1 ISPOR 15th Annual European Congress 3-7 November 2012, ICC Berlin, Berlin, Germany Forum: PATIENTS AND THEIR ROLE IN MARKET ACCESS: WHERE IS THE PLACE AND WHAT IS THE ROLE OF PATIENTS IN REIMBURSEMENT SYSTEMS? - Romania - Speaker: Paul Radu, MD, PhD, ISPOR Romania Market Access Manager Roche Romania ISPOR Romania Presentation for Berlin Authors: – Paul Radu, MD, PhD Market Access Manager, Roche Romania [email protected] – Ioana BIANCHI, MD, Public Health Specialist President, ISPOR Romania Regional Chapter and counselor to the Minister of Health, Romania [email protected] – Sorin PAVELIU, MD, PhD Associate Professor at “Titu Maiorescu” University, Pharmacoeconomics Department, Bucharest, Romania [email protected] 2

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
1
ISPOR 15th Annual European Congress 3-7 November 2012, ICC Berlin, Berlin, Germany
Forum:
PATIENTS AND THEIR ROLE IN MARKET ACCESS: WHERE IS THE PLACE AND WHAT IS THE ROLE OF
PATIENTS IN REIMBURSEMENT SYSTEMS?
- Romania -
Speaker: Paul Radu, MD, PhD, ISPOR Romania
Market Access Manager Roche Romania
ISPOR Romania Presentation for Berlin
Authors:
– Paul Radu, MD, PhD Market Access Manager, Roche Romania [email protected]
– Ioana BIANCHI, MD, Public Health Specialist President, ISPOR Romania Regional Chapter and counselor to the Minister of Health, Romania [email protected]
– Sorin PAVELIU, MD, PhD Associate Professor at “Titu Maiorescu” University, Pharmacoeconomics Department, Bucharest, Romania [email protected]
2
2
Presentation Content
• Market access and reimbursement systems
• Role of patients
• Romanian situation
• Conclusions
3
Market access in health care
• Reflects the openness of the health care market to goods (drugs, materials, medical devices, etc.) and health care services
• Particularities are derived from the specifics of the health care market: – Not a free market
– High costs for many goods and services
– Very often conditioned by the role of the third-party
payer (insurance company, Government etc.)
– Strongly regulated
4

3
Market access (MA) in pharmacoeconomics (1)
• The process used by a company to bring a drug on the market and to make it available (accessible) to the patients
• Multiple stakeholders involved in the MA process, with different perspectives: – Medical/clinical developers
– Product marketing teams
– Health care providers
– Patients
– Payers
– Regulatory bodies etc.
5
Market access (MA) in pharmacoeconomics (2)
• Emerging aspects influencing MA:
– Rising costs of drugs increase pressure on/from payers
– Increasing concern over safety and ensuring benefits exceed risks
– Role of HTA in providing evidence on the drug “added
value”
– Greater demand for evidence development on drug effectiveness that translates into improved health outcomes
6
4
Reimbursement system (1)
• The key stakeholder influencing market access in health care is the third-party payer (i.e. reimbursement system)
• Most European countries have reimbursement systems based on compulsory insurance schemes via: – Public general taxation (e.g. UK, Italy, Spain etc.)
– Social health insurance run by public /private institutions
(e.g. Austria, France, Germany, Romania, Slovakia, etc.)
• Few countries have reimbursement systems based on voluntary insurance schemes (Swiss, US)
7
Reimbursement system (2)
• The system needs to be strongly regulated to maintain a balance between parties :
– The insured/patient who asks for more services and less payment
– The providers want to get more value for their goods or health care services
– The payer who has to maximize benefits for patients within available funds and satisfy own interests (e.g. profit, political influence etc.)
