Isoimmunization & Fetal Hydrops Gillor Moshe Kaplan Medical Center

Isoimmunization & Fetal Hydrops Gillor Moshe Kaplan Medical Center.
Dec 21, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Isoimmunization & Fetal Hydrops
Gillor Moshe
Kaplan Medical Center

Hydrops Fetalis- Definition
- General fetal edema
- Accumulation of fluid in ≥2 body cavities:• Pleural• Pericardial• Peritoneal• Soft tissue - subcutaneous
• Mostly coupled with placentomegaly & polyhydramnios


Pathophysiology
Dysregulation of the net fluid movement
between the vascular & interstitial spaces:
•Primary heart failure
•High cardiac output failure - anemia
•Decreased colloid oncotic pressure
•Increased capillary permeability
•Obstruction of venous and lymphatic flow

Appearance of hydrops
Pericardial effusion
Ascites
Polyhydramnios
Scalp edema
Pleural effusions
Oligohydramnios

Hydrops Fetalis- Etiology
ImmuneImmune Non-immuneNon-immune
Hydrops Fetalis- Etiology
ImmuneImmune Non-immuneNon-immune10%-15%10%-15% 85%-90%85%-90%
RhD Isoimmunization in pregnancy

Introduction• 29 known blood groups
• >600 known red cell antigens (Ag’s)
• Exposure to foreign red cell Ag’s → anti–red cell antibodies(Ab’s) → red cell alloimmunization
• These Ab’s may cross the placenta →– Fetal anemia – Hyperbilirubinemia– Hydrops fetalis

Historic landmarks1609- Hemolytic disease of the fetus and newborn (HDFN) was first described by a French midwife
1939- An Ab was identified in a mother to a stillborn (Levine)
1941- RhD Ab’s in an RhD(-) mother serum & HDFN of her newborn (Levine)
1945- Amniotic fluid bilirubin assessment is an indirect measurement for the degree of fetal hemolysis (Liley)
1964- Anti-D prophylaxis (Freda)
1981- Intravascular fetal transfusion (Rodeck)
2000- Noninvasive detection of fetal anemia by Doppler ultrasound of the fetal middle cerebral artery (MCA)
2002- Fetal typing via cell free DNA in maternal plasma

Incidence• 15% of whites are Rh(-)
• Father is Rh(+) 85% of cases with 40% homozygous → ~60% of
infants are Rh(+)
• Only 16% isoimmunization (mostly postpartum) *
• In Rh(-) alloimmunized mother:– 25% mild-moderate HDFN – 25% hydrops fetalis
• Males are x13 more likely to develop hydrops & x3 more likely
to die* Before the introduction of anti-D prophylaxis

Incidence- cont.• Anti red cell Ab’s are found in 1% of pregnancies• Anti-D prophylaxis shifted the cause of HDFN to less
common red cell antigens
Incidence of maternal anti-red cell antibodies associated with hemolytic disease of the fetus and newborn
(HDFN) in a Dutch population of pregnant women. (From van der Schoot CE, Tax GH, Rijnders RJP, et al: Prenatal typing of Rh and Kell blood group system antigens: The edge of the watershed. Trans Med Rev 17:31, 2003.)
)Kell( )Kidd()Duffy(

