Standardizing handoff communications throughout an entire organization is a daunting and elusive challenge for health care organizations. Indeed, Wall Street Journal health columnist Laura Landro once referred to patient handoffs as “The Bermuda Triangle of health care.” 1 Nevertheless, health care organizations have an obligation to take up this chal- lenge for the sake of their patients. Ineffective handoff communications put patients at the following direct risks 2 : • Medication errors • Surgical errors • Violations of do-not-resuscitate orders • Delays in treatment • Incorrect diagnoses • Longer hospital stays • Other health problems A malpractice insurance provider that serves the Harvard medical community, reports that handoff-related cases represent Effective Handoff Communication, Part 2: Standardizing Processes Throughout Your Organization CONTENTS Effective Handoff Communication, Part 2: Standardizing Processes Throughout Your Organization 1 Patient Safety Pulse Your Patient Safety News The Joint Commission Center for Transforming Healthcare Unveils Targeted Solutions Tool 2 Moving Your Hospital to a New Facility, Part 2: Patient Safety on the Move 6 Alternative Surgical Site Marking: Compliance Strategies for the Joint Commission Universal Protocol for Preventing Wrong Site, Wrong Procedure, Wrong Person Surgery 9 www.jcrinc.com The Joint Commission Perspectives on Patient Safety TM November 2010 Volume 10 Issue 11 (continued on page 3) Handoffs should occur in a space where staff are unlikely to be interrupted. By Michael S. Woods, M.D., M.M.M.

Joint Commission- SBAR Pt2- Dec10 copy
Aug 08, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Standardizing handoff communicationsthroughout an entire organization is adaunting and elusive challenge for healthcare organizations. Indeed, Wall StreetJournal health columnist Laura Landroonce referred to patient handoffs as “TheBermuda Triangle of health care.”1
Nevertheless, health care organizationshave an obligation to take up this chal-lenge for the sake of their patients.
Ineffective handoff communicationsput patients at the following direct risks2:
• Medication errors• Surgical errors • Violations of do-not-resuscitate
orders• Delays in treatment• Incorrect diagnoses• Longer hospital stays• Other health problems
A malpractice insurance provider thatserves the Harvard medical community,reports that handoff-related cases represent
Effective Handoff Communication, Part 2:Standardizing Processes Throughout Your Organization
CONTENTS
Effective HandoffCommunication, Part 2: Standardizing ProcessesThroughout Your Organization 1
Patient Safety PulseYour Patient Safety NewsThe Joint Commission Centerfor Transforming HealthcareUnveils Targeted SolutionsTool 2
Moving Your Hospital to a NewFacility, Part 2: Patient Safety on the Move 6
Alternative Surgical Site Marking:Compliance Strategies for theJoint Commission UniversalProtocol for Preventing WrongSite, Wrong Procedure, WrongPerson Surgery 9
www.jcrinc.com
The Joint Commission
Perspectives on Patient Safety TM
November 2010 Volume 10 Issue 11
(continued on page 3)
Handoffs should occur in a space where staff are unlikely to be interrupted.
By Michael S. Woods, M.D., M.M.M.
www.jcrinc.com
Patient SafetyPulseYour Patient Safety News
The Joint Commission Center for TransformingHealthcare Unveils Targeted Solutions Tool
2 THE JOINT COMMISSION PERSPECTIVES ON PATIENT SAFETY November 2010
Top 5 in the News
Senior Editor: Jim ParkerProject Manager: Bridget ChambersManager, Publications: Helen M. Fry, M.A.Executive Director of Publications:
Catherine Chopp Hinckley, Ph.DContributors: Meghan Pillow, R.N.; Kathy Vega
Subscription Information: The Joint Commission Perspectives on Patient SafetyTM (ISSN 1534-5181) is published monthly(12 issues per year) by
Joint Commission ResourcesOne Renaissance BoulevardOakbrook Terrace, IL 60181
Send address corrections to The Joint Commission Superior Fulfillment131 West First StreetDuluth, MN 55802-2065
Annual subscription rates for 2010:Domestic $319 for print and online, $299 foronline only; international $410 for print and on line,$299 for online only. Back is sues are $25 each(postage paid). To begin your subscription, call800/746-6578, fax orders to 218/723-9437, or mailorders to Joint Commission Resources, 16442 Col-lections Center Drive, Chicago, IL 60693.
Editorial policy: Reference to a name, an organization, a product, or a service in The Joint Commission Perspectives on Patient SafetyTM
should not be construed as an en dorsement byJoint Com mission Resources, nor is failure toinclude a name, an organization, a product, or aservice to be construed as disapproval.
© 2010 by The Joint Commission. No part of thispublication may be reproduced or transmitted inany form or by any means without written permis-sion.
Joint Commission Resources, Inc. (JCR), an affiliate of The Joint Commission, has been designated by The Joint Commission to publishpublications and multi media products. JCR reproduces and distributes these materials underlicense from The Joint Commission.
Visit us on the Web, at http://www.jcrinc.com.
1Complication Found inDetermining Coronary Event Risk
Physicians who use a simplified version of the Framingham riskassessment tool may be miscalculat-ing patients’ likelihood of a majorcoronary event, according to a studythat appeared in the September 8issue of the Journal of GeneralInternal Medicine.
2IOM Studies IT Impact on SafetyThe Institute of Medicine (IOM) is
conducting a one-year study examiningthe ways health information technology(HIT) can improve patient safety. Thestudy will examine a comprehensiverange of patient safety–related issues.
3New Agency to Tackle HealthDisparities The National Institutes
of Health have launched the newNational Institute on Minority Healthand Health Disparities (NIMHD) to helpaddress differences in the burden ofdisease and other health conditionsamong special population groups.
4FDA Issues Final Rule on ClinicalTrials The U.S. Food and Drug
Administration (FDA) issued a finalrule in the September 29 FederalRegister clarifying what safety infor-mation should be reported duringclinical trials of investigational drugsand biologics.
5CDC Revises Flu Guidance TheCenters for Disease Control and
Prevention (CDC) have issued revisedguidance for flu prevention in healthcare settings. The guidance calls forthe use of surgical masks rather thanN-95 respirators, improved handhygiene, early identification of illpatients and staff, and the vaccinationof everyone in the United States.
