Introduction to Tuberculosis VDH TB Control and Prevention Program 2011

Introduction to Tuberculosis VDH TB Control and Prevention Program 2011.
Dec 22, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Introduction to Tuberculosis
VDH TB Control and Prevention Program2011
VDH TB Prevention and Control Policies and Procedures
Based on USPHS/CDC, ATS, IDSA and Pediatric “Red Book” guidelines
Adapted to address uniquely Virginia issues
The Causative Agent
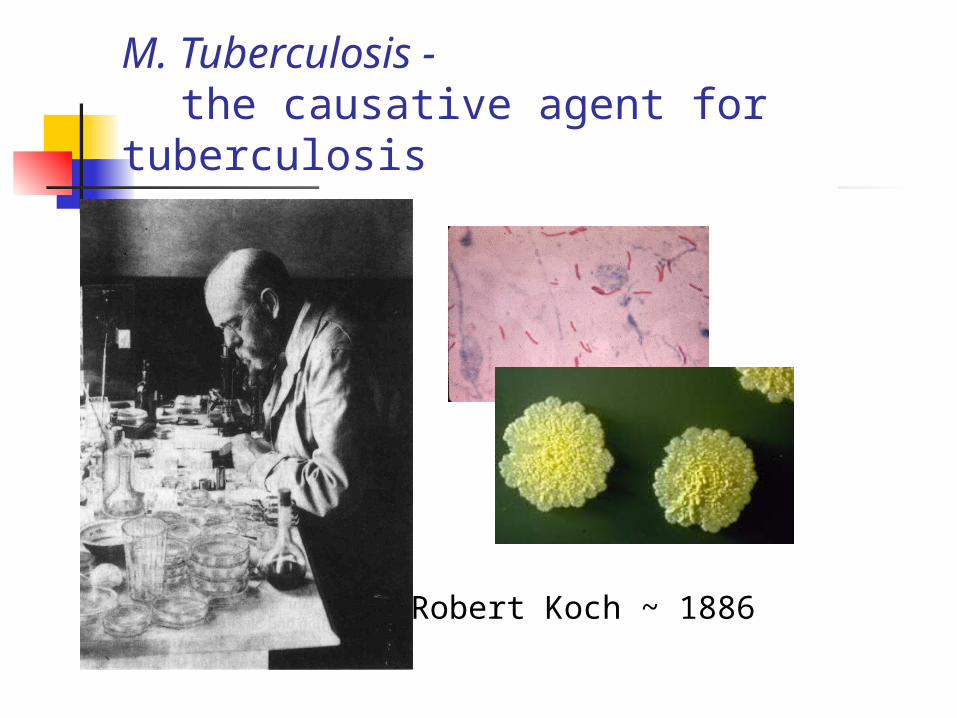
M. Tuberculosis - the causative agent for tuberculosis
Robert Koch ~ 1886
Mycobacterium tuberculosis
Bacteria A weakly gram positive rod Appears “rough and buff” in standard culture An organism that holds a red stain even in the
presence of acid, i.e. “acid fast” Slow growing
The Mycobacteria
Human pathogens M. tuberculosis complex includes:
M. tb, M. bovis, M. africanum,
M. microti, M. canetti M. leprae
NTM – non-tuberculous mycobacteria
Transmission and Pathogenesis of Tuberculosis
Transmission of TB
Spread person to person through the air
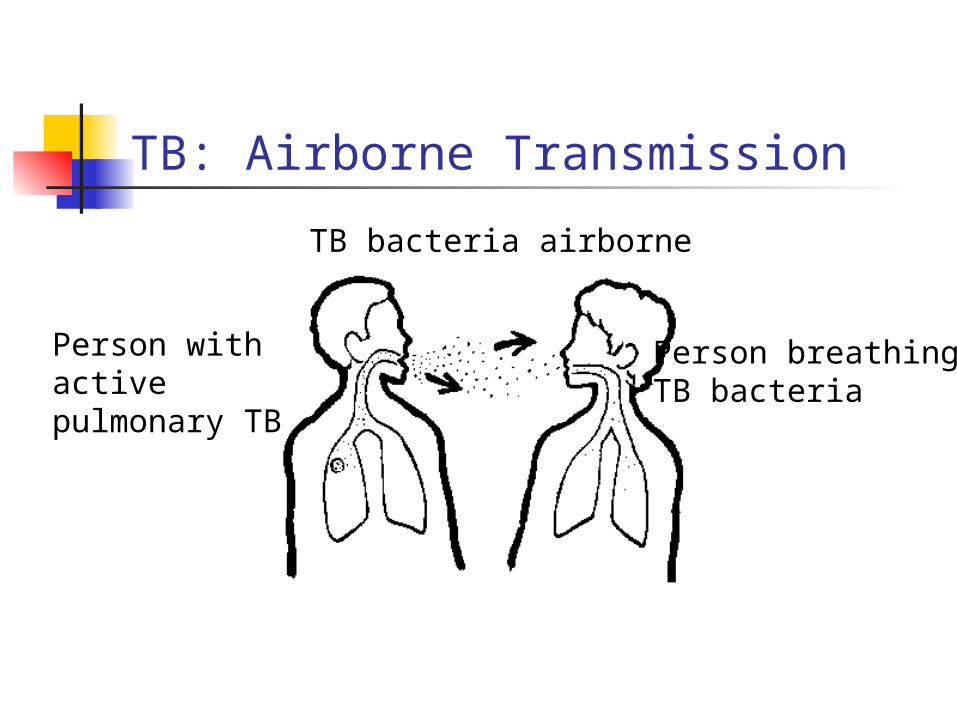
TB: Airborne Transmission
Person withactive pulmonary TB
Person breathing TB bacteria
TB bacteria airborne
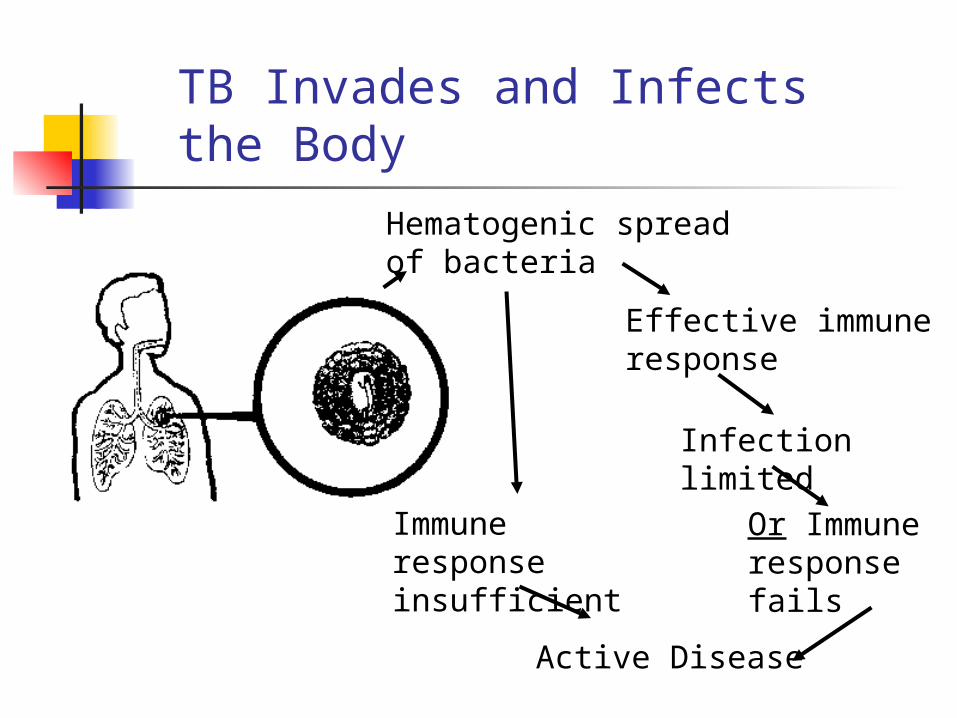
TB Invades and Infects the Body
Effective immuneresponse
Infection limited
Immune responseinsufficient
Active Disease
Hematogenic spread of bacteria
Or Immune response fails
Pathogenesis of TB
Infection begins when the inhaled droplets reach the alveoli of lungs
Tubercle bacilli multiply A number of tubercle bacilli enter the bloodstream
and spread throughout the body (lungs, kidneys, brain, bone)
Within 2-10 weeks, the immune system produces an immune response which encapsulates the bacteria, and is detectable with a TST or IGRA blood test
