Jo-Ann Ford, RN, MSN Jo-Ann Ford, RN, MSN Associate Director Associate Director BC Hepatitis Program BC Hepatitis Program Diamond Centre, VGH Diamond Centre, VGH Advances in HCV Treatment - Advances in HCV Treatment - Where Where Are we Going? Are we Going?

Jo-Ann Ford, RN, MSN Associate Director BC Hepatitis Program Diamond Centre, VGH Advances in HCV Treatment - Where Are we Going? Where Are we Going?
Dec 24, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Jo-Ann Ford, RN, MSNJo-Ann Ford, RN, MSNAssociate DirectorAssociate DirectorBC Hepatitis ProgramBC Hepatitis ProgramDiamond Centre, VGHDiamond Centre, VGH
Advances in HCV Treatment -Advances in HCV Treatment - Where Are we Going?Where Are we Going?

Disclosures – J. FordDisclosures – J. Ford
• Clinical Trials:
– Hoffmann LaRoche, Merck Canada, Vertex Inc., Pfizer Canada, Johnson & Johnson, Gilead Sciences, Human Genome Sciences, Boehringer Ingelheim
• Advisory Boards:
– Merck Canada, Hoffmann LaRoche, Gilead Sciences, Vertex Inc.
IntroductionIntroduction
• Prevalence HCV in Canada: 1-2%
• BC: Estimated 60,000 – 100,000 chronic carriers
• HCV in Canada
– Yesterday: recipients of blood transfusions
– Today: horizontal transmission (IVDU)

U.S.A. 4 M
SOUTH
AMERICA
10 M
AFRICA 32 M
EAST MEDITERRANEAN
20M
SOUTH EAST ASIA30 M
AUSTRALIA0.2 M
SOURCE, WHO
WEST EUROPE
9 M
FAR EAST ASIA60 M
170 Million Carriers Worldwide
3% of World Population
HCV: A Global Health Problem
CANADA 300,000
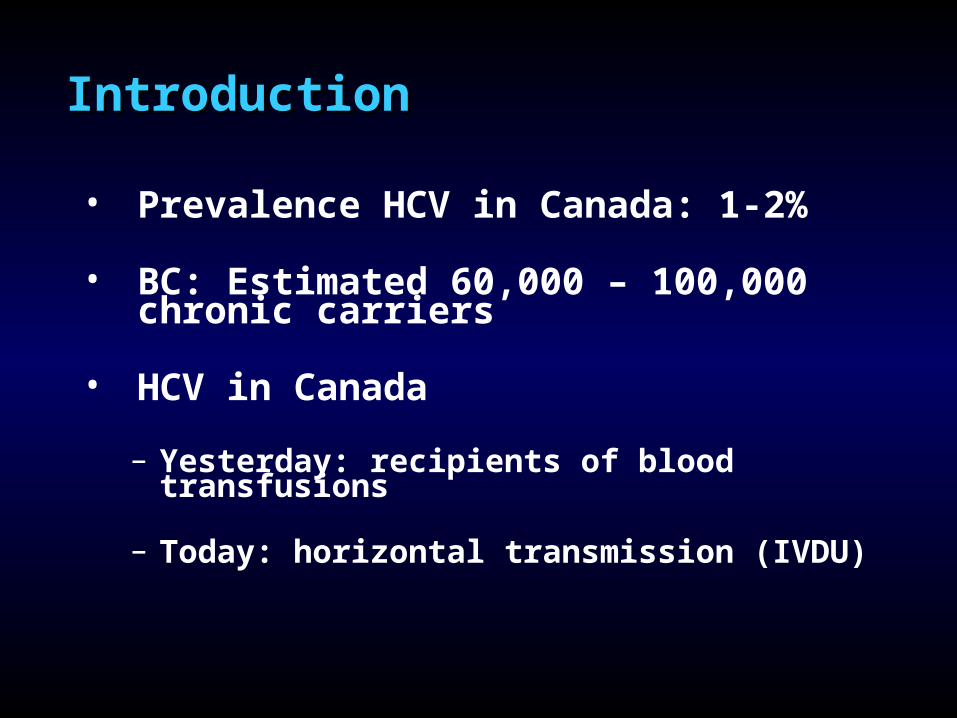
Hepatitis C Disease Progression
Acute Infection Chronic Infection Cirrhosis Death
5% of chronic HCV-infected cirrhotic individuals per year
Liver Failure (Decompensation)
10-20% of chronic HCV-infected individuals
• 80% of infected patients progress to chronic disease
• acute infection often silent
Approx 20% of patients decompensate within 5 years of developing cirrhosis
Liver Cancer (HCC)
Chronic HCV is the leading cause of liver transplantation in the US and Canada
Liver Transplantation
Goals of TreatmentGoals of Treatment
• Cure HCV infection
• Suppress disease activity
• Halt or reverse fibrosis progression
• Reduce risk of hepatocellular carcinoma
• Control extrahepatic consequences of HCV infection

