Infection with M. tuberculosis and atopy in children Charles C. Obihara

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Infection withM. tuberculosis and
atopy in children
Charles C. Obihara

Infection with M. tuberculosis and atopy in children

Infection withM. tuberculosis and
atopy in children
Infectie met M. tuberculosis en atopie in kinderen(met een samenvatting in het Nederlands)
Proefschrift
Ter verkrijging van de graad van doctor aan de Universiteit Utrecht op gezag van de Rector MagniÞ cus, Prof. Dr. W.H. Gispen, ingevolge het besluit van het College voor Promoties in het openbaar te verdedigen op dinsdag 7 maart 2006 des middags te 2.30 uur
door Charles Obiharageboren 12 februari 1965 te Owerri, Nigeria

Promotor: Prof. Dr. J.L.L. KimpenCo-promotor: Prof. Dr. N. Beyers
The research described in this thesis was Þ nancially supported by the Wilhelmina Children�s Hospital Research Funds and the Stellenbosch University (through funding from the South African Department of Trade and Industry, THRIP fund). The researcher is a recipient of a grant from the Ter Meulen Fund, Royal Netherlands Academy of Arts and Sciences.

� Als je reist maak je steeds nieuwe vriendenEn hoef je niet steeds dag in dag uitMet ze op te trekken.Wanneer je steeds dezelfde mensen zietGaan die tenslotte deel uitmakenVan je eigen leven.En omdat ze deel uitmaken van je levenWillen ze dat ook bijsturen.Als je niet wordt zoals zij willen dat je wordtZijn ze boosWant iedereen kan je precies vertellen hoe je moet levenTerwijl ze zich geen raad weten van hun eigen leven�.
De alchemist
voor D


vii
Contents
Foreword ix
Chapter 1 General introduction 1Chapter 2 The clinical epidemiology of childhood pulmonary tuberculosis:
a critical review of literature from pre-chemotherapy era 23 Int J Tuberc Lung Dis 2004; 8:278-285Chapter 3 The prevalence of symptoms associated with pulmonary tuberculosis
in randomly selected children from a high burden community 39 Arch Dis Child 2005; 90:1166-1170Chapter 4 Does mycobacterial infection prevent the development of atopy
in childhood? A systematic review 49 Submitted
Chapter 5 Mycobacterium tuberculosis infection may protect against allergy in a tuberculosis endemic area 63
Clin Exp Allergy; 2006; 36:70-76Chapter 6 Inverse association between Mycobacterium tuberculosis infection
and atopic rhinitis in children 77 Allergy 2005; 9:1121-1125. Chapter 7 Respiratory atopic disease, Ascaris-IgE and tuberculin test
in urban South African children 87 Clin Exp Allergy; 2006; in pressChapter 8 The association of prolonged breastfeeding and allergic disease
in poor urban children 103 Eur Respir J 2005; 25:970-977 Chapter 9 General discussion 117
Summary / Samenvatting 127Acknowledgements / DankwoordCurriculum VitaeList of publications

ix
Foreword
In the past 3 years, I have frequently been asked why I chose to do my PhD research in South Africa.
It is difÞ cult to give precisely the moment when the seed of this PhD was sown. It was a combination of factors which led to it. Among these are my personal curiosity for new challenges, the urge to make some relevant scientiÞ c contribution in a developing country and the determination to avoid the boredom of routine and a midlife crisis.
That the topic of research involved two diseases, of which one causes a substantial health burden, especially in children living in industrialized countries, while the other, one of the major causes of death in children in less industrialized countries, was not a coinci-dence. This choice reß ects my unique position in the two different worlds and the chal-lenge I feel to make a valuable contribution to both. In one of these worlds, my adopted one in which I live, both the healthcare and education systems are well and functioning, and in the other world, in which I have my roots, the health care and education systems are sick and in shambles. Therefore, the challenge is, at least for me, to link these different worlds positively.
This thesis would not have materialized without the broad-mindedness of Professor Jan Kimpen, my promotor. From the moment I approached Jan towards the end of the 4th year of my pediatric training, with my wish to do research on a topic which not only would address a relevant health problem in the Netherlands, but which would also contribute to scientiÞ c research in a developing country, he involved himself actively to make me realize these objectives. Jan�s enthusiasm was clear right from the start.
There was however one element of coincidence: the fact that Jan met Professor Nulda Beyers, my co-promoter, a few months previously and they had agreed to cooperate on re-search projects. It did not take long for Nulda to accommodate our study proposal.
A lion�s share of the decision making rested on my family and me. After the gentleman�s agreement to cooperate on the project, to me was left the difÞ cult task of convincing my wife to abandon her job and family, and my children to leave their friends, secure and har-monious life behind, for a country unknown to us. For a country whose many social prob-lems have frequently been imported into our homes through the mass media.
As would be expected, the intention to carry out my PhD research in South Africa turned out to be the easiest part of the whole bargain. The proposal still had to be writ-ten and funding realized. This all took place between July and October 2001, in the Þ nal year of pediatric training. In October 2001, the Ter Meulen Funds (TMF), the Netherlands awarded me a research-grant for personal subsistence and that of my family. The two de-partments involved agreed to Þ nance the research-project. I left the Netherlands for Cape Town, South Africa in March 2002; my family joined me 3 months later. The Þ eldwork of this study was conducted between July 2002 and December 2003.
x
Infection with M. tuberculosis and atopy in children
Being that all my medical study took place in Europe (Italy and The Netherlands), I per-ceived in this project a unique opportunity to broaden my knowledge of tuberculosis, and other tropical (the so called �exotic�) diseases. I also saw in it an opportunity to contribute to the search for the cause(s) of increasing global incidence of allergic diseases, such as asth-ma and hay fever, in the past three decades or more, especially in industrialized countries.
In addition, the research would offer an extra �spin-off� effect: an opportunity for a tem-porary �brain-impute� for South Africa, the opposite of the �brain-drain� (a phenomenon which started since the dismantling of apartheid, in which qualiÞ ed young professionals, including doctors migrate with their expertise to a foreign country, usually an industrial-ized one).
Although the choice for the Western Cape was purely coincidental, it created the chance to make contributions on yet another dimension. In The Netherlands, I was used to being the only black face during conferences and other (medical) meetings with colleagues. This was surprisingly not different from the experience in South Africa, particularly in Cape Town. I know that this situation will change in the future.
Despite the fact that I may not have played a much active role in this respect, I however, take the liberty to believe that the door will open easier for black doctors who embark on projects with my South African supervisors and colleagues who worked with me in the past 3 years. I believe that both the success of this cooperation and the successful completion of my project have helped to uproot some weed of prejudice and historical uneasiness on different levels.
South Africa took us off the feet, right from the start. This was not only due to the natu-ral beauty of the country for which tourists ß ock or the incredible hospitality of my new hosts, but also the wide social and racial divide, with the mixture of Þ rst (in the predomi-nantly white neighborhoods) and third (in the predominantly black or coloured neighbor-hoods) world parts.
The immense social problems of the country also contribute to a vast majority of its medical problems, especially in the pediatric population. The relatively high child morbid-ity and mortality in South Africa is caused by a diversity of factors, among which are unem-ployment of parents; alcoholism (with its historical origin in the �dop� system of the pre-apartheid era), especially of women in child bearing age, with the resultant high rate of fetal alcohol syndrome (FAS) in children, domestic violence; child abuse and insecurity; (gang) rape and malnutrition. Among the major infectious causes of morbidity and mortality are pediatric HIV-AIDS (PAIDS), tuberculosis, intestinal parasites and others. Most of these intertwined social and medical problems are concentrated in the poor black and coloured neighborhoods of urban centres. The regular visits to homes, schools and healthcare centres in the communities in which my research project was conducted, gave me a Þ rst-hand expo-sure to the magnitude of these problems. Majority of these medical problems would, in my opinion, only be solved if the social problems are equally addressed.
However, in spite of all these myriads of problems, the courage, optimism and dedica-tion with which the (non-)medical staff of the Desmond Tutu TB Research Centre of the Department of Pediatrics of the Stellenbosch University (under the leadership of Prof. Nulda Beyers) affronted their tasks is very commendable.

Infection with M. tuberculosis and atopy in children

Infection withM. tuberculosis and
atopy in children
Infectie met M. tuberculosis en atopie in kinderen(met een samenvatting in het Nederlands)
Proefschrift
Ter verkrijging van de graad van doctor aan de Universiteit Utrecht op gezag van de Rector MagniÞ cus, Prof. Dr. W.H. Gispen, ingevolge het besluit van het College voor Promoties in het openbaar te verdedigen op dinsdag 7 maart 2006 des middags te 2.30 uur
door Charles Obiharageboren 12 februari 1965 te Owerri, Nigeria

Promotor: Prof. Dr. J.L.L. KimpenCo-promotor: Prof. Dr. N. Beyers
The research described in this thesis was Þ nancially supported by the Wilhelmina Children�s Hospital Research Funds and the Stellenbosch University (through funding from the South African Department of Trade and Industry, THRIP fund). The researcher is a recipient of a grant from the Ter Meulen Fund, Royal Netherlands Academy of Arts and Sciences.

v
Contents
Foreword / Voorwoord vii
Chapter 1 General introduction 1Chapter 2 The clinical epidemiology of childhood pulmonary tuberculosis:
a critical review of literature from pre-chemotherapy era 23 Int J Tuberc Lung Dis 2004; 8:278-285Chapter 3 The prevalence of symptoms associated with pulmonary tuberculosis
in randomly selected children from a high burden community 39 Arch Dis Child 2005; 90:1166-1170Chapter 4 Does mycobacterial infection prevent the development of atopy
in childhood? A systematic review 49 Submitted
Chapter 5 Mycobacterium tuberculosis infection may protect against allergy in a tuberculosis endemic area 63
Clin Exp Allergy; 2006; 36:70-76Chapter 6 Inverse association between Mycobacterium tuberculosis infection
and atopic rhinitis in children 77 Allergy 2005; 9:1121-1125. Chapter 7 Respiratory atopic disease, Ascaris-IgE and tuberculin test
in urban South African children 87 Clin Exp Allergy; 2006; in pressChapter 8 The association of prolonged breastfeeding and allergic disease
in poor urban children 103 Eur Respir J 2005; 25:970-977 Chapter 9 General discussion 117
Summary / Samenvatting 127Acknowledgements / DankwoordCurriculum VitaeList of publications

vii
Foreword
In the past 3 years, I have frequently been asked why I chose to do my PhD research in South Africa.
It is difÞ cult to give precisely the moment when the seed of this PhD was sown. It was a combination of factors which led to it. Among these are my personal curiosity for new challenges, the urge to make some relevant scientiÞ c contribution in a developing country and the determination to avoid the boredom of routine and a midlife crisis.
That the topic of research involved two diseases, of which one causes a substantial health burden, especially in children living in industrialized countries, while the other, one of the major causes of death in children in less industrialized countries, was not a coinci-dence. This choice reß ects my unique position in the two different worlds and the chal-lenge I feel to make a valuable contribution to both. In one of these worlds, my adopted one in which I live, both the healthcare and education systems are well and functioning, and in the other world, in which I have my roots, the health care and education systems are sick and in shambles. Therefore, the challenge is, at least for me, to link these different worlds positively.
This thesis would not have materialized without the broad-mindedness of Professor Jan Kimpen, my promotor. From the moment I approached Jan towards the end of the 4th year of my pediatric training, with my wish to do research on a topic which not only would address a relevant health problem in the Netherlands, but which would also contribute to scientiÞ c research in a developing country, he involved himself actively to make me realize these objectives. Jan�s enthusiasm was clear right from the start.
There was however one element of coincidence: the fact that Jan met Professor Nulda Beyers, my co-promoter, a few months previously and they had agreed to cooperate on re-search projects. It did not take long for Nulda to accommodate our study proposal.
A lion�s share of the decision making rested on my family and me. After the gentleman�s agreement to cooperate on the project, to me was left the difÞ cult task of convincing my wife to abandon her job and family, and my children to leave their friends, secure and har-monious life behind, for a country unknown to us. For a country whose many social prob-lems have frequently been imported into our homes through the mass media.
As would be expected, the intention to carry out my PhD research in South Africa turned out to be the easiest part of the whole bargain. The proposal still had to be writ-ten and funding realized. This all took place between July and October 2001, in the Þ nal year of pediatric training. In October 2001, the Ter Meulen Funds (TMF), the Netherlands awarded me a research-grant for personal subsistence and that of my family. The two de-partments involved agreed to Þ nance the research-project. I left the Netherlands for Cape Town, South Africa in March 2002; my family joined me 3 months later. The Þ eldwork of this study was conducted between July 2002 and December 2003.
viii
Infection with M. tuberculosis and atopy in children
Being that all my medical study took place in Europe (Italy and The Netherlands), I per-ceived in this project a unique opportunity to broaden my knowledge of tuberculosis, and other tropical (the so called �exotic�) diseases. I also saw in it an opportunity to contribute to the search for the cause(s) of increasing global incidence of allergic diseases, such as asth-ma and hay fever, in the past three decades or more, especially in industrialized countries.
In addition, the research would offer an extra �spin-off� effect: an opportunity for a tem-porary �brain-impute� for South Africa, the opposite of the �brain-drain� (a phenomenon which started since the dismantling of apartheid, in which qualiÞ ed young professionals, including doctors migrate with their expertise to a foreign country, usually an industrial-ized one).
Although the choice for the Western Cape was purely coincidental, it created the chance to make contributions on yet another dimension. In The Netherlands, I was used to being the only black face during conferences and other (medical) meetings with colleagues. This was surprisingly not different from the experience in South Africa, particularly in Cape Town. I know that this situation will change in the future.
Despite the fact that I may not have played a much active role in this respect, I however, take the liberty to believe that the door will open easier for black doctors who embark on projects with my South African supervisors and colleagues who worked with me in the past 3 years. I believe that both the success of this cooperation and the successful completion of my project have helped to uproot some weed of prejudice and historical uneasiness on different levels.
South Africa took us off the feet, right from the start. This was not only due to the natu-ral beauty of the country for which tourists ß ock or the incredible hospitality of my new hosts, but also the wide social and racial divide, with the mixture of Þ rst (in the predomi-nantly white neighborhoods) and third (in the predominantly black or coloured neighbor-hoods) world parts.
The immense social problems of the country also contribute to a vast majority of its medical problems, especially in the pediatric population. The relatively high child morbid-ity and mortality in South Africa is caused by a diversity of factors, among which are unem-ployment of parents; alcoholism (with its historical origin in the �dop� system of the pre-apartheid era), especially of women in child bearing age, with the resultant high rate of fetal alcohol syndrome (FAS) in children, domestic violence; child abuse and insecurity; (gang) rape and malnutrition. Among the major infectious causes of morbidity and mortality are pediatric HIV-AIDS (PAIDS), tuberculosis, intestinal parasites and others. Most of these intertwined social and medical problems are concentrated in the poor black and coloured neighborhoods of urban centres. The regular visits to homes, schools and healthcare centres in the communities in which my research project was conducted, gave me a Þ rst-hand expo-sure to the magnitude of these problems. Majority of these medical problems would, in my opinion, only be solved if the social problems are equally addressed.
However, in spite of all these myriads of problems, the courage, optimism and dedica-tion with which the (non-)medical staff of the Desmond Tutu TB Research Centre of the Department of Pediatrics of the Stellenbosch University (under the leadership of Prof. Nulda Beyers) affronted their tasks is very commendable.
1
C H A P T E R 1
Introduction
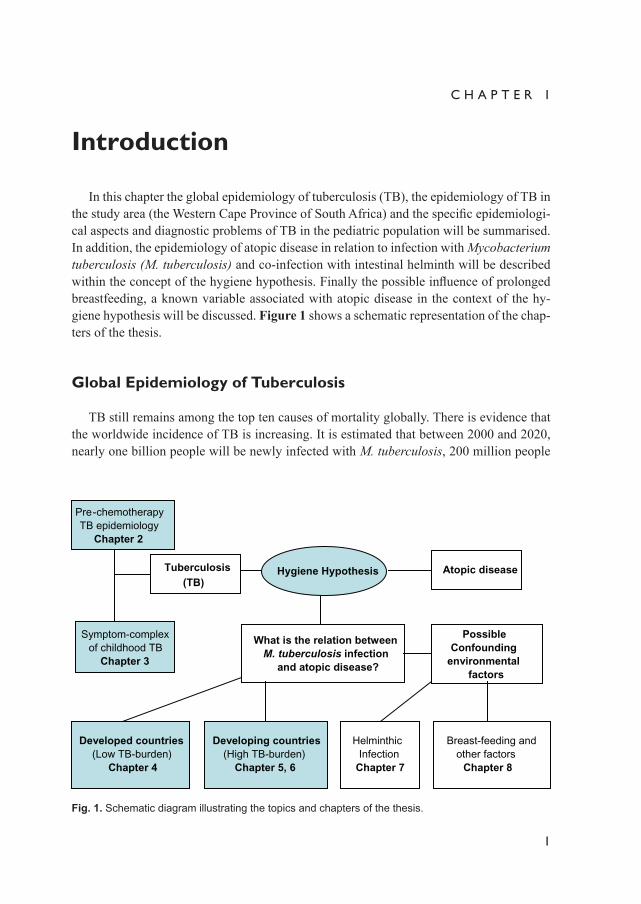
In this chapter the global epidemiology of tuberculosis (TB), the epidemiology of TB in the study area (the Western Cape Province of South Africa) and the speciÞ c epidemiologi-cal aspects and diagnostic problems of TB in the pediatric population will be summarised. In addition, the epidemiology of atopic disease in relation to infection with Mycobacterium tuberculosis (M. tuberculosis) and co-infection with intestinal helminth will be described within the concept of the hygiene hypothesis. Finally the possible inß uence of prolonged breastfeeding, a known variable associated with atopic disease in the context of the hy-giene hypothesis will be discussed. Figure 1 shows a schematic representation of the chap-ters of the thesis.
Global Epidemiology of Tuberculosis
TB still remains among the top ten causes of mortality globally. There is evidence that the worldwide incidence of TB is increasing. It is estimated that between 2000 and 2020, nearly one billion people will be newly infected with M. tuberculosis, 200 million people
Tuberculosis(TB)
Atopic diseaseHygiene Hypothesis
What is the relation betweenM. tuberculosis infection
and atopic disease?
Developed countries(Low TB-burden)
Chapter 4
Developing countries(High TB-burden)
Chapter 5, 6
HelminthicInfection
Chapter 7
Breast-feeding andother factors
Chapter 8
Pre-chemotherapyTB epidemiology
Chapter 2
Symptom-complexof childhood TB
Chapter 3
PossibleConfounding
environmentalfactors
Fig. 1. Schematic diagram illustrating the topics and chapters of the thesis.
2
Infection with M. tuberculosis and atopy in children
will develop disease and 35 million will die from TB.1 Africa as a continent has the high-est estimated TB incidence in the world. Even the developed nations, such as the United States and Europe, have recently experienced a dramatic resurgence of TB.2 TB epidemi-ology has changed in the past two decades due to the inß uence of the Acquired Immune DeÞ ciency Syndrome (AIDS) epidemic. Human immunodeÞ ciency virus (HIV) infection has been estimated to account for an excess of 34% of new cases of TB.3 About 70% of the estimated 36.1 million people in the world with HIV and AIDS live in sub-Saharan Africa.4
Other factors contributing to the global TB resurgence include poverty, overcrowding, in-creased global travel and immigration, breakdown of national TB control programmes, the emergence of multi-drug resistant tuberculosis (MDR-TB), and incomplete or erratic treatment.5,6
TB is caused by M. tuberculosis, a microorganism for which humans are the principal reservoir. TB is transmitted by inhalation of airborne droplet nuclei of 1-5 μm in diameter that contain M. tuberculosis, coughed into the air by a person with smear-positive pulmo-nary TB. Because of their small size, the particles can remain airborne for minutes to hours after expectoration.7,8 The inhaled infectious droplets lodge in the alveoli in the distal air-ways where M. tuberculosis is taken up by alveolar macrophages and dendritic cells which leads to the initiation of a cascade of events that results in either successful containment of the infection or progression to primary progressive TB. The estimated lifetime risk of disease is 10% (Figure 2),4 meaning that of every ten persons becoming infected, one will develop TB disease in a lifetime, after an asymptomatic period ranging from weeks to decades.9 The development of active TB disease is dependent on time since infection, age and host immunity. The risk for developing TB disease is highest within the Þ rst 12 months following primary infection and declines with time.10
After being phagocytosed by alveolar macrophages, M. tuberculosis replicates and spreads via the lymphatic system to the hilar nodes (hilar lymphadenopathy). In most in-fected individuals, cell-mediated immunity develops 2-8 weeks after infection. Activated T lymphocytes and macrophages form granulomas that limit further spread of the micro-organism.11 In most individuals with normal cell-mediated immunity the infection remains contained and does not progress to active disease (latent TB infection, LTBI) (Figure 2).
An efÞ cient T-helper 1 (Th1) immune response is required for the elimination of M. tu-berculosis and deÞ ciency or mutations of genes involved in Th1 responses lead to extreme sensitivity to mycobacterial infection in laboratory animals and in humans.11,12 Activated alveolar macrophages infected with M. tuberculosis interact with T lymphocytes via a cy-tokine network, involving among others interleukin (IL)-12 and IL-18 which stimulate T lymphocytes (principally CD4+ T lymphocytes) to release gamma interferon (IFN-γ).12 IFN-γ stimulates the phagocytosis of M. tuberculosis in the macrophage, and the release of TNF-α, important for granuloma formation and control of the extent of disease.13,14 Failure of the host immune response to contain replication of M. tuberculosis during initial infec-tion results eventually in active disease, characterised by uncontrolled bacillary prolifera-tion, dissemination of organisms to distal sites and development of symptoms. Alterna-tively, if the infected host is immune-competent, the host�s immune system will typically resolve or control the initial infection, using mechanisms that prevent bacterial spread,

1 Introduction
3
limit bacterial dissemination, and concentrate immune response mechanisms directly to sites of infection.15 These individuals remain latent carriers of M. tuberculosis bacilli, but they do not exhibit overt signs and symptoms of disease, and are not infectious. However, they do test positive for delayed type hypersensitivity (DTH) response. The Þ nal stage of infection is characterised by reactivation of latent M. tuberculosis bacilli and subsequent development of secondary active infection in the host (Figure 2). The mechanisms respon-sible for the reactivation of mycobacterial growth after a variable period of latency are not clear; however this is likely to be inß uenced by factors associated with the host�s immune status, such as HIV, age, immunosuppressive therapy and malnutrition.15 Activation of cell-mediated immunity against M. tuberculosis is associated with the development of a cutane-ous DTH reaction to tuberculin. Tuberculin reactivity becomes apparent 3-6 weeks after initial M. tuberculosis infection and may remain positive for the lifetime of the individual.16 A positive tuberculin skin test (TST) reaction is an accepted marker of primary infection with M. tuberculosis.16,17
Susceptibility to M. tuberculosis is determined by genetic as well as environmental factors that regulate the immune response.18-21 Population-based studies have shown an association between TB and some HLA alleles, as well as polymorphisms in the genes en-coding for the natural resistance-associated macrophage protein (NRAMP1), the vitamin D receptor, and IL-1 receptors.19-24 The functional importance of these polymorphisms is still unclear, although NRAMP1 polymorphisms could inß uence TB susceptibility by regula-tion of IL-10.25
Exposure to M. tuberculosis
Infection Transient infectionwith clearance
No infection
Latent TB infectionPrimary TBIn the first 1-2years after infection
5% 95%
Long-termimmune control
Lifelongcontainment
95%
Reactivation TB
5%
Fig. 2. Pathogenesis of Mycobacterium tuberculosis infection.
4
Infection with M. tuberculosis and atopy in children
Epidemiology of tuberculosis in the Western Cape Province of South Africa
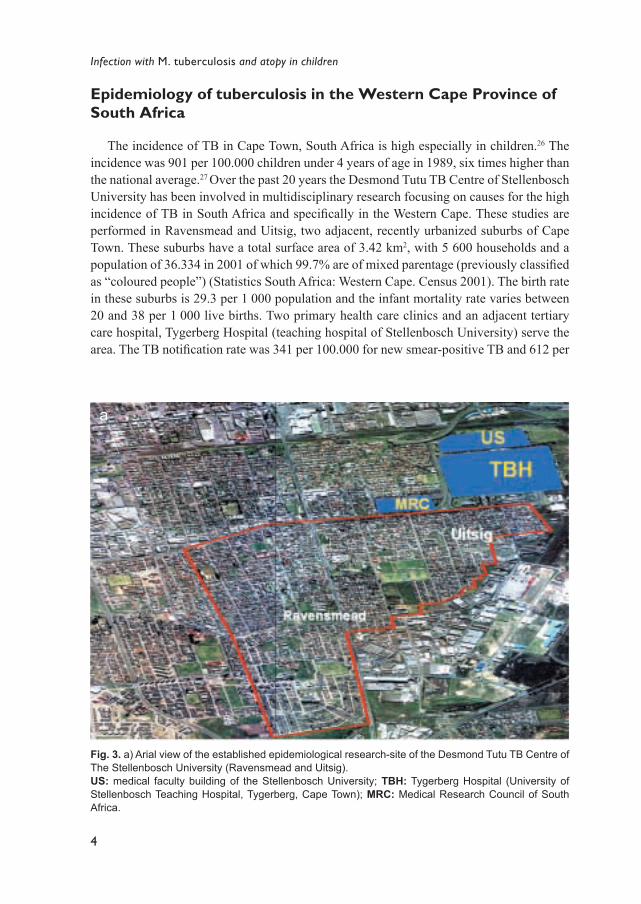
The incidence of TB in Cape Town, South Africa is high especially in children.26 The incidence was 901 per 100.000 children under 4 years of age in 1989, six times higher than the national average.27 Over the past 20 years the Desmond Tutu TB Centre of Stellenbosch University has been involved in multidisciplinary research focusing on causes for the high incidence of TB in South Africa and speciÞ cally in the Western Cape. These studies are performed in Ravensmead and Uitsig, two adjacent, recently urbanized suburbs of Cape Town. These suburbs have a total surface area of 3.42 km2, with 5 600 households and a population of 36.334 in 2001 of which 99.7% are of mixed parentage (previously classiÞ ed as �coloured people�) (Statistics South Africa: Western Cape. Census 2001). The birth rate in these suburbs is 29.3 per 1 000 population and the infant mortality rate varies between 20 and 38 per 1 000 live births. Two primary health care clinics and an adjacent tertiary care hospital, Tygerberg Hospital (teaching hospital of Stellenbosch University) serve the area. The TB notiÞ cation rate was 341 per 100.000 for new smear-positive TB and 612 per
Fig. 3. a) Arial view of the established epidemiological research-site of the Desmond Tutu TB Centre of The Stellenbosch University (Ravensmead and Uitsig).US: medical faculty building of the Stellenbosch University; TBH: Tygerberg Hospital (University of Stellenbosch Teaching Hospital, Tygerberg, Cape Town); MRC: Medical Research Council of South Africa.
a

1 Introduction
5
100.000 for bacteriologically conÞ rmed TB in 2002 (Statistical Support and Informatics. Statistics South Africa: Western Cape. Census 2001). Childhood TB cases comprise 39% of all notiÞ cations, and TB incidence in the pediatric population correlates directly with crowding and inversely with parental education and annual household income.6 A geo-graphical information system (GIS) of these suburbs has been established and the notiÞ ca-tion and TB register data of all TB patients since 1985 have been linked to the GIS (Fig-ure 3). Over a 10 year period (1985-1994) there were 4 530 cases of TB in Ravensmead and Uitsig occurring in 2 138 houses. TB is concentrated in the enumerator subdistrists (ESDs) with the smallest houses, the lowest per capita income and the lowest level of education.6
The national TB programme, which is delivered on primary health care clinic level by the local authority, contains all the elements of the directly observed treatment, short
Fig. 3. b) Random Sampling methods of households for the study. Households from the original sampling (green spots) which refused to participate were systematically replaced (red spots).
b
6
Infection with M. tuberculosis and atopy in children
course (DOTS) strategy as recommended by the World Health Organization (WHO). All adult household members and children under the age of 5 years living in the same house-hold as an adult TB index-case are requested to visit the clinic to be screened for TB. Chil-dren under the age of 5 years with either a positive TST or a contact with an infectious case of TB receive chemoprophylaxis. Since 1972 BCG vaccination in the neonatal period has been compulsory and the BCG coverage in the area is greater than 97%, thus universal ac-cording to WHO criteria.
A tuberculin survey to estimate the Annual Risk of TB Infection (ARTI) was done in 1998/1999. Four thousand Þ ve-hundred and eighty-one (4581) school children out of a total of 5779 in the nine primary schools of the study communities (79.3% aged between 5 and 15 years) were examined with a TST. In those aged 15 years, 50% were TST posi-tive (≥ 10 mm) and the overall ARTI was 3.5%. This was much higher than a similar study done in 1978 (ARTI 1.8%). These results indicate that there is presently more transmission of TB than 20 years ago and might explain why 39% of notiÞ ed cases in these suburbs are children.6
Since 1993, more than 3000 sputum samples from more than 1200 patients in Ra-vensmead and Uitsig have been strain-typed using a DNA restriction fragment length poly-morphism (RFLP) method and the IS 6110 probe. When analysing the whole database, results indicate that about half of the patients have unique organisms, indicating endoge-nous reactivation of previous TB infection, and about half have TB organisms with similar RFLP patterns (clusters) indicating recent transmission.28 In patients with �relapse� of TB after successful treatment, the second episode was due to re-infection and not reactivation of latent TB in more than 70% of cases.29 The RFLP studies therefore conÞ rm the high transmission and infection rate documented in the ARTI study of 1999. An ineffective TB control strategy may contribute to these high transmission rates. However, the TB control programme has improved in recent years with rapid availability of sputum smear results and the full implementation of DOTS. The cure rates for new smear positive adults in the area are now 80%. At present the high rates of transmission of TB in the area cannot be ascribed solely to HIV infection, as the prevalence of HIV is among the lowest in South Africa.30
Epidemiological aspects and diagnostic problems of childhood tuberculosis
TB in children remains a signiÞ cant cause of morbidity and mortality in less developed nations.31,32 Estimates by the WHO indicate that every year 450 000 TB related deaths oc-cur in children under 15 years of age.33 The TB epidemic is maintained by people with cavitating disease, who are responsible for disease transmission within the community. Cavitating disease is rare in young children, but common in adults and children older than 10 years of age.34 TB in children results from recent transmission within the household or within the community.34 More than 90% of children who develop primary TB, do so within the Þ rst 12 months after infection.34,35 Therefore, the occurrence of TB in children is an

1 Introduction
7
indicator of the level of ongoing TB transmission in a particular community and deÞ cien-cies in current public health efforts.36 Immune competent adults with TB infection have a 5-10% lifetime risk of developing disease if untreated.5 The risk for children is higher � up to 43% of infants, 24% of children 1-5 years of age, and 15% of adolescents aged 11 to 15 years with untreated TB infection will develop detectable pulmonary TB.31 If untreated, ap-proximately 30% of children with pulmonary TB will eventually develop extra-pulmonary forms of TB disease.37
Following initial exposure to a case of infectious TB, the accepted hallmark of TB infection is conversion of the TST. Subsequent TB disease is characterised by the devel-opment of signs and symptoms and/or radiographic changes. Without chemoprophylaxis, 40-50% of infants and 15% of older children with infection will develop disease in 1-2 years.31,38 Younger children, particularly those less than 6 years of age, can develop pulmo-nary, disseminated, and central nervous system (CNS) TB in less than 3 months due to a shorter incubation period.31
Although childhood TB contributes to only 3-6% of the total TB case-load in industri-alised countries, it makes up a large proportion (up to 15-20%) of all TB cases in devel-oping countries.39 In areas with a high prevalence of TB, children may even contribute a higher proportion (up to 40%) of TB case-load and experience considerable morbidity and mortality related to TB.40 Pulmonary TB rivals common bacterial pneumonia as a respira-tory cause of death in African children older than 6 months of age.41 Infection with HIV is the most important risk factor so far identiÞ ed to accelerate the progression of LTBI to disease and the added impact of HIV on TB disease in children is contributing to the esca-lating TB epidemic in children globally.42
Positive culture of M. tuberculosis is the gold standard by which the diagnosis of TB can be proven in the adult population. TB in children is pauci-bacillary and therefore usu-ally smear-negative.16,31,43 Whereas sputum smears detect up to 75-80% of adult pulmonary TB, less than 10% of children with pulmonary TB have a positive acid-fast smear of spu-tum or gastric aspirate. Bacteriological conÞ rmation by culture of M. tuberculosis, rarely exceeds 30-40% in the pediatric population.27,39 In resource-poor countries this Þ gure is probably lower. The poor sensitivity of current laboratory tests is partly attributable to the pauci-bacillary nature of pulmonary TB in children. The vast majority of studies on diag-nostic tests in children utilised gastric aspirate samples. Limitations of this method include low gastric pH which is known to kill TB bacilli which may inß uence the survival of bacilli for culture, peristalsis in the evening and during sleep which makes it possible that many of the bacilli swallowed by the child have migrated beyond the gastric environment by time of collection, the need for and cost of a 3-day hospitalisation and the invasive nature of the procedure. Nasopharyngeal aspirate and induced sputum are promising less invasive meth-ods and preliminary results (culture and PCR sensitivity) are comparable to that of gastric aspirate.31 Symptoms of childhood TB are non-speciÞ c, and up to 50% of children may be asymptomatic in the early stages of disease.39 If their infection remains unrecognized these children serve as a latent reservoir of M. tuberculosis, LTBI. Chest radiography is regard-ed as a valuable diagnostic tool of childhood TB, but it is often difÞ cult to identify hilar and paratracheal lymphadenopathy, considered to be the most consistent sign of primary

8
Infection with M. tuberculosis and atopy in children
pulmonary TB.44 In addition, the distinction between recent primary infection and active disease is problematic.34 The major reason for making a distinction between infection and disease is because each is treated differently. Infection is generally treated with a single anti-TB drug, while disease is treated with three or more anti-TB drugs.
Initial pulmonary TB infection is characterised by a Ghon focus with regional lymph-adenopathy (�primary complex�), which may not be obvious radiologically.44 In most chil-dren this resolves spontaneously with residual calciÞ cation or scarring in the lung tissue. Some children may develop progressive lymphadenopathy.44 The primary complex may progress to a caseating lesion, progressive primary TB (PPTB). This may rupture into the pleural or pericardial spaces leading to pleural or pericardial effusions. Caseating lesions may erode into pulmonary vessels resulting in hematogenous dissemination to the lung and distant anatomical sites. The most severe manifestations of this are miliary TB and CNS TB. Miliary TB is an early complication of primary infection and usually affects young children and immune-compromised adults. Older children and adolescents usually develop adult-type reactivation pulmonary disease, post-primary TB disease.44 Extrapul-monary TB disease is more often seen in children than in adults. It occurs in approximately 25% of infants and young children less than 4 years of age with PPTB disease.16 The most common manifestation of extra-pulmonary TB in childhood is superÞ cial lymphadenitis, usually involving supraclavicular, anterior cervical, tonsillar, and submandibular lymph nodes. CNS TB, especially TB-meningitis is the most serious complication of TB in chil-dren and the incidence is about 4% in children with primary TB.16 It has a high morbidity and a mortality rate of about 13%. Bone and joint TB may involve weight-bearing bones and joints, particularly the vertebrae in Pott�s disease. Other extrapulmonary predilection sites are the gastrointestinal tract and the kidneys. This latter site is rarely involved in chil-dren.16 Young children infected with M. tuberculosis are at increased risk of developing TB compared to older children and adults. In one study of persons with a history of recent TST conversion conducted in the pre-chemotherapy era, children aged under 6 years developed active TB more frequently than adults (73% vs. 25%).35 Furthermore, infants aged under 1 year developed meningeal and disseminated TB more frequently than older children and adults.16
In summary, childhood TB is an indicator of the level of ongoing TB transmission most commonly from an infectious adult-case in a particular community and deÞ ciencies in current public health efforts. Children are at greater risk of developing serious pulmonary, extra-pulmonary and disseminated TB than adults. The paucity of epidemiological data on childhood TB is partly due to lack of adequate diagnostic methods available to detect cases of TB and the low priority to children in national and global TB control programs. Bacte-riologic conÞ rmation of childhood TB is problematic due to the pauci-bacillary nature of disease. More sensitive diagnostic methods are needed to address this problem.
Study aimTo review the epidemiology of childhood tuberculosis in the pre-chemotherapy and chemotherapy era. (Chapters 2 and 3)

1 Introduction
9
Tuberculin skin test In response to infection, a positive DTH response, evidenced by skin induration in re-
sponse to intradermal injection of puriÞ ed protein derivative (PPD), develops in 80 to 90% of children.43,45,46 However, young children less than 2 years of age and/or children with disseminated disease are less likely to have a positive TST response. PPD is a term applied to culture Þ ltrates of mycobacteria that have been precipitated with either trichloroacetic acid or ammonium sulphate, and standardised as to protein content. International standards exist for PPD, and dosage strength is deÞ ned in international units (IU) - a unit of biologi-cal activity, contained in a deÞ ned amount, weight or volume of the particular international standard preparation. One of the most widely used tuberculins today, namely PPD RT 23 (Statens Serum Institute, Copenhagen, Denmark) is expressed in tuberculin units (TU). Di-agnostic use of the Mantoux test can be carried out using inoculum strength of 2 TU.
As indicated earlier, a positive TST is an accepted hallmark of infection with M. tuber-culosis. In most children, TST reactivity becomes apparent in 3-6 weeks, but occasionally can take up to 3 months after initial M. tuberculosis infection and may remain positive for the lifetime of the individual, even after treatment.16 Two major techniques are currently used for TST; the technique according to Mantoux (�Mantoux test�) and the multi-puncture technique. The Mantoux test is the standard method used in many countries for detecting infection with M. tuberculosis. The test involves the intradermal injection of PPD solution into the superÞ cial layer of the skin in the forearm, which raises an immediate wheal. The skin reaction is measured as millimetres of induration (not erythema) after 48-72 hours. False-negative TST may occur in children with severe disseminated TB disease (such as miliary TB) soon after infection, those with debilitating or immunosuppressive illnesses, severe malnutrition, or other severe infections. The rate of false-negative TST in children with TB who are co-infected with HIV is unknown and is dependent of the degree of immunosuppression.16
False-positive TST is often attributed to infection with mycobacteria other than tubercu-losis (MOTT; other synonyms are non-tuberculous mycobacteria (NTM) and environmen-tal mycobacteria), including M. bovis BCG vaccine, which, because of shared antigenic properties, may lead to a TST response even if the individual has not been infected with M. tuberculosis. Increased sensitivity may also be induced by repeated skin testing, a phe-nomenon known as �boosting�, especially if the previous test was given within the previ-ous year. There has been uncertainty regarding the effect of BCG immunization on TST results. BCG immunization may cause a transiently reactive TST, but studies have shown that most children who received BCG as infants have weak or non-reactive TST at 5 years of age.47-49 A recent study has demonstrated that BCG immunization has little impact on the interpretation of TST in children during a contact investigation.50
Epidemiology of atopic disease
During the last few decades, the prevalence of atopic disease has increased dramatically in countries with a western lifestyle.51 This increase cannot only be accounted for by im-
10
Infection with M. tuberculosis and atopy in children
proved awareness of the physician to diagnose atopic disease or by the efÞ cient media pub-licity of the topic.51-55 This dramatic increase in the prevalence of atopic disease has been associated with exposure to environmental stimuli such as allergens, environmental tobac-co smoke (ETS) exposure, the presence of elevated serum immunoglobulin E (IgE) levels during the Þ rst year of life and viral respiratory infections in the Þ rst years of life.56-60
It is generally assumed that asthma and other allergic diseases are less prevalent in non-industrialised than in industrialised countries.51 The prevalence of asthmatic symptoms in 13 and 14-year-old schoolchildren was found to vary widely in African countries from highest in South Africa (13.1%) to lowest in Ethiopia (2.5%), the prevalence of recent allergic rhino-conjunctivitis ranged from lowest in Ethiopia (2.5%) to highest in Nigeria (39%), and of atopic eczema from lowest to highest in the two centres from Ethiopia (4% and 20%).51 Comparatively, the overall prevalence of atopic diseases in African countries was not lower than in some industrialized countries.51 This is supported by results from one study, in which the prevalence of atopic symptoms was compared between Australian and Nigerian children in the same age category, using the same methodology.61 There was no signiÞ cant difference in the prevalence of atopic outcome between Australian children (32.5%) and their Nigerian counterparts (28.2%). Differences have been reported from Africa on the prevalence of atopy between children from different socio-economic back-grounds, living in the same geographical area.62 In Cape Town, South Africa, the preva-lence of childhood asthma is 10.8 -13.3%, allergic rhinitis 16 % and eczema 9%.51,63
Although the exact cause(s) of the increase in the incidence of atopic disease is still unknown, different possible hypotheses have been proposed. Of these, only the hygiene hypothesis will be discussed in this thesis.
The hygiene hypothesis: biological explanation
EpidemiologyThe �hygiene hypothesis�, Þ rst proposed by Strachan in 1989, suggests that lack of in-
fections in early life underlies the increasing incidence of atopic disease in westernized so-cieties.64 The uniÞ cation of East and West Germany offered a unique setting to study the in-ß uence of different environments on a genetically similar population. Against all odds, Von Mutius et al. found a lower sensitisation to local allergens and lower asthma prevalence in East than in West Germany and the authors suggested that the difference was due to the lower rate of early childhood infections in West German children.65 Riedler et al. found in a cross sectional survey in Austria, Germany and Switzerland that long-term and early ex-posure (before 12 months of age) to stables and farm milk induces a strong protective effect against development of asthma, allergic rhinitis and atopic sensitisation.66 In Sweden it has been shown that atopic and non-atopic children differed signiÞ cantly in the types of fae-cal bacteria.67 A signiÞ cantly lower prevalence of atopy was found in children who entered the nursery or day care at an age of less than 24 months.68,69 A strong inverse relation has been found between the number of older siblings and the prevalence of allergic rhinitis in childhood and early adult life in a British national birth cohort study, between the number

1 Introduction
11
of older siblings and the prevalence of wheeze in children and between the total number of siblings and the prevalence of skin-test reactivity to common aeroallergens.64,70,71 An increased prevalence of atopic disease in children raised in cities compared to children raised in rural areas has been reported from different Western countries.66,72,73 Although the factor responsible for this effect is not clear, it was hypothesized that exposure to bacte-rial endotoxin is involved since endotoxin levels in house dust were signiÞ cantly higher in house dust from farming households compared to non-farming households.72-74 Other in-fectious diseases which have been inversely linked to the rate of atopic disease are measles in Guinea Bissau, hepatitis A in Italian military recruits and BCG immunization in both Japanese children and children from Guinea-Bissau.75-78 However, the hygiene hypothesis was challenged by other studies.49,79-83
Th1/Th2 paradigmThe biological explanation for the rising incidence of allergic disease in westernized
countries is that allergen-speciÞ c T cell memory responses become Th2 skewed in the absence of stimulating Th1 immunity.84-86 This model, coined the Th1/Th2 paradigm, fo-cused on the induction phase and initial maturation of the immune response against envi-ronmental allergens early in life.85 Th1 and Th2 cells are not distinct CD4+ T-cell subsets, but they simply represent polarized forms of the highly heterogeneous T-cell-mediated im-mune responses.86 The two types of immune response can be distinguished on the basis of the cytokines involved; Th1 cells producing IFN-γ, IL-2 and TNF-β and Th2 cells produc-ing IL-4, IL-5, IL-9 and IL-13.86 Naturally Th1 cells are paramount in the defence against invading intracellular microorganisms such as mycobacteria and some viruses. Th2 cells, on the other hand, cause, through a complex cytokine and mediator network, eosinophil and basophil activation resulting in the protection against extracellular organisms, such as parasites.87 Although the Th1/Th2 paradigm was a useful model to explain the rising incidence of allergies, it has been challenged on a few important points.88 For instance, it proposed the existence of a �window of opportunity� in infancy (in the Þ rst 5 years) in which infection-driven protection from allergy is supposed to occur. This does not, howev-er, explain the observation of adult migrants from countries with a low prevalence of atopy developing atopic disease when they move to a country with a westernized life-style.89 This suggests that abrogation of protection from allergy can still lead to the development of atopic inß ammation in genetically predisposed individuals even after the childhood �win-dow of opportunity�. It has also been shown that the remission of atopic disease can be induced by infections acquired after childhood.90 Moreover, if both T helper-cell types were mutually exclusive or strictly down-regulated each other as initially suggested by the Th1/Th2 paradigm, then the hygiene hypothesis could not logically explain the rising incidences of both Th1-mediated autoimmune diseases and Th2-mediated atopic allergy globally.91
Anti-infl ammatory regulatory networksRecently, an alternative view has emerged that suggests the importance of reduced im-
mune suppression rather than of missing immune deviation to explain the hygiene hy-

12
Infection with M. tuberculosis and atopy in children
pothesis. According to this view, lower microbial burden does not act by inducing a lower production of Th1-inducing cytokines but by decreasing the activity of regulatory T cells (Tregs).87 In this new model, in which CD4+ Tregs play a central role, it is proposed that infections would inhibit allergic, as well as other immune-mediated inß ammatory diseases through the stimulation of anti-inß ammatory networks (immune suppression).87,89 Reduced immune suppression, thus, is seen as the reason for increasing prevalence of allergies in westernized societies. This model could logically explain not only the increase in Th2 but also in Th1-mediated inß ammatory diseases.87,89 At present the most important CD4+ Treg cell subsets are represented by CD4+CD25+ T cells. Removal of this T cell subset from normal mice leads to the spontaneous development of various autoimmune disorders and the number of CD4+CD25+ T cells appears to be reduced in different autoimmune diseases in humans.92 The mechanism of suppression by Treg cells is mediated through the produc-tion of inhibitory or anti-inß ammatory cytokines, such as IL-10 and TGF-β.87,93 Pathogens that cause persistent or chronic infections may have evolved strategies to subvert the host�s immune responses, through stimulating an increased production of anti-inß ammatory or immunosuppressive responses, which normally function to control the protective immune effector-responses of the host.94
One important implication of the revised immunologic model of the hygiene hypothesis is that the interaction between infection and allergens is not limited to the �window of op-portunity� in early life, but retains some ß exibility well into adulthood. Secondly, the role of pathogens that cause intense and persistent infection is highlighted.87,89 It has been sug-gested that in hygienic settings, as in most industrialised countries, a single shot of BCG immunization, even if given in infancy, would not be sufÞ cient to prevent the development of atopy or its inß ammatory consequences.89 Furthermore, that BCG immunization can-not mimic the persistent immune stimulation provided by an intense and chronic natural exposure to pathogenic and non-pathogenic mycobacteria.89 This is supported by studies showing that BCG is a poorer inducer of IL-12 than natural M. tuberculosis infection.95 This may partly explain the differences in epidemiological Þ ndings on the relation between mycobacterial infection and the development of atopy, as a majority of studies has been conducted in countries with low natural M. tuberculosis burden. This is supported by sug-gestions that a strong regulatory network stimulated by chronic infections, both Th1 skew-ing (such as M. tuberculosis) and Th2 skewing (such as parasites), may be the predominant allergy-protective mechanism among populations living in developing countries.87,89 This implies that the relevance of this mechanism may be less in countries whose populations are less frequently exposed to these chronic infections.89
In summary, despite contradicting epidemiological Þ ndings in humans, it is still possible that, under certain conditions, mycobacterial infection may contribute to protection against atopy.87,89 This is supported by evidence from both experimental and animal models.93,96,97 In addition, it is supported by indirect epidemiological observations that in many countries where M. tuberculosis infection is more common, allergy seems to be less frequent.98

1 Introduction
13
Mycobacterial infection and atopic disease
Since Shirakawa and colleagues noted an inverse relation between hypersensitivity to M. tuberculosis (positive TST) and atopic disease in Japanese children, there has been in-creased interest in the role of the immune response directed against mycobacteria and its potential protective role in atopic diseases.77 This is of particular relevance given interest in the use of mycobacterial proteins as a potential vaccine against atopic disease.99 Recent evidence suggests that chronic infections, such as mycobacterial infection may modulate the expression of atopic disease.88 M. tuberculosis infection, which is a potent inducer of Th1-mediated immune responses resulting in the production of IFN-γ and IL-2 may re-duce atopy-associated Th2 responses.77,98-101 There is ample evidence from animal studies supporting an inverse relation of mycobacterial infection or exposure and different atopic manifestations.93,96,97 In mice models, M. vaccae or M. bovis, administered via different routes has been associated with a reduction in atopic responses.96,97 In a recent review Mat-ricardi and Yazdanbakhsh noted that of the 12 studies which evaluated the association of tuberculin response and allergic disease or atopy, no inverse association was found in 11.89 Only one study in Japanese children reported an inverse association.77 Of the 8 studies which analysed the association of BCG immunization and allergic response or atopy, none found an inverse association.89 Only one study reported a lower prevalence of allergy skin test sensitization to common environmental aeroallergens in children from Guinea Bissau immunized with BCG in infancy, suggesting a protective effect of BCG immunization ear-ly in life.78 Of the 4 reports which studied the association of TB disease or TB notiÞ cation rate and allergic disease and atopy, an inverse association was found in 3 and partial in-verse association in 1.98,102,103 In this latter study an inverse association was found between TB disease during childhood and allergic disease only in women.102
In summary, the epidemiological relation between infection with mycobacterial infec-tion and atopic disease is still controversial. A few studies observed an inverse relation, others did not. Majority of studies were conducted in westernised countries with low bur-den of M. tuberculosis infection. However, differences in study design, populations stud-ied, BCG preparations, pattern of natural exposure to M. tuberculosis or MOTT and in the deÞ nition of mycobacterial infection may partly explain differences in Þ ndings.89
Study aimWhat is the epidemiological relation between mycobacterial infection and atopic disease in low and in high tuberculosis-burden settings? (Chapters 4, 5 and 6)
Intestinal helminth infection and atopic disease
The epidemiological relation between helminthic infection and atopic disease, both as-sociated with a Th-2 immune response, is controversial, since it has been reported that helminth infection may either suppress104-107 or predispose to atopic disease.108,109 It has also

