Archives of Cardiovascular Disease (2008) 101, 391—397 Disponible en ligne sur www.sciencedirect.com CLINICAL RESEARCH Is the aortic root dilated in obstructive sleep apnoea syndrome? Dilatation aortique et syndrome d’apnée du sommeil Catherine Meuleman a , Franck Boccara a , Xuan-Lan Nguyen b , Emanuele Di Angelantonio a , Stéphane Ederhy a , Sandra Janower a , Ghislaine Dufaitre a , Nabila Haddour a , Louise Boyer-Chatenet a , Dominique Rakotonanahary b , Bernard Fleury b , Ariel Cohen a,∗ a Department of Cardiology, Saint-Antoine University and Medical School, Université Pierre-et-Marie-Curie, 184, rue du Faubourg-Saint-Antoine, 75571 Paris cedex 12,France b Department of Respiratory Medicine, Saint-Antoine University and Medical School, université Pierre-et-Marie-Curie, Paris, France Received 8 April 2008; accepted 9 June 2008 Available online 28 August 2008 KEYWORDS Obstructive sleep apnoea syndrome; Aortic root dilatation; Pulse wave velocity Summary Background. — Obstructive sleep apnoea syndrome (OSAS) is associated with an increased risk of arterial hypertension (AH), coronary artery disease, atrial arrhythmias, heart failure, stroke and death. Whether OSAS influences aortic root size has not been fully investigated. The aim of our study was to investigate aortic root diameter and aortic stiffness in OSAS. Methods. — Using transthoracic Doppler echocardiography, we evaluated 76 patients with OSAS (mean age 52.7 ± 9.5 years, 70 men [92%]) with no overt cardiovascular disease. The follow- ing parameters were measured offline: aortic diameter at Valsalva sinuses, aortic regurgitation (AR) grade, left ventricular (LV) mass, LV ejection fraction (LVEF, Simpson rule), systolic pul- monary artery pressure (sPAP). Aortic stiffness (carotid-femoral pulse wave velocity, PWV) was measured non-invasively using SphygmoCor technology. Abbreviations: AH, arterial hypertension; AHI, apnoea-hypopnoea index; AR, aortic regurgitation; BMI, body mass index; CPAP, con- tinuous positive airway pressure; LV, left ventricle; LVEDD, left ventricular end-diastolic diameter; LVEF, left ventricular ejection fraction; OSAS, obstructive sleep apnoea syndrome; PWV, pulse wave velocity; sPAP, systolic pulmonary arterial pressure. ∗ Corresponding author. E-mail address: [email protected] (A. Cohen). 1875-2136/$ — see front matter © 2008 Published by Elsevier Masson SAS. doi:10.1016/j.acvd.2008.06.007

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Archives of Cardiovascular Disease (2008) 101, 391—397
Disponib le en l igne sur www.sc iencedi rec t .com
CLINICAL RESEARCH
Is the aortic root dilated in obstructive sleepapnoea syndrome?
Dilatation aortique et syndrome d’apnée du sommeil
Catherine Meulemana, Franck Boccaraa,Xuan-Lan Nguyenb, Emanuele Di Angelantonioa,Stéphane Ederhya, Sandra Janowera,Ghislaine Dufaitrea, Nabila Haddoura,Louise Boyer-Chateneta, DominiqueRakotonanaharyb, Bernard Fleuryb, Ariel Cohena,∗
a Department of Cardiology, Saint-Antoine University and Medical School, UniversitéPierre-et-Marie-Curie, 184, rue du Faubourg-Saint-Antoine, 75571 Paris cedex 12,Franceb Department of Respiratory Medicine, Saint-Antoine University and Medical School,université Pierre-et-Marie-Curie, Paris, France
Received 8 April 2008; accepted 9 June 2008Available online 28 August 2008
KEYWORDSObstructive sleepapnoea syndrome;Aortic rootdilatation;Pulse wave velocity
SummaryBackground. — Obstructive sleep apnoea syndrome (OSAS) is associated with an increased riskof arterial hypertension (AH), coronary artery disease, atrial arrhythmias, heart failure, strokeand death. Whether OSAS influences aortic root size has not been fully investigated. The aimof our study was to investigate aortic root diameter and aortic stiffness in OSAS.Methods. — Using transthoracic Doppler echocardiography, we evaluated 76 patients with OSAS(mean age 52.7 ± 9.5 years, 70 men [92%]) with no overt cardiovascular disease. The follow-
ing parameters were measured offline: aortic diameter at Valsalva sinuses, aortic regurgitation(AR) grade, left ventricular (LV) mass, LV ejection fraction (LVEF, Simpson rule), systolic pul-monary artery pressure (sPAP). Aortic stiffness (carotid-femoral pulse wave velocity, PWV) wasmeasured non-invasively using SphygmoCor technology.Abbreviations: AH, arterial hypertension; AHI, apnoea-hypopnoea index; AR, aortic regurgitation; BMI, body mass index; CPAP, con-tinuous positive airway pressure; LV, left ventricle; LVEDD, left ventricular end-diastolic diameter; LVEF, left ventricular ejection fraction;OSAS, obstructive sleep apnoea syndrome; PWV, pulse wave velocity; sPAP, systolic pulmonary arterial pressure.