Pathophysiology
• Feto-maternal hemorrhage (↑ w GA)
• Materno-fetal hemorrhage (‘grandmother theory’)
• IgG response
• ABO incompatibility is protective
• Ab’s can be detected 5-16W post- exposure
• 50% of alloimmunized are “sensibilized” = Ab levels are very low and can’t be detected
• Fetal anemia→ ↑ CO + extramedullary hematopoesis
• Hydrops is a late finding. Pathophysiology unknown (↓ oncotic P/ iron overload/ ↑ capillary permeability)
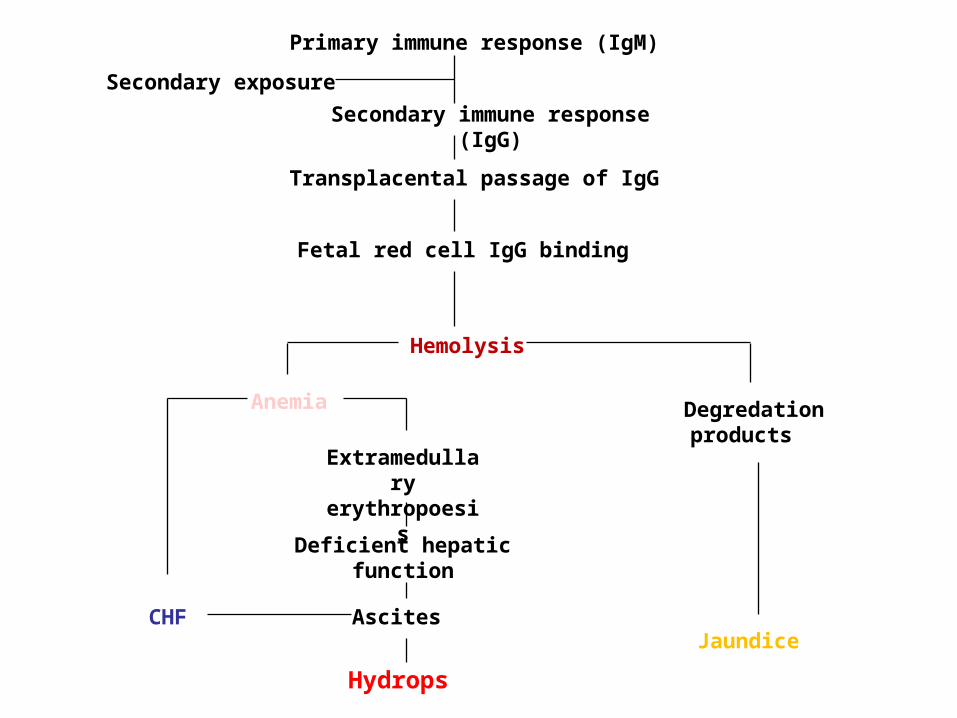
Primary immune response (IgM)
Secondary immune response (IgG)
Transplacental passage of IgG
Fetal red cell IgG binding
Hemolysis
Anemia Degredation products
Jaundice
Extramedullaryerythropoesis
Deficient hepaticfunction
Ascites
Hydrops
CHF
Secondary exposure

Prevention
• Anti-D Ig ↓ alloimmunization by 90% postpartum & 2→0.1% in 3rd trimester
• 300μg counteract 30ml of Rh(+) blood or 15ml RBCs
• Anti-D Ig t½ = 16 days
• Risk from anti-D Ig is minimal/absent → whenever there is a doubt → anti-D Ig should be administered

Prevention- indications:
• At 28 weeks
• After delivery (within 72h, ±KB )• After abortion
• Abdominal trauma
• Maternal bleeding
• Invasive procedures

Prevention- cont.
• Failure of prevention= 0.1-0.2%
• Currently, no prophylactic Ig exists for
other forms of red cell alloimmunization
• For subsequent pregnancy- PGD

Diagnosis
• Indirect Coomb’s• Ab titer• Critical titer→ 1:8 – 1:32• Paternity status (zygosity)• Determine fetal genotype:
– AC (CVS→↑FMH)– ccff DNA in maternal plasma
ccff- circulating cell free fetal

Diagnosis- cont.
• F/U on severity of HDFN:– AC– Fetal blood sampling (a.k.a PUBS or
cordocentesis)→ 1-2% fetal loss, 50% FMH– US:
• Hydrops→ -7g% Hb• Splenic perimeter & hepatic length
– US Doppler

