PEDIATRIC EPIDEMIOLOGY Investigating spatio-temporal similarities in the epidemiology of childhood leukaemia and diabetes Samuel O. M. Manda Richard G. Feltbower Mark S. Gilthorpe Received: 16 March 2009 / Accepted: 16 September 2009 / Published online: 26 September 2009 Ó Springer Science+Business Media B.V. 2009 Abstract Childhood acute lymphoblastic leukaemia (ALL) and Type 1 diabetes (T1D) share some common epidemiological features, including rising incidence rates and links with an infectious aetiology. Previous work has shown a significant positive correlation in incidence between the two conditions both at the international and small-area level. The aim was to extend the methodology by including shared spatial and temporal trends using a more extensive dataset among individuals diagnosed with ALL and T1D in Yorkshire (UK) aged 0–14 years from 1978–2003. Cases with ALL and T1D were ascertained from 2 high quality population-based disease registers covering the Yorkshire region of the UK and linked to an electoral ward from the 1991 UK census. A Bayesian model was fitted where similarities and differences in risk profiles of the two diseases were captured by the shared and disease-specific components using a shared-component model, with space-time interactions. The extended model revealed a positive correlation of at least 0.70 between diseases across all time periods, and an increasing risk across time for both diseases, which was more evident for T1D. Furthermore, both diseases exhibited lower rates in the more urban county of West Yorkshire and higher rates in the more rural northern and eastern part of the region. A differential effect of T1D over ALL was found in the south-eastern part of the region, which had a more pro- nounced association with population mixing than with population density or deprivation. Our approach has dem- onstrated the utility in modelling temporally and spatially varying disease incidence patterns across small geograph- ical areas. The findings suggest searching for environ- mental factors that exhibit similar geographical-temporal variation in prevalence may help in the development and testing of plausible aetiological hypotheses. Furthermore, identifying environmental exposures specific to the south- eastern part of the region, especially locally varying risk factors which may differentially affect the development of T1D and ALL, may also be fruitful. Keywords Leukemia Type 1 diabetes Infection Epidemiology Children Bayesian Hierarchical Temporal-spatial Introduction Childhood acute lymphoblastic leukaemia (ALL) and Type 1 diabetes (T1D) share some common epidemiological features, including rising incidence rates [1–4] and potential links with an infectious aetiology [5, 6]. Previous work has shown a significant positive correlation in incidence between the two conditions both at the international [7] and small-area level [8]. For the latter, we considered a Bayesian hierarchical joint spatial analysis investigating the variation in the occurrence of these diseases across electoral wards in the Yorkshire region in the north of England using data from two co-terminus population-based registers, limited to a S. O. M. Manda (&) Biostatistics Unit, South African Medical Research Council, 1 Soutpansberg Road, Pretoria, South Africa e-mail: [email protected] R. G. Feltbower Paediatric Epidemiology Group, Centre for Epidemiology and Biostatistics, University of Leeds, Worsley Building, Leeds LS2 9NL, UK M. S. Gilthorpe Biostatistics Unit, Centre for Epidemiology and Biostatistics, University of Leeds, Worsley Building, Leeds LS2 9NL, UK 123 Eur J Epidemiol (2009) 24:743–752 DOI 10.1007/s10654-009-9391-2

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
PEDIATRIC EPIDEMIOLOGY
Investigating spatio-temporal similarities in the epidemiologyof childhood leukaemia and diabetes
Samuel O. M. Manda Æ Richard G. Feltbower ÆMark S. Gilthorpe
Received: 16 March 2009 / Accepted: 16 September 2009 / Published online: 26 September 2009
� Springer Science+Business Media B.V. 2009
Abstract Childhood acute lymphoblastic leukaemia
(ALL) and Type 1 diabetes (T1D) share some common
epidemiological features, including rising incidence rates
and links with an infectious aetiology. Previous work has
shown a significant positive correlation in incidence
between the two conditions both at the international and
small-area level. The aim was to extend the methodology
by including shared spatial and temporal trends using a
more extensive dataset among individuals diagnosed with
ALL and T1D in Yorkshire (UK) aged 0–14 years from
1978–2003. Cases with ALL and T1D were ascertained
from 2 high quality population-based disease registers
covering the Yorkshire region of the UK and linked to an
electoral ward from the 1991 UK census. A Bayesian
model was fitted where similarities and differences in risk
profiles of the two diseases were captured by the shared
and disease-specific components using a shared-component
model, with space-time interactions. The extended model
revealed a positive correlation of at least 0.70 between
diseases across all time periods, and an increasing risk
across time for both diseases, which was more evident for
T1D. Furthermore, both diseases exhibited lower rates in
the more urban county of West Yorkshire and higher rates
in the more rural northern and eastern part of the region. A
differential effect of T1D over ALL was found in the
south-eastern part of the region, which had a more pro-
nounced association with population mixing than with
population density or deprivation. Our approach has dem-
onstrated the utility in modelling temporally and spatially
varying disease incidence patterns across small geograph-
ical areas. The findings suggest searching for environ-
mental factors that exhibit similar geographical-temporal
variation in prevalence may help in the development and
testing of plausible aetiological hypotheses. Furthermore,
identifying environmental exposures specific to the south-
eastern part of the region, especially locally varying risk
factors which may differentially affect the development of
T1D and ALL, may also be fruitful.
