IRL Case Study Karen Abed, MT(ASCP), SBB Director, Technical Services Transfusion Medicine Symposium August 6, 2016

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

IRL Case Study
Karen Abed, MT(ASCP), SBB
Director, Technical Services
Transfusion Medicine Symposium
August 6, 2016
Disclosures
• I have no financial relationships
related to this presentation.
• I will not be speaking about any
specific commercial product,
device, or medication.
• I will not be speaking of any off
label use of medications or
devices

Objectives
• Identify 2 antibody workup
situations in which red cell
genotyping should be
considered
• Name 2 patient populations that
would benefit from prospective
phenotype/genotype matched
red cells

Case Presentation
• 17 year old African-
American male
• Two day history of:
– Fever
– Shortness of breath
– Productive cough
– Chest pain
• Presumptive diagnosis:
– Acute chest syndrome

Past Medical History
• Sickle cell anemia
– Recurrent pain crises
– Recurrent episodes of acute chest syndrome
– h/o multiple transfusions – last transfusion 4 months ago
• Just moved from mainland
• No red cell phenotype is available
Laboratory Evaluation
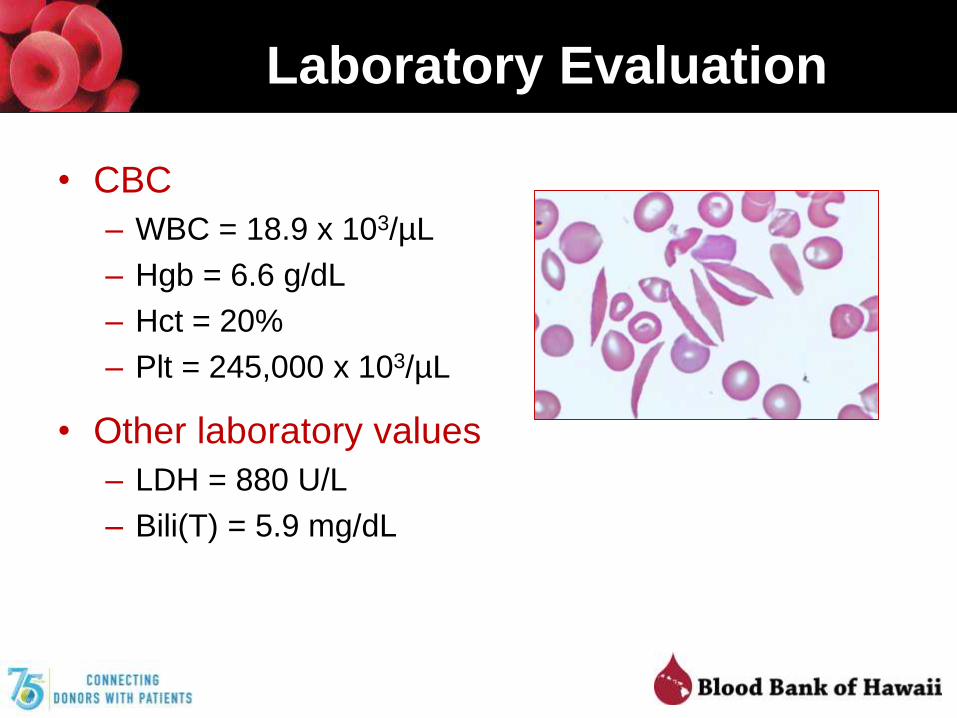
• CBC
– WBC = 18.9 x 103/µL
– Hgb = 6.6 g/dL
– Hct = 20%
– Plt = 245,000 x 103/µL
• Other laboratory values
– LDH = 880 U/L
– Bili(T) = 5.9 mg/dL

Transfusion Order
• Request for 3 units red cells ASAP
• Simple transfusion
Blood Type
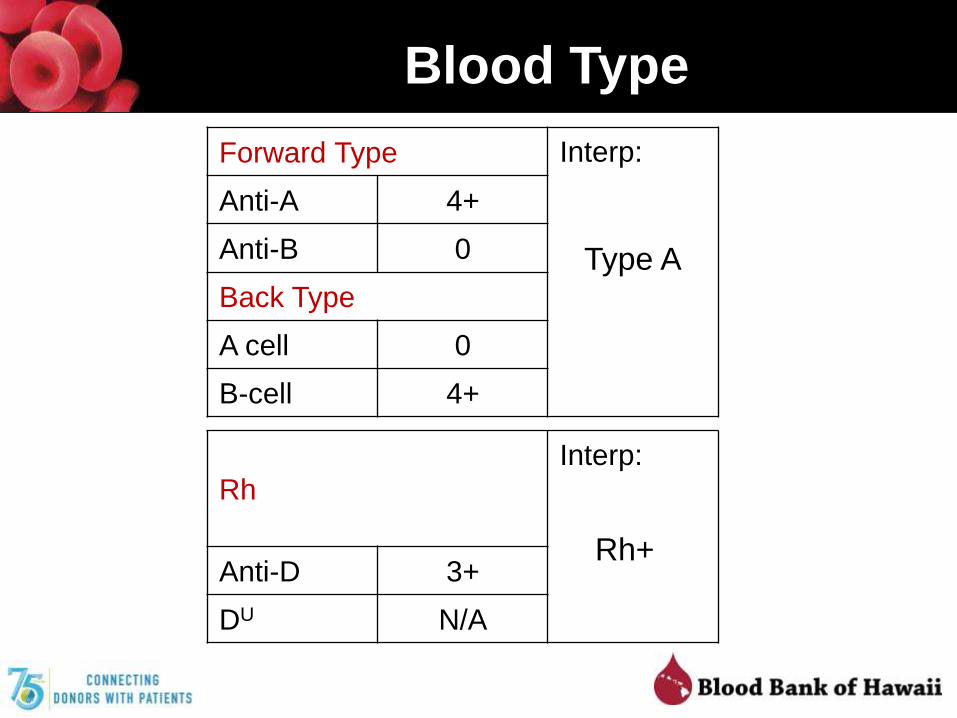
Forward Type Interp:
Type A
Anti-A 4+
Anti-B 0
Back Type
A cell 0
B-cell 4+
Rh
Interp:
Rh+Anti-D 3+
DU N/A

