of Barnet Cllr Graham D’Amiral - London Borough of Bexley Cllr Chris Leaman - London Borough of Brent Cllr Carole Hubbard - London Borough of Bromley Cllr David Abrahams - London Borough of Camden Cllr Bass - London Borough of Croydon Cllr Mark Reen - London Borough of Ealing Cllr Jonathan McShane - London Borough of Hackney Cllr Martin Newton - London Borough of Haringey Cllr Vina Mithani - London Borough of Harrow Cllr Mary O Connor - London Borough of Hillingdon (Chairman) Cllr Jon Hardy - London Borough of Hounslow Cllr Merel Ece - London Borough of Islington (Vice Chairman) Cllr Helen O’Malley - London Borough of Lambeth Cllr Alan Hall - London Borough of Lewisham Cllr Gilli Lewis-Lavender - London Borough of Merton Cllr Megan Harris Mitchell - London Borough of Newham Cllr Alan Burgess - London Borough of Redbridge Cllr Nicola Urquart - London Borough of Richmond upon Thames Cllr Stuart Gordon Bullock - London Borough of Sutton Cllr Stephanie Eaton - London Borough of Tower Hamlets Cllr Richard Sweden - London Borough of Waltham Forest Cllr Ian Hart - London Borough of Wandsworth Cllr Barrie Taylor - London Borough of Westminster (Vice Chairman) Cllr Chris Pond - Essex County Council Cllr. Chris Pitt - Surrey County Council ALSO PRESENT: Officers: Tim Pearce – L.B.Barking & Dagenham Bathsheeba Mali – LB Barnet Louise Peek – L.B.Bexley Jacqueline Casson – L.B.Brent Graham Walton – L.B.Bromley Michael Carr – L.B. Camden Shama Smith – L.B.Camden Neal Hounsell – City of London Corporation Trevor Harness – L.B. Croydon Alain Lodge – L.B.Greenwich Ben Vinter – L.B.Hackney Tracey Anderson – L.B.Hackney
Page 19
2
Sue Perrin – L.B. Hammersmith & Fulham Nahreen Matlib – L.B.Harrow Guy Fiegehen – L.B.Hillingdon David Coombs – L.B.Hillingdon Sunita Sharma – L.B.Hounslow Deepa Patel – L.B.Hounslow Peter Moore – L.B.Islington Gavin Wilson – R.B. Kensington & Chelsea Elaine Carter – L.B. Lambeth Barbara Jarvis – L.B.Merton Greg Leahy – L.B. Newham Jilly Mushington L.B. Redbridge Jeanette Phillips – L.B.Richmond Upon Thames Shanara Matin – L.B. Tower Hamlets Phil Williams – L.B.Waltham Forest Tasneem Mueen – L.B.Westminster Phillipa Stone – L.B. Westminster Derek Cunningham – Surrey County Council Speakers Dr Martin Wake – Joint Medical Director of Sutton and Merton Primary Care Trust Dr Chris Streather – Medical Director of St Georges Healthcare NHS Trust Dr Fiona Campbell – healthcare consultant
CHAIR’S ANNOUNCMENTS
Future meetings
All future meetings will start at 10:30 and conclude at 4:30pm, with the option of a 30 minute extension.
The Joint Overview and Scrutiny Committee (JOSC) and Officer Support Group will be available for ½ hour before each meeting to discuss the approach to questioning in advance of receiving evidence.
The Officer Support Group will circulate suggested lines of questioning in advance of each meeting.
The minutes from last week’s meeting and today will be circulated with the agenda of our next full meeting.
Dates
The following timescale for meetings was proposed;
1. 18th January
2. 22nd February 3. 14th March
Page 20

3
4. 28th March 5. 25th April – Final meeting and consideration of the scrutiny report.
The deadline for the final scrutiny report is 2nd May 2008.
Venue for next meeting
Venues and speakers will be confirmed with the agenda pack for our next meeting. It is proposed that the next meeting will take place at the Corporation of London (Guildhall) on 18th January 2008.
The JOSC Scrutiny Report
It is presently envisaged that the Officer Support Group will assist the committee in preparing the report. However requests may, in due course, be made for additional support, if this is required.
Submissions
All submissions proposed for consideration in the formal papers for this committee need to be submitted to the Officer Support Group no later than 2 weeks in advance of any of the declared meeting dates.
The Chairman and Vice Chairs will exercise the final decision about what papers will be included in an agenda dispatch.
Written submissions are invited from any affected local authority, local Overview and Scrutiny Committee or interested organisation. Any such documents should be submitted to the Officer Support Group no later than 29th February 2008.
Legal Advice
Legal advice has been sought from legal officers in relation to the operation of the JOSC. The London Borough of Hackney’s legal representatives were at the last meeting of the committee and are happy to continue to contribute.
