Gut, 1984, 25, 839-845 Is raised breath hydrogen related to the pathogenesis of pneumatosis coli? N W READ. M N AL-JANABI, AND P A CANN From tile Clinical Research Unit, Royal Hallamshire Hospital, Sheffield, and Department of Physiology, Universitv of Sheffield, Sheffield SUMMARY Clinical and physiological studies were carried out in five patients with pneumatosis coli in order to investigate the origin of the high fasting breath hydrogen concentration in this condition and to determine its possible significance in the pathogenesis of the disease. All five patients excreted abnormally high fasting concentrations of hydrogen in their breath (69±9 ppm, mean ± SEM). Moreover, analysis of the contents of the gas filled cysts revealed between 2% and 8% of hydrogen gas. Colonic washout significantly reduced breath hydrogen cohcentrations to 9±6 ppm, but did not abolish the cysts. Conversely, deflation of the cysts was achieved with oxygen or antibiotics, though this only reduced breath hydrogen concentrations to about 66% of their original value. After feeding a radiolabelled meal, breath hydrogen concentrations rose before the meal appeared to reach the colon, suggesting overgrowth of anaerobic bacteria in the small intestine. Despite this, 14C glycocholate breath tests were within normal limits. An alternative possibility is that the high levels of hydrogen excreted in the breath may be produced in the intestinal lumen possibly from the fermentation of copious amounts of colonic mucus. Finally, measurement of whole gut transit time and stool weight suggested that patients were constipated despite passing mucus and blood. The relevance of our observations to the pathogenesis of submucosal cysts is unclear, but the data favour the hypothesis that these are produced by invasion of the colonic submucosa with anaerobic bacteria. Pneumatosis coli is an uncommon condition of unknown aetiology. characterised by the presence of multiple gas filled cysts within the wall of the colon. A recent report of raised breath hydrogen concen- trations in these patients suggested that increased bacterial fermentation of carbohydrate may be implicated in the pathogenesis of the condition. 1 We have carried out a series of studies to investigate the origin of the raised fasting breath hydrogen concen- trations in five patients with pneumatosis coli in an attempt to shed some light on the pathogenesis of the condition. Methods PATIENTS These were three female and two male patients aged between 45 and 60 years who all had submucosal gas filled cysts of the large bowel (Fig. 1). but had no Address for correspondence: Dr N W Read. Clinical Research Unit. H Floor. Roval Hallamshire Hospital. Glossop Road. Sheffield S10 2JF. Received for publication: 1() October 1983 evidence of small bowel cysts. For comparison, results were compared with those from 23 normal healthy volunteers (11 men and 12 women, aged 21-70 years), who had no bowel complaints, and 29 patients with the irritable bowel syndrome (10 men and 19 women, aged 19-69 years). Case reports CASE NO 1 (AS) This 69 year old women presented with a two month history of increasing flatulence, associated with passage of blood and mucus per rectum and abdominal pain which was intermittent in nature, and relieved by defaecation. She admitted to constipation and had lost 15 87 kg in six months. She had suffered with progressive angina for several years and had been treated with oxprenolol (120 mg tds). She had undergone a cholecystectomy for gall stones eight years previously. There was no history of chronic obstructive airways disease. Rectal biopsy revealed melanosis coli. 839 on 9 September 2018 by guest. Protected by copyright. http://gut.bmj.com/ Gut: first published as 10.1136/gut.25.8.839 on 1 August 1984. Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Gut, 1984, 25, 839-845
Is raised breath hydrogen related to the pathogenesis ofpneumatosis coli?N W READ. M N AL-JANABI, AND P A CANN
From tile Clinical Research Unit, Royal Hallamshire Hospital, Sheffield, and Department of Physiology,Universitv of Sheffield, Sheffield
SUMMARY Clinical and physiological studies were carried out in five patients with pneumatosiscoli in order to investigate the origin of the high fasting breath hydrogen concentration in thiscondition and to determine its possible significance in the pathogenesis of the disease. All fivepatients excreted abnormally high fasting concentrations of hydrogen in their breath(69±9 ppm, mean ± SEM). Moreover, analysis of the contents of the gas filled cysts revealedbetween 2% and 8% of hydrogen gas. Colonic washout significantly reduced breath hydrogencohcentrations to 9±6 ppm, but did not abolish the cysts. Conversely, deflation of the cysts was
achieved with oxygen or antibiotics, though this only reduced breath hydrogen concentrations toabout 66% of their original value. After feeding a radiolabelled meal, breath hydrogenconcentrations rose before the meal appeared to reach the colon, suggesting overgrowth ofanaerobic bacteria in the small intestine. Despite this, 14C glycocholate breath tests were withinnormal limits. An alternative possibility is that the high levels of hydrogen excreted in the breathmay be produced in the intestinal lumen possibly from the fermentation of copious amounts ofcolonic mucus. Finally, measurement of whole gut transit time and stool weight suggested thatpatients were constipated despite passing mucus and blood. The relevance of our observations tothe pathogenesis of submucosal cysts is unclear, but the data favour the hypothesis that these are
produced by invasion of the colonic submucosa with anaerobic bacteria.
