January 2008 AADEP San Antonio Discography and the Evaluation of LBP Eugene J Carragee, MD Stanford University

January 2008 AADEP San Antonio Discography and the Evaluation of LBP Eugene J Carragee, MD Stanford University.
Dec 14, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

January 2008AADEP San Antonio
Discography and the Evaluation of LBP
Eugene J Carragee, MDStanford University

LBP Evaluation in Context
• Primary Diagnostic Evaluation (<50% ?)– LBP short duration (days - weeks)– Hx, PE, “rule out “red flags” of serious pathology
• Secondary Diagnostic Evaluation (<5%)– LBP not improving (weeks to1-2 months)– Add ESR, CRP, MRI, motion study X-Rays– Rule out “Yellow Flags”, psychosocial/neurophysiologic
factors that inhibit recovery OR coping.
• Teritiary Diagnostic Evaluation (<1%)– Persistent pain, considering specific rx (months to 1
year)– Only common degenerative findings on imaging so far– Consider discography to identify disc as “pain
generator”
Common MRI Findings and Pain
• DDD– Poor correlation with sx (Jensen, Boden)
• Anular Disruption and HIZ– Poor PPV or NPV (Jensen, Boden, Carragee, etc)
– Relative > in CLBP vs Asx (50% vs 15 -25%)
• Disc Protrusion and Stenosis– Extrusion (large) rarely seen in Asx (< 5%)– SS neural compression less common in Asx (15%)– Sx -> radicular; not a good LBP predictor
• Endplate Changes -- latest flavor
Common MRI Findings and Pain
• Modic I - II changes (mod - sev)– 10% Asx subjects (Weishaupt Rad 98)
– 100% PPV at disocgraphy in sx (Weishaupt Radiology 2000)
• Prediction of future LBP – Best but very modest correlation of future
LBP• Boos Spine (2000)• Carragee Spine J (2004)
– Much worse than:• DRAM, FABQ, Work Comp, Chronic Pain, Smoking
Imaging Findings
• If MRI, CT and Bone Scan are not specific for LBP illness
• Then, how do we finds the “pain generator”
But first - Defining a Clinically Relevant Pain
Generator • The “Pain Generator” in LBP illness
– as an isolated local pathoanatomic structure • Not a physiologic process or psychogenic
complaint
– independent of co-morbid factors • (chronic pain states, depression, somatic
distress, litigation, secondary gain, etc)
– Reasonable accounts for the chronic LBP illness of the patient
• When do “Positive” disc injections identify the true “pain generator”?
Discography GoalDiscography Goal
• To be a reliable, objective test that can identify a disc as the primary pathology in patients suffering from significant LBP illness.
• How reliably does discography “identify the pathological feature causing Low Back Pain Illness?” -- [specificity]
• Or “rule out” a disc as a significant pain source? -- [Sensitivity]

The Good Discogram of San Francisco
• 54 yo master chef.• 3 years severe LBP, radiates to gluteals only. • No medical problems (really!).
• Barely able to work.• VAS 7-9, Oswestry 45, Daily NSAIDS, occ narcs.• Psychometric: normal psychometrics, pain
drawing.• No WC, litigation, high prestige job, stable
marriage
• X-Ray, collapse and retrolisth L5/S1• MRI: nl L2/3, DDD L3/4, L4/5
The Good Discogram of San Francisco
• In this case…discography, may be key to treatment-->– Nl L2/3– Anular Disruption L3/4, L4/5
• No pain to 50 p.s.i., mild pain at 100.– L5/S1 not injected.
• ALIF L5/S1 -- 1998• Returned to work, 2 months p-op, full duty 4
months p-op. (regular 50# lift/carry)• 2 yr f/u VAS 0-2, Oswestry 5, occ NSAIDS• 5 yr f/u VAS 1-3, Oswestry 8, no meds• Some further DDD at L4/5 (now 59 yo)
Reliability of Pain Reporting in Discography
Note in this Case #1:1. No concurrent or history of other
chronic pain processes.2. No litigation, WC or secondary gain
issues.3. Normal psychometric, no “reactive
depression, anxiety, somatic distress…”
4. Ablation of the suspected “Pain Generator” give high-quality outcome which lasts.
Factors Affecting Reported Pain on Disc Injections
• Disc– Anular Disruption– Pressure Applied
• Local Pain Sensitivity– Regional chronic pain,
previous injury/surgery
• Generalized Pain Sensitivity– Narcotics, Central Pain
Syndromes, – Incentives (Financial, Social)– Disincentives (Financial
Social)
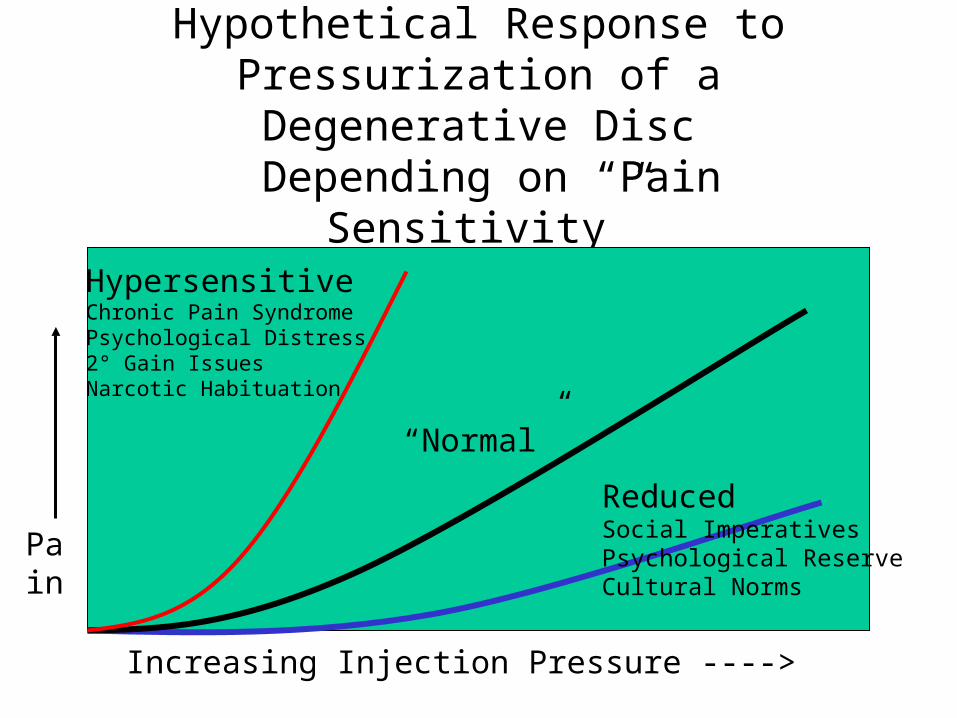
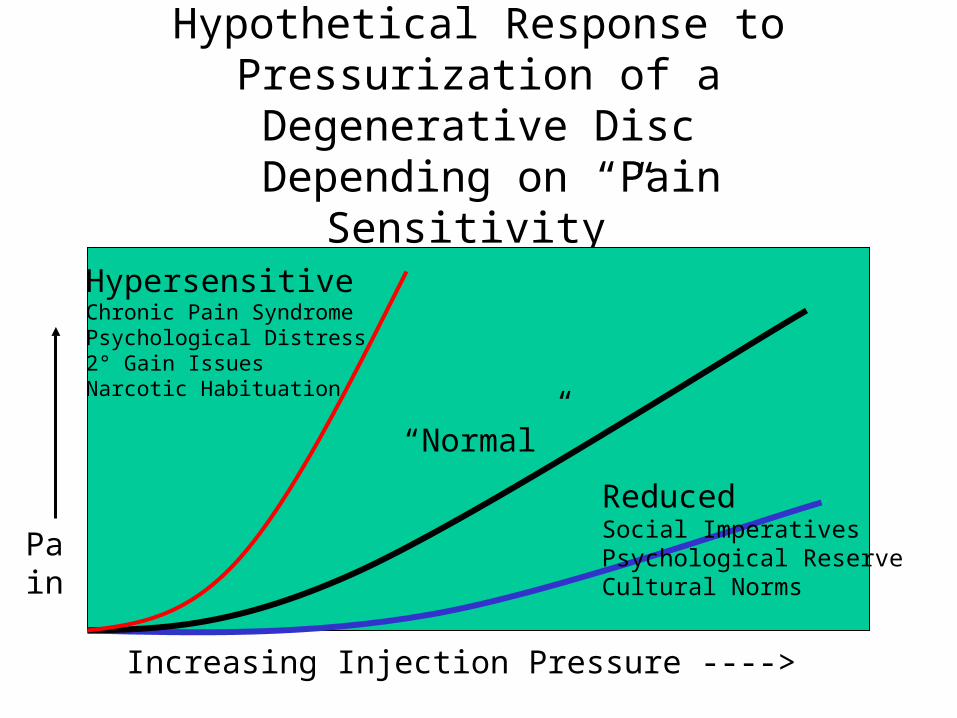
Hypothetical Response to Pressurization of a Degenerative
Disc Depending on “Pain Sensitivity”
“Normal”
Increasing Injection Pressure ---->
Pain
HypersensitiveChronic Pain SyndromePsychological Distress2° Gain IssuesNarcotic Habituation
ReducedSocial ImperativesPsychological ReserveCultural Norms
Evidence for Validity and Usefulness of Discography
• Sackett and Hayes (Br. Med J: 324) Evidence -base criteria for Evaluation of Diagnostic Tests
Four Phases - • 1. Dx test results in completely normals / no
sx / no co-morbidities.• 2. Dx test results in subjects w/o the disease
BUT w/ sx of disease • 3. Dx test applied in subjects w/o the disease
BUT epidemiologically likely to have disease (i.e. co-morbidies of the disease)
• 4. Does having the test result improve outcomes
• What is the evidence in discography?