∗ Corresponding author.E-mail address: [email protected] (A. Cohen).
1875-2136/$ — see front matter © 2008 Published by Elsevier Masson SAS.doi:10.1016/j.acvd.2008.06.007

392 C. Meuleman et al.
Results. — Mean duration of OSAS was four years and 84% of patients were being treated withcontinuous positive airway pressure. AH was documented in 39 (51%) patients. The mean aorticroot diameter was 35.3 ± 3.8 mm (26.9—44.6 mm) and the prevalence of aortic root dilatationwas 3.9% (3 of 76 patients). On univariate analysis, age and sex were significant predictors ofaortic root dilatation whereas arterial hypertension was not.Conclusions. — The prevalence of aortic root enlargement was not increased in OSAS. Only ageand sex and not arterial hypertension, were associated with aortic dilatation.© 2008 Published by Elsevier Masson SAS.
MOTS CLÉSSyndrome d’apnéeobstructive dusommeil ;Dilatation aortique ;Vitesse de l’onde depouls
RésuméBut de l’étude. — Le syndrome d’apnée obstructive du sommeil (SAOS) est associé à une aug-mentation du risque d’hypertension artérielle, de maladie coronaire, de fibrillation auriculaire,d’insuffisance cardiaque, d’accident vasculaire cérébral et de décès. Une éventuelle relationentre le syndrome d’apnées du sommeil et la dilatation aortique n’a jamais été étudiée. Lebut de cette étude était de mesurer les diamètres aortiques et la rigidité aortique chez despatients présentant un SAOS.Méthodes. — Une échocardiographie transthoracique a été réalisée chez 76 patients présen-tant un SAOS (âge moyen 52.7 ± 9.5 years, 70 hommes [92 %]) sans antécédent cardiovasculaireconnu. Les paramètres suivants ont été mesurés off-line : diamètre aortique au niveau dessinus de Valsalva, insuffisance aortique (IA), masse ventriculaire gauche, rapport h/R, fractiond’éjection ventriculaire gauche (par la méthode de Simpson) et les pressions artérielles pul-monaires. La rigidité aortique a été évaluée par la mesure de la vitesse de l’onde de poulscarotido-fémorale (VOP).Résultats. — La durée moyenne du SAOS était de quatre années et 84 % des patients étaienttraités par pression positive continue. Une hypertension artérielle (HTA) a été documentéechez 39 patients (51 %). Le diamètre aortique moyen était de 35.3 ± 3.8 mm (26.9—44.6 mm)et la prévalence de la dilatation aortique était de 3.9 % (3/76 patients). En analyse univariée,l’âge et le sexe étaient des facteurs prédictifs significatifs de dilatation aortique mais nonl’hypertension artérielle.Conclusion. — La prévalence de la dilatation aortique n’est pas augmentée dans le syndromed’apnées du sommeil. Seuls l’âge et le sexe et non l’hypertension artérielle étaient associés à
r Ma
I
Obiofctt[da[Othtph
M
S
WOlbfrtp
mt
la dilatation aortique.© 2008 Published by Elsevie
ntroduction
bstructive sleep apnoea syndrome (OSAS) is a disorderedreathing in which the upper airway closes repeatedly dur-ng sleep. These repetitive partial or complete cessationsf airflow during sleep result in oxygen desaturation, sleepragmentation and excessive daytime sleepiness. OSAS isommon and affects up to 4% of middle-aged men and upo 2% of women [1]. It is associated with vascular risk fac-ors and increased cardiovascular morbidity and mortality2]. Several studies have reported that OSAS is indepen-ently associated with arterial hypertension [3], coronaryrtery disease [4,5], heart failure [6,7], stroke and death8]. An association has also been demonstrated betweenSAS and aortic stiffness [9] and an increased risk of aor-
ic dissection [10]. Whether OSAS influences aortic root sizeas not yet been investigated. The aim of our study waso investigate aortic root diameter and aortic stiffness inatients with OSAS and to evaluate the influence of arterialypertension.D(1tb
sson SAS.
ethods
tudy population
e conducted an observational cohort study in patients withSAS who were referred consecutively for a cardiovascu-
ar evaluation by the Saint-Antoine sleep disorders centreetween March 2005 and March 2007. The study was per-ormed in patients included in our outpatient clinic, withegular examinations that did not require the patient’s writ-en consent. All information was, however, given to theatients.