Probability of TB Transmission
Transmission dependent on three factors Infectiousness of the person with TB Host factors of the exposed person Environment in which the transmission occurs
Likelihood of Developing TB Disease
Once infected with tubercle bacilli 10% life time chance that TB disease will develop
Half the risk within the first 2 years Gradually decreasing risk after the first 2 years
90% chance of never developing the disease Other personal health factors can influence risk
HIV infection - single highest risk for progress to active disease, at 10% risk annually
Diabetes – 30% risk over lifetime
Sites of TB Disease
Pulmonary TB (TB of the lungs) – 80-85% of TB cases Potential for transmission – infectious until proven otherwise
Extra-pulmonary TB (outside the lungs) Can occur anywhere in body Typical sites include larynx, lymph nodes, the pleura, brain,
kidneys, bones, or joints Usually not infectious – always rule out pulmonary! Laryngeal TB is extremely contagious - hoarseness
Diagnosis of TB Disease
SymptomsTST or IGRA
CXRBacteriology
Diagnosis of TB Disease: Symptoms
Pulmonary symptoms Cough Pain in the chest
when breathing or coughing
Coughing up sputum or blood
Systemic symptoms Fatigue / malaise Decreased appetite Weight loss Fever Night sweats Other symptoms
specific to the site of the TB disease
Evaluation for TB Disease
Medical History Symptoms of TB Exposure to TB, Hx previous TB infection, or Hx TB disease Risk factors for progression to TB disease
TB skin test or IGRA Chest x-ray or CT Bacteriologic Examination of sputa, including:
Smears (+AFB) MTD or PCR “direct test (RNA based) Culture results “DNA probes” or traditional culture
