DR. KEIM Dr . McLaughlin, your new book, Facial and Dental Planning for Orthodontists and Oral Surgeons, co-authored with Dr . Bill Arnett, 1 focuses on diagnosis and treatment plan- ning. What do you see as the new, unique, and different aspects of the philosophy of diagnosis and treatment planning? DR. MCLAUGHLIN Emphasis is on three areas of evaluation—the temporomandibular joints, the face, and the dentition—with new and easier-to-use information in each area. In addi- tion to the traditional methods of TMJ evaluation and treatment, there is the challenging area of TMJ remodeling with emphasis on stabilization and medical management. Important contribu- tions are made in the book by Dr. Tom Eggleton (physical therapy), Dr. Richard Gevirtz (biofeed- back), and Dr. Steve Milam (medical manage- ment and TMJ lavage). Next there are more thor- ough and objective methods of facial planning. In the past, due to incomplete clinical examina- tion and inadequate information from cephalo- metric x-rays, more subjective facial planning decisions have been made. While this may pro- duce adequate results, there is a greater chance of error. In my opinion, the above areas are two of Dr. Arnett’s great contributions to both orthodon- tics and oral surgery. Finally, once a decision has been made concerning the angulation and the anteroposterior and vertical position of the incisors from the facial analysis, specific infor- mation is provided for calculating the orthodon- tic movements required for the midlines, cus- pids, and molars. This, too, reduces errors in the dental alignment of our cases. DR. KEIM What do you see as the appropriate goals for treatment planning? DR. MCLAUGHLIN The goals of treatment in- clude: • Healthy musculature and temporomandibular joints • Facial balance • Correct static and functional occlusion • Periodontal health • Resolving the patient’s chief complaints • Stability of dental and skeletal changes • Improved airway DR. KEIM What are the requirements for a sys- tematized and objective approach to diagnosis and treatment planning? DR. MCLAUGHLIN It is important that very specific methods and techniques be carried out from the initial contact with the patient to the presentation of the treatment plan. Important steps cannot be eliminated along the way, and VOLUME XXXVIII NUMBER 4 © 2004 JCO, Inc. 199 JCO INTER VIEWS Richard P. McLaughlin, DDS on Facial and Dental Planning Dr . McLaughlin is a Contributing Editor of the Journal of Clinical Orthodontics and in the private practice of orthodontics at 1831 Sunset Cliffs Blvd., San Diego, CA 92107; e-mail: rpmclaugh@aol. com. Dr. Keim is Editor of the Journal of Clinical Orthodontics. Dr . McLaughlin Dr. Keim ©2004 JCO, Inc. May not be distributed without permission. www.jco-online.com

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
DR. KEIM Dr. McLaughlin, your new book,Facial and Dental Planning for Orthodontistsand Oral Surgeons, co-authored with Dr. BillArnett,1 focuses on diagnosis and treatment plan-ning. What do you see as the new, unique, anddifferent aspects of the philosophy of diagnosisand treatment planning?
DR. MCLAUGHLIN Emphasis is on threeareas of evaluation—the temporomandibularjoints, the face, and the dentition—with new andeasier-to-use information in each area. In addi-tion to the traditional methods of TMJ evaluationand treatment, there is the challenging area ofTMJ remodeling with emphasis on stabilizationand medical management. Important contribu-tions are made in the book by Dr. Tom Eggleton(physical therapy), Dr. Richard Gevirtz (biofeed-back), and Dr. Steve Milam (medical manage-ment and TMJ lavage). Next there are more thor-
ough and objective methods of facial planning.In the past, due to incomplete clinical examina-tion and inadequate information from cephalo-metric x-rays, more subjective facial planningdecisions have been made. While this may pro-duce adequate results, there is a greater chance oferror. In my opinion, the above areas are two ofDr. Arnett’s great contributions to both orthodon-tics and oral surgery. Finally, once a decision hasbeen made concerning the angulation and theanteroposterior and vertical position of theincisors from the facial analysis, specific infor-mation is provided for calculating the orthodon-tic movements required for the midlines, cus-pids, and molars. This, too, reduces errors in thedental alignment of our cases.
DR. KEIM What do you see as the appropriategoals for treatment planning?