• The reimbursement systems are key to market access
8
5
Role of patients (1)
• Different perspective between patients and “potential patients” (i.e. the insured healthy population)
• The insured healthy population:
– Pay the premium/taxes thinking at its potential health care needs
– Have the willingness to participate in decisions who support a rationale and efficient use of resources (in order to be sure that they can benefit in case of need)
9
Role of patients (2)
• The patients (“the consumers”):
– Think and live for the present
– Ask for the best NOW!
– Want to feel that they get “what they need”, based on their payments
• Both patients and insured population have to be involved in the decisions about their health and health care through Patient Empowerment (PE):
– Individual empowerment – linked with patients
– Community empowerment – linked with insured people
10
6
Individual patient empowerment
• The individual’s ability to make decisions and have control over his or her personal life and health
• Patient empowerment – Begins with information and education,
– Seeking out information about own illness or condition,
– Actively participating in treatment decisions
• Empowerment requires an individual to take care of him and make choices from the options recommended by the doctor
11
Community patient empowerment
• Individuals act together to gain greater influence and control over the determinants of health and quality of life in their community
• A person has to take an informed position and make an informed choice; it involves conscious effort at the policy-making level to ensure that informed participation is possible
• Community empowerment becomes an integral element of the health care reform
12

7
Patient empowerment and reimbursement
• Empowerment key word = adherence, i.e. the involvement in joint decisions (with payer) regarding use of resources.
• Challenges:
– How much funding for health care/drugs?
– Which illness to cover (allocative efficiency)?
– Which treatments to reimburse (technical efficiency)?
– Patients’ requests vs. patients’ needs
– People mobility (more specific for EU)
– Access of patients to new drugs/technologies
13
Romania example – some data
• Population – 21,7 million , 10% are working abroad
• GDP =12.300 USD/per capita (PPP-2011)
• GDP growth in 2010 = -1,3%, in 2011 = +1,5%
• Inflation rate 2011 = 5,7%, expected in 2012 = 3%
• 520 hospitals (public and private) and around 137.000 beds (6,3 beds/1000 inhabitants)
• 50.267 doctors in 2008 (2,3 doctors per 1000 population)
• Life expectancy: 76,7 years (female), 69.5 (male) in 2008
• Infant mortality: 11/1000 (2008) 14
8
• Compulsory health care insurance system run by the National Health Insurance House (NHIH)
• Financed mainly from employer and employee taxes (5,2+5,5%), contributions of free entrepreneurs and State Budget subsidies: – ~ 4,0 bn Euro in 2011 from ~ 6 mil. contributors
• Very small market for voluntary private health insurance (~ 10 mil. Euro), mainly for ambulatory services and emergency transportation