Keywords Leukemia � Type 1 diabetes � Infection �Epidemiology � Children � Bayesian � Hierarchical �Temporal-spatial
Introduction
Childhood acute lymphoblastic leukaemia (ALL) and Type
1 diabetes (T1D) share some common epidemiological
features, including rising incidence rates [1–4] and potential
links with an infectious aetiology [5, 6]. Previous work has
shown a significant positive correlation in incidence
between the two conditions both at the international [7] and
small-area level [8]. For the latter, we considered a Bayesian
hierarchical joint spatial analysis investigating the variation
in the occurrence of these diseases across electoral wards in
the Yorkshire region in the north of England using data from
two co-terminus population-based registers, limited to a
S. O. M. Manda (&)
Biostatistics Unit, South African Medical Research Council,
1 Soutpansberg Road, Pretoria, South Africa
e-mail: [email protected]
R. G. Feltbower
Paediatric Epidemiology Group, Centre for Epidemiology and
Biostatistics, University of Leeds, Worsley Building,
Leeds LS2 9NL, UK
M. S. Gilthorpe
Biostatistics Unit, Centre for Epidemiology and Biostatistics,
University of Leeds, Worsley Building, Leeds LS2 9NL, UK
123
Eur J Epidemiol (2009) 24:743–752
DOI 10.1007/s10654-009-9391-2

period around the 1991 UK decadal census (1986–1998).
Specifically, we examined the spatial association between
the two conditions by including unstructured and spatially
structured area-level random components, which were
assigned a multivariate normal prior distribution, and we
assessed how the level of the spatial correlation differed
after adjusting for ecological factors previously associated
with disease risk (deprivation, population density and pop-
ulation mixing/migration).
In the current work, we present a novel extension to this
methodology by including a time-varying component to
take account of the change in incidence over time of ALL
and T1D, and we used a more extensive dataset for indi-
viduals diagnosed from 1978–2003. In particular, we aimed
to conduct a joint spatio-temporal analysis of the variation
of risk of childhood (ages 0–14 years) ALL and T1D in
Yorkshire by incorporating this time-varying component
[9]. Rather than using a multivariate normal prior to ana-
lyse the spatial association between the two diseases, we
investigated a shared-component model with temporal
dimensions. This was implemented using a Bayesian
hierarchical model, where we examined space- and time-
effects within an ecological framework to assess the
plausibility for a common aetiology between these two
diseases, thus enabling us to determine the extent of vari-
ation exhibited through shared unobserved environmental
risk factors. The proposed model allowed for both shared
local space and time dependence, in addition to disease-
specific components. This model also enabled us to
investigate persistence of disease patterns over time and
highlight unusual features of the data, both of which are
additional advantages over a purely spatial analysis [9, 10].
The analysis was underpinned by the unique availability of
high quality population-based disease register data on
childhood cancer [11] and diabetes [12] covering the same
period and study region.
Materials and methods
Case data
Information on individuals diagnosed with childhood (ages
0–14 years) ALL and T1D in the former Yorkshire
Regional Health Authority between 1978 and 2003 was
extracted from two co-terminus population-based disease
registers [11, 12]. Both registers accrue data on new
patients from multiple sources of ascertainment. Each
individual’s postcode at diagnosis was linked to an elec-
toral ward (n = 532) in existence at the time of the 1991
census. Both registers have extremely high levels of
completeness, through extensive cross-checks with multi-
ple sources of ascertainment. For example, capture-
recapture methods have shown that the diabetes register is
99.5% complete [12, 13].
We also derived three socio-demographic factors pre-
viously linked to disease onset [8]. These included:
(a) population mixing, reflecting the diversity of origins of
incomers into each Ward and calculated for the childhood
(0–14 years) population; (b) person-based childhood pop-
ulation density, which was calculated as a population
weighted average of the population density (persons per
hectare) for each census enumeration district, which then
was aggregated to electoral ward to provide a person-based
measure of population density; and (c) deprivation, mea-
sured using the Townsend Score, standardized to all Wards
in Yorkshire with the following variables contributing to
the index—unemployment, household overcrowding, car
ownership and housing tenure. Since these values were
fixed near the mid-point of the analysis (1991), they were
excluded from the temporal modeling but examined in
relation to the resulting smoothed spatial effects.
The spatial-temporal model
Our approach is an extension to that described previously
[8] whereby a Bayesian model was modified to include
correlated spatial terms using a multivariate normal struc-
ture. In the present study, similarities and differences in
risk profiles of the two diseases were captured by the
shared and disease-specific components using a shared-
component model, with space-time interactions [9, 10].
We supposed that the region under consideration was
divided into I contiguous sub-regions; in our case, these were
electoral wards for the Yorkshire region. Furthermore, we
assumed that data were collected at T successive discrete-
time periods. Now, let Oit1 and Oit2 represent the observed
number of cases from two diseases in area i at time period t,
which were five periods from 1978 to 2003, with period 1988
to 1993 being 6 years long; the other periods were 5 years
long (1 B t B T = 5; 1 B i B I = 532, in our case). It was
assumed that the observed counts followed Poisson distri-
butions with mean, litj = EitjRitj, where Eitj and Ritj were the
known expected number of cases and the unknown relative
risk, respectively, in area i at period t for disease j (j = 1, 2).
Expected counts were derived from average age-sex specific
incidence rates for the region and the entire period 1978–2003.
The maximum likelihood estimate of the relative risk of
disease j in area i at time-point t is the usual standardised
incidence (morbidity) ratio (SIR) Ritj ¼ Oitj=Eitj. It is
widely acknowledged that these crude risk ratios are mis-
leading, particularly when the diseases are rare or the areas
are small. Thus, more reliable estimates of relative risks for
rare diseases or small areas can be obtained by borrowing
information from neighbouring areas. A commonly used
744 S. O. M. Manda et al.
123
model for spatial smoothing of relative risks is the one
introduced by Besag et al. [14], abbreviated as the BYM
model. The basic BYM model decomposes the log of
disease-specific area-level relative risks into the sum of two
random effects: one that is unstructured (heterogeneous),
the other that is spatially structured (dependent). A char-
acterisation of these components of the BYM models is
detailed in ‘‘Appendix’’, where areas with common border
define neighbourhood in space.
