Fructose Malabsorption ............................................................................................................................. 3 Introduction.............................................................................................................................................. 3 Metabolism .............................................................................................................................................. 4 Fructose Malabsorption ......................................................................................................................... 5 Diagnosis ................................................................................................................................................. 6 Diet ........................................................................................................................................................... 7 Fructose Malabsorption: A Possible Factor in Functional Bowel Disorders........................... 7 Functional Bowel Disorders .............................................................................................................. 8 Fructose Malabsorption ..................................................................................................................... 8 ................................................................................................................................................................ 10 Pathophysiology of Fructose Malabsorption ............................................................................. 10 Assessment of Dietary Fructose Intake ....................................................................................... 10 Fructose Malabsorption in IBS ....................................................................................................... 11 Fructose-Restricted Diet .................................................................................................................. 11

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Fructose Malabsorption ............................................................................................................................. 3
Introduction .............................................................................................................................................. 3
Metabolism .............................................................................................................................................. 4
Fructose Malabsorption ......................................................................................................................... 5
Diagnosis ................................................................................................................................................. 6
Diet ........................................................................................................................................................... 7
Fructose Malabsorption: A Possible Factor in Functional Bowel Disorders ........................... 7
Functional Bowel Disorders .............................................................................................................. 8
Fructose Malabsorption ..................................................................................................................... 8
................................................................................................................................................................ 10
Pathophysiology of Fructose Malabsorption ............................................................................. 10
Assessment of Dietary Fructose Intake ....................................................................................... 10
Fructose Malabsorption in IBS ....................................................................................................... 11
Fructose-Restricted Diet .................................................................................................................. 11

Role of the Pharmacist ..................................................................................................................... 11
REFERENCES ..................................................................................................................................... 12
Fructose malabsorption .......................................................................................................................... 14
Pathophysiology ................................................................................................................................... 14
Symptoms .............................................................................................................................................. 15
Diagnosis ............................................................................................................................................... 15
Treatment .............................................................................................................................................. 15
Xylose isomerase ............................................................................................................................. 15
Diet ..................................................................................................................................................... 15
Dietary guidelines for the management of fructose malabsorption[edit].................................. 17
Food-labeling ........................................................................................................................................ 17
New research ......................................................................................................................................... 18
See also .................................................................................................................................................. 18
References ............................................................................................................................................. 18
Use and abuse of hydrogen breath tests .............................................................................................. 19
Abstract .................................................................................................................................................. 19
Hydrogen breath tests ......................................................................................................................... 20
Carbohydrate malabsorption .............................................................................................................. 21
Carbohydrate digestion and absorption ........................................................................................ 21
Lactose malabsorption .................................................................................................................... 21
Fructose malabsorption ................................................................................................................... 23
Small intestinal bacterial overgrowth ................................................................................................. 24
Normal bowel flora ........................................................................................................................... 25
Definition of SIBO ............................................................................................................................. 25
Tests for SIBO .................................................................................................................................. 26
Is there a link between SIBO and IBS? ........................................................................................ 28
Conclusion ............................................................................................................................................. 29
Abbreviations ........................................................................................................................................ 29
Footnotes ............................................................................................................................................... 29
References ............................................................................................................................................ 29
FOFMAPs to the rescue…………………..38

Fructose Malabsorption Fructose malabsorption is a digestive disorder in which the absorption capacity of the sugar fructose
in the small intestine is reduced. This leads to an increase of fructose in the large intestine where the
sugar is degraded by intestinal bacteria to several chemical compounds which will then cause
symptoms like bloating, wind, abdominal pain, diarrhea and/or constipation.
Introduction
The natural occurrence of fructose as a monosaccharide (molecular fructose) is mainly in fruits and
vegetables. It is also a component of the disaccharide sucrose, the table sugar, which is composed
of one molecule glucose and one molecule fructose. Molecular fructose is sweeter than glucose and
is therefore often used as sweetener in pastries, sweets and sodas. The average daily intake of
fructose has increased dramatically over the last 40 years mainly due to the increased usage of this
High Fructose Corn Syrup (HFCS) as a sweetener.
Fig. 1:Sucrose (Disaccharid)
Fig. 2:Molecular Fructose (Monosaccharid)
Fructose is absorbed in the small intestine via the GLUT-5 transporter. This transport from the
intestinal lumen into the enterocytes, the intestinal absorptive cells, is passive and driven by the
concentration difference of fructose between the intestinal lumen and the plasma of the cells. The
capacity of this transport system is limited and varies greatly between individuals. About 40% of the
population show signs of malabsorption after a single dose of 25g of fructose, a dosis far below the
average daily intake which is estimated to be around 70g per day. Sorbitol, a sugar alcohol which is

widely used as sugar substitute in industrial foods, further reduces the fructose absorption capacity
by binding to the GLUT-5 transporter.
Concomitant consumption of glucose with a fructose-rich meal can increase the absorption capacity
of fructose which is why most of patients suffering from fructose malabsorption tolerate table sugar
quite well. It is believed that this effect may be due to an increased integration of the GLUT-2
transporter into the membrane of the enterocytes. GLUT-2 acts as a passive transporter for glucose,
galactose and fructose with low affinity (that means it only transports these sugars if their
concentration is high). This transporter is only integrated into the membrane after a meal when the
sugar concentration in the intestine is high. This detection of sugar in the intestinal lumen only works
with glucose and therefore a fructose-rich meal will not trigger this integration of GLUT-2.
Metabolism
Unlike glucose fructose can only be utilized by a few cells of the body directly. Most of the absorbed
fructose is transported to the liver where it is phosphorylated and converted into fat, glucose or
energy (figure 3).
Currently there is an ongoing discussion whether fructose may induce obesity and non-alcoholic
fatty liver disease. Until now there is no hard evidence to support this thesis as most studies
investigating this effect yielded conflicting results. But considering the differences between fructose
and glucose metabolism it is a reasonable conclusion:
Fructose has no effect on insulin secretion which in turn may reduce the satiation experienced
after a meal.
Fructose is metabolized primarily in the liver putting more strain on the liver cells. Furthermore
the energy available in the liver cells is increased which can affect the synthesis of fat (excess
energy is stored as body fat).
There is little difference between the free fructose of high fructose corn syrup and the bound fructose
in table sugar. Both have very similar effects on the body. This does not mean that the fructose from
fruits is also detrimental. In the western civilizations only a small portion of the average daily intake
of fructose comes from natural sources and this comparatively low amount of fructose has no
detrimental effect on health.
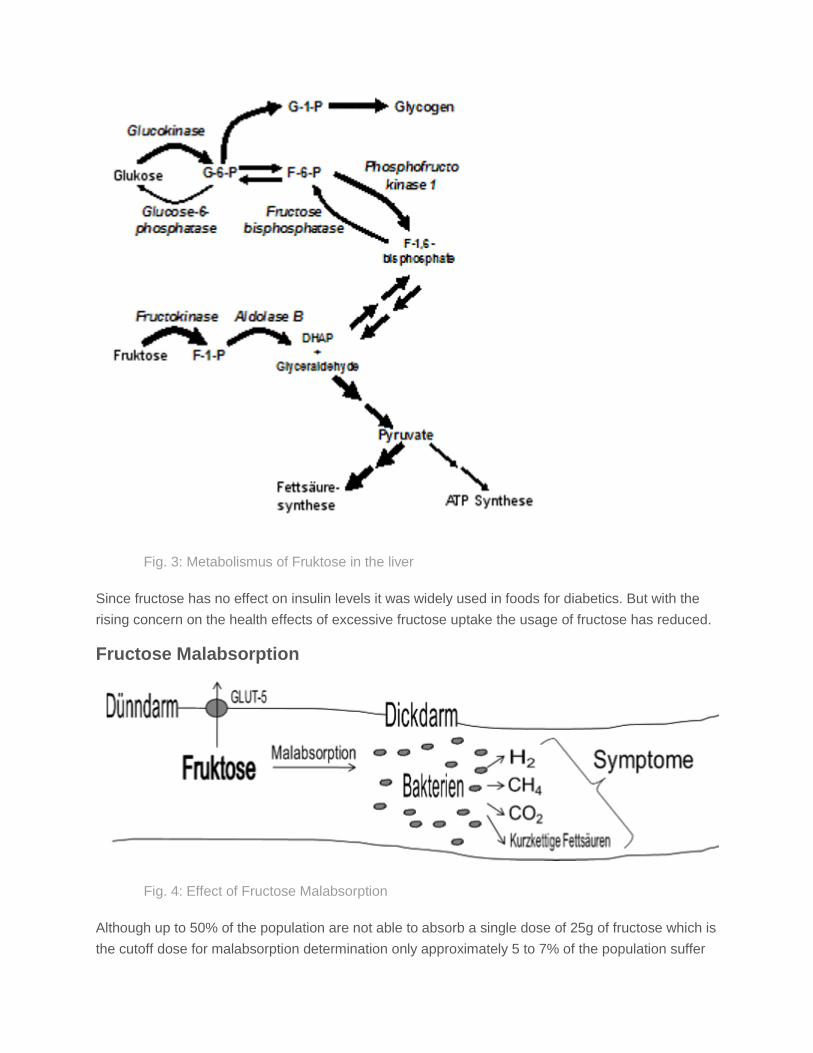
Fig. 3: Metabolismus of Fruktose in the liver
Since fructose has no effect on insulin levels it was widely used in foods for diabetics. But with the
rising concern on the health effects of excessive fructose uptake the usage of fructose has reduced.
Fructose Malabsorption
Fig. 4: Effect of Fructose Malabsorption
Although up to 50% of the population are not able to absorb a single dose of 25g of fructose which is
the cutoff dose for malabsorption determination only approximately 5 to 7% of the population suffer

from symptomatic fructose malabsorption. Only these 5 to 7% will develop symptoms after a
fructose-rich meal. The malabsorption alone cannot be seen as a disorder but occurs throughout the
population.
The symptoms are triggered by the degradation products that arise from the decomposition of the
fructose in the large intestine by the intestinal bacteria. Mainly Hydrogen (H2), Methane (CH4),
Carbon Dioxide (CO2) and short chain fatty acids (SCFAs) are generated. These compounds can
cause the typical symptoms like bloating, wind, abdominal pain, diarrhea and/or constipation. Since
the composition of the intestinal bacterial population varies between humans also the amount and
composition of the generated degradation products varies. Furthermore the tolerance of the intestine
to negative influences is affected by several parameters like stress, inflammation and others. Both
these factors influence the severity of the symptoms the patient with fructose malabsorption will
experience after a fructose rich meal.
There is also no guideline that can tell which amount of fructose is needed to invoke symptoms. The
absorption capacity of patients suffering from fructose malabsorption is reduced but still significant. If
the ingested amount of fructose is below this absorption capacity no symptoms should be generated.
The factors influencing this absorption capacity are not well understood. For example inflammation
of the small intestine will decrease the amount of absorbed fructose. But until now no reason for the
innate difference of the absorption capacity for fructose between the individuals could be found.
Additionally it is of great importance how the fructose is ingested. Free fructose is taken up
differently than sucrose.
Fructose malabsorption must not be confused with the hereditary fructose intolerance, a disease
caused by a rare genetic defect of the liver enzyme Aldolase B. In this disease the body can no
longer process dietary fructose which causes symptoms like hypoglycemia and vomiting after a
fructose containing meal. Repeated exposure to fructose will lead to hepatomegalia and liver failure.
The prevalence of this potentially fatal disease is approximately 1 in 25000 in Western Europe.
Diagnosis
Medical tests require a hydrogen breath test with fructose. During this test the patient is
administered a single dose of 25g of fructose in 100ml water on an empty stomach. Then over the
course of 3 hours the amount of hydrogen in the exhaled air is measured. If the fructose is not
absorbed completely it will be degraded by the bacteria in the large intestine into hydrogen which
travels through the blood stream to the lungs where it is exhaled. The test is considered positive if
the concentration of hydrogen in the exhaled breath rises to 20ppm.
About 10% of the population have no hydrogen producing bacteria in their intestine. For these
patients the test can be done by measuring the methane in the exhaled air.
The best indication for a symptomatic fructose malabsorption is the disappearance of digestional

problems during an exclusion diet. A fructose malabsorption can be assumed if after 4 weeks
without dietary fructose the symptoms have disappeared.
Diet
The first step is a 4 week long strictly fructose-free diet. This should help to bring the digestion
system into balance again. After this period increasing amounts of fructose can be introduced into
the diet. Every patient should test how much fructose he/she can tolerate without suffering from
symptoms. It is recommendable to eat as much fructose as tolerated if the source is natural because
the absorption capacity for fructose can decline if the GLUT-5 transporter is not used (no fructose is
ingested).
Generally foods with high fructose corn syrup (HFCS) or table sugar should be avoided when
dealing with fructose malabsorption. [Link]Here[/Link] is a list of foods and their fructose, glucose,
sucrose and sorbitol contents. As a rule of thumb foods with a balanced amount of fructose and
glucose are generally well tolerated. This may not be true for all patients suffering from fructose
malabsorption because some even develop symptoms from small amounts of table sugar which is
chemically an equimolar mixture of glucose and fructose. Sorbitol should be avoided as it
temporarily reduces the absorption capacity of fructose.
For the composition of a detailed diet sheet a nutritionist should be consulted. Very often dietary
supplements are needed to ensure an optimal supply of the patient with vitamins and trace
elements.
Fructose Malabsorption: A Possible Factor in Functional Bowel Disorders
Sheri Helms, PharmD Director of Professional Program Laboratories Purdue University College of Pharmacy West Lafayette, Indiana
Fang Z. Ni, PharmD
Rutgers Pharmaceutical Industry Fellow Rutgers University New Brunswick, New Jersey
Patricia L. Darbishire, PharmD Clinical Associate Professor of Pharmacy Practice Director of Introductory Pharmacy Practice Experience Purdue University College of Pharmacy West Lafayette, Indiana