Hadziyannis. J Eur Acad Dermatol Venereol. 1998.
HCV Infection: Extrahepatic Manifestations
Haematological• Mixed cryoglobulinemia• Aplastic anaemia• Thrombocytopenia• Non-Hodgkin’s -cell lymphoma
Dermatological• Porphyria cutanea tarda• Lichen planus• Cutaneous necrotising
vasculitis
Renal• Glomerulonephritis• Nephrotic syndrome
Endocrine• Anti-thyroid antibodies• Diabetes mellitus
Salivary• Sialadenitis
Ocular• Corneal ulcer• Uveitis
Vascular• Necrotising vasculitis• Polyarteritis nodosa• Pulmonary fibrosis
Neuromuscular• Weakness/myalgia• Peripheral neuropathy• Arthritis/arthralgia
AutoimmunePhenomena• CREST syndrome• Granuloma• Autoantibodies
88
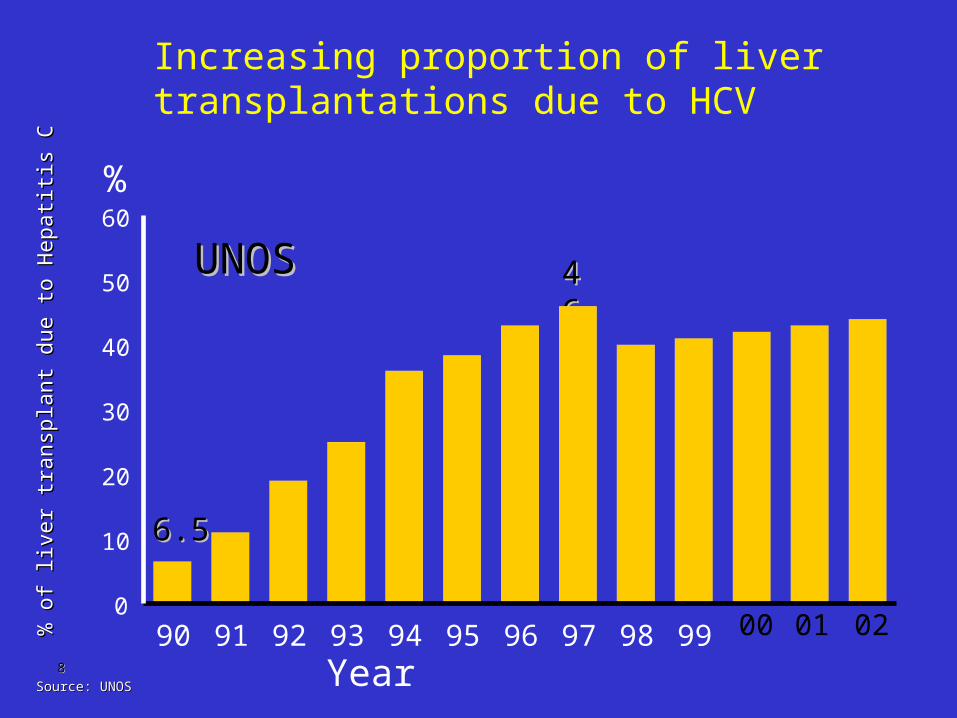
Increasing proportion of liver transplantations due to HCV
0100 02
6.56.5
4646
%
Year
UNOSUNOS
% o
f liv
er tr
ansp
lant
due
to H
epat
itis
C%
of l
iver
tran
spla
nt d
ue to
Hep
atiti
s C
90 91 92 93 94 95 96 97 98 990
10
20
30
40
50
60
Source: UNOSSource: UNOS
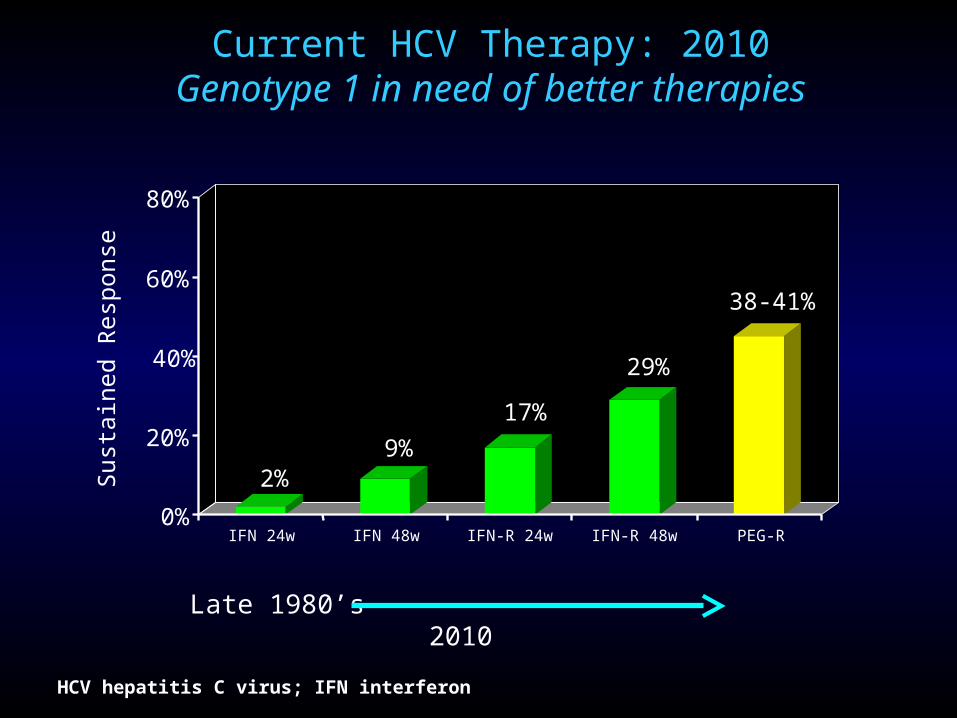
Current HCV Therapy: 2010Genotype 1 in need of better therapies
2%9%
17%
29%
38-41%
0%
20%
40%
60%
80%
Sus
tain
ed R
espo
nse
IFN 24w IFN 48w IFN-R 24w IFN-R 48w PEG-R
HCV hepatitis C virus; IFN interferon
Late 1980’s 2010

IDEALPeginterferon Alfa-2b
or Alfa-2a with Ribavirin forTreatment of Hepatitis C Infection
McHutchison J et al.
N Engl J Med 2009; 361:580-93.

Study Schema and Treatment Regimens
N = 1019 PEG-IFN alfa-2b 1.5 μg/kg/wk
+ RBV 800-1400 mg/d× 48 weeks
N = 1019 PEG-IFN alfa-2b 1.5 μg/kg/wk
+ RBV 800-1400 mg/d× 48 weeks
N = 1035PEG-IFN alfa-2a 180 μg/wk
+ RBV 1000-1200 mg/d× 48 weeks
N = 1035PEG-IFN alfa-2a 180 μg/wk
+ RBV 1000-1200 mg/d× 48 weeks
N = 1016 PEG-IFN alfa-2b 1.0 μg/kg/wk
+ RBV 800-1400 mg/d× 48 weeks
N = 1016 PEG-IFN alfa-2b 1.0 μg/kg/wk
+ RBV 800-1400 mg/d× 48 weeks
ScreeningScreening
Follow-up24 weeksFollow-up24 weeks
Follow-up24 weeksFollow-up24 weeks
Follow-up24 weeksFollow-up24 weeks
2 4 12 24 48 4 12 24
Stratified by baseline viral load (> or ≤ 600,000 IU/mL) and race (African American)Stratified by baseline viral load (> or ≤ 600,000 IU/mL) and race (African American) Standard response stop criteria applied at weeks 12 (no EVR) and 24 (HCV RNA-positive) Standard response stop criteria applied at weeks 12 (no EVR) and 24 (HCV RNA-positive)
HCV RNAa
a LLQ <27 IU/mL (COBAS TaqMan; RocheLLQ <27 IU/mL (COBAS TaqMan; Roche))

Treatment Discontinuation:Non-Response
• Week 12– Subjects with TW12 HCV RNA decline < 2 log10 were
discontinued – Subjects with TW12 HCV RNA decline >2 log10 but not
aviremic were continued on therapy and re-assessed at treatment week 24
• Week 24– Subjects who did not achieve aviremia by TW 24 were
discontinued
• Note: similar to current community practice!

Screening, Treatment, and Follow-up
4469 patients screened
3083 met inclusion criteriaand randomised
1654 completed treatment:540 standard-dose PEG-IFN alfa-2b + RBV
493 low-dose PEG-IFN alfa-2b + RBV621 PEG-IFN alfa-2a + RBV
13 randomised but not treated
1416 discontinued treatment: 830 had treatment failure, 362 had adverse event, 224 had other reason;Of these, 383 never entered follow-up
2417 completed follow-up:812 standard-dose PEG-IFN alfa-2b + RBV
779 low-dose PEG-IFN alfa-2b + RBV826 PEG-IFN alfa-2a + RBV
1386 excluded due to:Ineligible for protocol, declined, lost to follow-up, noncompliant, adverse event
3070 treated:1019 standard-dose PEG-IFN alfa-2b + RBV
1016 low-dose PEG-IFN alfa-2b + RBV1035 PEG-IFN alfa-2a + RBV

SVR Similar Across Treatment Regimens
0
20
40
60
80
38%
41%
% o
f P
atie
nts
Wit
hU
nd
etec
tab
le H
CV
RN
A
PEG 2b 1.0 /R(n=1016)
PEG 2a /R(n=1035)
40%
PEG 2b 1.5 /R(n=1019)
1.5/RBV PEG-IFN alfa-2b vs. PEG-IFN alfa-2a 180/RBV, P=0.57
PEG-IFN alfa-2b 1.5/RBV vs. PEG-IFN alfa-2b 1.0/RBV, P= 0.20

Advances in Therapy
No treatmentNo treatment
IFNIFN(6 months(6 months))
IFNIFN(12 months(12 months))
IFN+IFN+ribavirinribavirin
(12 months(12 months))PeginterferonPeginterferon(12 months(12 months))
Peginterferon Peginterferon ribavirinribavirin
STAT-CSTAT-C
??
19911991 19981998 20002000
100%100%
50%50%
SustainedSustainedvirologicvirologicresponseresponse
raterate