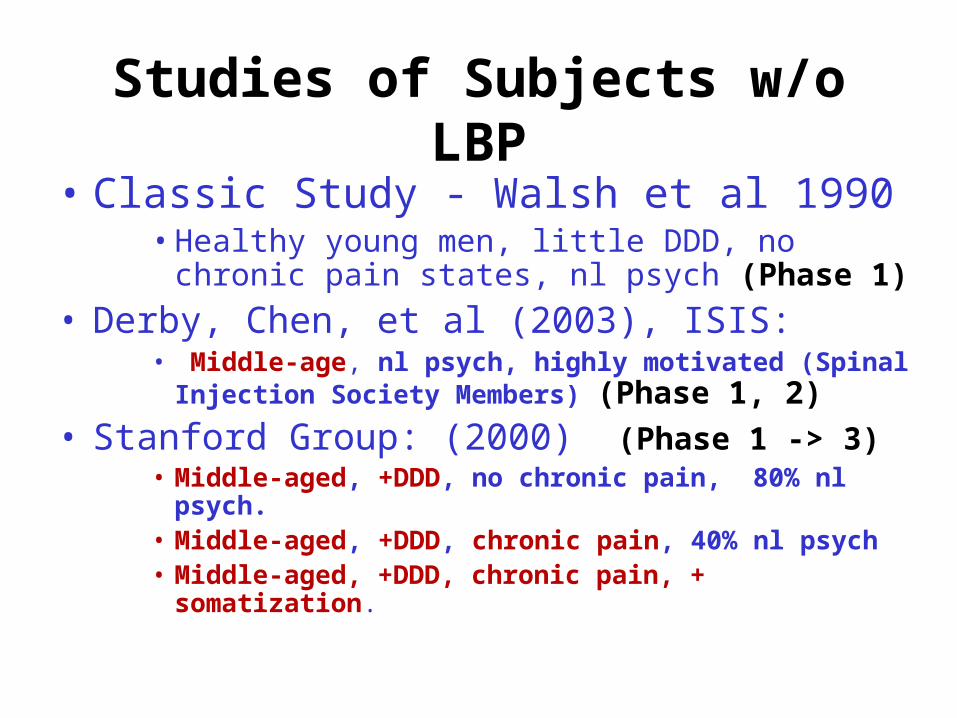
Studies of Subjects w/o LBP
• Classic Study - Walsh et al 1990 • Healthy young men, little DDD, no chronic
pain states, nl psych (Phase 1)
• Derby, Chen, et al (2003), ISIS:• Middle-age, nl psych, highly motivated (Spinal
Injection Society Members) (Phase 1, 2)• Stanford Group: (2000) (Phase 1 -> 3)
• Middle-aged, +DDD, no chronic pain, 80% nl psych.
• Middle-aged, +DDD, chronic pain, 40% nl psych• Middle-aged, +DDD, chronic pain, +
somatization.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
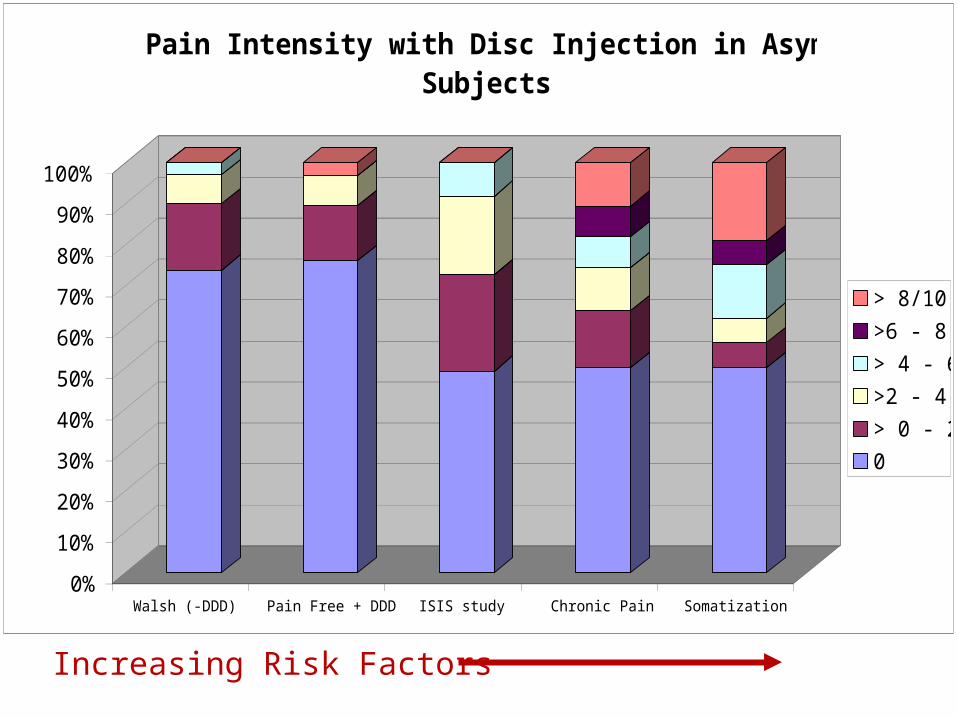
Walsh (-DDD) Pain Free + DDD ISIS study Chronic Pain Somatization
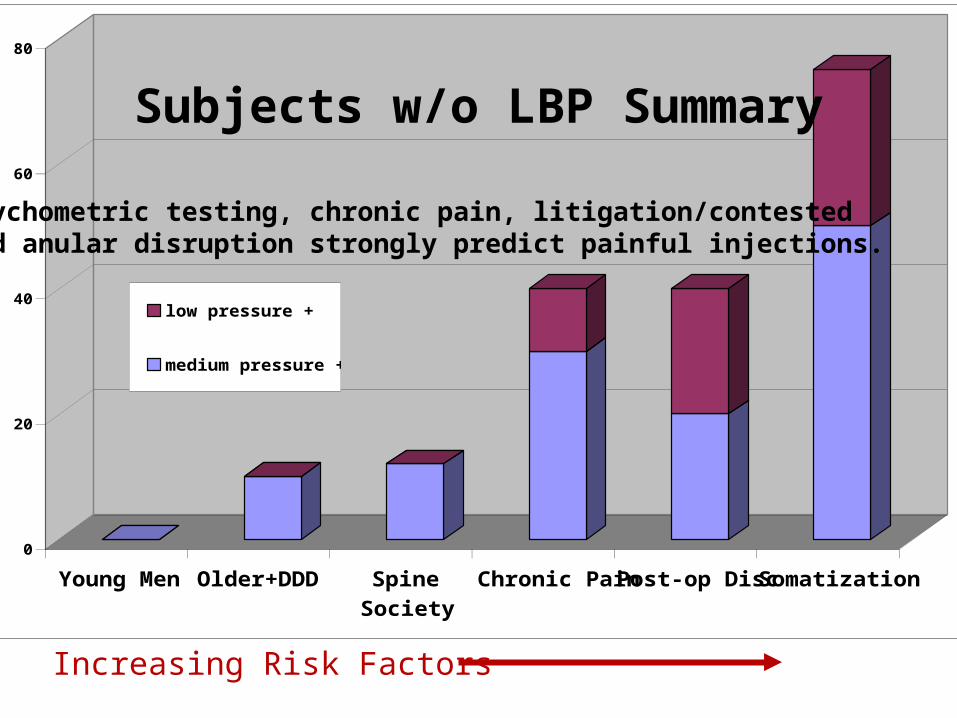
Pain Intensity with Disc Injection in Asymptomatic Subjects
> 8/10
>6 - 8
> 4 - 6
>2 - 4
> 0 - 2
0
Increasing Risk Factors
0
20
40
60
80
Young MenOlder+DDD SpineSociety
Chronic PainPost-op DiscSomatization
low pressure +
medium pressure +
Subjects w/o LBP Summary
Psychometric testing, chronic pain, litigation/contested and anular disruption strongly predict painful injections.