In our previous analysis [8], a Bayesian hierarchical
joint spatial model was used to investigate the variation in
the occurrence of ALL and T1D in Yorkshire. The spatial
effects of the two diseases were assigned a multivariate
normal distribution. For this earlier work, we used the
techniques presented by Langford et al. [15] and Leyland
et al. [16] based on a multiple membership prior within a
multilevel structure, but differed in that our approach was
Bayesian. We have subsequently extended the methodol-
ogy by including time varying components to take into
account both the change in incidence of both diseases and a
more extensive dataset for individuals diagnosed from
1978–2003. Rather than using a multivariate normal prior
to assess spatial correlations, we used a shared-component
model [17, 18], though now extended to include temporal
effects, to determine the extent of the variation exhibited
through shared unobserved environmental risk factors in
space and time. Thus, following Richardson et al. [9], we
proposed a modification of (1) to include both main shared
spatial, temporal and space-time interaction effects, and
disease-specific effects within the framework of the BYM
model. These extensions permitted an investigation into
persistence of disease patterns over time and to highlight
unusual features of the data. These were additional
advantages over a purely spatial analysis [9]. These mod-
ifications are presented in ‘‘Appendix’’.
For a Bayesian model to be properly specified, all
unknown parameters whether fixed or random must be
given prior distributions. Where prior knowledge is avail-
able, this should be reflected in the prior distributions,
otherwise prior ignorance is assumed on the distributions of
parameters. We required priors that combine the BYM
framework to link risk in space at every time period and
time series techniques to link risk in time at every area. For
the purpose of this application, the shared spatial random
effects ui were given a CAR Normal W ; r2u
� �prior dis-
tribution to capture local dependence in space. Similarly,
we assumed that the disease 2 (T1D) specific spatial ran-
dom effects follow a conditional autoregressive normal
prior distribution: hi�CAR Normal W ; r2h
� �.
In order to capture local dependence in time, the shared
temporal trends wt were given a first order random walk
prior, which is simply a one dimensional version of the CAR
Normal prior distribution. Thus wt�CAR Normal D; r2w
� �
where the weight matrix D defines the temporal neighbours
of period t as periods t - 1 and t ? 1 for periods t = 2, 3, 4,
otherwise periods t = 1 and t = 5 have single neighbouring
periods t ? 1 and t - 1, respectively. The same first order
random walk prior was used to define the specific time trend
ct such that ct�CAR Normal D; r2c
� �.
In this analysis, we follow Richardson et al. [9] in fixing
the shared-temporal differential gradient x = 1 to improve
identifiability when using only five time periods for esti-
mating the temporal patterns. For the remaining scaling
parameter, an independent Normal (0, 5) prior distribution
was assigned to its logarithm, log j. All precision param-
eters were assigned independent hyper-prior Gamma (0.5,
0.0005) distributions. The inverse of covariance matrix
R-1 was assigned a Wishart (Q, 2) prior distribution, where
the scale parameter Q was assigned informative values as
described previously [8]. A complete specification of the
priors is in ‘‘Appendix’’.
Presently, we are unable to include period-specific data
on the three factors, population mixing; population density
and deprivation, as they are not available. In our pre-
liminary analyses when we included 1988–1993 data for
the other periods, the effects of the three contextual factors
were exceedingly high during the period, which we sus-
pected arose as an artefact of the data since these were
measured around the period 1991.
We fitted four variations of the joint spatio-temporal
model (3). The first two included only temporal trends
(Model A) or spatial trends (Model B) separately, thereby
demonstrating the impact of considering trends but only in
one dimension. We then included space-time interaction
terms (Model C), thereby demonstrating the impact of
considering trends in both dimensions. Model D was an
extension to Model C where heterogeneity terms were
added. Models C and D thus provided much greater flexi-
bility to identify salient patterns inherent in the data [9]. All
models were fitted to the data using full Bayesian estima-
tion within the WinBUGS software [19]. For each of the
four models, three independent chains were run for 40,000
iterations, and convergence was assessed by examining
trace plots as well as Brooks-Gelman Rubin diagnostics. A
burn-in period of 20,000 iterations was more than ade-
quate. The results reported were based on the remaining
20,000 posterior samples, keeping every 10th in order to
reduce serial correlation among samples of variance chains.
The performance of the four models was assessed using
the Deviance Information Criterion (DIC) [20], defined as
DIC ¼ Dþ pD where D is the posterior mean of the
deviance and measures model fit; pD is the effective
number of model parameters and measures model com-
plexity. The DIC works on similar principles as the non-
Investigating spatio-temporal similarities in the epidemiology 745
123

Bayesian Akaike Information Criterion (AIC), where the
model with a smaller DIC provides better support to the
data.
Results
Data summary
In total, 587 and 3195 individuals with ALL and T1D,
respectively, were included in the analysis. The number of
subjects diagnosed by 5-years time periods are shown in
Table 1. The number of cases aggregated across each
period for ALL (range 103–141) was much lower than T1D
(range 490–825). The proportion of wards containing zero
cases within each period for ALL and T1D ranged from 77
to 84 and 38 to 51%, respectively. The distribution of
unsmoothed SIR by ward (maps not shown but available on
request) showed a large number of areas with zero cases
and large standardised incidence ratios, indicating that the
observed data were sparse. The noise in the data was also
evident from time series plots of raw SIR for each disease
in five randomly selected wards (plots not shown but
available on request). This illustrated the need to generate
and model smoothed estimates of disease risk in order to
extract important features from the data.
Model selection
A comparison of the fitted models is presented in Table 2,
showing the different terms which comprised the DIC
criteria. The temporal trend model (A) had the largest
expected deviance, indicating a poorer overall fit compared
to the other three models. It also had the greatest com-
plexity according to the DIC. These criteria point to an
additional risk structure for both diseases beyond such a
simple model only capturing temporal effects. Model D,
which included both space-time interaction and heteroge-
neity terms, had the best overall model fit, although the
highest effective number of parameters resulting in a
slightly larger DIC.
In terms of the DIC values, models B, C and D were
equally valid, although with parsimony in mind; models B
and C were preferred. Model C was chosen as the final
model, since a model encapsulating space-time effects
permitted greater flexibility to study the persistence of
disease patterns over time and highlight unusual features of
the data: the results presented below were derived from this
model.
Posterior risk estimates
Rather than using maps showing posterior means of
smoothed SIR, we present maps showing the posterior
probability that the area-specific smoothed SIR exceeds 1.