The Joint Commission Center for Transforming Healthcare has developed aninteractive tool that facilitates a simple process for resolving health care qualityand safety challenges. Called the Targeted Solutions Tool™ (TST), the onlineresource helps organizations perform several essential functions, including per-formance measurement, identification of barriers to performanceimprovement, and the implementation of solutions. Joint Commission–accredited health care organizations can access the TST through The JointCommission ConnectTM extranet site.
The TST’s first set of targeted solutions addresses hand-hygiene compli-ance. A group of eight hospitals and health systems worked with the Center todevelop the solutions. At the start of the project in April 2009, the participat-ing hospitals were surprised to learn that their rate of hand-hygienecompliance averaged 48%. By June 2010 they had reached an average rate of82%. To date, they have sustained that performance for nearly a year.Nineteen small, medium, and large hospitals across the country also collabo-rated with the Center to test the work of the original eight hospitals andprovide guidance on the development of the solutions that are now availablethrough the TST. These hospitals are experiencing similar gains in hand-hygiene compliance as the original eight.
The TST provides the foundation and framework of an improvementmethod that, if implemented well, will improve an organization’s handhygiene compliance and contribute substantially to its efforts to reduce thefrequency of health care–associated infections. The complimentary data-driventool provides validated and customized solutions to address an organization’sparticular barriers to excellent performance. Self paced and confidential, theTST offers instantaneous data analysis. PS

losses of more than $173 million for itsclients during a five-year period. Nearly400 physicians and more than 70nurses in health care organizationsinsured by the insurance provider havebeen named in 268 claims and suitswith a handoff-related complaint, morethan half of which involve patientinjuries of high-severity.3
This is the second of two articlesthat address safe and effective handoffcommunications. The first article,which appeared in the October 2010issue of Perspectives on Patient Safety,discussed the risks associated withpatient handoffs, and a tool developedfor implementing the SBAR techniquefor handoffs.* This article discussesstrategies for organization-wide stan-dard-ization of handoff processes.
The Importance ofStandardizationExperts and patient safety advocates have called for standardization of hand-off processes as a means to improvehandoff communications. Also, JointCommission standards require organiza-tions to follow a standardized handoffprocess. However, organizations continueto struggle to meet this goal. Despite theappearance of simplicity, very few organ-izations have been able to implementsystemwide standardization. Successrequires the close coordination ofnumerous stakeholders within the organization to do do the following:
• Develop and implement theprocess
• Allocate resources• Obtain leadership and staff
buy-in
• Train personnel• Evaluate performance
Put simply, standardizing handoffprocesses requires a large-scale culturalchange.
Hierarchical relationships amongstaff can hinder effective communica-tion, including handoffs. Statusdifferences can discourage team mem-bers perceived as juniors or subordinatesfrom speaking up, pointing out discrep-ancies or potential errors, or even fromasking questions. Research from otherindustries illustrates this dynamic.Airplane cockpit communication hasbeen shown to be deficient betweenpersons who are unequal in status, suchas between the captain and the flightengineer. This problem may be evenmore prevalent in health care than inother industries due to the rigid hierar-chies that have existed for nearly acentury and have become deeplyembedded in the industry’s culture.
In a survey of 1,033 health care work-ers, from intensive care units andoperating theaters, and more than30,000 cockpit crew members, 70% ofthe total respondents said that it wasappropriate for a junior team member toquestion senior staff. However, therespondents differed depending on posi-tion and discipline. Only 55% ofconsultant surgeons said they would sup-port a flat hierarchy versus 94% ofcockpit crew members and intensive carestaff.4 The previous success of creating anenvironment in which all members ofthe team have an equal voice is essential,yet support for creating such an environ-ment by the very group who wouldlikely benefit, based upon this study, isminimally better than a coin toss.
Also, the standardized protocol mustbe tailored to meet the needs of differ-ent disciplines and organizations. Manydisciplines have unique needs, so theremust be recognition of those aspects ofthe process that may or may not beable to be generalized. The process
must be tailored to meet the needs ofthe end user.5
What Does StandardizationLook Like?A standardized process should includea means to educate staff about theprocess and a plan for organizationwideimplementation. The standardizedprocess should also inlcude a list ofhandoff situations that occur withinthe organization for example, a patientmoving from the ER to the medical-surgical inpatient unit, or a patientmoving from the post-anesthesia unitto the medical-surgical inpatient unit.
Partners HealthCare Systems developeda list of clinical data that the receivingclinician requires to provide safe careduring the first 72 hours after transfer.The list included the followingelements6:
• Focused history• Focused physical exam• Pertinent past medical history• Pre-admission medications• Allergies• Medication reactions/drug
intolerances• All significant critical conditions• Procedures• Hospital course• Pertinent test results• Future care plans• Results pending that require
follow-up• Name/number of discharging
physician and primary carephysician
• Discharge medications withdiagnoses
A list such as this can be customizedto meet your organization’s specific needs.Whatever the process used, it should befocused on identifying critical contentthat should be transferred during a handoff.5 Content omissions are a significantsource of communication failure during
www.jcrinc.com THE JOINT COMMISSION PERSPECTIVES ON PATIENT SAFETY November 2010 3
Effective Handoff Communication, Part 2(continued from page 1)
(continued on page 4)
* SBAR is an acronym for Situation,Background, Assessment, andRecommendation. The U.S. Navy origi-nally developed SBAR for use onnuclear submarines. Later, staff at KaiserPermanente adapted the process toapply to hand offs in health care.

hand offs. It can be helpful to develop achecklist of necessary information andincorporate that into the process, andinvolve staff in selecting what informa-tion should be included on the checklist.5
A Top-Down Team ApproachOnce you decide to embark on a pathof standardization, the first step is togain C-suite support, including, at aminimum, the CEO, the vice presidentof medical affairs/chief medical officer,and the vice president of nursing (orequivalent). The likelihood of successfor clinical initiatives, like SBAR, ismaximized by close cooperationbetween the medical staff and nursing.This top-down leadership endorsementis not just nice to have… it isabsolutely necessary. C-suite leadershipshould very clearly communicate itssupport (and expectation) that all staffwill participate in the process.
When OSF St. Joseph MedicalCenterin Bloomington, Illinois beganis handoff standardization project, thechief nursing officer served as executivedirector of the team, and a portion ofher compensation was contingent onmeeting implementation goals. Medicaldirectors were named as sponsors tochampion the use of the process amongmedical staff peers. The patient safetyofficer was the day-to-day project man-ager for the team.8 This is an excellent
example of how leadership can supportthe process.