Increasing Risk Factors
Hypothetical Response to Pressurization of a Degenerative
Disc Depending on “Pain Sensitivity”
“Normal”
Increasing Injection Pressure ---->
Pain
HypersensitiveChronic Pain SyndromePsychological Distress2° Gain IssuesNarcotic Habituation
ReducedSocial ImperativesPsychological ReserveCultural Norms
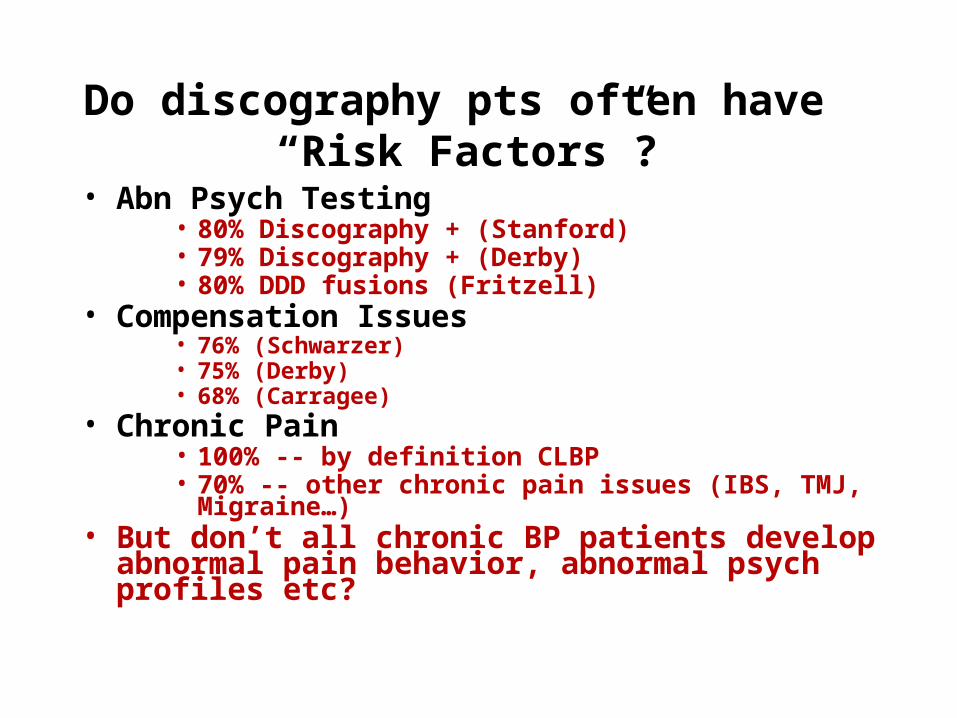
Do discography pts often have “Risk Factors”?
• Abn Psych Testing• 80% Discography + (Stanford)• 79% Discography + (Derby)• 80% DDD fusions (Fritzell)
• Compensation Issues• 76% (Schwarzer)• 75% (Derby)• 68% (Carragee)
• Chronic Pain• 100% -- by definition CLBP• 70% -- other chronic pain issues (IBS, TMJ,
Migraine…)• But don’t all chronic BP patients develop
abnormal pain behavior, abnormal psych profiles etc?
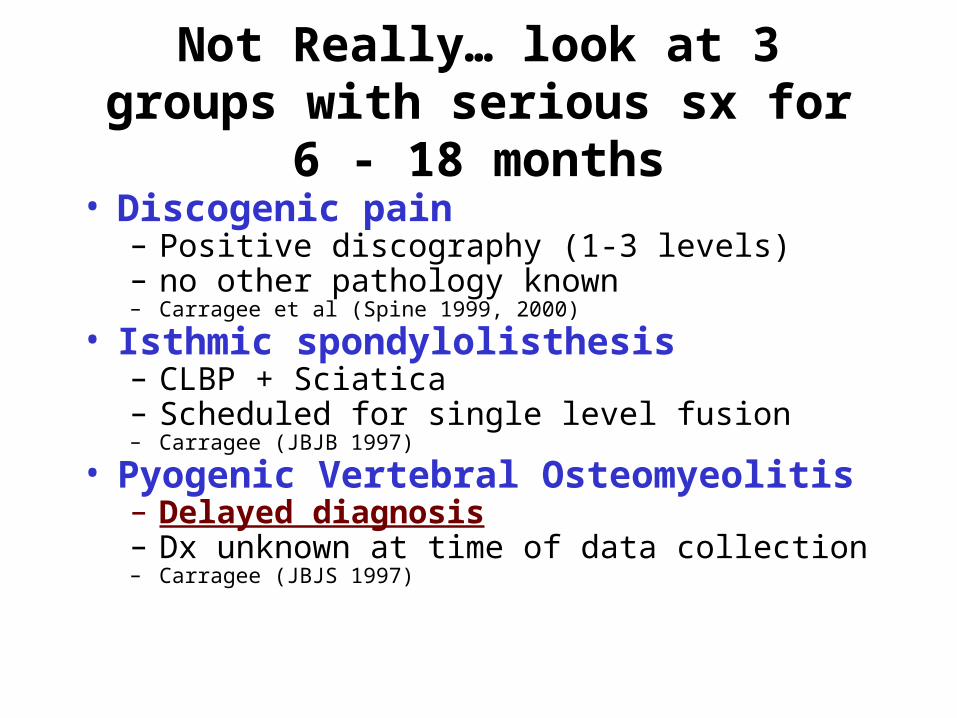
Not Really… look at 3 groups with serious sx for 6 - 18
months• Discogenic pain
– Positive discography (1-3 levels)– no other pathology known– Carragee et al (Spine 1999, 2000)
• Isthmic spondylolisthesis – CLBP + Sciatica– Scheduled for single level fusion– Carragee (JBJB 1997)
• Pyogenic Vertebral Osteomyeolitis– Delayed diagnosis– Dx unknown at time of data collection– Carragee (JBJS 1997)