Data on patient’s demographic characteristics, sleep andedical history, cardiovascular risk factors and medica-
ion use and habits were obtained during a consultation.
ata on risk factors included a history of hypertensiondefined as systolic blood pressure greater or equal to40 mmHg and/or diastolic blood pressure greater or equalo 90 mmHg and/or use of antihypertensive medication,eing measured with a standard sphygmomanometer on
me?
MtDort
P
Aimif1wardt[
P
ArFteeasaa
atactawg(tStswc
S
Dtt
Is the aortic root dilated in obstructive sleep apnoea syndro
three different occasions with the subject in the supineposition, or blood pressure greater than 125/80 mmHg dur-ing 24-hour ambulatory blood pressure monitoring [11]),diabetes mellitus, hyperlipidaemia, and current or formersmoking with an indication of the number of pack-years andcoronary heredity. Metabolic syndrome was defined accord-ing to the National Cholesterol Education Program—AdultTreatment Panel III (NCEP ATP-III) guidelines [12]. Thediagnosis required at least three of the following crite-ria: fasting glycaemia greater than 6.1 mmol/L (1.1 g/L),fasting triglycerides greater than 1.7 mmol/L (1.5 g/L),high-density lipoprotein cholesterol lesser than 1 mmol/L(men) or 1.3 mmol/L (women) (0.6 and 0.5 g/L), bloodpressure greater than 130/85 mmHg, and waist circumfer-ence greater than 102 cm (men) or greater than 88 cm(women). Data regarding medications included the daily useof beta-blockers, angiotensin converting-enzyme inhibitorsor angiotensin-receptor antagonists, diuretics, calcium-channel blockers, oral medications or insulin for thetreatment of diabetes, and lipid-lowering medications.Each patient’s height and weight were recorded to deter-mine their body mass index (BMI). Patients underwent aclinical examination, including biological samples (routinebiochemical investigation, fasting glucose, insulin, lipidsand high-sensitivity C-reactive protein), an electrocardio-gram, a chest X-ray, ambulatory blood pressure monitoring,Holter monitoring, and transthoracic echocardiography.Aortic stiffness (carotid-femoral pulse wave velocity[PWV]) was measured non-invasively using SphygmoCor®
technology.
Echocardiography
Transthoracic echocardiography was performed with a GEVingmed Vivid 7 dimension with a 2.5-MHz transduceraccording to the recommendations of the American Soci-ety of Echocardiography [13]. All echocardiograms werereviewed and were excluded from the analysis if they hadinadequate two-dimensional images for the assessment ofascending aorta dimensions. Aortic root diameter was mea-sured according to Roman et al.’s [14] recommendations atend-diastole, in the parasternal long-axis view at four levels:• the annulus;• the sinuses of Valsalva;• the supra-aortic ridge;• the proximal ascending aorta.
Aortic root dilatation was identified when aortic rootdiameter at the sinus of Valsalva was greater than two stan-dard deviations (SD) above the regression line with bodysurface area in a previously studied reference population[14]. Aortic regurgitation was semiquantified as mild, mod-erate, or severe, based on other flow mapping and usualindices [15].
Left ventricular end-diastolic diameter and end-systolicdiameter were measured by M-mode echocardiographyfrom two-dimensional echocardiography according to the
recommendations of the American Society of Echocar-diography [16]. The left ventricular mass index wascalculated according to Devereux et al. [17]. LVEF wasestimated visually. sPAP was calculated using the mod-ified Bernoulli equation on tricuspid regurgitation [18].galss
393
easurements were made in three cardiac cycles, andhe average was calculated for subsequent analyses. Alloppler and echocardiographic recordings were stored onptical disks and were analysed off-line by a single expe-ienced investigator blinded to the patient’s status andreatment.
WV measurement
ortic stiffness (carotid-femoral PWV) was measured non-nvasively using SphygmoCor® technology. All arterialeasurements were carried out during the consultation
n a central core laboratory. Measurements were per-ormed in a controlled environment at 22 ± 1 ◦C after5 minutes of rest. Transcutaneous Doppler flow recordingsere carried out simultaneously at the carotid and femoralrteries. PWV was calculated as the distance betweenecording sites measured over the surface of the bodyivided by the time travelled by the reflected wave. Theime delay was averaged over 10 to 15 cardiac cycles19].
olysomnography
ll participants underwent attended overnight polysomnog-aphy with the use of the Cidelec® system (Angers,rance). The recordings included a two-channel elec-roencephalogram, electromyogram, electrocardiogram,lectro-oculogram, body position, chest and abdominalxcursions, naso-oral airflow assessed by a nasal cannula,nd oxyhaemoglobin saturation (finger pulse oximetry). Aingle, attended polysomnographic study conducted duringn entire night was used to establish the presence of sleeppnoea [20].