Pneumatosis coli is an uncommon condition ofunknown aetiology. characterised by the presence ofmultiple gas filled cysts within the wall of the colon.A recent report of raised breath hydrogen concen-trations in these patients suggested that increasedbacterial fermentation of carbohydrate may beimplicated in the pathogenesis of the condition.1 Wehave carried out a series of studies to investigate theorigin of the raised fasting breath hydrogen concen-trations in five patients with pneumatosis coli in anattempt to shed some light on the pathogenesis ofthe condition.
Methods
PATIENTSThese were three female and two male patients agedbetween 45 and 60 years who all had submucosal gasfilled cysts of the large bowel (Fig. 1). but had noAddress for correspondence: Dr N W Read. Clinical Research Unit. H Floor.Roval Hallamshire Hospital. Glossop Road. Sheffield S10 2JF.Received for publication: 1() October 1983
evidence of small bowel cysts. For comparison,results were compared with those from 23 normalhealthy volunteers (11 men and 12 women, aged21-70 years), who had no bowel complaints, and 29patients with the irritable bowel syndrome (10 menand 19 women, aged 19-69 years).
Case reports
CASE NO 1 (AS)This 69 year old women presented with a two monthhistory of increasing flatulence, associated withpassage of blood and mucus per rectum andabdominal pain which was intermittent in nature,and relieved by defaecation. She admitted toconstipation and had lost 15 87 kg in six months. Shehad suffered with progressive angina for severalyears and had been treated with oxprenolol (120 mgtds). She had undergone a cholecystectomy for gallstones eight years previously. There was no historyof chronic obstructive airways disease. Rectal biopsyrevealed melanosis coli.
839
on 9 Septem
ber 2018 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.25.8.839 on 1 August 1984. D
ownloaded from

Read, Al-Janabi, and Cann
Fig. Double contrast barium enema showing presence ofgasfilled cysts in a tortuiouis loop ofsigmoid coloni.
CASE NO 2 (JR)This 65 year old retired steelworker presented withsymptoms of lower abdominal pain and the passageof blood and mucus per rectum, which began shortlyafter a transurethral prostatectomy for benignprostatic hyperplasia in 1978. He admitted toconstipation and was taking oxprenolol (160 mgdaily), digoxin (0 25 mg daily), and glyceryltrinitrate tablets for increasing angina of effort andhypertension which he had had for five years. He didnot suffer from chronic obstructive airways disease.
CASE NO 3 (AF)This 59 year old woman had suffered with pro-gressive disseminated sclerosis for three years,which had resulted in a spastic paralysis of both legsand ataxia of the upper limbs. Six months beforeadmission she developed diarrhoea which waswatery in consistency and contained no blood ormucus. Bowels were open between four and sixtimes per day, but she did not complain ofabdominal pain or the passage of gas per rectum.She gave no history of constipation and deniedtaking laxatives, though rectal biopsies showedevidence of melanosis coli. She gave no previoushistory of obstructive airways disease.