Phase IPhase I
Phase IIPhase II
Phase IIIPhase IIIOthersOthers
Non-Nuc Polymerase inhibitors
Non-Nuc Polymerase inhibitors
Nuc-Polymerase inhibitors
Nuc-Polymerase inhibitors
NS5A inhibitors inhibitors
NS5A inhibitors inhibitors
Protease inhibitorsProtease inhibitors
HCV Pipeline* by MOA and Stage of Development
3/2/2010 – selected compounds only
PreclinicalPreclinical
Telaprevir (J&J/Vertex)
Boceprevir(MRK)
MK7009(MRK)
MK5172(Merck)
GS9256(Gilead)
BMS650032 (BMS)
ITMN-191/R7227 (Roche/Intermune)
TMC-435 (J&J/Tibotec)
BI201335 (BI)
ABT450 (ABT) ACH1625 (Achillion)
GS9190(Gilead)
ANA598(Anadys) VX22
(Vertex)
filibuvir(PFE)
IDX375(Idenix/NVS)
ABT333. ABT072(ABT)
BI201127 (BI)
BMS-791325 (nuc or non-nuc)(BMS)
INX189(Inhibitex)
Biocryst
PSI938(Pharmasset)
GL59393 (GSK)
Medivir/Tibotec
R0622 (Roche)
BI
Japan
Tobacco
IDX-184 (Idenix)
PSI-7977(Pharmasset)
R7128 (Roche/Pharmasset)
Vertex
Enanta
PresidioGSK
Idenix
Merck
AZD7259 NS5A (AZN)
BMS790052 NS5A (BMS)
BMS824393 NS5A (BMS)
Taribavirin (Valeant)
Caspase inhib (Gilead)
Nitazoxanide(Romark)
Debio025 and NIM811 cyclophilins (Novartis)
INF lambda (Zymogen/ NovoNordisk)
Roche
BMSVertex
Gilead
STAT-C Combinations
FiledFiledALBUFERON
(HGS/Novartis)
*Publicly available information via press release, corporate presentations and assumptions based on patent filings

What will be the
Standard of Care for
Genotype 1 Patients?
24 wks Follow-up
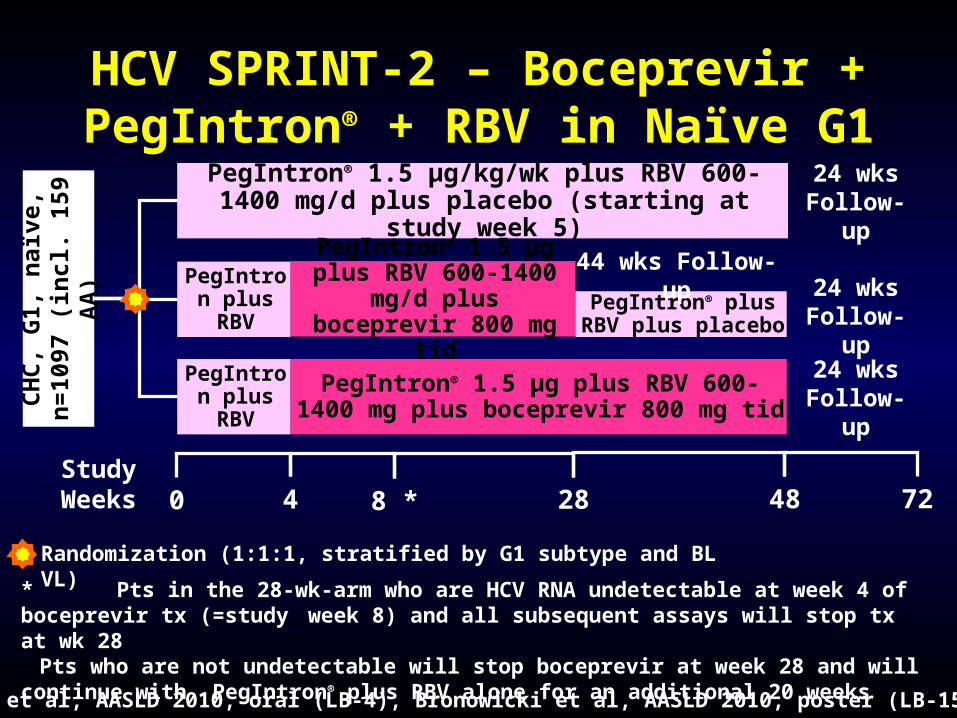
HCV SPRINT-2 – Boceprevir + PegIntron® + RBV in Naïve G1 –
Phase III
Randomization (1:1:1, stratified by G1 subtype and BL VL)
Study Weeks 480 72
CH
C,
G1,
naï
ve,
n=
1097
(in
cl.
159
AA
) PegIntron® 1.5 µg/kg/wk plus RBV 600-1400 mg/d plus placebo (starting at study week 5)
PegIntron® 1.5 µg plus RBV 600-1400 mg/d plus
boceprevir 800 mg tid
PegIntron® 1.5 µg plus RBV 600-1400 mg plus boceprevir 800 mg tid
284
* Pts in the 28-wk-arm who are HCV RNA undetectable at week 4 of boceprevir tx (=study week 8) and all subsequent assays will stop tx at wk 28Pts who are not undetectable will stop boceprevir at week 28 and will continue with PegIntron® plus RBV alone for an additional 20 weeks
PegIntron plus RBV
PegIntron plus RBV
8 *
24 wks Follow-up
24 wks Follow-up
PegIntron® plus RBV plus placebo
44 wks Follow-up
Poordad et al, AASLD 2010, oral (LB-4), Bronowicki et al, AASLD 2010, poster (LB-15)

SPRINT-2 – SVR (ITT)
* *
* p<0.0001Per protocol, if a pt did not have a 24-week post-tx assessment, the patient’s 12-week post-tx assessment was utilizedPress release, August 4, 2010

SPRINT-2: SVR Rates in Patients Who Qualified For 28 Weeks of Therapy
44% of patients qualified for 28 weeks of therapy (assessment at Week 4 of BOC, ie Week 8 of therapy) in response-guided arm
0
20
40
60
80
100
Non-blacks
SV
R (
%)
Blacks
8797
n/N = 143/147 13/15

SPRINT-2: SVR and Relapse Rates (ITT)
0
20
40
60
80
100
Pat
ien
ts (
%)
SVR Relapse
4-wk PR + 44 weeks BOC/PR4-wk PR + response-guided BOC/PR 48-wk PR
67 68
40
8
23
9
0
20
40
60
80
100
Pat
ien
ts (
%)
SVR Relapse
42
53
2317 1412
Nonblack Patients Black Patients
P < .0001P = .044
P = .004
Poordad F, et al. AASLD 2010. Abstract LB-4
n = 211 213 125 21 18 37 22 29 12 3 6 2