Once these alliances have beenformed, the next step is to build a teamthat will oversee development andimplementation. The team shouldinclude representatives of all stakehold-ers, including division chiefs, front lineattendings, fellows, residents, physicianassistants, nurse practitioners, registerednurses, and other key staff members.9
The team should conduct a needsassessment. They need to know in whatsituations within their organization arehandoffs necessary, how they are cur-rently being done, what informationneeds to be shared during those hand-offs, and whether that essentialinformation is actually being shared.6 Anumber of methods are available forconducting this assessment, includingstaff surveys, direct observation, and for-mal techniques such as Failure Modeand Effects Analysis (FMEA).6 Theteam should attempt to craft answers tothe following key questions6:
• What problems exist with thecurrent handoff process (if any)and what effect do they have?
• What will happen if no changeoccurs?
• Why should action be taken now?• How will success be measured? • What will the new processes
require?• How will things be different if we
make the intended change?
• What is the cost of changingversus the cost of staying thesame?
It is also helpful for staff to under-stand the ways in which the changeswill benefit them. For example, stan-dardized processes can help reduceunnecessary or duplicate work.2
Some organizations have had successusing pilot programs within individualdepartments or groups of departmentsand gradually rolling out the programthroughout. OSF St. Joseph MedicalCenter initially implemented their stan-dardized SBAR process in a generalmedical nursing unit in 2004; organiza-tionwide implementation was completeby the following spring. Among otheractivities, OSF St. Joseph started a“secret shopper program” in which staffmembers were called at random andasked questions about SBAR. Results ofthese surveys were shared throughoutthe organization. Stickers and postersreminding staff to use SBAR were posi-tioned throughout units, and training inSBAR was included in annual staff edu-cation programs. For Fiscal Year 2005,OSF St. Joseph reported a mean of 96%use of SBAR.9
Brigham and Women’s Hospital inBoston implemented its handoff processin phases; beginning by targeting nurse-to-nurse, resident-to-resident, andoperating room–to–post anesthesia careunit handoffs. The second phase targeted
Patient Safety Editorial Advisory Board
www.jcrinc.com4 THE JOINT COMMISSION PERSPECTIVES ON PATIENT SAFETY November 2010
Bonnie M. Barnard,M.P.H., C.I.C., QualitySpecialist, St. Peter’sHospital, Helena, Montana
Hedy Cohen, R.N., M.S.,Vice President, Institute forSafe Medication Practices
Kathy Connolly, R.N.,M.S.Ed., C.P.H.R.M.,Assistant Vice President,Risk Management, PremierInsurance ManagementServices, Inc.
Nilda Conrad, M.B.A.,C.P.M.S.M., C.P.C.S.,President, NationalAssociation of Medical StaffServices
Diane D. Cousins, R.Ph.,National Quality Forum’sExpert Panel
David Fuller, Senior SpaceSystems and OperationsEngineer and AssociateFellow of the AmericanInstitute of Aeronautics andAstronautics
Suzanne Graham, R.N.,Ph.D., Director of PatientSafety, California Regions,Kaiser Permanente
Robert S. Lagasse, M.D.,Vice Chairman, Departmentof Anesthesiology, AlbertEinstein College of Medicine& Montefiore MedicalCenter, New York
Jeannell M. Mansur, R.Ph.,Pharm.D., F.A.S.H.P.,Practice Leader, MedicationSafety, Joint CommissionResources
David Marx, Head of thePaediatric GastroenterologyTeam, University Hospital,Czech Republic
Deborah Nadzam, Ph.D.,R.N., F.A.A.N., Director,International Quality andPerformance Measurement,Joint CommissionResources
Rita Shane, Pharm.D.,F.A.S.H.P., Director,Pharmacy Services, andAssistant Dean, ClinicalPharmacy, UCSF School of
Pharmacy, Cedars-SinaiMedical Center, Los Angeles
Paula Spears, D.N.Sc.,R.N., Corporate Director,Professional Practice andAdvancement, Methodist LeBonheur Healthcare,Memphis
Sherry Umhoefer, R.Ph.,M.B.A., Vice President,Quality and Compliance,McKesson MedicationManagement
Effective Handoff Communication, Part 2(continued from page 3)
attending-attending, procedural area,and ambulatory setting handoffs.10 Theorganization developed guidelines toaddress interdisciplinary problems thataffected handoffs, launched a traininginitiative for staff, and created ID badgeinserts describing best practices toremind staff. Their team evaluated theprocess one month and six months afterfull implementation and found that thetime to complete a handoff was reducedby an average of seven minutes, dupli-cate information had been minimized,and feedback from frontline providerswas positive.10
Sustaining Positive ChangeOrganizations that have achieved successin this area have recognized that� in theend� it isn’t just about creating a solu-tion. The roads of mediocrity are