12/20/2011 US Pharm. 2011;36(12):41-44.
Functional bowel disorders (FBDs) are gastrointestinal (GI) disorders related to the middle or lower GI tract that lack identifiable pathoetiology.
1,2 FBDs include irritable bowel syndrome (IBS); recurrent abdominal pain (RAP); chronic
bloating, constipation, and/or diarrhea; and other unspecified chronic bowel disorders.1 Hadler et al reported FBDs in
up to 40% of the community.3 In 2004, it was estimated that 4 out of every 100 emergency department visits were
due to FBDs, accounting for more than 11 million visits.2 In a study of 3,933 subjects, 18% reported chronic diarrhea,
16% chronic constipation, 15% abdominal pain, 10% symptoms of IBS, and 2% dyspepsia. The economic burden is estimated to be as high as $1.6 billion for IBS and $621 million for chronic diarrhea.
4
Functional Bowel Disorders
Irritable Bowel Syndrome: Despite the research dedicated to IBS, there is little known about its cause or development process. The most recent comprehensive prevalence study, conducted in 2002, found that IBS occurred in 3% to 20% of North Americans.
5 IBS is a similar issue globally in both developed and developing countries.
6 Chang
et al estimated that in 1 year, IBS accounted for 500,000 inpatient hospital stays.7 Women reported an incidence of
2:1 compared to men.5 Triggers for IBS include stress, hormonal fluctuations, and certain foods, including chocolate,
alcohol, carbonated beverages, fruits, and vegetables.5,8
Diagnosis is predominantly based on symptoms, defined as abdominal pain and altered bowel activity with no organic origin.
5
IBS affects the large intestine, causing cramping, abdominal pain, bloating, gas, diarrhea, and constipation. It is classified into several subtypes: diarrhea (IBS-D), constipation (IBS-C), and a mixed subtype (IBS-M). Fortunately, IBS does not cause permanent damage to the colon and few people have disabling symptoms. IBS is generally managed through diet, lifestyle changes, and stress reduction techniques. When these techniques fail, symptom-based pharmacotherapy is employed. Constipation may be treated with prokinetic agents, while diarrhea may be treated with antispasmodics, opioids, 5-HT3 antagonists, and/or anticholinergics.
5
Recurrent Abdominal Pain: RAP is another major form of FBD that is common in children. It is considered pain severe enough to interfere with normal functioning at least once per month for 3 consecutive months.
9 For decades,
the pathophysiology of RAP has remained unclear. The original research and defining of RAP came from a British pediatrician, John Apley, MD. In establishing the definition of RAP, Apley and Naish surveyed 1,000 primary and secondary school children.
9 Approximately 11% of the children met the criteria for RAP. Another study conducted by
Hyams et al evaluated 507 adolescents in an American suburban area.10
Of the adolescents studied, approximately 15% experienced abdominal pain on a weekly basis. However, only half sought medical attention, implying the potential for a higher rate of occurrence than seen in clinical practice.
11 Many pediatricians treat RAP predominantly
with emotional support and reassurance for the family that no serious disease is present.12
Fructose Malabsorption
One area gaining interest with those who study FBD is fructose malabsorption, a condition characterized by gas, bloating, discomfort, nausea, disturbed bowel function, and occasionally gastroesophageal reflux (TABLE 1).
13 During fructose malabsorption, the small intestines are unable to fully absorb ingested fructose, leading to
increased osmotic load and bacterial fermentation, as well as promotion of mucosal biofilm formation.14
This is
distinguished from fructose intolerance, a hereditary disease caused by a mutation in the aldolase B gene that renders patients unable to metabolize fructose. This metabolic disease may result in hepatic and renal injury, growth retardation, and, in severe cases, even death.
15-17
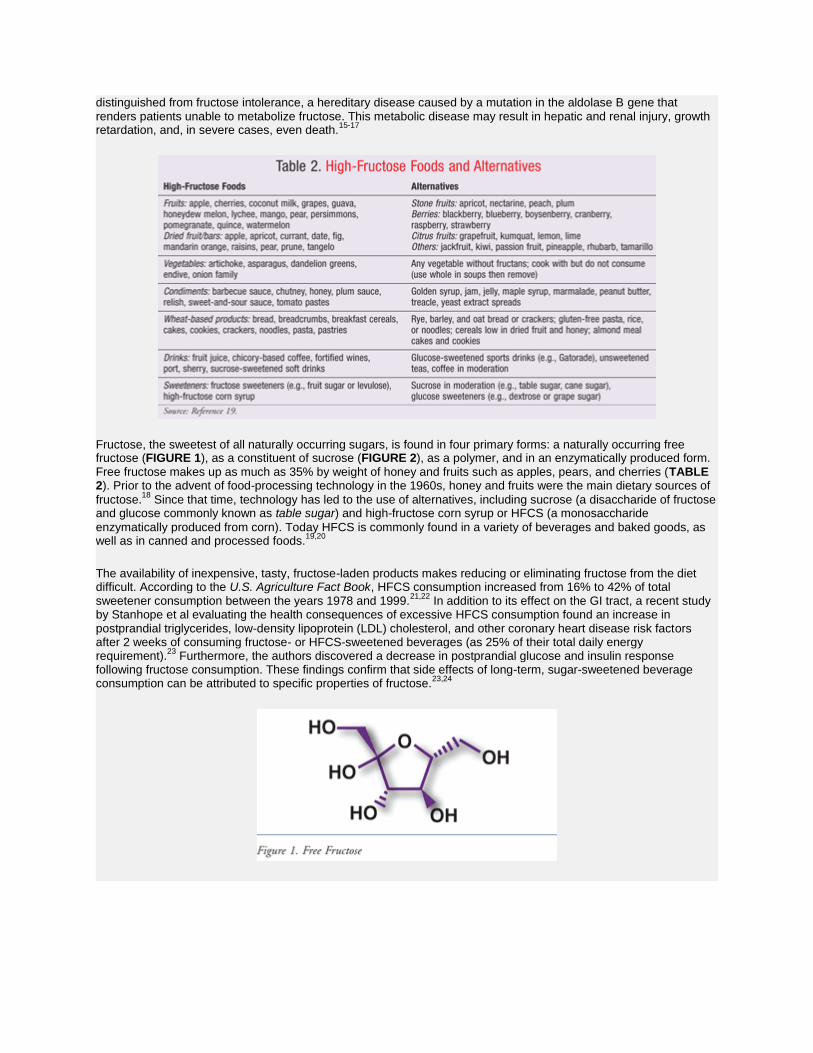
Fructose, the sweetest of all naturally occurring sugars, is found in four primary forms: a naturally occurring free fructose (FIGURE 1), as a constituent of sucrose (FIGURE 2), as a polymer, and in an enzymatically produced form. Free fructose makes up as much as 35% by weight of honey and fruits such as apples, pears, and cherries (TABLE 2). Prior to the advent of food-processing technology in the 1960s, honey and fruits were the main dietary sources of
fructose.18
Since that time, technology has led to the use of alternatives, including sucrose (a disaccharide of fructose and glucose commonly known as table sugar) and high-fructose corn syrup or HFCS (a monosaccharide
enzymatically produced from corn). Today HFCS is commonly found in a variety of beverages and baked goods, as well as in canned and processed foods.
19,20
The availability of inexpensive, tasty, fructose-laden products makes reducing or eliminating fructose from the diet difficult. According to the U.S. Agriculture Fact Book, HFCS consumption increased from 16% to 42% of total sweetener consumption between the years 1978 and 1999.
21,22 In addition to its effect on the GI tract, a recent study
by Stanhope et al evaluating the health consequences of excessive HFCS consumption found an increase in postprandial triglycerides, low-density lipoprotein (LDL) cholesterol, and other coronary heart disease risk factors after 2 weeks of consuming fructose- or HFCS-sweetened beverages (as 25% of their total daily energy requirement).
23 Furthermore, the authors discovered a decrease in postprandial glucose and insulin response
following fructose consumption. These findings confirm that side effects of long-term, sugar-sweetened beverage consumption can be attributed to specific properties of fructose.
23,24
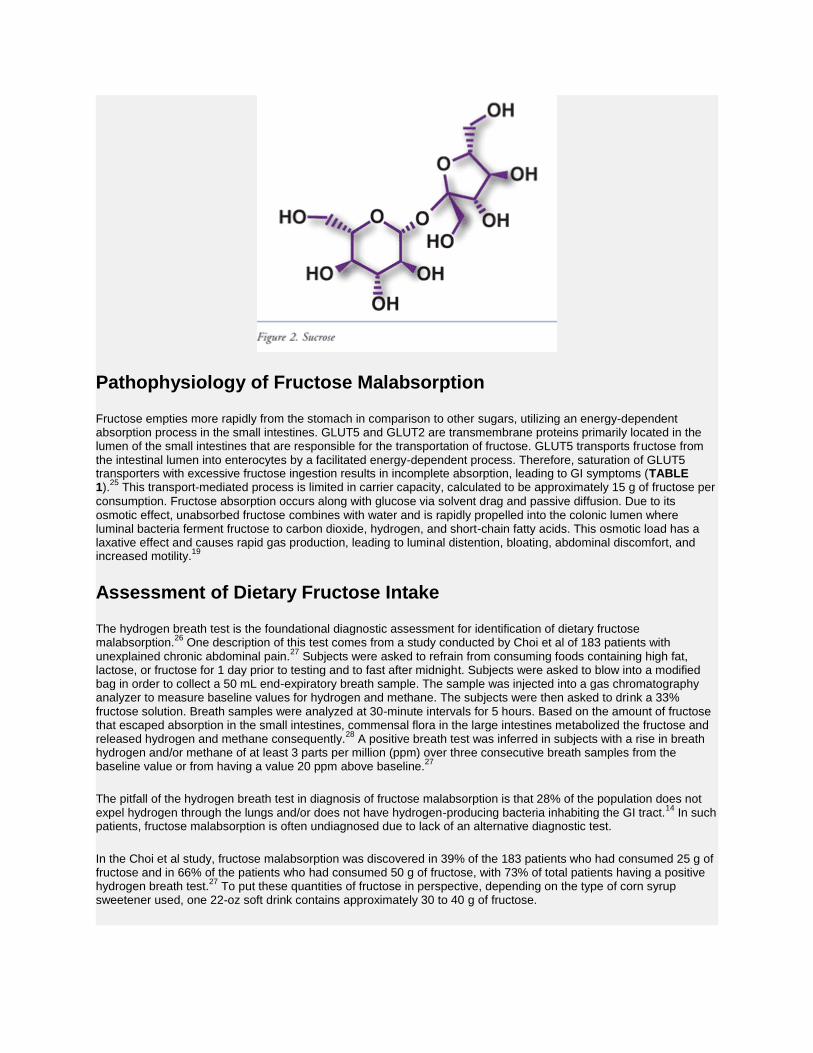
Pathophysiology of Fructose Malabsorption
Fructose empties more rapidly from the stomach in comparison to other sugars, utilizing an energy-dependent absorption process in the small intestines. GLUT5 and GLUT2 are transmembrane proteins primarily located in the lumen of the small intestines that are responsible for the transportation of fructose. GLUT5 transports fructose from the intestinal lumen into enterocytes by a facilitated energy-dependent process. Therefore, saturation of GLUT5 transporters with excessive fructose ingestion results in incomplete absorption, leading to GI symptoms (TABLE 1).
25 This transport-mediated process is limited in carrier capacity, calculated to be approximately 15 g of fructose per
consumption. Fructose absorption occurs along with glucose via solvent drag and passive diffusion. Due to its osmotic effect, unabsorbed fructose combines with water and is rapidly propelled into the colonic lumen where luminal bacteria ferment fructose to carbon dioxide, hydrogen, and short-chain fatty acids. This osmotic load has a laxative effect and causes rapid gas production, leading to luminal distention, bloating, abdominal discomfort, and increased motility.
19
Assessment of Dietary Fructose Intake
The hydrogen breath test is the foundational diagnostic assessment for identification of dietary fructose malabsorption.
26 One description of this test comes from a study conducted by Choi et al of 183 patients with
unexplained chronic abdominal pain.27
Subjects were asked to refrain from consuming foods containing high fat, lactose, or fructose for 1 day prior to testing and to fast after midnight. Subjects were asked to blow into a modified bag in order to collect a 50 mL end-expiratory breath sample. The sample was injected into a gas chromatography analyzer to measure baseline values for hydrogen and methane. The subjects were then asked to drink a 33% fructose solution. Breath samples were analyzed at 30-minute intervals for 5 hours. Based on the amount of fructose that escaped absorption in the small intestines, commensal flora in the large intestines metabolized the fructose and released hydrogen and methane consequently.
28 A positive breath test was inferred in subjects with a rise in breath
hydrogen and/or methane of at least 3 parts per million (ppm) over three consecutive breath samples from the baseline value or from having a value 20 ppm above baseline.
27
The pitfall of the hydrogen breath test in diagnosis of fructose malabsorption is that 28% of the population does not expel hydrogen through the lungs and/or does not have hydrogen-producing bacteria inhabiting the GI tract.
14 In such
patients, fructose malabsorption is often undiagnosed due to lack of an alternative diagnostic test.
In the Choi et al study, fructose malabsorption was discovered in 39% of the 183 patients who had consumed 25 g of fructose and in 66% of the patients who had consumed 50 g of fructose, with 73% of total patients having a positive hydrogen breath test.
27 To put these quantities of fructose in perspective, depending on the type of corn syrup
sweetener used, one 22-oz soft drink contains approximately 30 to 40 g of fructose.

