ORIGINAL ARTICLE In vivo reflectance confocal microscopy to monitor the response of lentigo maligna to imiquimod Ivette Alarcon, MD, a,b Cristina Carrera, MD, a,b,c Llucia Alos, MD, d,e Josep Palou, MD, d Josep Malvehy, MD, PhD, a,b,c and Susana Puig, MD, PhD a,b,c,e Barcelona, Spain Background: Imiquimod has been used for treating lentigo maligna (LM) in selected cases when surgery is not an appropriate option because of functional or aesthetic impairment. Reflectance confocal microscopy (RCM) is a noninvasive method that has not been validated for monitoring the treatment of LM with imiquimod. Objective: We sought to evaluate the use of in vivo RCM to accurately monitor the response of LM to nonsurgical treatment with topical imiquimod. Methods: Twenty patients with confirmed facial LM, not amenable to surgical treatment or radiation therapy, were included prospectively. Clinical evaluation was performed by dermoscopy, RCM, and histopathology. Patients applied imiquimod 5% for 8 weeks. The affected area was assessed using the previously described LM score on RCM, and target sample biopsies were performed to confirm or discard RCM findings. Results: Fifteen of the 20 patients (75%) presented histologic tumor clearance. Confocal microscopy identified 70% of these responders with no false-negative results, and when compared with histopathology, there was no significant difference in evaluating the response to imiquimod. Limitations: The impossibility of examining the entire lesion by means of histopathology is a limitation. Conclusion: In vivo RCM evaluation was useful in accurately monitoring the response of LM to nonsurgical treatment with topical imiquimod in patients when surgery is contraindicated. ( J Am Acad Dermatol http:// dx.doi.org/10.1016/j.jaad.2014.02.043.) Key words: dermoscopy; imiquimod; lentigo maligna; melanoma; noninvasive diagnosis; nonsurgical treatment; reflectance confocal microscopy. L entigo maligna (LM) is an early form of melanoma with an incidence that has increased during the past 2 decades. 1 Clinically, it is a pigmented lesion that occurs on sun-exposed skin, particularly the head and neck areas, of elderly patients. 2,3 It accounts for 79% to 83% of all melanoma in situ tumors, ranking as the most prevalent subtype. 1 Untreated, LM is associated with a 5% to 50% risk of progressing to LM mela- noma, the invasive counterpart, which is also increasing in individuals older than 45 years. 3,4 For many years, surgical excision with 5-mm clinical margins was the mainstay for the treatment of LM, but this recommendation was based on a 1992 From the Dermatology a and Pathology d Departments, Melanoma Unit, Hospital Clinic of Barcelona; Institut de Recerca Biom edica August Pi i Sunyer (IDIBAPS) b ; Centro de Investigaci on Biom edica en Red de Enfermedades Raras (CIBERER), Instituto de Salud Carlos III (ISCIII) c ; and Universitat de Barcelona. e The research at the Melanoma Unit in Barcelona is partially funded by grants 09/1393 and 12/00840 from Fondo de Investigaciones Sanitarias, Spain; by the Centro de Investigaci on Biom edica en Red (CIBER) de Enfermedades Raras of the Instituto de Salud Carlos III, Spain, cofunded by ‘‘Fondo Europeo de Desarrollo Regional, Uni on Europea, Una manera de hacer Europa’’; by the Ag encia de Gesti o d’Ajuts Universitaris i de Recerca (AGAUR) 2009 SGR 1337 of the Catalan Government, Spain; by the European Commission under the Sixth Framework Programme, Contract no. LSHC-CT-2006-018702 (GenoMEL); and by the National Cancer Institute of the US National Institutes of Health (CA83115). The sponsors had no role in the design and conduct of the study; in the collection, analysis, and interpretation of data; or in the preparation, review, or approval of the manuscript. Conflicts of interest: None declared. Accepted for publication February 27, 2014. Reprint requests: Susana Puig, MD, PhD, Dermatology Department, Melanoma Unit, Hospital Clinic Barcelona, Villarroel 170, 08036 Barcelona, Spain. E-mail: [email protected]. Published online April 8, 2014. 0190-9622/$36.00 Ó 2014 by the American Academy of Dermatology, Inc. http://dx.doi.org/10.1016/j.jaad.2014.02.043 1

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

ORIGINAL ARTICLE
In vivo reflectance confocal microscopy to monitorthe response of lentigo maligna to imiquimod
Ivette Alarcon, MD,a,b Cristina Carrera, MD,a,b,c Llucia Alos, MD,d,e Josep Palou, MD,d
Josep Malvehy, MD, PhD,a,b,c and Susana Puig, MD, PhDa,b,c,e
Barcelona, Spain
From
U
A
Bi
de
The r
by
Sa
Re
C
Re
A
20
Eu
Background: Imiquimod has been used for treating lentigo maligna (LM) in selected cases when surgery isnot an appropriate option because of functional or aesthetic impairment. Reflectance confocal microscopy(RCM) is a noninvasive method that has not been validated for monitoring the treatment of LM withimiquimod.