Antibody Screen (Gel)
• Autoantibodies
• Alloantibodies
• Drug-induced antibodies
• Reagent-related antibodies
Rh-hr KELL DUFFY KIDD LEWIS MNS LUTH TEST RESULTS
Cell
#D C E c e F Cw V K k Kpa Kpb Jsa Jsb Fya Fyb Jka Jkb Xga Lea Leb S s M N P1 Lua Lub AHG
1 + + 0 0 + 0 0 0 0 + 0 + 0 + + 0 0 + + 0 + + 0 + 0 + 0 + 3+
2 + 0 + + 0 0 0 0 0 + 0 + 0 + + 0 + 0 + 0 0 0 + + + 0 0 + 3+
3 0 0 0 + + 0 0 0 + + 0 + 0 + 0 + + + + + 0 + + + + +s 0 + 3+

Antibody Identification Panel
Rh-hr KELL DUFFY KIDD LEWIS MNS LUTHTEST
RESULTS
Cell
#D C E c e F Cw V K k Kpa Kpb Jsa Jsb Fya Fyb Jka Jkb Xga Lea Leb S s M N P1 Lua Lub AHG
1 + + 0 0 + 0 + 0 0 + 0 + 0 + + + + + + 0 + 0 + 0 + + + + 3+
2 + + 0 0 + 0 0 0 0 + 0 + 0 + 0 + + 0 + + 0 + + + 0 + 0 + 3+
3 + 0 + + 0 0 0 0 0 + 0 + 0 + 0 + 0 + + 0 + 0 + 0 + 0 0 + 2+
4 + 0 0 + + + 0 + 0 + 0 + 0 + 0 0 + + + 0 0 + 0 + + +s 0 + 3+
5 0 + 0 + + + 0 0 0 + 0 + 0 + + + + 0 + 0 + 0 + + + + 0 + 3+
6 0 0 + + + + 0 0 0 + 0 + 0 + + 0 0 + + 0 0 0 + + + 0 0 + 3+
7 0 0 0 + + + 0 0 + + 0 + 0 + 0 + 0 + + + 0 + 0 + 0 + 0 + 3+
8 0 0 0 + + + 0 0 0 + 0 + 0 + + 0 + 0 + 0 + + + + + 0 0 + 3+
9 0 0 0 + + + 0 0 0 + 0 + 0 + 0 + + + + 0 + + + 0 + + 0 + 2+
10 0 0 0 + + + 0 0 + + 0 + 0 + + + + + + 0 + 0 + + 0 +s 0 + 3+
11 + + 0 0 + 0 0 0 + + 0 + 0 + 0 + + 0 + 0 + 0 + 0 + + 0 + 3+
PC 3+

Attempted Crossmatch
• 3 A-positive red cell units crossmatched
• 3 of 3 incompatible
– AHG
– 1-3+ reactivity

Panel Interpretation
• Panreactive = 2-3+
• Autocontrol: 3+
• Possible interpretations:
– Autoantibodies
– Alloantibodies
» Antibody to a high frequency antigen
» Multiple alloantibodies
» Recently transfused

Direct Antiglobulin Test
• DAT: positive
– Autoantibodies
– Delayed reaction
– Drug-induced antibodies
– Non-specific protein
binding
Forward Type Interp:
Type A
Anti-A 4+
Anti-B 0
Back Type
A cell 0
B-cell 4+
Rh Interp:
Rh+Anti-D 3+
DU N/A
DAT
Poly IgG C3d
3+ 3+ 1+
Evaluation Goals
• Identify clinically significant relevant antibodies
• Select appropriate red cells for transfusion
• Plan for future transfusions
Two questions:
1. What antibodies in plasma?
2. What’s patient’s phenotype?

Evaluation Goals
• Identify clinically significant relevant antibodies
• Select appropriate red cells for transfusion
• Plan for future transfusions
Two questions:
1. What antibodies in plasma?
2. What’s patient’s phenotype?

Adsorptions
• Autoadsorption– Use the patient’s RBCs
– If there is no history of transfusion or pregnancy within the last 3 months
– If there are sufficient patient red cells
• Alloadsorption– Use reagent or donor RBCs of known and complementary
phenotype
– If there is a history of transfusion or pregnancy within the last 3 months
– If there are not enough patient RBCs available for an autoadsorption