Diagnosis of TB Disease
Evaluate all patients with symptoms of TB for
TB disease, regardless of the patient’s skin test reaction
1/4 to 1/3 of all active MTB cases have negative
TST at onset of treatment
Diagnosis of TB Disease: Chest X-Ray
Check for lung abnormalities suggestive of TB disease
Typical findings may include cavities, infiltrates, effusions, opacities
A chest x-ray does not confirm TB disease A chest x-ray does not rule out active TB in
immune compromised individuals and children
Diagnosis of TB Disease:Bacteriologic Examinations
Sputum collection – those symptomatic or with abnormal chest x-rays consistent with TB, for AFB smear and culture: A series of three samples Spontaneous or induced At least 8 hrs. apart, and one in early AM
All specimens should be cultured, regardless of smear result Smear/stain results in 1 day, culture results take up to 6-8 weeks M.tb can be cultured from any body fluid or tissue Specimen collected depends on the site of potential disease
Direct Tests for TB
MTD – Mycobacterium tuberculosis direct or TB PCR These rapid tests are done directly on raw respiratory
samples; culture growth is not needed Very sensitive on samples with higher smear positivity A negative test does not rule out TB, especially with negative
smear results Does not provide enough evidence to release from isolation
Antituberculosis Drugs Currently in Use in the US
First-line Drugs Isoniazid* Rifampin* Ethambutol* Pyrazinamide* Rifapentine Rifabutin
Second-line Drugs Cycloserine Ethionamide Levofloxacin Moxifloxacin Gatifloxacin P-Aminosalicylic acid Streptomycin Amikacin/kanamycin Capreomycin Linezolid
TB is usually treated for 6 to 9 months.Drug resistant cases can take years to treat.