Drugs reimbursement in Romania (1)
15
• Ministry of Health (MoH) covers emergency care, public health, National Health Programs and investments:
– Revenues from the earmarked taxation of alcohol, tobacco etc. and from the State Budget
– ~1 bn Euro in 2011
• Main decision bodies: – Ministry of Health (MoH)
– National Health Insurance House (NHIH)
– ANMDM (National Agency for Drugs and Medical Devices)
– Local authorities (for public hospitals)
Drugs reimbursement in Romania (2)
16
9
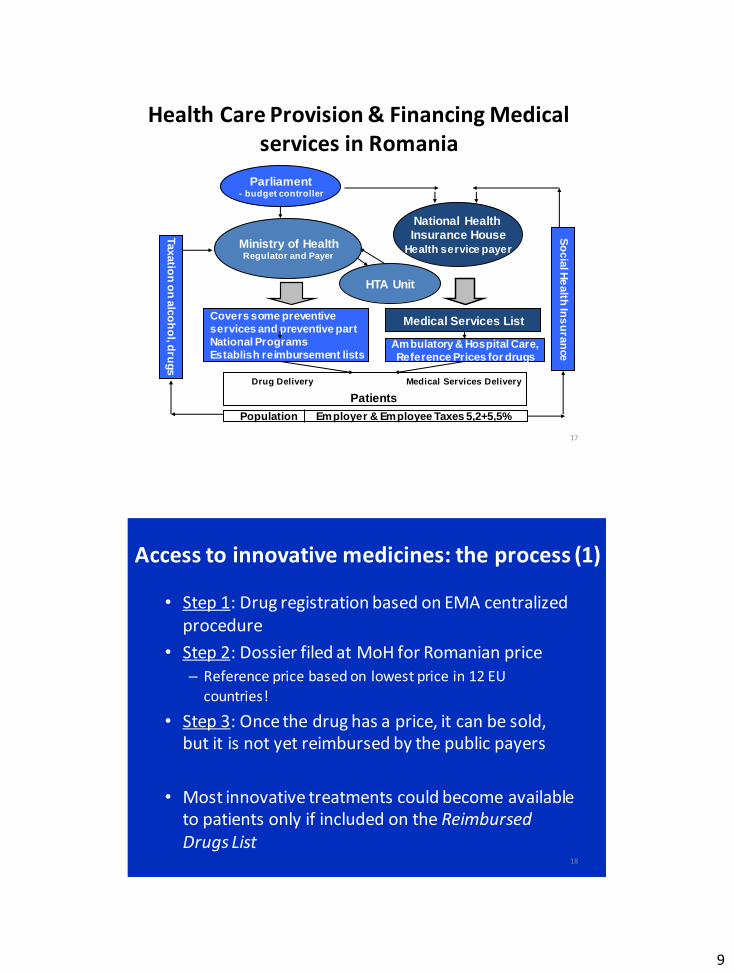
Parliament - budget controller
National Health Insurance House
Health service payer Ministry of Health Regulator and Payer
Ambulatory & Hospital Care,
Reference Prices for drugs
Medical Services List
Patients
Population Employer & Employee Taxes 5,2+5,5%
So
cia
l He
alth
Ins
ura
nce
Covers some preventive
services and preventive part
National Programs
Establish reimbursement lists
Budget financing Insurance based financing
Drug Delivery Medical Services Delivery
Health Care Provision & Financing Medical services in Romania
HTA Unit
Budget financing
Taxatio
n o
n a
lco
ho
l, dru
gs
17
Access to innovative medicines: the process (1)
• Step 1: Drug registration based on EMA centralized procedure
• Step 2: Dossier filed at MoH for Romanian price – Reference price based on lowest price in 12 EU
countries!
• Step 3: Once the drug has a price, it can be sold, but it is not yet reimbursed by the public payers
• Most innovative treatments could become available to patients only if included on the Reimbursed Drugs List
18
10
• Reimbursed Drugs List last updated in 2008 (a politically driven process and requires a Government Decision)
• The official process to gain access to the List:
– Appraisal and positive recommendations from the MoH Transparency Commission (to be replaced by the approval of the HTA Unit from MoH)
– Approval from the MoH
– Publication though a Government Decision of the new List
• There is a constant struggle from pharma companies and patients associations, for better patient access to innovative treatments.
Access to innovative medicines: the process (2)
19
• A formal HTA unit was created within MoH to evaluate the new medicines or new indications and to support decision-making (the unit will most likely functional as of December 2012)
• Increased pressure on the public funds for the health system
• Decreased budget for drugs in 2012 compared with drugs expenditures in 2011
• Existing clawback taxation reduces the Government expenditures on drugs (5,9 mil. RON in 2012 ~ 1,3 bn Euro).
Access to innovative medicines: the process (3)
20
11
• The HTA Unit is not yet functional
• …but criteria were developed for the Reimbursement Dossier:
– Relevant clinical studies results
– Relevant cost–effectiveness studies from France and UK
– Status and level of reimbursement in the EU countries
– Price approved in Romania
– Prices approved in other EU countries
– Daily cost and average total cost of treatment
– Cost comparison with drugs used for same indication etc.