CASE No 4 (cw)This 61 year old man presented in 1978 with a threeweek history of passing red blood and mucus perrectum, accompanied by urgency, tenesmus, andpassage of copious flatus. There was little abdominalpain and no previous history of constipation. He wastaking atenolol (100 mg daily) and hydralazine (100mg bd) for hypertension, and had sustained amyocardial infarction in 1974. His past medicalhistory included polycythaemia, gout, agitateddepression, primary hyperparathyroidism, and abladder tumour. There was no history of chronicobstructive airways disease.
CASE NO 5 (BC)This 45 year old woman presented with a two yearhistory of watery diarrhoea associated with mucusand occasional red blood. The condition had pro-gressively worsened until she was passing motionsup to 15 times per day, associated with a copiousflatus, but no abdominal pain. There was no historyof constipation. She had been treated for one yearwith amitryptilene (25 mg bd) and carbamezepine(200 mg tds) for frontal headaches associated withvomiting. There was no previous history of ob-structive airways disease or ischaemic heart disease.
840)
on 9 Septem
ber 2018 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.25.8.839 on 1 August 1984. D
ownloaded from

Is raised breath hydrogen related to the pathogenesis of pneumizatosis coli?
INVESTIGATIVE PROTOCOL
All patients underwent extensive clinical investi-gations as outpatients. The following tests were
carried out in all patients: full blood count; bloodurea and electrolytes; liver function tests; Serum B12and folate; 14C glycocholate breath test,2 bariummeal and follow through, barium enema, plainabdominal radiograph, and sigmoidoscopy. Inaddition, jejunal biopsy and colonoscopy were
carried out in three patients.Patients were admitted to our gastrointestinal
ward for at least a week so that the special testscould be carried out in the following order: fastingbreath hydrogen analysis, measurement of gastro-intestinal transit times (three days), further fastingbreath hydrogen analysis (24 hour fast), colonicirrigation, analysis of contents of submucosal cysts,response to treatment. Patient 5 was unwilling todelay treatment and only underwent fasting breathhydrogen analysis and colonic irrigation beforetreatment.
BREATH HYI)ROGEN CONCENTRATIONSSamples of end expiratory air (50 ml) were collectedafter fasts of at least 14 hours, and 24 hours (fourpatients), after colonic irrigation using mannitol bymouth and rectal enemas, and after therapy withoxygen and antibiotics. Samples were taken in
triplicate and the concentration of hydrogen in thesesamples was determined by means of a detectorwhich incorporated a metallised membrane gas
sensitive electrode (GMI, Renfrew; Hansatech,Kings Lynn). 4
MEASUREMENT OF INTESTINAI TRANSIT TIMES
The time taken for food to pass through the samllintestine and colon was investigated by feeding a
standard meal, containing mashed potato, bakedbeans, sausages, and a dessert consisting ofhomogenised pineapple in custard. The mashedpotato was labelled with 500 ACie 99mTechnetiumsulphur colloid and 50 radio-opaque plasticmarkers]. Small bowel transit time of the radio-labelled test meal and the rate of colonic filling wasestimated by breath hydrogen analysis4 and by a
system incorporating a gamma camera anddedicated minicomputer." Previous studies carriedout in patients with terminal ileostomies had shownthat radioactive technetium99 incorporated inmashed potato provides an accurate marker for thedelivery of both liquid and solid residues from a
similar solid test meal through the terminal ileum.7Whole gut transit time was determined by asking
patients to collect the contents of each individualbowel movement in plastic bags for three days afteringestion of the standard meal. These were
inspected, weighed, and radiographed to determinethe number of radio-opaque plastic markers passedwithin 72 hours of ingestion of the meal.5 x
ANAL YSIS OF CONTENTS OF SUBMUCOSAL CYSTS
This was carried out in three patients who had cystsin the high rectum or low sigmoid colon. Aftercolonic washout, the rectum and sigmoid colon wereexamined with the flexible sigmoidoscope. Thesurface of a cyst was washed by irrigation with a finecatheter inserted through the biopsy channel andthen punctured with the end of a 21 gauge needleattached to another catheter and inserted throughthe biopsy channel of the instrument. The gas in thecyst was aspirated using a 5 ml syringe. The contentsof several cysts were sampled in this way. Theconcentration of hydrogen in these samples wasestimated by the detector after suitable dilutions.