Objective: We sought to evaluate the use of in vivo RCM to accurately monitor the response of LM tononsurgical treatment with topical imiquimod.
Methods: Twenty patients with confirmed facial LM, not amenable to surgical treatment or radiation therapy,were included prospectively. Clinical evaluation was performed by dermoscopy, RCM, and histopathology.Patients applied imiquimod 5% for 8 weeks. The affected area was assessed using the previously describedLM score on RCM, and target sample biopsies were performed to confirm or discard RCM findings.
Results: Fifteen of the 20 patients (75%) presented histologic tumor clearance. Confocal microscopyidentified 70% of these responders with no false-negative results, and when compared with histopathology,there was no significant difference in evaluating the response to imiquimod.
Limitations: The impossibility of examining the entire lesion by means of histopathology is a limitation.
Conclusion: In vivo RCM evaluation was useful in accurately monitoring the response of LM to nonsurgicaltreatment with topical imiquimod in patients when surgery is contraindicated. ( J Am Acad Dermatol http://dx.doi.org/10.1016/j.jaad.2014.02.043.)
Key words: dermoscopy; imiquimod; lentigo maligna; melanoma; noninvasive diagnosis; nonsurgicaltreatment; reflectance confocal microscopy.
1
Lentigo maligna (LM) is an early form ofmelanoma with an incidence that hasincreased during the past 2 decades.1
Clinically, it is a pigmented lesion that occurs onsun-exposed skin, particularly the head and neckareas, of elderly patients.2,3 It accounts for 79% to83% of all melanoma in situ tumors, ranking as the
the Dermatologya and Pathologyd Departments, Melanoma
nit, Hospital Clinic of Barcelona; Institut de Recerca Biom�edica
ugust Pi i Sunyer (IDIBAPS)b; Centro de Investigaci�on
om�edica en Red de Enfermedades Raras (CIBERER), Instituto
Salud Carlos III (ISCIII)c; and Universitat de Barcelona.e
esearch at the Melanoma Unit in Barcelona is partially funded
grants 09/1393 and 12/00840 from Fondo de Investigaciones
nitarias, Spain; by the Centro de Investigaci�on Biom�edica en
d (CIBER) de Enfermedades Raras of the Instituto de Salud
arlos III, Spain, cofunded by ‘‘Fondo Europeo de Desarrollo
gional, Uni�on Europea, Una manera de hacer Europa’’; by the
g�encia de Gesti�o d’Ajuts Universitaris i de Recerca (AGAUR)
09 SGR 1337 of the Catalan Government, Spain; by the
ropean Commission under the Sixth Framework Programme,
most prevalent subtype. Untreated, LM is associatedwith a 5% to 50% risk of progressing to LM mela-noma, the invasive counterpart, which is alsoincreasing in individuals older than 45 years.3,4
For many years, surgical excision with 5-mmclinical margins was the mainstay for the treatmentof LM, but this recommendation was based on a 1992
Contract no. LSHC-CT-2006-018702 (GenoMEL); and by the
National Cancer Institute of the US National Institutes of Health
(CA83115). The sponsors had no role in the design and conduct
of the study; in the collection, analysis, and interpretationof data;
or in the preparation, review, or approval of the manuscript.
Conflicts of interest: None declared.
Accepted for publication February 27, 2014.
Reprint requests: Susana Puig, MD, PhD, Dermatology Department,
Melanoma Unit, Hospital Clinic Barcelona, Villarroel 170, 08036
Barcelona, Spain. E-mail: [email protected].
Published online April 8, 2014.