Fructose Malabsorption in IBS
One in three adults with IBS presents with the inability to absorb fructose in 25- to 50-g increments. However, fructose malabsorption is not limited to patients with IBS. Although GI symptoms associated with fructose malabsorption are generally magnified (TABLE 1), the perception that fructose does not play a major role in patients
with IBS often leads to a lack of treatment.19
Fructose-Restricted Diet
International consensus on treatment of traditional IBS starts with increased fiber intake as first-line therapy.
29 However, there are no published guidelines to assist the patient with fructose malabsorption in constructing
a manageable diet.11
Despite the lack of specific guidelines, three separate studies demonstrated that identification and dietary monitoring of fructose consumption in patients with fructose malabsorption was clinically significant in reducing abdominal symptoms.
19,30,31 For instance, in the Choi et al study, 31 patients with positive hydrogen breath tests received verbal
and written instructions on fructose restriction or exclusion, and then were followed up to 1 year later. Fourteen of the subjects were considered compliant patients and experienced a statistically significant reduction in abdominal pain, belching, bloating, fullness, indigestion, and diarrhea symptom scores compared to baseline 1 year prior.
27
In another study, Fernandez-Banares et al found that when given recommendations to eliminate all foods with free fructose, patients showed clinical symptom improvement after just 1 month of dietary adjustment. Furthermore, a group of these patients continued to have symptomatic improvement for up to 1 year later.
32
These two studies demonstrate positive impact on clinical symptoms with dietary intervention.27,32
Lack of guidelines on fructose restriction in patients suffering from fructose malabsorption should not deter pharmacists from making such dietary recommendations.
Role of the Pharmacist
As a member of the health care team, pharmacists need to be aware of the common symptoms of fructose malabsorption, in addition to the foods that contain high amounts of fructose.
19,33 Although the normal capacity for
absorption of fructose is unknown, in general, consumption of fructose in excess of 15 to 25 g in one sitting can lead
to malabsorption and FBDs.12,19
Recommendations to substitute foods and beverages containing high amounts of fructose for those containing lower amounts (TABLE 3) can be helpful to patients suffering from fructose
malabsorption symptoms. Pharmacists should encourage patients to focus on food alternatives. Realistic goals can positively impact symptoms and improve quality of life.
27 Patients should be encouraged to consult with a registered
dietitian if they are unable to self-manage dietary needs.

REFERENCES
1. Longstreth GF, Thompson WG, Chey WD, et al. Functional bowel disorders. Gastroenterology. 2006;130:1480-
1491. 2. Porter CK, Gormley R, Tribble DR, et al. The incidence and gastrointestinal infectious risk of functional gastrointestinal disorders in a healthy US adult population. Am J Gastroenterol. 2011;106:130-138. 3. Hadler SL, Locke GR III, Chleck CD, et al. Natural history of functional gastrointestinal disorders: a 12-year longitudinal population-based study. Gastroenterology. 2007;133:799-807. 4. Lembo AJ. The clinical and economic burden of irritable bowel syndrome. Pract Gastroenterol. 2007;31(suppl)3-9. 5. Grundmann O, Yoon SL. Irritable bowel syndrome: epidemiology, diagnosis and treatment: an update for health-care practitioners. J Gastroenterol Hepatol. 2010;25:691-699. 6. Tally NJ. Functional gastrointestinal disorders as a public health problem. Neurogastroenterol Motil. 2008;20(suppl 1):121-129. 7. Chang JY, Locke GR, McNally MA, et al. Impact of functional gastrointestinal disorders on survival in the community. Am J Gastroenterol. 2010;105:822-832. 8. Chang L. The role of stress on physiologic responses and clinical symptoms in irritable bowel syndrome. Gastroenterology. 2011;140:761-765. 9. Apley J, Naish N. Recurrent abdominal pains: a field survey of 1,000 school children. Arch Dis Child. 1958;33:165-170. 10. Hyams JS, Burke G, Davis PM, et al. Abdominal pain and irritable bowel syndrome in adolescents: a community-based study. J Pediatr. 1996:129:220-226. 11. Rao SS, Attaluri A, Anderson L, Stumbo P. The ability of the normal human small intestine to absorb fructose: evaluation of breath testing. Clin Gastroenterol Hepatol. 2007;5:959-963. 12. Weydert JA, Ball TM, Davis MF. Systemic review of treatments for recurrent abdominal pain. Pediatrics. 2003;111:e1-e11. 13. Piche T, Des Varannes SB, Sacher-Huvelin S, et al. Colonic fermentation influences lower esophageal sphincter function in gastroesophageal reflux disease. Gastroenterology. 2003;124:894-902. 14. Gibson PR, Newnham E, Barrett JS, et al. Review article: fructose malabsorption and the bigger picture. Aliment Pharmacol Ther. 2007;25:349-363. 15. Wong D. Hereditary fructose intolerance. Mol Genet Metab. 2005;85:165-167. 16. Ali M, Rellos P, Cox TM. Hereditary fructose intolerance. J Med Genet. 1998;35:353-365. 17. Bouteldja N, Timson DJ. The biochemical basis of hereditary fructose intolerance. J Inherit Metab

Dis. 2010;33:105-112. 18. Hanover LM, White JS. Manufacturing, composition and applications of fructose. Am J Clin Nutr. 1993;58(suppl):724S-732S. 19. Shepherd SJ, Gibson PR. Fructose malabsorption and symptoms of irritable bowel syndrome: guidelines for effective dietary management. J Am Diet Assoc. 2006;106:1631-1639. 20. Skoog SM, Bharucha AE. Dietary fructose and gastrointestinal symptoms: a review. Am J Gastroenterol. 2004;99:2046-2050. 21. Agriculture Fact Book 2000. Washington, DC: U.S. Department of Agriculture; 2000:314.
www.usda.gov/news/pubs/ fbook00/factbook2000.pdf. Accessed September 9, 2011.
22. Marriott BP, Cole N, Lee E. National estimates of dietary fructose intake increased from 1977 to 2004 in the United States. J Nutr. 2009;139:1228S-1235S. 23. Stanhope KL, Bremer AA, Medici V, et al. Consumption of fructose and high fructose corn syrup increase postprandial triglycerides, LDL-cholesterol, and apolipoprotein-B in young men and women. J Clin Endocrinol
Metab. 2011;96:E1596-E1605. 24. Hu FB, Malik VS. Sugar-sweetened beverages and risk of obesity and type 2 diabetes: epidemiologic evidence. Physiol Behav. 2010;100:47-54. 25. Douard V, Ferraris RP. Regulation of the fructose transporter GLUT5 in health and disease. Am J Physiol Endocriol Metab. 2008;295:E227-E237. 26. Romagnuolo JM, Schiller D, Bailey RJ. Using breath tests wisely in a gastroenterological practice: an evidence based review of indications and pitfalls in interpretation. Am J Gastroenterol. 2002;97:1113-1126. 27. Choi YK, Johlin FC, Summers RW, et al. Fructose intolerance: an under-recognized problem. Am J Gastroenterol. 2003;98:1348-1353. 28. Jones HF, Butler RN, Brooks DA. Intestinal fructose transport and malabsorption in humans. Am J Physiol Gastrointest Liver Physiol. 2011;300:G202-G206. 29. DecisionBase. Irritable Bowel Syndrome: A New Therapy for Non-Constipation-Predominant IBS With Greatly Improved Efficacy Will Reach Near-Blockbuster Status. Decision Resources. Inc. March 2010.
http://decisionresources.com/ Products-and-Services/Report? r=dbaspd2510. Accessed September 9, 2011.
30. Choi YK, Kraft N, Zimmerman B, et al. Fructose intolerance in IBS and utility of fructose-restricted diet. J Clin Gastroenterol. 2008;42:233-238. 31. Johlin FC Jr, Panther M, Kraft N. Dietary fructose intolerance: diet modification can impact self-rated health and symptom control. Nutr Clin Care. 2004;7:92-97. 32. Fernandez-Banares F, Rosinach M, Esteve M, et al. Sugar malabsorption in functional abdominal bloating: a pilot study on the long-term effect of dietary treatment. Clin Nutr. 2006;25:824-831.
33. Nutrition Data Laboratory. USDA. www.nal.usda.gov/fnic/ foodcomp/search/. Accessed September 9, 2011
Fructose malabsorption
Fructose malabsorption
Classification and external resources
Fructose
ICD-10 E74.3
ICD-9 271
OMIM 138230
Fructose malabsorption, formerly named "dietary fructose intolerance" (DFI), is a digestive disorder[1] in which absorption of fructose is impaired by deficient fructose carriers in the small intestine's enterocytes. This results in an increased concentration of fructose in the entire intestine.
Occurrence in patients identified to be suffering symptoms of irritable bowel syndrome is not higher than occurrence in the normal population. However, due to the similarity in symptoms, patients with fructose malabsorption often fit the profile of those with irritable bowel syndrome.[2] A small proportion of patients with both fructose malabsorption and lactose intolerance also suffer from celiac disease.
Fructose malabsorption is not to be confused with hereditary fructose intolerance, a potentially fatal condition in which the liver enzymes that break up fructose are deficient.
Pathophysiology
Fructose is absorbed in the small intestine without help of digestive enzymes. Even in healthy persons, however, only about 25–50g of fructose per sitting can be properly absorbed. People with

fructose malabsorption absorb less than 25g per sitting.[3] In the large intestine, fructose that has not been adequately absorbed reduces the absorption of water osmotically and is metabolized by colonic bacteria into short chain fatty acids, producing the byproduct gases hydrogen, carbon dioxide and methane.[citation needed] This abnormal increase in hydrogen is detectable with the hydrogen breath test.
The physiological consequences of fructose malabsorption include increased osmotic load, rapid bacterial fermentation, altered gastrointestinal motility, the formation of mucosal biofilm and altered profile of bacteria. These effects are additive with other short-chain poorly absorbed carbohydrates such as sorbitol. The clinical significance of these events depends upon the response of the bowel to such changes. Some effects of fructose malabsorption are decreased tryptophan,[4] folic acid[5] and zinc in the blood.[5]
Restricting dietary intake of free fructose and/or fructans may provide symptom relief in a high proportion of patients with functional gut disorders.[6]
Symptoms
Bloating (from fermentation in the small and large intestine)
Diarrhea and/or constipation
Flatulence
Reflux
Stomach pain (as a result of muscle spasms, the intensity of which can vary from mild and chronic to acute but erratic)
Vomiting (if great quantities are consumed)
Early signs of mental depression[7]
Nausea
Diagnosis
The diagnostic test, when used, is similar to that used to diagnose lactose intolerance. It is called a hydrogen breath test and is the method currently used for a clinical diagnosis.
Treatment
There is no known cure, but an appropriate diet and the enzyme xylose isomerase can help.
Xylose isomerase
Xylose isomerase acts to convert fructose sugars into glucose. Dietary supplements are limited in the amount of fructose they can convert, thus the amount of fructose in a meal must be estimated and an appropriate dosage taken to work.[citation needed]
Diet
Foods that should be avoided by people with fructose malabsorption include:
Foods and beverages containing greater than 0.5 g fructose in excess of glucose per 100 g and greater than 0.2 g of fructans per serving should be avoided. Foods with >3 g of fructose per serving are termed a 'high fructose load' and possibly present a risk of inducing symptoms. However, the concept of a 'high fructose load' has not been evaluated in terms of its importance in the success of the diet.[8]

Foods with high fructose-to-glucose ratio. Glucose enhances absorption of fructose, so fructose from foods with fructose-to-glucose ratio <1, like white potatoes, are readily absorbed, whereas foods with fructose-to-glucose ratio >1, like apples and pears, are often problematic regardless of the total amount of fructose in the food.[9]
Foods rich in fructans and other fermentable oligo-, di- and mono-saccharides and polyols (FODMAPs), including artichokes, asparagus, leeks, onions, and wheat-containing products, including breads, cakes, biscuits, breakfast cereals, pies, pastas, pizzas, and wheat noodles.
Foods containing sorbitol, present in some diet drinks and foods, and occurring naturally in some stone fruits, or xylitol, present in some berries, and other polyols (sugar alcohols), such as erythritol, mannitol, and other ingredients that end with -tol, commonly added as artificial sweeteners in commercial foods.
Foods with a high glucose content ingested with foods containing excess fructose may help sufferers absorb the excess fructose.[10]
The role that fructans play in fructose malabsorption is still under investigation. However, it is recommended that fructan intake for fructose malabsorbers should be kept to less than 0.5 grams/serving,[11] and supplements with inulin and fructooligosaccharide (FOS), both fructans, should be avoided.[11]
Foods with high fructose content[edit]
According to the USDA database,[12] foods with more fructose than glucose include:
Food Fructose (grams / 100 grams) Glucose (grams / 100 grams)
Sucrose
(for reference) 50 50
Apples 5.9 2.4
Pears 6.2 2.8
Fruit juice
e.g. Apples,
Pears
5–7 2–3
Watermelon 3.4 1.6
Raisins 29.8 27.8