Adsorptions
• Top 5 reasons to perform an adsorption
1. Identify underlying clinically significant alloantibodies
2. Identify underlying clinically significant alloantibodies
3. Identify underlying clinically significant alloantibodies
4. Identify underlying clinically significant alloantibodies
5. Identify underlying clinically significant alloantibodies
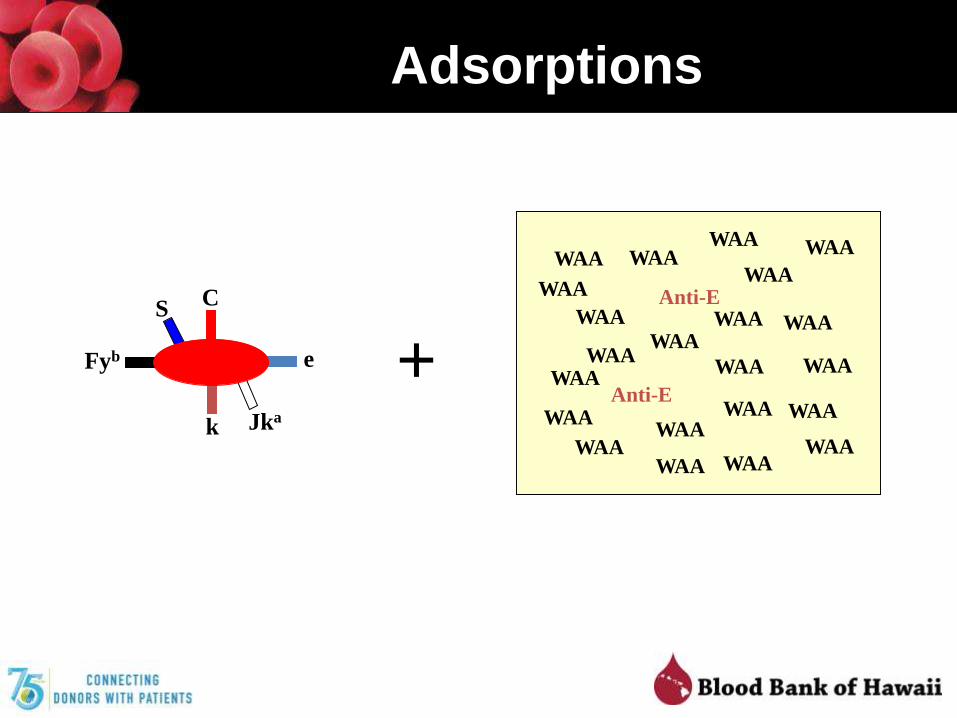
Adsorptions
S
k Jka
e
C
Fyb
WAA
WAA
WAAWAA
WAA
WAA
WAAWAA
WAAWAAWAA
WAA
Anti-E
WAA
Anti-E
WAA
WAA
WAA
WAA
WAA
WAA
WAA
WAA
WAA
+

Adsorptions
S
k Jka
e
C
Fyb
Anti-E
Anti-E
WAAWAA
WAA
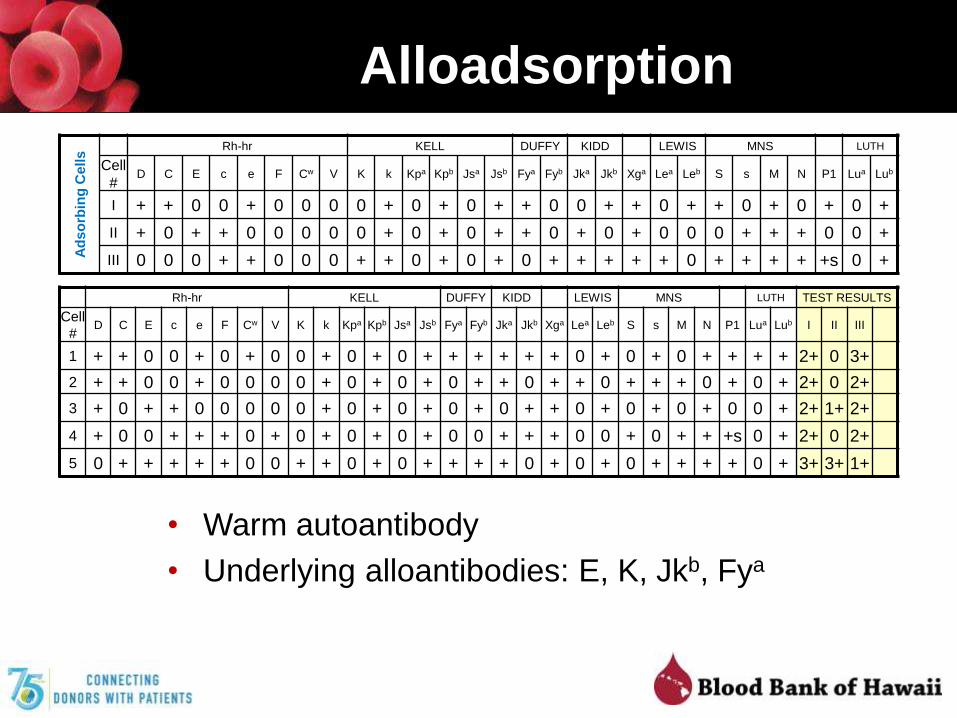
Alloadsorption
• Warm autoantibody
• Underlying alloantibodies: E, K, Jkb, Fya
Ad
so
rbin
g C
ells
Rh-hr KELL DUFFY KIDD LEWIS MNS LUTH
Cell
#D C E c e F Cw V K k Kpa Kpb Jsa Jsb Fya Fyb Jka Jkb Xga Lea Leb S s M N P1 Lua Lub
I + + 0 0 + 0 0 0 0 + 0 + 0 + + 0 0 + + 0 + + 0 + 0 + 0 +
II + 0 + + 0 0 0 0 0 + 0 + 0 + + 0 + 0 + 0 0 0 + + + 0 0 +
III 0 0 0 + + 0 0 0 + + 0 + 0 + 0 + + + + + 0 + + + + +s 0 +
Rh-hr KELL DUFFY KIDD LEWIS MNS LUTH TEST RESULTS
Cell
#D C E c e F Cw V K k Kpa Kpb Jsa Jsb Fya Fyb Jka Jkb Xga Lea Leb S s M N P1 Lua Lub I II III
1 + + 0 0 + 0 + 0 0 + 0 + 0 + + + + + + 0 + 0 + 0 + + + + 2+ 0 3+