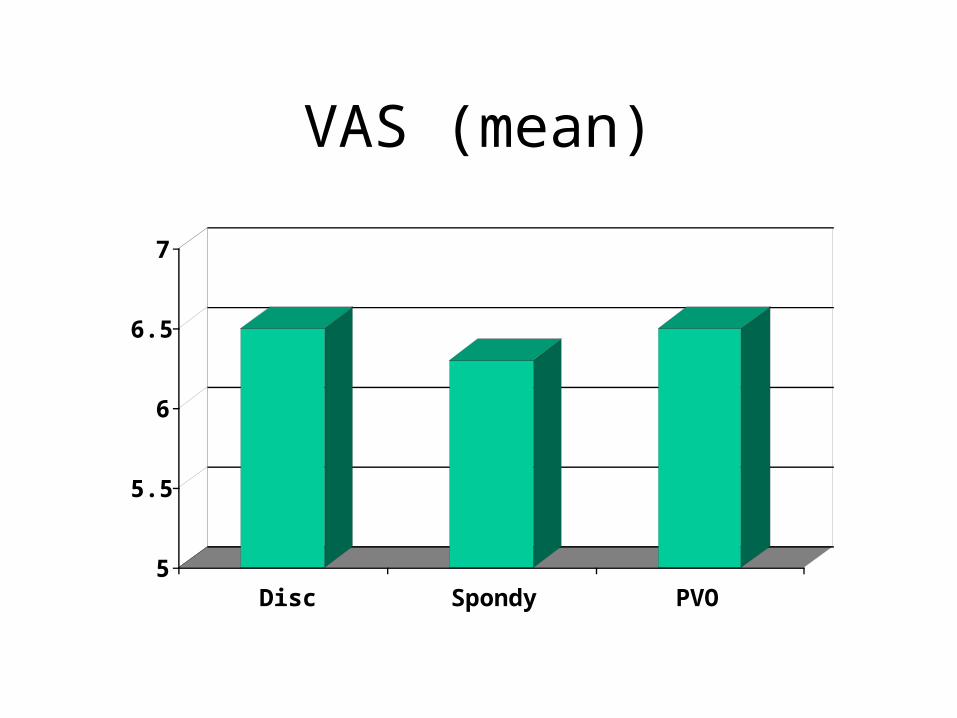
VAS (mean)
5
5.5
6
6.5
7
Disc Spondy PVO
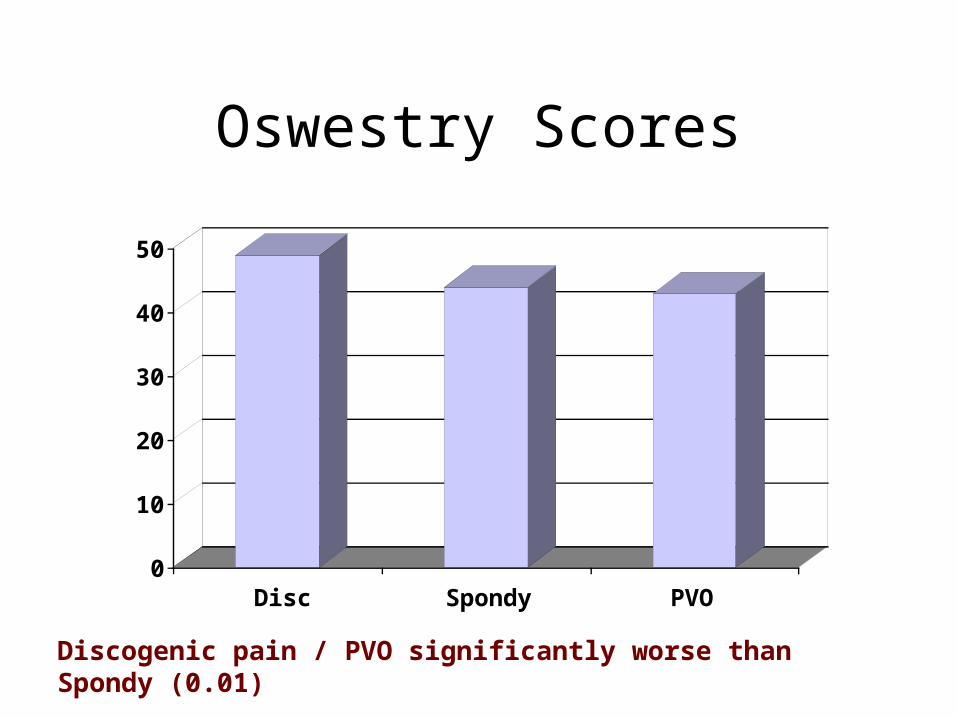
Oswestry Scores
0
10
20
30
40
50
Disc Spondy PVO
Discogenic pain / PVO significantly worse than Spondy (0.01)
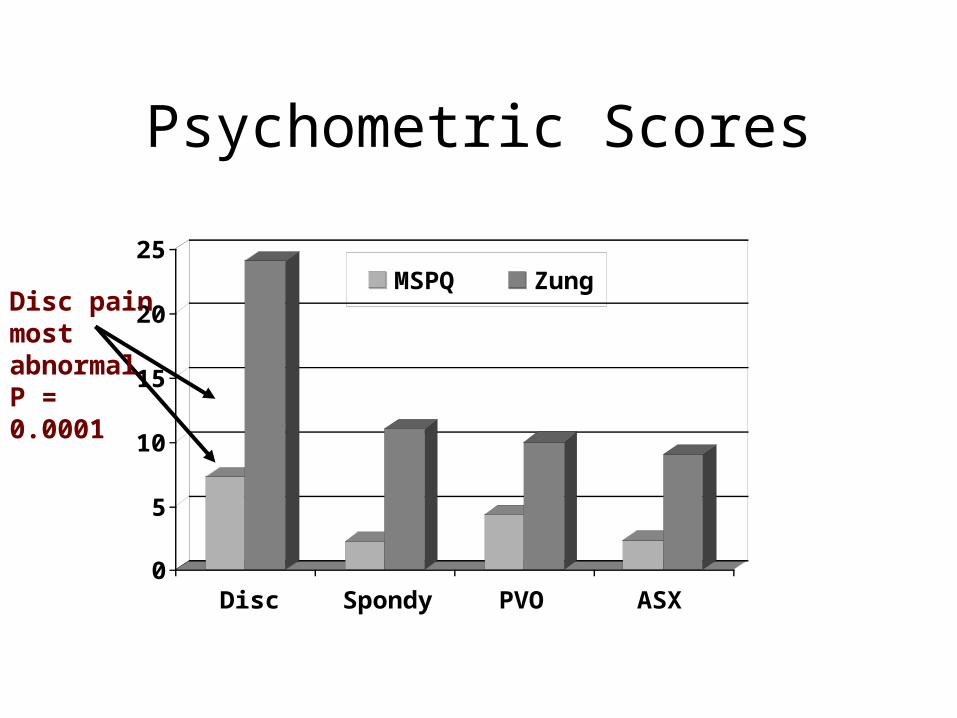
Psychometric Scores
0
5
10
15
20
25
Disc Spondy PVO ASX
MSPQ ZungDisc pain most abnormalP = 0.0001
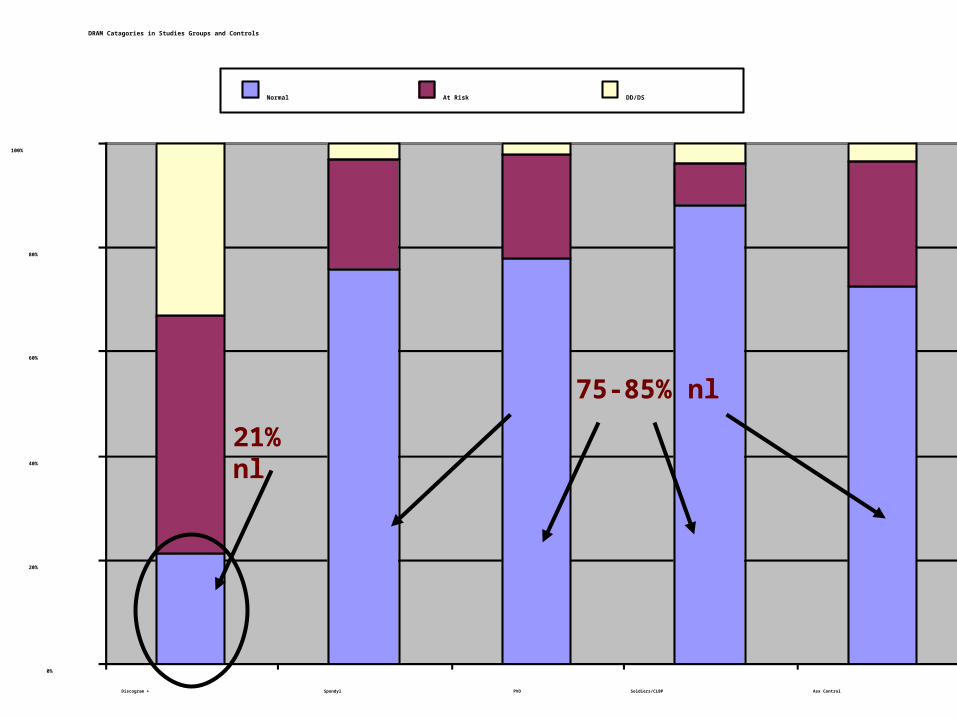
DRAM Catagories in Studies Groups and Controls
0%
20%
40%
60%
80%
100%
Discogram + Spondyl PVO Soldiers/CLBP Asx Control
Normal At Risk DD/DS
21% nl
75-85% nl
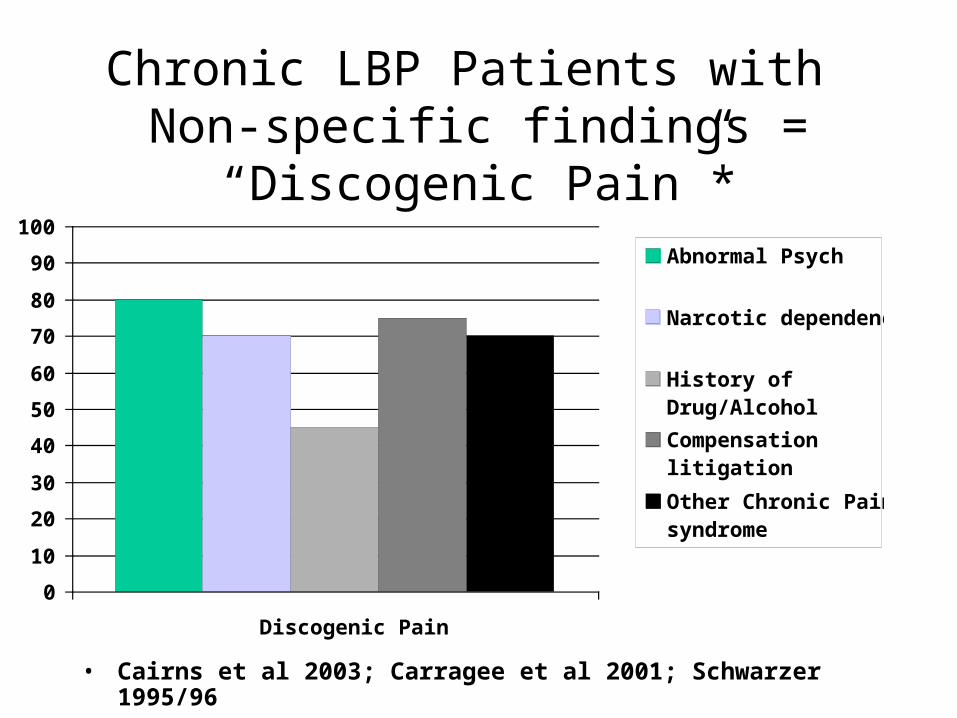
Chronic LBP Patients with Non-specific findings =
“Discogenic Pain”*
0
10
20
30
40
50
60
70
80
90
100
Discogenic Pain
Abnormal Psych
Narcotic dependency
History ofDrug/Alcohol
Compensationlitigation
Other Chronic Painsyndrome
• Cairns et al 2003; Carragee et al 2001; Schwarzer 1995/96
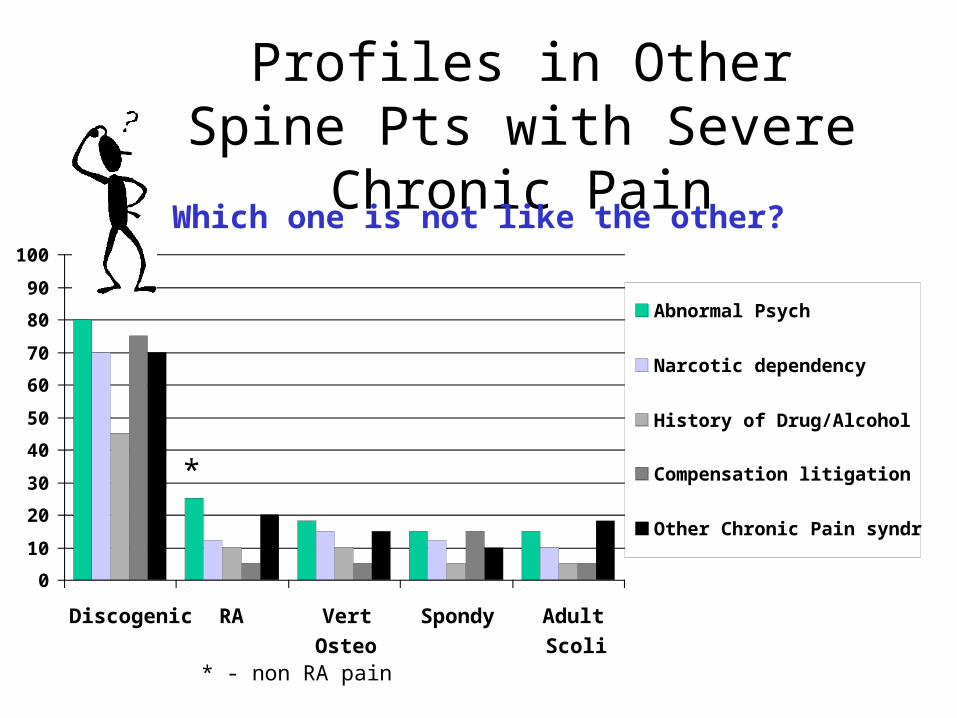
Profiles in Other Spine Pts with Severe Chronic Pain
0
10
20
30
40
50
60
70
80
90
100
Discogenic RA VertOsteo
Spondy AdultScoli
Abnormal Psych
Narcotic dependency
History of Drug/Alcohol
Compensation litigation
Other Chronic Pain syndrome
Which one is not like the other?