14
Infection with M. tuberculosis and atopy in children
been shown that anthelminthic treatment may inß uence atopic conditions, or modulate the severity of symptoms or sensitization.110-112 The effect of intestinal helminth infection on atopic symptoms seems to depend on the duration and intensity of infection.87,113 With chronic and intense infection, atopic symptoms may be suppressed, while mild and inter-mittent infection may result in enhanced reaction to environmental allergens and atopic re-sponse.88,114 The mechanisms to explain this effect are still not completely known. Although it has been hypothesized that polyclonal IgE produced during helminth infection may block allergic reaction by either suppressing antigen-speciÞ c IgE production or by saturation of IgE receptors on mast cells,111,114-116 other studies which demonstrated lack of saturation of mast cell capacity in vitro or in vivo argue against this mechanism.117,118 Recent evidence suggests that chronic infections, such as helminth and M. tuberculosis may lead to CD4+
Treg stimulation with subsequent production of high levels of anti-inß ammatory cytokines, which may inhibit allergic inß ammation.87 This effect may depend on the intensity and persistence of infection.87,89 With intense and persistent infection, atopic responses may be suppressed by strong stimulation of Tregs and anti-inß ammatory cytokines.87 In contrast, mild helminth infection may lead to moderate or no stimulation of anti-inß ammatory net-works and this may result in an enhanced reaction to environmental allergens and atopic response.87,89
In summary, there is evidence that helminth infection can inß uence the prevalence of atopy and this inß uence may depend on the duration and intensity of infection.
Study aimWhat is the relation between intestinal helminth co-infection and atopic disease in an area with high TB burden? (Chapter 7)
Breastfeeding in infancy and atopic disease
SpeciÞ c microbial stimuli are thought to stimulate Th1 immune responses, thus reduc-ing the activity of the atopy-associated Th2 response.77 Breast-milk inß uences the bacterial ß ora in the infant gut,119 which may provide an important immune stimulus in infancy.120 The possible protective effect of breastfeeding on atopic disease remains controversial and epidemiological studies have yielded variable results, with little information from develop-ing countries where the infection pressure and frequency of breastfeeding are higher. 121-124
The mechanisms responsible for the protective effect of breastfeeding against allergic disease are not well understood, but several factors may contribute. Breast-milk stimu-lates, through its high oligosaccharide contents, intestinal colonisation with speciÞ c bacte-rial ß ora, such as lactobacilli, biÞ dobacteria and non-pathogenic Escherichia coli which may inß uence the development of gut-driven immune responses.119,120,126-129 Gut colonisa-tion with these bacteria induces the production of Th1 cytokines, which counterbalance Th2 activity.120 This is supported by studies which have shown that atopic children are less frequently colonized with lactobacilli and biÞ dobacteria than non-atopic children.130,131 In

1 Introduction
15
addition, breast-milk may provide direct protection against allergic sensitisation through decreased exposure to food antigens, by enhanced maturation of the intestinal mucosal bar-rier and via immunoglobulins (such as secretory IgA) secreted in the milk.129,132
Study aimWhat is the relation between prolonged breastfeeding and atopic disease in an area with high TB burden? (Chapter 8)
In conclusion, in this introduction chapter of the thesis we provided an overview of the epidemiology of TB, particularly in the study area and illustrated the speciÞ c epidemio-logical aspects and diagnostic problems of TB in the pediatric population. In addition, we described the epidemiology of atopic disease in relation to infection with M. tuberculosis and co-infection with intestinal helminth within the concept of the hygiene hypothesis, and the inß uence of breastfeeding, which has been inversely associated with the development of atopic disease.
16
Infection with M. tuberculosis and atopy in children
References
1. WHO. Global tuberculosis control. Geneva, Switzerland: WHO, 2001. 2. Schwartzman K. Latent tuberculosis infection: old problem, new priorities. CMAJ 2002;
166:759-61. 3. Cantwell M, Binkin N. Impact of HIV on tuberculosis in sub-Saharan Africa: a regional perspec-
tive. Int J Tuberc Lung Dis 1997; 1:205-14. 4. UNAIDS. AIDS epidemic update. Geneva: WHO, December 2000. 5. Bothamley GH, Rowan JP, GrifÞ ths CJ, Beeks M, McDonald M, Beasley E, Van den Bosch C,
Feder G. Screening for tuberculosis: the port of arrival scheme compared with screening in gen-eral practice and homeless. Thorax 2002; 57:45-9.
6. Van Rie A, Beyers N, Gie RP, Kunneke M, Zietsman L, Donald PR. Childhood tuberculosis in an urban population in South Africa: burden and risk factor. Arch Dis Child 1999; 80:433�7.
7. Wells WF. On air-borne infection, study II, droplets and droplet nuclei. Am J Hygiene 1934; 20:611-18.
8. Louden RG, Roberts RM. Droplet expulsion from the respiratory tract. Am Rev Respir Dis 1966; 95:435-42.
9. Raviglione M, Snider D, Kochi A. Global epidemiology of tuberculosis. JAMA 1995; 273: 220-6.
10. Marais BJ, Gie RP, Schaaf HS, Hesseling AC, Obihara CC, Nelson LJ, Enarson DA, Donald PR, Beyers N. The clinical epidemiology of childhood pulmonary tuberculosis: a critical review of literature from the pre-chemotherapy era. Int J Tuberc Lung Dis 2004; 8:278-85.
11. Schluger NW, Rom WN. The host immune response to tuberculosis. Am J Respir Crit Care Med 1998; 157:679-91.
12. Sodhi A, Gong J, Silva C, Qian D, Barnes PF. Clinical correlates of interferon gamma production in patients with tuberculosis. Clin Infect Dis 1997; 25: 617-20.
13. Flynn JL, Goldstein MM, Chan J, Triebold KJ, Pfeffer K, Lowenstein CJ, Schreiber R, Mak TW, Bloom BR. Tumor necrosis factor-alpha is required in the protective immune response against Mycobacterium tuberculosis in mice. Immunity 1995; 2:561-72.
14. Bean AG, Roach DR, Briscoe H, France MP, Korner H, Sedgwick JD, Britton WJ. Structural deÞ ciencies in granuloma formation in TNF gene-targeted mice underlie the heightened suscep-tibility to aerosol Mycobacterium tuberculosis infection, which is not compensated for by lym-photoxin. J Immunol 1999; 162:3504-11.
15. Zahrt TC. Molecular mechanisms regulating persistent Mycobacterium tuberculosis infection. Microbes and Infection 2003; 5:159-67.
16. Shingadia D, Novelli V. Diagnosis and treatment of tuberculosis in children. Lancet Infect Dis 2003; 3:624-32.
17. Committee of Infectious Disease. Screening for tuberculosis in infants and children. Pediatrics 1994; 93:131�34.
18. Bellamy R, Beyers N, McAdam KP, Ruwende C, Gie R, Samaai P, Bester D, Meyer M, Corrah T, Collin M, Camidge DR, Wilkinson D, Hoal-Van Helden E, Whittle HC, Amos W, van Helden P, Hill AV. Genetic susceptibility to tuberculosis in Africans: a genome-wide scan. Proc Natl Acad Sci U S A. 2000; 97:8005-9.
19. Bellamy R. Interferon-γ and host susceptibility to tuberculosis. Am J Respir Crit Care Med 2003; 167:946-47.
20. Altare F, Durandy A, Lammas D, Emile JF, Lamhamedi S, Le Deist F, Drysdale P, Jouanguy E, DofÞ nger R, Bernaudin F, Jeppsson O, Gollob JA, Meinl E, Segal AW, Fischer A, Kumararatne D, Casanova JL. Impairment of mycobacterial immunity in human interleukin-12 receptor deÞ -ciency. Science 1998; 280:1432-5.
1 Introduction
17
21. Singh SP, Mehra NK, Dingley HB, Pande JN, Vaidya MC. Human leukocyte antigen (HLA)-linked control of susceptibility to pulmonary tuberculosis and association of HLA-DR types. J Infect Dis 1983; 148:676-81.
22. Bellamy R, Ruwende C, Corrah T, McAdam KP, Whittle HC, Hill AV. Variations in the NRAMP1 gene and susceptibility to tuberculosis in West Africans. N Engl J Med 1998; 338:640-44.
23. Bellamy R, Ruwende C, Corrah T, McAdam KP, Thursz M, Whittle HC, Hill AV. Tuberculosis and chronic hepatitis B virus infection in Africans and variation in vitamin D receptor gene. J Infect Dis 1999; 179:721-24.
24. Wilkinson RJ, Patel P, Llewelyn M, Hirsch CS, Pasvol G, Snounou G, Davidson RN, Toossi Z. Inß uence of polymorphism in the genes for the interleukin (IL)-1 receptor antagonist and IL-1 beta on tuberculosis. J Exp Med 1999; 189:1863-74.
25. Awomoyi A, Marchant A, Howson JMM, McAdam KP, Blackwell JM, Newport MJ. Interleukin-10, polymorphism in SLC11A1 (formerly NRAMP1) and susceptibility to tuberculosis. J Infect Dis 2002; 186:1808-14.
26. City of Cape Town/Metropole region TB control Programme: progress report 1997-2002. http://gw.capetown.gov.za/wcms/eDocument/TB-report-1997-2002.
27. Houwert KA, Borggreven PA, Schaaf HS, Nel E, Donald PR, Stolk J. Prospective evaluation of World Health Organization criteria to assist diagnosis of tuberculosis in children. Eur Respir J 1998; 11:1116-20.
28. Warren R, Richardson M, van der Spuy G, Victor T, Sampson S, Beyers N, van Helden P. DNA Þ ngerprinting and molecular epidemiology of tuberculosis: use and interpretation in an epidemic setting. Electrophoresis 1999; 20:1807-12.
29. Van Rie A, Warren R, Richardson M, Victor TC, Gie RP, Enarson DA, Beyers N, van Helden PD. DNA Þ ngerprinting and molecular epidemiology of tuberculosis: use and interpretation in an epidemic setting. N Engl J Med 1999; 341:1174-9.
30. National HIV and Syphilis antenatal sero-prevalence survey in South Africa 2002. The South African Department of Health. http://www.doh.gov.za/docs/reports/2002/hiv-syphilis.pdf.
31. Eamranond P, Jaramillo E. Tuberculosis in children: reassessing the need for improved diagnosis in global control strategies. Int J Tuberc Lung Dis 2001; 5:594-603.
32. Kochi A. The global tuberculosis situation and the new control strategy of the World Health Or-ganization. Tubercle 1991; 72:1-6.
33. World Health Organization. Childhood tuberculosis and BCG vaccine: EPI update supplement. Geneva: WHO, 1989.
34. Marais BJ, Gie RP, Schaaf HS, Hesseling AC, Obihara CC, Nelson LJ, Enarson DA, Donald PR, Beyers N. The natural history of childhood intra-thoracic tuberculosis � a critical review of the literature from the pre-chemotherapy era. Int J Tuberc Lung Dis 2004; 8:392-402
35. Gedde-Dahl T. Tuberculosis infection in light of tuberculin matriculation. Am J Hygiene 1952; 56:139-214.
36. Sun SJ, Bennett DE, Flood J, Loefß er AM, Kammerer S, Ellis BA. Identifying the sources of tu-berculosis in young children: a multistate investigation. Emerging Infect Dis 2002; 11:1216-23.
37. Starke JR, Jacobs RF, Jereb J. Resurgence of tuberculosis in children. J Pediatr 1992; 120:839-55.
38. Khan E, Starke J. Diagnosis of tuberculosis in children: increased need for better methods. Emerg Infect Dis 1995; 1:115-23.
39. Hesseling AC, Schaaf HS, Gie RP, Starke JR, Beyers N. A critical review of diagnostic approach-es used in the diagnosis of childhood tuberculosis. Int J Tuberc Lung Dis 2002; 6:1038-45.
40. Donald PR. Childhood tuberculosis: out of control? Curr Opin Pulm Med 2002; 8:178-82. 41. Chintu C, Mudenda V, Lucas S, Nunn A, Lishimpi K, Maswahu D, Kasolo F, Mwaba P, Bhat G,
Terunuma H, Zumla A; UNZA-UCLMS Project Paediatric Post-mortem Study Group. Lung dis-

18
Infection with M. tuberculosis and atopy in children
eases at necropsy in African children dying from respiratory illnesses: a descriptive necropsy study. Lancet 2002; 360:985-90.
42. Stryblo K. The global aspects of tuberculosis and HIV infection. Bull Int Union Tuberc Lung Dis 1990; 65:28-32.
43. Starke JR, Taylor-Watts KT. Tuberculosis in the pediatric population of Houston, Texas. Pediat-rics 1989; 84:28-35.
44. Marais BJ, Gie RP, Schaaf HS, Starke JR, Hesseling AC, Donald PR, Beyers N. A proposed radio-logical classiÞ cation of childhood intra-thoracic tuberculosis. Pediatr Radiol 2004; 34:886-94.
45. Lewinsohn DA, Gennaro ML, Scholvinck L, Lewinsohn DM. tuberculosis immunology in children: diagnostic and therapeutic challenges and opportunities. Int J Tuberc Lung Dis 2004; 8:658-74.
46. Vallejo JG, Ong LT, Starke JR. Clinical features, diagnosis, and treatment of tuberculosis in in-fants. Pediatrics 1994; 94:1-7.
47. Lifschitz M. The value of the tuberculin skin test as a screening test for tuberculosis among BCG-vaccinated children. Paediatrics 1965; 36:624-27
48. Lienhardt C, Sillah J, Fielding K, Donkor S, Manneh K, Warndorff D, et al. Risk factors for tu-berculosis infection in children with contact with infectious tuberculosis cases in The Gambia, West Africa. Pediatrics 2003; 111:e608�14.
49. Grüber C, Kulig M, Bergmann R, Guggenmoos-Holzmann I, Wahn U, the MAS-90 Study Group. Delayed hypersensitivity to tuberculin, total immunoglobulin E, speciÞ c sensitization, and atopic manifestation in longitudinally followed early Bacille Calmette-Guérin-vaccinated and non-vac-cinated children. Pediatrics 2001; 107:e36.
50. Almeida L, Barbieri M, da Paixao A, Cuevas L. Use of puriÞ ed protein derivative to assess the risk of infection in children in close contact with adults in a population with high Calmette-Guérin bacillus coverage. Paediatr Infect Dis J 2001; 20:1061-5.
51. The International Study on Asthma and allergies in Childhood (ISAAC) Steering Committee. Worldwide variations in the prevalence of asthma symptoms: the International Study on Asthma and allergies in Childhood (ISAAC). Eur Respir J 1998; 12:315-35.
52. Beasley R, Crane J, Christopher K, Lai D, Pearce N. Prevalence and etiology of asthma. J Allergy Clin Immunol 2000; 105:S466-72.
53. Mar A, Marks R. The descriptive epidemiology of atopic dermatitis in the community. Austral-asian J Dermatol 1999; 40:73-8.
54. Downs S, Marks G, Sporik R, Belosouva E, Car N, Peat J. Continued increase in the prevalence of asthma and atopy. Arch Dis Child 2001; 84:20-3.
55. Helms PJ, Christie G. Prospects for preventing asthma. Arch Dis Child 1990; 80:401-5.56. Martinez FD, Wright AL, Taussig LM, Holbert CJ, Halonen M, Morgen WJ. Asthma and wheez-
ing in the Þ rst six year of life. N Engl J Med 1995; 332:133- 8.57. Sporik R, Holgate ST, Cogswell JJ. Natural history of asthma in childhood: a birth cohort study.
Arch Dis Child 1991; 66:1050-53.58. Weitzman M, Gortmakers S, Klein Walker D, Sobol A. Maternal smoking and childhood asthma.
Pediatrics 1990; 85:505- 11.59. Kjellman N, Croner S. Cord blood IgE determination for allergy prediction: a follow-up to 7
years of age in 1661 children. Ann Allergy 1984; 53:167-71.60. Sigurs N, Bjarnason R, Sigurbergsson F, Kjellman B, Bjorksten B. Asthma and immunoglobu-
lin E antibodies after respiratory syncytial virus bronchiolitis: a prospective cohort study with matched controls. Pediatrics 1995; 95:500-5.
61. Faniran AO, Peat JK, Woolcock AJ. Prevalence of atopy, asthma symptoms and diagnosis, and the management of asthma: comparison of an afß uent and a non-afß uent country. Thorax 1999; 54:606-10.

1 Introduction
19
62. Addo Yobo EO, Custovic A, Taggart SC, Asafo-Agyei AP, Woodcock A. Exercise induced bron-chospasm in Ghana: differences in prevalence between urban and rural schoolchildren. Thorax 1997; 52:161-5.
63. Ehrlich RI, Du Toit D, Jordaan E, Volmink JA, Weinberg EG, Zwarenstein M. Prevalence and re-liability of asthma symptoms in primary school children in Cape Town. Int J Epidemiology 1995; 24:1138-45.
64. Strachnan DP. Hay fever, hygiene and household size. BMJ 1989; 299:1259-60.65. Von Mutius E, Martinez FD, Fritzsch C, Nicolai T, Roell G, Thiemann H. Prevalence of asthma and
atopy in two areas of West and East Germany. Am J Respir Crit Care Med 1994; 149:358-64. 66. Riedler J, Braun-Fahrlander C, Eder W, Schreuer M, Waser M, Maisch S, Carr D, Schierl R,
Nowak D, von Mutius E, and the ALEX study team. Exposure to farming in early life and devel-opment of asthma and allergy: a cross sectional survey. Lancet 2001; 358:1129-33.
67. Sepp E, Julge K, Vasar M, Naaber P, Björkstén B, Mikelsaar M. Intestinal microß ora of Estonian and Swedish infants. Acta Paediatr 1997; 86:956-61.
68. Krämer U, Heinrich J, Wjst M, Wichmann H-E. Age of entry to day nursery and allergy later in childhood. Lancet 1998; 352:450-54.
69. Haby M, Marks G, Peat J, Leeder S. Daycare attendance before the age of two protects against atopy in preschool age children. Pediatr Pulmonol 2000; 30:377-84.
70. Crane J, Pearce N, Shaw R, Fitzharris P, Mayes C. Asthma and having siblings. BMJ 1994; 309:272.
71. Von Mutius E, Martinez FD, Fritsch C et al. Skin test reactivity and number of siblings. BMJ 1994; 308:692-5.
72. Braun-Fahrlander CB, Riedler J, Herz U, Eder W, Waser M, Grize L, Maisch S, Carr D, Gerlach F, Bufe A, Lauener RP, Schierl R, Renz H, Nowak D, Von Mutius E. Environmental exposure to endotoxin and its relation to asthma in school-age children. N Engl J Med 2002; 347:869-77.
73. Leynaert B, Neukirch C, Jarvis D, Chinn S, Burney P, Neukirch F. Does living on a farm during childhood protect against asthma, allergic rhinitis, and atopy in adulthood? Am J Respir Crit Care Med 2001; 164:1829-34.
74. Holla AD, Roy SR, Liu AH. Endotoxin, atopy and asthma. Curr Opin Allergy Clin Immunol 2002; 2:141-5.
75. Shaheen S, Aaby P, Hall A, Barker D, Heyes C, Shiell A, Goudiaby A. Measles and atopy in Guinea-Bissau. Lancet 1996; 347:1792-6.
76. Matricardi P, Rosmini F, Ferrigno L, Nasini R, Rapicetta M, Chionne P, Stroffolini T, Pascuini P, D�Amelio R. Cross sectional retrospective study of prevalence of atopy among Italian military students with antibodies against hepatitis A virus. BMJ 1997; 314:999-1003.
77. Shirakawa T, Enomoto T, Shimazu S, Hopkin J. The inverse association between tuberculin re-sponses and atopic disorder. Science 1997;275:77-9.
78. Aaby P, Shaheen SO, Heyes CB, Goudiaby A, Hall AJ, Shiell AW, Jensen H, Marchant A. Early BCG vaccination and the reduction in atopy in Guinea-Bissau. Clin Exp Allergy 1999; 30:644-50.
79. Strannegård I, Larsson L, Wennergren G, Strannegård Ö. Prevalence of allergy in children in relation to prior BCG vaccination and infection with atypical mycobacteria. Allergy 1998; 53:249-54.
80. Ota M, van der Sande M, Walraven G, Jeffries D, Nyan O, Marchant A, McAdam KP. Absence of association between delayed type hypersensitivity to tuberculin and atopy in children in The Gambia. Clin Exp Allergy 2003; 33:731-36.
81. Wong G, Hui D, Tam C, Chan H, Fok T, Chan-Yeung M, Lai C. Asthma, atopy and tuberculin responses in chinese schoolchildren in Hong Kong. Thorax 2001; 56:770-3.
82. Omenaas E, Jentoft H, Vollmer W, Gulsvik A. Absence of relationship between tuberculin reac-

20
Infection with M. tuberculosis and atopy in children
tivity and atopy in BCG vaccinated young adults. Thorax 2000; 55:454-8. 83. Alm JS, Lilja G, Pershagen G, Scheynius A. Early BCG vaccination and development of atopy.
Lancet 1997; 350:400-3. 84. Abbas AK, Murphy KM, Sher A. Functional diversity of helper T lymphocytes. Nature 1996;
383:787-93. 85. Romagnani S. Regulation of the development of type 2 T helper cells in allergy. Curr Opin Im-
munol 1994; 6:838-46. 86. Romagnani S. Immunologic inß uences on allergy and TH1/ TH2 balance. J Allergy Clin Immu-
nol 2004; 113:395-400. 87. Yazdanbakhsh M, Van den Biggelaar, Maizels RM. Th2 responses without atopy: immuno-
regulation in chronic helminth infections and reduced allergic disease. Trends Immunol 2001; 22:372-77.
88. Matricardi PM. Infections preventing atopy: facts and new questions. Allergy 1997; 52:879-82.
89. Matricardi PM, Yazdanbakhsh M. Mycobacteria and atopy, 6 years later: a fascinating, still un-Þ nished, business. Clin Exp Allergy 2003; 33:717-720.
90. SeraÞ ni U. Do infections have a protective effect on asthma and atopy? Allergy 1997; 52:955-7.
91. Sheikh A, Smeeth L, Hubbard R. There is no evidence of an inverse relationship between TH2- mediated atopy and TH1-mediated autoimmune disorders: lack of support for the hygiene hy-pothesis. J Allergy Clin Immunol 2003; 111:131-5.
92. Bluestone JA, Abbas AK. Natural versus adaptive regulatory T cells. Nat Rev Immunol 2003; 3:253-7.
93. Zuany-Amorim C, Sawicka E, Manlius C, Le Moine A, Brunet LR, Kemeny DM, Bowen G, Rook G, Walker C. Suppression of airway eosinophilia by killed Mycobacterium vaccae-in-duced allergen-speciÞ c regulatory T-cells. Nat Med 2002; 8:625�9.
94. Mills KH. Regulatory T cells: friend or foe in immunity to infection? Nat Rev Immunol 2004; 4:841-55.
95. Trincheri G. Cytokines acting on or secreted by macrophages during intracellular infection (IL-10, IL-12, IFN-γ). Curr Opin Immunol 1997; 9:17-23.
96. Wang CC, Rook GA. Inhibition of an established allergic response to ovalbumin in BALB/c mice by killed Mycobacterium vaccae. Immunology 1998; 93:307�13.
97. Erb K, Holloway J, Sobeck A, Moll H, Le Gros G. Infection of mice with Mycobacterium bo-vis-Bacillus Calmette-Guérin (BCG) suppresses allergen-induced airway eosinophilia. J Exp Med 1998; 187:561�9.
98. Von Mutius E, Pearce N, Beasley R, Cheng S, von Ehrenstein O, Björksten B, Weiland S. International patterns of tuberculosis and the prevalence of symptoms of asthma, rhinitis and eczema. Thorax 2000; 55:449-53.
99. Von Hertzen LC, Haahtela T. Could the risk of asthma and atopy be reduced by a vaccine that induces a strong T-helper type 1 response? Am J Respir Cell Mol Biol 2000; 22:139-42.
100. Cooper A, Roberts A, Rhoades E, Callahan J, Getzy D, Orme I. The role of interleukin-12 in acquired immunity to Mycobacterium tuberculosis infection. Immunol 1995; 84:423�32.
101. Orme I, Andersen P, Boom W. T cell response to Mycobacterium tuberculosis. J Infect Dis 1993; 167:1481�97.
102. Von Hertzen L, Klaukka T, Mattila H, Haahtela T. Mycobacterium tuberculosis infection and the subsequent development of asthma and allergic conditions. J Allergy Clin Immunol 1999; 104:1211-4.
103. Shirtcliffe P, Weatherall M, Beasley R; International Study of Asthma and Allergies in Child-hood. An inverse correlation between estimated tuberculosis notiÞ cation rates and asthma
1 Introduction
21
symptoms. Respirology 2002; 7:153-5.104. Cooper PJ, Chico ME, Bland M, GrifÞ n G, Nutman B. Allergic symptoms, atopy, and geohel-
minth infections in a rural area of Ecuador. Am J Respir Crit Care Med 2003; 168:313-317.105. Nyan OA, Walraven G, Banya W, Milligan P, Van der Sande M, Ceesay SM, Del Prete G,
McAdam K. Atopy, intestinal helminth infection and total serum IgE in rural and urban adult Gambian communities. Clin Exp Allergy 2001; 31:1672-78.
106. Scrivener S, Yemaneberhan H, Zebenigus M, Tilahun D, Girma S, Ali S, McElroy P, Custovic A, Woodcock A, Pritchard D, Venn A, Britton J. Independent effects of intestinal parasite infec-tion and domestic allergen exposure on the risk of wheeze in Ethiopia: a nested case-control study. Lancet 2001; 358:1493-99.
107. Dagoye D, Bekele Z, Woldemichael K, Nida H, Yimam M, Hall A, Venn AJ, Britton JR, Hub-bard R, Lewis SA. Wheezing, allergy, and parasite infection in children in urban and rural Ethiopia. Am J Respir Crit Care Med 2003; 167:1369-73.
108. Palmer LJ, Celedón J, Weiss ST, Wang B, Fang Z, Xu X. Ascaris lumbricoides infection is asso-ciated with increased risk of childhood asthma and atopy in rural China. Am J Respir Crit Care Med 2002; 165:1489-93.
109. Joubert JR, De Klerk HC, Malan C. Ascaris lumbricoides and allergic asthma: a new perspec-tive. S Afr Med J 1979; 56:599-602.
110. Lynch NR, Palenque M, Hagel I, DiPrisco M. Clinical improvement of asthma after anthelmin-thic treatment in a tropical situation. Am J Respir Crit Care Med 1997; 156:50-54.
111. Lynch NR, Hagel I, Perez M, Di Prisco M, Lopez R, Alvarez N. Effect of anthelmintic treat-ment on the allergic reactivity of children in a tropical slum. J Allergy Clin Immunol 1993; 92:404-11.
112. Van den Biggelaar AHJ, Rodrigues LC, van Ree R, van der Zee JS, Hoeksman-Kruize YCM, Souverijn JHM, Missinou MA, Borrmann S, Kremsner PG, Yazdanbakhsh M. Long-term treat-ment of intestinal helminths increases mite skin-test reactivity in Gabonese schoolchildren. J Infect Dis 2004; 189:892-900.
113. Cooper PJ. Can intestinal helminth infections (geohelminths) affect the development and ex-pression of asthma and allergic disease? Clin Exp Immunol 2002; 128:398-404.
114. Mitre E, Norwood S, Nutman TB. Saturation of immunoglobulin E (IgE) binding sites by poly-clonal IgE does not explain the protective effect of helminth infections against atopy. Infect Im-mun 2005; 73:4106-11.
115. Godfrey RC, Gradidge CF. Allergic sensitization of human lung fragments prevented by satura-tion of IgE binding sites. Nature 1976; 259:484-486.
116. Hagel I, Lynch NR, DiPrisco MC, Lopez R, Garcia N. Allergic reactivity of children of different socio-economic levels in tropical populations. Int Arch Allergy Immunol 1993; 101:209-214.
117. Larrick JW, Buckley CF, Machamer CE, Schlagel GD, Yost JA, Blessing-Moore J, Levy D. Does hyperimmunoglobulinemia-E protect tropical populations from allergic disease? J Allergy Clin Immunol 1983; 71:184-88.
118. Van den Biggelaar AH, van Ree R, Rodriguez LC, Lell B, Deelder AM, Kremsner PG, Yazdan-bakhsh M. Decreased atopy in children infected with Schistosoma haematobium: role for para-site-induced interleukin-10. Lancet 2000; 356:1723-27.
119. Yashioka H, Fujita F. Development and differences of intestinal ß ora in neonatal period of breast-fed and bottle-fed infants. Pediatrics 1983; 72:317-21.
120. Hessle C, Hanson A, Wold AE. Lactobacilli from human gastrointestinal mucosa are strong stimulators of IL-12 production. Clin Exp Immunol 1999; 116:276-82.
121. Saarinen UM, Kajosaari M, Backman A, Siimes MA. Prolonged breastfeeding as prophylaxis for atopic disease. Lancet 1979; 2:163-6.
122. Saarinen UM, Kajosaari M. Breastfeeding as prophylaxis against atopic diseases: prospective
22
Infection with M. tuberculosis and atopy in children
follow-up until 17 years old. Lancet 1995; 346:1065-69. 123. Wright AL, Holberg CJ, Taussig LM, Martinez FD. Relationship of infant feeding to recurrent
wheezing at age 6 years. Arch Pediatr Adolesc Med 1995; 149:758-763.124. Sears M, Greene J, Willan A, Taylor DR, Flannery EM, Cowan JO, Herbison GP, Poulton R.
Long-term relation between breastfeeding and development of atopy and asthma in children and young adults: a longitudinal study. Lancet 2002; 360:901-07.
125. Rook G, Stanford J. Give us this day our daily germs. Immunol Today 1998; 19:113-6.126. Sepp E, Julge K, Vasar M, Naaber P, Björkstén B, Mikelsaar M. Intestinal microß ora of Esto-
nian and Swedish infants. Acta Paediatr 1997; 86:956-61.127. Lodinová R, Jouja V. Antibody production by mammary gland in mothers after artiÞ cial oral
colonization of their infants with non-pathogenic strain E. coli. Acta Paediatr Scand 1977; 66:705-8.
128. Prescott SL, Macaubas C, Holt BJ, Smallacombe TB, Loh R, Sly PD, Holt PG. Transplacental priming of the human immune system to environmental allergens: universal skewing of initial T cell responses toward the Th2 cytokine proÞ le. J. Immunol 1998; 160:4730-37.
129. Hoppu U, Kalliomäki M, Laiho K, Isolauri E. Breast milk � immunomodulatory signals against allergic diseases. Allergy 2001; 56(Suppl 67):23-6.
130. Björkstén B, Naaber P, Sepp E, Mikelsaar M. The intestinal microß ora in allergic Estonian and Swedish 2-year-old children. Clin Exp Allergy 1999; 29:342-46.
131. Kalliomäki M, Seppo S, Arvilommi H, Kero P, Koskinen P, Isolauri E. Probiotics in primary pre-vention of atopic disease: a randomised placebo-controlled trial. Lancet 2001; 357:1076-79.
132. Brandtzaeg P. Current understanding of gastrointestinal immunoregulation and its relation to food allergy. Ann N.Y. Acad Sci 2002; 964:13-45.

C H A P T E R 2
The clinical epidemiology of childhood pulmonary tuberculosis: a critical review of literature from the pre-chemotherapy era
Ben J. MaraisRobert P. GieH.Simon SchaafAnneke C. HesselingCharles C. ObiharaLisa. J. NelsonDonald A. EnarsonPeter R. DonaldNulda Beyers
International Journal of Tuberculosis and Lung Disease2004; 8:278-285

24
Infection with M. tuberculosis and atopy in children
Abstract
The pre-chemotherapy literature represents an impressive body of evidence that clari-Þ es important epidemiological concepts in childhood tuberculosis (TB). Reports describe the major transitions in TB; from exposure to infection and from infection to disease (mor-bidity and mortality), without the inß uence of chemotherapy. Children with household exposure to a sputum smear-positive source case experienced the greatest risk to become infected and of developing subsequent disease. Household exposure to a sputum smear-negative source case or non-household exposure still posed an appreciable, although greatly reduced, risk. Infection in children less than 2 years of age indicated a probable household source case. The majority of older children who were infected did not have a household source identiÞ ed and presumably became infected in the community. The annual risk of infection (ARI) was not constant across all ages, but seemed to increase during periods of widening social contact. Infants and adolescents were the groups at highest risk for disease development and death following primary infection.

2 The clinical epidemiology of childhood pulmonary tuberculosis
25
Introduction
The twentieth century witnessed major advances in the understanding of the pathophys-iology of childhood tuberculosis (TB) as well as its diagnosis and treatment. In particular, the period from 1920, when chest radiography became available for diagnosis, to 1950, when effective chemotherapy became available, represented an optimal window for the documentation of the natural history of TB.
During this period TB was still highly prevalent in Europe and America, where ad-equate infrastructure allowed the careful diagnosis and follow-up of TB patients. Detec-tion of infection was possible with the tuberculin skin test (TST), while chest radiography allowed a more accurate diagnosis of pulmonary TB in children.
The aim of this review is to document the Þ ndings from the pre-chemotherapy litera-ture, concerning the clinical epidemiology of childhood pulmonary TB, in a critical man-ner. The relevance of these historic Þ ndings is interpreted for the public health challenges faced today.
Methods and materials
Original studies on childhood pulmonary TB, including the period 1920 to 1950 and published in the English literature, were identiÞ ed from textbook references and extensive cross-referencing. Only studies reporting on more than 1000 children, with maximum fol-low-up periods of at least 10 years were included. 1-8 The database collected was compared to the International Union Against TB and Lung Disease (IUATLD) archive in order to en-sure that no major study was excluded. One exception was made with the inclusion of To-bias Gedde-Dahl�s community based article on tuberculin conversion. He followed patients for a maximum of 8 years, before the Second World War interrupted the study. However, his unique approach provided valuable insight by documenting tuberculin conversion and sub-sequent disease development in the community. Hospital-based studies introduced bias by pre-selection and therefore the inclusion of community-based studies was essential. Studies are reported in chronological order to illustrate the progression in knowledge. This review summarizes the clinical epidemiological aspects of pulmonary TB in children. During this same period, basic science studies also improved the understanding of the epidemiology of TB by the accurate description of droplet airborne infection. These studies have been re-viewed previously and are not included.9
A brief description of the individual studies and the study design employed in each is provided. (Table 1) This is followed by a summary of the key Þ ndings and major limita-tions of each individual study. (Table 2) The combined study results summarize the most important Þ ndings; with reference to the individual studies described in tables 1 and 2.
The risk of developing disease (morbidity) or of dying from TB (mortality), follow-ing primary infection within a speciÞ c age group, was calculated from the original data reported by Bentley et al.5 (Table 3). The percentage of children who developed primary infection within a speciÞ c age period, was calculated by deducting the cumulative percent-
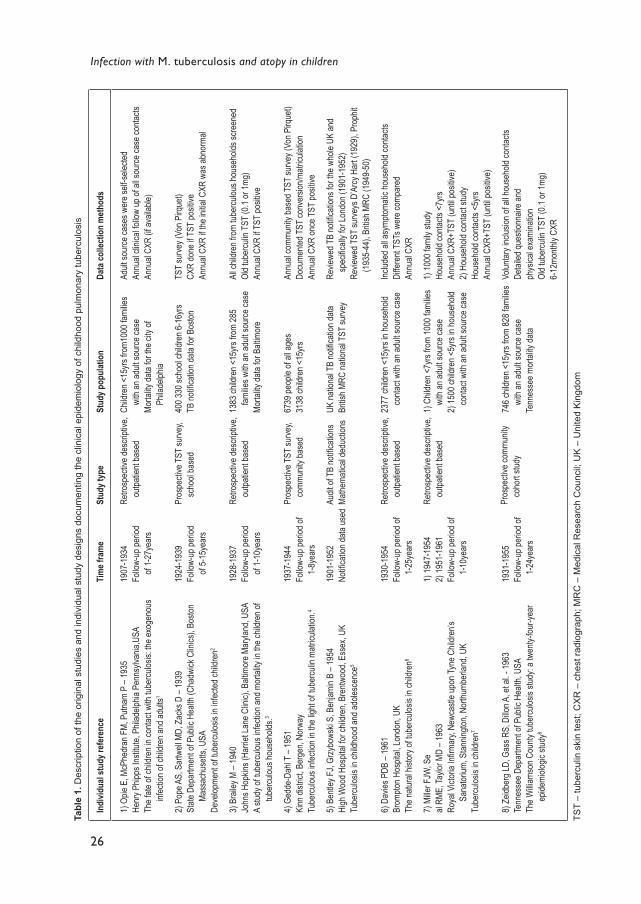
26
Infection with M. tuberculosis and atopy in childrenTa
ble
1. D
escr
iptio
n of
the
orig
inal
stu
dies
and
indi
vidu
al s
tudy
des
igns
doc
umen
ting
the
clin
ical
epi
dem
iolo
gy o
f chi
ldho
od p
ulm
onar
y tu
berc
ulos
is
Indi
vidua
l stu
dy re
fere
nce
Tim
e fra
me
Stud
y typ
eSt
udy p
opul
atio
nDa
ta co
llect
ion
met
hods
1) O
pie E
, McP
hedr
an F
M, P
utnam
P �
1935
Henr
y Phip
ps In
stitut
e, Ph
ilade
lphia
Penn
sylva
nia,U
SATh
e fate
of ch
ildre
n in c
ontac
t with
tube
rculos
is: th
e exo
geno
us
infec
tion o
f chil
dren
and a
dults
1
2) P
ope A
S, S
artw
ell M
D, Z
acks
D �
1939
State
Dep
artm
ent o
f Pub
lic H
ealth
(Cha
dwick
Clin
ics),
Bosto
n Ma
ssac
huse
tts, U
SADe
velop
ment
of tub
ercu
losis
in inf
ected
child
ren2
3) B
raile
y M �
1940
John
s Hop
kins (
Harri
et La
ne C
linic)
, Balt
imor
e Mar
yland
, USA
A stu
dy of
tube
rculou
s infe
ction
and m
ortal
ity in
the c
hildr
en of
tub
ercu
lous h
ouse
holds
.3
4) G
edde
-Dah
l T �
1951
Kinn
distr
ict, B
erge
n, No
rway
Tube
rculou
s infe
ction
in th
e ligh
t of tu
bercu
lin m
atricu
lation
.4
5) B
entle
y FJ,
Grzy
bows
ki S,
Ben
jamin
B � 1
954
High
Woo
d Hos
pital
for ch
ildre
n, Br
entw
ood,
Esse
x, UK
Tube
rculos
is in
child
hood
and a
doles
cenc
e5
6) D
avies
PDB
� 19
61Br
ompto
n Hos
pital,
Lond
on, U
KTh
e natu
ral h
istor
y of tu
bercu
losis
in ch
ildre
n6
7) M
iller F
JW, S
eal
RME,
Taylo
r MD
� 196
3Ro
yal V
ictor
ia InÞ
rmar
y, Ne
wcas
tle up
on Ty
ne C
hildr
en�s
Sana
torium
, Stan
ningto
n, No
rthum
berla
nd, U
KTu
bercu
losis
in ch
ildre
n7
8) Z
eidbe
rg LD
, Gas
s RS,
Dillo
n A, e
t al. -
1963
Tenn
esse
e Dep
artm
ent o
f Pub
lic H
ealth
, USA
The W
illiam
son C
ounty
tube
rculos
is stu
dy: a
twen
ty-fou
r-yea
r ep
idemi
ologic
stud
y8
1907
-193
4Fo
llow-
up pe
riod
of 1-
27ye
ars
1924
-193
9Fo
llow-
up pe
riod
of 5-
15ye
ars
1928
-193
7Fo
llow-
up pe
riod
of 1-
10ye
ars
1937
-194
4Fo
llow-
up pe
riod o
f 1-
8yea
rs
1901
-195
2 No
tiÞ ca
tion d
ata us
ed
1930
-195
4Fo
llow-
up pe
riod o
f 1-
25ye
ars
1) 19
47-1
954
2) 19
51-1
961
Follo
w-up
perio
d of
1-10
year
s
1931
-195
5Fo
llow-
up pe
riod o
f 1-
24ye
ars
Retro
spec
tive d
escri
ptive
, ou
tpatie
nt ba
sed
Pros
pecti
ve T
ST su
rvey,
scho
ol ba
sed
Retro
spec
tive d
escri
ptive
, ou
tpatie
nt ba
sed
Pros
pecti
ve T
ST su
rvey,
comm
unity
base
d
Audit
of T
B no
tiÞ ca
tions
Mathe
matic
al de
ducti
ons
Retro
spec
tive d
escri
ptive
, ou
tpatie
nt ba
sed
Retro
spec
tive d
escri
ptive
, ou
tpatie
nt ba
sed
Pros
pecti
ve co
mmun
ity
coho
rt stu
dy
Child
ren <
15yrs
from
1000
fami
lies
with
an ad
ult so
urce
case
Morta
lity da
ta for
the c
ity of
Ph
ilade
lphia
400 3
30 sc
hool
child
ren 6
-16y
rs TB
notiÞ
catio
n data
for B
oston
1383
child
ren <
15yrs
from
285
familie
s with
an ad
ult so
urce
case
Morta
lity da
ta for
Balt
imor
e
6739
peop
le of
all ag
es31
38 ch
ildre
n <15
yrs
UK na
tiona
l TB
notiÞ
catio
n data
Britis
h MRC
natio
nal T
ST su
rvey
2377
child
ren <
15yrs
in ho
useh
old
conta
ct wi
th an
adult
sour
ce ca
se
1) C
hildr
en <
7yrs
from
1000
fami
lies
with
an ad
ult so
urce
case
2) 15
00 ch
ildre
n <5y
rs in
hous
ehold
co
ntact
with
an ad
ult so
urce
case
746 c
hildr
en <
15yrs
from
828 f
amilie
s wi
th an
adult
sour
ce ca
seTe
nnes
see m
ortal
ity da
ta
Adult
sour
ce ca
ses w
ere s
elf-se
lected
Annu
al cli
nical
follow
up of
all s
ource
case
conta
ctsAn
nual
CXR
(if av
ailab
le)
TST
surve
y (Vo
n Pirq
uet)
CXR
done
if TS
T po
sitive
An
nual
CXR
if the
initia
l CXR
was
abno
rmal
All c
hildr
en fr
om tu
bercu
lous h
ouse
holds
scre
ened
Old t
uber
culin
TST
(0.1
or 1m
g)
Annu
al CX
R if T
ST po
sitive
Annu
al co
mmun
ity ba
sed T
ST su
rvey (
Von P
irque
t)Do
cume
nted T
ST co
nver
sion/m
atricu
lation
An
nual
CXR
once
TST
posit
ive
Revie
wed T
B no
tiÞ ca
tions
for t
he w
hole
UK an
d sp
eciÞ c
ally f
or Lo
ndon
(190
1-19
52)
Revie
wed T
ST su
rveys
D�A
rcy H
art (
1929
), Pr
ophit
(1
935-
44),
Britis
h MRC
(194
9-50
)
Includ
ed al
l asy
mptom
atic h
ouse
hold
conta
ctsDi
ffere
nt TS
Ts w
ere c
ompa
red
Annu
al CX
R
1) 10
00 fa
mily
study
Hous
ehold
conta
cts <
7yrs
Annu
al CX
R+TS
T (u
ntil p
ositiv
e)2)
Hou
seho
ld co
ntact
study
Hous
ehold
conta
cts <
5yrs
Annu
al CX
R+TS
T (u
ntil p
ositiv
e)
Volun
tary i
nclus
ion of
all h
ouse
hold
conta
ctsDe
tailed
ques
tionn
aire a
ndph
ysica
l exa
mina
tion
Old t
uber
culin
TST
(0.1
or 1m
g)6-
12mo
nthly
CXR
TST
� tu
berc
ulin
ski
n te
st; C
XR
� c
hest
radi
ogra
ph; M
RC
� M
edic
al R
esea
rch
Cou
ncil;
UK
� U
nite
d K
ingd
om

2 The clinical epidemiology of childhood pulmonary tuberculosis
27
Tabl
e 2.
Sum
mar
y of
key
Þ nd
ings
and
maj
or li
mita
tions
of t
he o
rigin
al s
tudi
es, d
ocum
entin
g th
e cl
inic
al e
pide
mio
logy
of c
hild
hood
pul
mon
ary
tube
rcul
osis
Cita
tion
Feat
ures
Key F
indi
ngs
Majo
r Lim
itatio
ns
Opie
et al.
Pope
et al
.
Brail
ey
Gedd
e-Da
hl
Bentl
ey et
al.
Davie
s
Mille
r et a
l.
Zeidb
erg e
t al.
First
to foc
us on
fami
lies a
nd
child
ren
TST
posit
ivity
Scho
ol su
rvey
Focu
s on c
hildr
en <
2yrs
of ag
e Ra
cial C
ompa
rison
TST
conv
ersio
nCo
mmun
ity su
rvey
Tube
rculos
is dis
ease
and
morta
lity sp
eciÞ e
d per
ag
e gro
upCo
ncep
t of r
elativ
e co
ntribu
tion
Long
term
follo
w-up
Persi
stenc
e of T
ST
conv
ersio
n
Comp
rehe
nsive
l lite
ratur
e re
view
Long
term
follo
w-up
in th
e co
mmun
ity
Sputu
m po
sitive
expo
sure
incre
ased
the f
requ
ency
and s
ever
ity of
dise
ase i
n ch
ildho
od co
ntacts
The l
ifetim
e risk
for t
he de
velop
ment
of ca
vitati
ng di
seas
e dep
ende
d on t
he ag
e at
prim
ary i
nfecti
on, in
creas
ing si
gniÞ c
antly
after
10 ye
ars o
f age
Only
30%
of in
fected
scho
ol ch
ildre
n had
hous
ehold
conta
ct wi
th a k
nown
sour
ce
case
Cavit
ating
pulm
onar
y tub
ercu
losis
was o
nly se
en in
child
ren o
lder t
han 1
0 yea
rs of
age
Infec
ted ch
ildre
n <2 y
ears
of ag
e ind
icated
an ac
tive h
ouse
hold
sour
ce ca
seTh
e majo
rity of
hous
ehold
conta
cts w
ere i
nfecte
d with
in 3 m
onths
of sy
mptom
on
set in
the a
dult s
ource
case
No ra
cial d
iffere
nce i
n infe
ction
follo
wing
expo
sure
DeÞ n
ite ra
cial d
iffere
nce i
n dise
ase a
nd m
ortal
ity fo
llowi
ng in
fectio
n
The r
ate of
TB
infec
tion a
nd T
B re
lated
mor
tality
was
incre
ased
in ur
ban a
reas
Radio
logica
l abn
orma
lities
wer
e visi
ble in
75%
of of
child
ren f
ollow
ing pr
imar
y TB
infec
tion
The a
nnua
l rate
of inf
ectio
n (AR
I) wa
s not
cons
tant, b
ut va
ried b
etwee
n diffe
rent
age g
roup
sTh
e majo
rity (9
0%) o
f TB-
relat
ed ra
diolog
ical a
bnor
maliti
es w
ere n
ot de
tected
in
routi
ne cl
inica
l pra
ctice
The r
isk of
dise
ase a
nd de
ath fo
llowi
ng in
fectio
n was
the h
ighes
t dur
ing in
fancy
The r
elativ
e con
tributi
on of
TB
to ag
e spe
ciÞ c
all-ca
use m
ortal
ity w
as th
e low
est
durin
g infa
ncy
TB co
ntribu
ted si
gniÞ c
antly
to al
l-cau
se m
ortal
ity th
roug
hout
child
hood
The M
antou
x skin
test
outpe
rform
ed ot
her T
STs
A po
sitive
tube
rculin
resp
onse
persi
sted f
or >
20ye
ars
Expo
sure
to a
sputu
m sm
ear-p
ositiv
e vs a
smea
r-neg
ative
sour
ce ca
se do
ubled
the
risk o
f infec
tion
Infec
tion a
fter e
xpos
ure t
o a sp
utum
smea
r-pos
itive s
ource
case
doub
led th
e risk
for
dise
ase a
nd de
ath.
Clar
iÞ ed t
he co
nfusio
n sur
roun
ding t
he in
terpr
etatio
n of d
iffere
nt tub
ercu
lin sk
in tes
t tech
nique
s and
dose
sDe
scrib
ed th
e imp
ortan
ce of
cultu
ral in
ß uen
ces a
nd th
e exte
nded
fami
lyVi
ral re
spira
tory i
nfecti
ons m
ight h
ave c
ontrib
uted t
o the
seas
onal
varia
tion i
n TB
infec
tion
Identi
Þ ed c
ritica
l per
iods o
f risk
for d
iseas
e dev
elopm
ent (
infan
cy, p
uber
ty)Do
cume
nted a
dras
tic re
ducti
on in
TB
relat
ed di
seas
e and
mor
tality
over
the 2
4 ye
ar st
udy p
eriod
in bl
ack p
atien
ts
Tube
rculin
skin
test n
ot re
cord
edAg
e gro
ups p
oorly
deÞ n
ed
Limite
d CXR
avail
abilit
ySp
utum
posit
ivity
not s
peciÞ
ed (s
mear
or cu
lture
)
Tube
rculin
skin
test c
onve
rsion
not r
ecor
ded
Selec
tive f
ollow
-up (
only
those
with
initia
l che
st ra
diogr
aph a
bnor
maliti
es w
ere
follow
ed)
Docu
mente
d cav
itatin
g dise
ase o
nly
Publi
c hea
lth en
try po
int se
lected
the p
oor
Resp
onse
to hi
gh do
se (1
mg) t
uber
culin
, use
d in a
small
mino
rity of
patie
nts, is
no
t spe
ciÞ c
for M
. tub
ercu
losis
infec
tion
Sputu
m po
sitivi
ty no
t spe
ciÞ ed
(sme
ar or
cultu
re)
Socio
-eco
nomi
c diffe
renc
es w
ere n
ot ev
aluate
d
Pre-
scho
ol ch
ildre
n wer
e sele
ctive
ly re
pres
ented
(only
conta
cts an
d sym
ptom-
atic c
ases
inclu
ded)
Resu
lts fr
om th
is iso
lated
comm
unity
may
be di
fÞ cult
to ge
nera
lize
Resp
onse
to hi
gh do
se (1
00 T
U) tu
bercu
lin, u
sed i
n 24%
of su
bjects
in th
e Br
itish M
RC su
rvey,
is no
t spe
ciÞ c
for M
.tube
rculo
sis in
fectio
nRe
lied e
xclus
ively
on T
B no
tiÞ ca
tion d
ata fo
r dise
ase a
nd m
ortal
ity an
alysis
Major
ity of
patie
nts w
ere a
lread
y infe
cted a
t stud
y entr
ySe
lected
only
asym
ptoma
tic ch
ildre
n at s
tudy e
ntry,
in or
der t
o ens
ure c
linica
l un
iform
ity
Few
dedu
ction
s wer
e mad
e fro
m ow
n stud
iesVa
lidity
of qu
oted s
tudies
wer
e not
evalu
ated
Relie
d exte
nsive
ly on
notiÞ
catio
n data
Age a
t prim
ary i
nfecti
on w
as no
t doc
umen
tedEn
try cr
iteria
wer
e ada
pted d
uring
the s
tudy
A co
ntrov
ersia
l Þ nd
ing, n
ot su
ppor
ted by
mor
tality
data
or re
sults
from
othe
r stu
dies r
eview
ed, w
as th
e dela
yed p
rogr
essio
n of d
iseas
e rep
orted
in
child
ren i
nfecte
d betw
een 1
-15y
ears
of ag
e
TST
� tu
berc
ulin
ski
n te
st; C
XR
� c
hest
radi
ogra
ph; M
RC
� M
edic
al R
esea
rch
Cou
ncil;
TU
� tu
berc
ulin
uni
ts