0190-9622/$36.00
� 2014 by the American Academy of Dermatology, Inc.
http://dx.doi.org/10.1016/j.jaad.2014.02.043
1

J AM ACAD DERMATOL2 Alarcon et al
consensus opinion.5 Since then, available data haveshown 5-mm margins to be inadequate for at leasthalf of LM6-10 probably because of the characteristicand potentially wide subclinical extension.Guidelines based on current evidence recommend5- to 10-mm margins11 and 1 study, based on a largeprospective series including 1072 patients,
CAPSULE SUMMARY
d In vivo reflectance confocal microscopymay improve diagnostic accuracy oflentigo maligna by providing betterdefinition of the extent of the lesion thanwith histopathology.
d In vivo reflectance confocal microscopyassists in monitoring the response oflentigo maligna to imiquimod treatmentand with long-term follow-up.
d Imiquimod therapy of lentigo malignamonitored by reflectance confocalmicroscopy is an option when surgery isnot indicated.
recommend a 9-mm marginfor all melanoma in situ.12
Although surgical excision isthe standard for LM treat-ment, it is not a reasonableoption for a group ofpatients, because of potentialfunctional or aestheticimpairment, comorbidity, orpatient’s choice. In thiscontext, nonsurgical moda-lities may be considered.
Imiquimod, a toll-likereceptor 7 agonist, is animmune-response modifierthat stimulatesboth the innateand adaptive arms of the im-mune system, resulting in anenhanced immune func-
tion.13 This effect of imiquimod, together with the insitu activation of signals such as proinflammatorycytokines and up-regulation of major histocompati-bility complex (MHC) class I/II molecules, may becritical in inducing an optimal T-cell-mediatedantitumor response.14 There is in vitro evidencedemonstrating a direct effect of imiquimodinhibiting melanogenesis and proliferation ofhuman melanocytes down-regulating the expressionof microphtalmia-associated transcription factor(MITF).15,16 The off-label use of topical imiquimodin LM has been proposed as an alternative treatmentto surgery and an adjunctive modality after surgicalexcision.17-23 Three case series using staged widelocal excision to assess imiquimod treatmentefficacy, with the largest study involving 40 patients,showed a histologic cure rate of 75%.17 This relativelylow cure rate for LM could be explained by theinaccurate assessment of the primary lesion usingsample biopsy specimens, with the major risk ofundertreating the invasive component.22,24,25Reflectance confocal microscopy (RCM) is anoninvasive imaging technique that allows thein vivo examination of the epidermis and papillarydermis providing a cellular resolution comparablewith histology.26 This technique is particularly usefulwhen evaluating pigmented lesions, as melaninappears bright under reflectance at near-infraredwavelengths,27 and has been shown to improve
melanoma diagnostic accuracy.28-30 One interestingfeature of RCM, related to the characteristic subclinicalextension of LM, refers to the possibility of navigationon a horizontal field of view of up to 8 3 8 mm,providing a better definition of the extent of the lesionthan routine histopathology. There is evidence thatthe use of RCM to distinguish LM and other macules
on the face can help both thediagnosis and the determina-tion of the LM margins.31
The aim of our study wasto evaluate the use of RCMin accurately monitoring theresponse of LM to nonsur-gical treatment with topicalimiquimod 5%.
METHODSA prospective study of 20
patients referred for treatmentof LM was conducted at theMelanoma Unit of HospitalClinic in Barcelona, betweenJune 2007 and June 2011. Alllesions were histologicallyconfirmed facial LM, not
amenable to surgical treatment or radiation therapy.Immunocompromised patients and those with clinicaland histologic evidence of LM melanoma wereexcluded. Informed consent for acquiring the images,taking sample biopsy specimens, and treatment wasobtained after discussing treatment alternatives withpatients.
Clinical baseline evaluation and after-treatmentassessment were performed by dermoscopy, bymeans of RCM and histopathology in all patients.After clinical diagnosis of LM, lesions were imagedwith a digital camera (Canon PowerShot G7 andG10,Canon, Tokyo, Japan) and high-resolution dermo-scope (DermLite Photo, 3GEN LLC, Dana Point, CA).Subsequently, RCM images were acquired, using acommercially availableRCMsystem (Vivascope1500,Lucid, Henrietta, NY) that uses a near-infrared laser at830 nm operating at a power of less than 20 mW. Theindividual images of 0.5 3 0.5 mm are stitchedtogether to form a mosaic of up to 8 3 8 mm2 fieldof view. The image acquisition protocol included atleast 3 serial optical sections obtained at the super-ficial epidermal layer, the dermoepidermal junction,and papillary dermis. In addition, vertical evaluationat different depths30 (Z-stacks) of areas with atypiawere included. For each lesion, imaging a sequenceof 3 ‘‘block’’ images took between 5 and 8 minutes.