DR. MCLAUGHLIN The goals of treatment in-clude:• Healthy musculature and temporomandibularjoints• Facial balance• Correct static and functional occlusion• Periodontal health• Resolving the patient’s chief complaints• Stability of dental and skeletal changes• Improved airway
DR. KEIM What are the requirements for a sys-tematized and objective approach to diagnosisand treatment planning?
DR. MCLAUGHLIN It is important that veryspecific methods and techniques be carried outfrom the initial contact with the patient to thepresentation of the treatment plan. Importantsteps cannot be eliminated along the way, and
VOLUME XXXVIII NUMBER 4 © 2004 JCO, Inc. 199
JCO INTERVIEWS
Richard P. McLaughlin, DDSon Facial and Dental Planning
Dr. McLaughlin is a Contributing Editor of the Journal of ClinicalOrthodontics and in the private practice of orthodontics at 1831Sunset Cliffs Blvd., San Diego, CA 92107; e-mail: [email protected]. Dr. Keim is Editor of the Journal of Clinical Orthodontics.
Dr. McLaughlin Dr. Keim
©2004 JCO, Inc. May not be distributed without permission. www.jco-online.com

checks and balances need to occur as the processproceeds. In addition, objective methods ratherthan subjective opinions should accompany theprocess.
DR. KEIM Where is the patient’s chief com-plaint addressed in this protocol?
DR. MCLAUGHLIN After obtaining personalinformation from the patient, a “Chief ComplaintForm”, as developed by Dr. Arnett, is complet-ed.2 The original form has been modified intotwo forms: a basic orthodontic form for routinecases, and a surgical form for more complexcases. Each form is in three sections, askingquestions concerning the face, the teeth, andsymptoms (the TMJs). This form is reviewedwith the patient at the initial examination andonce again at the consultation to insure that thepatient’s concerns are being addressed.
DR. KEIM What are the essential elements of aclinical patient exam?
DR. MCLAUGHLIN The clinical exam con-sists of three parts: the TMJ exam, the facialexam (frontal view and profile view), and theintraoral exam. A screening TMJ examination isindicated for all patients, whether they do or donot describe symptoms. Two palpation positions(over the condyles externally and using the smallfingers in the ear canal) are used during threemandibular movements (opening and closing,left and right lateral, and protrusion). These pro-vide information concerning the patient’s rangeof movement, deviation from normal move-ments, any pain during movement, and jointsounds. The protocol for the facial examinationwas published by Dr. Arnett and Dr. RobertBergman,3 but both the frontal and profile facialexams have been modified slightly since theoriginal publication. Lastly, the intraoral exam iscompleted, recording necessary information.
DR. KEIM What do you see as the main areas ofdiagnosis?
DR. MCLAUGHLIN The main areas of diagno-
sis follow the main areas of the clinical exam.Concerning the temporomandibular joints, it isimportant to determine if the problem is purelymuscular, strictly limited to the joints, or, morecommonly, a combination of the two. It is criti-cal to determine the location and extent of TMJdamage—in other words, local or total remodel-ing of the condyle. A main emphasis of the bookis to evaluate the face three-dimensionally andobjectively determine and quantify the areas offacial deformity. By doing this, we can be moreaccurate in determining the best method of treat-ment as well as alternative options. In the past,this has been an area of subjective estimates, andmistakes are possible with such an approach.Concerning the dentition, accurate determina-tions need to be made of molar relationships,midlines, occlusal cants, arch widths, archcrowding, and planes of occlusion. This can thenbe combined with information on ideal incisorpositioning from the facial plan. With this infor-mation, a more accurate determination can bemade concerning tooth movements needed andanchorage requirements.
DR. KEIM How is “facial planning” differentfrom traditional orthodontic treatment planning?
DR. MCLAUGHLIN Facial planning involvestwo key components that have not been as thor-oughly addressed as possible in the past. The firstkey is a thorough clinical facial examination.This provides us with important soft-tissue, den-tal, and skeletal information in the frontal (trans-verse and vertical) dimension and the sagittal(vertical and horizontal) dimension. This infor-mation can be developed and objectified by thesecond key, which is Soft Tissue CephalometricAnalysis (STCA) and Cephalometric TreatmentPlanning (CTP). These two methods help us tominimize the weaknesses inherent in cranial basereferences and provide us with significantlygreater soft-tissue information.
DR. KEIM How does facial planning differfrom traditional facial planning based on cranialbase measurements?