Total cessation of airflow at the nose and mouth fort least 10 seconds was classified as apnoea (as obstruc-ive if respiratory effort was present and as centralpnoea if respiratory efforts were absent). Partial airwaylosure resulting in a diminution of airflow by greaterhan 30% for greater or equal to 10 seconds associ-ted with oxygen desaturation greater or equal to 4%as classified as hypopnoea [21]. Calculated polysomno-raphic variables included the apnoea-hypopnoea indexAHI) and the percentage of total sleep time during whichhe oxygen saturation was lesser than 90% (SaO2 < 90%).leep history data included a validated measure of day-ime sleepiness (Epworth sleepiness scale) [22]. Sleeptudies were performed in the sleep laboratory andere supervised throughout by an experienced techni-ian.
tatistical analysis
ata are expressed as means ± SD or medians with interquar-ile ranges. Pearson’s correlation analysis was used to assesshe possible relation between aortic dimensions and demo-
raphic or echocardiographic parameters, with significancet a critical level of five per cent or lower. A probability valueess than 0.05 was considered statistically significant. Alltatistical analysis was performed using STATA 9 statisticaloftware.
3 C. Meuleman et al.
R
T753optdpptdie
Table 2 Characteristics of obstructive sleep apnoeasyndrome.
Characteristics
Duration of OSAS, years 4 (1, 7)Apnoea-hypopnoea index 56.5 (33.6, 79.0)Time spent with oxygen
desaturation lesser than 90%12.2 (3.7, 28.0)
Epworth Sleepiness Scale score 10 (7, 16)Treatment of OSAS 66 (87)Treatment with CPAP, n (%) 64 (84)Duration of CPAP, years* 1.0 (0.3, 6.0)
94
esults
able 1 summarizes the baseline characteristics of the6 patients included in the study. The mean age was2.7 ± 9.6 years, 70 (92%) were men, and the mean BMI was1.5 ± 5.8 kg/m2. Thirty-nine (51%) patients had evidencef hypertension at baseline examination. Of these, 25 (64%)atients had a history of hypertension with a mean dura-ion of 6.4 ± 4.7 years and 14 (36%) were newly diagnoseduring the cardiovascular evaluation or by ambulatory bloodressure monitoring. A history of hypercholesterolaemia wasresent in 39 (51%) patients of whom 17 (44%) were being
reated with statins or fibrates. Thirteen (17%) patients hadiabetes mellitus, two of whom were being treated withnsulin and four with oral hypoglycaemic drugs, and the oth-rs with diet. Metabolic syndrome was present in 37 (49%)Table 1 Baseline characteristics of the study popula-tion (n = 76).
Baseline characteristics
Age, years 52.7 ± 9.6Male sex, n (%) 70 (92)Current smoker, n (%) 26 (34)Hypertension, n (%) 39 (51)
Newly-diagnosed hypertension, n (%) 14 (36)History of hypertension, n (%) 25 (64)Time from hypertension diagnosis,
years*6.4 (4.7)
Antihypertensive treatment, n (%)* 23 (92)Hypercholesterolaemia 39 (51)
Lipid-lowering treatment 17 (44)History of diabetes mellitus, n (%) 13 (17)
Diabetes mellitus treatment, n (%) 6 (46)Metabolic syndrome, n (%) 37 (49)Family history of coronary artery disease,
n (%)9 (12)
Physical measurementsBMI, kg/m2 31.5 ± 5.8Waist/hip ratio 1.00 ± 0.06Systolic blood pressure, mmHg 137 ± 16Diastolic blood pressure, mmHg 81 ± 8Pulse pressure, mmHg 56 ± 13Heart rate, bpm 71 ± 12Pulse wave velocity, m/s 9.8 ± 1.7
Blood measurementsFasting glucose, mmol/L 5.82 ± 2.30Fasting insulin, mU/L 11.81 ± 6.22HOMA-IR 3.19 ± 2.35Total cholesterol, g/L 1.97 ± 0.38Triglycerides, g/L 1.40 ± 0.71HDL-cholesterol, g/L 0.45 ± 0.12LDL-cholesterol, g/L 1.27 ± 0.33Creatinine, �mol/L 95.45 ± 12.28C-reactive protein, mg/L 5.15 ± 9.75
Values are mean ± SD unless otherwise specified.HDL, high-density lipoprotein; HOMA-IR, homeostasis modelassessment—insulin resistance; LDL, low-density lipoprotein.* Only available for patients with a history of hypertension.
Mandibular advancement device, n(%)
7 (9)
Duration of mandibularadvancement device, years
0.6 (0.2, 2.0)
Values are median (interquartile range) unless otherwise speci-fied.CPAP: continuous positive airway pressure; OSAS: obstructivesleep apnoea syndrome.
pvfiv
tTwm1
Na3tas
* Only available for patients treated with CPAP and mandibularadvancement device.
atients. None of these patients had a history of cardio-ascular disease (myocardial infarction, heart failure, atrialbrillation, stroke, or aortic disease). No patient had a pre-ious diagnosis of Marfan syndrome or related disease.
