http://acc.sagepub.com/ Care European Heart Journal: Acute Cardiovascular http://acc.sagepub.com/content/early/2014/05/20/2048872614534921 The online version of this article can be found at: DOI: 10.1177/2048872614534921 published online 22 May 2014 European Heart Journal: Acute Cardiovascular Care Lucas S Carmo, Diego C Baima, Valdecir Blefari, Vaniela Zonta, Luiz EA Troncon and Marcos A Rossi Involvement of the microvasculature in the pathogenesis of terlipressin-related myocardial infarction Published by: European Society of Cardiology ESC Working Group on Acute Cardiac Care and http://www.sagepublications.com can be found at: European Heart Journal: Acute Cardiovascular Care Additional services and information for http://acc.sagepub.com/cgi/alerts Email Alerts: http://acc.sagepub.com/subscriptions Subscriptions: http://www.sagepub.com/journalsReprints.nav Reprints: http://www.sagepub.com/journalsPermissions.nav Permissions: What is This? - May 22, 2014 OnlineFirst Version of Record >> at MUSEU PAULISTA USP on May 23, 2014 acc.sagepub.com Downloaded from at MUSEU PAULISTA USP on May 23, 2014 acc.sagepub.com Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
http://acc.sagepub.com/Care
European Heart Journal: Acute Cardiovascular
http://acc.sagepub.com/content/early/2014/05/20/2048872614534921The online version of this article can be found at:
DOI: 10.1177/2048872614534921
published online 22 May 2014European Heart Journal: Acute Cardiovascular CareLucas S Carmo, Diego C Baima, Valdecir Blefari, Vaniela Zonta, Luiz EA Troncon and Marcos A Rossi
Involvement of the microvasculature in the pathogenesis of terlipressin-related myocardial infarction
Published by:
European Society of Cardiology
ESC Working Group on Acute Cardiac Care
and http://www.sagepublications.com
can be found at:European Heart Journal: Acute Cardiovascular CareAdditional services and information for
http://acc.sagepub.com/cgi/alertsEmail Alerts:
http://acc.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
What is This?
- May 22, 2014OnlineFirst Version of Record >>
at MUSEU PAULISTA USP on May 23, 2014acc.sagepub.comDownloaded from at MUSEU PAULISTA USP on May 23, 2014acc.sagepub.comDownloaded from
European Heart Journal: Acute Cardiovascular Care 1 –7© The European Society of Cardiology 2014Reprints and permissions: sagepub.co.uk/journalsPermissions.navDOI: 10.1177/2048872614534921acc.sagepub.com
EUROPEANSOCIETY OFCARDIOLOGY ®
Introduction
Variceal bleeding into the upper gastrointestinal tract is a serious medical emergency in patients with liver cirrhosis and portal hypertension with high rates of recurrence and mortality. The management of acute hemorrhage from esophagogastric varices implicates endoscopic and phar-macological procedures or a combination of both.
Terlipressin (Glypressin®, Ferring Pharmaceuticals A/S, Copenhagen, Denmark), a synthetic analog of vasopressin, has been shown to be an effective pharmacologic drug in controlling hemorrhagic esophageal varices in patients with liver cirrhosis and to support endoscopic treatment.1–3 It represents the only drug to show survival advantage against a placebo. Because terlipressin is a prodrug, the active metabolite of which, lysine vasopressin, is gradually released over several hours, the typical vasopressinergic adverse events, such as release of coagulation factors and myocardial ischemia, are supposedly prevented.
Three cases of terlipressin-related cardiac ischemia events were previously reported in patients showing typical
electrocardiographic and echocardiographic changes and elevated serial cardiac markers.4–6
We report here the first case of myocardial infarction with anatomopathological evidence in a 24-year-old man with liver cirrhosis and bleeding esophageal varices treated with terlipressin. The findings allow insight into the clear involvement of the microcirculation in the pathogenesis of terlipressin-related myocardial ischemia.