SPRINT-2 – Discontinuation due to Adverse Events
Poordad et al, AASLD 2010, oral (LB-4)
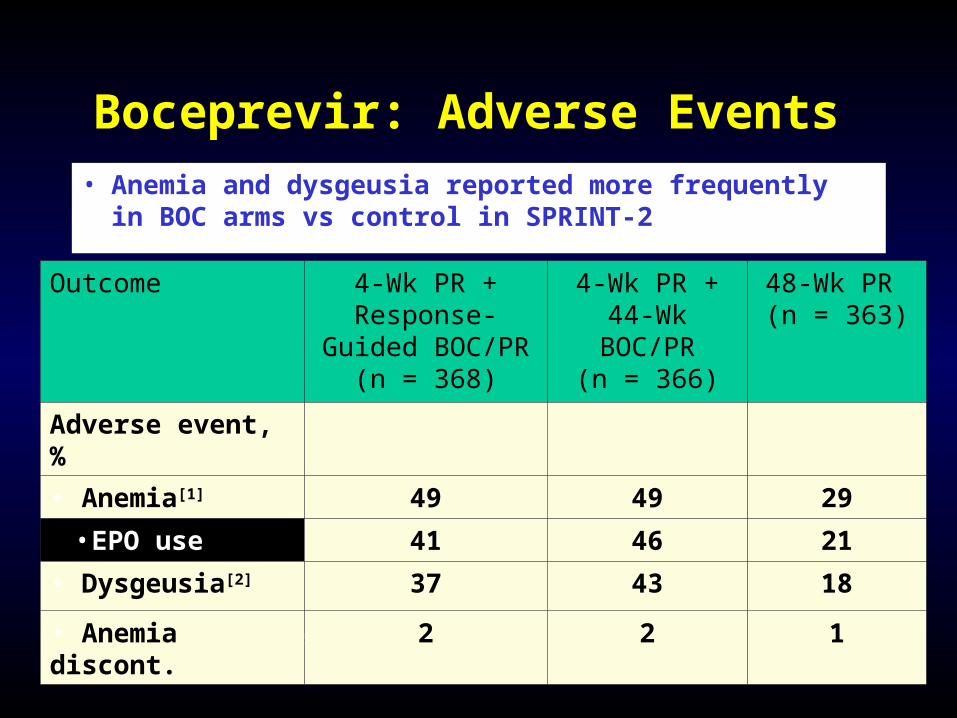
Boceprevir: Adverse Events
1. Poordad F, et al. AASLD 2010. Abstract LB-4.
• Anemia and dysgeusia reported more frequently in BOC arms vs control in SPRINT-2
Outcome 4-Wk PR + Response-Guided
BOC/PR(n = 368)
4-Wk PR + 44-Wk BOC/PR
(n = 366)
48-Wk PR (n = 363)
Adverse event, %
• Anemia[1] 49 49 29
• EPO use 41 46 21
• Dysgeusia[2] 37 43 18
• Anemia discont. 2 2 1
Ira M. Jacobson, John G. McHutchison, Geoffrey M. Dusheiko, Adrian M. Di Bisceglie, Rajender Reddy, Natalie H. Bzowej,
Patrick Marcellin, Andrew J. Muir, Leif Bengtsson, Ann Marie Dunne, Nathalie Adda, Shelley George, Robert S. Kauffman
and Stefan Zeuzem
Telaprevir in Combination with Peginterferon Alfa-2a and Ribavirin in
Genotype 1 HCV Treatment-Naïve patients:
Final Results of Phase 3 ADVANCE Study
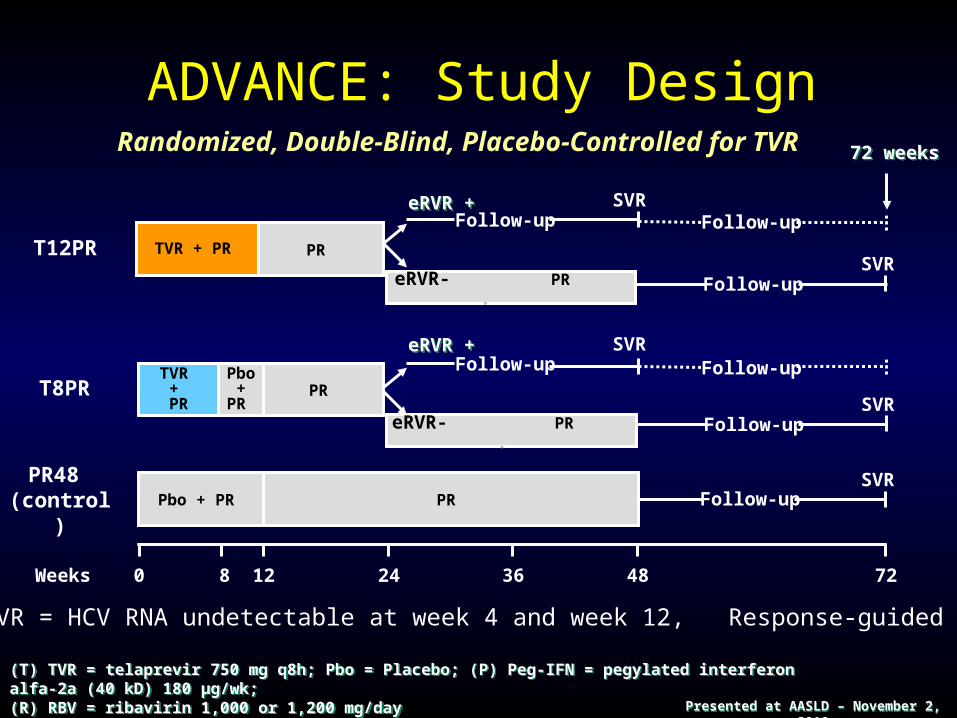
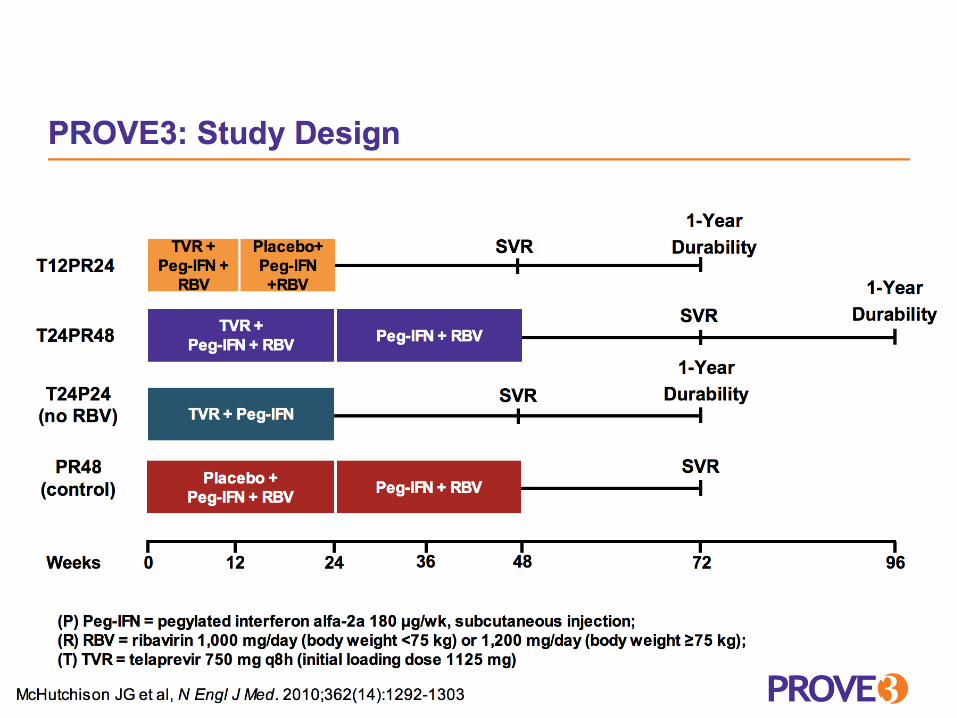
ADVANCE: Study Design
(T) TVR = telaprevir 750 mg q8h; Pbo = Placebo; (P) Peg-IFN = pegylated interferon alfa-2a (40 kD) 180 µg/wk; (R) RBV = ribavirin 1,000 or 1,200 mg/dayRoche Taqman® v2 LLOQ of 25 IU/mL
(T) TVR = telaprevir 750 mg q8h; Pbo = Placebo; (P) Peg-IFN = pegylated interferon alfa-2a (40 kD) 180 µg/wk; (R) RBV = ribavirin 1,000 or 1,200 mg/dayRoche Taqman® v2 LLOQ of 25 IU/mL
eRVR = HCV RNA undetectable at week 4 and week 12, Response-guided therapy
240 48 72Weeks 128 36
Follow-upPR48
(control)
SVRPbo + PR PR
T12PR TVR + PR
Follow-upSVR
eRVR- PR .
eRVR +eRVR +Follow-up
SVR
PR
Follow-upSVR
TVR + PR
T8PR
eRVR- PR .
Pbo +
PR
Follow-upSVReRVR +eRVR +
PR
72 weeks72 weeks
Follow-up
Follow-up
Randomized, Double-Blind, Placebo-Controlled for TVR
Presented at AASLD – November 2, 2010Presented at AASLD – November 2, 2010
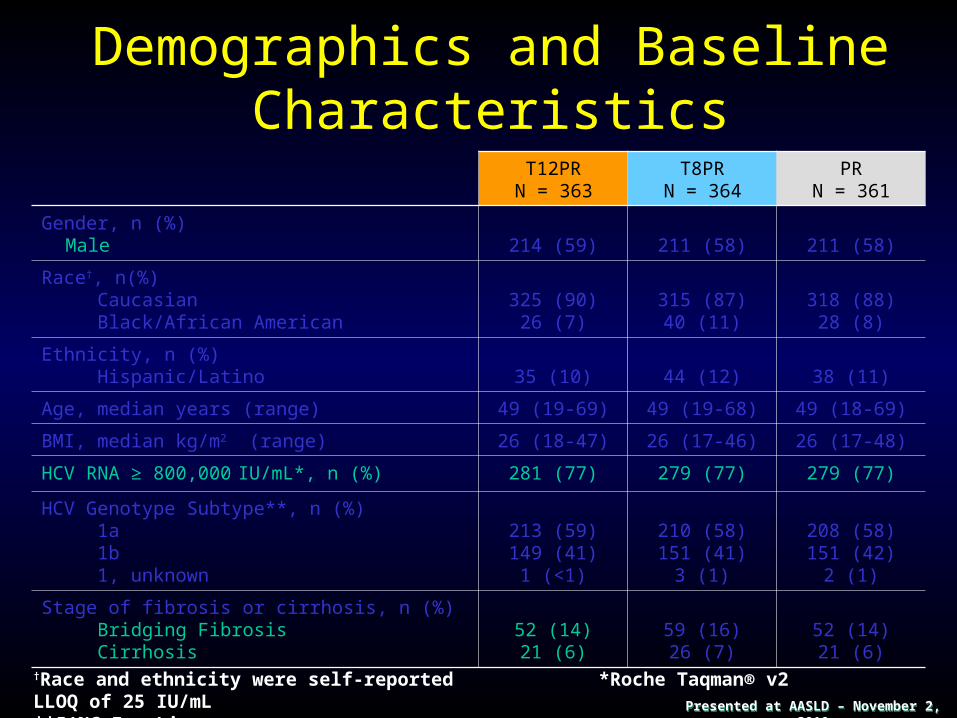
Demographics and Baseline Characteristics
T12PRN = 363
T8PRN = 364
PRN = 361
Gender, n (%)Male 214 (59) 211 (58) 211 (58)
Race†, n(%) Caucasian Black/African American
325 (90)26 (7)
315 (87)40 (11)
318 (88)28 (8)
Ethnicity, n (%) Hispanic/Latino 35 (10) 44 (12) 38 (11)
Age, median years (range) 49 (19-69) 49 (19-68) 49 (18-69)
BMI, median kg/m2 (range) 26 (18-47) 26 (17-46) 26 (17-48)
HCV RNA ≥ 800,000 IU/mL*, n (%) 281 (77) 279 (77) 279 (77)
HCV Genotype Subtype**, n (%) 1a 1b 1, unknown
213 (59)149 (41)1 (<1)
210 (58)151 (41)
3 (1)
208 (58)151 (42)
2 (1)
Stage of fibrosis or cirrhosis, n (%) Bridging Fibrosis Cirrhosis
52 (14)21 (6)
59 (16)26 (7)
52 (14)21 (6)
†Race and ethnicity were self-reported *Roche Taqman® v2 LLOQ of 25 IU/mL**5’NC InnoLipa assay Presented at AASLD – November 2, 2010Presented at AASLD – November 2, 2010