To diagnose LM, a biopsy was performedin selected areas guided by clinical examination,

Fig 1. Outcome of treatment according to each method ofassessment. RCM, Reflectance confocal microscopy.
Table I. Statistical measures calculated for eachmethod to identify lentigo maligna
Clinical
evaluation Dermoscopy RCM
Sensitivity, %95% CI
200.5-71.6
6014.6-94.7
10047.8-100
Specificity, %95% CI
86.659.4-98.3
66.638.3-88.1
93.368-99.8
PPV, % 33.3 37.5 83.3NPV, % 76.4 51.9 100No. of false-negativeresults
4 2 0
CI, Confidence interval; NPV, negative predictive value; PPV,
positive predictive value; RCM, reflectance confocal microscopy.
Table II. Evolution of lentigo maligna score bygroup
LM score
Prior therapy
(mean 6 SD)
Posttherapy
(mean 6 SD)
Responders 2.86 6 0.8 0 6 0Nonresponders 2.2 6 0.4 2 6 0
LM, Lentigo maligna.
J AM ACAD DERMATOL Alarcon et al 3
dermoscopy, and RCM. All the lesions included wereflat under clinical examination.
Patients were instructed to apply imiquimodcream 5%, covering the affected area and a 1-cmmargin surrounding skin, once daily, 5 days a weekfor 8 weeks. During this period, if excessive inflam-matory reaction was elicited by applying imiquimod,the frequency was decreased to 3 days a week untilinflammation subsided or interrupted if severecutaneous toxicity presented. Twelve weeks afterthe completion of treatment and 12 months later, tocheck for residual/recurrent melanoma, the entiretreated area was assessed by means of RCM andtarget sample biopsies were performed to confirm ordiscard RCM findings in suspicious areas. If theevaluated area did not show any criteria for LMunder RCM, a single biopsy specimen was taken toconfirm the response to the therapy.
A new simplified algorithm described by Guiteraet al31 was calculated for each lesion. This algorithm,termed ‘‘LM score,’’ evaluates the presence of 2 majorfeatures that scored 2 points each (nonedged papillaeand round pagetoid cells [20 mm), and 4 minorfeatures. Of these minor criteria, 3 positive featuresscored 1 point each ($ 3 atypical cells at the junctionin 5 images, follicular localization of pagetoid cells,and/or atypical junctional cells, nucleated cellswithinthe dermal papillae), and 1 negative feature scoredminus 1 point (broadened honeycomb pattern). Thethreshold of greater than or equal to 2 has a sensitivityof 85% and a specificity of 76% (odds ratio 18.6; 95%confidence interval 9.3-37.1). To avoid false-negativeresults in the study, the complete response toimiquimod was defined by a score of 0 and absenceof response by the presence of any positive criteria.With this threshold greater than or equal to 1 theexpected sensitivity was increased to 93%.31
Histologically, LM and persistence after treatmentwas defined by a proliferation of atypical melano-cytes arranged as single cells or nests in confluencealong the dermoepidermal junction or extensionof melanocytes down adnexal structures.32,33 Finalhistopathological diagnosis was obtained by theconsensus opinion of 2 experienced dermato-pathologists (J. P. and L. A.).
Twoexpert observers (S. P. and J.M.) described thefeatures of RCM of each lesion. The images acquiredfor each case were encoded and then analyzedaccording to the LM score by a trained observer(I. A.) and verified by an expert observer (J. M.).
To define the final outcome, we evaluated thehistopathological result and the recurrence rate afterthe follow-up period, according to this, tumorclearance was defined as the absence of histologiccriteria for LM and absence of recurrence.34,35
False-positive results were defined as areasdiagnosed as LM by the LM score on RCM withoutconfirmation by histopathology analysis and theareas diagnosed as LM by histopathology butnot by RCM examination were characterized asfalse-negative results.