littered with unimplemented or unsus-tained solutions. Rather, the goal is tosustain positive change based upon thesolution. The success of any patientsafety initiative depends on a commit-ment from all stakeholders, includingleadership and staff, to build and sustaina systemwide positive shift to a cultureof safety. Noticeable change is likely tobe gradual. Organizations should intro-duce staff to new concepts, new ways ofthinking about how they do their jobs,and should provide the tools they needto implement these concepts.2
End-user staff is more likely toembrace change if they are involved inthe decision-making process. The teamapproach is helpful in engaging indi-viduals across the organization in thedevelopment process. Make sure staff isinformed and educated about why the
changes are necessary. But educationalone is not enough. The followingthree components should be integratedin to each step of the developmentpathway to a solution:
1. Creating awareness(education/learning)
2. Developing accountability (bothpersonal and organizational)
3. Building in routine follow-up todocument meaningful change
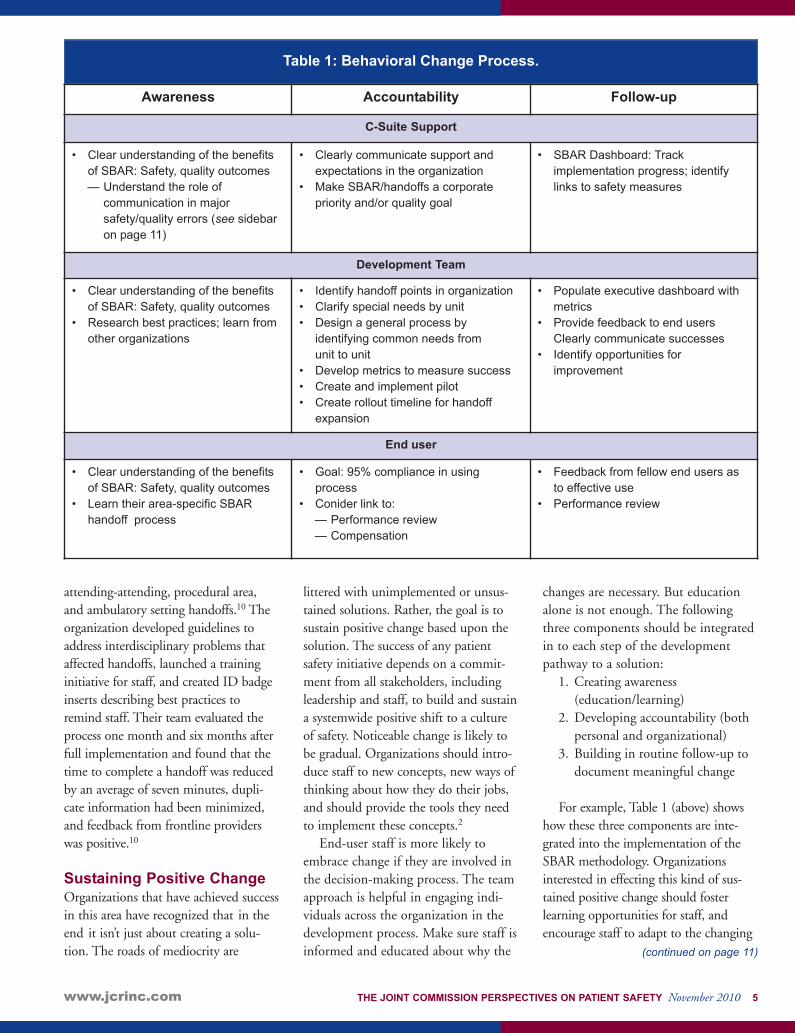
For example, Table 1 (above) showshow these three components are inte-grated into the implementation of theSBAR methodology. Organizationsinterested in effecting this kind of sus-tained positive change should fosterlearning opportunities for staff, andencourage staff to adapt to the changing
www.jcrinc.com THE JOINT COMMISSION PERSPECTIVES ON PATIENT SAFETY November 2010 5
(continued on page 11)
Awareness Accountability Follow-up
C-Suite Support
• Clear understanding of the benefitsof SBAR: Safety, quality outcomes— Understand the role of
communication in majorsafety/quality errors (see sidebaron page 11)
• Clearly communicate support andexpectations in the organization
• Make SBAR/handoffs a corporatepriority and/or quality goal
• SBAR Dashboard: Trackimplementation progress; identifylinks to safety measures
Development Team
• Clear understanding of the benefitsof SBAR: Safety, quality outcomes
• Research best practices; learn fromother organizations
• Identify handoff points in organization• Clarify special needs by unit• Design a general process by
identifying common needs from unit to unit
• Develop metrics to measure success• Create and implement pilot• Create rollout timeline for handoff
expansion
• Populate executive dashboard withmetrics
• Provide feedback to end usersClearly communicate successes
• Identify opportunities forimprovement
End user
• Clear understanding of the benefitsof SBAR: Safety, quality outcomes
• Learn their area-specific SBARhandoff process
• Goal: 95% compliance in usingprocess
• Conider link to:— Performance review— Compensation
• Feedback from fellow end users asto effective use
• Performance review
Table 1: Behavioral Change Process.
Pat Stack, vice president ofTransition Planning, arrived atNorthwest Community Hospital
(NCH), in Arlington Heights, Illinois,at 3:00 A.M. on Saturday, May 1, 2010.
She and the rest of the staff at NCHwere faced with moving 140 adultpatients plus 6 infants from the SpecialCare Nursery to a new facility. Theyhad to accomplish this in about 4½hours without any adverse events, med-ication errors, or delays in patient care.Similarly, in 2012, staff at the JohnsHopkins Children’s Center inBaltimore, Maryland, will be facing thesame goals when they transport pedi-atric patients to the new Charlotte R.Bloomberg Children’s Center.
Planning for the safe transport ofpatients to new hospital buildings has
become more common, as evidencedby the 121 new or replacement hospi-tals completed in 2004, and theincreasing number of consulting busi-nesses that offer transitional planningservices to growing hospitals.1
For more information on the prepa-ration that takes place prior to movingday (such as designing a new hospitalwith patient safety and family-centeredcare in mind, and teaching staff how toprovide care in the new hospital), seethe first article in this two-part series,which published in the October 2010issue of Perspectives on Patient Safety.
Moving Equipment andSuppliesOrganizations may choose to purchaseall new equipment for the new or
replacement building, which is benefi-cial for the day of the move becausefewer items go on the moving list.However, moving current equipmentover to the new building can reducecosts. At Hopkins Children’s, 70% ofthe equipment and supplies will bepurchased for the new facility, but 30%will be reused from the current build-ing. “It has complicated things a bit bynot buying all new equipment,” saysMichael Iati, senior director ofArchitecture and Planning, JohnsHopkins. “You can’t just close downthe old building and run to the newbuilding and start taking care ofpatients. It’s more complicated to moveequipment in addition to the patients,and we’ll have to recalibrate equipmentin a leapfrog effect as we move.”
Move equipmentfirst. When possible, move equipmentbefore transporting patients to the new building to reduce congestion.2
Furthermore, label items to be movedprior to moving day to reduce confusion.