The upper cut-point of the probability is set at 0.8, which
has a high specificity (95%) and reasonable sensitivity to
pick out areas whose true RR is around 2 [9]. Ranta and
Penttinen [21] also point out that a map of posterior mean
RRs show point estimates and certain high values may
simply correspond to long tails of marginal distributions.
Basing inferences on probability maps is more reliable.
Furthermore, a cut point of 0.8 is less subjective in iden-
tifying electoral wards with high risk.
Maps showing the posterior probability that the electoral
ward smoothed SIR for each diseases exceeds 1 in each are
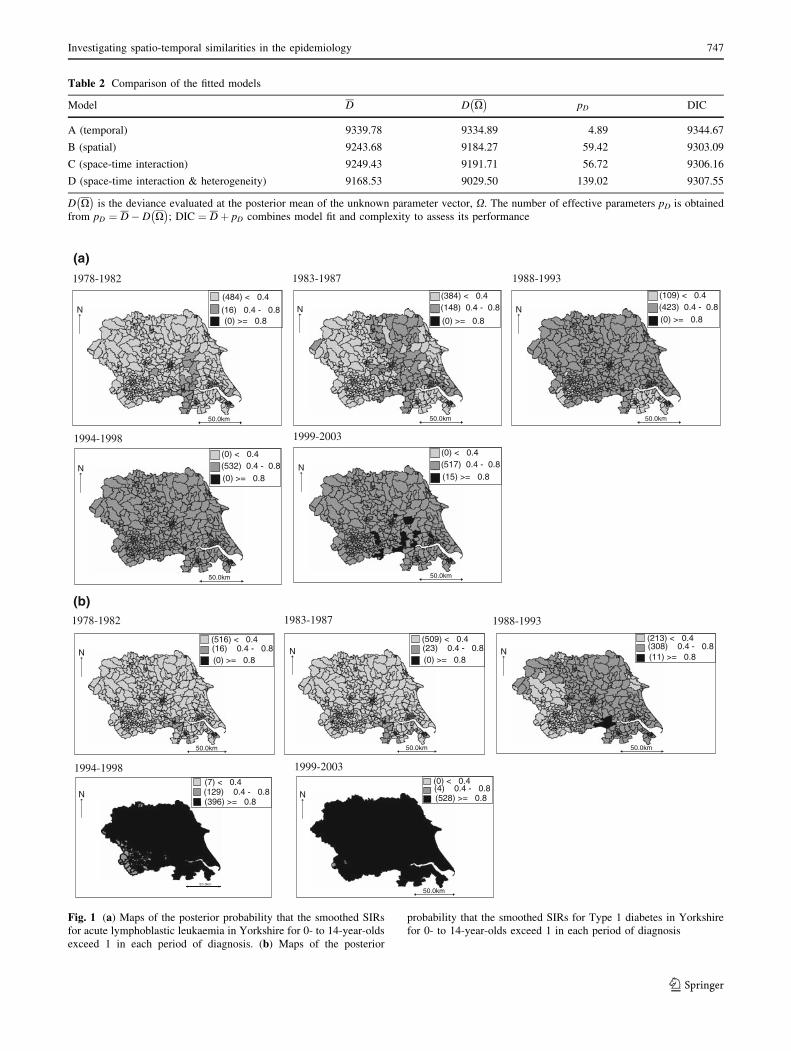
presented in Fig. 1a and b. Both diseases exhibited steady
rising incidence rates over the study period with a more
pronounced rise for T1D, reflected by the increasing
number of wards with high posterior probability that their
smoothed SIR exceeds 1. Rising incidence rates of both
diseases is demonstrated more clearly by time series plots
of raw and smoothed SIRs (Fig. 2).
Furthermore, it is evident that both diseases show pos-
terior probabilities that are consistently higher in the more
rural northern and eastern parts of the region with lower
probabilities observed in the more urban county of West
Yorkshire (south west corner of Yorkshire). The distribu-
tion of the probabilities shown in Fig. 1a and b is rein-
forced by the examination of the spatial patterns of the
posterior probabilities of the shared and differential com-
ponents of risk between diseases in Fig. 3. The shared
component probability map (Fig. 3a) shows lower proba-
bilities around the urban areas of West Yorkshire and
higher probabilities in the more rural county of North
Yorkshire. The ratio or relative weight, of the shared spa-
tial component for ALL to T1D was estimated with a
median of 0.74 (95% CI, 0.22–3.60). This shows that the
shared spatial component was less important for ALL than
for T1D, though the ratio was not statistically different
from 1.