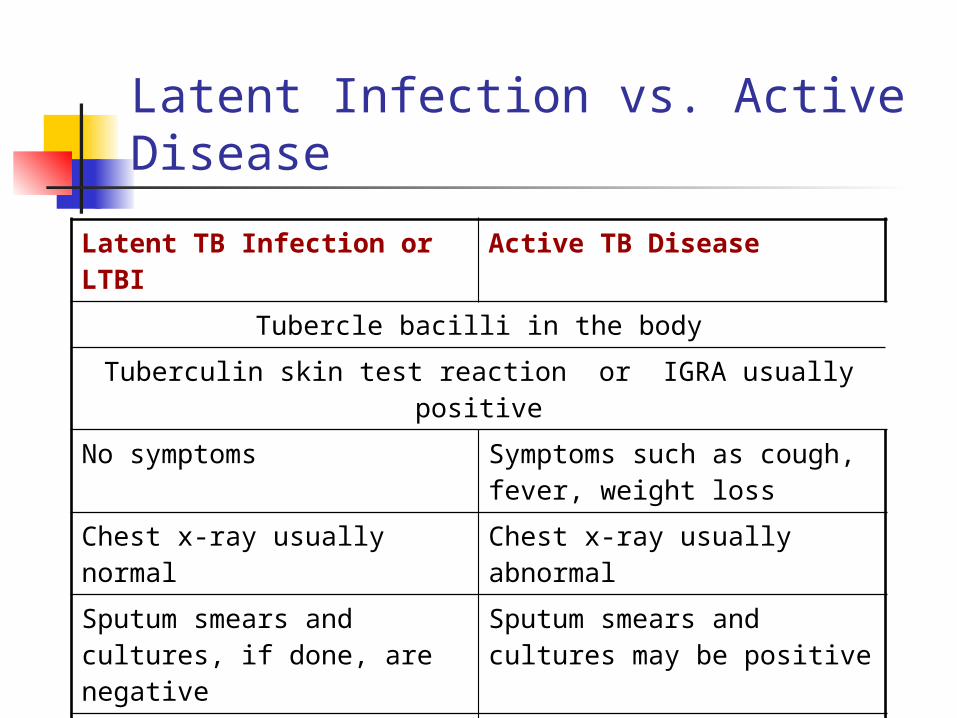
Latent Infection vs. Active Disease
Latent TB Infection or LTBI Active TB Disease
Tubercle bacilli in the body
Tuberculin skin test reaction or IGRA usually positive
No symptoms Symptoms such as cough, fever, weight loss
Chest x-ray usually normal Chest x-ray usually abnormal
Sputum smears and cultures, if done, are negative
Sputum smears and cultures may be positive
Not infectious Often infectious before treatment
Not a case of TB, but risk for future disease
A current case of TB
LTBI Treatment Regimens
Targeted Tuberculin Testing and Treatment of Latent Tuberculosis Infection
As tuberculosis (TB) disease rates in the United States (U.S.) decrease, finding and treating persons at high risk for latent TB infection (LTBI) has become a priority.
Before Initiating Treatment
Rule out TB disease (i.e., wait for culture result if specimen obtained)
Determine prior history of treatment for LTBI or TB disease
Assess risks and benefits of treatment Determine current and previous drug therapy
Isoniazid Regimens 9-month regimen of isoniazid (INH) is the
preferred regimen (270 doses) 6-month regimen is less effective but may be
used if unable to complete 9 months May be given daily or intermittently (twice
weekly) Use directly observed therapy (DOT) for
intermittent regimen
Rifampin Regimens (1)
Rifampin (RIF) given daily for 4 months is an acceptable alternative when treatment with INH is not feasible.
In situations where RIF cannot be used (e.g., HIV-infected persons receiving protease inhibitors), rifabutin may be substituted.
Rifampin Regimens
RIF daily for 4 months (120 doses within 6 months)
RIF and PZA for 2 months should generally not be offered due to risk of severe adverse events
MMWR August 8, 2003; 52 (31): 735-739
Completion of Therapy
Completion of therapy is based on the total number of doses administered, not on duration alone.