28
Infection with M. tuberculosis and atopy in children
age of children with a positive TST recorded at entry, from the cumulative percentage of children with a positive TST at exit from that age category. Multiplying this percentage with the average number of children who entered that age category annually provided an estimate of the number of children who developed primary infection within that age period. This number was used as denominator. The annual number of notiÞ cations for TB-related disease and death within that age group was used as numerator when calculating the dis-ease and mortality percentages. (Table 3)
Combined study results
Exposure to infection The Mantoux TST using 5 tuberculin units (TU) was identiÞ ed as the optimal test to
indicate TB infection.6,7 The use of different techniques and tuberculin strengths, compli-cated the interpretation of TST results and comparison between studies.7 Reaction to high-dose tuberculin (1 mg or 100 TU) only, probably represented exposure to environmen-
Table 3. The calculated risk of developing primary tuberculosis (TB) infection, compared to the calculated risk of being notiÞ ed with TB-related disease or death following primary TB infection, within speciÞ c age groups.
Age group (years)
Calculated risk to develop primary TB infection * (%)
Calculated risk to be notiÞ ed with TB-related disease, following primary TB infection �(%)
Calculated risk to be notiÞ ed with TB-related death, following primary TB infection �(%)
Relative TB-related mortality §(%)
<1 <1% 11.9% 6% 0.6% 1�4 10% 5.6% 1% 12.1% 5�9 20% 3.8% 0.3% 9.1%10�14 10% 6.4% 0.5% 9.1%15�24 30% 10% males
13% females1.5% males2.6% females
16.7% males39.4% females
* Indicates the calculated percentage of children who develop primary infection (TST conversion) within a speciÞ c age group.� Indicates the number of children notiÞ ed with TB, as a percentage of the total number expected to have developed primary TB infection, within a speciÞ c age group.� Indicates the number of children notiÞ ed with death due to TB, as a percentage of the total number expected to have developed primary TB infection within a speciÞ c age group.§ Indicates the percentage of TB-related mortality compared to all-cause mortality within a speciÞ c age group.Data on primary TB infection was collected from the British MRC tuberculin skin test survey for London (1949-1950).5 This was converted into the number of children expected to develop primary infection within a speciÞ c age group, using national census data for London (1951). Data on TB-related disease and death was collected from TB notiÞ cations and death certiÞ cates for London (1945-1949).5 Absolute notiÞ cation numbers were converted into percentages, using the expected number to develop primary infection within a speciÞ c age group as numerator and accepting that all notiÞ cations result from recent primary infection. Relative TB-related mortality was calculated from death certiÞ cates for England and Wales (1950), comparing TB-related mortality with all-cause mortality.5

2 The clinical epidemiology of childhood pulmonary tuberculosis
29
tal mycobacteria and not infection with Mycobacterium tuberculosis (M. tuberculosis).7,8 High-dose tuberculin was used following a negative reaction to standard-dose tuberculin in three of the studies.3,5,8 Those with a positive reaction to high-dose tuberculin were in-cluded amongst the infected group without further sub-analysis, but they represented a small minority. The degree of induration induced by BCG vaccination was usually less than 10 mm, compared to natural infection, which was usually more than 10 mm.7 BCG-induced hypersensitivity diminished with time and TST responses reverted after variable time periods, depending on the BCG strain used. After natural infection, permanent rever-sion occurred in less than 0.5% of children.4,6-8 Temporary inhibition of TST responses did occur and was associated with malnutrition, viral illnesses or severe forms of TB.7
Following prolonged household contact with a sputum smear-positive source case, 60�80% of children became infected.3,6-8 When the source case was smear-negative, 30�40% of children became infected.4,7,8 The probability of infection in children depended on the infectivity of the source case together with the proximity and duration of contact with the source case. Local cultural practices, e.g. extensive socialisation within rural African vil-lages or the isolation of children and women in certain cultures, may have contributed to different epidemiological patterns of disease spread.7 Miriam Brailey was the only author who related the time of TST conversion in the child contact to the time of symptom on-set in the adult source case. More than 60% of the children who became infected, did so within 3 months of symptom onset in the adult source case.3 Infection was often delayed in household contacts under 2 years of age compared to older children, suggesting some protection from their reduced social contact within the family.3 This observation was not evaluated separately when the primary caregiver was the source case, in which case it might be expected that this delay will not exist. Viral upper respiratory tract infections may have increased the likelihood of TB infection and contributed to the observed peak in infec-tion during winter months.7
Most children (80%) who became infected before 2 years of age were infected by a household source case.3,5,7 Additional caregivers outside the household were also impor-tant, especially grandparents or extended family members who took care of the children during the day, if both parents worked.7 The majority of children who became infected after 2 years of age had no household contact identiÞ ed, and were therefore likely to have been infected in the community.2,3,5,7,8
A separate issue raised by these studies was how the contribution of household exposure to primary infection, varied according to the prevalence of TB in a speciÞ c community. In high prevalence areas, household exposure contributed to primary infection up until 15 years of age, by which time most children were already infected.5,8 In low prevalence areas household exposure remained an important contributor to primary infection until old age.5,8 The risk of infection following household exposure was reduced under good socio-economic conditions.5,8 There were no racial differences in the rate of infection following household exposure.3,8
The annual risk of infection (ARI) was not constant across all ages.5,7 There were specif-ic age periods when infection rates increased.5 These age periods seemed to correlate with times of widening social contact. This occurred with increased mobility after 2 years of

30
Infection with M. tuberculosis and atopy in children
age, school entry at 5 to 7 years of age and school exit at 15 to 20 years of age5,7 (Table 3). Primary infection occurred at a younger age in low-income, urban areas with a high popu-lation density.4-7 The age-speciÞ c infection rate was the single most important public health indicator of the prevalence of disease in a given community.5,7,8
Infection to disease (Morbidity)To describe the progression from infection to disease accurately, a clear case deÞ nition
of disease is required. DeÞ nitions of disease were poor and inconsistent. NotiÞ cation data, reporting any radiological abnormality attributed to TB as disease, was used routinely. Cases were identiÞ ed after either active or passive case Þ nding.
With constant community surveillance and active case Þ nding it was found that a high percentage of children (50�70%) developed radiological abnormalities following primary infection. This was most common (60-�80%) following primary infection before 2 years of age.3-5 On comparison with notiÞ cation data, it was clear that only 5-10% of children who developed radiological abnormalities during the natural course of the disease, were noti-Þ ed as diseased (Table 3). This implied that more than 90% of radiological abnormalities passed undetected in routine clinical practice and is probably transient.5,7
The risk of radiological abnormality in children with household exposure to a sputum smear-positive source case and a positive TST was 30�50%.1,4,6-8 This risk was reduced by 50% when the source case was sputum smear-negative or not a household member.1,4,6-8
Duration since primary infection and age at primary infection determined the risk for dis-ease development.4,5,7 Nearly all disease developed within the Þ rst year following primary infection.1,3,4,5,7 Children with primary infection before 2 years or after 10 years of age5,7 and black children1,3,7,8 were at increased risk for disease development. This increased suscepti-bility of black children declined drastically during the Tennessee study, as socio-economic conditions improved.8
The risk to develop cavitating pulmonary TB depended on the age at primary infection. The highest risk for cavitating disease (10�20%) occurred in children who were Þ rst in-fected after 10 years of age, with peri-menarchal girls being most vulnerable.1,2,5-8
Mortality TB-related mortality following infection from a sputum smear-positive household
source case was twice as high as when infection occurred from an unknown source case.6-8 All-cause mortality was similar in both groups, indicating that the difference was not due to general increased mortality in the households of sputum smear-positive patients.1,3,7,8 The highest risk for TB-related mortality following primary infection (5�10%), occurred during infancy.1,3-5,7,8 This risk declined to 1% between 1 to 4 years of age, with the lowest levels maintained at less than 0.5% from 5 to14 years of age, before rising to more than 2% from 15 to 25 years of age.5,7 (Table 3) Most deaths from TB occurred within the Þ rst year following primary infection in children under 10 years of age,1,3,4,5,7 but mortality lagged further behind the onset of cavitating disease in older children.8
All-cause mortality exhibited a similar age-related pattern as TB-related mortality.5 Therefore, the relative TB-related mortality best described the impact of TB on all-cause

2 The clinical epidemiology of childhood pulmonary tuberculosis
31
mortality within a speciÞ c age group.5 TB contributed signiÞ cantly to all-cause mortality in all age groups, except in infancy.3,5 The low rate of infection and the high mortality from other causes during infancy explain this contradiction3,5,8 (Table 3). Urbanised, densely populated areas suffered increased mortality both from TB and other causes.4,6
Black children suffered double the TB-related mortality and four times the all-cause mortality compared to white children.3,7,8 The TB-related mortality in black children de-clined by 80% during the course of the Tennessee study.8 A 10-fold decline in TB-related mortality occurred in Britain between 1900 and 1950, without a comparable decrease in TB infection.5,7
Discussion
The combined studies represent an impressive body of evidence and clarify some im-portant epidemiological concepts in childhood TB. Household exposure to a sputum smear-positive source case posed the greatest risk to children. Household exposure to a sputum smear-negative source case or non-household exposure to a sputum smear-positive source case posed a reduced, but still appreciable risk.
It is a public health priority to identify and treat all sputum smear-positive source cases in the community. Therefore, prudent public health policy should encourage active case Þ nding amongst household members of children infected before 2 years of age, as part of an expanded (�reverse�) contact investigation. In low prevalence areas this active case Þ nding may be extended to household members of all recently infected or diseased chil-dren, irrespective of their age.
After 2 years of age, the majority of children from high prevalence areas became in-fected in the community. However, household exposure to a sputum smear-positive source case remained an important contributor to primary infection up until 5�10 years of age. Children with primary infection at 5�10 years of age had the lowest risk of disease de-velopment and death. In low-prevalence areas household exposure remains an important contributor to primary infection throughout life and all household contacts, irrespective of age, require screening. These studies provided the scientiÞ c basis for classical contact in-vestigation practices, which focus on children less than 5 years of age in most developing countries and all household contacts in most industrialised countries.
Another public health priority is the identiÞ cation of children at risk of disease devel-opment and death. The calculated risk for disease development and death following pri-mary infection within a speciÞ c age group represents a re-interpretation of original data as outlined under methods (Table 3). Infants were at highest risk of disease development and death following primary infection. However, the use of accumulated TST positivity as denominator in the original publication,5 instead of TST converters within a speciÞ c age group, obscured the emergence of the second high-risk period around puberty. Children who were uninfected at 10 years of age were at considerable risk to develop adult-type cav-itating disease following primary infection. This marked increase in risk may be obscured by analysis of notiÞ cation data, due to the delay in disease notiÞ cation that results from
32
Infection with M. tuberculosis and atopy in children
passive case Þ nding in adult-type disease. Disease and mortality data for the age group 15 to 25 years probably contain a signiÞ cant contribution from delayed disease notiÞ cation, following primary infection in the 10 to 14 year age group (Table 3).
Previously uninfected adolescents, is a particularly vulnerable group, especially in high-prevalence communities where the risk of future infection is high. Performing a TST at 7�10 years of age will identify most children who are still uninfected. Effective immuni-zation or active case Þ nding may be warranted in this vulnerable group to reduce individual morbidity and disease transmission within the community. Children with a positive TST, without prior anti-TB treatment, may be offered treatment of latent infection to eliminate the risk of possible future re-activation.
The relative TB-related mortality indicates that TB contributes signiÞ cantly to all-cause mortality in high burden areas, throughout childhood. Although the relative contribution to all-cause mortality is the lowest in infancy, this does not detract from the important obser-vation that infected infants represent the group at highest risk of death from TB.
It is difÞ cult to separate racial and genetic factors from socio-economic and cultural inß uences. However, the dramatic decline in disease and mortality documented within a single generation, without a comparable decrease in infection,5,8 emphasises the consider-able inß uence of socio-economic improvement. This is contrary to the natural selection view proposed by Grigg in his inß uential article, �The Arcana of Tuberculosis� (1958).10 The nature versus nurture issue is complex, and is far from resolved,11 but improvement in the environment rather than genetic selection seems to be the main contributor to the dra-matic reduction in TB witnessed in the developed world during the 20th century.
Important limitations of the individual studies were identiÞ ed and although the com-bined study results compensate for many of the individual study deÞ ciencies, major lim-itations remain. Different methods of TST administration were used with the Mantoux intra-dermal technique established as the best method to establish the presence of M. tuber-culosis infection. Different strengths of tuberculin were used with 5 TU providing the best sensitivity whilst retaining speciÞ city. TST sensitivity could not be measured due to lack of a gold standard, but it correlated well with exposure and radiographic proof of infection. Even with the advent of more sensitive and speciÞ c T-cell based assays (e.g. ELISPOT),12 the sensitivity and speciÞ city of the Mantoux TST remains favourable and its simplicity unsurpassed.
The most important limitation to this analysis was the absence of a clear deÞ nition of disease. To gain a better understanding of the crucial transition from infection to disease, it is important to accurately deÞ ne disease. Pulmonary TB represents a whole spectrum of pa-thology and different disease entities need to be separated. NotiÞ cation data often provide unreliable information due to under- or over-reporting of disease and inaccurate cause of death identiÞ cation. Under-reporting of primary pulmonary TB in children was a particular problem.7 In addition, the reported rate of infection varied considerably between studies, especially within the important younger age groups. The rate of primary infection accepted at a speciÞ c age, inß uences the calculated risk of subsequent disease and mortality. Due to these limitations risk calculations may vary widely. The optimal way to deÞ ne risk and to describe exact disease entities is by prospectively following an unselected cohort of chil-

2 The clinical epidemiology of childhood pulmonary tuberculosis
33
dren with recent primary infection for subsequent disease development and death. Studies that documented the natural history of disease achieved this.
Despite the limitations of the articles reviewed, valuable epidemiological information is provided, which may assist with the formulation of evidence-based public health policies. The recent emergence of human immunodeÞ ciency virus (HIV) infection in many high-prevalence areas, and its inß uence on morbidity and mortality, establish the need for new epidemiological data and the global surveillance of TB in children.
34
Infection with M. tuberculosis and atopy in children
References
1. Opie E, McPhedran FM, Putnam P. The fate of children in contact with tuberculosis: the exog-enous infection of children and adults. Am J Hygiene 1935; 22: 644-682
2. Pope AS, Sartwell MD, Zacks D. Development of tuberculosis in infected children. Am J Public Health 1939; 29: 1318-1325
3. Brailey M. A study of tuberculous infection and mortality in the children of tuberculous house-holds. Am J Hygiene 1940; 31: Sec.A1-43
4. Gedde-Dahl T. Tuberculous infection in the light of tuberculin matriculation. Am J Hygiene 1952; 56: 139-214
5. Bentley FJ, Grzybowski S, Benjamin B. Tuberculosis in childhood and adolescence. The Na-tional Association for the Prevention of Tuberculosis. Waterlow and Sons Ltd, London 1954: 217-238
6. Davies PDB. The natural history of tuberculosis in children. Tubercle 1961; 42(suppl): 1-40 7. Miller FJW, Seal RME, Taylor MD. Tuberculosis in children. J and A Churchill Ltd, London
1963: 79-163 8. Zeidberg LD, Gass RS, Dillon A, Hutcheson RH. The Williamson County tuberculosis study: a
twenty-four-year epidemiologic study.. Am Rev Resp Pulm Dis 1962; 87: 1-41 9. Rieder HL. Epidemiologic basis of tuberculosis control. International Union Against Tuberculo-
sis and Lung Disease (IUATLD), Paris 1999: 11-2610. Grigg ERN. The arcana of tuberculosis. Am Rev Tuberc Pulm Dis 1958; 78: 151-172 and
426-60311. Grange JM, Gandy M, Farmer P, Zumla A. Historical declines in tuberculosis: nature, nurture and
the biosocial model. Int J Tuberc Lung Dis 2001; 5: 208-21212. Ewer K, Deeks J, Alvarez L et al. Comparison of T-cell-based assay with tuberculin skin test
for diagnosis of Mycobacterium tuberculosis infection in a school tuberculosis outbreak. Lancet 2003; 361: 1168-1173

C H A P T E R 3
The prevalence of symptoms associated with pulmonary tuberculosis in randomly selected children from a high burden community
Ben J. MaraisCharles C. ObiharaRobert P. GieH. Simon SchaafAnneke C. HesselingCarl J. LombardDon EnarsonEric BatemanN Beyers
Archives of Disease in Childhood2005; 90:1166�1170.

40
Infection with M. tuberculosis and atopy in children
Abstract
BackgroundDiagnosis of childhood tuberculosis (TB) is problematic and symptom based diagnostic
approaches are often promoted in high burden settings. This study aimed (i) to document the prevalence of symptoms associated with TB among randomly selected children living in a high burden community, and (ii) to compare the prevalence of these symptoms in chil-dren without TB to those in children with newly diagnosed TB.
MethodsA cross sectional, community based survey was performed on a 15% random sample of
residential addresses. A symptom based questionnaire and tuberculin skin test (TST) were completed in all children. Chest radiographs were performed according to South African National Tuberculosis Control Program guidelines.
ResultsResults were available in 1415 children of whom 451 (31.9%) were TST positive. TB
was diagnosed in 18 (1.3%) children. Of the 1397 children without TB, 253 (26.4%) report-ed a cough during the preceding 3 months. Comparison of individual symptoms (cough, dyspnoea, chest pain, haemoptysis, anorexia, weight loss, fatigue, fever, night sweats) in children with and without TB revealed that only weight loss differed signiÞ cantly (OR = 4.5, 95% CI 1.5 to 12.3), while the combination of cough and weight loss was most sig-niÞ cant (OR = 5.4, 95% CI 1.7 to 16.9). Children with newly diagnosed TB reported no symptoms in 50% of cases.
ConclusionChildren from this high burden community frequently reported symptoms associated
with TB. These symptoms had limited value to differentiate children diagnosed with TB from those without TB. Improved case deÞ nitions and symptom characterisation are re-quired when evaluating the diagnostic value of symptoms.

3 The prevalence of symptoms associated with pulmonary tuberculosis
41
Introduction
In areas with a high prevalence of tuberculosis (TB), children contribute a signiÞ cant proportion of the disease burden and experience considerable morbidity and mortality re-lated to TB.1 2 This is demonstrated by the fact that pulmonary TB rivals bacterial pneu-monia as a respiratory cause of death in African children older than 6 months of age.3 The diagnosis of TB in children is difÞ cult because bacteriological conÞ rmation is rarely achieved and is often not even attempted.4�8 Chest radiography is regarded as a valuable diagnostic tool, but it is often impossible to identify hilar adenopathy, considered to be the most consistent sign of primary pulmonary TB, with certainty.9 In addition, the distinction between recent primary infection and active disease is highly problematic.10 Most diag-nostic algorithms are partly symptom based, but these algorithms are poorly validated and lack standard symptom deÞ nitions.11 To our knowledge, no previous study has documented the prevalence of symptoms associated with TB in randomly selected children living in a high burden community. In these communities a large number of individuals become in-fected with Mycobacterium tuberculosis (M. tuberculosis) during childhood,12 and symp-tom based diagnostic approaches are often promoted to screen children for active TB. The literature on TB related symptomatology in children is almost exclusively hospital based, which does not reß ect the prevalence of symptoms in the general population. A recent re-view of studies from the pre-chemotherapy era documented the natural history of TB in childhood. It conÞ rmed that immune competent children, older than 2 years of age, are at low risk of disease progression following primary infection.10 The presence of symptoms associated with TB had deÞ nite diagnostic value in these low risk children, in whom the principal diagnostic challenge was to distinguish self contained infection from progressive disease.10 The aims of this community based study were (i) to document the prevalence of symptoms associated with TB among randomly selected children living in a high burden community, and (ii) to compare the prevalence of these symptoms in children without TB to those in children with newly diagnosed TB.
Methods
A cross sectional community based survey was carried out between July and December 2002. A questionnaire was completed and a tuberculin skin test (TST) administered to each child (< 15 years of age). Chest radiographs (CXR) were performed according to the South African National Tuberculosis Control Program (NTCP) guidelines.
Study settingThe study area is an established epidemiological Þ eld site in Cape Town, South Africa,
comprising two suburbs with a population of 38 656 (census 1996) and a high burden of TB (average notiÞ cation rate of new bacteriologically conÞ rmed cases 320/100 000 per year).13 Childhood TB constitutes a high percentage (39%) of the total caseload.14 The pro-portion of the population infected with human immunodeÞ ciency virus (HIV) is relatively

42
Infection with M. tuberculosis and atopy in children
low, less than the average of 8.8% (95% CI 4.9 to 12.7%) calculated for the Cape Town/Metropole region in 2001.15
Sample selectionA 15% sample of residential addresses was randomly selected, based on a geographical
information system of the area. Trained Þ eld workers enumerated the people at each of the 839 residential addresses selected. Written informed consent was obtained from the par-ent or legal guardian. The 218 addresses (26%) that refused consent were systematically replaced by neighbouring addresses. A CXR was performed in children less than 5 years of age who had been in household contact with a sputum smear positive source case or had a positive TST (induration >15 mm in diameter), and in all children with suspect symp-toms according to World Health Organisation (WHO) guidelines (loss of weight, cough > 3 weeks, fever > 1 week, or haemoptysis).16
QuestionnaireA standard questionnaire recorded symptoms that are commonly associated with TB,
experienced during the preceding 3 months (Table 1). The duration of each symptom (oth-er than haemoptysis) was categorised as less than 1 week, 1�2 weeks, 2�3 weeks, or more than 3 weeks. Questionnaires were completed by the parent under supervision of a trained Þ eld worker. Parents were requested (but put under no obligation) to conÞ dentially report previous HIV tests and results.
Tuberculin skin testTrained Þ eld nurses performed TST by intra-dermal injection of 2 tuberculin units (TU)
of M. tuberculosis PPD RT 23 (Statens Serum Institut, Copenhagen, Denmark) on the vo-lar aspect of the left forearm. The largest transverse diameter of induration was measured after 48�72 h.
Chest radiographStandard antero-posterior (AP) and lateral views were taken, using the same x ray ma-
chine in all children. A single expert screened all CXR. A second independent expert was used to conÞ rm that the radiographical signs were suggestive of TB in all children identi-Þ ed with possible TB during the initial screening. Children with conÞ rmed radiographical signs suggestive of TB had sputum or gastric aspirate samples taken for culture. A probable TB case was deÞ ned as a child with a ��diagnostic�� CXR, conÞ rmed by two independent observers (modiÞ ed WHO guidelines).17 A conÞ rmed TB case was deÞ ned as a child with bacteriological proof of TB. All children with probable or conÞ rmed TB were referred to a local clinic for treatment, in accordance with the NTCP guidelines. Children aged less than 5 years, in household contact with a sputum smear positive source case or with a positive TST, were referred for chemoprophylaxis or treatment of latent infection after active TB was excluded. The study was approved by the Ethics Review Board of Stellenbosch Uni-versity and by the Department of Health, City of Cape Town.
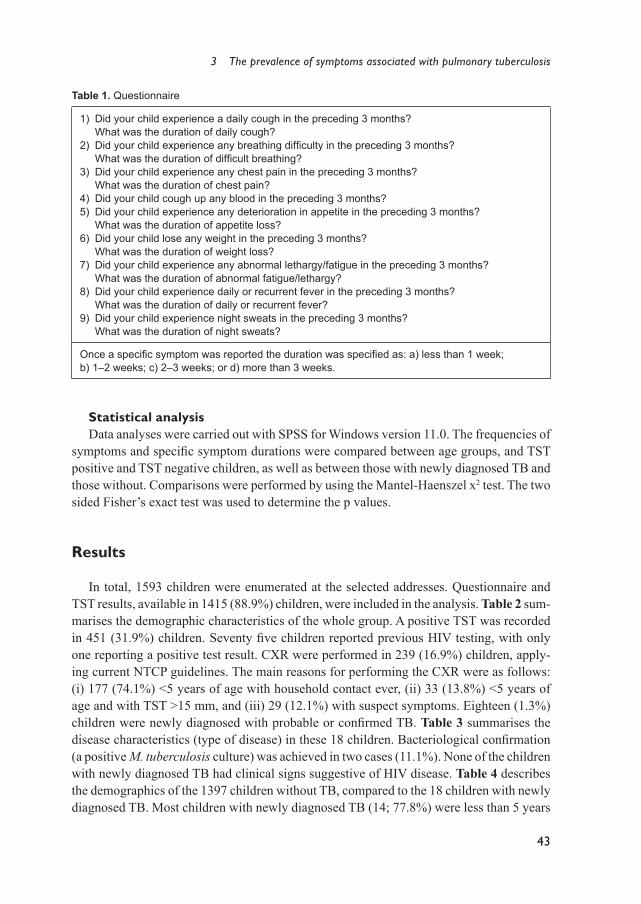
3 The prevalence of symptoms associated with pulmonary tuberculosis
43
Statistical analysisData analyses were carried out with SPSS for Windows version 11.0. The frequencies of
symptoms and speciÞ c symptom durations were compared between age groups, and TST positive and TST negative children, as well as between those with newly diagnosed TB and those without. Comparisons were performed by using the Mantel-Haenszel x2 test. The two sided Fisher�s exact test was used to determine the p values.
Results
In total, 1593 children were enumerated at the selected addresses. Questionnaire and TST results, available in 1415 (88.9%) children, were included in the analysis. Table 2 sum-marises the demographic characteristics of the whole group. A positive TST was recorded in 451 (31.9%) children. Seventy Þ ve children reported previous HIV testing, with only one reporting a positive test result. CXR were performed in 239 (16.9%) children, apply-ing current NTCP guidelines. The main reasons for performing the CXR were as follows: (i) 177 (74.1%) <5 years of age with household contact ever, (ii) 33 (13.8%) <5 years of age and with TST >15 mm, and (iii) 29 (12.1%) with suspect symptoms. Eighteen (1.3%) children were newly diagnosed with probable or conÞ rmed TB. Table 3 summarises the disease characteristics (type of disease) in these 18 children. Bacteriological conÞ rmation (a positive M. tuberculosis culture) was achieved in two cases (11.1%). None of the children with newly diagnosed TB had clinical signs suggestive of HIV disease. Table 4 describes the demographics of the 1397 children without TB, compared to the 18 children with newly diagnosed TB. Most children with newly diagnosed TB (14; 77.8%) were less than 5 years
Table 1. Questionnaire
1) Did your child experience a daily cough in the preceding 3 months? What was the duration of daily cough?2) Did your child experience any breathing difÞ culty in the preceding 3 months? What was the duration of difÞ cult breathing?3) Did your child experience any chest pain in the preceding 3 months? What was the duration of chest pain?4) Did your child cough up any blood in the preceding 3 months?5) Did your child experience any deterioration in appetite in the preceding 3 months? What was the duration of appetite loss?6) Did your child lose any weight in the preceding 3 months? What was the duration of weight loss?7) Did your child experience any abnormal lethargy/fatigue in the preceding 3 months? What was the duration of abnormal fatigue/lethargy?8) Did your child experience daily or recurrent fever in the preceding 3 months? What was the duration of daily or recurrent fever?9) Did your child experience night sweats in the preceding 3 months? What was the duration of night sweats?
Once a speciÞ c symptom was reported the duration was speciÞ ed as: a) less than 1 week; b) 1�2 weeks; c) 2�3 weeks; or d) more than 3 weeks.
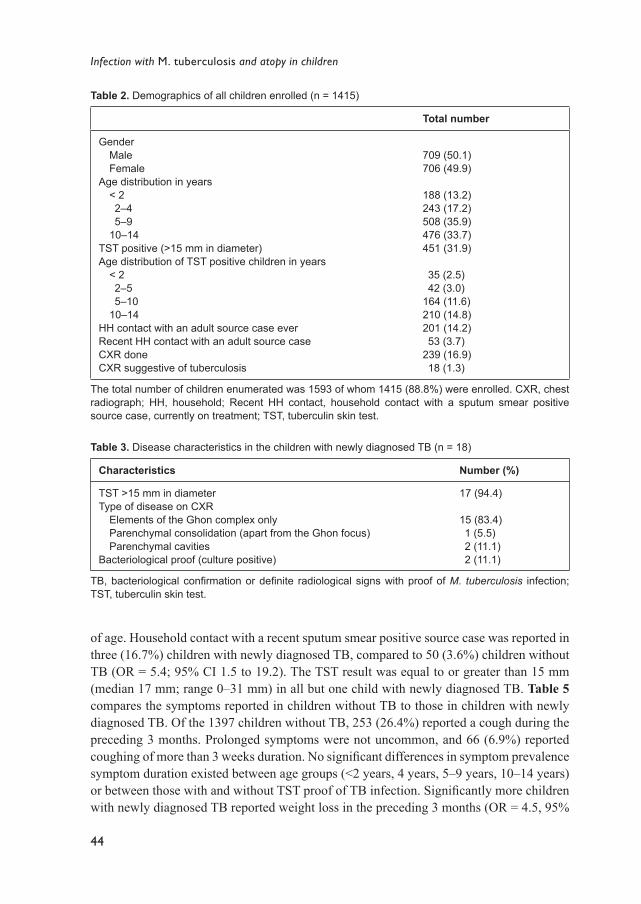
44
Infection with M. tuberculosis and atopy in children
of age. Household contact with a recent sputum smear positive source case was reported in three (16.7%) children with newly diagnosed TB, compared to 50 (3.6%) children without TB (OR = 5.4; 95% CI 1.5 to 19.2). The TST result was equal to or greater than 15 mm (median 17 mm; range 0�31 mm) in all but one child with newly diagnosed TB. Table 5 compares the symptoms reported in children without TB to those in children with newly diagnosed TB. Of the 1397 children without TB, 253 (26.4%) reported a cough during the preceding 3 months. Prolonged symptoms were not uncommon, and 66 (6.9%) reported coughing of more than 3 weeks duration. No signiÞ cant differences in symptom prevalence symptom duration existed between age groups (<2 years, 4 years, 5�9 years, 10�14 years) or between those with and without TST proof of TB infection. SigniÞ cantly more children with newly diagnosed TB reported weight loss in the preceding 3 months (OR = 4.5, 95%
Table 2. Demographics of all children enrolled (n = 1415)
Total number
Gender Male FemaleAge distribution in years < 2 2�4 5�9 10�14TST positive (>15 mm in diameter)Age distribution of TST positive children in years < 2 2�5 5�10 10�14HH contact with an adult source case everRecent HH contact with an adult source caseCXR doneCXR suggestive of tuberculosis
709 (50.1)706 (49.9)
188 (13.2)243 (17.2)508 (35.9)476 (33.7)451 (31.9)
35 (2.5) 42 (3.0)164 (11.6)210 (14.8)201 (14.2) 53 (3.7)239 (16.9) 18 (1.3)
The total number of children enumerated was 1593 of whom 1415 (88.8%) were enrolled. CXR, chest radiograph; HH, household; Recent HH contact, household contact with a sputum smear positive source case, currently on treatment; TST, tuberculin skin test.
Table 3. Disease characteristics in the children with newly diagnosed TB (n = 18)
Characteristics Number (%)
TST >15 mm in diameterType of disease on CXR Elements of the Ghon complex only Parenchymal consolidation (apart from the Ghon focus) Parenchymal cavitiesBacteriological proof (culture positive)
17 (94.4)
15 (83.4) 1 (5.5) 2 (11.1) 2 (11.1)
TB, bacteriological conÞ rmation or deÞ nite radiological signs with proof of M. tuberculosis infection; TST, tuberculin skin test.
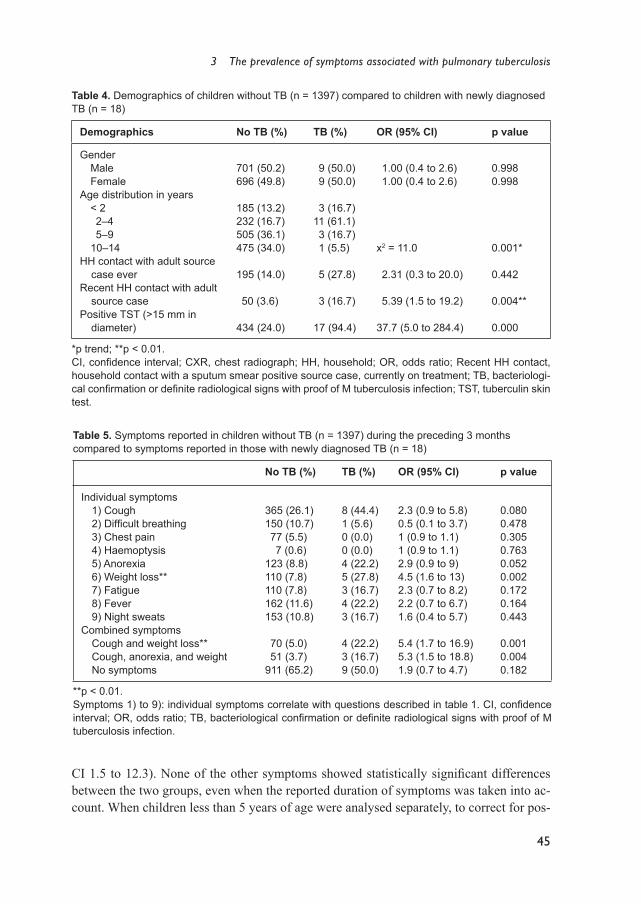
3 The prevalence of symptoms associated with pulmonary tuberculosis
45
Table 4. Demographics of children without TB (n = 1397) compared to children with newly diagnosed TB (n = 18)
Demographics No TB (%) TB (%) OR (95% CI) p value
Gender Male FemaleAge distribution in years < 2 2�4 5�9 10�14HH contact with adult source
case everRecent HH contact with adult
source casePositive TST (>15 mm in
diameter)
701 (50.2)696 (49.8)
185 (13.2)232 (16.7)505 (36.1)475 (34.0)
195 (14.0)
50 (3.6)
434 (24.0)
9 (50.0) 9 (50.0)
3 (16.7)11 (61.1) 3 (16.7) 1 (5.5)
5 (27.8)
3 (16.7)
17 (94.4)
1.00 (0.4 to 2.6) 1.00 (0.4 to 2.6)
x2 = 11.0
2.31 (0.3 to 20.0)
5.39 (1.5 to 19.2)
37.7 (5.0 to 284.4)
0.9980.998
0.001*
0.442
0.004**
0.000
*p trend; **p < 0.01.CI, conÞ dence interval; CXR, chest radiograph; HH, household; OR, odds ratio; Recent HH contact, household contact with a sputum smear positive source case, currently on treatment; TB, bacteriologi-cal conÞ rmation or deÞ nite radiological signs with proof of M tuberculosis infection; TST, tuberculin skin test.
CI 1.5 to 12.3). None of the other symptoms showed statistically signiÞ cant differences between the two groups, even when the reported duration of symptoms was taken into ac-count. When children less than 5 years of age were analysed separately, to correct for pos-
Table 5. Symptoms reported in children without TB (n = 1397) during the preceding 3 months compared to symptoms reported in those with newly diagnosed TB (n = 18)
No TB (%) TB (%) OR (95% CI) p value
Individual symptoms 1) Cough 2) DifÞ cult breathing 3) Chest pain 4) Haemoptysis 5) Anorexia 6) Weight loss** 7) Fatigue 8) Fever 9) Night sweatsCombined symptoms Cough and weight loss** Cough, anorexia, and weight No symptoms
365 (26.1)150 (10.7) 77 (5.5) 7 (0.6)123 (8.8)110 (7.8)110 (7.8)162 (11.6)153 (10.8)
70 (5.0) 51 (3.7)911 (65.2)
8 (44.4)1 (5.6)0 (0.0)0 (0.0)4 (22.2)5 (27.8)3 (16.7)4 (22.2)3 (16.7)
4 (22.2)3 (16.7)9 (50.0)
2.3 (0.9 to 5.8)0.5 (0.1 to 3.7)1 (0.9 to 1.1)1 (0.9 to 1.1)2.9 (0.9 to 9)4.5 (1.6 to 13)2.3 (0.7 to 8.2)2.2 (0.7 to 6.7)1.6 (0.4 to 5.7)
5.4 (1.7 to 16.9)5.3 (1.5 to 18.8)1.9 (0.7 to 4.7)
0.0800.4780.3050.7630.0520.0020.1720.1640.443
0.0010.0040.182
**p < 0.01.Symptoms 1) to 9): individual symptoms correlate with questions described in table 1. CI, conÞ dence interval; OR, odds ratio; TB, bacteriological conÞ rmation or deÞ nite radiological signs with proof of M tuberculosis infection.

46
Infection with M. tuberculosis and atopy in children
sible selection bias in the older children, the results were similar. The presence of more than one symptom increased the odds for TB, but this reached signiÞ cance only with the inclu-sion of weight loss. The combination of cough and weight loss was most signiÞ cant (OR = 5.4, 95% CI 1.7 to 16.9). Nine (50%) children with newly diagnosed TB reported no symp-toms at all, compared to 910 (65.2%) of those without TB (OR = 1.9, 95% CI 0.7 to 4.7).
Discussion
This community based survey documents the prevalence of symptoms associated with pulmonary TB in the average child living in a high burden community. The results demon-strate that within this setting, these symptoms are common in the general paediatric popu-lation. Only weight loss, alone or in combination with other symptoms, was signiÞ cantly more common in children with newly diagnosed TB. Combinations of symptoms (symp-tom complexes) were more likely to be associated with TB than individual symptoms, but the small number of TB cases limited the analysis. This is an inevitable limitation of community based surveys that document relatively rare events.18 The detection of 18 new TB cases during this survey demonstrate a high prevalence of undiagnosed childhood TB within this community (1272/100 000 of the child population). The observation that nearly a third of children coughed in the preceding 3 months may be explained by the fact that both viral and bacterial infections are common in this community, especially during the winter months (May to September). It is also common practice for children to share a bed with their parents, which may increase parental awareness of night time symptoms such as cough, fever, or sweating. Similar to previous observations, some (exactly 50%) of the children with newly diagnosed TB reported no symptoms.19�21 Although signiÞ cant differ-ences were found between the symptoms reported in children with TB and those without, these differences are of limited diagnostic value and only relevant from an epidemiologi-cal perspective. This is illustrated by the fact that the symptom complex with the highest signiÞ cance, cough and weight loss, had a positive predictive value of only 5%. The study had several limitations; of most importance is the fact that CXR were performed on a selec-tive subgroup of children. Only children under 5 years of age were radiologically screened following household exposure or a positive TST and as a result older children with asymp-tomatic primary infection may not have been diagnosed. Although this could have biased the results, the statistical Þ ndings in children less than 5 years of age and in the group as a whole were similar when comparing symptoms in those with and without TB. This po-tential bias seems unavoidable as both the WHO and NTCP guidelines recommend that a CXR should only be performed in older children if they are symptomatic. It may even be argued that it is unethical to perform a CXR in an asymptomatic child older than 5 years of age, as the risk of developing disease following primary infection is less than 1%.10 The group diagnosed with TB during this survey represents a true reß ection of children who would have been diagnosed with TB in a ��real life�� setting, where resources permit ac-tive contact tracing and adequate investigation. The majority of children diagnosed with TB had signs indicative of recent primary infection only (positive TST and elements of the

3 The prevalence of symptoms associated with pulmonary tuberculosis
47
Ghon complex on CXR). The natural history of TB in children illustrates that following primary pulmonary infection, transient visibility of the Ghon complex is common and does not necessarily indicate disease.10 22 23 The fact that current, internationally accepted deÞ ni-tions of disease often reß ect recent primary infection, especially in children who are diag-nosed after active contact tracing, does hamper the interpretation. Therefore, it is important to point out that, although the study indicates that symptoms have limited diagnostic value, their value for differentiating active disease from recent primary infection requires further investigation.
Questionnaire driven surveys are inherently limited by recall bias and subjectivity. Bias was reduced by the use of standardised questionnaires and the fact that the diagnostic tests (TST and CXR) were performed after completion of the questionnaire. Reported weight loss reß ected a subjective impression and objective weight measurements were not taken into account, as these were not routinely done in all children. In addition, the questions used may have been too imprecise, as the pre-chemotherapy literature identiÞ es important symptom characteristics, associated with progressive TB, that were not elucidated in the present study. These characteristics include persistent, non-remitting symptoms of recent onset.10 Careful symptom characterisation may be essential to improve their diagnostic value. Nearly a third (5, 27.8%) of children with newly diagnosed TB reported previous household contact with a sputum smear positive source case. This is in agreement with a study from the same community that employed restriction fragment length polymorphism (RFLP) analysis, providing proof that 34% of children acquired disease following infection from a source case within the household.24 In high burden settings, most infection, particu-larly in children older than 2 years of age, is contracted outside the household within the community.9 13 24 In conclusion, this study illustrates the importance of community based research. It describes symptomatology within the general community and highlights the danger of extrapolating Þ ndings from hospital based studies to the community level. It is essential to know the prevalence of symptoms within the general community in order to evaluate the value of any particular symptom based diagnostic approach. Comparing the symptoms reported in children without TB to those in children with newly diagnosed TB demonstrates why current symptom based scoring systems perform poorly in clinical prac-tice. Most importantly, the study emphasises the need for improved symptom characterisa-tion and accurate outcome deÞ nitions which will adequately differentiate M. tuberculosis infection from active disease.

48
Infection with M. tuberculosis and atopy in children
References
1. Donald PR. Childhood tuberculosis: out of control? Curr Opin Pulm Med 2002; 8:178�82. 2. Walls T, Shingadia D. Global epidemiology of paediatric tuberculosis. J Infect 2004; 48:13�22. 3. Chintu C, Mudenda V, Lucas S, et al. Lung diseases at necropsy in African children dying from
respiratory illnesses: a descriptive necropsy study. Lancet 2002 ;360:985�90. 4. Donald PR. Childhood tuberculosis: the hidden epidemic. Int J Tuberc Lung Dis 2004; 8:627�9. 5. Nelson LJ, Wells CD. Global epidemiology of childhood tuberculosis. Int J Tuberc Lung Dis
2004; 8:636�47. 6. Eamranond P, Jaramillo E. Tuberculosis in children: reassessing the need for improved diagnosis
in global control strategies. Int J Tuberc Lung Dis 2001; 5:594�603. 7. Starke JR. Childhood tuberculosis: a diagnostic dilemma. Chest 1993; 104:329�30. 8. Osborne CM. The challenge of diagnosing childhood tuberculosis in a developing country. Arch
Dis Child 1995; 72:369�74. 9. Marais BJ, Gie RP, Starke JR, et al. A proposed radiological classiÞ cation of childhood intra-tho-
racic tuberculosis. Pediatr Radiol 2004; 34(11):886�94.10. Marais BJ, Gie RP, Schaaf HS, et al. The natural history of childhood intrathoracic tuberculosis
� a critical review of the literature from the prechemotherapy era. Int J Tuberc Lung Dis 2004; 8:392�402.
11. Hesseling AC, Schaaf HS, Beyers N, et al. A critical review of diagnostic approaches used in the diagnosis of childhood tuberculosis. Int J Tuberc Lung Dis 2002; 6:1038�45.
12. Marais BJ, Gie RP, Schaaf HS, et al. The clinical epidemiology of childhood pulmonary tuber-culosis: a critical review of literature from the prechemotherapy era. Int J Tuberc Lung Dis 2004; 8:278�85.
13. Verver S, Warren RM, Munch Z, et al. Proportion of tuberculosis transmission that takes place in households in a high-incidence area. Lancet 2004; 363:212�14.
14. van Rie, Beyers N, Gie R, et al. Childhood tuberculosis in an urban population in South Africa: burden and risk factors. Arch Dis Child 1999; 80:433�7.
15. Department of Health, South Africa. 12th National HIV and syphilis seroprevalence survey of women attending public antenatal clinics in South Africa 2001. Epidemiol Comments 2002; 5:2�15.
16. Shingadia D, Novelli V. Diagnosis and treatment of tuberculosis in children. Lancet Infect Dis 2003; 3:624�32.
17. Stoltz AP, Donald PR, Strebel PM, et al. Criteria for the notiÞ cation of childhood tuberculosis in a high-incidence area of the western Cape Province. S Afr Med J 1990; 77:385�6.
18. Grimes AD, Schults KF. An overview of clinical research: the lay of the land. Lancet 2002; 359:57�61.
19. Schaaf HS, Beyers N, Gie RP, et al. Respiratory tuberculosis in childhood: the diagnostic value of clinical features and special investigations. Pediatr Infect Dis J 1995; 14:189�94.
20. Salazar GE, Schmidtz TL, Cama R, et al. Pulmonary tuberculosis in children in a developing country. Pediatrics 2001; 108:448�53.
21. Starke JR, Taylor-Watts KT. Tuberculosis in the pediatric population of Houston, Texas. Pediat-rics 1989; 84:28�35.
22. Gedde-Dahl T. Tuberculous infection in the light of tuberculin matriculation. Am J Hyg 1952; 56:139�214.
23. Delacourt C, Mani TM, Bonnerot V, et al. Computed tomography with normal chest radiograph in tuberculous infection. Arch Dis Child 1993; 69:430�2.
24. Schaaf HS, Michaelis IA, Richardson M, et al. Adult-to-child transmission of tuberculosis: household or community contact? Int J Tuberc Lung Dis 2003; 7:426�31.

C H A P T E R 4
Does mycobacterial infection prevent the development of atopy in childhood? A systematic review
Charles C. ObiharaCasper W. BollenNulda BeyersJan L.L. Kimpen
Submitted

50
Infection with M. tuberculosis and atopy in children
Abstract
The epidemiologic relation between mycobacterial infection and the prevalence of atopic disease in humans is still unclear. This contrasts with studies in murine models in which a clear suppression of atopic symptoms was observed after exposure to mycobacte-ria or mycobacterial products.
We aim to provide a systematic overview of the literature on the relationship between mycobacterial infection and atopic disease and to evaluate the causal relationship in a meta-analysis.
The Embase and Medline databases were searched systematically for papers published in the English literature on the relation between mycobacterial infection and atopic disease. Original observational or interventional studies involving the pediatric population were included. Of a total of 1201 hits, 23 studies (19 cross sectional, 3 case-control, 1 prospec-tive cohort) met the inclusion criteria. Only a minority of studies (10) observed an associa-tion between mycobacterial infection and the prevalence of atopic disease outcome. In the meta-analysis only studies containing complete data on exposure and atopic disease out-come variables were included. Only cross sectional studies, in which the relation between a positive tuberculin skin test and allergic symptoms was evaluated, showed statistically signiÞ cant negative correlation (odds ratio 0.63; 95% conÞ dence interval 0.51 to 0.79). There was a high level of heterogeneity (I2) observed in studies. This may be explained by differences in the type and deÞ nition of mycobacterial infection and lack of uniformity in the deÞ nition of atopy.
These results strongly stress the urgent need for prospective studies to answer the ques-tion if mycobacterial exposure or infection prevents the development of atopy, especial-ly with regard to the possible use of mycobacterial products as vaccines against atopic disease.

