Ischemic Outcomes After Coronary Intervention of Calcified Vessels in Acute Coronary Syndromes Pooled Analysis From the HORIZONS-AMI (Harmonizing Outcomes With Revascularization and Stents in Acute Myocardial Infarction) and ACUITY (Acute Catheterization and Urgent Intervention Triage Strategy) Trials Philippe Généreux, MD,*yz Mahesh V. Madhavan, BA,* Gary S. Mintz, MD,*y Akiko Maehara, MD,*y Tullio Palmerini, MD,x Laura LaSalle, BA,y Ke Xu, PHD,y Tom McAndrew, MS,y Ajay Kirtane, MD, SM,*y Alexandra J. Lansky, MD,k Sorin J. Brener, MD,y{ Roxana Mehran, MD,y# Gregg W. Stone, MD*y New York, New York; Montréal, Québec, Canada; Bologna, Italy; and New Haven, Connecticut Objectives This study sought to determine the frequency and impact of coronary calcification among patients undergoing percutaneous coronary intervention (PCI) for acute coronary syndromes (ACS). Background Small studies in patients with stable coronary artery disease have suggested a worse prognosis after PCI of calcified compared with noncalcified lesions. Little is known about the impact of coronary calcification on outcomes after PCI for patients presenting with non–ST-segment elevation and ST-segment elevation ACS. Methods Data from 6,855 patients presenting with ACS in whom PCI was performed were pooled from 2 large-scale randomized, controlled trials, ACUITY (Acute Catheterization and Urgent Intervention Triage Strategy) and HORIZONS-AMI (Harmonizing Outcomes With Revascularization and Stents in Acute Myocardial Infarction). One-year outcomes were analyzed according to the severity of PCI target lesion calcification (none/mild, moderate, or severe) as assessed by an independent angiographic core laboratory. Results Target lesion calcification was severe in 402 patients (5.9%), moderate in 1,788 (26.1%), and none/mild in 4,665 (68.1%). Moderate/severe target lesion calcification was more frequent in older patients, men, hypertensive patients, and those presenting with ST-segment elevation myocardial infarction (STEMI). The unadjusted 1-year rates of death, cardiac death, definite stent thrombosis, and ischemic target lesion revascularization (TLR) and target vessel revascularization were significantly increased in patients with moderate/severe target lesion calcification. By multivariable analysis, the presence of moderate/severe target lesion calcification was an independent predictor of 1-year definite stent thrombosis (hazard ratio [HR]: 1.62; 95% confidence interval [CI]: 1.14 to 2.30; p ¼ 0.007) and ischemic TLR (HR: 1.44; 95% CI: 1.17 to 1.78; p ¼ 0.0007). Conclusions Moderate/severe lesion calcification was relatively frequent in patients with non–ST-segment elevation ACS and STEMI and was strongly predictive of stent thrombosis and ischemic TLR at 1 year. (Comparison of Angiomax Versus Heparin in Acute Coronary Syndromes [ACS]; NCT00093158; Harmonizing Outcomes With Revascularization and Stents in Acute Myocardial Infarction; NCT00433966) (J Am Coll Cardiol 2014;63:1845–54) ª 2014 by the American College of Cardiology Foundation From the *New York-Presbyterian Hospital and Columbia University Medical Center, New York, New York; yCardiovascular Research Foundation, New York, New York; zHôpital du Sacré-Coeur de Montréal, Université de Montréal, Montréal, Québec, Canada; xIstituto di Cardiologia, University of Bologna, Bologna, Italy; kYale School of Medicine, New Haven, Connecticut; {New York Methodist Hospital, New York, New York; and the #Mount Sinai Medical Center, New York, New York. Drs. Généreux and Palmerini have received speaker fees from Abbott Vascular. Mr. Madhavan was supported by a clinical research fellowship grant from the Doris Duke Charitable Foundation to Columbia University. Dr. Mintz has served as a consultant for ACIST Medical Systems; and has served as a consultant and received grant or fellowship support from Volcano Corporation, Boston Scientific, and Infraredx. Dr. Mehran has received research grants from Sanofi-Aventis, The Medicines Company, Abbott Vascular, Boston Scientific, Bristol-Myers Squibb, and AstraZeneca; has served as a consultant/advisory board member for Abbott Vascular, Covidien, CSL Behring, Janssen Pharmaceuticals, Maya Medical, Merck & Co., Inc., Regado Biosciences, Sanofi-Aventis, Eli Lilly and Company, and Journal of the American College of Cardiology Vol. 63, No. 18, 2014 Ó 2014 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00 Published by Elsevier Inc. http://dx.doi.org/10.1016/j.jacc.2014.01.034

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Journal of the American College of Cardiology Vol. 63, No. 18, 2014� 2014 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00Published by Elsevier Inc. http://dx.doi.org/10.1016/j.jacc.2014.01.034
Ischemic Outcomes After CoronaryIntervention of Calcified Vesselsin Acute Coronary Syndromes
Pooled Analysis From the HORIZONS-AMI(Harmonizing Outcomes With Revascularization andStents in Acute Myocardial Infarction) and ACUITY(Acute Catheterization and Urgent Intervention Triage Strategy) TrialsPhilippe Généreux, MD,*yz Mahesh V. Madhavan, BA,* Gary S. Mintz, MD,*y Akiko Maehara, MD,*yTullio Palmerini, MD,x Laura LaSalle, BA,y Ke Xu, PHD,y Tom McAndrew, MS,yAjay Kirtane, MD, SM,*y Alexandra J. Lansky, MD,k Sorin J. Brener, MD,y{ Roxana Mehran, MD,y#Gregg W. Stone, MD*yNew York, New York; Montréal, Québec, Canada; Bologna, Italy; and New Haven, Connecticut
From the *N
New York, N
zHôpital du
Canada; xIsof Medicine
New York;
Généreux a
Madhavan
Objectives T
ew York-Presbyterian Ho
ew York; yCardiovasculaSacré-Coeur de Montré
tituto di Cardiologia, Univ
, New Haven, Connecticu
and the #Mount Sinai
nd Palmerini have recei
was supported by a clini
his study sought to determine the frequency and impact of coronary calcification among patients undergoingpercutaneous coronary intervention (PCI) for acute coronary syndromes (ACS).
Background S
mall studies in patients with stable coronary artery disease have suggested a worse prognosis after PCI of calcifiedcompared with noncalcified lesions. Little is known about the impact of coronary calcification on outcomes after PCIfor patients presenting with non–ST-segment elevation and ST-segment elevation ACS.Methods D
ata from 6,855 patients presenting with ACS in whom PCI was performed were pooled from 2 large-scalerandomized, controlled trials, ACUITY (Acute Catheterization and Urgent Intervention Triage Strategy) andHORIZONS-AMI (Harmonizing Outcomes With Revascularization and Stents in Acute Myocardial Infarction). One-yearoutcomes were analyzed according to the severity of PCI target lesion calcification (none/mild, moderate, or severe)as assessed by an independent angiographic core laboratory.Results T
arget lesion calcification was severe in 402 patients (5.9%), moderate in 1,788 (26.1%), and none/mild in 4,665(68.1%). Moderate/severe target lesion calcification was more frequent in older patients, men, hypertensivepatients, and those presenting with ST-segment elevation myocardial infarction (STEMI). The unadjusted 1-year ratesof death, cardiac death, definite stent thrombosis, and ischemic target lesion revascularization (TLR) and targetvessel revascularization were significantly increased in patients with moderate/severe target lesion calcification. Bymultivariable analysis, the presence of moderate/severe target lesion calcification was an independent predictor of1-year definite stent thrombosis (hazard ratio [HR]: 1.62; 95% confidence interval [CI]: 1.14 to 2.30; p ¼ 0.007) andischemic TLR (HR: 1.44; 95% CI: 1.17 to 1.78; p ¼ 0.0007).Conclusions M
oderate/severe lesion calcification was relatively frequent in patients with non–ST-segment elevation ACS andSTEMI and was strongly predictive of stent thrombosis and ischemic TLR at 1 year. (Comparison of Angiomax VersusHeparin in Acute Coronary Syndromes [ACS]; NCT00093158; Harmonizing Outcomes With Revascularization andStents in Acute Myocardial Infarction; NCT00433966) (J Am Coll Cardiol 2014;63:1845–54) ª 2014 by theAmerican College of Cardiology Foundationspital and Columbia University Medical Center,
r Research Foundation, New York, New York;
al, Université de Montréal, Montréal, Québec,
ersity of Bologna, Bologna, Italy; kYale Schoolt; {New York Methodist Hospital, New York,
Medical Center, New York, New York. Drs.
ved speaker fees from Abbott Vascular. Mr.
cal research fellowship grant from the Doris
Duke Charitable Foundation to Columbia University. Dr. Mintz has served as a
consultant for ACIST Medical Systems; and has served as a consultant and
received grant or fellowship support from Volcano Corporation, Boston Scientific,
and Infraredx. Dr. Mehran has received research grants from Sanofi-Aventis, The
Medicines Company, Abbott Vascular, Boston Scientific, Bristol-Myers Squibb,
and AstraZeneca; has served as a consultant/advisory board member for Abbott
Vascular, Covidien, CSL Behring, Janssen Pharmaceuticals, Maya Medical, Merck
& Co., Inc., Regado Biosciences, Sanofi-Aventis, Eli Lilly and Company, and
Daiichi Sankyo; and is a sharehold
consultant for Boston Scientific and
have reported that they have no relat
to disclose. The first 2 authors cont
Manuscript received June 19, 2013
accepted January 6, 2014.