Involvement of the microvasculature in the pathogenesis of terlipressin-related myocardial infarction
Lucas S Carmo1, Diego C Baima2, Valdecir Blefari1, Vaniela Zonta2, Luiz EA Troncon2 and Marcos A Rossi1†
AbstractWe report an autopsy case of a 24-year-old man with diagnoses of advanced alcoholic liver cirrhosis, portal hypertension, and esophageal variceal bleeding that presented extensive myocardial infarction after treatment with terlipressin. On postmortem examination the cut surface of the heart presented myocardial infarction implicating the left ventricle free wall, apex of the heart and ventricular septum. Light microscopic examination revealed that the extensive area of cardiac infarction was the result of the sum of diffuse foci of microinfarction of various ages interspersed with small clusters of preserved myocytes. Moreover, the epicardial vessels were patent while the small intramyocardial vessels presented thickened wall, apparent reduction in lumen diameter and disruption of endothelial cells indicative of spasm. The observations in this case allow clear insight into the involvement of the microcirculation in the pathogenesis of myocardial infarction with the use of terlipressin.
KeywordsTerlipressin, liver cirrhosis, upper gastrointestinal bleeding, myocardial infarction, microvasculature, vasospasm
Date received: 11 September 2013; accepted: 18 April 2014
1 Department of Pathology, Ribeirão Preto Medical School, University of São Paulo, Brazil
2 Department of Medicine, Division of Gastroenterology, Ribeirão Preto Medical School, University of São Paulo, Brazil
†Marcos A Rossi passed away on 9 May 2013.
Corresponding author:Luiz EA Troncon, Department of Medicine, Ribeirao Preto Medical School, University of São Paulo, Av. Bandeirantes 3900, 14049-900 Ribeirão Preto, SP, Brazil. Email: [email protected]
534921 ACC0010.1177/2048872614534921European Heart Journal: Acute Cardiovascular CareCarmo et alresearch-article2014
Clinical practice
at MUSEU PAULISTA USP on May 23, 2014acc.sagepub.comDownloaded from
2 European Heart Journal: Acute Cardiovascular Care
Case presentation
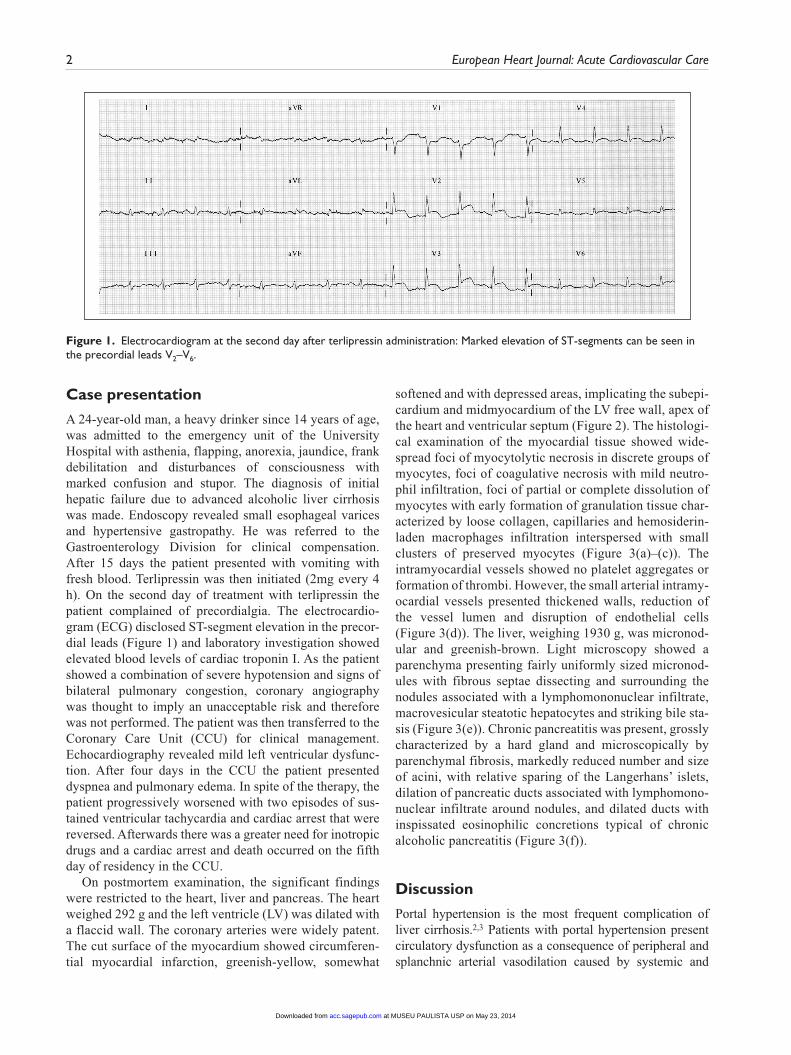
A 24-year-old man, a heavy drinker since 14 years of age, was admitted to the emergency unit of the University Hospital with asthenia, flapping, anorexia, jaundice, frank debilitation and disturbances of consciousness with marked confusion and stupor. The diagnosis of initial hepatic failure due to advanced alcoholic liver cirrhosis was made. Endoscopy revealed small esophageal varices and hypertensive gastropathy. He was referred to the Gastroenterology Division for clinical compensation. After 15 days the patient presented with vomiting with fresh blood. Terlipressin was then initiated (2mg every 4 h). On the second day of treatment with terlipressin the patient complained of precordialgia. The electrocardio-gram (ECG) disclosed ST-segment elevation