4 Does mycobacterial infection prevent the development of atopy in childhood?
51
Introduction
During the last few decades, the prevalence of atopic disease in children has increased in countries with a Western lifestyle.1 The �hygiene hypothesis� suggests that a relationship exists between improved hygiene and increase in atopic diseases.2 An underlying mecha-nism for this hypothesis is that the lack of microbial stimulation leads to either an inappro-priate T helper (Th) type response or inappropriate Th cell regulatory mechanisms.3,4
A speciÞ c infectious agent responsible for the hygiene hypothesis has not yet been iden-tiÞ ed, although many candidate diseases have been suggested, such as measles, hepatitis A and respiratory infections.5-7 Animal models have identiÞ ed mycobacteria as important potential candidates in the hygiene hypothesis by demonstrating that exposure to mycobac-teria led to regulatory mechanisms that restored the immune homeostasis.4,8,9 This has led to the suggestion that absence of infections, such as that caused by mycobacteria, may be an underlying factor in the rising prevalence of atopic diseases in developed countries (the so-called Th1/Th2 paradigm). In contrast, the epidemiologic relation between mycobacte-rial infection and atopic disease in humans is still unclear and controversial.10-13
We reviewed systematically the evidence for this causal relation.
Methods
Search strategy The Embase and Medline databases were searched systematically to identify all papers
published in the English literature on the relation between mycobacterial infection and atopic disease, including the period January 1966 and September 2005. The following key words were utilised both individually and in different combinations: �M. tuberculo-sis (M. tuberculosis) infection, tuberculin response, mycobacteria other than tuberculosis (MOTTs) infection, M. bovis bacille Calmette-Guérin (BCG)-immunization and/or tuber-culosis�, and �atopy, atopic disease, allergic disease or symptom and/or allergy�. Cross-referencing of important articles was also applied. All identiÞ ed papers on the relation between mycobacteria and atopic disease were published after 1997, when Shirakawa et al. reported on this relation for the Þ rst time.13
Selection CriteriaOriginal observational or interventional population or hospital based studies involving
the pediatric population (≤ 18 years of age) in which the relation between mycobacterial infection and atopic disease outcome was studied were included. The age range was chosen because it is assumed that immune deviation caused by infectious agents and the protective effect on the development of atopy mainly occurs in childhood.14 In addition, only studies with well-deÞ ned participants� characteristics and quantiÞ able numbers of patients with and without exposure and numbers of patients with and without atopic outcome measure(s) were included in the meta-analysis.
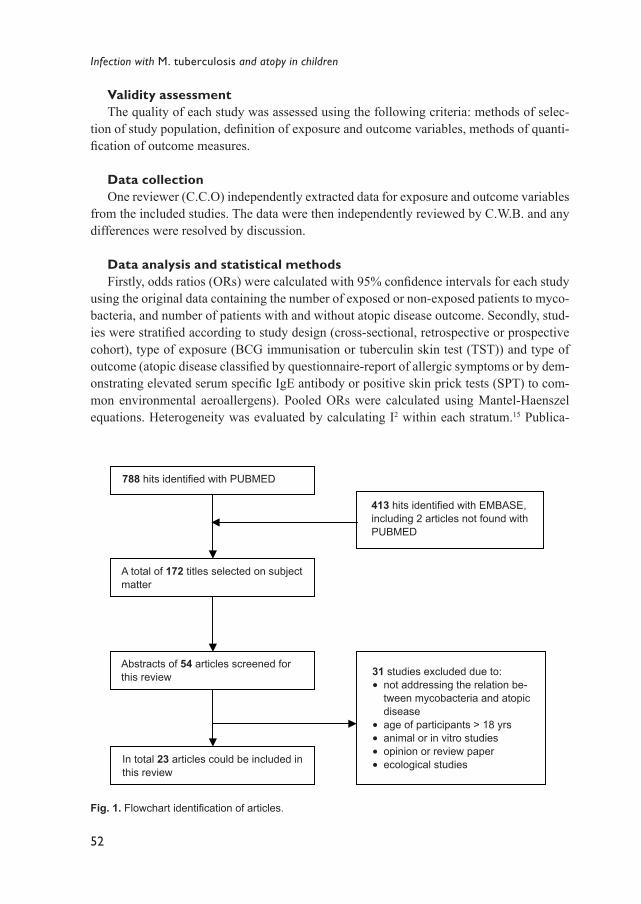
52
Infection with M. tuberculosis and atopy in children
Validity assessmentThe quality of each study was assessed using the following criteria: methods of selec-
tion of study population, deÞ nition of exposure and outcome variables, methods of quanti-Þ cation of outcome measures.
Data collectionOne reviewer (C.C.O) independently extracted data for exposure and outcome variables
from the included studies. The data were then independently reviewed by C.W.B. and any differences were resolved by discussion.
Data analysis and statistical methodsFirstly, odds ratios (ORs) were calculated with 95% conÞ dence intervals for each study
using the original data containing the number of exposed or non-exposed patients to myco-bacteria, and number of patients with and without atopic disease outcome. Secondly, stud-ies were stratiÞ ed according to study design (cross-sectional, retrospective or prospective cohort), type of exposure (BCG immunisation or tuberculin skin test (TST)) and type of outcome (atopic disease classiÞ ed by questionnaire-report of allergic symptoms or by dem-onstrating elevated serum speciÞ c IgE antibody or positive skin prick tests (SPT) to com-mon environmental aeroallergens). Pooled ORs were calculated using Mantel-Haenszel equations. Heterogeneity was evaluated by calculating I2 within each stratum.15 Publica-
Fig. 1. Flowchart identiÞ cation of articles.
A total of 172 titles selected on subject matter
413 hits identiÞ ed with EMBASE, including 2 articles not found with PUBMED
Abstracts of 54 articles screened for this review 31 studies excluded due to:
● not addressing the relation be-tween mycobacteria and atopic disease
● age of participants > 18 yrs● animal or in vitro studies● opinion or review paper ● ecological studies In total 23 articles could be included in
this review
788 hits identiÞ ed with PUBMED
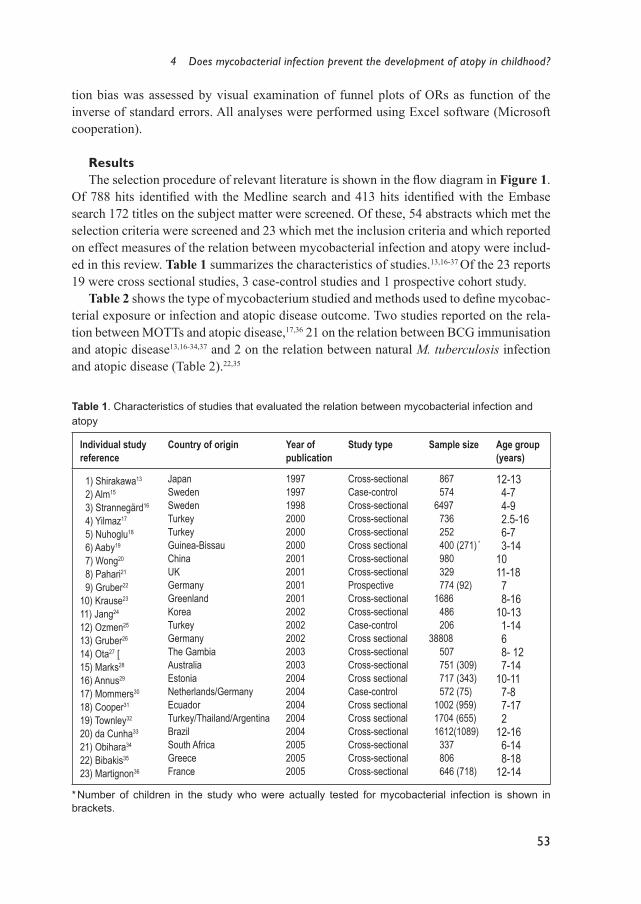
4 Does mycobacterial infection prevent the development of atopy in childhood?
53
tion bias was assessed by visual examination of funnel plots of ORs as function of the inverse of standard errors. All analyses were performed using Excel software (Microsoft cooperation).
ResultsThe selection procedure of relevant literature is shown in the ß ow diagram in Figure 1.
Of 788 hits identiÞ ed with the Medline search and 413 hits identiÞ ed with the Embase search 172 titles on the subject matter were screened. Of these, 54 abstracts which met the selection criteria were screened and 23 which met the inclusion criteria and which reported on effect measures of the relation between mycobacterial infection and atopy were includ-ed in this review. Table 1 summarizes the characteristics of studies.13,16-37 Of the 23 reports 19 were cross sectional studies, 3 case-control studies and 1 prospective cohort study.
Table 2 shows the type of mycobacterium studied and methods used to deÞ ne mycobac-terial exposure or infection and atopic disease outcome. Two studies reported on the rela-tion between MOTTs and atopic disease,17,36 21 on the relation between BCG immunisation and atopic disease13,16-34,37 and 2 on the relation between natural M. tuberculosis infection and atopic disease (Table 2).22,35
Table 1. Characteristics of studies that evaluated the relation between mycobacterial infection and atopy
Individual study reference
Country of origin Year of publication
Study type Sample size Age group (years)
1) Shirakawa13
2) Alm15
3) Strannegärd16
4) Yilmaz17
5) Nuhoglu18
6) Aaby19
7) Wong20
8) Pahari21
9) Gruber22
10) Krause23
11) Jang24
12) Ozmen25
13) Gruber26
14) Ota27 [15) Marks28
16) Annus29
17) Mommers30
18) Cooper31
19) Townley32
20) da Cunha33
21) Obihara34
22) Bibakis35
23) Martignon36
JapanSwedenSwedenTurkeyTurkeyGuinea-BissauChinaUKGermanyGreenlandKoreaTurkeyGermanyThe GambiaAustraliaEstoniaNetherlands/GermanyEcuadorTurkey/Thailand/ArgentinaBrazilSouth AfricaGreeceFrance
199719971998200020002000200120012001200120022002200220032003200420042004200420042005 20052005
Cross-sectionalCase-controlCross-sectionalCross-sectionalCross-sectionalCross sectionalCross-sectionalCross-sectionalProspectiveCross-sectionalCross-sectionalCase-controlCross sectionalCross-sectionalCross-sectionalCross sectionalCase-controlCross sectionalCross sectionalCross-sectionalCross-sectionalCross-sectionalCross-sectional
867 574 6497 736 252 400 (271) * 980 329 774 (92) 1686 486 20638808 507 751 (309) 717 (343) 572 (75) 1002 (959) 1704 (655) 1612(1089) 337 806 646 (718)
12-13 4-7 4-9 2.5-16 6-7 3-141011-18 7 8-1610-13 1-14 6 8- 12 7-1410-11 7-8 7-17 2 12-16 6-14 8-1812-14
* Number of children in the study who were actually tested for mycobacterial infection is shown in brackets.
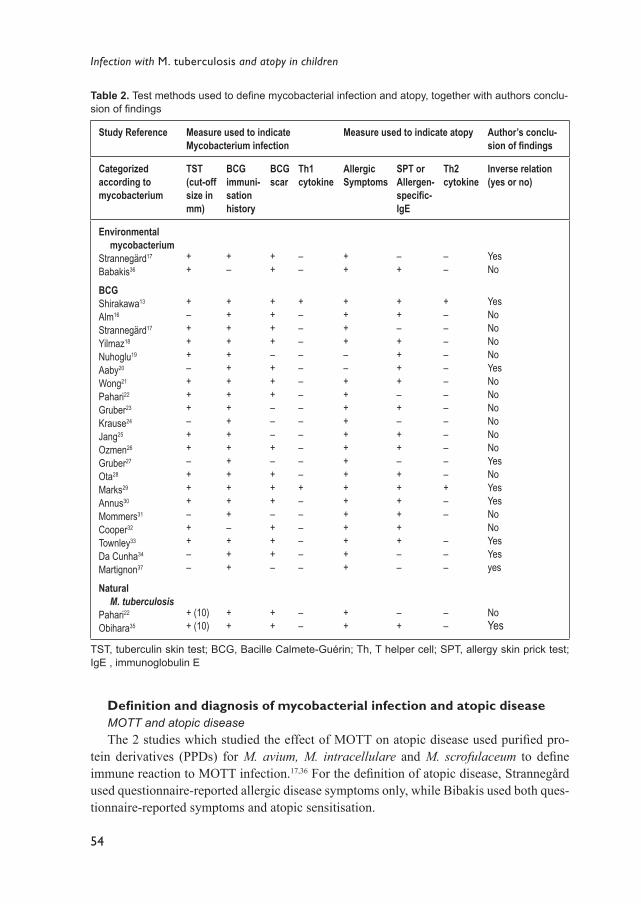
54
Infection with M. tuberculosis and atopy in children
Defi nition and diagnosis of mycobacterial infection and atopic diseaseMOTT and atopic diseaseThe 2 studies which studied the effect of MOTT on atopic disease used puriÞ ed pro-
tein derivatives (PPDs) for M. avium, M. intracellulare and M. scrofulaceum to deÞ ne immune reaction to MOTT infection.17,36 For the deÞ nition of atopic disease, Strannegård used questionnaire-reported allergic disease symptoms only, while Bibakis used both ques-tionnaire-reported symptoms and atopic sensitisation.
Table 2. Test methods used to deÞ ne mycobacterial infection and atopy, together with authors conclu-sion of Þ ndings
Study Reference Measure used to indicate Mycobacterium infection
Measure used to indicate atopy Author�s conclu-sion of Þ ndings
Categorized according to mycobacterium
TST (cut-off size in mm)
BCG immuni-sation history
BCGscar
Th1 cytokine
Allergic Symptoms
SPT or Allergen-speciÞ c-IgE
Th2cytokine
Inverse relation(yes or no)
Environmental mycobacterium
Strannegärd17
Babakis36
BCGShirakawa13
Alm16
Strannegärd17
Yilmaz18
Nuhoglu19
Aaby20
Wong21
Pahari22
Gruber23
Krause24
Jang25
Ozmen26
Gruber27
Ota28
Marks29
Annus30
Mommers31
Cooper32
Townley33
Da Cunha34
Martignon37
Natural M. tuberculosis
Pahari22
Obihara35
++
+ �+++ �+ + + �+ + �+++�++��
+ (10)+ (10)
+�
+++++++++++++++++�+++
++
++
++++�+++���+�+++�+++�
++
��
+�������������+������
��
++
++++��+++++++++++++++
++
�+
++�++++�+�++�++++++��
�+
��
+�������������+��
���
��
YesNo
YesNoNoNoNoYesNoNoNoNoNoNoYes NoYesYesNoNoYesYesyes
NoYes
TST, tuberculin skin test; BCG, Bacille Calmete-Guérin; Th, T helper cell; SPT, allergy skin prick test; IgE , immunoglobulin E
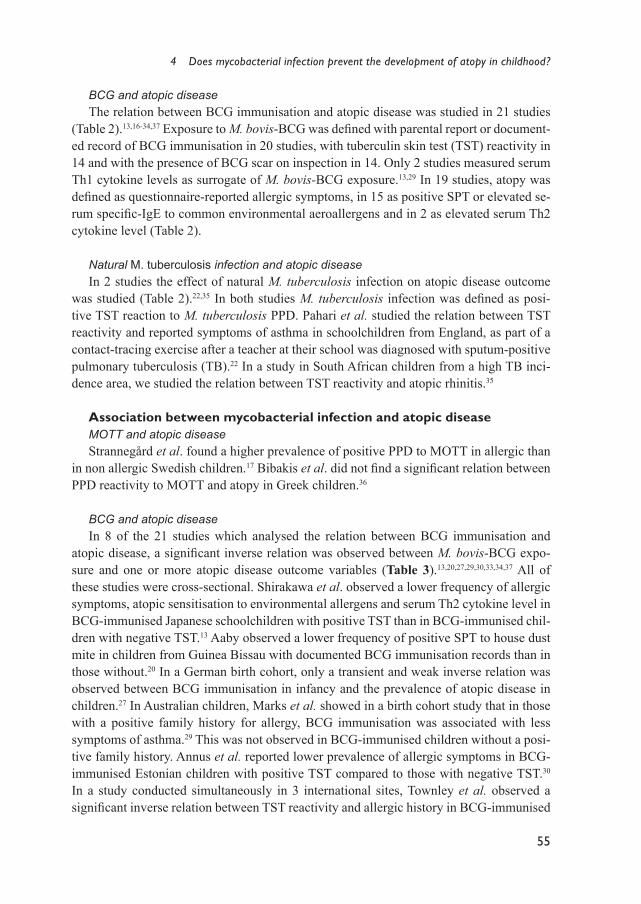
4 Does mycobacterial infection prevent the development of atopy in childhood?
55
BCG and atopic diseaseThe relation between BCG immunisation and atopic disease was studied in 21 studies
(Table 2).13,16-34,37 Exposure to M. bovis-BCG was deÞ ned with parental report or document-ed record of BCG immunisation in 20 studies, with tuberculin skin test (TST) reactivity in 14 and with the presence of BCG scar on inspection in 14. Only 2 studies measured serum Th1 cytokine levels as surrogate of M. bovis-BCG exposure.13,29 In 19 studies, atopy was deÞ ned as questionnaire-reported allergic symptoms, in 15 as positive SPT or elevated se-rum speciÞ c-IgE to common environmental aeroallergens and in 2 as elevated serum Th2 cytokine level (Table 2).
Natural M. tuberculosis infection and atopic disease In 2 studies the effect of natural M. tuberculosis infection on atopic disease outcome
was studied (Table 2).22,35 In both studies M. tuberculosis infection was deÞ ned as posi-tive TST reaction to M. tuberculosis PPD. Pahari et al. studied the relation between TST reactivity and reported symptoms of asthma in schoolchildren from England, as part of a contact-tracing exercise after a teacher at their school was diagnosed with sputum-positive pulmonary tuberculosis (TB).22 In a study in South African children from a high TB inci-dence area, we studied the relation between TST reactivity and atopic rhinitis.35
Association between mycobacterial infection and atopic diseaseMOTT and atopic diseaseStrannegård et al. found a higher prevalence of positive PPD to MOTT in allergic than
in non allergic Swedish children.17 Bibakis et al. did not Þ nd a signiÞ cant relation between PPD reactivity to MOTT and atopy in Greek children.36
BCG and atopic diseaseIn 8 of the 21 studies which analysed the relation between BCG immunisation and
atopic disease, a signiÞ cant inverse relation was observed between M. bovis-BCG expo-sure and one or more atopic disease outcome variables (Table 3).13,20,27,29,30,33,34,37 All of these studies were cross-sectional. Shirakawa et al. observed a lower frequency of allergic symptoms, atopic sensitisation to environmental allergens and serum Th2 cytokine level in BCG-immunised Japanese schoolchildren with positive TST than in BCG-immunised chil-dren with negative TST.13 Aaby observed a lower frequency of positive SPT to house dust mite in children from Guinea Bissau with documented BCG immunisation records than in those without.20 In a German birth cohort, only a transient and weak inverse relation was observed between BCG immunisation in infancy and the prevalence of atopic disease in children.27 In Australian children, Marks et al. showed in a birth cohort study that in those with a positive family history for allergy, BCG immunisation was associated with less symptoms of asthma.29 This was not observed in BCG-immunised children without a posi-tive family history. Annus et al. reported lower prevalence of allergic symptoms in BCG-immunised Estonian children with positive TST compared to those with negative TST.30 In a study conducted simultaneously in 3 international sites, Townley et al. observed a signiÞ cant inverse relation between TST reactivity and allergic history in BCG-immunised

56
Infection with M. tuberculosis and atopy in children
children from Turkey and Thailand, but not in BCG-immunised children from Argentina.33
In Brazilian children, Da Cunha et al. observed lower risk of asthma only in children with neonatal BCG scar and a past history of allergic rhinitis, but not in those without a history of allergic rhinitis.34 In another study, French children with a positive BCG immunisation history had less allergic disease symptoms than those without BCG immunisation.37
Natural M. tuberculosis infection and atopic disease One of the two studies which evaluated the relation between natural M. tuberculosis in-
fection and atopic disease observed an inverse relation. In the study in schoolchildren from England, Pahari et al. did not Þ nd an inverse relation between TST reactivity and asthmatic symptoms.22 In the study in South African children, we observed a signiÞ cant inverse as-sociation between M. tuberculosis infection and atopic rhinitis, and reduced prevalence of allergy skin prick test (SPT) reactivity in allergic children with positive TST, when com-pared to allergic children with negative TST.35
Meta-analysis of studiesStudies which did not report the original data containing the number of exposed and non-
exposed subjects to mycobacteria, and the number of patients with and without the atopic disease outcome were excluded from the meta-analysis. For the meta-analyses the studies were stratiÞ ed according to study design, type of exposure and deÞ nition of atopic outcome. The results of these stratiÞ ed pooled analyses are shown in Table 3. We assessed publication bias of studies by visual inspection of the relation between the inverse of precision (1/p) and strength of the reported relation and the result was not suggestive of publication bias for the different strata. As shown in Table 3 cross sectional studies that investigated the relation between BCG immunisation or TST reactivity and atopic disease showed a large degree of unexplained heterogeneity. Therefore, these pooled results were not readily interpretable. Only the relation between positive TST and allergic symptoms was signiÞ cant (OR 0.63;
Table 3. Results of the meta-analysis pooled according to study design
Study Design Number of studies
Number of patients
Exposure Outcome Test OR 95% CI I2
Lower Upper
Cross SectionalCross Sectional
Cross SectionalCross Sectional
Cross SectionalCross Sectional
Cross SectionalCross Sectional
Case ControlCase Control
41
15
21
37
12
40453 451
6497 4122
482 153
3554 3567
574 1145
BCG BCG
BCG BCG
TSTTST
TSTTST
BCG BCG
AsthmaAsthma
AtopyAtopy
AsthmaAsthma
AtopyAtopy
AtopyAtopy
ClinicalMCIT
ClinicalSPT
ClinicalMCIT
ClinicalSPT
ClinicalSPT
0.961.10
0.861.01
0.821.73
0.630.92
0.810.91
0.880.72
0.640.83
0.460.77
0.510.76
0.570.68
1.051.69
1.151.23
1.463.89
0.791.12
1.151.21
0%NA
NA61%
0%NA
90%12%
NA13%
I2: coefÞ cient of heterogeneity; CI: conÞ dence interval
4 Does mycobacterial infection prevent the development of atopy in childhood?
57
95% CI 0.51-0.79) (Table 3). The individual and pooled ORs of these studies are illustrated in Figure 2. The Þ rst study by Shirakawa reported a signiÞ cant association that was not reproduced by the other two analogous studies.13,21,25 Three case control studies, one inves-tigating the relation between BCG immunisation and symptomatic atopic disease and two studies deÞ ning atopy by SPT did not show a signiÞ cant relationship.16,26,31
Discussion
The results of this systematic review of the literature on the relation between myco-bacterial infection or exposure and atopic disease show that only a minority of epidemio-logic studies found evidence to support a protective effect of mycobacterial infection on the development of atopic disease. This contrasts with studies in murine models showing a suppression of atopic symptoms after exposure to mycobacteria or mycobacterial prod-ucts.4,8,9 Moreover, this review reveals a high level of heterogeneity of studies. Among the most important factors which could explain this heterogeneity, next to differences in the study population, design or methodology, are differences in type, deÞ nition, intensity and persistence (chronicity) of mycobacterial exposure or infection of the population studied, and lack of uniformity in the deÞ nition of atopic disease outcome variables.
Immune activation after mycobacterial infection is dependent on the mycobacterial spe-cies.38 This is supported by the observation that BCG is a poorer inducer of interleukin (IL)-12, the major cytokine in the induction of the Th1 response, than M. tuberculosis.39
Protective immunity in reaction to mycobacterial exposure or infection is mediated primar-ily by Th1 cells directed against mycobacterial proteins.38 An important marker of Th1-mediated immunity is the development of delayed-type hypersensitivity (DTH), which can
0.1
1
10
Shirakawa Wong Jang Pooled
Fig. 2. Calculated and pooled odds ratios (OR) of cross sectional studies which studied the relation between tuberculin skin test (TST) and symptoms of atopic disease as outcome variable.
58
Infection with M. tuberculosis and atopy in children
be evaluated by TST. TST reactivity becomes apparent in 3 to 6 weeks following M. tu-berculosis infection and may remain positive for the lifetime of the individual.40,41 The size of TST induration has been directly correlated with serum levels of IFN-γ, implying that a large TST size may reß ect strong Th1 immunity.42 A very strong TST response is more frequently associated with M. tuberculosis infection than with M. bovis-BCG or MOTT in-fection.40,41 Although BCG immunisation may cause a transiently reactive TST, most chil-dren who received BCG as infants have a weak or non-reactive TST at 5 years of age.23,43 Moreover, BCG immunisation had little impact on the interpretation of TST in children during a TB contact tracing investigation.44 It has been observed that BCG immunisation (even in early life) cannot possibly mimic qualitatively or quantitatively the persistent im-mune stimulation provided by natural exposure to mycobacteria.45 Although differences in the species of mycobacterium may contribute in explaining some of the heterogeneity in Þ ndings between studies, they cannot logically explain the differences in results of studies which used the same mycobacterium type.
Recent explanations of the hygiene hypothesis suggest that intensity, frequency or per-sistence of exposure or infection to pathogens may inß uence the level of immune protec-tion.45,46 Pathogens that cause intense and/or chronic infections, such as Mycobacterium tu-berculosis or parasites may have evolved strategies to subvert the host�s immune responses, by stimulating an increased production of anti-inß ammatory or immunosuppressive me-diators, which normally function to control or terminate the protective immune effector-responses of the host.47 For instance, the Japanese children investigated by Shirakawa et al. received BCG immunization three times (at birth, at the age of 6 and 12 years).13 This is reß ected by the high prevalence of positive TST reactivity (58%) and by the fact that the strongest effect was observed in the group of children which remained TST positive at 6 and 12 years. Moreover the possible inß uence of natural M. tuberculosis infection was suggested. This contrasts with the majority of other studies in which the effect of BCG was tested, especially those from central and northern Europe and Asia, in which children gen-erally received only a single BCG immunisation in the neonatal period. In children from Guinea Bissau, Aaby found less positive SPT reactivity to aeroallergens among the BCG-immunised group compared to the non-immunised group.20 However, BCG exposure was deÞ ned as positive history of neonatal BCG immunisation or the presence of BCG-scar only. The lack of TST measurement in this study makes it difÞ cult to correct for the possi-ble additive inß uence of other mycobacteria on the results. In early BCG-immunised Esto-nian children, Annus et al. observed signiÞ cant inverse relation between TST response and the prevalence of allergic symptoms, but not of allergy SPT to common aeroallergens.30 Measurement of BCG immunisation in the children was based on school records. In a study in French children to evaluate the effect of early vaccination on allergic disease symptoms, Martignon et al. found lower prevalence of reported symptoms in children who received early BCG immunisation compared to non-immunised ones.37 The 2 studies on the effect of natural M. tuberculosis infection also differed with respect to duration of infection. In the UK study Pahari et al. investigated children with a recent (short) history of natural M. tuberculosis infection, after their teacher was diagnosed with pulmonary TB.22 In the study in South African children, we investigated children living in a TB endemic area (with TB
4 Does mycobacterial infection prevent the development of atopy in childhood?
59
notiÞ cation rate of 341/100 000 conÞ rmed smear positive TB in 2002).35 These children not only have a high cumulative burden of M. tuberculosis infection from the community, but the possible additive inß uence of MOTTs or M. bovis-BCG was not observed.
Differences in the efÞ cacy of BCG vaccine strains and the known regional differences in the vaccine efÞ cacy may contribute to the heterogeneity of study results, as this may lead to variability in immune response.48 There is evidence that this may partly be ascribed to differences in exposure to MOTT. This is demonstrated for instance, by the higher pre-vac-cination Th1 cytokine (IFN-γ) responses to MOTT antigens in Malawi than in the UK and greater BCG-attributable increases in IFN-γ responses in UK than in Malawi.49 Although it is not known if variability in the efÞ cacy of BCG immunisation against TB is related to the immune stimulation required to suppress the development of atopic inß ammation, it poses a relevant topic for future research.
Lack of uniformity in the deÞ nition of atopy makes it difÞ cult to compare results. This may also account for the heterogeneity of study results. While some studies deÞ ned atopy as questionnaire-reported symptoms or hypersensitivity to common environmental aller-gens, others used both deÞ nitions. The utilisation of the recently accepted World Allergy Organization (WAO) deÞ nition of atopy, as clinical allergic symptoms in combination with a positive SPT and/or an elevated serum IgE antibody level makes it possible for future studies to deÞ ne atopy more uniformly.50 Finally, heterogeneity in genetic background of the different study populations may strongly inß uence the outcome of the interaction be-tween mycobacterial infection and atopic disease. This has been reviewed elsewhere by Smit et al.51
In conclusion, this review on the relation between mycobacterial infection and atopy reveals that in contrast to studies in murine models, only a minority of studies in humans show evidence to support a protective effect of mycobacterial infection on the development of atopic disease. It further reveals a high level of heterogeneity of studies. Among possible explanations for the heterogeneity are differences in type, deÞ nition, dose and duration of mycobacterial exposure or infection, and lack of uniformity in the deÞ nition of atopy. Based on these Þ ndings, we believe that the causal relationship between mycobacterial in-fection and atopic disease can only be resolved with large scale prospective studies.

60
Infection with M. tuberculosis and atopy in children
References
1. ISAAC Steering Committee. Worldwide variation in prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and atopic eczema: ISAAC. Lancet 1998; 351:1225-32.
2. Strachan D. Hay fever, hygiene and household size. Br Med J 1989; 289:1259-60. 3. Hopkin JM. Atopy, asthma and the mycobacteria. Thorax 2000; 55:443-5. 4 Zuany-Amorim C, Sawicka E, Manlius C, Le Moine A, Brunet LR, Kemeny DM, et al. Suppres-
sion of airway eosinophilia by killed Mycobacterium vaccae-induced allergen-speciÞ c regula-tory T-cells. Nat Med 2002; 8:625�9.
5. Shaheen S, Aaby P, Hall A, Barker D, Heyes C, Shiell A, Goudiaby A. Measles and atopy in Guinea-Bissau. Lancet 1996; 347:1792-6.
6. Matricardi P, Rosmini F, Ferrigno L, Nasini R, Rapicetta M, Chionne P, Stroffolini T, Pascuini P, D�Amelio R.. Cross sectional retrospective study of prevalence of atopy among Italian military students with antibodies against hepatitis A virus. BMJ 1997; 314:999-1003.
7. Martinez FD, Wright AL, Taussig LM, Holbert CJ, Halonen M, Morgen WJ. Asthma and wheez-ing in the Þ rst six year of life. N Engl J Med 1995; 332:133- 8.
8.Wang CC, Rook GA. Inhibition of an established allergic response to ovalbumin in BALB/c mice by killed Mycobacterium vaccae. Immunology 1998; 93:307�13.
9. Erb K, Holloway J, Sobeck A, Moll H, Le Gros G. Infection of mice with Mycobacterium bovis-Bacillus Calmette-Guérin (BCG) suppresses allergen-induced airway eosinophilia. J Exp Med 1998; 187:561�9.
10. Von Mutius E, Pearce N, Beasley R, Cheng S, von Ehrenstein O, Björksten B, Weiland S. Inter-national patterns of tuberculosis and the prevalence of symptoms of asthma, rhinitis and eczema. Thorax 2000; 55:449-53.
11. Von Hertzen L, Klaukka T, Mattila H, Haahtela T. Mycobacterium tuberculosis infection and the subsequent development of asthma and allergic conditions. J Allergy Clin Immunol 1999; 104:1211-4.
12. Omenaas E, Jentoft H, Vollmer W, Buist A, Gulsvik A. Absence of relationship between tubercu-lin reactivity and atopy in BCG vaccinated adults. Thorax 2000; 5:454-8.
13. Shirakawa T, Enomoto T, Shimazu S, Hopkin J. The inverse association between tuberculin re-sponses and atopic disorder. Science 1997; 275:77-9.
14. Prescott S, Macaubas C, Smallacombe T, Holt B, Sly P, Holt P. Development of allergen-speciÞ c T-cell memory in atopic and normal children. Lancet 1999; 353:196-200.
15. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ 2003; 327:557-60.
16. Alm JS, Lilja G, Pershagen G, Scheynius A. Early BCG vaccination and development of atopy. Lancet 1997; 350:400-3.
17. Strannegård I, Larsson L, Wennergren G, Strannegård Ö. Prevalence of allergy in children in relation to prior BCG vaccination and infection with atypical mycobacteria. Allergy 1998; 53:249-54.
18. Yilmaz M, Bingöl G, Altintas D, Kendirli S. Correlation between atopic diseases and tuberculin responses. Allergy 2000; 55:664-7.
19. Nuhoglu Y, Nuhoglu C, Ozcay S. The association between delayed type hypersensitivity reaction to Mycobacterium tuberculosis and atopy in asthmatic children. Allergol et Immunopathol 2003; 31:14-7
20. Aaby P, Shaheen SO, Heyes CB, Goudiaby A, Hall AJ, Shiell AW, Jensen H, Marchant A. Early BCG vaccination and the reduction in atopy in Guinea-Bissau. Clin Exp Allergy 1999; 30:644-50.
21. Wong G, Hui D, Tam C, Chan H, Fok T, Chan-Yeung M, Lai C. Asthma, atopy and tuberculin
4 Does mycobacterial infection prevent the development of atopy in childhood?
61
responses in chinese schoolchildren in Hong Kong. Thorax 2001; 56:770-3.22. Pahari A, Welch S, Lingam S. BCG, tuberculin skin-test results and asthma prevalence in school
children in north London. Indian Pediatr 2002; 39:254-8.23. Grüber C, Kulig M, Bergmann R, Guggenmoos-Holzmann I, Wahn U, the MAS-90 group. De-
layed hypersensitivity to tuberculin, total immunoglobulin E, speciÞ c sensitization, and atopic manifestation in longitudinally followed early bacille Calmette-Guérin-vaccinated and non-vac-conated children. Pediatrics 2001; 107:e36.
24. Krause T, Hviid A, Koch A, Friborg J, Hjuler T, Wohlfahrt J, et.al. BCG vaccination and risk of atopy. JAMA 2003; 289:1012-5.
25. Jang A, Son M. The association of airway hyperresponsiveness and tuberculin responses. Allergy 2002; 57:341-5.
26. Ozmen S, Tomac N, Uysal A, Arslan Z, Kuyucu N, Yoney A. Tuberculin responses in children with allergic diseases. Allergy 2002; 57:1059-62.
27. Gruber C, Meinlschmidt G, Bergmann R, Wahn U, Stark K. Is early BCG vaccination asociated with less atopic disease? An epidemiological study in German preschool children with different ethnic backgrounds. Pediatr Allergy Immunol 2002; 13:177-81.
28. Ota M, van der Sande M, Walraven G, Jeffries D, Nyan O, Marchant A, et al. Absence of asso-ciation between delayed type hypersensitivity to tuberculin and atopy in children in The Gambia. Clin Exp Allergy 2003; 33:731-6.
29. Marks G, Ng K, Zhou J, Toelle B, Xuan W, Belousova E, et. al. The effect of neonatal BCG vac-cination on atopy and asthma at age 7 to 14 years: an historical cohort study in a community with a very low prevalence of tuberculosis infection and a high prevalence of atopic disease. J Allergy Clin Immunol 2003; 111:541-9.
30. Annus T, Montgomery S, Riikjärv M, Björkstén B. Atopic disorders among Estonian school-children in relation to tuberculin reactivity and the age at BCG vaccination. Allergy 2004; 59:1068-73.
31. Mommers M, Weishoff-Houben M, Swaen G, Creemers H, Freund H, Dott W, et al. Infant im-munization and the occurrence of atopic disease in Dutch and German children: a nested case-control study. Pediatric Pulmonology 2004; 38:329-34.
32. Cooper P, Chico M, Rodriguez L, Strachan D, Anderson H, Rodriguez E, et al. risk factors for at-opy among school children in a rural area of Latin America. Clin Exp Allergy 2004; 34:845-52.
33. Townley R, Barlan I, Patino C, Vichyanond P, Minervini M, Simasathien T, et al. The effect of BCG vaccine at birth on the development of atopy or allergic disease in young children. Ann Al-lergy Asthma Immunol 2004; 92:350-5.
34. Da Cunha S, Cruz A, Dourado I, Barreto M, Ferreira L, Rodriguez L. Lower prevalence of re-ported asthma in adolescents with symptoms of rhinitis that received neonatal BCG. Allergy 2004; 59:857-62.
35. Obihara C, beyers N, Gie R, Potter P, Marais B, Lombard C, Enarson D, Kimpen J. Inverse as-sociation between Mycobacterium tuberculosis infection and atopic rhinitis in children. Allergy 2005; 60:1121-5.
36. Bibakis I, Zekveld C, Dimitroulis I, Pedioti A, Gerakianaki T, Fanourgiaki S, et al. Childhood atopy and allergic disease and skin test responses to environmental mycobacteria in rural Crete: a cross-sectional study. Clin Exp Allergy 2005; 35:624-9.
37. Martignon G, Oryszczyn M, Annesi-Maesano I. Does childhood immunization against infec-tious diseases protect from the development of atopic disease? Pediatr Allergy Immunol 2005; 16:193-200.
38. Von Hertzen LC, Haahtela T. Could the risk of asthma and atopy be reduced by vaccine that in-duces a strong T-helper type 1 response? Am J Respir Cell Mol Biol 2000; 22:139-42.
39. Trincheri G. Cytokines acting on or secreted by macrophages during intracellular infection (IL-

62
Infection with M. tuberculosis and atopy in children
10, IL-12, IFN-γ). Curr Opin Immunol 1997; 9:17-23.40. Shingadia D, Novelli V. Diagnosis and treatment of tuberculosis in children. Lancet Infect Dis
2003; 3:624-32.41. Committee of Infectious Disease. Screening for tuberculosis in infants and children. Pediatrics
1994; 93:131�4.42. Black GF, Fine PEM, Warndorff DK, Floyd S, Weir RE, Blackwell JM, et al. Relationship be-
tween IFN-γ and skin test responsiveness to Mycobacterium tuberculosis PPD in healthy, non-BCG-vaccinated young adults in Northern Malawi. Int J Tuberc Lung Dis 2001; 7:664�72.
43. Lienhardt C, Sillah J, Fielding K, Donkor S, Manneh K, Warndorff D, et al. Risk factors for tu-berculosis infection in children with contact with infectious tuberculosis cases in The Gambia, West Africa. Pediatrics 2003; 111:e608.
44. Johnson H, Lee B, Doherty E, Kelly E, McDonnell T. Tuberculin sensitivity and the CG scar in tuberculosis contacts. Tuberc Lung Dis 1995; 76:122-5.
45. Matricardi PM, Yazdanbakhsh M. Mycobacteria and atopy, 6 years later: a fascinating, still unÞ -nished, business. Clin Exp Allergy 2003 ; 33 :717-20.
46. Yazdanbakhsh M, Van den Biggelaar A, Maizels RM. Th2 responses without atopy: immuno-regulation in chronic helminth infections and reduced allergic disease. Trends in Immunology 2001; 22:372-7.
47. Mills KH. Regulatory T cells: friend or foe in immunity to infection? Nat Rev Immunol 2004; 4: 841-55
48. Fine PEM. Variation in protection by BCG: implications of and for heterologous immunity. Lan-cet 1995; 346:1339-45.
49. Black GF, Weir RE, Floyd S, Bliss L, Warndorff DK, Crampin AC, et al. BCG-induced increase in interferon-gamma response to mycobacterial antigens and efÞ cacy of BCG vaccination in Ma-lawi and the UK: two randomised controlled studies. Lancet 2002; 359:1393-401.
50. Johansson SGO, Bieber T, Dahl R, Friedmann P, Lanier BQ, Lockey RF, Motala C, Ortega Mar-tell JA, Platt-Mills TA, Ring J, et al. Revised nomenclature for allergy for global use: report of the Nomenclature Review Committee of the World Allergy Organization, October 2003. J Al-lergy Clin Immunol 2004;113:832-6.
51. Smit JJ, Folkerts G, Nijkamp FP. Mycobacteria, genes and the �hygiene hypothesis�. Curr Opin Allergy Clin Immunol 2004; 4:57-62.

C H A P T E R 5
Mycobacterium tuberculosis infection may protect against allergy in a tuberculosis endemic area
Charles C. ObiharaJan L.L. KimpenRobert P. GieSchalk W. van LillMaarten O. HoekstraBen J. MaraisH. Simon SchaafKatherine LawrencePaul C. PotterEric D. BatemanCarl J. LombardNulda Beyers
Clinical and Experimental Allergy2006; 36:70-6
64
Infection with M. tuberculosis and atopy in children
Abstract
BackgroundEpidemiological studies have shown an inverse relation of mycobacterial infection and
the frequency of allergic diseases and asthma. Recent evidence suggests that allergic in-ß ammation may be inhibited in the presence of chronic and persistent infections, such as that by Mycobacterium tuberculosis (M. tuberculosis). The relation of tuberculin skin test (TST) size, an accepted marker of M. tuberculosis infection and the frequency of allergic disease symptoms has not been reported from an area where M. tuberculosis infection is endemic.
ObjectiveTo investigate the association of TST and allergic disease symptoms, in children living
in a tuberculosis endemic area.
Methods:In this cross-sectional study, 841 children aged 6-14 years from randomly selected
household-addresses in two poor communities of Cape Town, South Africa, were inves-tigated with TST and standardized International Study on Asthma and Allergies in Child-hood-based questionnaire on allergic disease symptoms.
ResultsChildren with positive TST (≥ 10 mm) were signiÞ cantly less likely to have allergic
disease symptoms, in particular allergic rhinitis (AR) (adjusted odds ratio 0.43; 95% conÞ -dence interval 0.24-0.79) than those with negative TST. This association remained signiÞ -cant after adjusting for possible confounders and correcting for the effect of clustering (>1 child per household address) in the sample. There was a signiÞ cant inverse linear trend in the relation of TST size in mm and the frequency of allergic disease symptoms, in particu-lar AR (P < 0.001).
ConclusionsThese results of inverse association of strong TST reaction and allergic disease symp-
toms in children from a tuberculosis endemic area are in support of the hypotheses that al-lergic inß ammation may be inhibited by chronic infections, such as M. tuberculosis.

