African Programme for Onchocerciasis Control (APOC) Prograrnme africain de lutte corltre l'onchocercose JAF-FAC I JOINT ACTION FORUM Office of the Chairman JOINT ACTION FORUM Fourth session Accra. 9-11 December 1998 FORUM D'ACTION COMMUNE Bureau du Pr6sident JAF4/INF/DOC.5 ENGLISH ONLY October 1998 REPORT OF THE FIFTH WORKSHOP ON THE PHILOSOPHY OF APOC, THE CONCE,PT AND HARMONIZATION OF COMMUNITY-DIRECTED TREATMENT WITH IVERMECTIN (CDTI) NAIROBT, (KENYA),20-25 APRIL 1998

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

African Programme for Onchocerciasis Control (APOC)Prograrnme africain de lutte corltre l'onchocercose
JAF-FAC
I
)t
JOINT ACTION FORUMOffice of the Chairman
JOINT ACTION FORUMFourth session
Accra. 9-11 December 1998
FORUM D'ACTION COMMUNEBureau du Pr6sident
JAF4/INF/DOC.5ENGLISH ONLYOctober 1998
REPORT OF THE FIFTH WORKSHOP ON THE PHILOSOPHY OF APOC,THE CONCE,PT AND HARMONIZATION OF COMMUNITY-DIRECTED
TREATMENT WITH IVERMECTIN (CDTI)NAIROBT, (KENYA),20-25 APRIL 1998
I
t

AFRICAI.{ PROGRAMMEFOR
t
Liberiaa
o\ts
I q MAI 1998
.,: :, ,: ,,
(APOC)
Workshop on the PhilosoPhY of theAfrican Programme for Onchocerciasis Control (APOC)
Concept and Harmonization ofCommunity-Directed Treatment with Ivermectin (CDTI)
20-25,April 1998Nairobi, Kenya

TABLE OF CONTENTS
LTST OF ACRONYMS
ACKNOWLEDGEMENTS
1. EXECUTIVE SUMMARY
OPENING CEREMONY. .
TECHNICAL SESSION
WORKSHOP SESSIONS
4.1. Philosophy of APOC
4.2. REMO/GIS...
4.3. Administration/Budget /Financial Management
4.4. Communitv Participation and Sustainabilitv of CDTI
4.5. Training and Health Education
4.6. Ordering, Procurement and Delivery of Ivermectin
4.7, Recording/Reporting & Feedback at all levels
4.8. Integration of CDTI into Health Services
4.9. National Plan and Project Proposal
4.10. Other Matters.
4.11. Conclusions and Recommendations
5) APPENDICES
Page
lv
1
)
)
4
4
5
6
7
9
10
12
t4
15
16
16
t7
1
3.
4.
I

APOC
LIST OF ACRONIYMS
African Programme for Onchocerciasis Control
Community - Directed Distributor
Community - Directed Treatment with Ivermectin
Continuing Professional Development
District Health Department
Expanded Programme on fmmunization
Food and Agriculture Organization
Geographical Information System
Health For All
Health Net International
Jomo Kenyatta International Airport
Mectizan Donation Programme
Mozambique Company for Exporting and Importing Drugs
Ministry of Health
Mombassa
Medical Supplies Coordinating Unit
National Drug Service
Non-Governmental Development Organization
National Onchocerciasis Task Force
Onchocerciasis Control Programme
Operation Life Line Sudan / Southern Sector
Rapid Epidemiological Assessment
Rapid Epidemiological Mapping for Onchocerciasis
CDD
CDTIt
CPD
DHD
EPI
FAO
GIS
HFA
HNI
JKIA
IVIDP
MEDIMOC
MOH
MSA
MSCU
NDS
NGDO
NOTF
OCP
OLS/SS
REA
REMO

TB
UN
RHB
RMS
SRRA
TCC
TDR
UNDP
TiNICEF
WHA
wHo
ZHI)
Regional IIeaIth Board
Regional Medical Stores
Sudan Relief and Rehabilitation Association
Tuberculosis
Technical Consultative Committee
Tropical Diseases Research
United Nations
United Nations Development Programme
United Nations Children's Fund
World Health Assembly
\1 orld Health Organization
Zonal Health Department
ill

ACKNOWLEDGEMENTS
We the participants from Ethiopa, Kenya, Liberia" Mozambique and Southern Sudan wishto express our sincere thanks and appreciation to the Government and people of theRepublic of Kenya for the hospitality accorded us during our stay in Nairobi.
We also highly appreciate the full participation and contributions made by representativesof the World Banh Mectizan Donation Programme, NGDOs and others. Wewholeheartedly commend the APOC management for the patience, guidance andexpertise exhibited during this workshop.
Last but not least, our sincere thanks goes to the Facilitators and Rapporteurs, whostayed behind and wrote a comprehensive report of the workshop. We will alwaysremember the week of sleepless nights they spent in Nairobi. No degree of gratirude but,the successful control or elimination of Onchocerciasis will be the appropriate reward.
lv
I
woRKSHoPoNTHEPHILOSOPHYoFTIIEAFRICANPR0GRAMMEFoRONCHOCERCIASISCONTROL(APOC)'
CONCEPT AND HARMONIZATION OF COMMUNITY-DIRECTEDTRBATMENT WITH IVERMECTIN (CDTI)
APRIL 20-25,1998Nairobi, KenYa
1. EXECUTIVE SUMMARY
Ethiopia, Kenya, Liberia, Mozambique, and Southern Sudan and are among the 19 countries
to be covered by the African Programme for onchocerciasis control (APOC)' This workshop
was organized to provide a forum through which onchocerciasis control programme issues
which face each country could be discussed. The issues addressed were :
l.l The concept of partnership within the NOTF and APoc for each participating
country in the implementation of CDTI
1.2 The execution and validation of REMo/REA to identify endemic communities
requiring treatment
1.3 Programme budgeting and establishment of an efficient flow of funds from all partners
for effective use in the treatment of endemic communities and ensuring proper
accounting st-stems for funds reieased at all levels'
1.4 Designing training and health education material and activities to properly train health
workers and mobilize the communities to participate actively and take ownership of
the control of Onchocerciasis
1.5 Approaching the community on the establishment and ownership of CDTI including
ways of ens[ring sustainabiiity of the programme after external funding ceases'
1.6 Procurement, delivery and distribution of ivermectin in an integrated and efficient
rumner to all eligible persons in endemic communities. Also ways of ensuring proper
management,ruf.tyandstorageofivermectinatalllevels'
1.7 How to record, report and monitor treated communities to ensure proper
imPlementation of CDTI'
l.SHowtointegrateCDTIintoexistinghealthsystemsaswellasin-countryandcomm*ity irog.*s that have piou"n successful, without jeopardizing the
technical aspects of the various progralnmes'
1.9 What requirements and steps need to be taken to develop National Action Plans and
qualitY APOC Project ProPosals'
1 . 10 Possible means of in-country and inter-country communication on APOC related
activities which will keep all participating countries abreast of innovative and
stimulating info rmat io n'
The working sessions were in the form of formal presentations by lead speakers, followed by
working groups (country specffic or mixed) and generaldiscussions at plenary. At the end ofdiscussions conclusions and recommendations were made.
2. OPENING CEREMONY
Dr. D.K. S*g, Kenya National Onchocerciasis Coordinator, welcomed participants and
thanked APOC for choosing Kenya as host for the workshop. He asked participants to feel at
home and enjoy the warm hospitality of Kenya.
Professor M. Homeida, APOC/TCC, spoke of the need for country teams to appreciate the
availability of free ivermectin for as long as is required. He stressed an awakening of all
members to strong partnerships in onchocerciasis control with emphasis on the importance ofsustainability and integrating CDTI into existing community structures.
In his opening remarks, the WHO Representative in Kenya, Dr. Paul Chuke represented by the
WHO Advisor on Disease Prevention and Control, Dr. D.M. Mutie stressed the need for
community involvement, participation and ownership of health prograrnmes. He emphasised
the need for "Continuing Professional Development" (CPD) of health workers to keep abreast
of current development in their field.
The Keny'a Minister of Healttr- Hon. Jackson Kalweo. represented by Dr. Ivlaina Kahindo
(Depury Director, Medical Serv-ices) w'ho officially opened the workshop and pointed out his
desire for the participants to avail themselves of the knowledge they could acquire from the
workshop (Appendix A).
3. TECHNTCAL SESSION
3.1 Workshop Agenda
A provisional workshop agenda which was presented to the facilitators and
participants was discussed, amended and adopted for the workshop. (Appendix B)
3.2 Participants and Facilitators
Participants for the workshop were drawn from Ministries of Healtll research
institutions, universities, LIN Agencies and NGDOs working on onchocerciasis in
Ethiopia, Keny4 Liberia, Mozambique, and Southern Sudan. Facilitators for the
workshop were from APOC/WHO and NGDOs (Appendix C).
3.3 Workshop Design
The workshop was in the form of initial presentations on the various topics in plenary
fotlowed by discussions. Country-specific working groups met to discuss issues raised
pertaining to their own situations. There were mixed groups to facilitate cross-
fertilization of ideas and sharing of experiences. This format was adopted in order to
create an atmosphere of open exchange of ideas and experiences with active
I
2
involvement of the participants who were mostly field officers. Issues were raised
regarding their field experiences and solutions proferred.
Dr. Uche AmaTigo, APOC, presented the objectives and eupected outcome as follows:
3.4 Workshop Objectives
3.4.1. To agree on the modalities for establishing CDTI projects and promoting community
ownership o f ivermectin distribution fo r sustainability.
3.4.2. To discuss the development of National Plans and CDTI Project Proposals for
submission to APOC.
3.4.3. To reach a common understanding on how to establish sustainable CDTI projects
integrated into the existing health care systems of each country represented.
3.4.4. To streamline procedures for financial and administrative nunagement of CDTIprojects in the spirit of APOC partnership.
3.4.5. To determine ways to avoid duplication of resources and minimize costs at all levels ofproject implementation by the National Onchocerciasis Task Forces (NOTFs).
3.4.6. To dialogue and harmonise the process of training communiry selected distributors.
3 .4.7 . To re-orient existing and new ivermectin delivery projects to the new strategy of full
community participation in and ownership of projects, as a stakeholder.
3.5 Expected Outcomes
3.5.1. Participants would have a clear understanding of the philosophy of APOC and the
steps for implementing CDTI.
3.5.2. Country teams would make recommendations on ways to integrate CDTI into existing
health systems for sustainability, procure and deliver ivermectin to the communities,
and determine how funds will flow from central to district levels.
3.5.3. Partnership spirit among key actors would be strengthened.
3.5.4. National Plans and feasible CDTI Project Proposals would be developed by country
representatives fo llo wing the wo rkshop.
3.5.5. Participants would understand the roles and responsibilities of the community, health
services, NGDOs, external donors and other partners of APOC .
3

4. woRKSHOP SESSIONS
The tbllowing topics were addressed during the workshop sesslons
4.1 Philosophy of APOC/Concept of CDTIOverview of Onchocerciasis (special session)
REMO/GISAd.ministratio n/ Bud getff inanc ial Management o f APOC Projects
Community Participation and Sustainability of CDTI
Training and Health Education
Ordering/Pro curement and Delivery o f Ivermectin
Recording/Reporting and Feedback at all levels
Integration of CDTI in the Health Services
National Ptans and Project Proposals
Other MattersCo nclusions/Reco mmendation o f the Workshop
4.2.4.3.4.4.4.5.4.6.4.7.4.8.4.9.4.1 0.
4.1 l.
The higtrlights and discussions of these topics are presented in the following secttons:
4.1 Philosophy of APOC/Concept of CDTI
Dr. D. Etya'ale, NGDO International Coalition Coordinator, WHO/Geneva and Dr. Uche
Amazigo. Scientist. APOC presented papers on the philosophy of APOC in which the
following issues were higtrlighted:
4.1.1 . ApOC is a multiple partnership involving participating goverrlments and theil
affected communities, NGDos, World Bank, wHo, LINDP and FAo;
4.1.2. In all ApOC assisted countries, the partnership is operationalised through the
National Onchocercerciasis Task Force (NOTF) in which governments and their
partnersQ..iGDosandotheragencies)areallrepresented;
4.1.3. In keeping with the APOC philosophy of partnership, emphasis should be placed
on NOTF rather than on individualplayers. Consequently, the NOTF should be
the focal point of all APOC assisted onchocerciasis control activities;
4.1.4. AII partners should ensure that any success achieved will be through and with the
NOTF.
4.1.5. CDTI is a new approach for the delivery of ivermectin to eligible persons and
empowers ufe"tea communities/villages to design and implement the distribution
o f ivermectin (Mectizan@)'
4.1.6. The CDTI approach confers project ownership to the communities and to the
health service as equal stakeholders'
4.1.7. To maintain a successful partnership, efforts should be made to improve
coordination and dialogue'
4.1 .g. The NOTF should ensure a minimum coverage of 650/o in treated communities to
achieve elimination of onchocerciasis as a public health problem.
4

A special session on the overview of onchocerciasis requested by the participants waspresented by Professor C. D. McKenzie of Michigan Srare University,Lsa. in trispresentation the following were highlighted:o Parasite and its biologyo Clinical presentation of the disease. Important characteristics of the disease that relate to treatmento The need to provide correct information on the disease and the treatment
c It was recommended that this component should be incorporated into future A1OCworkshops in counny.
4.2. Rapid Epidemiologicar Mapping of onchocerciasis (REMO) andGeographical Information System (GIS)
Dr' H' Edeghere of APOC gave a presentation on the status of REMO/GIS in the planning,design and implementation of REMo. The following issues were discussed:
4'2'l' REMO is e:tremely important to APOC & NOTF for determining endemicitylevels and planning control activities in participating countries. triaadition.REMO is a prerequisite for consideration by APOC/TCC of national plans andproject proposals. APOC management anticipates that each country should haveits REMO completed by the fonowin.s tentative dates:
4.2.1.1. Ethiopia4.2.1.2. Kenya4.2.1.3. Liberia4.2.1.4. Mozambique4.2.1.5. Southern Sudan
December, 1998November, 1998June,1998?July, 1998Will conduct REA through December 199g
4'2'2' Data from each of the REMO exercises must be cross-validated independently,using internal or external validators.
4'2'3' There is a great need for training of trainers for REMO/GIS and therefore allparticipating countries need to discuss with APOC nrurnagement the mostappropriate dates for this to be undertaken in their countries.
4'2'4' APOC numagement will ensure that all activities related to the above are wellsupported. In particular, adequate support will be provided for the transfer ofcapacity and resources to assist the countries in generating essential data andmaps and ensure that they are readily available to all partners.
4-2.5. REMO activities were officialry handed over by wHo/TDR to Apoc inSeptember 1997.lt is therefore recommended that all requests related to REMoare forwarded to ApOC management.
4'2'6' In dfficult situations (civil unrest and wars) it is recommended that un-validatedREMO results could be used for start of treatment. Where REMO is found to bestrategically unacceptable, comprehensive REA results could be used as analternative.
5

4.2.1 In areas of insecurity where people have not stayed for more than 3 years,
women may be included in the sampling for REA in the absence of the required
number of males if they meet the requirements.
4.2.8 All countries should ensure that high risk groups in inaccessible areas are notdropped because of the inconvenience to the REMO team rather, more effortsshould be made to access such areas.
4.2.9. Countries should try to get multiple atlases to update maps for REMO.
4.2.l0.Information on endemic villages to be sampled for REMO, should be donejointly by all three members of the team (Geographer, Epidemiologist, and
Entomologist).
4.2.11. REMO/REA is a continuous exercise which should be refined and updated fromtime to time.
A special REMO session was conducted by Dr. H. Edeghere at the request of the participants
to clarify the following rssaes.'
. Step-by-step REMO/REA methodologtc Training needs
. GISo Internal and external validation of REMO/REA resultsc Technical expertise from external sources by APOC
4.3. Administration /Budget/Financial Management of APOC Project
The two presentations on guidelines for preparation of the budget for APOC funded
CDTI projects by Professor M. Homeida, and APOC Financial and Administrative
rumagement presented by Mr. Y.M. Aholou, APOC Administrator, highlighted the
following:
4.3.1. Prerequisites for good projects that will be in line with the budget guidelines
include the following:
4.3.1 . I . well defined activities and requirements for carrying these out
effectively4.3.1.2. population to be treated4.3.1.3. distances to be covered4.3.1.4. strategy to be used for administering treatment
4.3.2. Justification of the budget must be detailed for each line item
4.3.3. Costs not covered bY APOC:4.3.3.1. Basic salaries, office space, transport of drugs from port of entry to
health centre.
4.3.4. Costs that may be covered by APOC:4.3.4.1. Materials for training, meetings/workshops, consultancies, capital
equipment.
6

4.3.5. ApOC FinancialGuidelines along with the WHO Imprest Accounting System
must be closely followed.
4.3.6. Atl activities in APOC assisted projects should be in consideration of full
community ownershiP in 5 Years.4.3.6.1. It is essential to ensure that the community accepts the programme's
financial support and management approaches'
4.3.6.2. Adapt the financial accounting procedures to unique situations (e.g.
receiPts not available).
4.3.1. The flow of finances for each of the participating countries goes through the
NOTF central account and to the project sites through the most appropriate and
efficient means for each country. NGDO and National Onchocerciasis
Coordinator representing MOH serve as signatories to the account.
4.3.8. The Southern Sudan finance flow is quite different due to the NOTF being in
Khartoum and the need to utilize NGDO systems to get funds to the project
sites.
4.3.9 . APOC only funds proposals from NOTF. It is therefore important that NOTFs
are formed immediately.
4.3.10. After project approval contracts are signed annually and fi:nds released on an
imprest basis.
4.3.1 l. APOC management would ensure minimum delays in the release of project
funds. Any reimbursement would be based on timely submission of accounts by
NOTF.
4.3.12. All partners in the CDTI projects must be involved in the disbursement,
utilization and accounting of funds from APOC.
4.3.l3.There is need for advocacy at high levels by the APOC Management (e.g'
Ethiopia) to countries with financial systerns which might not facilitate the
APOC trust fund requirements. However, flexibility on this matter should be
both on the part of APOC and the host government.
4.3.14. Since most countries in Africa do not budget as much as $2.00 per person for
health, it is important to ensure that the cost of treatment in APOC projects is
reduced to a minimum that can be sustained by the government and the
communities.
Country working groups were assigned the task of designing administrotive andfinanciol Jlowcharts which is attached in Appendix 4.
4.4. Community Participation and Sustainabilty of CDTI
Drs. Etizabeth Elhassan, J.B. Roungou and Josephine Namboze of APOC, presented papers on
CDTI implementation with reference to approaching the community and issues of community
involvement and ownership of CDTI projects. The APOC CDTI training video, which
highlights vital steps in the implementation of CDTI was shown to participants to further
enhance their understanding of the concepts of CDTI. Drs. Elhassan and Amazigo also
1

1
presented a paper on issues related to sustainability of CDTI. After these presentations and
iubsequent discussions, participants were divided into mixed working groups to examine issues
of community involvement, ownership and sustainability of CDTI with special reference to re-
orientation of on-going ivermectin distribution projects. It was noted that CDTI could initiate
and induce communities toward improvement of their health. Conclusions and recommendations
were made on the various issues discussed as follows:
4.4.1. The socio-cultural norrns and practices of the people should be taken into
consideration prior to approaching the community to introduce the concept ofCDTI. The team approaching the community should be as simple as possible,
without giving the impression of overt wealth (e.g. moving with a large convoy
of vehicles).
4.4.2. Women should be involved in the prograrnme at all levels
4.4.3.
4.4.4.
4.4.5.
4.4.6
To implement the CDTI approach, there is need to re-orient existing and new
projecis to the CDTI strategy of full community participation and ownership of
the programme.
There is need for clearly defined roles for partners in CDTI and ensuring
commitment and full participation at all levels.
NOTF should clearly define roles and responsibiJities of the communities
especiall-r- as pertains to decision making. prograrnme rvlnasement- suneillance
and mobilisation roles.
Communities should be given a free hand to ptan and implement the CDTI
activities.
4.4.7. Health workers should be sensitized to accept CDTI as a partnership between
them and the communities. They should facilitate the successfuIimplementation
of the prograrnme.
4.4.8. The social and political structures should not be disturbed or antagonised but can
be used when approaching the communities for CDTI'
4.4.g. Communities and other partners must accept the responsibilities related to CDTI
and assure compliance over a long period; adequate and consistent advocacy and
health education should be provided at all levels'
4.4.10. Adequate numbers of CDDs should be nominated by each community'
Communities should be allowed to increase the number of CDDs to be trained or
change as necessary.
4.4.1L There should be no payments of incentives to CDDs by extemalsources, rather'
communities should be allowed to decide on the issue of motivation or incentives
for their distributors.
4.4.12.The ownership of the CDTI should be at all levels of implementation -- not just
at the communitY level.
8

4.4.13. Health education messages should be clear, standardized and emphasize
community involvement and ownership of the progralrlme'
4.4.l4.There is need to identify and target key personalities in the political and social
structures for advocac), to raise the levelof awareness and accord priority to the
programme.
4.4.15.It is important that programmes are built towards sustenance by both
communities and governments after cessation of external support.
4.4.16.partners in the projects should think of ways of promoting community self image
and self-confidence and implement this early in order to facilitate community
acceptance and ownership of the prograrnme'
4.5. Training and llealth Education
Mr. J. Watson, APOC, presented a paper on various aspects of training and health education
requirements for implementation of CDTI projects, drawing from field experiences. During the
g.orp work, participants identified the target groups to be trained and health educated at all
ieu"ts including the approach, topics and materials to be used. Generally, it was agreed that
those to be trained oi health educated should be persons who will support, facilitate, and
mobilize resources for the successful implementation of the CDTI prograrnme. It was noted that
the ke.v- componenrs for successful implemenrarion of CDTI w'ere training. health education and
mobiliali6n of the communitv. It was recommended that:
4.5.1. Health Education, being the foundation of successful implementation of CDTI,
should be approached systematically and carefully,
4.5.2. Trainers should be more of facilitators in discussions/activities using a
participatory approach to learning rather than lecturing to the trainees.
4.5.3. The number of CDDs to be trained per community should be related to the
number of persons to be treated. It was suggested that projects train at least 2
CDDs Per 250 Persons to be treated.
4.5.4. Health education and mobilisation of communities is a key component of the
CDTI approach.
4.5.5. Target groups for training & health education at the national level should include
students, health workers, key policy makers, (including those of other
ministries), the media, NOTF members, NGDO personnel and teachers'
4.5.6. Target groups for training and health education at the county, region and district
leveis should include health workers, media, staffof related ministries (e.g.
Educatioru Agriculture), NGDO personnel and teachers'
4.5.7. Target groups for training and health education at the community level should
inctuae nealih workers, local development organization, community members,
CDDs, teachers, traditional and religious leaders and healers.
4.5.8. Health education and training topics should include information about the
disease, the use of ivermectin for treatment, community mobilization, record
9

keeping, and the need for the community to embrace the programme as their
own.
4.5.9. There is a need to establish a subcommittee within NOTF to develop prototype
training and health education materials which can be modified/adapted for use in
various project areas in the country.
4.5.10. Most materials need to be developed at the national, state, local government and
community levels, however, materials such as field manuals, flipcharts, and
calendars could be designed and printed at the national level.
4.5.1 l. Posters and village level health education materials (e.g. jingles in local
languages) should be developed in the villages with community member
participation.
4.5.12. APOC to provide technical support to NOTFs in various aspects of programme
implementation and capacity building as the need arises.
4.5.13. APOC should help provide prototype health education and training materials and
make them available to member countries.
Country working groups were assigned the task of determining the target groups at all
levels for training and health education (See Appendlx 4)
4.6. Ordering, Procurement and Delivery of lvermectin
Nfu. J. Watson, APOC, presented guidelines using the Nigerian experience on procurement and
delivery of ivermectin at all levels. Dr. Mary Allemaq MDP, provided background information
on the Mectizan Donation Programme with emphasis on requirements for drug procuement
and retirement by NOTFs. Dr. H. Edeghere, APOC gave an overview of areas of integration ofivermectin procurement and delivery into the national system. Drs. H. Edeghere and Josephine
Namboze, presented a paper on the management, safety and storage of ivermectin at all levels.
Since ivermectin procurement and delivery is one of the important aspects of the CDTIprograrnme, adequate time was allowed for extensive discussion of the topics. At the end ofdeliberations, the following recommendations and conclusions were made:
Procurement
4.6.1. Ivermectin procurement and delivery should be integrated into existing national
drug procurement and delivery system(s).
4.6.2. NOTF should ensure that ivermectin is ordered on time (at least 8 months prior
to the treatment period) and be responsible for customs clearance, tax
exemptions, transport to the project sites and fulIaccountability for the
ivermectin.
4.6.3. The community is responsible for picking up the ivermectin from agreed
collection points.
4.6.4. Community leveldecision making on procurement of ivermectin should involve
the community leaders, members, health workers, village volunteers, and
goverrlment, and other sector representatives.
t0
t