Statistical testsTo conduct the statistical analysis we used a
statistical package (SPSS, Release 15.0, IBM Corp,Armonk, NY). We used x2 test to assess the statisticalsignificance (defined as P value \ .05) of associa-tions of complete response assessed by LM score andfinal outcome. We also compared the 2 diagnostic
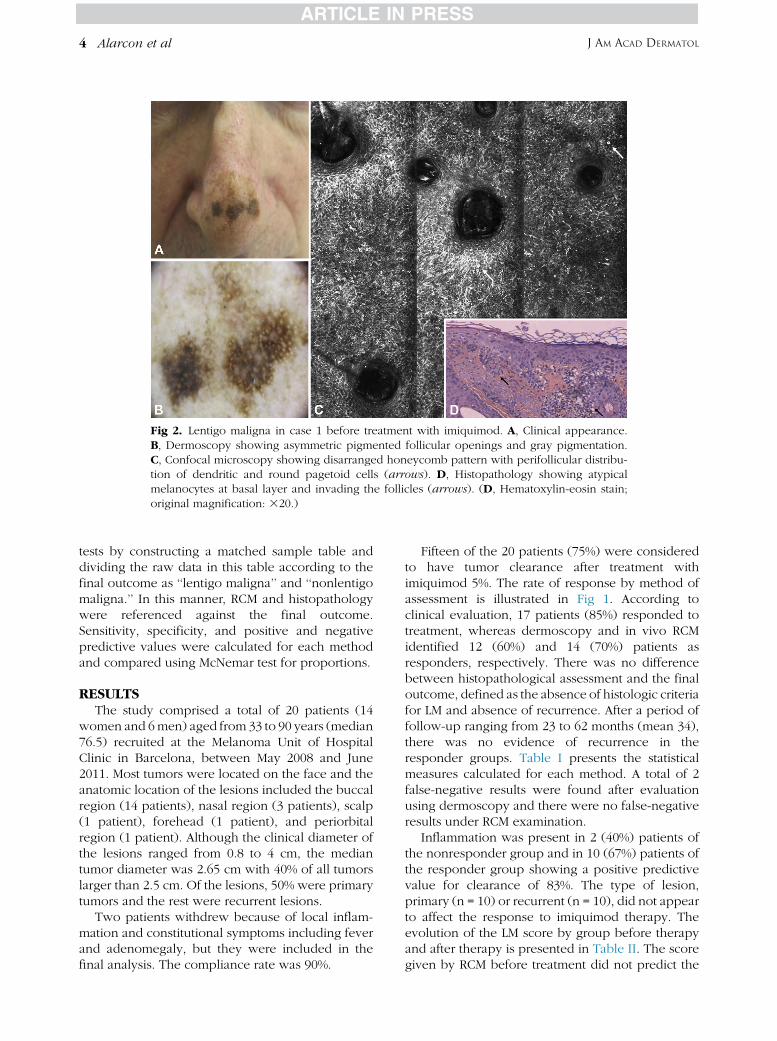
Fig 2. Lentigo maligna in case 1 before treatment with imiquimod. A, Clinical appearance.B, Dermoscopy showing asymmetric pigmented follicular openings and gray pigmentation.C, Confocal microscopy showing disarranged honeycomb pattern with perifollicular distribu-tion of dendritic and round pagetoid cells (arrows). D, Histopathology showing atypicalmelanocytes at basal layer and invading the follicles (arrows). (D, Hematoxylin-eosin stain;original magnification: 320.)
J AM ACAD DERMATOL4 Alarcon et al
tests by constructing a matched sample table anddividing the raw data in this table according to thefinal outcome as ‘‘lentigo maligna’’ and ‘‘nonlentigomaligna.’’ In this manner, RCM and histopathologywere referenced against the final outcome.Sensitivity, specificity, and positive and negativepredictive values were calculated for each methodand compared using McNemar test for proportions.
RESULTSThe study comprised a total of 20 patients (14
women and 6men) aged from 33 to 90 years (median76.5) recruited at the Melanoma Unit of HospitalClinic in Barcelona, between May 2008 and June2011. Most tumors were located on the face and theanatomic location of the lesions included the buccalregion (14 patients), nasal region (3 patients), scalp(1 patient), forehead (1 patient), and periorbitalregion (1 patient). Although the clinical diameter ofthe lesions ranged from 0.8 to 4 cm, the mediantumor diameter was 2.65 cm with 40% of all tumorslarger than 2.5 cm. Of the lesions, 50% were primarytumors and the rest were recurrent lesions.
Two patients withdrew because of local inflam-mation and constitutional symptoms including feverand adenomegaly, but they were included in thefinal analysis. The compliance rate was 90%.