The median duration of OSAS was four years and 84% werereated with continuous positive airway pressure (CPAP).he median AHI was 56.5/h (minimum 11.8, maximum 188),ith a median time spent with SaO2 < 90% of 12.2%. Theedian Epworth Sleepiness Scale score was 10 (minimum
, maximum 16) (Table 2).Echocardiographic characteristics are shown in Table 3.
o patients had left ventricular dysfunction or pulmonaryrterial hypertension. The mean aortic root diameter was
5.3 ± 3.8 mm (26.9—44.6 mm). According to the defini-ion by Roman et al. [14], only three (3.9%) patients hadortic dilatation defined by aortic root diameter at theinus of Valsalva greater than two SD above the regres-Table 3 Two-dimensional echocardiographic character-istics (n = 76).
Echocardiographic parameters
Aortic root diameter at Valsalva sinus, mm 35.3 ± 3.8Aortic regurgitation (grade 1), n (%) 13 (17)LVEDD, mm 52.5 ± 5.0LVESD, mm 32.2 ± 4.9Septal thickness, mm 10.4 ± 1.5Posterior wall thickness, mm 9.1 ± 1.7Left ventricular mass, g 89.9 ± 19.0Fractional shortening, n (%) 38.7 ± 6.9sPAP, mmHg 30.4 ± 5.5
Values are mean ± SD unless otherwise specified.LVEDD, left ventricular end diastolic diameter; LVESD, leftventricular end systolic diameter; sPAP systolic pulmonaryartery pressure.
Is the aortic root dilated in obstructive sleep apnoea syndrome? 395
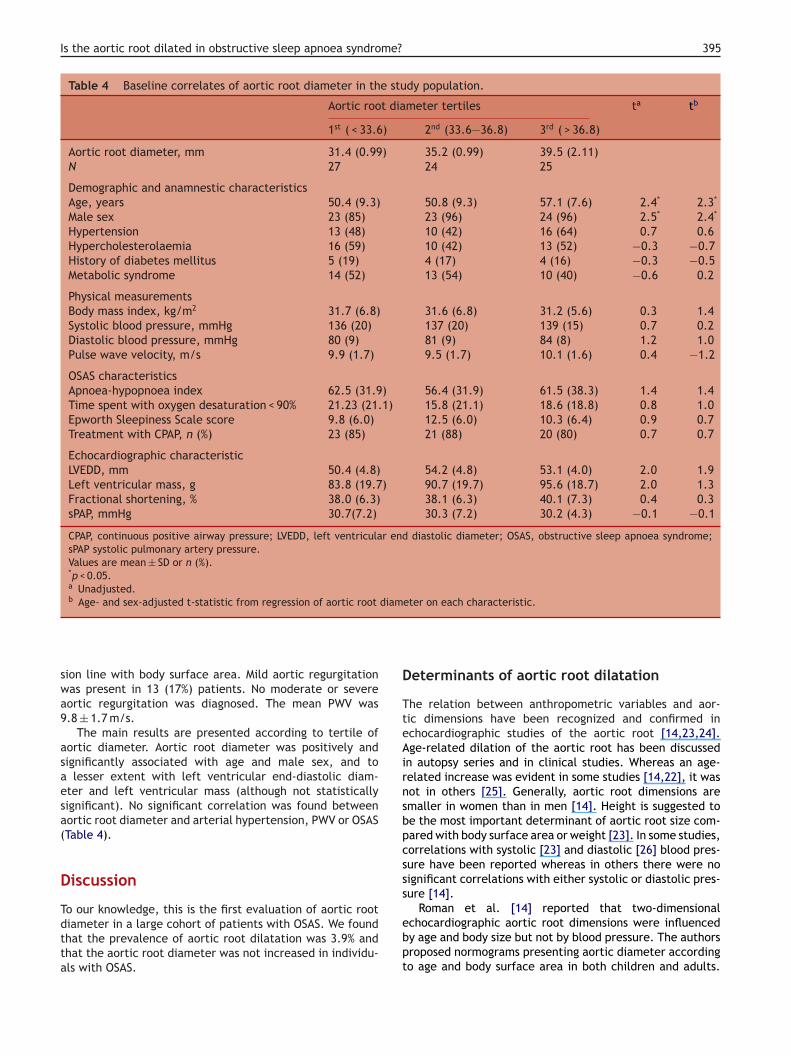
Table 4 Baseline correlates of aortic root diameter in the study population.