in the precor-dial leads (Figure 1) and laboratory investigation showed elevated blood levels of cardiac troponin I. As the patient showed a combination of severe hypotension and signs of bilateral pulmonary congestion, coronary angiography was thought to imply an unacceptable risk and therefore was not performed. The patient was then transferred to the Coronary Care Unit (CCU) for clinical management. Echocardiography revealed mild left ventricular dysfunc-tion. After four days in the CCU the patient presented dyspnea and pulmonary edema. In spite of the therapy, the patient progressively worsened with two episodes of sus-tained ventricular tachycardia and cardiac arrest that were reversed. Afterwards there was a greater need for inotropic drugs and a cardiac arrest and death occurred on the fifth day of residency in the CCU.
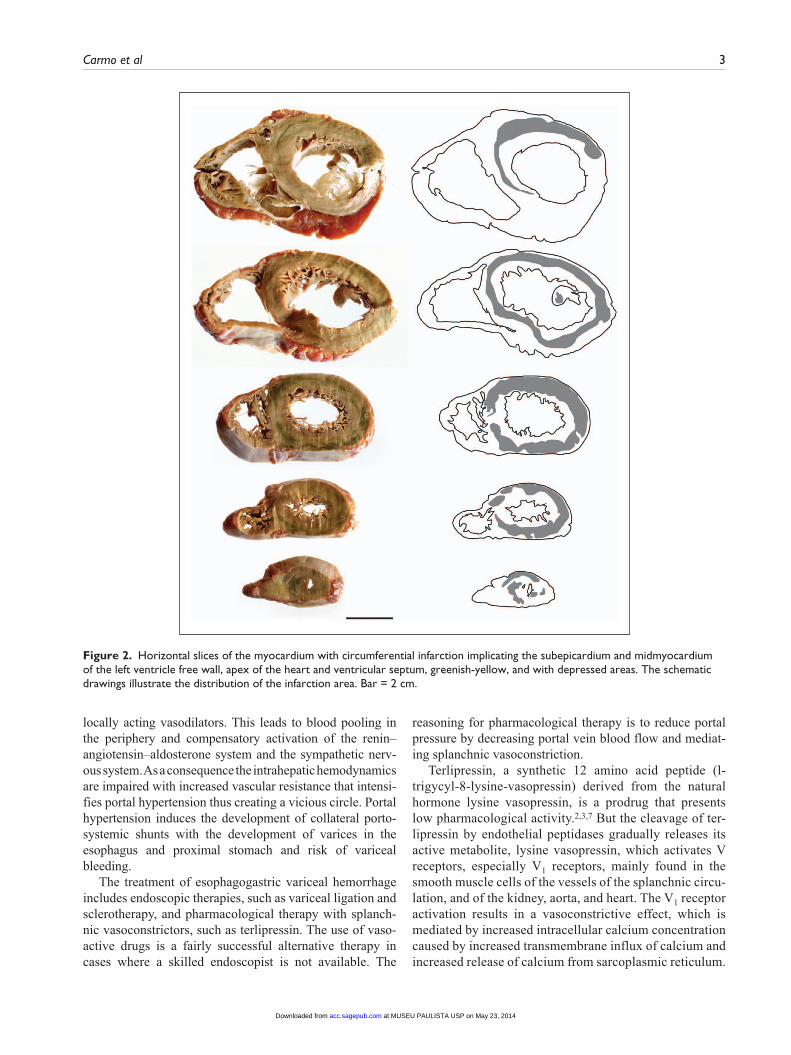
On postmortem examination, the significant findings were restricted to the heart, liver and pancreas. The heart weighed 292 g and the left ventricle (LV) was dilated with a flaccid wall. The coronary arteries were widely patent. The cut surface of the myocardium showed circumferen-tial myocardial infarction, greenish-yellow, somewhat
softened and with depressed areas, implicating the subepi-cardium and midmyocardium of the LV free wall, apex of the heart and ventricular septum (Figure 2). The histologi-cal examination of the myocardial tissue showed wide-spread foci of myocytolytic necrosis in discrete groups of myocytes, foci of coagulative necrosis with mild neutro-phil infiltration, foci of partial or complete dissolution of myocytes with early formation of granulation tissue char-acterized by loose collagen, capillaries and hemosiderin-laden macrophages infiltration interspersed with small clusters of preserved myocytes (Figure 3(a)–(c)). The intramyocardial vessels showed no platelet aggregates or formation of thrombi. However, the small arterial intramy-ocardial vessels presented thickened walls, reduction of the vessel lumen and disruption of endothelial cells (Figure 3(d)). The liver, weighing 1930 g, was micronod-ular and greenish-brown. Light microscopy showed a parenchyma presenting fairly uniformly sized micronod-ules with fibrous septae dissecting and surrounding the nodules associated with a lymphomononuclear infiltrate, macrovesicular steatotic hepatocytes and striking bile sta-sis (Figure 3(e)). Chronic pancreatitis was present, grossly characterized by a hard gland and microscopically by parenchymal fibrosis, markedly reduced number and size of acini, with relative sparing of the Langerhans’ islets, dilation of pancreatic ducts associated with lymphomono-nuclear infiltrate around nodules, and dilated ducts with inspissated eosinophilic concretions typical of chronic alcoholic pancreatitis (Figure 3(f)).
Discussion