200 JCO/APRIL 2004
JCO INTERVIEWS

DR. MCLAUGHLIN Utilizing cranial baselandmarks to evaluate difficult cases has alwaysbeen problematic, since these landmarks vary inposition from patient to patient, and are oftenhard to locate on the head film. Also, traditionalcephalometric treatment planning has focused ondentoskeletal factors, with only minimal empha-sis on soft tissues. Surgeons in the 1980s (Epker,Wolford, and others) began focusing more onsoft tissue by utilizing a line perpendicular toFrankfort horizontal and through subnasale.Such a method provided a greater focus on softtissue; however, it was still subject to the prob-lems associated with the cranial base landmark,Frankfort horizontal. Studies by various authorsin the 1980s and 1990s (for example, Lundstromand Lundstrom4) suggested that utilizing naturalhead posture was a more accurate reference thancranial base references. The True Vertical Line isa vertical line through subnasale with the patientin natural head posture. Dr. Arnett used this lineto develop his analysis,5 which provides us withthorough information on virtually all of theimportant dentoskeletal and soft-tissue measure-ments in the vertical and horizontal planes.
DR. KEIM What kind of standards are used inan objective treatment-planning system?
DR. MCLAUGHLIN We have had objectivestandards relative to static occlusion, such as Dr.Andrews’s six keys, and functional occlusion,such as the goals described by Dr. Roth. Admit-tedly, we are unable to achieve these goals inevery case, and the reasons are multiple. Thisdoes not mean that we discard them as irrelevant.They continue to serve as objective referencesand reasonable goals to achieve whenever possi-ble. In the same way, we can benefit from objec-tive standards relative to facial planning, eventhough we are unable to achieve such results ineach case. More research is needed so that objec-tive standards are established for different ethnicgroups. In addition to the Arnett norms (essen-tially a Caucasian Southern California group),the Japanese are well on the way to completingand publishing their norms. Studies are also on-
going in Korea and India to my knowledge. Thisis a very exciting project, and the minor differ-ences are enlightening.
DR. KEIM What role does condylar positionplay in this method of case documentation?
DR. MCLAUGHLIN Consistent condyle posi-tioning is critical in the case documentationprocess. If this is not done, critical errors can bemade in treatment planning. A wax bite withproper condyle positioning is placed when takingfacial photographs and cephalometric x-rays andwhen mounting study models. In this way, thereis a consistency of records when evaluating thecase.
DR. KEIM Where should the condyle be placedduring record taking?
DR. MCLAUGHLIN The condyle needs to beseated superiorly in the fossa in an uncompressedposition during record taking. The position mayvary slightly from patient to patient and is prob-ably a very small area vs. a pinpoint position.This perspective is not a license to be sloppy dur-ing record taking, but a realistic awareness. Theimportance of the seated condyle position is welldocumented with extensive literature on condy-lar sag in surgical cases, relapse with functionalappliances, mandibular positional changes withrheumatoid and degenerative arthritis, and gener-ally unstable occlusions associated with unseatedcondyles. Treating patients to unseated condylepositions has consistently led to treatment fail-ure. We do not need to beat this subject to deathany longer. On the other hand, in our zeal to pro-vide a seated condyle position, we have at timesplaced the condyle in a compressed position.There is a growing body of evidence showingthat condylar compression leads to local or eventotal condylar remodeling. Therefore, the goal isto place the condyle in a seated but uncom-pressed position. This is not the easiest of tasks.
DR. KEIM How do you assure that the condylesare in this position during record taking?
VOLUME XXXVIII NUMBER 4 201
Richard P. McLaughlin, DDS

DR. MCLAUGHLIN For bite registration, thepatient is seated in the chair at approximately a45° angle. The mandible is manipulated withgentle seating pressure, using the thumb on thechin and two fingers under each side of the man-dible. Once this has been practiced with thepatient, the initial wax bite is taken. The selectedwax is a sheet of medium-hardness pink base-plate wax, folded in half and then folded again to1cm width in the incisor area (open bites needmore thickness in the anterior area). The wax isthen trimmed to the general shape of the patient’supper arch. With the wax in place, the patient isclosed in the seated condyle position to firsttooth contact. The wax bite is removed, and asharp pair of scissors is used to accurately trimjust behind the most distal molars, through theupper buccal cusps, and along the edge of theincisors. This avoids soft-tissue distortion duringthe next two wax-bite checks and when mount-ing the models. The wax bite is then repositionedonto the maxillary teeth, and the bite is retaken inthe same way. The lower incisors must fit pre-cisely into the incisor indentations. If not, thewax bite is discarded and the process is begunagain. This repeated wax bite is removed andchilled in cold water. It is then repositioned andtaken a third time. Once again, the lower incisorsmust fit accurately, or the entire process isrepeated. If it is not possible to obtain repeatedincisor positioning, then the patient is most like-ly in need of a phase of splint therapy. Also, if theTMJ examination reveals joint or muscle symp-toms, then the patient should undergo a phase ofsplint therapy. Using the above technique hasproven to be the best method of avoiding mandi-bular positioning errors.