SVR rates in Telaprevir-Treated Patients Compared to Peginterferon/Ribavirin Alone
SVRSVR
75756969
4444
P<0.0001
P<0.0001
271/363271/363 250/364250/364 158/361158/361n/N =n/N =
Per
cen
t o
f p
atie
nts
wit
h S
VR
Per
cen
t o
f p
atie
nts
wit
h S
VR
0
10
20
30
40
50
60
70
80
90
100
T12PRT12PR T8PRT8PR PRPR
Presented at AASLD – November 2, 2010Presented at AASLD – November 2, 2010
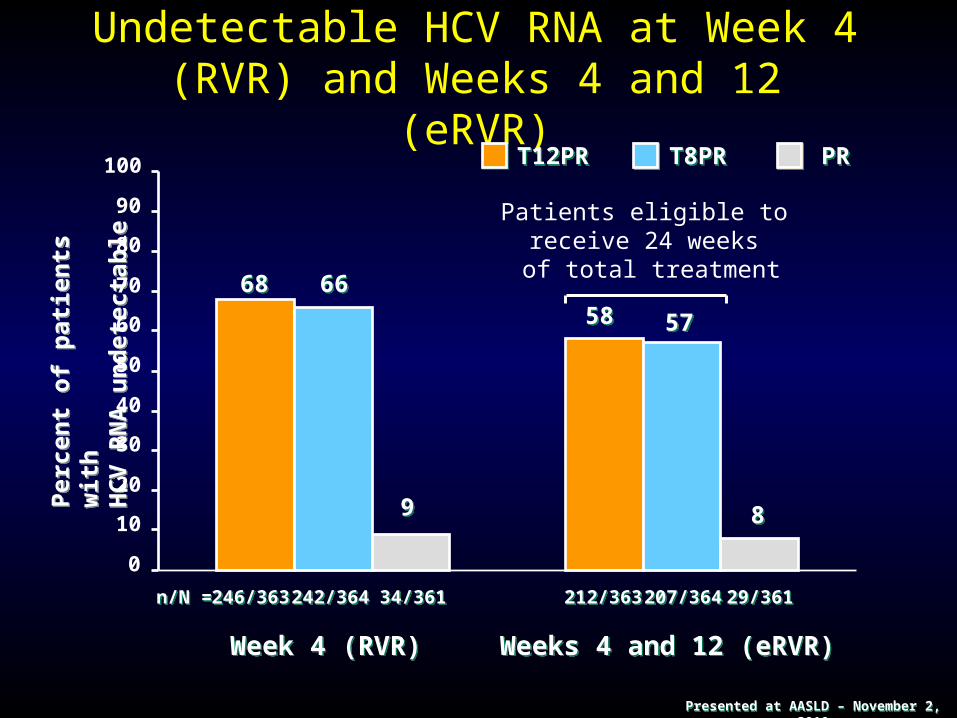
Undetectable HCV RNA at Week 4 (RVR) and Weeks 4 and 12 (eRVR)
246/363246/363 242/364242/364 34/36134/361 29/36129/361207/364207/364212/363212/363
6868 6666
99
5858 5757
88
Per
cen
t o
f p
atie
nts
wit
h
HC
V R
NA
un
det
ecta
ble
Per
cen
t o
f p
atie
nts
wit
h
HC
V R
NA
un
det
ecta
ble
Week 4 (RVR)Week 4 (RVR) Weeks 4 and 12 (eRVR)Weeks 4 and 12 (eRVR)
n/N =n/N =
0
10
20
30
40
50
60
70
80
90
100
Patients eligible to receive 24 weeks of total treatment
T12PRT12PR T8PRT8PR PRPR
Presented at AASLD – November 2, 2010Presented at AASLD – November 2, 2010