TREATMENT PROTOCOLSAll patients were eventually treated with 100%oxygen,9 "' delivered via a face mask for periods ofbetween four and seven days. On this regime thePaO2 varied from 23-7 to 35 2 kPa (normal=13 2kPa).
In two patients, treatment of the condition wasinitially attempted with courses of antibiotics (eithermetronidazole 200 mg tds, or oxytetracycline 250 mgqds, or trimethoprimsulfamethoxazole 2 tabs bd, orerythromycin 250 mg qds for a total period of threemonths).
STATISTICAL METHODSThe statistical significance of differences betweenthe data was analysed using Student's paired orunpaired t test, whichever was appropriate.
Results
CLINICAL INVESTIGATIONSRadiological and endoscopic investigation revealedevidence of gas filled submucosal cysts in the colonof all five subjects (Fig. 1). The extent of the diseasevaried from the whole colon (cases 3 and 4) to thedescending colon, sigmoid colon, and rectum (cases1, 2, and 5). In each case the presence of cysts wasassociated with large amounts of faecal residue inthe proximal colon.
In contrast, radiological examination did notreveal gas filled cysts in the small intestine, nor didthey show any evidence of any other small intestinaldisease. None of the biochemical or haematologicaltests indicated any evidence of malabsorption.Moreover, the results of the '4glycocholate breathtests were within normal limits and did not suggestbacterial overgrowth of the small intestine.
841
on 9 Septem
ber 2018 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.25.8.839 on 1 August 1984. D
ownloaded from

Read, Al-Janabi, and Cann
BREATH HYDROGEN ANALYSISAll patients excreted high concentrations ofhydrogen in their breath after fasting overnight andafter fasting for 24 hours (Table 1). These weresignificantly higher than those observed in normalsubjects or in patients presenting with idiopathicconstipation or diarrhoea. After colonic wash outwith enemas and mannitol by mouth for three days,breath hydrogen concentrations fell to less than 10ppm in all except one subject (p<0.01), even thoughthis treatment did not cause any apparent reductionin the number and size of the cysts. Treatment oftwo patients with metronidazole for two weekscaused a small reduction in breath hydrogen concen-tration to values that were still abnormally high andcaused temporary disappearance of the cysts in onepatient. Oxygen treatment abolished the cysts (Fig.2) and the patients' symptoms, but even after thistreatment, breath hydrogen concentrations wereonly reduced from an average of 69 to 42 ppm.
SMALL BOWEL TRANSIT TIMEBreath hydrogen concentrations increased within100 minutes of ingesting a solid meal in all patientstested (Table 2). In contrast, analysis of the gamma
Table I Breath hydrogen concentrations (ppm) in fivepatients with pneumatosis coli compared with valuesobtained in normal subjects ofpatients with diarrhoea orconstipation
Aftermetronid-
Fasting After azolecolonic for After 02
14 h 24 h washout 2 weeks therapyPatients
1 60 52 3 52 332 64 60 5 40 253 52 56 2 - 384 64 50 32 - 155 102 - 5 - 101
Mean + SEM 69±9 55±2 9±6t 46 42±15*Normal
subjects(n =23) 11±2+ - -
Diarrhoea(n= 15) 10+2t -
Constipation(n= 14) 14±5 - -
Results from different groups are expressed as mean ± SEM.Degree of significance of the difference between the valueindicated and 14 h fasting hydrogen levels from patients withpneumatosis coli: *p<0-05, tp<0 01, tp<0-001.
Fig. 2 Plain radiograph of the abdomen in patient with pneumatosis coli before (left) and after (right) treatment withoxygen. Fasting breath hydrogen concentrations, measured at timefilm was taken, are inserted underneath each film.
842
on 9 Septem
ber 2018 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.25.8.839 on 1 August 1984. D
ownloaded from
Is raised breath hydrogen related to the pathogenesis of pneumatosis coli?