Portal hypertension is the most frequent complication of liver cirrhosis.2,3 Patients with portal hypertension present circulatory dysfunction as a consequence of peripheral and splanchnic arterial vasodilation caused by systemic and
Figure 1. Electrocardiogram at the second day after terlipressin administration: Marked elevation of ST-segments can be seen in the precordial leads V2–V6.
at MUSEU PAULISTA USP on May 23, 2014acc.sagepub.comDownloaded from
Carmo et al 3
locally acting vasodilators. This leads to blood pooling in the periphery and compensatory activation of the renin–angiotensin–aldosterone system and the sympathetic nerv-ous system. As a consequence the intrahepatic hemodynamics are impaired with increased vascular resistance that intensi-fies portal hypertension thus creating a vicious circle. Portal hypertension induces the development of collateral porto-systemic shunts with the development of varices in the esophagus and proximal stomach and risk of variceal bleeding.
The treatment of esophagogastric variceal hemorrhage includes endoscopic therapies, such as variceal ligation and sclerotherapy, and pharmacological therapy with splanch-nic vasoconstrictors, such as terlipressin. The use of vaso-active drugs is a fairly successful alternative therapy in cases where a skilled endoscopist is not available. The
reasoning for pharmacological therapy is to reduce portal pressure by decreasing portal vein blood flow and mediat-ing splanchnic vasoconstriction.
Terlipressin, a synthetic 12 amino acid peptide (l- trigycyl-8-lysine-vasopressin) derived from the natural hormone lysine vasopressin, is a prodrug that presents low pharmacological activity.2,3,7 But the cleavage of ter-lipressin by endothelial peptidases gradually releases its active metabolite, lysine vasopressin, which activates V receptors, especially V1 receptors, mainly found in the smooth muscle cells of the vessels of the splanchnic circu-lation, and of the kidney, aorta, and heart. The V1 receptor activation results in a vasoconstrictive effect, which is mediated by increased intracellular calcium concentration caused by increased transmembrane influx of calcium and increased release of calcium from sarcoplasmic reticulum.
Figure 2. Horizontal slices of the myocardium with circumferential infarction implicating the subepicardium and midmyocardium of the left ventricle free wall, apex of the heart and ventricular septum, greenish-yellow, and with depressed areas. The schematic drawings illustrate the distribution of the infarction area. Bar = 2 cm.
at MUSEU PAULISTA USP on May 23, 2014acc.sagepub.comDownloaded from
4 European Heart Journal: Acute Cardiovascular Care
Due to this vasoconstrictive activity, terlipressin has been demonstrated to reduce flow into the portal vein and, thus, to reduce portal venous pressure and the blood flow through the portosystemic shunts. Simultaneously, terli-pressin increases arterial blood resistance and decreased cardiac output and heart rate.