Involve Patients and FamiliesMore than two years before the plannedmove to the Charlotte R. BloombergChildren’s Center, staff at HopkinsChildren’s started meeting with familymembers to understand any concernsthey might have and solicit their advicefor the move. Involving patients andfamily members in any organizationdecision is nothing new to HopkinsChildren’s, where a Family AdvisoryCouncil meets monthly and a full-timeparent advisor helps enhance communi-cation between parents and staff. “Theparent advisor also attends planningmeetings for the new hospital and sharesher insights as a parent as well as the
STRATEGY
www.jcrinc.com6 THE JOINT COMMISSION PERSPECTIVES ON PATIENT SAFETY November 2010
Moving Your Hospital to a New Facility, Part 2:Patient Safety on the Move
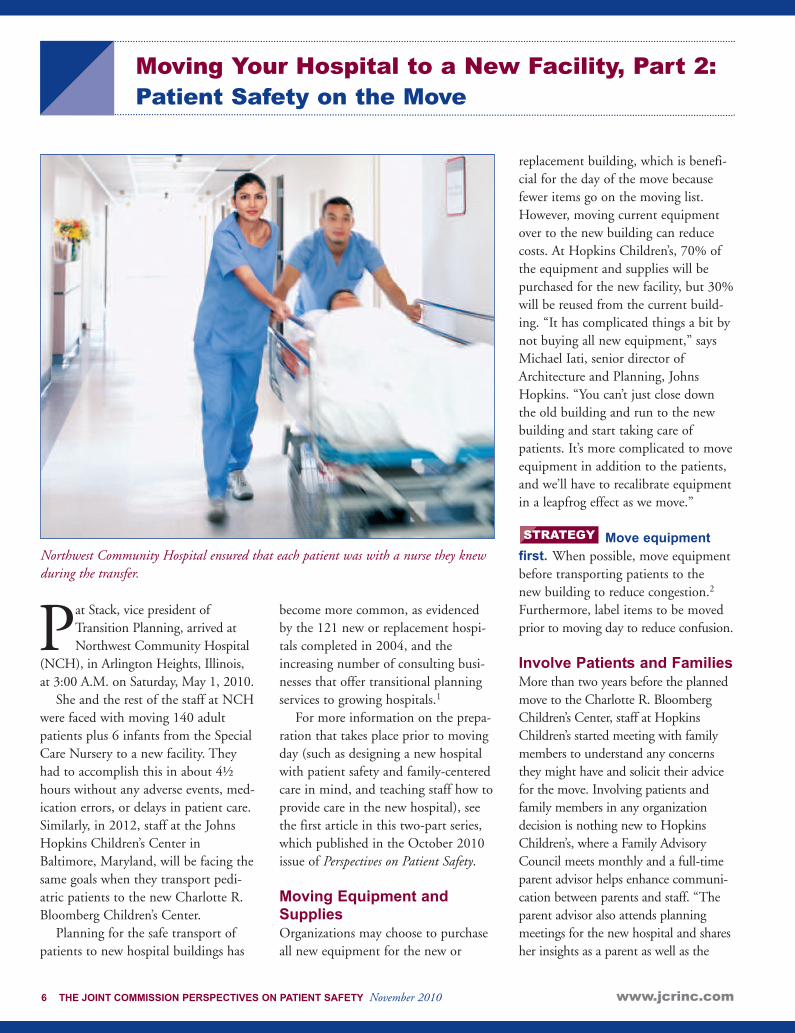
Northwest Community Hospital ensured that each patient was with a nurse they knewduring the transfer.
www.jcrinc.com THE JOINT COMMISSION PERSPECTIVES ON PATIENT SAFETY November 2010 7
opinions of other parents she meets withon a routine basis,” says Ted Chambers,pediatrics administrator at JohnsHopkins Children’s Center.
Deciding how involved family mem-bers should be on the actual moving daycan be difficult. “On the one hand, if wehave families with us during the move, itwill take longer,” said Stack, “But notallowing family members the option ofcoming didn’t seem fitting with ouroverall vision of family-centered care. Sowe talked to patients and family mem-bers on the Thursday before the move,and gave them an information packetexplaining the move. We said that familymembers were welcome to be with thepatient during the move, but noted thatit might be easier if they didn’t come tillthe afternoon when the move was over.”Hopkins Children’s is dealing with howto handle the same issue. “We’ve had alot of discussions with family memberson how to conduct the move with fam-ily,” says Chambers, “and we’ve come tothe conclusion that it’s better to have onefamily representative (for example, a par-ent) present during transport and havethe rest of the family waiting in the newfacility.”
Keep family mem-bers informed on moving day.Even if family members choose not togo along with the patient during theactual transport, organizations can keepfamily members involved andinformed. “On the moving day, we setup a family lounge in the cafeteria withfree breakfast and lunch,” Stack says.“We also had a computer tracking sys-tem available so family members knewexactly when patients had been movedto the new building and were tuckedsafely into bed.” Similarly, HopkinsChildren’s plans to keep the lines ofcommunication open between familymembers and staff during the move.“We know that the more we communi-cate, the better things go,” Chamberssays. “Family members need to be
aware of what’s going on with theirpatient the day of the move. Thisreduces stress and anxiety and reassuresfamily members that their loved one issafe.”
Transport Patients SafelyPlanning to transport dozens of patientsat once to a new building takes a greatdeal of planning and coordination.Stack, Chambers, and Iati suggest thefollowing strategies to ensure a smoothtransition to the new building.
Decide on the lengthof moving day. The length of themove depends on the anticipated num-ber of patients to be transported, theacuity of those patients, the length ofthe moving route, and the amount ofequipment to be moved. NCH used asoftware simulation modeling system todetermine the cycle time for each indi-vidual patient transport and thendetermine the length of the move basedon the amount of patients to bemoved. “The simulation softwareallowed us to optimize our transportroutes and create an elevator utilizationplan because we didn’t want patientson beds in elevator lobbies waiting tobe moved,” says Stack. “The modelworked—it predicted that our move
would take 4 hours and 30 minutes,and we actually took 4 hours and 35minutes.”
Overall, keeping the length of themove as short as possible is importantfor patient safety. “It is best to move asquickly as possible and then recover,”says Chambers. “With a prolongedmove, it spreads the institution and itsresources thinly over into two parts ofthe campus for too long, which is lesssafe than a structured, well-orchestratedmove.”
Pick the transportroutes ahead of time and runmock moves. Everything is simplified when patientsonly need to be transported throughcompletely enclosed corridors to thenew building. But not all organizationshave the luxury of building new orreplacement towers on the currentcampus. In some cases, organizationshave to transfer patients with ambu-lances to the replacement hospital fivemiles down the road. In these cases,organizations must consider what isgoing on within the community, suchas marathons or festivals, before sched-uling the moving date. The season mayalso affect the moving date (for example,
STRATEGYSTRATEGY STRATEGY
Extensive preparation is necessary when moving patients to an new facility.
(continued on page 8)
www.jcrinc.com8 THE JOINT COMMISSION PERSPECTIVES ON PATIENT SAFETY November 2010
winter storms may cause delays inambulance transport).