Food Fructose (grams / 100 grams) Glucose (grams / 100 grams)
Honey 40.9 35.7
High fructose
corn syrup
42–55 45–58
Mango 4.68 2.01
Agave nectar 55.6 12.43
The USDA food database reveals that many common fruits contain nearly equal amounts of the fructose and glucose, and they do not present problems for those individuals with fructose malabsorption.[13] Some fruits with a greater ratio of fructose than glucose are apples, pears and watermelon, which contain more than twice as much fructose as glucose. Fructose levels in grapes varies depending on ripeness and variety, where unripe grapes contain more glucose.
Dietary guidelines for the management of fructose malabsorption[edit]
Researchers at Monash University in Australia developed dietary guidelines[11] for managing fructose malabsorption, particularly for individuals with IBS.
Unfavorable foods (i.e. more fructose than glucose)[edit]
Fruit – apple, pear, guava, honeydew melon, nashi pear, pawpaw, papaya, quince, star fruit, watermelon;
Dried fruit – apple, currant, date, fig, pear, raisin, sultana;
Fortified wines
Foods containing added sugars, such as agave nectar, some corn syrups, and fruit juice concentrates.
Favorable foods (i.e. fructose equal to or less than glucose)[edit]
The following list of favorable foods was cited in the paper: "Fructose malabsorption and symptoms of Irritable Bowel Syndrome Guidelines for effective dietary management".[11] The fructose and glucose contents of foods listed on the Australian food standards[14]would appear to indicate that most of the listed foods have higher fructose levels.
Stone fruit: apricot, nectarine, peach, plum (caution — these fruits contain sorbitol);
Berry fruit: blueberry, blackberry, boysenberry, cranberry, raspberry, strawberry, loganberry;
Citrus fruit: kumquat, grapefruit, lemon, lime, mandarin, orange, tangelo;
Other fruits: ripe banana, jackfruit, kiwi fruit, passion fruit, pineapple, rhubarb, tamarillo.
Food-labeling
Producers of processed food in most or all countries, including the USA, are not currently required by law to mark foods containing "fructose in excess of glucose." This can cause some surprises and pitfalls for fructose malabsorbers.
Foods (such as bread) marked "gluten-free" are usually suitable for fructose malabsorbers, though sufferers need to be careful of gluten-free foods that contain dried fruit or high fructose corn syrup or fructose itself in sugar form. However, fructose malabsorbers donot need to avoid gluten, as those with celiac disease must.
Many fructose malabsorbers can eat breads made from rye and corn flour. However, these may contain wheat unless marked "wheat-free" (or "gluten-free") (Note: Rye bread is not gluten-free.) Although often assumed to be an acceptable alternative to wheat, spelt flour is not suitable for sufferers of fructose malabsorption[citation needed], just as it is not appropriate for those with wheat allergies or celiac disease. However, some fructose malabsorbers do not have difficulty with fructans from wheat products while they may have problems with foods that contain excess free fructose.[citation
needed]
There are many breads on the market that boast having no high fructose corn syrup. In lieu of high fructose corn syrup, however, one may find the production of special breads with a high inulin content, where inulin is a replacement in the baking process for the following: high fructose corn syrup, flour and fat. Because of the caloric reduction, lower fat content, dramatic fiber increase and prebiotic tendencies of the replacement inulin, these breads are considered a healthier alternative to traditionally prepared leaveningbreads. Though the touted health benefits may exist, sufferers of fructose malabsorption will likely find no difference between these new breads and traditionally prepared breads in alleviating their symptoms because inulin is a fructan, and, again, consumption of fructans should be reduced dramatically in those with fructose malabsorption in an effort to appease symptoms.
New research
Fructose and fructans which are polymers of fructose are FODMAPs (Fermentable Oligo-, Di- and Mono-saccharides and Polyols) known to cause gastrointestinal discomfort in susceptible individuals. A low FODMAP diet has widespread application for managing functional gastrointestinal disorders such as IBS.[8]
See also
Hereditary fructose intolerance
FODMAP
Gastroenterology
Hydrogen breath test
Invisible disability
Food intolerance
Irritable bowel syndrome
Malabsorption
References
1. MayoClinic.com
2. Ledochowski M, et al. (2001). "Fruktosemalabsorption". Journal für Ernährungsmedizin (in German) 3 (1): 15–19.
3. http://www.uihealthcare.com/kxic/2008/06/fructose.html
4. Ledochowski M, Widner B, Murr C, Sperner-Unterweger B, Fuchs D (2001). "Fructose malabsorption is associated with decreased plasma tryptophan". Scand. J. Gastroenterol. 36 (4): 367–71. doi:10.1080/003655201300051135. PMID 11336160.
5. ^ Jump up to:a b Ledochowski M, Uberall F, Propst T, Fuchs D (1999). "Fructose malabsorption is associated with lower plasma folic acid concentrations in middle-aged subjects". Clin. Chem. 45 (11): 2013–4. PMID 10545075.
6. Gibson PR, Newnham E, Barrett JS, Shepherd SJ, Muir JG (2007). "Review article: fructose malabsorption and the bigger picture".Aliment. Pharmacol. Ther. 25 (4): 349–63. doi:10.1111/j.1365-2036.2006.03186.x. PMID 17217453.
7. Ledochowski M, Sperner-Unterweger B, Widner B, Fuchs D. (2010). "Fructose malabsorption is associated with early signs of mental depression.". European Journal of Medical Research 3 (6): 295–8. PMID 9620891.
8. ^ Jump up to:a b Gibson PR, Shepherd SJ (2010). "Evidence-based dietary management of functional gastrointestinal symptoms: The FODMAP approach". Advances in Clinical Practice 25 (2): 252–8. doi:10.1111/j.1440-1746.2009.06149.x. PMID 20136989.
9. http://www.healthsystem.virginia.edu/internet/digestive-health/nutrition/BarrettArticle.pdf
10. Skoog SM, Bharucha AE (2004). "Dietary fructose and gastrointestinal symptoms: a review". Am. J. Gastroenterol. 99 (10): 2046–50.doi:10.1111/j.1572-0241.2004.40266.x. PMID 15447771.
11. ^ b c d Shepherd SJ, Gibson PR (2006). "Fructose malabsorption and symptoms of irritable bowel syndrome: guidelines for effective dietary management" (PDF). Journal of the American Dietetic Association 106 (10): 1631–9. doi:10.1016/j.jada.2006.07.010.PMID 17000196.
12. USDA National Nutrient Database Release 20, September 2007
13. Sugar Content of Selected Foods: Individual and Total Sugars Ruth H. Matthews, Pamela R. Pehrsson, and Mojgan Farhat-Sabet, (1987) U.S.D.A.
14. "NUTTAB 2010 Online Searchable Database". Food Standards Australia New Zealand. Archived from the original on 2012-03-24. Retrieved 7 July 2013.
Use and abuse of hydrogen breath tests
M Simrén and P‐O Stotzer
Author information ► Article notes ► Copyright and License information ►
This article has been cited by other articles in PMC.
Abstract
Within the field of gastroenterology, the majority of symptoms cannot be explained by structural
abnormalities detected on routine investigations.1 Many of these symptoms are clustered together
forming the functional gastrointestinal disorders, as defined by the Rome II criteria.2,3 The
pathophysiology behind these disorders is still incompletely known.4 In the search for possible
pathophysiological factors of functional gastrointestinal disorders, several authors have used
different hydrogen breath tests in recent years to detect various abnormalities, such as
carbohydrate malabsorption5,6,7 and small intestinal bacterial overgrowth (SIBO).8,9 However,
these tests are indirect, with several drawbacks and pitfalls. In this article, we will review the

literature on the use of hydrogen breath tests to detect carbohydrate malabsorption and SIBO,
and highlight the controversies and inconsistencies in the interpretation of these tests, especially
regarding the relevance of fructose malabsorption and SIBO in patients with functional
gastrointestinal disorders.
Go to:
Hydrogen breath tests
Hydrogen breath tests are based on the fact that there is no source for hydrogen gas in humans
other than bacterial metabolism of carbohydrates.10 For these tests different carbohydrates are
administered orally and the concentration of hydrogen is measured in expired air. When
defective sugar absorption is present, unabsorbed sugars are available in the colon for bacterial
fermentation, and in the case of SIBO the bacterial population migrates proximally in the small
intestine gaining access to the sugars. When exposed to bacteria in the bowel, the substrate will
be metabolised to hydrogen, which is quickly absorbed, expired, and possible to measure in
expired air (fig 11).). The different tests are performed in the fasting state after at least one day of
a low fibre diet. Smoking raises and exercise lowers hydrogen concentrations and is therefore not
allowed during the test.11 Glucose12,13 or lactulose14 are the most commonly used substrates for
diagnosis of SIBO whereas the different sugars tested for carbohydrates malabsorption are given
to detect these disorders.15
Figure 1 Schematic drawing showing the principles behind breath tests.
“Hydrogen breath tests are based on the fact that there is no source for hydrogen gas in humans
other than bacterial metabolism of carbohydrates”
The hydrogen breath test depends on the presence of hydrogen producing bacteria. However, a
considerable proportion of non‐hydrogen producing bacteria, which can yield false negative
results, has been observed in some12,16,17 but not all studies.18,19,20 Several other potential sources of
error exist, such as carbohydrate malabsorption in chronic pancreatitis and coeliac disease, with
false positive tests for SIBO due to colonic fermentation and gas production,20,21,22,23 and
gastrointestinal motor disorders, where delayed gastric emptying may cause false negative
tests24 and rapid transit through the small bowel will produce false positive breath
tests.22,25,26,27 False positive results may also be due to the oral bacterial flora and if the subject has
failed to adhere to a low fibre diet the day before the test.
Go to:
Carbohydrate malabsorption
Carbohydrate digestion and absorption
Almost all carbohydrates from the diet are large polysaccharides or disaccharides. In order to be
adequately absorbed from the intestine into portal blood, poly‐ and disaccharides must undergo
digestion in order to become absorbable monosaccharides (glucose, galactose, and fructose). For
this, different enzymes are required, such as pancreatic amylase and intestinal epithelial enzymes
(that is, lactase, sucrase, and maltase). Absorption is mainly an active transport, with selectivity
for specific monosaccharides and competition between different sugars. Therefore, the
composition of the diet influences the efficiency of carbohydrate absorption and the amount of
carbohydrates that reaches the colon unabsorbed.
Carbohydrates that reach the colon unabsorbed are fermented by bacteria and have been
proposed to be of importance for symptoms such as bloating, abdominal distension, and
diarrhoea. In particular, lactose,7,28,29,30 fructose, and sorbitol5,31 has been extensively studied in
patients with functional gastrointestinal disorders but more complex carbohydrates that escape
small bowel absorption may be of even greater importance.32
Lactose malabsorption
Lactose absorption
Lactose, found in milk, is a disaccharide composed of galactose and glucose. It is digested by
lactase, which is found on the brush border of small intestine epithelium, into glucose and
galactose, and these monosaccharides can then be absorbed. Lactose maldigestion is the
incomplete hydrolysis of lactose due to lactase deficiency, which may occur as a primary
disorder33 or secondary to another disorder of the small intestinal mucosa, for instance coeliac
disease.34 The vast majority of patients with the primary form have an acquired deficiency (that
is, enzyme activity is normal during the first years of life but then declines with ageing). Because
lactose cannot be absorbed it passes into the colon and through increased fluid secretion and gas
production it can lead to gastrointestinal symptoms referred to as lactose intolerance. There are
marked racial differences in the prevalence of lactase deficiency, with the prevalence being 3–
8% in Scandinavia and Northwest Europe, increasing to close to 100% in Southeast Asia. In
Europe, the frequency increases in southern and eastern directions, reaching 70% in southern
Italy and Turkey.15
Testing for lactose malabsorption
The most common test today to diagnose lactose malabsorption is the lactose hydrogen breath
test. Breath hydrogen is measured following ingestion of 25–50 g lactose dissolved in 100–500
ml of water, and after intake hydrogen concentration in end expiratory air is determined at 15–30
minutes intervals for 4–5 hours. The definition of a positive test has varied but a rise of 10–20
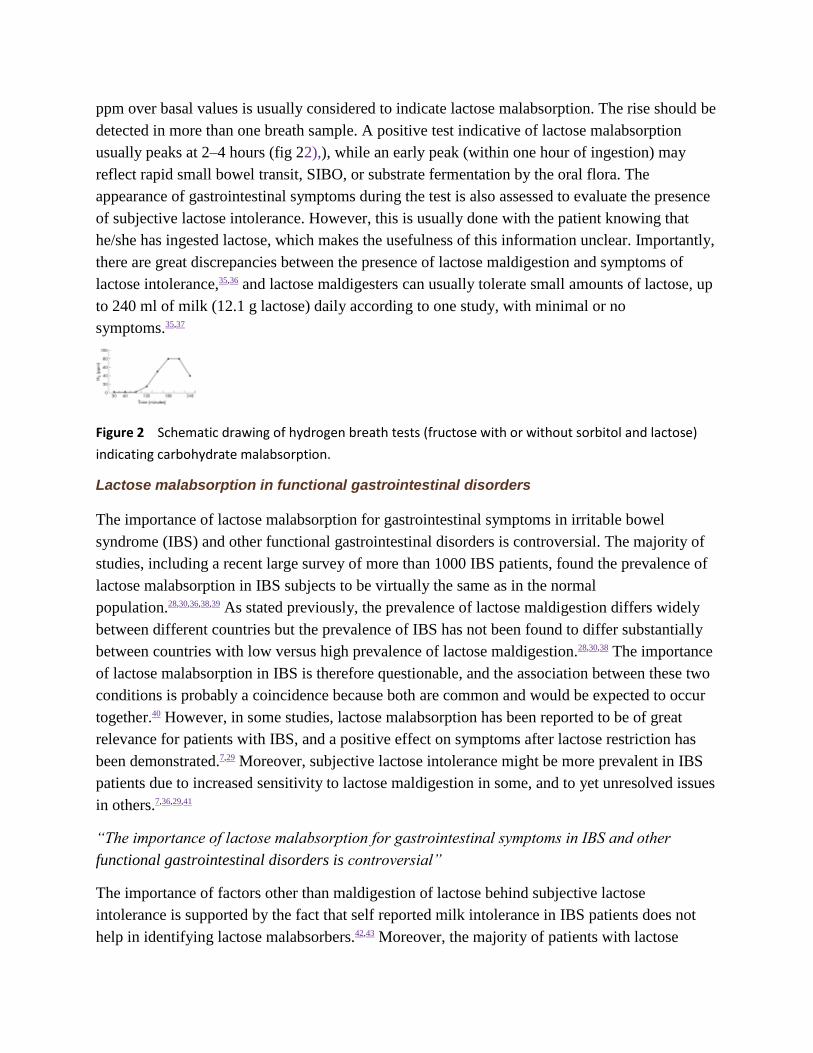
ppm over basal values is usually considered to indicate lactose malabsorption. The rise should be
detected in more than one breath sample. A positive test indicative of lactose malabsorption
usually peaks at 2–4 hours (fig 22),), while an early peak (within one hour of ingestion) may
reflect rapid small bowel transit, SIBO, or substrate fermentation by the oral flora. The
appearance of gastrointestinal symptoms during the test is also assessed to evaluate the presence
of subjective lactose intolerance. However, this is usually done with the patient knowing that
he/she has ingested lactose, which makes the usefulness of this information unclear. Importantly,
there are great discrepancies between the presence of lactose maldigestion and symptoms of
lactose intolerance,35,36 and lactose maldigesters can usually tolerate small amounts of lactose, up
to 240 ml of milk (12.1 g lactose) daily according to one study, with minimal or no
symptoms.35,37
Figure 2 Schematic drawing of hydrogen breath tests (fructose with or without sorbitol and lactose)
indicating carbohydrate malabsorption.
Lactose malabsorption in functional gastrointestinal disorders
The importance of lactose malabsorption for gastrointestinal symptoms in irritable bowel
syndrome (IBS) and other functional gastrointestinal disorders is controversial. The majority of
studies, including a recent large survey of more than 1000 IBS patients, found the prevalence of
lactose malabsorption in IBS subjects to be virtually the same as in the normal
population.28,30,36,38,39 As stated previously, the prevalence of lactose maldigestion differs widely
between different countries but the prevalence of IBS has not been found to differ substantially
between countries with low versus high prevalence of lactose maldigestion.28,30,38 The importance
of lactose malabsorption in IBS is therefore questionable, and the association between these two
conditions is probably a coincidence because both are common and would be expected to occur
together.40 However, in some studies, lactose malabsorption has been reported to be of great
relevance for patients with IBS, and a positive effect on symptoms after lactose restriction has
been demonstrated.7,29 Moreover, subjective lactose intolerance might be more prevalent in IBS
patients due to increased sensitivity to lactose maldigestion in some, and to yet unresolved issues
in others.7,36,29,41
“The importance of lactose malabsorption for gastrointestinal symptoms in IBS and other
functional gastrointestinal disorders is controversial”
The importance of factors other than maldigestion of lactose behind subjective lactose
intolerance is supported by the fact that self reported milk intolerance in IBS patients does not
help in identifying lactose malabsorbers.42,43 Moreover, the majority of patients with lactose