DR. KEIM The role of condylar remodeling inthe long-term instability of many cases has onlyrecently been fully understood. Could you speakto this issue?
DR. MCLAUGHLIN The work of Dr. Arnett,Dr. Milam, and others has been very helpful inthis area. They often refer to condylar remodel-ing as the “last frontier” in the TMJ management
issue. The book presents an up-to-date discus-sion of this subject. In summary, condylar re-modeling can be local (confined to smaller areason the head of the condyle) or total (involvingthe entire head of the condyle). Local remodelingis also being referred to as “functional” remodel-ing, since it is observed in nearly everyone as aresult of normal functioning. With this type ofremodeling, ramus height is not affected and theocclusion remains stable. Total remodeling,which fortunately occurs in a small number ofpatients, is referred to as “dysfunctional remod-eling”. This is the orthodontist’s and surgeon’snightmare, since the ramus height is affected andthe bite is unstable. It is also significant for theorthodontist, since it can disturb normal growthand development. Joint stabilization with splinttherapy is important for these patients. Also, pro-tocols for medical management of the joint arebeing developed, and, hopefully, this will allowus to begin improving our ability to help thesepatients.
DR. KEIM You define three groups of cases:Group 1 is non-surgical, Group 3 is surgical, andGroup 2 is borderline cases that could be treatedsurgically or non-surgically. Where do you drawthe line between a Group 2 and a Group 3 case,one that definitely requires surgery?
DR. MCLAUGHLIN It is impossible to draw aclear line between surgical and non-surgicalcases. This is due to cultural differences, person-al patient preferences, the orthodontist’s biasesand preferences, financial factors, and availabili-ty of surgical treatment. Having said this, themore we can objectively evaluate our cases, thebetter our decision making will be. The ArnettSTCA and CTP protocol allows us to do this. Inaddition, computerized access to these programsallows us to quickly evaluate cases as orthodon-tic and/or surgical. Also, options can be present-ed to the patient in a clear and concise manner,allowing them to participate more fully in theseimportant decisions.
DR. KEIM What do you mean by “double
JCO INTERVIEWS
202 JCO/APRIL 2004

assessment” of the difficult borderline surgicalcases?
DR. MCLAUGHLIN Group 1 cases are evalu-ated only for orthodontic treatment, as they donot present with skeletal disharmonies thatrequire a surgical assessment. Group 3 cases pre-sent with such severe skeletal disharmonies thatit is readily apparent that an acceptable resultcannot be achieved non-surgically. Therefore,these cases are evaluated for surgical-orthodontictreatment. Group 2 borderline cases, which canmake up a fairly large group in the orthodonticpractice, can benefit from a “double assessment”.That is, they can be evaluated for orthodontictreatment only and also for surgical-orthodontictreatment. In the past, this has been a tediousprocess, and has not been fully completed formost cases. However, the computerized STCAand CTP allow the clinician to do it quickly andaccurately.
DR. KEIM Do you handle a Group 2 borderlinecase that opts for non-surgical treatment differ-ently from a Group 1 non-surgical case?
DR. MCLAUGHLIN These patients are fre-quently our most difficult cases to manage ortho-dontically. It is often necessary to move teethlong distances, with added anchorage, periodon-tal, and instability concerns. Long-term retentionis often required. These factors should be care-fully explained to the patient, who may alterna-tively reconsider the surgical option.
DR. KEIM What is the role of the doctor’s sub-jective artistic and clinical judgment in such asystem?
DR. MCLAUGHLIN Clinical judgment comesinto play with each part of the clinical examina-tion: the TMJs, the face three-dimensionally, andthe condition of the dentition in its entirety. Thisjudgment is also critical in the analysis of all ofthe records, and is essential in treatment planningof all aspects of the case. Objective norms serveas points of reference to improve our clinicaljudgment. Also, the doctor’s subjective artistic
judgment can be coordinated with the patient’sconcerns to fine-tune and guide the case to a sat-isfactory completion. The two patients shown onthe following pages are examples of how weused facial and dental planning in borderlinecases—one Class II and one Class III.