Storage
4.6.5. Adequate arrangements should be made for the storage of ivermectin from portof entry to the delivery in the community to avoid pilferage or damage.
4.6.6. The two months shelf-life of an opened 3 mg tablet bottle (500 tabs), after theremoval of the foil seal requires that distribution activities be undertaken withinthis period to avoid expiration and therefore wastage of ivermectin tablets.
4.6.7. Efforts should be made to avoid situations which lead to exptation of theivermectin as this could jeopardize the prograrnme.
4.6.8
Delivery
NOTF and the communities should agree on the suitable central collection pointswhere the communities can collect ivermectin.
4.6.9. Communities should be informed well in advance about the availability ofivermectin at the central location for collection.
4.6.10. There is need for appropriate timing in the communitl' for ivermectin delivenand distribution. takine into consideration the socio-cultural and economicactivities of the people.
Safefy
4.6.11. Adequate training should be given to the distributors to ensue:4.6.11.1. Adequate health education information is passed to community
members4.6.11.2. Adherence to eligibility criteria4.6.11.3. Correct dosage (especially with the new 3 mg tablet formulation)4.6.11.4. Adequate recording and reporting4.6.11.5. Adequate management and referral of cases of adverse reactions
4.6.12. Special efforts must be made to educate the communities prior to treatment onpossible adverse reactions. There must be careful monitoring of cases of severereactions to reassure treated persons.
4.6.13. Where there are severe reactions health education should be intensified to avoidincreased number of refusals/absentees during the next round of treatment.Mechanism should be put in place to train health workers to effectively dealwithsevere reactions especially at the community level.
4.6.14. Expired ivermectin should be disposed of by burning the tablets in a controlledenvironment.
Professor C.D. McKenzie also presented a paper on numagement of minor and severeadverse reactions to ivermectin treatment. This was by request of the participants. Following thepresentation and discussion recommendations are as addressed n 4.6.11, 4.6.12 and 4.6.13.
lt
4.7. Recording/Reporting and Feedback at all levels
Papers were presented by Dr. Elizabeth Elhassan providing information on data collection,reporting, analysis, and feedback on onchocerciasis control activities at all levels. Drs. J.B.Roungou, and Terese Aparicio presented papers on monitoring of CDTI while Dr. JosephineNamboze, gave an overview of key issues considered in evaluating CDTI projects using theAPOC forms.
During the country group work, the various components of data collection, analysis, andreporting at all levels of programme implementation were discussed. Also, issues related toproject monitoring were addressed. It was noted that the importance of data collection, timelyand routine reporting of data and monitoring activities cannot be over emphasized for thesuccess of the CDTI prograrnme. It is therefore recorunended that:
4.7.1. commitments from all participating partners in Ethiopia, Kenya, Liberia,Mozambique and Southern Sudan is necessary for the collection of informationrequired at all levels. There is need to adhere to recording/reporting formatsdevised/revised by NOTF as necessary.
4.7.2. Information required from the CDDs should be kept to a minimum and be simpleand straight-forward and should include the following:
4.7 .2.1. Total population of the community (census)4.7.2.2. Total eligible population/number of ineligible population4.7.2.3. Number of people treated4.7 .2.4. Number of refusals/absentees4.7.2.5. Number of severe reactions (treated/referred)4.7 .2.6. Household ffirmation
4.7 .2.6.1. PHC number of household (where applicable)4.7.2.6.2. Information on Household members (name, age. sex)4.7.2.6.3. Number of tablets given to each person4.7.2.6.4. Year of treatment
4.7.3. Methods of data collection:4.7.3.1. CDDs should use simple exercise or register books which the
communities can afford for recording and reporting.4.7.3.2. The community should be given the responsibility of designing their
own ways of recording and reporting of CDTI activities.4.7.3.3. The NOTF should decide with CDDs in the mobile communities,
where the records should be kept if the community is moving toanother location.
4.7 .3.4. For the purpose of uniformity of reporting and recording, it isrecommended that the NOTF should design a simple and uniformmethod of data collection for all levels of CDTI (county, regions,zones, districts).
t2

4.7.4. Repeated training activities for the community and their CDDs is required foradequate and timely reporting. These training sessions should also extend to thehealth facilities and county/district level.
4 -7 .5 - A checklist of indicators for recording and reporting should be developed at alllevels.
4.1-6. Provision of adequate logistical support by partners (e.g. vehicles, motorcycles,communications) to prograrnmes is required in order to initiate frequent andadequate data collection and monitoring of CDTI activities.
4-1.7. Where feasible, reporting, recording and feedback activities for CDTI could beintegrated into other health or development activities as appropriate.
4.7.8. NOTF should ensure adequate and timely reporting of CDTI activities to MDpand APOC as appropriate.
4.7.9. There is need for annual feedback on prograrnme implementation to all partners.
Monitoring
4.7.10. Project monitoring is used to improve operational plans for CDTI and to identifistreng.rhs and weaknesses in its implementation.
4.7.11. Standard monitoring indicators, which include input, output and effects havebeen identified for use in all projects.
4.7.12. There is need to carry out routine monitoring by the NOTF to assure effectiveimplementation of the CDTI projects. Independent monitoring should also beundertaken by APOC to ensure that programme objectives are accomplished.
Evaluation
4.1.13. APOC evaluation forms for CDTI projects should be filled annually for eachprolect
4.7.14. Evaluation forms consist rnainly of five parts which are all supposed to be filledincluding:4.7.14.1. Project profile and management4.7.14.2. Ivermectin procurement, delivery system and distribution4.1.14.3. Capacity of the NOTF/Oncho Coordinators/support staffand PHC
system4.7.14.4. Performance indicators4.7.14.5. Other comments
4.8. Integration of CDTI into Health Services
Drs. J.B. Roungou and Elizabeth Elhassan, from APOC, gave a presentation highlightingreasons for, implications and constraints, possible steps/processes and mechanisms ofintegrating CDTI into the Primary Health Care systenr, and some of the CDTI activities thatcould be integrated into the primary health system. Considering the importance of integrationof CDTI into the health system to ensure sustainability, extensive discussions were allowed.These discussions centred on the various levels of integration, when and where to integrate inrelation to the existence of functional PHC system in the country. Country working groups wereassigned the task of developing strategies for integration of CDTI into health services andidentify constraints of integration and strategies for overcoming them.
4.8.1. Steps towards integration may include:
4.8.1.1.4.8.1.2.4.8.1.3.4.8.t.4.4.8.1.5.
4.8. 1.6.
Ident ification o f health structures/institutions;Identification of level of integration;Sensitizatio n/re-orientation o f health staff;Advocacy to health planners and managers;Integrate training of cDDs into existing training activities for otherhealth prograrnmes;Set up (or re-activate) community health committees for overseeingCDTI and other health activities.
4.8.2
4.8.3
4.8.4
Health w'orkers should not onlv be trained on the health aspects of the diseasebut also on advocacy and management, which helps them to understand theirroles and expectations of the prograrnme.
Integration will only be successful if all partners are convinced of the approachand that this will not in any way affect the technical aspects of the variousprograrnmes.
Some aspects of reporting may not easily be integrated as varioui-prograrnmeshave differing requirements and expectations.
4.8.5. CDTI could be used as an entry point upon which PHC could be buiit andstrengthened
4.8.6. For compatibility, CDTI integration should be carried out gradually identifyingthe priority areas to be integrated.
4.8.7. For long term sustainability, it is necessary to integrate CDTI into existing healthsystems, and development based activities. Areas and programmes with goodpotential for integration are training, drug distribution, EpI, TB/Leprosy, etc.
4.8.8. Integration should not jeopardise either CDTI or the prograrnme(s) with which itis being integrated.
4.8'9. Inventory of the community mechanisms/structures should be done to identifythose that can be used in the implementation of CDTI whether or not PHCstructures exist.
t4
4.8.10. There is need to establish as soon as possible enabling policies at the highestlevelin support of integration of CDTI into the health sysrem.
4.8.1 l. Where cost-sharing is introduced, this should be done in such a way that eligiblepersons are not excluded.
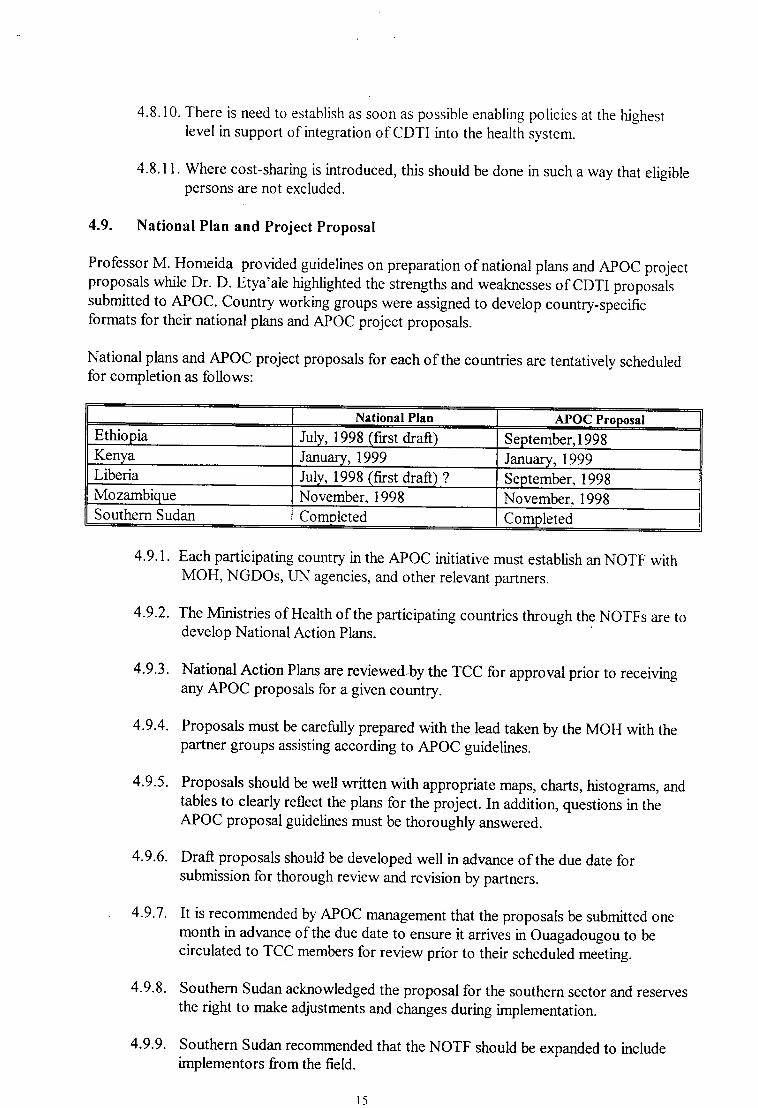
4.9. National Plan and Project Proposal
Professor M. Homeida provided guidelines on preparation of national plans and APOC projectproposals while Dr. D. Etya'ale higtrlighted the strengths and weaknesses of CDTI proposalssubmitted to APOC. Country working groups were assigned to develop country-specificformats for their national plans and APOC project proposals.
National plans and APOC project proposals for each of the countries are tentatively scheduledfor completion as follows:
4.9.1. Each participating country in the APOC initiative must establish an NOTF withMOH, NGDOs, IJN agencies, and other relevant partners.
4-9.2. The Ministries of Health of the participating countries through the NOTFs are todevelop National Action Plans.
4.9.3. National Action Plans are reviewed by the TCC for approval prior to receivingany APOC proposals for a given country.
4.9.4. Proposals must be carefully prepared with the lead taken by the MOH with thepartner groups assisting according to ApOC guidetines.
4.9.5.
4.9.6.
4.9.7.
4.9.8.
4.9.9.
Proposals should be well written with appropriate maps, charts, histograms, andtables to clearly reflect the plans for the project. In addition, questions in theAPOC proposal guidelines must be thoroughly answered.
Draft proposals should be developed well in advance of the due date forsubmission for thorough review and revision by partners.
It is recommended by APOC numagement that the proposals be submitted onemonth in advance of the due date to ensure it arrivei in ouagadougou to becirculated to TCC members for review prior to their scheduled meeting.
Southern Sudan acknowledged the proposal for the southern sector and reservesthe right to make adjustments and changes during imprementation.
Southern Sudan recommended that the NorF should be expanded to includeimplementors from the field.
National Plan APOQ ProposalEthiopia July, 1998 (first draft) September,l998Kenya January, 1999 January,1999Liberia July, 1998 (fust draft) ? SeptembeL 1998Mozambique November, 1998 November. 1998Southern Sudan Completed Completed
t5
4.9.10 Ethiopia, Kenya, Liberia, and Mozambique have prepared backgroundinformation for the development of National Plans and APOC project proposals.
4.9.11. APOC Project Proposals for Ethiopia, Kenya, Liberia and Mozambique will be
developed as indicated in the preceding table.
See Appendix 4 for ffirmation required for National Plans
4.10. Other Matters
Other issues discussed with appropriate recommendations were as follows
410.1. Idea of APOC Newsletter as well as in-country newsletters to communicateoverall progress and information concerning the prograrnme
4.11. Conclusions/Recommendations of the Workshop
Professor C. D. McKenzie led an open discussion on the sunmary report of the workshop.Issues covering specific items were discussed and changes were made upon consensus opinion.
The final summary document containing conclusions and recommendations were given to
participants.
l6

18
22
28
35
44
53
62
7l
80
86
D
J)
Appendices
Appendix
A) Opening CeremonY SPeeches..
B) Workshop Agenda
C) List of ParticiPants.........
D) Ethiopia Country RePort....
E) Kenya Country Report.............
F) Liberia Country Report.............'
G) MozambiqueCountryReport..........
H) Southern Sudan CountrY RePort.
Monitoring Form
Evaluation Form
t7


APOC/NOTF WORKSHOP ON COMMUNITY DTRECTEDTREATMENT WITH TVERMECTIN
Welcoming remarks by the National Coordinator
The Hon. Minister for Health, Prof. M. Hemeida, Dr. Paul Chuke, DrDaniel Etya'ale', Dr. Uche Amazigo, distinguished guests, fellowparticipants, ladies and gentlemen.
Welcome to Nairobi for the African Programme for OnchocerciaasisControl and National Onchocerciasis Task Force workshop.
We are going to deliberate on important issues on the operations and
sustenability of community based programmes, mainly of drugdistribution and also vector control in liited foci.
As you know the disease is onchocerciasis (oncho). commonly known as
river blindness is caused by a nematode Onchocerca volvulus whichparasitizes the skin and is transmiffed by blackflies of the genusSimulium. Details of the importance of the disease, its endemicity andmorbidity in various countries will be given during this workshop, insufficient detail to enable us to see the way forward in terms of control.
Once again Karibu Kenya!!
l8
t'

WHO STATENTENT BY DR. PAUL CHUKE, WHO REPRESENTATIVE,KET{YA
(READ BY DR D M MUTTE, DISEASE CONTROL OFFICER. WR'S OFFICE,KEI.IYA)
Mr. Chairman of this session,
Hon. Minister for Health,Director of Medical Services,
Dr. Danniel Etya'ale, NGDO CoordinatorDr. Uche Amazigo, APOCWHO Representatives of HQ and AFRODistinguished DelegatesLadies and Gentlemerq
On behalf of the WHO Country office Kenya and on behalf of Prof. Paul Chuke the WHORepresentative, I have the honour and pleasure of welcoming you all to Nairobi and to this
inter-country APOC Workshop. Cognizant of the role played by infections and parasitic
diseases in Africa as major contributors of "Burden of Disease" VIHO, the World Bank
and their collaborators have had a strong hand in programmes such as the APOC. [n this
connection, Dr. Nakajima the Director General of WHO, has a messa-ee of hope in the
1996 World Health Report. In part he says, and I quote. ull/e stand on the threshold ofa neu, era, in which hundreds of millions of people will at least be safe from some ofthe worlds most tenible diseases. Sooner rather than later, poliomyelitis, leprosy,
guinea worm diseose, iver blindness chagas disease and neonatal tetanus will joinsmall pox as diseases of the past" end of quote.
Your meeting should be yet another important milestone on the road towards the
elimination of onchocerciasis, as a public health problem in APOC countries-of sub-
Saharan Africa.
Cost effectiveness, affordability, access and use of health care services are fashionable
terms within WHO's 9th Programme of Work, which runs from 1996 - 2001. The goals
and targets in this particular Programme of Work are an expression of commitment of the
international health community, in achieving improvements in health status including the
reduction of disabilities such as blindness caused by oncho. Disease.
Your meeting comes at another important point in time. Two weeks ago, on the 7th April1998, WHO celebrated it's 5fth anniversary. In his message to mark this day, the WHO
Regional Director for Africa Dr. Samba said and I quote: "Half a century ago, in a spiitof equity and solidaity, the member states of United Nations Organizttions gottogether and made a solemn pledge to set up a technical body equipped with the
necessary resources and erpertise to address various health isszes, diseases and other
causes of suffering and death" end ofquote.
l9
As you press on with your relentless fight against river blindness, the WHO's commitmentremains unaltered. Already on the agenda of the WHA next month is an item of RenewingFIFA Strategy for the 2l st century. Disease control, elimination and, were feasible,eradication are important components of this renewing of FIFA in the new century.Onchocerciasis elimination is on the firing line.
The 1997 WHO World Health Report w:uns us that with many governments andinternational aid agenciesforced to tighten spending in recent years, funding for essentialservices is in short supply. The challenge now is to find ways of improving health deliverysystems at costs people can afford while ensuring the sustainability of programmes andservices. In this connection I commend APOC on their innovative strategy to be discussedduring this meeting,i.e. Community Directed Treatment with Ivermectin (QDTI).
The WHO and UMCEF have, over a considerable period of time, talked aboutCommunity involvemenl Later on Community panicipation was preferred - ( I guessthat one can be involved in a certain event without necessary participating!). Andcurrpntly the best term seems tobe Community ownerchip of health It is my hope thatyou will explore ways and means to place CDTI on the community ownership's account .
Since 1994, the IITIO Regional Office for A-frica has been promoting the concept of a"ilIipimum Health Package" alternatively called the Essential Clinical and Public HealthPacfage for acceleration of [IFA. It is my hope that within the APOC countries,Onqhocerciasis control will form an ingredient of the "Nfinimam Package". One of thetools for this approach is " Essential Medical Care" and treatment with ivermectin shouldbe considered as an integral part of essential medical care within the "minimum Package".
Last but not the least, may I remind you that such gatherings as this week's meetings is animportant forum for "Continuing Education,'l for health workers. [n some of the latestissues of the LANCET, one of the renowned medical journals published in the U K ( fthink it was the 4th, April, 1998 issue) I read that "continuing education" is now beingreferred to asuContinuing Professional Development" or CPD. The author of thearticle says that there is an educative value in professional workers attending a meetingeven for those who finally find out that there is no reason to change their practice. [nother words, even if at the end you find that you know almost everything discussed, thatrealization is a form of learning. There are also many aspects of learning that are noteasily measurable.
I hope you will learn a great deal during your deliberations.
Thank you and good luck!
20

APOCNOTF WORKSHOP ONCOMMUNITY DIRECTED TREATMENT WITH IVERMECTIN
(cDrr)NAIROBI, KENYA, APRrL 20_25, lggg
SPEECH BY TFM DIRECTOR OF MEDICAL SERVICES, DR. JAMES N MWANZIA
Prof M. Homeida, Dr. Daniel E. Etya'ale', Dr. Uche Amazigo, Dr. paul Chuke, Members ofSponsoring Agencies, distinguished guests, participants from ApOC countries, ladies andgentlemen.
It is with great pleasure for us to host this workshop on community directed treatment ofoncho with ivermectin. oncho remains a serious put[" health p.obl.* in much of tropicalAfrica affecting 17.6 million people, of who l5 million (or more than 85%) now live outsidethe oCP areas of west Africa. Prior to 1987 no safe drug for a community based treatment ofoncho was available, until ivermectin was registered for ho-* use. The most seriousconsequences of the disease is blindness and a very severe skin disease accompanied by anintense itching.
APOC has a goalof implementing a community based sustainable control of oncho in up to l6countries of Africa where the disease is still a public health problern The programme (ApOC)will control the disease by designing and implementin-s a communitv based ir.Jrmectindistribution systenl supplemented by vector eradication in a few isolated foci.
This approach ensures ownership of the prograrnme by the community with minimum buteffective medical supervision. It forms an important step in eliminating the disease as a publichealth and socio-economic problem in Africa outside the eleven OCp countries of WestAfrica.
The drug ivermectin (Mectizan) has been provided free of charge for as long as it is needed.APOC will take advantage of this window of opportunity to bring oncho *i.. control. Isincerely thank Merck & co. for this generous donation of Mectizan.
Community self treatment with ivermectin will provide an important entry point for othercommunity based health interventions, and thus help to develop a practicaibasis forstrengthening primary health care (pHC) in some of the poorest communities.
Kenya eliminated onchocerciasis by instituting antivector measures in certain well defined fociin the western part of the country in the 1950s and 1960s. However, residual foci persisted onMt. Elgon on the common boundary with Uganda and in the surrounding hills where thedisease was recently detected. The disease has also been detected in refugees and otherimmigrants living in Kenya, particularly from Sudan. This and the p..r..rJ. of the vector inKenya makes re-establishment of the disease as a public health protl"rn a real possibility.
An epidemiological assessment is necessary to establish the level of the disease in the country.
Thank you.
21
Appendix B
TVORKSHOP ON THE PHILOSOPHY OF THE AFRICAN PROGRAMME FORONCHOCERCIASIS CONTROL (APOC), CONCEPT AND HARIVIONIZATION OF
COMMUNITY -DIRECTED TREATMENT WITE TYERIVIECTTN (CDTI).NAIROBI, KENYA (20 - 25 APRrL 1998).
ANNOTATED AGENDA (Revision l)
Sunday 19/04/98
Informal meeting with participants/ election of Rapporteurs/
introduction of Facilitators19H30 - 20H30
Monday 20/04/98
SESSION 1: Opening / General Announcements
ll
Chairman:Rapporteurs:Facilitators:Election of officersChairmanVice-Charman
08H00 - 08H10
1.2 Adoption of Workshop Agenda 08H10 - 08H20
I.3 Objectives, Expected outcome of Worksho,p (Amazigo) 08H20 - 08H35
1.4 Pre-test ( Roungou and Namboze) 08H35 - 08H50
1.5 APOC/ CDTI Training video fiLn 08H50- 09H30
1.6 09H30 -10H30
COFFEE BREAK r0H30 - 10H45
SESSION 2: Philosophy of APOC/ Concept of CDTIChairman:Rapporteurs:Facilitator:
2.1 Philosophy of APOC @tya ale) 10H45 - I lH00Ccrncept of Community Directed Treatment with ivermectin (Amazigo) I IH00 - I lHl0
2.2 Partrrership in APOC @tya ale/ Goepp) I lHl0 - 11H30
Opening CeremonyVideo from Sudan (7-8 mins)Welcome address by Natiural Coord:nator/ KenyaAd&ess by Dr. P. Chuke (WHO Represortative in Kenya)Prof M. Homeida /Technical Consultative Commiuee, APOC
Ope"iog address by Hon. Minister of Heahh, Kerya
')')