The Chairman summarised the key points from the witness session JOSC: 30th November 2007:
• Decisions on the future of health services should be taken as locally as possible: i.e. by individual PCTs or small groups of PCTs rather than a pan-London JCPCT.
• The Darzi report presents an opportunity to ensure health services meet future needs of London. However there are concerns about whether the NHS will be able to implement reforms due to the financial systems in place, and the lack of incentives for NHS Trusts to reform.
Page 21

4
In particular there is concern about the autonomy of Foundation Trusts. Note that previous attempts at reform have failed.
• It is vital to future-proof reforms to health services: i.e. the NHS must plan for future demographic changes including the population growth in the Thames Gateway.
• There are concerns and uncertainty about how the proposals could be implemented and in which order. There is a danger of a ‘salami slicing’ of services away from some district hospitals and this could lead to uncertainty in NHS Trusts in their financial and service planning.
• There are still some uncertainties about the future of PCTs: another round of organisational restructuring of PCTs could undermine or distract from the implementation of any of the Darzi proposals.
• This JOSC is only the start of the involvement of scrutiny councillors: the NHS must continue to informally discuss proposals for health services with local health scrutiny councillors outside of the formal scrutiny committees. This will enable local councillors to feed in views from the local community and help manage future formal consultations.
1. APOLOGIES FOR ABSENCE Cllr Ken Ayers - City of London Cllr Marie Pearce - London Borough of Enfield Cllr Janet Gilman – London Borough of Greenwich Cllr Peter Tobias - London Borough of Hammersmith and Fulham Councillor Ted Eden - London Borough of Havering Cllr Christopher Buckmaster - London Borough of Kensington and Chelsea Cllr Ken Smith - London Borough of Kingston upon Thames Cllr Micheal Seaton - London Borough of Southwark Cllr Gideon Bull – London Borough of Haringey 2. DECLARATIONS OF INTEREST Cllr Carole Hubbard - London Borough of Bromley, declared that she is an employee of Bromley PCT Cllr Vina Mithani - London Borough of Harrow, declared that she is employed by the Health Protection Agency 3. PRESENTATION: ‘HEALTHCARE FOR LONDON’: A FRAMEWORK
FOR ACTION Dr Martin Wake – Joint Medical Director of Sutton and Merton Primary Care Trust and Chairman of the “Planned Care” Pathway Clinical Working Group in the Darzi Report Review Team and Dr Chris Streather – Medical Director of St Georges Healthcare NHS Trust and member of the “Acute Care” Pathway Clinical Working Group in the Darzi Report Review Team, addressed the
Page 22
5
committee to give a presentation and answer questions on the background and rationale behind the Darzi review, including how and why the proposed models of care and delivery were developed. Dr Streather explained that the Darzi report went back to the experience of patients and considered the quality of care, unlike previous health reviews that have focused more upon health institutions. A great deal of diagnostic work has been carried out, as well as the research agency MORI providing consultation information, asking patients what they perceive as problems in the health service and health inequalities. The acute care pathway is very complicated for patients. 70% of calls that go to NHS Direct have to be redirected. A lot of people therefore choose Accident and Emergency as the simplest option. One of the Lord Darzi’s objectives is to make patients’ choice simpler and easier to discern. There is a need to provide accessible community care in community based settings near to where people live and urgent primary care located where patients are; to localise where possible and centralise where necessary; the “hub and spoke” model. There are some services that may be better centralised, e.g. complex trauma, stroke care. At the moment there is a mortality cost in providing stroke care in local settings; this is a cost of not centralising. There is a need to take active measures to improve stroke care in London. 70 – 80% of patients would still be treated in local stroke units, but with high tech care to the smaller number of people who need it. The vast majority of care should still be delivered in local hospitals, so there is a need to maintain skills and quality of care in district hospital units. Big institutions would be overwhelmed if large amount of care currently provided by district hospitals moved to large specialist centres; centralising should only take place where this improves the quality of care for the minority of patients that need specialist care. Dr Wake explained he is also a GP with 25 years experience had has seen health care change hugely during that time noting he had been chairman of the Planned Care group; one of the sub committee groups contributing to the background to the Darzi investigation and report. He said that although health services are not poor in London overall, they are patently poor in some areas. He said that specialist care would be improved by a degree of centralisation in specialist centres e.g. the Marsden Hospital and that some services would be better decentralised. He said that surgery in London is way behind the best in the country. Centralising care can be achieved in a variety of ways. Elective care, e.g. hip and knee replacements, eye surgery etc can be located in stand alone areas separate from emergency care. On the other hand, other services such as cancer surgery could be delivered through worldwide centres where a large number of specialist surgeries can be performed. This type of surgery is
Page 23

6
better provided in a small number of centres, providing more economic and better quality outcomes. The Darzi report envisages a shift towards community-based care, where routine diagnostic tests can be carried out locally. Community support and rehabilitation services have suffered from a lack of investment up until now, which means that people are being cared for in a hospital setting when it would be better to receive care at home. More investment here would promote independence and support early discharge from hospital and also prevent admission for people where hospital based care is inappropriate. This would also improve choice for end of life support services; the choice to die at home. At the moment approximately 20% of deaths take place at home, but more than 50% of people would choose to die at home as a first choice. He said there was a need to integrate some pre and post care pathways, e.g. integration of nursing care, intermediate care and end of life care. Overall there is a need to keep the strategic focus on the patient as an individual. The Darzi report envisages the emergence of “polyclinics”; which can be a building or a network of buildings that have services appropriate for a locality, e.g. a network of GPs. The proposal is to have a polyclinic attached to each hospital site which includes an urgent care centre run by primary care. Polyclinics will have to be sensitive to local needs and no polyclinic will look exactly like another. This could provide a great opportunity for social care to bring together services for older people. Questions
Q It was asked why these reforms will be implemented when other attempts to improve hospitals have not.