2 + + 0 0 + 0 0 0 0 + 0 + 0 + 0 + + 0 + + 0 + + + 0 + 0 + 2+ 0 2+
3 + 0 + + 0 0 0 0 0 + 0 + 0 + 0 + 0 + + 0 + 0 + 0 + 0 0 + 2+ 1+ 2+
4 + 0 0 + + + 0 + 0 + 0 + 0 + 0 0 + + + 0 0 + 0 + + +s 0 + 2+ 0 2+
5 0 + + + + + 0 0 + + 0 + 0 + + + + 0 + 0 + 0 + + + + 0 + 3+ 3+ 1+
Evaluation Goals
• Identify clinically significant relevant antibodies
• Select appropriate red cells for transfusion
• Plan for future transfusions
Two questions:
1. What antibodies in plasma?
2. What’s patient’s phenotype?
Phenotype
• Importance
– Shortens list of possible alloantibodies
– Predicts difficulty in finding compatible blood
– Needed if phenotype-matched blood is desired
• What if patient has positive DAT?
– EGA-treatment
• What if patient has been recently transfused?
– Reticulocyte separation
– Hypotonic lysis (sickle cell patients)
– Genotyping
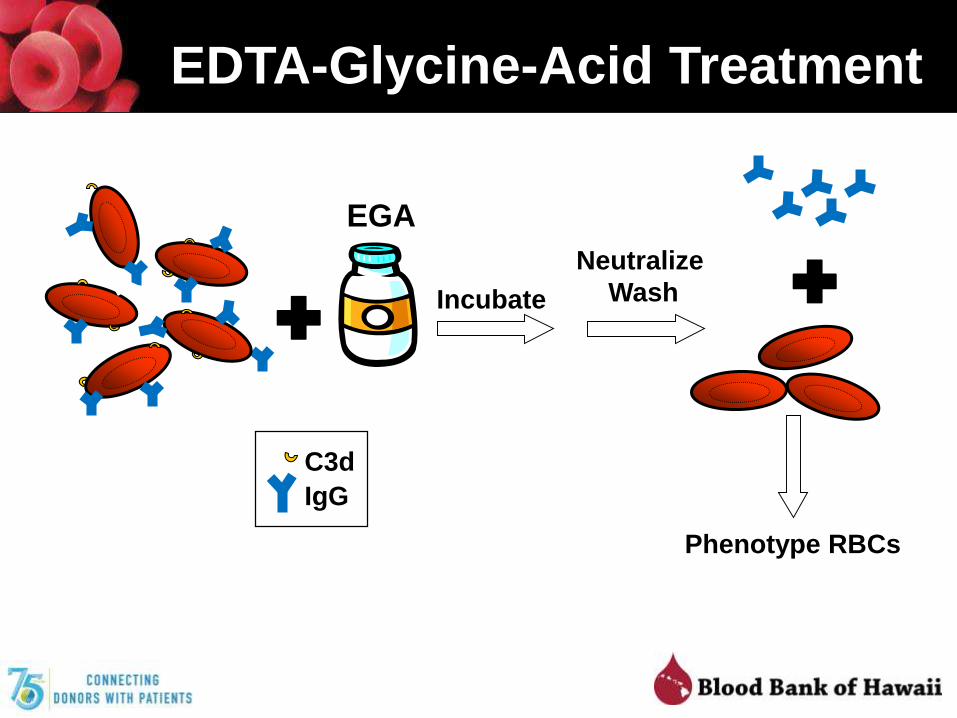
EDTA-Glycine-Acid Treatment
C3d
IgG
EGA
Phenotype RBCs
Incubate
Neutralize
Wash
EGA Treatment
• Cannot be used for phenotyping RBCs from recently transfused (within 2-3 months) patients
• Destroys Kell system (K, k), Bg, and Era antigens– Cannot be used to phenotype for Kell antigens
– Consider K-negative RBCs - if anti-K can’t be ruled-out