Hopkins Children’s will be luckyenough to move their patients throughenclosed corridors. “An internal movesaves us a great deal of anxiety,” saysChambers. “Our biggest concern iscoordinating how fast patients can gointo the elevators.” NCH also had anenclosed move, which helped simplifythe move, says Stack. “We knew thecycle time for each patient transportroute,” says Stack. “We made a movingpocket guide for everyone involved inthe move. The guide spelled out theirspecific transport route, including amap, and provided resource numbers,including Incident Command Center’snumber.”
Decrease patientcensus levels. The move will gomuch quicker if there are fewer patientsto transport. Hopkins Children’s plansto decrease census levels by reducing theamount of elective surgeries prior to themoving date. In addition, organizationscan encourage physicians to dischargeany patients prior to the move, if it canbe done safely.2
Increase staffinglevels. Extra staff will obviously beneeded to transport patients, butincreased staff in other areas of the hos-pital will also be necessary. “Weincreased staffing in the emergencydepartment because we knew patientsmay have to be held there for a longertime before they could be admitted tothe new building,” says Stack. “In addi-tion, we decided we were not going tohave any babies born in elevators, soanyone in active labor would not betransported to the new labor and deliv-ery unit. As a result, we ran twocompletely staffed, parallel labor anddelivery units on the moving day. Both
units had enough obstetricians, anes-thesiologists, and neonatologistsavailable for vaginal births or cesareansections.”
Set up an incidentcommand unit and a move command center. “Our incidentcommand was a group made up of fourto six people making decisions, withone person in charge. We had radiosfor communication with the transfer-ring and receiving teams, Stack said.” Itmay also be helpful to control traffic inthe command center so that communi-cation via radios is not disrupted.2
Create transportingand receiving teams. At NCH, itwas important for a nurse who knew thepatient to be with the patient at alltimes throughout the move. Therefore,at the beginning of moving day, twonurses heard a report on each patientand one nurse became part of the trans-port team from the old building whilethe other nurse became part of thereceiving team in the new building. “Soif you were a nurse on the transportteam with four patients, you would havetwo helpers to get your first patientready for transfer, transport that patientto the new building, and hand off thepatient to the nurse on the receivingteam,” says Stack. “The transport nursewould update the receiving nurse withany new information on the patientsince report. Then, the transport nursewould return to the old building, whereher next patient would be packed andready to go. The nurse on the transportteam also had the authority to saywhether or not a patient was stableenough to be transported to the newbuilding.”
For intensive care patients, thepatient-to-nurse ratio was kept close to1:1 so that the same nurse who trans-ported the patient would remain withthe patient on the new unit. The trans-port teams for intensive care patients
might also include respiratory thera-pists if a patient was on a ventilator.“In intensive care, the intensivist wasalso available to assist during themove,” says Stack. “And the neonatolo-gists in the Special Care Nurseryactually accompanied some of thebabies to the new hospital.”
On moving day, Hopkins Children’splans to use three teams of nurses to dothe following:
1. Prepare patients for transport2. Actually transport the patient3. Receive the patient on the new
unit.
Hopkins Children’s will also includeway stations along transport routeswith essential staff, such as anesthesiol-ogists, to ensure safe patient transfers.
Get informationtechnology (IT) staff involved.“Our IT staff was on each unit to makesure that as soon as a patient was trans-ferred to their new room, the patient’sstatus was updated in the system sothat pharmacy, physicians, laboratory,and dietary knew where the patientwas,” says Stack.
References1. Romano M.: Moving day: Relocating to a new
hospital puts staff's logistics skills to the test.Mod Healthc 35:28, 30, Oct. 2005.
2. Schaufele M.: Moving day: Emergency com-mand model helps children’s hospital Relocate.Health Facil Manage 18:29–34, Nov. 2005.
STRATEGY
STRATEGY
STRATEGY
STRATEGY
STRATEGY
PS
Call for PapersAre you or your organization
working on a project or policy thatwill improve patient safety?
Why not share your ideas andresults with your colleagues
nationwide?
If you have a paper you would liketo submit for potential publicationin Perspectives on Patient Safety,
please send us an e-mail, [email protected].
Moving Your Hospital to a New Facility,Part 2:(continued from page 7)
Wrong site, wrong proce-dure, wrong personsurgery happens when a
procedure is executed on the wrongbody part, the wrong side of thepatient’s body, or the wrong patient.1
Wrong surgery procedures are consid-ered “never events,” which means theyare, in theory, completely preventableand thus should never happen.2
Marking the procedure site prior tobeginning the procedure is a criticalprevention activity. The JointCommission addresses this in require-ment UP.01.02.01. (See sidebar onpage 11). According to this require-ment, an appropriate site marking isdistinct, unambiguous, and visible afterthe patient has been prepped anddraped. The mark is located at or nearthe incision site and is sufficiently permanent to remain visible after com-pletion of skin preparation. This mark
can be the word “Yes,” the surgeon'sinitials, or some other unambiguousindication.
Although The Joint Commission rec-ommends marking all surgical sites,health care organizations are required, ata minimum, to mark all cases involvinglaterality, multiple structures (for exam-ple, fingers, toes, lesions), or multiplelevels (for example, the spine). If apatient requires multiple surgeries whilein a health care organization, the sitemark should be removed at the end ofthe procedure unless the next surgicalprocedure will continue on the same site.
To address situations in which aphysical site mark is not effective, prac-tical, or sanctioned by the patient,organizations must have an alternativesite marking process in place. AlthoughThe Joint Commission is not prescrip-tive as to what this alternative processshould be, it does require organizations
to define the process in writing andensure compliance with the process.
Addressing ChallengesAssociated with Site MarkingSituations in which physically markingthe site may be anatomically impossibleor impractical include the followingexamples:
• Gynecological procedures• Dental procedures• Procedures involving premature
infants, for whom the mark maycause a permanent tattoo
In addition, the skin of some patientsmay preclude effective site marking. Forexample, a standard site mark may notbe visible on a patient with a significantnumber of body tattoos or on a patientwhose skin has been severely burned. Anindividual’s skin tone can also make sitemarks hard to see.
Patients may also refuse site markingin some cases. For example, patientsreceiving facial surgery or breast sur-gery may not wish to have the surgicalsite marked with a permanent marker.In such cases, the alternative processshould include patient education aboutwhy site marking is appropriate, theimplications of refusing site marking,and a clear description of the alterna-tive site marking methods.