*
* - non RA pain
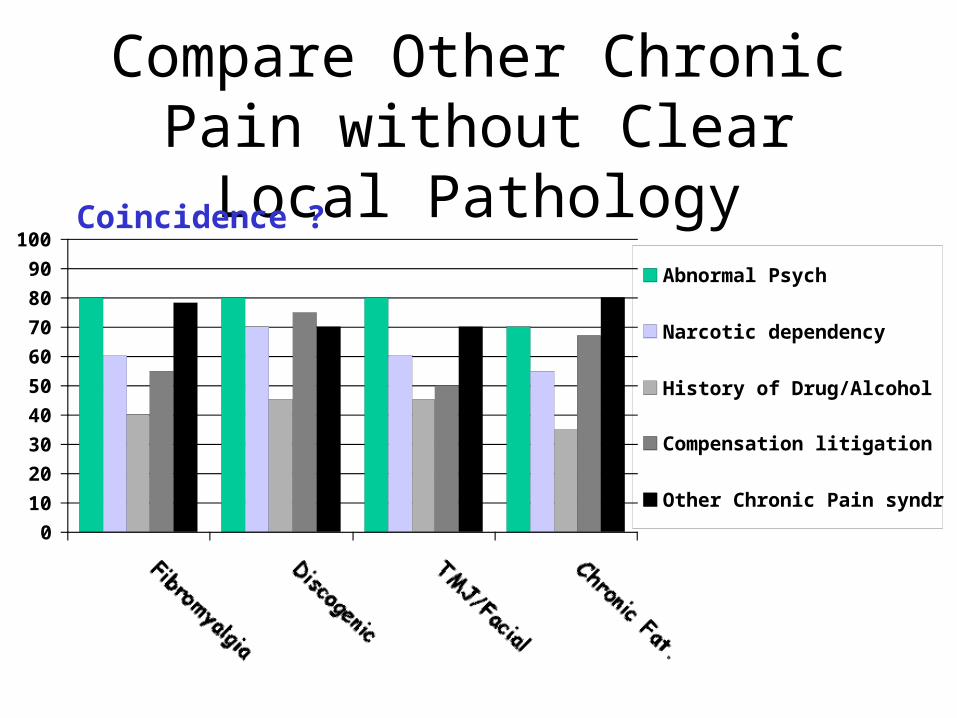
Compare Other Chronic Pain without Clear Local
Pathology
0
10
20
30
40
50
60
70
80
90
100
FibromyalgiaDiscogenic TMJ/Facial Chronic Fat.
Abnormal Psych
Narcotic dependency
History of Drug/Alcohol
Compensation litigation
Other Chronic Pain syndrome
Coincidence ?
How reliable is “Concordancy” Experimental LBP Model (Phase 3)
• Subjects scheduled for posterior ICBG – for non-lumbar problems (fracture non-union,
tumor)
• Screened for LBP before ICBG– No current of life-time hx of LBP– LBP hx screening 3 x before study
• All with normal psychometric testing• Discography done after ICGB
– pain concordancy rated at discography to ICBG pain
– Will disc stimulation pain reproduce ICBG pain
• Completing Study - 8 pts / 24 disc injections
» Carragee et al Spine 1999
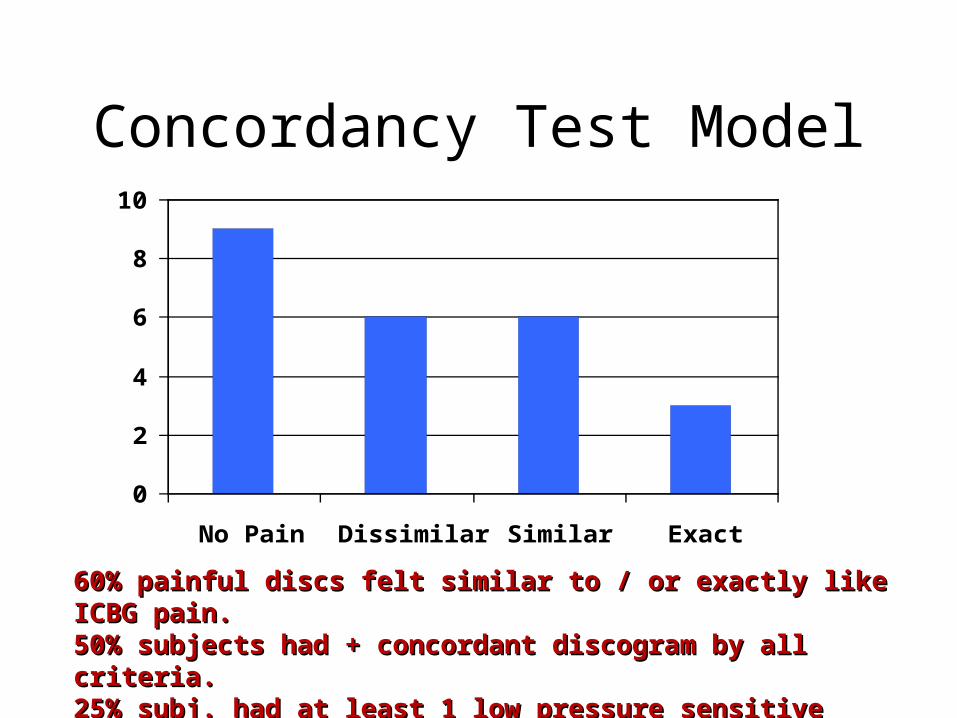
Concordancy Test Model
0
2
4
6
8
10
No Pain Dissimilar Similar Exact
60% painful discs felt similar to / or exactly like ICBG 60% painful discs felt similar to / or exactly like ICBG pain.pain.50% subjects had + concordant discogram by all 50% subjects had + concordant discogram by all criteria.criteria.25% subj. had at least 1 low pressure sensitive disc.25% subj. had at least 1 low pressure sensitive disc.
Schematic Approach to Back Pain
Perception and Discography

MuscularFacetBone
L3/4 Disc
L4/5 Disc
L5/S1 Disc
SimilarSclerotom
alAfferents
Perception
DRG
Cord
Thalamus
Cerebral
VisceralVascular
Pelvic
Concordancy and The LBP Pathway
Pathway Modulation1 Adjacent tissue injury2 Local AnaestheticLocal Anaesthetic3 Nearby tissue injury4 Regional Chronic Pain5 Narcotic AnalgesiaNarcotic Analgesia6 Narcotic Habituation7 Depression8 Social ImperitivesSocial Imperitives9 Social Disincentives
1
2
3
4
5 6
78 9
MuscularFacetBone
L3/4 Disc
L4/5 Disc
L5/S1 Disc
SimilarSclerotom
alAfferents
That’s my Pain!!!!