Reticulocyte Separation
• Reticulocytes have lower specific gravity than
mature erythrocytes
• Patient’s reticulocytes can be separated from
donor RBCs by centrifugation
– Gradients
– Microhematocrit capillary tubes
• Reticulocytes can then be used for phenotyping

Limitations
• Patient’s reticulocyte count must be adequate
• Large patient blood sample needed
• Separated reticulocytes may be a mixture of
recipient and donor cells
– Wait 1-2 weeks after most recent transfusion so donor
reticulocytes have already matured
– If phenotyping yields mixed field reactions → mixture
of patient and donor reticulocytes
Hypotonic Lysis
• Red cells from sickle cell disease patients more
resistant to lysis in hypotonic NaCl solutions
• Procedure:
– Wash cells in 0.3% NaCl until supernatant no longer
contains grossly visible hemoglobin
– Wash in 0.9% NaCl x 2
– Resuspend and test
Genotyping
• Relies on allele specific single nucleotide polymorphisms
• Uses DNA from recipient WBCs
• Leukopenic patients generally acceptable
• Some assays can use buccal swabs
• Eliminates donor red cell contamination issue
• Eliminates IgG coated red cell interference issue
• Can be done on stored patient DNA
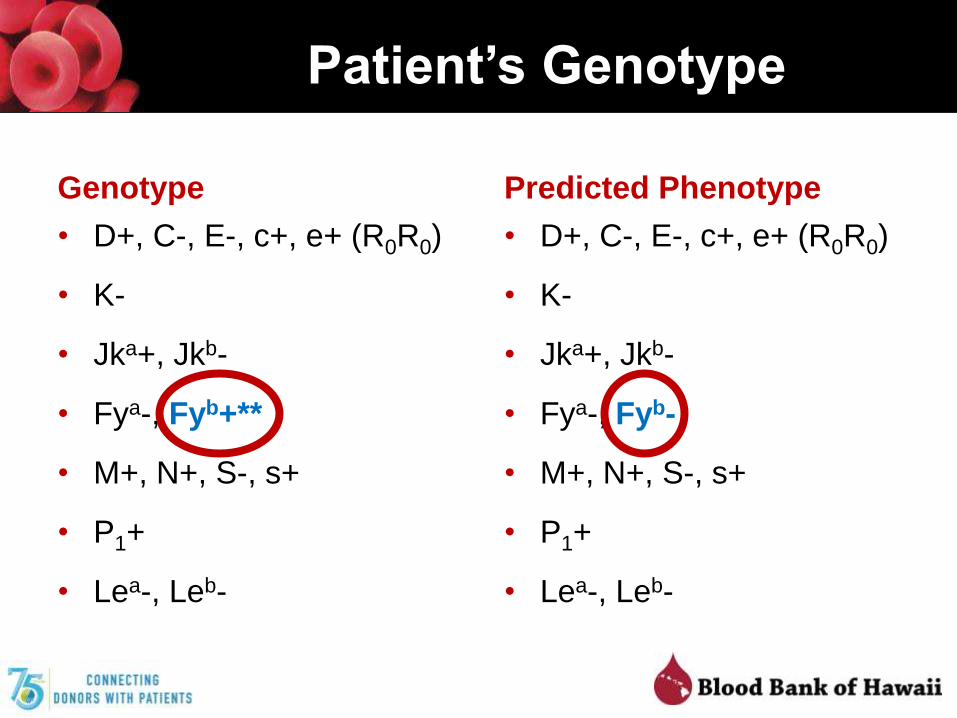
Patient’s Genotype
Genotype
• D+, C-, E-, c+, e+ (R0R0)
• K-
• Jka+, Jkb-
• Fya-, Fyb+**
• M+, N+, S-, s+
• P1+
• Lea-, Leb-
Predicted Phenotype
• D+, C-, E-, c+, e+ (R0R0)
• K-
• Jka+, Jkb-
• Fya-, Fyb-
• M+, N+, S-, s+
• P1+
• Lea-, Leb-
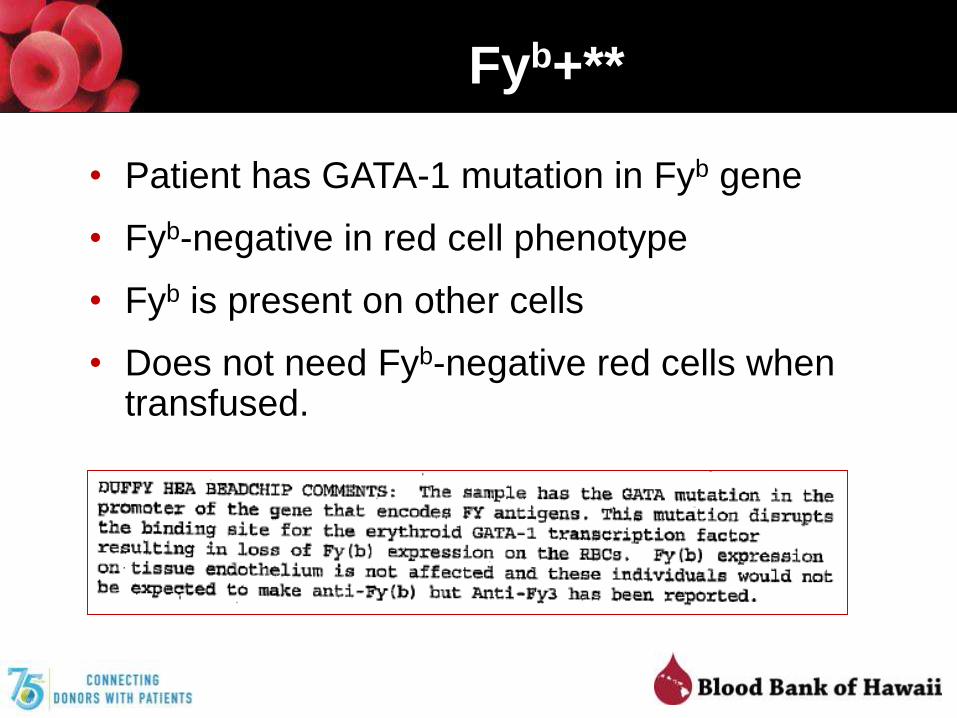
Fyb+**
• Patient has GATA-1 mutation in Fyb gene
• Fyb-negative in red cell phenotype
• Fyb is present on other cells
• Does not need Fyb-negative red cells when transfused.

Transfusion
• 3 units red cells ordered
– Type-compatible (A+)
– E, K, Fya, and Jkb – negative

Antigen Frequencies
Antigen African Americans Asians Caucasians
C 27% 93% 68%
c 96% 80% 47%
E 22% 49% 29%
e 98% 98% 96%
K 2% < 0.01% 9%
Jka 92% 73% 77%
Jkb 49% 76% 74%
Fya 10% 99% 66%
Fyb 23% 8% 83%

Antigen Frequencies
Antigen African Americans Asians Caucasians
C 27% 93% 68%
c 96% 80% 47%
E 22% 49% 29%
e 98% 98% 96%
K 2% < 0.01% 9%
Jka 92% 73% 77%
Jkb 49% 76% 74%
Fya 10% 99% 66%
Fyb 23% 8% 83%

Antigen Frequencies
Antigen African Americans Asians Caucasians
C 27% 93% 68%
c 96% 80% 47%
E 22% 49% 29%
e 98% 98% 96%
K 2% < 0.01% 9%
Jka 92% 73% 77%
Jkb 49% 76% 74%
Fya 10% 99% 66%
Fyb 23% 8% 83%