2.3
3.5
3.6
LUNCH BREAK 12H30-14H30
SESSION 3. Administration, Budget, Financial Management of APOC projectsChairman:Rapporteurs:Facilitator: Edeghere
3.1 Guidelines for elaboration of budget @rof. Homeida) 14H30 - 14H50
3.2 Administration & Management of APOC Fund (Aholu) 14H50 - 15H30
3.3 Discussion l5FI30 - 16H00
COFFEE break: 16H00 - 16H15
3.4 Working goups (5 countryteams) on Administration, Financial Management
- Frnancial Flow (chart) from Central -District Levels l6Hl5 - l8Hl5- Administration/ Financial Reporting Systems
Tuesday 2l/04198
Rapid Epidemiological Mapping of Onchocerciasis (REMO)Obj eaive/ methodologyitmportant steps (Edeghere)
Status of REMO /GIS for APOC countries @deghere)C o n clu s i o n/ Re co mmen dation s
Plarary . Presentation of Financial Flow charts and Administration/Financial Reporting Systems by country teams
C o n clu s io n u n d Reco mmen datio n s
I IH30-l2Hl0
l2Hl0-12H30
7H30 - 08H30
08H30 - 09H00
09H00 - 09H1509H15 - 09H3009H30 - 09H5009H50 - l0Hl5
l0Hl5 - 10H30
r0H30 - 12H00
12H00 - 12H30
SESSION 4: Community Participation & Sustainabilty of CDTIChairman:Rapporteurs:Facilitator:
4.1 Approaching the Community @lhassan)4.2 Filrn (lSmrns)4.3 Other roles & responsibilities of communities (Roungou/ Namboze)
4.4 Discussion (Questions)
COFFEE BREAK
4.5 lYorking groups an: Approaching communrty & responsibililies
in ivermectin distribution
Plenary on Approaching community & responsibilitiesReports from groups:
4.6
LTINCH BREAK
23
t2H30 - 14H30

Reports from groups on Approaching community & responsibilrties
Co n cl u sio n an d Reco mmen dat io n s
Community involvement and ownership of CDTVSustainability of CDTI (Amazigo/Elhassan)(With special reference to reorientation of on-going proiects/Lessons from participating NGDOs)
COFFEE BREAK
Working groups on Communrty rnvolvement and ownership of CDTU
Sustainability of CDTI
Participants' assessment ofthe organization of the Workshop
- What needs to be improved? / What is going on well? (Etya ale)
Wednesd ay 22104198
Plenary: Presentation of workrng groups on:
Community involvement and ownership of CDTVSustarnabrlrry of CDTIC o n cl u sio ns and Reco mmen datio n s
SESSION 5: TRAINING AND HEALTH EDUCATION
4.7
4.8
4.9
5.1
14H30 - 15H0015H00 - 15H30
r5H30 - 16H00
I6H00 - 16H30
16H30 - 17H00
17H00 - 18H30
18H30 - 19H00
08H00 - 08H30
08H30 - 09H00
08H00 - 08H3008H30 - 08H45
o8Hls - 09H0009H00 - 90H30
09H30 - l0Hl5
l0Hl5 - 10H30
10H30 -I lH30
l lH30 - 12H00
5.2
5.3
Chairman:Rapporteurs:Facilitator:Training & IEC materials in the context of CDTI
(JeffWatsur)Country Experiences: Training & IEC matenalsTraining video (section on training CDDs) & APOCCDTI Training manual (Amazigo)Harmonizatisp sf Jl3ining /Heahh EducationmAhods and materials (JeffWatson)
-process
-materials-budgeting for lEC/Traurmg materials in CDTI projectsWorking Groups (mixed): Training/fleahh Education/ tEC for CDTI
COFFEE BREAK Group photograph
Plenary on Harmonization of Training /Heahh Education/IECPresentations by working groups
54
5.5
5.6
5.7 ConclusionsondRecommcndations
24

LUNCH BREAK
SESSION 6: Ordering, Procurement and delivery of ivermectinChairman:Rapporteurs:Facilrtators:
6. I Introduction: Procurement and delivery of ivermectin (Watson)
-Procedure for Ordenng Mectizan@ (MDP)
-lntegration of ivermectin procurement & delivery in the national
system @deghere)6.2 Management, Safety and Storage of ivermectrn
at all levels @deghereAlamboze)Discussions
COFFEE BREAK
6.3 Working grouPs (by country) on Ordering, ProcuremerU
Drug Delivery circuit and integration of ivermectin
into the national delivery sYstem
6.4 Plenary on Orderrng, ProcuremenU Drug delivery circurt
and integration of ivermectln in the national heahh system
6 5 Conclusions and Reconunendalions6.6 Management of mmor and severe adverse reactions
12H45 - 14H30
14H30 - 14H45
t4H45 - 15H05
15H05 - 15H20
15H20 - 15H45
15H45 - 16H00
16H00 - l6Hl0
16H10 - 17H10
17H10 - 17H40
17H40 - l8Hl0l8Hl0 - 18H40
09H45 - I lHl5lrHl5 - l2Hl5
l2Hl5 - 12H45
Thursday 23104198
SESSION 7: RECORDING, REPORTING AND FEEDBACK AT ALL LEVELSChairman:RapporteursFacilitator:
7 .l Collection of information/ Recordurg/Reportrng/Feedback @lhassan) 08H00 - 08H30
7.2 Monitoring of CDTI Projects @oungou) 08H30 -08H45
7.3 Participatory monitorurg of Projects (Aparicio) 08H45 - 09H00
7 .4 Forms for Evaluation of CDTI Projects (Namboze) 09H00 - 09H30
COFFEE BREAK 09H30 - 09H45
7.5
7.6
Working groups on Recordrng/ Reporting/Monitoring/Evaluation ( at all levels)
Plenary on Recording/ Reporting/ Monitomg/Evaluation ( at all levels)
Recommendations on Recording, Reportingand Feedback
7.7
LUNCH BREAK
25
12H45 - 14H30
SESSION 8: Integration of CDTI in the Health Care Service
8.1
Chairman:Rapporteurs:Facilitator:
lntroduction: Integration rnto Health Care Service (Roungor.r/ Elhassan) 14H30 - 14H50
8. I . I Importance of ntegration of CDTI8.1.2 Process of integration of CDTI
8.2 Working groups on integration into Heafth Service
COFFEE BREAK
14H50 - 16H00
16H00 - l6Hl5
16H15 -I7HI5
l7Hl5 -18H00
08H00 - 08H2008H20 - 08H40
08H40 - 09H0009H00 - 10H00
838.4
Plenary on Integration of CDTI in the Heahh Care servrce
Presentations by working groups
8.5 Conclusionandrecommendations
Friday'24104198
SESSION 9: National Plan and Project ProposalChairman:Rapporteurs:Facilitator:
9.1 Guidelines on National Plan and Project Proposal (Homeida)
9.2 Strengths & Wealaresses of Proposals submiued by NOTFs -and lessons leamed (Etya ale)
9.3 Discussions/Questions9.4 Working groups ( country teams) on national Plan & Prqect Pro,posals
9.69.7
COFFEE BREAK:
9.5 Country Working Groups session on National Plan and ProJect proposalcontrnue.Presentation of Country Reports
Conclusions and Recommendations
LUNCH BREAK
SESSION l0: Other mattersChairman:Rapporteurs:Facilitator:Any other matters ( on all issues)
10H00 - r0H15
l0Hl5 - 10H45
10H45 - 11H45
l rH45 - l2Hl5
l2Hl5 - 14H30
26
14H30 - I5H00
SESSION 1l: Conclusions/Recommendations of the WorkshopChairman:Rapporteurs:Facilitators:
l0.l Adoption of Plan of the Workshop Report
by country delegates and participants10.2 Adoption of the Conclusions and Recommendations of the Workshop
COFFEE BREAK:
10.3 Post Test (Roungou/ Namboze)
SESSION 12
Closure of the l{orkshop
t5H00 - 15H30
15H30 - 17H00
17H00 - l0Hl5
17H15 - 17H45
r7H45 - l8IU5
27

Appendix C
WORKSHOP ON THE PHILOSOPHY OF THE AFRICAN PROGRAfuTME FORONCHOCERCUSIS CONTROL (APOC), CONCEPT AND HARMONIZATION OF
C O MMU N ITY- D I RE CT E D T REATME NT II/ITH IYE RME CT IN, NA I RO B I, K E NYA,20 - 25 APRIL 199E
Provisional List of Participants
Participants
Ethiopia
l. Dr. Desta Alamerew, Epidemiologist, Malaria & Other Vector Borne Diseases Control Unit,Ministry of Health P.O. Box 1234, Addis-Ababa, Ethiopia -Tel: (251) 1 51 6617 - Fax: (251) I 5193 66
2. Dt. Tekle-Mariam Shiferaw , Head, Health Researches and Public Health Lab., p.O. Box 149,Awassa, Ethiopia - Tel: (25 t) 6 20 t6 45 - Fax: (25 t) 6 ZO t6 76
3. Dr Wondwosen Yimam Getahun, Head of Rigenal. Maleria and Other Vector Borne DiseasesControl Department, Benshangul-Gumuz Health Bureau Assosa, P.O. Box 71, Ethiopia -Tel: (25t)7 6t 10 87
4. Mr. Sheleme Chibsa Tujuba , Head, Malaria and Other Vector Borne Diseases ControlDepartment for the Region of Oromia, Oromia Health Bureau, Addis Ababa, Ethiopia - Tel: (251)r sl40 76 (A.A)
5. Mr. Yeshiwondim Asnakew Kebede, Team Leader, Malaria and Other Vector Borne Diseasescontrol, P.o. Box 495, Bahir Dar, Ethiopia, Tel: (z5l) 8 20 09 22 -Fax: (251) g zo t5 17
Ken!a
6. Dr. Maina Kahindo, Head, Division of Communicable of Veector Diseases Control (DCVDC),Ministry of HealttL AFYA House, P.O. Box z}T}l,Nairobi, Kenya -Tel. Qs$2720 533 or (254)2727 809 or (254)2716 515 - For. (2s4)2720 533 or (254)2713824
7. Dr. David S*9, APOC National Coordinator, Division of Vector Borne Diseases, Ministry ofHealt[ P.o Box 20750, Nairobi, Keny4 TeI. (254) z 724 3oz or (254) z 725 833 -Fax. (254)2 72s 624 -Emul: SCHISTO@|KEN.HEALTHNET.ORG
8. Mr. David Koectq Officer in Charge DVBD Rift Valley Province, P.O. Box 5, Kapsabet, Kenya,Tel Q5\ 326 2020
28
9. Mr. Wesiela Francis Chemasweti, Prov. Clinical Lab. Technologist, P.O Box 15, Kakamega,
Kenya, Tel. (254) 331 30052
10. Mr. Langat Alfred Kipngeno, Senior Public Health Officer, Ministry of Health, P.O. Box 30016,
Nairobi, Kenya, Tel. (254) 2717 077
I 1. Mrs. Obel Millie Chepkemoi, Faculty ofHealth Science, Moi University, P.O. Box 4606 Eldoret,
Kenya, Tel. Q5$ 321 32569
12. Mr. John Oluoch, Officer in charge, Division of Vector borne Diseases (DVBD), P.O. Box 92,
Kisil, Kenya, Tel: (254) 381 20801
13. Dr. Akhwale Willis Simon, District Medical Officer of Health, Trans NZOIA - P.O. Box 98
Kitale, Kenya, Tel: (254) 0325 70451 - Fax: (254) 0325 31900
14. Dr. Aba Nwachukwu, Zoology Department, University of Nairobi, P.O. Box 30197, Nairobi,
Kenya, Tel: (245) 2 72 40 13
15. Dr. Phoebe Josiah, Research Consultant, Health Environment & Population Consultancy, P.O.
Box 42679, Nairobi, Kenya, Tel: (254) 2 823 100 or (254) 2 350 002 - Fax (254) 2 542 090
Liberia
16. Dr. Samuel T. Dopoe, National Coordinator, Onchocerciasis Programme c/o Ministry of Health
& Social Welfare c/o Wortd Health Organization (WHO) Liberia" P.O. Box 316, Monrovia, Liberia,
Tel. (23r) 226 208 - Fax: (231) 226 Zo8
17 . Dr.Dolopei Eugene Ddi, Deputy Director, Liberian Institute for Biomedical Researctq P.O. Box
3 1, Charlesville, Margibi County, Liberia, Tel: (23 l\ 22 62 08 - Fax: (231) 22 62 0$
18. Mr. David K. Franklin, Data Analyst, Christian Health Association of Liberia (CHAL), P.O. Box
9056, Monrovia Liberia Tel (231) 22 68 23 -Fax (231) 226 187
19. Dr. Fatorma K. Bolay, Disease Prevention and Control Officer (DPCO), World Health
Organization (WHO), P.O. Box 316, Monrovia, Liberia,Tel'. (231)226 208 - Fax: (231)226208
Mozambique
20. Dra. Maria Ivone Ferrdo Teimizira, Ministry of Health, P.O. Box 264Maputo, Mozambique,
Tel: (258) I 430814(2s8) I 427131 - Fax(2s8) | 426s471(2s8) 1 33320
27. Dra. Lorna Maria Fialho Gujral, National Institute of Health, Ministry of Healtb P.O. Box 264
Maputo, Mozambique, Tel: (258) 1 431103 or (258) 1 430970 - Fax: (258) 1 431103 or (258) I
43097 0 - Email. [email protected]
29

South Sudan
?2. Mr . Gordon Solomon Alebe, PHCP Senior Supervisor/OV Supervisor, Senior Medical Assistant,PHCP - Maridi County, South Sudan
23. Prof Mackenzie Charles, Adviser, Gl00, Dean's Office, VMC, Michigan State University EastLansing, \ytr,48824, USA Tel: (517) 432 2388 - Fax. (517) 432 1037 -Email: mackenzie@ cvm. msu. edu.
24. Mr. Lawrence Bona. Brock, OV Supervisor, A/?HC/Supervisor, Sanetarian, Mundri County,South Sudan
25. Mr. PeremunaWuraAmaya, SeniorPHC Supervisor, CHD/PHCP, Mundri/I(otobi, SouthSudan
26. Mr. Mangu Wandege Michael, OV County Supervisor, OV County Office, Tambura, SouthSudan
27. Dr. Deng Samuel Mayak, Medical Doctor, Volunteer Medical Officer, CCM, Alpha CivilHospital, Billing, Rumbek County, South Sudan
28 Mr. Gabriel Chol Dhuor, Nurse, Bilin-e Hospital. Rumbek Countv. South Sudan
29. Mr. Bith Maguruk Macol, Laboratory Assistant, Alpha Civil Hospital, Billing Hospital, RumbekCounty, South Sudan
30. Mr. Gordon Makuek Marol, Community Health Worker, Kolcum, PHCU, Billing Hospital,Rumbek County, South Sudan
3 l. Mr. Simon Kuot Kuot, Health Coordinator, Medical Assistant, Responsible for Nyamlell PHCC,Aweil West County, South Sudan
32. Dr. AmaMorrisTimothy,M.ScStudent,LondonSchoolofHygiene&TropicalMedicine,JohnAstor House, 3 Foley Street, Londorg WIP 8AN, United Kingdonq Tel'. +44 0171 380 9l 19 - Fax.+ 44 0171 436 5389 - Email: [email protected]
33. IvIr. Camillo Yee Mangieamanga, SRRA Secretary, Tambura County, South Sudan
34. Mr. Philip Caiaphas, PHC Coordinator/OV Supervisor, East Mundri, New Sudan, c/o MundriReliefandDevelopment Association(MRDA), P.O. Box60837Nairobi, Kenyq Tel. Q592720995- Fax: (254)2720977
35. Mr. Emannuel Ezam4 ov Supervisor, PHCP-CHD, Yambio County, South Sudan
30
Facilitatorc
36' Dr' Josephine Namboze, Disease Prevention and Control Medical Officer, p.O. Box 149Kampala, uganda. Tel. (256) 41 344038/34405g - Email: [email protected]
37' Mr' Jeffrey Watson, Oncho Programme Coordinator, Christoffel Blindenmission (CBM) 34Gomwalk Close, Jos, plateau State, NigeriaTel: (234) 73 45 65 78, Fax: (234) 73 45 42 30, E-mail <Jeffivatson@maf org>
38 Dr' Henry Edeghere, wHo, zonalNPl Surveillance coordinator, wHo, I Golf Course Road,Kaduna, Nigeria, Tel: (234) 62 237925 or (234) 62 2t3432 or (234) 62 ztt 764 - Celtphone: 09080 50 87 - Fax: (234\ 62 237 924 or (234) 62 238 360 - Email: [email protected]
39' Dr' Elisabeth osim Elhassan, Country Representative, Sight Savers International (SSD, I GolfCourse Road, P.o. Box 503, Kadunq Ngerii, Tet. (234) 62 23g360 - Home: (234) 62 2lo 723 -Fax. (234) 62 238360
40 Profl Mamoun M. A. Homeida, National Coordinator & Chairman of NoTF/Sudan, p.o Box12810, Khartoum, Sudan, Tel: (249) lt 72 47 62 -Fax. (z4g) lt Tz 47 gg
4l Ms Joyce Msuya' Health Speciaiist, the World Bank, Africa Region-onchocerciasiscoordination Unit, 18r8 H street, N.w., washington D.c., 2033, usATel (202) 4sB 77 tz - Fax: (2oz) 5zz 3157 -r,mail: JMSITYA@WORLDBANK oRG
42. Ms. Teresa Aparicio-Gabarq Social Anthropologist, LCSES, the world Banh lglg H StreetN.w., washington, D C., 20433,Ter. (zoz) 45& 90r; - Fax (2oD) 676 9373
WHO/APOC Stafr, Geneva
43. Dr. Daniel Etya'ale, wHo/Apoc, Geneva 27, cH 1211, switzerland,Tel @122) 791 26 4Z,Fax. (4122) 7gt477T
WHO/APOC Staff, Burkina Faso
44. Dr. Uche Amazigo, wHo/Apoc, p.o. Box 549, ouagadougou, Burkina FasoTet. (226) 30 23 t2/30 23 t3/30 23 ot,Fax: (226) 30 2r +1tpzi134 26 4843. Dr. Jean-Baptiste Roungou, OTD/AFRO, p.o. Box 549, ouagadougou, Burkina Faso,Tel. (226) 30 23 12/30 23 t3t3o 23 ot,Fax: (226) 30 zt 47/(226) 34 za qg
45' Mr' Yaovi Mokpoko Aholou, WHO/APOC, P.O. Box 549, Ouagadougou, Burkina Faso,Tel: (226) 30 23 rzl30 23 t3/30 23 ot,Fax: (226) 30 zr 47/(226) li zo qa
46. Ms. Patricia Mensah, wHo/Apoc, Box 549, ouagadougou, Burkina Faso,Tet. (226) 30 23 12t30 23 r3t3o 23 ot,Fax. (226) tO it 47/A2q 34 26 48
3l

WHO KENYA
47. Dr. Zagana Nevio, Medical Officer, CTD Division, Onchocerciasis Unit, World Health
Organization WHOA{airobi, Kenya, Tel: (254) 7 7212 534 - Fax: (254) 2 7214 777 - Email:
48. Dr. Mutie Dominic Makaa, WR a.i., World Health Organization (WHO), P. O. Box Nairobi,
Kenya, Tel: (254) 2 72 30 69 - Fax: (254) 2 72 00 50
NGDOs
49. Ms. Irene Goepp, Programme Manager, OlS/Southern Sudan OV Control Programme,
HealtlNetlnternational, SuguttaRoadP.O.Box40643,Nairobi,Kenya,TeL.(25$2573704-Fax:(254) 2 574 452,E-mul: [email protected]
50. Mr. Fasil B. Chane, HealthNet International, Sugutta Road P.O. Box 40643, Nairobi, Kenya,
Tel. (254) 2 573 704 - Fax: (254) 2 574 452, E-mail: [email protected]
51. Dr. Mary M. Alleman, Associate Director, Mectizan Donation Program, 750 Commerce Drive
Suit 400, Decatur, GA 30030, Atlanta, USA Tel. (404) 371 1460 - Fax: (404) 371 1138 - Email:
malleman@asldorce org
52.Mr.Ben Male, Programme Support Manager, Sight Savers lnternational - East Central Southern
Africa Region, P.O. Box 34690, Nairobi, Kenya, Tel. (254) 2 50 38 35 - Fax: (254) 2 50 55 48 -
Email: benmale@ africaonline. co. ke
53. h/k. Cox Ross, Resident Advisor, Global 2000, The Carter Center, P.O. Box 51911, Nairobi ,
Kenya, Tel'.Q54)2245697 -Fax:(254) 2245690-Email:GLOB2000@AFRICAONUNE CO.KE
54. Dr. Ayodele Benjamin Aderinola, Endemic Diseases Coordinator, Aktion Afrika Hilfe (AAH -
Sudan Programme), P.O. Box 76598, Nairobi, Kenya - Tel. (254) 2 571 978 or (254) 2 571 979 'Fax. (254) 2 574 969 - Email: akafri@form net comm
55 Gathigira Julie Wachera" lnternational Rescue Committee (IRC), P.O. Box 62727, Nairobi,
Kenya, Tel. (254)Z 574 488, Fax: (254)2 574 495
56. Ms. Roslind Awando, Health Officer/OV Coordinator, South Sudarq World Vision lnternational
(WVD), P. O. Box 56527, Nairobi, Kenya; Tel. (254) 2 Ml 777 - Fax'. (254) 2 441 819
57. Dr Bellario Ahoy Ngong Geng, Chiefl Health Coordinator, Sudan Relief and Rehabilitation
Association (SRRA)New Cush New Sudan, P.O. Box 39892, Nairobi, KenyaTel: (254) 2 44 0l 56 or (254) 2 44 80 75 - Fax: (254) 2 44 80 78
58. Dr. Eyamba Albert, Project Advisor, Carter Center, P. O. Box 4794, Yaounde, Cameroorq
Tel/Fax: (237) 20 50 12
32

Other Participants
59. Prof. Braide Ekanem Ikpi, Temporary Advisor to WHO on Impact Assessment, l6 Ibom Layout,P.O. Box 3679, Calabar, Nigeria -TeL. (234) 87 222 87? or (234) 87 220 452 - Fax: (234) | 87 222 872 or (234) 87 220 452
60. Mr. Davies Rowland, Observer, c/o P.O. Box 10018, Nairobi, Kenya
PWANC 2J.OJ.I99E
))

34

EthiopiaAppendix D
Unselected Areas for REMO
Oncho Free Areas
CDTI to refine
REMO
35
ffi
CDTI Areas
Afar