DR. KEIM Rick, on behalf of our readers, I’dlike to thank you for this discussion.
ACKNOWLEDGMENTS: Dr. McLaughlin would like to thank Dr.John Bennett for his help in writing the book, as well as his com-pletion of the line drawings and coordination with the publishers.He would also like to thank Michaele Carnahan and Patty Knechtfor their assistance in his and Dr. Arnett’s office.
REFERENCES
1. Arnett, G.W. and McLaughlin, R.P.: Facial and Dental Planningfor Orthodontists and Oral Surgeons, Mosby, St. Louis, 2004.
2. Arnett, G.W. and Worley, C.M. Jr.: The treatment motivationsurvey: Defining patient motivation for treatment, Am. J.Orthod. 115:233-238, 1999.
3. Arnett, G.W.; Jelic, J.S.; Kim, J.; Cummings, D.R.; Beress, A.;Worley, C.M. Jr.; Chung, B.; and Bergman, R.: Soft tissuecephalometric analysis: Diagnosis and treatment planning ofdentofacial deformity, Am. J. Orthod. 116:239-253, 1999.
4. Lundstrom, F. and Lundstrom, A.: Clinical evaluation of maxil-lary and mandibular prognathism, Eur. J. Orthod. 11:408-413,1989.
5. Arnett, G.W. and Bergman, R.T.: Facial keys to orthodonticdiagnosis and treatment planning, Parts I and II, Am. J. Orthod.103:299-312, 395-411, 1993.
Richard P. McLaughlin, DDS
203VOLUME XXXVIII NUMBER 4
204 JCO/APRIL 2004
A B
A
A
C
D
Richard P. McLaughlin, DDS
205VOLUME XXXVIII NUMBER 4
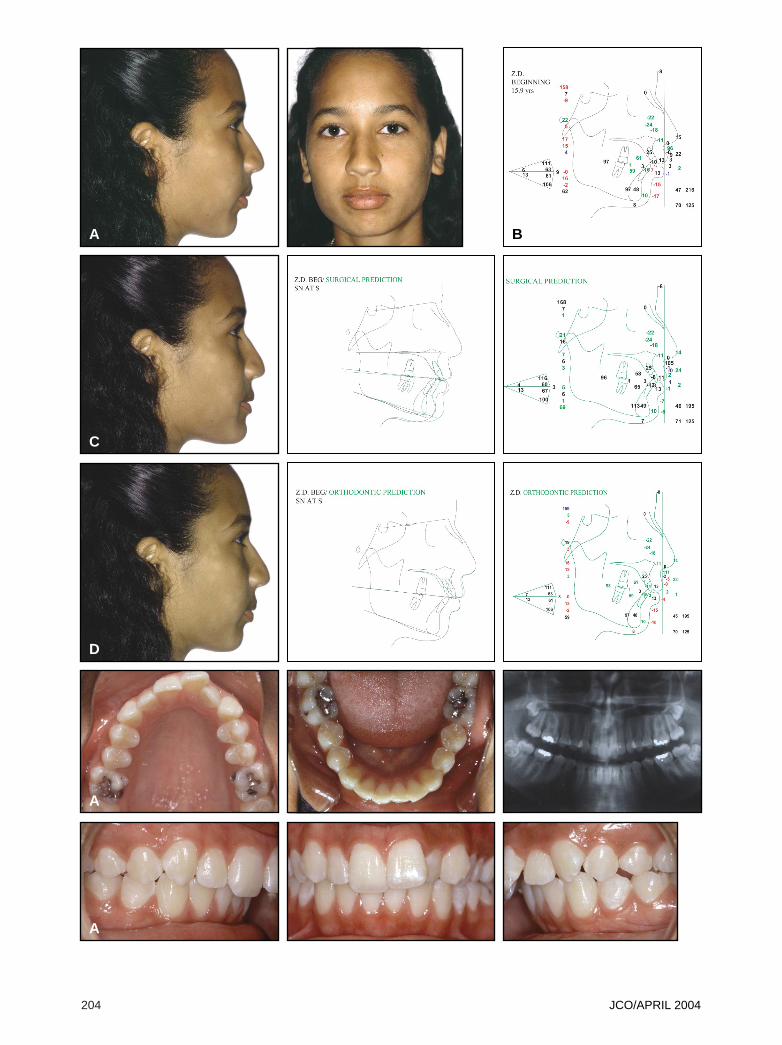
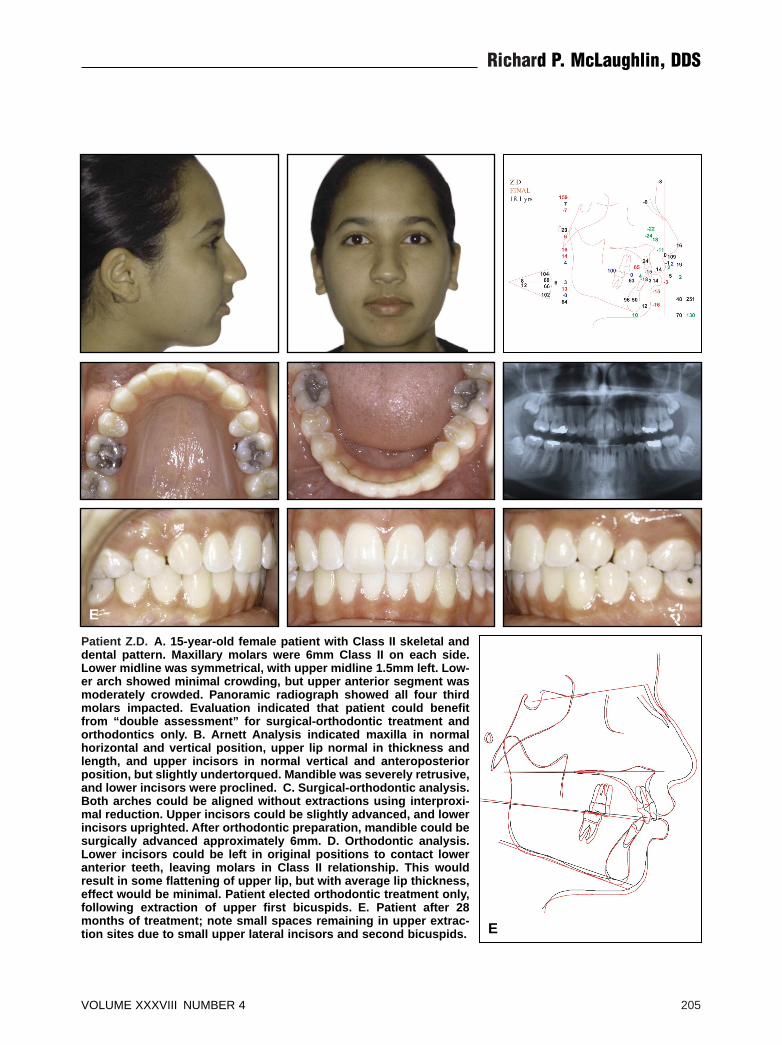