It was responded that an important strength of the Darzi review is that it has considered the perspective of pathways to care by patients rather than a purely institutional perspective. It is also more clinically driven and the clinician’s perceptive is important in making proposals feasible and credible in the NHS.
Q It was asked how the review will attempt to change people’s perception of pathways to care and the new approach.
It was responded that we need to start by changing the reality of care provision, e.g. choice about the use of GP services and GP surgery opening hours, e.g. evenings and weekends. Some patients want to be seen quickly, some want continuity and we need to ensure that both of these objectives can be met within polyclinics.
Page 24
7
Q It was stated that the past few years has seen pressures to close local hospitals and health services and that some of the Darzi proposals seem to suggest a reversal of this.
It was responded that we need to consider the costs and benefits of the localisation of care, but that there needs to be a presumption in favour of local provision, e.g. blood testing can be carried out in GP clinics. Hospice care should continue, although at the moment a lack of capacity means that more patients cannot be provided for. End of life care at home is not cheaper than hospitals and services can be difficult to co-ordinate. A significant problem is the overuse of Accident and Emergency in hospitals. This is caused by reduced opening hours and under capacity at GP surgeries, but it is also the result of a more mobile population in London, where many people are not registered with a GP. A&E services are also a victim of their own success, as people know that they will be seen.
Q It was asked if NHS London was ready and able to introduce the big changes implied from the Darzi report.
It was responded that there is a real change in the tone about strategy and strategic planning in the NHS. A lot of emphasis has been focused upon meeting performance indicators and budgets and this review is an attempt to change this towards a more strategic approach. In addition, there are a lot of people who have profound influence within the NHS involved in this review.
Q It was asked if it will be possible to provide more flexible GP opening hours and if the GP contract can be re-negotiated to accommodate this.
Dr Martin responded that he was not aware of any national negotiations to extend GP contracts but that GP contracts are now subject to local negotiation. The introduction of polyclinics could be a mechanism by which to review GP contracts.
Q It was asked about the sites for possible infrastructure developments, and given the shortage of land in London, if this was already being considered.
Dr Martin responded that the NHS is aware of how long it can take to bring about change of this level and the NHS is reviewing the estates it already has, some of which are not currently being put to full use. One of the fears is that the Darzi review could lead to an over-centralised model, and this needs to be avoided, as it could impact upon the capacity of local hospitals to carry out elective work. There is the possibility of elective centres in district hospitals.
Q It was asked what guarantee there is that Londoners would have improved access to GP services.
Page 25
8
Dr Wake agreed that patients should not have to wait for GP appointments and that the onus will have to be on PCTs to commission effective GP services. PCTs are variable in their effectiveness in monitoring GP contracts and they are increasingly their role is one of commissioning hospital and GP services. He said that there needs to be pressure to provide better services and that there is a need to work closely with local authorities.
Q It was asked if the Darzi review will bring in a centralised model of care under the guise of polyclinics. Can it be assured that the model will not be too prescriptive?
Dr Streather responded that local proposals will be drawn up in consultation borough by borough and that there was no appetite for a prescriptive model for the whole of London. It is part of the role of overview and scrutiny to hold the NHS to account for the scale of localisation. Type 2 diabetes care, for example, should be provided close to the patient’s home as far as possible.
Q It was asked if the Darzi review will actually increase the scope for patient choice.
There should be flexibility and the non prescriptive nature of the new polyclinics should provide for patient choice. PCTs should seek to commission services that are appropriate and affordable in consultation with local people.