ETHIOPTA
General information
Ethiopia is located in the Horn of Africa. [t shares borders with five countries, Eritrea inthe norttr, Sudan in the west, Kenya and Somalia in the south and Djibouti in the east.
According to a recent census, the population of Ethiopia is about 57 million and 85 % ofthis is rural. More than 60To of the population lives in the highland plateau where thepopulation density is very high. In the low lands, the land is sparsely populated.
Topography, climate and accessibility
Ethiopia is a mountainous country with a highland plateau that is divided into several parts
by tlre five major river basins (Tekeze, Abbay, Barro, Omo and Genalle). The country is
divided in to two parts by the great Rift Valley which crosses from south-west to north-east.
The,long rainy season in the country extends from June to September and the short one,
occurs between January and February, covering some parts of the country. The dryseason starts in October and ends in June.
Due to the rugged terrain and the numerous rivers in the country, access to many ruralareas is very limited. Up to the zonal level, there are usually all weather roads connectingthe zones to the regional capitals. Beyond the district capitals, most of the roads can onlybe accessed during the dry season.
Administration
Administratively, the country is divided into ten autonomous regional states which are
then sub-divided into 55 zones and more than 500 districts. The health managementsystenL follows the same set up. At the central level, there is the Federal Ministry ofHealttU at the regional level- the regional health office, at the zonal level - the zonal healthdepartment and at district level - the district health office.
The health care delivery systern, starts from bottom upwards with the primary health care
units @HC unit), the district hospital, Regional referral hospital and specialized centralhospital. The current health service coverage is about 45%o, that is, the population thathas access to health facilities.
Onchocerciasis endemicity
The existence of Onchocerciasis in Ethiopia was established in 1940 by ttalianinvestigators, in Keffa region. Subsequent studies have identified the disease to beprevalent in the western and southern parts of Ethiopia. The REMO survey, that wascarried out in 1997, showed that the population living in meso- to hyper - endemic areas is
about 2.5 million. These areas are isolated foci in south - western and north - westernparts of the country. The number of endemic communities is expected to expand after therefinement of REMO, by end of 1998.
36
Objectives
General objective:
To reduce the prevalence of Onchocerciasis to the extent that it will no longer be a majorpublic health problem.
Specific objectives:
l. To complete and refine REMO in the remaining parts of the country
2. To attain 80% CDTI coverage in meso and hyper endemic communities by theyear 2003.
3. To initiate vector control activities in selected endemic foci.
Strategies
1. Advocate support for onchocerciasis control at all levels.
2. Conduct training on implementation of CDTI at all levels.
3. Establish onchocerciasis task forces at different levels.
4. Appoint onchocerciasis coordinators at different levels.
5. Integrate CDTI activities into existing systems.
Administration of the programme
1. The NOTF has not been established yet.
2. The proposed composition of NOTF is as follows:
Head of Epidemiology and AIDS department - Chair person
National onchocerciasis coordinator - Secretary
NGDO representative - Vice chairman
Other NGDOs - Members
Regional onchocerciasis coordinators - Members
WHO representative - Member
LINICEF representative - Member
NGDOs
To date, Africare, Global 2000, Sight Savers International and Bahai community haveexpressed their interests in Onchocerciasis control in the country, informally.
37

Eth'opiaF inance Flow Chart
APOC/WHOWorld Bank Trust Fund
/I
Federal MOIJ.INOTF
Sisnatories:?
Regional HealthBureau
/I
Zonal HealthDepartment
/I
District HealthOffice
/I
Community? to be settled between
APOC & MOH
<- Fund Transfer* Reporting Flow
38

Eth'opiaMectizanFlow Chart
6 months
# Mectizan Flow* Reporting Flow
2 weeks
2 weeks
2 weeks
1 week
1 week
MSD(France)
MSI)(usA)
II
\
IFMOH
Federal MinistrYof Health
NOTFEthiopia NOTF
/I
RHBRegional Health
BoardI
I
ZILDZonal HealthDepartment
/I
DHI)District Health DePt.
/
I
Health Facility
CDDs(Community Directed'
Distributors)
1 week

EthiopiaReporting Flow Chart
---+ Report Submission
Community
Health Facility
/I
District HealthOffice
Zonal HealthDepartment
I
I
Regional HealthBureau
/
I
Federal MOHINOTF
/I
APOC/WHOWorld Bank Trust Fund
40 <- Feedback
41
sq
tdLE
U)0).-+i.l
.l+iCJ
o0tI.-tI.-GLFr-
aI
!sI
UU2.-lU2(!.-(.)li()Iot-Ia
I
o(:+)U).-
F]
ao
Er
0loEO.r.96clt-o()
-aEEU
ach o-)1a=7e)9 6-)-.C!c='oI-(CO(gC)L
c,3Z-2(, 6.) --c!6 (Jtr6o(got-
6?o)=cr=U 0)-E! e='<.>trqoO(q (.) l-
aaG)-a-=(J 6)-.crQG'oC(go(gorrE ..1 Fq
aao)ic.n=e c-)_.cr9 q '<-r
HCCO(!0)L
tha()ao=(J 0)-c
EG tlH(dO(g0)l-
a:j9)=th=e 0)-c!E'oqcgo(q()L:E ,.t ca
frEE
$)t=(/)oOEootrar U .- Viz> A
c!a'a u)
o!U)C5E (0
<'E i(
(d
ih u)
o'E(/)E5E (d
<.8 iE
ag'6 cr: .Yc0
=.i
E;T>;dii
0)thP
o.Y!o.(,=Er Q< fr.
ch ,,
GIA
=9.dE>IE
dAA
F',)C=t
(o<,(6A
.H€6l .l)Lr rrHA
et=oogotro.(, :.t
'f>o
oF9li ^\ U)
oE td
J>o
>EqrF 9l- ^\ l,)
oE (B
"35fi
HE ci5(utroE l.t
":5dIo&
t.!Eovv8Ed50JL6)AOI
cn
lZ v')otr3#oo!()
o>HE agotroE:1,35d
t6l(,o
l.]
(o-o(!
C)
(d-o(d-o
.9
CdpCd
-o
.2c0 0.ocg/, a)
th(g
cd .=OCtrNQ
-9o(!'E .=.e H- o
'J
q)
al&o
Fi
oc
o.oa
€6Ot
joo
a(!E$
Ica
c/)
Cg
$I
c.l
a
$I
ca
ah>.(0!$
Ica
rl,
!<f
tco
aaL
cl
Iclt=
*c,dtrU);
9.2L,r trOrO<()
uc0
atJrFz
Foz
friFozFo&
FoN
oo5UP_o()lJr
ET
ah
E6l
IhGltr
IEe>2..E I-'.eZs:-sda, L/€ELF
Foz
>.0.oU)o
AOp<
IJ.](ozrq&
CAh6)JA,Eo )
-q.r!4ctp<-r r+{ l- (/).e,A7EEXHE
0')--F0)
i: 8,ec6;2(u;Yc)trdc)..lEEEbEE oI)Eq̂)tr(rF.o(J(g-N
dE>Ab-c>.=oB
oU)do.9QBq)
E(.)
oG)trtr(dl-o0oh
o<
c.t
rq(o2rI]&
uCO
Ev).= .+rU0 O. -to o=c,&z
E;(L)i-lr C)
;\ 0)Eoo€cd.cAA(d):()Erd C).,8bEEo06e(H O<oAEH.Nto.E€>zb-c>.EA>
q)t/)(dc).2o3()Looo
ECIlrboo
c.l
(htro)
JZCd
F2 X.E bE Eo0 = >. irie,8,&,2
rq(osl
EeF(l)
u8,(L)P(dUr6C
EHEndG)-== .g Ea)E='<0)Uf g oo9be-(HO<voHo E=H
N
F,.A €o>zp. 9tjlc6'E
rrloin
OFIEsR=z
rq(o\<rzE]&
E;q'trFG)
:\ aitso0P(o,;EcdXC)EL(d 0.).,Eor iIEbo6e<*AorH.S>-o6-9'tzb.c>.=oB
0)U)(cq).2o<B.9L.q)
oo)EE(dl-aoolrA
(f|
onU
lI](oH&
b-11b:gi;
H;*F TE TJ]
-eEFo)
;\ C)Eoo#(d
iE(l)E(gQoECEbEEc06e
tHAoOH2n.0€>a!=o3
C)(r)Cd(l).gQB.9e()
oC)tE(g
boo
o<
\o

42
EDUCATION/MOBILIZATTON TARGET GROUPSEthio la
Target Group Level(Nat., State, LocalGovt.,Community)
Message/Information
Who willcommunicate the
informstion
Means ofCommunication
NOTF National EndemicityCommencement of the
Program
NOTF WorkshopsLeaflets
NOTF WorkshopsLeaflets
Policy Makers National Key Health EducationMessages
CRDA -Christian Relief& Dev. Assoc.
National Advocacy NOTF WorkshopsLeaflets
Religious LeadersUniversity
National Advocacy NOTF WorkshopsLeaflets
NGDO, Reg.Policy makers,Reg.Healthbureau
Regional Advocacy and BasicInformation
ROTF WorkshopsLeaflets
NlOtvMoEMOAAIGDO
Zonal Basic InformationAdvocacy
ZOTF WorkshopsLeaflets
Council/MOHMOA/MOEMOE/ReligiousLeader
District Advocacy and BasicInformation
DOTF WorkshopsLeaflets
Comm. LeadersTeachersRel. LeaderLocal Assoc.Health Workers
Community Basic InformationAdvocacy
DOTF WorkshopsLeaflets

43a
3a \ \ \ \
laz^ \
9a
o\o\
ach
*ai€\
=eEo.
{aEo\
iaL6€\E6,
Ea \
!a \
E.o \
lozo\ \
qG \
308 \ \
*a;€\ \ \
=B\ \
Eo;a, \
a6Es\
.ts8
trc)U)0)
(.,
.jian6tF
c)
q)
q)tr
o2rdil
c)
E<n
o 040tr.= GtEC)
LF
I
q)
tah
oFZri
I
ar)
an
ct
o6t
oU
I
L
q)t-
oFa.ri
o
c)
trB
I
fiFZ.r)
clqA
Hal
GlltroGz
q)
trEQaitrq)
a?a
oL
Qo
q)
ooq)
It
a0
GILFFQrf)
?trLooBO rtrC)a*.=-t€Elr.qFvz
I
(J
t-,)
oid
Gt
oN
I
3aaQ
I
qlcqCJo
q)
q)
(l
clz\o
()cq(,
c)
q)
C!
oa0o
I
c)()
(J
Lah
€Gt
NI
ctI
q)
c)
oU
l
FriL
aHFiFtsrFU
i
riz|tjE]t-a-t-riHFFzrdF

43b
6tdd
ol'.c!q)
6l
clln
a3e0a
E
{2
ea
Eo
!;3, E
.i=
Eo
i=\
g^3e \
S= \
E=
C2
LaO<e \
LaoE€
E=
E-.=
t-(JU26)e
I
.:ianGI
H
.Icq2 a)x9
Lq)
€:l()EEO9:=EIe,i
r-
AI€.ELtroc)!e/:t5.EEc)H
U)
€
u0
Loq)
o\
C)
c)t-(u
GTtru0oL
L.Egtr>.9 orcJ .=<tr-O
=€GI
F(
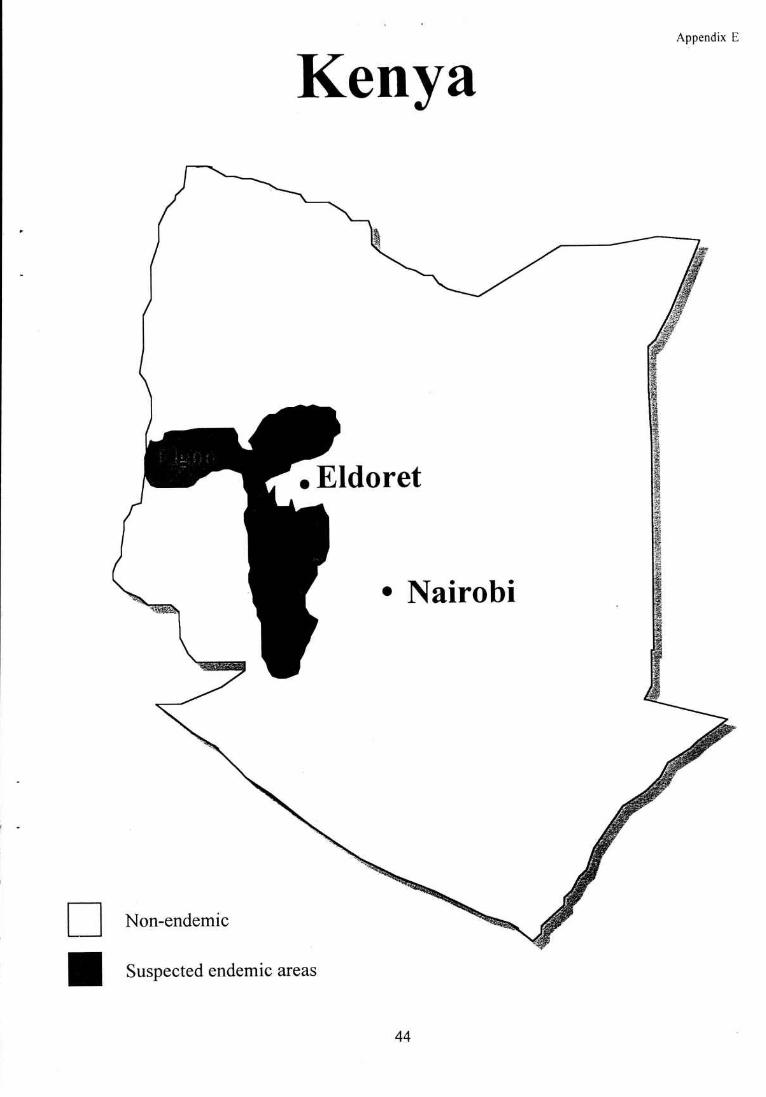
Appendix E
Kenya
. Eldoret
. Nairobi
Non-endemic
Suspected endemic areas
44
KEI{YA
General Information
Kenya is situated on the eastern seaboard of Africa, lying astride the Equator between 4o 30'N and
S, respectively and between 35" E and 41" E. To the south east is the Indian Ocean, Tanzania in the
south, Uganda in the west, Ethiopia in the north and Somalia to the north east.
Topography, Climate and Accessibility
The territory covers 58?,647 sq km ofwhich 13,096 sq km is water and 488,100 sq km (82%) is arid
and semi arid lowlands. The latter occupies the northern and eastern parts of the country.Approximat ely 90Yo ofthe total population (30 million) live in the highlands, the Lake Victoria basin
of Nyanza, Western provinces and on the Coast. This comprises 104,000 sq km (18%) of the totalarea of the country.The landscape is dominated by the south west higtrlands bisected by the Great Rift Valley, which runs
from north to south. Most of the rainfall occurs between March to September, with the short rains
in December. The dry season is mainly between October and March.
A central railway runs from the Port of Mombasa on the Indian Ocean, through Nairobi, Nakuru
and Eldoret to Uganda. At Lake Victori4 there is water transport to other East African Ports.
Road transport runs alon,e the main railway to Uganda.
There are several river systems with their sources in the highlands The largest of these is the Tana
which together with the Athi, drain into the Indian Ocean. Rivers Sondu, Nzoia and Yala run
westwards and drain into Lake Victoria, while Rivers Turkwel and Kerio run northwards and drain
into Lake Turkana..
Administration
Kenya is divided into eight provinces: Rift Valley, Nyanza, Coast, Eastern, North Eastern, Central,
Western and Nairobi, the capital city. The provinces are divided into sixty eight (68) districts.
The Ministry of Health is headed by a Minister, Permanent Secretary and Director of Medical
Services. It is divided into several Divisions, including Preventive and Promotive, Primary Health
Care, Curative Services and Environmental Health.
The control ofvector borne diseases, including Onchocerciasis falls under Preventive and Promotive
Health Division which together with PHC deals with prevention and control of infectious diseases.
Community Structure
The Districts are divided into Locations, which are governed by Chiefs. The Chiefs are assisted by
Assistant Chiefs, who govern several villages in each Location. Each village is represenled by an
Elder, who together wiitr the Assistant Chieiare elected by the community, while the Chiefs are Civil
Servants.In villages are women groups and cooperative societies, which extend to the district and national
levels.
45
Onchocerciasis Endemicity
Onchocerciasis was first detected in Kenya n l92l among the Kipsigis and Kisii communities livingin the vicinity of the well watered Chemosit and Kipsonoi, tributaries of the River Sondu.In an epidemiological study conducted in Kakamega in 1939, a prevalence rate of 50%owasrecordedamong 6l patientg detected. The disease occurred in the Kakamega and Kaimosi forests and in theTiriki and Nandi \ills, and further into the western plains as far as Marach and Buhayo.
Onchocerciasis occurs in the highlands, west of the Rift Valley, Nyanza and Western provinces inmore or less clearly demarcated foci. This is within an area of high rainfall and drained by the RiverSondu and Yala and their tributaries. In the south the areas affected are Bomet, Kisii, Kericho andRachuonyo while in the central areas Nandi, Kakamega and Vihiga are affected.The northern foci occur on Mount Elgon and the Cherangany Hills. The latter hills occur on thecommon boundary between Trans Nzoia, West Pokot, Uasin Gshu and Marakwet-districts.
Objectives:
To determine the prevalence of Onchocerciasis in the original foci and suspected areas.
To control Onchocerciasis using CDTI strategy and focal vector control.
Strategies
REMO/REA will be carried out in all foci and in areas within the range of the vectorSimulium naevei.
2. CDTI strategy to be adopted for control of Onchocerciasis
3. Focal vector control on the slopes of Mount Elgon in collaboration with Uganda.
NOTF
The NOTF will be established in January,l999, after the completion of REMO/REA.
2
46
I
I
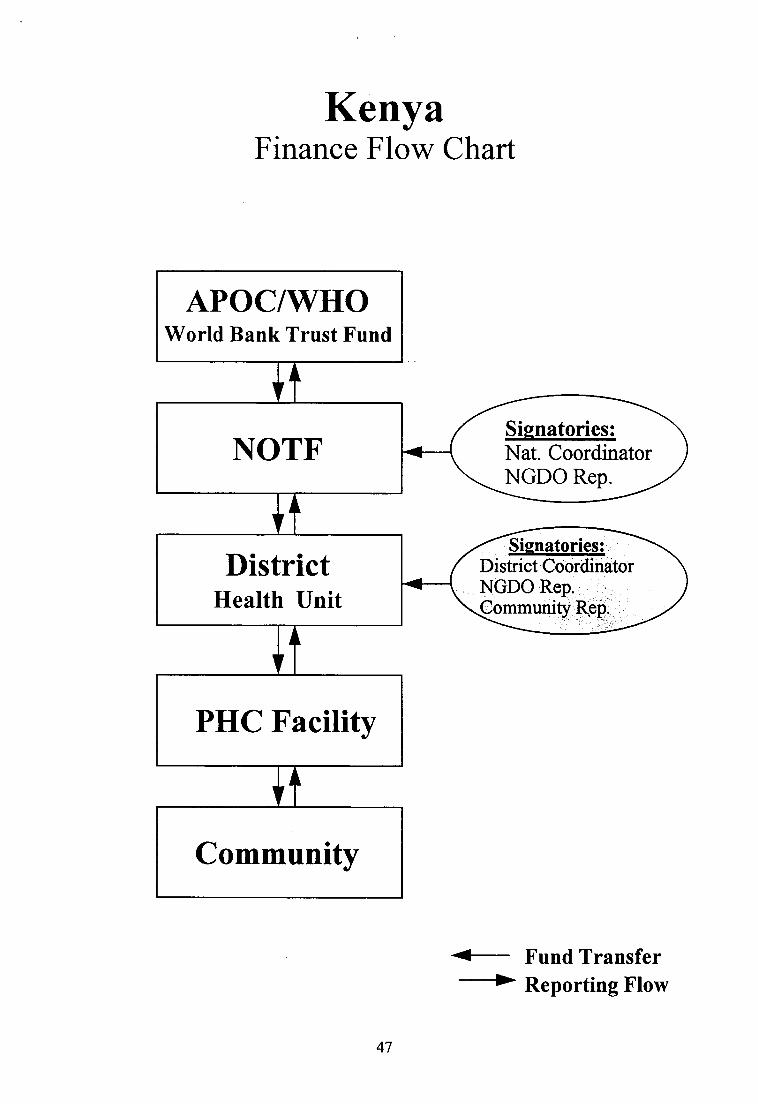
KenyaFinance Flow Chart
APOC/WHOWorld Bank Trust Fund
/I
NOTF Nat. CoordinatorSignatories:
NGDO Rep.
/I
DistrictHealth Unit
District CoordinatorNGDO Rep.
Rgp,. ,
Sisnatories:
II
PHC Facility
/I
Community
#_ Fund rransfer
47
* Reporting Flow

KenyaMectizanFlow Chart
1 week
L week
2 weeks
1 week
3 days
-1
I
I
I
I
I
I
I
I
I
I
I
I
I
I
I
I
I
I
I
I
I
I
_l
# Mectizan x'low-* Reporting Flow
MSD(France)
MSD(usA)
/I
\
I JKIAMSA Sea Port
EldoretKNOTFKenya NOTF
/I
MSCUMedical SuPPortCoordinating Unit
II
RMS DepotRegional Medical Stores
/I
6 months
District MedicalStores
/
I
FacilityIlealth Centre DisPensarY
CDDs(CommunitY Directed
Distributors)48
1 day