See
Abbreviationsand Acronyms
BMS = bare-metal stent(s)
DES = drug-eluting stent(s)
GPI = glycoprotein IIb/IIIa
inhibitor
NSTEACS = non–ST-segment
elevation acute coronary
syndromes
PCI = percutaneous coronary
intervention
QCA = quantitative coronary
angiography
STEMI = ST-segment
elevation myocardial
infarction
TLR = target lesion
revascularization
Généreux et al. JACC Vol. 63, No. 18, 2014Coronary Calcification and Percutaneous Coronary Intervention May 13, 2014:1845–54
1846
Compared with bare-metal stents(BMS), drug-eluting stents (DES)improve clinical and angiographicoutcomes in patients with coro-nary artery disease undergoingpercutaneous coronary interven-tion (PCI) (1,2). Although favo-rable results may be achieved withPCI in complex lesions (3–6),patients with moderately andseverely calcified lesions havebeen excluded from enrollment inmost stent trials and still repre-sent a challenge even in the DESera. Coronary calcification mayimpair stent delivery and expan-sion and damage the polymer/drug coating, resulting in im-paired drug delivery and predis-
position to restenosis and stent thrombosis (7). Whereassmall studies in the BMS era demonstrated reduced event-free survival after PCI of calcified compared with non-calcified lesions, surprisingly little is known about the effectof coronary calcification on outcomes after PCI with DES
page 1855
(8–12). Moreover, no studies have evaluated the frequencyand impact of coronary calcification in patients presentingwith non–ST-segment elevation acute coronary syndromes(NSTEACS) and ST-segment elevation myocardial infarc-tion (STEMI). We therefore sought to determine the fre-quency and impact of target lesion coronary calcification onclinical events in patients in whom PCI was performed inthe setting of NSTEACS or STEMI in a pooled analysisfrom the large-scale ACUITY (Acute Catheterization andUrgent Intervention Triage Strategy) andHORIZONS-AMI(Harmonizing Outcomes With Revascularization and Stentsin Acute Myocardial Infarction) trials (13,14).
Methods
Study designs and patients. The ACUITY andHORIZONS-AMI trial designs and results have previouslybeen described in detail (13–16). In brief, ACUITY was amulticenter, prospective, randomized trial of 13,819 patientswith moderate- and high-risk NSTEACS who were treatedwith an early invasive strategy. Prior to coronary angiog-raphy, patients were randomly assigned to heparin (unfrac-tionated or low-molecular-weight) plus a glycoprotein IIb/
er in Endothelix. Dr. Stone has served as a
Cardiovascular Systems, Inc. All other authors
ionships relevant to the contents of this paper
ributed equally to this paper.
; revised manuscript received January 5, 2014,
IIIa inhibitor (GPI), bivalirudin plus a GPI, or bivalirudinmonotherapy. Angiography was performed within 72 h ofrandomization, and depending on coronary anatomy, patientswere triaged to PCI, coronary artery bypass graft (CABG)surgery, or medical therapy. In patients undergoing PCI,stent choice (BMS or DES) was per operator discretion. Dualantiplatelet therapy with aspirin and clopidogrel was recom-mended for at least 1 year. In HORIZONS-AMI, 3,602patients with STEMI presenting within 12 h of symptomonset were randomly assigned to unfractionated heparin plusGPI or bivalirudin monotherapy. Immediate coronary angi-ographywas performed after randomization, followed byPCI,CABG, or medical management at physician discretion.Eligible patients were randomized again (3:1) to receivepaclitaxel-eluting stents (Boston Scientific, Natick, Massa-chusetts) or otherwise identical BMS (Boston Scientific).Aspirin and clopidogrel were administered before catheteri-zation; aspirin was continued indefinitely and clopidogrel forat least 1 year (14,16). Patients with severe renal insufficiency(calculated creatinine clearance <30 ml/min) were notincluded in either trial.
Patients in whom qualitative and quantitative coronaryangiography (QCA) was performed comprised the presentstudy population. QCA was performed at the Cardiovas-cular Research Foundation (New York, New York) bytechnicians blinded to randomization and outcomes in allpatients in the HORIZONS-AMI trial and in those en-rolled in the formal ACUITY angiographic substudy, aspreviously described (17). Interobserver and intraobserverQCA core laboratory variability kappa values (50 coronaryangiograms assessed twice [8 weeks apart] by 12 angio-graphic core laboratory technicians) for the degree of targetlesion calcification were 0.83 and 0.89, respectively, repre-senting excellent agreement. Independent clinical eventscommittees, blinded to treatment assignment, adjudicatedall major adverse events in both trials.Objectives and angiographic analysis. The primary studyobjective was to assess the relationship between the presenceand extent of target lesion coronary calcification and the1-year rate of ischemic events, including death, cardiacdeath, reinfarction, definite stent thrombosis, and ischemictarget lesion revascularization (TLR) and target vesselrevascularization. For the present report, we limited ouranalyses to the patients with STEMI in whom PCI wasperformed in the HORIZONS-AMI trial and to thepatients with NSTEACS in whom PCI was performed inthe formal angiographic substudy from ACUITY (17).Endpoint definitions and statistical analysis. The ACUITYand HORIZONS databases were combined, and patientsfrom this pooled population were stratified on the basis ofseverity of coronary artery calcification (none/mild, moder-ate, and severe). The pre-specified angiographic core labo-ratory definition of moderate calcification was radiopaquedensities noted only during the cardiac cycle and typicallyinvolving only one side of the vascular wall. Severe calcifi-cation was defined as radiopaque densities noted without