PSV in MCA
• Mainstay of surveillance for fetal anemia
• Fetal anemia causes:
– ↑CO – ↓blood viscosity– Blood flow centralization
• Begin at 18W
• After 35W → ↑False (-)
↑blood velocity


Treatment- Intrauterine transfusion
• Umbilical cord or intrahepatic portion of UV
• Fetal blood sampling for initial Hct
• Fetal paralysis (e.g. vecuronium)
• Fresh (<1W old), O(-), CMV(-), HIV(-), HCV(-), leukoreduced, irradiated, cross-matched, Hct 75% PC
• PSV in MCA is not predictive after 2nd Tx.
Treatment- Intrauterine transfusion
• Transfusion is not preformed past 35W
• Complications:– Procedure related fetal death ~5% – Emergent CS (5% after 32W)– Transient fetal bradycardia– PPROM is rare
• Alternative Tx.:IVIG Plasmapheresis
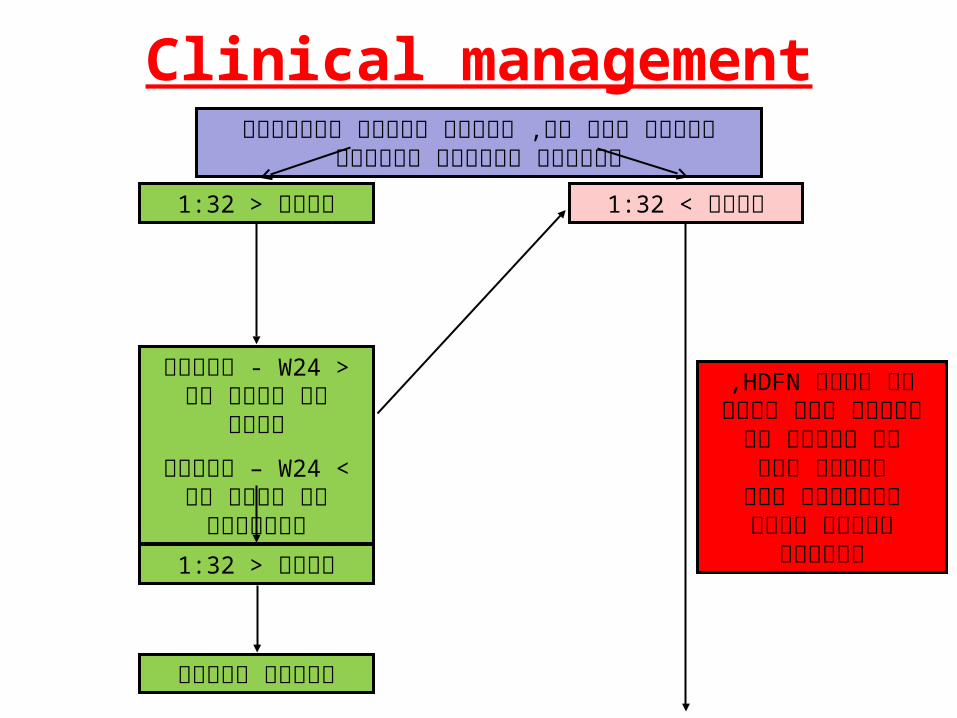
Clinical management
1:32טיטר < 1:32טיטר >
>W24 לחזור על - טיטר כל חודש
<W24 לחזור על – טיטר כל שבועיים
1:32טיטר <
יילוד במועד
בדיקת סוג דם, קומבס וטיטר נוגדנים בביקור הראשון בהריון
, עירוי HDFNאם ברקע תוך רחמי או החלפת דם בילוד אין קורלציה
בין הטיטר ורמת האנמיה