KenyaReporting Flow Chart
Community
/I
Health Centre
/I
DistrictHospital
/I
NOTF
II
APOC/WHOWorld Bank Trust Fund
* Report Submission<- Feedback
49
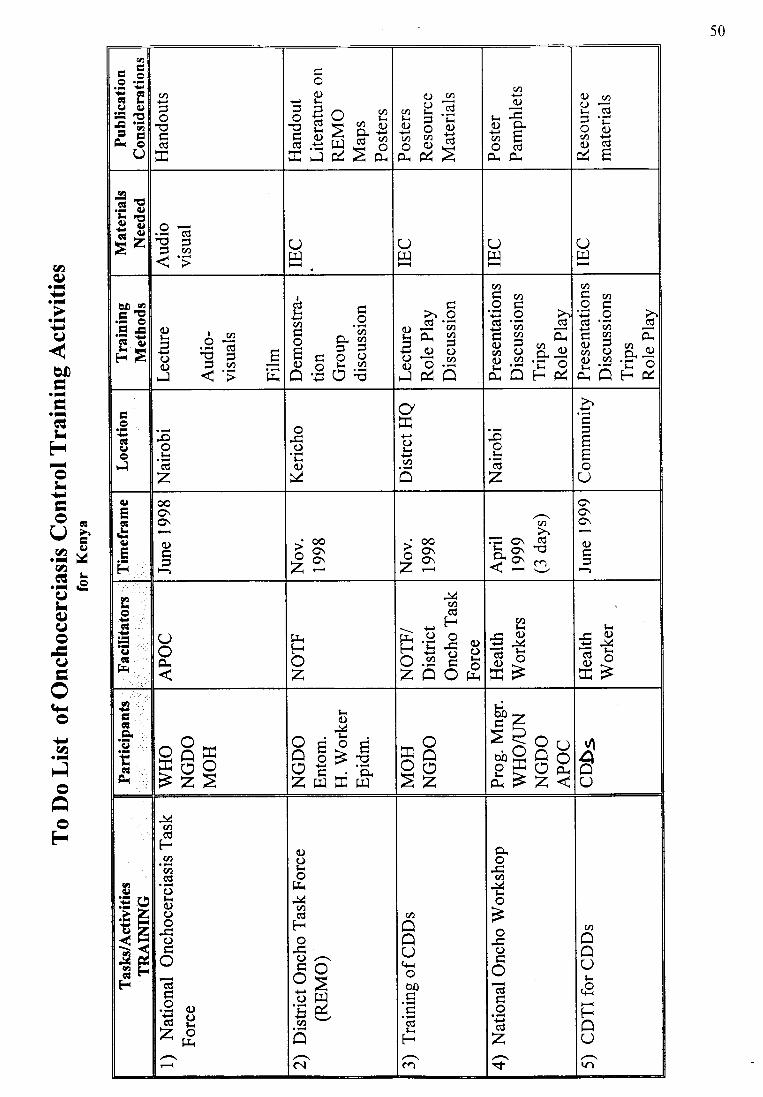
50
t,
U)
EEO.-t€EclL()c)=rc=nfiE
U
U)
o
(d
oC):) L.
i C^ aii co= a hE ba 3#S.E ll * o;jiF.] XZtu
c)(no=cnL.=E t b8rEA.&Z
aI
a)O.atrodOro.
Q)ao-r- Cg
oc)U)Pc;t<d&E
frEE
.9c'1,
==<n<'t Qtr.l
(Jrr.l
(JF]
(Jtr.l
.H€tl -rrF at)
-E FlFA E
fri
.i#'o=Av)<'i
(l)l<
o(D
El
ICdlJ l-.4.9E afr-t f )
EE9?,O.EOE
d
>rOd.isii fr
J{Jq)O0()= aS;E
U)l<aotr'5O>'c0 '= cd
!v)f; 3,^o.Ao7.i C)6) O.==.
&ElE&,
v)Laotrs'a str9 o.9 d 3 c)O t/).57&E15J,
AoclIorl
-oo.E
z
oOLov
q+)ot<(n
-oohcdz
>,l<
E
o()q)
ql,!q)
F{
00O,o\
otr
-' oo
2=-' oo<o\2z
U)
=O\ C0ho,-o
i"9 sr
o.6C)
i,L
cl
Iclf=
QoOr
friFoz
J4U)c0(r
!(
FE.f I^A=tiV.Hl-aAZAOri
v)(iC)+r -:(cd=(D *-Ef
l-r(i (!)':a
-YdXo..r Jfrf
,,EctEILGIti
oR:cEiEO>2>
lroil
.l-(.rcocnEli!/E:O.ZIA;E t! E9
L:!z> Q 6,,p8I H&Fz<
u1IQ
IErr.?ZizETHFrFr
J<n
c0FU)(n(0oa)oootrocdtr.9clHgZo' tr{
c)oo
trr.VU)CdFo()^c-o<66'E&'u)
-i5
c\
0ooOqrobo
trdl<F
ca
Ao(AJit-oBootroCBtrocdz.t
C')coOl-
€Fo()\r|
cl
oVLe
U)q).-{.).-
.l+J(J
o0AI.--I.lGLEi-oL!-L
Qa.-U2G.-ILq)c)o--I-Hot-o+.a.-F]oAl-lot'l
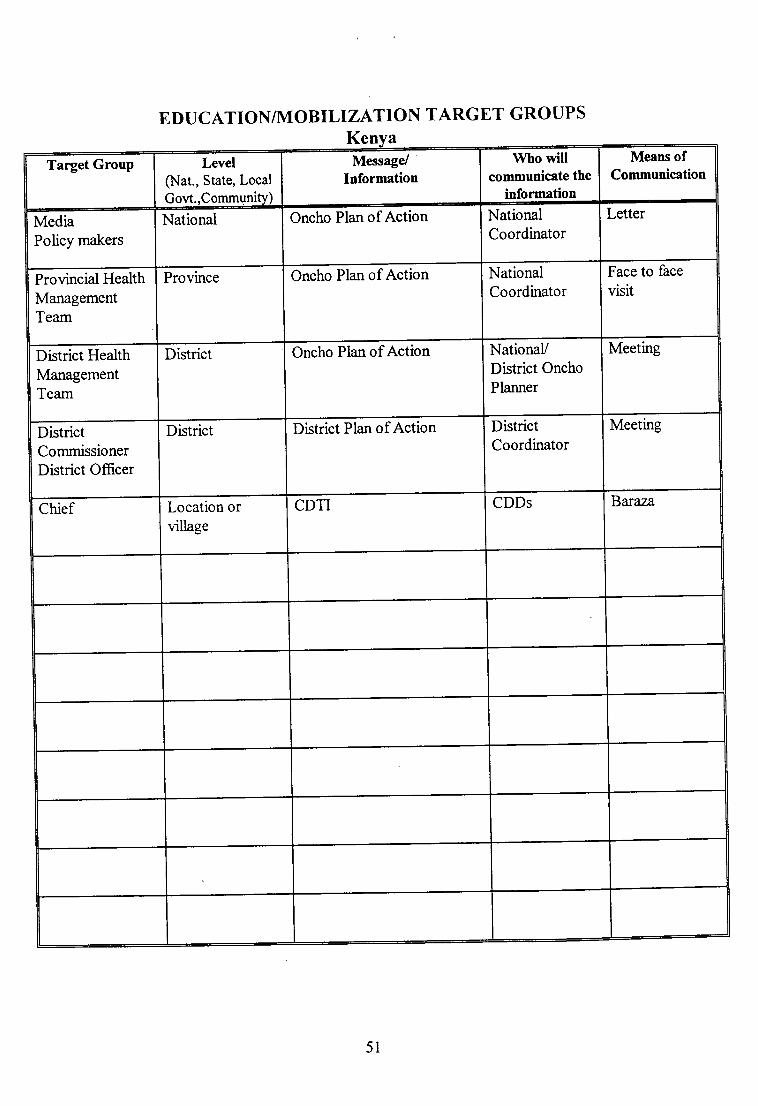
EDUC ATIONTM O BILIZATION T ARGET GROUPSKe
Means ofCommunication
Who willcommunicate the
information
Message/Information
Level(Nat., State, Local
Gow.,Commun!ryL
Target Group
LetterNationalCoordinator
Oncho Plan of ActionNationalMediaPolicy makers
Face to face
visitNationalCoordinator
Oncho Plan of ActionProvinceProvincial HealthManagementTeam
MeetingNationaVDistrict Oncho
Planner
Oncho Plan of ActionDistrictDisrict HealthManagementTeam
MeetingDistrictCoordinator
District Plan of ActionDistrictDistrictCommissionerDistrict Officer
BafizaCDDsCDTILocation orvillage
Chief
5l

25
a
Ea
laz6
9a
Ea
o\au \
Ea\ \
\ \ \ \
€aEo\
\ \ \
iaLc6Ea
\
Ea \
El \ \
3o \
ioz6 \ \
!- \
Gv)
E \
=6;6 \ \
aa;a
az
iro
frI.r2q)
h
I
!U)GI
t-{
rio!(arEl&
Iq)
o
DOtrhq)
oN
-arr]
6
clt
(r)
d(iO.iIG-Ccno-clzt
cq
-cqcqEotlcqzra
6l.t)
o(t
a) (r)q)Fi
or<
F{\o
6lqh
Orc
Error<
r-
6an
o
otho
a6
Eao
c!N
rr)trq)ao\
FzoDO
cttrF
orrrr5Cpoo'EEI:
GIlrFGI
(J
tr
c!N
U'rlq)
U)
(.)
o-tr6eN(ll .da);!Uazfr(.1
L
{o0
fr
trr-al-(aU.(l
zfrlVL
al.lrrlFrtl
rrtFU
xof-lzt-]r-'tTi-2.-:-r-'l-FFzrcF
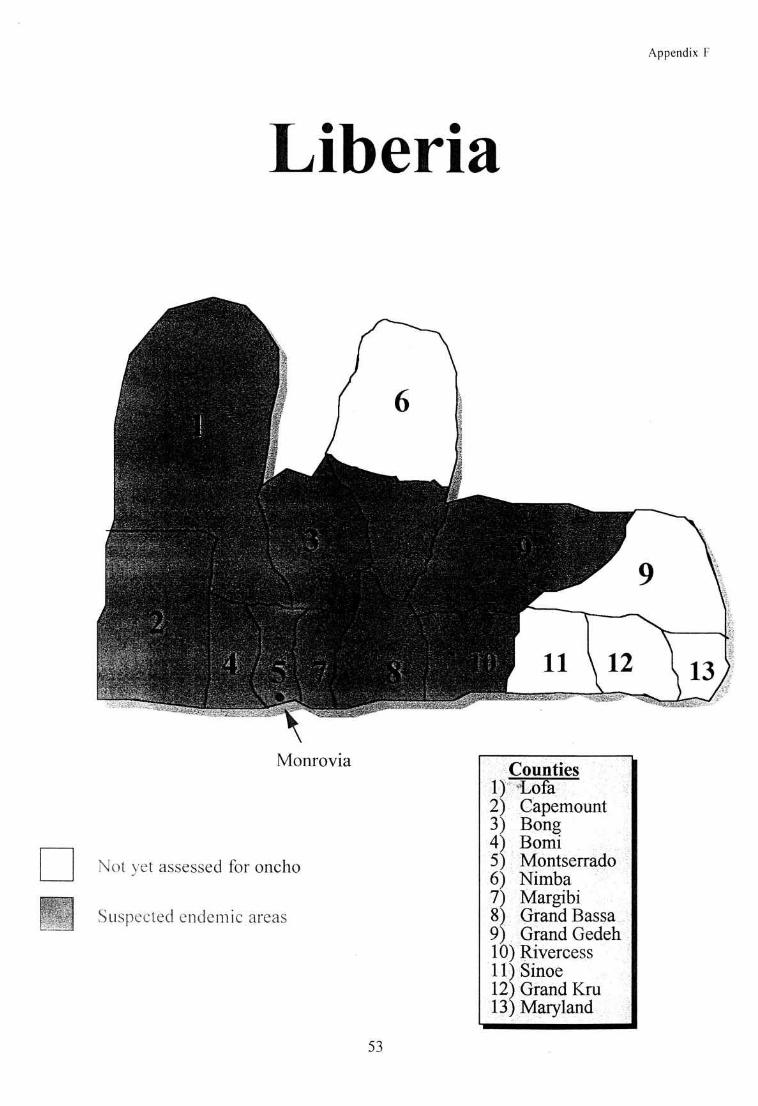
Appendix F
Liberia
Monrovia
Not yet assessed for oncho
Counties
CapemountBongBomiMontserradoNimbaMargibiGrand Bassa
SinoeGrand KruMqryland
2J4)
89I1
I
Sr,rspected endernic areas
53
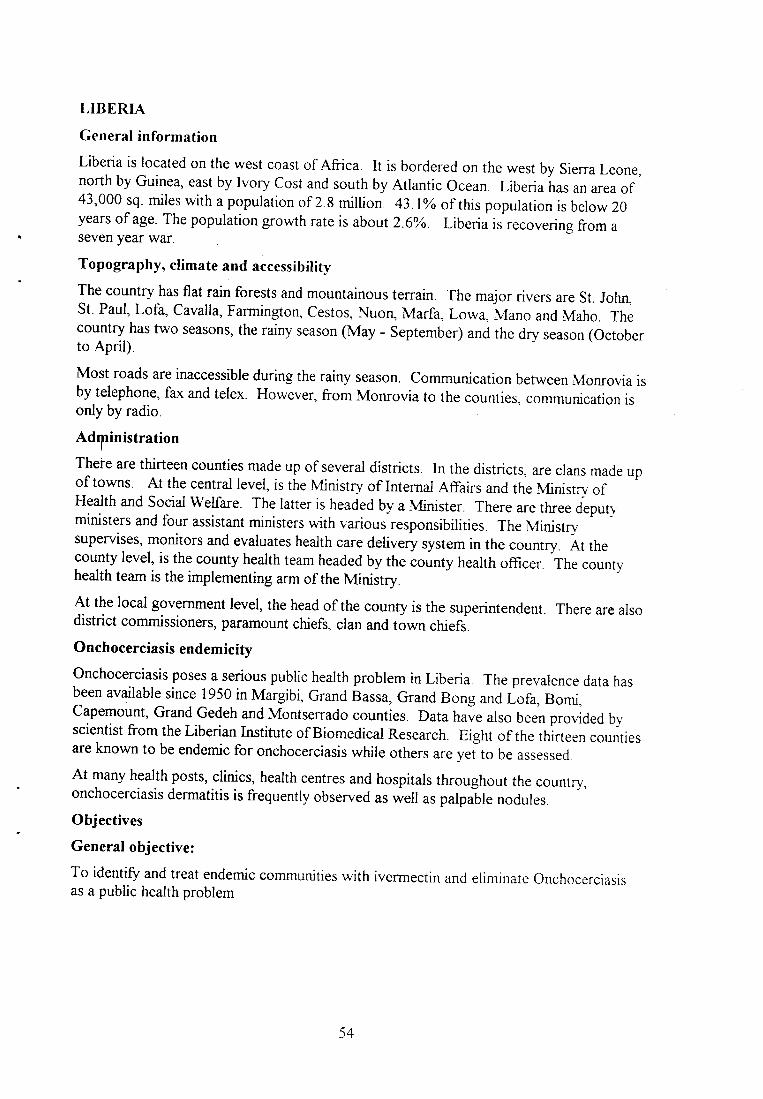
LIBERIA
General information
Liberia is located on the west coast of Africa. It is bordered on the west by Sierra Leone,north by Guinea, east by Ivory Cost and south by Atlantic Ocean. Liberia
-hu, un area of
43,000 sq. miles with a population of 2.8 million. 43.1o of this population is below 20years of age. The population growth rate is about 2.6%. Liberia is recovering from aseven year war
Topography, climate and accessibiliqv
The country has flat rain forests and mountainous terrain. The major rivers are St. John,St. Paul, Lofa, cavalla, Farmington, cestos, Nuon, Marfa Low4 Mano and Maho. Thecountry has two seasons, the rainy season (May - September) and the dry season (Octoberto April)
Most roads are inaccessible during the rainy season. Communication between Monrovia isby telephone, fax and telex. However, from Monrovia to the counties, communication isonly by radio.
Adlinistration
There are thirteen counties made up of several districts. In the districts, are clans made upof towns. At the central level, is the Ministry of Internal Affairs and the Ministry ofHealth and Social Welfare. The laner is headed by a Minister. There are three deputy-ministers and four assistant ministers with various responsibilities. The Ministrv.supervises, monitors and evaluates health care delivery system in the country. At thecounty level, is the county health team headed by the county health officer. The countyhealth team is the implementing arm of the MinistryAt the local government level, the head of the county is the superintendent. There are alsodistrict commissioners, paramount chiefs, clan and town chiefs.
Onchocerciasis endemicity
Onchocerciasis poses a serious public health problem in Liberia. The prevalence data hasbeen available since 1950 in Mar_eibi, Grand Bass4 Grand Bong and Lofa, Bomi,Capemount, Grand Gedeh and Monrserrado counties. Data have also been prol.ided bvscientist from the Liberian Institute of Biomedical Research. Eight of the thirteen counriesare known to be endemic for onchocerciasis while otherc u." y"i to be assessed
At many health posts, clinics, health centres and hospitals throughout the country,onchocerciasis dermatitis is frequently observed as well as palpa-ble nodules.
Objectives
General objective:
To identify and treat endemic communities with ivermectin and eliminate Onchocerciasisas a public health problem
54

Specific objectives:
I To determine the prevalence of Onchocerciasis in the country
2. To establish a sustainable CDTI programme
Strategies:
l. Awareness workshops at National, County and community levels
2. REMO training and assessment of endemic communities
3 Treatment of endemic communities using CDTI
NOTF
The NOTF is not yet formed but the Ministry has appointed a National Onchocerciasis
Coordinator.
55

LiberiaFinance Flow Chart
APOC/WHOWorld Bank Trust Fund
National
County
<- Fund Transfer
II
NOTF Nat. CoordinatorNGDO Rep.
I tories:
wHo Rep.I
I
CountyOncho Unit
County Health OfficerNGDO Rep.
'Control Off.
Sienatories:
/I
Health Facility
/I
Community
56
* Reporting Flow
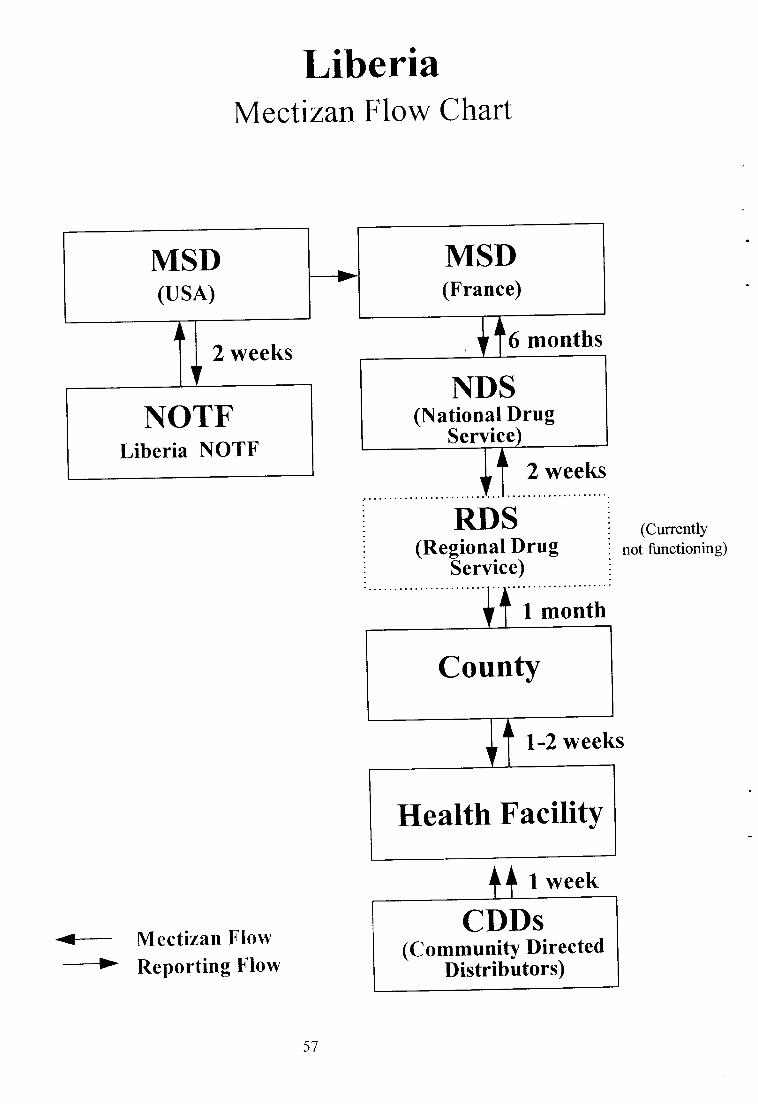
LiberiaMecti zan f low Chart
2 weeks6 months
RDS(Regional Drug
Service)
2 weeks
1 month
1-2 weeks
1 week
(CurrentlYnot functioning)
<-- Mectizan Flow
-* Reporting Flow
MSD(France)
MST)(usA)
\
INDS
(National DrugService)
NOTFLiberia NOTF
County
/I
Health Facility
CDDs(CommunitY Directed
Distributors)
57
t1

LiberiaReporting Flow Chart
Community
II
Health Facility
/I
CountyOncho Unit
/I
NOTF
/I
APOC/WHOWorld Bank Trust Fund
-_>ReportSubmission<- Feedback58

59
0
HC)
edCqL()0)
a20.6U
oo(,
co
CO
o0.)
9tr
lurJli*C6)()cd.= tr
H 'i AJ< El \J
0(.)ao=
o92a=q)I&z
aI
(Jo.AEOc€Oi O.
a)
.= 6)
sg;z
I
ALi!.= =i €HcSHtrL(-)(-6
LJdiJ X'-=F.] Efi5 3
Qtrl
(-)trl
()t!
a0 ,)tr€.iOtr-tr'FtFE
rhO.l-
o)
oa
O. ca
a\otra
O
oCg
C)a0.)L<
ch
;ia
l-< Agiv)00.)7,O.L .= 'r-A_HV9
otr'.= >. Od c0'=U_ii^AH-9cldp6.sEc4O
a
li \J
at-A
.RatA00)1a()6) A
do
6l
.sot-
o 9
(-)
I
E
q)
6lU()
F
=a.\ co cdtsorE36"n
l-: # \-/
ooA,,,^
t)
oq6Po)99
*p" Bi#o
ooo\o\
L<CS
z
a
=o\ cB
ko.Et.9 eU)LoG
Icq
'cjL.,O- c)A'r I
a.U SoQ. rt () f )E 658z> c <
Fz
FZ
ali
.a 0)'+, -Y
c) r-
a)
6l
()
LCq
a _C,l<e9E>T ? g,vtu 'e
6ese€8EeEE55$ E?BES H
l<0.)()E
>,o)LL9*t<;<P;H_.Y = (dHOoETL)IE
Ltl (,)E.V(D
-v
a
Q
41o.: \J>zetZd t-t-.,0 -'t,!, frk Et3
aa'5l-0.)(-)
()
oa)O
cdh5tLe -:Zcd rzr'7c6'- ?-^
ozr!
c.l
Ft-.,1(-)
ca
bo
'='6
L<F
aC)
$
C)
JL€
U)q)./+).-o-+l
CJ
b0aI.--L.-GLF-
IifI
Uu2.-U)€E.-I-(c)Ia-(JtI
\J+r
+)a.aF]
A-F

60
EDUCATIONTM O BILIZATION TARGET GROUPS
LiberiaTarget GrouP Level
(Nat., State, LocalGovt.,CommunitY)
Message/Information
Who willcommunicate the
information
Means ofCommunication
NationalAuthoritiesMOFVAgric.Internal Affairs
National APOC Philosophy of CDTIInformation about the threat
of onchocerciasis
NOTF VideoVisitGroup meeting
County Health I
Team and CGR(Country Gov.Representative)
County Information about oncho
Philosophy of APOCNOTF Visit
IECGroupdiscussions
Community Community Philosophy of APOCPrinciples of CDTI
County HealthWorkers
IEC materials

6l
,;llaz6
aa
a.aa
u_:eEa
aaE6
L€aEa
\
3e
a=
3o
lez6 \
q6
66a
€ \
\ \ \ \ \
Ee;a \ \
€6
I
E \ \
o.99
CJqq)
>.
(.)
!aac!F
Fz
At.tCJ
c{
6Z6l
C!(-
C0
Gz(r)
a€
oEdz.d.
O
Qal
L
rr)
c, ll
L
0
0a
0r-.
U)
za
aO
6
co
HU
.9Eq')Eac,Eq)6
(\'aCE
a
h
QU
GI
riF]
k:
aFFT
-rFQ
r-
r-'l-zJF1Fa-Fri
FFzr-'l-lF

Mozambique Appendix G
Indian Ocean
Non-endemic
Suspected endemic areas
Malawi
Tanzanta
o la
e
Zambia
Zimbabwe
GazaInhamb
South Africa 62
'-\ i,:'
I ''i l'' ,:-',, t.
l- r i'-a, l
{