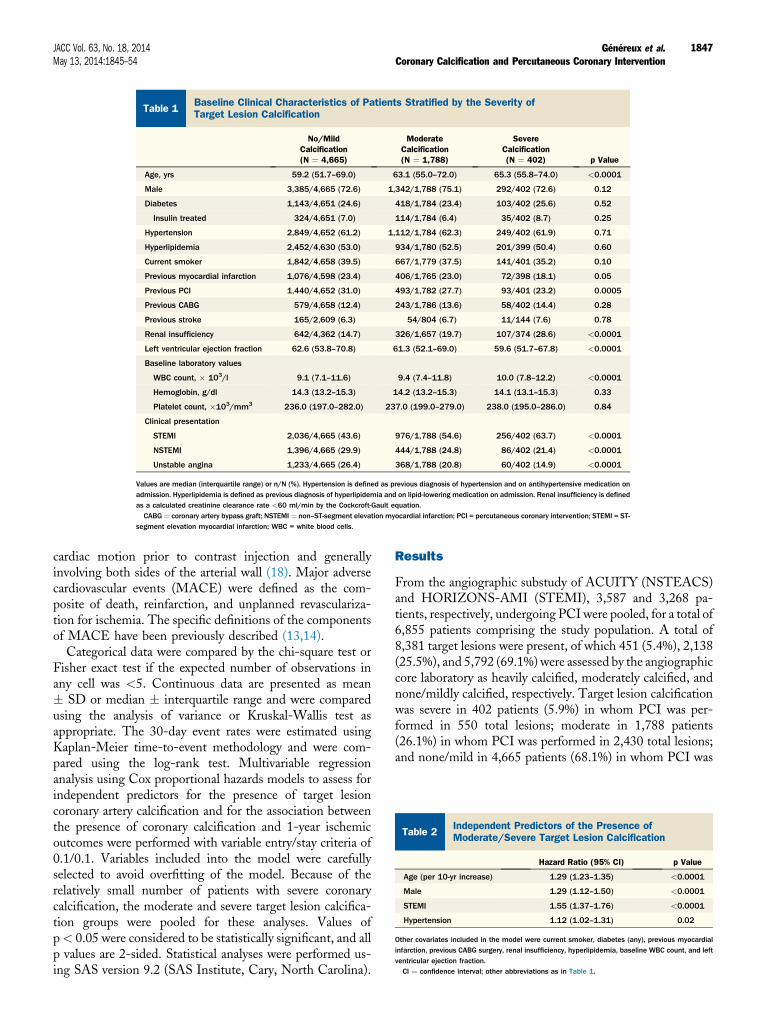
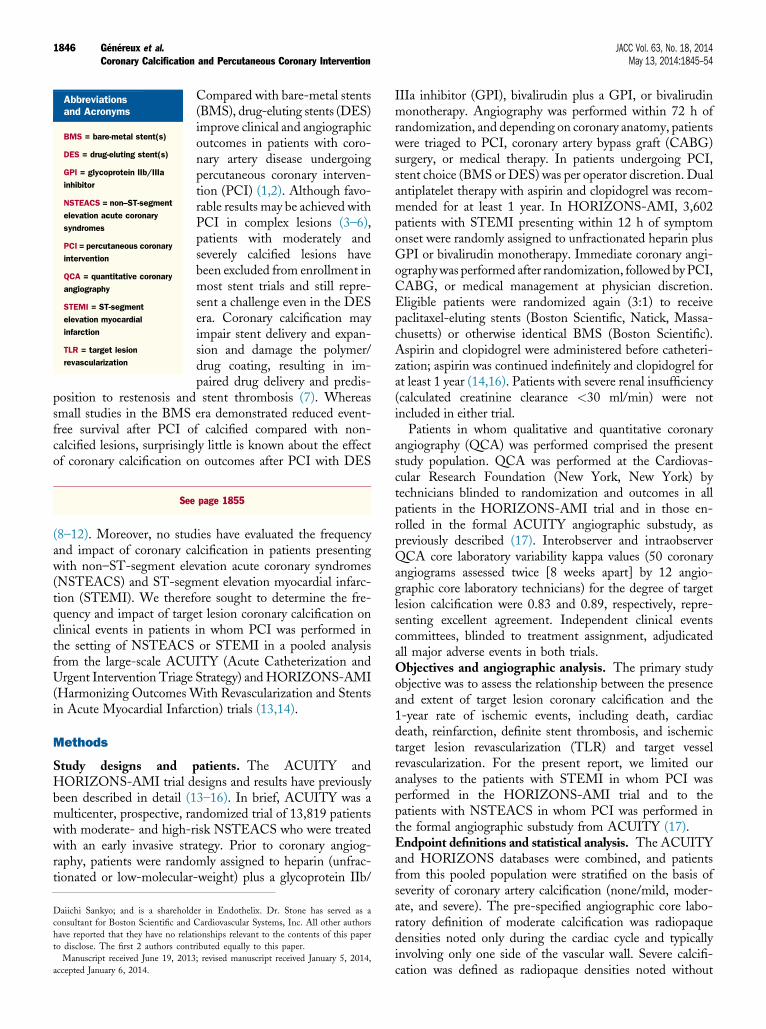
Table 1Baseline Clinical Characteristics of Patients Stratified by the Severity ofTarget Lesion Calcification
No/MildCalcification(N ¼ 4,665)
ModerateCalcification(N ¼ 1,788)
SevereCalcification(N ¼ 402) p Value
Age, yrs 59.2 (51.7–69.0) 63.1 (55.0–72.0) 65.3 (55.8–74.0) <0.0001
Male 3,385/4,665 (72.6) 1,342/1,788 (75.1) 292/402 (72.6) 0.12
Diabetes 1,143/4,651 (24.6) 418/1,784 (23.4) 103/402 (25.6) 0.52
Insulin treated 324/4,651 (7.0) 114/1,784 (6.4) 35/402 (8.7) 0.25
Hypertension 2,849/4,652 (61.2) 1,112/1,784 (62.3) 249/402 (61.9) 0.71
Hyperlipidemia 2,452/4,630 (53.0) 934/1,780 (52.5) 201/399 (50.4) 0.60
Current smoker 1,842/4,658 (39.5) 667/1,779 (37.5) 141/401 (35.2) 0.10
Previous myocardial infarction 1,076/4,598 (23.4) 406/1,765 (23.0) 72/398 (18.1) 0.05
Previous PCI 1,440/4,652 (31.0) 493/1,782 (27.7) 93/401 (23.2) 0.0005
Previous CABG 579/4,658 (12.4) 243/1,786 (13.6) 58/402 (14.4) 0.28
Previous stroke 165/2,609 (6.3) 54/804 (6.7) 11/144 (7.6) 0.78
Renal insufficiency 642/4,362 (14.7) 326/1,657 (19.7) 107/374 (28.6) <0.0001
Left ventricular ejection fraction 62.6 (53.8–70.8) 61.3 (52.1–69.0) 59.6 (51.7–67.8) <0.0001
Baseline laboratory values
WBC count, � 103/l 9.1 (7.1–11.6) 9.4 (7.4–11.8) 10.0 (7.8–12.2) <0.0001
Hemoglobin, g/dl 14.3 (13.2–15.3) 14.2 (13.2–15.3) 14.1 (13.1–15.3) 0.33
Platelet count, �103/mm3 236.0 (197.0–282.0) 237.0 (199.0–279.0) 238.0 (195.0–286.0) 0.84
Clinical presentation
STEMI 2,036/4,665 (43.6) 976/1,788 (54.6) 256/402 (63.7) <0.0001
NSTEMI 1,396/4,665 (29.9) 444/1,788 (24.8) 86/402 (21.4) <0.0001
Unstable angina 1,233/4,665 (26.4) 368/1,788 (20.8) 60/402 (14.9) <0.0001
Values are median (interquartile range) or n/N (%). Hypertension is defined as previous diagnosis of hypertension and on antihypertensive medication onadmission. Hyperlipidemia is defined as previous diagnosis of hyperlipidemia and on lipid-lowering medication on admission. Renal insufficiency is definedas a calculated creatinine clearance rate <60 ml/min by the Cockcroft-Gault equation.CABG ¼ coronary artery bypass graft; NSTEMI ¼ non–ST-segment elevation myocardial infarction; PCI = percutaneous coronary intervention; STEMI = ST-
segment elevation myocardial infarction; WBC = white blood cells.
Table 2Independent Predictors of the Presence ofModerate/Severe Target Lesion Calcification
Hazard Ratio (95% CI) p Value
Age (per 10-yr increase) 1.29 (1.23–1.35) <0.0001
Male 1.29 (1.12–1.50) <0.0001
STEMI 1.55 (1.37–1.76) <0.0001
Hypertension 1.12 (1.02–1.31) 0.02
Other covariates included in the model were current smoker, diabetes (any), previous myocardialinfarction, previous CABG surgery, renal insufficiency, hyperlipidemia, baseline WBC count, and leftventricular ejection fraction.CI ¼ confidence interval; other abbreviations as in Table 1.
JACC Vol. 63, No. 18, 2014 Généreux et al.May 13, 2014:1845–54 Coronary Calcification and Percutaneous Coronary Intervention
1847
cardiac motion prior to contrast injection and generallyinvolving both sides of the arterial wall (18). Major adversecardiovascular events (MACE) were defined as the com-posite of death, reinfarction, and unplanned revasculariza-tion for ischemia. The specific definitions of the componentsof MACE have been previously described (13,14).
Categorical data were compared by the chi-square test orFisher exact test if the expected number of observations inany cell was <5. Continuous data are presented as mean� SD or median � interquartile range and were comparedusing the analysis of variance or Kruskal-Wallis test asappropriate. The 30-day event rates were estimated usingKaplan-Meier time-to-event methodology and were com-pared using the log-rank test. Multivariable regressionanalysis using Cox proportional hazards models to assess forindependent predictors for the presence of target lesioncoronary artery calcification and for the association betweenthe presence of coronary calcification and 1-year ischemicoutcomes were performed with variable entry/stay criteria of0.1/0.1. Variables included into the model were carefullyselected to avoid overfitting of the model. Because of therelatively small number of patients with severe coronarycalcification, the moderate and severe target lesion calcifica-tion groups were pooled for these analyses. Values ofp< 0.05 were considered to be statistically significant, and allp values are 2-sided. Statistical analyses were performed us-ing SAS version 9.2 (SAS Institute, Cary, North Carolina).
Results
From the angiographic substudy of ACUITY (NSTEACS)and HORIZONS-AMI (STEMI), 3,587 and 3,268 pa-tients, respectively, undergoing PCI were pooled, for a total of6,855 patients comprising the study population. A total of8,381 target lesions were present, of which 451 (5.4%), 2,138(25.5%), and 5,792 (69.1%) were assessed by the angiographiccore laboratory as heavily calcified, moderately calcified, andnone/mildly calcified, respectively. Target lesion calcificationwas severe in 402 patients (5.9%) in whom PCI was per-formed in 550 total lesions; moderate in 1,788 patients(26.1%) in whom PCI was performed in 2,430 total lesions;and none/mild in 4,665 patients (68.1%) in whom PCI was