Types of Alternative SiteMarkingOrganizations have used a variety ofmethods to comply with this require-ment. “Although there are many typesof alternative site marking approaches,there are two we hear about most fre-quently,” says Pat Adamski, R.N.,M.S., M.B.A., executive director of
www.jcrinc.com THE JOINT COMMISSION PERSPECTIVES ON PATIENT SAFETY November 2010 9
Alternative Surgical Site MarkingCompliance Strategies for the Joint Commission Universal Protocol forPreventing Wrong Site, Wrong Procedure, Wrong Person Surgery
Organizations need clear, specific policies on when alternative surgical site markingprocesses could or should be used.
(continued on page 10)
The Joint Commission’s StandardsInterpretation Group. “The firstinvolves marking the procedure site onan anatomical drawing kept near thepatient before and during the proce-dure. To be effective, the drawing mustbe displayed in a highly visible locationand must face the same direction as thepatient.” This approach may be helpfulwhen identifying the site of surgery forpremature infants, gynecologicalpatients, or during dental procedures.As with standard site marking, a verifi-cation process should exist that ensuresthe drawing is marked correctly.
“The other approach is appropriatein situations in which the site has beenmarked, but the drape will cover thatmark,” says Adamski. “In these cases,the provider would mark the site andthen as the patient is draped, mark thedrape.” Similar verification processesshould be involved in marking the siteand marking the drape to ensure themarkings are consistent. Staff shouldalso ensure that the drape is secure, sothat it does not inadvertently move offthe site before or during the procedure,according to Adamski.
Some organizations also use fluo-roscopy and other radiologicaltechniques to help with site marking ininternal procedures such as spine sur-gery. “In most cases, these are used inconjunction with an outer form of sitemarking to identify the general loca-tion of the surgery and then pinpointthe specific location,” says Adamski.
Standardizing the ApproachTo ensure consistent and appropriateuse of alternative site-marking proce-dures, such procedures should bestandardized throughout an organiza-tion where possible. “Having aconsistent method for alternative sitemarking helps build familiarity withthe process and can prevent error andmisunderstanding,” Adamski says.
Organizations may want to analyzethe surgical procedures occurringwithin their facilities and determinewhich qualify for alternative site mark-ing, then develop a consistent approachto the process and train staff on whenand how to use that approach.
Organizations should considerincluding alternative site marking ontheir presurgical checklist. This can notonly help document the use of the alter-native approach, but also help staffremember that when traditional sitemarking is not appropriate, a definedalternative approach should be followed.
Involving the Patient IsImportantRegardless of the type of alternative site-marking process an organization uses,this process should involve the patient.For this to be done in a meaningful way,site marking should happen before thepatient is significantly sedated.Participation may be precluded by a dis-ease state or heavy sedation; however,sedation by itself does not necessarilyprevent the patient from participating inthe alternative site marking process. Thepatient’s capacity to participate must bebased on an individual assessment. Incases of nonspeaking, comatose, orincompetent patients or children, the“patient involvement” in the site-mark-ing process should be handled in thesame way as the informed consentprocess. Whoever has authority to pro-vide informed consent for the patient toundergo the procedure would, as appro-priate, participate in the alternativesite-marking process.
Monitoring to EnsureComplianceSimply having an alternative site marking process is not sufficient to be in compliance with the UniversalProtocol. Organizations must ensure theprocess is used correctly. “Organizationsshould be monitoring their use of alter-native site-marking procedures,”
Adamski says. “This can be done inmany ways, including through chartreviews, checklist reviews, direct observa-tions, conversations with surgical teammembers, and so on.”
Organizations should ensure staffmembers are familiar with the organiza-tion’s alternative site-marking proceduresand know when to use them.Organizations should also identify howfrequently such alternative proceduresoccur and whether they are used appro-priately. If monitoring efforts show thatalternative procedures are occurringmore frequently than standard markingprocedures, a closer examination of theissue may be warranted.
Wrong-Site Surgery aPersistent ProblemDespite the fact they are preventable,wrong surgery errors continue to plaguehealth care organizations around theworld. Although the frequency of thesetypes of errors is difficult to quantifybecause of underreporting issues, avail-able data is nevertheless alarming. Forexample, since 1995, when The JointCommission began reviewing sentinelevents and their root causes, wrong sitesurgery has become the most frequentlyreported category of sentinel events.3
Although greater awareness and report-ing may contribute to the numbers,surgical errors of this type clearly con-tinue to occur.4
One recent study suggests wrong-site surgery happens in 1 out of112,994 cases.5 These numbers repre-sent actual cases; however, the numberof near misses is much higher.6
The Patient Safety Authority ofPennsylvania—which collects data onwrong-site surgery, both actual andprevented—indicates receiving reportsof an average of one wrong-site surgeryevent (either actual or near miss) everysix days since mandatory state report-ing began in the early 2000s.7
Although many of these near missesand surgical confusions cause little or
www.jcrinc.com10 THE JOINT COMMISSION PERSPECTIVES ON PATIENT SAFETY November 2010
Alternative Surgical Site Marking(continued from page 9)

www.jcrinc.com THE JOINT COMMISSION PERSPECTIVES ON PATIENT SAFETY November 2010 11
no permanent injury, the risks are pres-ent for a serious, irreversible event thatcan permanently scar a patient, family,and provider.8
References:1. Senders J., Kanzki R.: The egocentric surgeon
or the roots of wrong-side surgery. Qual SafHealth Care 17:396–398, Dec. 2008.
2. Stahel P., Mehler P., Clarke T., et al.: The 5thanniversary of the “Universal Protocol”: Pitfallsand perils revisited. Patient Safety in Surgery, Jul.2009. http://www.ncbi.nlm.nih.gov/pmc/
articles/PMC2712460 (accessed Sept. 1, 2010). 3. Joint Commission International: Performance
of Correct Procedure at Correct Body Site.Patient Safety Solutions 1, May 2007.
4. Wrong-site surgery is No.1 among sentinelevents—Are you at risk? Same-Day Surgery31:113–124, Oct. 2007.
5. Kwan M., Studdert D., Zinner M., et al.:Incidence, patterns, and prevention of wrong-site surgery. Archives of Surgery 141:353–357,Apr. 2006.
6. Edwards P.: Ensuring correct-site surgery.Provenance and Peer Review 18:168–171, Apr.2008.
7. Blanco M., Clarke J., Martindell D.: Wrongsite surgery, near misses, and actual occur-rences. AORN Journal 90:215–217, Aug.2009.