A similar pattern to that of the shared component was
observed when we mapped the probabilities for the dif-
ferential effect of T1D over ALL, but with higher
Table 1 Number of patients diagnosed by time period and disease
group
Time period Acute lymphoblastic
leukaemia
Type 1
diabetes
1978–1982 103 492
1983–1987 106 490
1988–1993 141 685
1994–1998 116 703
1999–2003 121 826
1978–2003 587 3196
746 S. O. M. Manda et al.
123
50.0km 50.0km
(0) >= 0.8
(384) < 0.4(148) 0.4 - 0.8
(0) >= 0.8
(484) < 0.4
50.0km
50.0km
(109) < 0.4(423) 0.4 - 0.8(0) >= 0.8
(0) < 0.4(532) 0.4 - 0.8(0) >= 0.8
50.0km
(0) < 0.4(517) 0.4 - 0.8(15) >= 0.8
1978-1982 1983-1987 1988-1993
1994-1998 1999-2003
50.0km 50.0km
(16) 0.4 - 0.8(0) >= 0.8
(516) < 0.4(23) 0.4 - 0.8(0) >= 0.8
(509) < 0.4
1978-1982 1983-1987
50.0km
(308) 0.4 - 0.8(11) >= 0.8
(213) < 0.4
(129) 0.4 - 0.8(396) >= 0.8
(7) < 0.4
50.0km
N(4) 0.4 - 0.8(528) >= 0.8
(0) < 0.4
1988-1993
1999-2003
(a)
(b)
(16) 0.4 - 0.8
50.0km
N
N
NN N
N
N N
N
1994-1998
Fig. 1 (a) Maps of the posterior probability that the smoothed SIRs
for acute lymphoblastic leukaemia in Yorkshire for 0- to 14-year-olds
exceed 1 in each period of diagnosis. (b) Maps of the posterior
probability that the smoothed SIRs for Type 1 diabetes in Yorkshire
for 0- to 14-year-olds exceed 1 in each period of diagnosis
Table 2 Comparison of the fitted models
Model D D X� �
pD DIC
A (temporal) 9339.78 9334.89 4.89 9344.67
B (spatial) 9243.68 9184.27 59.42 9303.09
C (space-time interaction) 9249.43 9191.71 56.72 9306.16
D (space-time interaction & heterogeneity) 9168.53 9029.50 139.02 9307.55
D X� �
is the deviance evaluated at the posterior mean of the unknown parameter vector, X. The number of effective parameters pD is obtained
from pD ¼ D� D X� �
; DIC ¼ Dþ pD combines model fit and complexity to assess its performance
Investigating spatio-temporal similarities in the epidemiology 747
123

probabilities present around the south-eastern part of the
region below the Humber estuary (Fig. 3b). The posterior
probability associated with the overall spatial distribution
of diabetes (Fig. 3c) shows that wards in the more urban
county of West Yorkshire had lower probabilities than in
the other parts of the region, while higher probabilities
were observed in the more rural eastern parts of the
region.
Inspection of the geographical variation in levels of risk
associated with each of the three contextual factors
(deprivation, population density and population mixing)
using Model C showed that lower rates of both childhood
ALL and T1D were present in areas with high deprivation,
population density and mixing. The same inverse associa-
tion was observed between the three contextual factors and
the shared and differential components.
We formally quantified the observed inverse relation-
ships between each of the three contextual variables and
shared and differential components by deriving correla-
tions using posterior samples of the smoothed SIRs. We
also quantified the correlations between the smoothed RRs
of the two diseases for each time period using the posterior
samples (Table 3), whereas previously we explicitly
included parameters to quantify the correlation between the
two diseases for the entire study period as a whole [8].
There was a significant positive correlation (0.74, 0.74,
0.74, 0.73 and 0.74, respectively, in periods 1–5) between
the two diseases, indicating that they may share common
environmental risk factors.
The shared component was significantly inversely
associated with population mixing, population density and
0.4
0.6
0.8
1
1.2
1.4
1.6
1978
-198
2
1983
-198
7
1988
-199
3
1994
-199
8
1999
-200
3
Period
SIR
Raw_T1D_SIR
Smoothed_T1D_SIR
Raw_ALL_SIR
Smoothed_ALL_SIR
Fig. 2 Plots of raw and smoothed Yorkshire-wide average temporal
SIRs for both diseases
50.0km
N(121) < 0.4
(411) 0.4 - 0.8(0) >= 0.8
50.0km
N
50.0km
N
(183) < 0.4
(341) 0.4 - 0.8
(8) >= 0.8
(158) < 0.4
(339) 0.4 - 0.8(35) >= 0.8
(a) (b)
(c)
Fig. 3 (a) Map of the posterior probability that the shared spatial
component smoothed SIR in Yorkshire for 0- to 14-year-olds, 1978–
2003, exceeds 1. (b) Map of the posterior probability that the spatial
smoothed SIR for Type 1 diabetes differential over lymphoblastic
leukaemia in Yorkshire for 0- to 14-year-olds, 1978–2003, exceeds 1.
(c) Map of the posterior probability that the overall smoothed SIR for
Type 1 diabetes in Yorkshire for 0- to 14-year olds, 1978–2003
748 S. O. M. Manda et al.
123
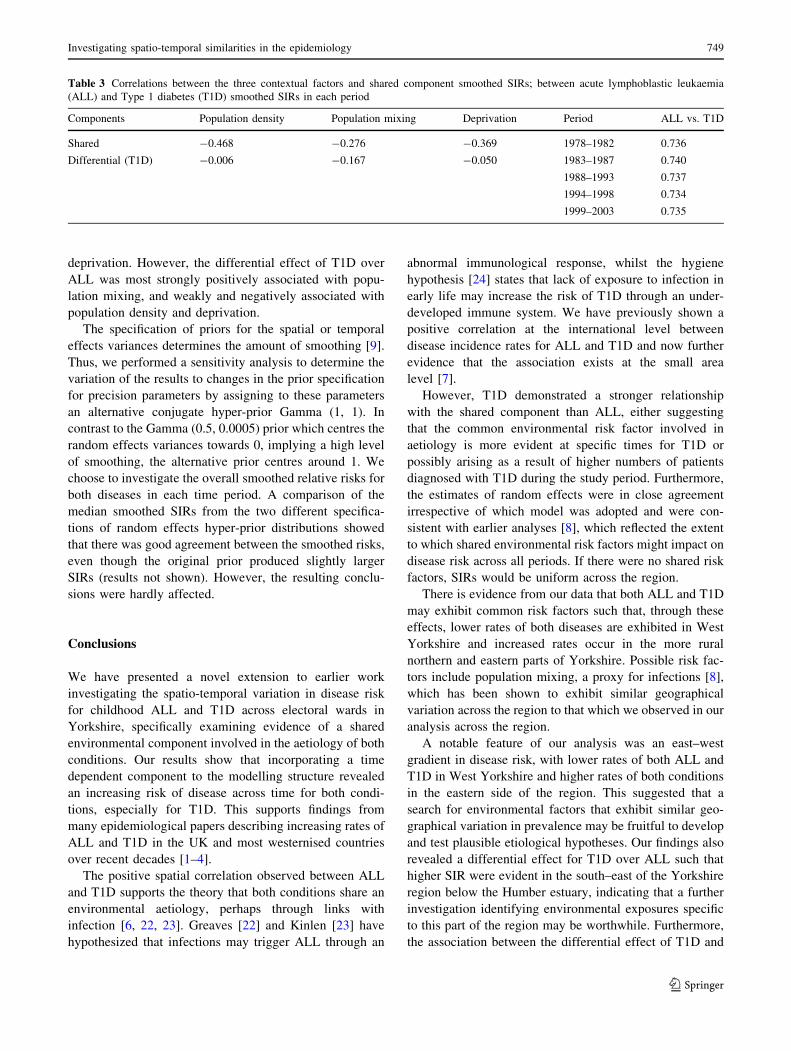
deprivation. However, the differential effect of T1D over
ALL was most strongly positively associated with popu-
lation mixing, and weakly and negatively associated with
population density and deprivation.