בירור סוג דם וגנוטיפ של האב
אנטיגן (-) באב אבהות ודאית
יילוד במועד
גנוטיפ הטרוזיגוטי באב
גנוטיפ הומוזיגוטי באב
MCA ב-PSVמדידת פעם בשבוע החל משבוע
18
MOM 1.5מדידה > כן לא
דיקור חבל טבור Hctלקביעת
עוברי
עירוי דם תוך > Hctרחמי אם 30%
פעם בשבוע. MCAמעקב זרימות ב- ΔOD450 לבשלות ריאתית ו- AC 35בשבוע
יילוד בשבוע 37
עובר בשל ΔOD450 לא בגבול
עליון
עובר לא בשלΔOD450בגבול עליון
יילוד בשבוע 36
עובר לא בשל ΔOD450לא בגבול עליון
תוך ACלחזור על שבועיים
AC/ccffDNA 14בשבוע
אנטיגן (-) לעובר
אנטיגן (+) לעובר

Hydrops fetalis- Etiology
Non-immune (87%) Immune (13%)
– Malformations• Cardiac (structural, CM, tumor, arrhythmia)
• Chest (diaphragmatic hernia, CCAM, 1⁰ chylothorax)
• Abdomen (tumor, obstruction, prune belly syn.)
• Placenta (TTTS, chorangioma)
• Misc. (sacrococcygeal teratoma, cystic hygroma)
– Chromosomal/genetic (trisomy 21, 45X0, triploidy, Noonan)
– Infectious (TORCH, Parvovirus, Listeria)
– Metabolic (lysosomal/glycogen storage diseases, hypothyroidism)
– Hematologic (α-thalassemia, Diamond Blackfan, FMH)

NIHF- Management
• Etiology dependent
• At term- delivery
• Treatment options include:– Conversion in heart failure caused by
SVT
– Intrauterine transfusion for fetal anemia caused by Parvovirus

Cardiovascular
• Isolated cardiac defect is uncommon, bad
prognosis
• Arrhythmias – SVT, atrial fibrillation/flutter, VT
(rare) elevated systemic venous pressure NIHF
treatment with antiarrhythmic drugs such as
digoxin, flecanaide,...
• A-V block – Anti Ro Ab., structural defect
poor prognosis

Hematology
HemoglobinopathiesHemoglobinopathies
thalassemia –deficiency of globin chain synthesis (Hb Bart’s dis)
• The most common cause of hydrops in southeast Asia
• Prenatal diagnosis of the gene mutation is possible

Hematology
• Enzyme def.- Pyruvate kinase def. & G6PD def.
• Diamond-Blackfan syn.– aplastic anemia
• Acquired causes: Fetal maternal hemorrhage

Infection• Viral, parasitic and bacterial causes• 5-10% of NIHF• Parvovirus, CMV, Syphilis & Toxoplasma• Parvovirus:
– Aplastic anemia, myocarditis– Transmission rate of 30%, IUFD rate of 5-10%– Cordocentesis– fetal anemia w/o reticulocytosis– Hydrops can be treated by intrauterine
transfusion of packed red blood cells– Can resolve spontaneously (1/3 of cases)

Twins
• TTTS – complicates 25% of monochorionic twins
• The ‘recipient’ fetus– hypervolemia -high output cardiac failure
• Twin reversed arterial perfusion (TARP)– Acardiac twin. The ‘pump twin’ perfuse an acardiac parasitic twin– leads to high output cardiac failure

Hydrops Fetalis- Maternal Complications
• Increased incidence of preeclampsia (mirror syndrome)
• Preterm labor because of polyhydramnios
• Post partum hemorrhage

Management Hydrops Fetalis-• Mother:
– CBC– Blood type, indirect Coombs– KB– TORCH, VDRL, Parvovirus– Hb electrophoresis
• Fetus:
– General survey + PSV in MCA– Echocardiography– AC for karyotype & cultures (toxo., CMV, parvovirus)

Questions?

Kleihauer-Betke
MBV(ml) x mHct x KB(%)
Fetal blood volume = nHct
300μg anti-D should protect an average size mother from 30ml of fetal whole blood


Spectral analysis of amniotic fluid
Related Documents