Q A concern was raised that despite the benefits of centralising trauma services and stroke services, access may be impaired because of London transport congestion. Have journey times been factored into the strategy?
Dr Streather said that the London Ambulance Service is very good at estimating journey times in London. Some periods, e.g., in the middle of the night journey times are relatively short. In the middle of the day there is a need to make sure that there are enough accessible rapid response centres e.g., (stroke centres etc.). Otherwise, centralised care can provide further health inequalities. It should be quite straight forward to define access as part of the quality description for those services.
Q If there is to be greater use of day surgery, this will provide real challenges especially to older people, as many people require after care support.
Hip replacements in hospitals are down to just a few days, but there is a need for very good home visiting therapists. It was commented that mental care and children’s care services are not given enough emphasis in the report but there is further work being carried out in these areas.
Page 26

9
Q It was asked if a weakness of the Darzi report was that it focussed too much on the NHS rather than looking at a spectrum of care including social care.
Dr Streather responded that there is a great deal of talk about improving linkages and breaking down some of the barriers between professionals in health, primary care/secondary care, and social care.
Q It was asked how the local consultation and process can be meaningful and clear since the principles in the Darzi report provide very little details for local areas.
It was responded that there is a consultation document available from NHS London, which will be delivered to every council. Dr Wake responded that details about local area consultation are deliberately absent from this document. PCTs are expected to consult locally on the principles of the document, consultation on a framework which may result in service changes.
Q It was asked which population statistics will be used given the high migration figures for London?
Dr Wake responded that there is a need to work with local authorities to get accurate population estimates but conceded that this is difficult in London with high rates of migration.
Q It was asked that, since there are difficulties recruiting GPs, how GPs will be retained and new GPs recruited into London.
Dr Wake responded that PCTs are very aware of the number of GPs coming up to retirement. It is easier for GPs to get employed status rather than to become practice partners, but this fits very well with the concept of polyclinics. There are large numbers of new GPs currently being trained.
Q It was asked what consideration has been given to cross-border issues e.g., people who commute into London.
Dr Streather responded that there was a tension between not imposing a single model and avoiding local arrangements which increase health inequalities. The approach should encourage high clinical standards and yet allowed local determination of how to deliver these. If we import people into our boundaries there is a need to ensure quality but also be open about the resource implication.
Q It was asked if GPs will sign up to employee status. Dr Wake said that a significant number of GPs want to be NHS employees, a younger generation often seem to prefer a salaried situation and that this is an increasing trend.
Page 27
10
Q It was asked if extra money will be made available by the government to introduce proposals from this review.
Dr Wake said that the NHS will be expected to make the best use of the resources it has as it has had a high level of funding in recent years, although it is possible to envisage extra government help with transitional arrangements.
Q A question was asked about public perceptions about how to access to services, in view of the range of access points available.
It was responded that it is important to consider access to care as it has been much too complex for patients.
Q It was asked what the role of the General Hospital will be in the context of the proposals for polyclinics. Is leaving this to PCTs to determine not putting too much strain on local commissioning services?
It was responded it is envisaged that most people who go to a General Hospital now will go there in the future.
Q It was asked what the government’s view was as to how GPs would work under the proposals.
Dr Wake responded that this depends on the model of GP care that is commissioned by the PCT and that there is scope for a variety of different models and different roles for GPs.
Q It was asked what is required and what the best process is for upgrading skills in line with the proposals.
Dr Streather responded that in the past there has been insufficient surgery in local hospitals to train local surgeons and that there is a need to manage this more proactively.
4. PRESENTATION: ‘HEALTHCARE FOR LONDON’: REPORT TO LONDON COUNCILS FOR LONDON BOROUGHS’ OVERVIEW & SCRUTINY COMMITTEES
Dr Fiona Campbell, healthcare consultant, delivered a presentation on the main findings and conclusions of the report. Dr Campbell said that although it may be in the nature of scrutiny to focus upon the negative aspects of proposals, it is important not to loose sight of the very positive aspects of the Darzi review, as she believes that it is a genuine attempt to improve health services in London. One of the key strengths of the review is that it has tended to take a patient's pathway perspective through healthcare.
Page 28

11
Dr Campbell set out the context for the review:
• It provides a ten-year vision
• Many of the issues are a focus of national attention
• Little detailed reference to social care
• Further work still being done She set out the key consultations being undertaken:
• Six clinical working groups and one on mental health with chief executives
• Opinion Leader consultation events (voluntary sector and public)
• Written consultation – 67 submissions
• Ipsos Mori telephone survey (7,000)
• Healthlink supporting consultation with traditionally excluded groups
• Other meetings and events The consultation document on the models of care was published on 30 November. Consultation ends 7th March 2008, with further work on mental health and children’s services after that. There is a parallel health inequalities impact assessment carried out by London Health Commission, but there are concerns that it may not be available until the end of the scrutiny process. The NHS is currently carrying out a review of its estates, but this review has not yet reported. Dr Campbell set out the proposals for the second stage consultation.