Aortic root diameter tertiles ta tb
1st ( < 33.6) 2nd (33.6—36.8) 3rd ( > 36.8)
Aortic root diameter, mm 31.4 (0.99) 35.2 (0.99) 39.5 (2.11)N 27 24 25
Demographic and anamnestic characteristicsAge, years 50.4 (9.3) 50.8 (9.3) 57.1 (7.6) 2.4* 2.3*
Male sex 23 (85) 23 (96) 24 (96) 2.5* 2.4*
Hypertension 13 (48) 10 (42) 16 (64) 0.7 0.6Hypercholesterolaemia 16 (59) 10 (42) 13 (52) −0.3 −0.7History of diabetes mellitus 5 (19) 4 (17) 4 (16) −0.3 −0.5Metabolic syndrome 14 (52) 13 (54) 10 (40) −0.6 0.2
Physical measurementsBody mass index, kg/m2 31.7 (6.8) 31.6 (6.8) 31.2 (5.6) 0.3 1.4Systolic blood pressure, mmHg 136 (20) 137 (20) 139 (15) 0.7 0.2Diastolic blood pressure, mmHg 80 (9) 81 (9) 84 (8) 1.2 1.0Pulse wave velocity, m/s 9.9 (1.7) 9.5 (1.7) 10.1 (1.6) 0.4 −1.2
OSAS characteristicsApnoea-hypopnoea index 62.5 (31.9) 56.4 (31.9) 61.5 (38.3) 1.4 1.4Time spent with oxygen desaturation < 90% 21.23 (21.1) 15.8 (21.1) 18.6 (18.8) 0.8 1.0Epworth Sleepiness Scale score 9.8 (6.0) 12.5 (6.0) 10.3 (6.4) 0.9 0.7Treatment with CPAP, n (%) 23 (85) 21 (88) 20 (80) 0.7 0.7
Echocardiographic characteristicLVEDD, mm 50.4 (4.8) 54.2 (4.8) 53.1 (4.0) 2.0 1.9Left ventricular mass, g 83.8 (19.7) 90.7 (19.7) 95.6 (18.7) 2.0 1.3Fractional shortening, % 38.0 (6.3) 38.1 (6.3) 40.1 (7.3) 0.4 0.3sPAP, mmHg 30.7(7.2) 30.3 (7.2) 30.2 (4.3) −0.1 −0.1
CPAP, continuous positive airway pressure; LVEDD, left ventricular end diastolic diameter; OSAS, obstructive sleep apnoea syndrome;sPAP systolic pulmonary artery pressure.Values are mean ± SD or n (%).*p < 0.05.a Unadjusted.b Age- and sex-adjusted t-statistic from regression of aortic root diameter on each characteristic.
D
TteAirnsbpcsss
sion line with body surface area. Mild aortic regurgitationwas present in 13 (17%) patients. No moderate or severeaortic regurgitation was diagnosed. The mean PWV was9.8 ± 1.7 m/s.
The main results are presented according to tertile ofaortic diameter. Aortic root diameter was positively andsignificantly associated with age and male sex, and toa lesser extent with left ventricular end-diastolic diam-eter and left ventricular mass (although not statisticallysignificant). No significant correlation was found betweenaortic root diameter and arterial hypertension, PWV or OSAS(Table 4).
Discussion
To our knowledge, this is the first evaluation of aortic rootdiameter in a large cohort of patients with OSAS. We foundthat the prevalence of aortic root dilatation was 3.9% andthat the aortic root diameter was not increased in individu-als with OSAS.
ebpt
eterminants of aortic root dilatation
he relation between anthropometric variables and aor-ic dimensions have been recognized and confirmed inchocardiographic studies of the aortic root [14,23,24].ge-related dilation of the aortic root has been discussed
n autopsy series and in clinical studies. Whereas an age-elated increase was evident in some studies [14,22], it wasot in others [25]. Generally, aortic root dimensions aremaller in women than in men [14]. Height is suggested toe the most important determinant of aortic root size com-ared with body surface area or weight [23]. In some studies,orrelations with systolic [23] and diastolic [26] blood pres-ure have been reported whereas in others there were noignificant correlations with either systolic or diastolic pres-ure [14].
Roman et al. [14] reported that two-dimensionalchocardiographic aortic root dimensions were influencedy age and body size but not by blood pressure. The authorsroposed normograms presenting aortic diameter accordingo age and body surface area in both children and adults.