Table 2 Measurements ofstool weight, rise in breathhydrogen concentration, and transit time offood through thesmall and large intestine in Jour patients with pneumatosiscoli and the average results from 23 normal subjects
Rise inbreatih H. On.set Dail! Percentageconcen- caecal stool of markerstration filling weight delivered(mnim) (otimi) (g) in 72 h
Patients1 25 325 70 02 60 160 0 03 30 345 50 04 20 295 0 0
Normal (23)(mean + SEM) 248+10 17(+'( 132±15 83±3
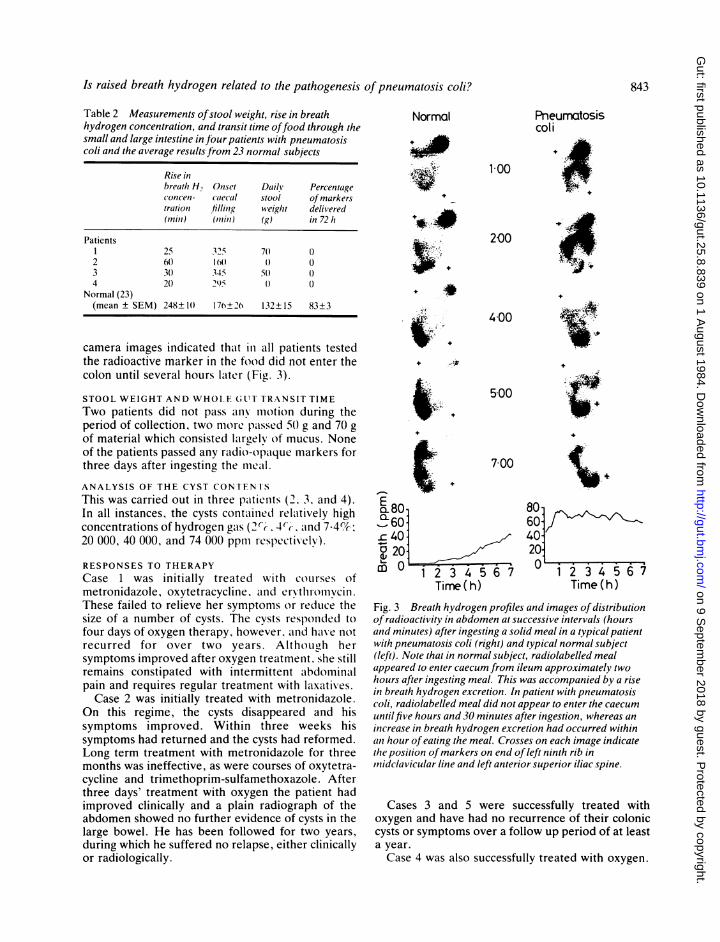
camera images indicated that in all patients testedthe radioactive marker in the food did not enter thecolon until several hours lalter (Fig. 3).
STOOL WEIGHT AND WHOLEhGLIT TRANSIT TIMETwo patients did not pass any moltion during theperiod of collection, two more paissed 5o g and 70 gof material which consisted largely of mucus. Noneof the patients passed any raidio-opaique markers forthree days after ingesting the meail.ANALYSIS OF THE CYST CONTEN I'SThis was carried out in three patients (2. 3. and 4).In all instances, the cysts contained relaitively highconcentrations of hydrogen gas (2'-C. 4(C. .and 7.4%20 000, 40 000, and 74 000 ppm respectively).
RESPONSES TO THERAPYCase 1 was initially treated with courses ofmetronidazole, oxytetracycline. anld ervthromvcin.These failed to relieve her symptoms o*r reduce thesize of a number of cysts. The cysts responlded tofour days of oxygen therapy, however. aind have notrecurred for over two years. Althoeugh hersymptoms improved after oxygen treatmenit. she stillremains constipated with intermittent abdominalpain and requires regular treatment with laxatives.Case 2 was initially treated with metronidazole.
On this regime, the cysts disappeared and hissymptoms improved. Within three weeks hissymptoms had returned and the cysts had reformed.Long term treatment with metronidazole for threemonths was ineffective, as were courses of oxytetra-cycline and trimethoprim-sulfamethoxazole. Afterthree days' treatment with oxygen the patient hadimproved clinically and a plain radiograph of theabdomen showed no further evidence of cysts in thelarge bowel. He has been followed for two years,during which he suffered no relapse, either clinicallyor radiologically.