Terlipressin has been regarded as safer than vasopressin, particularly concerning cardiovascular side effects, with adverse reactions thought to be rare but rather varied.3–7 This variability could be explained by a number of possible mechanisms, including pharmacogenomic interactions. Variability concerning therapeutic and adverse effects in
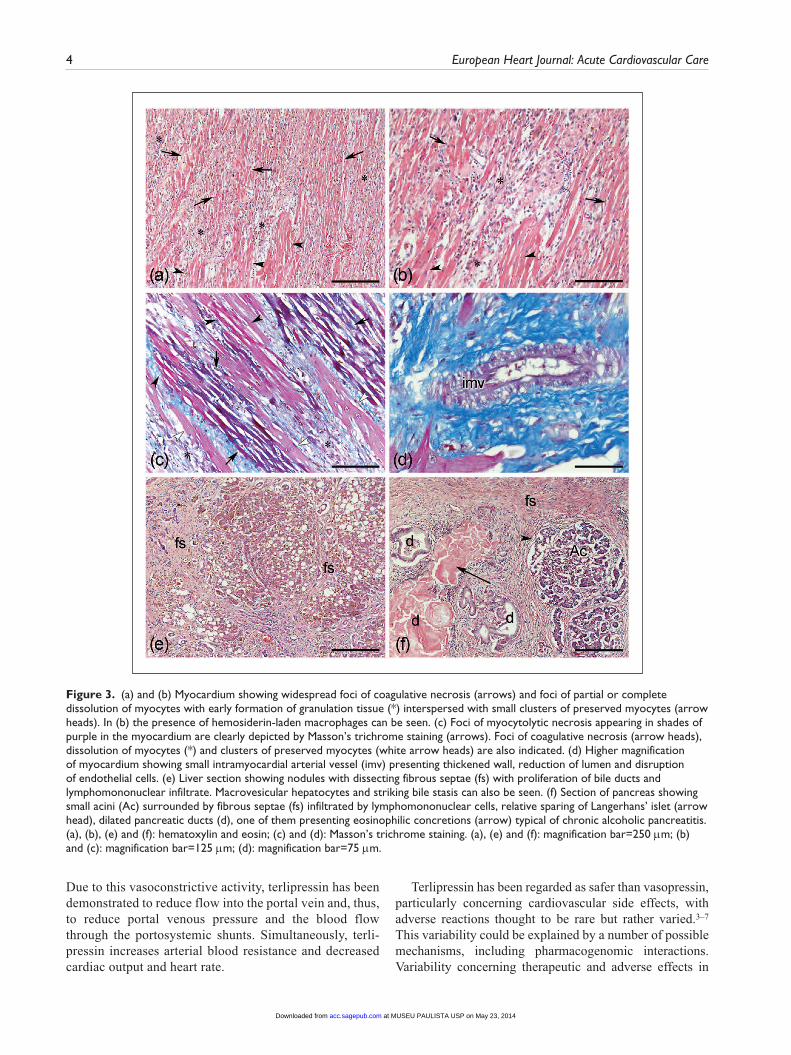
Figure 3. (a) and (b) Myocardium showing widespread foci of coagulative necrosis (arrows) and foci of partial or complete dissolution of myocytes with early formation of granulation tissue (*) interspersed with small clusters of preserved myocytes (arrow heads). In (b) the presence of hemosiderin-laden macrophages can be seen. (c) Foci of myocytolytic necrosis appearing in shades of purple in the myocardium are clearly depicted by Masson’s trichrome staining (arrows). Foci of coagulative necrosis (arrow heads), dissolution of myocytes (*) and clusters of preserved myocytes (white arrow heads) are also indicated. (d) Higher magnification of myocardium showing small intramyocardial arterial vessel (imv) presenting thickened wall, reduction of lumen and disruption of endothelial cells. (e) Liver section showing nodules with dissecting fibrous septae (fs) with proliferation of bile ducts and lymphomononuclear infiltrate. Macrovesicular hepatocytes and striking bile stasis can also be seen. (f) Section of pancreas showing small acini (Ac) surrounded by fibrous septae (fs) infiltrated by lymphomononuclear cells, relative sparing of Langerhans’ islet (arrow head), dilated pancreatic ducts (d), one of them presenting eosinophilic concretions (arrow) typical of chronic alcoholic pancreatitis. (a), (b), (e) and (f): hematoxylin and eosin; (c) and (d): Masson’s trichrome staining. (a), (e) and (f): magnification bar=250 µm; (b) and (c): magnification bar=125 µm; (d): magnification bar=75 µm.