DRG
Cord
Thalamus
Cerebral
Visceral Pelvic
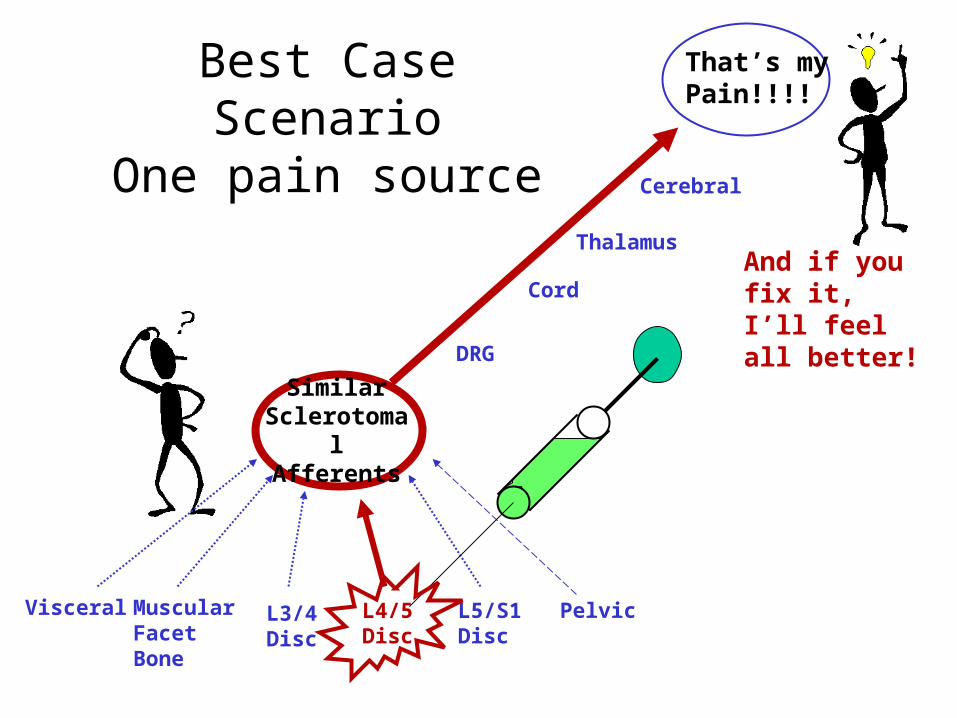
Best Case ScenarioOne pain source
And if you fix it, I’ll feel all better!
Muscular L3/4 Disc
L4/5 Disc
L5/S1 Disc
SimilarSclerotom
alAfferents
That’s my Pain! ! !
DRG
Cord
Thalamus
Cerebral
Visceral Pelvic
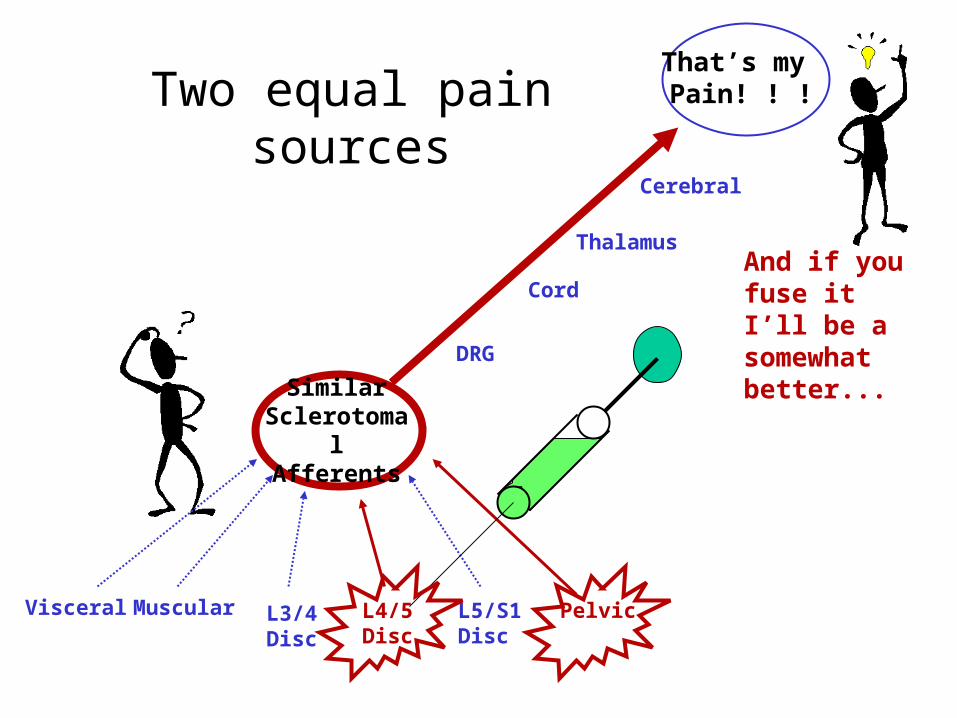
Two equal pain sources
And if you fuse it I’ll be a somewhat better...
FacetBoneMuscular
L3/4 Disc
L4/5 Disc
L5/S1 Disc
SimilarSclerotom
alAfferents
That’s my Pain!!!!
DRG
Cord
Thalamus
Cerebral
VisceralVascular
Pelvic
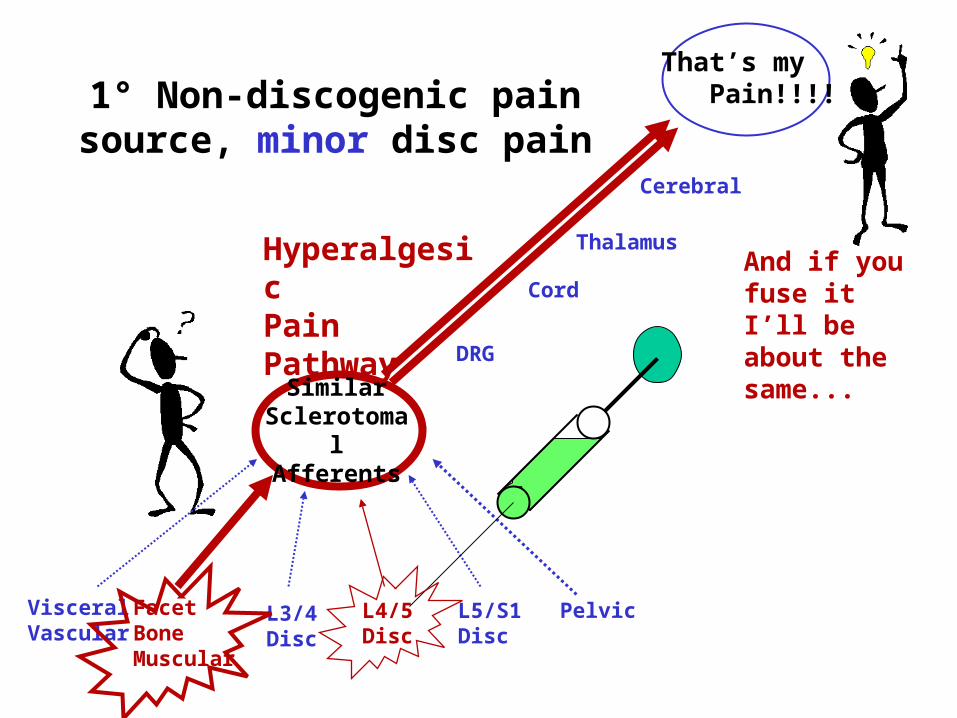
1° Non-discogenic pain source, minor disc pain
HyperalgesicPain Pathway
And if you fuse it I’ll be about the same...
Case 2• 35 yo man, severe LBP x 7 mo.• Unable to work x 3 month.
• VAS 9-10, Oswestry 50, • Psych “At risk”• Meds Daily Narcotics
• X-ray nl, MRI DDD + HIZ L5/S1• Discogram: 10/10 concordant pain
L5/S1• Nl L4/5, L3/4, but CT sclerosis L4 pedicle.
Case 2
• Bone Spec Scan, hot at L4• Excisional biopsy, “osteiod osteoma”• Fusion L3-4, unilateral pedicle screws.• RTW, 2 month post-op• 3 year f/u
– VAS 1-2, Oswestry 10, occ. NSAID– Stanford Score 8.8 (0-10)
• Why did the L5/S1 disc have a severe concordant pain with injection?

FacetBoneMuscular
L3/4 Disc
L4/5 Disc
L5/S1 Disc
SimilarSclerotom
alAfferents
That’s my Pain!!!!
DRG
Cord
Thalamus
Cerebral
VisceralVascular
Pelvic
Multiply Operated Back
HyperalgesicPain Pathway
DepressionSomatization
And if you fuse another level, I’ll be as miserable as ever...