Antigen Frequencies
Antigen African Americans Asians Caucasians
C 27% 93% 68%
c 96% 80% 47%
E 22% 49% 29%
e 98% 98% 96%
K 2% < 0.01% 9%
Jka 92% 73% 77%
Jkb 49% 76% 74%
Fya 10% 99% 66%
Fyb 23% 8% 83%
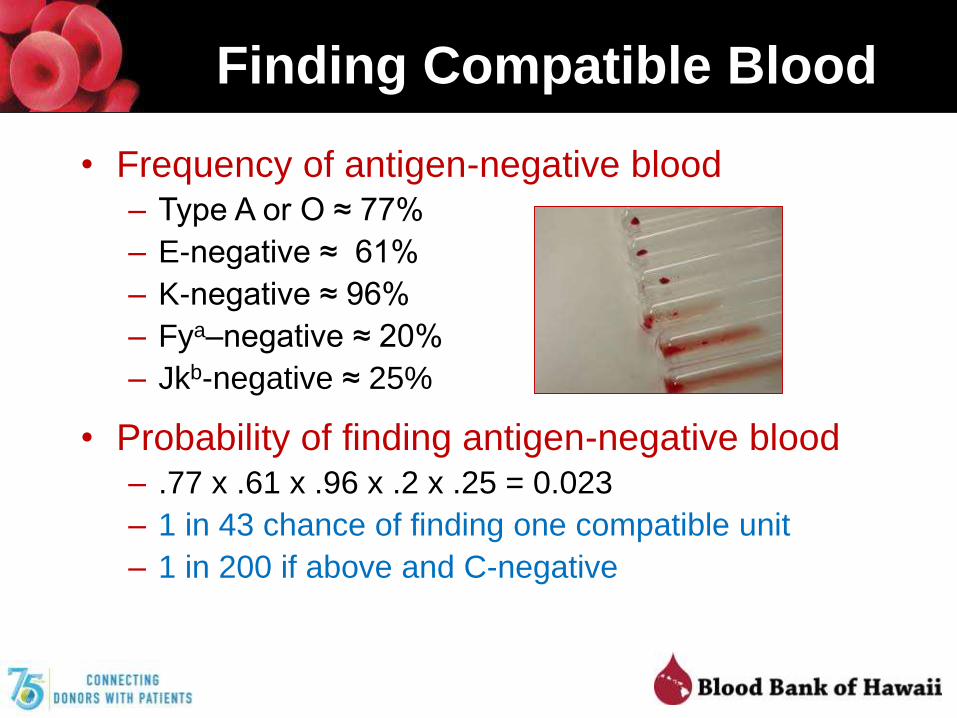
Finding Compatible Blood
• Frequency of antigen-negative blood– Type A or O ≈ 77%
– E-negative ≈ 61%
– K-negative ≈ 96%
– Fya–negative ≈ 20%
– Jkb-negative ≈ 25%
• Probability of finding antigen-negative blood– .77 x .61 x .96 x .2 x .25 = 0.023
– 1 in 43 chance of finding one compatible unit
– 1 in 200 if above and C-negative
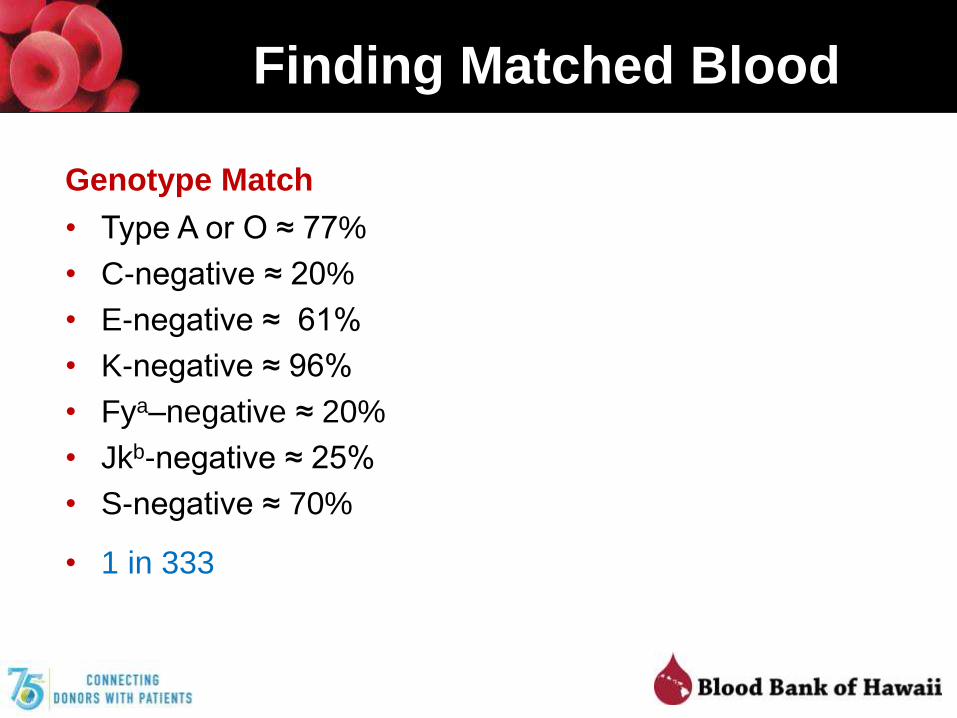
Finding Matched Blood
Full Phenotype Match
• Type A or O ≈ 77%
• C-negative ≈ 20%
• E-negative ≈ 61%
• K-negative ≈ 96%
• Fya/Fyb–negative ≈ 0.01%
• Jkb-negative ≈ 25%
• S-negative ≈ 70%
• Less than 1 in 10,000
Genotype Match
• Type A or O ≈ 77%
• C-negative ≈ 20%
• E-negative ≈ 61%
• K-negative ≈ 96%
• Fya–negative ≈ 20%
• Jkb-negative ≈ 25%
• S-negative ≈ 70%
• 1 in 333
Case Wrap-Up
• 3 units requested (E-, K-, Fya-, Jkb-)
– 3 units identified
– Transfused without transfusion reaction
• If full prospective matching required
– 1 frozen unit available
– 2 imported from mainland
Conclusion
• Multiply transfused patients can be challenging– Alloantibodies
– Autoantibodies
• Evaluations can be time-consuming
• Phenotypes can be helpful but often not possible in these patients
• Genotyping is now readily available– Multiply-transfused patients
– Sickle-cell disease
– Thalassemia
– daratumumab