Fifteen of the 20 patients (75%) were consideredto have tumor clearance after treatment withimiquimod 5%. The rate of response by method ofassessment is illustrated in Fig 1. According toclinical evaluation, 17 patients (85%) responded totreatment, whereas dermoscopy and in vivo RCMidentified 12 (60%) and 14 (70%) patients asresponders, respectively. There was no differencebetween histopathological assessment and the finaloutcome, defined as the absence of histologic criteriafor LM and absence of recurrence. After a period offollow-up ranging from 23 to 62 months (mean 34),there was no evidence of recurrence in theresponder groups. Table I presents the statisticalmeasures calculated for each method. A total of 2false-negative results were found after evaluationusing dermoscopy and there were no false-negativeresults under RCM examination.
Inflammation was present in 2 (40%) patients ofthe nonresponder group and in 10 (67%) patients ofthe responder group showing a positive predictivevalue for clearance of 83%. The type of lesion,primary (n = 10) or recurrent (n = 10), did not appearto affect the response to imiquimod therapy. Theevolution of the LM score by group before therapyand after therapy is presented in Table II. The scoregiven by RCM before treatment did not predict the

Fig 3. Lentigo maligna case 1 after treatment with imiquimod. A, Clinical appearance showingclearance of disease. B, Dermoscopy showing clearance of disease, lack of pigmentation. C,Confocal microscopy showing a preserved honeycomb (asterisk) with preserved follicularopenings (arrows). D, Histopathology showing normal epidermis without atypical melano-cytes at basal layer. (D, Hematoxylin-eosin stain; original magnification: 320.)
J AM ACAD DERMATOL Alarcon et al 5
final outcome and even though we found a higherscore in the group of responders, this difference wasnot statistically significant (P = .2).
After comparing RCM and histopathologyagainst absence of recurrence, our gold standard,we found no statistically significant differencebetween sensitivity (P = 1) or specificity (P [ .05)of both methods in assessing clearance of LM (Fig 1).
Figs 2 and 3 present a case classified bydermoscopy and RCM as having clearance ofLM after treatment with imiquimod. The biopsyspecimen, taken in areas guided by RCM, confirmedthe absence of atypical cells.
DISCUSSIONAccording to a review of the literature regarding
treatment of LM with topical imiquimod,4 the studiesshowing the highest clearance rates for imiquimod(up to 91%) were those where the evaluation oftumor clearance was based on clinical evaluation20
or after treatment biopsies, with the risk of over-valuing the response. The efficacy rates reported bystudies performing standard wide local excision22,23
or staged excision17 after imiquimod treatment werelower: 53%,22 68%,23 and 75%17 of response rate,respectively.
Our study showed a response rate to imiquimodof 75%, which is in line with the tumor clearance
rate obtained by wide local excision.17 In ourinvestigation, clinical evaluation seemed to over-estimate the tumor clearance after imiquimodtherapy (85%), with a high number of false-negative results (4), whereas dermoscopy underes-timates the response (60%), but presents fewerfalse-negative results than clinical examination (2).Confocal microscopy identified 70% of patients asresponders without false-negative results, andwhen compared with histopathology, there wasno statistically significant difference between RCMand histopathology in evaluating the response toimiquimod.
The LM score before treatment did not reachstatistical significance to be considered as aprognostic factor of response, but a tendency exists.This LM score was also useful for detectingunrecognized subclinical extension of LM in 4patients. We even selected a score greater than orequal to 1 to increase the sensitivity of the LM score;all the persistent lesions after treatment obtained ascore greater than or equal to 2.
In a recent study published by Guitera et al36
aimed at determining whether in vivo RCM mappingof difficult LM cases might alter patient care andtreatment, they found that RCM mapping changedthe treatment in 27 patients (73%) with 11 patientshaving a major change in their surgical procedure,

J AM ACAD DERMATOL6 Alarcon et al
and 16 being offered radiotherapy or imiquimodtreatment as a consequence of the RCM findings.
The main limitation of our study refers to theimpossibility of examining the entire lesion bymeans of histopathology. Nevertheless, the abilityof RCM to assess optical sections of intact skin makesthis new technology suitable for guiding the site toobtain biopsy specimens and to noninvasivelymonitor the response.