FacetBoneMuscular
L3/4 Disc
L4/5 Disc
L5/S1 Disc
SimilarSclerotom
alAfferents
That’s my Pain!!!!
DRG
Cord
Thalamus
Cerebral
VisceralVascular
Pelvic
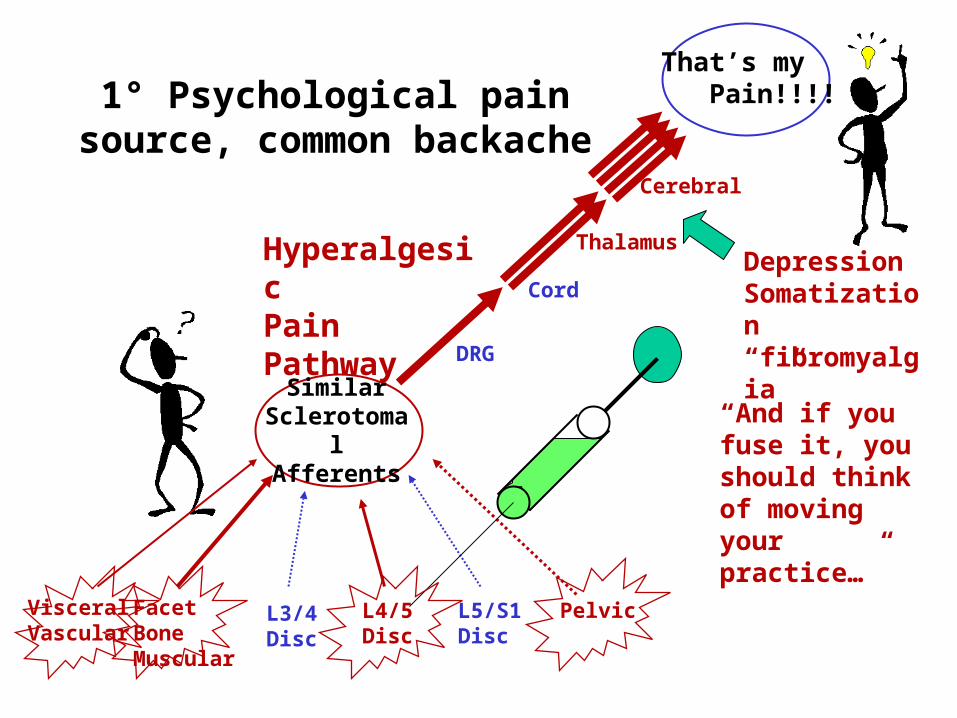
1° Psychological pain source, common backache
HyperalgesicPain Pathway
DepressionSomatization“fibromyalgia”
“And if you fuse it, you should think of moving your practice…”
Case 3
• 49 yo woman, severe LBP, no WC BUT...• Disabled for years, conserv. Rx makes worse.
Injections give transient relief.• Also CTS, migraines, pelvic pain, palpitations,
irritable bowel syndrome.• CTR, appy, chole (no help) in past• In ER 1 week PTA “unable to move legs”.• Sister says: “ She has a very high pain
threshold…”

Case 3• Work up shows collapsing weakness and DDD
in spine, MRI no tumor, infection, cord compression.
• Returns 6 weeks later with outside w/u:– Discography L4/5 and L5/S1 10/10 concordant and
fissured, low pressure.– L3/4 mild DDD 2/10 discordant pain– Psych interview feels emotiomal sx due to chronic
pain.
• A surgeon recommends fusion based on the “objective findings on discography…”
Case 3-- ”She’s Back”• Returns 2 years later had surgery• L4-S1 solid 360° fusion• Still terrible pain but feels surgery “helped” for
a few months…(would do it again).• Recent Discogram shows 10/10 L3/4 pain. • Negative L2/3 “control”• Another surgeon now recommends to fuse
L3/4 based on positive discogram.• How did we get into this mess...
Do people with common backache have painful disc
injections?• Phase 2 discography protocol...• 25 volunteers with persistent LBP
– > 2 year, OSW < 15– No work loss, No activity restriction– No meds, not seeking medical rx.– Nl psych– MRI Signal loss in at least 1 lumbar disc
• That is: People with “common backache.”– Carragee et al, The Spine Journal, 2002
Common Backache Study Protocol
• Full Walsh protocol for experimental discography.
• Question: – What kind of pain response?– Will it be concordant if present?– Can we differential using discography
CLBP patients from Common Backache?

Bachache and Discography
•36% “Backache group” had “bad” concordant pain•Most are low pressure sensitive discs•It is possible discography cannot tell common
clinically-irrelevent BP from CLBP illness.
0
10
20
30
40
50
60
70
Negative Positive 2 or more + discs
FacetBoneMuscular
L3/4 Disc
L4/5 Disc
L5/S1 Disc
SimilarSclerotom
alAfferents
That’s my Pain!!!!
DRG
Cord
Thalamus
Cerebral
VisceralVascular
Pelvic
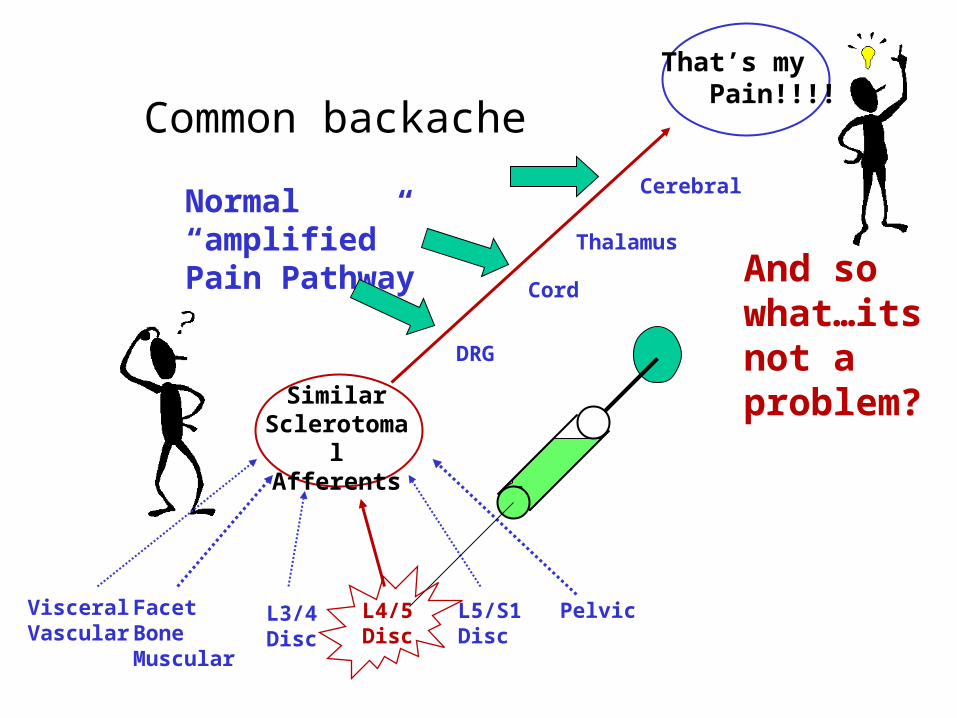
Common backache
Normal “amplified”Pain Pathway And so
what…its not a problem?

Or is it a problem…Case 4
• 48 yo man, long hx LBP, occ. treatment
• MVA 1997, pt claims “different LBP” since accident and totally disabled.
• Seen after work-up, referred for discography.
• MRI shows DDD, L4/5, L5/1• HIZ at L4/5
Working the system…Case 4
• Diffuse pain.• Bizarre pain drawing.• OSW = 62; VAS (mn) = 8; Daily Narc.• DRAM - Distressed Despressed• Pre-existing “Anxiety Disorder”• Will discography clear up this
picture?
Working the System• Seen 8 months later at request of his
attorney.• Discography done in community:
• L3/4 minor fissuring; 8/10 concord.• L4/5 and L5/S1 anular tear; 10/10 concord.• L2/3 “neg control disc”
• Report reads “3 level symptomatic anular tears …caused by recent accident since [injection] only reproduces new pain since accident…causation in legal action clearly determined by discographic findings”.
FacetBoneMuscular
L3/4 Disc
L4/5 Disc
L5/S1 Disc
SimilarSclerotom
alAfferents
That’s my Pain!!!!