Access to innovative medicines: the process (4)
21
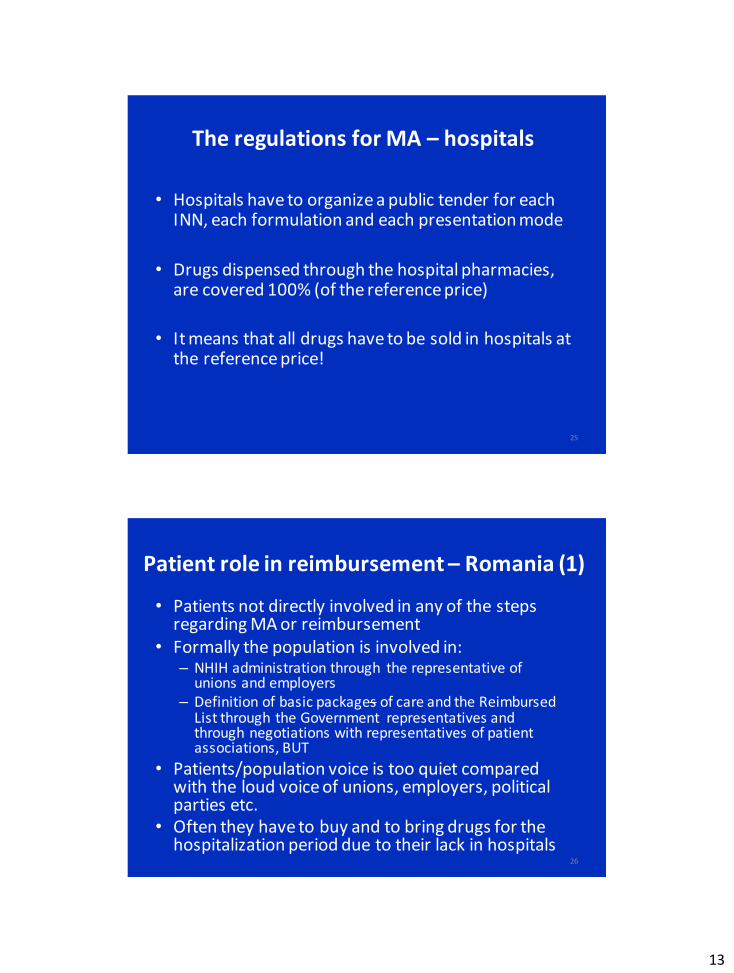
Drugs reimbursed by the NHIH, incl. those in National Programs
The Reimbursed List in Romania
22
To tal reimbursement expenses
N a t ional Health Insurance House M i nistry of Health
Hospitals d rugs R e i mbursement lis ts
Sub lis t A, 90% reimbursement
Sub lis t B, 50% reimbursement
Sub lis ts C1, C3 100% reimbursement
N a t ional Health Programs
Sub lis t C2, 1 00% reimbursement
t hrough transfer of funds to N HIH

12
• Drugs from the Reimbursement List for ambulatory care are dispensed as follows:
– For drugs from sublists A, B, C1 and C3 (oral, IV, IM or SC
formulation) through the open-circuit pharmacies
– For drugs from sublists C2, oral formulation through the
open-circuit pharmacies
– For drugs from sublists C2, IV, IM or SC formulation
through hospital pharmacies
– Maximum prices for open and hospital pharmacies are
established by the MoH
The regulations for MA – pharmacies (1)
23
• For all drugs the prescription has to be done on generic name (INN) with brand name only for post-transplant drugs
• Physicians could prescribe also in some cases on brand name, but providing a clear documentation of the case
• In open-circuit pharmacies the patient should cover the % from the reference price not covered by the NHIH, and the difference from the reference price to the pharmacy price
24
The regulations for MA – pharmacies (2)
13
• Hospitals have to organize a public tender for each INN, each formulation and each presentation mode
• Drugs dispensed through the hospital pharmacies, are covered 100% (of the reference price)
• It means that all drugs have to be sold in hospitals at the reference price!