8. Sime J., Ngo Y., Khan S.: Surgical confusionsin ophthalmology. Arch Ophthalmology125:1515–1521, Nov. 2007.
PS
Effective Handoff Communication, Part 2(continued from page 5)
environment and develop clear expecta-tions for which each individual,department, patient care team, andadministrator will be held accountable.Finally, organizations also need to regu-larly evaluate how well their new systems,policies, and procedures are working andmake adjustments when necessary.
What is the end result of this kind ofsustained, positive change? Creating theculture you wanted in the first place.
Michael S. Woods, M.D., M.M.M. is a lead-
ership expert, surgeon, and author of several books,
including In a Blink, Healing Words, Civil
Leadership, and was editor of Cultural
Sensitivity: A Pocket Guide for Providers.
Dr. Woods is a recognized authority on
provider–patient communication and relation-
ships, patient satisfaction, and strategies to reduce
medical malpractice. Dr. Woods is the founder of
Civility Mutual® Educational Services, an organi-
zation dedicated to helping physicians and health
care staff with relationship-based care and improv-
ing patient–provider communication. He is the
vice president of medical affairs for the Johnson
Memorial Medical Center in Stafford Springs, CT.
References1. Landro L.: Hospitals combat errors at the
‘hand-off.’ Wall Street Journal. June 28, 2006.2. The Joint Commission: Improving Handoff
Communication. Oak Brook, IL: JointCommission Resources, 2007.
3. Hoffman J.: CRICO’s Handoff-related cases.Forum 25:4, Mar. 2007. http://www.rmf.harvard.edu//files/documents/Forum_V25N1.pdf (accessed Sept. 20, 2010).
4. Solet D., Norvell M., Rutan G., et. al.: Lost intranslation: Challenges and opportunities inphysician-to-physician communication duringpatient handoffs. Acad Med 80:1094-1099,Dec. 2005.
5. Arora V., Johnson J.: A model for building astandardized handoff protocol. Jt Comm JQual Patient Saf 32:646–655, Nov. 2006.
6. The Joint Commission: HandoffCommunications: Toolkit for Implementing theNational Patient Safety Goal. Oak Brook, IL:Joint Commission Resources, 2008.
7. Chan-Macrae M., O’Malley T., Poon E.:Partners HealthCare clinical transitions project.Forum 25:16–17, Mar. 2007.
http://www.rmf.harvard.edu//files/documents/Forum_V25N1.pdf (accessed Sept. 20, 2010).
8. Haig K., Sutton S., Whittington J.: SBAR: Ashared mental model for improving communi-cation between clinicians. Jt Comm J QualPatient Saf 32:167–175, Mar. 2006.
9. Shaw T.: Communication: Making transitionssafer with standardized handoffs. Paper presentedat the Society for Pediatric Anesthesia 23rdAnnual Meeting, New Orleans, Oct. 16, 2009.
10. Greenberg C., Wilkie A.: CommunicationHandoffs: One hospital’s approach. Forum25:10–11, Mar. 2007. http://www.rmf.harvard.edu//files/documents/Forum_V25N1.pdf (accessed September 20, 2010).
The Joint Commission on Handoff Communication
The Joint Commission defines handoff as “the real-time process of passing patient-specific information form one caregiver to another or from one team of caregivers toanother for the purpose of ensuring the continuity and safety of a patient’s care.”4
In 2006, in order to guide health care organizations through the process of improvinghandoff communication processes, The Joint Commission created National PatientSafety Goal 2E (later known as NPSG.02.05.01). As of January 1, 2010, handoff com-munications transitioned out of the National Patient Safety Goals and into StandardPC.02.02.01, Element of Performance 2: “The hospital’s process for handoff communi-cations provides for the opportunity for discussion between the giver and receiver ofpatient information.”
According to The Joint Commission’s Sentinel Events Database, communication break-downs are a contributing factor in 65% of sentinel events, the number one driver of all rootcauses in the database. (Note that the Sentinel Events Database information is collectedthrough voluntary reporting and potentially represents only a fraction of actual events.)
The Joint Commission Center for Transforming Healthcare is currently working on animprovement project related to handoff communications. The project began in August2009, and published solutions are expected in December 2010. Selected by eight lead-ing hospitals and health systems, the Hand-Off Communications Project team includeshospital leadership, clinicians and staff, and the Center’s Black Belts and Green Belts.
The Joint Commission Center for Transforming Healthcare uses Robust ProcessImprovement™ (RPI) methods and tools in the development of its solutions. RPI is afact-based, systematic, and data-driven problem-solving methodology. It incorporatesspecific tools and methods from Lean Six Sigma and change management methodolo-gies. The handoff solutions will be integrated in the center’s Targeted Solutions Tool™(TST). (See page 2 for more information about the TST.)
Volume 10, Issue 11, November 2010Send address corrections to: The Joint Commission Perspectives on Patient SafetySuperior Fulfillment131 W. First St.Duluth, MN 55802-2065800/746-6578
Non-ProfitOrganizationU.S. Postage
PAIDPermit No. 174
Palatine, IL
Safe Surgery Guide focuses on improving safety notonly in procedural and operative areas in any type ororganization, but also across the entire continuum ofa patient’s surgical experience. In presenting practicaltips, strategies, tools, and case studies from a varietyof caregivers and organizations worldwide, SafeSurgery Guide addresses how to avoid the mostserious adverse events that occur in the surgicalsetting, including wrong-site, wrong-procedure,wrong-patient surgery; problems with anesthesia ormedications; retained foreign objects; and surgicalfires.
For more information, or to order this publication, please visit our Web site at http://www.jcrinc.comor call our toll-free Customer Service Center at 877/223-6866. Our Customer Service Center is openfrom 8 A.M. to 8 P.M. EST, Monday through Friday.
Available Now!186 pages
Hardcover book: $85Item number: SSW10ISBN: 978-1-59940-407-3
eBook: $75Item number: EBSSW10ISBN: 978-1-59940-638-1
New book from Joint Commission Resources!
Safe Surgery Guide“By using the tools in this book and continuing to advance the science of health care delivery, surgeons,anesthesiologists, nurses, and others can substantiallyreduce preventable harm and death of patients.” —Peter J. Pronovost, M.D., Ph.D., from his Foreword to
Safe Surgery Guide
Related Documents