The recurrence rate after a long follow-up periodis the main confirmation of the cure rate in skincancer. In LM the surgical cure rate is considered after5 years of follow-up, in our study the mean time offollow-up is 34 months without signs of recurrence.
With the current approach, we tried to addressseveral issues in the management of LM withimiquimod therapy. The results obtained showedthe reliability of RCM evaluation of the response ofLM to nonsurgical treatment with topical imiquimod.RCM is a complementary tool for the evaluation ofLM that has clinical benefits for the patients in termsof presurgical assessment and monitoring responseof treatment and detection of subclinical recur-rences. The clearance rates accomplished by imiqui-mod in the current and previous studies maintain thistherapy as a second-line treatment option in caseswhere surgical excision is not indicated.
REFERENCES
1. Swetter SM, Boldrick JC, Jung SY, Egbert BM, Harvell JD.
Increasing incidence of lentigo maligna melanoma subtypes:
northern California and national trends 1990-2000. J Invest
Dermatol 2005;125:685-91.
2. Cohen LM. Lentigo maligna and lentigo maligna melanoma.
J Am Acad Dermatol 1995;3:923-36.
3. Ellis LZ, Cohen JL, High W, Stewart L. Melanoma in situ treated
successfully using imiquimod after nonclearance with surgery:
review of the literature. Dermatol Surg 2012;38:937-46.
4. Erickson C, Miller SJ. Treatment options in melanoma in situ:
topical and radiation therapy, excision and Mohs surgery. Int J
Dermatol 2010;49:482-91.
5. National Institutes of Health consensus development confer-
ence statement on diagnosis and treatment of early melanoma,
January 27-29, 1992. Am J Dermatopathol 1993;15:34-43.
6. Agarwal-Antal N, Bowen GM, Gerwels JW. Histologic evalua-
tion of lentigo maligna with permanent sections: implications
regarding current guidelines. J Am Acad Dermatol 2002;47:
743-8.
7. Bienert TN, Trotter MJ, Arlette JP. Treatment of cutaneous
melanoma of the face by Mohs micrographic surgery. J Cutan
Med Surg 2003;7:25-30.
8. Albertini JG, Elston DM, Libow LF, Smith SB, Farley MF. Mohs
micrographic surgery for melanoma: a case series, a compar-
ative study of immunostains, an informative case report, and a
unique mapping technique. Dermatol Surg 2002;28:656-65.
9. Zalla MJ, Lim KK, Dicaudo DJ, Gagnot MM. Mohs micrographic
excision of melanoma using immunostains. Dermatol Surg
2000;26:771-84.
10. McKenna JK, Florell SR, Goldman GD, Bowen GM. Lentigo
maligna/lentigo maligna melanoma: current state of diagnosis
and treatment. Dermatol Surg 2006;32:493-504.
11. Bichakjian CK, Halpern AC, Johnson TM, Foote Hood A,
Grichnik JM, Swetter SM, et al. Guidelines of care for the
management of primary cutaneous melanoma. J Am Acad
Dermatol 2011;65:1032-47.
12. Kunishige JH, Brodland DG, Zitelli J. Surgical margins for
melanoma in situ. J Am Acad Dermatol 2012;66:438-44.
13. Sauder DN. Imiquimod: modes of action. Br J Dermatol 2003;
149(Suppl):5-8.
14. Michalopoulos P, Yawalkar N, Bronnimann M, Kappeler A,
Braathen LR. Characterization of the cellular infiltrate during
successful topical treatment of lentigo maligna with
imiquimod. Br J Dermatol 2004;151:903-6.
15. Kang HY, Park TJ, Jin SH. Imiquimod, a toll-like receptor 7
agonist, inhibits melanogenesis and proliferation of human
melanocytes. J Invest Dermatol 2009;129:243-6.
16. Park H-Y, Wu C, Yonemoto L, Murphy-Smith M, Wu H,
Stachur CM, et al. MITF mediates cAMP-induced protein
kinase C-beta expression in human melanocytes. Biochem J
2006;395:571-8.
17. Cotter M, McKenna JK, Bowen GM. Treatment of lentigo
maligna with imiquimod before staged excision. Dermatol
Surg 2008;34:147-51.
18. Naylor MF, Crowson N, Kuwahara R, Teague K, Garcia C,
Mackinnis C, et al. Treatment of lentigo maligna with topical
imiquimod. Br J Dermatol 2003;149(Suppl):66-70.