The specification of priors for the spatial or temporal
effects variances determines the amount of smoothing [9].
Thus, we performed a sensitivity analysis to determine the
variation of the results to changes in the prior specification
for precision parameters by assigning to these parameters
an alternative conjugate hyper-prior Gamma (1, 1). In
contrast to the Gamma (0.5, 0.0005) prior which centres the
random effects variances towards 0, implying a high level
of smoothing, the alternative prior centres around 1. We
choose to investigate the overall smoothed relative risks for
both diseases in each time period. A comparison of the
median smoothed SIRs from the two different specifica-
tions of random effects hyper-prior distributions showed
that there was good agreement between the smoothed risks,
even though the original prior produced slightly larger
SIRs (results not shown). However, the resulting conclu-
sions were hardly affected.
Conclusions
We have presented a novel extension to earlier work
investigating the spatio-temporal variation in disease risk
for childhood ALL and T1D across electoral wards in
Yorkshire, specifically examining evidence of a shared
environmental component involved in the aetiology of both
conditions. Our results show that incorporating a time
dependent component to the modelling structure revealed
an increasing risk of disease across time for both condi-
tions, especially for T1D. This supports findings from
many epidemiological papers describing increasing rates of
ALL and T1D in the UK and most westernised countries
over recent decades [1–4].
The positive spatial correlation observed between ALL
and T1D supports the theory that both conditions share an
environmental aetiology, perhaps through links with
infection [6, 22, 23]. Greaves [22] and Kinlen [23] have
hypothesized that infections may trigger ALL through an
abnormal immunological response, whilst the hygiene
hypothesis [24] states that lack of exposure to infection in
early life may increase the risk of T1D through an under-
developed immune system. We have previously shown a
positive correlation at the international level between
disease incidence rates for ALL and T1D and now further
evidence that the association exists at the small area
level [7].
However, T1D demonstrated a stronger relationship
with the shared component than ALL, either suggesting
that the common environmental risk factor involved in
aetiology is more evident at specific times for T1D or
possibly arising as a result of higher numbers of patients
diagnosed with T1D during the study period. Furthermore,
the estimates of random effects were in close agreement
irrespective of which model was adopted and were con-
sistent with earlier analyses [8], which reflected the extent
to which shared environmental risk factors might impact on
disease risk across all periods. If there were no shared risk
factors, SIRs would be uniform across the region.
There is evidence from our data that both ALL and T1D
may exhibit common risk factors such that, through these
effects, lower rates of both diseases are exhibited in West
Yorkshire and increased rates occur in the more rural
northern and eastern parts of Yorkshire. Possible risk fac-
tors include population mixing, a proxy for infections [8],
which has been shown to exhibit similar geographical
variation across the region to that which we observed in our
analysis across the region.
A notable feature of our analysis was an east–west
gradient in disease risk, with lower rates of both ALL and
T1D in West Yorkshire and higher rates of both conditions
in the eastern side of the region. This suggested that a
search for environmental factors that exhibit similar geo-
graphical variation in prevalence may be fruitful to develop
and test plausible etiological hypotheses. Our findings also
revealed a differential effect for T1D over ALL such that
higher SIR were evident in the south–east of the Yorkshire
region below the Humber estuary, indicating that a further
investigation identifying environmental exposures specific
to this part of the region may be worthwhile. Furthermore,
the association between the differential effect of T1D and
Table 3 Correlations between the three contextual factors and shared component smoothed SIRs; between acute lymphoblastic leukaemia
(ALL) and Type 1 diabetes (T1D) smoothed SIRs in each period
Components Population density Population mixing Deprivation Period ALL vs. T1D
Shared -0.468 -0.276 -0.369 1978–1982 0.736
Differential (T1D) -0.006 -0.167 -0.050 1983–1987 0.740
1988–1993 0.737
1994–1998 0.734
1999–2003 0.735
Investigating spatio-temporal similarities in the epidemiology 749
123

population mixing was more pronounced than population
density or deprivation, suggesting that other risk factors
may exist within the south-eastern parts of the region
which differentially affect the development of diabetes and
ALL.
We found a much greater positive correlation between
the diseases than in [8]. This may be partly due to sup-
pression such that when incorporating temporal smoothing,
we have ‘explained’ some of the ‘noise’ in the association,
resulting in stronger residual associations than before. It
may also be due to the modelling of the correlation struc-
tures. Previously, we had explicitly modelled these in a
multivariate normal model which needed prior elicitation
for possible values. It is well known that these priors are
problematic to elicit and specify. On the other hand, we
have now empirically computed the associations using the
posterior samples of the smoothed relative risks.
Future work is planned using latent variable analysis
(LVA) [25] to model unobserved exposures such as
infections, using measured covariates such as population
mixing, density and deprivation. Structural equation mod-
elling, which encompasses LVA, can then be applied to test
etiological hypotheses whilst adjusting appropriately for
confounders and explanatory factors [25]. This approach
would be particularly useful in dealing with the correlation
between population density, deprivation and migration,
factors previously linked to both ALL and T1D.
A further extension of the work is planned by including
potential risk factors such as deprivation, population den-
sity and population migration in the model for each period.
This will enable us to use time-varying fixed effects and
determine the amount of spatial and temporal variation
present after accounting for known and measured spatial
and temporal risk factors.