Généreux et al. JACC Vol. 63, No. 18, 2014Coronary Calcification and Percutaneous Coronary Intervention May 13, 2014:1845–54
1848
performed in 5,829 total lesions. A total of 54 patients hadboth moderately and severely calcified lesions.Patient characteristics, angiographic findings, and treatmentrandomization. As shown in Table 1 and Online Table 1,compared with patients without calcified lesions, patients with
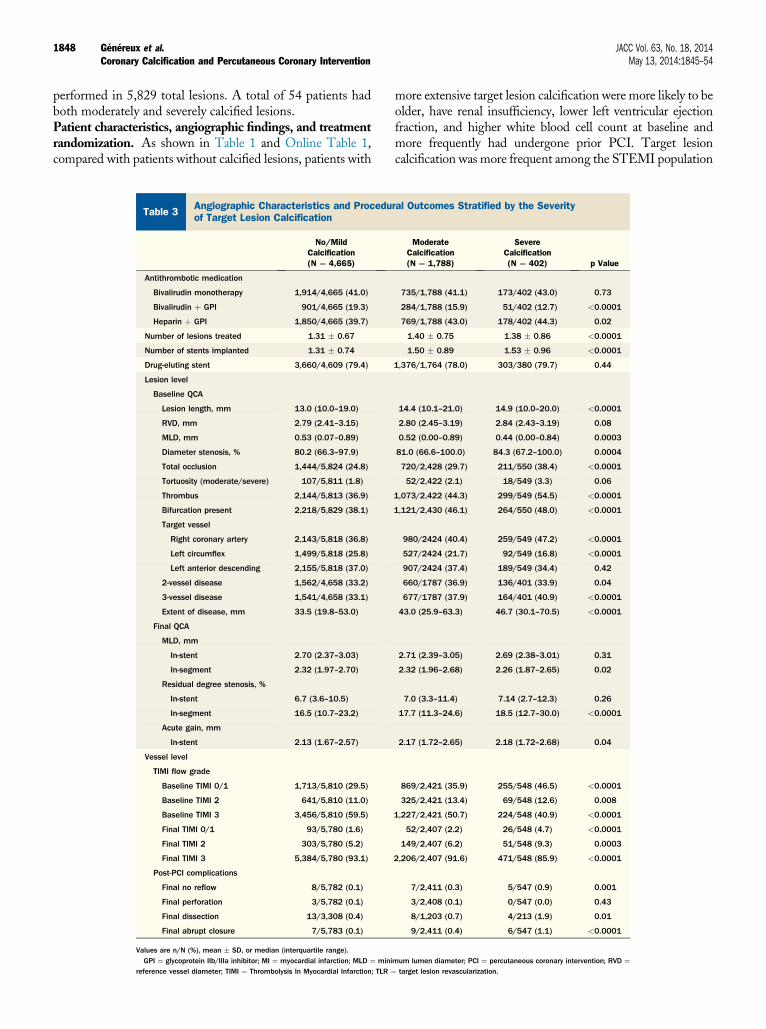
Table 3Angiographic Characteristics and Proceduof Target Lesion Calcification
No/MildCalcification(N ¼ 4,665)
Antithrombotic medication
Bivalirudin monotherapy 1,914/4,665 (41.0)
Bivalirudin þ GPI 901/4,665 (19.3)
Heparin þ GPI 1,850/4,665 (39.7)
Number of lesions treated 1.31 � 0.67
Number of stents implanted 1.31 � 0.74
Drug-eluting stent 3,660/4,609 (79.4)
Lesion level
Baseline QCA
Lesion length, mm 13.0 (10.0–19.0)
RVD, mm 2.79 (2.41–3.15)
MLD, mm 0.53 (0.07–0.89)
Diameter stenosis, % 80.2 (66.3–97.9)
Total occlusion 1,444/5,824 (24.8)
Tortuosity (moderate/severe) 107/5,811 (1.8)
Thrombus 2,144/5,813 (36.9)
Bifurcation present 2,218/5,829 (38.1)
Target vessel
Right coronary artery 2,143/5,818 (36.8)
Left circumflex 1,499/5,818 (25.8)
Left anterior descending 2,155/5,818 (37.0)
2-vessel disease 1,562/4,658 (33.2)
3-vessel disease 1,541/4,658 (33.1)
Extent of disease, mm 33.5 (19.8–53.0)
Final QCA
MLD, mm
In-stent 2.70 (2.37–3.03)
In-segment 2.32 (1.97–2.70)
Residual degree stenosis, %
In-stent 6.7 (3.6–10.5)
In-segment 16.5 (10.7–23.2)
Acute gain, mm
In-stent 2.13 (1.67–2.57)
Vessel level
TIMI flow grade
Baseline TIMI 0/1 1,713/5,810 (29.5)
Baseline TIMI 2 641/5,810 (11.0)
Baseline TIMI 3 3,456/5,810 (59.5)
Final TIMI 0/1 93/5,780 (1.6)
Final TIMI 2 303/5,780 (5.2)
Final TIMI 3 5,384/5,780 (93.1)
Post-PCI complications
Final no reflow 8/5,782 (0.1)
Final perforation 3/5,782 (0.1)
Final dissection 13/3,308 (0.4)
Final abrupt closure 7/5,783 (0.1)
Values are n/N (%), mean � SD, or median (interquartile range).GPI ¼ glycoprotein IIb/IIIa inhibitor; MI ¼ myocardial infarction; MLD ¼ mini
reference vessel diameter; TIMI ¼ Thrombolysis In Myocardial Infarction; TLR ¼
more extensive target lesion calcification were more likely to beolder, have renal insufficiency, lower left ventricular ejectionfraction, and higher white blood cell count at baseline andmore frequently had undergone prior PCI. Target lesioncalcification was more frequent among the STEMI population
ral Outcomes Stratified by the Severity
ModerateCalcification(N ¼ 1,788)
SevereCalcification(N ¼ 402) p Value
735/1,788 (41.1) 173/402 (43.0) 0.73
284/1,788 (15.9) 51/402 (12.7) <0.0001
769/1,788 (43.0) 178/402 (44.3) 0.02
1.40 � 0.75 1.38 � 0.86 <0.0001
1.50 � 0.89 1.53 � 0.96 <0.0001
1,376/1,764 (78.0) 303/380 (79.7) 0.44
14.4 (10.1–21.0) 14.9 (10.0–20.0) <0.0001
2.80 (2.45–3.19) 2.84 (2.43–3.19) 0.08
0.52 (0.00–0.89) 0.44 (0.00–0.84) 0.0003
81.0 (66.6–100.0) 84.3 (67.2–100.0) 0.0004
720/2,428 (29.7) 211/550 (38.4) <0.0001
52/2,422 (2.1) 18/549 (3.3) 0.06
1,073/2,422 (44.3) 299/549 (54.5) <0.0001
1,121/2,430 (46.1) 264/550 (48.0) <0.0001
980/2424 (40.4) 259/549 (47.2) <0.0001
527/2424 (21.7) 92/549 (16.8) <0.0001
907/2424 (37.4) 189/549 (34.4) 0.42
660/1787 (36.9) 136/401 (33.9) 0.04
677/1787 (37.9) 164/401 (40.9) <0.0001
43.0 (25.9–63.3) 46.7 (30.1–70.5) <0.0001
2.71 (2.39–3.05) 2.69 (2.38–3.01) 0.31
2.32 (1.96–2.68) 2.26 (1.87–2.65) 0.02
7.0 (3.3–11.4) 7.14 (2.7–12.3) 0.26
17.7 (11.3–24.6) 18.5 (12.7–30.0) <0.0001
2.17 (1.72–2.65) 2.18 (1.72–2.68) 0.04
869/2,421 (35.9) 255/548 (46.5) <0.0001
325/2,421 (13.4) 69/548 (12.6) 0.008
1,227/2,421 (50.7) 224/548 (40.9) <0.0001
52/2,407 (2.2) 26/548 (4.7) <0.0001
149/2,407 (6.2) 51/548 (9.3) 0.0003
2,206/2,407 (91.6) 471/548 (85.9) <0.0001
7/2,411 (0.3) 5/547 (0.9) 0.001
3/2,408 (0.1) 0/547 (0.0) 0.43
8/1,203 (0.7) 4/213 (1.9) 0.01
9/2,411 (0.4) 6/547 (1.1) <0.0001
mum lumen diameter; PCI ¼ percutaneous coronary intervention; RVD ¼target lesion revascularization.
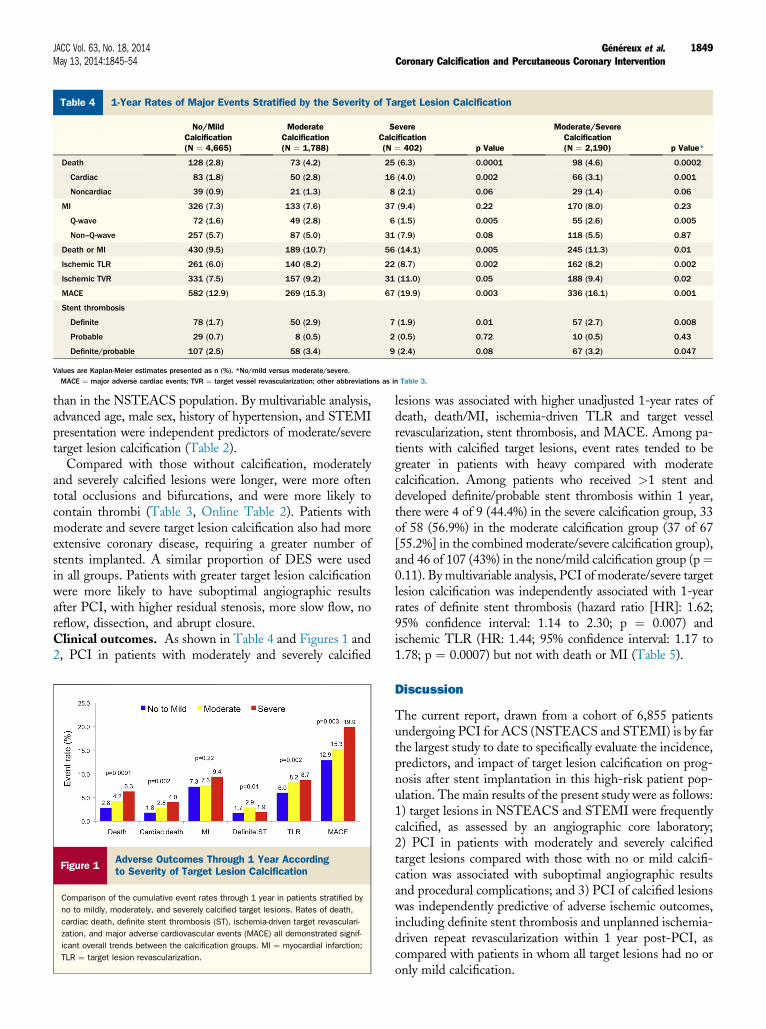
Table 4 1-Year Rates of Major Events Stratified by the Severity of Target Lesion Calcification
No/MildCalcification(N ¼ 4,665)
ModerateCalcification(N ¼ 1,788)
SevereCalcification(N ¼ 402) p Value
Moderate/SevereCalcification(N ¼ 2,190) p Value*
Death 128 (2.8) 73 (4.2) 25 (6.3) 0.0001 98 (4.6) 0.0002
Cardiac 83 (1.8) 50 (2.8) 16 (4.0) 0.002 66 (3.1) 0.001
Noncardiac 39 (0.9) 21 (1.3) 8 (2.1) 0.06 29 (1.4) 0.06
MI 326 (7.3) 133 (7.6) 37 (9.4) 0.22 170 (8.0) 0.23
Q-wave 72 (1.6) 49 (2.8) 6 (1.5) 0.005 55 (2.6) 0.005
Non–Q-wave 257 (5.7) 87 (5.0) 31 (7.9) 0.08 118 (5.5) 0.87
Death or MI 430 (9.5) 189 (10.7) 56 (14.1) 0.005 245 (11.3) 0.01
Ischemic TLR 261 (6.0) 140 (8.2) 22 (8.7) 0.002 162 (8.2) 0.002
Ischemic TVR 331 (7.5) 157 (9.2) 31 (11.0) 0.05 188 (9.4) 0.02
MACE 582 (12.9) 269 (15.3) 67 (19.9) 0.003 336 (16.1) 0.001
Stent thrombosis
Definite 78 (1.7) 50 (2.9) 7 (1.9) 0.01 57 (2.7) 0.008
Probable 29 (0.7) 8 (0.5) 2 (0.5) 0.72 10 (0.5) 0.43
Definite/probable 107 (2.5) 58 (3.4) 9 (2.4) 0.08 67 (3.2) 0.047
Values are Kaplan-Meier estimates presented as n (%). *No/mild versus moderate/severe.MACE ¼ major adverse cardiac events; TVR ¼ target vessel revascularization; other abbreviations as in Table 3.