MOZAMBIQUE
General information
Mozambique shares borders with Tanzania in the north, Malawi and Zanfria to the north-west, Zimbabwe to the west, Swaziland to the south-west, South Africa to the south andsouth - east and the Indian Ocean to the east and the north-east. The major rivers in thecountry are Zambezi and Rovuma,
The population is about l7 million made of Bantu and other races. There are variousreligious groupings made up of Catholics, Anglicans, Moslems and,Ziorletc. Subsistencefarming accounts for 7SYo of the major economic activity There is a high level of mobilityacross Malawi. A peace agreement was signed about five years ago, following a ten yearscivil war.
Topography, climate, accessibility
The vegetation is almost all savanna except for the Milange forest areas. The rainy seasonis frpm November to March and the dry season April to October. There are still a lot ofland'mines which makes access difficult. The roads are currently being rehabilitated.
-Colmunication between districts and provincial levels is by radio while the telephone and
fax gan be used in the provinces.
Administration
Mozambique has l0 provinces, each being is divided into distrios. Each district is sub-divided into localities and the localities sub-divided into villages. At the central level,therp is the Ministry of Health made up of National Directorates of Health. Under theseare fhe Provincial Directorates of Healttr, responsible for hospitals and health centres.
I
The'District Directorates of health are responsible for rural hospitals and health centreswhile the localities are responsible for health posts.
AII community health activities are carried out by indMduals selected by the community.These are trained for six months by MOH as community health workers. Their mainactiYities after training are health education for communities, mobilization and treatment ofsonle diseases that are locally endemic. By national law, these people are the only onesallowed to manage and administer drugs. It is therefore likely that these are the samepeople that will be used in this programme
Onchocerciasis endemicity
Knowledge of onchocerciasis in the country was reported about 30 years ago but was notdocpmented. The possible endemic provinces are Tete, Manica, Zambezia,Nampula,Nia$sa and Cabo Delgado. A survey in Milange district inZanbena showed thai thedistrict is endemic for onchocerciasis.
There may be cross-border considerations in areas bordering Malawi and Tanzania. Thepresence of other filaria infections have been reported in the country.
63

Objective:
To control Onchocerciasis in the endemic communities in the country
Strategies:
I Conduct REMO and review other relevant information that is available
2. Streamline structures pertaining to ivermectin procurement, delivery and
distribution
3. Integrate CDTI into the existing system of MOH
For long term sustainablity, the programme will use village appointed health workers. Therefugee populations have already been integrated into villages thus will require no
additional attention.
NOTF
This is yet to be formed. The NGDO's to work on the prograrnme have not yet been
identified.
64
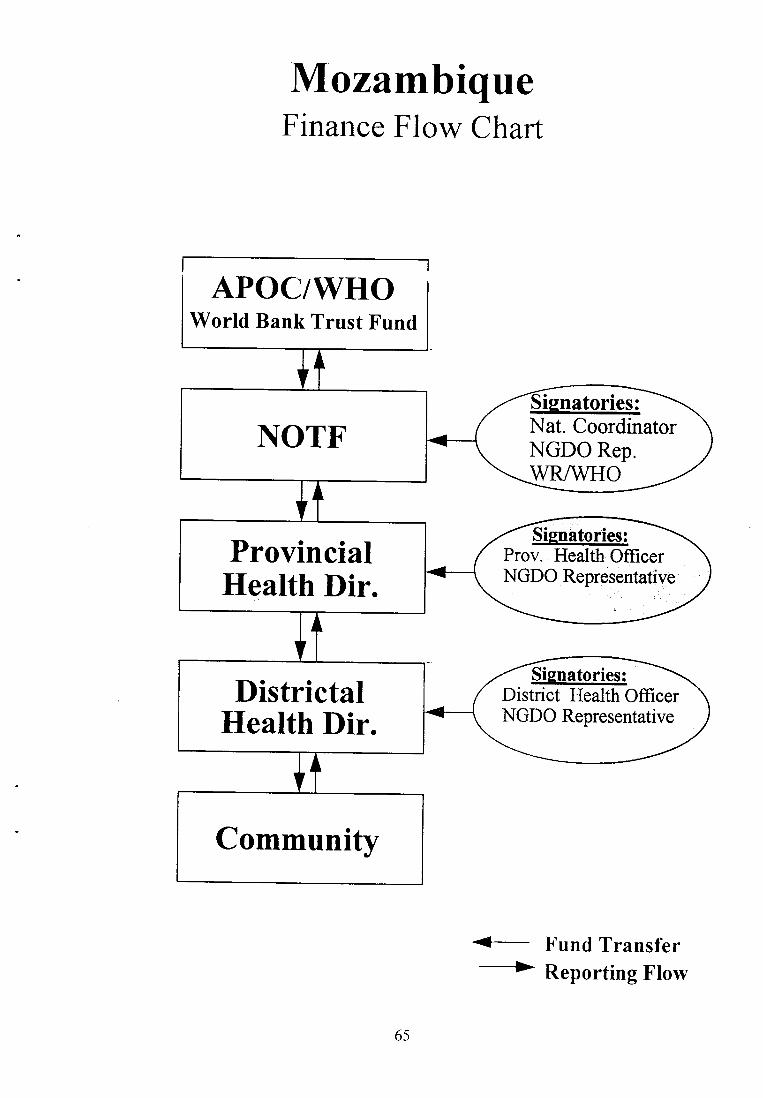
MozambiqueFinance Flow Chart
APOC/WHOWorld Bank Trust Fund
<- Fund Transfer
/I
NOTF Nat. CoordinatorNGDO Rep.
rgnatories:
wR/wHo/
I
ProvincialHealth Dir.
Prov. Health OfficerNGDO Representative
/
I
DistrictalHealth Dir.
District Health OfficerNGDO Representative
Signatories:
/I
Community
65
-----> Reporting Flow
Sisnatories:
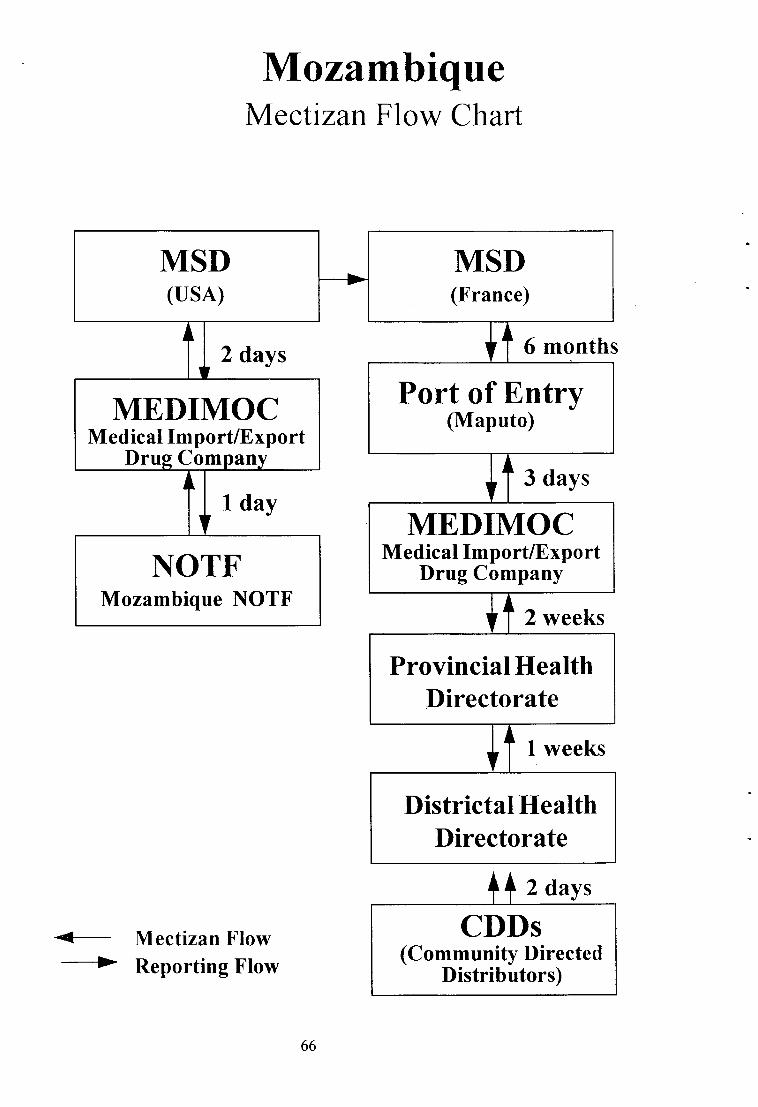
MozambiqueMectizan Flow Chart
2 days
1 day
6 months
3 days
2 weeks
1 weeks
2 days
<- Mectizan Flow-----> Reporting Flow
MST)(usA)
MSI)(France)
/I
Port of Entry(Maputo)MEDIMOC
Medical Import/ExportDrug Company I
I\
\ MEDIMOCMedical Import/Export
Drug CompanyNOTFMozambique NOTF /
I
Provincial HealthDirectorate
/
I
Districtal HealthDirectorate
CDDs(Community Directed
Distributors)
66

MozambiqueReporting Flow Chart
Community
II
DistrictLevel
ProvinciaLevel
I
/
I
NOTF
II
APOC/WHOWorld Bank Trust Fund
--->ReportSubmission<- Feedback
67
tl

68
q)
r'lN
e
U)o.-{-).l
.-+JI
b0aI.-dt.-cqLH-
t-+)dIoUU)
.ElU2-,.-aII0)CJ
/-()dtAvtr(
+JU).-IoAt-ot-t
0HO
ec{(LOo)
E=U
dzebor'io.= c)cs'ot-. >
cd
zElo r-
.H C)d-OF>
!C)
r<a'=!trHcd cg
F.l Q
atrC6
q.,;rO-aO
fugi
bt|i na
tr 0.)tr-oO=()O
OO-dCd
.5 0)cd;
l-F
3_.= o)
gEezia
U)fia
cdaA- O.= d!#V J HA|/r,(d<'i !E
arl (n
cB=A- O
.: cd!1,, ) Lr
=u)cd<'i E
cr.)t!)(€=.98€-
irJ)l-<
=u)cB<'iE
3€Y(h.1cdE,t-
r^r \JBEU.2H6>Eii
0.)
a .!lUL)d a(a4Lv().l5tgsEfr< Ar Er
aft -Y.= /-cd5(u ;ra=
.E',€AEFq)
_H liJA
t)\La!olg
-l LJi C).=oE cd6l .r LJ>m
ELa!o.)r yL,:U)H9V.r()E CT
0):- !-l>cQ
,F9ivE C).=o! d0) :* l-rJ>CQ
t-Y I
E ie$1FEE€o(,Jc4
a-Y
E aq#EdE€o(,Jc(
a_94Ytr(J
-'1-o tjl()Otoc>
t6lIoI
o)q(d
z
a,r, G)gBO':.r
_(jl?FHO{o.
aC)
A.=\J()z,E
-OaG)-
-c) .i-j!+{ V)
<c
I
#!0())l)Lio=f,EB<QE
-oq0);.i<..1 'E02;8E
otrcl&c)
F
ooo\o\q(.)a
oo
o\
o-. ooiorz2
o\o\o\
.oC)trr
o\o\o\
-o0)tu
O\/)r o.4a
?,,
6l
C.)
c(fr
'r- a
u)yu=\rtrO.O( t-r
;-afa
Fz
aFOz
9-
alr<Foz
E= EZ E EOTEF
E(A
Qo0r
U)
GI
C)
frGti
. .h-LJ.idic;\)QE:2;, I
rr bO
+O(!X c6(Hi.0)gZV v)
()
OO(-.,!AO:1oH.
(!.. (H
s)a;-(E.aat
r<(- (1 O)o riE_v?,EE:) o oiZOEf
4H
!voUt< H!b EEZl-,tu
thq)
.= \J>zeZi#9&e,)hcc(
F{
o.oaa -y,
a;.
Q7t-()c)ot
o(tAbo\JO
L<
cd r{
cdtr,2 (Jol)
()F
()
o()
ccn
o
o
(-.l
a
C)
u(g
a
zca
oF
cd0.)
L)k
iJa
$
(d0)F
cOC)
oQ\at
oo
ac0L<
Fo(c
(g
czIJt
I
l\O

69
EDUCATION/MO BILIZATION TARG ET GROUPSMozam ue
Means ofCommunicstion
Who willcommunicate the
information
Message/Information
[,evel(Nat., State, LocalGovt.,Community)
Target Group
VisitVideo/TVNews Paper
Radio
NationalCoordinator
Meetings and
Documentation
VisitVideo/TVNews Paper
Radio
NationatCoordinator
Meetings and
Documentation
National Leaders National
ProvinceProvincialLeaders
VisitsSeminars
Posters
National CoordProv. Worker
District Meetings and
DocumentationDistrict Leaders
VisitsPosters
District Dh. ofHealthA{OTF
Meetings and
DocumentationAdmin. Workers District
VisitsPosters
District Dir. ofHealth/NOTF
Advocacy and BasicInformation
DistrictPolitial leaders
VisitsPosters
Disrict Dir. ofHealthNOTF
Basic InformationReligious Leaders Communiw
VisitsSeminarsPosters
District Dir. ofHealthAlOTF
Meetings and
DocumentationCommunityCommunity
Health Workers
VisitsPosters
District Dir. ofHealth/I.,lOTF
Basic InformationCommunityTraditionalHealers
VisitsPosters
CommunityHealth Worker
Community MeetingsMidwives
VisitsPosters
CommumtyHealth Worker
Community Basic OrientationTeachers
VisitsHealth Education
messages
CommunityHealth Worker
Community Key Health EducationMessages
Groups at-risk ofoncho infection
VisitsHealth Education
messages
CommunityHealth \\'orker
Key Health EducationMessages
CommunityFamilies

t0
Fr2Nfr2,-
ar-lE
FFT
-FU
-z-Jf-lFa-Fri
FFzHF
il[il
\
iai-6
aa^6
s )a'ael
u^
Ea+6
E^
c62
\ \ \
of,e\ \
L<€\Eq\
\
E-.:;i \
!a \ \
!o \ \
ioz6 \ \
g6 \ \ \
6U) \ \
1aia \
=€ \ \
:€
a€
in
()qq)
<J
a)C!
F
(!CJ
FTa.f.l
ac)!tr>.=
Ad<aari
N
cq
Fz(-)
dri0.iQqtotr
clzt
€
-6€trolr6zia
6U)
c.EOqq
(J.a(,) t-(
\o
dU)
Ace) '-rolro
r*.
cllo
O0
a€
haqEr-q)0a-t- cqa.9u0EEq)AZ6t
Fo\
tr6\Jc
ao€trqJL
(]
q)
c!
(,)
L
aii(€ooc)2-z
(\t
!NcE .-:,c)5c)EEfr?.)
o
0)
e
q)
\o
€
t
Appendix IJ
SouthernSudan
Aweill TwicGogrral
Raga
l--l llt f|-!r-f:r U
l1
E. Equa
Lakes
SOUTHERN SUDAN
General information
South Sudan is bordered in the west by the central African Republic' in the south by
Democratic Republic of Congo ura ugunJa' in the east by Kenya and Ethiopia and in the
nont, the bo.rrrJary is contentious a::f, :l!-defined
Topography, climate, accessibility
The water flow is mainly towards the white Nile in the north-eastern direction in the
south-western area. The latter is divided into:
i) Southern water shed zone (Nile/ congo divide) o-f forest and savanna with good
annual rainfall and fertile soil. There i-s a gtadual slope of streams and rivers
iD lron stone plateau zone ( intermediate) of savanna with unreliable annual rainfall
andshallow,oironironstone.Streamsandriversarefastflowing.
iii) Alluvial plains towards Bahr El Arab (10 N) and White Nile (33 0 E)' Grasslands
with patchy;;;, unreliable ranrurt-una flat alluvial plains with wide shallow slow
flowine rivers'
There are two main seasons. The dry season (Iiovember-- March) during which fishing
and hunting activities occur and the *.ir.uron (April - October) mainly for farming
activities.
only one all season road exists ( western Equatoria- Lakes); most roads being seasonal
due to destruction of bridges, lack of maintenance or military barricades resulting from the
war. Access by OLiAS Indsenio. Snne tturis possible by air only from Kenya' Four
wheel drive vehicr.rl*o,otuikes and bicycles are used internally' But by far the
commonest means of transport is by foot'
Administration
Southern Sudan is divided into six regions each consisting of a number of counties'
Except for upper Nile, these regions u,..*t,ouy ( Western_Equatoria and Lakes) or largely
controlled by the Sudan Peoples I-iberation Mo"*tnt (sPLIvD Each county.consists of
a number of Payams each of which in turn is made up of several villages' civil
administrative structures have been set;;f1.* the village.level ( Village Councils) to the
national level (National Executiu. CounJifi. In additiof tf SPLM has a humanitarian
wing, the Sudan n ri"i-a Rehabilitation,{ssociation (SRRA)- Together with ols/ss
and other NGOs, this body is responsible for relief and rehabilitation actirities
Health services are delivered by oLS/SS and other NGOs in coordination with SRR*A
health sector headed by the Chief SRRA coo.ainator. Delivery is through the PHC
system which still requires complete structural development in some areas' About fwenty-
72
three NGOs are involved in the delivery of health services in the SRRA accessible areas
However, due to the war situation'this number of NGO's fluctuates
Community structure
Many ethnic groups, subsistence economy is related to zones of permanent residence;
i) Sedentary farmers found in the southern water shed zone
ii) Mixed sedentary farmers/fishernerL hunters and semi-nomadic pastoralists found
in the iron stone Plateau zones.
iii) Semi-nomadic pastoralists found in the alluvial plain zone.
The leadership structure is principally the same for these groups and consi:l o-f u
paramount chief with several exetutive chiefs below him. The executive chief rules over a
number of sub-chiefs below him, each of whom has several Gol leaders (headmen) under
ni.] n.iig,ous leaders, women associations and traditional healers are among the
influential social grouPings.
Onchocerciasis endemicitY
Onchocerciasis was first reported by Bryant in 1933. He also associated it with endemic
blindness in Bahr EI Ghazi and calied ii "Jur blindness" because of it's prevalence then
amons the Jur and Balanda tribes near tributaries of the Jur river (Bryant1935) By 1959'
more foci had been identified and reported in Bahr El Ghazal, Western Equatori4 Upper
Nile and Jonglei. Further investigations in the 1960's, 1970's and 1980's confirmed
former findings and revealed additional foci in Lakes and Eastern Equatoria regions' It is
therefore clear that the disease is prevalent in all the regions of South Sudan with a total
population of about 2.5 million persons at risk. However, the magnitude of the problem
remains undefined as epidemiotogical surveys done so far have covered seleot
communities onlY.
Objective
To control onchocerciasis by mass annual ivermectin treatment in endemic communities
tkough APOC PaternershiP.
Strategies
Determination of onchocerciasis endemicity levels
Establishment of sustainable CDTI project
NOTF
To ensure sustainability and full coverage of all SRRA accessible areas' a New Sudan
Onchocerciasis task force ( NSOTF), a partnership of SRRA and NGDO's is to replace
the SSOCp Field implementors *iilbe included in the NSOTF' Health Net International
(HIII), the principat Ncoo shall be the NSOTF coordinator and shall represent it in all
NOTF cooidination meetings. The NSOTF shall be located in Nairobi, Kenya'
73

Southern SudanFinance Flow Chart
APOC/WHOWorld Bank Trust Fund
/I
NOTF Nat. CoordinatorNGDO RepWR/WHO
ignatories:
/I
NairobiIlealthNet Int.
Sisnatories:HealthNetNGDO Rep.
/
I
NGDO/SRRAHNI Store
/I
CountiesNGDO/SRRA Store
/I
PHC Facility
CDDs(Community Directed
Distributors)
+_ Fund rransfer
-> Reporting Flow
14

Southern SudanMectizanflow Chart
3 months
I -2 weeks
I -3 weeks
I week
1 week
<- Mectizan Flow
MSD(usA)
MSD(France)
II
\
\
NairobiSchenker AgentNOTF
Health NetI
I
LokiHNI Store
/I
CountiesNGDO Store
/
I
PHC FacilitylPayam Store
CDDs(Community Directed
Distributors)------> Reporting Flow
t5
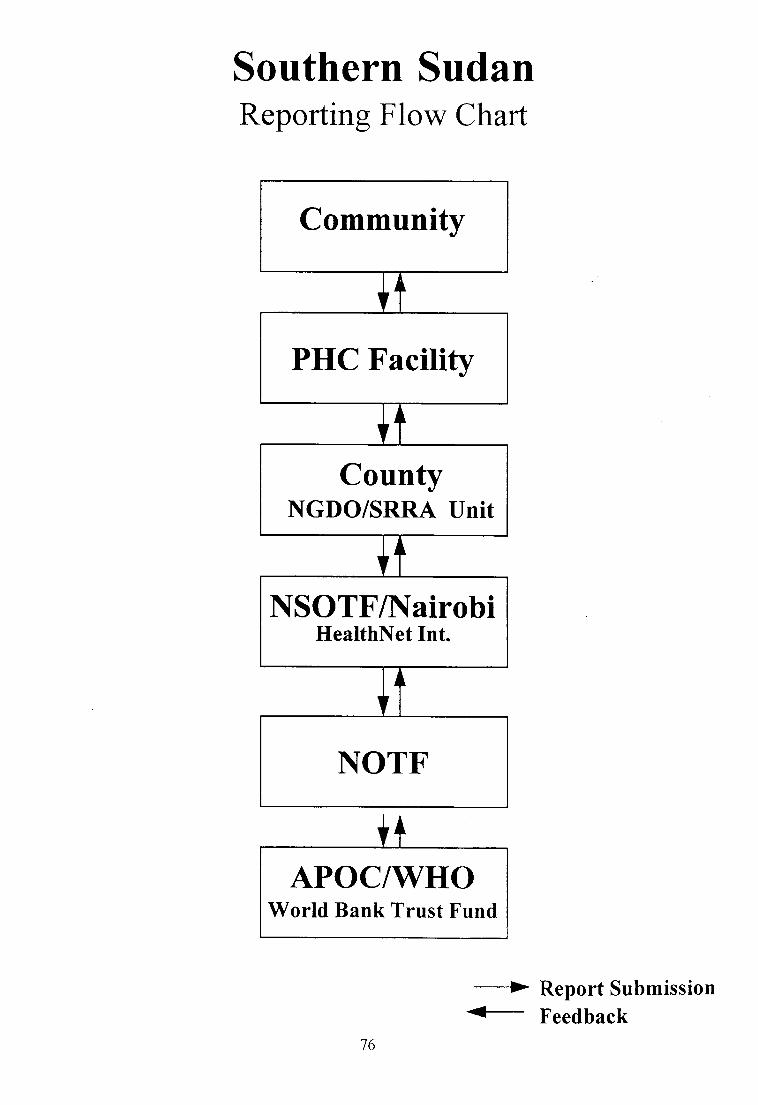
Southern SudanReportirrg Flow Chart
Community
/I
PHC Facility
/I
CountyNGDO/SRRA Unit
/I
NSOTF/NairobiHealthNet Int.
I
I
NOTF
--> Report Submission
# Feedback
APOC/WHOWorld Bank Trust Fund
76