• Second stage consultation will be focused on practical application of the proposals
• Second stage consultation will be subject to outcome of first stage consultation
The second stage consultation will be likely to be at different levels depending on the scale of the proposal being consulted upon:
• pan London
• regional/cluster (e.g. NE London/SW London)
• individual PCT/LA area
• surrounding counties This may need further joint overview and scrutiny committees; which may imply further work for this established committee. Dr Campbell outlined Lord Darzi’s case for change:
• Healthcare in London is not good enough
• Specific London challenges
• Low levels of satisfaction
• Inequalities
• Moving out of hospital
• Centralising emergency care
• London’s historical role
• Effective use of workforce and buildings
Page 29
12
• Funding issues – e.g. reducing hospital stays to England average “would save £200m”.
Dr Campbell outlined the principles of the review:
• Focus on individual needs and choices
• Localise where possible, centralise where necessary
• Truly integrated care and partnership working
• Prevention is better than cure
• Focus on health inequalities and diversity Dr Campbell outlined the focus of the report:
• Maternity and newborn care
• Staying healthy (i.e. prevention of ill health and health improvement)
• Mental health
• Acute care (i.e. “accident and emergency”)
• Planned care (i.e. elective treatment which can be planned in advance, e.g. hip replacements)
• Long-term conditions (e.g. diabetes, asthma)
• End-of-life care (issues such as giving people a choice about where they die)
Dr Campbell outlined some key questions for scrutiny committee – listed in Appendix One. Questions
Q It was asked if the NHS would be able to deliver the proposals. Dr Campbell responded that the approach has been to involve clinicians and that this may prove more successful than in the past.
Q A question was asked about preventative healthcare. Dr Campbell responded that prevention may not always be more expensive than treatment but that upfront investment is needed and an ‘invest to save’ approach.
Q Concerns were raised as to the relocation of healthcare services where distance from home is too great, for example, issues of removing personal links with family and friends, culture and knowledge of the area.
It was responded that distances for treatment are a trade off between individual’s own priorities and the best health outcomes.
Q It was stated that there is a lack of clarity about how urgent healthcare centres are envisaged as opposed to A&E.
Page 30

13
It was responded that both urgent care and A&E will be attached to polyclinics but that it is envisaged to have separate centres for ‘urgent care’ from A&E. Dr Campbell suggested that comparisons can be drawn with New York, which has already gone down the road of centralisation. Expert witnesses from New York may be useful to talk about this experience.
Q Given less dense population, it was asked if the notion that polyclinics should serve an area of 50,000 people and yet be local is not a contradiction in terms for outer London.
It was responded that this population area figure is an average and that each borough will have to consider the implications for populations served for their own area. Planning and infrastructure issues will be considered in phase 2 of the consultation.
Q It was asked what the implications might be for information technology, e.g., costs, use of IT and service delivery, implications for privacy and security.
It was responded that there is a proposal for a common database for NHS patients, although this may run into problems. It was suggested to ask the NHS ‘Connecting for Health’ programme that is considering this.
Q It was asked what the impact on local authorities might be and what investment there might be for local authorities.
Dr Campbell said that it was assumed that any resultant savings would either invested in prevention or subsidise social care.
Q The provisions for local accountability of polyclinics was raised; if polyclinics are to deliver 60% of healthcare, what kind of accountability and input from patient and user groups will we have.
It was responded that the new government commission may be able to give a view to the Scrutiny Committee as part of this Scrutiny review. The chairman thanked Dr Campbell for her presentation. 5. ANY OTHER ORAL OR WRITTEN ITEMS WHICH THE CHAIR
CONSIDERS URGENT None.
MINUTES END
Page 31

14
Appendix One - key questions for scrutiny committee General �How interdependent are the models e.g. does centralisation depend on further devolution? �How dependent are the models on improved information technology? Patient and public involvement �What involvement is there in further development of the proposals? �What involvement will there be in proposed clinical networks? �What are the views of older people? Health Equalities �Under doctored areas �Inequalities in funding �Proposal to site polyclinics on existing hospital sites “to support financial viability of local hospitals” – how will this address location of healthcare by need? �The relationship with the Mayor’s health inequalities strategy? �The representative nature of the NHS workforce esp. language and translation issues. Impact on social service and local govt �Involvement of Directors of adult and children’s services – is there any work on a model of social care to mirror and integrate with Darzi models? �How far do the proposed models of healthcare and the pathways extend to social care – are they medical or social models? �Is there any analysis of the potential impact on social care e.g. from early discharge? Questions for scrutiny – impact on social service and local govt �Social care moving to greater care for fewer people. �Darzi models imply more people need to receive a broader range of personal care. �NHS is universal free service, social care is means tested with eligibility criteria. How are these contradictions to be resolved? Impact on “local” hospitals �Given reduction in core functions, will local hospitals have sufficient volume and throughput to be sustainable? �Are they in danger of becoming “sinks”? �How will they retain expertise to cope with non-routine procedures? �Wouldn’t there be enormous duplication? �How would night-time cover work?