Tuberculosis Control and Prevention – it takes a Team!
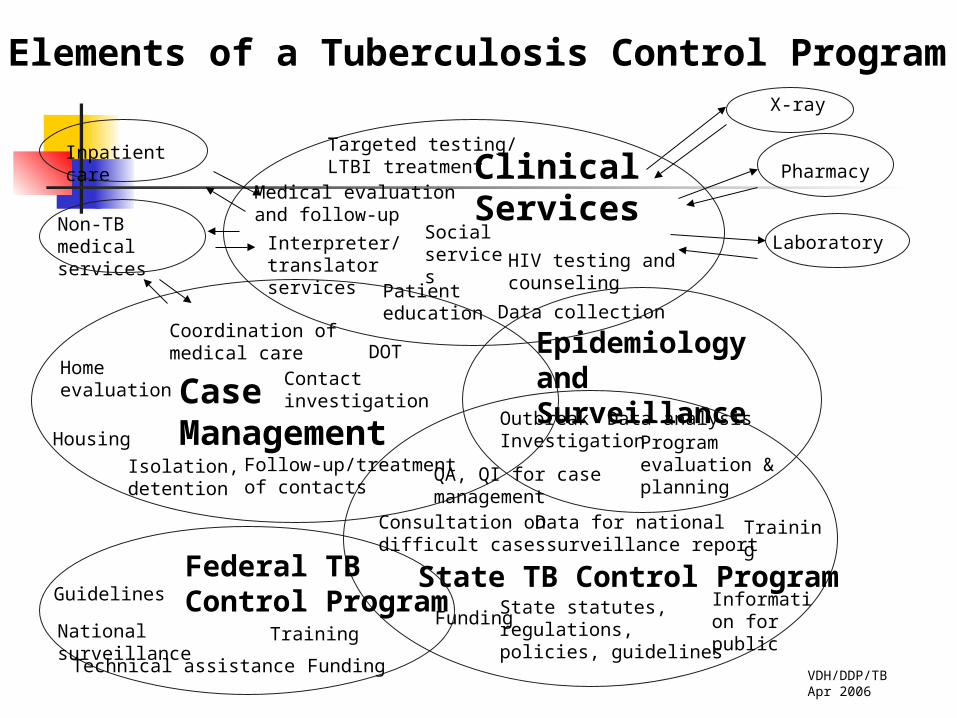
Elements of a Tuberculosis Control Program
Clinical Services
CaseManagement
Data analysis
Inpatient care
Medical evaluation and follow-up
X-ray
Laboratory
Pharmacy
Social services
Interpreter/translatorservices
Home evaluation
Housing
Isolation,detention
Contact investigation
Coordination of medical care DOT
Programevaluation &planning
VDH/DDP/TBApr 2006
Epidemiology and Surveillance
HIV testing andcounseling
State TB Control ProgramFederal TB Control ProgramGuidelines
Training
Funding
National surveillance
Non-TB medicalservices
Data collection
State statutes,regulations,policies, guidelines
Consultation on difficult cases
Outbreak Investigation
Training
FundingInformation for public
Technical assistance
QA, QI for case management
Data for national surveillance report
Follow-up/treatment of contacts
Patienteducation
Targeted testing/LTBI treatment
What is Reportable According to VA Regulation?
By medical provider or designee Confirmed or suspected TB disease Positive TST in children under age 4 years
By directors of medical laboratories Positive AFB smears or cultures
The Public Health Nurse – TB Case Management
Education Assure treatment according to national standards Contact investigation Assure treatment adherence and adequate therapy
DOT as international program standard Identify adverse drug reactions Monitor clinical improvement Recognize patient behaviors Develop strategies to problem-solve
Teamwork!!
Tuberculosis is suspected, diagnosed, and treated as a team.
Treatment of LTBI prevents future TB disease It takes all of us to get the job done! Know your local TB health department staff and ask
questions! Only with knowledgeable and trained personnel can
tuberculosis be quickly identified and completely managed.
Related Documents