DRG
Cord
Thalamus
Cerebral
VisceralVascular
Pelvic
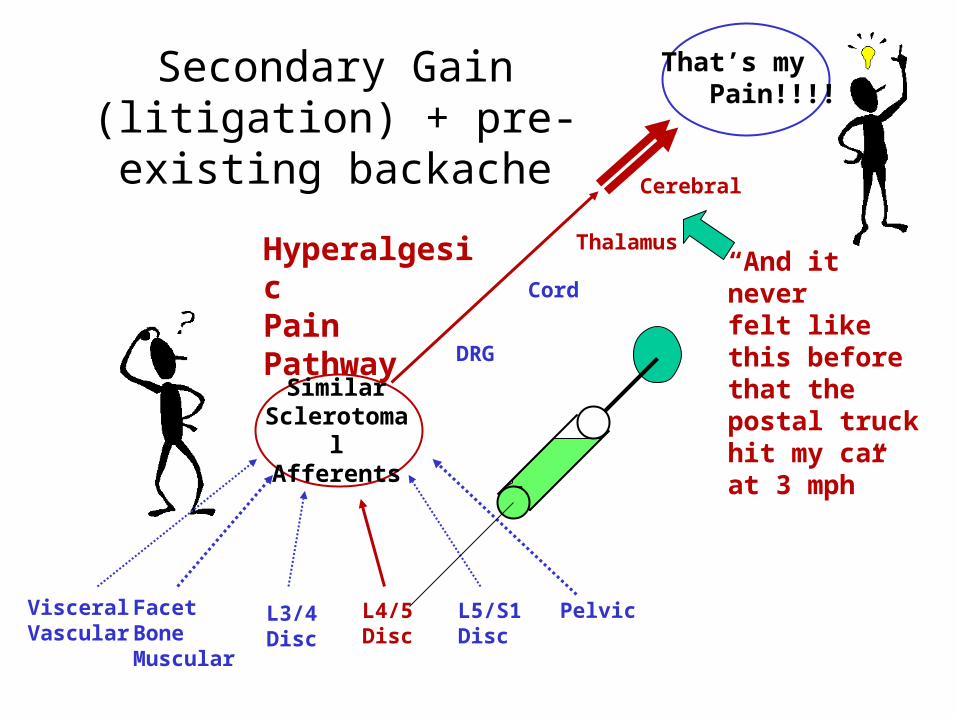
Secondary Gain (litigation) + pre-existing backache
HyperalgesicPain Pathway
“And it neverfelt like this before that the postal truck hit my car at 3 mph”
Acid TestDoes discography improve outcomes
• Mixed– Comparing fusion surgerys in different studies w/ and
w/o discography– No differences (Cohen, et al 2003)
• British retrospective study with very different patient groups (Calhoun) – Modestly improved outcomes in discography group.
• New York Group(2003 J Spinal Dis)– Prospective– Historical control– No difference in discography group: using discography
did not improve outcomes in this controlled study.
Outcome as Gold Standard
• Usually Outcome is considered poor diagnostic gold standard:– Failure related to patient selection– Failure related to operative morbidity
• Controlled “Pain Generator” Study– Single Level “Discography +” group versus– An ideal single segment “Pain Generator”
• Unstable spondylolisthesis (>4 mm / >11°)
– Do identical operation -- 360° fusion– No Comorbidites--
Outcome as Gold Standard
• Exclusions:– > 18 months of current episode– Not working prior to latest episode– Abnormal DRAM– More than 1 abnormal segment (adjacent
segments are NORMAL discogram)– No work comp / no litigation– No other chronic pain history
• No alibi’s! Best case scenario…
Hypothesis
• IF -- both groups are correctly diagnosing a single segment pain generator
• AND -- both have equal patient selections and surgical risks/morbidity
• THEN -- the surgical outcomes should be the same.
• IF NOT -- the difference will = false positive rate.
Subjects
• 30 “discography +” DDD– 5 years to recruit
• 32 unstable spondylolisthesis– Same time period
• No significant difference in baseline– VAS, ODI, work loss, smoking, DRAM,
FABQ, sx duration, medication use.
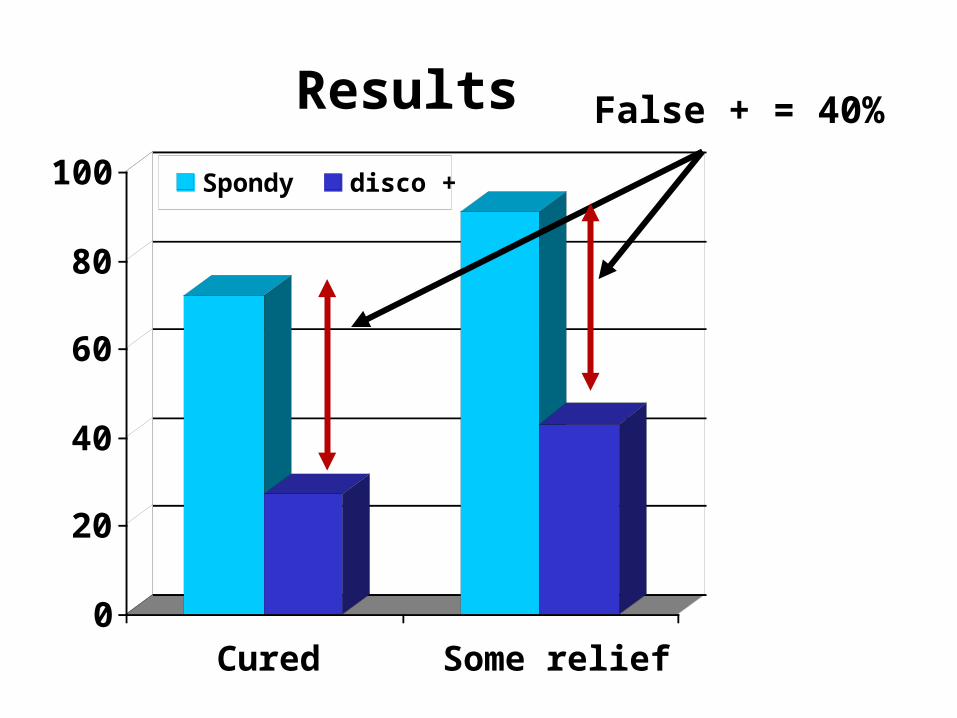
Results
0
20
40
60
80
100
Cured Some relief
Spondy disco +
False + = 40%
Summary
– Phase 1 studies were encouraging with low risk of false positive in completely normal subjects.
– Phase 2 and 3 studies show higher risk with increasing co-morbidities associated with CLBP illness (30 - 80%)
– Phase 4 studies are inconclusive or non-supportive for discography validity at this point.
– Still not answer to distinguishing severely painful from common DDD in spine…
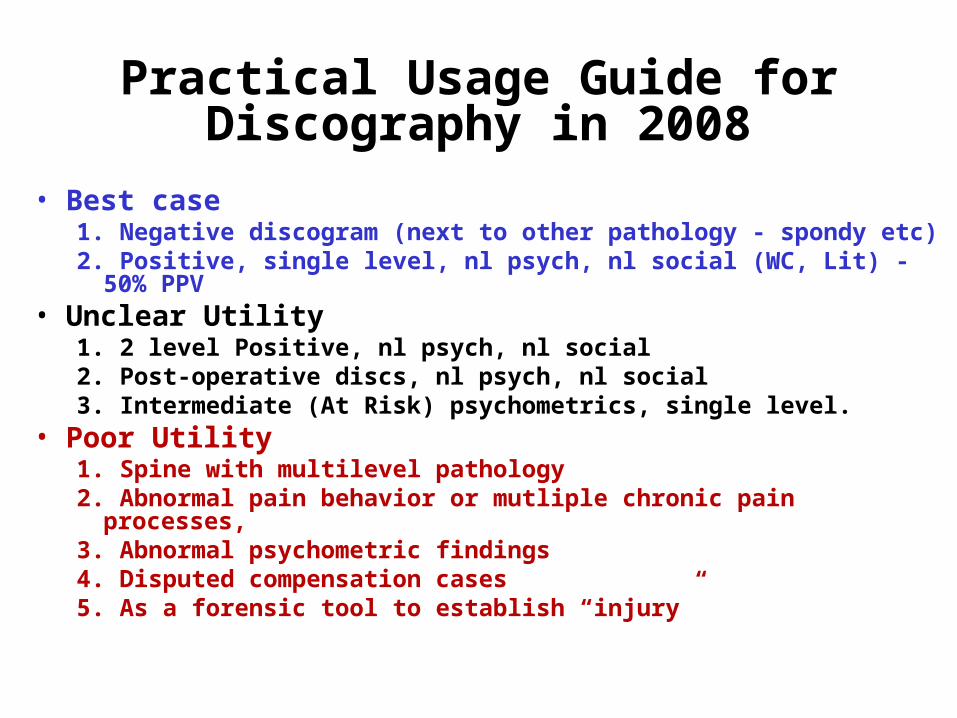
Practical Usage Guide for Discography in 2008
• Best case1. Negative discogram (next to other pathology - spondy etc)2. Positive, single level, nl psych, nl social (WC, Lit) - 50%
PPV• Unclear Utility
1. 2 level Positive, nl psych, nl social2. Post-operative discs, nl psych, nl social3. Intermediate (At Risk) psychometrics, single level.
• Poor Utility1. Spine with multilevel pathology2. Abnormal pain behavior or mutliple chronic pain
processes, 3. Abnormal psychometric findings4. Disputed compensation cases5. As a forensic tool to establish “injury”
Thank you
Related Documents