25
The regulations for MA – hospitals
• Patients not directly involved in any of the steps regarding MA or reimbursement
• Formally the population is involved in: – NHIH administration through the representative of
unions and employers – Definition of basic packages of care and the Reimbursed
List through the Government representatives and through negotiations with representatives of patient associations, BUT
• Patients/population voice is too quiet compared with the loud voice of unions, employers, political parties etc.
• Often they have to buy and to bring drugs for the hospitalization period due to their lack in hospitals
26
Patient role in reimbursement – Romania (1)
14
• Example 1 : – The new law regarding co-payment established a direct
negotiation with patient associations in the moment of establishing the co-payment
– Results: the process of co-payment regulation is blocked, because the patients refuse any type of co-payment in the social insurance scheme (in addition to unofficial out-of-pocket payments)!
– Whilst the Government is pressured to introduce co-payment as part of the Memorandum with IMF, WB and UE
27
Patient role in reimbursement – Romania (2)
• According to regulation and because of INN prescription, the patients could decide on the drugs delivered in open-circuit pharmacies, but…:
28
Patient role in MA– Romania (1)

15
• There are several issues and alternatives for patients: – They have to pay the user charges above the reference
price and the % from reference price not covered by the health insurance
– Usually they follow the recommendations of the prescribing physician (as long as funding is available as copayment
– The pharmacies should dispense the drugs at the reference price (unless the patient declares that he wants a specific brand within the same INN), BUT in case of several brands the availability of drugs is based on their commercial benefits.
29
Patient role in MA– Romania (2)
• Example 2: – The prescription on INN is compulsory in Romania
– Based on some AEs from switching the post-transplant
immuno-suppression medication, physicians and patients requested a change in prescription and reimbursement of such medication
– Consequently the authorities modified the rules and for this medication the prescription should be done both on INN and brand level, therefore the reimbursement is 100% from the full price of the drug (not the reference price only!)
30
Patient role in MA – Romania (3)
16
• The new HTA legislation considers patient involvement: patients are invited to participate in discussions over the resolution of decision regarding the drugs that were not approved for introduction on the list
• Patients associations are very active in supporting the reimbursement of new drugs … as long as they don’t have to make any additional out of pocket payments.
• Also the patient associations and media are pushing for removal of the waiting lists, which reduce patient access to drugs for several serious conditions (e.g. cancer).
31
Patient role in MA – Romania (4)
• Example 3: The MoH published the draft of a new Health Reform Law, waiting for feed-back from the different stakeholders (incl. patients): – In several public conferences, the Minister of Health
declared that the feed-back from the society is very reduced and it seems that the health system reform is not on the public agenda of the population/patients
– Even if patient associations, professional associations, unions etc. claim that they are not involved in the health reform, there are situations when they don’t participate in the public debate, or their messages are not consistent: • It reflects a lack of education on their specific role!
32
Patient role in MA– Romania (5)

17
• IMAS published (Sept. 2012) results of a survey on the behavior of Romanian citizens facing drugs consumptions – Most Romanians would like to get access to modern
medicines (including drugs), but without additional payment,
– 88,5% from Romanians consider that it’s necessary to get access to new drugs for serious diseases (hepatitis, cancer, diabetes etc.), but most of them do not agree to pay more for health insurance premium and
– Most of the responders (72%) don’t agree an increase of the health insurance premium with 1,5% (which would affect 7% of their income).
33
Patient opinion regarding reimbursement in Romania
• There are too few visible initiatives to increase patient education and information regarding health/health care
• In Romania patients are seldom involved in the consultations regarding the reimbursement process
• Most of discussions regarding reimbursement are on the level of payment/co-payment and there is little room for other aspects (effectiveness, efficiency, ethics etc.)
• Patients are not seen as key stakeholders in the decision-making processes
• Patients become important (are used? ) when there are reimbursement decisions with … quick political impact!
34
Conclusions
Related Documents