SVR Rates by eRVR Status
189/212189/212 171/207171/207 28/2928/29 130/332130/33279/15779/15782/15182/151
89898383
9797
54545050
3939
eRVR+eRVR+ eRVR- eRVR-
n/N =n/N =
Per
cen
t o
f p
atie
nts
w
ith
SV
RP
erce
nt
of
pat
ien
ts
wit
h S
VR
0
10
20
30
40
50
60
70
80
90
100
48-week regimen 24-week regimen
T12PRT12PR T8PRT8PR PRPR
Presented at AASLD – November 2, 2010Presented at AASLD – November 2, 2010

ADVANCE AEs leading to DC and most common AEs
% Pts. with T12PR T8PR PR
Any AE 99 99 98
Fatigue 57 58 57
Pruritus 50 45 36
Headache 41 43 39
Nausea 43 40 31
Rash 37 35 24
Anemia 37 39 19
Insomnia 32 32 31
Diarrhea 28 32 22
Flu-like symptoms
28 29 28
Pyrexia 26 30 24
Events occurring >10% in any TVR group vs. Placebo are shaded.

ADVANCE – Discontinuation of Treatment due to Rash and Anemia
Jacobson et al, AASLD 2010, oral (211)
What will be the
Approach for
PegIFN and Ribavirin Failures?
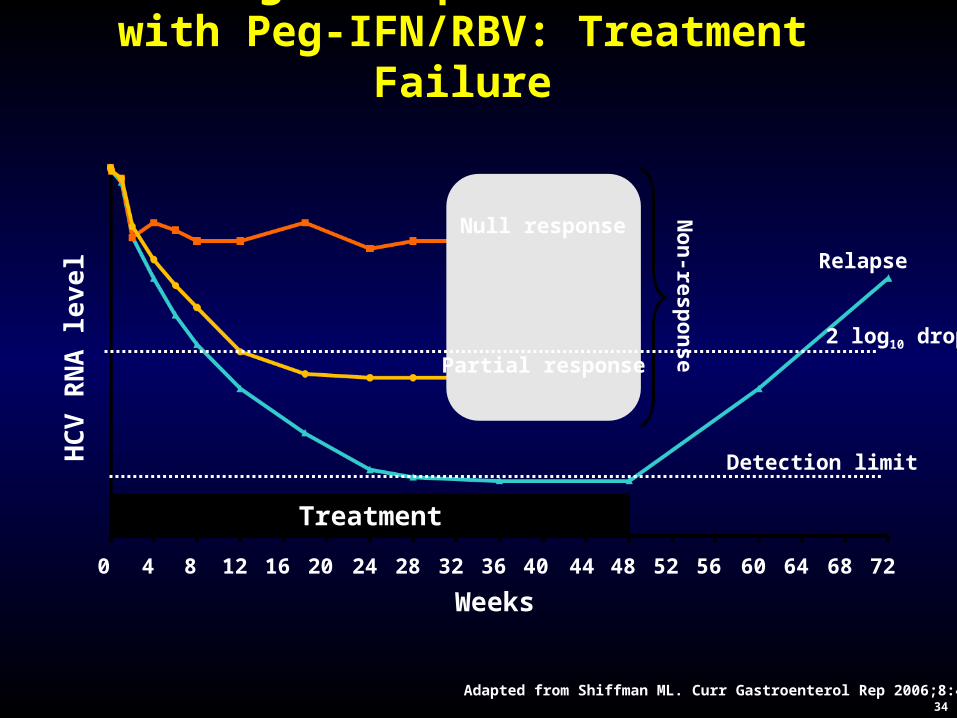
Virologic Response Patterns with Peg-IFN/RBV: Treatment Failure
Detection limit
Relapse
Null response
Partial response
Treatment
No
n-resp
on
se
0 4 8 12 16 20 24 28 32 36 40 44 48 52 56 60 64 68 72
HC
V R
NA
lev
el
Weeks
34Adapted from Shiffman ML. Curr Gastroenterol Rep 2006;8:46–52
2 log10 drop
HCV RESPOND-2 Final Results High Sustained Virologic Response Among Genotype 1
Previous Non-Responders and Relapsers to Peginterferon/Ribavirin when Re-Treated with Boceprevir
Plus PEGINTRON (Peginterferon alfa-2b)/Ribavirin
Bruce R. Bacon, Stuart C. Gordon, Eric Lawitz, Patrick Marcellin, John M. Vierling, Stefan Zeuzem, Fred Poordad, Navdeep Boparai, Margaret Burroughs, Clifford A. Brass,
Janice K. Albrecht, and Rafael Esteban
For the RESPOND-2 Investigators
RESPOND-2: Study ObjectivesRESPOND-2: Study Objectives
• Compare safety/efficacy of two treatment strategies with boceprevir added to peginterferon/ribavirin (PR) versus PR alone in genotype 1 patients who failed treatment with PR
• Evaluate safety/efficacy independently in two patient populations, history PR non-responders (decrease of HCV-RNA ≥2-log by week 12 of prior therapy but with detectable HCV-RNA throughout the course of therapy) and relapsers
• Explore response-guided therapy (RGT) vs. 44 weeks of therapy with boceprevir regimen (BOC/PR48)
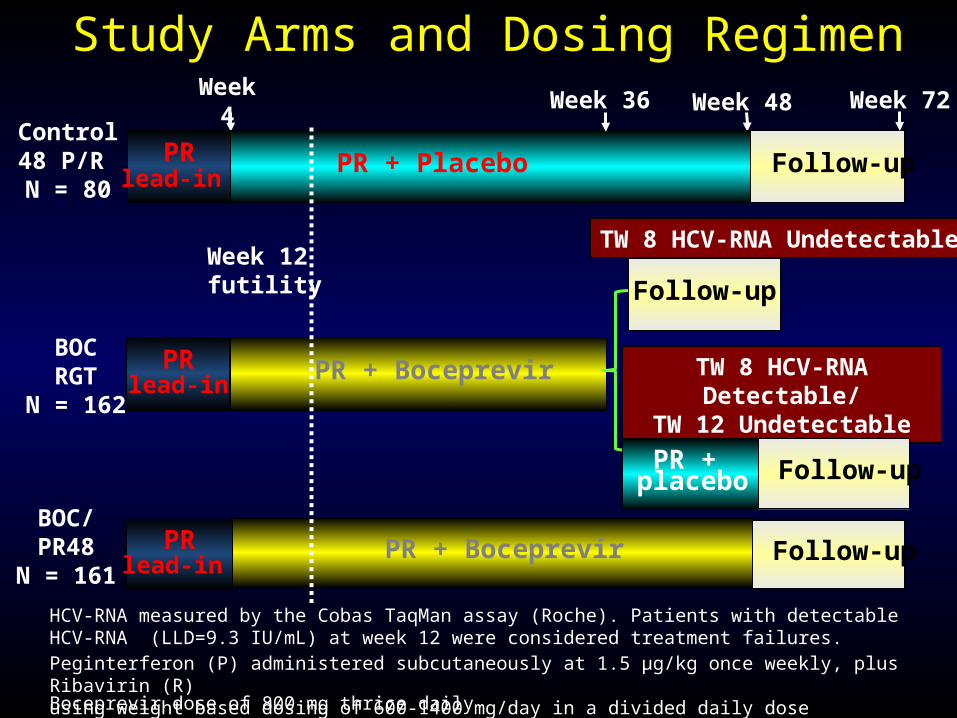
Week 4
Week 48
PR + Placebo Follow-up
PRlead-in
PR + Boceprevir
PRlead-in
Week 36 Week 72
TW 8 HCV-RNA Undetectable
TW 8 HCV-RNA Detectable/
TW 12 Undetectable
PR + placebo Follow-up
Follow-up
Study Arms and Dosing Regimen
Control48 P/R N = 80
BOCRGT
N = 162
Peginterferon (P) administered subcutaneously at 1.5 μg/kg once weekly, plus Ribavirin (R) using weight based dosing of 600-1400 mg/day in a divided daily doseBoceprevir dose of 800 mg thrice daily
PR + BoceprevirPRlead-in
Follow-upBOC/PR48
N = 161
HCV-RNA measured by the Cobas TaqMan assay (Roche). Patients with detectable HCV-RNA (LLD=9.3 IU/mL) at week 12 were considered treatment failures.
Week 12 futility
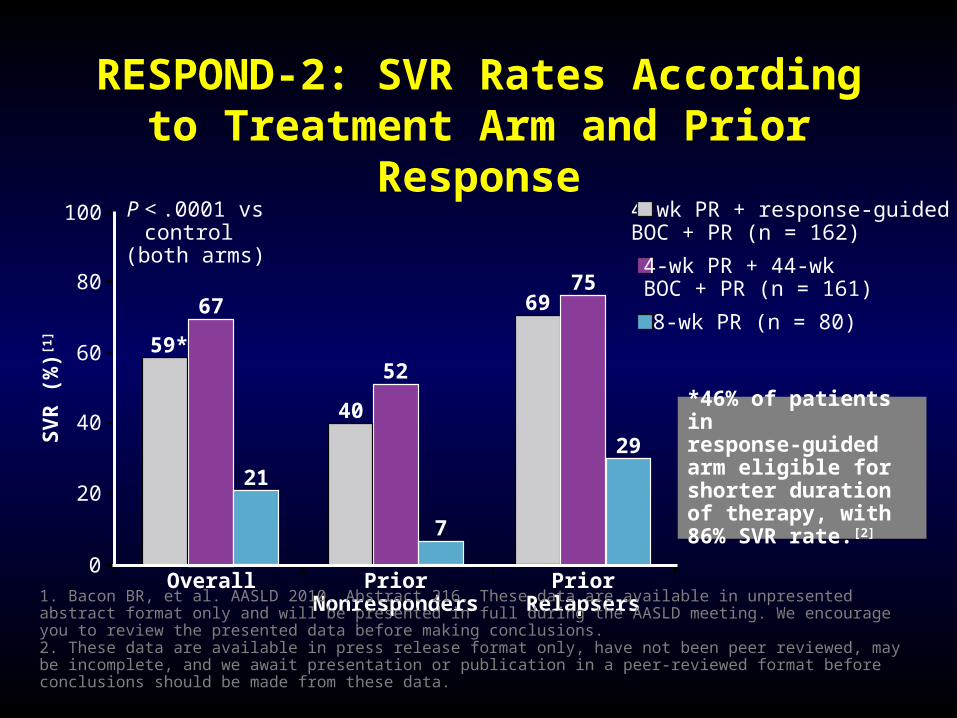
RESPOND-2: SVR Rates According to Treatment Arm and Prior Response
0
20
40
60
80
100
Overall
SV
R (
%)[1
]
4-wk PR + 44-wk BOC + PR (n = 161)
59*
PriorNonresponders
PriorRelapsers
48-wk PR (n = 80)
4-wk PR + response-guided BOC + PR (n = 162)
67
21
40
52
7
75
29
69
P < .0001 vs control
(both arms)
1. Bacon BR, et al. AASLD 2010. Abstract 216. These data are available in unpresented abstract format only and will be presented in full during the AASLD meeting. We encourage you to review the presented data before making conclusions.2. These data are available in press release format only, have not been peer reviewed, may be incomplete, and we await presentation or publication in a peer-reviewed format before conclusions should be made from these data.
*46% of patients inresponse-guided arm eligible for shorter duration of therapy, with 86% SVR rate.[2]