5 Mycobacterium tuberculosis infection may protect against allergy
65
Introduction
The immune response against Mycobacterium tuberculosis (M. tuberculosis) has poten-tial protective effect on the development of atopic disease and asthma.1,2 This is of particu-lar relevance given the interest in the use of mycobacterial products as a potential vaccine against atopic disease. M. tuberculosis infection induces a strong T helper (Th) 1 immune response, with production of gamma-interferon (IFN-γ).3,4 The expression of Th2 skewed immunity against antigens resulting in the production of cytokines that promote IgE pro-duction and eosinophilia is recognized as the primary cause of allergic inß ammation in atopic individuals.5
An important marker of Th1�mediated immunity is the development of delayed-type hypersensitivity (DTH), which can be evaluated by the tuberculin skin test (TST).1,6 TST reactivity becomes apparent in 3-6 weeks after initial M. tuberculosis infection and may remain positive for the lifetime of the individual.7 The size of TST induration has been directly correlated with serum levels of IFN-γ, implying that a large TST size may reß ect strong Th1 immunity.6
Decline in infection with mycobacteria may be an underlying factor in the rising preva-lence of allergic diseases in developed countries.1,2 Although some research groups have reported an inverse association of a positive TST and atopic disease, the linear relationship between the size of TST and allergic disease symptoms has not been investigated. In addi-tion most previous studies were carried out in populations with low incidence of M. tuber-culosis infection.2,8,9 It is not clear how TST reactivity and tuberculosis (TB) impact on the development of atopy in developing countries, where M. tuberculosis infection is endemic and allergy common. This study was conducted in a third-world community with a very high incidence of M. tuberculosis infection, where allergic disease symptoms are also com-mon.10-13 We tested the association of TST reactivity or size of TST and the frequency of allergic disease symptoms in the paediatric population.
Methods
Study areaThe study area is an established epidemiological Þ eld-site comprising of two urban
communities in metropolitan Cape Town, South Africa, with a population of 36.334 in 2001, predominantly of mixed ethnicity (previously categorized as �coloured�).10 The pop-ulation density is high (average of 6 to14 persons per household). The people live in poor socioeconomic conditions, although all households have running water and electricity. The TB notiÞ cation rate was 341 per 100.000 for new smear-positive TB and 612 per 100.000 for bacteriological conÞ rmed TB in 2002. Childhood TB cases comprise up to 39% of to-tal TB case-load.11 The prevalence of asthma in children in Cape Town is 13.3%, allergic rhinoconjunctivitis 16%, and eczema 9%.13 The vaccination policy in the area requires all children to receive a single dose of M. bovis BCG immunization (Tokyo BCG strain) dur-ing the Þ rst week of life.
66
Infection with M. tuberculosis and atopy in children
Between July and December 2002 a 15% sample of household-addresses was randomly selected. Trained community workers enumerated the people at each address and children aged 6-14 years were invited to participate in the study. Written informed consent for each child was obtained from a parent or legal guardian before enrolment in the study.
A TST was performed, an allergy-questionnaire completed and the presence (or ab-sence) of a BCG scar recorded for each child. Children with known immune compromis-ing diseases or active symptomatic TB were excluded. Children less than 6 years of age were not included in order to reduce diagnostic bias, in particular the problem of transient wheeze due to recurrent respiratory tract viral infections in this age category. The propor-tion of HIV-1-infected persons in the area is among the lowest in South Africa.12 However, children with questionnaire-reported positive HIV test were excluded, because of the pos-sible effect on T cell immunity.
Parents completed a questionnaire for each child, under supervision of a trained com-munity worker. Questions on allergic disease symptoms were based on a standardized, val-idated Phase-I International Study on Asthma and Allergies in Childhood (ISAAC) ques-tionnaire translated into the local language (Afrikaans). Questions were asked on previous and recent (≤12 months) symptoms of asthma, allergic rhinitis (AR) and eczema. Other questions were on neonatal BCG immunization, previous TB disease, parental allergic his-tory, number of siblings, environmental tobacco smoke (ETS) exposure in the household, maternal education and household income.
TST was carried out by experienced research-nurses by administering 2 tuberculin units (TU) of puriÞ ed protein derivative (PPD) RT 23 (Statens, Serum Institut, Copenhagen, Denmark) intradermally on the volar aspect of the left arm. The largest transverse diam-eter of induration was recorded after 2 to 3 days. Based on the American Thoracic Society guidelines, a positive TST was deÞ ned as an induration of 10 mm or more.14
Children with symptoms and/or chest radiograph suggestive of active TB disease were referred for further diagnosis and treatment in accordance with the National TB programme. They were excluded from the analysis.
Defi nitions AR, asthma and eczema refer to questionnaire-reported symptoms. �Any allergic symp-
tom� in this paper refers to the presence of any reported allergic disease symptom (AR, asthma or eczema).
Statistical analysis Univariate and linear-trend analyses of the relation of TST reactivity and allergic dis-
ease symptoms were performed using the Chi-squared test (SPSS version 11·0). Regression analyses were performed using a random-effects logistic regression (LR) model (STATA 8·0). In this model allergic disease symptoms were used as the dependent variable and TST reactivity as the independent variable, and correction was made for potential confounders: demographic (age and sex) genetic (parental allergic history), socioeconomic variables (household income and number of siblings) and ETS exposure in the household. A total of 506 household-addresses were included in the study, with an average of 1.6 children per
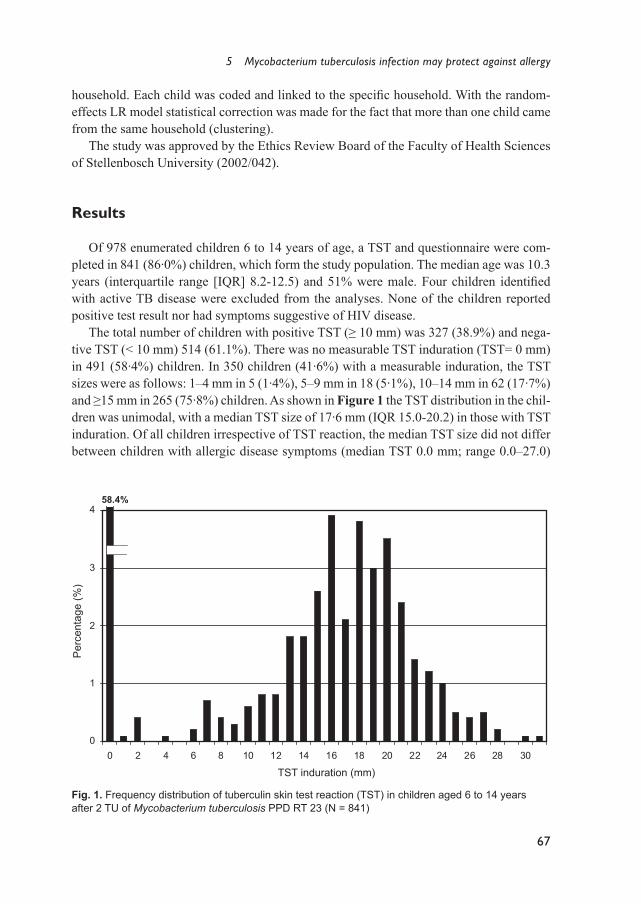
5 Mycobacterium tuberculosis infection may protect against allergy
67
household. Each child was coded and linked to the speciÞ c household. With the random-effects LR model statistical correction was made for the fact that more than one child came from the same household (clustering).
The study was approved by the Ethics Review Board of the Faculty of Health Sciences of Stellenbosch University (2002/042).
Results
Of 978 enumerated children 6 to 14 years of age, a TST and questionnaire were com-pleted in 841 (86·0%) children, which form the study population. The median age was 10.3 years (interquartile range [IQR] 8.2-12.5) and 51% were male. Four children identiÞ ed with active TB disease were excluded from the analyses. None of the children reported positive test result nor had symptoms suggestive of HIV disease.
The total number of children with positive TST (≥ 10 mm) was 327 (38.9%) and nega-tive TST (< 10 mm) 514 (61.1%). There was no measurable TST induration (TST= 0 mm) in 491 (58·4%) children. In 350 children (41·6%) with a measurable induration, the TST sizes were as follows: 1�4 mm in 5 (1·4%), 5�9 mm in 18 (5·1%), 10�14 mm in 62 (17·7%) and ≥15 mm in 265 (75·8%) children. As shown in Figure 1 the TST distribution in the chil-dren was unimodal, with a median TST size of 17·6 mm (IQR 15.0-20.2) in those with TST induration. Of all children irrespective of TST reaction, the median TST size did not differ between children with allergic disease symptoms (median TST 0.0 mm; range 0.0�27.0)
0
1
2
3
4
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30
TST induration (mm)
Per
cent
age
(%)
58.4%
TST induration (mm)
Per
cent
age
(%)
Fig. 1. Frequency distribution of tuberculin skin test reaction (TST) in children aged 6 to 14 years after 2 TU of Mycobacterium tuberculosis PPD RT 23 (N = 841)
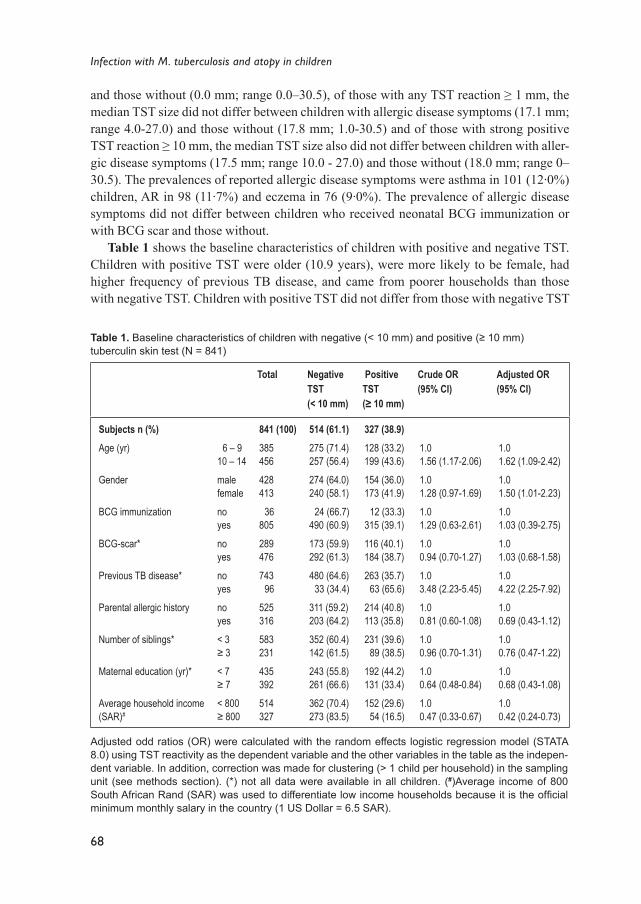
68
Infection with M. tuberculosis and atopy in children
Table 1. Baseline characteristics of children with negative (< 10 mm) and positive (≥ 10 mm) tuberculin skin test (N = 841)
Total Negative TST (< 10 mm)
Positive TST (≥ 10 mm)
Crude OR(95% CI)
Adjusted OR(95% CI)
Subjects n (%)Age (yr)
Gender
BCG immunization
BCG-scar*
Previous TB disease*
Parental allergic history
Number of siblings*
Maternal education (yr)*
Average household income (SAR)#
6 � 910 � 14
malefemale
noyes
noyes
noyes
noyes
< 3≥ 3
< 7 ≥ 7
< 800≥ 800
841 (100)385 456
428 413
36 805
289 476
743 96
525 316
583 231
435 392
514 327
514 (61.1)275 (71.4)257 (56.4)
274 (64.0)240 (58.1)
24 (66.7)490 (60.9)
173 (59.9)292 (61.3)
480 (64.6) 33 (34.4)
311 (59.2)203 (64.2)
352 (60.4)142 (61.5)
243 (55.8)261 (66.6)
362 (70.4)273 (83.5)
327 (38.9)128 (33.2)199 (43.6)
154 (36.0)173 (41.9)
12 (33.3)315 (39.1)
116 (40.1)184 (38.7)
263 (35.7) 63 (65.6)
214 (40.8)113 (35.8)
231 (39.6) 89 (38.5)
192 (44.2)131 (33.4)
152 (29.6) 54 (16.5)
1.01.56 (1.17-2.06)
1.01.28 (0.97-1.69)
1.01.29 (0.63-2.61)
1.00.94 (0.70-1.27)
1.03.48 (2.23-5.45)
1.00.81 (0.60-1.08)
1.00.96 (0.70-1.31)
1.00.64 (0.48-0.84)
1.00.47 (0.33-0.67)
1.01.62 (1.09-2.42)
1.01.50 (1.01-2.23)
1.01.03 (0.39-2.75)
1.01.03 (0.68-1.58)
1.04.22 (2.25-7.92)
1.00.69 (0.43-1.12)
1.00.76 (0.47-1.22)
1.00.68 (0.43-1.08)
1.00.42 (0.24-0.73)
Adjusted odd ratios (OR) were calculated with the random effects logistic regression model (STATA 8.0) using TST reactivity as the dependent variable and the other variables in the table as the indepen-dent variable. In addition, correction was made for clustering (> 1 child per household) in the sampling unit (see methods section). (*) not all data were available in all children. (#)Average income of 800 South African Rand (SAR) was used to differentiate low income households because it is the ofÞ cial minimum monthly salary in the country (1 US Dollar = 6.5 SAR).
and those without (0.0 mm; range 0.0�30.5), of those with any TST reaction ≥ 1 mm, the median TST size did not differ between children with allergic disease symptoms (17.1 mm; range 4.0-27.0) and those without (17.8 mm; 1.0-30.5) and of those with strong positive TST reaction ≥ 10 mm, the median TST size also did not differ between children with aller-gic disease symptoms (17.5 mm; range 10.0 - 27.0) and those without (18.0 mm; range 0� 30.5). The prevalences of reported allergic disease symptoms were asthma in 101 (12·0%) children, AR in 98 (11·7%) and eczema in 76 (9·0%). The prevalence of allergic disease symptoms did not differ between children who received neonatal BCG immunization or with BCG scar and those without.
Table 1 shows the baseline characteristics of children with positive and negative TST. Children with positive TST were older (10.9 years), were more likely to be female, had higher frequency of previous TB disease, and came from poorer households than those with negative TST. Children with positive TST did not differ from those with negative TST
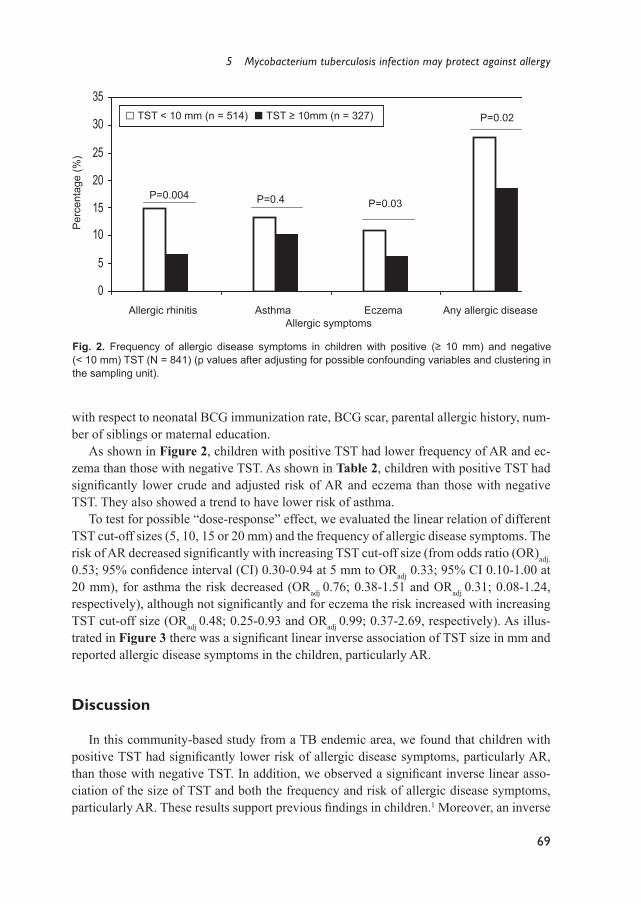
5 Mycobacterium tuberculosis infection may protect against allergy
69
Fig. 2. Frequency of allergic disease symptoms in children with positive (≥ 10 mm) and negative (< 10 mm) TST (N = 841) (p values after adjusting for possible confounding variables and clustering in the sampling unit).
0
5
10
15
20
25
30
35
Allergic rhinitis Asthma Eczema Any allergic disea
Allergic symptoms
Percentage(%
)
P=0.004 P=0.4 P=0.03
P=0.02
Per
cent
age
(%)
Allergic rhinitis Asthma Eczema Any allergic diseaseAllergic symptoms
with respect to neonatal BCG immunization rate, BCG scar, parental allergic history, num-ber of siblings or maternal education.
As shown in Figure 2, children with positive TST had lower frequency of AR and ec-zema than those with negative TST. As shown in Table 2, children with positive TST had signiÞ cantly lower crude and adjusted risk of AR and eczema than those with negative TST. They also showed a trend to have lower risk of asthma.
To test for possible �dose-response� effect, we evaluated the linear relation of different TST cut-off sizes (5, 10, 15 or 20 mm) and the frequency of allergic disease symptoms. The risk of AR decreased signiÞ cantly with increasing TST cut-off size (from odds ratio (OR)adj. 0.53; 95% conÞ dence interval (CI) 0.30-0.94 at 5 mm to ORadj 0.33; 95% CI 0.10-1.00 at 20 mm), for asthma the risk decreased (ORadj 0.76; 0.38-1.51 and ORadj 0.31; 0.08-1.24, respectively), although not signiÞ cantly and for eczema the risk increased with increasing TST cut-off size (ORadj 0.48; 0.25-0.93 and ORadj 0.99; 0.37-2.69, respectively). As illus-trated in Figure 3 there was a signiÞ cant linear inverse association of TST size in mm and reported allergic disease symptoms in the children, particularly AR.
Discussion
In this community-based study from a TB endemic area, we found that children with positive TST had signiÞ cantly lower risk of allergic disease symptoms, particularly AR, than those with negative TST. In addition, we observed a signiÞ cant inverse linear asso-ciation of the size of TST and both the frequency and risk of allergic disease symptoms, particularly AR. These results support previous Þ ndings in children.1 Moreover, an inverse
□ TST < 10 mm (n = 514) ■ TST ≥ 10mm (n = 327)

70
Infection with M. tuberculosis and atopy in children
Tabl
e 2.
Cru
de a
nd a
djus
ted
risk
of d
iffer
ent a
llerg
ic s
ympt
oms
in c
hild
ren
with
pos
itive
(≥ 1
0 m
m) a
nd n
egat
ive
(< 1
0 m
m) t
uber
culin
ski
n te
st (T
ST)
, tog
ethe
r with
con
foun
ding
va
riabl
es in
clud
ed
Varia
ble
Aller
gic r
hini
tisAs
thm
aEc
zem
a
n/N
(%)
Crud
e OR
(95%
CI)
Adju
sted
OR*
(95%
CI)
n/N
(%)
Crud
e OR
(95%
CI)
Adju
sted
OR*
(95%
CI)
n/N
(%)
Crud
e OR
(95%
CI)
Adju
sted
OR*
(95%
CI)
TST
size (
mm)
<
10
≥ 10
Age (
yr)
6-9
10
-14
Gend
er
Male
Fe
male
Pare
ntal a
llerg
ic his
tory
No
Ye
s
Aver
age h
ouse
hold
incom
e (SA
R)
< 80
0
≥ 80
0
Numb
er of
sibli
ngs
<
3
≥ 3
ETS
expo
sure
in th
e hou
seho
ld
No
Yes
76/51
4 (14
.8)22
/327 (
6.7)
39/38
4 (9.9
)60
/456 (
13.2)
54/42
7 (12
.6)45
/413 (
10.7)
48/61
3 (7.8
)50
/227 (
22.0)
56/63
4 (8.8
)42
/206 (
20.4)
79/58
2 (13
.6)17
/231 (
7.4)
44/33
7 (13
.1)53
/499 (
10.6)
1.0 0.42 (
0.25-
0.68)
1.0 1.38 (
0.90-
2.12)
1.0 0.82 (
0.54-
1.26)
1.0 3.32 (
2.16-
5.11)
1.0 2.64 (
1.70-
4.01)
1.0 0.51 (
0.29-
0.88)
1.0 0.79 (
0.52-
1.21)
1.0 0.43 (
0.24-
0.79)
1.0 1.80 (
1.06-
3.08)
1.0 0.87 (
0.52-
1.47)
1.0 3.57 (
2.01-
6.34)
1.0 2.21 (
1.20-
4.07)
1.0 0.53 (
0.27-
1.06)
1.0 0.96 (
0.55-
1.67)
68/51
1 (13
.3)33
/325 (
10.2)
56/38
3 (14
.6)45
/453 (
9.9)
61/42
5 (14
.4)40
/411 (
9.7)
55/61
1 (9.0
)46
/225 (
20.4)
71/63
1 (11
.3)30
/205 (
14.6)
77/57
9 (13
.3)18
/230 (
7.8)
34/33
6 (10
.1)66
/496 (
13.3)
1.0 0.74 (
0.47-
1.15)
1.0 0.64 (
0.42-
0.98)
1.0 0.64 (
0.42-
0.98)
1.0 2.60 (
1.70-
3.98)
1.0 1.35 (
0.85-
2.14)
1.0 0.55 (
0.32-
0.95)
1.0 1.36 (
0.88-
2.12)
1.0 0.72 (
0.35-
1.45)
1.0 0.52 (
0.27-
0.98)
1.0 0.52 (
0.26-
1.01)
1.0 4.16 (
1.84-
9.41)
1.0 1.33 (
0.57-
3.08)
1.0 0.56 (
0.24-
1.29)
1.0 1.72 (
0.80-
3.69)
56/51
0 (11
.0)20
/324 (
6.2)
36/38
3 (9.4
)40
/451 (
8.9)
36/42
5 (8.5
)40
/409 (
9.8)
44/60
8 (7.2
)32
/226 (
14.2)
57/62
9 (9.1
)19
/205 (
9.3)
54/57
8 (9.3
)18
/230 (
7.8)
33/33
4 (9.9
)42
/496 (
8.5)
1.0 0.53 (
0.31-
0.91)
1.0 0.94 (
0.59-
1.51)
1.0 1.17 (
0.73-
1.88)
1.0 2.11 (
1.30-
3.43)
1.0 1.03 (
0.59-
1.77)
1.0 0.82 (
0.47-
1.44)
1.0 0.84 (
0.52-
1.36)
1.0 0.50 (
0.26-
0.99)
1.0 1.00 (
0.59-
1.61)
1.0 1.35 (
0.83-
2.76)
1.0 2.58 (
1.34-
4.96)
1.0 0.75 (
0.43-
1.56)
1.0 0.74 (
0.36-
1.53)
1.0 0.82 (
0.43-
1.56)
* Adj
uste
d od
ds ra
tio (O
R):
calc
ulat
ed w
ith th
e ra
ndom
-effe
cts
logi
stic
regr
essi
on (L
R) m
odel
, usi
ng a
llerg
ic s
ympt
om a
s th
e de
pend
ent v
aria
ble
and
TST
size
toge
ther
with
all
the
othe
r pos
sibl
e co
nfou
ndin
g va
riabl
es in
clud
ed in
the
tabl
e as
inde
pend
ent v
aria
ble.
In a
dditi
on, c
orre
ctio
n w
as m
ade
for c
lust
erin
g (>
1 c
hild
per
hou
seho
ld) i
n th
e sa
mpl
ing
unit
(see
met
hods
sec
tion)
. SA
R =
Sou
th A
frica
n R
and
(1 U
S D
olla
r = 6
.5 S
AR
). Av
erag
e in
com
e of
800
Sou
th A
frica
n R
and
(SA
R) w
as u
sed
to d
iffer
entia
te lo
w in
com
e ho
useh
olds
be
caus
e it
is th
e ofÞ c
ial m
inim
um m
onth
ly s
alar
y in
the
coun
try. E
TS=
envi
ronm
enta
l tob
acco
sm
oke
expo
sure
is d
eÞ n
ed a
s qu
estio
nnai
re-r
epor
ted
expo
sure
to to
bacc
o sm
oke
at h
ome
by a
n ad
ult l
ivin
g in
the
sam
e ho
useh
old
as th
e ch
ild.

5 Mycobacterium tuberculosis infection may protect against allergy
71
linear association of TST size and the frequency of allergic disease symptoms especially AR in children is being shown for the Þ rst time.
Recent evidence suggests that M. tuberculosis infection, a strong Th1 stimulator, may inhibit Th2 associated allergic inß ammation.1,2 The size of the TST has been correlated with the serum level of IFN-γ,6 implying that a large TST size reß ects strong Th1 activity which may antagonize Th2 activity.1 The large median TST induration and typical pattern of the TST distribution in the children implies more of natural M. tuberculosis infection than of BCG or non-tuberculous mycobacteria (NTM) infection, which generally provoke a weak-er TST induration.7,14 The demonstration of an inverse linear association of the size of TST and allergic disease symptoms suggests a �dose-response� effect which may be evident in the presence of strong Th1 activity, caused by M. tuberculosis.15 This �dose-response� as-sociation suggests causal relationship, according to the epidemiological criteria of causal relation proposed by Liu and Murphy.16 In the light of novel explanatory models of the hygiene hypothesis it has been postulated that expression of allergic inß ammation may be inhibited in persons exposed to chronic infections such as that caused by M. tuberculosis, through the stimulation of regulatory T cells (Tregs) and anti-inß ammatory networks.15,17,18 In animal models, Tregs, induced by killed mycobacteria inhibited allergen-induced airway inß ammation, via the anti-inß ammatory cytokines, interleukin (IL)-10 and TGF-β.18 Some researchers have suggested that decreased or defective cell-mediated immunity in atopic children leading to impaired DTH reactivity, may explain the inverse association of TST size and allergic disease.8,19 We could not exclude that children with allergic disease symp-toms or predisposed to allergic disease, tend to mount less intense Th1-type responses to M. tuberculosis infection. However, the evidence against this argument in our study is that although there was a signiÞ cant difference in the prevalence of allergic disease symptoms in children with positive TST compared to those with negative TST, the median TST size did not differ between children with and without allergic disease symptoms, irrespective of the TST size. This seems to indicate that both these groups mount a comparable and adequate Th1 response. Although there was a trend towards reduced risk of positive TST reactivity in children of allergic parents, this difference was not statistically signiÞ cant.
In our study the strongest effect was observed in children with AR. This is in support of previous Þ ndings in Japanese children and may be explained by the fact that AR has a stronger correlation with atopy, than asthma or eczema.1,20,21 Epidemiological differences have been described between different allergic diseases.20 For instance, one review showed that only 25 to 63 % of asthmatic symptoms in children may be of atopic origin.21 The weaker inverse linear association of TST size and eczema may partly be explained by the high prevalence of other skin disorders in poor children, such as non-atopic dermatitis, or infections with Sarcoptes scabiei, which health-workers may confuse with eczema. Alter-natively, eczema may have a different immune mechanism as suggested by its more com-plex natural history.22
Although it has been reported that BCG immunization in the Þ rst week of life may be protective against the development of atopic sensitisation, the same results could not be reproduced in Sweden or Greenland.23-25 In the present study we did not Þ nd less allergic disease symptoms in children who received BCG vaccination in the Þ rst week of life. The
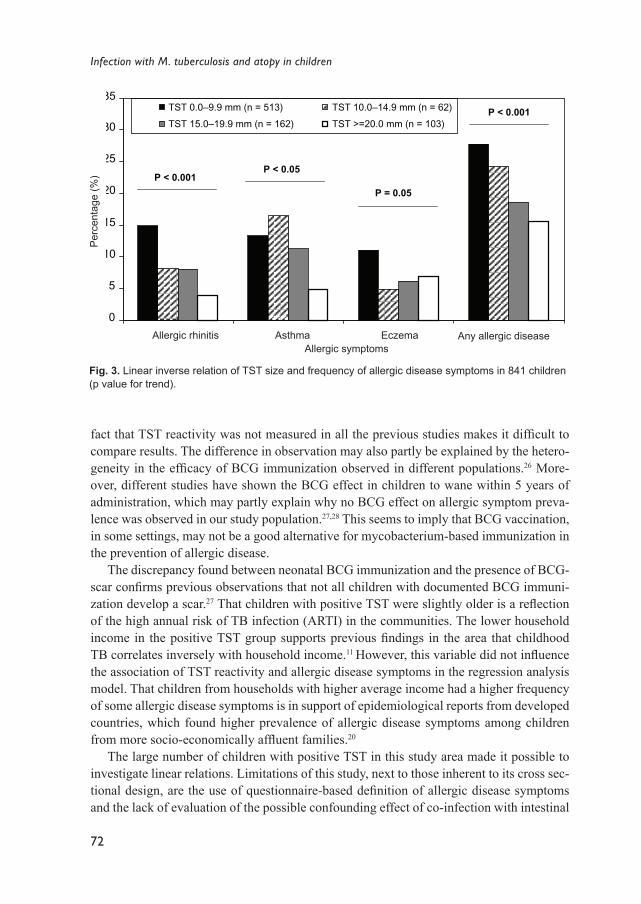
72
Infection with M. tuberculosis and atopy in children
fact that TST reactivity was not measured in all the previous studies makes it difÞ cult to compare results. The difference in observation may also partly be explained by the hetero-geneity in the efÞ cacy of BCG immunization observed in different populations.26 More-over, different studies have shown the BCG effect in children to wane within 5 years of administration, which may partly explain why no BCG effect on allergic symptom preva-lence was observed in our study population.27,28 This seems to imply that BCG vaccination, in some settings, may not be a good alternative for mycobacterium-based immunization in the prevention of allergic disease.
The discrepancy found between neonatal BCG immunization and the presence of BCG-scar conÞ rms previous observations that not all children with documented BCG immuni-zation develop a scar.27 That children with positive TST were slightly older is a reß ection of the high annual risk of TB infection (ARTI) in the communities. The lower household income in the positive TST group supports previous Þ ndings in the area that childhood TB correlates inversely with household income.11 However, this variable did not inß uence the association of TST reactivity and allergic disease symptoms in the regression analysis model. That children from households with higher average income had a higher frequency of some allergic disease symptoms is in support of epidemiological reports from developed countries, which found higher prevalence of allergic disease symptoms among children from more socio-economically afß uent families.20
The large number of children with positive TST in this study area made it possible to investigate linear relations. Limitations of this study, next to those inherent to its cross sec-tional design, are the use of questionnaire-based deÞ nition of allergic disease symptoms and the lack of evaluation of the possible confounding effect of co-infection with intestinal
0
5
10
15
20
25
30
35
Allergic rhinitis Asthma Eczema Any allergic symptom
Allergic symptoms
P < 0.001P < 0.05
P = 0.05
P < 0.001TST 0.0–9.9 mm (n = 513)
TST 15.0–19.9 mm (n = 162)
TST 10.0–14.9 mm (n = 62)
TST >=20.0 mm (n = 103)
Per
cent
age
(%)
Allergic rhinitis Asthma Eczema Any allergic diseaseAllergic symptoms
Fig. 3. Linear inverse relation of TST size and frequency of allergic disease symptoms in 841 children (p value for trend).
5 Mycobacterium tuberculosis infection may protect against allergy
73
parasites. Limitation of questionnaire-based deÞ nition of allergic disease symptom was reduced by using the standardized validated ISAAC questionnaire. A more objective mea-sure of atopy, such as skin prick testing would have further strengthened the study design.
In conclusion, our data show an inverse association of strong TST reaction and allergic disease symptoms, especially AR, in children living in a TB endemic area. This data is in support of new insights in the explanation of the hygiene hypothesis, of possible inhibition of allergic inß ammation in the presence of chronic and persistent infections, such as M. tu-berculosis, probably through the stimulation of Tregs and production of anti-inß ammatory networks. More detailed studies in similar settings are needed to conÞ rm the present Þ nd-ings, considering the possibility of the future use of mycobacterial products as a potential vaccine against atopic disease.
74
Infection with M. tuberculosis and atopy in children
References
1. Shirakawa T, Enomoto T, Shimazu S, Hopkin J. The inverse association between tuberculin re-sponses and atopic disorder. Science 1997; 275:77�9.
2. Von Mutius E, Pearce N, Beasley R, Cheng S, von Ehrenstein O, Björkstén B, et al. International patterns of tuberculosis and the prevalence of symptoms of asthma, rhinitis and atopic dermatitis. Thorax 2000; 55:449�53.
3. Cooper A, Roberts A, Rhoades E, Callahan J, Getzy D, Orme I. The role of interleukin- 12 in acquired immunity to Mycobacterium tuberculosis infection. Immunology 1995; 84:423�32.
4. Orme I, Andersen P, Boom W. T cell response to Mycobacterium tuberculosis. J Infect Dis 1993; 167:1481�97.
5. Romagnani S. Regulation of the development of type 2 T-cells in allergy. Curr Opinion Immunol 1994; 6:838�46.
6. Black GF, Fine PEM, Warndorff DK, Floyd S, Weir RE, Blackwell JM, et al. Relationship be-tween IFN-γ and skin test responsiveness to Mycobacterium tuberculosis PPD in healthy, non-BCG-vaccinated young adults in Northern Malawi. Int J Tuberc Lung Dis 2001; 7:664�72.
7. Shingadia D, Novelli V. Diagnosis and treatment of tuberculosis in children. Lancet Infect Dis 2003; 3:624-32.
8. Strannegård I, Larsson L, Wennergren G, Strannegård Ö. Prevalence of allergy in children in relation to prior BCG vaccination and infection with atypical mycobacteria. Allergy 1998; 53:249�54.
9. Von Hertzen L, Klaukka T, Mattila H, Haahtela T. Mycobacterium tuberculosis infection and the subsequent development of asthma and allergic conditions. J Allergy Clin Immunol 1999; 104:1211�4.
10. Statistical Support and Informatics. Statistics South Africa: Western Cape. Census 2001.11. Van Rie A, Beyers N, Gie RP, Kunneke M, Zietsman L, Donald PR. Childhood tuberculosis in an
urban population in South Africa: burden and risk factor. Arch Dis Child 1999; 80:433�7.12. Verver S, Warren RM, Munch Z, Richardson M, van der Spuy GD, Borgdorff Mw, et al. Pro-
portion of tuberculosis transmission that takes place in a high-incidence area. Lancet 2004; 363:212�4.
13. ISAAC Steering Committee. Worldwide variation in prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and atopic eczema: ISAAC. Lancet 1998; 351:1225�32.
14. Committee of Infectious Disease. Screening for tuberculosis in infants and children. Pediatrics 1994; 93:131�4.
15. Matricardi PM, Yazdanbakhsh M. Mycobacteria and atopy, 6 years later: a fascinating, still un-Þ nished, business. Clin Exp Allergy 2003; 33:717-20.
16. Liu AH, Murphy JR. Hygiene hypothesis: fact or Þ ction. J Allergy Clin Immunol 2003; 111:471-8.
17. Romagnani S. Immunologic inß uences on allergy and TH1/ TH2 balance. J Allergy Clin Immunol 2004; 113:395-400.
18. Zuany-Amorim C, Sawicka E, Manlius C, Le Moine A, Brunet LR, Kemeny DM, et al. Suppres-sion of airway eosinophilia by killed Mycobacterium vaccae-induced allergen-speciÞ c regula-tory T-cells. Nat Med 2002; 8:625�9.
19. Reinhold U, Wehrmann W, Kukel S, Kreysel H. Evidence that defective interferon-gamma pro-duction in atopic dermatitis patients is due to intrinsic abnormalities. Clin Exp Immunol 1990; 79:374-9.
20. Strachan DP. Family size, infection and atopy: the Þ rst decade of the �hygiene hypothesis�. Tho-rax 2000; 55 (Suppl 1):S2�S10.
21. Pearce N, Pekkanen J, Beasley R. How much asthma is really attributable to atopy? Thorax 1999;
5 Mycobacterium tuberculosis infection may protect against allergy
75
54:268�72.22. Saarinen UM, Kajosaari M. Breastfeeding as prophylaxis against atopic diseases: prospective
follow-up until 17 years old. Lancet 1995; 346:1065�9.23. Aaby P, Shaheen SO, Heyes CB, Goudiaby A, Hall AJ, Shiell AW, et al. Early BCG vaccination
and the reduction in atopy in Guinea-Bissau. Clin Exp Allergy 1999; 30:644�50.24. Alm J, Lilja G, Pershagen G, Scheynius A. Early BCG vaccination and development of atopy.
Lancet 1997; 350:400�03.25. Krause TG, Hviid A, Koch A, Friborg J, Hjuler T, Wohlfahrt J et al. JAMA 2003; 289:1012-5.26. Fine PEM. Variation in protection by BCG: implications of and for heterologous immunity. Lan-
cet 1995; 346:1339-45.27. Lienhardt C, Sillah J, Fielding K, Donkor S, Manneh K, Warndorff D, et al. Risk factors for tu-
berculosis infection in children with contact with infectious tuberculosis cases in The Gambia, West Africa. Pediatrics 2003; 111:e608.
28. Grüber C, Kulig M, Bergmann R, Guggenmoos-Holzmann I, Wahn U, the MAS-90 Study Group. Delayed hypersensitivity to tuberculin, total immunoglobulin E, speciÞ c sensitization, and atopic manifestation in longitudinally followed early Bacille Calmette-Guérin-vaccinated and nonvac-cinated children. Pediatrics 2001; 107:e36.


C H A P T E R 6
Inverse association between Mycobacterium tuberculosis infection and atopic rhinitis in children
Charles C. ObiharaNulda BeyersRobert P. GiePaul C. PotterBen J. MaraisCarl J. LombardDonald A. EnarsonJan L.L. Kimpen
Allergy2005; 60:1121-1125
78
Infection with M. tuberculosis and atopy in children
Abstract
BackgroundThe association between Mycobacterium tuberculosis (M. tuberculosis) infection and
atopy remains controversial.
AimTo investigate the association between M. tuberculosis infection and atopic rhinitis in
children living in a high TB incidence area.
MethodsIn this cross-sectional study 418 children aged 6 to 14 years from an established epide-
miological research-site in a poor urban community were invited to participate. They were assessed for allergic rhinitis (ISAAC questionnaire) and skin responses to tuberculin and eight environmental allergens. The presence of a BCG scar was documented, intestinal parasites and total and Ascaris lumbricoides-speciÞ c IgE levels were measured.
Atopic rhinitis was deÞ ned, using the new World Allergy Organization (WAO) deÞ -nition, as reported allergic rhinitis and a positive skin prick test (SPT ≥ 3 mm) to any allergen.
ResultsAmong the 337 children enrolled 10.4% had allergic rhinitis, 17.5% a positive SPT and
53% a positive tuberculin skin test (TST ≥ 10 mm). Children with a positive TST were signiÞ cantly less likely to have recent atopic rhinitis
(adjusted odds ratio [ORadj] 0.06; 95% conÞ dence interval (CI) 0.007-0.5) than those with a negative TST. SPTs were signiÞ cantly more common in children with negative TST who had recent allergic rhinitis (ORadj 34.0; 95% CI 7.6-152.6), but not in children with positive TST and recent allergic rhinitis (ORadj 0.6; 95% CI 0.07-5.2).
ConclusionsM. tuberculosis infection seems to reduce the prevalence of atopic rhinitis, and inß u-
ences SPT reactivity in children with allergic rhinitis from a high TB incidence area.

6 Inverse association between Mycobacterium tuberculosis infection and atopic rhinitis
79
Introduction
Recent evidence suggests that chronic infections, such as Mycobacterium tuberculosis (M. tuberculosis) may modulate the expression of atopic disease.1-3 M. tuberculosis infection is a potent inducer of T helper 1 (Th1) responses which inhibit T helper 2 (Th2) responses.1,2 Epidemiological studies have yielded conß icting results for an inverse association between M. tuberculosis infection and atopic disease in children.2,4,5 This may partly be explained by the lack of a universal deÞ nition of atopy. According to the recent deÞ nitions of the World Allergy Organization (WAO), the term atopy refers to clinical allergic disease in combina-tion with a positive allergy skin prick test (SPT) or elevated serum IgE antibody level.5
We hypothesized that M. tuberculosis infection is inversely associated with atopic rhini-tis and the aim was to evaluate the association between tuberculin skin test (TST) response and atopic rhinitis.
Materials and methods
This cross-sectional study was conducted between June and October 2003, in an epi-demiological research-site (population 38565 in 1996) in Cape Town, South Africa. The incidence of M. tuberculosis infection is high (320 bacteriologically conÞ rmed cases per 100 000 per year) and neonatal BCG vaccination coverage is universal (>90%).6
All children 6-14 years living in a 15% randomly selected sample of households in the southern part of the research-site were enumerated and invited to participate. Exclusion cri-teria included known immune compromising disease, active tuberculosis, pregnancy and refusal to participate. Parents or legal guardians gave written signed informed consent.
Supervised by a trained Þ eld-worker, each parent or legal guardian completed a writ-ten validated ISAAC (Phase I) questionnaire on previous (ever) and recent (in the last 12 months) symptoms of allergic rhinitis. Information on neonatal BCG vaccination history, number of siblings, household income and parental atopic history were collected.
TST was performed by injecting 2 TU (tuberculin units) of PPD RT 23 (Statens Serum Institut, Copenhagen, Denmark) and the transverse diameter of the induration measured after 2 to 3 days. A positive TST was deÞ ned as induration ≥ 10 mm.
SPTs were performed after collection of questionnaire data. SPTs to eight common al-lergens (ALK-Abelló, Denmark): Dermatophagoides pteronyssinus, Bermuda grass, Rye grass, cat dander, dog dander, Alternaria alternata, Cladosporium herbarium and aspergil-lus together with positive (histamine chloride 10mg/ml) and negative (glycerol) controls were performed. A positive SPT reaction was deÞ ned as a mean wheal diameter of ≥ 3 mm in excess of the negative control.
Total serum and Ascaris lumbricoides-speciÞ c IgE levels were measured with the Phar-macia CAP system (Pharmacia, Uppsala, Sweden). As there are no reference values for non-Caucasian children, total serum IgE level higher than the median value of the study children (138 IU/ml) and A. lumbricoides-speciÞ c IgE level ≥ 0.35 IU/ml was considered elevated. Two stool samples of each child were analyzed for intestinal parasite eggs and in-
80
Infection with M. tuberculosis and atopy in children
fection was deÞ ned as the presence of any parasite egg. Weight and height were measured and BCG scar documented.
Defi nition of allergy and atopyAllergic rhinitis was deÞ ned as questionnaire-reported symptom only and atopic rhi-
nitis as questionnaire reported allergic rhinitis with at least a positive SPT (new WAO deÞ nition).5
Statistical analysisBivariate data analyses were done with chi-squared test (SPSS 11.0). Regression analy-
ses were done by generalized estimation equation (GEE) logistic regression (STATA 8.0), using atopic rhinitis as a dependent variable and TST as an independent variable. The as-sociation was adjusted for possible confounding variables: demographic (age and sex), socioeconomic factors (number of siblings and household income), genetic predisposition (parental allergy) and intestinal parasite infection. Adjustment was made for clustering within the household. Continuous variables were categorized and total IgE levels log-trans-formed for the analysis.
The study was approved by the Ethics Review Board of the University of Stellenbosch.
Results
Of 418 enumerated children 6-14 years, 337 (81%) were enrolled in the study, 39 (9%) had moved away from the area, 14 refused consent and 28 were excluded (23 due to in-complete data, 3 due to pregnancy and 2 exceeded the age limit). The median age of the included children was 11 (range 6-14) years and 177 (53%) were female. The excluded children did not differ in age or gender from those who were included. The total number of children with a positive TST was 179 (53%) (Table 1).
Allergic rhinitis was reported in 35 (10.4%) children. A positive SPT was recorded in 59 (17.5%) children and the most common allergen was Dermatophagoides pteronyssinus (12.5%). Children with positive SPT did not differ signiÞ cantly in age, sex, number of sib-lings, household income, positive TST, intestinal parasite infection or elevated A. lumbri-coides-speciÞ c IgE from those with negative SPT (Table 1). Neither did they differ in the rate of BCG vaccination or scar, the median weight or height, nor parental allergic disease. Children with a positive SPT had a higher median serum IgE level (p ≤ 0.001) than those with a negative SPT.
Positive SPTs were more common in children with questionnaire reported allergic rhi-nitis (ever or recent) than those without (Table 1). SPTs were signiÞ cantly more common in children with negative TST who had recent allergic rhinitis (adjusted odds ratio [ORadj] 34.0; 95% conÞ dence interval (CI) 7.6-152.6), but not in children with positive TST and recent allergic rhinitis (ORadj 0.6; 95% CI 0.07-5.2) (Figure 1). Similarly, allergic rhinitis was associated with elevated total serum IgE in children with negative TST, but not in chil-dren with positive TST.

6 Inverse association between Mycobacterium tuberculosis infection and atopic rhinitis
81
Table 1. Distribution of demographic and socioeconomic parameters, prevalence of allergic rhinitis (ever or recent) and test results in allergy skin test positive children and in all children.
Baseline parameter All children (n = 337)
Positive SPT(n = 59)
Percentage (%)
Unadjusted OR (95% CI)
Adjusted OR**(95% CI)
Age (years): 6�9 157 23 14.6 1 1 10�14 180 36 20.0 1.50 (0.80-2.60) 1.26 (0.66-2.40)
Sex: Female 177 34 19.2 1 1 Male 159 25 15.7 0.80 (0.5-1.40) 0.70 (0.37-1.30)
Number of siblings: < 3 217 34 15.7 1 1 ≥ 3 120 25 20.8 1.42 (0.80-2.5) 1.80 (0.95-3.40)
Average HH income (SAR)*: < 800 273 47 17.2 1 1 ≥ 800 40 8 20.0 1.20 (0.5-2.8) 1.37 (0.54-3.44)
Reported allergic rhinitis: ever: no 302 46 15.2 1 1
yes 35 13 37.1 3.29 (1.55-7.0) 3.70 (1.64-8.40) recent (≤ 12 months): no 308 47 15.3 1 1
yes 29 12 41.4 3.92 (1.76-8.7) 5.0 (2.05-12.10)
Tuberculosis infection: negative TST (< 10 mm) 158 29 18.4 1 1 positive TST (≥ 10 mm) 179 30 16.8 0.90 (0.50- 1.60) 0.99 (0.53-1.86)
Presence of any parasite egg in stool: no 188 36 19.1 1 1
yes 149 23 15.4 0.80 (0.43- 1.37) 0.70 (0.37-1.40)
Elevated Ascaris IgE (IU/ml) < 0.35 177 24 13.6 1 1 ≥ 0.35 158 34 21.5 1.75 (0.99-3.10) 1.79 (0.95-3.38)
SPT: allegy skin prick test; TST: tuberculin skin test; IgE: immunoglobulin E; OR: odds ratio; CI: conÞ -dence interval.* South African Rand (1 US $ =6.5 SAR). Cut-off of household income based on ofÞ cial monthly mini-mum salary (800 SAR)** In the logistic regression model, SPT was used as dependent variable and all the other variables in the table as independent variable.
Children with a positive TST were signiÞ cantly less likely to have atopic rhinitis than those with a negative TST (0.6% vs. 7.0%). This effect was stronger in children with re-cent atopic rhinitis (Table 2) than in those with atopic rhinitis ever (ORadj 0.14; 95% CI, 0.03-0.7).

82
Infection with M. tuberculosis and atopy in children
Discussion
This study demonstrates a signiÞ cant inverse association between M. tuberculosis in-fection and atopic rhinitis in children suggesting that M. tuberculosis infection reduces the expression of atopy, as was found in Japanese children.2 Our study also demonstrates sig-niÞ cantly reduced SPT reactivity in allergic children with M. tuberculosis infection, when compared to allergic children without M. tuberculosis infection, suggesting that M. tuber-culosis infection may suppress allergic sensitisation.
Different mechanisms could explain these Þ ndings. Chronic infections such as tuber-culosis may down-regulate atopic response through the induction of T-regulatory cells and production of anti-inß ammatory cytokines.7,8 Animal studies have shown that simultane-ous M. tuberculosis infection and allergen challenge may stimulate a Th1 reaction strong enough to suppress Th2 activity signiÞ cantly.9 If this phenomenon, where both M. tubercu-losis and allergens are simultaneously presented by antigen-presenting cells (APC) to the T-cell, also applies to humans, then it is most likely to occur when M. tuberculosis infection and allergen exposure are both highly prevalent, as in our study population. The mecha-nism of concurrent antigen presentation may partly explain the reduced SPT reactivity in allergic individuals infected with M. tuberculosis.
0
10
20
30
40
50
60
70
80
All children (n=337) TST negative children(n = 158)
TST positive children (n=179)
Pos
itive
SP
T(%
)
Recent allergic rhinitis
No allergic rhinitis
P = 0.001 P < 0.001
P = 0.7
Fig. 1. Allergy skin prick test (SPT) positivity in the presence of reported recent allergic rhinitis for all children; TST negative (< 10 mm) and TST positive ( ≥ 10 mm) children
Recent allergic rhinitis
No allergic rhinitis
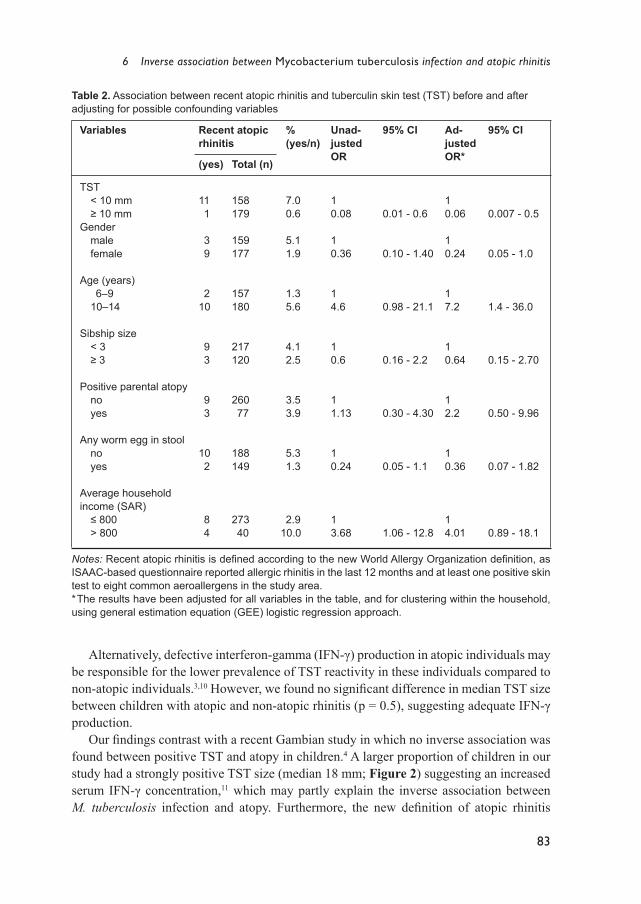
6 Inverse association between Mycobacterium tuberculosis infection and atopic rhinitis
83
Alternatively, defective interferon-gamma (IFN-γ) production in atopic individuals may be responsible for the lower prevalence of TST reactivity in these individuals compared to non-atopic individuals.3,10 However, we found no signiÞ cant difference in median TST size between children with atopic and non-atopic rhinitis (p = 0.5), suggesting adequate IFN-γ production.
Our Þ ndings contrast with a recent Gambian study in which no inverse association was found between positive TST and atopy in children.4 A larger proportion of children in our study had a strongly positive TST size (median 18 mm; Figure 2) suggesting an increased serum IFN-γ concentration,11 which may partly explain the inverse association between M. tuberculosis infection and atopy. Furthermore, the new deÞ nition of atopic rhinitis
Table 2. Association between recent atopic rhinitis and tuberculin skin test (TST) before and after adjusting for possible confounding variables
Variables Recent atopic rhinitis
% (yes/n)
Unad-justed OR
95% CI Ad-justed OR*
95% CI
(yes) Total (n)
TST < 10 mm 11 158 7.0 1 1 ≥ 10 mm 1 179 0.6 0.08 0.01 - 0.6 0.06 0.007 - 0.5Gender male 3 159 5.1 1 1 female 9 177 1.9 0.36 0.10 - 1.40 0.24 0.05 - 1.0
Age (years) 6�9 2 157 1.3 1 1 10�14 10 180 5.6 4.6 0.98 - 21.1 7.2 1.4 - 36.0
Sibship size < 3 9 217 4.1 1 1 ≥ 3 3 120 2.5 0.6 0.16 - 2.2 0.64 0.15 - 2.70
Positive parental atopy no 9 260 3.5 1 1 yes 3 77 3.9 1.13 0.30 - 4.30 2.2 0.50 - 9.96
Any worm egg in stool no 10 188 5.3 1 1 yes 2 149 1.3 0.24 0.05 - 1.1 0.36 0.07 - 1.82
Average household income (SAR) ≤ 800 8 273 2.9 1 1 > 800 4 40 10.0 3.68 1.06 - 12.8 4.01 0.89 - 18.1
Notes: Recent atopic rhinitis is deÞ ned according to the new World Allergy Organization deÞ nition, as ISAAC-based questionnaire reported allergic rhinitis in the last 12 months and at least one positive skin test to eight common aeroallergens in the study area. * The results have been adjusted for all variables in the table, and for clustering within the household, using general estimation equation (GEE) logistic regression approach.

84
Infection with M. tuberculosis and atopy in children
was used in our study,5 while in the Gambian study atopy was deÞ ned as a positive SPT only.4
Important strengths of our study are the use of an objective measure of atopy (SPT) to differentiate children with atopic and non-atopic rhinitis and the correction for intestinal parasite infection. The fact that both biomarkers (SPT and serum IgE) showed similar trends of association increases biological plausibility of the Þ ndings.
Main limitations are the cross-sectional design and questionnaire-based diagnosis of al-lergic rhinitis. Limitations inherent to the cross-sectional design are recall bias and lack of temporal association between M. tuberculosis infection, allergen exposure and the devel-opment of atopic rhinitis. Questionnaire-based limitations were reduced by using the vali-dated ISAAC questionnaire. The reliability of questionnaire generated data is supported by its signiÞ cant association with objectively measured SPT and serum IgE and by the fact that the prevalence of reported allergic rhinitis was comparable to that of the previous ISAAC-study in Cape Town.12 Although selection-bias due to the inclusion of only children from the southern part of the study area remains a possibility, we think it is not signiÞ cant, because we chose a random sample and although we focused on a speciÞ c geographical area, the values of most baseline factors were similar to the whole community.
Some of the conß icting reports in the literature on the association between M. tubercu-losis infection and atopy may be due to the use of different deÞ nitions of atopy. Using the recent deÞ nitions,5 our data showed a strong inverse association between M. tuberculosis infection and atopic rhinitis, and lower SPT reactivity in allergic children with M. tubercu-losis infection. This suggests possible immune modulation by M. tuberculosis. Prospective studies are needed to validate these Þ ndings.
0
1
2
3
4
5
6
7
8
9
10
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30
TST induration (mm)
Pe
rcen
tage
(%)
45.1%
Median TST size (larger than 0 mm) = 18.0 mm
Fig. 2. Frequency distribution of TST responses in 337 children (after 2 TU of M. tuberculosis PPD RT 23).