at MUSEU PAULISTA USP on May 23, 2014acc.sagepub.comDownloaded from

Carmo et al 5
patients of drugs that target neurotransmitter systems is likely to have a genetic basis.8 Although a variety of muta-tions and polymorphisms have been described affecting the V2 vasopressin receptor,9 there are, to the best of our knowledge, no studies on pharmacogenetics of V1 recep-tors, which seem to be the main target for the terlipressin vasoconstrictive effect.2
Myocardial ischemia and infarction after terlipressin administration is considered an uncommon event, at least from the standpoint of clinically significant event, and eventually fatal.
A first case of terlipressin-related acute myocardial infarction was reported in a 46-year-old man with liver cir-rhosis and hemorrhagic esophageal varices.4 The patient presented ventricular tachycardia (VT) immediately after administration of 2 mg of terlipressin. Following the end of VT, the ECG showed ST-segment elevation in V1-V5 leads and echocardiography disclosed hypokinesia in the antero-apical segment of the LV. Because coronary angiography showed normal vessels, the authors suggested that coronary vasospasm caused the myocardial infarction.
A second case was reported in a 73-year-old woman admitted to the emergency department due to episodes of vomiting with fresh blood and drowsiness for the previous 24 hours.5 Emergency endoscopy detected bleeding from protuberant esophageal varices. Treatment included endo-scopic ligation of the esophageal varices and blood transfu-sion. Terlipressin (2 mg intravenously (i.v.) in a bolus) was also given for active bleeding control followed by a second dose 8 h later. Four hours later the patient complained of cold sweating, dyspnea and abdominal cramping. The ECG showed diffuse ST-segment elevation in the precordial leads. Emergency coronariography revealed 90% stenosis in the bifurcation of the left anterior descending-diagonal 1 branch without thrombosis and no critically stenosed cir-cumflex and right coronary arteries. Blood cardiac enzymes (creatine phosphokinase CK and CK-MB) and cardiac tro-ponin I were markedly elevated. Echocardiography revealed hypokinesia of the anterior and apico-septal seg-ments of the LV. The patient progressively worsened evolv-ing to cardiogenic shock, multiple organ failure and death 10 days after admission to the CCU. In spite of the signifi-cant atherosclerotic lesions of the heart ischemic territories associated with cardiogenic shock, the authors implicated vasospastic mechanism related to terlipressin as cause of the myocardial infarction.
More recently, a third case of non-ST-segment elevation myocardial infarction was reported.6 A 52-year-old man was admitted to the emergency room complaining of epi-gastric discomfort, dizziness and black stool for one day. The patient had been previously diagnosed with crypto-genic liver cirrhosis and esophageal varices. The patient underwent endoscopy that disclosed esophageal variceal eradication and bleeding gastric varices. Terlipressin was immediately initiated (4 mg i.v.) followed by 2 mg every
6 h for two days. The bleeding stopped but the patient had lung edema and shock that required mechanical ventilation, inotropic support and discontinuation of terlipressin admin-istration. The ECG revealed myocardial infarction with non-ST-segment elevation and blood examination disclosed markedly increased serial CK-MB and serial cardiac tro-ponin T. Three days later the patient improved and was dis-connected from the mechanical ventilator and inotropic support. Echocardiography performed two weeks later showed normal ventricular function. Thereafter, coronary angiography demonstrated pervious left and right coronary arteries. The authors concluded that high doses of terlipres-sin could induce serious cardiac complications secondary to coronary spasm.
The present report is about a first case of terlipressin-related extensive myocardial infarction implicating the LV free wall, apex of the heart, and ventricular septum with anatomopathological evidence. ST-segment elevation in the ECG and high blood levels of cardiac troponin I occurred in the second day after initiation of terlipressin.