19. Powell AM, Robson AM, Russell-Jones R, Barlow RJ. Imiquimod
and lentigo maligna: a search for prognostic features in a
clinicopathological study with long-term follow-up. Br J
Dermatol 2009;160:994-8.
20. Buettiker UV, Yawalkar NY, Braathen LR, Hunger RE. Imiqui-
mod treatment of lentigo maligna: an open-label study of 34
primary lesions in 32 patients. Arch Dermatol 2008;144:
943-5.
21. Spenny ML, Walford J, Werchniak AE, Beltrani V, Brennick JB,
Storm CA, et al. Lentigo maligna (melanoma in situ) treated
with imiquimod cream 5%: 12 case reports. Cutis 2007;79:
149-52.
22. Ly L, Kelly JW, Keefe RO, Sutton T, Dowling JP, Swain S, et al.
Efficacy of imiquimod cream, 5%, for lentigo maligna after
complete excision. Arch Dermatol 2011;147:1191-5.
23. Fleming CJ, Bryden AM, Evans A, Dawe RS, Ibbotson SH. A
pilot study of treatment of lentigo maligna with 5% imiqui-
mod cream. Br J Dermatol 2004;151:485-8.
24. Missall T, Hurley MY, Fosko SW. Lentiginous melanoma in situ
treatment with topical imiquimod: need for individualized
regimens. Arch Dermatol 2010;146:1309-10.
25. Somach SC, Taira JW, Pitha JV, Everett MA. Pigmented lesions
in actinically damaged skin: histopathologic comparison of
biopsy and excisional specimens. Arch Dermatol 1996;132:
1297-302.
26. Rajadhyaksha M, Gonz�alez S, Zavislan JM, Anderson RR, Webb
RH. In vivo confocal scanning laser microscopy of human skin
II: advances in instrumentation and comparison with histol-
ogy. J Invest Dermatol 1999;113:293-303.
27. Rajadhyaksha M, Grossman M, Esterowitz D, Webb RH,
Anderson RR. In vivo confocal scanning laser microscopy of
human skin: melanin provides strong contrast. J Invest
Dermatol 1995;104:946-52.
28. Pellacani G, Guitera P, Longo C, Avramidis M, Seidenari S,
Menzies S. The impact of in vivo reflectance confocal
microscopy for the diagnostic accuracy of melanoma and

J AM ACAD DERMATOL Alarcon et al 7
equivocal melanocytic lesions. J Invest Dermatol 2007;127:
2759-65.
29. Guitera P, Pellacani G, Longo C, Seidenari S, Avramidis M,
Menzies SW. In vivo reflectance confocal microscopy enhances
secondary evaluation of melanocytic lesions. J Invest Dermatol
2009;129:131-8.
30. Wurm EMT, Curchin CES, Lambie D, Longo C, Pellacani G,
Soyer HP. Confocal features of equivocal facial lesions on
severely sun-damaged skin: four case studies with dermato-
scopic, confocal, and histopathologic correlation. J Am Acad
Dermatol 2012;66:463-73.
31. Guitera P, Pellacani G, Crotty KA, Scolyer RA, Li LX, Bassoli S,
et al. The impact of in vivo reflectance confocal microscopy on
the diagnostic accuracy of lentigo maligna and equivocal
pigmented and nonpigmented macules of the face. J Invest
Dermatol 2010;130:2080-91.
32. Clark WH, Elder DE, Van Horn M. The biologic forms of
malignant melanoma. Hum Pathol 1986;17:443-50.
33. McGovern VJ, Mihm MC, Bailly C, Booth JC, Clark WH, Cochran
AJ, et al. The classification of malignant melanoma and its
histologic reporting. Cancer 1973;32:1446-57.
34. Osborne JE, Hutchinson PE. A follow-up study to investigate
the efficacy of initial treatment of lentigo maligna with
surgical excision. Br J Plast Surg 2002;55:611-5.
35. Bosbous MW, Dzwierzynski WW, Neuburg M. Staged
excision of lentigo maligna and lentigo maligna mela-
noma: a 10-year experience. Plast Reconstr Surg 2009;124:
1947-55.
36. Guitera P, Moloney FJ, Menzies SW, Stretch JR, Quinn MJ,
Hong A, et al. Improving management and patient care in
lentigo maligna by mapping with in vivo confocal microscopy.
JAMA Dermatol 2013;149:692-8.
Related Documents