77
0
HOo.-+. atlCl Liq)()
=r)iEU
a
oE
CdF
frgE
a
Oc6O==0.)Y aE
).a.d
a
oEEA
Hh.;: o&ootrEEld r
EO,|EE.-Otr .E.FE-L. tsr?A
Lo:)(d
oL(d
Ar
oaO. u)
9A\J'O
oO.o(€tu
ocdO.o-bofu trr
(do+)o(€L
oGCJoFl
-oolrcdz
!oJ
o*'E al-(Dtrg)! )668
.9adC)trboo(tfi>
q)
6l.Lq)
F{
0) xU)
bo)Ia.C)a
ozrr,Lro6l
q)6lfr
QF"6F-i,oz<2fr
.9N
Uq-H MX ,7 ..'o?EA>
EobEbo'r=(t)(oez o
(-)
OY<?>
rn
tr6lq(,trcl
F.{
l-rocd (n
.=t E 5 aE.2VFr\rh1_e&UYL'L'V)AA
,hlEyl(') u)-c-ci<i'EEp.E E{ i XE -
{-)Ado(+io Eoirr-U!H*;rpHH,^A cd tr 63,-ro (I) o o\-/(J!EQfrZ
a.l Oooccd 0)
>+v\) F: a(JEEbL.l o oll>QOrr.l
atc)
.: l,..7c,l Zdl-<<ied^fFrFr
aJ
&az(d
oCdz
cd
oooo)
d.,
c\
Ic)o
(-)
en
2-r
o()$
oI!r',
ta)
Gl
(n
t-q)
oaL
(r)q)
o-+r.-.-*lI
b0aIt./tI.-Gl.F-litsI
U0.lU2G
o-(JliG)C.)
arI()at
^q\,(rr
+.a.-l]
A-toi'{
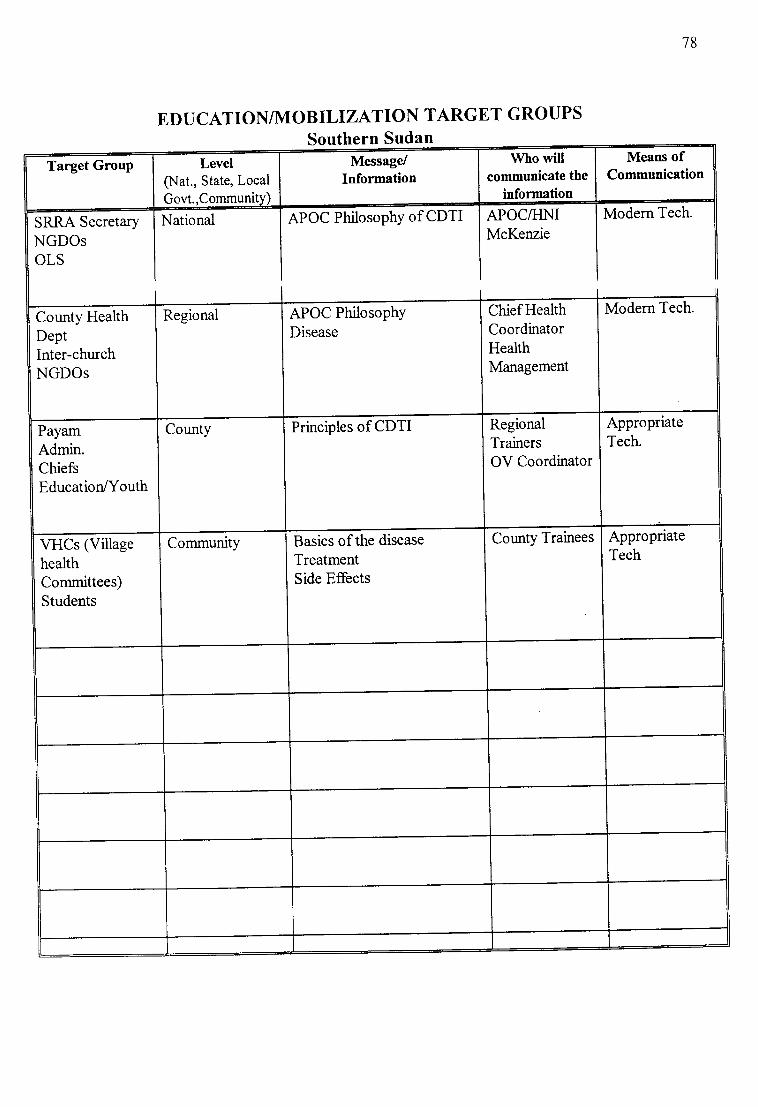
78
EDUCATION/MOBILTZATION TARGET GROUPS
Southern Sudan
SRRA Secretary
NGDOsOLS
National APOC PhilosophY of CDTI APOC/HMMcKenzie
Modern Tech.
Mesns ofCommunication
Who willcommunicate the
information
Message/Information
Level(Nat., State, Local
Govt.,Community)
Target GrouP
Modern Tech.Chief HealthCoordinatorHealthManagement
APOC PhilosophY
DiseaseRegionalCounty Health
DeptInter-churchNGDOs
AppropriateTech.
RegionalTrainersOV Coordinator
Principles of CDTICountyPayamAdmin.ChiefsEducationlYouth
AppropriateTech
County TraineesBasics of the disease
TreatmentSide Effects
CommunityVHCs (ViilagehealthCommittees)Students
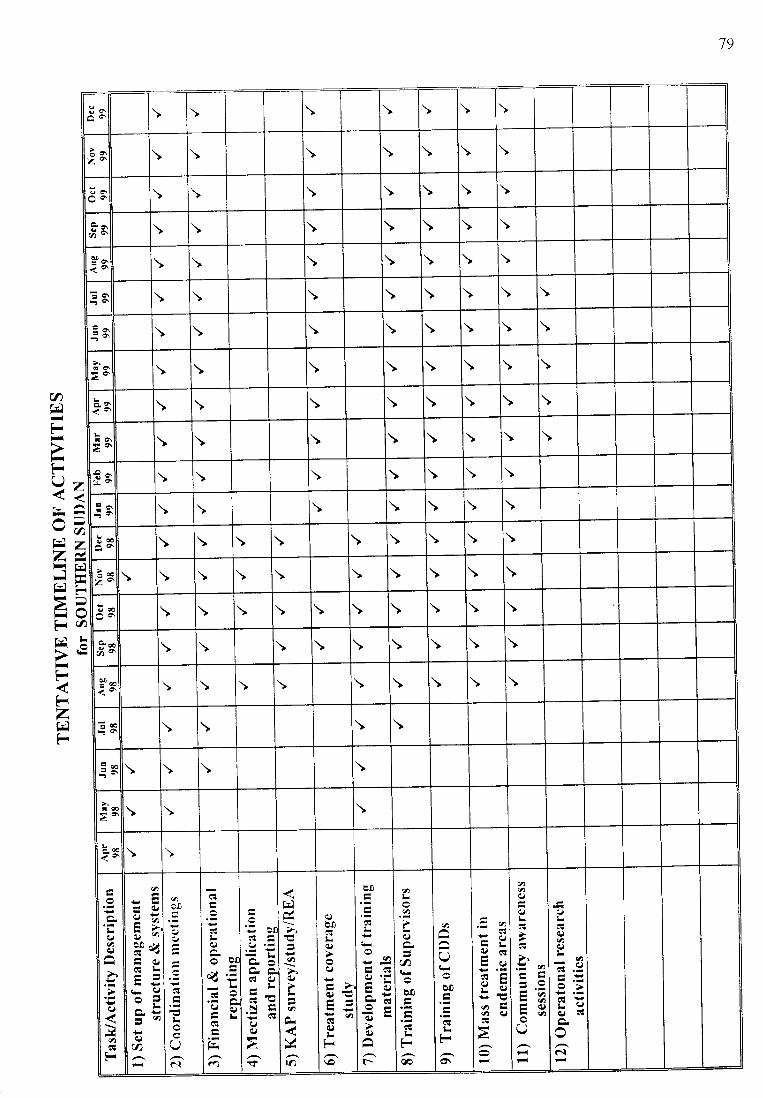
79
z
=azr-l
F=Otr€
U)tiFtl
-FU
rdzjHFaFTFrd
FF-zHF
3a^6
\ \ \ \ \ \ \
iaZ6 \ \ \ \ \ \ \
UA \ \ \ \ \ \ \
o\6o \ \ \ \ \ \ \
606 \ \ \ \ \ \ \
=a \ \ \ \ \ \ \ \
Ea;a \ \ \ \ \ \ \ \
daE6 \ \ \ \ \ \ \ \
oEe \ \ \ \ \ \ \ \
LdO\>o\ \ \ \ \ \ \ \ \
!a \ \ \ \ \ \ \
aa' \ \ \ \ \ \ \
Eo \ \ \ \ \ \ \ \ \
loZ^ \ \ \ \ \ \ \ \ \ \
q6 \ \ \ \ \ \ \ \ \ \
\ \ \ \ \ \ \ \ \
9-i6 \ \ \ \ \ \ \ \ \
;a \ \ \ \
=6 \ \ \ \
a€2 \ \ \
6a \ \
Iaq)
q)
.jlq)(qF
a
oa
€q,)
c,)
q)
q)E!
cl
Ia
ait
q)
d
Uc..l
q,)
€q)
.t
CqN
Iq)
zs
q)
q)
P
o
rr}
q)
cs
q)
q,)
0)
C\toF\o
co
y3
Eq)
()
r-
.'0
Ec)
a
oo
cq
F€
a
Q
E!
€Fo\
.=q
trEC)GEU
ic)!tqj q)
2.
qqo
.:0trtr=.9tra)tr()U
IL6q)qq)
U)
cl '!n
c)cll
(\l

Appendix I
Alrican Prograrttttte titr Ortcitoccrciasis Corttrol (APOC)Proqranrnre africain dc lLltte contre ['onchocercose
JOINT ACTION FORUIvI
Office of the Chairrnan
JAF'-FAC FORUM D'ACTION COMlvl UNE
Bureau du Pr6sident
JOINT ACTION FORUIVI
l'.,ird sess^orr
Liveroool. 4-5 December 1997
JAF3/INF/DOC.8r^'^y\rl,
rll\ii. )LL
OCTOBER I997
APOC PROJECTS MONITOzuNG FORM
80

JAF3/INF/DOC 8
Pagc I
Bockgroutd. This document is a forrnat tbr Monrtoring CDTI projects. The background intbrntation or.r
Evaluatton and Monitoring tenns is explanatory, necessary to understand the process used in dcvelopin_umonitortng indicators. You may rvish to skip this section and refer drrectly to the Monitoring Forms if you arefanriliar ',vith the differences as rvell as gray areas betrveen the two terms.
Prograntnte evaluation otletttpts lo cletennine the cortgntetlce between petfornnttce (i.e., what occurretl)attd llte rtb,iet'lit,es (i.e. y'ltQt tt,o.s rrrnnnqp,l lo occtrr.l nrrrl ln irnlnto Iho gnlrn/cl nf n "^o-ifir, .ttt-^,',.' /.,11
pt'ogt'Qtttttt(ltic change.s.. outputs, elJeus, ancl intpacts). Programme evaluation focuses pnncipally, although notexclusively, on internal validity of the programme: did this programmc rvork in this setting, and did it producethe observed change?
One assumption in programme evaluation is that the model or theoretical basis of the intervention has beenconfirmed by previous evaluation research (in this case the TDR multi-country study).
There are three interrelated levels of the general characteristics of evaluation which are described rn table I
belorv:
Table I : General characteristics of levels of Evaluation
Ler.el
l. Process evaluarion: Programme Qualitl, AssuranceRevie*'
Selected general characteristics
Applies non experimental designs
Assesses operating procedures
Examines structure and process
Conducts observational analysis
Performs qual itative observations
Monitors efforts-activity
Reviews-audits data and records
Applies quasi-experimental and expcrimentaldesigns
Assesses behavioural impact
2. Programme evaluation: Effectit,eness Assessment
Uses non-random or random assignment
Emphasizes internal validity
Uses simple analysis and comparisons
Applics tested interventions
3. [:r'aluation resc:trclr Appl ies expcrimental designs
Uses randomization and controls
Tests hypothesis on bchaviour chanqc
Uses multivariate analyses
lmprovcs knorvlcdgc base
Is groundcd in thcory
asizcs intcrnal and cxtcrnal vllidr ty
.IAIT3/INF/DOC 8
Page 2
MONITORTNG
Definition: "Periotlic collectiott artcl atrolys'is of selected indicators to erruble ntonager:i to determine wltethet
key activities are being corriecl out as planned and are lnvhtg the expected effects on tlte target populaliott".Monitoring is herern considered as process evaluation.
Objectives of utorritoring CDTI projects.
(i) to provide t'eedback to the NOTF and the APOC management on CDTI implementation,(ii) to improve operational plans for CDTI,(iii) to assist the NOTF and APOC Management to identify strengths and weaknesses in CDTI
implementation and to apply if necessary corrective measures.
Scope of CDTI project fu[onitorirry
(i) Target area: CDTI specific project areas'
(ii) Faciliries:- Drug delrvery circuit (port to distrrct)- Involvement of the health services- Comn-runiry mobrlization- Collectron of rhe drug by the communir'- (cost covered by'the communlr\')- Trainrng of CBDs- Dtstributton of ivermecttn- Supervrsion- Reporting and leedback to communiry
(iii) Pers orr nc l:- NOTF personnel from central level to the communily- Health workers at various levels- Administrative officers at dislrict ievel (financial support to CDTI)- Community leaders- Communiry dtstributors
(w) Duration of ntonitorittg
Three options on the duration of monitoring are suggested below
for as long as project is funded from APOC Trust Fund (5 years).
as long as CDTI implemcntation is necessary (longer than 5 years).
fbr 3 years and discontinr-re monitoring if the project performance is considered as satisfactoryand rn addition the n-rediurn-term evaluation shows a similar lrend.
(i)( ii)(iii)
Indicalors
For tht'i)Lrrp()sc ol.ntonitoring CDTI pro1ects, the team identrfied and defined three categorres oIindicators namell,: eltect. output and input rndicators. Qr-restions rvere developed covering the three indicatorsas prese nted in thc Atrncxes below.
Definitiorts of rlte rlrrea indicators foltl[ottiroring
l. Effect indicators
Effects are defined as the knowledge, attitude, and behaviour/practice that result from the outputs82

JAF3/INF/DOC 8
Pagc 3
t .I . behaviorrt'/coveruge ( comniunity particrpatiort. coverage)
1.2. knowledge (Knorvledge of why taking ivermectin fbr many years is inrportant)
t 3 .skills ( appropnate skrlls developed by the actors in CDTI)
., n"+'..'+ i-rlinafrrrc
Outputs are immcdiate prodr.rcts and services produced by the programmc
2.1 . utilization o.f'sen,ice (acceptors/users, pro.;ect continuation, drop-outs. cost)2.2. clualitt, of CDTI service (management of cases, education, contacts. access to CDTIl
3. [nput indicators
lnputs are resources needed to carry out CD'fl activities
3.1 . persontrel. (manporver developed at vital levels for CDTI implementation)3 2. Logistics ( iunds. ivermectrn supply. transportation etc)
3.3.reporting (ararlabrlinoimatenalslorreportrns-notebooks.tbrms.summan'booksetc)
83
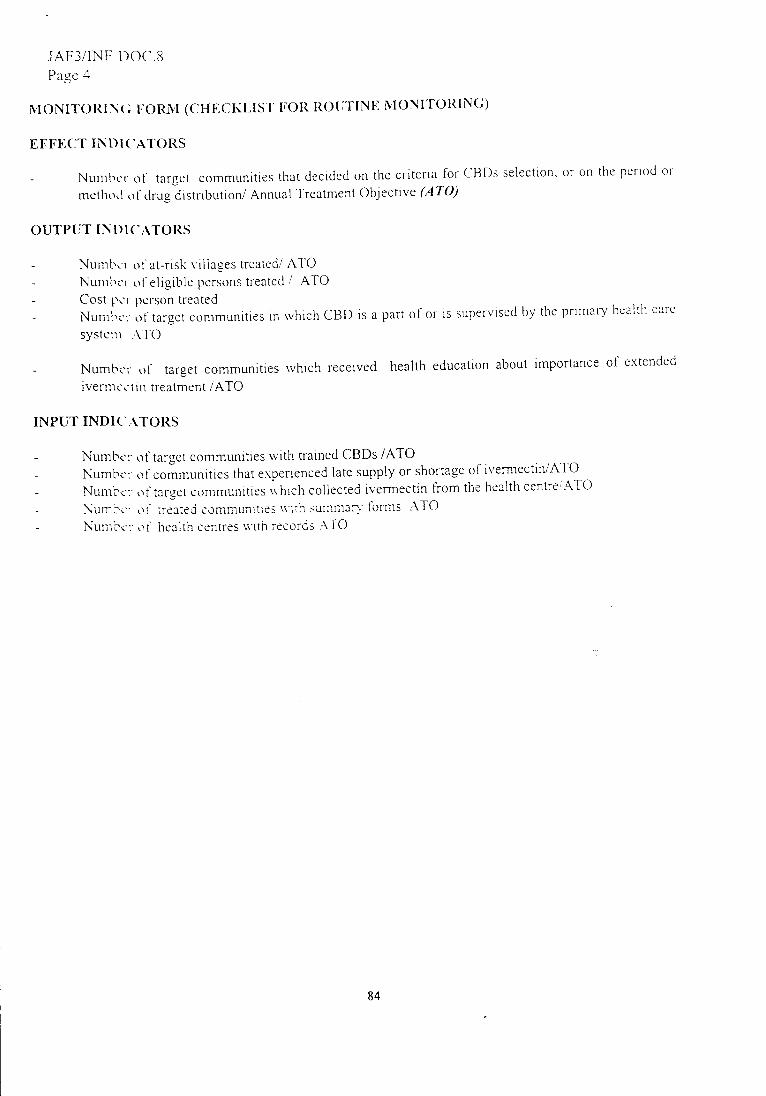
iAF3/tNF r)OC.8Pagc .1
iVI ONITO ITI \ ( ] IiORr\I (C] I{ ECK I, IST IIO II I{O Ti'I' I N E N I ONI'IO RI N G)
EFFECT INI)l(-r\TORS
Nuu.rt.t.r ot' target communities that decrded on the critena for CBDs selection, or on the pcrttlcl or
nretlrt'.I o t' cirug ciistribution/ Annual'lreatment Oblective (A'tO)
OUTPUT INI)I('ATOIIS
Nunri..'r ot'at-rrsk r r[[ages treated/ ATONunri.i'r trt'eligrble persons treated / ATOCost p.'r [)crson treated
Nunrt.t.r ot'target conrmunities rn rvhich CBD rs a part of or is supervrsed by the pnnlary healtl'r carc
systeru \TO
Numtrr ot' target communities s'hich received
ivernrcit irr treatment iATOhealth education about importance of extended
TNPUT INDT(..\TORS
NumL'cr' (rt target communities u'tth trained CBDs /ATONumL's: trf communitres that erperienced late supply or shortage of ivermectin/ATO
Numrc: oi target conlmunlties rvhtch collected ivermectin fiom the health centreIATO
\urr,l.': ot' irealei commuilllles sirh surnman tonns -l'TO
Numci: oi health cenlres u'tth records -\TO
84

JAF3iINF/DOC 8
Page 5
vroNrroRING FORI{ (CHECKLIST FOR INDEPENDENT MONITORS)
Independent monitors ',vill be required to use elaborate social science methods to address these indicators
in addition to others they may select and submit a comprehensive report to APOC.
EFFECT INDTCATORS
Nu'tt_..'- rc t::-3,.- :omnrunitres rvl.i.|., decid"d the period s1 msthnd oI trextment
Number of target communities that decided on the criteria for CBDs selection
OUTPUT INDTCATORS
Number of refusals two months after drstributionNumber of eligible persons that dropped-out of the fteatment due to cost (Cameroon), side-etfects,
feeling of well-being (all countries). (From year 2)
Number of at-risk villages lreatedCost per person treated
Number of communities where CBDs were changed by the communiry after the first treatment
Number of target communities in which the CBD is a part of or is supen'ised by the primary health care
systemNumber oi targel communities rvhich received health education about tmportance oI ertended
lverrnectin treStment
Number of children 5 vears and above u'ho recetved lvermecttn
TNPUT INDICATORS
Number of target communities with lrained CBDsNumber of communities/ projects that experienced late supply or shortage of ivermectinNumber of pro.lects rvhich experienced late supply of funds
Number of target communities which collected ivermectin from the heaith centre
Number of CBDs rvith measuring device for heightNumber of treated communities with summary formsNumber of health centres without records
85

JOIN'f ACTION FORUMOf tlce ol the Chairman
iOINT ACTION FORUIvIThird session
Af'rican I)rograntntc titr Onchocerciasis Control (APOC)[)r'ograrr.rnrc alricain rlc lutte cor]tre I'onchocercose
JAF-FAC
APOC PROJECTS EVALUATION FOfuVI
F'ORUNI D'ACTION COMIVIU NE
Bureau du Pr6sident
JAF3/INF/DOC.7ORIGINAL:ENGLISHOCTOBER 1997
86

WORLD HEALTH ORGANZATIONAFRICAN REGION
ORGANISATION MONDIALE DE LA SANTE
REGION DE L'AFRIQUE
AFRICAN PROGRAMME FOR ONCHOCERCIASIS CONTROL (APOC)
PROGRAMME AFRICAIN DE LUTTE CONTRE L'ONCHOCERCOSE
B.P. 549 OUAGADOUGOU, Burkina Faso T6169r': ONCHO OUAGADOUGOU
Tel-.. (226)30 23 01 -1[23 12- 30 23 13 Telex: ONCHO 5241 BF Fax (226\3021 47
APOC PROJECTS EVALUATION FORM
EVALUATIoNoFcoMMUNITYDIRECTEDTREATMENTWITHIVERMECTIN(cDTl) PROJECTS
please complete this form by providing detailed answers to all of the question: b"l9Y: You are required to give the
exact figures and where n""Li.rry a Jescriptive explanation. The programme's actjvities will eventually be
evalua6d against sustainability and coverage indicators'
THE EVALUATION FORM HAS FIVE SECTIONS: please complete allsections'
For each approved project a separate evaruation form should be completed. Please return the completed copy(ies)
to APOC Headquarters in Ouagadougou'
Country State Region
Project Phase Project Code Period being evaluated
Form completed and endorsed bY
DateSignatureNational Onchocerciasis coordinator [Mrs] tMsl [Md [Dr]
e-mailFaxPhone
DateSignatureNOTF Chairperson/chairman [Mrs] [Ms] tMr] tDrl
e-mail:Fax:Phone
87