malabsorption can consume a considerable amount of lactose before having symptoms,35 and the
use of lactase treatment seems to be of limited value.44Therefore, subjective lactose intolerance is
probably relevant only for a subgroup of IBS patients, especially in those consuming large
amounts of dairy products. In these patients a lactose reduced diet might have a positive effect on
some of the symptoms, especially diarrhoea and gas/bloating, but the general impression is that
the importance of lactose malabsorption in IBS has been overestimated during the past, and that
dietary lactose exclusion rarely ameliorates the symptoms to any large extent in these patients.40
Fructose malabsorption
Fructose absorption
Fructose is a ketohexose occurring naturally in its free form or as sucrose (glucose+fructose). It
is widely used as a sweetener in different foods, beverages, and candy, and it is also present in
fruits such as apples, peaches, cherries, and pears.45 It is absorbed by carrier mediated facilitated
diffusion and results indicate that the capacity for fructose absorption is small compared with
that for sucrose and glucose.46 The absorptive capacity for fructose varies greatly, but as high as
30–80% of healthy individuals tested with a hydrogen breath test demonstrated incomplete
absorption of a 10% solution of 50 g of fructose.47,48,49 These studies also demonstrated that the
absorptive capacity was unrelated to age or sex but that it was dose and concentration dependent.
To put this dose into perspective, mean daily intake of free fructose (sucrose excluded) in the US
population has been found to be 16 g/day but “heavy” consumers may reach 60–100 g/day.50
Testing for fructose malabsorption
When testing for fructose malabsorption, 25–50 g of fructose dissolved in 150–250 ml of water
have been used. Methodology and interpretation of results is otherwise similar to lactose, as
described above (fig 22).). It is unclear what the optimal dosage of fructose is to detect clinically
meaningful malabsorption. Another unresolved issue is how symptoms should be assessed
during the test and to what extent these are reliable, as very few blinded studies have been
performed and the majority of studies are also uncontrolled. Of great importance is also the fact
that simultaneous ingestion of glucose increases fructose absorption,48,49 and the majority of
dietary sources of fructose also contain glucose. On the other hand, simultaneous ingestion of
sorbitol, a naturally found sugar alcohol often used as a “sugar free” sweetener by the food
industry, increases malabsorption of fructose.51 Therefore, breath testing of fructose alone
probably does not reflect fructose ingestion in everyday life, making interpretation of the test
extremely unreliable from a clinical point of view.
Fructose malabsorption in functional gastrointestinal disorders
A controversial issue is the importance of symptomatic malabsorption of fructose and/or sorbitol
in IBS and other functional gastrointestinal disorders. Based on the few direct comparisons
existing in the literature, malabsorption of fructose and/or sorbitol is not more frequent in IBS
patients than in healthy subjects.6,31,52,53 However, one study demonstrated that IBS patients with
incomplete absorption of fructose had significantly more severe symptoms after ingestion of
fructose than IBS subjects without malabsorption, and the symptoms were enhanced by adding
sorbitol, supporting the role of symptomatic fructose‐sorbitol malabsorption in IBS.5 A
subsequent large study reported a similar proportion of fructose‐sorbitol malabsorption in IBS
patients with and without symptoms after intake of fructose and sorbitol, opposing the view of an
important role for fructose‐sorbitol malabsorption in IBS.31 A Spanish study found more severe
symptoms after intake of a fructose‐sorbitol mixture in patients with functional gastrointestinal
disorders than after intake of sucrose as a control solution6whereas we found similar symptoms
in IBS patients with subjective fruit intolerance after intake of a fructose‐sorbitol mixture versus
glucose (control), irrespective of the presence of fructose malabsorption.54
“Malabsorption of fructose and/or sorbitol is not more frequent in IBS patients than in healthy
subjects”
As stated in a recent review, there is need for controlled studies clarifying the relation between
incomplete fructose absorption and symptoms, and also assessing the effects of co‐ingestion of
other sugars on fructose absorption.55 Until we have this information the role of fructose
malabsorption tests in clinical practice remains uncertain. For IBS patients ingesting large
amounts of fruits and/or products where artificial sweeteners are used, diets where fructose is
empirically restricted might be tested.
Go to:
Small intestinal bacterial overgrowth
SIBO is a condition caused by an abnormal number of bacteria in the small intestine. Symptoms
related to bacterial overgrowth in the small intestine are diarrhoea, weight loss, anaemia, and
malabsorption.56,57,58,59SIBO is a common cause of malabsorption and malnutrition,56,60 especially
among the elderly61,62 and in patients with blind loops,59 stenosis,63 diverticula,64,65 and motor
disorders.66,67 Recently, SIBO has been suggested to be associated with a large number of
different conditions, such as coeliac disease,34 chronic
pancreatitis,68,69 hypothyroidism,70 Parkinson's disease,71 and fibromyalgia.72 However, the
proposed contribution of SIBO to IBS has received the greatest attention, with studies
demonstrating prevalence values of 38–84% of SIBO in IBS,8,9,72,73,74 but these studies have been
heavily criticised,75,76,77,78,79 and contradictory results exist.80,81 In most cases the diagnosis of SIBO
has been established by the use of hydrogen breath tests, usually with glucose or lactulose.
However, the use of breath tests and interpretation of the result require knowledge about these
tests. In some studies discussion around possible sources of errors with the test has been very
sparse, as well as alternative interpretations of the results.68,82,83,84,85
“SIBO is a condition caused by an abnormal number of bacteria in the small intestine”
Normal bowel flora
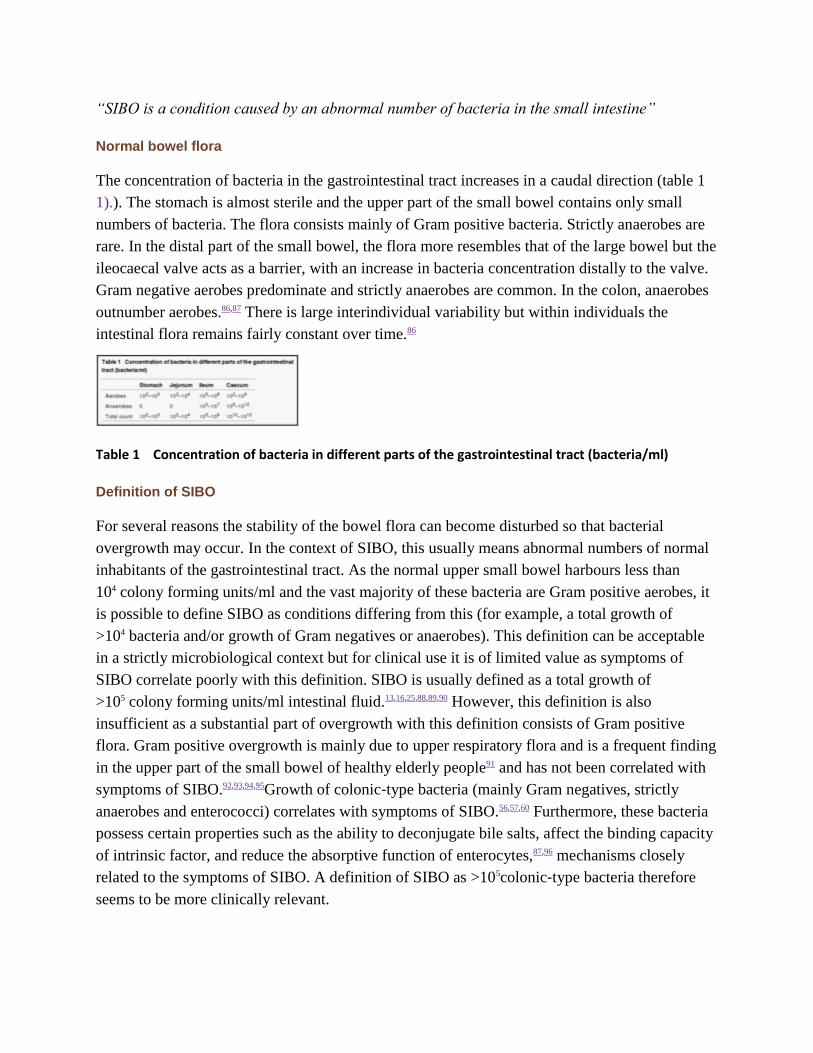
The concentration of bacteria in the gastrointestinal tract increases in a caudal direction (table 1
1).). The stomach is almost sterile and the upper part of the small bowel contains only small
numbers of bacteria. The flora consists mainly of Gram positive bacteria. Strictly anaerobes are
rare. In the distal part of the small bowel, the flora more resembles that of the large bowel but the
ileocaecal valve acts as a barrier, with an increase in bacteria concentration distally to the valve.
Gram negative aerobes predominate and strictly anaerobes are common. In the colon, anaerobes
outnumber aerobes.86,87 There is large interindividual variability but within individuals the
intestinal flora remains fairly constant over time.86
Table 1 Concentration of bacteria in different parts of the gastrointestinal tract (bacteria/ml)
Definition of SIBO
For several reasons the stability of the bowel flora can become disturbed so that bacterial
overgrowth may occur. In the context of SIBO, this usually means abnormal numbers of normal
inhabitants of the gastrointestinal tract. As the normal upper small bowel harbours less than
104 colony forming units/ml and the vast majority of these bacteria are Gram positive aerobes, it
is possible to define SIBO as conditions differing from this (for example, a total growth of
>104 bacteria and/or growth of Gram negatives or anaerobes). This definition can be acceptable
in a strictly microbiological context but for clinical use it is of limited value as symptoms of
SIBO correlate poorly with this definition. SIBO is usually defined as a total growth of
>105 colony forming units/ml intestinal fluid.13,16,25,88,89,90 However, this definition is also
insufficient as a substantial part of overgrowth with this definition consists of Gram positive
flora. Gram positive overgrowth is mainly due to upper respiratory flora and is a frequent finding
in the upper part of the small bowel of healthy elderly people91 and has not been correlated with
symptoms of SIBO.92,93,94,95Growth of colonic‐type bacteria (mainly Gram negatives, strictly
anaerobes and enterococci) correlates with symptoms of SIBO.56,57,60 Furthermore, these bacteria
possess certain properties such as the ability to deconjugate bile salts, affect the binding capacity
of intrinsic factor, and reduce the absorptive function of enterocytes,87,96 mechanisms closely
related to the symptoms of SIBO. A definition of SIBO as >105colonic‐type bacteria therefore
seems to be more clinically relevant.
Tests for SIBO
Small intestinal culturing
Culture of small bowel content is the most direct method for diagnosing SIBO and culture of
jejunal aspirate is by many considered to be the gold standard. However, there are several
difficulties associated with culturing. Obtaining aspirate for cultures is cumbersome and results
of culturing are not always representative. It is a common belief that cultures are often false
negative, especially concerning obligate anaerobes.60,97 Furthermore, only the upper part of the
small bowel is accessible for culturing and bacteria have been proven to grow only at the actual
location of the predisposing abnormality.98 On the other hand, false positive cultures due to
contamination, mainly from the oral flora, are also believed to be common.99
Breath tests
Because of the disadvantages with cultures, different breath tests have been developed. All of
these are indirect tests based on certain metabolic characteristics unique for bacteria. There are
three main types of breath tests used for diagnosing SIBO. The original breath test for diagnosing
SIBO was the bile acid breath test,100,101 depending on the ability of many types of bacteria to
deconjugate bile acids,56 but this test is rarely used today. In the 1 g 14C‐D‐xylose breath
test,102,103 patients are given 1 g of 14C labelled xylose which after absorption is normally secreted
through the kidneys with only minor endogenous metabolism. In the case of bacteria in the small
bowel, xylose is metabolised to 14CO2 which is absorbed and expired and thus possible to detect
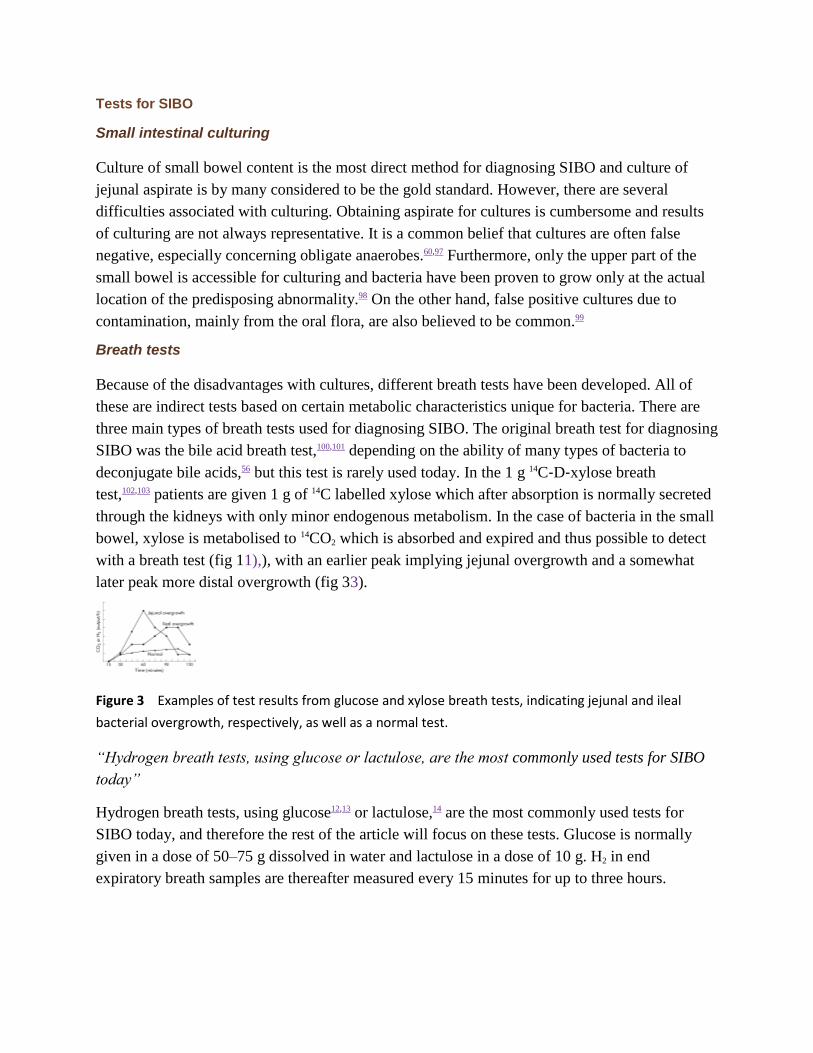
with a breath test (fig 11),), with an earlier peak implying jejunal overgrowth and a somewhat
later peak more distal overgrowth (fig 33).
Figure 3 Examples of test results from glucose and xylose breath tests, indicating jejunal and ileal
bacterial overgrowth, respectively, as well as a normal test.
“Hydrogen breath tests, using glucose or lactulose, are the most commonly used tests for SIBO
today”
Hydrogen breath tests, using glucose12,13 or lactulose,14 are the most commonly used tests for
SIBO today, and therefore the rest of the article will focus on these tests. Glucose is normally
given in a dose of 50–75 g dissolved in water and lactulose in a dose of 10 g. H2 in end
expiratory breath samples are thereafter measured every 15 minutes for up to three hours.