JACC Vol. 63, No. 18, 2014 Généreux et al.May 13, 2014:1845–54 Coronary Calcification and Percutaneous Coronary Intervention
1849
than in the NSTEACS population. By multivariable analysis,advanced age, male sex, history of hypertension, and STEMIpresentation were independent predictors of moderate/severetarget lesion calcification (Table 2).
Compared with those without calcification, moderatelyand severely calcified lesions were longer, were more oftentotal occlusions and bifurcations, and were more likely tocontain thrombi (Table 3, Online Table 2). Patients withmoderate and severe target lesion calcification also had moreextensive coronary disease, requiring a greater number ofstents implanted. A similar proportion of DES were usedin all groups. Patients with greater target lesion calcificationwere more likely to have suboptimal angiographic resultsafter PCI, with higher residual stenosis, more slow flow, noreflow, dissection, and abrupt closure.Clinical outcomes. As shown in Table 4 and Figures 1 and2, PCI in patients with moderately and severely calcified
Figure 1Adverse Outcomes Through 1 Year Accordingto Severity of Target Lesion Calcification
Comparison of the cumulative event rates through 1 year in patients stratified by
no to mildly, moderately, and severely calcified target lesions. Rates of death,
cardiac death, definite stent thrombosis (ST), ischemia-driven target revasculari-
zation, and major adverse cardiovascular events (MACE) all demonstrated signif-
icant overall trends between the calcification groups. MI ¼ myocardial infarction;
TLR ¼ target lesion revascularization.
lesions was associated with higher unadjusted 1-year rates ofdeath, death/MI, ischemia-driven TLR and target vesselrevascularization, stent thrombosis, and MACE. Among pa-tients with calcified target lesions, event rates tended to begreater in patients with heavy compared with moderatecalcification. Among patients who received >1 stent anddeveloped definite/probable stent thrombosis within 1 year,there were 4 of 9 (44.4%) in the severe calcification group, 33of 58 (56.9%) in the moderate calcification group (37 of 67[55.2%] in the combined moderate/severe calcification group),and 46 of 107 (43%) in the none/mild calcification group (p¼0.11). By multivariable analysis, PCI of moderate/severe targetlesion calcification was independently associated with 1-yearrates of definite stent thrombosis (hazard ratio [HR]: 1.62;95% confidence interval: 1.14 to 2.30; p ¼ 0.007) andischemic TLR (HR: 1.44; 95% confidence interval: 1.17 to1.78; p ¼ 0.0007) but not with death or MI (Table 5).
Discussion
The current report, drawn from a cohort of 6,855 patientsundergoing PCI for ACS (NSTEACS and STEMI) is by farthe largest study to date to specifically evaluate the incidence,predictors, and impact of target lesion calcification on prog-nosis after stent implantation in this high-risk patient pop-ulation. The main results of the present study were as follows:1) target lesions in NSTEACS and STEMI were frequentlycalcified, as assessed by an angiographic core laboratory;2) PCI in patients with moderately and severely calcifiedtarget lesions compared with those with no or mild calcifi-cation was associated with suboptimal angiographic resultsand procedural complications; and 3) PCI of calcified lesionswas independently predictive of adverse ischemic outcomes,including definite stent thrombosis and unplanned ischemia-driven repeat revascularization within 1 year post-PCI, ascompared with patients in whom all target lesions had no oronly mild calcification.
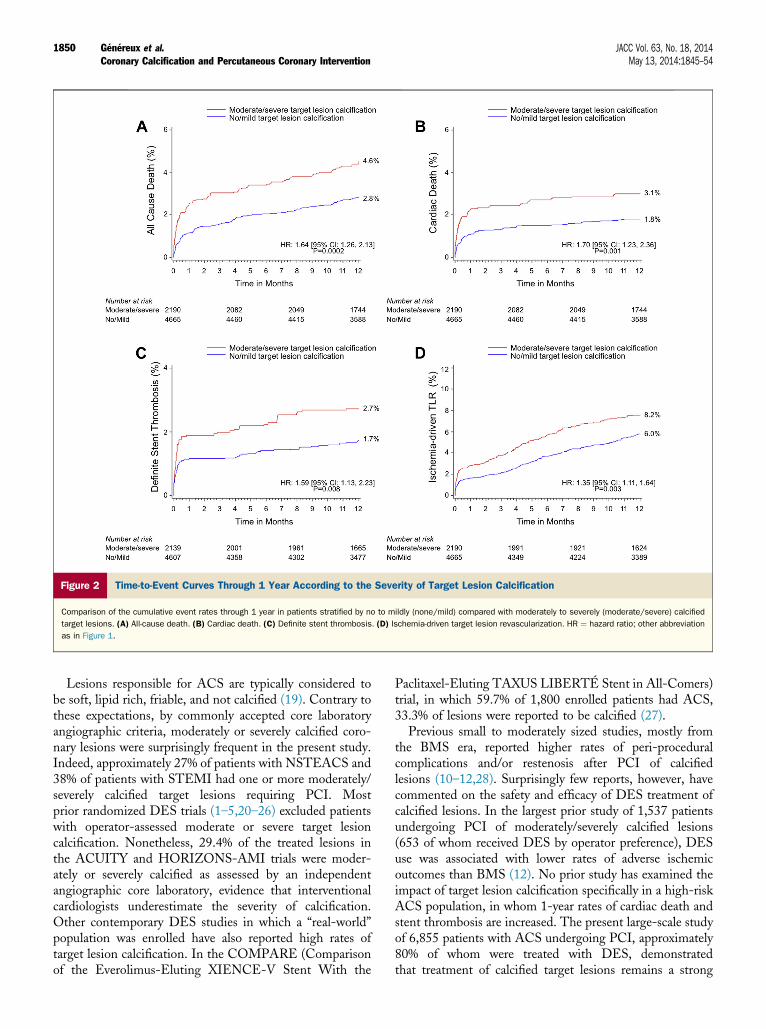
Figure 2 Time-to-Event Curves Through 1 Year According to the Severity of Target Lesion Calcification
Comparison of the cumulative event rates through 1 year in patients stratified by no to mildly (none/mild) compared with moderately to severely (moderate/severe) calcified
target lesions. (A) All-cause death. (B) Cardiac death. (C) Definite stent thrombosis. (D) Ischemia-driven target lesion revascularization. HR ¼ hazard ratio; other abbreviation
as in Figure 1.
Généreux et al. JACC Vol. 63, No. 18, 2014Coronary Calcification and Percutaneous Coronary Intervention May 13, 2014:1845–54
1850
Lesions responsible for ACS are typically considered tobe soft, lipid rich, friable, and not calcified (19). Contrary tothese expectations, by commonly accepted core laboratoryangiographic criteria, moderately or severely calcified coro-nary lesions were surprisingly frequent in the present study.Indeed, approximately 27% of patients with NSTEACS and38% of patients with STEMI had one or more moderately/severely calcified target lesions requiring PCI. Mostprior randomized DES trials (1–5,20–26) excluded patientswith operator-assessed moderate or severe target lesioncalcification. Nonetheless, 29.4% of the treated lesions inthe ACUITY and HORIZONS-AMI trials were moder-ately or severely calcified as assessed by an independentangiographic core laboratory, evidence that interventionalcardiologists underestimate the severity of calcification.Other contemporary DES studies in which a “real-world”population was enrolled have also reported high rates oftarget lesion calcification. In the COMPARE (Comparisonof the Everolimus-Eluting XIENCE-V Stent With the
Paclitaxel-Eluting TAXUS LIBERTÉ Stent in All-Comers)trial, in which 59.7% of 1,800 enrolled patients had ACS,33.3% of lesions were reported to be calcified (27).