PART I PROJECT PROFILE AND MANAGEMENT
1. Project Profile
2. Management RePorting SYstem
. please, list the principal activities of the project carried out during the period being
evaluated:
Are activities being carried out according to the plans of NOTF and on schedule?
lf not please, state the major constraint(s) experienced
o
a
anization in the project dr€? (name & number)administrative org
Number of target communitiesNumber of communities
Population of target communitiesPopulation of communities
Major constraints
88
Solutions

o Were record forms from the prolect area accurate and completed on time?
Expected report forms(S'l ) Received record forms(52) Form reporting rate e6) (S3)53 = (S2:S1)x 100
Report forms co,mPletelY filled
Report forms PartiallY filled
Report forms received on time
Report forms not received on time
3. Administrative and Financial Management of the CDTI project
Please attached the twelve month financial report
. Which is the month of the last statement received from the bank?
o Which is the month of the last bank reconciliation in the accounts of the project?
. Have any of the accounts been audited?
. lf yes, give the date
. Are the NOTF accounts being operated to the satisfaction of the NOTF?
. Have there been any complaints or financial irregularities?
. Give the exact amount and date the Trust Fund money was last credited into NOTF
account. Amount credited (US $). Date:
. Did the date of receipt of Trust Fund money meet your expectation?
. Did the NOTF experience any administrative problem(s) with the bank?
. lf yes, state succinctly the problem(s)
What should be done to avoid the problem (if any) in future bank transactions?
89
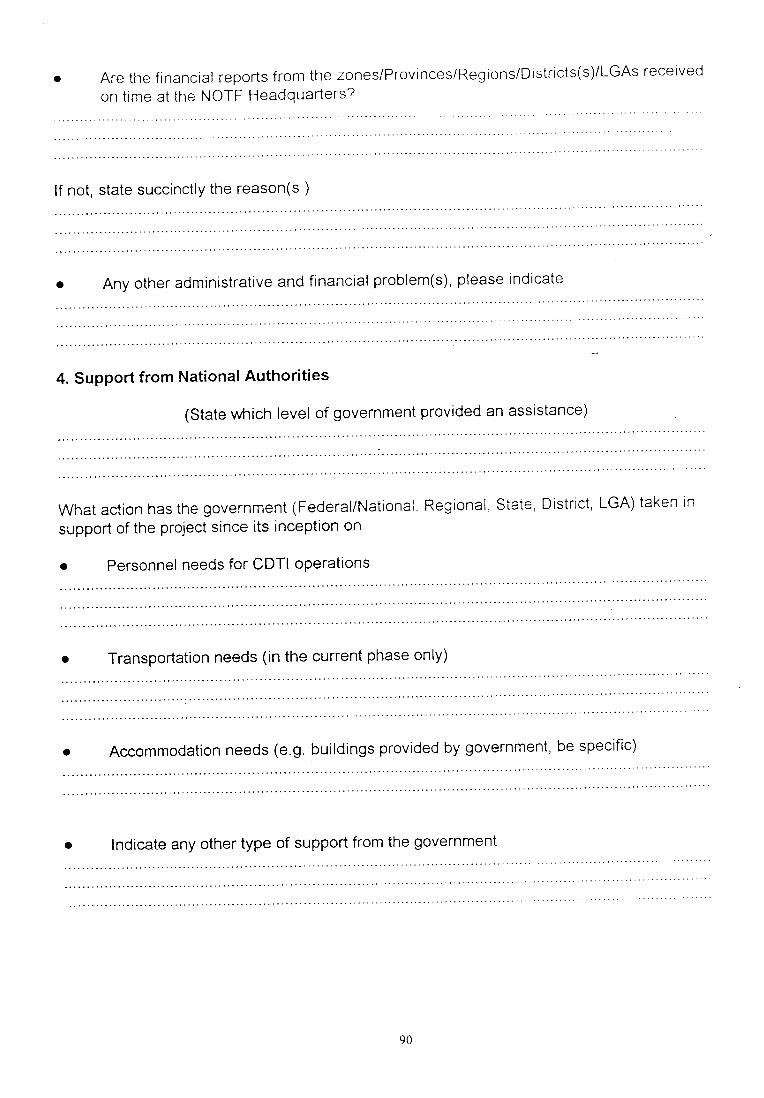
Are the financial reports from the zones/ProvincesiRegionsiDistricts(s)/LGAs received
on time at the NOTF Headquarters?
lf not, state succinctly the reason(s )
o
a
4. Support from National Authorities
(state which level of government provided an assistance)
What action has the government (Federal/National. Regional. State District, LGA) taken in
support of the project since its inception on
. Personnel needs for CDTI operations
Transportation needs (in the current phase only)o
a Accommodation needs (e.g. buildings provided by government, be specific)
a lndicate any other type of support from the government
90
t

5. Effectiveness of communication
please indicate (X) beside your response the type of communication frequently used in the current
year and which you found most efficient
APOC HQ andoffice ofNOTF HQ
NOTF HQ &office of chairmanNGDO coalition
NOTF HA &Zonal or Regionaloffices
Zonal /Regionaloffices DistricULGAoffice ofthe coordiriator
DistricULGAoffice of thecoordinator &
community leader
Type ofCommunication
Effective Noteffective
Effective Noteffective
Effective Noteffective
Eff ective Noteffectrve
Effective Notef fectrve
Radio
Telephone
Fax
lnternet (E-Mail)
Courier
Ordinary mail
Messenger
Any suggestions to improve communication for better management of the project?Please indicate
9l

WORLD HEALTH ORGANZATIONAFRICAN REGION
ORGANISATION MONDIALE DE LA SANTEREGION DE L'AFRIQUE
1
AFRICAN PROGRAMME FOR ONCHOCERCIASIS CONTROL (APOC)PROGRAMME AFRICAIN DE LUTTE CONTRE L'ONCHOCERCOSE
B P. 549 OUAGADOUGOU, Burkina Faso Telegr.: ONCHO OUAGADOUGOU
Tel. (226) 30 23 01 - 9 23 12 - 30 23 1 3 Telcx: ONCHO 5241 BF Fax. (226) N 21 47
APOC PROJECTS EVALUATION FORM - Project Code
EVALUATTON OF COMMUNTTY DTRECTED TREATMENT WITH IVERMECTTN (CDTI) PROJECTS
PART II IVERMECTIN PROCUREMENT, DELIVERY SYSTEM AND DISTRIBUTION
Procurement and movement from the Mectizan Donation to the national store house
What date was the order to Mectizan Donation Program made by the NOTF?
On Which date did the drug arrive at the port?
On which date was the clearance from port completed and drug taken to central store house?
Who cleared the drug from the port? (Check below)
Does the Govemment accord an exemption from taxes and customs duties?
Did the MOH or partner /WHO pay any fees/charges for drug procurement from port of entry?
a lf yes, how much US $ to whom were the fees/charges paid?
Any other problem(s) in connection with the movement of the drug from Mectizan DonationProgram to the store house? Please indicate
o
O
O
o
o
a
Office of the NGDO partner WHO
NOTF Secretariat Ministry of Health (MOH)
Others Please specify
92
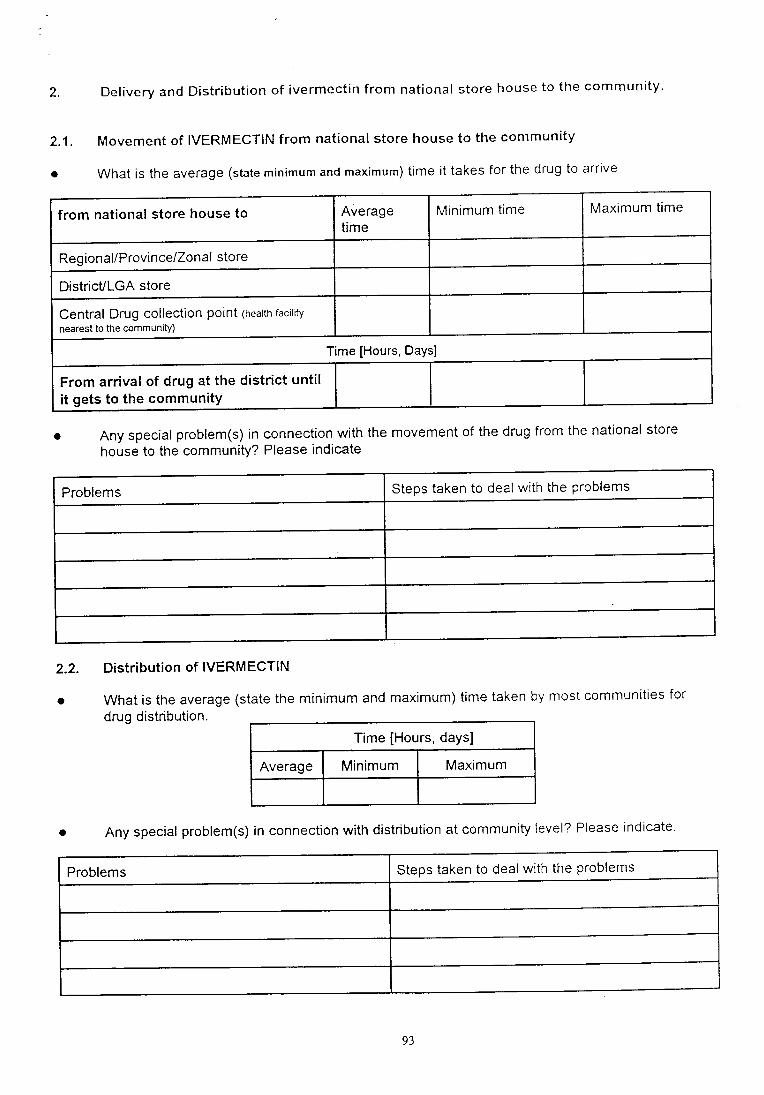
a
2 Delivery and Distribution of ivermectin from national store house to the community
2.1 Movement of IVERMECTIN from national store house to the community
What is the average (state minimum and maximum) time it takes for the drug to arrive
a Any special problem(s) in connection with the movement of the drug from the national store
house to the community? Please indicate
Problems Steps taken to deal with the problems
Distribution of IVERMECTIN
What is the average (state the minimum and maximum) time taken by most communities for
drug distribution
Time [Hours, days]
Average Minimum Maximum
a Any special problem(s) in connection with distribution at communi$ level? Please indicate
Problems Steps taken to deal with the problems
2.2
a
from national store house to Averagetime
Minimum time Maximum time
Regional/Province/Zonal store
DistricULGA store
Central Drug collection point (health racilitv
nearest to the communitY)
Time [Hours, Days]
From arrival of drug at the district untilit gets to the communitY
93
I

lf several other sfeps more than stated below are involved, please specify
94

WORLD HEALTH ORGANIZATIONAFRICAN REGION
ORGANISATION MONDIALE DE LA SANTEREGION DE L'AFRIQUE
AFRICAN PROGRAMME FOR ONCHOCERCIASIS CONTROL (APOC)PROGRAMME AFRICAIN DE LUTTE CONTRE L'ONCHOCERCOSE
B.P. 549 OUAGADOUGOU, Burkina Faso Telegr.: ONCHO OUAGADOUGOU
Tel..: (226) 30 23 01 -{23 12 - 30 23 13 Telex: ONCHO 5241 BF Far (226)3o21 47
APOC PROJECTS EVALUATION FORM- Project Code:
EVALUATION OF COMMUNITY DIRECTED TREATMENT WITH IVERMECTIN (CDTI) PROJECTS
PART III CAPACITY OF THE NOTF/ONCHO COORDINATORS/SUPPORTS STAFFAND THE PHC SYSTEM
Please provide below information on the size of the NOTF (full and part-time staff) by giving the numberand category of staff involved in CDTI at:
Fulltime Part-time
Level Category of staff Number Category of staff Number
Central
RegionalZonal
DistricVLocal G overn m ent
Community
95

o How many different categories of personnel lptease srate number in each category) are involvedin the training of.
Government Staff NGDO Staff
Activity Category Numberby category
Category Number bycategory
Communitydirecteddistributors(cDD)
DistricVLGAcoordinators
Healthpersonnelinvolved in CDTI
Healtheducation andinformation tocommunity
I
a
a Please provide below information
- days CDDs were trained in all project communities (averase, minimum, maximum)
tr Average number of training days o Minimum... ...... o Maximum
- Total number of CDDs trained: o Female o Male
- Number of trained CDDs still on job o Female r Male
Number and proportion of the health staff at the districULGA levels involved in theproject with:
Number of health staff Proportion
Training the community directed distributors
Supervision of ivermectin distribution
Management of severe adverse reactions
How many of the CDDs are health workers?a
96
I
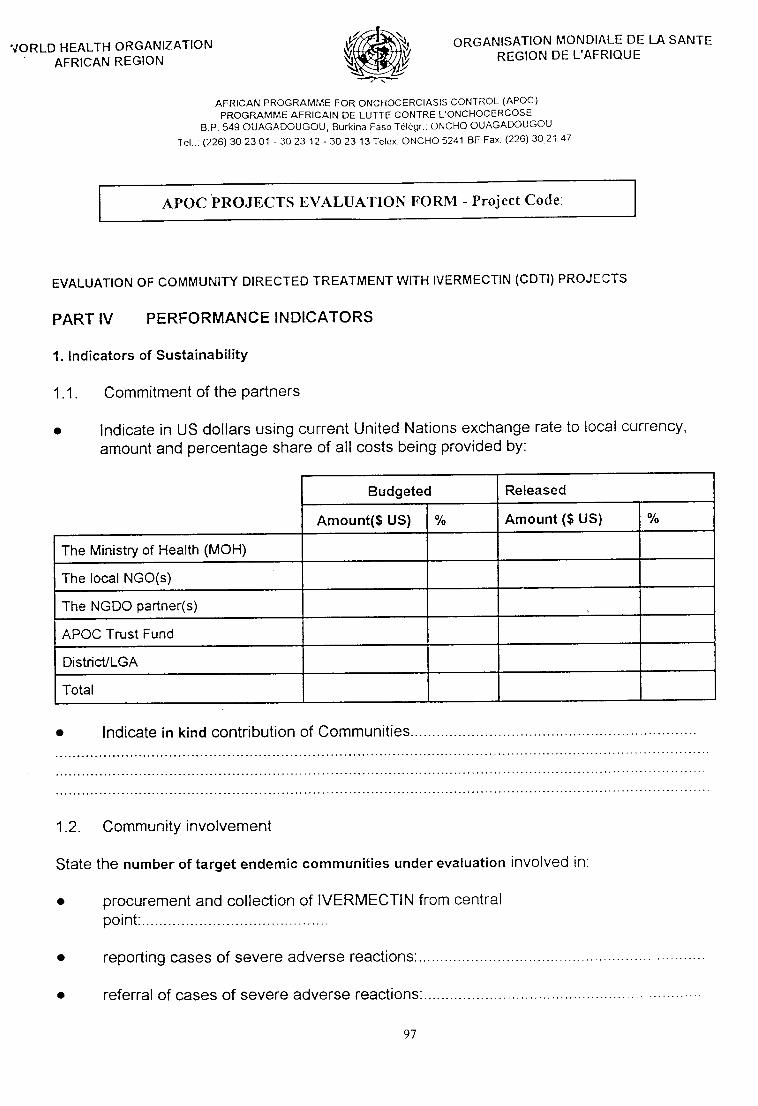
./ORLD H EALTH ORGANIZATION.
AFRICAN REGION
ORGANISATION MONDIALE DE LA SANTEREGION DE L'AFRIQUE
AFRICAN PROGRAMI\4E FOR ONCHOCERCIASIS CONTROL (APOC)
PROGRAMME AFRICAIN DE LUTTE CONTRE L'ONCHOCERCOSEB.P. 549 OUAGADOUGOU, Burkina Faso Til6gr.. ONCHO OUAGADOUGOU
Tel..: (226)302301 -3023 12-3023 l3Telex ONCHO5241 BFFax (226)3021 47
APOC PROJECTS EVALUATION FORM - Project Code
EVALUATION OF COMMUNITY DIRECTED TREATMENT WITH IVERMECTIN (CDTI) PROJf CTS
PART IV PERFORMANCE INDICATORS
1. lndicators of SustainabilitY
1.1. Commitment of the Partners
o lndicate in US dollars using current United Nations exchange rate to local currency,
amount and percentage share of all costs being provided by:
o lndicate in kind contribution of Communities
1.2. Communityinvolvement
State the number of target endemic communities under evaluation involved in
. procurement and collection of IVERMECTIN from centralpoint:..
o reporting cases of severe adverse reactions:.
o referral of cases of severe adverse reactions:.
97
Budgeted Released
A,mount($ US) otlo Amount ($ US) otto
The Ministry of Health (MOH)
The local NGO(s)
The NGDO partner(s)
APOC Trust Fund
Districl/LGA
Total
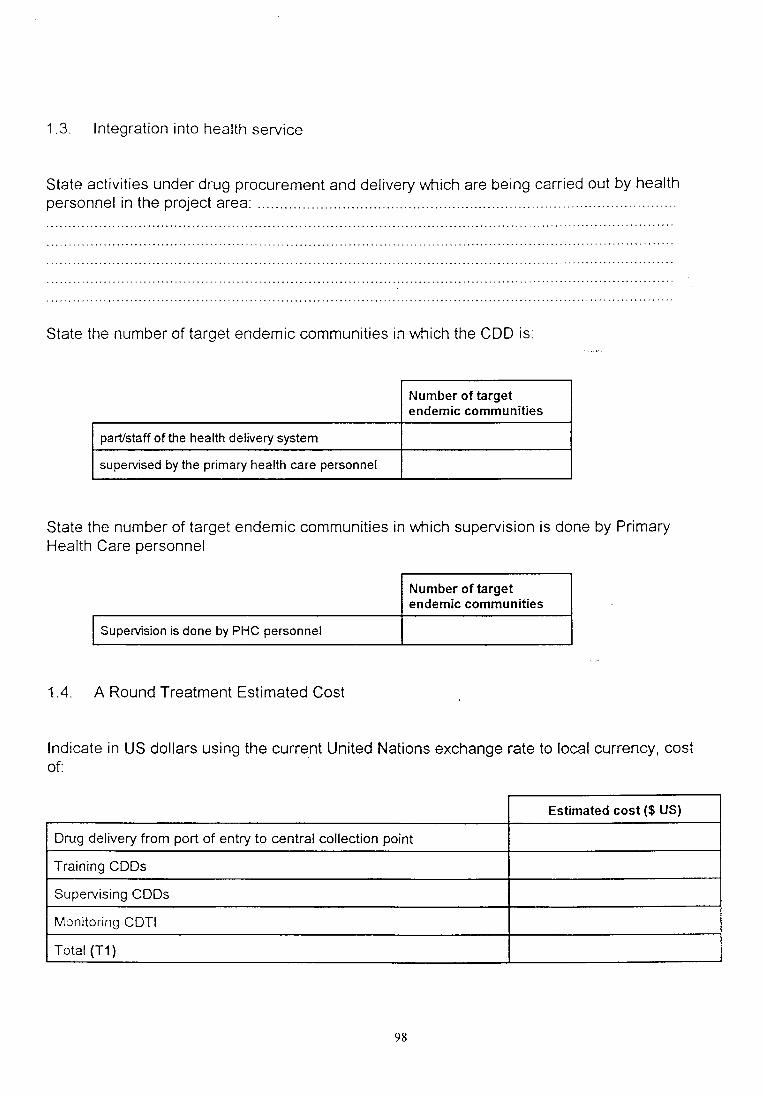
1.3 lntegration into health service
State activities under drug procurement and delivery which are being carried out by healthpersonnel in the project area:
State the number of target endemic communities in wfrich the CDD is
Number of targetendemic communities
parUstaff of the health delivery system
supeMsed by the primary health care personnel
State the number of target endemic communities in wl^rich supervision is done by PrimaryHealth Care personnel
Number of targetendemic communities
SupeMsion is done by PHC personnel
1.4. A Round Treatment Estimated Cost
lndicate in US dollars using the current United Nations exchange rate to local currency, costof:
a
a
Estimated cost ($ US)
Drug delivery from port of entry to central collection point
Training CDDs
Supervising CDDs
Monitoring CDTI
Total (T1)
98

a
z Ref usal/absentees
2.1. Refusals
Please state
Number
Number of communities in the districUlGA where cases of refusal have been recorded
number of people who refused treatment in this phase lrzy
Average number of refusals per community
State the three frequent reasons for refusals
How did the NOTF deal wrth the problem of refusals lrorp€riodbeinsevatuated)?
2.2. Absenteeism
What is Number
the number of communities in the districts (LGA) where absenteeism is the main reasonfor not receiving treatment?
Total number of people who were absent from their treatment areas during this phase 6rs1
average number of absentees per communi\p
Please state, howdid the NOTF deal wth the problem of absenteeism (rorperiodbeinsevaruated) ?
99

Number of targeted
CDTI communities treated with IVERMECTIN
CDTI communities not treated with IVERMECTIN
Population in the CDTI communities (A)
Eligible persons not treated (for one of the following reasons)
- pregnancy (cl)
- breastfeeding 1cz1
- sickness 1cs1
Total Population not treated (B) = (cl + c2 + 63 + fl + T3)
Total Population treated (T41 = 4 - t
3. lndicators of coverage of CDTI
Please indicate below the number of targeted
a
4.
a
a
o
Reporting/Management of cases of severe adverse reaction
Have you had reporting of severe adverse reactions during the period under
evaluation? .....
lf yes, is the NOTF satisfied with the reporting of cases of severe adverse reactions?
Please indicate who reported cases of severe adverse reactions (multiplechoice) ?
o Communities a Community Distributors a Health staff
ls the NOTF satisfied with the management of cases of adverse reactions in the project
arca?.
D lf yes, what are the major causes of satisfaction?
o lf not, what are the major problems and how is the NOTF addressing them?
a
r00
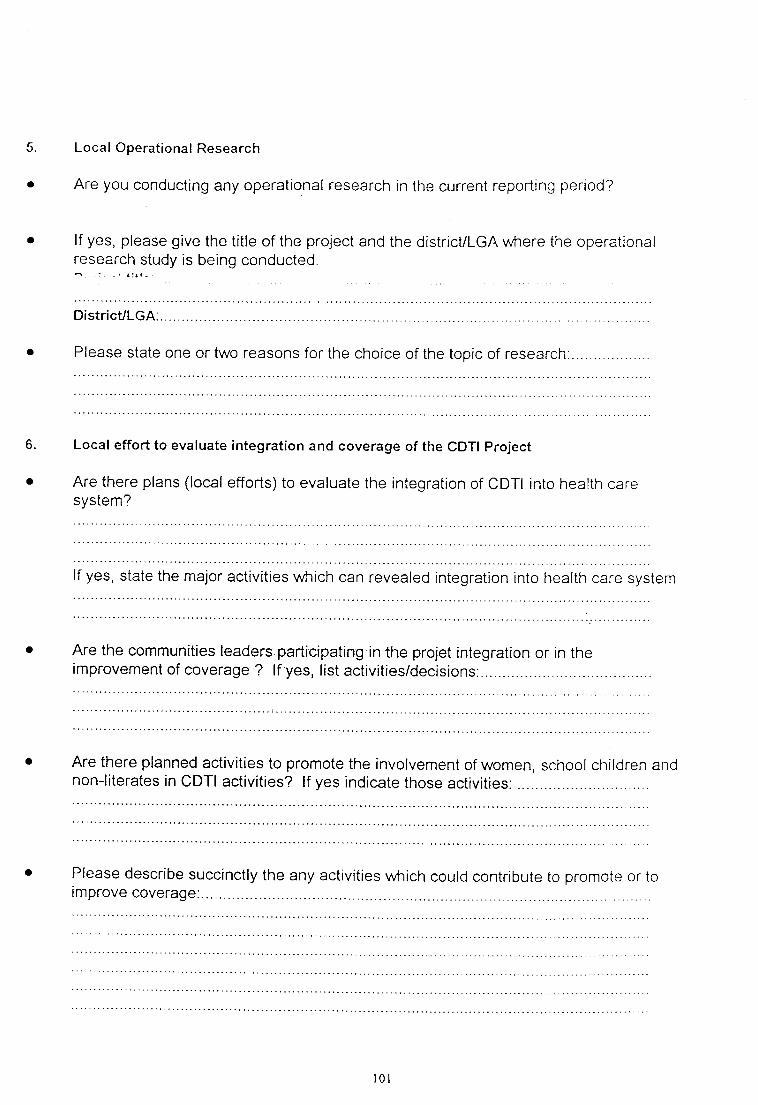
5
a
Local Operational Research
Are you conducting any operational research in the current reporting period?
a lf yes, please give the title of the project and the districulcA vr,trere the operationalresearch study is being conducted.
ll
DistricULGA
a Please state one or two reasons for the choice of the topic of research
6. Local effort to evaluate integration and coverage of the CDTI Project
O Are there plans (local efforts) to evaluate the integration of CDTI into health caresystem?
a Are the communities leaders participating in the projet integration or in theimprovement of coverage ? lf yes, list activities/decisions;....
a Are there planned activities to promote the involvement of women, school children andnon-literates in cDTl activities? lf yes indicate those activities:
a
a Please describe succinctly the any activities which could contribute to promote or tormprove coverage
r0l
PART V
Please write freely but succinctly on any aspects of the execution of this project that miglrt not
have been adequately covered in the preceding structured questionnaire.
a
t02
Related Documents










![JAF Collection Manual - digitster.com Collection Manual.pdf · 2020. 11. 1. · JAF [ Just A Filter ] COLLECTION MANUAL V 1.3 JAF COLLECTION ( Full Version ) The JAF Collection is](https://static.cupdf.com/doc/110x72/612e082b1ecc515869428eee/jaf-collection-manual-collection-manualpdf-2020-11-1-jaf-just-a-filter.jpg)