Mechanism or mechanisms underlying the pathogenesis of myocardial infarction related to terlipressin have not yet been clarified. Vasoconstriction of the coronary arteries and increased procoagulant activity caused by activation of V2 receptors in endothelial cells and release of von Willebrand factor that enhances platelet aggregation and increases the risk of thrombosis have been proposed.7,10,11
In the present case, the ill-defined area of extensive myocardial infarction, as seen grossly, results from the sum of asynchronous microinfarction events of varying ages. Early acute myocardial microinfarction lesion or myocyto-lytic necrosis indiscrete groups of myocytes, as detected by Masson’s trichrome staining,12 small foci of coagulative necrosis accompanied with mild neutrophilic infiltration, small foci of almost complete removal of myocytes with granulation tissue and early collagen deposition were inter-spersed with small clusters of preserved myocytes. These observations clearly suggest that the microcirculation is most likely involved, that is, the primary site of disease could be at a level able to cause focal microinfarction of myocytes in discrete groups. This observation was made possible by the completion of autopsy. The occurrence of small intramyocardial vessel changes characterized by apparent thickened walls, reduction in lumen diameter and disruption of endothelial cells might suggest that spasm of these small intramyocardial arterial vessels could be involved in the pathogenesis of ischemic lesions of small clusters of myocytes.13,14 A similar mechanism has been demonstrated in chronic Chagas cardiomyopathy15,16 and septic cardiomyopathy.17–19
The features of the case herein presented indicate that the microcirculation is clearly involved in the pathogenesis of terlipressin-related myocardial ischemia. Nevertheless, the precise mechanisms of myocardial damage are not clear. Taking into account the vasoconstrictive effect of
at MUSEU PAULISTA USP on May 23, 2014acc.sagepub.comDownloaded from

6 European Heart Journal: Acute Cardiovascular Care
intravenous terlipressin on coronary circulation7,10 it is highly likely that microvascular spasm played a role. However, transient thrombosis and epicardial spasm cannot be excluded as alternative possibilities. A sustained epicar-dial spasm capable of inducing an EKG ST elevation would certainly cause a luminal thrombus and if resolved either spontaneously or by interventional treatment (which was not performed in our patient) would provide a diffuse area of microvascular obstruction secondary to the embolization of the fragments. Our pathological results do not support this hypothesis. Transient thrombosis may occur due to the already described presence of V1 receptors on the plate-lets20 but, as our pathological specimens demonstrate, no thrombi were found in either the microvascular or epicar-dial levels. On the other hand, it has been described that the vasoconstrictor response is not uniform in the distinct ves-sel beds21 and may even be prolonged.22 Our findings clearly indicate a widespread small vessel vasoconstriction that can reproduce clinical and electrocardiographical man-ifestations of an epicardial vessel obstruction. It is also interesting to mention that, as in other conditions associ-ated with increased cardiovascular risks, liver cirrhosis has been recently shown to be associated with systemic endothelial dysfunction,23 which might also have contrib-uted to the pathogenetic mechanisms leading to extensive myocardial infarction in this case.
In summary, during the management of esophagogastric variceal bleeding, terlipressin therapy can cause myocar-dial infarction as a result of the coalescence of diffuse and extensive foci of microinfarction of varying ages secondary to spasm of intramyocardial vessels. Further studies are needed to establish whether the risk of similar events but of lesser intensity are occasional or frequent with the use of terlipressin; in other words, to establish the incidence and frequency of microinfarctions in the heart of patients treated with terlipressin.
Acknowledgements
The authors are grateful to Dr André Schmidt, Associate Professor, Division of Cardiology, Department of Medicine, who kindly helped with the final version of this manuscript. MAR was Investigator (1A) of the CNPq.
Conflict of interest
None declared.
Funding
This work was supported by Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP), Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES) and Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq).
References
1. Garcia-Tsao G, Sanyal AJ and Grace ND. Prevention and management of gastroesophageal varices and variceal hem-orrhage in cirrhosis. Hepatology 2007; 46: 922–938.
2. Döhler KD and Meyer M. Vasopressin analogues in the treatment of hepatorenal syndrome and gastrointestinal haemorrhage. Best Pract Res Clin Anaesthesiol 2008; 22: 335–350.
3. Krag A, Borup T, Møller S, et al. Efficacy and safety of terli-pressin in cirrhotic patients with Variceal bleeding or hepato-renal syndrome. Adv Ther 2008; 25: 1105–1140.
4. Rosario R, Lalanne B, Lèbre P, et al. Infarctus du myocarde après injection de terlipressine pour hémorragie digestive. Gastroenterol Clin Biol 1996; 20: 712–713.
5. Lee MY, Chu CS, Lee KT, et al. Terlipressin-related acute myocardial infarction: A case report and literature review. Kaohsiung J Med Sci 2004; 20: 604–608.
6. Elzouki AN, El-Menyar A, Ahmed E, et al. Terlipressin-induced severe left and right ventricular dysfunction in patient presented with upper gastrointestinal bleeding: Case report and literature review. Am J Emerg Med 2010; 28: 540.e1–540.e6.