Page 32

15
Polyclinics �How flexible is the model? �What will be the status of GPs? �Flexibility for practice-base commissioning? �Extent of new providers? �Governance model? �Will the model make efficient and effective use of consultant and specialist time? Further workforce issues �Is there capacity in numbers and skills? �Current vacancy levels? �Model appears to suggest fewer consultants and more GPs – is there capacity for this? �Models suggest training needs – budgets? Commissioning �How will commissioning cover local, sectoral and London-wide strategic planning? A bigger role for NHS London? �Balance between PBC and PCT commissioning? �How will commissioning shift balance from acute to prevention? Is it realistic to expect it to do so? �Will commissioning be powerful enough to align budgets with needs? Funding and investment �How is it possible to estimate affordability without estimate of capital costs? �Will there be a double running/transition fund? Where will it come from? �How will additional social care be funded? �Where will capital funding come from?
–How confident is NHS London that funding can be released from NHS estates?
–What is the position of NHS Foundation Trusts?
–How will current LIFT projects be affected? Transport and travel �Has any modelling been done to show impact of models on number and length of journeys for LAS? �Has any modelling been done to show impact on number and length of journeys for patients e.g.
–Pregnant women
–Older people
–People with long term conditions? �Is there any information on the net effect on staff time and demand for parking?
Page 33

Page 34
This page is intentionally left blank

Matters Arising
JOSC CHAIR’S ANNOUNCEMENTS MADE ON 7/12/08 Future meetings Meetings will start at 10:30 and conclude at 4pm. With the option of a 30 minute extension The Chair and Vice Chair of the JOSC propose to be available for ½ hour before each meeting to informally meet with JOSC colleagues to discuss our approach to questioning in advance of receiving our evidence The Officer Support Group will circulate in advance of each meeting some suggested lines of questioning. These will not be exhaustive or replace your own borough preparations but will, we hope, aid preparation. Dates A statement from the JPCT is appended. This offers clarity as to their expectations and, I hope, allays some Member comments made at earlier meetings about timescales and the role of the JOSC At our December meeting we agreed that our meetings would be as follows;
1. 18th January 2. 22nd February 3. 14th March 4. 28th March 5. 25th April – Final meeting considering report.
Venues and speakers will be confirmed with the agenda packs for our meetings JOSC Member Input As a Member of the JOSC your input in to this process is invaluable and we welcome your full contribution and suggestions. We presently envisage a process where the Officer Support Group will assist us in preparing the report. However requests may, in due course, be made for additional capacity should we determine this is required Submissions As Chair I wish to state for the record that all submissions proposed for consideration in the formal paperwork for this body need to be submitted to the Officer Support Group no later than 2 weeks in advance of any of the already declared meeting dates
Page 35
As Chair I will with my colleagues (Vice Chairs) exercise the final decision about what papers will be included in an agenda dispatch We invite written submissions from any affected Local Authority, local Overview and Scrutiny Committee or interested organisation and would ask that any such documents are submitted to the Officer Support Group by no later than 29th February 2008 Legal Advice I have sought legal advice from my legal officers already in relation to the operation of the JOSC. You will also recall Hackney’s legal rep was at out last meeting and are happy to continue contributing. I would ask that the JOSC is mindful of such contributions. We welcome all offers of support but also I think we should agree that any offers for legal advice are channelled through the OSG
JPCT comment following Chair’s enquiry re conclusion of the work of JOSC ‘The following proposal will be put for consideration to the next meeting of the Joint Committee of PCTs on the 19 Dec: The Joint Committee of PCTs' current timetable has consultation closing on 7 March, followed by drafting of the independent consultant's report and draft London Commissioning Group (LCG) recommendations during March/April. We would like to invite the JOSC to finalise and supply its report to the programme office and independent consultants by 2 May 2008
In order to avoid Mayoral election purdah, we propose that the independent consultant's report is presented to public, PPIs, PCT Boards, the JOSC and other invitees as soon as possible after the Mayoral elections. To avoid the election count and the bank holiday the first potential date is the 6 May. We would like to invite the JOSC to present at this meeting. The independent report, responses to the consultation and LCG recommendations would then be shared with the PCT Boards and JOSC. We would like the final report to go to the JCPCT on the 30 May, taking account of PCT Board views and JOSC views amongst others’.