6 Inverse association between Mycobacterium tuberculosis infection and atopic rhinitis
85
References
1. Hopkin JM. Atopy, asthma, and the mycobacteria. Thorax 2000; 55:443-5. 2. Shirakawa T, Enomoto T, Shimazu S, Hopkin J. The inverse association between tuberculin re-
sponses and atopic disorder. Science 1997; 275:77-9. 3. Strannegård I, Larsson L, Wennergren G, Strannegård Ö. Prevalence of allergy in children
in relation to prior BCG vaccination and infection with atypical mycobacteria. Allergy 1998; 53:249-54.
4. Ota M, van der Sande M, Walraven G, Jeffries D, Nyan O, Marchant A, et al. Absence of asso-ciation between delayed type hypersensitivity to tuberculin and atopy in children in The Gambia. Clin Exp Allergy 2003; 33:731-6.
5. Johansson SGO, Bieber T, Dahl R, Friedmann P, Lanier BQ, Lockey RF, et al. Revised nomen-clature for allergy for global use: report of the Nomenclature Review Committee of the World Allergy Organization, October 2003. J Allergy Clin Immunol 2004; 113:832-6.
6. Verver S, Warren RM, Munch Z, Richardson M, van der Spuy GD, Borgdorff Mw, et al. Pro-portion of tuberculosis transmission that takes place in a high-incidence area. Lancet 2004; 363:212-4.
7. Yazdanbakhsh M, Van den Biggelaar A, Maizels RM. Th2 responses without atopy: immuno-regulation in chronic helminth infections and reduced allergic disease. Trends Immunol 2001; 22:372-7.
8. Zuany-Amorin C, Sawicka E, Manlius C, Le Moine A, Brunet L, Kemeny D, et al. Suppression of airway eosinophilia by killed Mycobacterium vaccae-induced allergen-speciÞ c regulatory T-cells. Nature Medicine 2002; 8:625-9.
9. Sano K, Haneda K, Tamura G, Shirato K. Ovalbumin (OVA) and Mycobacterium tuberculosis bacilli cooperatively polarize anti-OVA T-helper (Th) cells towards a Th1-dominant phenotype and ameliorate murine tracheal eosinophilia. Am J Respir Cell Mol Biol 1999; 20:1260-7.
10. Reinhold U, Wehrmann W, Kukel S, Kreysel H. Evidence that defective interferon-gamma pro-duction in atopic dermatitis patients is due to intrinsic abnormalities. Clin Exp Immunol 1990; 79:374-9.
11. Black GF, Fine PEM, Warndorff DK, Floyd S, Weir RE, Blackwell JM, et al. Relationship be-tween IFN-γ and skin test responsiveness to Mycobacterium tuberculosis PPD in healthy, non-BCG-vaccinated young adults in Northern Malawi. Int J Tuberc Lung Dis 2001; 7:664-72.
12. The International Study of Asthma and Allergies in Childhood (ISAAC) Steering Committee. Worldwide variation in prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and atop-ic eczema. Lancet 1998; 351:1225-32.


C H A P T E R 7
Respiratory atopic disease, Ascaris-IgE and tuberculin test in urban South African children
Charles C. Obihara,Nulda BeyersRobert P. GieMaarten O. HoekstraJohn E. FinchamBen J. MaraisCarl J. LombardLeigh A. DiniJan L.L. Kimpen
Clin Exp Allergy, 2006; in press

88
Infection with M. tuberculosis and atopy in children
Abstract
Background Epidemiological relation of intestinal helminth infection and atopic disease, both as-
sociated with a Th2 immune response, is controversial, since it has been reported that hel-minth infection may either suppress or predispose to atopic disease. This relation has not been tested in an area with high burden of M. tuberculosis (M. tuberculosis) infection, a known Th1 stimulating infection.
Objective To study the association of intestinal helminth infection and atopic disease in a commu-
nity where helminth infection is endemic and M. tuberculosis infection high.
MethodsThree-hundred and Þ fty-nine randomly selected children aged 6-14 years from a poor
urban suburb were tested with allergy questionnaire, skin prick test (SPT) to common aer-oallergens, Ascaris speciÞ c IgE (Ascaris-sIgE), fecal examination for pathogenic intestinal helminths and tuberculin skin testing (TST). Histamine bronchoprovocation was tested in the group of children aged 10 years and older. Results were corrected for demographic variables, socioeconomic status, parental allergy, environmental tobacco smoke (ETS) ex-posure in the household, recent anthelminthic treatment and for clustering in the sampling unit.
Results Ascaris-sIgE was elevated in 48% of children, Ascaris eggs were found in 15% and
TST was positive in 53%. Children with elevated Ascaris-sIgE had signiÞ cantly increased risk of positive SPT to aeroallergens, particularly house dust mite, atopic asthma (ever and recent), atopic rhinitis (ever and recent), and increased atopy-related bronchial hyperre-sponsiveness. In children with negative TST (< 10 mm), elevated Ascaris-sIgE was associ-ated with signiÞ cantly increased risk of atopic symptoms (ORadjusted 6.5; 1.9-22.4), while in those with positive TST (≥ 10 mm) this association disappeared (ORadjusted 0.96; 0.4-2.8).
ConclusionsThese results suggest that immune response to Ascaris (Ascaris-sIgE) may be a risk
factor of atopic disease in populations exposed to mild Ascaris infection and that M. tu-berculosis infection may be protective against this risk, probably by stimulation of anti-inß ammatory networks.
7 Respiratory atopic disease, Ascaris-IgE and tuberculin test in urban South African children
89
Introduction
Although infection with helminths can stimulate polyclonal IgE synthesis, their role in the development of atopic disease remains uncertain.1,2 The epidemiological relation of hel-minth infection and atopic disease, both associated with a T-helper (Th) 2 immune response, is controversial, since it has been reported that helminth infection may either suppress atop-ic disease3-6 or predispose to it.7,8 Anthelminthic treatment may inß uence atopic conditions, or modulate the severity of symptoms or sensitization.9-11 It is generally assumed that the prevalence of allergies is low in populations heavily infested with helminth.12-15
The effect of intestinal helminth infection on atopic symptoms seems to depend on the duration and intensity of infection.12,13 With chronic and intense infection, atopic symptoms may be suppressed, while mild and intermittent infection may result in enhanced reaction to environmental allergens and atopic response.12,13
Previous epidemiological surveys often used different deÞ nitions of atopy, which made it difÞ cult to compare results. Recently the World Allergy Organization (WAO) published a new deÞ nition of atopic disease as clinical allergic symptoms in combination with a positive allergy skin prick test (SPT) and/or an elevated serum IgE antibody level,16 which makes it possible to deÞ ne atopic diseases more uniformly.
Although Mycobacterium tuberculosis (M. tuberculosis) infection is high in most hel-minth-infested populations in the developing world, the possible inß uence of M. tuberculo-sis, a strong stimulator of Th1 immunity, on the effect of helminth infection on the develop-ment of atopic disease has not been investigated.
In a resource-poor urban suburb of South Africa, where helminth infection is endemic and tuberculosis (TB) incidence high,17,18 we investigated the associations of Ascaris lum-bricoides infection (speciÞ c-IgE or eggs), and atopic sensitization to common aeroaller-gens or atopic diseases in the pediatric population, using the new WAO deÞ nitions. In addition, we tested the inß uence of positive tuberculin skin test (TST) on the associations investigated.
Materials and methods
This cross-sectional study was conducted between June and October 2003, in an es-tablished epidemiological research-site in Cape Town, South Africa, with a population of 36.334 in 2001 (Statistics South Africa: Western Cape, Census 2001) and predominantly of mixed ancestry. Although most of the families live in brick houses and have access to clean water and electricity, the general socioeconomic conditions are poor. The prevalence of childhood asthma is 10.8 -13.3% and of allergic rhinitis 16 %.19,20 The vaccination policy in South Africa requires all children to receive a single dose of M. bovis BCG-vaccine during the Þ rst week of life. Based on the WHO criteria, neonatal BCG vaccination in the study area is universal (≥ 90%).
All children aged 6-14 years living in a 15% randomly selected sample of household-addresses were enumerated and invited to participate in the study. Exclusion criteria in-

90
Infection with M. tuberculosis and atopy in children
cluded known immune-compromising disease (such as HIV), active tuberculosis disease, pregnancy or parental refusal. Parents or legal guardians gave written, signed, informed consent.
Under the supervision of a trained Þ eld-worker, each parent completed a written vali-dated International Study of Asthma and Allergies in Children (ISAAC) Phase I question-naire on previous (ever) and recent (<12 months) symptoms of asthma or allergic rhinitis. In addition, the questionnaire included questions on socioeconomic variables, parental al-lergic history, BCG immunization, anthelminthic treatment, environmental tobacco smoke (ETS) exposure in the household and HIV-status.
The proportion of HIV-1-infected persons in the area is among the lowest in South Af-rica.21 Children with questionnaire-reported positive HIV-status were excluded, because of the possible effect on T cell immunity. The presence of BCG scar was noted in each child.
SPT to eight common aeroallergens (ALK-Abelló, Denmark) based on local allergen exposure (house dust mite (HDM), Bermuda grass, Rye grass, cat dander, dog dander, Al-ternaria alternata, Cladosporium herbarium and Aspergillus) together with a positive (his-tamine chloride 10mg/ml) and negative (glycerol) control were performed after completion of the questionnaire. A positive SPT reaction was deÞ ned as a mean wheal diameter of ≥ 3mm in excess of the negative control.
Total serum IgE and Ascaris-sIgE levels were measured with the CAP RAST (Pharma-cia®, Uppsala, Sweden). Due to the lack of reference values for non-Caucasian children for this analysis total serum IgE level higher than the median value of the children in the study and Ascaris-sIgE level ≥ 0.35 IU/ml was considered elevated. Two stool samples, taken at least 24 hours apart, were collected from each child. A portion (0.5-1 gram) was weighed, added to formalin, concentrated by formalin-ether sedimentation and examined by light microscopy. The presence of helminth eggs was deÞ ned as helminth infection. Helminth infection intensity (eggs per gram (epg) stool) was classiÞ ed according to the proposed WHO classiÞ cation (WHO/CTD/SIP/98.1).
The histamine bronchoprovocation test was used to assess bronchial hyper-respon-siveness (BHR). The spirometry (with a calibrated Jaeger Masterscope, software version: 4.52i) was repeated until the best of three reproducible baseline measurements of forced expiratory volume at 1 second (FEV1) was obtained, this was taken as reference. During the pilot spirometry testing, a majority of the children less than 10 years of age failed to achieve reproducible readings within the allocated time-frame of the test. This was mainly due to lack of motivation or difÞ culty with understanding the instructions. Because of this difÞ culty the study coordinators decided to limit the histamine bronchoprovocation test to all children 10 years of age and older. The test was conducted according to the modiÞ ed Cockcroft protocol, as described by Steinbrugger.22 It consisted of a 2-minute inhalation of nebulized histamine (Pari LC PLUS nebulizer) through a mouthpiece of a Pari-Boy (37:00; 50 Hz; 1.3 bar −2700 l/min; Pari, Starnberg, Germany). During inhalation, the nose was closed by a clip. The histamine concentration (0.03 to 7.8 mg/ml) was doubled in a standardized way and the FEV1 measured after inhalation of each concentration. The test was continued until a decrease in FEV1 from baseline of 20% or the maximum dose was reached. The response to the histamine challenge was expressed as PC20; the concentration
7 Respiratory atopic disease, Ascaris-IgE and tuberculin test in urban South African children
91
that caused a fall in FEV1 of 20% from baseline calculated by linear interpolation of log-lin-ear dose-response curve. A subject was regarded as having an increased BHR if PC20 was ≤ 8.0 mg/ml. Children with a FEV1 fall of ≥ 10 % after histamine challenge were treated with two inhalations of 200μg salbutamol and FEV1 measurement was repeated 5 minutes later.
The research-site has a very high TB incidence.18 The TB notiÞ cation rate was 341 per 100.000 for new smear-positive TB and 612 per 100.000 for bacteriological conÞ rmed TB in 2002. Tuberculin reactivity becomes apparent in 3-6 weeks after initial M. tuberculosis infection and may remain positive for the lifetime of the individual.23 A positive TST reac-tion is an accepted hallmark of primary infection with M. tuberculosis.23 TST response was documented in the children. TST was performed by injecting 2 TU (tuberculin units) of PPD RT 23 (Statens Serum Institut, Copenhagen, Denmark) and measuring the transverse induration diameter after 2 to 3 days. In accordance with the American Thoracic Society guidelines, a positive TST was deÞ ned as an induration of 10 mm or more.24
Defi nition of atopic disease outcome variablesAllergic symptoms represent ISAAC-questionnaire-reported symptoms. A positive SPT
was used to differentiate children with atopic symptoms from those with non-atopic symp-toms. Atopic asthma and rhinitis were deÞ ned according to the new WAO deÞ nition, as questionnaire reported asthma or allergic rhinitis together with a positive SPT.16 Atopy-re-lated BHR was deÞ ned as increased BHR with positive SPT (BHR with SPT).
Statistical analysisBivariate data analyses were performed using the chi-squared test (SPSS 11.0). Re-
gression analyses were performed with the generalized estimated equation (GEE) logistic regression (LR) (STATA 8.0), using reported allergic symptoms, SPT reactivity, atopic diseases or BHR with SPT as the dependent variable and Ascaris-sIgE as the independent variable. The association was adjusted for possible confounding variables: demographic (age and gender), genetic- (parental allergic history), socioeconomic- (household income), environmental (ETS exposure in the household) factors and anthelminthic treatment. In addition, the association was stratiÞ ed for the presence or absence of a positive TST, in a LR model. Results were corrected for clustering (> 1 child per household) in the sampling unit. The sampling unit in the study is the household. There was a total of 201 households in the study, with an average of 1·5 children per household. For the analysis, each child was coded and linked to the speciÞ c household. The study protocol was approved by the Ethics Review Board of the University of Stellenbosch.
Results
Of 418 enumerated children aged 6-14 years, 359 (86%) were enrolled in the study, 39 had moved away from the area, 14 refused consent, 3 were pregnant and 3 exceeded the age limit. The median age was 11.0 (range, 6-14) years. The children excluded from the study did not differ in age or gender from those included.
92
Infection with M. tuberculosis and atopy in children
Table 1 describes the most important characteristics of the 359 children analyzed, to-gether with prevalences of reported allergic symptoms, atopic sensitization, atopic dis-eases, increased BHR, helminth infection and anthelminthic treatment, serum IgE antibody levels, parental allergic history, positive TST reaction, environmental tobacco smoke (ETS) exposure in the household and BCG immunization. All children in the study reported to have received neonatal BCG immunisation. The prevalence of BCG scar did not differ be-tween children with positive TST and those with negative TST.
Of children with helminth infection, 14.8% (53) were infected with Ascaris and 40% (144) with Trichuris trichiura (Trichuris). Other helminth eggs found were Enterobius vermicularis in 4 children and Hymenolepsis nana in 1. The median infection intensity and IgE values were log-transformed because the values were not normally distributed. The median (range) infection intensity among the children infected with Ascaris was 182 (0-5888) epg and Trichuris 58 (0-10.000) epg. The median (range) total IgE level was 143.00 IU/ml (2.33-18080.00) and Ascaris-sIgE 0.35 IU/ml (<0.35-63.10). Fifty percent (178) of children had an elevated total IgE level and 48% (171) an elevated Ascaris-sIgE level. Of children who underwent histamine bronchoprovocation 55 % (133) had increased BHR and 13.3% (32) had both increased BHR and positive SPT. TST was positive in 53% (179) of children. The TST distribution of the children was unimodal and the median TST size in those with any TST induration was 18 mm (range 1-30.5). The prevalence of parental allergic history or recent (<12 months) anthelminthic treatment did not dif-fer between children with elevated Ascaris-sIgE or Ascaris eggs in the stool and those without.
Children with Ascaris eggs in the stool were more likely to have an elevated Ascaris-sIgE level (adjusted odds ratio [ORadj] 2.4; 95% CI 1.3-4.5) and had a higher mean log Ascaris-sIgE (p< 0.005) than those without. In contrast, children with Trichuris infection were not more likely to have an elevated Ascaris-sIgE level (ORadj 1.50; 95% CI 0.92-2.80) or a higher mean log Ascaris-sIgE (p = 0.10).
Ascaris-sIgE and atopic diseaseChildren with elevated Ascaris-sIgE had a higher frequency of allergic symptoms, atop-
ic diseases, positive SPT to HDM, BHR and BHR with SPT than those without elevated Ascaris-sIgE. For reported asthma ever (p < 0.05), atopic asthma ever (p < 0.05) and recent (p < 0.005)), atopic rhinitis ever (p < 0.05) and recent (p < 0.05), positive SPT to HDM (p < 0.05) and BHR (p < 0.05) the differences were signiÞ cant.
Figure 1 shows a signiÞ cant linear association of log Ascaris-sIgE and the frequency of atopic diseases, positive SPT to HDM or BHR with SPT in the children. Table 2 shows that children with elevated Ascaris-sIgE had signiÞ cantly increased risk of atopic sensitiza-tion, particularly HDM and atopic diseases than those without. They also showed a trend to have higher risk of reported allergic symptoms, BHR and BHR with SPT. The increase in risk of atopic disease or positive SPT for HDM observed in children with elevated Ascaris-sIgE remained signiÞ cant after adjusting for possible confounding variables (Table 3). In a linear regression analysis, log Ascaris-sIgE was signiÞ cantly inversely related to log PC20 (Regression coefÞ cient [ß] = �0.206, SE 0.06, p = 0.02).

7 Respiratory atopic disease, Ascaris-IgE and tuberculin test in urban South African children
93
Table 1. Characteristics of the study population (total = 359)
Number/ Total (%)Demographics:Sex Male 188/359 (52.4)
Female 171/359 (47.6)Age (years) 6-10 167/359 (46.5)
11-14 192/359 (53.5)Respiratory allergic symptoms: Asthma ever yes 49/359 (13.6) recent (≤ 12 months) yes 27/359 (7.5)
Allergic rhinitis ever yes 41/359 (11.4) recent yes 34/359 (9.5)Atopic sensitization: Skin prick test (SPT) reaction ≥ 3 mm house dust mite 48/359 (13,4)
rye grass 17/359 (4.7)Alternaria 15/359 (4.2)Bermuda grass 12/359 (3.3)cat 9/359 (2.5)Aspergillus 4/359 (1.1)dog 4/359 (1.1)Cladosporium 3/359 (0.8)any allergen 66/359 (18.4)
Respiratory atopic diseases (*): Atopic asthma ever yes 16/359 (4.5) recent yes 11/359 (3.1) Atopic rhinitis ever yes 15/359 (4.2) recent yes 14/359 (3.9)Histamine bronchoprovocation (�): Increased BHR yes 133/242 (54.9) Increased BHR with positive SPT yes 32/242 (13.3)Helminth infection: Helminth egg in stool sample Ascaris lumbricoides 53/359 (14.8)
Trichuris trichiura 144/359 (40.1) Anthelminthic treatment ≤ 12 months yes 75/359 (20.9)Serum IgE antibody levels (IU/ml): Ascaris speciÞ c-IgE (≥ 0.35) 171/ 357 (47.9)
total IgE (≥ median:143.0) 178/357 (49.9)Parental allergic history yes 83/359 (23.1)Environmental exposures: Positive tuberculin skin test (TST) ≥10 mm 179/337 (53.1) Environmental tobacco smoke (ETS) exposure in the household yes 217/359 (60.4) BCG immunization yes 359/359 (100)
(*) DeÞ ned as combination of reported allergic symptom and a positive SPT, according to the new World Allergy Organization nomenclature.(�) Histamine challenge was performed only in children ≥ 10 years of age (explanation in the methods section).

94
Infection with M. tuberculosis and atopy in children
Children with Ascaris eggs in the stool did not have an increased risk of positive SPT (OR 0.57; 95% CI 0.23-1.40), atopic asthma (OR 0.85; 95% CI 0.81-0.86), atopic rhinitis (OR1.04; 95% CI 0.22-4.82), or atopy-related BHR (OR 0.74; 95% CI 0.21-2.60) than those without. This did not change after adjusting for the possible confounding variables.
TST, Ascaris-sIgE and atopic disease Adjusted stratiÞ ed analysis in a LR model, according to TST reactivity showed that in
children with negative TST elevated Ascaris-sIgE was associated with increased risk of atopic symptoms (ORadj 6.5; 95 % CI 1.9-22.4), while in those with a positive TST elevated Ascaris-sIgE was not associated with increased risk (ORadj 0.96; 95% CI 0.4-2.8). There was a signiÞ cant interaction-factor between a positive TST and an elevated Ascaris-sIgE (p = 0.02) in the LR model.
Discussion
This study in children from a resource-poor urban suburb of South Africa shows a sig-niÞ cant association of elevated Ascaris-sIgE level and increased risk of atopic asthma, atopic rhinitis or hypersensitivity to common aeroallergens. It also shows that a positive TST, a hallmark of M. tuberculosis infection, may inß uence the association of Ascaris-sIgE and atopic disease. In children with negative TST elevated Ascaris-sIgE was associ-ated with increased risk of atopy, while in those with positive TST no increased risk was observed.
Fig. 1. Frequency of atopic diseases, positive skin prick test (SPT) to HDM and BHR with positive SPT showing direct linear increase with log Ascaris speciiÞ c IgE (Ascaris-sIgE) level (p value for linear relation)
0
5
10
15
20
25
30(%)
P=0.02P=0.05
Atopic disease
P=0.02
P=0.007
P=0.04
P=0.003
Atopic asthma ever Recent atopic asthma Atopic rhinitis ever Recent atopic rhinitis Positive SPT for HDM BHR+SPT
□ Log Ascaris-sigE ≤ 0.46 iu/ml (n = 188)■ Log Ascaris-sigE 0.46�0.54 iu/ml (n= 114)■ Log Ascaris-sigE > 0.54 iu/ml (n = 55)
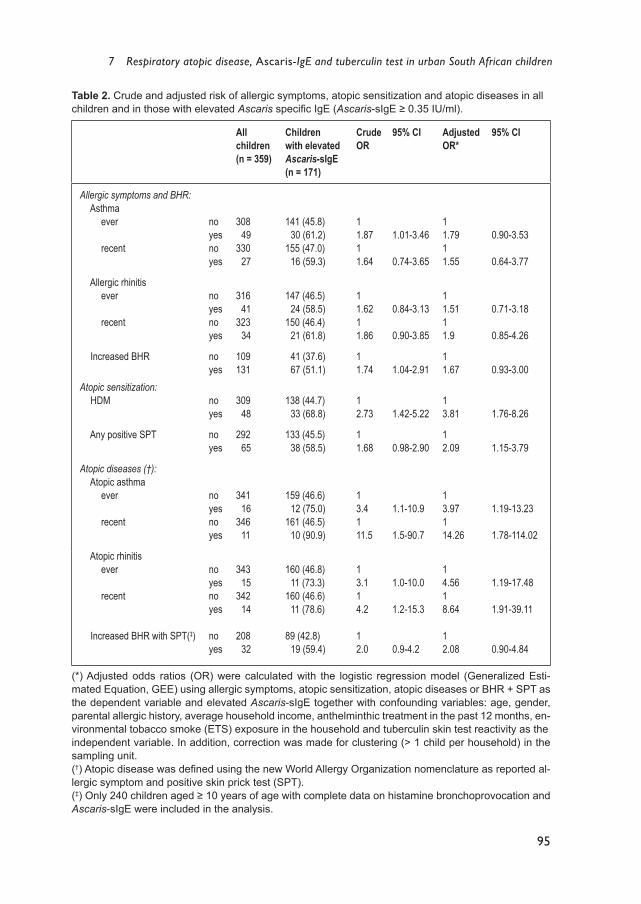
7 Respiratory atopic disease, Ascaris-IgE and tuberculin test in urban South African children
95
Table 2. Crude and adjusted risk of allergic symptoms, atopic sensitization and atopic diseases in all children and in those with elevated Ascaris speciÞ c IgE (Ascaris-sIgE ≥ 0.35 IU/ml).
All children(n = 359)
Children with elevatedAscaris-sIgE(n = 171)
Crude OR
95% CI Adjusted OR*
95% CI
Allergic symptoms and BHR: Asthma ever no 308 141 (45.8) 1 1
yes 49 30 (61.2) 1.87 1.01-3.46 1.79 0.90-3.53 recent no 330 155 (47.0) 1 1
yes 27 16 (59.3) 1.64 0.74-3.65 1.55 0.64-3.77
Allergic rhinitis ever no 316 147 (46.5) 1 1
yes 41 24 (58.5) 1.62 0.84-3.13 1.51 0.71-3.18 recent no 323 150 (46.4) 1 1
yes 34 21 (61.8) 1.86 0.90-3.85 1.9 0.85-4.26
Increased BHR no 109 41 (37.6) 1 1yes 131 67 (51.1) 1.74 1.04-2.91 1.67 0.93-3.00
Atopic sensitization: HDM no 309 138 (44.7) 1 1
yes 48 33 (68.8) 2.73 1.42-5.22 3.81 1.76-8.26
Any positive SPT no 292 133 (45.5) 1 1yes 65 38 (58.5) 1.68 0.98-2.90 2.09 1.15-3.79
Atopic diseases (�): Atopic asthma ever no 341 159 (46.6) 1 1
yes 16 12 (75.0) 3.4 1.1-10.9 3.97 1.19-13.23 recent no 346 161 (46.5) 1 1
yes 11 10 (90.9) 11.5 1.5-90.7 14.26 1.78-114.02
Atopic rhinitis ever no 343 160 (46.8) 1 1
yes 15 11 (73.3) 3.1 1.0-10.0 4.56 1.19-17.48 recent no 342 160 (46.6) 1 1
yes 14 11 (78.6) 4.2 1.2-15.3 8.64 1.91-39.11
Increased BHR with SPT(�) no 208 89 (42.8) 1 1yes 32 19 (59.4) 2.0 0.9-4.2 2.08 0.90-4.84
(*) Adjusted odds ratios (OR) were calculated with the logistic regression model (Generalized Esti-mated Equation, GEE) using allergic symptoms, atopic sensitization, atopic diseases or BHR + SPT as the dependent variable and elevated Ascaris-sIgE together with confounding variables: age, gender, parental allergic history, average household income, anthelminthic treatment in the past 12 months, en-vironmental tobacco smoke (ETS) exposure in the household and tuberculin skin test reactivity as the independent variable. In addition, correction was made for clustering (> 1 child per household) in the sampling unit.(�) Atopic disease was deÞ ned using the new World Allergy Organization nomenclature as reported al-lergic symptom and positive skin prick test (SPT). (�) Only 240 children aged ≥ 10 years of age with complete data on histamine bronchoprovocation and Ascaris-sIgE were included in the analysis.

96
Infection with M. tuberculosis and atopy in children
These Þ ndings suggest that elevated Ascaris-sIgE may be a risk factor of respiratory atopic disease and is in support of previous studies in South Africa,8,14,25 South America10 and China.7
Although it has been hypothesized that polyclonal IgE produced during helminth infec-tion may block allergic reaction by either suppressing antigen-speciÞ c IgE production or
Table 3. Crude and adjusted risk of atopic disease outcomes, positive skin test to house dust mite (HDM) and Ascaris speciÞ c IgE (Ascaris-sIgE), together with confounding variables used in the logis-tic regression model.
Adjusted OR (95% CI)
Variable (categories)
Atopic asthma ever
Recent atopic asthma
Atopic rhinitis ever
Recent atopic rhinitis
Positive SPT to HDM
Ascaris-sIgE (IU/ml ) < 0.35 ≥ 0.35
Age (yr) 6-10 11-14
Gender Male Female
Household income (SAR) < 800 ≥ 800
Parental allergy No Yes
TST (mm) <10 ≥ 10
Recent helminthic treatment No Yes
Current smokeexposure No Yes
1.03.97 (1.19-13.23)
1.01.83 (0.55-6.13)
1.01.75 (0.59-5.21)
1.02.04 (0.48-8.62)
1.01.75 (0.55-5.56)
1.00.62 (0.21-1.83)
1.00.29 (0.03-2.50)
1.00.92 (0.30-2.88)
1.014.26 (1.78-114.02)
1.03.0 (0.60-14.89)
1.01.17 (0.86-15.06)
1.02.72 (0.52-14.16)
1.01.29 (0.30-5.57)
1.00.43 (0.12-1.58)
1.00.48 (0.05-4.67)
1.00.81 (0.21-3.10)
1.04.56 (1.19-17.48)
1.03.04 (0.71-12.94)
1.03.61 (0.07-1.16)
1.03.99 (0.94-16.88)
1.01.13 (0.26-4.91)
1.00.12 (0.02-0.64)
1.00.71 (0.13-3.96)
1.00.24 (0.07-0.90)
1.08.64 (1.91-39.12)
1.04.94 (0.98-25.04)
1.02.99 (0.70-12.73)
1.06.16 (1.17-32.43)
1.01.56 (0.33-7.40)
1.00.05 (0.01-0.41)
1.00.98 (0.16-5.98)
1.00.17 (0.04-0.79)
1.03.81 (1.76-8.26)
1.02.26 (1.04-4.89)
1.01.85 (0.89-3.85)
1.01.84 (0.65-5.20)
1.01.46 (0.65-3.30)
1.00.89 (0.43-1.82)
1.01.18 (0.48-2.93)
1.00.26 (0.26-1.20)
Adjusted odds ratios (ORadj) were calculated with the Generalized Estimated Equation (GEE) logistic regression (LR) model (STATA 8.0), using atopic asthma, atopic rhinitis and positive SPT to house dust mite (HDM) as the dependent variable and Ascaris-sIgE and the other confounding variables in the ta-ble as independent variable. In addition, correction was made for clustering (> 1 child per household) in the sampling unit. Atopic disease was deÞ ned using the new World Allergy Organization nomenclature as reported allergic symptom and a positive skin prick test (SPT).
7 Respiratory atopic disease, Ascaris-IgE and tuberculin test in urban South African children
97
by saturation of IgE receptors on mast cells,10,26-28 other studies which demonstrated lack of saturation of mast cell capacity in vitro or in vivo argue against this mechanism.29,30 Recent evidence suggests that chronic infections, such as helminth and M. tuberculosis may lead to CD4+ regulatory T cell (Treg) stimulation with subsequent production of high levels of anti-inß ammatory cytokines, which may inhibit allergic inß ammation.13 This effect may depend on the intensity and persistence of infection.13,31 With intense and persistent infec-tion, atopic responses may be suppressed by strong stimulation of Tregs and anti-inß am-matory cytokines.13 In contrast, mild helminth infection (as in our study population) may lead to moderate or no stimulation of anti-inß ammatory networks and this may result in an enhanced reaction to environmental allergens and atopic response.13,31
The mild intensity of Ascaris infection in our study population may be explained by the frequent single-dose anthelminthic therapy with benzimidazoles being used by children in the area.32 This reduces the intensity of parasitic infestation and interrupts the persistence (or chronicity) of infection. The higher prevalence of Trichuris infection, which is less sen-sitive to a single dosage of anthelminthic therapy, supports this assumption.32
A rather surprising Þ nding is that the presence of Ascaris eggs in the stool was not asso-ciated with increased prevalence of atopic disease. This observation may reß ect important differences in the immunological proÞ le between Ascaris eggs in the stool and elevated Ascaris-sIgE, especially in populations where intestinal helminth infection is of mild in-tensity. This is supported by reports that an elevated Ascaris-sIgE level and the presence of Ascaris eggs in the stool may measure different entities.33 An elevated Ascaris-sIgE level reß ects the competency of the host Th-2 immune response to Ascaris antigen. The presence of Ascaris eggs in the stool reß ects active infection, although the impact of this infection on the host immune response may depend on different factors, including the severity and chro-nicity of infection.13,31 The lack of association between Ascaris eggs and atopic disease may partly be related to the low prevalence and mild intensity of Ascaris eggs in the children.
Our Þ ndings differ from those of another research group who reported a lower preva-lence of hypersensitivity to HDM in African children with urinary schistosomiasis.30 The authors considered the anti-inß ammatory cytokine, IL-10 produced during Schistosoma infection to be responsible for the effect. The enhanced production of IL-10 seen with chronic tissue helminth infections such as Þ lariasis and schistosomiasis has not been ob-served in ascariasis.34 This, and the mild intensity of helminth infection, may account for the different observations.
Consistent with previous Þ ndings, we found that a positive TST was inversely associ-ated with the risk of atopic disease.35 This is in support of recent evidence that chronic infections, such as M. tuberculosis may down-regulate the atopic response through the stimulation of anti-inß ammatory networks.13,31 The strong median TST reaction (18 mm) in the children indicates hypersensitivity to natural M. tuberculosis infection which is highly prevalent in the community and not to BCG or environmental mycobacteria which gener-ally stimulate a weaker TST reaction.23,24,35,36 Our present Þ ndings contrast with the results of a study in Gambian children, in which no inverse association was found between posi-tive TST and atopy in children.37 The difference in Þ ndings could be explained by the fact that a larger proportion of children in our study had a strongly positive TST size than in the

98
Infection with M. tuberculosis and atopy in children
Gambian study. This is supported by observations that the size of TST is directly related to serum IFN-γ level, suggesting that increased serum IFN-γ concentration may partly ex-plain the inverse association between M. tuberculosis infection and atopy.38 Furthermore, the new globally accepted WAO deÞ nition of atopic rhinitis was used in our study.16 This contrasts with the Gambian study in which atopy was deÞ ned as a positive SPT only.
Particular strength of this study is the use of objective measures (SPT) to differentiate children with atopic and non-atopic symptoms, based on the new WAO deÞ nitions.16 Most previous studies deÞ ned atopic outcome either as a positive SPT or an elevated serum IgE only.6,11 The inß uence of M. tuberculosis infection was taken into account, and this, to our knowledge, has not been reported previously in this context. The main limitations are the cross-sectional design and questionnaire-based diagnosis of allergic symptoms. Limi-tations inherent to the cross-sectional design are recall-bias and the inability to analyze temporal relationship of Ascaris eggs, Ascaris-sIgE, the development of atopic disease and TST reactivity. Questionnaire-based limitations were reduced by using the validated ISAAC questionnaire and collecting questionnaire data before performing objective tests. The reliability of questionnaire-generated data is supported by the fact that the prevalences of allergic symptoms were comparable to those of the ISAAC study in Cape Town.20 That reliable spirometric tests could not be achieved in younger children does not bias the re-sults, but rather reß ects an important difÞ culty which may be encountered in performing such a standardized test in otherwise healthy voluntary children. Although the factors re-sponsible for the high frequency of increased BHR were not investigated, it may be related to the high prevalence of ETS exposure and other non-atopic environmental airway pollut-ants in the area. ETS is a known risk factor for airway hyper-responsiveness in children.39
In conclusion, this study shows a signiÞ cant association of elevated Ascaris-sIgE and atopic sensitization and symptoms, suggesting that elevated Ascaris-sIgE may be an en-vironmental risk factor of atopic manifestation, particularly in helminth-infected children with mild infection. It also shows the inß uence of natural M. tuberculosis infection on the association, which may be attributed to stimulation of anti-inß ammatory immune networks during M. tuberculosis infection. There is a need for prospective community-based studies to conÞ rm these Þ ndings.

7 Respiratory atopic disease, Ascaris-IgE and tuberculin test in urban South African children
99
References
1. Britton J. Parasites, allergy, and asthma. Am J Respir Crit Care Med 2003; 168:266-7. 2. King C, Low C, Nutman T. IgE production in human helminth infection. J Immunol 1993;
150:1873-80. 3. Cooper PJ, Chico ME, Bland M, GrifÞ n G, Nutman B. Allergic symptoms, atopy, and geohel-
minth infections in a rural area of Ecuador. Am J Respir Crit Care Med 2003; 168:313-7. 4. Nyan OA, Walraven G, Banya W, Milligan P, Van der Sande M, Ceesay SM, Del Prete G, McAd-
am K. Atopy, intestinal helminth infection and total serum IgE in rural and urban adult Gambian communities. Clin Exp Allergy 2001; 31:1672-8.
5. Scrivener S, Yemaneberhan H, Zebenigus M, Tilahun D, Girma S, Ali S, McElroy P, Custovic A, Woodcock A, Pritchard D, et al. Independent effects of intestinal parasite infection and domestic allergen exposure on the risk of wheeze in Ethiopia: a nested case-control study. Lancet 2001; 358:1493-9.
6. Dagoye D, Bekele Z, Woldemichael K, Nida H, Yimam M, Hall A, Venn AJ, Britton JR, Hubbard R, Lewis SA. Wheezing, allergy, and parasite infection in children in urban and rural Ethiopia. Am J Respir Crit Care Med 2003; 167:1369-73.
7. Palmer LJ, Celedón J, Weiss ST, Wang B, Fang Z, Xu X. Ascaris lumbricoides infection is as-sociated with increased risk of childhood asthma and atopy in rural China. Am J Respir Crit Care Med 2002; 165:1489-93.
8. Joubert JR, De Klerk HC, Malan C. Ascaris lumbricoides and allergic asthma: a new perspective. S Afr Med J 1979; 56:599-602.
9. Lynch NR, Palenque M, Hagel I, DiPrisco M. Clinical improvement of asthma after anthelmin-thic treatment in a tropical situation. Am J Respir Crit Care Med 1997; 156:50-4.
10. Lynch NR, Hagel I, Perez M, Di Prisco M, Lopez R, Alvarez N. Effect of anthelmintic treat-ment on the allergic reactivity of children in a tropical slum. J Allergy Clin Immunol 1993; 92:404-11.
11. Van den Biggelaar AHJ, Rodrigues LC, van Ree R, van der Zee JS, Hoeksman-Kruize YCM, Souverijn JHM, Missinou MA, Borrmann S, Kremsner PG, Yazdanbakhsh M. Long-term treat-ment of intestinal helminths increases mite skin-test reactivity in Gabonese schoolchildren. J Infect Dis 2004; 189:892-900.
12. Cooper PJ. Can intestinal helminth infections (geohelminths) affect the development and expres-sion of asthma and allergic disease? Clin Exp Immunol 2002; 128:398-404.
13. Yazdanbakhsh M, Van den Biggelaar, Maizels RM. Th2 responses without atopy: immunoreg-ulation in chronic helminth infections and reduced allergic disease. Trends Immunol 2001; 22:372-7.
14. Joubert JR, van Schalkwyk DJ, Turner KJ. Ascaris lumbricoides and human immunogenic re-sponse: enhanced IgE-mediated reactivity to common inhaled allergens. S Afr Med J 1980; 57:409-12.
15. Lynch NR, Medouze L, di Prisco-Fuenmayor MC, Verde O, Lopez RI, Malave C. Incidence of atopic disease in a tropical environment: partial independence from intestinal helminthiasis. J Al-lergy Clin Immunol 1984; 73:229-33.
16. Johansson SGO, Bieber T, Dahl R, Friedmann P, Lanier BQ, Lockey RF, Motala C, Ortega Mar-tell JA, Platts-Mills TA, Ring J, et al. Revised nomenclature for allergy for global use: report of the Nomenclature Review Committee of the World Allergy Organization, October 2003. J Al-lergy Clin Immunol 2004; 113:832-6.
17. Gunders AE, Cotton M, Nel E, Hendriks M, Ebrecht K, Hahne H, Redecker R, Shaw ML, van der Walt J, Williams A. Prevalence and intensity of intestinal worm infections in crèche attenders in urban and peri-urban settings in greater Cape Town. S Afr J Epidemiol Infect 1993; 8:48-51.

100
Infection with M. tuberculosis and atopy in children
18. Verver S, Warren RM, Munch Z, Richardson M, van der Spuy GD, Borgdorff MW, Behr MA, Beyers N, van Helden PD. Proportion of tuberculosis transmission that takes place in households in a high-incidence area. Lancet 2004; 363:212-4.
19. Ehrlich RI, Du Toit D, Jordaan E, Volmink JA, Weinberg EG, Zwarenstein M. Prevalence and re-liability of asthma symptoms in primary school children in Cape Town. Int J Epidemiology 1995; 24:1138-45.
20. The International Study of Asthma and Allergies in Childhood (ISAAC) Steering Committee. Worldwide variation in prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and at-opic eczema. Lancet 1998; 351:1225-32.
21. National HIV and Syphilis antenatal sero-prevalence survey in South Africa 2002. The South African Department of Health. http://www.doh.gov.za/docs/reports/2002/hiv-syphilis.pdf.
22. Steinbrugger B, Eber E, Modl M, Weinhandl E, Zach S. A comparison of a single-step cold air challenge and routine histamine provocation for the assessment of bronchial hyperresponsive-ness in children and adolescents. Chest 1995; 103:741-5.
23. Shingadia D, Novelli V. Diagnosis and treatment of tuberculosis in children. Lancet Infect Dis 2003; 3:624-32.
24. American Academy of Paediatrics. Pickering LK, editor. Red Book: 2003 Report of the Com-mittee on Infectious Diseases. 26th ed. Elk Grove Village, IL: American Academy of Paediatrics; 2003: 643.
25. Joubert JR, Brink S, Hentzen GM. Allergic asthma in different population groups in the Western Cape. S Afr Med J 1988; 73:150-4.
26. Mitre E, Norwood S, Nutman TB. Saturation of immunoglobulin E (IgE) binding sites by poly-clonal IgE does not explain the protective effect of helminth infections against atopy. Infect Im-mun 2005; 73:4106-11.
27. Godfrey RC, Gradidge CF. Allergic sensitization of human lung fragments prevented by satura-tion of IgE binding sites. Nature 1976; 259:484-6.
28. Hagel I, Lynch NR, DiPrisco MC, Lopez R, Garcia N. Allergic reactivity of children of different socio-economic levels in tropical populations. Int Arch Allergy Immunol 1993; 101:209-14.
29. Larrick JW, Buckley CF, Machamer CE, Schlagel GD, Yost JA, Blessing-Moore J, Levy D. Does hyperimmunoglobulinemia-E protect tropical populations from allergic disease? J Allergy Clin Immunol 1983; 71:184-8.
30. Van den Biggelaar AH, van Ree R, Rodriguez LC, Lell B, Deelder AM, Kremsner PG, Yazdanba-khsh M. Decreased atopy in children infected with Schistosoma haematobium: role for parasite-induced interleukin-10. Lancet 2000; 356:1723-7.
31. Matricardi PM, Yazdanbakhsh M. Mycobacteria and atopy, 6 years later: a fascinating, still un-Þ nished, business. Clin Exp Allergy 2003; 33:717-20.
32. Fincham JE, Markus MB, Adams VJ, Lombard CJ, Bentwich Z, Mansvelt EPG, Dhansay MA, Schoeman SE. Association of deworming with reduced eosinophilia: implications for HIV/AIDS and co-endemic diseases. S Afr J Sc 2003; 99:182-3.
33. Dold S, Heinrich J, Wichmann H-E, Wjst M. Ascaris-speciÞ c IgE and allergic sensitization in a co-hort of school children in the former East Germany. J Allergy Clin Immunol 1998; 102:414-20.
34. Cooper PJ, Chico ME, Sandoval C, Espinel I, Guevara A, Kennedy MW, Urban JF, GrifÞ n GE, Nutman TB. Human infection with Ascaris lumbricoides is associated with a polarized cytokine response. J Infect Dis 2000; 182:1207-1213.
35. Shirakawa T, Enomoto T, Shimazu S, Hopkin JM. The inverse association between tuberculin responses and atopic disorder. Science 1997; 275:77-9.
36. Obihara CC, Beyers N, Gie RP, Potter PC, Marais BJ, Lombard CJ, Enarson DA, Kimpen JLL. Inverse association between Mycobacterium tuberculosis infection and atopic rhinitis in chil-dren. Allergy 2005; 60:1121-5.

7 Respiratory atopic disease, Ascaris-IgE and tuberculin test in urban South African children
101
37. Ota M, van der Sande M, Walraven G, Jeffries D, Nyan O, Marchant A, McAdam KP. Absence of association between delayed type hypersensitivity to tuberculin and atopy in children in The Gambia. Clin Exp Allergy 2003; 33:731-6.
38. Black GF, Fine PEM, Warndorff DK, Floyd S, Weir RE, Blackwell JM, et al. Relationship be-tween IFN-γ and skin test responsiveness to Mycobacterium tuberculosis PPD in healthy, non-BCG-vaccinated young adults in Northern Malawi. Int J Tuberc Lung Dis 2001; 7:664-72.
39. Stocks J, Dezateux C. The effect of parental smoking on lung function and development of the child. Respirology 2003; 8:266-85.

C H A P T E R 8
The association of prolonged breastfeeding and allergic disease in poor urban children
C.C. ObiharaB.J. MaraisR.P. GieP. PotterE.D. BatemanC.J. LombardN. BeyersJ.L.L. Kimpen
European Respiratory Journal2005; 25: 970-977

104
Infection with M. tuberculosis and atopy in children
Abstract
The fact that breastfeeding may protect against allergic disease remains controversial, with hardly any reports from developing countries. We investigated the association be-tween allergic disease in children and prolonged breastfeeding.
Data were collected from a 15% random sample of households from two poor suburbs of Cape Town, South Africa. Parents completed a validated ISAAC questionnaire on aller-gic diseases, for children aged 6-14 years. Other questions included breastfeeding duration, maternal smoking and parental allergy. Results were adjusted for possible confounders and for possible clustering within the household.
Out of 861 children included in the study, allergic disease in general, and hay fever in particular were signiÞ cantly less frequent in those with prolonged (≥ 6 months) breastfeed-ing. There was a signiÞ cant linear inverse association between breastfeeding duration and allergic disease in children without allergic parents, but not in children with an allergic predisposition.
In conclusion, these results from a developing country, suggest a protective effect of prolonged breastfeeding on the development of allergic disease, particularly hay fever, in children born to nonallergic parents. This protective effect was not found in children with an allergic predisposition.