7. Kam PC, Williams S and Yoong FF. Vasopressin and terli-pressin: Pharmacology and its clinical relevance. Anaesthesia 2004; 59: 993–1001.
8. Small KM, Mcgraw DW and Liggett SB. Pharmacology and physiology of human adrenergic receptor polymorphisms. Annu Rev Pharmacol Toxicol 2003; 43: 381–411.
9. Thompson MD, Burnham WM and Cole DE. The G protein-coupled receptors: Pharmacogenetics and disease. Crit Rev Clin Lab Sci 2005; 42: 311–392.
10. Ryckwaert F, Virsolvy A, Fort A, et al. Terlipressin, a pro-vasopressin drug exhibits direct vasoconstrictor properties: Consequences on heart perfusion and performance. Crit Care Med 2009; 37: 876–881.
11. Pinelli A, Trivulzio S, Tomasoni L, et al. Cardiac necrosis markers associated with low nitric oxide levels in the plasma of rabbits after treatment with vasopressin: Protective effects of nitroglycerin administration. Pharmacol Res 2002; 45: 427–434.
12. Ouyang J, Guzman M, Desoto-Lapaix F, et al. Utility of desmin and a Masson’s trichrome method to detect early acute myocardial infarction in autopsy tissues. Int J Clin Exp Pathol 2009; 3: 98–105.
13. Vitullo JC, Karam R, Mekhail N, et al. Cocaine-induced small vessel spasm in isolated rat hearts. Am J Pathol 1989; 135: 85–91.
14. Ulusal I, Tari R, Ozturk G, et al. Dose-dependent ultrastruc-tural and morphometric alterations after erythropoietin treat-ment in rat femoral artery vasospasm model. Acta Neurochir 2010; 152: 2161–2166.
15. Rossi MA, Gonçalves S and Ribeiro-dos-Santos R. Experimental Trypanosoma cruzi cardiomyopathy in BALB/c mice. The potential role of intravascular platelet aggregation in its genesis. Am J Pathol 1984; 114: 209–216.
16. Rossi MA. Microvascular changes as a cause of chronic cardiomyopathy in Chagas’ disease. Am Heart J 1990; 120: 233–236.
17. Rossi MA and Santos CS. Sepsis-related microvascular myo-cardial damage with giant cell inflammation and calcifica-tion. Virchows Arch 2003; 443: 87–92.
18. Celes MR, Torres-Dueñas D, Prado CM, et al. Increased sarcolemmal permeability as an early event in experimental septic cardiomyopathy: A potential role for oxidative dam-age to lipids and proteins. Shock 2010; 33: 322–331.
at MUSEU PAULISTA USP on May 23, 2014acc.sagepub.comDownloaded from

Carmo et al 7
19. Celes MR, Prado CM and Rossi MA. Sepsis: Going to the heart of the matter. Pathobiology 2013; 80: 70–86.
20. Pedersen OS and Reichelt KL. The effect of arginine vaso-pressin, lysine vasopressin or oxytocin on ADP or arginine vasopressin-induced Ca2+ increase in human platelets. Clin Physiol 1999; 19: 305–310.
21. Altura BM. Dose-response relationships for arginine vaso-pressin and synthetic analogs on three types of rat blood vessels: possible evidence for regional differences in
vasopressin receptor sites within a mammal. J Pharmacol Exp Ther 1975; 193: 413–423.
22. Müller S, How OJ, Hermansen SE, et al. Vasopressin impairs brain, heart and kidney perfusion: An experimental study in pigs after transient myocardial ischemia. Crit Care 2008; 12: R20.
23. Berzigotti A, Erice E, Gilabert R, et al. Cardiovascular risk factors and systemic endothelial function in patients with cir-rhosis. Am J Gastroenterol 2013; 108: 75–82.
at MUSEU PAULISTA USP on May 23, 2014acc.sagepub.comDownloaded from
Related Documents






![Terlipressin versus other vasoactive drugs for hepatorenal ...[Intervention Review] Terlipressin versus other vasoactive drugs for hepatorenal syndrome Mads Israelsen 1, Aleksander](https://static.cupdf.com/doc/110x72/60a7d279a5295c2888291ae4/terlipressin-versus-other-vasoactive-drugs-for-hepatorenal-intervention-review.jpg)