Page 36
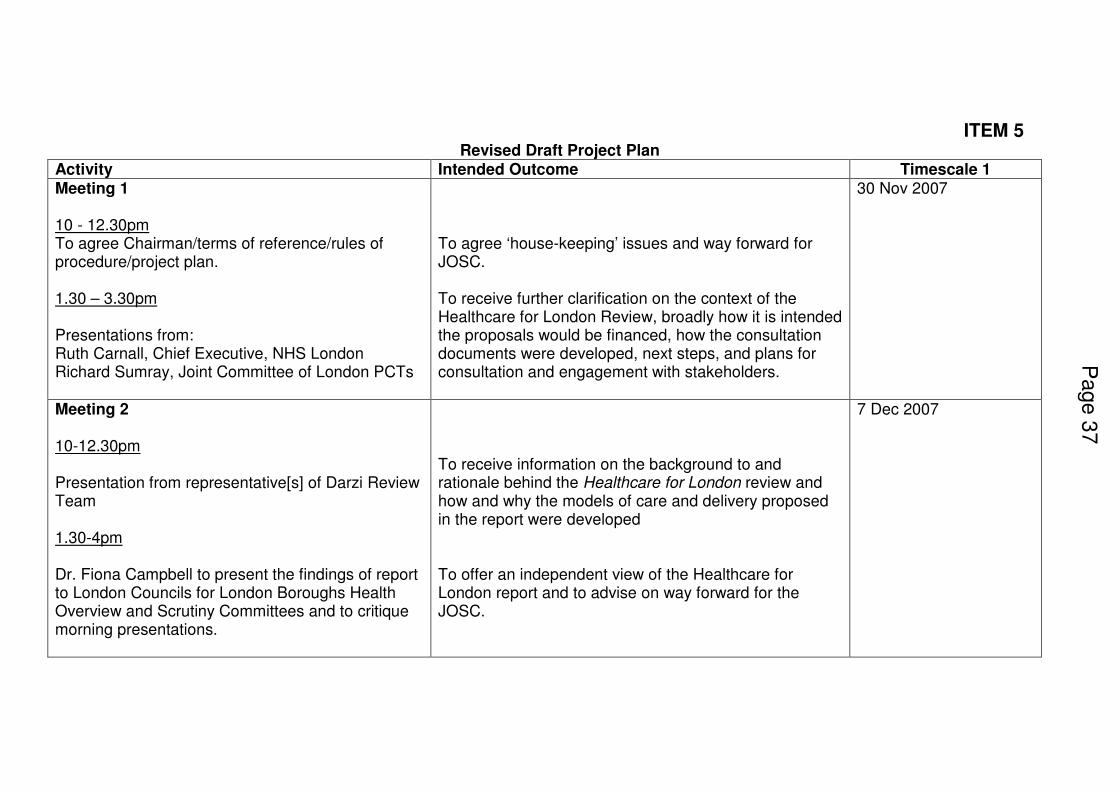
ITEM 5 Revised Draft Project Plan
Activity Intended Outcome Timescale 1 Meeting 1 10 - 12.30pm To agree Chairman/terms of reference/rules of procedure/project plan. 1.30 – 3.30pm Presentations from: Ruth Carnall, Chief Executive, NHS London Richard Sumray, Joint Committee of London PCTs
To agree ‘house-keeping’ issues and way forward for JOSC. To receive further clarification on the context of the Healthcare for London Review, broadly how it is intended the proposals would be financed, how the consultation documents were developed, next steps, and plans for consultation and engagement with stakeholders.
30 Nov 2007
Meeting 2 10-12.30pm Presentation from representative[s] of Darzi Review Team 1.30-4pm Dr. Fiona Campbell to present the findings of report to London Councils for London Boroughs Health Overview and Scrutiny Committees and to critique morning presentations.
To receive information on the background to and rationale behind the Healthcare for London review and how and why the models of care and delivery proposed in the report were developed To offer an independent view of the Healthcare for London report and to advise on way forward for the JOSC.
7 Dec 2007
Page 3
7

Meeting 3 – Local Authorities, social care and reality checking 10:30 -1.00pm Interviewing of 2 panels of witnesses in connection with JOSC identified key themes 1.45 – 4:30pm Interviewing of 2 panels of witnesses in connection with JOSC identified key themes
Covering, context, partnerships, infrastructure, economics Evidence gathering and testing of proposals set out in Healthcare for London report. Evidence gathering and testing of proposals set out in Healthcare for London report.