8 The association of prolonged breastfeeding and allergic disease in poor urban children
105
Introduction
The prevalence of allergic disease in developed countries has shown a dramatic in-crease in recent decades, and the relationship between breastfeeding and allergic disease in these countries remains uncertain. In developing countries, allergic disease also contin-ues to rise,1 and the relationship between breastfeeding and allergic disease has not been evaluated.
The increasing prevalence of allergic disease has been linked to reduced microbial ex-posure in early life.2,3 SpeciÞ c microbial stimuli are thought to stimulate T helper (Th) 1 immune responses, thus reducing the activity of the atopy-associated Th2 response.3 Breast-milk inß uences the bacterial ß ora in the infant gut, which may provide an important immune stimulus in infancy.4,5 The possible protective effect of breastfeeding on allergic disease remains controversial and epidemiological studies have yielded variable results,6-9 with little information from developing countries where the infection pressure is higher.
We set out to test the hypothesis that prolonged breastfeeding duration (based on the World Health Organization (WHO) deÞ nition), in children from a poor urban setting in a developing country, would be associated with less allergic disease than a shorter breast-feeding duration.
Material and methods
Study setting The current study was conducted in two suburbs (population 38,565 in 1996) of Cape
Town, South Africa, with poor socio-economic conditions (average household income in US dollars, US$ 98.77). The population-density is high (6-14 occupants per household), but all households had running water and electricity. A previous International Study on Asthma and Allergies in Childhood (ISAAC) survey done in Cape Town, within a simi-lar age group, had estimated the prevalence of different allergic disease manifestations as the following: asthma 13.3 %, allergic rhinoconjunctivitis 16%, and eczema 9%.10 In ac-cordance with World Health Organization (WHO) recommendations, mothers are routinely encouraged to practice prolonged breastfeeding. This is based on the generally accepted beneÞ ts of breast-milk against serious childhood infections, such as gastroenteritis.
Sample selection A 15% sample of household addresses was randomly selected. Trained Þ eldworkers
enumerated the people at each selected household, and all children aged 6-14 years were invited to participate in the study. Written informed consent was obtained from a parent or legal guardian before study enrolment.
Study design A cross-sectional, questionnaire-based survey was conducted from July-December,
2002, in children aged 6-14 years.
106
Infection with M. tuberculosis and atopy in children
QuestionnaireParents completed a questionnaire for each child, under the supervision of a trained
Þ eld worker. Questions on allergic disease were based on the validated ISAAC Phase-I questionnaire, translated into the local language (Afrikaans). Questions were asked on both previous (ever) and recent (≤ 12 months) asthma, hay fever and eczema. Additional questions included breastfeeding duration, maternal smoking during pregnancy and current household exposure to cigarette smoke; number of siblings; maternal education; household income; allergic history of the mother and father; and previous serious infectious illnesses (upper and lower respiratory tract infections, gastroenteritis, urinary tract infections, ear, nose and throat infections, measles, ß u and other viral infections) other than tuberculosis (TB), for which the child had to visit a doctor, a health-centre or be admitted to a hospi-tal. Data on the breastfeeding duration was collected as a categorical variable as follows; breastfed < 6 months, 6-12 months or > 12 months.
Tuberculin skin test The burden of TB is very high in the study area. The average notiÞ cation rate of new
bacteriologically conÞ rmed TB is 320 per 100,000·yr-1.11 A positive tuberculin skin test (TST) is a hallmark of primary infection with Mycobacterium tuberculosis (MTB).12 TST reactivity becomes apparent in 3-6 weeks after initial MTB infection and may remain posi-tive for the lifetime of the individual.12 As MTB is known to stimulate a Th1 immune reac-tion,3 the TST response was documented in the children. Experienced study nurses carried out the TST by injecting 2 TU of PPD RT 23 (Statens Serum Institut, Copenhagen, Den-mark) intradermally on the volar aspect of the left forearm. The largest transverse diameter of induration was recorded after 2-3 days and in accordance with the American Thoracic Society (ATS) guidelines, a positive TST was deÞ ned as an induration of ≥ 10 mm.12
Defi nitions Allergic disease in general refers to the presence of at least one allergic disease: hay fe-
ver, asthma or eczema. Prolonged breastfeeding is deÞ ned as breastfeeding for > 6 months, and included all children that were breastfed, irrespective of the exclusivity of breast-feeding.
Statistical analysis The Chi-squared test was used to calculate associations between different allergic dis-
eases and the duration of breastfeeding and the Chi-squared test for linear-by-linear asso-ciation was used to detect linear trends. Logistic regression (LR) analyses were done with a random-effects LR model, using different allergic disease phenotypes as the dependent variable and breastfeeding duration as the independent variable. Adjustment was made for potential confounding variables such as demographic (age and sex), socioeconomic (av-erage household income and number of siblings), genetic (parental allergic history) and environmental factors (maternal smoking during pregnancy and TST response). Results were corrected for possible clustering in the sampling unit. The sampling unit in this study (cluster-survey) was the household. In total, there were 500 households in the study, with

8 The association of prolonged breastfeeding and allergic disease in poor urban children
107
an average of 1·6 children per household. For the analysis, each individual child was coded and linked to the speciÞ c household. By using the random-effects LR model for the mul-tivariate analyses correction was made for the possibility that more than one child came from the same household.
The study received ethics approval from the University of Stellenbosch (Stellenbosch, South Africa) and the relevant local authorities.
Results
Out of the 978 children enumerated, 884 (90.4%) consented to participation in the study. Of these, 861 children (97.4%) with data on breastfeeding duration were included in the analysis. The gender distribution was equal and the mean ± SD age was 10.4 ± 2.5 yrs. Since only 2.6% (23) of consenting children were never breastfed and the small size of this group provided insufÞ cient power for a separate analysis; together with the fact that the study question focused on association of breastfeeding duration and allergic disease, these children were excluded from the analysis. The baseline demographic parameters did not differ in those children who were excluded.
Table 1 describes the most important characteristics of the 861 children analysed. Of the children, 381 (44.3%) were breastfed for > 6 months. Children exposed to short- and prolonged- breastfeeding duration did not differ with respect to age, gender, maternal edu-cation level, maternal or paternal allergic history, maternal smoking during the pregnancy or positive TST (Table 1). Neither did they differ in the reported frequency of previous seri-ous infections other than tuberculosis (P = 0.25) nor rate of hospital admissions (P = 0.40). However, children who received prolonged breastfeeding were more likely to come from low income households and to have ≥ 3 siblings (Table 1).
Figure 1 illustrates the differences in frequency of different allergic disease phenotypes, between children exposed to short-breastfeeding and prolonged breastfeeding duration. The risk of allergic disease in general and hay fever in particular was signiÞ cantly lower in children with prolonged breastfeeding than in those with short breastfeeding duration (adjusted odds ratio (OR): 0.50; 95% conÞ dence interval (CI): 0.31-0.82 and adjusted OR: 0.53; 95% CI: 0.29-0.99, respectively), while this was not statistically signiÞ cant for asth-ma (ORadj 0.67; 95% CI 0.31-1.49) or eczema (adjusted OR: 0.56; 95% CI: 0.29-1.08).
There was a signiÞ cant linear inverse association between the breastfeeding duration and the frequency of allergic disease in general, and hay fever in particular, but not for asthma or eczema (Table 2).
The relationship between different categories of breastfeeding duration and allergic dis-ease phenotypes was evaluated in a random-effects LR model, together with possible con-founding variables. In this model, the risk of different allergic diseases was compared be-tween group 1 (breastfed < 6 months), group 2 (6-12 months) and group 3 (> 12 months). Compared to group 1, group 2 had signiÞ cantly less risk of allergic disease in general (ad-justed OR: 0.52; 95% CI: 0.28-0.97), while group 3 had signiÞ cantly less risk of allergic disease in general and hay fever in particular. While the difference in risk of allergic dis-
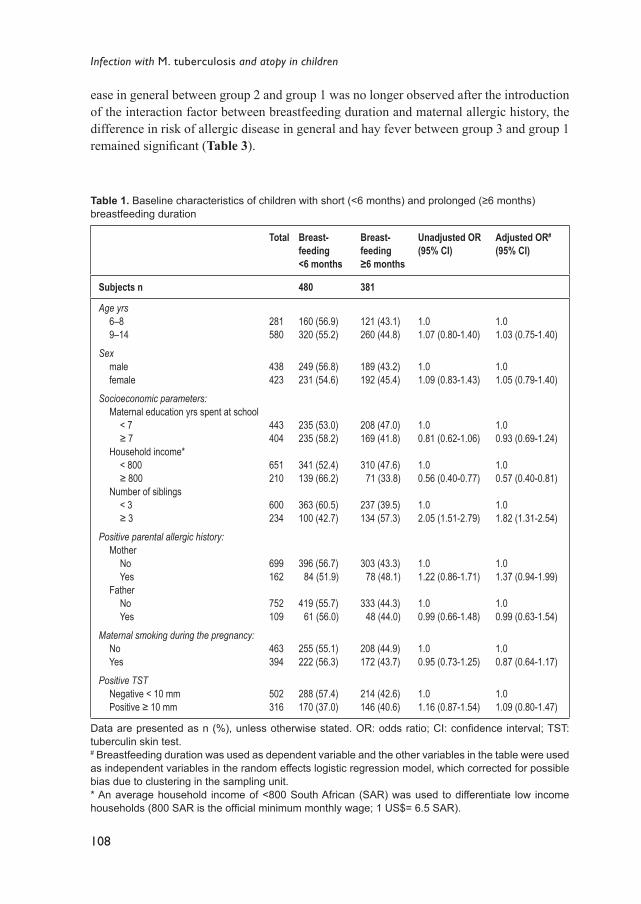
108
Infection with M. tuberculosis and atopy in children
Table 1. Baseline characteristics of children with short (<6 months) and prolonged (≥6 months) breastfeeding duration
Total Breast-feeding <6 months
Breast-feeding ≥6 months
Unadjusted OR (95% CI)
Adjusted OR#
(95% CI)
Subjects n 480 381
Age yrs 6�8 9�14
Sex male female
Socioeconomic parameters: Maternal education yrs spent at school < 7 ≥ 7 Household income* < 800 ≥ 800 Number of siblings < 3 ≥ 3
Positive parental allergic history: Mother No Yes Father No Yes
Maternal smoking during the pregnancy: No Yes
Positive TST Negative < 10 mm Positive ≥ 10 mm
281580
438423
443404
651210
600234
699162
752109
463394
502316
160 (56.9)320 (55.2)
249 (56.8)231 (54.6)
235 (53.0)235 (58.2)
341 (52.4)139 (66.2)
363 (60.5)100 (42.7)
396 (56.7) 84 (51.9)
419 (55.7) 61 (56.0)
255 (55.1)222 (56.3)
288 (57.4)170 (37.0)
121 (43.1)260 (44.8)
189 (43.2)192 (45.4)
208 (47.0)169 (41.8)
310 (47.6) 71 (33.8)
237 (39.5)134 (57.3)
303 (43.3) 78 (48.1)
333 (44.3) 48 (44.0)
208 (44.9)172 (43.7)
214 (42.6)146 (40.6)
1.01.07 (0.80-1.40)
1.01.09 (0.83-1.43)
1.00.81 (0.62-1.06)
1.00.56 (0.40-0.77)
1.02.05 (1.51-2.79)
1.01.22 (0.86-1.71)
1.00.99 (0.66-1.48)
1.00.95 (0.73-1.25)
1.01.16 (0.87-1.54)
1.01.03 (0.75-1.40)
1.01.05 (0.79-1.40)
1.00.93 (0.69-1.24)
1.00.57 (0.40-0.81)
1.01.82 (1.31-2.54)
1.01.37 (0.94-1.99)
1.00.99 (0.63-1.54)
1.00.87 (0.64-1.17)
1.01.09 (0.80-1.47)
Data are presented as n (%), unless otherwise stated. OR: odds ratio; CI: conÞ dence interval; TST: tuberculin skin test. # Breastfeeding duration was used as dependent variable and the other variables in the table were used as independent variables in the random effects logistic regression model, which corrected for possible bias due to clustering in the sampling unit.* An average household income of <800 South African (SAR) was used to differentiate low income households (800 SAR is the ofÞ cial minimum monthly wage; 1 US$= 6.5 SAR).
ease in general between group 2 and group 1 was no longer observed after the introduction of the interaction factor between breastfeeding duration and maternal allergic history, the difference in risk of allergic disease in general and hay fever between group 3 and group 1 remained signiÞ cant (Table 3).
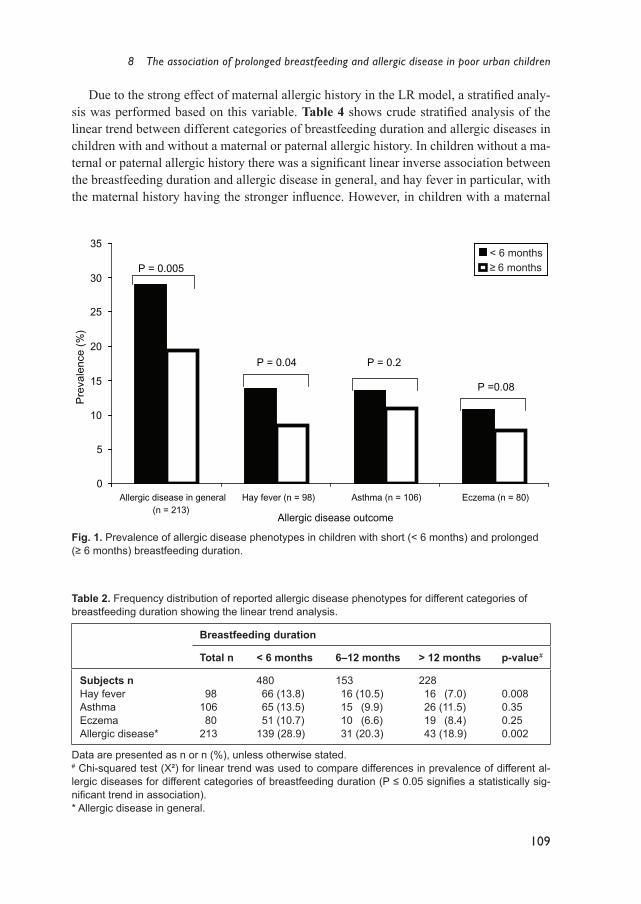
8 The association of prolonged breastfeeding and allergic disease in poor urban children
109
Due to the strong effect of maternal allergic history in the LR model, a stratiÞ ed analy-sis was performed based on this variable. Table 4 shows crude stratiÞ ed analysis of the linear trend between different categories of breastfeeding duration and allergic diseases in children with and without a maternal or paternal allergic history. In children without a ma-ternal or paternal allergic history there was a signiÞ cant linear inverse association between the breastfeeding duration and allergic disease in general, and hay fever in particular, with the maternal history having the stronger inß uence. However, in children with a maternal
Table 2. Frequency distribution of reported allergic disease phenotypes for different categories of breastfeeding duration showing the linear trend analysis.
Breastfeeding duration
Total n < 6 months 6�12 months > 12 months p-value #
Subjects nHay feverAsthma EczemaAllergic disease*
98106 80213
480 66 (13.8) 65 (13.5) 51 (10.7)139 (28.9)
153 16 (10.5) 15 (9.9) 10 (6.6) 31 (20.3)
228 16 (7.0) 26 (11.5) 19 (8.4) 43 (18.9)
0.0080.350.250.002
Data are presented as n or n (%), unless otherwise stated. # Chi-squared test (Χ²) for linear trend was used to compare differences in prevalence of different al-lergic diseases for different categories of breastfeeding duration (P ≤ 0.05 signiÞ es a statistically sig-niÞ cant trend in association). * Allergic disease in general.
0
5
10
15
20
25
30
35
Allergic disease in general(n = 213)
Hay fever (n = 98) Asthma (n = 106) Eczema (n = 80)
Allergic disease outcome
Pre
vale
nce
(%)
P = 0.005
P = 0.04 P = 0.2
P =0.08
< 6 months≥ 6 months
Fig. 1. Prevalence of allergic disease phenotypes in children with short (< 6 months) and prolonged (≥ 6 months) breastfeeding duration.

110
Infection with M. tuberculosis and atopy in childrenTa
ble
3. O
dds
ratio
s (O
R) o
f the
ass
ocia
tion
of d
iffer
ent a
llerg
ic d
isea
se p
heno
type
s an
d ca
tego
ries
of b
reas
tfeed
ing
dura
tion,
bef
ore
and
afte
r adj
ustin
g fo
r pos
sibl
e co
nfou
ndin
g va
riabl
es in
clud
ed in
the
mod
el (N
=861
)
Varia
ble
Aller
gic d
iseas
e in
gene
ral
Hay f
ever
Asth
ma
Ecze
ma
Unad
just
ed O
R(9
5% C
I)Ad
just
ed O
R(9
5% C
I)Un
adju
sted
OR
(95%
CI)
Adju
sted
OR
(95%
CI)
Unad
just
ed O
R (9
5% C
I)Ad
just
ed O
R(9
5% C
I)Un
adju
sted
OR
(95%
CI)
Adju
sted
OR
(95%
CI)
Brea
stfee
ding
dura
tion
mon
ths
<
6 #
6�
12 ̂
> 12
*
Sex
Ma
le
Fema
le
Age
yrs
6�
8
9�14
Num
ber o
f sibl
ings
<
3
≥ 3
Hous
ehold
inco
me
SAR
<
800
≥
800
Mat
erna
l pos
itive
aller
gic h
istor
y
No
Yes
Mat
erna
l sm
oking
durin
g pr
egna
ncy
No
Ye
s
TST
Ne
gativ
e <10
mm
Po
sitive
≥ 10
mm
1.0 0.63 (
0.40-
0.97)
0.57 (
0.39-
0.84)
1.0 0.87 (
0.64-
1.18)
1.0 1.07 (
0.77-
1.49)
1.0 0.64 (
0.44-
0.93)
1.0 1.67 (
1.19-
2.36)
1.0 2.58 (
1.80-
3.71)
1.0 1.15 (
0.84-
1.57)
1.0 0.61 (
0.43-
0.85)
1.0 0.74 (
0.37-
1.48)
0.37 (
0.19-
0.72)
1.0 1.07 (
0.70-
1.64)
1.0 1.18 (
0.75-
1.87)
1.0 0.59 (
0.34-
1.01)
1.0 1.48 (
0.86-
2.54)
1.0 3.31 (
1.60-
6.86)
1.0 1.55 (
0.98-
2.47)
1.0 0.58 (
0.36-
0.93)
1.0 0.73 (
0.41-
1.31)
0.47 (
0.27-
0.84)
1.0 0.82 (
0.54-
1.27)
1.0 1.65 (
1.01-
2.70)
1.0 0.48 (
0.27-
0.83)
1.0 2.65 (
1.72-
4.10)
1.0 3.47 (
2.22-
5.43)
1.0 0.85 (
0.55-
1.30)
1.0 0.43 (
0.26-
0.71)
1.0 0.97 (
0.39-
2.40)
0.29 (
0.10-
0.84)
1.0 0.93 (
0.53-
1.63)
1.0 2.20 (
1.12-
4.30)
1.0 0.53 (
0.25-
1.12)
1.0 2.35 (
1.21-
4.56)
1.0 4.46 (
1.91-
10.41
)
1.0 1.40 (
0.77-
2.57)
1.0 0.40 (
0.21-
0.77)
1.0 0.70 (
0.39-
1.28)
0.83 (
0.51-
1.35)
1.0 0.67 (
0.44-
1.02)
1.0 0.93 (
0.60-
1.42)
1.0 0.60 (
0.36-
1.00)
1.0 1.55 (
1.0-2
.41)
1.0 2.22 (
1.41-
3.49)
1.0 1.71 (
1.13-
2.58)
1.0 0.73 (
0.47-
1.14)
1.0 0.79 (
0.26-
2.44)
0.49 (
0.18-
1.35)
1.0 0.52 (
0.26-
1.05)
1.0 0.78 (
0.38-
1.60)
1.0 0.47 (
0.19-
1.13)
1.0 1.69 (
0.70-
4.13)
1.0 2.49 (
0.76-
8.16)
1.0 3.51 (
1.51-
8.15)
1.0 0.69 (
0.33-
1.44)
1.0 0.59 (
0.29-
1.19)
0.77 (
0.44-
1.34)
1.0 1.04 (
0.66-
1.65)
1.0 1.06 (
0.65-
1.75)
1.0 0.84 (
0.49-
1.44)
1.0 0.89 (
0.51-
1.53)
1.0 1.86 (
1.11-
3.12)
1.0 1.01 (
0.64-
1.61)
1.0 0.56 (
0.33-
0.96)
1.0 0.57 (
0.20-
1.65)
0.52 (
0.21-
1.32)
1.0 1.63 (
0.88-
3.04)
1.0 1.25 (
0.65-
2.41)
1.0 0.75 (
0.35-
1.59)
1.0 0.70 (
0.32-
1.53)
1.0 2.51 (
0.97-
6.51)
1.0
1.04
(0.5
4-1.
99)
1.0
0.49
(0.2
4-0.
98)
CI:
conÞ
den
ce in
terv
al; S
AR
: Sou
th A
frica
n R
and
(1 U
SD
= 6
.5 S
AR
); TS
T= tu
berc
ulin
ski
n te
st; # g
roup
1; ^
gro
up 2
; * g
roup
3; I
nter
actio
n te
rms
betw
een
brea
stfe
edin
g du
ratio
n an
d m
ater
nal a
llerg
ic h
isto
ry w
ere
adde
d to
the
mod
els
and
test
ed: f
or a
llerg
ic d
isea
se in
gen
eral
(p =
0.0
2), h
ay fe
ver (
p =
0.3)
, as
thm
a (p
= 0
.03)
and
ecz
ema
(p =
0.5
). In
the
rand
om-e
ffect
s lo
gist
ic re
gres
sion
mod
el, a
llerg
ic d
isea
se p
heno
type
s w
ere
used
as
the
depe
nden
t var
iabl
e, w
hile
cat
egor
ies
of b
reas
tfeed
ing
dura
-tio
n an
d co
nfou
ndin
g va
riabl
es a
s in
depe
nden
t var
iabl
e. R
esul
ts w
ere
adju
sted
for a
ll th
e va
riabl
es in
the
tabl
e: d
emog
raph
ic (
age,
sex
), so
cioe
cono
mic
(n
umbe
r of s
iblin
gs a
nd a
vera
ge h
ouse
hold
inco
me)
, gen
etic
pre
disp
ositi
on (m
ater
nal a
llerg
ic h
isto
ry w
as u
sed
beca
use
its e
ffect
was
stro
nger
than
pa-
tern
al a
llerg
ic h
isto
ry) a
nd e
nviro
nmen
tal e
xpos
ures
(mat
erna
l sm
okin
g du
ring
preg
nanc
y an
d TS
T re
activ
ity).
We
also
cor
rect
ed fo
r pos
sibl
e bi
as d
ue to
cl
uste
ring
in th
e sa
mpl
ing
unit
(hou
seho
ld).
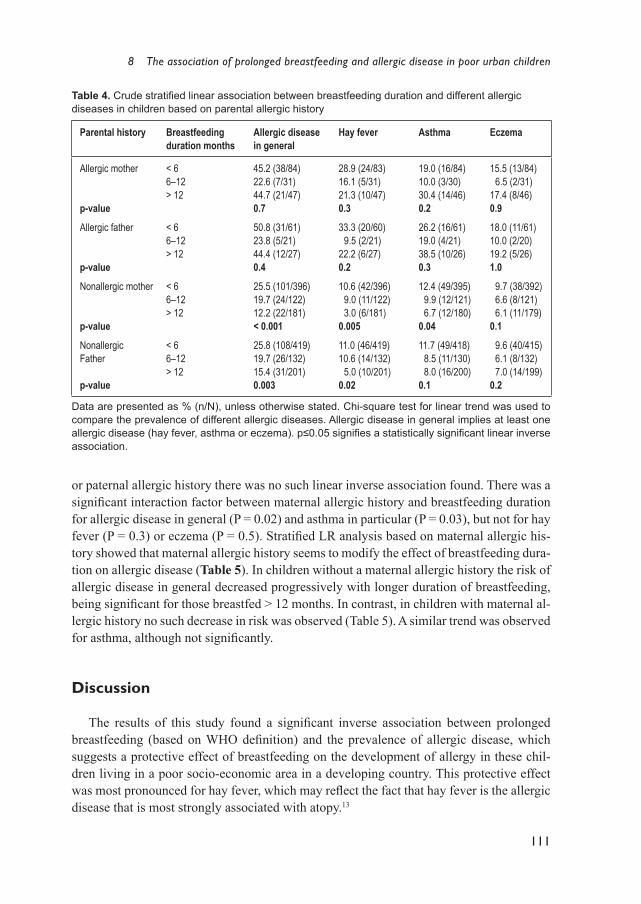
8 The association of prolonged breastfeeding and allergic disease in poor urban children
111
or paternal allergic history there was no such linear inverse association found. There was a signiÞ cant interaction factor between maternal allergic history and breastfeeding duration for allergic disease in general (P = 0.02) and asthma in particular (P = 0.03), but not for hay fever (P = 0.3) or eczema (P = 0.5). StratiÞ ed LR analysis based on maternal allergic his-tory showed that maternal allergic history seems to modify the effect of breastfeeding dura-tion on allergic disease (Table 5). In children without a maternal allergic history the risk of allergic disease in general decreased progressively with longer duration of breastfeeding, being signiÞ cant for those breastfed > 12 months. In contrast, in children with maternal al-lergic history no such decrease in risk was observed (Table 5). A similar trend was observed for asthma, although not signiÞ cantly.
Discussion
The results of this study found a signiÞ cant inverse association between prolonged breastfeeding (based on WHO deÞ nition) and the prevalence of allergic disease, which suggests a protective effect of breastfeeding on the development of allergy in these chil-dren living in a poor socio-economic area in a developing country. This protective effect was most pronounced for hay fever, which may reß ect the fact that hay fever is the allergic disease that is most strongly associated with atopy.13
Table 4. Crude stratiÞ ed linear association between breastfeeding duration and different allergic diseases in children based on parental allergic history
Parental history Breastfeeding duration months
Allergic diseasein general
Hay fever Asthma Eczema
Allergic mother
p-value
< 66�12> 12
45.2 (38/84)22.6 (7/31)44.7 (21/47)0.7
28.9 (24/83)16.1 (5/31)21.3 (10/47)0.3
19.0 (16/84)10.0 (3/30)30.4 (14/46)0.2
15.5 (13/84) 6.5 (2/31)17.4 (8/46)0.9
Allergic father
p-value
< 66�12> 12
50.8 (31/61)23.8 (5/21)44.4 (12/27)0.4
33.3 (20/60) 9.5 (2/21)22.2 (6/27)0.2
26.2 (16/61)19.0 (4/21)38.5 (10/26)0.3
18.0 (11/61)10.0 (2/20)19.2 (5/26)1.0
Nonallergic mother
p-value
< 66�12> 12
25.5 (101/396)19.7 (24/122)12.2 (22/181)< 0.001
10.6 (42/396) 9.0 (11/122) 3.0 (6/181)0.005
12.4 (49/395) 9.9 (12/121) 6.7 (12/180)0.04
9.7 (38/392) 6.6 (8/121) 6.1 (11/179)0.1
Nonallergic Father
p-value
< 66�12> 12
25.8 (108/419)19.7 (26/132)15.4 (31/201)0.003
11.0 (46/419)10.6 (14/132) 5.0 (10/201)0.02
11.7 (49/418) 8.5 (11/130) 8.0 (16/200)0.1
9.6 (40/415) 6.1 (8/132) 7.0 (14/199)0.2
Data are presented as % (n/N), unless otherwise stated. Chi-square test for linear trend was used to compare the prevalence of different allergic diseases. Allergic disease in general implies at least one allergic disease (hay fever, asthma or eczema). p≤0.05 signiÞ es a statistically signiÞ cant linear inverse association.

112
Infection with M. tuberculosis and atopy in children
The mechanisms responsible for the protective effect of breastfeeding against allergic disease are not well understood, but several factors may contribute. The hygiene hypoth-esis suggests that reduced microbial exposure in childhood results in reduced Th1 activity, with resultant Th2 dominance and an increased incidence of allergy.2,3,14
Breast-milk stimulates, through its high oligosaccharide contents, intestinal colonisation with speciÞ c bacterial ß ora, such as lactobacilli, biÞ dobacteria and non-pathogenic Esche-richia coli which may inß uence the development of gut-driven immune responses.4,5,15-18 Gut colonisation with these bacteria induces the production of Th1 cytokines, which counterbal-ance Th2 activity.5 This is supported by studies which have shown that allergic children are less frequently colonized with lactobacilli and biÞ dobacteria than non-allergic children.19,20 In addition, breast-milk may provide direct protection against allergic sensitisation through decreased exposure to food antigens, by enhanced maturation of the intestinal mucosal bar-rier and via immunoglobulins (Ig), such as secretory IgA, secreted in the milk.18,21
A striking feature of the results is the observation of an inverse association of breast-feeding duration and the risk of allergic disease in children without an allergic predispo-sition. A history of allergy in either parent appeared to neutralise the protective effect of prolonged breastfeeding. This observation has been reported previously,22 but the study evaluated a select group of hospitalised patients whose mothers were encouraged to carry on breastfeeding as long as possible. Differences in the breast milk content between aller-gic and non-allergic mothers have been proposed as a possible explanation for this obser-vation, because the breast-milk of allergic mothers has lower levels of ovalbumin-speciÞ c IgA, salivary SIgA, alpha-linoleic and polyunsaturated fatty acids (PUFA) and higher lev-els of Th2 promoting cytokines.23-26 However, the fact that the inverse association between prolonged breastfeeding and allergic disease was negated by an allergic family history, irrespective of whether it was maternal or paternal, suggests that genetic predisposition is probably the overriding factor. Even though a history of maternal allergy was associated
Table 5. Odds ratios (OR) showing effect modiÞ cation of the association of allergic disease and breastfeeding duration by maternal allergic history #
Breastfeeding duration months
Allergic disease in general Asthma
No maternal allergic history
Maternal allergic history
No maternal allergic history
Maternal allergic history
< 6 6-12> 12
1.00.71 (0.35-1.44)0.36 (0.18-0.73)
1.00.28 (0.08-0.91)1.27 (0.53-3.02)
1.00.55 (0.11-2.76)0.43 (0.11-1.65)
1.00.27 (0.03-2.06)3.57 (1.00-12.79)
Data are presented as OR (95% conÞ dence interval). The analysis was limited to the two allergic dis-ease phenotypes with a signiÞ cant interaction coefÞ cient with maternal allergic history, in the logistic re-gression (LR) analysis (Table 3). The random-effects LR model was used, with allergic disease pheno-types as a dependent variable, and breastfeeding duration and confounding variables as independent variables. Results were corrected for possible bias due to the clustering in the sampling unit. # Adjusted for possible confounding variables: demographic (age and sex), socioeconomic (number of siblings and household income), genetic predisposition (maternal allergic history was used in the model because its effect was stronger than paternal allergic history) and environmental exposures (maternal smoking during the pregnancy and tuberculin skin test reactivity).

8 The association of prolonged breastfeeding and allergic disease in poor urban children
113
with increased risk of allergic disease in the children in our study, this did not inß uence the association of prolonged breastfeeding and allergic disease in the multivariate analysis.
A few important characteristics differentiate our study from the less recent ones.6-9,22 Firstly, this study was conducted in a socio-economically disadvantaged urban community, within a developing country. Secondly, more than a quarter of the children were breastfed for >12 months, which enabled us to analyse the results of prolonged breastfeeding in two categories (6-12 months and >12 months). Thirdly, a random, community-based sampling method, without pre-selection of particular groups where the healthcare provider or re-searcher could have biased the choice or duration of infant feeding method, was used.
An interesting observation was the association found between maternal smoking during pregnancy and the risk of asthma in the child; this was not inß uenced by present smoking exposure. This is consistent with results from developed countries, which demonstrate that maternal smoking remains an important environmental risk factor for the development of asthma in children, even in poor settings.27-29
The present study does have several limitations inherent to its cross-sectional design and the retrospective questionnaire-based diagnosis. These include recall bias, reporter subjectivity and the fact that allergic disease was self-reported. Using the validated ISAAC-based questionnaire reduced some of the limitations associated with questionnaire-based evaluation. The possibility that health workers may have exerted a biased inß uence on the mother�s decision to prolong breastfeeding depending on the perceived risk of allergy in the child seems unlikely, as the frequency of maternal allergic history did not differ be-tween children with prolonged breastfeeding duration and those with a short breastfeeding duration.
Even though the presence of a positive TST was independently associated with a re-duced risk of allergic disease, it did not inß uence the association found between breastfeed-ing duration and allergic disease in the multivariate analysis. The reported prevalence of childhood infections other than MTB was also similar in the different breastfeeding groups. There is a possibility that the lack of association of breastfeeding duration and previous infection between the groups analyzed may be related to the fact that all previous infections were analysed as a single variable. However, this does not seem to inß uence the results as the frequency did not differ between the different categories of breastfeeding duration.
We were unable to analyse the results of children who were not breastfed, the statisti-cal power was limited by the small size of this group. Data on exclusive breastfeeding was not available, which made it impossible to differentiate between the effects of exclusive breastfeeding and mixed feeding, but it is known that few mothers in the study area breast-feed exclusively.30
The World Health Organization promotes prolonged breastfeeding (for ≥6 months) as the preferred method of infant feeding, especially in settings with poor healthcare services and unhygienic living conditions, to reduce serious infections in infancy.31 An additional advantage of promoting prolonged breastfeeding as a public health strategy may be the reduction of allergic disease, especially hay fever, in children without an allergic predispo-sition. There is a need for prospective community-based studies to evaluate the relation of breastfeeding duration and atopy.
114
Infection with M. tuberculosis and atopy in children
References
1. Weinberg EG. Urbanization and childhood asthma: an African perspective. J Allergy Clin Immu-nol 2000; 105:224-31.
2. Strachan D. Hay fever, hygiene and household size. Br Med J 1989; 289:1259-60. 3. Shirakawa T, Enomoto T, Shimazu S, Hopkin J. The inverse association between tuberculin re-
sponses and atopic disorder. Science 1997; 275:77-9. 4. Yashioka H, Fujita F. Development and differences of intestinal ß ora in neonatal period of breast-
fed and bottle-fed infants. Pediatrics 1983; 72:317-21. 5. Hessle C, Hanson A, Wold AE. Lactobacilli from human gastrointestinal mucosa are strong stim-
ulators of IL-12 production. Clin Exp Immunol 1999; 116:276-282. 6. Saarinen UM, Kajosaari M, Backman A, Siimes MA. Prolonged breastfeeding as prophylaxis for
atopic disease. Lancet 1979; 2:163-6. 7. Saarinen UM, Kajosaari M. Breastfeeding as prophylaxis against atopic diseases: prospective
follow-up until 17 years old. Lancet 1995; 346:1065-9. 8. Wright AL, Holberg CJ, Taussig LM, Martinez FD. Relationship of infant feeding to recurrent
wheezing at age 6 years. Arch Pediatr Adolesc Med 1995; 149:758-63. 9. Sears M, Greene J, Willan A, et al. Long-term relation between breastfeeding and development of
atopy and asthma in children and young adults: a longitudinal study. Lancet 2002; 360:901-7.10. ISAAC Steering Committee. Worldwide variation in prevalence of symptoms of asthma, allergic
rhinoconjunctivitis, and atopic eczema: ISAAC. Lancet 1998; 351:1225-32.11. Verver S, Warren RM, Munch Z, et al. Proportion of tuberculosis transmission that takes place in
a high-incidence area. Lancet 2004; 363:212-4.12. Shingadia D, Novelli V. Diagnosis and treatment of tuberculosis in children. Lancet Infectious
Disease 2003; 3:624-32.13. Pearce N, Pekkanen J, Beasley R. How much asthma is really attributable to atopy? Thorax 1999;
54:268-72.14. Rook G, Stanford J. Give us this day our daily germs. Immunol Today 1998; 19:113-6.15. Sepp E, Julge K, Vasar M, Naaber P, Björkstén B, Mikelsaar M. Intestinal microß ora of Estonian
and Swedish infants. Acta Paediatr 1997; 86:956-61.16. Lodinová R, Jouja V. Antibody production by mammary gland in mothers after artiÞ cial oral
colonization of their infants with non-pathogenic strain E. coli. Acta Paediatr Scand 1977; 66:705-8.
17. Prescott S, Macaubas C, Holt B, et al. Transplacental priming of the human immune system to environmental allergens: universal skewing of initial T cell responses toward the Th2 cytokine proÞ le. J. Immunol 1999; 160:4730-7.
18. Hoppu U, Kalliomäki M, Laiho K, Isolauri E. Breast milk � immunomodulatory signals against allergic diseases. Allergy 2001; 56(Suppl 67):23-6.
19. Björkstén B, Naaber P, Sepp E, Mikelsaar M. The intestinal microß ora in allergic Estonian and Swedish 2-year-old children. Clin Exp Allergy 1999; 29:342-6.
20. Kalliomäki M, Seppo S, Arvilommi H, Kero P, Koskinen P, Isolauri E. Probiotics in primary pre-vention of atopic disease: a randomised placebo-controlled trial. Lancet 2001; 357:1076-9.
21. Brandtzaeg P. Current understanding of gastrointestinal immunoregulation and its relation to food allergy. Ann N.Y. Acad Sci 2002; 964:13-45.
22. Savilahti E, Tainio V-M, Salmenperä L, Siimes MA, Perheentupa J. Prolonged exclusive breast-feeding and heredity as determinants in infantile atopy. Arch Dis Child 1987; 62:269-73.
23. Casas R, Böttcher MF, Duchén K, Björkstén B. Detection of IgA antibodies to cat, β-lactoglobu-lin, and ovalbumin allergens in human milk. J Allergy Clin Immunol 2000; 105:1236-40.
24. Van Asperen PP, Gleeson M, Kemp AS. The relationship between atopy and salivary IgA deÞ -
8 The association of prolonged breastfeeding and allergic disease in poor urban children
115
ciency in infancy. Clin Exp Immunol 1985; 62:753-7.25. Duchén K, Casas R, Böttcher MF, Yu G, Björkstén B. Human milk polyunsaturated long-chain
fatty acids and secretory immunoglobulin A antibodies and early childhood allergy. Pediatr Al-lergy Immunol 2000; 11:29-39.
26. Böttcher MF, Jenmalm MC, Garofalo RP, Björkstén B. Cytokines in breast milk from allergic and nonallergic mothers. Pediatr Res 2000; 47:157-62.
27. Martinez FD, Cline M, Burrows B. Increased incidence of asthma in children of smoking moth-ers. Pediatrics 1992; 89:21-6.
28. Cook DG, Strachan DP. Health effects of passive smoking � 10: summary of effects of paren-tal smoking on the respiratory health of children and implications for research. Thorax 1999; 54:357-66.
29. Cook DG, Strachan DP, Carey IM. Parental smoking and spirometric indices in children. Thorax 1998; 53:884-93.
30. Van der Elst CW, Pick W, Isaacs S, Malan AF. Current trends in infant feeding. S Afr Med J 1989; 76:434-7.
31. Black R, Cesar V. Optimal duration of exclusive breastfeeding in low income countries. Br Med J 2002; 325:1252-3.


117
C H A P T E R 9
General conclusion and recommendations for future studies
What is known about the protective effect of mycobacterial infection on atopic disease?
The assumption that the protective effect of Mycobacterium tuberculosis (M. tuberculo-sis) infection on atopic disease would logically be more evident in the pediatric population of a high tuberculosis (TB) burden area (where exposure to TB bacilli is more likely to be intense and persistent) than in children from a low TB burden area (where exposure to TB bacilli is more likely to be sporadic and intermittent) stimulated us to perform the studies described in this thesis.
During the last few decades, the prevalence of atopic disease has increased in coun-tries with a Western lifestyle.1 The �hygiene hypothesis� suggests that a relationship exists between improved hygiene and an increase in atopic diseases prevalence.2 An underly-ing mechanism for this hypothesis is that the lack of microbial stimulation leads to either an inappropriate T helper (Th) type immune response or inappropriate Th cell regulatory mechanisms. A speciÞ c infectious agent responsible for the hygiene hypothesis has not yet been identiÞ ed, although many candidate diseases have been suggested, such as measles, hepatitis A and respiratory infections. Animal models have identiÞ ed mycobacteria as an important potential candidate in the hygiene hypothesis by demonstrating that infection with mycobacteria or exposure to mycobacterial products leads to regulatory mechanisms which restored the immune homeostasis.3 In contrast, the epidemiologic relation between mycobacterial infection and atopic disease in humans is still unclear and controversial. The current evidence on this topic is reviewed in Chapter 4. The majority of studies did not Þ nd evidence for a protective effect of mycobacterial infection on the development of atopic disease. This is in contrast with studies in murine models which showed a clear sup-pression of atopic symptoms after exposure to mycobacterial products.3 Most of the previ-ous studies were carried out in populations with low incidence of mycobacterial infection. It is not clear how M. tuberculosis infection and/or tuberculosis (TB) disease impact on the development of atopy in developing countries, where M. tuberculosis infection is endemic and allergic disease common. Among the possible factors which may explain these differ-ent Þ ndings, next to heterogeneity in the study design and methodology, are differences in type and deÞ nition of mycobacterial infection, in the intensity and persistence exposure to the mycobacterium, variability in dosage and strain of BCG vaccine, lack of uniformity in the deÞ nition of atopic disease and genetic variability. Given the importance of chronic infections, such as those caused by mycobacteria, in inß uencing both the induction and ef-

118
Infection with M. tuberculosis and atopy in children
fector phases of the immune response against allergens, through the stimulation of a strong regulatory network, it is relevant for future studies to take into account the type, intensity and persistence of mycobacterial exposure of the speciÞ c population being studied. In con-clusion, the prevalence of atopy in a population may be inß uenced by the intensity and persistence of mycobacterial infection in that same population.
What is the relation between M. tuberculosis infection and atopic disease in a tuberculosis endemic area?
We have demonstrated an inverse association between tuberculin skin test (TST) re-activity, an accepted marker of M. tuberculosis infection, and the prevalence of allergic symptoms, particularly allergic rhinitis in children from a high TB burden area (Chap-ter 5). In addition, we observed a signiÞ cant inverse linear association of the size of TST and both the frequency and risk of allergic symptoms, particularly allergic rhinitis. These Þ ndings support our hypothesis that M. tuberculosis infection may inß uence atopic disease in children from a high TB burden area.
In a separate study we further demonstrated a signiÞ cant inverse association between M. tuberculosis infection and atopic rhinitis, and reduced prevalence of allergy skin prick test (SPT) reactivity in allergic children with positive TST, when compared to allergic chil-dren with negative TST, suggesting that M. tuberculosis infection inß uences the expression of atopy (Chapter 6). These results conÞ rm previous Þ ndings and are in support of new insights in the explanation of the hygiene hypothesis. It has been suggested that inhibition of allergic inß ammation in the presence of chronic and persistent infections, such as M. tuberculosis, probably occurs through the stimulation of regulatory and anti-inß amma-tory networks.4,5 Recent reports have suggested that differences in mycobacterial expo-sure and thus, variability in the degree of possible immunomodulation may differ between populations and this may partly explain the differences in epidemiological Þ ndings in the literature.5 Some studies in humans have shown that the size of TST is directly correlated with serum levels of gamma interferon (IFN-γ), implying that a large TST size may reß ect strong Th1 immunity.6 Moreover, very strong TST responses are more strongly associated with natural M. tuberculosis infection than with M. bovis-bacille Calmette-Guérin (BCG) or mycobacteria other than tuberculosis (MOTT).7,8 Based on these observations, the in-verse association found in the present study may be explained by the high percentage of TST positivity in the study population. This seems to suggest that a strong cell-mediated immunity against M. tuberculosis may stimulate immunomodulation to an extent which inß uences the development of atopy.5
In conclusion, the results suggest that in the presence of intense and persistent natural infection with M. tuberculosis cell-mediated immunity of the host against M. tuberculosis may stimulate regulatory and anti-inß ammatory networks to such an extent as to inhibit the development of atopic disease.

9 General conclusion and recommendations for future studies
119
What is the infl uence of other endemic co-infections on the relationship between M. tuberculosis infection and atopic disease?
To test the effect of endemic co-infections in the study population on the protective effect of M. tuberculosis infection on atopic disease we tested the relation of Ascaris lum-bricoides infection (Ascaris eggs in stool samples and Ascaris speciÞ c IgE), atopic disease and tuberculin reactivity. This relation has not been observed previously in an area with high burden of M. tuberculosis infection. In Chapter 7 we demonstrated that Ascaris spe-ciÞ c IgE (Ascaris-sIgE) is a signiÞ cant risk factor for the development of atopic disease in children. This is in support of some previous Þ ndings, but contrasts with others. Although earlier studies hypothesized that polyclonal IgE produced during helminth infection may block allergic reaction by either suppressing antigen-speciÞ c IgE production or by satura-tion of IgE receptors on mast cells, other studies which demonstrated lack of saturation of mast cell capacity in vitro or in vivo argue against this mechanism.9-12 Recent evidence sug-gests that helminthic infection may inß uence allergic disease manifestation.4,13 This effect may depend on the intensity and persistence of infection. With chronic and intense infec-tion, atopic symptoms may be suppressed through the stimulation of regulatory networks and anti-inß ammatory cytokines, while mild and intermittent infection may result in en-hanced reaction to environmental allergens.4 Our Þ nding of increased atopic manifestation in children with elevated Ascaris-sIgE reß ects the mild intensity of helminthic infection in our study population due to periodic anthelminthic therapy in school children in the area. The fact that we did not observe the same effect in the presence of Ascaris egg in the stool sample suggests a difference of effect between Ascaris eggs in the stool and an elevated Ascaris-sIgE, especially in populations where intestinal helminth infection is of mild in-tensity. This is supported by studies suggesting that an elevated Ascaris-sIgE level and the presence of Ascaris eggs in the stool may measure different entities.14 An elevated Ascaris-sIgE level reß ects the competency of the host Th2 immune response to Ascaris antigen. The presence of Ascaris eggs in the stool reß ects active infection, although the impact of this infection on the host immune response may depend on different factors, including the severity and persistence of infection. In addition, we demonstrated in this study that M. tu-berculosis infection may be protective against the risk of developing atopy in the presence of Ascaris-sIgE. These Þ ndings support our hypothesis that M. tuberculosis infection, a strong Th1 immune stimulator may suppress atopic disease manifestation.
In conclusion, these results suggest that immune response to Ascaris (Ascaris-sIgE) may be a risk factor of atopic disease in populations exposed to mild Ascaris infection and that M. tuberculosis infection may be protective against this risk, probably by stimulation of anti-inß ammatory networks.

120
Infection with M. tuberculosis and atopy in children
What is the infl uence of prolonged breastfeeding and other environmental factors on the association between M. tuberculosis infection and atopic disease?
To further assess the effect of other known risk factors for the development of atopy on the association between M. tuberculosis infection and atopic disease, we tested the effect of prolonged breastfeeding and maternal smoking during pregnancy, environmental to-bacco smoke (ETS) exposure, household income, the number of siblings, parental allergic history and allergic symptoms (Chapter 8). We showed that prolonged breastfeeding was inversely associated with allergic symptoms, in general, and allergic rhinitis in particular. Although similar Þ ndings have been shown in industrialised countries, this has not been investigated in a community-based study in non-industrialised countries where a majority of mothers breastfeed their child. We also demonstrated a signiÞ cant linear inverse associa-tion between the duration of breastfeeding in months and the prevalence of allergic symp-toms in children without allergic parents, but not in children with a positive family history of allergic disease. We observed that maternal smoking during pregnancy was associated with a higher prevalence of asthma in the child and as expected we also found that children from households with higher income, lesser number of siblings or allergic predisposition had a higher prevalence of allergic symptoms than those without. This is in support of Þ nd-ings from industrialised countries. These Þ ndings however, did not inß uence the associa-tion between M. tuberculosis infection and atopic disease in a regression analysis model, indicating a different mechanism of action.
The mechanisms responsible for the protective effect of breastfeeding against allergic disease are not well understood, but several factors may contribute. The hygiene hypoth-esis suggests that reduced microbial exposure in childhood results in reduced Th1 activity, with resultant Th2 dominance and an increased incidence of allergy.2,8 Breast-milk stimu-lates, through its high oligosaccharide contents, intestinal colonisation with speciÞ c bacte-rial ß ora, such as lactobacilli, biÞ dobacteria and non-pathogenic Escherichia coli which may inß uence the development of gut-driven immune responses.15-20 Gut colonisation with these bacteria induces the production of Th1 cytokines, which counterbalance Th2 activ-ity.16 This is supported by studies which have shown that allergic children are less frequent-ly colonized with lactobacilli and biÞ dobacteria than non-allergic children.21,22 In addition, breast-milk may provide direct protection against allergic sensitisation through decreased exposure to food antigens, by enhanced maturation of the intestinal mucosal barrier and via immunoglobulins (such as secretory IgA) secreted in the milk.23
The observation that the protective effect of prolonged breastfeeding is limited to chil-dren without a family history of allergy has been reported previously in a selected group of hospitalised patients whose mothers were encouraged to carry on breastfeeding as long as possible.24 Differences in breast-milk between allergic and non-allergic mothers have been proposed as a possible explanation for this observation, because the breast-milk of allergic mothers has lower levels of ovalbumin-speciÞ c IgA, salivary SIgA, alpha-linoleic and polyunsaturated fatty acids (PUFA) and higher levels of Th2 promoting cytokines.25-28
However, the observation that the inverse association of prolonged breastfeeding and al-
9 General conclusion and recommendations for future studies
121
lergic disease was negated by an allergic family history, irrespective of whether it was maternal or paternal, suggests that genetic predisposition is probably the overriding factor. The increased frequency of asthma in children whose mother smoked during pregnancy is consistent with studies from industrialised countries, which demonstrate that maternal smoking remains an important environmental risk factor for the development of asthma in children, even in poor settings.29-31
In conclusion, we observed a strong inverse association between prolonged breastfeed-ing and the prevalence of allergic disease, which suggests a protective effect of breastfeed-ing on the development of atopy. However, the effect of prolonged breastfeeding was only found in children without an allergic predisposition. These results suggest that prolonged breastfeeding might be a possible public health strategy for reducing the prevalence of al-lergic disease, especially allergic rhinitis, in children with non-allergic parents. The study also highlights the importance of reducing environmental tobacco smoke exposure and the need to include women from non-industrialised countries in intensive efforts to reduce tobacco smoking.
Recommendations for future research
It is relevant that future studies on the protective effect of mycobacterial infection on atopic disease take into account the intensity and persistence of mycobacterial exposure or infection in the population being investigated. More reliable evidence can be obtained with a large population-based prospective study.
In contrast with Þ ndings in animal models which observed suppression of atopic mani-festation after exposure to mycobacterial products, epidemiological evidence in humans on this topic is inconclusive. Next to heterogeneity in the study design and methodology, differences in type and deÞ nition of mycobacterial infection, in the intensity and persis-tence of exposure to the mycobacterium, variability in dosage and strain of BCG vaccine, lack of uniformity in the deÞ nition of atopic disease and genetic variability may contrib-ute to differences in Þ ndings. Given new insights in the possible importance of intense and persistent infections in inß uencing immune responses against allergens, it is relevant for future studies to be performed in populations with persistent and intense exposure to mycobacterial infection. Moreover, stronger evidence is more likely to be achieved with a population-based prospective study design.
Future studies investigating the protective effect of mycobacterial infection on the development of atopic disease need to identify objective and speciÞ c prospective param-eters for measuring the immune response to mycobacterial exposure and/or infection. This may be realized by prospectively measuring speciÞ c Th1- and anti-inß ammatory cytokines in response to mycobacterial antigens, in addition to the delayed-type hyper-sensitivity reaction to tuberculin.
122
Infection with M. tuberculosis and atopy in children
Among possible new areas of investigation to assess the protective effect of mycobacte-rial infection on the development of atopic disease, recently proposed by Matricardi et al., is measuring anti-inß ammatory cytokine levels instead of TST responses in response to mycobacterial antigens.5 A shortcoming of the use of anti-inß ammatory- and Th1 cytokine assays in population-based studies is the intra- and inter-personal variability in the serum level of cytokines which may not always reß ect the concentration at the site of infection or inß ammation. In addition, the interpretation of prospective anti-inß ammatory cytokine levels may be more difÞ cult in populations which are continuously exposed to endemic infections (such as mycobacteria and helminths). Future studies using serum cytokine lev-els to measure immune response to mycobacterial infection should take into account indi-vidual and population differences in baseline serum cytokine levels.
Genetic variability between populations should be taken into account by future stud-ies on the protective effect of mycobacterial infection on atopic disease
An efÞ cient Th1 immune response is required for the elimination of M. tuberculosis and deÞ ciency or mutations of genes involved in Th1 responses lead to extreme sensitiv-ity to mycobacterium infection in laboratory animals and in humans. In addition, both the expression of atopic disease and baseline cytokine levels may also be under the inß uence of genetic variability.
Novel diagnostic methods using antigen-speciÞ c T cell detection may improve sensi-tivity in differentiating between M. tuberculosis infection and other mycobacterial infec-tions such as M. bovis-BCG or other MOTTs.
In addition to the known shortcomings of delayed-type-hypersensitivity reaction to tu-berculin in diagnosing TB infection, diagnostic difÞ culties inherent to childhood TB, which lead to under-diagnosis (e.g., non-speciÞ c symptom-complex, difÞ culty with identiÞ cation of hilar lymphadenopathy on chest radiograph, pauci-bacillary TB and lower frequency of cavitating disease) may limit the use of pulmonary TB to investigate the relationship between mycobacterial infection or disease and atopy, especially in resource-poor areas. Novel speciÞ c diagnostic methods using antigen-speciÞ c T cell detection may improve the sensitivity and speciÞ city of TST response in differentiating between infection with M. tu-berculosis and that with M. bovis or other mycobacteria. However, the use of these tests in epidemiological studies has yet to be established.
Future studies investigating the protective effect of mycobacteria on atopic disease need to use globally accepted deÞ nitions of atopy, such as that recently proposed by the World Allergy Organization and must take into account the possible confounding or effect-modiÞ cation by other co-infections and/or environmental risk factors in the population.