Normal
1 00
Pneumatosiscoli
.F8T
200
_ .x#
_'K
17 +
400
500
700
E80Q60-40'a 20
m 0 1 2 3 4 56 7Timne ( h)
'.- ,A
+
4
'.
80-60-4020
ime 4 5 6Time (h)
Fig. 3 Breath hydrogen profiles and images ofdistributionof radioactivity in abdomen at successive intervals (hoursand minutes) after ingesting a solid meal in a typical patientwith pneumatosis coli (right) and typical normal subject(left). Note that in normal subject, radiolabelled mealappeared to enter caecum from ileum approximately twohours after ingesting meal. This was accompanied by a risein breath hydrogen excretion. In patient with pneumatosiscoli, radiolabelled meal did not appear to enter the caecumuntilfive hours and 30 minutes after ingestion, whereas anincrease in breath hydrogen excretion had occurred withinatn hour of eating the meal. Crosses on each image indicatethe position ofmarkers on end of left ninth rib in,nidclavicular line and left anterior superior iliac spine.
Cases 3 and 5 were successfully treated withoxygen and have had no recurrence of their coloniccysts or symptoms over a follow up period of at leasta year.Case 4 was also successfully treated with oxygen.
843
on 9 Septem
ber 2018 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.25.8.839 on 1 August 1984. D
ownloaded from

Read, Al-Janabi, and Cann
He remained free of abdominal symptoms until1981, when his condition recurred, but againresponded to treatment with oxygen. He hassuffered a further relapse, requiring oxygen, thisyear.
Discussion
Hydrogen gas cannot be produced by themetabolism of mammalian cells and can only beformed in the body by bacterial fermentation ofcarbohydrate. As such, hydrogen is usually formedin normal subjects when the unabsorbed carbo-hydrate in the diet enters the colon and is fermentedby colonic micro-organisms.5 The persistentlyraised concentrations of hydrogen excreted in thebreath of patients with pneumatosis coli implies thata population of enteric bacteria is encountering anabundant source of carbohydrate, even many hoursafter eating a meal. One possibility is that themajority of hydrogen is formed in the cysts them-selves by fermentation of plasma glucose. In supportof this is the observation that high concentrations ofH2 can be found within the cysts;9 12 13 a result thatwe have confirmed in these studies. Against it is thefinding that the breath hydrogen excretion can bereduced to basal values by colonic irrigation withoutaffecting the size or the number of the cysts, and theobservation that after abolition of the cysts byantibiotics or oxygen, the breath hydrogen excretionwas still abnormally high. These results stronglysuggest that the abnormally high hydrogenproduction is coming from the bowel lumen itself.Among the possibilities which could explain thisphenomenon are chronic ingestion of largequantities of unabsorbable carbohydrate, carbo-hydrate malabsorption, overgrowth of the smallintestine with gas forming bacteria, or the fermenta-tion of a copious secretion of mucus in the largeintestine.14 A careful dietary history showed that thepatients were not ingesting large amounts ofunabsorbable carbohydrate in their normal diet.Moreover, all of our patients were well nourishedand had no clinical evidence of malabsorption,though we did not carry out formal tests ofpancreatic function or lactose tolerance in any ofthem.Measurement of breath hydrogen after ingesting a
meal indicated that the hydrogen concentrationsrose at a time when the radioactive markers in themeal had not reached the colon. As there is anormally close correlation between the rise inhydrogen and the entry of a radiolabelled meal intothe colon,> 6 and since the radioactive marker is inthe liquid phase of the meal, this discrepancy isunlikely to be due to an unusually early arrival of the