Previous small to moderately sized studies, mostly fromthe BMS era, reported higher rates of peri-proceduralcomplications and/or restenosis after PCI of calcifiedlesions (10–12,28). Surprisingly few reports, however, havecommented on the safety and efficacy of DES treatment ofcalcified lesions. In the largest prior study of 1,537 patientsundergoing PCI of moderately/severely calcified lesions(653 of whom received DES by operator preference), DESuse was associated with lower rates of adverse ischemicoutcomes than BMS (12). No prior study has examined theimpact of target lesion calcification specifically in a high-riskACS population, in whom 1-year rates of cardiac death andstent thrombosis are increased. The present large-scale studyof 6,855 patients with ACS undergoing PCI, approximately80% of whom were treated with DES, demonstratedthat treatment of calcified target lesions remains a strong
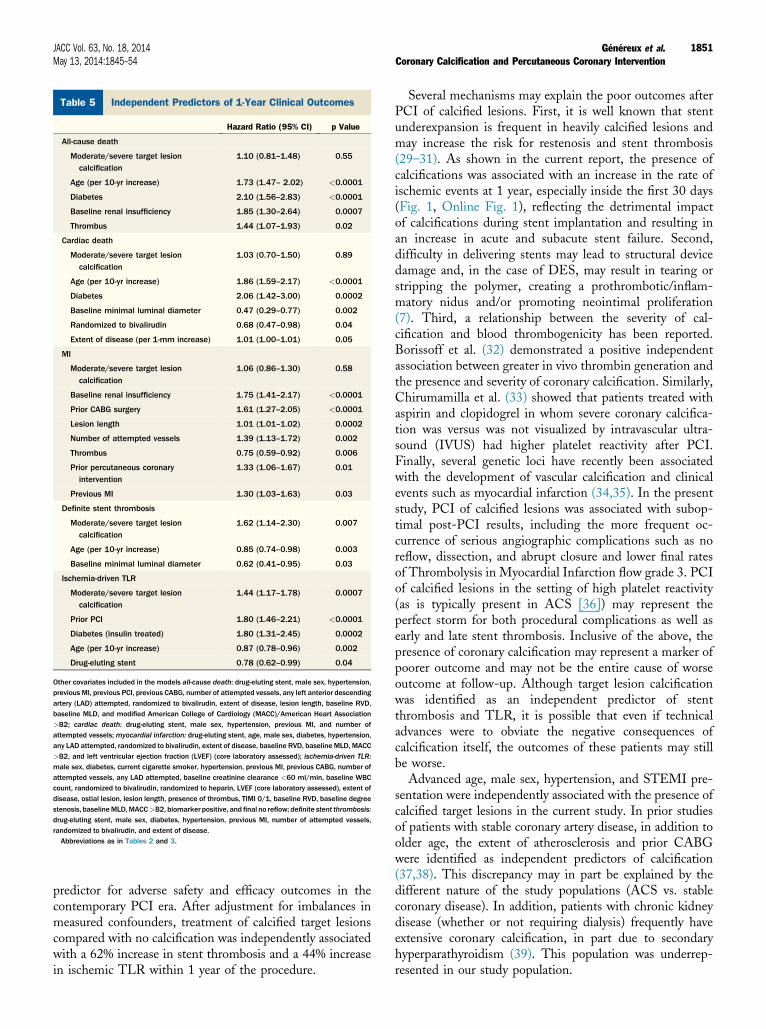
Table 5 Independent Predictors of 1-Year Clinical Outcomes
Hazard Ratio (95% CI) p Value
All-cause death
Moderate/severe target lesioncalcification
1.10 (0.81–1.48) 0.55
Age (per 10-yr increase) 1.73 (1.47– 2.02) <0.0001
Diabetes 2.10 (1.56–2.83) <0.0001
Baseline renal insufficiency 1.85 (1.30–2.64) 0.0007
Thrombus 1.44 (1.07–1.93) 0.02
Cardiac death
Moderate/severe target lesioncalcification
1.03 (0.70–1.50) 0.89
Age (per 10-yr increase) 1.86 (1.59–2.17) <0.0001
Diabetes 2.06 (1.42–3.00) 0.0002
Baseline minimal luminal diameter 0.47 (0.29–0.77) 0.002
Randomized to bivalirudin 0.68 (0.47–0.98) 0.04
Extent of disease (per 1-mm increase) 1.01 (1.00–1.01) 0.05
MI
Moderate/severe target lesioncalcification
1.06 (0.86–1.30) 0.58
Baseline renal insufficiency 1.75 (1.41–2.17) <0.0001
Prior CABG surgery 1.61 (1.27–2.05) <0.0001
Lesion length 1.01 (1.01–1.02) 0.0002
Number of attempted vessels 1.39 (1.13–1.72) 0.002
Thrombus 0.75 (0.59–0.92) 0.006
Prior percutaneous coronaryintervention
1.33 (1.06–1.67) 0.01
Previous MI 1.30 (1.03–1.63) 0.03
Definite stent thrombosis
Moderate/severe target lesioncalcification
1.62 (1.14–2.30) 0.007
Age (per 10-yr increase) 0.85 (0.74–0.98) 0.003
Baseline minimal luminal diameter 0.62 (0.41–0.95) 0.03
Ischemia-driven TLR
Moderate/severe target lesioncalcification
1.44 (1.17–1.78) 0.0007
Prior PCI 1.80 (1.46–2.21) <0.0001
Diabetes (insulin treated) 1.80 (1.31–2.45) 0.0002
Age (per 10-yr increase) 0.87 (0.78–0.96) 0.002
Drug-eluting stent 0.78 (0.62–0.99) 0.04
Other covariates included in the models all-cause death: drug-eluting stent, male sex, hypertension,previous MI, previous PCI, previous CABG, number of attempted vessels, any left anterior descendingartery (LAD) attempted, randomized to bivalirudin, extent of disease, lesion length, baseline RVD,baseline MLD, and modified American College of Cardiology (MACC)/American Heart Association>B2; cardiac death: drug-eluting stent, male sex, hypertension, previous MI, and number ofattempted vessels;myocardial infarction: drug-eluting stent, age, male sex, diabetes, hypertension,any LAD attempted, randomized to bivalirudin, extent of disease, baseline RVD, baseline MLD, MACC>B2, and left ventricular ejection fraction (LVEF) (core laboratory assessed); ischemia-driven TLR:male sex, diabetes, current cigarette smoker, hypertension, previous MI, previous CABG, number ofattempted vessels, any LAD attempted, baseline creatinine clearance <60 ml/min, baseline WBCcount, randomized to bivalirudin, randomized to heparin, LVEF (core laboratory assessed), extent ofdisease, ostial lesion, lesion length, presence of thrombus, TIMI 0/1, baseline RVD, baseline degreestenosis, baselineMLD,MACC>B2, biomarker positive, and final no reflow; definite stent thrombosis:drug-eluting stent, male sex, diabetes, hypertension, previous MI, number of attempted vessels,randomized to bivalirudin, and extent of disease.Abbreviations as in Tables 2 and 3.
JACC Vol. 63, No. 18, 2014 Généreux et al.May 13, 2014:1845–54 Coronary Calcification and Percutaneous Coronary Intervention
1851
predictor for adverse safety and efficacy outcomes in thecontemporary PCI era. After adjustment for imbalances inmeasured confounders, treatment of calcified target lesionscompared with no calcification was independently associatedwith a 62% increase in stent thrombosis and a 44% increasein ischemic TLR within 1 year of the procedure.
Several mechanisms may explain the poor outcomes afterPCI of calcified lesions. First, it is well known that stentunderexpansion is frequent in heavily calcified lesions andmay increase the risk for restenosis and stent thrombosis(29–31). As shown in the current report, the presence ofcalcifications was associated with an increase in the rate ofischemic events at 1 year, especially inside the first 30 days(Fig. 1, Online Fig. 1), reflecting the detrimental impactof calcifications during stent implantation and resulting inan increase in acute and subacute stent failure. Second,difficulty in delivering stents may lead to structural devicedamage and, in the case of DES, may result in tearing orstripping the polymer, creating a prothrombotic/inflam-matory nidus and/or promoting neointimal proliferation(7). Third, a relationship between the severity of cal-cification and blood thrombogenicity has been reported.Borissoff et al. (32) demonstrated a positive independentassociation between greater in vivo thrombin generation andthe presence and severity of coronary calcification. Similarly,Chirumamilla et al. (33) showed that patients treated withaspirin and clopidogrel in whom severe coronary calcifica-tion was versus was not visualized by intravascular ultra-sound (IVUS) had higher platelet reactivity after PCI.Finally, several genetic loci have recently been associatedwith the development of vascular calcification and clinicalevents such as myocardial infarction (34,35). In the presentstudy, PCI of calcified lesions was associated with subop-timal post-PCI results, including the more frequent oc-currence of serious angiographic complications such as noreflow, dissection, and abrupt closure and lower final ratesof Thrombolysis in Myocardial Infarction flow grade 3. PCIof calcified lesions in the setting of high platelet reactivity(as is typically present in ACS [36]) may represent theperfect storm for both procedural complications as well asearly and late stent thrombosis. Inclusive of the above, thepresence of coronary calcification may represent a marker ofpoorer outcome and may not be the entire cause of worseoutcome at follow-up. Although target lesion calcificationwas identified as an independent predictor of stentthrombosis and TLR, it is possible that even if technicaladvances were to obviate the negative consequences ofcalcification itself, the outcomes of these patients may stillbe worse.
Advanced age, male sex, hypertension, and STEMI pre-sentation were independently associated with the presence ofcalcified target lesions in the current study. In prior studiesof patients with stable coronary artery disease, in addition toolder age, the extent of atherosclerosis and prior CABGwere identified as independent predictors of calcification(37,38). This discrepancy may in part be explained by thedifferent nature of the study populations (ACS vs. stablecoronary disease). In addition, patients with chronic kidneydisease (whether or not requiring dialysis) frequently haveextensive coronary calcification, in part due to secondaryhyperparathyroidism (39). This population was underrep-resented in our study population.