9 General conclusion and recommendations for future studies
123
The heterogeneity in the deÞ nition and outcome of atopy used in the literature calls for uniformity in the deÞ nition of atopy for future studies. The new World Allergy Organiza-tion (WAO) deÞ nition of atopy, which makes it possible to deÞ ne atopic diseases more uniformly, will make it easier to compare future studies.32
Evidence that other chronic (co-)infections, such as that by parasites or other environ-mental factors such as breastfeeding, environmental tobacco smoke exposure, number of siblings and socioeconomic factors, may also stimulate anti-inß ammatory networks that inß uence atopic disease manifestation necessitates future studies on the relationship be-tween mycobacterial infection and atopy to seriously take co-infections and other environ-mental factors into account.
124
Infection with M. tuberculosis and atopy in children
References
1. ISAAC Steering Committee. Worldwide variation in prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and atopic eczema: ISAAC. Lancet 1998; 351:1225-32.
2. Strachan D. Hay fever, hygiene and household size. BMJ 1989; 289:1259-60. 3. Zuany-Amorim C, Sawicka E, Manlius C, Le Moine A, Brunet LR, Kemeny DM, et al. Suppres-
sion of airway eosinophilia by killed Mycobacterium vaccae-induced allergen-speciÞ c regula-tory T-cells. Nat Med 2002; 8:625�9.
4. Yazdanbakhsh M, Van den Biggelaar A, Maizels RM. Th2 responses without atopy: immunoreg-ulation in chronic helminth infections and reduced allergic disease. Trends in Immunology 2001; 22:372-7.
5. Matricardi PM, Yazdanbakhsh M. Mycobacteria and atopy, 6 years later : a fascinating, still un-Þ nished business. Clin Exp Allergy 2003; 33 :717-20.
6. Black GF, Fine PEM, Warndorff DK, Floyd S, Weir RE, Blackwell JM, et al. Relationship be-tween IFN-γ and skin test responsiveness to Mycobacterium tuberculosis PPD in healthy, non-BCG-vaccinated young adults in Northern Malawi. Int J Tuberc Lung Dis 2001; 7:664�72.
7. Shingadia D, Novelli V. Diagnosis and treatment of tuberculosis in children. Lancet Infect Dis 2003; 3:624-32.
8. Shirakawa T, Enomoto T, Shimazu S, Hopkin J. The inverse association between tuberculin re-sponses and atopic disorder. Science 1997; 275:77�9.
9. Godfrey RC, Gradidge CF. Allergic sensitization of human lung fragments prevented by satura-tion of IgE binding sites. Nature 1976; 259:484-6.
10. Hagel I, Lynch NR, DiPrisco MC, Lopez R, Garcia N. Allergic reactivity of children of different socio-economic levels in tropical populations. Int Arch Allergy Immunol 1993; 101:209-14.
11. Larrick JW, Buckley CF, Machamer CE, Schlagel GD, Yost JA, Blessing-Moore J, Levy D. Does hyperimmunoglobulinemia-E protect tropical populations from allergic disease? J Allergy Clin Immunol 1983; 71:184-8.
12. Van den Biggelaar AH, van Ree R, Rodriguez LC, Lell B, Deelder AM, Kremsner PG, Yazdan-bakhsh M. Decreased atopy in children infected with Schistosoma haematobium: role for para-site-induced interleukin-10. Lancet 2000; 356:1723-7.
13. Cooper PJ. Can intestinal helminth infections (geohelminths) affect the development and expres-sion of asthma and allergic disease? Clin Exp Immunol 2002; 128:398-404.
14. Dold S, Heinrich J, Wichmann H-E, Wjst M. Ascaris-speciÞ c IgE and allergic sensitization in a co-hort of school children in the former East Germany. J Allergy Clin Immunol 1998; 102:414-20.
15. Yashioka H, Fujita F. Development and differences of intestinal ß ora in neonatal period of breast-fed and bottle-fed infants. Pediatrics 1983; 72:317-21.
16. Hessle C, Hanson A, Wold AE. Lactobacilli from human gastrointestinal mucosa are strong stim-ulators of IL-12 production. Clin Exp Immunol 1999; 116:276-82.
17. Sepp E, Julge K, Vasar M, Naaber P, Björkstén B, Mikelsaar M. Intestinal microß ora of Estonian and Swedish infants. Acta Paediatr 1997; 86:956-61.
18. Lodinová R, Jouja V. Antibody production by mammary gland in mothers after artiÞ cial oral colonization of their infants with non-pathogenic strain E. coli. Acta Paediatr Scand 1977; 66:705-8.
19. Prescott SL, Macaubas C, Holt BJ, Smallacombe TB, Loh R, Sly PD, Holt PG. Transplacental priming of the human immune system to environmental allergens: universal skewing of initial T cell responses toward the Th2 cytokine proÞ le. J. Immunol 1998; 160:4730-7.
20. Hoppu U, Kalliomäki M, Laiho K, Isolauri E. Breast milk � immunomodulatory signals against allergic diseases. Allergy 2001; 56(Suppl 67):23-6.
21. Björkstén B, Naaber P, Sepp E, Mikelsaar M. The intestinal microß ora in allergic Estonian and

9 General conclusion and recommendations for future studies
125
Swedish 2-year-old children. Clin Exp Allergy 1999; 29: 342-6. 22. Kalliomäki M, Seppo S, Arvilommi H, Kero P, Koskinen P, Isolauri E. Probiotics in primary pre-
vention of atopic disease: a randomised placebo-controlled trial. Lancet 2001; 357:1076-79.23. Brandtzaeg P. Current understanding of gastrointestinal immunoregulation and its relation to
food allergy. Ann N.Y. Acad Sci 2002; 964:13-45. 24. Savilahti E, Tainio V-M, Salmenperä L, Siimes MA, Perheentupa J. Prolonged exclusive breast-
feeding and heredity as determinants in infantile atopy. Arch Dis Child 1987; 62:269-73.25. Casas R, Böttcher MF, Duchén K, Björkstén B. Detection of IgA antibodies to cat, β-lactoglobu-
lin, and ovalbumin allergens in human milk. J Allergy Clin Immunol 2000; 105:1236-40.26. Van Asperen PP, Gleeson M, Kemp AS. The relationship between atopy and salivary IgA deÞ -
ciency in infancy. Clin Exp Immunol 1985; 62:753-7.27. Duchén K, Casas R, Böttcher MF, Yu G, Björkstén B. Human milk polyunsaturated long-chain
fatty acids and secretory immunoglobulin A antibodies and early childhood allergy. Pediatr Al-lergy Immunol 2000; 11:29-39.
28. Böttcher MF, Jenmalm MC, Garofalo RP, Björkstén B. Cytokines in breast milk from allergic and nonallergic mothers. Pediatr Res 2000; 47:157-62.
29. Martinez FD, Cline M, Burrows B. Increased incidence of asthma in children of smoking moth-ers. Pediatrics 1992; 89:21-6.
30. Cook DG, Strachan DP. Health effects of passive smoking � 10: summary of effects of paren-tal smoking on the respiratory health of children and implications for research. Thorax 1999; 54:357-66.
31. Cook DG, Strachan DP, Carey IM. Parental smoking and spirometric indices in children. Thorax 1998; 53:884-93.
32. Johansson SGO, Bieber T, Dahl R, Friedmann P, Lanier BQ, Lockey RF, Motala C, Ortega Mar-tell JA, Platts-Mills TA, Ring J, et al. Revised nomenclature for allergy for global use: report of the Nomenclature Review Committee of the World Allergy Organization, October 2003. J Al-lergy Clin Immunol 2004; 113:832-6.


127
Summary / Samenvatting
The incidence of atopic disease has increased dramatically in countries with a western life-style. Although the exact cause(s) of the increase is still unknown, different hypotheses have been proposed. The hygiene hypothesis ascribes the rising incidence of atopic disease to reduction in incidence of serious infectious diseases, such as mycobacteria. Efforts are being made to investigate the possible protective effects of mycobacterial infection on the development of atopy, as this may be relevant for the production of mycobacterial-based vaccines against the development of atopic disease.
This thesis focuses on the relationship between Mycobacterium tuberculosis (M. tu-berculosis) infection and the prevalence of atopic disease manifestations in children. In addition, it evaluates the inß uence of co-morbidity with intestinal helminthic infection and other possible confounding or disease modifying environmental factors, such as prolonged breastfeeding, maternal smoking, number of siblings and socioeconomic variables, on this relation. A general introduction to the subject is given in Chapter 1, with a short summary of the epidemiology of tuberculosis (TB), particularly describing the diagnostic problems in the pediatric population. In addition, the epidemiology of atopic disease and the hygiene hypothesis in relation to infection with M. tuberculosis, co-infection with intestinal hel-minth and the inß uence of prolonged breastfeeding, is also discussed.
Optimal analysis of the interaction between infection with M. tuberculosis and allergic disease or atopy requires an excellent understanding of what happens when children become infected with M. tuberculosis and/or progress to disease. The period from 1920, when chest radiography was applied for diagnosis, to 1950, when effective chemotherapy against TB became available, represented a window of opportunity to document the natural history of TB in children (Chapter 2). This chapter reviews Þ ndings from the pre-chemotherapy era on the clinical epidemiology and natural history of TB in children. It discusses the two ma-jor transitions in childhood TB; from exposure to infection, and from infection to disease. Household exposure to a sputum smear-positive index-case posed the greatest transmis-sion risk (60-80%) to children. Household exposure to a sputum smear-negative index-case posed a reduced, but still appreciable risk (30-40%) of transmission. The high transmission risk posed by sputum smear-positive index-cases in the community, explains why TB con-trol programs focus predominantly on their identiÞ cation and treatment. The majority of children who became infected did so within 3 months of symptom onset in the adult index-case. In low TB prevalence areas, household exposure remained an important contributor to primary TB infection until old age. However, in high prevalence areas the majority of those who became infected after 2 years of age had no known household contact. They were more likely to be infected in the community. These Þ ndings provide the scientiÞ c basis for cur-rent TB contact investigation practices. The tuberculin skin test (TST), using the Mantoux method, was identiÞ ed as the optimal test to identify primary M. tuberculosis infection. The

128
Infection with M. tuberculosis and atopy in children
degree of skin induration induced by BCG immunization was usually < 10 mm, compared to natural M. tuberculosis infection, which was usually > 10 mm. BCG-induced skin hyper-sensitivity diminished with time and tuberculin responses frequently reverted after variable time periods depending on the BCG strain used. Children with primary TB infection before 2 years or after 10 years of age were at increased risk for disease development. The highest risk for cavitating pulmonary TB disease occurred in children who were Þ rst infected after 10 years of age. A high percentage of children developed transient radiological abnormali-ties following primary infection, which complicates the deÞ nition of disease as the major-ity of these children did not progress to disease. The highest risk for TB-related mortality following primary infection occurred during infancy and the lowest risk between 5 and 14 years. The diagnosis of childhood TB is difÞ cult because bacteriological conÞ rmation is rarely achieved and identiÞ cation of hilar lymphadenopathy on chest radiography is often impossible. Symptom-based diagnostic approaches are often promoted in high-burden set-tings. The literature on TB-related symptomatology in children is almost exclusively hospi-tal-based, which does not reß ect the prevalence of symptoms in the general population.
We documented in Chapter 3 the prevalence of symptoms associated with TB among randomly selected children living in a high-burden community and compared the preva-lence of these symptoms in children without TB and in children with newly diagnosed TB. We observed that these symptoms are common in the general pediatric population. Only weight loss, alone or in combination with other symptoms, was signiÞ cantly more common in children with newly diagnosed TB. Combinations of symptoms (symptom complexes) were more likely to be associated with TB than individual symptoms.
In Chapter 4 we provided an overview of the present literature on the relation between mycobacterial infection and atopy and systematically evaluated the causal relation. The majority of studies were conducted in countries with a Westernized lifestyle and relatively lower burden of TB. In contrast to studies in murine models, only a minority of studies observed evidence to support a protective effect of mycobacterial infection on the develop-ment of atopic disease. The results further revealed a high level of heterogeneity of studies. Possible explanations for the heterogeneity are differences in type, deÞ nition, intensity and persistence (chronicity) of mycobacterial exposure or infection, and lack of uniformity in the deÞ nition, type and test-method of atopic disease outcome variables.
The hygiene hypothesis suggests that infections, such as mycobacteria may protect against the development of atopic disease. This is supported by animal models demonstrat-ing that infection with mycobacteria or exposure to mycobacterial products led to regu-latory mechanisms which restored the immune homeostasis. In contrast, epidemiologic relationship between mycobacterial infection or exposure and atopic disease in humans is still unclear and controversial. As most of the previous studies were carried out in low TB burden countries, we studied in this thesis the protective effect of M. tuberculosis infection on atopy in the pediatric population in a community where M. tuberculosis infection rate is very high (Chapter 5). We observed that children with a positive TST, had a signiÞ cantly lower risk of allergic symptoms, particularly allergic rhinitis, than those with negative TST. We also observed a signiÞ cant inverse linear relation of the size of TST and both the fre-quency and risk of allergic symptoms, particularly allergic rhinitis.
Summary / Samenvatting
129
To further determine the protective effect of M. tuberculosis infection on atopic disease or allergic sensitization, we investigated the association between TST reactivity, atopic rhi-nitis and atopic sensitisation to common environmental aeroallergens in children (Chap-ter 6). We observed a signiÞ cant inverse association between M. tuberculosis infection and atopic rhinitis in children suggesting that M. tuberculosis infection may reduce the expres-sion of atopy. We also observed signiÞ cantly reduced allergy skin prick test (SPT) reactiv-ity in allergic children with M. tuberculosis infection, when compared to allergic children without M. tuberculosis infection, suggesting that M. tuberculosis infection may suppress atopic sensitisation. These Þ ndings are in support of a protective effect of M. tuberculosis infection on the development of atopic disease in this setting.
The epidemiologic relation between intestinal helminthic infection and atopic disease, both associated with a T helper (Th) 2 immune response, is controversial, since it has been reported that helminth infection may either suppress or predispose to atopic disease. Al-though M. tuberculosis infection is endemic in most helminth-infested populations in the developing world, the possible inß uence of M. tuberculosis, a strong stimulator of Th1 immunity on the effect of helminth infection on the development of atopic disease has not been investigated. We investigated the association of Ascaris lumbricoides infection (spe-ciÞ c-IgE or eggs), and atopic sensitization to common aeroallergens or atopic diseases in the pediatric population (Chapter 7). In addition, we tested the inß uence of positive TST on the associations investigated. We observed a signiÞ cant association between elevated Ascaris speciÞ c-IgE level and increased risk of atopic asthma, atopic rhinitis or atopic sen-sitization to common environmental aeroallergens. This study also shows that a positive TST may inß uence the association of Ascaris speciÞ c-IgE and atopic disease. In children with negative TST elevated Ascaris speciÞ c-IgE level was associated with increased risk of atopy, while in those with positive TST no increased risk was observed. Our Þ ndings suggest that immune response to Ascaris (elevated Ascaris speciÞ c-IgE level) may be a risk factor of atopic disease in populations exposed to mild Ascaris infection and that M. tuberculosis infection may be protective against this risk.
The protective effect of prolonged breastfeeding duration (based on the WHO deÞ ni-tion, ≥ 6 months) on allergic disease remains controversial and epidemiological studies have yielded variable results, with little information from developing countries where in-fectious diseases, such as TB, are endemic. We set out to test the hypothesis that prolonged breastfeeding duration in children from a poor urban setting in a developing country would be associated with less allergic disease than short breastfeeding duration (Chapter 8). We also tested whether this effect would be independent from the effect of M. tuberculosis infection. Our study results showed a signiÞ cant inverse association between prolonged breastfeeding duration and the prevalence of allergic disease, especially allergic rhinitis. This effect was independent of the relation between M. tuberculosis infection and atopic disease. We also found a signiÞ cant inverse linear association between breastfeeding dura-tion and allergic disease prevalence in children without allergic parents, but not in children with allergic parents. These results suggest a protective effect of prolonged breastfeeding duration on the development of allergic disease, particularly allergic rhinitis, in children born to non-allergic parents. This protective effect was not found in children with an aller-

130
Infection with M. tuberculosis and atopy in children
gic predisposition, suggesting that genetic predisposition is probably the overriding factor. Another interesting observation was the association found between maternal smoking dur-ing pregnancy and the risk of asthma in the child (this effect was not inß uenced by present environmental tobacco smoke exposure). This is consistent with results from developed countries, which showed that maternal smoking remains an important environmental risk factor for the development of asthma in children, even in poor settings.
Based on the present Þ ndings, we recommend that prospective community-based stud-ies are needed to investigate the causal relation between mycobacterial infection and atopic disease, preferably in areas with high TB burden. We also recommend the use of a glob-ally accepted deÞ nition of atopy by future studies on this topic to increase uniformity. We call for the development and use of more sensitive and speciÞ c methods for diagnosing and differentiating between different mycobacterial infections and that other infectious co-morbidity and disease modiÞ ers as well the genetic variability in populations, be taken into account.
In de afgelopen decennia is er, vooral in landen met een westerse levensstijl, sprake van een toename van atopische ziekten. De oorzaak hiervoor is nog steeds onduidelijk. In de laatste tien jaar zijn verschillende hypothesen voorgesteld om deze toename te verklaren. Een van de meest bekende is de hygiëne hypothese. Deze veronderstelt dat de recente toe-name van de incidentie van atopische ziekten te verklaren is door de afname van ernstige infectieziekten, zoals tuberculose en parasitaire infecties. Er zijn steeds meer aanwijzingen dat infectie door met name mycobacteriën het afweerapparaat stimuleert tot de productie van anti-inß ammatoire cytokinen, zodat de ontstekingscytokinen die atopische verschijn-selen veroorzaken geremd worden.
De hygiëne hypothese wordt ondersteund door bevindingen bij dieren en door epidemi-ologische studies bij mensen. Studies in proefdieren hebben aangetoond dat infectie door mycobacteriën, of de blootstelling aan mycobacteriële producten, stimulatie van regula-toire mechanismen van het immuunsysteem veroorzaakt. Dit zou als gevolg hebben dat de immuunhomeostase zich herstelt en het risico op ontwikkelen van atopische verschijnselen afneemt. Sommige epidemiologische onderzoeken hebben een omgekeerde relatie aange-toond tussen infectie met mycobacteriën (o.a. M. tuberculosis, de bacterie die tuberculose veroorzaakt) en atopische ziekten.
Daarnaast wordt de hygiëne hypothese door recente studies ondersteund, die hebben laten zien dat de prevalentie van atopische ziekten relatief lager is in niet-geïndustriali-seerde landen. Dit alles heeft geleid tot belangstelling voor het beschermende effect van infectieziekten op de ontwikkeling van allergische ziekten. De kans op de productie van op mycobacteriële componenten gebaseerde vaccins tegen de ontwikkeling van atopische ziekten in de toekomst onderstreept het belang van dit effect. Over dit onderwerp is echter nauwelijks literatuur uit gebieden met hoge prevalentie van tuberculose. De meeste studies zijn uitgevoerd in landen met lage prevalentie van tuberculose.

Summary / Samenvatting
131
Het primaire doel van het onderzoek, beschreven in dit proefschrift, is de studie naar de relatie tussen atopische ziekteverschijnselen en infectie door M. tuberculosis, bij kinderen in een hoog tuberculose endemisch-gebied. Een secundair doel is het analyseren van het effect van co-infectie met parasieten (o.a. wormen) op deze relatie. Tenslotte is gekeken naar de invloed van andere bekende omgevingsfactoren (o.a. de duur van borstvoeding, het rookgedrag van de ouders en het aantal kinderen in het gezin) en socio-economische variabelen (o.a. gezinsinkomen) die deze relatie kunnen beïnvloeden.
Hoofdstuk 1 is een beknopte algemene introductie van de onderwerpen van het proef-schrift. Er wordt een korte samenvatting van de epidemiologie van tuberculose in de wereld gegeven, met daarbij speciÞ eke aandacht voor de tuberculoseproblematiek in het onder-zoeksgebied (de Westkaap provincie van Zuid-Afrika) en de speciÞ eke epidemiologische en diagnostische problemen van tuberculose bij kinderen. Daarnaast worden ook de recen-te epidemiologische data van atopische ziekten en de hygiëne hypothese geïntroduceerd, in relatie tot infectie door M. tuberculosis en co-infectie met wormen. Als laatste wordt de relatie tussen borstvoeding en atopische ziekten beschreven.
Kennis van de verschillende fasen van het tuberculose ziekteproces, vanaf het moment van besmetting met de tuberculosebacterie tot de progressie naar ziekte, is onontbeerlijk om de invloed van infectie met M. tuberculosis op de ontwikkeling van atopische ziekten te kunnen begrijpen. Daarom begonnen wij dit onderzoek met een studie naar het natuurlijke beloop van het tuberculose ziekteproces in de prechemotherapie periode (voor de ontdek-king van tuberculostatica). De periode vanaf 1920, toen de röntgenfoto voor het eerst als diagnostische methode van tuberculose toegepast werd, tot 1950, toen effectieve chemo-therapie ontdekt en toegepast werd, bood een unieke kans om het natuurlijke beloop van tuberculose bij kinderen te bestuderen. In deze periode kon men het beloop van tuberculose zonder de invloed van medicijnen documenteren, door kinderen die in contact waren met een volwassen met tuberculose, decennia lang klinisch te volgen. Dit werd gedaan met pe-riodieke Mantouxtesten, onderzoek naar symptomen en thoraxfoto�s.
Hoofdstuk 2 is een review van de literatuur in de prechemotherapie periode. De twee fasen van tuberculose op de kinderleeftijd, van transmissie (expositie) aan M. tuberculosis tot infectie en van infectie tot ziekte (tuberculose) worden in dit hoofdstuk beschreven. De meeste kinderen met infectie raken binnen 3 maanden nadat de index tuberculosepatiënt symptomen heeft ontwikkeld, besmet. Kinderen die thuis in contact zijn met een sputum-positieve tuberculose patiënt (vaak een volwassene) lopen het grootse risico op infectie met M. tuberculosis (60-80%). Kinderen die thuis in contact komen met een sputum-negatieve tuberculose patiënt lopen minder, maar toch nog een aanzienlijk risico (30-40%) om met M. tuberculosis geïnfecteerd te worden. Het hoge risico op besmetting door een sputum-po-sitieve tuberculose patiënt in de directe woonomgeving vormt de wetenschappelijke basis voor de opsporingsmethode van de huidige tuberculose preventie programma�s. Het effect van blootstelling aan een tuberculose patiënt in het gezin op de ontwikkeling van primaire tuberculose infectie is afhankelijk van de prevalentie van tuberculose in het gebied. In ge-bieden met een lage prevalentie van tuberculose is blootstelling van kinderen aan een tu-berculose patiënt in het gezin tot oudere leeftijd een belangrijke epidemiologische factor voor het ontwikkelen van een primaire tuberculose infectie. Daarentegen is in gebieden

132
Infection with M. tuberculosis and atopy in children
met hoge prevalentie van tuberculose, blootstelling van kinderen aan een tuberculose pa-tiënt in het gezin alleen in de eerste 2 levensjaren een signiÞ cante epidemiologische factor voor het ontwikkelen van een primaire tuberculose infectie, aangezien in een meerderheid van de kinderen de kans groter is om buiten de directe woonomgeving met tuberculose geïnfecteerd te worden dan thuis. De tuberculine huidtest (tuberculin skin test, TST) vol-gens Mantoux (de Mantouxtest), is de beste test voor de detectie van primaire infectie door M. tuberculosis. De grootte van de Mantouxreactie bij kinderen na vaccinatie met BCG was vaker < 10 mm, terwijl de Mantouxreactie vaker > 10 mm was na infectie met natuurlijke (wilde type) M. tuberculosis. De Mantouxreactie na vaccinatie met BCG werd na verloop van tijd minder in omvang en verdween uiteindelijk, afhankelijk van het type BCG-stam in het vaccin. Kinderen die voor de leeftijd van 2 jaar of na de leeftijd van 10 jaar een primaire infectie met M. tuberculosis kregen, hadden een toegenomen risico op de ontwikkeling van tuberculose (ziekte). Het hoogste risico op de ontwikkeling van een holte in de longen (caverne) door tuberculose werd gezien bij kinderen die na de leeftijd van 10 jaar voor de eerste keer geïnfecteerd werden. Een hoog percentage kinderen vertoonde voorbijgaande radiologische afwijkingen na een primaire infectie met M. tuberculosis. Het feit dat slechts een minderheid van deze kinderen uiteindelijk tuberculose ziekte ontwikkelde, is illustratief voor de moeilijkheden van de radiologische classiÞ catie van longtuberculose bij kinderen. Het hoogste risico op mortaliteit na primaire infectie met tuberculose, werd waargenomen bij zuigelingen, en het laagste risico in de leeftijdsgroep tussen 5 en 14 jaar.
Het stellen van de diagnose tuberculose bij kinderen is moeilijk omdat vaak geen bac-teriologische bevestiging kan worden verkregen. Daarnaast is het moeilijk om hilaire lym-fadenopathie op röntgenfoto�s te identiÞ ceren. Diagnose gebaseerd op symptomen, wordt gestimuleerd in hoog tuberculose-endemische gebieden. Echter de literatuur met betrek-king tot de symptomatologie van tuberculose bij kinderen is exclusief gebaseerd op onder-zoeken bij symptomatische kinderen opgenomen in het ziekenhuis. Dit weerspiegelt dus niet de werkelijke prevalentie van deze symptomen in de algemene populatie. In hoofd-stuk 3 wordt de prevalentie van bekende tuberculose-geassocieerde symptomen beschre-ven in de algemene pediatrische populatie in een hoog tuberculose-endemisch gebied. De prevalentie van deze symptomen wordt vergeleken tussen kinderen zonder tuberculose en kinderen met recent gediagnosticeerde tuberculose. Uit de studieresultaten blijkt dat deze symptomen veel voorkomen in de algemene pediatrische populatie, ook bij kinderen zon-der tuberculose. Alleen het symptoom gewichtsverlies (alleen of in combinatie met andere bekende symptomen) blijkt signiÞ cant vaker voor te komen bij kinderen met recent gedi-agnosticeerde tuberculose. De combinatie van symptomen (symptoomcomplexen) blijkt meer voorspelbaar te zijn voor tuberculose dan individuele symptomen.
Hoofdstuk 4 is een sytematische review van de literatuur over de relatie tussen atopi-sche ziekten en infectie met mycobacteriën. Een aantal van de studies vond geen evidentie voor het beschermende effect van een mycobacteriële infectie op het ontwikkelen van ato-pie. De meeste van deze studies zijn uitgevoerd in landen met een westerse levensstijl waar de prevalentie van tuberculose relatief laag is. De resultaten van de review tonen echter een hoog percentage van heterogeniteit aan tussen de studies, niet alleen door diversiteit in de studieopzet, maar ook door verschillen in het type, de deÞ nitie, de intensiteit en de

133
persistentie van de mycobacteriële infectie. Daarnaast was er sprake van een gebrek aan uniformiteit in de deÞ nitie en in het type atopische ziekte dat bestudeerd werd, alsook in de diagnostische methode die gebruikt werd om atopie aan te tonen.
Gezien het feit dat de meeste studies in de literatuur uitgevoerd zijn in landen met een relatief lage prevalentie van tuberculose, besloten wij het onderzoek naar de relatie tussen infectie met M. tuberculosis en atopische ziekten te verrichten in de pediatrische popula-tie van een hoog tuberculose-endemisch gebied (hoofdstukken 5 en 6). In hoofdstuk 5 wordt het onderzoek naar de relatie tussen infectie met M. tuberculosis en symptomen van atopische ziekten bij kinderen beschreven. De resultaten laten zien dat kinderen die geïnfecteerd zijn met M. tuberculosis (TST ≥ 10 mm) signiÞ cant minder risico hebben op atopische symptomen, vooral allergische rhinitis (hooikoorts) dan kinderen zonder infectie met M. tuberculosis (TST < 10 mm). Er was een signiÞ cante omgekeerde lineare relatie tussen de grootte van de Mantouxreactie (in mm) en zowel de frequentie als het risico van allergische ziekten, met name allergische rhinitis. Dit wordt voor het eerst in dit onderzoek aangetoond.
In hoofdstuk 6 wordt de relatie tussen infectie met M. tuberculosis en atopische rhinitis (gedeÞ neerd volgens de deÞ nitie van de Wereld Allergie Organisatie, als het hebben van zowel allergische symptomen als positieve allergietest) beschreven. De resultaten tonen aan dat kinderen met infectie door M. tuberculosis signiÞ cant minder atopische rhinitis hebben dan kinderen zonder infectie door M. tuberculosis. Het verschil was gebleven na correctie voor alle mogelijke confounders in een multivariaat analyse. Dit suggereert dat infectie met M. tuberculosis de expressie van atopische ziekteverschijnselen onderdrukt. Deze bevindingen ondersteunen de veronderstelling dat infectie door M. tuberculosis, on-der bepaalde omstandigheden, een beschermend effect kan hebben op de ontwikkeling van atopische ziekten.
Er zijn aanwijzingen dat infectie met parasieten (zoals worminfectie) atopische ziekten kan beïnvloeden. De epidemiologische relatie tussen infectie met wormen en atopische ziekte, beide geassocieerd met een T-helper (Th) 2 immuunrespons, is nog niet volledig opgehelderd. Hoewel sommige epidemiologische studies melden dat infectie door wormen tot onderdrukking van atopische verschijnselen kan leiden, vinden andere studies juist dat worminfecties tot het ontstaan van atopische verschijnselen predisponeert. Er zijn steeds meer aanwijzingen dat dit verschil in bevindingen op de prevalentie van parasitaire infectie in de populatie lijkt te berusten. Populaties met een lage prevalentie van wormen zouden meer atopische ziekten hebben, terwijl in populaties met een hoge prevalentie van para-sitaire infecties atopische aandoeningen minder zouden vookomen. Ondanks het feit dat infectie door M. tuberculosis in de meeste niet-geïndustrialiseerde landen met een hoge incidentie van worminfecties voorkomt, is de invloed van M. tuberculosis op de relatie tussen infectie met wormen en atopische ziekten nooit eerder onderzocht. In hoofdstuk 7 wordt de relatie tussen infectie met Ascaris lumbricoides of spoelworm (verhoogde serum Ascaris-speciÞ eke IgE of positieve Ascaris eieren in de feces) en atopische ziekten of sen-sibilisatie (positieve allergie huidtesten) in de pediatrische populatie van een gebied waar infectie door wormen mild endemisch voorkomt beschreven. Daarnaast werd de invloed van infectie door M. tuberculosis op deze relatie bestudeerd. De resultaten laten zien dat
Samenvatting
134
Infection with M. tuberculosis and atopy in children
kinderen met een verhoogd serum Ascaris speciÞ eke IgE signiÞ cant meer verschijnselen van respiratoire atopische ziekten hebben (vooral atopische astma en atopische rhinitis), alsook meer positieve allergie huidtesten en meer bronchiale hyperreactiviteit. De resul-taten laten verder zien dat het effect van infectie met Ascaris lumbricoides op atopische ziekten verschilt tussen kinderen met en kinderen zonder infectie door M. tuberculosis. Bij kinderen zonder infectie door M. tuberculosis was het hebben van een verhoogde Ascaris speciÞ eke IgE geassocieerd met een signiÞ cant hoger risico op atopische ziekteverschijn-selen, atopische sensibilisatie en bronchiale hyperreactiviteit. In kinderen met M. tuber-culosis infectie was een verhoogde serum Ascaris speciÞ eke IgE niet geassocieerd met verhoogd risico op atopie of allergische symptomatologie. Deze bevindingen suggereren dat de immuunrespons tegen Ascaris lumbricoides een risicofactor is voor de ontwikkeling van atopische ziekten in populaties met milde worminfectiedruk en dat infectie met M. tu-berculosis tegen dit risico beschermt.
De literatuur is tegenstrijd over de beschermende effecten van langdurige borstvoe-ding (≥ 6 maanden volgens het WHO criteria) op de ontwikkeling van atopische ziekten bij kinderen. Borstvoeding stimuleert de groei van speciÞ eke bacteriën (o.a. lactobacilli, biÞ dobacteria en non-pathogene Escherichia coli) die een Th1 immuunrespons stimuleren, wat de ontwikkeling van atopische ziekten zou kunnen beïnvloeden. Borstvoeding zou daarnaast direct tegen de ontwikkeling van atopische sensibilisatie beschermen, door de verminderde blootstelling aan voedingsallergenen, de stimulatie van de uitrijping van het darmslijmvlies en de productie van secretorisch IgA in de melk.
Sommige van de studies vonden evidentie voor een beschermend effect van langdu-rige borstvoeding op atopische ziekten, terwijl andere geen beschermend effect vonden. Over dit onderwerp is geen literatuur uit derde wereld landen te vinden, ondanks het feit dat vrouwen in deze landen gedurende langere duur borstvoeding geven dan vrouwen in westerse landen. Het is mogelijk dat het effect van borstvoeding kan verschillen, door variabiliteit in persoonlijke hygiënische maatregelen rondom de borstvoeding in verschil-lende populaties. In hoofdstuk 8 wordt de hypothese getoetst dat langdurige borstvoeding in kinderen uit een arme stedelijke wijk gepaard zou gaan met minder allergische ziekten. Daarnaast wordt onderzocht of de invloed van langdurige borstvoeding op atopische ver-schijnselen onafhankelijk is van het effect van infectie met M. tuberculosis in de studie po-pulatie. De resultaten laten zien dat kinderen die langdurig borstvoeding kregen signiÞ cant minder atopische ziekteverschijnselen hebben. De duur van borstvoeding (in maanden) was omgekeerd gecorreleerd met de prevalentie van atopische ziekten. Opvallend is de bevinding dat het effect van borstvoeding op allergische ziekten beperkt was tot kinderen zonder allergische ouders, en niet waargenomen werd bij kinderen met allergische ouders. In een multivariaat analyse blijkt het beschermende effect van langdurige borstvoeding op allergische ziekten onafhankelijk te zijn van het beschermende effect van infectie door M. tuberculosis. Dit wijst op een ander werkingsmechanisme. Uit de resultaten kan gecon-cludeerd worden dat langdurige borstvoeding een beschermend effect heeft op de ontwik-keling van allergische ziekte, vooral hooikoorts, bij kinderen zonder allergische predispo-sitie. Hetzelfde kan niet gezegd worden voor kinderen met allergische predispositie, wat op een sterkere invloed van genetische factoren op de ontwikkeling van atopische ziekten

135
wijst. Een andere interessante bevinding is dat kinderen wier moeder tijdens de zwanger-schap gerookt heeft een meer dan 3 keer hoger risico hebben op symptomen van astma dan kinderen wier moeder tijdens de zwangerschap niet gerookt heeft. Dit effect werd niet be-invloed door het huidige rookgedrag van de volwassenen thuis. Vergelijkbare bevindingen zijn beschreven in studies uit westerse landen. Dit betekent dat het roken door de moeder een belangrijke beïnvloedbare omgevingsfactor is voor astmatische klachten bij kinderen, ook in zich ontwikkelende landen. Dit pleit voor meer betrokkenheid van vrouwen in der-dewereld landen in de strijd tegen blootstelling van kinderen aan sigarettenrook, vooral in de thuisomgeving.
In conclusie suggereren de resultaten van de studies beschreven in dit proefschrift dat infectie met M. tuberculosis, onder bepaalde omstandigheden, in hoog endemische gebie-den, een beschermend effect kan hebben op de ontwikkeling van atopische ziekten. Pros-pectieve onderzoeken in vergelijkbare omstandigheden zijn noodzakelijk om het causaal verband verder uit te diepen. Het is belangrijk dat de studies in de toekomst gebruik maken van internationaal geaccepteerde deÞ nities van atopische ziekten. Dit zal de vergelijking van studieresultaten vergemakkelijken. Verder zijn meer sensitieve en speciÞ eke methoden nodig voor de diagnose van infectie door M. tuberculosis bij kinderen. Nieuwe diagnos-tische methoden in de immunologie bieden mogelijkheden om in de toekomst de infectie door M. tuberculosis te onderscheiden van infectie door andere mycobacteriën. Over de speciÞ citeit en sensitiviteit van deze nieuwe methoden in grote populatiestudies zijn nog te weinig data gepubliceerd. Als laatste vinden wij het van belang dat toekomstige studies rekening houden met andere co-morbiditeitsvariabelen in de analyse van de resultaten, zo-als co-infecties in de bestudeerde populatie, langdurige borstvoeding en blootstelling aan tabaksrook, en de invloed van genetische factoren.
Samenvatting

Summary / Samenvatting
137
Acknowledgements / Dankwoord
I here with thank different persons who contributed, directly or indirectly, to the realiza-tion of this thesis.
Professor Jan Kimpen, my promoter; dear Jan, I thank you especially for seeing the potential under the surface and for the conÞ dence. Although there were moments when we doubted if any of the manuscripts would be published, we never doubted we were on the right track. Your tendency to see the clear lines, combined with your positive attitude made me see the pebbles in the sand. What I appreciated most in our joint venture is your punc-tuality, rationality and stability, while at the same time giving some degrees of freedom to do things my own way.
Prof. Nulda Beyers, my copromoter; dear Nulda, your optimism is contagious and your hospitality, a lesson for many. Although I cannot match your inexhaustible energy nor be as much African as you are, I have been able to learn from you to see small successes and failures in the context of a bigger and longer term perspective - the bigger picture, as you called it.
Prof. Robert Gie, Rob, you taught me to read pediatric chest radiographs (the �rules of 3�). But most of all you taught me that �what one cannot sketch, one cannot explain properly�. I am trying to teach the same to our students. Your logical approach to problems and the schematic manner of solving issues are both intimidating and accommodating.
Professor Paul Potter; dear Paul, without your knowledge of the allergic conditions in the Western Cape, this thesis may not have been concluded as quickly as now. Thanks for your invaluable contribution.
Dr. Maarten Hoekstra; dear Maarten, although you joined the bandwagon at a later stage, your detailed critique in a gentlemanly manner and your suggestions came at an ap-propriate moment to open doors of ideas which may otherwise have remained shut.
Dr. Ben Marais; dear Ben, one of my best investments in friendship was to have been the Þ rst and only colleague to invite you, Karen and Richard to my home during your work-visit to Utrecht. This became even more obvious during our stay in Cape Town. You made us experience unlimited hospitality, even before you became a colleague. Although I came to respect and appreciate the way you sometimes �destroyed� my manuscripts-drafts with your red pen, I must confess that sometimes it was hard not to take it personal against you. The fact that we published so many papers together in such a short time period is evidence of the productive friendship. Thanks for the brilliant arguments and discussions both in the ofÞ ce as during the many braais. I am proud to have offered you the African hospitality when I did.
Dr. Anneke Hesseling; dear Anneke, although we did not write papers together, I am grateful for the many corrections of my manuscripts and for our brainstorming (and gossips).

138
Infection with M. tuberculosis and atopy in children
To all the other persons who were directly involved in my study: Schalk van Lill, Ann Toerien, Jerome Cornelius, Kathy Lawrence, Sterna Brand, Karen Truter, Wena Moe-lich, Jan Mouton, Edwin Videler, Mr. Abrahams (Mr. A) and Richard Leen (the Axeman). Thanks for the priority given to my time constraint.
I cannot thank the Lung Health Study team enough for helping produce the details which facilitated the realization of the ideas that formed the foundation of this thesis: Professors Eric Bateman, Elvis Irusen, Don Enarson and Neil White (posthumous); Drs. Carl Lombard, Anamika Jithoo, Emmerentia van Schalkwyk and David Carmen) and the Desmond Tutu TB Research Centre team, for accommodating me: Annie Bakker, Dani-ta Bester, Elsabe Botha, Mari De Klerk, Dalene Gallant, Lameze Hercules, Magdalene Kennedy, Emma Murray, Cathy Marsch, Charize Pedro, Faeeza Salker, Priscilla Samaai, Ronell Taylor, Mirna Van Aardt, Susan van Zyl and Rhenda Venter). I am most privileged to have crossed your paths. I am indebted to Suzanne Verver and Saskia Den Boon of the KNCV, The Netherlands for the epidemiological comments and the correction of some manuscripts.
Ik ben dank schuldig aan Kors van der Ent en Tom Wolfs voor de aanbeveling voor de sponsoring.
Dear Angela, Augusta, Chidi, Martina, Chioma, Ugo, Chisa and Oluchi, thanks for be-ing there. With you I will never lack new challenges.
To Nma and Npa, am grateful for your love and guidance from the start, and for letting me dream freely.
Lieve Nikem and Ndidi, jullie geduld en begrip in de afgelopen 3 jaar, waarin ik vaak �krom achter de computer� moest zitten, heeft mij bewust gemaakt dat er veel is om nog in te halen. Ik hoop dat de ervaringen in de afgelopen jaren jullie iets van de wereld buiten de eigen grenzen heeft geleerd, en vooral dat wat aanvankelijk onbekend en beangstigend was ook heel vertrouwd en veilig kan worden.
En tot slot, Dorian, mijn liefste. Vanaf het eerste moment in Italië werd het duidelijk dat wij niet de makkelijkste wegen kiezen. Aan uitdagingen hebben wij nooit gebrek ge-had. Had je ooit dit van onze vakantieliefde kunnen verwachten? Zonder jou was dit nooit geworden.

� Your tide blossomedLike a seasonal riverThrough the rainy seasonHonest, light and greenFruitful and completedYour place of restSafe beside your fatherIn the dry season�
C.O
To the memory of V.C.O, who could not be here to witness the realisation of his dream

Rise, riseMy sisterRise ye, upRise up and ß yRelax your jointsLoosen your beautiful limbsOpen your sweet vocal cordsSway yourself in ecstasyLike a butterß y caught in whirlwindSpin yourself highHigher and higherFar above the gravityAnd the forces of povertyCatapult yourselfOut of the gripOf your oppressors
C.O
Dedicated to the children and women of Africa

141
Curriculum Vitae
Charles Chukwuma Obihara was born on the 12th of February 1965 in Owerri, Nige-ria. After secondary education, he left in April 1983 to Italy for further studies. After one month of studying the Italian language (�Universita Per Stranieri� Perugia), he registered for Industrial Chemistry (Instituto Biochimico Industriale Statale �Aldo Gastaldi� in Gen-ua) from where he graduated in May 1986. From September 1986 to April 1990 he studied medicine at the University of Genua Italy, after which he moved to the Netherlands be-cause of his Dutch partner, whom he met in Perugia. Through intensive self study he passed the NT2 Dutch language exam four months later. In September 1990 he was admitted to the second year of the study of Medicine at the University of Utrecht from which he passed the medical theory examinations (doctoraal diploma) in 1993 and the medical examination (artsexamen) in 1995. He was registered as a physician in September 1995.
From October 1995 to December 1995 he worked as a surgical resident in the Depart-ment of Thoracic Surgery �De Wezenlanden� Hospital, Zwolle and from January to Decem-ber 1996 as a resident in the Department of Pediatrics, St. Antonius Hospital, Nieuwegein (trainer: Dr. J.A.A.M van Diemen-Steenvoorde). From January 1997 to January 2002 he was a pediatric resident-in-training at the Wilhelmina Children�s Hospital, Utrecht (train-ers: Prof. Dr. A. Okken and Prof. Dr. J.L.L. Kimpen). In this period he also trained for 2 years at Catharina Hospital Eindhoven (trainer: Dr. J.J. Waelkens). During his pediatric training, he also obtained a certiÞ cate in Tropical Pediatrics from the University of Am-sterdam Medical Centre (AMC) and the Liverpool School of Tropical Medicine (trainer: Prof Dr. B. Brabian). He was registered as a pediatrician in January 2001, with the Roy-al Netherlands Medical Association (KNMG). From March 2002 to November 2004 he lived in Cape Town, South Africa, together with his wife and children, where he worked as a pediatric research-fellow at the Stellenbosch University (supervisor: Prof. Dr. Nulda Beyers).
The author participated in several scientiÞ c activities while a student and as a pediatric resident which led to different scientiÞ c reports. Among these are: �Post-operative prog-nosis of meconium peritonitis in children� (supervisor: Prof. Dr. N.M.A. Bax, pediatric surgeon), Reß ex Sympathic Dystrophy in Children (supervisors: Dr. A. Felius, pediatri-cian and Prof. Dr. W. Kuis, pediatric immunologist), and Lyme Borreliosis in the Region of Utrecht (supervisors: Prof. Dr. J.A.M.M. van Diemen-Steenvoorde, pediatrician en Dr. B.M. De Jongh, microbiologist, St. Anthonius Hospital, Nieuwegein). These activities led to 2 publications in medical journals.
The author was involved, both as a medical student and a paediatric resident, in differ-ent extra-curricula activities. He was a member of the medical students� union (MSFU-SAMS). During the pediatric training he coordinated an academic cooperative activity between the departments of pediatrics of Wilhelmina Children�s Hospital Utrecht, the Uni-

142
Infection with M. tuberculosis and atopy in children
versity of Harare, Zimbabwe and the Stellenbosch University, South Africa (supervisor: Prof. Dr. T.W.J. Schulpen). He also wrote papers on different actual health-care issues for migrant newspapers and journals in the Netherlands.
In June 2001, the author founded, together with his wife, the IBEM Foundation, a non-proÞ t organization with the scope of improving the standard of life of children and their families in his home village in Nigeria, through the stimulation and improvement of the quality of education in the area and awarding of scholarships based on merit.
The author is presently employed as pediatrician-fellow Pediatric Infectious Diseases with the Wilhelmina Children�s Hospital/University Medical Center, Utrecht.
He is happily married to the woman for whom he moved to the Netherlands and has 2 children.
143
List of publications
Respiratory atopic disease, Ascaris-IgE and tuberculin test in urban South African children.CC Obihara, N Beyers, RP Gie, MO Hoekstra, JE Fincham, BJ Marais, CJ Lombard, LA
Dini, JLL Kimpen.Clinical and Experimental Allergy 2006; in pressMycobacterium tuberculosis infection may protect against allergy in a tuberculosis
endemic area. CC Obihara, JLL Kimpen, RP Gie, SW van Lill, MO Hoekstra, BJ Marais,
HS Schaaf, K Lawrence, PC Potter, ED Bateman, CJ Lombard, N Beyers. Clinical and Experimental Allergy 2006; 36: 70-76.Inverse association between Mycobacterium tuberculosis infection and atopic rhinitis in
children CC Obihara, N Beyers, RP Gie, PC Potter, BJ Marais, CJ Lombard, DA Enarson,
JLL Kimpen. Allergy 2005; 60: 1121-1125 The association of prolonged breastfeeding and allergic disease in poor urban children. CC Obihara, BJ Marais, RP Gie, PC Potter, CJ Lombard, N Beyers, JLL Kimpen. European Respiratory Journal 2005; 25:970-977 The burden of childhood tuberculosis: a public health perspective BJ Marais, CC Obihara, RM Warren, HS Schaaf, RP Gie, PR Donald International Journal of Tuberculosis and Lung Disease 2005; 9(12):1305�1313.The prevalence of symptoms associated with pulmonary tuberculosis in randomly
selected children from a high burden community. BJ Marais, CC Obihara, RP Gie, HS Schaaf, AC Hesseling, C Lombard, D Enarson,
E Bateman, N Beyers. Archives of Disease in Childhood 2005; 90: 1166-1170.Well-deÞ ned symptoms are of value in the diagnosis of childhood pulmonary
tuberculosis. BJ Marais, RP Gie, CC Obihara, AC Hesseling, HS Schaaf, N Beyers. Archives of Disease in Childhood 2005; 90: 1162-1165.Paradoxical helminthiasis and giardiasis in Cape Town, South Africa: epidemiology and
control. VJ Adams, MB Markus, JF Adams, E Jordaan, B Curtis, MA Dhansay, CC Obihara,
JE Fincham. African Health Science. 2005; 5: 131-136.

144
Infection with M. tuberculosis and atopy in children
The clinical epidemiology of childhood pulmonary tuberculosis: a critical review of literature from the pre-chemotherapy era.
BJ Marais, RP Gie, HS Schaaf, AC Hesseling, CC Obihara, DA Enarson, PR Donald, N Beyers.
International Journal of Tuberculosis and Lung Disease 2004; 8: 278-285. The natural history of childhood intra-thoracic tuberculosis: a critical review of literature
from the pre-chemotherapy literature. BJ Marais, RP Gie, HS Schaaf, AC Hesseling, CC Obihara, JJ Starke, DA Enarson,
PR Donald, N Beyers. International Journal of Tuberculosis and Lung Disease 2004; 8: 392-402. The prevalence of tuberculosis in a high incidence area in the Western Cape, South
Africa. N Beyers, M Borgdorff, A Jithoo, K Lawrence, R Gie, N White, E Irusen,
CC Obihara, S van Lill, I Toms, ED Bateman, D Enarson. South African Respiratory Journal 2003; 9:123.Pulmonary sequelae after accidental aspiration; the importance of the patient�s history. CC Obihara, CK van der Ent. Pediatric Clinic Amsterdam 2001; 12 (3): 1-2.Missed infections in immigrant children. CC Obihara, C Blok, TW Schulpen, K de Meer. Nederlands Tijdschrift voor Geneeskunde 1999; 143:1545-1549. Borrelia lymphocytoma �winter ears� in children. CC Obihara, DB de Geer, JA van Diemen-Steenvoorde, BM de Jongh. Nederlands Tijdschrift voor Geneeskunde 1997; 141: 482-484.
Related Documents