Abnormal versus normal results
Definitions of normal and abnormal results of breath tests are even more variable than for
cultures. The lack of generally accepted definitions raises a situation where you can almost
choose the test and definition that best suits your purpose. It is not uncommon to see the same
authors change their definitions of a positive test in different papers.8,9,72 Only a few papers have
described adequately their reasons for choosing a certain cut off point.23,24,25,104
Glucose is readily absorbed in the proximal small bowel, and in the absence of severe transit
abnormalities it rarely reaches the colon,26,105 making it an attractive substrate to detect at least
proximal SIBO. The glucose hydrogen breath test is considered positive if there is a clearly
recognisable hydrogen peak, exceeding 10–20 ppm (fig 33).12,13,89 High fasting concentrations
may be due to SIBO but this is a very unspecific finding which may also be due to slow
intestinal transit leaving a residue of poorly absorbable carbohydrates remaining in the
colon.16 Mostly, however, high fasting concentrations occur when the instruction to follow a low
fibre diet before the test not has been followed.
Lactulose passes unabsorbed through the small bowel and into the colon. Therefore, apart from
detecting SIBO, it can also be used as a measure of orocaecal transit.106 The original definition of
a positive lactulose test (that is, indicating SIBO) was an easily detected early hydrogen peak
(>20 ppm), due to small intestinal bacteria, occurring at least 15 minutes before the later
prolonged peak, corresponding to the passage of the remaining lactulose into the colon (fig 4
4).14 However, in some of the more recent studies, other less restrictive definitions, such as a rise
in H2 within 90 minutes, have been used,9,72,74 which should be compared with the fact that the
mean orocaecal transit time assessed with lactulose breath testing in healthy controls is slightly
above 90 minutes.106,107 Therefore, using this definition, 50% of healthy controls would be
expected to suffer from SIBO!79
Figure 4 A positive lactulose hydrogen breath test indicating small intestinal bacterial overgrowth with
an easily detected early peak due to small bowel bacteria, clearly distinguishable from the later
prolonged peak corresponding to the passage ...
“The sensitivity and specificity of the lactulose hydrogen breath test in detecting SIBO has been
reported to be only 68% and 44%, and for the glucose breath test 62% and 83%”
Moreover, without a clear second peak in the lactulose breath test, it is impossible to distinguish
SIBO from colonic fermentation, often caused by rapid transit,81,108 and importantly lactulose
itself accelerates small bowel transit.107 However, not even detection of two easily
distinguishable hydrogen peaks is a safe criterion as it has been shown in transit studies that a
bolus can reach the caecum, imitating the first peak followed by the body of lumen contents,
producing a second peak, yielding false positive lactulose tests.108,109 Therefore, it is not
surprising that the sensitivity and specificity of the lactulose hydrogen breath test in detecting
SIBO has been reported to be only 68% and 44%, and for the glucose breath test 62% and 83%.16
Which test should be used?
There is no general agreement as to which breath test is preferable.25,88,89,104 In some investigations
the 1 g 14C‐D‐xylose breath test has shown excellent results but this has not been confirmed in
more recent studies.23,25,104 However, as stated above, the hydrogen breath test with lactulose was
found to have both lower specificity and sensitivity than other breath tests.16,89 Although
sensitivity in general is acceptable, because of the low specificity for diagnosing SIBO compared
with jejunal cultures, it has even been questioned if breath tests are useful at all for diagnosing
SIBO.16,20,23,24,81,90,104,108
Is there a link between SIBO and IBS?
Recent studies suggest a strong link between SIBO and IBS, using the lactulose breath
test,8,9,72,74,110 but others, using lactulose, glucose, and xylose breath tests, as well as jejunal
cultures, have failed to confirm these findings.80,81 It has been proposed that the reason for the
poor concordance between the lactulose breath test and jejunal cultures and the other breath tests
is that lactulose is not absorbed in the small bowel. Because of this, the lactulose breath test is
thought to be superior in detecting ileal bacterial overgrowth.8,9As this part of the small bowel
has other functions than the upper part, bacterial overgrowth of the distal small bowel may also
cause different symptoms. Theoretically, it is possible that distal bacterial overgrowth would not
cause malabsorption, but instead IBS symptoms. However, evidence of the existence of culture
proven ileal bacterial overgrowth is lacking.
“Recent studies suggest a strong link between SIBO and IBS, using the lactulose breath test, but
others, using lactulose, glucose, and xylose breath tests, as well as jejunal cultures, have failed
to confirm these findings”
Pimentel et al have shown that the lactulose hydrogen breath test is often positive in IBS
patients8,9,72 and that treatment with antibiotics or a low fibre diet in patients with IBS and a
positive lactulose hydrogen breath test improves symptoms and reduces breath hydrogen
concentration.9,111 Are these results really explained by the presence of SIBO? An alternative
interpretation is that the positive breath test is due to hydrogen production by colonic bacteria
and that treatment reduces the number of bacteria and their production of hydrogen. This is
supported by preliminary findings from King and colleagues of abnormal colonic fermentation in
IBS112 and a more recent study from the same group113 where they demonstrated that treatment of
subjects with IBS with metronidazole or a low fibre diet improved symptoms, reduced gas
excretion, and produced a corresponding decrease in the concentration of faecal bacteria.
The studies by Pimentel and others have paved the way towards studying alterations in the gut
flora of IBS and other functional gastrointestinal disorders. The story of SIBO and IBS has not
come to an end and hopefully future studies will be performed using appropriate methods and
correct interpretation of the results.
Go to:
Conclusion
Hydrogen breath tests are simple and safe, providing us with an easy tool to unravel the
pathophysiological alterations behind symptoms difficult to explain. However, these tests have a
number of limitations. The importance of SIBO and bacteria in other parts of the gut for
functional gastrointestinal symptoms remains to be determined, and breath tests used wisely can
be important together with other techniques in future studies. Today, regular use of the lactulose
breath test in clinical practice in the evaluation of symptoms in patients with suspected functional
gastrointestinal disorders cannot be recommended. The relevance of maldigestion of specific
carbohydrates, such as lactose and fructose, in functional gastrointestinal disorders is probably
overestimated. However, in some patients with a large intake of products containing these
sugars, a hydrogen breath test, followed by dietary restriction of the sugar in case of a positive
test, may be advised. Hopefully, the occasional abuse of hydrogen breath tests seen today can be
turned into proper clinical and scientific use in the future.
Go to:
Abbreviations
SIBO - small intestinal bacterial overgrowth
IBS - irritable bowel syndrome
Go to:
Footnotes
Conflict of interest: None declared.
Go to:
References
1. Kroenke K, Mangelsdorff A D. Common symptoms in ambulatory care: incidence, evaluation, therapy,
and outcome. Am J Med 1989. 86262–266.266 [PubMed]
2. Talley N J, Stanghellini V, Heading R C. et al Functional gastroduodenal disorders. Gut 1999. 45(suppl
2)II37–II42.II42 [PMC free article] [PubMed]

3. Thompson W G, Longstreth G F, Drossman D A. et al Functional bowel disorders and functional
abdominal pain. Gut 1999. 45(suppl 2)II43–II47.II47 [PMC free article] [PubMed]
4. Mayer E A, Naliboff B D, Chang L. Basic pathophysiologic mechanisms in irritable bowel syndrome. Dig
Dis 2001. 19212–218.218 [PubMed]
5. Rumessen J J, Gudmand‐Hoyer E. Functional bowel disease: malabsorption and abdominal distress
after ingestion of fructose, sorbitol, and fructose‐sorbitol mixtures. Gastroenterology 1988. 95694–
700.700[PubMed]
6. Fernandez‐Banares F, Esteve‐Pardo M, de Leon R. et al Sugar malabsorption in functional bowel
disease: clinical implications. Am J Gastroenterol 1993. 882044–2050.2050 [PubMed]
7. Böhmer C J, Tuynman H A. The clinical relevance of lactose malabsorption in irritable bowel
syndrome.Eur J Gastroenterol Hepatol 1996. 81013–1016.1016 [PubMed]
8. Pimentel M, Chow E J, Lin H C. Eradication of small intestinal bacterial overgrowth reduces symptoms
of irritable bowel syndrome. Am J Gastroenterol 2000. 953503–3506.3506 [PubMed]
9. Pimentel M, Chow E J, Lin H C. Normalization of lactulose breath testing correlates with symptom
improvement in irritable bowel syndrome. a double‐blind, randomized, placebo‐controlled study. Am J
Gastroenterol 2003. 98412–419.419 [PubMed]
10. Levitt M D. Production and excretion of hydrogen gas in man. N Engl J Med 1969. 281122–
127.127[PubMed]
11. Thompson D G, Binfield P, De Belder A. et al Extra intestinal influences on exhaled breath hydrogen
measurements during the investigation of gastrointestinal disease. Gut 1985. 261349–1352.1352[PMC
free article] [PubMed]
12. Metz G, Gassull M A, Drasar B S. et al Breath‐hydrogen test for small‐intestinal bacterial
colonisation.Lancet 1976. 1668–669.669 [PubMed]
13. Kerlin P, Wong L. Breath hydrogen testing in bacterial overgrowth of the small
intestine.Gastroenterology 1988. 95982–988.988 [PubMed]
14. Rhodes J M, Middleton P, Jewell D P. The lactulose hydrogen breath test as a diagnostic test for
small‐bowel bacterial overgrowth. Scand J Gastroenterol 1979. 14333–336.336 [PubMed]
15. Gudmand‐Hoyer E. The clinical significance of disaccharide maldigestion. Am J Clin
Nutr 1994. 59735–41S.41S [PubMed]