Généreux et al. JACC Vol. 63, No. 18, 2014Coronary Calcification and Percutaneous Coronary Intervention May 13, 2014:1845–54
1852
Whether lesion decalcification prior to stent implantationcan improve event-free survival of patients with calcifiedlesions is an area of ongoing investigation. Despite initialenthusiasm (40–44), the use of rotational atherectomy priorto paclitaxel-eluting stent implantation in severely calcifiedlesions did not improve 9-month clinical or angiographicoutcomes in the ROTAXUS (Rotational Atherectomy Priorto Taxus Stent Treatment for Complex Native CoronaryArtery Disease) randomized trial (45). Although rotationalatherectomy facilitated stent delivery and allowed a higherrate of immediate procedural success in this study, in-stent late loss at 9 months was greater after rotationalatherectomy compared with lesion preparation with con-ventional balloon angioplasty alone prior to stenting (0.44 �0.58 mm vs. 0.31 � 0.52 mm; p ¼ 0.04). These data areconsistent with the results from studies in the balloon an-gioplasty and BMS eras, which reported higher rates ofrestenosis with rotational atherectomy (40,43,46–53).Greater neointimal hyperplasia with rotational atherectomymay be due to thermal injury, platelet activation, and medialinjury (54,55). Moreover, use of rotational atherectomy inthe setting of NSTEACS and STEMI in which thrombus isalmost always present (even if angiographically unapparent)is considered an absolute contraindication. It is not thereforesurprising that only 48 patients (0.7%) underwent rotationalatherectomy in the present study. Ongoing and plannedstudies will determine whether the prognosis after PCI ofcalcified lesions can be improved by use of novel, less trau-matic devices for plaque debulking (56), perhaps coupledwith current-generation metallic DES or bioresorbablevascular scaffolds, both of which are more potent thanpaclitaxel-eluting stents at reducing restenosis.Study limitations. The fact that an experienced indepen-dent angiographic core laboratory analyzed all 6,855 an-giograms in the present report is a major strength, removingthe element of operator variability and bias inherent in allprior studies. The large sample size of the present analysisalso affords robust identification of predictors of target lesioncalcification and adverse events. Independent adjudicationof clinical events blinded to the angiographic findings isalso notable. However, as an observational post-hoc analysis,the present analysis can only identify correlations, notprove causality. Despite adjustment for measured covari-ates, residual confounding may be present. The results ofthe present study should therefore be considered hypothe-sis generating. Even though the degree of calcificationwas assessed by experienced angiographic core laboratorytechnicians, the severity of calcification is underestimatedby angiography compared with IVUS (57,58). The presentstudy was underpowered to determine whether PCI ofseverely calcified as compared with moderately calcifiedtarget lesions was an independent predictor of adverse out-comes, as suggested in unadjusted analyses. Moreover, byarbitrary convention, only heavy calcification contributesto the SYNTAX score (59), a definition equivalent to thatof severe calcification by QCA (18). The present report
suggests that in addition to heavy or severe calcification,moderate calcification, as assessed by an experienced an-giographic core laboratory, also has significant impact onischemic outcomes and therefore might be included in futurerisk models. Prospective validation of this concept isrequired. The studies pooled in the current report includedimplantation of approximately 20% of BMS and 80% first-generation DES. Given recent reports showing superioroutcomes with second-generation DES (60), our findingsmay have been different had more contemporary stents beenused. However, whether second-generation DES performbetter in severely calcified lesions has yet to be demonstrated.IVUS was not required in the present study, and whether itsuse would improve risk stratification or treatment outcomesin calcified ACS lesions is unknown. Finally, the currentreport was limited to a 1-year follow-up after stent im-plantation. Longer-term patient assessment is required todetermine if the adverse outcomes after PCI of calcifiedtarget lesions continue to accrue over time.
Conclusions
Target lesions in patients with NSTEACS and STEMI arefrequently moderately or severely calcified, and PCI of suchlesions was independently predictive of stent thrombosis andunplanned ischemia-driven TLR at 1 year, as compared withtreatment of lesions with absent or only mild calcification.Novel approaches are urgently needed to improve outcomesof high-risk patients with ACS with calcified lesionsundergoing PCI.
Reprint requests and correspondence: Dr. Gregg W. Stone,Columbia University Medical Center, Cardiovascular ResearchFoundation, 111 East. 59th Street, 11th Floor, New York, NewYork 10022. E-mail: [email protected].
REFERENCES
1. Moses JW, Leon MB, Popma JJ, et al. Sirolimus-eluting stents versusstandard stents in patients with stenosis in a native coronary artery.N Engl J Med 2003;349:1315–23.
2. Stone GW, Ellis SG, Cox DA, et al. A polymer-based, paclitaxel-eluting stent in patients with coronary artery disease. N Engl J Med2004;350:221–31.
3. Schofer J, Schluter M, Gershlick AH, et al. Sirolimus-eluting stents fortreatment of patients with long atherosclerotic lesions in small coronaryarteries: double-blind, randomised controlled trial (E-SIRIUS). Lancet2003;362:1093–9.
4. Schampaert E, Cohen EA, Schluter M, et al. The Canadian study ofthe sirolimus-eluting stent in the treatment of patients with long denovo lesions in small native coronary arteries (C-SIRIUS). J Am CollCardiol 2004;43:1110–5.
5. Takebayashi H, Kobayashi Y, Mintz GS, et al. Intravascular ultrasoundassessment of lesions with target vessel failure after sirolimus-elutingstent implantation. Am J Cardiol 2005;95:498–502.
6. Stefanini GG, Serruys PW, Silber S, et al. The impact of patient andlesion complexity on clinical and angiographic outcomes after revascu-larization with zotarolimus- and everolimus-eluting stents: a substudy ofthe RESOLUTE All Comers trial (a randomized comparison of azotarolimus-eluting stent with an everolimus-eluting stent for percuta-neous coronary intervention). J Am Coll Cardiol 2011;57:2221–32.
JACC Vol. 63, No. 18, 2014 Généreux et al.May 13, 2014:1845–54 Coronary Calcification and Percutaneous Coronary Intervention
1853
7. Kuriyama N, Kobayashi Y, Yamaguchi M, Shibata Y. Usefulness ofrotational atherectomy in preventing polymer damage of everolimus-eluting stent in calcified coronary artery. J Am Coll Cardiol Intv2011;4:588–9.
8. Hoffmann R, Mintz GS, Popma JJ, et al. Treatment of calcified cor-onary lesions with Palmaz-Schatz stents. An intravascular ultrasoundstudy. Eur Heart J 1998;19:1224–31.
9. Mosseri M, Satler LF, Pichard AD, Waksman R. Impact of vesselcalcification on outcomes after coronary stenting. Cardiovasc RevascMed 2005;6:147–53.
10. Moussa I, Ellis SG, Jones M, et al. Impact of coronary culprit lesioncalcium in patients undergoing paclitaxel-eluting stent implantation(a TAXUS-IV sub study). Am J Cardiol 2005;96:1242–7.
11. Seo A, Fujii T, Inoue T, et al. Initial and long-term outcomes ofsirolimus-eluting stents for calcified lesions compared with bare-metalstents. Int Heart J 2007;48:137–47.
12. Bangalore S, Vlachos HA, Selzer F, et al. Percutaneous coronaryintervention of moderate to severe calcified coronary lesions: insightsfrom the National Heart, Lung, and Blood Institute Dynamic Registry.Catheter Cardiovasc Interv 2011;77:22–8.
13. Stone GW, McLaurin BT, Cox DA, et al. Bivalirudin for patients withacute coronary syndromes. N Engl J Med 2006;355:2203–16.
14. Stone GW, Witzenbichler B, Guagliumi G, et al. Bivalirudin duringprimary PCI in acute myocardial infarction. N Engl J Med 2008;358:2218–30.
15. Stone GW, Bertrand M, Colombo A, et al. Acute Catheterization andUrgent Intervention Triage Strategy (ACUITY) trial: study design andrationale. Am Heart J 2004;148:764–75.
16. Mehran R, Brodie B, Cox DA, et al. The Harmonizing OutcomesWith Revascularization and Stents in Acute Myocardial Infarction(HORIZONS-AMI) trial: study design and rationale. Am Heart J2008;156:44–56.
17. Aoki J, Lansky AJ, Mehran R, et al. Early stent thrombosis in patientswith acute coronary syndromes treated with drug-eluting and baremetal stents: the Acute Catheterization and Urgent Intervention TriageStrategy trial. Circulation 2009;119:687–98.
18. Popma J, Bashore T. Qualitative and quantitative angiography. In:Topol E, editor. Textbook of Interventional Cardiology. Philadelphia,PA: WB Saunders; 1994:1052–68.
19. Stone GW, Maehara A, Lansky AJ, et al. A prospective natural-historystudy of coronary atherosclerosis. N Engl J Med 2011;364:226–35.
20. Morice MC, Serruys PW, Sousa JE, et al. A randomized comparison ofa sirolimus-eluting stent with a standard stent for coronary revascu-larization. N Engl J Med 2002;346:1773–80.
21. Dawkins KD, Grube E, Guagliumi G, et al. Clinical efficacy ofpolymer-based paclitaxel-eluting stents in the treatment of complex,long coronary artery lesions from a multicenter, randomized trial:support for the use of drug-eluting stents in contemporary clinicalpractice. Circulation 2005;112:3306–13.
22. Kandzari DE, Leon MB, Popma JJ, et al. Comparison of zotarolimus-eluting and sirolimus-eluting stents in patients with native coronaryartery disease: a randomized controlled trial. J Am Coll Cardiol 2006;48:2440–7.
23. Serruys PW, Ruygrok P, Neuzner J, et al. A randomised comparison ofan everolimus-eluting coronary stent with a paclitaxel-eluting coronarystent: the SPIRIT II trial. EuroIntervention 2006;2:286–94.