18 January 2008 Location Corporation of London
Meeting 4 – Clinicians 10:30 -1.00pm Interviewing of 2 panels of witnesses in connection with JOSC identified key themes 1.45 – 4:00pm Interviewing of 2 panels of witnesses in connection with JOSC identified key themes
Covering, Primary, Secondary and Specialist Care, Maternity and Mental health Evidence gathering and testing of proposals set out in Healthcare for London report. Evidence gathering and testing of proposals set out in Healthcare for London report
22 Feb 2008 Location Tower Hamlets
Pa
ge 3
8

Meeting 5 – Access and Public Health 10:30 -1.00pm Interviewing of 2 panels of witnesses in connection with JOSC identified key themes 1.45 – 4:00pm Interviewing of 2 panels of witnesses in connection with JOSC identified key themes
Covering; Access, Accessibility, Equalities, Social Care, public health and participation Evidence gathering and testing of proposals set out in Healthcare for London report. Evidence gathering and testing of proposals set out in Healthcare for London report.
14 March 2008 Location tbc
Meeting 6 – 10:30 -1.00pm Consideration of Equalities Impact Assessment and any early feedback on consultation outcomes (if available) 1.45 – 4:00pm Agreement of conclusions and recommendations (paper to be circulated in advance based on previous evidence gathering).
Covering; consultation activities, independent review and conclusions Evidence gathering and testing of proposals set out in Healthcare for London report. Allow for preparation of final report
28th March 2008 Location tbc
Drafting of report 28th March – 16 April 2008
Page 3
9
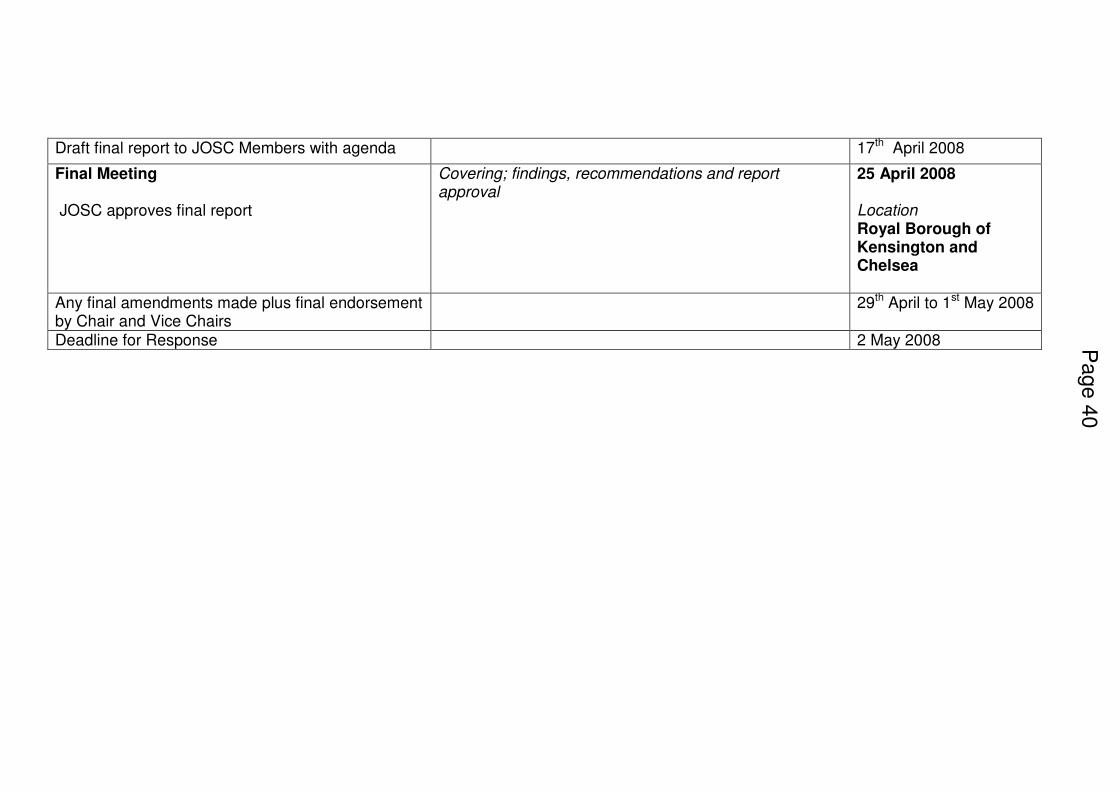
Draft final report to JOSC Members with agenda 17th April 2008
Final Meeting JOSC approves final report
Covering; findings, recommendations and report approval
25 April 2008 Location Royal Borough of Kensington and Chelsea
Any final amendments made plus final endorsement by Chair and Vice Chairs
29th April to 1st May 2008
Deadline for Response 2 May 2008
Pa
ge 4
0
Related Documents