liquid phase of the meal at the caecum. It is alsounlikely to be caused by fermentation by bacteria inthe mouth'S as the rises in breath hydrogen concen-tration observed in samples of end respiratory airfrom our patients are much higher and occur laterand have a longer duration than the transient risesreported for buccal fermentation of a bean meal innormal subjects.'i Instead the result suggests thatcarbohydrate may have been encountering gasforming bacteria in the small intestine before themeal had reached the colon. In support of thisinterpretation is the observation that the radio-labelled meal reached the colon very slowly in threeof our patients. Against it is the observation that the14C glycocholate test did not confirm bacterialovergrowth in any of our patients, though falsenegative results for this test are not uncommon,"1and the observation that high breath hydrogenconcentrations were recorded even in patients thathad been fasted for over 24 hours. A furtherpossibility is that the raised fasting hydrogen levelswere generated by fermentation of the largeamounts of colonic mucus,14 which may in turn bestimulated after meal ingestion. Our data do notpermit us to convincingly decide which, if either, ofthese two possibilities accounts for the high fastingbreath hydrogen concentrations.Although patients with pneumatosis coli pass
large quantities of blood stained mucus, they passlittle stool and measurement of colonic transit timesindicate that they are very constipated. This may beexplained in part by obstruction of the passage ofstools by the cysts, though two of our patientsremained constipated even after the cysts haddisappeared.Whether excessive hydrogen production in the
intestinal lumen plays any role in the production ofthe gas filled cysts is unclear from our data. Severaldifferent theories exist to explain the origin of thecysts. Previous experimental studies have shownthat it is possible for air which has leaked into themediastinum through a ruptured emphysematousbulla - for example, to track down and produce gasbubbles in the subserosa of the intestine.17 It is lesseasy to envisage how this mechanism could result insubmucosal cysts, just confined to the colon. More-over, none of the patients that we studied hadchronic obstructive airways disease. A secondtheory proposes that gas, produced in the intestinallumen, could enter the submucosa through breachesin the epithelium. This explanation has beeninvoked to explain cysts found in association withduodenal ulceration, at surgical anastomoses,19and after sigmoidoscopy.2" We did not observe anyobvious breach of the colonic mucosa atcolonoscopy in any of our patients, and none had
844
on 9 Septem
ber 2018 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.25.8.839 on 1 August 1984. D
ownloaded from

Is raised breath hydrogen related to the pathogenesis of pneulnatosis coli? 845
undergone a sigmoidoscopy before the onset of theirdisease. Moreover, if gas were entering from thelumen continuously via a mucosal breach, it isunlikely that the cysts would disappear on oxygentherapy or antibiotics when clearly this therapy doesnot prevent gas formation within the colonic lumen,and it is equally unlikely that cysts would remainwhen the colonic contents were flushed out.
In our opinion, the mnost likely explanation for theorigin of the cysts is the invatsion of the colonic wallby gas forming anaerobic bacteria. In support ofthis, pneumatosis coli hias been produced experi-mentally by injecting bacteria under the intestinalmucosa.212 If this is true, increasing the POG orgiving antibiotics would prevent cyst formation bycreating an unfavourable environment for theanaerobic bacteria within the bowel wall, althoughthis treatment would be unlikely to influencemarkedly the anaerobic populations and gas pro-duction in the colonic mass of faeces. On the otherhand, it is necessary to postulate a low oxygentension within the bowel wall for survival ofanaerobic bacteria in the colonic submucosa ofpatients with pneumatosis coli. This could occur inrespiratory failure or in colonic ischaemia, and mayexplain the observed relationships betweenpneumatosis coli and cystic fibrosis, 23 obstructiveairways disease,'6 24 or arteriosclerosis.' In thisregard, it is notable that three patients we studiedwere arteriopathic.
In conclusion, our data suggest that the highfasting breath hydrogen concentrations found inpatients with pneumatosis coli mavy be produced inthe intestinal lumen, either bv the fermentation ofcopious amounts of mucus in the colon, or byfermentation of dietary carbohydrate by bacteria inthe small intestine. We have beeni unable to discernany clear relationship between the riaised breathhydrogen concentrations and the formaition of cysts.
References
1 Gillon J. Tadesse K, Logan RFA. Holt S. Sircus W.Breath hydrogen in pneumatosis cystoides intestinalis.Gut 1979; 20: 1008-1 1.