Patient Z.D. A. 15-year-old female patient with Class II skeletal anddental pattern. Maxillary molars were 6mm Class II on each side.Lower midline was symmetrical, with upper midline 1.5mm left. Low-er arch showed minimal crowding, but upper anterior segment wasmoderately crowded. Panoramic radiograph showed all four thirdmolars impacted. Evaluation indicated that patient could benefitfrom “double assessment” for surgical-orthodontic treatment andorthodontics only. B. Arnett Analysis indicated maxilla in normalhorizontal and vertical position, upper lip normal in thickness andlength, and upper incisors in normal vertical and anteroposteriorposition, but slightly undertorqued. Mandible was severely retrusive,and lower incisors were proclined. C. Surgical-orthodontic analysis.Both arches could be aligned without extractions using interproxi-mal reduction. Upper incisors could be slightly advanced, and lowerincisors uprighted. After orthodontic preparation, mandible could besurgically advanced approximately 6mm. D. Orthodontic analysis.Lower incisors could be left in original positions to contact loweranterior teeth, leaving molars in Class II relationship. This wouldresult in some flattening of upper lip, but with average lip thickness,effect would be minimal. Patient elected orthodontic treatment only,following extraction of upper first bicuspids. E. Patient after 28months of treatment; note small spaces remaining in upper extrac-tion sites due to small upper lateral incisors and second bicuspids.