3
Vwt2ss
A
Ihspptacnittaqv[[
P
PeneatpnbaocP
L
T(rurao
C
Tipw
C
N
R
[
[
[
[
[
[
[
96
asan et al. [24] showed that age, height, weight, and sexere the principal determinants of aortic root dimensions in
he Framingham Heart study, which included 1849 men and152 women. Our study confirmed a relation between age,ex, and aortic dilatation but showed that arterial hyperten-ion was not a predictor of aortic root dilatation.
ortic disease in patients with OSAS
n one study, patients with aortic dissection presented aigh prevalence of previously undiagnosed and frequentlyevere OSAS [10]. A higher mean AHI was found in theseatients compared with a control group of hypertensiveatients. Arterial hypertension, marked increase in sympa-hetic activity, and increased transmural pressure of theorta wall during apnoeas are suggested mechanisms thatould explain aortic dissection in OSAS [10]. These mecha-isms have been previously described in Marfan’s syndrome,n which a high prevalence of OSAS was detected [27]. OSASreatment with nasal CPAP was associated with attenua-ion of aortic root dilatation [28,29]. This treatment haslso been shown to alleviate daytime sleepiness, improveuality of life, decrease the occurrence of new cardio-ascular events in patients with coronary artery disease30], and may reduce cardiovascular morbidity and mortality31—33].
WV and OSAS
WV is an indicator of arterial stiffness [34,35]. Nagahamat al. [36] have shown that brachial-ankle PWV was sig-ificantly higher in patients with OSAS than in controlsven when the degree of risk factors was equal or in thebsence of risk factors. Tanriverdi et al. [37] reported thathe elastic properties of the aorta were deteriorated inatients with OSAS, characterized by increased aortic stiff-ess and lower distensibility. Increased aortic stiffness mighte responsible for the alteration of left ventricular systolicnd diastolic function reported in OSAS syndrome [36]. Inur study, mean PWV was 9.8 ± 1.7 m/s, and no significantorrelation was found between aortic root diameter andWV.
imitations
he main limitation of this study was the absence of controlsBMI and age-matched control patients). Moreover, its ret-ospective design and the absence of follow-up do not allows to draw definite conclusions. To extend these preliminaryesults, it is necessary to undertake a case-control studynd a longitudinal follow-up to evaluate the determinantsf cardiovascular events.
onclusion
hese results suggest that aortic root enlargement is notncreased in individuals with OSAS. Aortic root dilatation inatients with OSAS was associated with age and sex, but notith arterial hypertension.
[
C. Meuleman et al.
onflicts of interest
one.
eferences
[1] Young T, Palta M, Dempsey J, et al. The occurrence of sleep-disordered breathing among middle-aged adults. N Engl J Med1993;328:1230—5.
[2] Young T, Peppard PE, Gottlieb DJ. Epidemiology of obstructivesleep apnea: a population health perspective. Am J Respir CritCare Med 2002;165:1217—39.
[3] Peppard PE, Young T, Palta M, Skatrud J. Prospective study ofthe association between sleep-disordered breathing and hyper-tension. N Engl J Med 2000;342:1378—84.
[4] Mooe T, Rabben T, Wiklund U, et al. Sleep-disordered breathingin men with coronary artery disease. Chest 1996;109:659—63.
[5] Schafer H, Koehler U, Ewig S, et al. Obstructive sleepapnea as a risk marker in coronary heart disease. Cardiology1999;92:79—84.
[6] Cormican LJ, Williams A. Sleep disordered breathingand its treatment in congestive in heart failure. Heart2005;91:1265—70.
[7] Laaban JP, Pascal-Sebaoun S, Bolch E, et al. Left ventriculardysfunction in patients with obstructive sleep apnea. Chest2002;122:1133—8.
[8] Yaggi Klar, Concato J, Kernan W, et al. Obstructive sleepapnea as a risk factor for stroke and death. N Engl J Med2005;353:2034—41.
[9] Phillips C, Hedner J, Berend N, et al. Diurnal and obstructivesleep apnea influences on arterial stiffness and central bloodpressure in men. Sleep 2005;28:604—9.
10] Sampol G, Romero O, Salas A, et al. Obstructive sleep apneaand thoracic aortic dissection. Am J Resp Crit Care Med2003;168:1528—31.
11] Mansia G, De Backer G, Dominiczak A et al.; European Societyof Hypertension; European Society of Cardiology 2007 ESH-ESCGuidelines for the management of arterial hypertension: thetask force for the management of arterial hypertension of theEuropean Society of Hypertension (ESH) and of the EuropeanSociety of Cardiology (ESC). Blood Press. 2007; 16(3):135-232.
12] Hanley AJ, Wagenknecht LE, D’Agostino Jr RB, Zinman B,Haffner SM. Identification of subjects with insulin resistanceand beta-cell dysfunction using alternative definitions of themetabolic syndrome. Diabetes 2003;52:2740—7.
13] Sahn DJ, De Maria A, Kisslo J, et al. The committee onM-mode standardization of the American society of echocardio-graphy; recommendations regarding quantification in M-modeechocardiography: results of a survey of echocardiographicsmeasurements. Circulation 1978;58:1072—81.
14] Roman MJ, Devereux RB, Kramer-Fox R, et al. Two-dimensionalechocardiographic aortic root dimensions in normal childrenand adults. Am J Cardiol 1989;64:507—12.