2 Scarpello JHB, Sladen GE. Appraisal of the '4Cglycocholate acid test with special reference to themeasurement of faecal '4C excretion. Gmt 1977: 18:742-8.
3 Bergman I, Coleman JE, Evans D. A simple gaschromatograph with an electrochemical detector forthe measurement of hydrogen and carbon monoxide inthe parts per million range, applied to exhaled air.Chromatographia 1975; 8: 581-3.
4 Corbett CL, Thomas S, Read NW. Hobson N.Bergman I. Holdsworth CD. Electrochemical detector
for breath hydrogen determination: measurement ofsmall bowel transit time in normal subhects and patientswith the irritable bowel syndrome. Gut 1981; 22:836-40.
5 Read NW, Miles CA, Fisher D et al. Transit of a mealthrough the stomach, small intestine and colon innormal subjects and its role in the pathogenesis ofdiarrhoea. Gastroenterology 1980; 79: 1276-82.
6 Read NW, Al-Janabi MN, Bates TE, Barber DC.Effect of gastrointestinal intubation on the passage of asolid meal through the stomatch and small intestine inhumans. Gastroenterology 1983; 84: 1568-72.
7 Holgate AM, Read NW. Can a rapid small boweltransit limit absorption. lAbstract I Gut 1982; 23: A 192.
8 Hinton JM, Lennard Jones JE, Young AC. A newmethod for studying gut transit times using radio-opaque markers. Gut 1979; 20: 842-7.
9 Forgacs P, Wright PH, Wyatt AP. Treatment ofintestinal gas cysts by oxygen breathing. Lanicet 1973; 1:579-81.
10 Down RHL, Castleden WM. Oxygen therapy forpneumatosis coli. Br Med J 1975; 1: 493-4.
11 Bond JH, Levitt MD. Investigation of small boweltransit in man, utilizing pulmonary hydrogen (H.,)measurements. J Lab Clin Med 1974; 85: 546-59.
12 Hughes DTD, Gordon KCD, Swann JC, Bolt GL.Pneumatosis cystoides intestinalis. Gut 1966; 7: 553-7.
13 Hoflin F, van der Linden W. Pneumatosis cystoidesintestinalis treated by oxygen breathing. Scand JGastroenterol 1974; 9: 427-30.
14 Perman JA, Modler S. Glycoproteins as substrates forproduction of hydrogen in the large intestine. Gastro-enterology 1982; 83: 388-93.
15 Thompson DG, O'Brien J, McCarthy M, Hardie J.Oral microflora affect postprandial exhaled breathhydrogen concentrations. [Abstracti Cut 1983; 24:A978.
16 Caspary WF. Breath tests. Clinics in gastroenterology1978; 7: 351-74.
17 Keyting WS, McCarver RR, Kovrik JL. Daywitt AL.Pneumatosis intestinalis: a new concept. Radiology1961; 76: 733-41.
18 Koss LG. Abdominal gas cysts (pneumatosis cystoidesintestinum hominis). Arch Pathol 1952; 53: 537-47.
19 Sicard GA, Vaughan R, Wise L. Pneumatosis cystoidesintestinalis: an unusual complication of jejuno-ilealbypass. Surgery 1976; 79: 480-4.
20 Marshak RH, Blum SD, Eliasoph J. Pneumatosisinvolving the left side of the colon. JAMA 1956; 161:1626-8.
21 Stone HH, Allen WB, Smith BB III, Haynes CD.Infantile pneumatosis intestinalis. J Surg Res 1968; 8:301-6.
22 Yale CE, Batish E, Wu JR. The bacterial etiology ofpneumatosis cystoides intestinalis. Arch Su4rg 1974;109: 89-94.
23 Wood RE, Herman CJ, Johnson KW, Di Sant'AgnesePA. Pneumatosis coli in cystic fibrosis. Am J Dis Child1975; 29: 246-8.
24 Elliott GB, Elliott KA. The roentgenologic pathologyof so-called pneumatosis cystoides intestinalis. AJR1963; 89: 720-9.
on 9 Septem
ber 2018 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.25.8.839 on 1 August 1984. D
ownloaded from
Related Documents