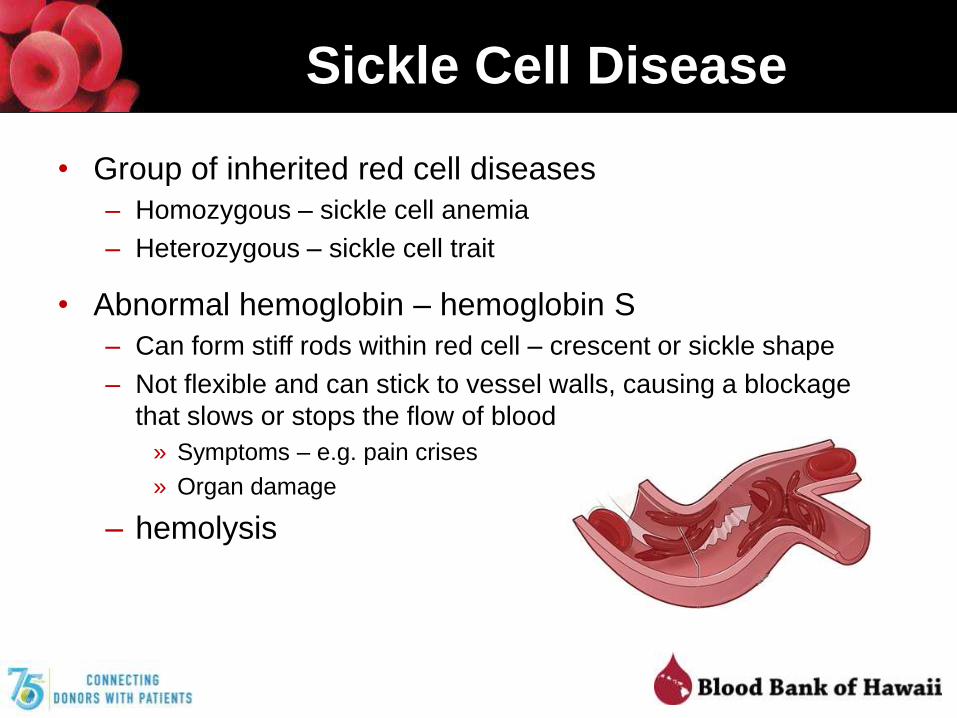
Sickle Cell Disease
• Group of inherited red cell diseases
– Homozygous – sickle cell anemia
– Heterozygous – sickle cell trait
• Abnormal hemoglobin – hemoglobin S
– Can form stiff rods within red cell – crescent or sickle shape
– Not flexible and can stick to vessel walls, causing a blockage
that slows or stops the flow of blood
» Symptoms – e.g. pain crises
» Organ damage
– hemolysis
SCD Prognosis
• Life-long disease
• Severity varies widely
• Life expectancy
– 1974 – 14 years
– Today – 40-60 years
• Cure – hematopoietic stem cell transplant (HSCT)
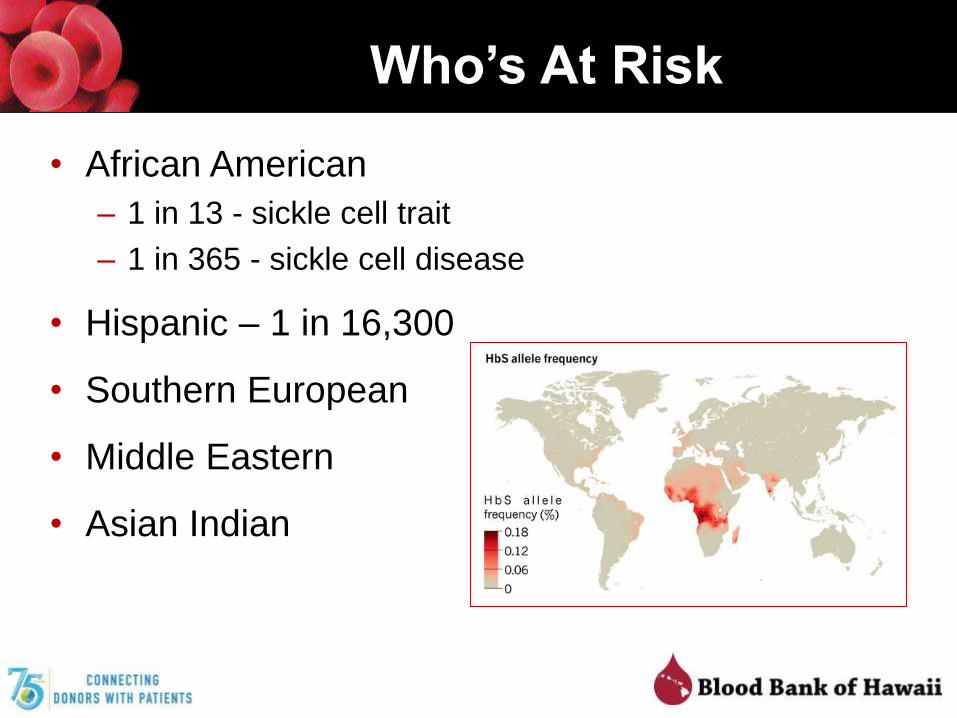
Who’s At Risk
• African American
– 1 in 13 - sickle cell trait
– 1 in 365 - sickle cell disease
• Hispanic – 1 in 16,300
• Southern European
• Middle Eastern
• Asian Indian