Acknowledgments We thank the Office for National Statistics for
the provision of population data and special migration statistics. We
are grateful to Margaret Buchan, Carolyn Stephenson, and Sheila
Jones for data collection and the co-operation of all pediatricians,
pediatric oncologists, physicians, Diabetes Specialist Nurses and
General Practitioners in Yorkshire. We thank the Candlelighters Trust
and Leeds Teaching Hospitals NHS Trust for supporting the costs of
running the cancer and diabetes registers. This diabetes registry work
was also undertaken by the University of Leeds who received funding
from the Department of Health. The views expressed in the publi-
cation are those of the authors and not necessarily those of the
Department of Health.
Appendix
The two diseases spatial temporal model
In the presence of longitudinal data for two diseases, an
extension of the BYM model is given by:
logðRit1Þ ¼ a0t1 þ bTt1xit þ uit1 þ vit1
logðRit2Þ ¼ a0t2 þ bT 0
t2 xit þ uit2 þ vit2
ð1Þ
where a0tj is an intercept term on the log relative risk scale
for disease j at time t; xit is a covariate risk vector with the
corresponding disease-specific coefficient parameter vector
btj at time t; and uitj and vitj represent unstructured and
spatially structured random effects, respectively, in area i at
time t for disease j. The unstructured random effects are
assumed to follow a normal distribution with time varying
variance such that uitj�N 0; r2tj
� �for j = 1, 2. The
spatially structured effects are modelled by the intrinsic
conditional autoregressive normal (CAR Normal) prior
[14, 26], which specifies a conditional distribution for a
specific spatially structured effect vitj as:
f ðvitjjvktj; k 6¼ iÞ ¼ N
Pk2Hi
WiktjvktjPk2Hi
Wiktj;
k2tjP
k2HiWiktj
!ð2Þ
at time t for disease j, where Hi is the set of areas adjacent
to area i; Wiktj is the weight reflecting spatial dependence
between area i and k at time t for disease j and k2tj is the
(conditional) structured variance. For simplicity, we
assume that the weighting factor Wiktj is constant over
time and disease, which seems reasonable as we do not
expect the influence of neighbouring areas to change over
time and to be different between the two diseases,
i.e. Wiktj = Wik. The most common and simplest
adjacent specification is to set Wik = 1 if areas i and k
are neighbours that share a common boundary and Wik = 0
otherwise. Thus, for disease j at time t, a CAR Normal
prior specifies the conditional distribution of each area-
specific effect vitj, given all the other v’s, to be a normal
distribution with mean equal to the average of the v’s of its
neighbours, and variance inversely proportional to the
number of neighbours; the more neighbours an area has,
the greater the precision for that area effect. This scenario
is reasonable for population density, as urban areas are
likely to have more neighbours that sparsely populated
rural areas. For brevity, following [14, 26], a conditional
autoregressive normal prior on the spatially structured
effects will be denoted by
vitj�CAR Normal W ; k2tj
� �
where W is simply the neighbourhood adjacency weight
matrix.
A common and specific spatial-temporal model
The spatio-temporal model we consider to estimate relative
risks of the two diseases in space and time is
750 S. O. M. Manda et al.
123

logðRit1Þ ¼ a01 þ bTt1xit þ /ijþ wtxþ fit þ eit1
logðRit2Þ ¼ a02 þ bTt2xit þ
/i
jþ wt
xþ fit þ hi þ ct þ eit2
ð3Þ
where now a0j is the overall risk for disease j (j = 1, 2),
ui and wt are the main shared spatial and temporal
effects, respectively; hi and ct represent disease 2 (T1D)
specific spatial and temporal components, which capture
the differential effect between the two diseases; fit are
the shared space-time interaction effects, capturing
departure from space and time main effects, which may
highlight space-time clusters of risk, and eitj are the
disease-specific heterogeneous effects, capturing possible
extra-Poisson variation not explained by terms included
above. Thus, the shared-temporal factor model (3) par-
titions the risk profile for the two diseases into disease-
specific components and shared spatial and time com-
ponents. Parameters j and x are included to allow for a
differential gradient on the main shared spatial and
temporal components, respectively. The ratio j2 com-
pares the risk of disease 1 (ALL) to the risk of disease 2
(T1D) associated with the main shared spatial component
and the ratio x2 compares the risk associated with the
main temporal effect.
Ideally, in model (3) we could have split the main shared
spatial components into unstructured and structured effects
or the main shared temporal component into unstructured
and structured time trends or similarly the diseases-specific
components. This could have resulted into 8 9 5 = 40
extra random effects, as well as the space-time interaction
terms. This seems overly complex and could lead to
identifiability problems, so we decided to minimise the
number of random effects. We could have also included
specific components for disease 1, but such a symmetric
formulation can result in identifiability problems [9].
Prior specification
There are various choices of prior distributions for the
space-time interaction effects, fit. They can simply be
taken to be independent for every period and time with a
constant variance over time, as in [9], or, depending on the
length of the time periods, can evolve smoothly over time
with a polynomial temporal trend as in [27, 28]. Alterna-
tively, they can be allowed to vary independently or be
spatially structured for every period, with variances that are
either independently and identically distributed or tempo-
rally structured as proposed in Nobre et al. [10]. In the
present study, we define only five periods, too few to show
any reliable space-time jumps in risk. Thus, we assume a
spatially structured prior distribution at every period for the
shared interaction term, fit �CAR Normal W ; r2ft
� �(i.e. a
time-independent prior but linked in space) with variances
that are allowed to change smoothly over time,log r21t ¼
log r21ðt�1Þ þ et, where et �N 0;r2
e
� �. The pair of disease-
specific heterogeneity terms ðeit1; eit2ÞT are also assumed to
evolve smoothly over time according to a first-order
autoregressive (AR(1)) multivariate normal prior distribu-
tion with covariance matrix R to allow for correlations
between the ALL and T1D risks in each space-time unit.