E
E
206 JCO/APRIL 2004
A
A
A B
C
D

Richard P. McLaughlin, DDS
VOLUME XXXVIII NUMBER 4 207
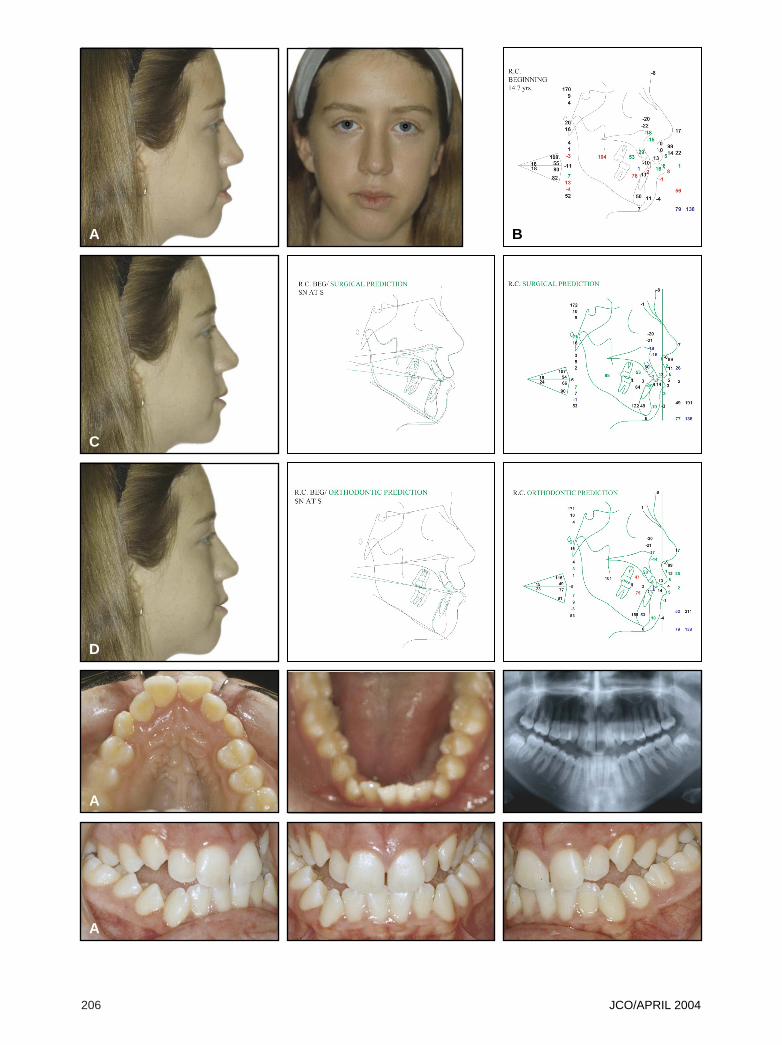
Patient R.C. A. 14-year-old female patient with Class III skeletal anddental pattern. Posterior segments were about 4mm Class III on eachside. Patient had narrow maxilla and bilateral crossbite. Lower ante-rior segment showed 7mm of crowding. Only lower third molarswere present. Evaluation indicated that patient could benefit from“double assessment” for surgical-orthodontic treatment and ortho-dontics only. B. Arnett Analysis indicated slight midface deficiencyand slight mandibular prominence. Maxillary occlusal plane wassteep, and lower incisors were extremely upright. C. Surgical-ortho-dontic analysis. Presurgical orthodontics would consist of rapidpalatal expansion, followed by arch alignment without extractions,along with advancement of lower incisors and some interproximalreduction in lower anterior segment. When patient’s growth wascomplete, two-jaw surgery would be performed with slight maxillaryadvancement, flattening of maxillary occlusal plane, and mandibularsetback. D. Orthodontic analysis. Maxillary arch would be expandedand upper incisors advanced, allowing alignment without extrac-tions. Mandibular crowding and lack of overbite created greatestchallenge. Nonextraction treatment would result in lower incisor ad-vancement and unacceptable overbite and overjet. Extraction oflower bicuspids was considered, but would create 14mm of space tooffset 7mm of crowding, limiting need for Class III elastics. Decisionwas made to extract second molars, allowing Class III elastics to beused to retract lower dentition and extrude lower incisors. E. Patientafter 38 months of treatment.
E
E
Related Documents