Telaprevir-based Therapy in Genotype 1 Hepatitis C Virus-infected Patients with
Prior Null Response, Partial Response or Relapse to Peginterferon/Ribavirin:
REALIZE Trial Final ResultsGraham R Foster,1 Stefan Zeuzem,2 Pietro Andreone,3 Stanislas Pol,4 Eric Lawitz,5 Moises Diago,6 Stuart Roberts,7 Roberto Focaccia,8 Zobair Younossi,9 Andrzej Horban,10 Rolf Van Heeswijk,11 Sandra De Meyer,11 Don Luo,12 Gaston Picchio,12 Maria Beumont11
1Queen Mary University of London, Institute of Cell and Molecular Science, London, UK; 2Johann Wolfgang Goethe University Medical Center, Frankfurt am Main, Germany; 3Università di Bologna, Bologna, Italy; 4Université Paris Descartes, INSERM Unité 567, and Assistance Publique–Hôpitaux de Paris, Cochin Hospital Paris, France; 5Alamo Medical Research, San Antonio, TX, USA; 6Hospital General de Valencia, Valencia, Spain; 7Department of Gastroenterology, Alfred Hospital, Melbourne, Australia; 8Emilio Ribas Infectious Diseases Institute, São Paulo, Brazil; 9Center for Liver Disease, Inova Fairfax Hospital, Falls Church, VA,USA; 10Medical University of Warsaw, Wolska, Warsaw, Poland; 11Tibotec BVBA, Beerse, Belgium; 12Tibotec Inc., Titusville, NJ, USA
44Presented at APASL, 18 February 2011 Presented at APASL, 18 February 2011
REALIZE: Study ObjectivesREALIZE: Study Objectives
• International, randomized, double-blind, multicentre, placebo-controlled Phase III trial
• Primary objective:– To evaluate superior efficacy (proportion of patients
achieving an SVR) of TVR-based therapy compared with standard treatment in patients within the prior relapser and prior-non-responder (partials/nulls) group
• Key secondary objectives:– Evaluation of effect of Peg-OFN/RBV lead-in on
efficacy of TVR-based treatment– Assessment of safety and tolerability of TVR-based
treatment
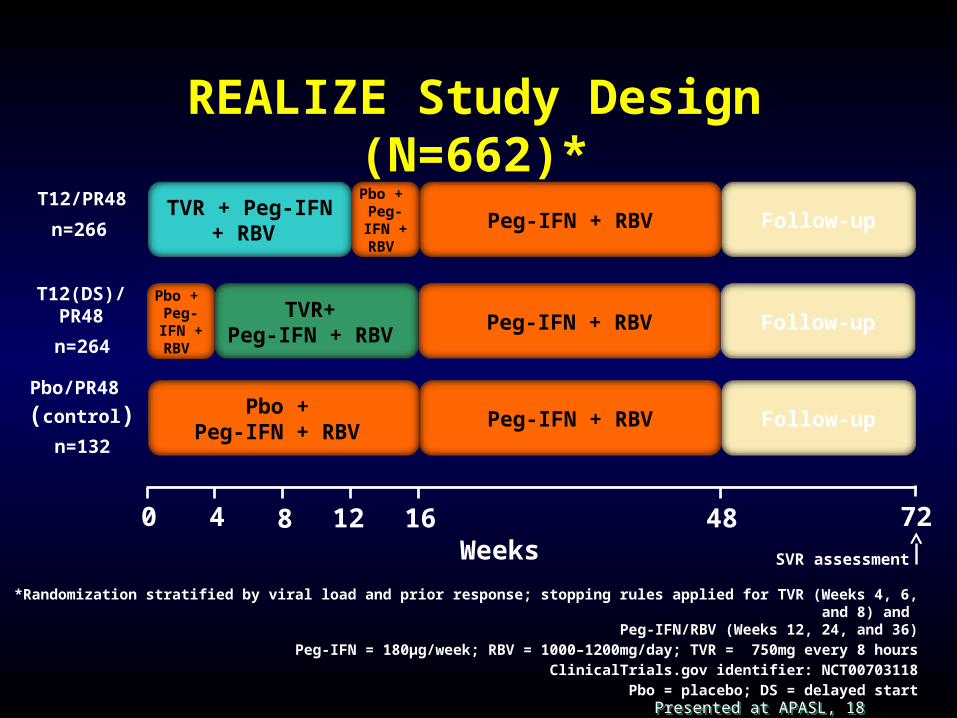
REALIZE Study Design (N=662)*
484 160 128Weeks
72
T12/PR48Peg-IFN + RBV
TVR + Peg-IFN + RBV
Pbo + Peg-IFN + RBV n=266 Follow-up
SVR assessment
TVR+ Peg-IFN + RBV
Peg-IFN + RBVT12(DS)/
PR48
n=264Follow-up
Pbo + Peg-IFN + RBV
*Randomization stratified by viral load and prior response; stopping rules applied for TVR (Weeks 4, 6, and 8) and Peg-IFN/RBV (Weeks 12, 24, and 36)
Peg-IFN = 180μg/week; RBV = 1000–1200mg/day; TVR = 750mg every 8 hoursClinicalTrials.gov identifier: NCT00703118
Pbo = placebo; DS = delayed start
Pbo/PR48 (control) Pbo +
Peg-IFN + RBV Peg-IFN + RBV
n=132
Follow-up
Presented at APASL, 18 February 2011 Presented at APASL, 18 February 2011