16. Corazza G R, Menozzi M G, Strocchi A. et al The diagnosis of small bowel bacterial overgrowth.
Reliability of jejunal culture and inadequacy of breath hydrogen testing. Gastroenterology 1990. 98302–
309.309 [PubMed]
17. Khin Maung U, Tin A, Ku Tin M. et al In vitro hydrogen production by enteric bacteria cultured from
children with small bowel bacterial overgrowth. J Pediatr Gastroenterol Nutr 1992. 14192–
197.197[PubMed]
18. Christl S U, Murgatroyd P R, Gibson G R. et al Production, metabolism, and excretion of hydrogen in
the large intestine. Gastroenterology 1992. 1021269–1277.1277 [PubMed]
19. Strocchi A, Levitt M D. Maintaining intestinal H2 balance: credit the colonic
bacteria. Gastroenterology1992. 1021424–1426.1426 [PubMed]
20. Riordan S M, McIver C J, Bolin T D. et al Fasting breath hydrogen concentrations in gastric and small‐
intestinal bacterial overgrowth. Scand J Gastroenterol 1995. 30252–257.257 [PubMed]
21. Kerlin P, Wong L, Harris B. et al Rice flour, breath hydrogen, and
malabsorption. Gastroenterology1984. 87578–585.585 [PubMed]
22. Corazza G R, Strocchi A, Gasbarrini G. Fasting breath hydrogen in celiac
disease. Gastroenterology1987. 9353–58.58 [PubMed]
23. Riordan S M, McIver C J, Duncombe V M. et al Factors influencing the 1‐g 14C‐D‐xylose breath test
for bacterial overgrowth. Am J Gastroenterol 1995. 901455–1460.1460 [PubMed]
24. Valdovinos M A, Camilleri M, Thomforde G M. et al Reduced accuracy of 14C‐D‐xylose breath test for
detecting bacterial overgrowth in gastrointestinal motility disorders. Scand J
Gastroenterol 1993. 28963–968.968 [PubMed]
25. Rumessen J J, Gudmand‐Hoyer E, Bachmann E. et al Diagnosis of bacterial overgrowth of the small
intestine. Comparison of the 14C‐D‐xylose breath test and jejunal cultures in 60 patients. Scand J
Gastroenterol 1985. 201267–1275.1275 [PubMed]
26. Sellin J H, Hart R. Glucose malabsorption associated with rapid intestinal transit. Am J
Gastroenterol1992. 87584–589.589 [PubMed]
27. Strocchi A, Corazza G, Ellis C J. et al Detection of malabsorption of low doses of carbohydrate:
accuracy of various breath H2 criteria. Gastroenterology 1993. 1051404–1410.1410 [PubMed]
28. Bozzani A, Penagini R, Velio P. et al Lactose malabsorption and intolerance in Italians. Clinical
implications. Dig Dis Sci 1986. 311313–1316.1316 [PubMed]
29. Böhmer C J, Tuynman H A. The effect of a lactose‐restricted diet in patients with a positive lactose
tolerance test, earlier diagnosed as irritable bowel syndrome: a 5‐year follow‐up study. Eur J
Gastroenterol Hepatol 2001. 13941–944.944 [PubMed]
30. Farup P G, Monsbakken K W, Vandvik P O. Lactose malabsorption in a population with irritable
bowel syndrome: prevalence and symptoms. A case‐control study. Scand J Gastroenterol 2004. 39645–
649.649[PubMed]
31. Nelis G F, Vermeeren M A, Jansen W. Role of fructose‐sorbitol malabsorption in the irritable bowel
syndrome. Gastroenterology 1990. 991016–1020.1020 [PubMed]
32. Levitt M D, Hirsh P, Fetzer C A. et al H2 excretion after ingestion of complex
carbohydrates.Gastroenterology 1987. 92383–389.389 [PubMed]
33. Huang S S, Bayless T M. Lactose intolerance in healthy children. N Engl J Med 1967. 2761283–
1287.1287 [PubMed]
34. Ghoshal U C, Ghoshal U, Misra A. et al Partially responsive celiac disease resulting from small
intestinal bacterial overgrowth and lactose intolerance. BMC Gastroenterol 2004. 410 [PMC free
article] [PubMed]
35. Suarez F L, Savaiano D A, Levitt M D. A comparison of symptoms after the consumption of milk or
lactose‐ hydrolyzed milk by people with self‐reported severe lactose intolerance. N Engl J
Med 1995. 3331–4.4 [PubMed]
36. Vesa T H, Seppo L M, Marteau P R. et al Role of irritable bowel syndrome in subjective lactose
intolerance. Am J Clin Nutr 1998. 67710–715.715 [PubMed]
37. Vesa T H, Korpela R A, Sahi T. Tolerance to small amounts of lactose in lactose maldigesters. Am J
Clin Nutr 1996. 64197–201.201 [PubMed]
38. Ferguson A, MacDonald D M, Brydon W G. Prevalence of lactase deficiency in British
adults. Gut1984. 25163–167.167 [PMC free article] [PubMed]
39. Hamm L R, Sorrells S C, Harding J P. et al Additional investigations fail to alter the diagnosis of
irritable bowel syndrome in subjects fulfilling the Rome criteria. Am J Gastroenterol 1999. 941279–
1282.1282[PubMed]
40. Turnbull G K. Lactose intolerance and irritable bowel syndrome. Nutrition 2000. 16665–
666.666[PubMed]
41. Simrén M, Månsson A, Langkilde A M. et al Food‐related gastrointestinal symptoms in the irritable
bowel syndrome. Digestion 2001. 63108–115.115 [PubMed]

42. Simrén M, Månsson A, Bengtsson U. et al Lactose maldigestion does not explain subjective
intolerance for dairy products in the irritable bowel syndrome (IBS). Gastroenterology 2001. 1204059
43. Vernia P, Marinaro V, Argnani F. et al Self‐reported milk intolerance in irritable bowel syndrome:
what should we believe? Clin Nutr 2004. 23996–1000.1000 [PubMed]
44. Lisker R, Solomons N W, Perez Briceno R. et al Lactase and placebo in the management of the
irritable bowel syndrome: a double‐blind, cross‐over study. Am J Gastroenterol 1989. 84756–
762.762 [PubMed]
45. Rumessen J J. Fructose and related food carbohydrates. Sources, intake, absorption, and clinical
implications. Scand J Gastroenterol 1992. 27819–828.828 [PubMed]
46. Riby J E, Fujisawa T, Kretchmer N. Fructose absorption. Am J Clin Nutr 1993. 58748–
53S.53S[PubMed]
47. Ravich W J, Bayless T M, Thomas M. Fructose: incomplete intestinal absorption in
humans.Gastroenterology 1983. 8426–29.29 [PubMed]
48. Rumessen J J, Gudmand‐Hoyer E. Absorption capacity of fructose in healthy adults. Comparison with
sucrose and its constituent monosaccharides. Gut 1986. 271161–1168.1168 [PMC free article] [PubMed]
49. Truswell A S, Seach J M, Thorburn A W. Incomplete absorption of pure fructose in healthy subjects
and the facilitating effect of glucose. Am J Clin Nutr 1988. 481424–1430.1430 [PubMed]
50. Glinsmann W H, Irausquin H, Park Y K. Evaluation of health aspects of sugars contained in
carbohydrate sweeteners. Report of Sugars Task Force, 1986. J Nutr 1986. 116S1–216.216 [PubMed]
51. Rumessen J J, Gudmand‐Hoyer E. Malabsorption of fructose‐sorbitol mixtures. Interactions causing
abdominal distress. Scand J Gastroenterol 1987. 22431–436.436 [PubMed]
52. Symons P, Jones M P, Kellow J E. Symptom provocation in irritable bowel syndrome. Effects of
differing doses of fructose‐sorbitol. Scand J Gastroenterol 1992. 27940–944.944 [PubMed]
53. Evans P R, Piesse C, Bak Y T. et al Fructose‐sorbitol malabsorption and symptom provocation in
irritable bowel syndrome: relationship to enteric hypersensitivity and dysmotility. Scand J
Gastroenterol1998. 331158–1163.1163 [PubMed]
54. Simrén M, Månsson A, Bengtsson U. et al Is malabsorption of fructose‐sorbitol really important in
the irritable bowel syndrome (IBS)? Gastroenterology 2001. 1203232
55. Skoog S M, Bharucha A E. Dietary fructose and gastrointestinal symptoms: a review. Am J
Gastroenterol 2004. 992046–2050.2050 [PubMed]
56. Donaldson R M. Role of enteric microorganisms in malabsorption. Fed Proc 1967. 261426–
1431.1431[PubMed]
57. King C E, Toskes P P. Small intestine bacterial overgrowth. Gastroenterology 1979. 761035–
1055.1055[PubMed]
58. Kirsch M. Bacterial overgrowth. Am J Gastroenterol 1990. 85231–237.237 [PubMed]
59. Toskes P P. Bacterial overgrowth of the gastrointestinal tract. Adv Intern Med 1993. 38387–
407.407[PubMed]
60. Tabaqchali S. The pathophysiological role of small intestinal bacterial flora. Scand J Gastroenterol
Suppl1970. 6139–163.163 [PubMed]
61. Roberts S H, James O, Jarvis E H. Bacterial overgrowth syndrome without "blind loop": A cause for
malnutrition in the elderly. Lancet 1977. 21193–1195.1195 [PubMed]
62. McEvoy A, Dutton J, James O F. Bacterial contamination of the small intestine is an important cause
of occult malabsorption in the elderly. Br Med J (Clin Res Ed) 1983. 287789–793.793 [PMC free
article][PubMed]
63. Bishop R F, Anderson C M. The bacterial flora of the stomach and small intestine in children with
intestinla obstruction. Arch Dis Child 1960. 35487–491.491 [PMC free article] [PubMed]
64. Farrar W E, Jr, O'Dell N M, Achord J L. et al Intestinal microflora and absorption in patients with
stagnation‐inducing lesions of the small intestine. Am J Dig Dis 1972. 171065–1074.1074 [PubMed]
65. Eggert A. Interdigestive Motilität bei duodenaldivertikeln. Langerbecks Arch Chir 1988. 37397–
103.103[PubMed]
66. Vantrappen G, Janssens J, Hellemans J. et al The interdigestive motor complex of normal subjects
and patients with bacterial overgrowth of the small intestine. J Clin Invest 1977. 591158–
1166.1166[PMC free article] [PubMed]
67. Stotzer P O, Björnsson E S, Abrahamsson H. Interdigestive and postprandial motility in small‐
intestinal bacterial overgrowth. Scand J Gastroenterol 1996. 31875–880.880 [PubMed]
68. Casellas F, Guarner L, Vaquero E. et al Hydrogen breath test with glucose in exocrine pancreatic
insufficiency. Pancreas 1998. 16481–486.486 [PubMed]
69. Trespi E, Ferrieri A. Intestinal bacterial overgrowth during chronic pancreatitis. Curr Med Res
Opin1999. 1547–52.52 [PubMed]