24. Stone GW, Midei M, Newman W, et al. Comparison of aneverolimus-eluting stent and a paclitaxel-eluting stent in patients withcoronary artery disease: a randomized trial. JAMA 2008;299:1903–13.
25. Leon MB, Nikolsky E, Cutlip DE, et al. Improved late clinical safetywith zotarolimus-eluting stents compared with paclitaxel-eluting stentsin patients with de novo coronary lesions: 3-year follow-up from theENDEAVOR IV (Randomized Comparison of Zotarolimus- andPaclitaxel-Eluting Stents in Patients With Coronary Artery Disease)trial. J Am Coll Cardiol Intv 2010;3:1043–50.
26. Grube E, Chevalier B, Smits P, et al. The SPIRIT V study: a clinicalevaluation of the XIENCE V everolimus-eluting coronary stent systemin the treatment of patients with de novo coronary artery lesions. J AmColl Cardiol Intv 2011;4:168–75.
27. Kedhi E, Joesoef KS, McFadden E, et al. Second-generationeverolimus-eluting and paclitaxel-eluting stents in real-life practice(COMPARE): a randomised trial. Lancet 2010;375:201–9.
28. Xu Y, Mintz GS, Tam A, et al. Prevalence, distribution, predictors,and outcomes of patients with calcified nodules in native coronary
arteries: a 3-vessel intravascular ultrasound analysis from ProvidingRegional Observations to Study Predictors of Events in the CoronaryTree (PROSPECT). Circulation 2012;126:537–45.
29. Fujii K, Carlier SG, Mintz GS, et al. Stent underexpansion andresidual reference segment stenosis are related to stent thrombosis aftersirolimus-eluting stent implantation: an intravascular ultrasound study.J Am Coll Cardiol 2005;45:995–8.
30. Liu X, Doi H, Maehara A, et al. A volumetric intravascular ultrasoundcomparison of early drug-eluting stent thrombosis versus restenosis.J Am Coll Cardiol Intv 2009;2:428–34.
31. Doi H, Maehara A, Mintz GS, et al. Impact of post-interventionminimal stent area on 9-month follow-up patency of paclitaxel-eluting stents: an integrated intravascular ultrasound analysis from theTAXUS IV, V, and VI and TAXUS ATLAS Workhorse, LongLesion, and Direct Stent Trials. J Am Coll Cardiol Intv 2009;2:1269–75.
32. Borissoff JI, Joosen IA, Versteylen MO, Spronk HM, Ten Cate H,Hofstra L. Accelerated in vivo thrombin formation independentlypredicts the presence and severity of CT angiographic coronaryatherosclerosis. J Am Coll Cardiol Img 2012;5:1201–10.
33. Chirumamilla AP, Maehara A, Mintz GS, et al. High platelet reactivityon clopidogrel therapy correlates with increased coronary atheroscle-rosis and calcification: a volumetric intravascular ultrasound study.J Am Coll Cardiol Img 2012;5:540–9.
34. Hofmann Bowman MA, McNally EM. Genetic pathways of vascularcalcification. Trends Cardiovasc Med 2012;22:93–8.
35. O’Donnell CJ, Kavousi M, Smith AV, et al. Genome-wide associationstudy for coronary artery calcification with follow-up in myocardialinfarction. Circulation 2011;124:2855–64.
36. Matetzky S, Shenkman B, Guetta V, et al. Clopidogrel resistance isassociated with increased risk of recurrent atherothrombotic events inpatients with acute myocardial infarction. Circulation 2004;109:3171–5.
37. Mintz GS, Douek P, Pichard AD, et al. Target lesion calcification incoronary artery disease: an intravascular ultrasound study. J Am CollCardiol 1992;20:1149–55.
38. Mintz GS, Pichard AD, Popma JJ, et al. Determinants and correlatesof target lesion calcium in coronary artery disease: a clinical, angio-graphic and intravascular ultrasound study. J Am Coll Cardiol 1997;29:268–74.
39. Block GA, Klassen PS, Lazarus JM, Ofsthun N, Lowrie EG,Chertow GM. Mineral metabolism, mortality, and morbidity inmaintenance hemodialysis. J Am Soc Nephrol 2004;15:2208–18.
40. Warth DC, Leon MB, O’Neill W, Zacca N, Polissar NL,Buchbinder M. Rotational atherectomy multicenter registry: acuteresults, complications and 6-month angiographic follow-up in 709patients. J Am Coll Cardiol 1994;24:641–8.
41. Moussa I, Di Mario C, Moses J, et al. Coronary stenting after rota-tional atherectomy in calcified and complex lesions. Angiographic andclinical follow-up results. Circulation 1997;96:128–36.
42. Hoffmann R, Mintz GS, Kent KM, et al. Comparative early and nine-month results of rotational atherectomy, stents, and the combination ofboth for calcified lesions in large coronary arteries. Am J Cardiol 1998;81:552–7.
43. Dill T, Dietz U, Hamm CW, et al. A randomized comparison ofballoon angioplasty versus rotational atherectomy in complex coronarylesions (COBRA study). Eur Heart J 2000;21:1759–66.
44. Abdel-Wahab M, Baev R, Dieker P, et al. Long-term clinical outcomeof rotational atherectomy followed by drug-eluting stent implantationin complex calcified coronary lesions. Catheter Cardiovasc Interv 2013;81:285–91.
45. Abdel-Wahab M, Richardt G, Joachim Buttner H, et al. High-speedrotational atherectomy before paclitaxel-eluting stent implantation incomplex calcified coronary lesions: the randomized ROTAXUS(Rotational Atherectomy Prior to Taxus Stent Treatment for ComplexNative Coronary Artery Disease) trial. J Am Coll Cardiol Intv 2013;6:10–9.
46. Mintz GS, Pichard AD, Popma JJ, Kent KM, Satler LF,Leon MB. Preliminary experience with adjunct directional coronaryatherectomy after high-speed rotational atherectomy in the treat-ment of calcific coronary artery disease. Am J Cardiol 1993;71:799–804.
47. Holmes DR Jr., Topol EJ, Adelman AG, Cohen EA, Califf RM.Randomized trials of directional coronary atherectomy: implications for

Généreux et al. JACC Vol. 63, No. 18, 2014Coronary Calcification and Percutaneous Coronary Intervention May 13, 2014:1845–54
1854
clinical practice and future investigation. J Am Coll Cardiol 1994;24:431–9.
48. MacIsaac AI, Bass TA, Buchbinder M, et al. High speed rotationalatherectomy: outcome in calcified and noncalcified coronary arterylesions. J Am Coll Cardiol 1995;26:731–6.
49. Reifart N, Vandormael M, Krajcar M, et al. Randomized comparisonof angioplasty of complex coronary lesions at a single center. ExcimerLaser, Rotational Atherectomy, and Balloon Angioplasty Comparison(ERBAC) study. Circulation 1997;96:91–8.
50. Safian RD, Feldman T, Muller DW, et al. Coronary Angioplasty andRotablator Atherectomy Trial (CARAT): immediate and late results ofa prospective multicenter randomized trial. Catheter Cardiovasc Interv2001;53:213–20.
51. Whitlow PL, Bass TA, Kipperman RM, et al. Results of the studyto determine rotablator and transluminal angioplasty strategy(STRATAS). Am J Cardiol 2001;87:699–705.
52. Mauri L, Reisman M, Buchbinder M, et al. Comparison of rotationalatherectomy with conventional balloon angioplasty in the prevention ofrestenosis of small coronary arteries: results of the Dilatation vs AblationRevascularization Trial Targeting Restenosis (DART). Am Heart J2003;145:847–54.
53. Bittl JA, Chew DP, Topol EJ, Kong DF, Califf RM. Meta-analysis ofrandomized trials of percutaneous transluminal coronary angioplastyversus atherectomy, cutting balloon atherotomy, or laser angioplasty.J Am Coll Cardiol 2004;43:936–42.
54. Reisman M, Shuman BJ, Harms V. Analysis of heat generation duringrotational atherectomy using different operational techniques. CathetCardiovasc Diagn 1998;44:453–5.
55. Reisman M, Shuman BJ, Dillard D, et al. Analysis of low-speedrotational atherectomy for the reduction of platelet aggregation.Cathet Cardiovasc Diagn 1998;45:208–14.
56. Parikh K, Chandra P, Choksi N, Khanna P, Chambers J. Safety andfeasibility of orbital atherectomy for the treatment of calcified coronarylesions: the ORBIT I trial. Catheter Cardiovasc Interv 2013;81:1134–9.
57. Mintz GS, Popma JJ, Pichard AD, et al. Patterns of calcification incoronary artery disease. A statistical analysis of intravascular ultrasoundand coronary angiography in 1155 lesions.Circulation1995;91:1959–65.
58. Tuzcu EM, Berkalp B, De Franco AC, et al. The dilemma of diag-nosing coronary calcification: angiography versus intravascular ultra-sound. J Am Coll Cardiol 1996;27:832–8.
59. Serruys PW, Morice MC, Kappetein AP, et al. Percutaneous coronaryintervention versus coronary-artery bypass grafting for severe coronaryartery disease. N Engl J Med 2009;360:961–72.
60. Bangalore S, Kumar S, Fusaro M, et al. Short- and long-term outcomeswith drug-eluting and bare-metal coronary stents: a mixed-treatmentcomparison analysis of 117 762 patient-years of follow-up from ran-domized trials. Circulation 2012;125:2873–91.
Key Words: coronary calcification - NSTEMI - PCI - STEMI.
APPENDIX
For supplemental tables and a figure, please see the online version of thisarticle.
Related Documents