47
REALIZE: Baseline Characteristics
*Determined using the COBAS TaqMan HCV assay version 2.0; ‡Determined by NS3 sequencing; §Defined by local pathologists
Presented at APASL, 18 February 2011 Presented at APASL, 18 February 2011
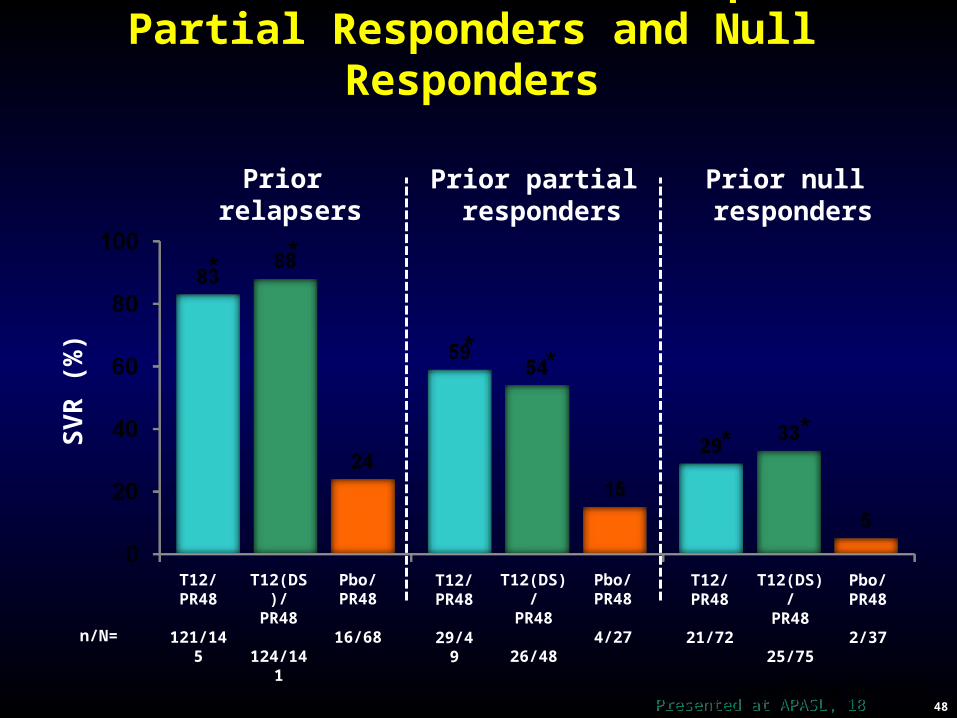
REALIZE: SVR in Prior Relapsers, Partial Responders and Null Responders
SV
R (
%)
Prior relapsers
Prior partial responders
Pbo/PR48
4/27
T12/PR48
29/49
T12(DS)/PR48
26/48n/N=
Pbo/PR48
2/37
T12/PR48
21/72
T12(DS)/PR48
25/75
Pbo/PR48
16/68
T12/PR48
121/145
T12(DS)/PR48
124/141
Prior null responders
48*p<0.001 vs Pbo/PR48
**
**
**
Presented at APASL, 18 February 2011 Presented at APASL, 18 February 2011

T12/PR48 (n=266)
T12(DS)/PR48
(n=264)Pbo/PR48
(n=132)Discontinuation of All Study Drugs during TVR Treatment Phase, n (%)
Any AE
Rash events
Anemia events
Pruritus
17 (6)
2 (1)
2 (1)
0
11 (4)
2 (1)
2 (1)
1 (<1)
4 (3)
0
0
0
Discontinuation of TVR during TVR Treatment Phase, n (%)
Any AE
Rash events
Anemia events
Pruritus
39 (15)
12 (5)
6 (2)
1 (<1)
29 (11)
10 (4)
9 (3)
3 (1)
4 (3)
0
0
0
49
AEs Leading to Study Drug Discontinuations
AE = adverse event
Presented at APASL, 18 February 2011 Presented at APASL, 18 February 2011

REALIZE: ConclusionsREALIZE: Conclusions
• TVR/Peg-IFN/RBV was superior to Peg-IFN/RBV in treatment experienced populations including null responders, partial responders and relapsers
• A lead-in strategy using TVR-based regimen did not improve SVR rates or reduce on-treatment virologic failure and relapse rates
• Safety data were comparable to previous TVR studies. Adverse events leading to permanent discontinuation (anemia and rash) were more frequent in the pooled telaprevir group then in the control group
Presented at APASL 18 Feb 2011Presented at APASL 18 Feb 2011
CONCLUSIONS
• The future is very bright, with greater opportunity for CURE
• Boceprevir/Telaprevir associated with higher SVR rates • Shorter duration (response-guided therapy)
• Protease inhibitors & PegIFN/Ribavirin expected to be the next standard of care for HCV Genotype 1

CONCLUSIONS
• The future is very bright for our Treatment Failure patients
• Boceprevir/Telaprevir will set a new standard for our treatment-experienced
Related Documents