15] Zoghbi WA, Enriquez-Sarano M, Foster E, et al. Recommen-dations for evaluation of the severity of native valvularregurgitation with two-dimensional and Doppler echocardio-graphy. J Am Soc Echocardiogr 2003;16:777—802.
16] Schiller NB, Shah PM, crawford M, et al. Recommendationsfor quantification of the left ventricle by two-dimensionalechocardiography: American Society of Echocardiography bycommittee on standards, Subcommittee on quantification of
two-dimensional Echoacrdiograms. J Am Soc Echocardiogr1989;2:358—67.17] Devereux RB, Alonso DR, Lutas EM, et al. Echocardiographicassessment of left ventricular hypertrophy: comparison tonecropsy findings. Am J Cardiol 1986;57:450—8.
me?
[
[
[
[
[
[
[
[
Is the aortic root dilated in obstructive sleep apnoea syndro
[18] Berger M, Haimowitz A, Van Tosh A, et al. Quantitative assess-ment of pulmonary hypertension in patients with tricuspidregurgitation using continuous wave doppler ultrasound. J AmColl Cardiol 1985;6:359—65.
[19] Laurent S, Boutourye P, Asmar E, et al. Aortic stiffness is anindependent predictor of all-cause and cardiovascular mortal-ity in hypertensive patients. Hypertension 2001;37:1236—41.
[20] Sleep-related breathing disorders in adults: recommandationsfor syndrome definition and measurement techniques in clin-ical research:th ereport of an American Academy of sleepMedicine Task Force. Sleep 1999; 22:667-89.
[21] Meoli AL, Casey KR, Clark RW, et al. Hypopnea in sleep-disordered breathing in adults. Sleep 2001;24:469—70.
[22] Johns MW. Daytime sleepiness, snoring and obstructive sleepapnea: the Epworth Sleepiness Scale. Chest 1993;103:30—6.
[23] Reed CM, Richey PA, Pulliam DA, Somes GW. Aortic dimensionsin tall men and women. Am J Cardiol 1993;71:608—10.
[24] Vasan RS, Larson MG, Levy D. Determinants of echocar-diographic aortic root size. The Framingham Heart Study.Circulation 1995;91:734—40.
[25] Valdez RS, Motta JA, London E, et al. Evaluation of theechocardiogram as an epidemiologic tool in an asymptomaticpopulation. Circulation 1979;60:921—9.
[26] Tell GS, Rutan GH, Kronmal RA, et al. Correlates of bloodpressure in community-dwelling older adults. Hypertension1994;23:59—67.
[27] Cistulli PA, Sullivan CE. Sleep-disordered breathing in Marfan’ssyndrome. Am Rev Respir Dis 1993;147:645—8.
[28] Cistulli P, Wilcox I, Jeremy R, et al. Aortic root dilatation in Mar-fan’s syndrome. A contribution from obstructive sleep apnea?Chest 1997;111:1763—6.
[
397
29] Verbraecken J, Paelinck B, Willemen M, et al. Aorticroot diameter and nasal intermittent positive airway pres-sure treatment in Marfan’s syndrome. Clin Genet 2003;63:131.
30] Milleron O, Pilliere R, Foucher A, et al. Benefits of obstruc-tive sleep apneoa treatment in coronary artery disease: a long—term follow-up study. Eur Heart J 2004;25:728—34.
31] Partinen M, Jamieson A, Guilleminault C. Long-term outcomefor obstructive sleep apnea syndrome patients. Mortality. Chest1988;94:1200—4.
32] Marin JM, Carrizo SJ, Vicente E, et al. Long-term cardio-vascular outcomes in men with obstructive sleep apnea-hypopnea syndrome with or without treatment with continuouspositive airway presure: an observationnal study. Lancet2005;365:1046—53.
33] Doherty LS, Kiely JL, Swan V, et al. Long-term effects ofnasal continuous positive airway pressure therapy on cardio-vascular outcomes in sleep apnea syndrome. Chest 2005;127:2076—84.
34] Lehmann ED. Clinical value of aortic pulse wave velocity mea-surement. Lancet 1999;164:528—9.
35] Asmar R, Benetos A, Topouchian J, et al. Assessment of arterialdistensibility by automatic pulse wave velocity measurement:validation and clinical applications studies. Hypertension1995;26:485—90.
36] Nagahama H, Soejima M, Uenomachi H, et al. Pulse wave veloc-
ity as an indicator of atherosclerosis in obstructive sleep apneasyndrome. Intern Med 2004;43:184—8.37] Tanriverdi H, Evrengul H, Kaftan A, et al. Effect of obstructivesleep apnea on aortic elastic parameters — relationship to leftventricular mass and function. Circ J 2006;70:737—43.
Related Documents