Thus, ðei11; ei12ÞT �MVNð0;RÞ and ðeit1; eit2ÞT �MVN
ðeiðt�1Þ1; eiðt�1Þ2Þ;R� �
; t ¼ 2; . . .; 5. Since we are using the
CAR Normal prior, with sum-to-zero constraints on the
random effect terms, we assign a flat prior on the overall
disease risk terms, a0j.
References
1. Draper GJ, Kroll ME, Stiller CA. Childhood cancer. In: Doll R,
Fraumeni JF, Muir CS, editors. Cancer surveys vol 19/20: trends
in cancer incidence and mortality. New York: Cold Spring Har-
bor Laboratory; 1994. p. 493–517.
2. Linet MS, Ries LA, Smith MA, Tarone RE, Devesa SS. Cancer
surveillance series: recent trends in childhood cancer incidence
and mortality in the United States. J Natl Cancer Inst. 1999;91:
1051–8.
3. Onkamo P, Vaananen S, Karvonen M, Tuomilehto J. Worldwide
increase in incidence of type I diabetes—the analysis of the data
on published incidence trends. Diabetologia. 1999;42:1395–403.
4. Green A, Patterson CC. Trends in the incidence of childhood-onset
diabetes in Europe 1989–1998. Diabetologia. 2001;44(Suppl 3):
B3–8.
5. Greaves M. Childhood leukemia. BMJ. 2002;324:283–7.
6. EURODIAB Substudy 2 Study Group. Infections and vaccinations
as risk factors for childhood type 1 (insulin dependent) diabetes
mellitus: a multi-centre case-control investigation. Diabetologia.
2000;43:47–53.
7. Feltbower RG, McKinney PA, Greaves MF, Parslow RC,
Bodansky HJ. International parallels in leukaemia and diabetes
epidemiology. Arch Dis Child. 2004;89:54–6.
8. Feltbower RG, Manda SOM, Gilthorpe MS, Greaves MF, Par-
slow RC, Kinsey SE, et al. Detecting small-area similarities in the
epidemiology of childhood acute lymphoblastic leukemia and
diabetes mellitus, Type 1: a Bayesian approach. Am J Epidemiol.
2005;161:1168–80.
9. Richardson S, Abellan JJ, Best N. Bayesian spatio-temporal
analysis of joint patterns of male and female lung cancer risks in
Yorkshire (UK). Stat Methods Med Res. 2006;15:385–407.
10. Nobre AA, Schmidt AM, Lopes HF. Spatio-temporal models for
mapping the incidence of malaria in Para. Environmetrics. 2005;16:
291–304.
11. McKinney PA, Parslow RC, Lane SA, et al. Epidemiology of
childhood brain tumors in Yorkshire, UK 1974–1995: changing
patterns of occurrence. Br J Cancer. 1998;78:974–9.
12. Feltbower RG, McKinney PA, Parslow RC, Stephenson CR,
Bodansky HJ. Type 1 diabetes in Yorkshire, UK: time trends in
0–14 and 15–29 year olds, age at onset and age-period-cohort
modeling. Diabetic Med. 2003;20:437–41.
13. Feltbower RG, McNally RJ, Kinsey SE, Lewis IJ, Picton SV,
Proctor SJ, et al. Epidemiology of leukaemia and lymphoma in
Investigating spatio-temporal similarities in the epidemiology 751
123

children and young adults from the north of England, 1990–2002.
Eur J Cancer. 2009;45:420–7.
14. Besag J, York J, Mollie A. Bayesian image restoration, with two
applications in spatial statistics. Ann Inst Statist Math. 1991;43:
1–59.
15. Leyland AH, Langford IH, Rabash J, Goldstein H. Multivariate
spatial models for event data. Stat Med. 2000;19:2469–78.
16. Langford IH, Leyland AH, Rasbash J, Goldstein H. Multilevel
modeling of the geographical distributions of diseases. J R Stat
Soc C. 1999;48:253–68.
17. Knorr-Held L, Best NG. A shared component model for detecting
joint and selective clustering of two diseases. J R Stat Soc A. 2001;
164:73–85.
18. Held L, Natario I, Fenton SE, Rue H, Becker N. Towards joint
disease mapping. Stat Methods Med Res. 2006;14:61–82.
19. Spiegelhalter D, Thomas A, Best N, Lunn D. BUGS: Bayesian
inference using Gibbs sampling, version 1.4. Cambridge: MRC
Biostatistics Unit; 2003.
20. Spiegelhalter DJ, Best NG, Carlin BP, van der Linde A. Bayesian
measures of model complexity and fit (with discussion). J R Stat
Soc B. 2002;64:583–640.
21. Ranta J, Penttinen A. Probabilistic small area risk assessment
using GIS-based data: a case study of Finnish childhood diabetes.
Stat Med. 2000;19:2345–59.
22. Greaves M. Etiology of acute leukemia. Lancet. 1997;349:344–9.
23. Kinlen L. Evidence for an infective cause of childhood leukemia:
comparison of a Scottish new town with nuclear reprocessing
sites in Britain. Lancet. 1988;2:1323–7.
24. Wills-Karp M, Santeliz J, Karp CL. The germless theory of allergic
disease: revisiting the hygiene hypothesis. Nat Rev Immunol.
2001;1:69–75.
25. Kline RB. Principles of structural equation modelling. LEA;
2005.
26. Mollie A. Bayesian mapping of disease. In: Gilks WR, Rich-
ardson S, Spiegelhater DJ, editors. Markov chain Monte Carlo in
practice. London: Chapman & Hall; 1996. p. 359–79.
27. Waller LA, Carlin BP, Xia H, Gelfand AE. Hierachical spatio-
temporal mapping of disease rates. J Am Stat Assoc. 1997;92:
607–17.
28. Gill P. Spatio-temporal modelling and mapping of teenage birth rates.
[Online], available: http://people.ok.ubc.ca/gillpara/research/Poster.
pdf. Accessed 13 Dec 2006.
752 S. O. M. Manda et al.
123
Related Documents