Transfusion
• Acute vs chronic
• Simple vs exchange

Transfusion in SCD
• Acute Complications
– Simple transfusion
» Symptomatic ACS + hgb ≥ 1g/dL
» Acute splenic sequestration + anemia
» Aplastic crisis
» Symptomatic anemia
– Exchange transfusion
» Symptomatic, severe ACS
– Simple or exchange
» Stroke
» Hepatic sequestration
» Intrahepatic cholestasis
» Multisystem organ failure
• Chronic complications
– Simple or exchange
» Previous stroke
» Increased transcranial Doppler
reading (> 200 cm/sec)
• Transfusion not indicated
– Acute complications» Uncomplicated pain crisis
» Priapism
» Asymptomatic anemia
» Acute kidney injury
– Chronic complications» Recurrent splenic sequestration
NHLBI, Evidence-based management of sickle cell disease: expert panel report, 2014
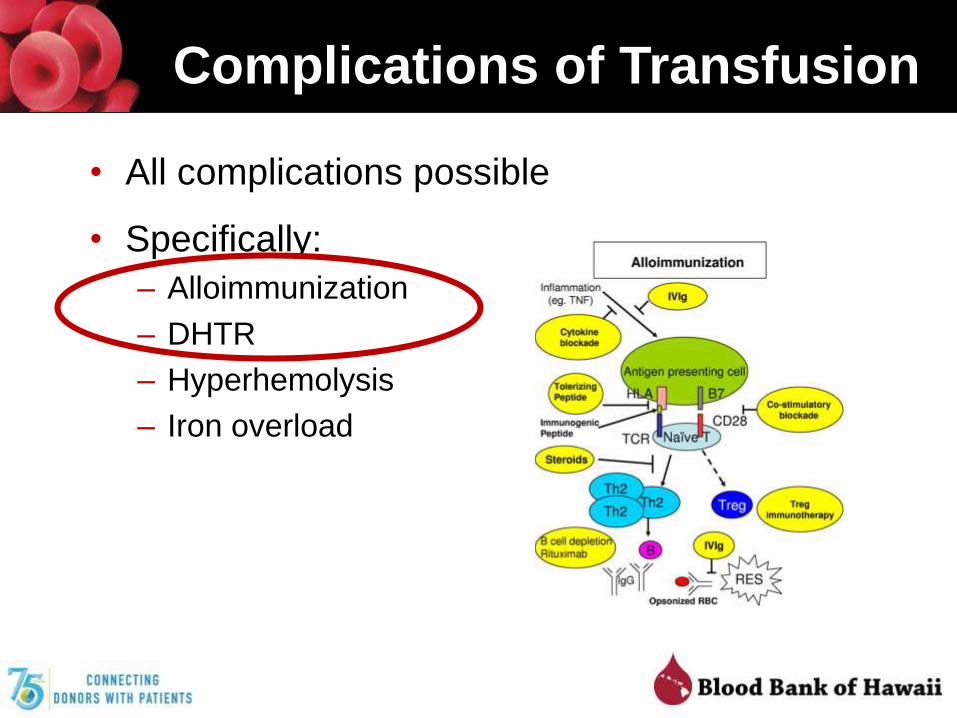
Complications of Transfusion
• All complications possible
• Specifically:
– Alloimmunization
– DHTR
– Hyperhemolysis
– Iron overload

Alloimmunization
• Rates– Alloimmunization ≈ 20-35% (6-85%)
– Autoantibody formation ≈ 4-10%
– DHTR ≈ 5-20%
• Antibodies– Rh antibodies ≈ 50-66%
– K and Jk ≈ 20%
• Phenotype-matching– 0-7% alloimmunization rate

Recommendations for Transfusion
• Leukoreduced
• Hemoglobin S–negative
• Phenotype-matching– Rh and Kell antigens
– Consider Kidd and Duffy
– Avoid known significant alloantibodies
• Chronic transfusion patients– Maintain HgbS level < 30%
– Immediately prior to next transfusion
• Acute transfusion– Not getting chronic transfusion therapy
– Keep target Hgb < 10 g/dL - hyperviscosity
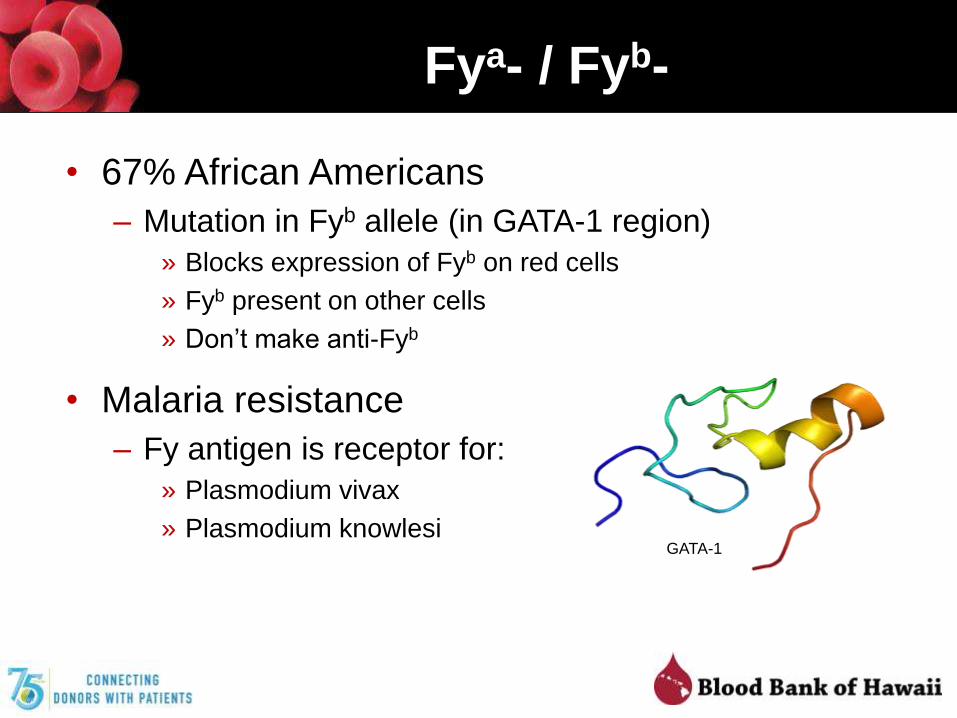
Fya- / Fyb-
• 67% African Americans
– Mutation in Fyb allele (in GATA-1 region)
» Blocks expression of Fyb on red cells
» Fyb present on other cells
» Don’t make anti-Fyb
• Malaria resistance
– Fy antigen is receptor for:
» Plasmodium vivax
» Plasmodium knowlesiGATA-1
Blood Bank of Hawaii
• Universal leukoreduction
• HgbS-negative
– Low rate in Hawaii donors
– Testing is available
• Phenotype-matched blood
– Prevention
– Alloimmunized
• Chronic therapy – similar to thalassemia patients
Antigen Typed Red Cells
• Increased typing of red cells – Rh and K– Donor testing laboratory
– Licensed reagents
– No need to serologically confirm
• Future– Additional screening for Jk, Fy, Ss
– Non-licensed reagents
• Genotyping– Patients who may require frequent transfusion
» Sickle cell disease
» Thalassemia
» Warm autoimmune hemolytic anemia
– Recently transfused
Related Documents