70. Lauritano E C, Lupascu A, Scarpellini E. et al Small intestinal bacterial overgrowth prevalence in
hypothyroidism. Gastroenterology 2005. 128W1743
71. Lupascu A, Lauritano C, Scarpellini E. et al Small intestinal bacterial overgrowth prevalence in
Parkinson's disease. Gastroenterology 2005. 128W1742
72. Pimentel M, Wallace D, Hallegua D. et al A link between irritable bowel syndrome and fibromyalgia
may be related to findings on lactulose breath testing. Ann Rheum Dis 2004. 63450–452.452[PMC free
article] [PubMed]
73. McCallum R, Schultz C, Sostarich S. Evaluating the role of small intestinal bacterial overgrowth (SIBO)
in diarrhea predominant IBS (IBS‐D) patients utilizing the glucose breath
test. Gastroenterology 2005.128T1118
74. Nucera G, Gabrielli M, Lupascu A. et al Abnormal breath tests to lactose, fructose and sorbitol in
irritable bowel syndrome may be explained by small intestinal bacterial overgrowth. Aliment Pharmacol
Ther2005. 211391–1395.1395 [PubMed]
75. Cuoco L, Cammarota G, Jorizzo R. et al Small intestinal bacterial overgrowth and symptoms of
irritable bowel syndrome. Am J Gastroenterol 2001. 962281–2282.2282 [PubMed]
76. Jones M P, Craig R, Olinger E. Small intestinal bacterial overgrowth is associated with irritable bowel
syndrome: the cart lands squarely in front of the horse. Am J Gastroenterol 2001. 963204–
3205.3205[PubMed]
77. Mishkin D, Mishkin S. Re: Pimentel et al. Eradication of small intestinal bacterial overgrowth reduces
symptoms of irritable bowel syndrome. Am J Gastroenterol 2001. 962505–2506.2506 [PubMed]
78. Riordan S M, McIver C J, Duncombe V M. et al Small intestinal bacterial overgrowth and the irritable
bowel syndrome. Am J Gastroenterol 2001. 962506–2508.2508 [PubMed]
79. Hasler W L. Lactulose breath testing, bacterial overgrowth, and IBS: just a lot of hot air?
Gastroenterology 2003. 1251898–1900.1900 [PubMed]
80. Posserud I, Ringström G, Stotzer P O. et al Small intestinal bacterial overgrowth (SIBO) in irritable
bowel syndrome (IBS). Neurogastroenterol Motil 2004. 16839
81. Walters B, Vanner S J. Detection of bacterial overgrowth in IBS using the lactulose H breath test:
comparison with C‐D‐xylose and healthy controls. Am J Gastroenterol 2005. 1001566–
1570.1570[PubMed]
82. Iivonen M K, Ahola T O, Matikainen M J. Bacterial overgrowth, intestinal transit, and nutrition after
total gastrectomy. Comparison of a jejunal pouch with Roux‐en‐Y reconstruction in a prospective
random study.Scand J Gastroenterol 1998. 3363–70.70 [PubMed]
83. Attar A, Flourie B, Rambaud J C. et al Antibiotic efficacy in small intestinal bacterial overgrowth‐
related chronic diarrhea: a crossover, randomized trial. Gastroenterology 1999. 117794–
797.797 [PubMed]
84. Castiglione F, Rispo A, Di Girolamo E. et al Antibiotic treatment of small bowel bacterial overgrowth
in patients with Crohn's disease. Aliment Pharmacol Ther 2003. 181107–1112.1112 [PubMed]
85. Di Stefano M, Miceli E, Missanelli A. et al Absorbable vs. non‐absorbable antibiotics in the treatment
of small intestine bacterial overgrowth in patients with blind‐loop syndrome. Aliment Pharmacol
Ther 2005.21985–992.992 [PubMed]
86. Donaldson R M. Normal bacterial populations of the intestine and their relation to intestinal
function. N Engl J Med 1964. 270938–945.945 [PubMed]
87. Simon G L, Gorbach S L. Intestinal flora in health and disease. Gastroenterology 1984. 86174–
193.193[PubMed]
88. Schneider A, Novis B, Chen V. et al Value of the 14C‐D‐xylose breath test in patients with intestinal
bacterial overgrowth. Digestion 1985. 3286–91.91 [PubMed]
89. King C E, Toskes P P. Comparison of the 1‐gram[14C]xylose, 10‐gram lactulose‐H2, and 80‐gram
glucose‐H2 breath tests in patients with small intestine bacterial
overgrowth. Gastroenterology 1986.911447–1451.1451 [PubMed]
90. Donald I P, Kitchingmam G, Donald F. et al The diagnosis of small bowel bacterial overgrowth in
elderly patients. J Am Geriatr Soc 1992. 40692–696.696 [PubMed]
91. Husebye E, Skar V, Hoverstad T. et al Fasting hypochlorhydria with gram positive gastric flora is
highly prevalent in healthy old people. Gut 1992. 331331–1337.1337 [PMC free article] [PubMed]
92. Holt P R, Rosenberg I H, Russell R M. Causes and consequences of hypochlorhydria in the elderly. Dig
Dis Sci 1989. 34933–937.937 [PubMed]
93. Lipski P S, Kelly P J, James O F. Bacterial contamination of the small bowel in elderly people: is it
necessarily pathological? Age Ageing 1992. 215–12.12 [PubMed]
94. MacMahon M, Lynch M, Mullins E. et al Small intestinal bacterial overgrowth—an incidental
finding? J Am Geriatr Soc 1994. 42146–149.149 [PubMed]
95. Saltzman J R, Kowdley K V, Pedrosa M C. et al Bacterial overgrowth without clinical malabsorption in
elderly hypochlorhydric subjects. Gastroenterology 1994. 106615–623.623 [PubMed]
96. Lewis R, Gorbach S. Modification of bile acids by intestinal bacteria. Arch Intern Med 1972. 130545–
549.549 [PubMed]
97. Drasar B S, Shiner M, McLeod G M. Studies on the intestinal flora. I. The bacterial flora of the
gastrointestinal tract in healthy and achlorhydric persons. Gastroenterology 1969. 5671–
79.79 [PubMed]
98. Gorbach S L, Plaut A G, Nahas L. et al Studies of intestinal microflora. II. Microorganisms of the small
intestine and their relations to oral and fecal flora. Gastroenterology 1967. 53856–867.867 [PubMed]
99. Hamilton I, Worsley B W, Cobden I. et al Simultaneous culture of saliva and jejunal aspirate in the
investigation of small bowel bacterial overgrowth. Gut 1982. 23847–853.853 [PMC free
article] [PubMed]
100. Fromm H, Hofmann A F. Breath test for altered bile‐acid metabolism. Lancet 1971. 2621–
625.625[PubMed]
101. Sherr H P, Sasaki Y, Newman A. et al Detection of bacterial deconjugation of bile salts by a
convenient breath‐analysis technic. N Engl J Med 1971. 285656–661.661 [PubMed]
102. Toskes P P, King C E, Spivey J C. et al Xylose catabolism in the experimental rat blind loop syndrome:
studies, including use of a newly developed d‐[14C]xylose breath test. Gastroenterology 1978. 74691–
697.697 [PubMed]
103. King C E, Toskes P P, Spivey J C. et al Detection of small intestine bacterial overgrowth by means of
a 14C‐D‐xylose breath test. Gastroenterology 1979. 7775–82.82 [PubMed]
104. Stotzer P O, Kilander A F. Comparison of the 1‐gram (14)C‐D‐xylose breath test and the 50‐gram
hydrogen glucose breath test for diagnosis of small intestinal bacterial
overgrowth. Digestion 2000. 61165–171.171 [PubMed]
105. Bond J H, Jr, Levitt M D. Use of pulmonary hydrogen (H 2 ) measurements to quantitate
carbohydrate absorption. Study of partially gastrectomized patients. J Clin Invest 1972. 511219–
1225.1225[PMC free article] [PubMed]
106. Hirakawa M, Iida M, Kohrogi N. et al Hydrogen breath test assessment of orocecal transit time:
comparison with barium meal study. Am J Gastroenterol 1988. 831361–1363.1363 [PubMed]
107. Bond J H, Jr, Levitt M D, Prentiss R. Investigation of small bowel transit time in man utilizing
pulmonary hydrogen (H2) measurements. J Lab Clin Med 1975. 85546–555.555 [PubMed]
108. Riordan S M, McIver C J, Walker B M. et al The lactulose breath hydrogen test and small intestinal
bacterial overgrowth. Am J Gastroenterol 1996. 911795–1803.1803 [PubMed]
109. Sadik R, Abrahamsson H, Stotzer P O. Gender differences in gut transit shown with a newly
developed radiological procedure. Scand J Gastroenterol 2003. 3836–42.42 [PubMed]
110. Pimentel M, Soffer E E, Chow E J. et al Lower frequency of MMC is found in IBS subjects with
abnormal lactulose breath test, suggesting bacterial overgrowth. Dig Dis Sci 2002. 472639–
2643.2643[PubMed]
111. Pimentel M, Constantino T, Kong Y. et al A 14‐day elemental diet is highly effective in normalizing
the lactulose breath test. Dig Dis Sci 2004. 4973–77.77 [PubMed]
112. King T S, Elia M, Hunter J O. Abnormal colonic fermentation in irritable bowel
syndrome. Lancet1998. 3521187–1189.1189 [PubMed]
113. Dear K L, Elia M, Hunter J O. Do interventions which reduce colonic bacterial fermentation improve
symptoms of irritable bowel syndrome? Dig Dis Sci 2005. 50758–766.766 [PubMed]
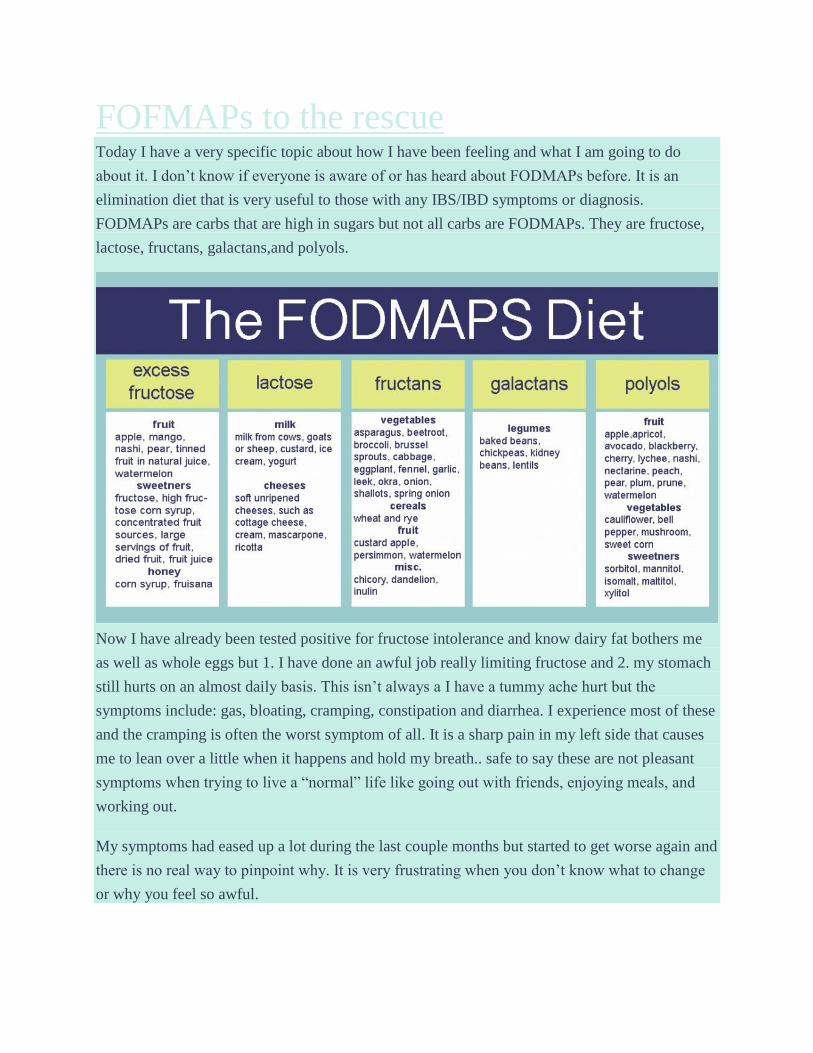
FOFMAPs to the rescue Today I have a very specific topic about how I have been feeling and what I am going to do
about it. I don’t know if everyone is aware of or has heard about FODMAPs before. It is an
elimination diet that is very useful to those with any IBS/IBD symptoms or diagnosis.
FODMAPs are carbs that are high in sugars but not all carbs are FODMAPs. They are fructose,
lactose, fructans, galactans,and polyols.
Now I have already been tested positive for fructose intolerance and know dairy fat bothers me
as well as whole eggs but 1. I have done an awful job really limiting fructose and 2. my stomach
still hurts on an almost daily basis. This isn’t always a I have a tummy ache hurt but the
symptoms include: gas, bloating, cramping, constipation and diarrhea. I experience most of these
and the cramping is often the worst symptom of all. It is a sharp pain in my left side that causes
me to lean over a little when it happens and hold my breath.. safe to say these are not pleasant
symptoms when trying to live a “normal” life like going out with friends, enjoying meals, and
working out.
My symptoms had eased up a lot during the last couple months but started to get worse again and
there is no real way to pinpoint why. It is very frustrating when you don’t know what to change
or why you feel so awful.

So now that I am home for two weeks I am going to fully commit to the FODMAPs ‘diet.’ This
is for my health and not weight reasons and I will say I am not googling my symptoms and
making these decisions based off half credible sources but that my GI doctor, the nutritionist I
saw, and the dietitian that did my fructose intolerance testing all have told me I really need to do
this in order to pinpoint irritants and help with my gut healing so I don’t have to deal with this
for the rest of my life. The reason I did not do it a year ago when I was first told about this was 1.
because I was intimidated by this disease I found out I had, a food intolerance, and no reason for
me getting it all and 2. because as a college student it is hard to cut out so many foods and still
get a variety of nutrients for collegiate training and 3. not wanting to waste my meal plan and
spend all my money on groceries.
I am going to do a 6 week elimination period starting today and then reintroduce foods one at a
time afterwards. I am really not a fan of cutting out whole food groups but I would much rather
figure this out for good and not feel so awful all the time. After looking at the do’s and don’ts I
do not think it will be as hard as I originally thought. I can still eat my blueberries, bananas,
some nuts, fish and egg whites, oatmeal, nut butter, gf flour, lettuce, yams, squash, quinoa, and
coffee! Plus some others, but no froyo but I will make sure to buy some lactose free ice cream at
the grocery store and probably save a lot of money not going so often.
It really helps to be home at the start of this to be able to have access to more foods and
hopefully get into the habit of not eating the other things. It also helps that i have limited those
items with fructose for the last year so it will not seem like too many more things off the list.
I look forward to hopefully feeling 100x better and being more comfortable going out in public
and being with people. I know this is the best decision for me after having multiple creditable
sources recommend it.
Here are some of the resources I am using to figure out what to eat and not eat and focus on what
I like that I can have!
http://stanfordhospital.org/digestivehealth/nutrition/DH-Low-FODMAP-Diet-Handout.pdf
http://www.ibsgroup.org/brochures/fodmap-intolerances.pdf

Related Documents











